
Abstract
Background:
Individuals with mental health conditions experience significant health disparities, including elevated rates of chronic illnesses and reduced life expectancy. These disparities are often exacerbated by healthcare providers’ challenges in addressing physical health needs when mental health symptoms are present.
Methods:
Professional development staff from a large home health organization spanning 2 states and 6 counties in the greater Philadelphia, Pennsylvania area created a training to enhance clinicians’ ability to care for individuals with mental health conditions. To accommodate diverse learning styles and geographic distribution, the training was delivered in a virtual, synchronous format, ensuring accessibility and real-time engagement across the organization. The program was grounded in Universal Design for Learning principles and employed multimodal instructional strategies to support varied learner needs. Training content focused on understanding mental health diagnoses, recognizing symptoms, applying trauma-informed care, and effective communication techniques.
Results:
A total of 974 clinicians completed the program, reporting increased confidence and competence in managing mental health conditions in the home setting. Participants noted a deeper understanding of mental health issues and felt better equipped to provide holistic care.
Conclusions:
These results suggest that targeted education can better prepare clinicians to integrate mental and physical health care in the home setting. Such approaches may represent an important strategy for reducing health disparities and promoting more holistic, person-centered care for individuals with mental health conditions.
Keywords
Introduction
Almost 5 million adults receive home health services each year in the United States. 1 Mental health conditions involve significant disturbances in thinking, emotional regulation, or behavior. 2 Approximately 1 in 5 adults in the United States experience a mental health concern each year, with 1 in 25 experiencing a serious mental illness during their lifetime. 3
For patients receiving care in their home, mental health concerns are prevalent. Almost half of all hospice patients report moderate to severe anxiety or depression in the last week of life, and these symptoms are associated with increased caregiver burden. 4 In a random sample of Medicare beneficiaries receiving home health care, 40% reported mental health disorders. 5 The most common mental health disorders seen in the home health setting are depression and anxiety, although substance abuse, psychotic disorders, and behavioral disturbances are also frequently observed. 5 Only about a third of people identified as having a mental health disorder receive mental health treatment during their home health episode. 5 Despite the prevalence of mental health disorders in home health care, home health clinicians often lack training in managing these conditions.
Lack of clinician confidence working with people with mental health conditions leads to health disparities. People living with mental health conditions experience health disparities, including higher rates of chronic health conditions and reduced life expectancy. The life expectancy of people with mental health conditions is reduced by preventable health conditions by an estimated 10 to 20 years. 2 For example, people with serious mental illness are 2 times as likely to have diabetes and 37% more likely to develop cardiovascular disease. 6 According to the Office of Disease Prevention and Health Promotion, one of the objectives of Healthy People 2030 aims to improve health and quality of life for people affected by mental health conditions and to eliminate health disparities. 7
Clinicians face unique challenges in the home health setting. They do not have the support of a team while working in often unpredictable situations. They must quickly assess the situation, including the patient’s behavior and environment. Patients with a history of mental illness or substance use disorder are more likely to threaten violence against a home health worker. 8 The CDC estimates that up to 65% of home health workers have experienced a verbal assault, while up to 44% have experienced a physical assault. 9 It is important for home health clinicians to develop the skills needed to interact with and treat people with mental health conditions to maximize clinician safety while meeting client healthcare needs.
Recognizing the need for clinicians to feel confident providing medical care in the home to people with mental health conditions, an educational program was developed to increase clinician competence in working with this population. This paper presents the results of a quality improvement project designed to evaluate the impact of a targeted education on mental health conditions for staff in a home health agency.
Methods
Project Development
This project took place in a home health agency in the greater Philadelphia area that employs 1152 clinicians. The agency is affiliated with an academic medical center. The agency offers 4 service lines: home health, hospice, palliative care, and home infusion services. The authors are members of the agency’s professional development team.
A learning needs assessment revealed that home health clinicians wanted more education on how to work with patients who had mental health conditions. Based on this staff feedback, mental health conditions were selected as the topic for the agency-wide annual competency for all clinical staff. Prior to developing the instructional content, the authors completed a literature review on mental health educational programs in the home health setting.
