
Abstract
Background:
Children with medical complexity (CMC) need coordinated home care beyond traditional healthcare, and how parents interact with these systems is central to shaping their children’s care pathways. While family-centered care emphasizes collaboration between providers and families, this study examined how parents engage with home care systems and the impact of these interactions on their children’s care pathways.
Methods:
A descriptive qualitative design was used, with reflexive thematic analysis. Fifteen parents (13 mothers, 2 fathers) were recruited through pediatric community organizations across Ontario, Canada. Virtual interviews, 45 to 90 minutes in length, explored experiences with care coordination, system interactions, and service navigation. Data were analyzed inductively using NVivo software.
Results:
Three overarching themes were generated: (1) systemic barriers in pediatric home care, (2) service delivery and information gaps in home care, and (3) Family-Managed Home Care (FMHC) alternative pathways and trade-offs. Limited funding led to inadequate staffing and poor care quality, resulting in some children losing developmental progress. Parents feared that speaking up about care issues could result in losing services. Information gaps and geographic disparities created systematic inequities. FMHC offered enhanced control but transferred substantial administrative burdens to families, creating new forms of stratification based on administrative capacity.
Conclusion:
Current home care systems for CMC in Ontario create structural barriers that limit family engagement and shift responsibilities onto families, potentially deepening inequities. Meaningful reform requires engaging families as partners in system design and policy development rather than relying on individual-level solutions.
Keywords
Background
Children with medical complexity (CMC) represent a growing population that requires coordinated healthcare services extending beyond traditional hospital and clinic settings.1,2 These children, characterized by chronic conditions, functional limitations, and high healthcare utilization, often depend on complex care routines that include technological supports, specialized therapies, and ongoing medical monitoring.1,3 As healthcare systems increasingly emphasize community-based care delivery, home care services have become a central resource to supporting these children and their families in managing intensive care needs.4,5
In Canada, home care is provincially administered, with Ontario’s system providing publicly funded services coordinated through regional health authorities, which assess needs, develop care plans, and coordinate service delivery. 6 Home care for CMC encompasses skilled nursing, personal support work, equipment provision, and care coordination,7,8 intended to reduce hospitalizations and enhance quality of life for children and families.9-11 However, coordinating multiple providers, navigating eligibility criteria, and managing service delivery create substantial challenges for families already carrying intensive caregiving responsibilities.2,12,13
Family-centered care principles emphasize partnership between providers and families, recognizing parents as experts in their child’s needs and key decision-makers in care planning.14,15 In home care, this translates into expectations that families will coordinate care, select providers, and participate in service planning.8,16 However, practice may diverge from policy intentions when families encounter systemic barriers or provincial service limitations. Power imbalances between families and healthcare systems can further complicate relationships, especially when families fear that advocacy could jeopardize access to services. 17 In Ontario, alternative delivery models such as Family-Managed Home Care (FMHC) and Special Services at Home provide eligible patients or substitute decision-makers with fundings to purchase services and directly employ providers.16,18 While these models offer greater control over provider selection and care delivery, they also shift administrative responsibilities to families, including managing providers, overseeing budgets, and meeting reporting requirements. 19
Research on family experiences in pediatric home care has focused mainly on coordination challenges, caregiver burden, and service satisfaction.11,20-22 However, much less is known about how families engage with system structures, navigate service limitations, and adapt their care strategies in response to system constraints. Little evidence describes how these parent–system interactions shape care pathways and outcomes for CMCs. The interplay between family needs, system limitations, and service delivery models creates diverse experiences that can significantly affect both family well-being and child outcomes.11,23 Understanding these dynamics are essential for designing home care systems that genuinely reflect family-centered care principles while ensuring equitable access to quality services.14,15 Given increasing reliance on home-based care and growing recognition of family expertise, research that capture parents’ lived experiences is important to informing policy and practice. Thus, this study explored how parents engage with existing home care systems and the ways these interactions influence care pathways for CMCs.
Methods
Design
This study employed a descriptive qualitative methodology to examine parents’ lived experiences navigating the home care system for CMCs in Ontario, Canada. The descriptive approach was chosen to capture the multidimensional nature of parents’ interactions with home care services and to illuminate the practical realities of care coordination within the home environment. Reflexive thematic analysis served as the analytical framework, enabling a systematic exploration of parents’ perspectives while maintaining sensitivity to the contextual factors that shaped their experiences.24,25 As such, our ontological and epistemological approach was social constructivist, in that the caregivers shared their subjective experiences of this healthcare system, which are relative to this region of Ontario.
