
Abstract
To determine the barriers, benefits, and enablers of acute home-based care in Australia for older people (aged 65 and over). A systematic review for people aged 65 and over receiving acute home-based care in Australia was conducted using various databases (CINAHL, Medline, PsycINFO, SCOPUS, Web of Science, PubMed, Informit) and citation searching in September 2023. The Critical Appraisal Skills Program (CASP) was used to assess the quality of the evidence and a thematic analysis approach was utilized to narratively synthesize results. Ten studies were included, consisting mostly of cohort studies in metropolitan areas. Barriers included inefficacy, patient demographics, and carers. Benefits included efficacy, high satisfaction, and medical management. Enablers included education, holistic assessments, and support interventions. Within the literature there was a significant research gap regarding HITH for older people in rural areas of Australia. Patient outcomes were closely aligned with admission pathways.
Background
Acute home-based care is utilized internationally and in Australia. Acute home-based care was formally introduced in Australia during the 1994 Hospital In The Home (HITH) pilot in Victoria. 1 Following the success of this trial, implementation of acute home-based care continued across Australia. Since then acute home-based care services have further expanded to enable remote delivery for a variety of non-acute inpatient and day procedure services in the home including chemotherapy, palliative care, Geriatric Evaluation & Management (GEM), and rehabilitation.2 -5 In the 2020 to 2021 Victorian budget, “Better at Home” funding was introduced to increase availability of acute, subacute, and rehabilitation care provided at home across Victoria highlighting its central importance to the healthcare landscape. 6
In the context of differences in healthcare systems and associated funding models, definitional consistency remains elusive and challenges the interpretation and application of the findings within the literature. Within Australia acute home-based care varies between states, operating under different funding models, and utilizing different models of care and service titles, 7 has increased the difficulty of comparing and interpreting Australian acute home-based care literature. Throughout this article acute home-based care is synonymous with HITH and the term will be used throughout this review to be inclusive of all acute home-based care models. Further complicating the synthesis of data, is the lack of consistency. HITH admission pathways are not universally reported and as a result there as conflicting results regarding the efficacy of HITH, difficulties finding and interpreting the literature, and confusion regarding patient eligibility for HITH.
There are generally 2 types of admission pathways to HITH services, direct admissions and transferred admissions. Direct admissions originate from the community, general practitioner or Emergency Department, known in the literature as Admission Avoidance (AA) to avoid an acute in hospital admission8,9 or Pure HITH.10,11 It is important to note that although admission avoidance infers the patient is not admitted they are an inpatient at a health service admitted to HITH. Transferred admissions on the other hand are admissions that are transferred to HITH following an inpatient admission, known as Early Supported Discharge (ESD)8,12 or Mixed HITH.10,11 The ESD admission pathway uses the word “discharge” even though the patient retains their inpatient status while receiving acute care at home. In addition, Australian acute home-based care varies between states and between health services which utilize different models of care, funding sources, and service titles. 7 Further confounding this is an expanding variety of HITH that has triggered an assortment of terminology, models and definitions within both the domestic7,10,13,14 and international literature.12,15 -17 These nuances in language, lack of specificity regarding admission type across the breadth of literature,11,18 differences in healthcare systems and associated funding models, challenge the interpretation and application of the findings within the literature to compare the outcomes of acute home-based care literature.
Older people make up the majority of in hospital patients, yet research has demonstrated older people using HITH had a lower risk of delirium and nosocomial infections. 19 While findings are promising, limited HITH research within Australia targets older people, meaning the real-world challenges and benefits are mostly unknown. Similarly, as the majority of research has been completed in metropolitan areas, the experience of older people in the rural health setting is limited. This is important because, 28% of the Australian population live outside of metropolitan areas and experience lower life expectancy and have an increased burden of disease.20,21 While many lessons can be learnt from HITH in metro areas, unique challenges are faced by rural communities and as such rural research is needed.