The educators who developed the course consisted of 2 nurse educators and an occupational therapist. An interprofessional advisory committee was developed to provide oversight of the project. The committee included a physical therapist, a nurse educator, a social worker, and a speech therapist.
Learning outcomes for the program were as follows:
Discuss the prevalence of mental health disorders in the home care population.
Understand common mental health diagnoses.
Identify mental health symptoms.
Discuss a trauma-informed approach to care.
Demonstrate effective communication strategies.
Identify action steps when mental health concerns are identified .
Identify non-pharmacological strategies to address mental health symptoms.
Discuss pharmacological management of mental health conditions.
Universal Design for Learning
The targeted interdisciplinary workforce is comprised of nurses, therapists, home health aides, and psychosocial team members. With this large interdisciplinary remote workforce in mind, implementing multimodal learning in our educational strategy was essential. When educating a large interdisciplinary workforce of clinicians in a remote work environment with diverse learning styles such as this content was intended for, it became essential to utilize Universal Design for Learning principles. Universal Design for Learning (UDL) is an educational framework that provides flexible ways for students to access, engage with, and demonstrate their knowledge, ensuring all learners have equal opportunities to succeed. 10
To properly ensure the content of this education utilized UDL principles the educators used the UDL Content Representation Checklist. The UDL Content Representation checklist includes a list of UDL strategies selected for their ease of implementation, that is, strategies that did not require a large investment of time or a high level of technical expertise to implement. 11 The checklist breaks down the presentation sections into media, readability, content structure, and links. The synchronous presentation format was planned with these sections in mind. The pictures and text in the presentation were kept simple, and the visuals used high-contrast colors for text and tables. The use of standard headings and bulleted texts throughout the presentation improved readability. Understanding various types of learners and the potential barriers, a multimodal design was implemented using UDL. 12 To ensure that multimodal learning was implemented into all phases, the Visual, Auditory, Reading-Writing, Kinesthetic (VARK) model was used.13,14 Visual elements were included via a video graph and images; auditory elements through spoken content; reading-writing through slides and the meeting chat; and kinesthetic elements through an interactive case study. Instead of using non-descriptive links, all follow-up resource links and emails were sent to staff in a separate email to improve ease of use and understanding. This education design strategy aimed to engage learners, encourage interaction, support multiple ways to interact with and apply information, and promote understanding and confidence in the content.
Session Design
The educational session was 90 minutes long. The course schedule is shown in Figure 1. The lecture component consisted of 3 sections. The first section discussed the prevalence of mental health conditions, defined common mental health conditions, and described common symptoms. It was emphasized that mental health is on a spectrum of wellness to illness. During this section, a video on mental health symptoms from the National Alliance on Mental Illness (NAMI) was shown. 15 The second section used a mental health stoplight (Figure 2) and discussed clinician interventions appropriate for all 3 levels. The third section of the competency discussed the need for clinicians to engage in mental health self-care and provided recommendations for dealing with potential mental health concerns in patients’ caregivers. One of the presenters monitored the chat and addressed written questions and comments throughout the presentation. After the lecture, a case-study was presented that described working with a patient with a mental health emergency. Breakout rooms were provided to discuss the case study with 10 to 15 clinicians each, and then a group debriefing was provided. The course concluded with an opportunity for clinicians to make comments or ask questions.
