
Abstract
This study aimed to create the foundation for developing infant home safety intervention programs by systematically reviewing the characteristics and effects of such programs designed for parents. A systematic literature search encompassing PubMed, Cochrane Library, Embase, and CINAHL was conducted to select studies reported in English or Korean from 2003 to 2023. Out of the 5419 studies extracted, 7 were selected for review. The infant home safety topics by development were varied such as integrated safety or specific like burn and scalds safety or car safety. Most studies reported positive effects on safety behavior or practice. Moreover, various intervention methods, such as home visitations, home safety kit, brochures, counseling, discussions, videos, etc., were utilized. The systematic review suggests that complex topics are essential for parents with infants and for expectant parents. The findings provide foundational data for evidence-based practices and directions for infant home safety programs for parents in community.
Introduction
There is, unfortunately, no such thing as a “child-proof” home. However, parents can create safe home environments and supervise infants to reduce the risk of injuries. 1 Homes that are primarily designed for adults can pose a threat to infants because of their limited physical abilities. Moreover, parents may lack an understanding of infant developmental characteristics or fail to create a safe environment, resulting in potential harm. 2 Thus, to prevent infant unintentional injuries and mitigate injury severity, parents must inspect and manage their home environment. 3
Unintentional injuries, that is, unintentional harm resulting from negligence and hazardous environments, 4 constitute a significant source of child mortality, triggering a critical global health concern. 5 Unintentional injuries in children under 14 are caused by slips, falls, bumps, overlay and wedging, foreign body ingestion, aspiration, injuries from high-temperature substances, poisoning, and others. Notably, 49.1% of child unintentional injuries occur in those under 3 years old, with an annual occurrence rate exceeding 87% for infants under 1 year. 6 Infancy experiences the highest mortality from unintentional injuries. 7
Infants cannot control their bodies nor can they sense danger; thus, they have an increased risk for unintentional injuries. 7 Given their limited mobility and the fact that the majority of their time is spent at home, most such injuries occur at home 6 and commonly include aspiration, suffocation, falls, burns, and drowning, resulting in hospital treatments for bruises, lacerated wounds, burns, concussions, and dislocations.8,9 Children affected by unintentional injuries may require extended treatment, face the risk for disability, and, in severe cases, may die. Such unintentional injuries inflict emotional distress on children and their parents, leading to financial challenges due to lost workdays and substantial medical expenses. 10 Consequently, unintentional injuries can inflict crucial physical and psychological harm.
The opportune time for infant home safety programs is during pregnancy, 11 with home safety education during pregnancy and the early postpartum period effectively reducing the incidence of unintentional injuries.12,13 Studies have also revealed a desire among pregnant women for safety education. 14 However, studies on infant home safety programs are minimal, 15 and those involving pregnant women are limited.
Research trend analyses and systematic reviews on unintentional injuries in infants have been conducted globally. However, previous studies have excluded pregnant women as participants 15 or included toddlers. 16 Moreover, such education primarily targeted infant teachers, 17 and the education setting was confined to childcare centers. 18 Existing programs have focused on specific topics such as neonatal transport safety 19 and sleep,20 -22 limiting possibilities of an integrated and comprehensive view of the effectiveness of prevention programs for unintentional injuries in infants as well as limiting safety programs of injury risks by stage of infant development from pre-mobile to mobile. This study aims to lay the foundation for the development of such prevention programs according to infant development stage, by systematically reviewing the characteristics and effects of such programs designed for parents.
Materials and Methods
Search Strategy
This study followed the guidelines outlined in the Cochrane Handbook for Systematic Reviews of Intervention 6.2, 23 Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA), 24 and the Systematic Review Manual by the National Evidence-based Healthcare Collaborating Agency (NECA). 25
Focused Questions
This study’s questions were formulated using the Participants, Intervention, Comparison, Outcomes, Study Design (PICO-SD) framework, with specific details regarding the effectiveness of infant safety intervention programs.
“What kind of infant home safety programs can prevent injuries?”
PICO Criteria
Mothers or parents of infants.
Evaluation of education programs for safety and accident prevention, encompassing various interventions such as treatment, education, therapy, counseling, and training.
Inclusion of all studies incorporating a control group.
Consideration of quantitative values measured after the program for participants, comprising outcome variables regardless of the significance of the effect.
No restrictions were imposed on the study design.
Inclusion and Exclusion Criteria
The inclusion criteria were as follows: the study must (1) focus on healthy infants and address safety intervention programs for parents or expecting parents, (2) be published in English or Korean between 2003 and 2023, and (3) be experimental in nature.
The exclusion criteria were as follows: the study (1) focused on the “child” rather than the infant, (2) was not interventional or experimental in nature, (3) was an unpolished study, a brief report; or (4) was a master’s dissertation or a doctoral thesis.
