
Abstract
Introduction
The American Academy of Pediatrics recognizes ADHD as the most common childhood neurobehavioral disorder (Subcommittee on Attention-Deficit/Hyperactivity Disorder et al., 2011). Moreover, the percentage of children aged 4 to 17 diagnosed with ADHD has risen dramatically in recent years, from 7.8% in 2003 to 9.5% in 2007 and finally to 11% in 2011 (Visser et al., 2014). Treatment plans for ADHD often involve medication (Subcommittee on Attention-Deficit/Hyperactivity Disorder et al., 2011), and thus, a corresponding increase in prescriptions has also been observed, with 6.1% of children taking some form of ADHD medication in 2011 compared with only 4.8% in 2007 (Visser et al., 2014). Concerns have been raised regarding the implications of a continued rise in ADHD and stimulant prescriptions, particularly with the recent release of the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-V; American Psychiatric Association, 2013), which broadened the criteria for ADHD diagnoses (Centers for Disease Control and Prevention, 2015). Increased availability of stimulant medication among adolescents creates more opportunity for the illegal diversion and unsafe misuse of these medications.
Using terminology as similarly defined by others (Wilens et al., 2008), “diversion” refers to the exchange (selling or giving away) of controlled medications, and “misuse” refers to the use of a controlled medication either in a way that was not prescribed or by a person who was not prescribed the medication by a licensed health care provider. Stimulant misuse and diversion in the adolescent population are problematic because of the associated health and legal consequences. The U.S. Drug Enforcement Administration classifies stimulants such as amphetamines and methylphenidate as Schedule II–controlled substances with a high potential for abuse and psychological or physical dependence (U.S. Department of Justice, n.d.). It is particularly dangerous when individuals who are not prescribed these medications misuse them, as their medical history may make them more susceptible to adverse cardiovascular and/or psychiatric side effects (Rabiner et al., 2009b; Shire, 2015). Aside from the health consequences of misuse, there are also serious legal consequences if a person diverts his or her stimulant medication, with punishments ranging from fines to incarceration (CriminalDefenseLawyer, n.d.). These legal consequences may have greater detrimental consequences than the immediate punishment, as studies show that arrest during adolescence is associated with an increased likelihood of dropping out of high school and decreased likelihood of enrolling in a 4-year college, both of which may lead to unemployment (Hjalmarsson, 2008; Kirk & Sampson, 2013).
Recent evidence suggests that stimulant misuse and diversion are prevalent in both the adolescent (Cottler, Striley, & Lasopa, 2013; McCabe, Teter, & Boyd, 2004; McCabe & West, 2013; McCauley et al., 2010; Poulin, 2001, 2007; Viana et al., 2012; Wilens et al., 2008) and college-aged populations (DeSantis, Webb, & Noar, 2008; Garnier-Dykstra, Caldeira, Vincent, O’Grady, & Arria, 2012; K. M. Hall, Irwin, Bowman, Frankenberger, & Jewett, 2005; Low & Gendaszek, 2002; McCabe & Boyd, 2005; Rabiner, 2013; Rabiner et al., 2009a; Singh, Bard, & Jackson, 2014; Teter, McCabe, LaGrange, Cranford, & Boyd, 2006; White, Becker-Blease, & Grace-Bishop, 2006; Wilens et al., 2008). One specific study examining non-medical use of stimulants among adolescents found that 2.0%, 8.2%, 9.0%, and 14.1% of students in grades 7, 9, 10, and 12, respectively, reported misusing amphetamines, and 2.2%, 7.6%, 7.4%, and 7.3% in the same corresponding grades reported non-medical use of methylphenidate (Poulin, 2007). Reports also suggest that many non-ADHD students who misuse stimulants obtain them from peers with ADHD who divert their medication (Garnier-Dykstra et al., 2012; McCabe & Boyd, 2005; McCabe et al., 2004; McCabe et al., 2011; Poulin, 2001, 2007; Rabiner, 2013; Wilens et al., 2008). In one study, approximately 26% of adolescents who were prescribed methylphenidate reported diverting their medication in the past month (Poulin, 2007). In addition, there has been speculation that some young adults are feigning ADHD symptoms to obtain stimulants—in essence, attempting to receive prescriptions for stimulants directly from physicians for misuse (Rabiner, 2013). It has also been suggested that physicians may increasingly encounter patients explicitly seeking medication for cognitive neuroenhancement (Larriviere, Williams, Rizzo, & Bonnie, 2009).
To prevent the illegal diversion and potentially unsafe misuse of prescription stimulants, it is important to further evaluate this issue from a physician’s perspective. Although the literature provides evidence that stimulant misuse and diversion among adolescents are issues of concern, there is a lack of studies that evaluate physician perceptions of these issues. To date, only three studies have evaluated physician concerns regarding prescription stimulant misuse and/or diversion. Stockl, Hughes, Jarrar, Secnik, and Perwien (2002) found that 19% of physicians were concerned about diversion when prescribing a controlled medication for ADHD. However, other than “concern,” this study did not ask any further questions regarding diversion of these medications. In addition, this study was geographically restricted to four states and was published more than 10 years ago. The second study, published in 2003, investigated family practitioner concerns when prescribing stimulants (Hellerstein & Biedermann, 2003). Physicians rated “abuse potential” as their highest concern when prescribing methylphenidate (tied with “adverse effects”), with a mean score of 3.3 out of 5 (where 1 denoted “never a concern” and 5 denoted “always a concern”), but there were no further questions about stimulant misuse. Finally, a 2004 survey found that only 25.3% of physicians were very confident in their ability to recognize when a person was attempting to obtain controlled medications for abuse and/or diversion; however, this unpublished study was focused neither on ADHD as a disorder nor on pediatric providers (The National Center on Addiction and Substance Abuse at Columbia University, 2005).