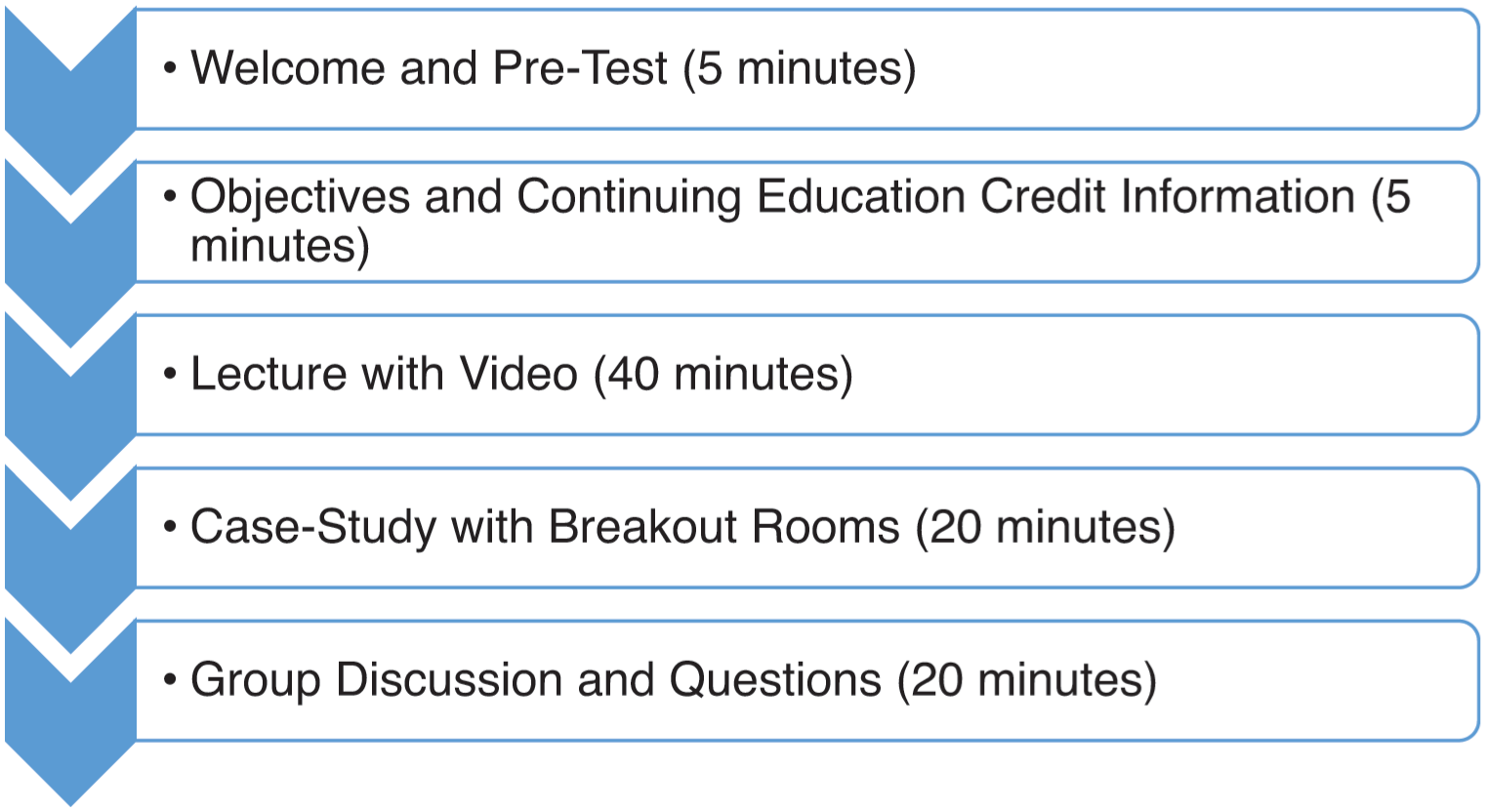
Competency schedule.