Search Words
To establish the search strategy before the main study, a preliminary search was conducted in November 2023 by combining keywords from the PubMed database into “(Infant, Newborn, Parents), (Safety, Accidents), and (Education, Program).” The central research question was defined and search terms selected on the basis of the literature obtained in the preliminary search. The search formula was established using the advanced search functionalities provided by each database. After confirming that the MeSH terms align with the keywords, the final search formula was selected based on the keywords. The keywords were Infant, Newborn, Parents, Neonatal, Postnatal, Baby, Pediatric, Mother, and Father. For interventions, terms such as Safety, Dangerous Behavior, Accidents, Home or Prevention and Control, Accidents, Safety Management, Accident Prevention, Accidental Falls, Fracture, Burns, Infant Death, Incidents, Injury, Education, Health Education, Health Promotion, Program Development, Program Evaluation, and Preventive Health Services were merged.
The search formula was established by integrating MeSH terms, CINAHL Heading, and operators, including text words and truncation. Before the data search, the database selection and search method setup process was validated via consultation with a researcher and specialist librarian at a medical university library. International databases, including PubMed, Cochrane Library, Embase, and CINAHL, were employed in this study.
The detailed search formula is as follows: #1 infant as “Infant”[mesh] OR “Infant, Newborn”[mesh] OR “Parents”[mesh] OR “infant” OR “newborn” OR “neonatal” OR “postnatal” OR “baby” OR “pediatric” OR “parents” OR “mother” OR “father”, #2 safety as “Safety”[mesh] OR “Dangerous Behavior”[mesh] OR “Accidents, Home/prevention and control”[mesh] OR “Safety Management”[mesh] OR “safe” OR “unintended” OR “unintentional” OR “unforeseen” OR “unplanned” OR “unanticipated” OR “dangerous” OR “hazardous” OR “management” OR “prevent” OR “control”, #3 injury as “Injury”[mesh] OR “accidents”[mesh] OR “Accidental Injuries”[mesh] OR “Accident Prevention”[mesh] OR “Accidents, Home”[mesh] OR “Accidental Falls”[mesh] OR “Fractures, Bone”[mesh] OR “Burns”[mesh] OR “Infant Death”[mesh] OR “Infant Equipment”[mesh] OR “Accidents, Home/prevention and control”[mesh] OR “accident” OR “incident” OR “event” OR “injury” OR “home” OR “household” OR “fall” OR “fracture” OR “burn” OR “death” OR “equipment” OR “swing” OR “walker” OR “furniture” OR “chair” OR “stroller” OR “crib” OR “restraint system” OR “safety restraint” OR “seat” OR “car” OR “automobile” OR “passenger” OR “pacifier”, #4 programs as “Education, Nonprofessional”[mesh] OR “Health Education”[mesh] OR “Health Promotion”[mesh] OR “Program Development”[mesh] OR “Program Evaluation”[mesh] OR “Preventive Health Services”[mesh] OR “Child Health Services”[mesh] OR “Health Knowledge, Attitudes, Practice”[mesh] OR “education” OR “promotion” OR “campaign” OR “program” OR “service” OR “knowledge” OR “practice” OR “visit” OR “delivery” Then, the main search terms above were combined such as #1 AND #2 AND #3 AND #4.
Literature Selection Process
Duplicate literature from the databases was removed using EndNote X7, a bibliographic management database. Additional confirmation of duplicates was conducted through a manual hand-search. The literature selection involved primary and secondary exclusion stages, with detailed criteria based on participants, intervention content, and full-text accessibility. To ensure clarity and appropriateness, a preliminary study on 30 randomly selected literature pieces was undertaken by researchers, and criteria were adjusted through discussion. The selection process involved 3 researchers trained in a systematic review or with relevant experience, ensuring consistency through a pre-session agreement. The first and second researchers independently conducted the selection process, resolving disagreements through discussions with a third researcher. In primary exclusion, titles and abstracts were reviewed to determine whether articles met the selection criteria. Cases with unclear selection status—based on titles and abstracts—were provisionally included, with the final decision made after reviewing the complete text during the primary exclusion process. The entire research process involved the collaboration of 3 researchers; disagreements on including literature were resolved through discussion.
Data Extraction and Analysis
The analysis framework was modified by researchers to suit this study by referring to previous analysis. Data were extracted from the included studies and encompassed “author, year of publication, country, academic field, research aim or objective, study design, setting, data collection, participants intervention, results/outcomes.”
Descriptive statistics were employed for data analysis. Two researchers independently analyzed the final selection of 11 studies. Disagreement between the researchers was resolved through discussion with a third researcher. The results were summarized and categorized into a table using an analytical framework, using IBM SPSS Statistics software V.22.
