
Abstract
In order to live independently at home, persons with spinal cord injury (SCI) often require professional home care. The role of the care coordinator remains unclear, as it can be fulfilled by the general practitioner or an SCI specialist, as well as by informal caregivers. We aimed to quantify satisfaction with professional home care among persons with SCI living in Switzerland and the association between first contact for care and having an informal caregiver with satisfaction with home care. Measurements were obtained from the national community survey of the Swiss Spinal Cord Injury Cohort Study. Logistic regression was used to determine the association between first contact for care, having an informal caregiver, and satisfaction with home care, adjusted for sociodemographic factors, SCI characteristics, and functional level. Overall satisfaction with professional home care was high, with 84% of participants reporting being either very satisfied or satisfied. Neither first contact for care nor availability of an informal caregiver was statistically significantly associated with satisfaction. The results showed that women (odds ratio 0.56, 95% CI 0.31-1.00) were statistically significantly less satisfied with home care than men. There was also variation by language region. These findings highlight the importance of providing personalized and culturally sensitive home care that takes into account the diverse preferences and expectations of persons with SCI, especially regarding gender and language region.
Keywords
Introduction
Spinal cord injury (SCI) is a complex medical condition that occurs due to damage to the spinal cord. This damage can be caused by an accident or a disease (e.g., cancer, infections, multiple sclerosis). 1 Persons with SCI are at high risk of developing secondary health conditions such as pain, urinary tract infections, or pressure injury, in addition to functional dependence in activities of daily living (ADL). 2 When returning to the community after initial rehabilitation, persons with SCI often rely on the support and care of informal or family caregivers as well as professional home care to maintain their highest possible independence and continue living at home.
Professional home care in Switzerland is provided by public and private agencies and includes a wide range of services, such as assessment of care needs, basic care, examination, treatment, assistance in ADL, and help with household tasks.3,4 Home care services are covered by social health insurance when prescribed by a physician, but require significant co-payments from the user. Help with household tasks is covered only by private insurance. Home care for persons with SCI is characterized by a high degree of interprofessionalism, requiring close collaboration between general practitioners (GPs), specialists, hospitals, and other health care professionals.5,6 Switzerland is divided into 3 main language regions (German-, French-, and Italian-speaking parts) with distinct local cultures, and while there are no fundamental differences in the structure of health care, apart from cantonal variations due to political self-determination, subtle variations exist between the language regions in terms of health care expectations, beliefs, norms, and preferences.
The current model of home care has been criticized for its inability to adequately meet the complex care needs of persons with SCI.5,7 This is due to several challenges, including limited service availability, limited working hours, high staff turnover, and a lack of specialized knowledge and skills in the field of SCI. 8 Care for persons with complex chronic conditions tends to be uncoordinated and fragmented, leading to delayed access to necessary services, redundant service provision, or conflicting treatment plans.7,9 With successful care coordination, higher quality of care can be achieved, including improved clinical outcomes and higher levels of patient satisfaction. 10
Effective care coordination is essential for persons with SCI and can be carried out by health care professionals, such as home care nurses or GPs, as well as informal caregivers or the individual with SCI themselves.10 -13 In the general population, GPs are usually the first point of contact for care and therefore they have the best overview of patients’ social situations, comorbidities, and medications.13,14 However, for persons with SCI, Touhami et al. 15 highlighted that an SCI specialist may also be chosen as first contact for care, who can then manage and coordinate all aspects of care for persons with SCI. Persons with SCI who initially consulted with either a GP or an SCI specialist reported equal levels of satisfaction with the care received. 16
Patient satisfaction is a key indicator of service quality and is associated with better health outcomes and reduced health care costs. 17 Limited attention has been paid to understand patient satisfaction with care provision and rehabilitation services in persons with SCI.18 -21 To date, no studies have investigated the determinants of satisfaction with home care services for persons with SCI in Switzerland.
In this study, we aimed to quantify satisfaction with home care services among persons with SCI living in Switzerland and to determine the association between first contact for care, whether it be a GP or an SCI specialist, and having an informal caregiver with satisfaction with home care services. Based on the existing research discussed earlier, we hypothesize that the type of first contact for care will not significantly affect satisfaction levels, as both GPs and SCI specialists can effectively coordinate care for persons with SCI. However, we do expect to find a significant association between having an informal caregiver and satisfaction levels, with individuals who receive informal care being more likely to receive coordinated care and report higher levels of satisfaction with home care services.