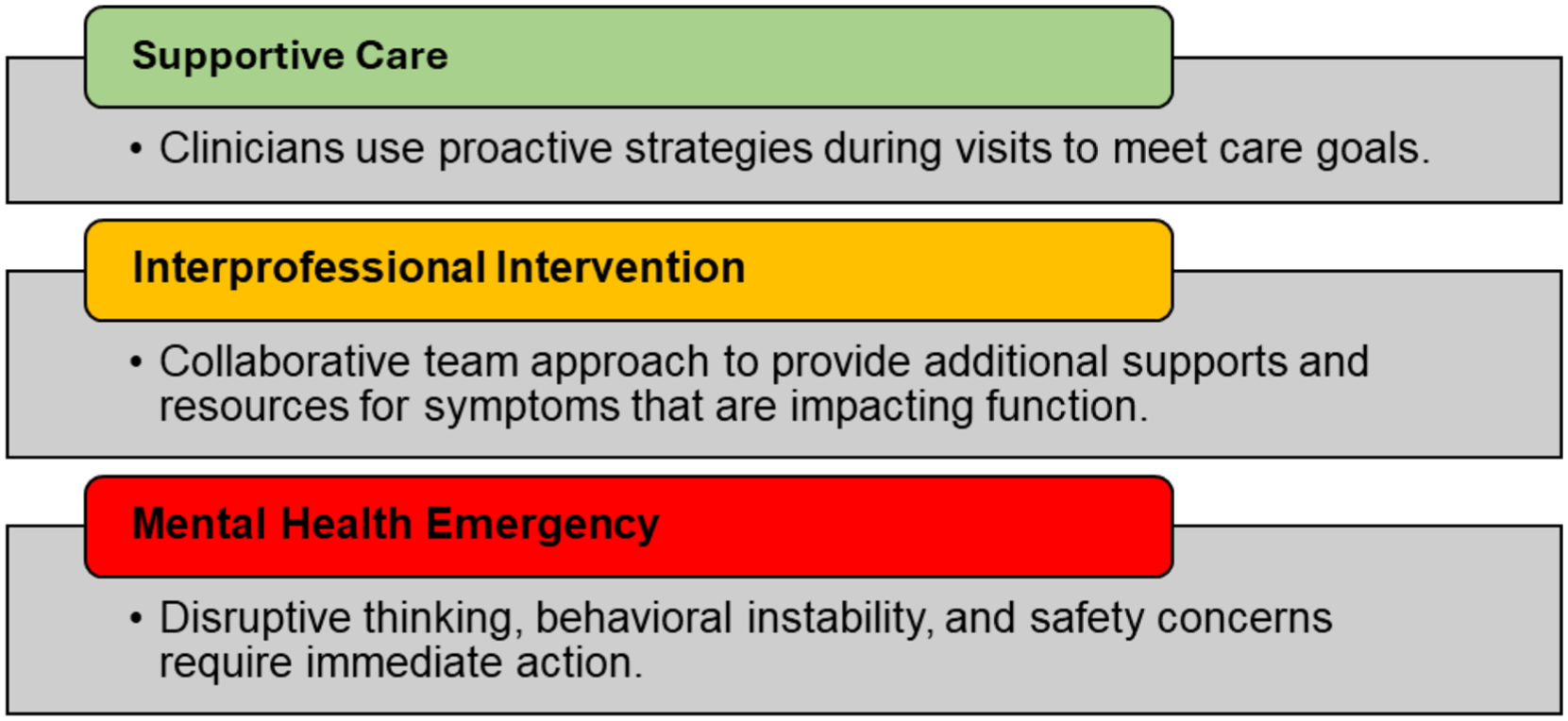
Mental health stoplight tool.
Project Implementation
All agency employees were invited to attend 1 of 4 synchronous educational sessions. Sessions were conducted using Microsoft TeamsTM. All employees who did not attend a live session were enrolled in an asynchronous module in the organization’s learning management system. The asynchronous module was recorded by the same presenters and offered an opportunity for reflective engagement in the case study instead of a discussion. Nurses, physical therapists, occupational therapists, speech therapists, and social workers received 1 continuing education credit for participating in the educational session.
Pre- and post-data were gathered via a Microsoft FormsTM survey. Survey questions were developed by the authors collaboratively and reviewed by an expert nurse educator. Data were gathered anonymously to prevent coercion. For clinicians attending the live sessions, the survey was provided at the beginning of the session. Then, a link to the post-survey was in a learning system module sent out 5 to 7 days after the live session, where they completed an affidavit for continuing education credit. For clinicians attending the asynchronous course, the pre-survey was provided as a link before the recorded module, and the post-survey was provided after. This project was reviewed by the organization’s Institutional Review Board. and determined to qualify as quality improvement.