It is currently unknown if HITH improves access to healthcare for older people in Australia and provides them with the opportunity to overcome healthcare barriers. Therefore, the purpose of this systematic review is to determine the benefits, barriers, and enablers of acute home-based care (HITH) for older people (aged 65 and over) in Australia.
Methods
This systematic review was completed in accordance with the recommendations of the “Preferred Reporting Items for Systematic Review and Meta-Analyses” 2020 (PRISMA). 22 The review protocol was registered in the “International Prospective Register of Systematic Reviews” (PROSPERO) in 2023 (ICRD42023408825). There were no other protocols regarding HITH for older people in Australia at the time of registration.
Data Sources and Searches
The search strategy utilized key terms relating to “home-based care,” “older people,” and “Australia.” Test searches were completed by the lead author to determine the efficacy of the search strategy. The search strategy and results were reviewed by a senior Librarian to ensure comprehensive results. The inclusion and exclusion criteria were determined by all authors. A search was performed in September 2023 using CINAHL, MEDLINE, PsycINFO, SCOPUS, Web of Science, PubMed, and Informit to obtain all primary research articles. There was no limitation applied to the years of publication to ensure all acute home-based literature could be included. Extensive citation searching, and review of author publications were completed to identify any potentially missed papers. Comprehensive search strategies used for this review are available in Supplemental Document 1.
Study Eligibility Criteria and Selection
The inclusion criteria were, (1) People aged 65 and over who were living at home. (2) Delivery of acute care by health professionals, within the admitted patient’s home, who would otherwise require acute inpatient admission. (3) The care was delivered within Australia.
Studies were excluded if the population only included residents living within a nursing home, as these patients would have access to a higher level of care and supervision in comparison to patients living in their homes. Studies were excluded if the services were provided following discharge (district nursing and post-acute care [PAC]) or as an outpatient service (rehabilitation at home, chemotherapy at home, dialysis at home, and palliative care at home) as these patients would not classify as an acute admission.
The initial literature search was completed by the lead author. Covidence was used to remove duplicates and for the title and abstract screening, full text review, and conflict resolution. 23 Title and abstract screening was completed by the lead author, and the full text review was completed by 3 authors. Minimal conflicts were identified during the screening process, conflicts were resolved by the JB. Additional articles were included following the citation search (completed by lead author), as decided by all authors.
Data Extraction
The lead author completed data extraction for all included studies using a customized table within Covidence. Data extraction included the participant data (sample size, demographics including age), health service data (state and town, classification as metropolitan or non-metropolitan, size and description of health service), study design, and HITH findings (admission type, patient admission outcomes, carer experience, impact on health service).
Evaluation of Scientific Evidence
The methodological quality of the articles were assessed by all authors using the Critical Appraisal Skills Programme (CASP) randomized controlled trial, 24 cohort, 25 and qualitative 26 checklists. The CASP checklist allows researchers to assess the validity of the study and identify limitations and bias. Each checklist specifically correlates to the methodology of the study to assess methodological rigor. Each article was reviewed by the lead author to assess methodological quality, results were then reviewed by all authors to ensure agreement of inclusion.
Data Analysis and Synthesis
The literature was examined utilising a Braun and Clarke approach to thematic analysis with findings classified as a barrier, benefit, or enabler for older people in HITH. 27 The synthesis was discussed with all authors until a consensus was reached.
Primary and Secondary Outcomes
The primary outcomes of this systematic review were to describe the barriers, benefits, and enablers of HITH for older people in Australia. The barriers, benefits and enablers were those highlighted within the included literature impacting patients or carers or impacted the efficacy of HITH. The secondary outcomes were to compare the location of the health service (metropolitan, non-metropolitan, or unknown) and the admission pathway (direct admission, transferred admission, or unknown).
Definitions
As there was no universal term for acute home-based care services or the different admission pathways within the literature, the following terms were used throughout this review.