Materials and Methods
Study Design and Study Population
Cross-sectional data were derived from the national community survey of the Swiss Spinal Cord Injury Cohort Study (SwiSCI), which was conducted between March 2017 and March 2018. 22 The survey was open to all Swiss residents who were over 16 years of age and living with either a traumatic or non-traumatic SCI. The study excluded persons with congenital conditions leading to SCI, new SCI in the context of palliative care, neurodegenerative disorders, and Guillain-Barré syndrome. 22 The study population was established using the registries of the 4 major specialized rehabilitation centers (Swiss Paraplegic Centre, Nottwil; REHAB Basel; Clinique Romande de Réadaptation, Sion; Balgrist University Hospital, Zurich) and 2 SCI support organizations in Switzerland (ParaHelp, Swiss Paraplegic Association). All individuals identified through these institutions were invited to participate in the study. The total number of eligible individuals invited to participate in the study was 3959, out of which 1294 completed the questionnaire (response rate 33%). 22 The study was approved by the Ethical Committee of Northwest and Central Switzerland (EKNZ, Project-ID: 11042 PB_2016-02608).
Measures
The outcome variable “satisfaction with professional home care” was assessed using a single item on a 5-point Likert scale asking participants: “How satisfied are you with the home care service?” Responses ranged from 1 (very satisfied) to 5 (very dissatisfied) and were dichotomized into 2 categories: 0 (very dissatisfied, dissatisfied, neither satisfied nor dissatisfied) and 1 (very satisfied, satisfied).
Participants were asked the question “Who is your first point of contact for health problems related to your spinal cord injury?” to identify the first point of contact for care. The response options included a GP, a medical specialist with private practice (referred to as “other specialist”), a medical specialist at one of the 4 paraplegic centers (referred to as “SCI specialist”), and other. A new variable was created by collapsing the categories “other specialist” and “other” into a single category.
Informal care was operationalized using 3 variables: living arrangement (living with someone/living alone), in a partnership (yes/no), and support from an informal caregiver in daily activities (yes/no).
Sociodemographic and SCI characteristics included participants’ age at the time of the questionnaire, gender (male/female), paid employment (yes/no), highest education level (compulsory/upper secondary level/tertiary), financial hardship (none/little/major), language region (German-/French-/Italian-speaking), years since injury, type of SCI (tetraplegia/paraplegia), and lesion severity (complete or incomplete loss of sensory or motor functions below the level of injury). The cause of SCI was categorized as traumatic (due to an external force) or non-traumatic (due to an underlying pathology). Functional level was assessed using the self-report version of the Spinal Cord Independence Measure (SCIM-SR). 23 The SCIM-SR score ranges from 0 to 100, with higher scores indicating greater independence.
Statistical Analysis
We conducted descriptive statistics to assess the characteristics of the sample and to compare satisfaction with professional home care across different subgroups, such as partnership status, living arrangement, support from an informal caregiver, and first contact for care. Differences between the groups were tested using the Student’s t-test, with p-values ≤ .05 considered statistically significant.
We used multivariable logistic regression to estimate the association between first contact for care and having an informal caregiver with satisfaction with professional home care services. The model was adjusted for socioeconomic factors, SCI characteristics, and functional level. Odds ratios (OR) with corresponding 95% confidence intervals (CI) were reported. We used multiple imputation (MI) by chained equations on 20 imputed datasets to address missing values, assuming that data were missing at random. All analyses were performed using Stata version 17.0 (StataCorp, College Station, TX, USA).
Results
Participants Characteristics
Of 1294 participants, 421 (33%) received professional home care and rated their satisfaction with the services (Table 1). The sample consisted of 280 men (67%) and 141 women (34%), with a mean age of 59 years (SD 15). Fifty-six percent of the respondents had paraplegia, 51% had an incomplete lesion, and 80% traumatic etiology. The mean time since injury was 19 years (SD 14). The GP was indicated by 38% of the respondents as first contact for care, and the SCI specialist by 43%. A small proportion of respondents (4%) chose another specialist, and 2% chose another health professional as first contact for care. The study participants frequently relied on informal care: 53% had a partner, and almost two-thirds (64%) lived with someone. In addition, 66% received support in ADL from an informal caregiver.