Assessing the Literature Quality
The quality of the literature selected in this study was assessed using the Critical Appraisal Checklist for Randomized Controlled Trials and the Critical Appraisal Checklist for Quasi-experimental Studies by JBI. 26 The first assessment comprises 13 items and the second comprises 9 items. Responses (“Yes,” “No,” “Unclear,” or “Not applicable”) are scored as 1 point for “Yes” and 0 points for others. Two researchers independently conducted an analysis, reaching a mutual agreement after resolving differing opinions through researcher meetings.
Results
Literature Extraction Results
Of the 5419 articles searched, 3452 were extracted after excluding 1967 duplicates through EndNote and hand-searching. Subsequently, 875 articles were selected through title and abstract review, after excluding 2577 articles. Among these, the final selection comprised 7 articles, excluding 868 articles that did not meet the criteria. These include studies with participants other than guardians of infants, involving toddlers and preschool children, lacking intervention related to infant safety, not meeting study design criteria, being unidentifiable in full text, or not written in English or Korean (Supplemental Figure S1). Characteristics of the 7 articles are described below (Figure 1 and Table 1).
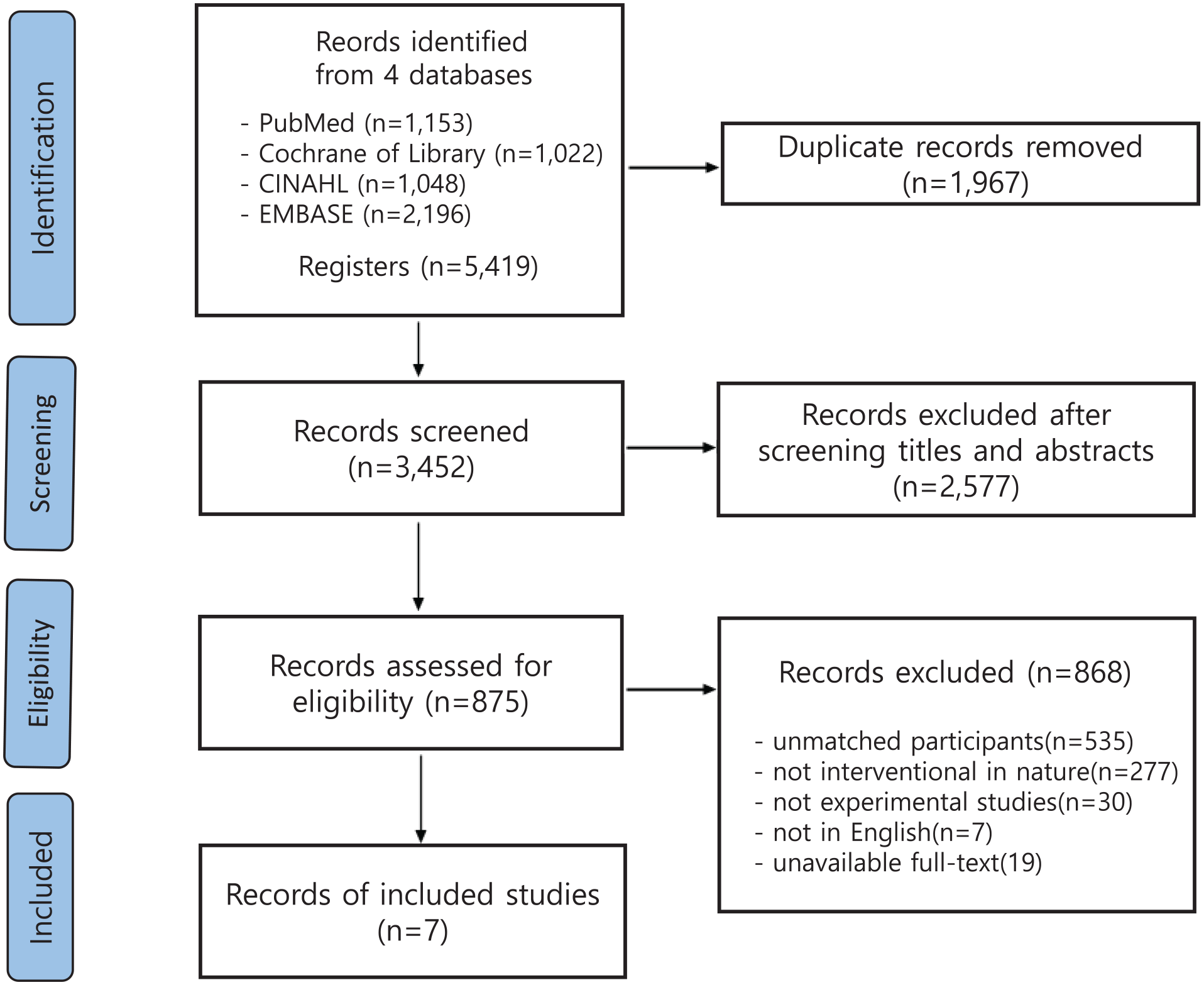
PRISMA flow chart of study selection.