This study assesses physician perceptions of the pervasiveness of ADHD stimulant diversion and misuse among their own adolescent patients and in general. Furthermore, this study focuses on a national sample of the three pediatric subspecialists with the greatest clinical focus on ADHD: child and adolescent psychiatrists (CAP), child neurologists (CN), and developmental–behavioral pediatricians (DBP). A better understanding of the perceptions of pediatric subspecialists regarding stimulant diversion and misuse will provide an important addition to the current literature on the potential pervasiveness of stimulant diversion and misuse, as recent studies mostly focus on prevalence estimates through self-report by adolescents. In addition, this study will help to elucidate physician awareness of an important issue pertaining to adolescents with ADHD.
Method
Study Design
A questionnaire focused on stimulant diversion and misuse by high-school students was developed and mailed to three groups of pediatric subspecialists in the United States: CAP, CN, and DBP. In addition to the questionnaire and a cover letter explaining implied consent and the voluntary nature of the study, the mailing included several participation incentives: a laminated ADHD Medication Guide and the opportunity to request educational materials on stimulant misuse and diversion, a Teen Fact Sheet to share with their patients with ADHD, and up to three additional copies of the ADHD Medication Guide.
The questionnaires were mailed in August 2013, and responses were received between August 2013 and May 2014. Mailing labels for CAP and CN were obtained from the American Medical Association. Questionnaires were sent to 3,021 CAP who were identified using the selection criteria “Primary Specialty: Child Psychiatry” and “Board Certification: Child & Adolescent Psychiatry,” and 907 CN who were identified using the selection criteria of “Primary Specialty: Child Neurology” and “Board Certification: Neurology With Special Qualifications in Child Neurology.” Mailing labels for DBP were obtained from the Society for Developmental and Behavioral Pediatricians, and questionnaires were sent to 579 DBP who were members of this society. In total, questionnaires were sent to 4,507 physicians. The study received approval from the North Shore-Long Island Jewish Institutional Review Board.
Measures
In addition to soliciting information regarding physician demographics, the four-page questionnaire assessed physician perceptions of the pervasiveness of stimulant diversion and misuse, knowledge and training regarding these issues, and clinical practices to prevent stimulant diversion.
Data Analysis
Distributional assumptions of all variables were checked using histograms, q-q plots, and Shapiro–Wilks tests before conducting statistical analyses. Differences in sample characteristics between groups were examined using chi-square analysis for categorical variables. Bivariable and multivariable (log-binomial) regression analyses (risk ratios [RR]) were carried out to identify differences between subspecialists regarding perceptions of stimulant diversion in their patients with ADHD and in general, perceptions of patients exaggerating and feigning ADHD symptoms, and perceived motivations of patients who were suspected of feigning ADHD symptoms, with adjusted risk ratios (aRR) reflecting adjustment for the following three confounders identified a priori: physician gender, physician stimulant prescribing volume, and recency of subspecialty training (except when these were effect measure modifiers) (McNutt, Wu, Xue, & Hafner, 2003). Effect measure modification was examined using interaction terms in regression models, and stratified effect estimates were reported for variables found to be effect measure modifiers (p < .2; Rothman & Greenland, 1998). Bivariable and multivariable (log-binomial) regression models were also used to examine the association between physician perceptions of how frequently their own patients divert their stimulant medication and how common they believed this practice to be in general. Regression models involving physician perceptions of their own patients used a threshold of suspecting at least one patient of improper behavior with regard to their stimulants in the past year. All analyses were performed using SAS (version 9.3) statistical software.
Results
In total, 894 health care professionals completed questionnaires, but only responses from pediatric subspecialists who currently prescribe stimulant medications and whose subspecialty was clearly identifiable were included in the analysis. The final sample consisted of 826 physicians: 579 CAP, 106 CN, and 141 DBP, with an overall response rate of 18%. Physicians in 49 states were represented in the sample, with a mean medical school graduation date of 1991 (SD = 10; range = 1957-2012). By subspecialty, CAP had a mean graduation date of 1992 (SD = 8; range = 1974-2012); CN, 1987 (SD = 12; range = 1959-2007); and DBP, 1986 (SD = 12; range = 1957-2010). Table 1 includes additional sample demographics.
Demographics of Physician Sample.