Samples and Recruitment
Parent participants were recruited through 3 pediatric community organizations across Ontario that provide family support, respite care, and therapies for children with complex medical needs. These organizations promoted the study through their communication channels. Recruitment used purposive sampling approaches to capture diverse caregiving experiences.26,27 Consistent with qualitative guidelines suggesting thematic saturation with 6 to 12 interviews in a relatively homogenous group, 28 saturation was achieved after 15 interviews with 15 parents.
Eligible participants were English-speaking primary caregivers of children (birth to 18 years) with neurological impairment and multisystem conditions requiring technological support (e.g., feeding tubes, mobility devices, respiratory assistance). Children were followed by a pediatric complex care team or at least 3 pediatric specialists and had current or prior experiences with home care services in Ontario. Participants required access to Microsoft Teams for virtual interviews. Families of children receiving end-of-life care were excluded to focus on ongoing care management experiences.
Data Collection
Two nurse researchers conducted the individual interviews: 1 with extensive pediatric experience and 1 with specialized qualitative training, combining clinical depth and methodological rigor. Virtual interviews via Microsoft Teams lasted 45 to 90 minutes (most ~60 minutes). Before each interview, participants completed a demographic questionnaire in REDCap. The semi-structured guide, informed by literature and clinical insights, used open-ended questions to explore care coordination, interactions with the healthcare system, and recommendations for improvement, including children’s care needs, service access, and systemic barriers. All interviews were audio-recorded with consent, transcribed verbatim, de-identified, checked for accuracy, and stored on secure, password-protected university servers.
Data Analysis
Data analysis followed an inductive thematic approach,24,25 using NVivo software for systematic coding and organization. Two nurse researchers (JTay and JTa) independently read and re-read transcripts, noting initial impressions. They independently coded the data, comparing and discussing discrepancies until consensus was reached. Initial coding attended to recurring patterns in system barriers, service delivery challenges, and family-managed care experiences. Codes were grouped into preliminary thematic clusters during team discussions. Themes were iteratively refined to reflect participants’ accounts and illustrated with rich, contextualized quotations.
Rigor and Credibility
Multiple strategies were used to enhance the study’s trustworthiness, including investigator reflection, comprehensive audit trails, and regular team discussions. 29 The research team’s diverse professional perspectives, combining clinical expertise with fresh analytical viewpoints, strengthened the interpretive validity of the findings. Regular debriefing sessions facilitated critical examination of emerging findings across different caregiving contexts. Recognizing our positions as healthcare providers with insider knowledge of pediatric complex care, we maintained reflexive awareness throughout data collection and analysis. This involved ongoing documentation of analytical decisions, critical examination of preconceptions, and commitment to grounding interpretations in participant narratives rather than professional assumptions.
Ethical Considerations
The University of Windsor Research Ethics Board approved this study (Reference: 24-113), with additional permissions from participating community organizations. Informed consent was obtained via REDCap, with participants receiving detailed study information in advance and reminded of their right to withdraw or skip any question. Given the sensitive nature of caregiving, all participants were provided with information on mental health resources, including local and provincial counseling services. Researchers monitored participants’ well-being during interviews and followed protocols for responding to distress. All data were anonymized and stored on secure, password-protected university servers, in accordance with institutional confidentiality requirements.
Results
Following the initial screening of 22 interested caregivers, 15 participants took part in the study. The 7 caregivers who did not participate failed to respond to follow-up emails after expressing initial interest. The final sample of caregivers consisted of 13 mothers and 2 fathers with an average age of 41. Majority (n = 11) have 1 child, work part-time (n = 7) with an income between $50,000 and $99,000, and need overnight care (n = 10). The average years of receiving home care is 5 years with the most common service being nursing support (n = 11). See Table 1 for an overview of participants’ characteristics. Each participant received a $25 appreciation gift card. Three overarching themes were generated: (1) systemic barriers in pediatric home care, (2) service delivery and information gaps in home care, and (3) FMHC alternative pathways and trade-offs. These 3 themes consisted of various subthemes which convey the complex relationship parents have with the current home healthcare system. See Table 2 for an overview of themes and subthemes.
Demographic Characteristics of Parents (N = 15).