Hospital In The Home (HITH), to be inclusive of all discussed acute-home-based care services within this review.
Direct Admission (DA), patients admitted to HITH from a non-admitted or non-inpatient setting including the Emergency Department, General Practice, or Specialist Rooms.
Transferred Admission (TA), patients transferred to HITH from an inpatient or in-hospital ward.
All HITH Pathways (All HITH), admission location not reported and therefore may be either a direct and transferred admission pathways or both.
If the location was stated as metropolitan or rural, they were classified as such. If rurality was not disclosed, it was classified as unclear. Readmission within 28 days was classified as any type of readmission following discharge. Treatment failure was classified as requiring transfer to in hospital care during HITH admission.
Results
A total of 1241 records were identified through database searches and 105 were identified through citation searching. Following removal of duplicates, citation searching, screening, and full text review, 10 articles were included in the systematic review. The Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) flow diagram (Figure 1) details the selection process utilized within this review.
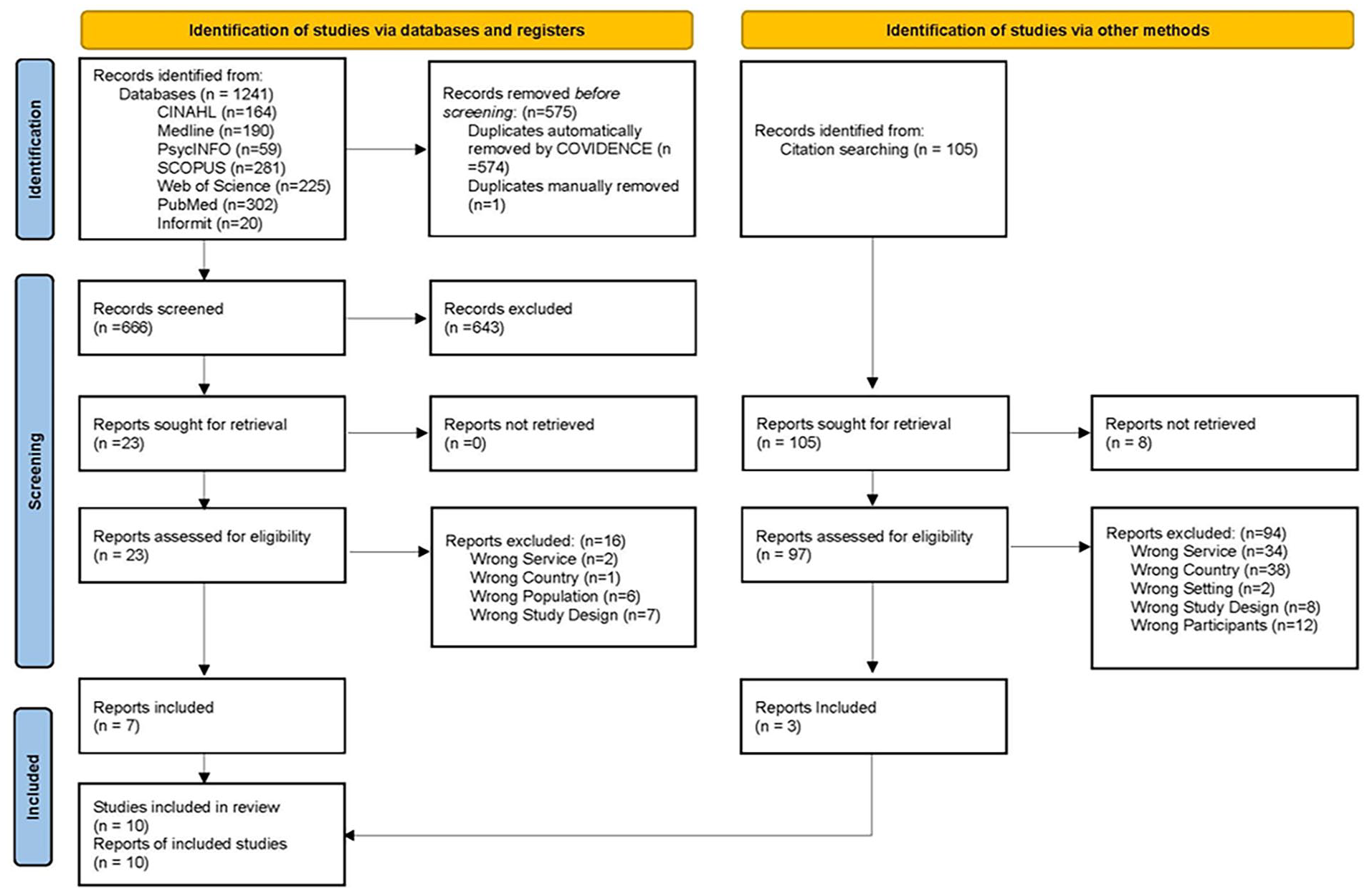
Flow diagram. 22
The majority of included articles were cohort studies (n = 8). There was 1 Randomized Control Trial (RCT), and 1 qualitative descriptive study. The sample sizes varied from 100 to 3552, and included admissions to HITH Australia wide, and in the states of Victoria, South Australia, and New South Wales. A summary of the study characteristics is provided in Table 1. Most of the research was completed using a metropolitan population (n = 7), 1 study was inclusive of metropolitan and non-metropolitan (rural) participants, and 2 studies did not identify the location. No studies targeted regional or rural populations solely.
Study Characteristics.
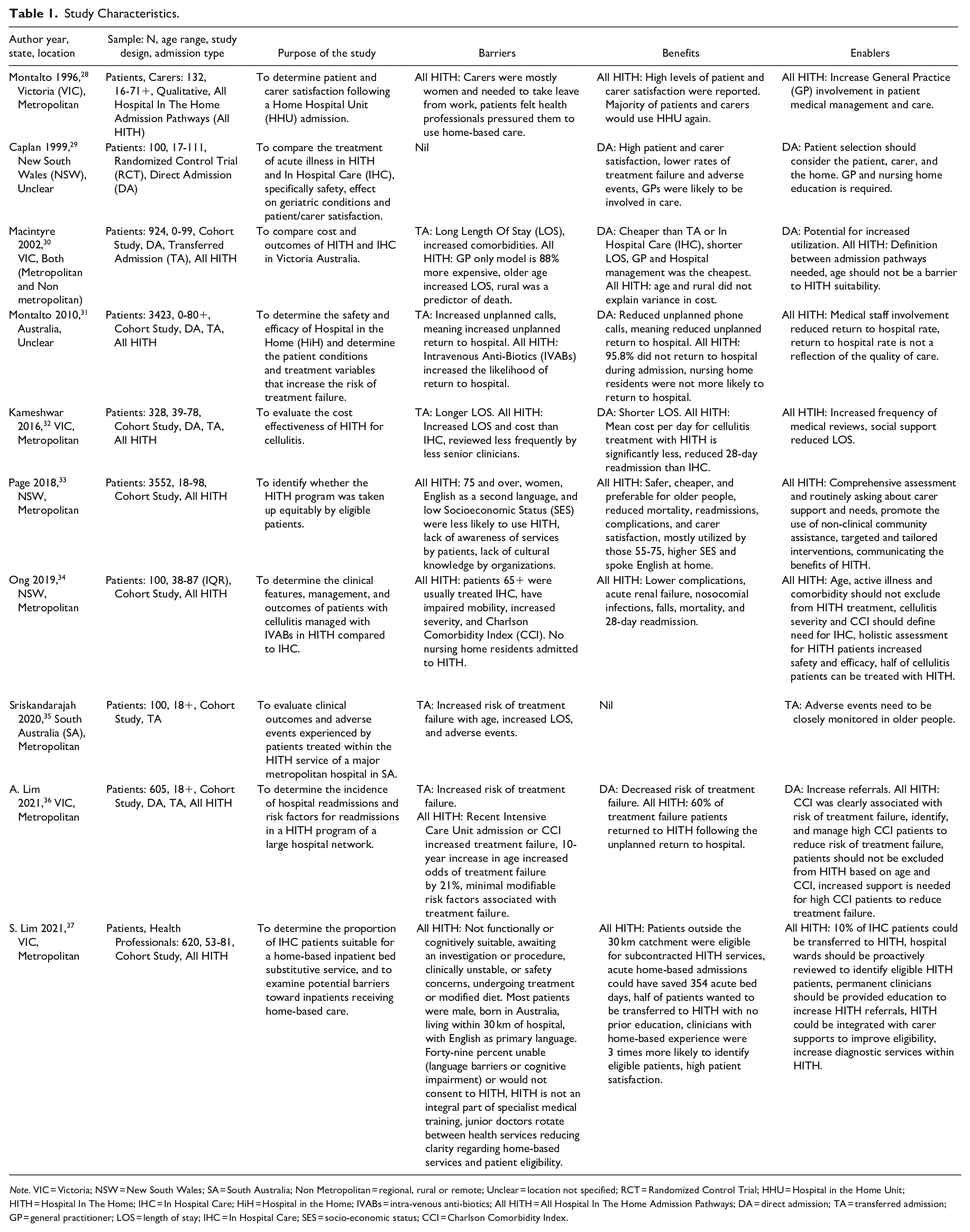