Characteristics of the Included Studies.
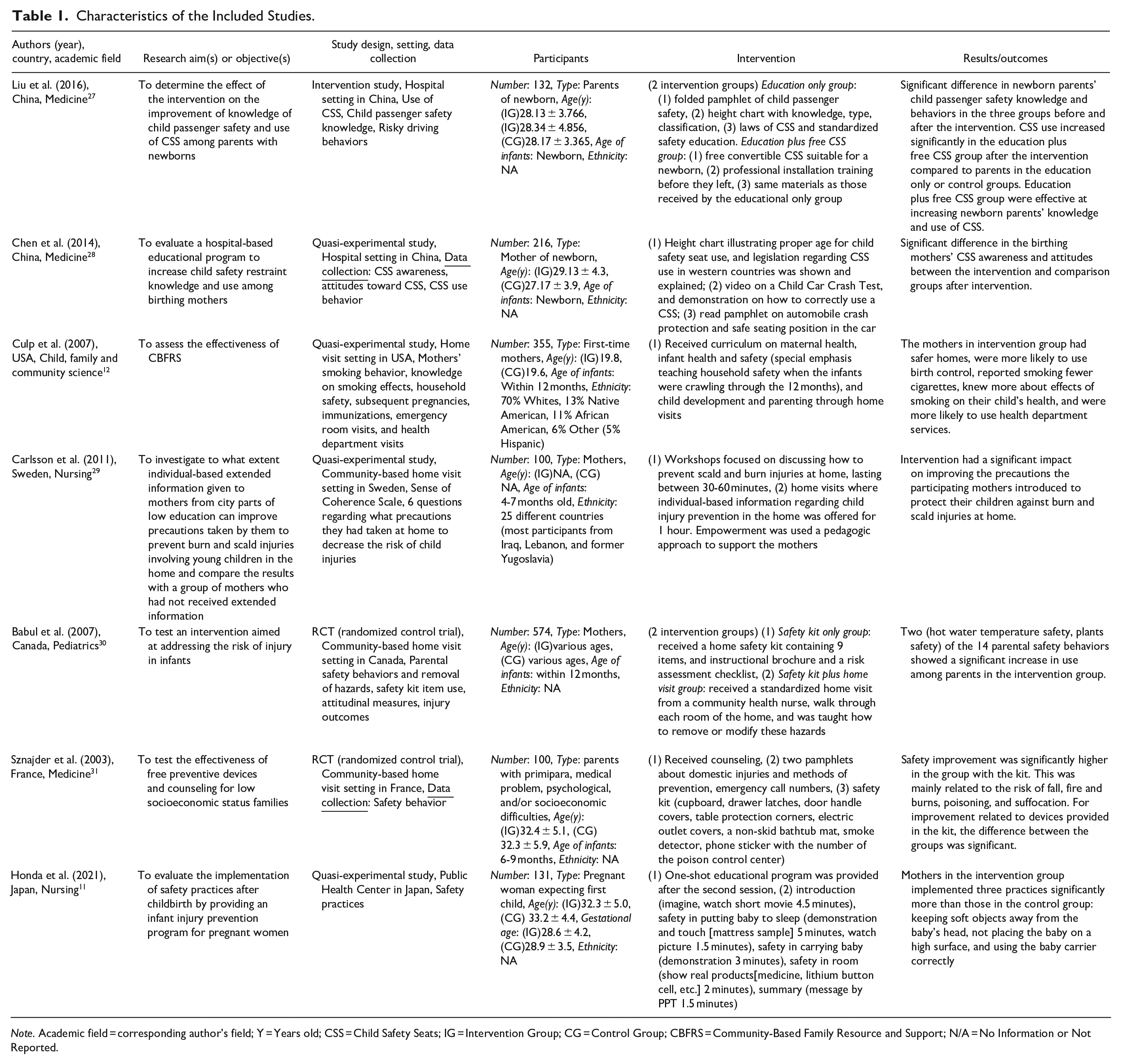
Note. Academic field = corresponding author’s field; Y = Years old; CSS = Child Safety Seats; IG = Intervention Group; CG = Control Group; CBFRS = Community-Based Family Resource and Support; N/A = No Information or Not Reported.
General Characteristics of Articles Selected for Final Analysis
The articles selected for final analysis were categorized by the following characteristics: publication year, country, academic field, study design, setting, participants, number of participants, ethnicity of participants, and home safety area by development of infant. The distribution of these characteristics can be seen in Table 2.