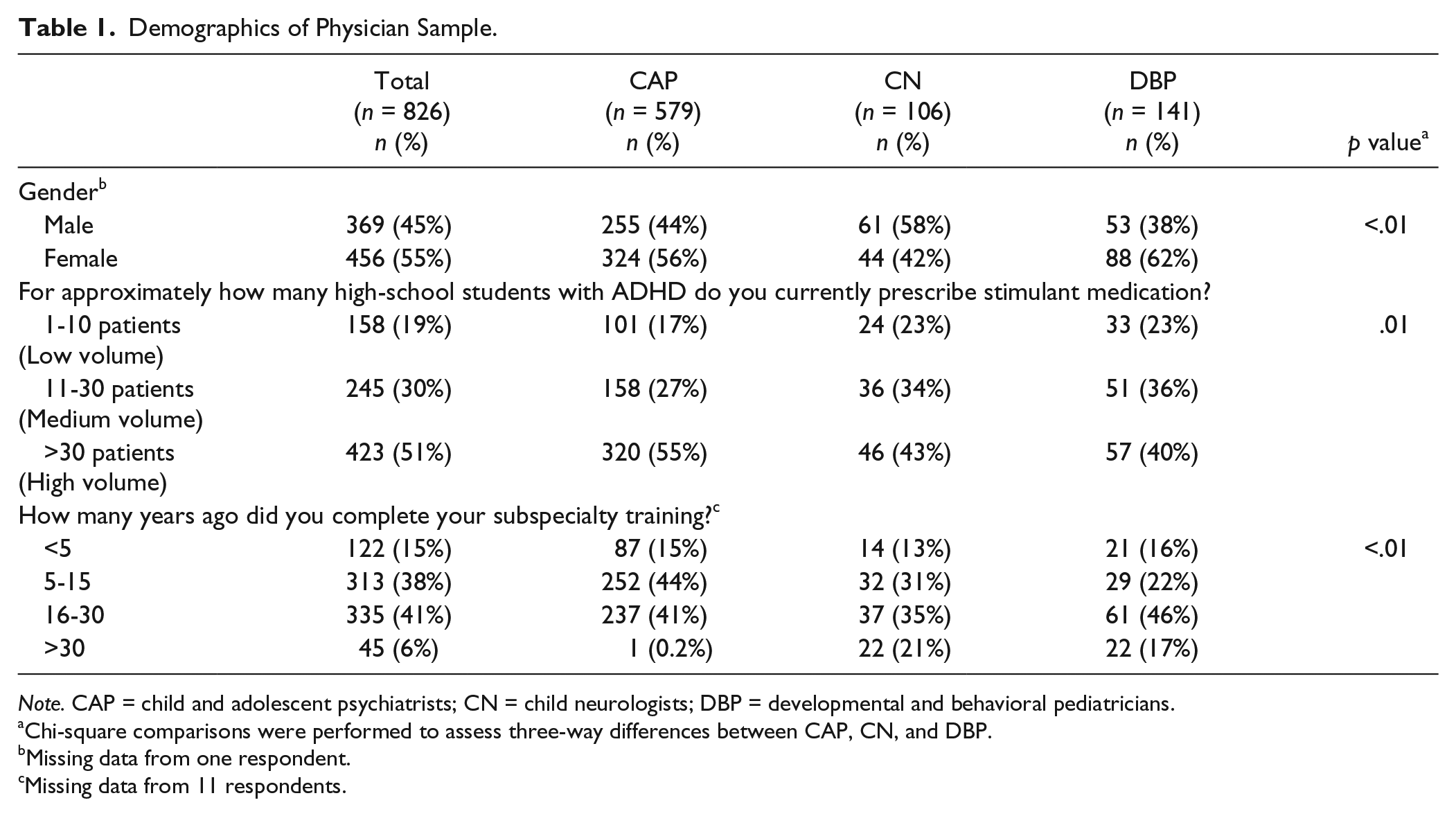
Note. CAP = child and adolescent psychiatrists; CN = child neurologists; DBP = developmental and behavioral pediatricians.
Chi-square comparisons were performed to assess three-way differences between CAP, CN, and DBP.
Missing data from one respondent.
Missing data from 11 respondents.
Physician Perceptions of Diversion and Exaggerated Symptoms by ADHD Patients
In the past 12 months, 59% of all physicians suspected at least one of their high-school patients with ADHD diverted stimulant medication to others and 10% of all physicians suspected five or more patients had diverted their medication. Perceptions differed by subspecialty (Table 2). Compared with other subspecialists, CAP were most likely to suspect diversion; 69% suspected one or more patients of selling or giving away their stimulant medication. Only 42% of CN suspected diversion by at least one patient and were much less likely to suspect diversion compared with CAP, even when controlling for gender, prescribing volume, and recency of subspecialty training (aRR = 0.68; 95% confidence interval [CI] = [0.54, 086]). DBP were also less likely to suspect diversion compared to CAP, and gender was found to be a significant effect measure modifier; more male DBP suspected diversion than female DBP, even when controlling for prescribing volume and recency of subspecialty training.
Physician Perceptions of Stimulant Diversion and Misuse Among Their Own Patients.
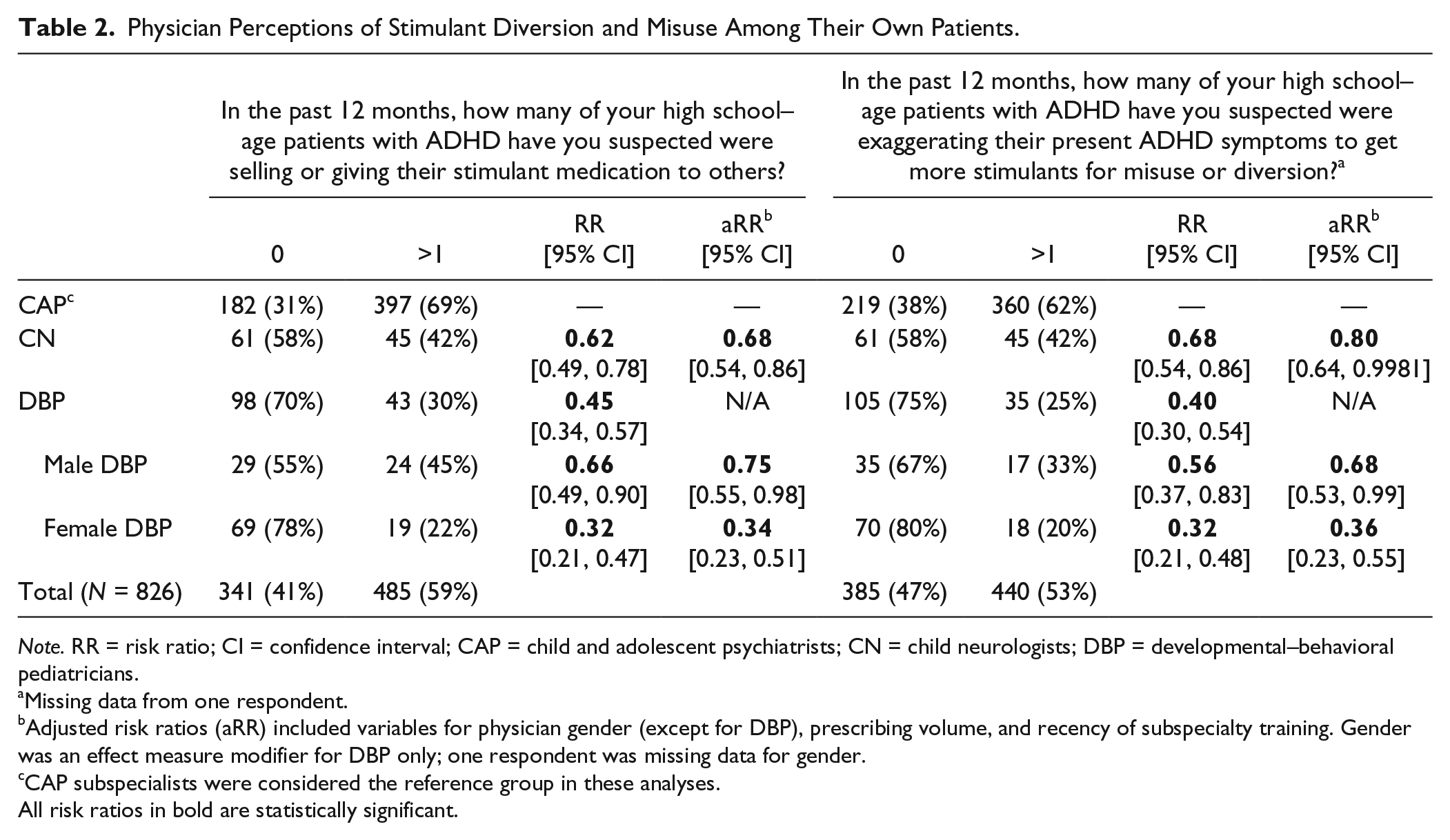
Note. RR = risk ratio; CI = confidence interval; CAP = child and adolescent psychiatrists; CN = child neurologists; DBP = developmental–behavioral pediatricians.
Missing data from one respondent.
Adjusted risk ratios (aRR) included variables for physician gender (except for DBP), prescribing volume, and recency of subspecialty training. Gender was an effect measure modifier for DBP only; one respondent was missing data for gender.
CAP subspecialists were considered the reference group in these analyses.