Note. VIC = Victoria; NSW = New South Wales; SA = South Australia; Non Metropolitan = regional, rural or remote; Unclear = location not specified; RCT = Randomized Control Trial; HHU = Hospital in the Home Unit; HITH = Hospital In The Home; IHC = In Hospital Care; HiH = Hospital in the Home; IVABs = intra-venous anti-biotics; All HITH = All Hospital In The Home Admission Pathways; DA = direct admission; TA = transferred admission; GP = general practitioner; LOS = length of stay; IHC = In Hospital Care; SES = socio-economic status; CCI = Charlson Comorbidity Index.
Risk of Bias and Overall Grading of the Scientific Evidence
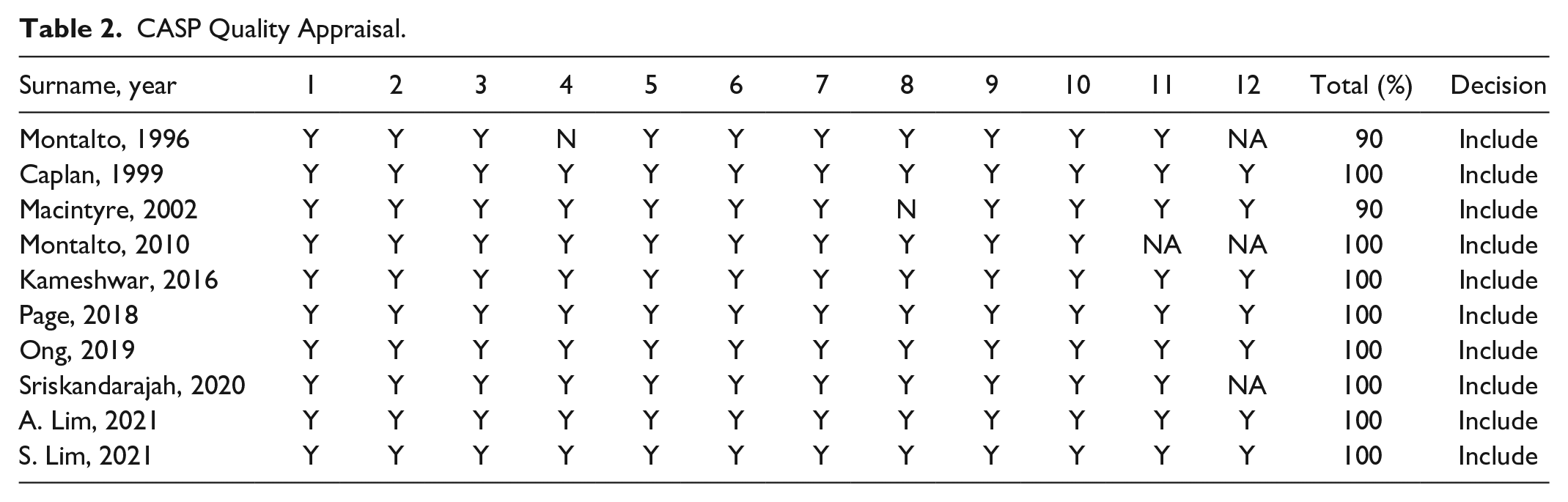
All included articles were assessed using CASP and showed low risk of bias for all applicable criteria regarding the study design.24 -26 After assessing the quality of evidence for each outcome across the included studies, the evidence was assessed to have a low risk for each outcome. All included articles were assessed as being of high quality (90% or above), as demonstrated by Table 2.