Participants’ Characteristics.
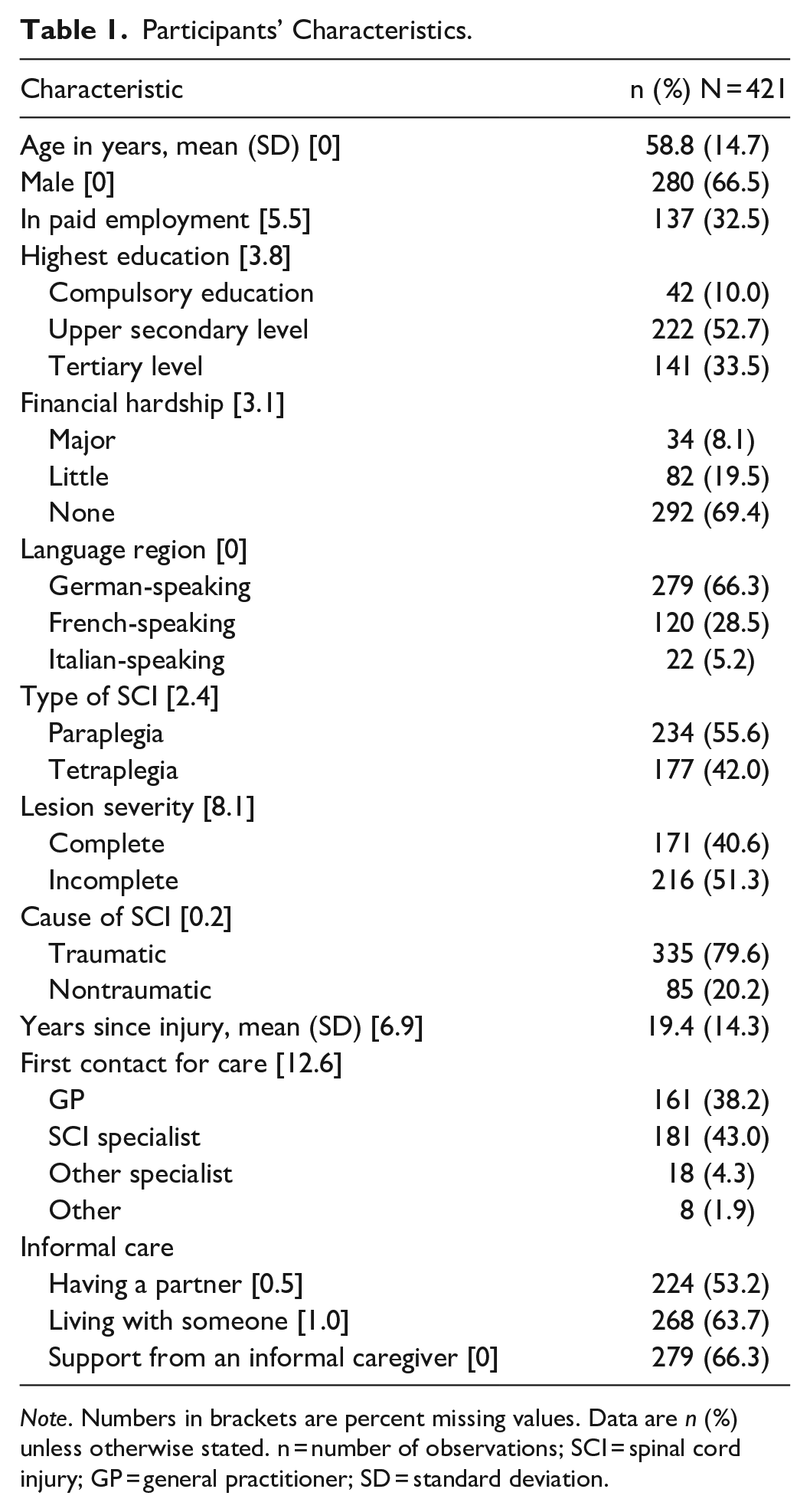
Note. Numbers in brackets are percent missing values. Data are n (%) unless otherwise stated. n = number of observations; SCI = spinal cord injury; GP = general practitioner; SD = standard deviation.