General Characteristics of Articles Selected for Final Analysis.
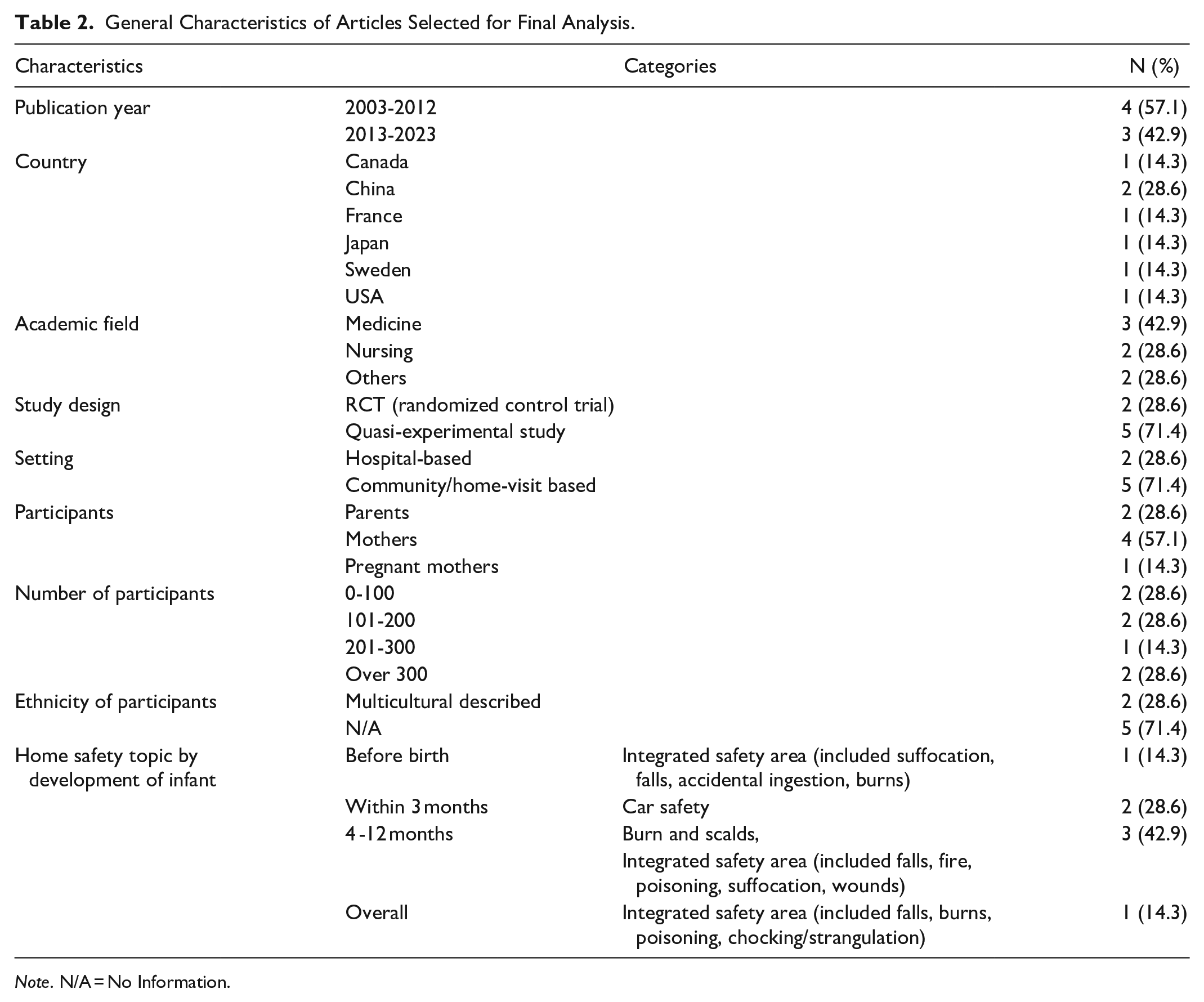
Note. N/A = No Information.
Characteristics of Infant Home Safety Intervention Method and Outcome Variables
The characteristics of infant home safety intervention methods were as follows: home visits, brochure and pamphlet, safety kit, show real products, counseling, video, and picture, training, discussions, demonstration and touch, PowerPoint slide. The characteristics of infant home safety intervention outcome variables were as follows: safety behaviors or practice, emergency room visits and health department visits or injury outcome, safety kit use, safety attitude, safety related precautions questions, use of child safety seats (CSS), awareness of CSS, attitudes toward CSS, child passenger safety knowledge, risky driving behaviors (Table 3).
Characteristics of Infant Safety Intervention and Outcome Variables.