CASP Quality Appraisal.
Synthesis of the Results
By synthesizing study design and acute home-based health care characteristics, clear identification of the barriers, benefits, and enables of HITH was achieved. Results were then separated into location (metropolitan, metropolitan, and non-metropolitan [both], non-metropolitan, and unclear), and categorized according to admission type (direct HITH admission, transferred HITH admission, direct, and transferred HITH admission). Table 3 provides a synthesis of the results according to location and admission type. The findings have been narratively summarized below as barriers, benefits, and enablers using the Braun and Clarke 27 approach, and included themes and subthemes as demonstrated in Table 3.
Synthesis of Results.
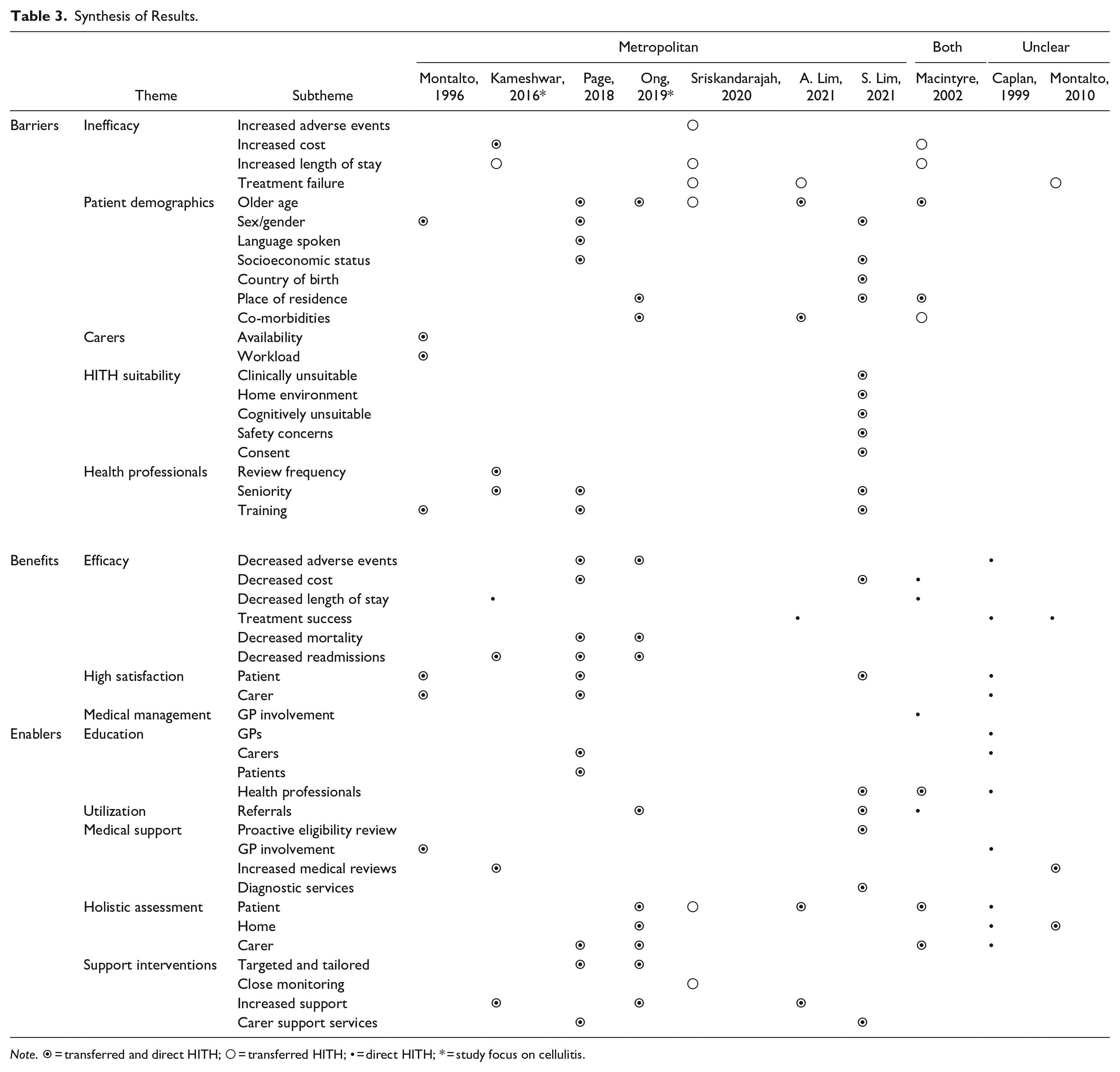
Note. ⦿ = transferred and direct HITH; ○ = transferred HITH; • = direct HITH; * = study focus on cellulitis.
Barriers
The reported barrier within Hospital in the Home care for older people was age.30,33 -36 However multiple studies included recommendations stating patients should not be excluded from HITH based solely on age.29,30,34,36 Multiple patient demographics were highlighted as barriers of HITH, such as gender, country of birth, and language spoken. However as all demographics were considered as individual factors, no study utilized an intersectional approach to understand if intersecting demographics (such as age and gender) further increased barriers of HITH care for these patients.
Benefits
Benefits were consistently reported for direct HITH admissions, and all HITH admissions. High satisfaction was the most commonly reported benefit among older HITH patients28,29,33,37 and their carers.28,29,33 The decreased incidence of adverse events,29,33,34 readmissions,32 -34 and reduced length of stay30,32 may have improved the perception and experience of HITH admissions.
Enablers