All risk ratios in bold are statistically significant.
Overall, 53% of all pediatric subspecialists suspected one or more patients with ADHD exaggerated symptoms in the past year to obtain more stimulants for misuse or diversion, and 12% of physicians suspected five or more patients had exaggerated their symptoms for this purpose. As shown in Table 2, 62% of CAP suspected at least one patient of exaggerating symptoms and were again most likely to suspect this behavior compared with other subspecialists. CN were 20% less likely to suspect patients of exaggerating symptoms compared with CAP when controlling for the three confounders. DBP, in general, were also less likely to suspect improper behavior of patients, and again, gender was found to be a significant effect measure modifier: 33% of male DBP suspected patients of exaggerating symptoms, compared with only 20% of female DBP.
Prescribing volume was found to be an effect measure modifier when evaluating subspecialty differences in perceptions, but only with regard to perceptions of patients diverting stimulants (Table 3). Differences among subspecialists were most pronounced among “low-volume” prescribers (currently prescribe stimulants to 1-10 patients); compared with CAP, CN were 94% less likely and DBP were 98% less likely to suspect patients of diverting their stimulants when controlling for gender and recency of subspecialty, although the number of physicians in some categories was small. Among “medium-volume” (currently prescribe stimulants to 11-30 patients) and “high-volume” (currently prescribe stimulants to >30 patients) prescribers, DBP were again less likely to suspect stimulant diversion compared with CAP, albeit to a lesser extent than among “low-volume” prescribers. CN perceptions, in contrast, were not significantly different from CAP perceptions when controlling for gender and recency of subspecialty training.
Physician Perceptions of Stimulant Diversion With Prescribing Volume as an Effect Measure Modifier.