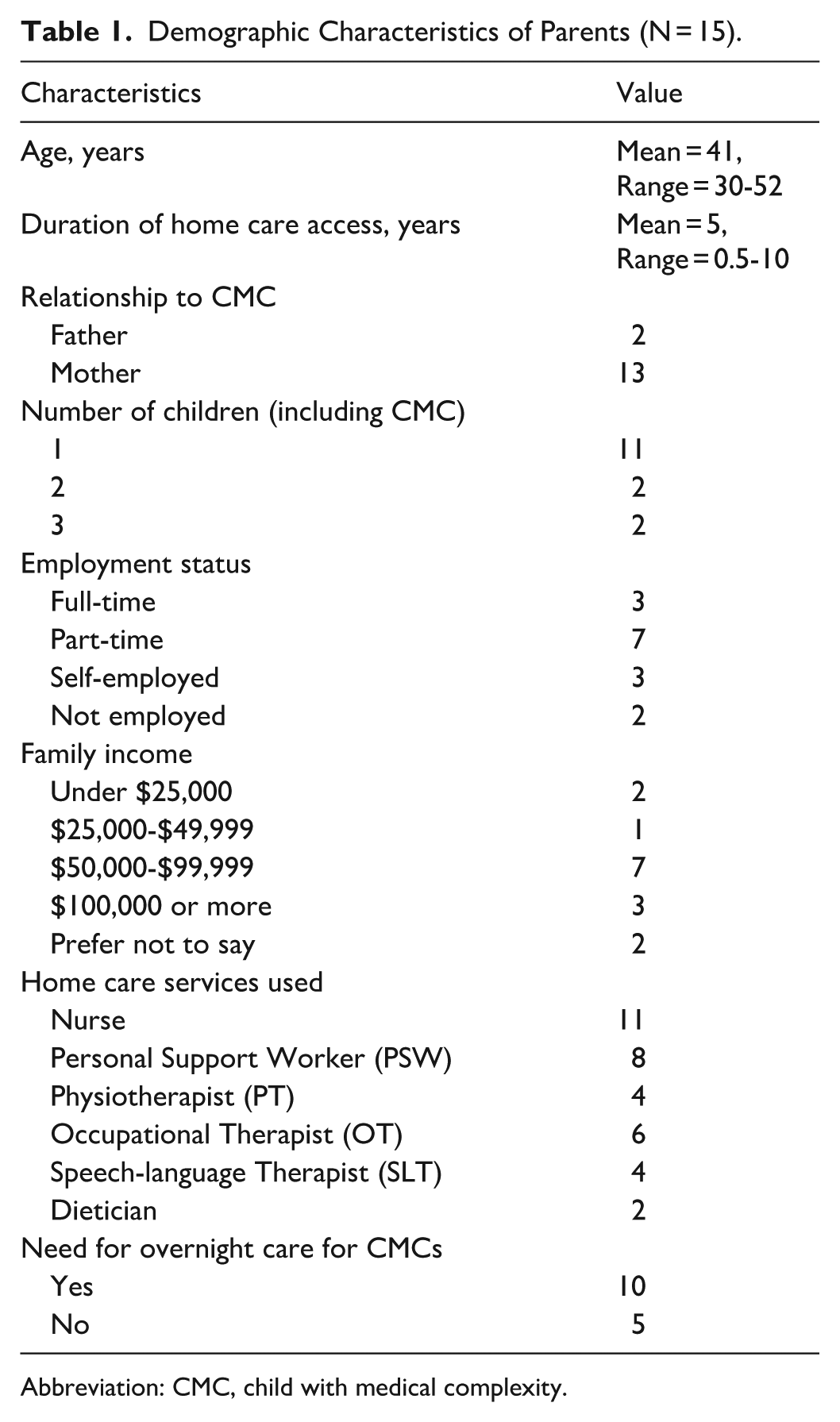
Abbreviation: CMC, child with medical complexity.
Overview of Themes and Subthemes.