Results
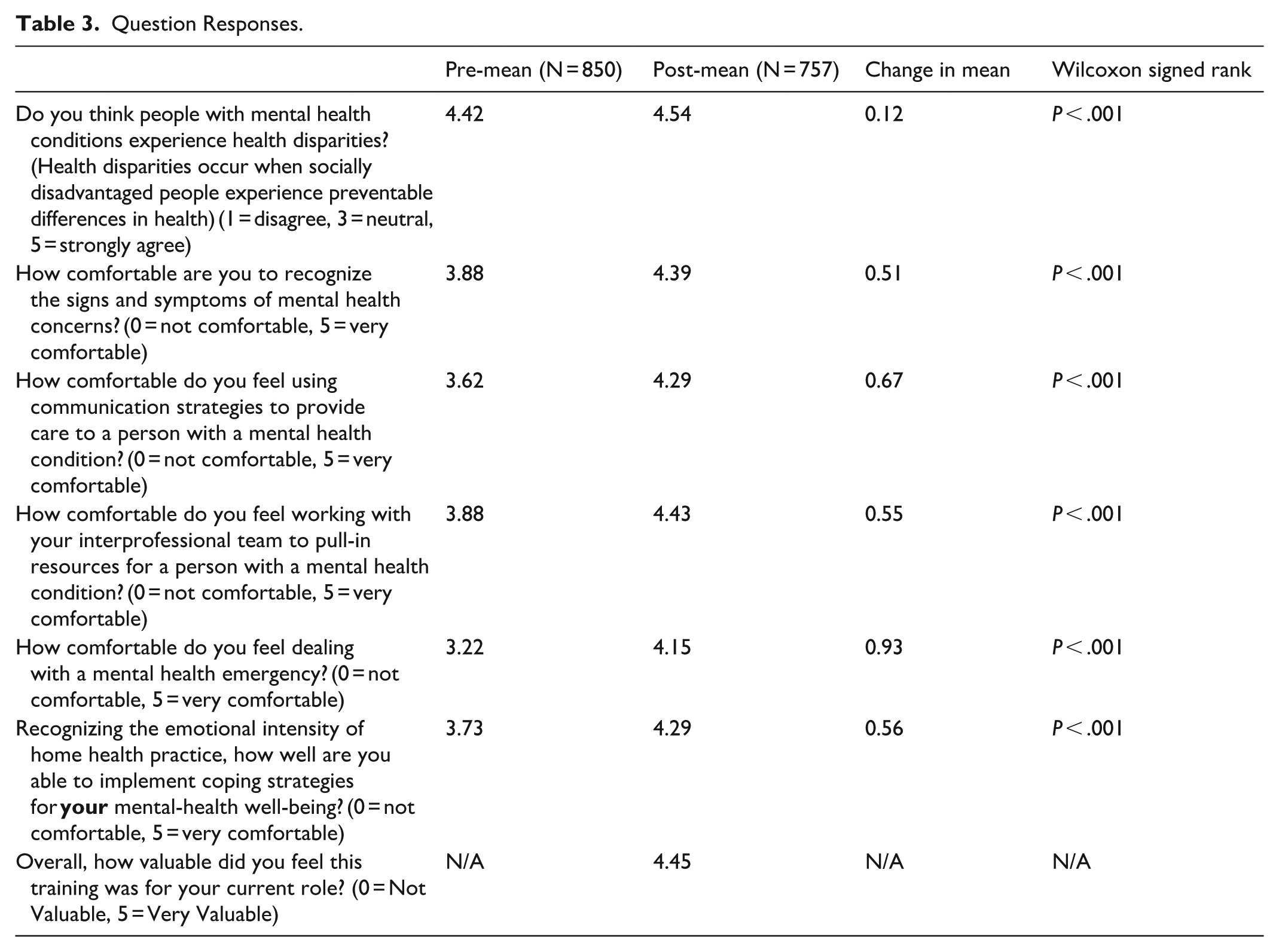
The educational program had a high attendance rate. The competency was completed by 974 clinicians, representing 84.5% of the organization’s clinicians. Among clinicians, 541 attended the live sessions, and 433 completed the asynchronous module. The pre-survey yielded 850 responses. The post survey yielded 757 responses. Table 1 shows the professional disciplines of the responding clinicians. Table 2 shows which service line the clinicians were employed within the organization. The largest groups completing the survey were registered nurses and staff working in the home health service line, consistent with the organization’s overall demographics. Table 3 shows the mean responses for content questions from the pre- and post-surveys as well as the results of a Wilcoxon Signed Rank inferential analysis. The mean response increased across all 6 content questions. The range for all clinical pre-survey questions was 1 to 5, while the range for all post-survey questions was 2 to 5. Inferential analysis using the Wilcoxon signed-rank test revealed statistically significant differences (P < .001) for all 6 pre-post survey questions. A final question in the post-survey asked about the value of the training, and the mean was 4.5/5, with a range of 1 to 5.