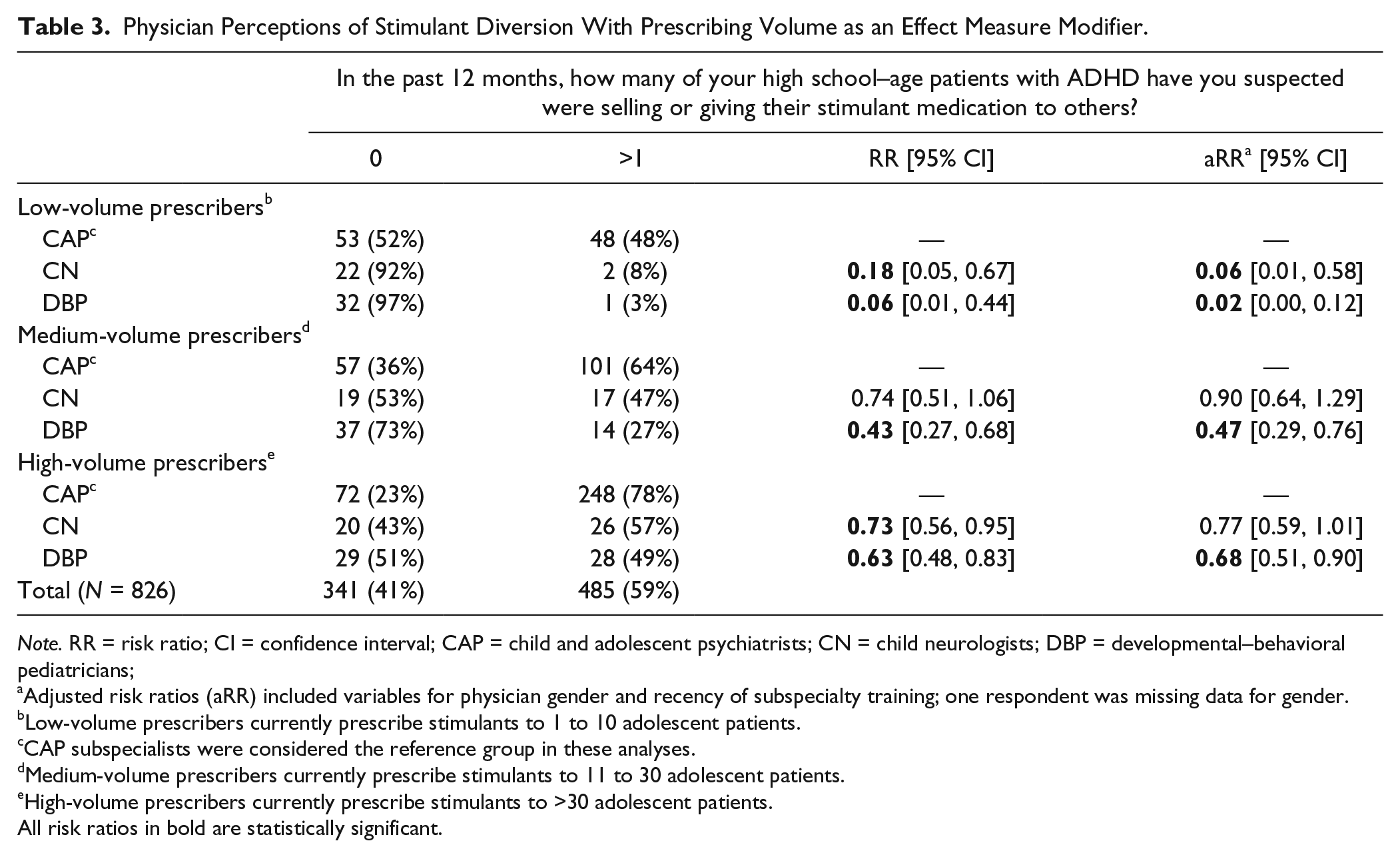
Note. RR = risk ratio; CI = confidence interval; CAP = child and adolescent psychiatrists; CN = child neurologists; DBP = developmental–behavioral pediatricians;
Adjusted risk ratios (aRR) included variables for physician gender and recency of subspecialty training; one respondent was missing data for gender.
Low-volume prescribers currently prescribe stimulants to 1 to 10 adolescent patients.
CAP subspecialists were considered the reference group in these analyses.
Medium-volume prescribers currently prescribe stimulants to 11 to 30 adolescent patients.
High-volume prescribers currently prescribe stimulants to >30 adolescent patients.
All risk ratios in bold are statistically significant.
Notably, 35% of physicians who currently treat 11 or more high-school patients with stimulants did not suspect diversion among any of their patients in the past year (46%: medium-volume prescribers; 29%: high-volume prescribers). Furthermore, among physicians who currently prescribe stimulants to more than 30 patients, 85% of physicians did not suspect diversion by five or more patients with ADHD in the past year. In addition, 42% of physicians who treat 11 or more patients with stimulants did not suspect even one patient of exaggerating symptoms to obtain more stimulants for misuse and/or diversion (55%: medium-volume prescribers; 34%: high-volume prescribers). Among physicians who currently prescribe stimulants to more than 30 patients, 82% did not suspect five or more patients of exaggerating symptoms to obtain more stimulants.
Physician Perceptions of Patients Feigning ADHD Symptoms
In the past 12 months, 74% of physicians suspected that one or more high-school students who presented in the past year for an initial diagnosis of ADHD had feigned symptoms to obtain stimulants, and 28% suspected four or more patients had done so. Table 4 shows further subspecialist differences in perceptions. Although 82% of CAP believed one or more patients feigned ADHD symptoms, CN were less likely to have this perception compared with CAP when controlling for gender, prescribing volume, and recency of subspecialty training (aRR = 0.76; 95% CI = [0.64, 0.90]). DBP were also less likely to suspect at least one patient of feigning ADHD symptoms, and gender played a significant role in DBP perceptions. Whereas male DBP were 27% less likely to suspect a patient of feigning ADHD symptoms compared with CAP when controlling for potential confounders, female DBP were 47% less likely to have this perception.
Physician Perceptions of Patients Feigning ADHD Symptoms to Obtain Stimulants for Non-Medical Purposes.