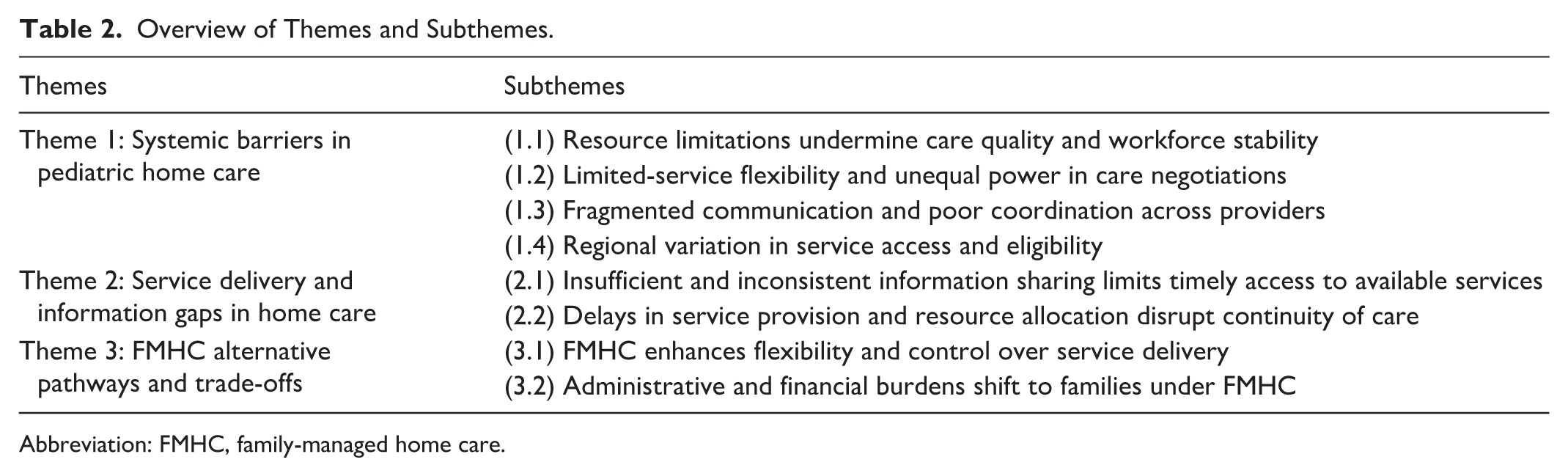
Abbreviation: FMHC, family-managed home care.
Theme 1: Systemic Barriers in Pediatric Home Care
Resource Limitations Undermine Care Quality and Workforce Stability
Parents consistently described how cost-containment priorities compromised care and workforce stability. They felt home care was organized around budgets rather than the needs of CMCs, producing underfunded, fragmented services where access, quality, and continuity were routinely undermined. As Parent 12 explained, . . . [home care] agencies don’t hire properly. They’ll fill shifts with whoever they can, even if they’re not trained for pediatrics. They piece together coverage, so we get a different nurse every day, which is unsafe and inconsistent.
Underfunding is extended into families’ daily realities. Parents were caught between stagnant funding models and rising care costs, often forced into untenable choices. Parent 09 highlighted, “our funding didn’t go up, but PSW wages did. Now they want $30 an hour under the table, and I can’t afford that. I barely get enough hours to make hiring someone even worth it.” These affordability constraints reflected deeper mismatches between system resources and the intensity of care CMCs require, with cascading effects on workforce stability.
Staffing shortages and high turnover were recurrent and distressing themes across interviews. Families described a relentless cycle of short-term workers, minimal training, and unfulfilled hours that undermined any sense of routine. Parent 03 recounted, “we had a new PSW or nurse every month. Some lasted only two weeks. It was exhausting training people over and over again.” Parents were expected not only to manage complex care, but also to repeatedly onboard new providers, often without adequate preparation. As Parent 10 noted, “there’s a lack of consistency. They say they’ll train PSWs, but then they send new people who haven’t been trained. Every single time, I have to explain everything from scratch.”
The revolving door of unfamiliar providers had harmful consequences for children’s emotional security and therapeutic progress. “They send a different nurse every time, so how is my child supposed to build trust?” asked Parent 11. “They don’t even know his name half the time.” Some children withdraw emotionally. As Parent 12 painfully shared, . . .My son regresses every time because he doesn’t consistently have the same person caring for him. Eventually, he just shuts down and only wants me [to do] everything. It just furthers my burnout.
Staffing gaps also disrupted schooling and community participation. “We were supposed to have home care nurses at school,” said Parent 13, “but my child missed an entire month of school because they had no one available to send.” Over time, many parents lowered expectations and normalized the unreliability as a coping strategy. “There were weeks, even months, where there was no availability of staff at all,” said Parent 15. “At one point, we just had to stop expecting anyone to show up.” These experiences illustrate a system constrained by fiscal priorities, where efforts to maximize efficiency compromise safety, erode trust, and shift responsibility onto families.
Limited Service Flexibility and Unequal Power in Care Negotiations
Parents consistently described feeling constrained by a home care system that offered little flexibility and virtually no room for negotiation. In the absence of viable alternatives, families felt they had no choice but to accept inadequate care, fearing that speaking out could result in reduced services or removal from programs. As Parent 7 reflected, The system traps parents. Either accept the inadequate care they offer or be left with nothing. We have no leverage to push for better services. . . The power dynamic in the system is broken. They control everything, and parents are left begging for what should be basic support.