Satisfaction With Professional Home Care
The results suggest that overall satisfaction with professional home care was high, with 84% of participants reporting they were either very satisfied or satisfied. While 11% were neither satisfied nor dissatisfied, only a small percentage of participants (6%) reported being dissatisfied or very dissatisfied with the services they received.
Figure 1 displays the relative frequencies and mean values of satisfaction with home care services across different variables including partnership status, living arrangement, informal caregiver support, and first contact for care. Respondents who had a partner (mean 1.8 vs 2.0, p = .023) or lived with someone (mean 1.8 vs 2.1, p = .017) expressed statistically significantly higher satisfaction with home care services than to those who did not have a partner or lived alone. No statistically significant difference in satisfaction was found between those who received support from an informal caregiver compared to those who did not (mean 1.9 vs 2.0, p = .527), or between those who reported a GP as their first contact for care compared to those who reported a SCI specialist or another specialist/other (mean 1.9 vs 2.0, p = .570).
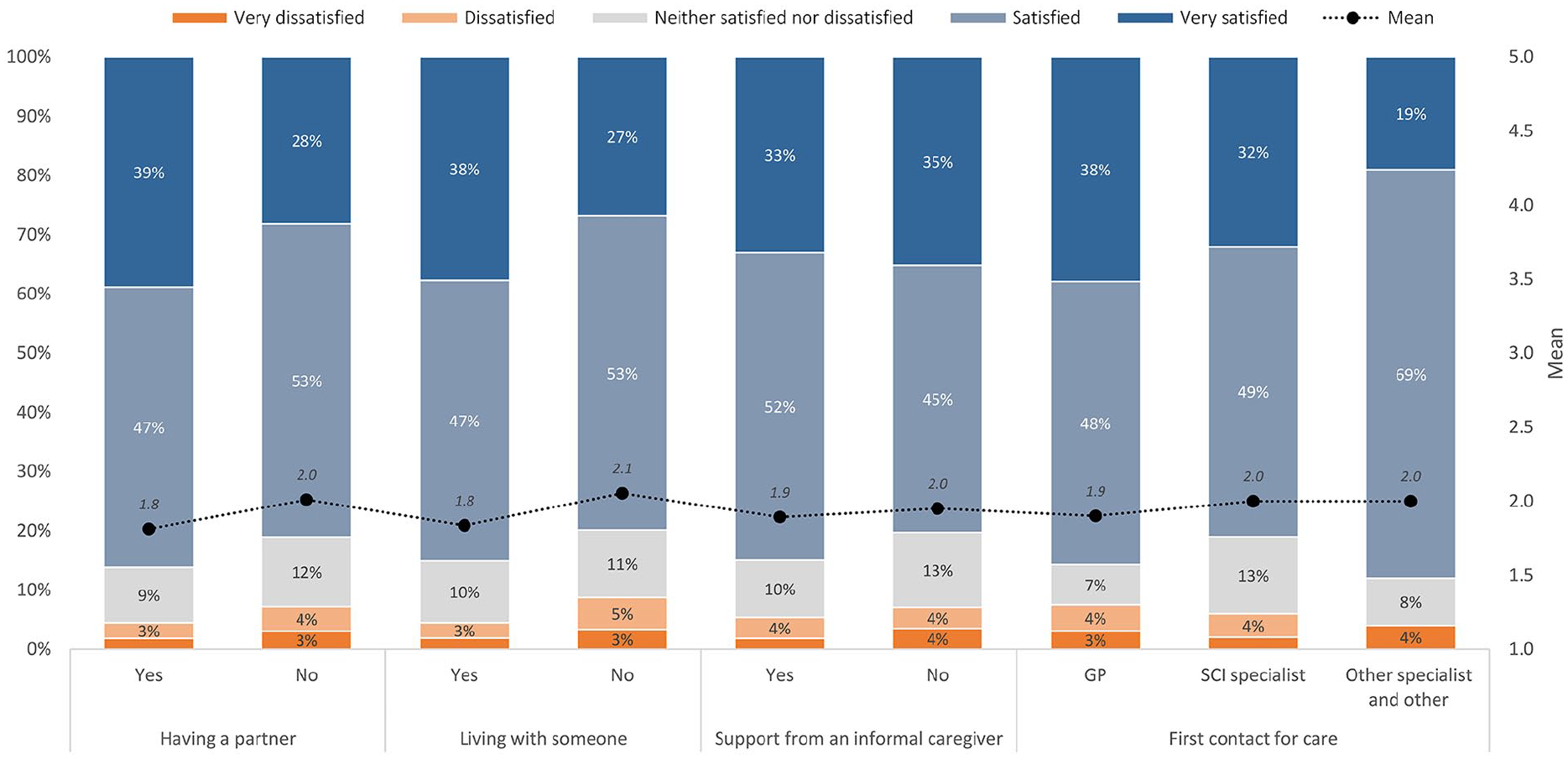
Satisfaction with professional home care (N = 421). Scale from 1 = very satisfied to 5 = very dissatisfied. The scale on the left Y-axis shows the percentage and the scale on the right Y-axis the mean value on the satisfaction scale.