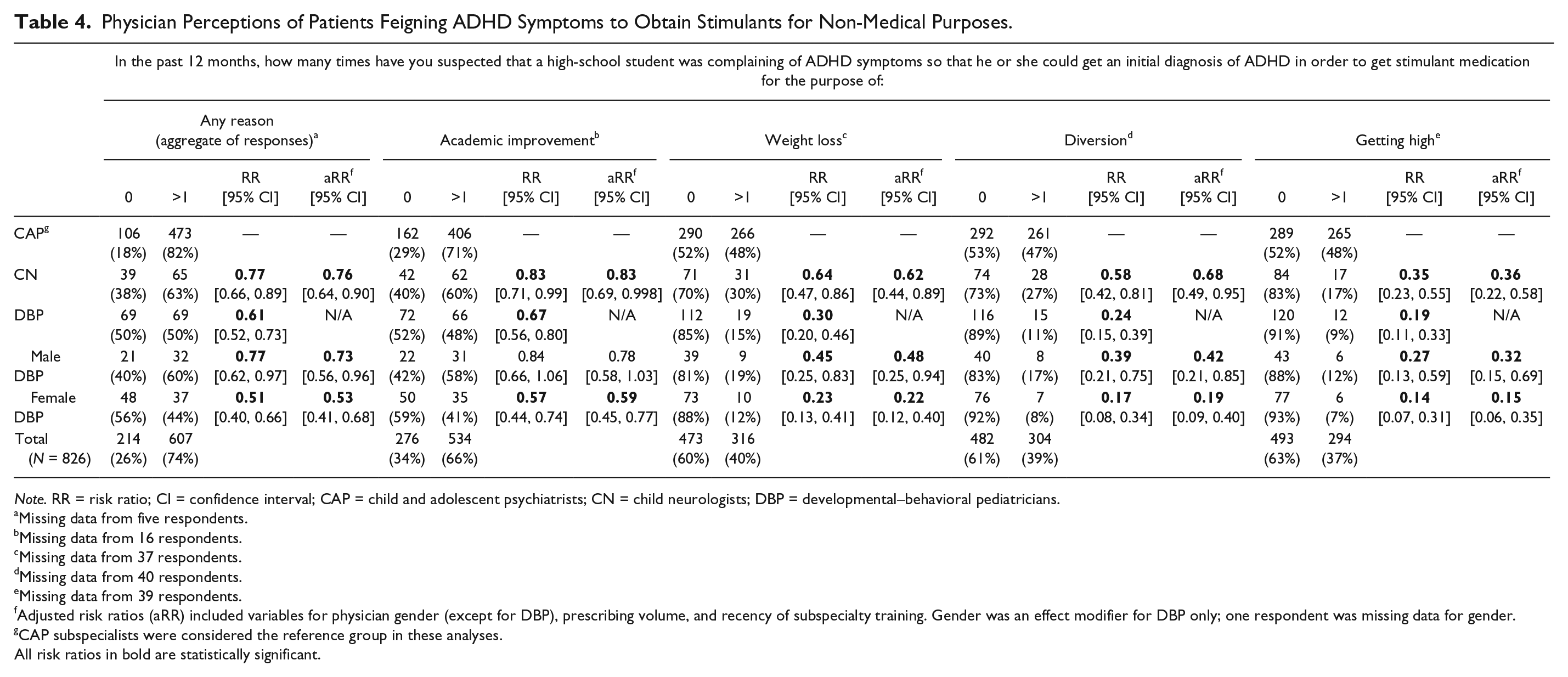
Note. RR = risk ratio; CI = confidence interval; CAP = child and adolescent psychiatrists; CN = child neurologists; DBP = developmental–behavioral pediatricians.
Missing data from five respondents.
Missing data from 16 respondents.
Missing data from 37 respondents.
Missing data from 40 respondents.
Missing data from 39 respondents.
Adjusted risk ratios (aRR) included variables for physician gender (except for DBP), prescribing volume, and recency of subspecialty training. Gender was an effect modifier for DBP only; one respondent was missing data for gender.
CAP subspecialists were considered the reference group in these analyses.
All risk ratios in bold are statistically significant.
With regard to the specific presumed motivations of patients who were suspected to be feigning ADHD symptoms, 66% of physicians believed at least one patient sought stimulants to improve their academic performance, 40% to lose weight, 39% to divert stimulant medication to others, and 37% to get high. CAP were most likely to suspect at least one patient of feigning symptoms for each reason, compared with both CN and DBP. However, gender was again found to modify associations between subspecialty and perceptions. Effect estimates for female DBP were consistently below and farther from the null than male DBP.
It should be noted that 22% of physicians who currently prescribe stimulants to 11 or more patients did not suspect any patients of feigning ADHD symptoms (28%: medium-volume prescribers; 19%: high-volume prescribers). Furthermore, among physicians who currently prescribe stimulants to more than 30 patients, 48% did not suspect four or more patients had feigned symptoms in the past year.
Physician Perceptions of Stimulant Diversion in General
Overall, 39% of physicians believed it was “common” or “very common” for high-school students with ADHD to divert stimulant medication to peers. By subspecialty, 41% of CAP, 27% of CN, and 40% of DBP thought stimulant diversion was “common” or “very common.” CN were 36% less likely to have this perception compared with CAP when controlling for potential confounding factors including physician gender, prescribing volume, and recency of subspecialty training (aRR = 0.64; 95% CI = [0.44, 0.93]). Gender was found to be an effect modifier for DBP; 43% of male DBP and 39% of female DBP believed stimulant diversion was at least “common.” Male DBP and female DBP were each as likely to perceive stimulant diversion as common as CAP when controlling for confounding variables including prescribing volume and recency of subspecialty training (male DBP: aRR = 1.43; 95% CI = [0.94, 2.15] and female DBP: aRR = 0.79; 95% CI = [0.58, 1.09]). Physician responses of “not sure” (n = 33) were excluded from this analysis.
Physicians who did not suspect any of their patients of diverting their stimulant medication were more likely to believe this practice was not “common” or “very common” in general (RR = 1.37; 95% CI = [1.13, 1.65]). Prescribing volume was not a significant confounder in this analysis.
Discussion
This is the first study to provide evidence that many pediatric subspecialists suspect stimulant diversion and misuse in their high-school patients with ADHD. More than half of physicians in this study suspected one or more of their own patients with ADHD sold or gave away their stimulants, and that one or more of their patients exaggerated symptoms to obtain more stimulants for misuse or diversion. Although we cannot make any conclusions regarding the accuracy of physician suspicions, these findings suggesting the potential pervasiveness of stimulant diversion are supported by previous research showing that a significant number of adolescents with ADHD divert their medication. One study in particular found that more than a quarter of middle- and high-school students had diverted their prescribed stimulant medication (Poulin, 2007).