This power imbalance left families feeling fearful and powerless. Parents’ efforts to advocate for changes, whether to request a different provider or report poor care, were often met with hostility or penalties. Parent 5 shared, The system assumes parents are just caretakers, not experts in their child’s needs. We are constantly having to fight to be heard. . . when we requested that a specific nurse not return due to issues, they marked us as ‘refusing care’ and made no effort to replace them.
Rather than working collaboratively with families, home care agencies often responded to complaints by reinforcing rigid rules and threatening to withdraw support, intensifying families’ sense of vulnerability. Parent 12 noted, “we were threatened with removal from the program multiple times if we didn’t comply with arbitrary rules. It’s a constant fear that we could lose what little support we have.” These interactions show how unequal power in care decisions prevent families from safely advocating for their child’s needs.
Families also faced structural barriers that prevented them from using approved services in ways that aligned with their needs. Even when hours were allocated, restrictions on how and when services could be used limited their usefulness. Parent 4 described: They need to allow us to move hours based on our needs. We went to camp in [the city] for two weeks and couldn’t hire anyone because they required specific pre-approved people. Then they wouldn’t let us move those unused hours to September. There has to be more flexibility.
This inflexibility extended into daily routines. As the same parent explained, “I was asking for PSW help because I had four little kids in my house and getting them out the door in the morning was a nightmare. But they refused to give me help.” These examples highlight a rigid system that cannot accommodate the practical demands of family life, particularly for households with multiple children and complex schedules. Despite policy rhetoric on family-centered care, parents were expected to organize their lives around inflexible services and risked punitive consequences for raising concerns. These strained dynamics were further compounded by persistent communication and coordination problems across the home care system, explored in the next theme.
Fragmented Communication and Poor Coordination Across Providers
Parents described a home care system characterized by disjointed communication and inconsistent coordination between providers, administrators, and care settings. Parents frequently encountered gaps in information sharing, unclear responsibilities, and conflicting guidance across home health care agencies. This lack of integration created not only confusion but also additional burdens for families already stretched thin. One parent described it as “too many hands in the pot,” with no one stepping back to ask what the family actually needed.
It’s [a] broken telephone. Too many people involved and nobody actually asks, ‘what do you actually need? What’s your ideal scenario?’ Instead, I’d get random PSWs sent to my house, sometimes travelling an hour by bus, just to work for one hour and not get paid for their travel time (Parent 04).
These inefficiencies disrupted continuity of care, added unnecessary stress to parents, and wasted provider time that could have been used for direct care. Administrative confusion around scheduling, staffing, and roles often left families scrambling to coordinate basic support that the system should have handled.
The lack of responsiveness from home health care teams deepened parents’ frustration and eroded trust. Administrative coordination failures further worsened these communication breakdowns, particularly during care transitions. Parent 08 shared, “there were things missed in the hand off, in our move with [provincial agency] . . . It was just [an] administrative nightmare. . . so frustrating.”
These issues extended across periods of care transitions as well. Coordination between inpatient hospital discharge teams and outpatient home care agencies was often described as fragmented, leaving families to navigate complex clinical follow-up on their own with little guidance or continuity. Even when services were in place, families often received care that was misaligned with their child’s complex needs. When parents raised concerns, they were frequently dismissed or ignored. As Parent 14 recalled, “when we were with the agency and [had] visiting nursing, we would say, ‘hey, the supplies are being ordered wrong,’ or, ‘you sent us an adult Operating Room nurse. We need a pediatric nurse who knows G-tube care.’ And they would say ‘That’s what we have and that’s what you get.’”
This lack of responsiveness reflected a broader systemic failure to prioritize clinical appropriateness or engage parents as partners. The system defaulted to prioritizing availability over quality, highlighting a disconnect between care organization and family needs. Beyond these systemic issues, families also found that their geographic location significantly influenced their access to services.
Regional Variation in Service Access and Eligibility
Families living in rural, remote, or underserved areas described significant challenges in accessing adequate home care services. Differences in service levels across regions left families feeling penalized based on geography rather than need. Parent 08 illustrated this vividly: We got less nursing hours when we moved to [City B] than we did in [City A], even though my child’s needs didn’t change. They told us the funding levels were just different in different regions. We moved out of [City A] to be closer to family, but the level of support we got dropped.
These disparities were not only about access but also about transparency and fairness. Parents frequently encountered unclear or contradictory eligibility criteria depending on their local Home and Community Care office. Parent 12 shared, Each Home and Community Care office works differently, with different rules and policies. There’s no transparency. I was constantly threatened with removal from the program if I didn’t meet arbitrary requirements that weren’t even the same across regions.