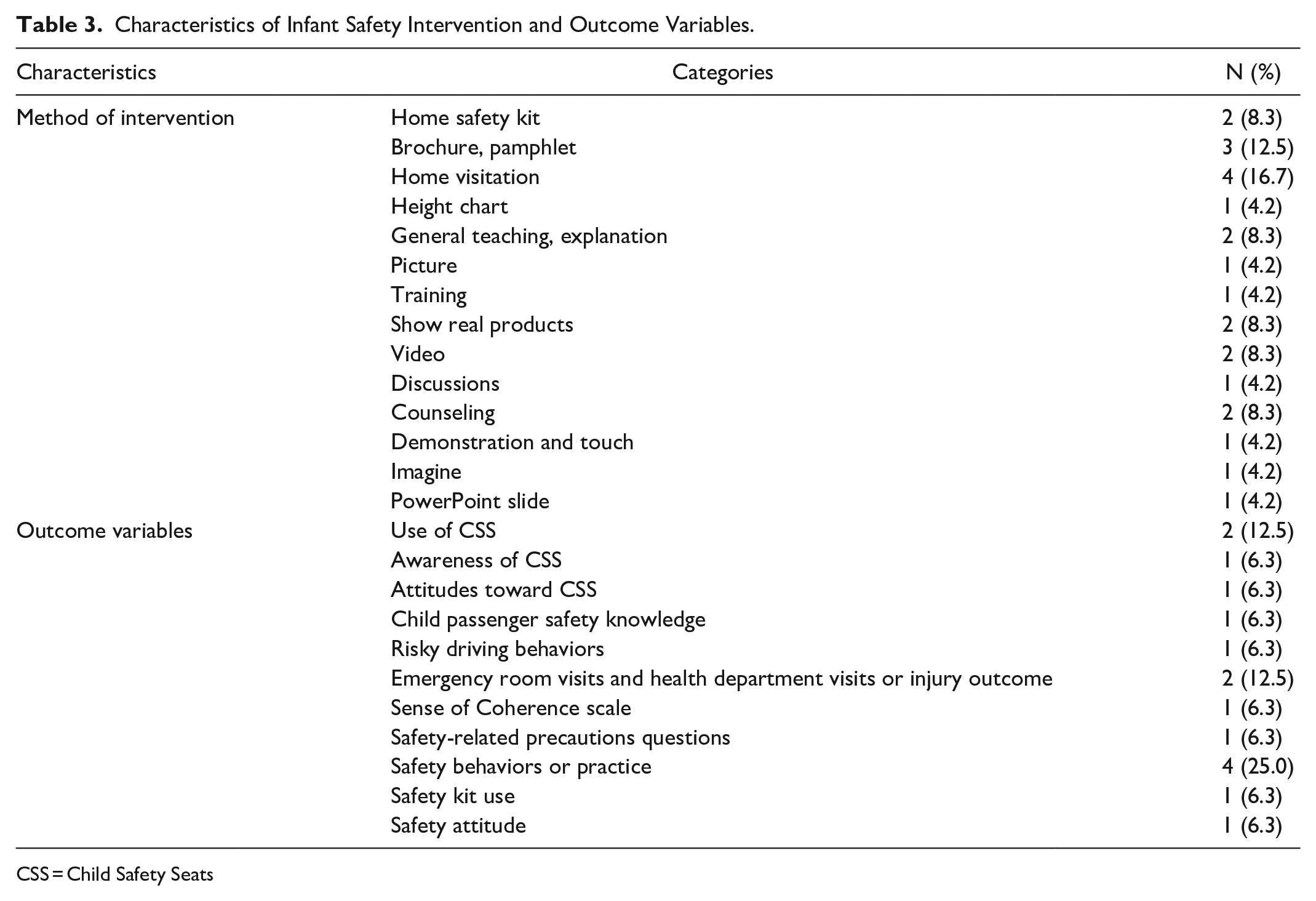
CSS = Child Safety Seats
Quality Assessment Results of Selected Literature
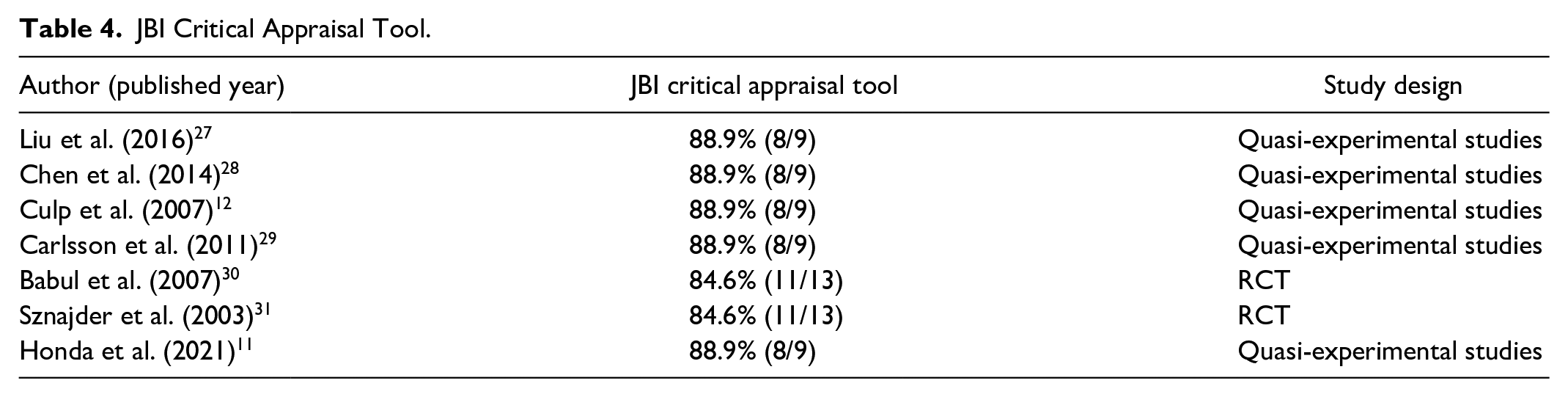
After classifying and assessing the quality of 2 randomized controlled trials and 5 quasi-experimental studies, all articles were found to be of over medium quality. In the 2 randomized controlled trials, only blinding or masking of the outcome assessors and reliability of measurement variables were assessed as “Unclear,” while other items were rated as “Yes,” accounting for 84.6%. For the quasi-experimental studies, 5 articles scored 88.9% indicating “Unclear” for the reliability of measurement variables (Table 4).
JBI Critical Appraisal Tool.
Discussion
This study analyzed the characteristics of parental infant home safety intervention programs, providing foundational data for designing and developing a program applicable to community practice.
Randomization in systematic reviews prevents systematic differences in baseline participant characteristics between intervention groups, ensuring more reliable cause-and-effects than other research designs. 24 This study tried to offer high-level, reliable evidence by analyzing randomized controlled trials globally, but there was an insufficient number of randomized controlled trials available. Therefore, both domestic and international randomized controlled trials, along with quasi-experimental designs, were included for analysis.
Seven articles were selected for this study, with integrated home safety topics or specific home safety topics such as burn and scalds or car safety. This was similar to a previous study that described 6 common injury threats that may appear in infancy: burns, cuts, drowning, poisoning and suffocation, strangulation, choking. 32 As infants develop, there are risk factors related to safety, and it seems that infant safety prevention programs were carried out in this regard. According to this study, integrated home safety programs were provided before birth, car safety education was provided immediately after the baby was born, and specific programs like burn and scalds or integrated programs were provided from the time when the infant became mobile. In other words, since infant stages shift from pre-mobile to mobile, it is important to provide safety programs that predict development, which comports with previous studies that indicated “safety” was the third most important topic among parents of infants within the first 3 months of life. 33