Almost three fourths of physicians in this study believed one or more of their patients in the past 12 months feigned symptoms to obtain an initial ADHD diagnosis to receive stimulants for non-medical use. These perceptions reflect a growing concern regarding students feigning ADHD symptoms (Rabiner, 2013). One recent study similarly found that almost 50% of students at one college who self-referred for an ADHD evaluation were suspected of exaggerating symptoms and/or dishonestly completing a neurological assessment in an effort to receive stimulant medication (Sullivan, May, & Galbally, 2007). Another study reported that almost 20% of individuals without ADHD who misused stimulants in the past year had obtained fraudulent prescriptions from physicians (Novak, Kroutil, Williams, & Van Brunt, 2007). This current study—focused on perceptions of pediatric subspecialists—provides additional evidence that young people may be trying to obtain stimulants for illicit purposes through legal means (i.e., from health care providers).
Most physicians in our sample suspected students of trying to obtain stimulant medication specifically to improve their academic performance. This finding is consistent with previously published investigations reporting that studying and improved concentration are the most common reasons for which students misuse stimulants (DeSantis et al., 2008; Garnier-Dykstra et al., 2012; Teter et al., 2006). DeSantis et al. (2008) found that 72% of students who reported illicitly using ADHD stimulants were doing so to stay awake to study longer, and 66% were doing so to concentrate on work. To a lesser extent, physicians in our study believed students were seeking stimulants for diversion, getting high, and weight loss. These perceptions are also supported by the DeSantis et al. study, in which a minority of students cited their motivation for stimulant misuse as “for the high (the good feeling)” (7%) or to suppress appetite (5%) (DeSantis et al., 2008).
Although physicians seem mindful of the different reasons for which patients might feign ADHD symptoms to obtain stimulants, it is important to note that we cannot validate the accuracy of physician suspicions through this study design. Furthermore, although many physicians in our sample suspected one or more patients of feigning symptoms to obtain a false diagnosis of ADHD, one recent study emphasized that most students who misuse stimulants obtained them from peers with ADHD, not from physicians as treatment for feigned symptoms (Arria & DuPont, 2010). Physicians who evaluate adolescents for a new diagnosis of ADHD are in a difficult position. On one hand, they must be vigilant to the possibility that a patient may be feigning ADHD symptoms to obtain stimulants; on the other hand, they must also recognize that some students with significant inattention may not present for clinical evaluation and treatment until adolescence.
Although most physicians in our sample suspected at least one patient of diverting stimulants or feigning ADHD symptoms in the past year, it is noteworthy that a sizable number of physicians did not suspect any of their patients of improper behavior with regard to their stimulants. Furthermore, the vast majority of physicians in our sample did not suspect five or more patients of diverting their stimulants. Although we cannot confirm the accuracy of physician suspicions, these results suggest a potential lack of awareness by physicians regarding stimulant misuse and/or diversion. This seeming lack of awareness is especially apparent among physicians who prescribe stimulants to many patients; a third of physicians who currently prescribe stimulants to more than 30 high-school patients with ADHD did not suspect even one of their patients had diverted their medication in the past year, and 85% of these high-volume prescribers did not suspect five or more patients had diverted stimulants.
In addition, almost 60% of physicians in our sample did not perceive stimulant diversion to be common or very common overall. An association was noted in this study between physician perceptions of stimulant diversion among their own patients and physician perceptions of diversion in general, although it is unclear which perception influenced the other because neither causality nor directionality can be inferred. Although the word “common” is imprecise and may be interpreted differently by individual respondents, this finding nevertheless also suggests a lack of physician awareness of these issues given the documented prevalence of stimulant diversion and misuse in the adolescent population (Poulin, 2007; Wilens et al., 2008). As noted in previous research, there is a need for heightened physician awareness of misuse and diversion of prescription stimulants (Arria & DuPont, 2010), potentially through increased medical education on these issues.
Another major study finding is that subspecialists differed in their perceptions of the pervasiveness of stimulant diversion and misuse. CAP were most likely to suspect their own patients of diverting stimulants or exaggerating symptoms, as well as feigning symptoms to obtain an initial ADHD diagnosis, while CN and DBP were less suspicious of their patients. However, when asked about the general prevalence of stimulant diversion, a similar percentage of CAP and DBP believed this to be common or very common among adolescents; CN were less likely to identify with this view.
Confounding factors may help to explain differences in perceptions of subspecialists. Physician prescribing volume was found to be a significant covariate, but only with regard to patients selling or giving their stimulants to others. Observed differences by subspecialty were magnified among low-volume prescribers and narrowed among high-volume prescribers. Low-volume prescribers may suspect diversion less often because they have a smaller sample of patients and/or less experience treating ADHD.
In addition, gender consistently modified DBP perceptions; male DBP were more likely to suspect their own patients of improper behavior involving stimulants. Research shows that patients tend to communicate more positive statements to female physicians (J. A. Hall & Roter, 2002), and patients may be less willing to disclose stimulant diversion and misuse to female physicians in an effort to maintain positive rapport. However, it remains unclear why this significant gender difference was only observed among DBP in this study.