Despite operating within a provincial system, families described significant regional differences in service coordination, eligibility decisions, and provider availability. Without standardized policies or clear guidelines, parents navigated vague, shifting expectations, adding cognitive and emotional burden to already demanding caregiving roles. These geographic inconsistencies intensified stress, constrained decisions about relocation and work, and made pediatric home care feel fragmented and inequitable, with some families receiving less support because they lived there.
Theme 2: Service Delivery and Information Gaps in Home Care
Insufficient and Inconsistent Information Sharing Limits Timely Access to Available Services
A major barrier to timely home care access was the lack of clear, comprehensive, and consistent information. Parents reported not being informed about eligibility criteria or available services. Even when clearly eligible, families were left uninformed, leading to delays and unnecessary hardship. As Parent 02 reflected, “I think that, really, ultimately, the responsibility was [hospital] and discharge planning. . . Clearly, we were always eligible for at least visiting nurse support, but no one told us.” Parent 07 shared a similar experience: . . .the hospital didn’t tell us about special funding programs. I only found out through other parents. It’s absurd that you have to be lucky enough to meet the right person to get the help you need.
After discharge, many families still did not receive structured information from home care coordinators. Instead, they learned about services and resources through peer networks and social media. Parent 12 explained, We only found out about home care through other parents. No one at the hospital told us anything. If we hadn’t been in Facebook groups, we never would have known what to ask for.
The system’s failure to proactively inform families created uneven access and widened disparities. Without guidance, parents managed complex care alone, often for years, unaware that help was available. Rigid assessments and eligibility criteria further delayed care and minimized the realities of children’s medical needs and caregiver strain. Parent 13 described, We were in survival mode for years before we even realized we could get help. I wish someone had sat us down at the beginning and explained what was available instead of making us figure it out on our own. . .We spent 2 ½ years just surviving, barely managing.
These accounts highlight systemic communication failures at key touchpoints, such as hospital discharge, and a reliance on informal networks that disadvantage families without connections or digital literacy. Many delays reflected information gaps rather than ineligibility, adding avoidable strain to already overburdened caregivers and prompting some to seek alternative approaches to regain control over their care.
Delays in Service Provision and Resource Allocation Disrupt Continuity of Care
Although home care is often promoted as a responsive and accessible system, families described persistent delays that interrupted care continuity and placed additional strain on caregivers. Parents frequently found themselves not only managing complex clinical tasks but also navigating administrative hurdles to secure basic services. These gaps were especially apparent during care transitions and urgent needs, where systemic inefficiencies delayed essential supports.
“It took six months to get PSW services at home,” recalled Parent 10. “And even once they approved my extra hours, it took another month just to get them actually scheduled. It took eight days to reinstate services. And even after that, PSWs weren’t trained in the stretching routine she needed.”
Rather than functioning as a coordinated system, service delivery was often reactive. Parents described being stuck in bureaucratic limbo during key moments of need, forced to reapply or restart processes after a hospitalization or service interruption—even when their child’s condition had not changed.
Delays extended beyond staffing and hours to include critical equipment and assistive devices. Parent 12 shared, “we have a stander and a walker on order, but it takes months. We had to apply to [company], which takes 10 to 12 weeks just for approval, and then we wait another 7 to 8 months for the vendor to actually get it to us.” These extended timelines restricted children’s mobility and independence, limiting their developmental progress and participation in daily activities.
Underlying these delays was a system that failed to recognize parents as knowledgeable partners. Rigid procedures and poor coordination between agencies created service bottlenecks, leaving families to compensate for systemic shortfalls. These recurring delays disrupted care consistency and children’s well-being, with developmental routines interrupted and therapies postponed due to bureaucratic inertia rather than medical necessity. The operational challenges extended beyond timing to encompass fundamental gaps in information sharing.
Theme 3: FMHC Alternative Pathways and Trade-Offs
FMHC Enhances Flexibility and Control Over Service Delivery
Faced with persistent systemic barriers and inflexible service models, many families turned to the FMHC program to regain control over their child’s care. Parents described FMHC as a way to bypass rotating staff, skill mismatches, and rigid scheduling that characterized agency-based care. By managing funding and hiring directly, families could better tailor services to their child’s needs and routines. As Parent 05 noted: We liked the idea of having a little more control of who was coming into our home, having more control over how they were trained, and flexibility with scheduling. . .we get to choose who spends time with our daughter, including her school nurses. It’s worth the administrative hassle because we can hire people who are a good fit.