Responses by Discipline.

Responses by Service Line.

Question Responses.
Discussion
This educational program on mental health conditions was effective in increasing home health clinicians’ perceived knowledge and competence, as evidenced by statistically significant changes in scores across all pre-post questions. The high attendance in the training indicates clinician motivation to develop their skills in this area.
Although all items showed statistically significant changes, the smallest mean change was in clinician perception of health disparities. Recognizing that clinicians advocated for this educational program, the authors believe that clinicians in this organization identified health disparities that needed to be addressed, which likely limited the magnititude of the change in post-training responses.
The greatest mean change was in clinician confidence dealing with a mental health emergency. In the discussion and question and answer section, many clinicians had further questions on how to address mental health emergencies, and many shared firsthand experiences dealing with difficult situations while providing care. This increase indicates that the training met clinicians’ needs for tools to deal with mental health emergencies.
This paper fills a gap in effective strategies to educate home health clinicians in caring for people with mental health conditions in the home health setting. In inpatient settings, targeted education for staff focusing on de-escalation techniques, communication, controlling behavioral symptoms, and restrictive measures increased staff confidence and reduced violent incidents. 16
Although initial results were extremely positive, it is unclear whether the impact will be sustained over time. Results from previous work training oncology nurses in communication skills reported 98% of attendees reported immediate benefits, but there was a significant decline in confidence at a 6-month follow-up. 17 These results reflect a need for refresher training to maintain clinician confidence.
One limitation of this project was that no concrete knowledge check was performed. The training focused on interpersonal strategies that did not lend themselves to a knowledge check. Furthermore, meeting clinician needs was the primary aim in this study. Another limitation was lack of matched-pairs for data analysis. However, it was felt that clinician anonymity was needed to gain objective feedback on outcomes.
Since the outcome of the objectives for this education were met with such high increases in clinical confidence, one recommendation would be a follow-up survey. The UDL principles refer to “building knowledge” as it pertains to building usable knowledge that is accessible for future decision-making. 10 Usable knowledge depends not upon merely perceiving information, but upon active skills like making connections, synthesizing information, asking questions, selective attending, integrating new information with prior knowledge, strategic categorization, and active memorization. 10 To determine the need for refresher education sessions the educators would need to understand whether current clinical confidence after mental health education will promote sustained knowledge and clinician confidence as long-term outcomes.
Recommendations for future research include incorporating a knowledge check to assess changes in learner knowledge. Furthermore, additional investigation is needed to determine whether the results of the training are maintained over time and, if not, at what frequency refresher courses are needed.
Conclusion
Clinicians providing home health services are likely to encounter a significant percentage of clients who have mental health conditions. Although the focus of home health is on physical health, confidence in addressing mental health concerns is needed to work effectively with these clients and prevent health disparities. Targeted education on mental health conditions can improve clinicians’ confidence in working with people with mental health conditions in the home setting.
Footnotes
Acknowledgements
The authors would like to thank Marcia Nettingham DNP, RN-BC, NE-BC for championing this project and Lindsay Bowler MSN, RN, NEA-BC, FACHE for her unparalleled leadership and support.
Ethical Considerations
This project was reviewed and determined to qualify as quality improvement by the University of Pennsylvania’s Institutional Review Board.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.