“Car safety,” as a topic of education, differs between the Republic of Korea and other countries. In the Republic of Korea, parents have poor awareness of car seats, failing to install or use them properly. In fact, car seat installation rates are significantly lower than in other advanced countries. 34 Some countries implement policies to increase the car seat installation rate, such as prohibiting discharge from the hospital after giving birth unless car seats for newborns are installed. 34 Such policies must be implemented and enforced in the Republic of Korea. One of the selected articles conducted education with complex topics related to home safety. The Raising Children Network website in Australia provides explanations on safety, with a variety of topics such as home environment and pet safety, household furniture safety, safety in bathing situations, burns, safety in environments outside the home, and car seats, 35 demonstrating that providing infant safety intervention education for different situations is important for expecting parents.
In most studies, the education location was in the home, while some studies conducted the education within the community. Some studies involved individual education through home visitation, walking through each room of home to provide individual instruction to mothers in the home after giving birth. Other studies on safety intervention were conducted in clinics or emergency rooms. However, considering that accidents can occur at any time, this education must provide at least a primary level of knowledge through group settings or individual settings. 11 Further, previous research demonstrates the importance of educational repetition based on children’s developmental stages, as in utero intervention is not enough to influence preventive behavior. 11 In particular, since the transition into motherhood starts before childbirth and continues well after childbirth, 36 it is important to receive preventive education throughout the process of becoming a parent. Thus, considering that the optimal time for infant home safety education is during pregnancy, 11 beginning educational interventions during the transition to parenthood may be more effective.