This ability to select and retain trusted caregivers gave families a sense of security that was often missing in traditional care models. For children with high needs and vulnerability, trust and familiarity were essential. Parent 08 emphasized: Family Managed [Home] Care allowed us to pick the people we trust to be in our home, in our child’s bedroom at night.
FMHC also addressed one of the most distressing issues under agency-based care: constant staff turnover. Instead of orienting new workers every few weeks, families could invest in stable care relationships. Parent 14 shared, “I switched to Family-Managed Care because agency nurses kept changing. Now I can hire consistent people who actually know my child.” This consistency improved children’s comfort and safety while reducing the emotional labor of repeatedly retraining staff.
However, FMHC also transformed parents from recipients of home health care into employers responsible for payroll, documentation, and training, often with limited formal support. Despite these substantial administrative demands, many families considered the trade-off worthwhile for greater control and reliability. Yet this autonomy came at a considerable personal cost, revealing how much burden families must absorb to secure care that aligns with their child’s needs.
Administrative and Financial Burdens Shift to Families Under FMHC
While FMHC offered families greater control and flexibility, it also transferred substantial administrative and financial responsibilities onto parents. Many described taking on roles typically reserved for health care administrators, such as recruiting, hiring, scheduling, training, and managing payroll without formal training, compensation, or infrastructural support. Parent 07 characterized it this way: We are given the funds but expected to manage all of it, hiring, training, payroll. . . I don’t have an HR background, yet I’m expected to handle everything like a business owner. It’s more work than we anticipated.
Families entering FMHC were often unprepared for the scale of unpaid labor required. These tasks were layered on top of intensive caregiving, and the workload in both time and complexity was frequently underestimated. Parent 09 explained, If you take on Family Managed [Home] Care, you save the system money, but it comes at the cost of your time and effort. You’re not paid for the work you do, even though agencies charge significantly more for the same care. People don’t realize that Family Managed [Home] Care is like running a business. You need a CRA number [Canada Revenue Agency], WSIB [Workplace Safety and Insurance Board], extra insurance, payroll, and have to schedule, hire, fire, and train people. We do all of this for free.
Beyond day-to-day operations, families also encountered bureaucratic hurdles in gaining access to the program. Eligibility criteria and documentation requirements were perceived as burdensome and insufficiently attuned to existing caregiver strain. Parent 13 recalled, The transition to Family Managed [Home] Care was difficult because we had to justify why we needed it and prove traditional nursing wasn’t working for us.
Although many parents valued FMHC’s flexibility and consistency, its heavy reliance on unpaid, unsupported labor raises serious equity concerns about who can realistically participate and benefit. By shifting administrative tasks to families, FMHC fills gaps left by traditional home care at the cost of caregivers’ time, energy, and finances. Families without the capacity, stability, or literacy to manage these demands are less able to use FMHC, reinforcing existing inequalities.
Discussion
This study highlights a gap between policy commitments to family-centered care and parents’ lived experiences within the home care system. While family-centered care principles emphasize partnership, respect for family expertise, and flexible service delivery, our findings demonstrate how structural barriers, operational failures, and inadequate alternative solutions create experiences that negate these ideals. The voices of parents in this study highlight the gap between policy rhetoric and lived reality, revealing how families navigate a system that often fails to provide timely and appropriate support.
Previous research has documented workforce shortages and resource limitations in home care, but our data reveal how these dynamics deepen existing problems for children and families.30,31 Parents described wide variability in provider availability and skill, and felt the system prioritized “filling shifts” over safe pediatric care.32-36 Our study extends prior work by showing that, for CMCs, staff turnover has consequences beyond operational disruption, undermining children’s emotional security, therapeutic progress, and developmental outcomes.33,36-38 When children “shut down” and regress in response to constantly changing caregivers, existing care challenges intensify, and additional supports are required.
Most studies on patient and family engagement focus on communication barriers.11,39 Our findings extend this work by showing how families’ dependence on services produces reluctance to speak up, for fear that complaints could jeopardize access or nursing hours. This dependence means those with the greatest needs feel least able to advocate, thereby suppressing feedback that could drive quality improvements and emerging as a structural barrier to “safe” engagement.11,40 Prior efforts to improve communication or processes may be insufficient when families fear consequences, especially within rigid administrative systems and geographic inequities that turn rights-based access into privilege-based navigation.11,15,41
In response to systemic constraints in pediatric home care, FMHC was introduced as an alternative that allows families to reclaim agency and control over their care experiences, addressing many traditional system failures.2,16,19 The benefits parents described, for example, greater consistency, trust, and flexibility, directly target core problems in agency-based care, such as constant provider changes and skill mismatches. However, this empowerment comes with significant trade-offs, such as families effectively becoming employers, assuming unpaid labor for hiring, firing, scheduling, training, and coordinating care. These demands create new stratification based on social capital, administrative capacity, and family resources. Cost-driven design offloads labor and costs onto parents, work that often falls to mothers and reinforces gendered assumptions about caregiving.21,42-44 Complex administrative requirements are especially challenging for single parents and for families with limited education or language proficiency, who may feel forced to return to traditional models. Echoing broader critiques of policies that emphasize individual responsibility over collective solutions, 24 our findings suggest that structural problems require system flexibility rather than further family adaptation to rigid procedures.