Factors Associated with Satisfaction with Professional Home Care
Neither first contact for care nor informal care, that is, living with someone, having a partner, or receiving support from an informal caregiver, were statistically significantly associated with satisfaction with professional home care services (Table 2). The only factors statistically significantly associated with satisfaction were gender and language region. Women (OR 0.56, 95% CI 0.31-1.00) compared to men and persons living in the French-speaking part of Switzerland (OR 0.36, 95% CI 0.19-0.68) compared to person living in the German-speaking part of Switzerland were less likely to be satisfied with professional home care.
Satisfaction With Professional Home Care: Adjusted Logistic Regression Model.

Note. GP = General practitioner; SCI = spinal cord injury; ref = reference category; OR = odds ratio; 95% CI = 95% confidence interval.
p ≤ .01 *p ≤ .05. SCIM-SR: Scale from 0 to 100, higher numbers indicate higher functional independence.
Discussion
This study showed that persons with SCI living in the community in Switzerland who receive professional home care report high levels of satisfaction with home care. Specifically, 34% of participants outlined being very satisfied with home care, while 50% reported being satisfied. These findings are consistent with previous studies conducted in both the SCI population 18 and the general population 24 in Switzerland, which have also reported high levels of satisfaction with health care services.
We found no statistically significant association between first contact for care and satisfaction with home care services. This result underlines the need to define the role and collaboration between GPs and SCI specialists to optimize health care and avoid misunderstanding. 14 The hypothesis of a difference in satisfaction based on having an informal caregiver could not be confirmed. While the univariate analysis suggested that respondents who had a partner or lived with someone expressed higher satisfaction with home care than those who did not have a partner or lived alone, we did not find such a relationship in the multivariable regression model. The systematic review by Batbaatar et al. 25 found contradictory evidence regarding partnership status as a determinant of satisfaction with health care with some studies showing that married patients tend to be more satisfied with health care26,27 and other studies showing the opposite. 28
Our results showed a statistically significant association between gender and satisfaction with professional home care. Specifically, women had 76% higher odds of being dissatisfied with home care compared to men. This finding is consistent with other studies conducted in Switzerland, which have shown that men tend to be more satisfied with overall health care than women. According to a report by the Swiss Health Observatory, 29 20% of men are very satisfied with health care, compared to 17% of women. However, international evidence on gender differences in satisfaction with health care is mixed. Some studies suggest that women are more satisfied with health care, while others suggest that men are more satisfied, especially with aspects such as nursing care, comfort, visiting, and cleanliness. 25
One possible explanation for the observed gender differences in satisfaction with home care is that men and women may have different expectations and preferences for care. 30 For example, women may prioritize certain aspects of care, such as communication and emotional support, more highly than men, while men may prioritize aspects such as speed and efficiency of care. In addition, gender roles and societal norms may influence the way that men and women interact with home care providers and perceive the care that they receive. Furthermore, the deeply intimate nature of SCI care, such as assistance with toileting, bathing, and feminine hygiene, may uniquely affect satisfaction and perceived comfort, especially if care is provided by a caregiver of the opposite gender. Overall, the factors that contribute to gender differences in satisfaction with home care are complex and not fully understood. Further research is needed to better understand the potential causes of these differences and to identify strategies to improve satisfaction with home care for all persons with SCI, regardless of gender.