Moreover, studies reveal that safety education methods preferred by parents include individual education through home visits (57.1%), education using applications or videos (38.1%), and group education (28.6%). 3 Individual education through home visits provides coaching by directly checking the risk factors in each home and eliminates the pressure of leaving home with a baby. Conversely, group education allows mothers in similar situations to share information to prevent infant injury. Combining group and individualized home education offers the benefits 3 of both expert and peer support. 37
This study reviewed research using home safety kit, brochure, pamphlets, video, picture, PowerPoint presentations, discussion, training, and demonstrations as educational tools, which aligned with previous research that applied various teaching methods such as diverse media, demonstrations, and practices. 16 Simulation training and video training were conducted as educational tools to bathe premature babies, which led to meaningful results, 38 and breastfeeding education using a newborn mannequin also improved the knowledge and practice of and self-efficacy in breastfeeding.39,40 Therefore, infant home safety education programs should consider utilizing simulations within the community.
One article, which included mothers from multicultural backgrounds, involved the use of empowerment as a pedagogic approach to support the mothers. The results showed an association between women’s empowerment and maternal and child health outcomes such as antenatal care, skilled attendance at birth, contraceptive use, child mortality, full vaccination, nutritional status and exposure to violence. 41 Thus, an approach to strengthening mother’s empowerment is needed for infant home safety programs to prevent injury.
The outcome variables for the infant home safety programs varied in terms of knowledge (awareness), attitude, and behavior (practice). Most outcome variables were significant. Some articles assessed emergency room visits, health department visits, or injury outcome. Thus, it seems necessary to conduct a follow-up evaluation after intervention. 42
Guide books for parents are crucial for the future development of infant home safety programs within the community. This approach encourages caregivers to have a future-oriented perspective, anticipating the growth and development of the fetus and baby, and preparing them accordingly. Specifically, anticipatory guidance education should proactively address potential injury, based on the baby’s development stages. 43 For instance, topics may include falls, scalds, sleeping safety, suffocation, and drowning for 2 to 5 months; falls, burns, medicine poisoning, drowning, and toy hazards for 6 months; concussion, drowning, driving hazards, and finger pinching for 9 months; poisoning, falls, sunburn, and driving hazards for 12 months; and poisoning, falls, sunburn, and driving hazards for 18 months. 44 Infant and child health nurses are poised to play a crucial role in this initiative.
Limitations and Future Directions
This study has some limitations. First, the effectiveness of the program could not be confirmed through effect size, due to the insufficient number of randomized studies. Second, because of the exclusion of qualitative research, richer material for discussing the benefits of various approaches in providing parental education and the limitations associated with each method could not be included. Thus, this study recommends that future research include qualitative studies to analyze the effectiveness of programs in a multidimensional manner.
Nevertheless, this study analyzed and reviewed 2 recent decades worth of data pertaining to infant home safety education programs for parents. Thus, data such as article characteristics, intervention characteristics, and outcome variable might be confirmed the research trends.
Overall, the study’s findings can serve as foundational data for developing infant home safety programs in the Republic of Korea. Prevention education programs for infant injury may be provided to pregnant mothers or to post-childbirth mothers or parents. It can also be provided to the increasing number of migrant mothers and partners, 45 as immigrant women from multicultural families with infants and toddlers in the Republic of Korea complained of infant safety difficulties. 46 The socioeconomic and cultural characteristics of married immigrant women from multicultural families are factors that make children vulnerable to injury. For example, multicultural families in Korea are largely comprised of Chinese and Vietnamese, etc. 47 In these cultures, awareness of seat belt use for infant is also low.48,49 Therefore, when conducting safety education for multicultural families in Korea, nurses are expected to provide cultural competency nursing that takes into account their cultural backgrounds. 50 In which it will be important to develop educational materials that reflect cultural characteristics and provide education through case-based and model-based applications.
Conclusions
This study systematically reviewed studies implementing infant home safety intervention programs for parents. The findings revealed that infant home safety topics by development stage were varied. The findings serve as foundational data for developing a standardized protocol for such programs, targeting primarily mothers before birth.
Footnotes
Acknowledgements
None.
Author Contributions
Conceptualization, MH.K, MS.K, and SH.P.; Data curation, MH.K.; Formal Analysis, MH.K and MS.K.; Funding acquisition, SH.P.; Investigation, MH.K.; Methodology, MH.K.; Project administration, SH.P.; Resources, SH.P.; Software, MS.K.; Supervision, SH.P.; Validation, MH.K., MS.K., and SH.P.; Visualization, MH.K and MS.K.; Writing – original draft, MH.K. and MS.K.; Writing – review & editing, MS.K. and SH.P. All authors have read and agreed to the published version of the manuscript.
Data Availability Statement
This article’s data will be shared by the corresponding author on request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korea government (MSIT) (RS—2023—00272660).
Ethical Considerations
The study design was approved by the appropriate ethics review board (IRB No. E-2nd-2023-001 by Chungcheong University).
Consent to Participate
Not applicable.