Limitations and Future Research
This descriptive qualitative study offers valuable insight into parental experiences but has several limitations. The sample was predominantly mothers (13 of 15 participants), limiting transferability to fathers’ and families not linked to support organizations. Virtual interviews with English-speaking participants may have excluded families with technology or language barriers. Findings reflect Ontario’s healthcare context and may not generalize to jurisdictions with different home care models. 13 Future work should incorporate multiple perspectives (e.g., frontline workers, administrators, and policymakers), use longitudinal and comparative designs, and include economic evaluations of hidden costs transferred to families. Building on this exploratory phase, future mixed-methods work will develop and refine a conceptual model of parent–system interactions and FMHC-related care pathways to inform system redesign.
Implications for Policy and Practice
These findings have implications for policymakers, health system leaders, and advocacy organizations, who can push for structural reforms without risking individual family care. Problems appear rooted in system design, such as limited pediatric expertise, fragmented models, and treating families as passive recipients rather than knowledgeable partners. Addressing service-dependent relationships that discourage advocacy will require co-designing home care with families, creating safe channels for feedback, and building quality-improvement structures that reflect CMC needs. Expanding FMHC without addressing underlying gaps risks new inequities and added administrative burdens; streamlining FMHC process is essential. Meaningful reform requires adequate pediatric-specific funding models, standardized information sharing, and regional coordination to reduce geographic disparities and support family choices. Performance measures should capture family experiences, continuity, provider consistency, and coordination, rather than simple administrative metrics. Recognizing parents as experts and collaborators in training, care planning, and improvement is key to advancing continuity, coordination, and equity in pediatric home care and realizing the accessibility and universality principles of the Canada Health Act. 45
Conclusion
This study explores how parents engage with pediatric home care systems and identifies a gap between family-centered care policy and implementation. Current structures create service-dependent relationships that limit families’ ability to provide feedback on care quality due to concerns about access to services. While alternative models like FMHC address some systemic limitations by providing families with greater control and consistency, they transfer administrative responsibilities to parents without a corresponding support infrastructure. These findings demonstrate that individual-level adaptations cannot resolve structural barriers within the system. Effective reform requires meaningful engagement with families as partners in system design and policy development, ensuring that those with lived experience of navigating complex care needs have decision-making roles in shaping the services intended to support them.
Supplemental Material
sj-docx-1-hhc-10.1177_10848223251408754 – Supplemental material for Realities of Home Care System for Children with Medical Complexity (CMC): A Qualitative Study of Parent Perspectives Experiences, Barriers, and Alternative Models
Supplemental material, sj-docx-1-hhc-10.1177_10848223251408754 for Realities of Home Care System for Children with Medical Complexity (CMC): A Qualitative Study of Parent Perspectives Experiences, Barriers, and Alternative Models by Joanne Tay, Adam Rapoport, Joanne Ta, Jamie Crawley and Jessica C. Kichler in Home Health Care Management & Practice
Footnotes
Acknowledgements
We want to thank all the participants for their willingness to participate and share their experiences.
Ethical Considerations
This study was cleared by the University of Windsor Research Ethics Board (Reference Number: 24-113) on September 23, 2024.
Consent to Participate
Parents reviewed and gave written consent and signatures before interviews were started.
Consent for Publication
Informed consent for publication was obtained from participants.
Author Contributions
JTay: Conceptualization, Methodology, Investigation, Writing – Original Draft, Review & Editing, Project Administration, AR: Conceptualization, Methodology, Investigation, Writing – Review & Editing, Funding acquisition, JTa: Data Curation, Writing – Original Draft, Review & Editing, JC: Conceptualization, Methodology, Writing – Review & Editing. JCK: Conceptualization, Methodology, Investigation Writing – Review & Editing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the University of Windsor, Research for Women Grant [grant no. 43666].
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data supporting this study are not publicly available due to their sensitive and personal nature. Additionally, participants did not provide consent for their data to be shared.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.