Prescribing volume, gender, and recency of subspecialty training—although important covariates to consider—do not fully explain subspecialist differences. Differences in patient populations may also contribute to these differences in subspecialist perceptions. For instance, CAP may suspect stimulant diversion or misuse more frequently among their patients because they are more likely to treat adolescents with conduct disorder and substance use disorder. Research suggests that these patients are more likely to misuse and divert stimulants; Wilens, Gignac, Swezey, Monuteaux, and Biederman (2006) found that every ADHD participant who reported diverting prescription stimulants had comorbid conduct disorder and/or substance use disorder, and 83% of ADHD participants who reported misusing their medication met criteria for at least one of these two comorbid disorders.
It is important to consider ways in which physicians can work to prevent these illegal and potentially dangerous activities. As suggested in several studies, physicians are in a unique position as prescribers of stimulant medication to prevent stimulant misuse and diversion (Arria & DuPont, 2010; Garnier et al., 2010). First, physicians can better educate themselves about the consequences of stimulant misuse and/or diversion and the clinical signs that a patient might be engaging in these activities. It is encouraging that many physicians in our sample requested the educational materials about stimulant misuse that were offered as an incentive for participation in this study. Hopefully, these educational materials will not only enable physicians to better inform their patients with ADHD regarding stimulant misuse and diversion, but also prompt an ongoing dialogue regarding these issues during the course of their treatment.
Physicians can also adopt specific prevention practices: using medication contracts (i.e., written agreements that commit the patient to adhering to a specified treatment plan and medication regimen), employing pill counts (i.e., counting the number of pills that patients have taken at the end of the month to measure adherence), distributing print materials about stimulant misuse and diversion, and prescribing long-acting stimulants or non-stimulants instead of immediate-release stimulants, as immediate-release stimulants have a higher potential for abuse (Levin, Evans, & Kleber, 1999; The National Center on Addiction and Substance Abuse at Columbia University, 2005). Furthermore, if physicians suspect stimulant misuse among particular patients, they should consider referring these patients for counseling and/or substance abuse treatment.
However, although physicians should be encouraged to implement practices designed to prevent and address stimulant misuse and diversion, they should also be cognizant of potential biases toward certain populations (e.g., a belief that patients with a substance use history may be misusing stimulants) and should be aware that their suspicions may ultimately be false. It is difficult to make general recommendations as to how physicians should treat patients with ADHD who they also suspect of misusing and/or diverting stimulants. Physicians must use their best clinical judgment to provide each of their patients with a treatment plan that is best suited for their individual needs, while taking into consideration concerns regarding stimulant misuse and diversion.
Although these findings have clinical relevance and important implications, several methodological weaknesses and limitations must be noted that limit our ability to make generalizations on this topic. First, although our sample was diverse in terms of age, gender, and patient volume, we cannot rule out sampling bias. For example, it is possible that responders varied from non-responders with respect to demographics or perceptions regarding misuse and/or diversion; this could not be evaluated with available data. In addition, our overall response rate was somewhat low, although surveys of physicians tend to have lower response rates (VanGeest, Johnson, & Welch, 2007) and the response rate in this study is similar to that noted in other recent studies (Bonevski, Magin, Horton, Foster, & Girgis, 2011). Because our data were based on physician self-report, estimates of the pervasiveness of diversion and/or misuse among their own patients may be subject to cognitive bias (i.e., a halo effect). Furthermore, there are many factors that might contribute to physician awareness of stimulant misuse and diversion, including previous training on these issues, extent of clinical experience, practice setting, previous exposure to these issues through colleagues or media reports, and prescribing volume. It is particularly important to note that almost half of physicians in our sample currently prescribe stimulants to fewer than 30 adolescent patients, which might have a significant impact on awareness. Our study design also precludes us from confirming or rejecting the accuracy of physician perceptions in this study. Also, physician perceptions of misuse and/or diversion might vary depending on the specific medication formulation (e.g., Adderall, Vyvanse, Concerta, etc.), but this study only inquired about stimulant medications in general. Last, because this study focused on pediatric subspecialists, our results may not be generalizable to primary care pediatricians.
Findings from this study suggest several different follow-up studies. First, research is needed to determine whether physician concerns about stimulant diversion influence their clinical management of adolescents with ADHD (e.g., patient education, prescribing practices). Second, investigators should explore whether physician concerns about patients feigning ADHD symptoms to get stimulants adversely influence clinical care. For example, whereas clinician skepticism may reduce over-diagnosis of ADHD, these suspicions may also pose obstacles to the accurate diagnosis and treatment of youth who have ADHD but do not present until adolescence. Research should also be done to examine the impact of various factors on physician perceptions of stimulant misuse and diversion. For example, to what extent do formal training, past clinical experience, and prescribing volume influence the accuracy of physician perceptions? Finally, because this study focused on pediatric subspecialists, a large-scale study assessing general pediatricians’ awareness of this issue is warranted.
The findings of this study—the first to evaluate the pervasiveness of stimulant misuse and diversion from a physician’s perspective—are concerning in several respects. First, the fact that a majority of physicians in our sample do indeed suspect illegal and potentially unsafe behavior by their patients with ADHD adds to mounting evidence suggesting that non-medical use of stimulant medication is a societal issue of escalating importance. Conversely, the finding that a sizable number of pediatric subspecialists do not suspect stimulant diversion or misuse among any of their adolescent patients and do not believe diversion to be common provides evidence that too many physicians are unaware of this issue. This lack of awareness must be remedied through increased training and continuing education efforts, as it is imperative that physicians be mindful of these issues when treating youth with ADHD. Moreover, given the health and legal consequences associated with stimulant misuse and diversion, physicians must take greater responsibility in the prevention of stimulant diversion and misuse by adolescents.
Footnotes
Acknowledgements
The authors wish to thank Majnu John, PhD, and Sujit Vettam, MS, for their assistance with the preliminary data analysis.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.