To overcome age being considered a barrier for HITH admissions, a need for the utilization of a holistic assessment for patients29,30,34 -36 and carers,29,30,33,34 was consistently reported. To mitigate risk from HITH admissions, increased support32,34,36 and carer support services33,37 could be utilized.
To overcome health professional related barriers of HITH, education was frequently reported for health professionals,29,30,37 as increasing awareness of and referrals to HITH for older patients.30,34,37 Increasing medical support for older HITH admissions through GP involvement,28,29 and increased medical reviews1,32 may improve outcomes further for older HITH admissions.
Discussion
While previous reviews of HITH have been completed,9,12,14,38 these reviews have utilized only Randomized Control Trials, and compared international HITH models. This systematic review narratively synthesizes the barriers, benefits, and enablers of HITH care for older people within the Australian context. As one-third of the Australian population live in non-metropolitan areas, 20 it is essential that research considers their experience of healthcare, and how that experience may differ for older people in these areas. While MacIntyre et al 30 included rural older people in their study population, sub-analysis only considered the rural location as a risk factor. As sufficient detail regarding these rural location characteristics was not included, findings from this study are unable to be generalized to older people in rural communities of Australia. 39
While patients and carers were considered in multiple studies, only one study from 1996 interviewed older patients and their carers to understand their experience. 28 Therefore, the contemporary Australian perceptions and experiences of older HITH patients and their carers, including the barriers, benefits, and enablers remain unknown. Recent international qualitative literature discusses barriers for older people in HITH such as technology, social roles, and decision making,40,41 as such, it would be interesting to understand if these barriers are reflected within the Australian context, and further if they are amplified within rural areas.