We found that persons with SCI living in the French-speaking part of Switzerland had 177% higher odds of being dissatisfied with home care compared to individuals living in the German-speaking part. According to Guillén et al., 31 several studies on various medical topics (e.g., organ donation, use of hearing aids, antibiotic consumption, patients’ needs in doctor-patient consultations) have shown cultural-based differences between the language regions. A report on the future of outpatient primary care in Switzerland 29 also found that persons from French- and Italian-speaking regions were significantly less satisfied with health care than persons from German-speaking regions. It remains unclear whether the differences in satisfaction with home care between the language regions reflect cultural differences or distinct care provisions. However, one possible explanation could be that in the French-speaking part of Switzerland, there may be less integration between home care providers and the wider health care system, particularly specialized SCI centers, which could impact coordination of care and communication between persons with SCI and providers.
No significant associations were found between various socioeconomic characteristics (including age, education level, financial hardship, functional independence) or SCI characteristics and satisfaction with home care. Although previous research has suggested that older individuals are more satisfied with health care services, our study did not find this relationship among persons with SCI. 20 Batbaatar et al. 25 reported that older patients tend to be more satisfied with health care services in primary care, especially if they prefer interpersonal care, and a study in the Swiss general population 29 showed that older persons are generally more satisfied with health care than younger persons. Ronca et al. 18 found that older persons with SCI tended to have a more favorable perception of care. Specifically, persons with SCI aged 61 years and older rated the availability and quality of health care 6% to 11% higher than younger individuals. 18
We did not find a significant association between education level or financial hardship and satisfaction with home care. However, previous research has shown that literate patients are generally more satisfied with primary health care services than those who are illiterate. 25 In addition, studies highlighted that among various socioeconomic variables, income is an important factor influencing satisfaction with health care. 25 Patients with a higher income tend to be more satisfied with overall health services, including access and technical quality, while those with lower income are more satisfied with nursing care. 25 In Switzerland, income and satisfaction with health care are positively correlated in the general population, with more persons in the lower income group reporting dissatisfaction with health care than in the highest income group. 24
Our study has several limitations, including the moderate sample size and the cross-sectional study design, which does not allow for causal inference. In addition, the SwiSCI survey did not collect detailed information, such as the duration of services received, which could influence satisfaction levels over time. Finally, our assessment of satisfaction was based on a single item rather than multiple items assessing specific aspects of home care. A single item provides only limited information about the reasons for satisfaction or dissatisfaction, making it difficult for health care providers to identify areas for improvement. In addition, using a single item may have resulted in a ceiling effect, where most individuals responded positively.
Conclusions
Persons with SCI receiving professional home care in Switzerland are generally satisfied with the service. Neither first contact for care nor the presence of an informal caregiver was associated with satisfaction with home care. Gender and language region were found to have a statistically significant association with satisfaction with home care, with women and individuals living in the French-speaking part of Switzerland being more likely to report dissatisfaction. Overall, the findings suggest the need for personalized and culturally sensitive home care that takes into account the different preferences and expectations of persons with SCI, especially regarding gender and language region.
Footnotes
Acknowledgements
We thank the SwiSCI Steering Committee with its members Xavier Jordan, Fabienne Reynard (Clinique Romande de Réadaptation, Sion); Michael Baumberger, Luca Jelmoni (Swiss Paraplegic Center, Nottwil); Armin Curt, Martin Schubert (Balgrist University Hospital, Zürich); Margret Hund-Georgiadis, NN (REHAB Basel, Basel); Laurent Prince (Swiss Paraplegic Association, Nottwil); Daniel Joggi (Representative of persons with SCI); NN (Parahelp, Nottwil); Mirjam Brach, Gerold Stucki (Swiss Paraplegic Research, Nottwil); Carla Sabariego (SwiSCI Coordination Group at Swiss Paraplegic Research, Nottwil).
Data Availability
Owing to our commitment to SwiSCI study participants and their privacy, datasets generated during the current study are not made publicly available but can be provided by the SwiSCI Study Center based on reasonable request (
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The present publication was funded by Swiss Paraplegic Research.
Ethical Considerations
Ethical approval for the SwiSCI Survey was granted by the leading ethical institution Ethics Committee Northwest and Central Switzerland (EKNZ 11042 PB_2016-02608, approved 21.12.2016). All survey participants provided written informed consent before agreeing to participate voluntarily. We certify that all applicable institutional and governmental regulations concerning the ethical use of human volunteers were followed during the course of this research.
Consent for Publication
Not applicable.