Reporting of HITH outcomes is inconsistent with some studies suggesting HITH is more expensive30,32 and others stating it is cost effective.30,33,37 However, the synthesis of results for this systematic review has demonstrated the importance of classifying the admission type, and further the utilization of clear definitions. This review has clearly demonstrated increased barriers for older people regarding transferred HITH admissions, and increased benefits for older people admitted directly to HITH. This is most likely due to the increased risk of complications older people face when admitted to hospital,42,43 which can be avoided using a direct HITH admission where appropriate. Further, as all research has considered older people as a homogenous group, it is likely that additional barriers, benefits, and enablers exist for certain populations within this group. Utilizing an intersectional lens in future research of older people in HITH would honor the heterogeneity of this population, might go some ways towards overcoming this issue. 44
Implications for Research and Practice
Future HITH research must explore the experiences of older people and their carers, utilizing an intersectional approach. Increasing HITH accessibility for older people will allow them to remain in their homes longer, maintain autonomy of their care and has the potential to improve quality of life within Australia. Increased synergy is needed regarding the terminology used within acute home-based care and in hospital care to increase the ability for health professionals to incorporate research findings into practice and home healthcare management. Further increasing effective admissions to HITH could reduce strain on hospital services, especially in rural areas.
Limitations
Some primary studies may have been missed due to the variations of terminology used to describe HITH between health services and Australian states and territories. However, extensive citation searching, and review of included articles were completed to minimize this. The gray literature was also excluded. Further, as the models of care were scarcely reported within the literature they have not been considered within this review. Understanding the models of care utilized within Australia may further shed light on how HITH can be utilized for older people, and those in rural areas.
Conclusion
This systematic review collated all Australian research regarding people aged 65 and over, receiving care via HITH. The lack of research regarding older people, especially those in rural areas highlights an important research gap within Australian literature and has the potential to impact future practice and the standard of care for older people. Clear definitions of admission pathways, and healthcare outcomes are required to ensure future research can be effectively utilized by researchers and health professionals both in Australia, and internationally. Many of the problems identified from this review center around synthesis of the outcome data. It is possible that an intersectional lens might go some way toward helping to frame the ways in which barriers and enablers to HITH participation by older people are considered and provide avenues for more targeted interventions, such as for those in rural areas. Not only will this increase knowledge of rural populations, but it will also increase the quality of HITH care provided in rural areas for older people.
Supplemental Material
sj-docx-1-hhc-10.1177_10848223241252931 – Supplemental material for Barriers, Benefits, and Enablers of Acute Home-Based Care (Hospital In The Home) in Australia for Older People: A Systematic Review
Supplemental material, sj-docx-1-hhc-10.1177_10848223241252931 for Barriers, Benefits, and Enablers of Acute Home-Based Care (Hospital In The Home) in Australia for Older People: A Systematic Review by Natalie J. Bransgrove, Joanne E. Porter, Blake Peck and Jaclyn Bishop in Home Health Care Management & Practice
Footnotes
Author Contributions
NB was responsible for the search strategy, identification, screening, full text review, extraction, analysis, writing, and editing the systematic review article. JP, BP, and JB were responsible for full text review, review of analysis, and editing the systematic review article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Commonwealth funded MRFF Rapid Applied Research Translation Grant (RARUR000072). NB is supported by an Australian Government Research Training Program (RTP) Stipend and RTP Fee-Offset Scholarship.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.