
Abstract
Palliative care is a comprehensive approach aimed at improving the quality of life of patients with serious illness and their families. Nevertheless, there exists a dearth of systematically synthesized empirical evidence regarding the key elements that contribute to good home palliative care (HPC) from a familial standpoint in the context of South and Southeast Asia. This paper aims to describe family perspectives on key elements of good home palliative care in both regions. We conducted a scoping review using Arksey and O’Malley’s methodological framework. The search was done in 6 electronic databases: PubMed, Ovid MEDLINE, EMBASE, Web of Science, APA PsycINFO, and APA PsycArticles Full Text. Inclusion criteria were (1) exploring family experiences of palliative care, (2) home setting, and (3) South and Southeast Asian countries. Twenty-four studies were included from Bangladesh (n = 1), India (n = 6), Indonesia (n = 7), Malaysia (n = 2), Singapore (n = 2), and Thailand (n = 6). Five key elements of HPC from family perspectives were comprehensive moral and psychological support; religious and spiritual activities with religious figures involvement; empathetic, responsive, and continued home palliative care; adequate access to information and skills training; and facilitation in dealing with systemic barriers. The crucial role of religious and spiritual activities and the need for facilitation in facing systemic barriers were specific to South and Southeast Asia. HPC teams should be able to provide holistic support for patients and their families, which is influential for the quality of care. Improving care on a systemic level in these regions should be a policy priority.
Introduction
Palliative care is an essential part of cancer and other serious illnesses, aiming to improve the quality of life for patients and their families.1,2 The concept of palliative care is widely discussed in the global north. In South and Southeast Asia, where our research is focused, palliative care availability and support are limited, except for Singapore. 2 Challenges include a lack of supportive policies, limited medication, inadequate education and training, insufficient resources, and difficulties in reaching remote areas.2,3
Given this lack of professional care, the role of the family is crucial. The patient returns home after medical appointments or any inpatient care they receive, then is cared for by family at home. In one study in Asia, home was reported as a comfortable environment for patients, especially with the presence of family members. 4 An integrative review of Southeast Asian studies found that receiving care and dying at home gave patients the sacred opportunity to be in a familiar place with beloved people. 5 A narrative review involving studies from high-income countries showed that the availability of professional home palliative care improves patients’ quality of life and care satisfaction. 6
Previous literature had described several important components of home palliative care from high-income countries such as in Europe and North America. These components were integrated teamwork; management of pain and physical symptoms; holistic care; caring, compassionate, and skilled providers; timely and responsive care; and patient and family preparedness. 7
Nevertheless, there exists a dearth of systematically synthesized empirical evidence regarding the key elements that contribute to good home palliative care from a familial standpoint in the context of South and Southeast Asia, especially with the regions’ specific nuances and circumstances. This paper is part of a more extensive study that explores the conceptualization and practice of home palliative care in rural Indonesia. Due to a scarcity of Indonesian studies, we include literature from the broader region of South Asia and Southeast Asia. This expansion of geographical coverage is justified by the similarity of demographic characteristics as well as some of the cultural norms and values, such as the important role of the family in providing care and the role of religion.8-17
This paper aims to describe family perspectives on key elements of good home palliative care in South and Southeast Asia. By directly analyzing how family experience home palliative care, we would benefit from the empirical data from a familial stand point that contribute to a good home palliative care. Increased knowledge about this topic will help improve the development and implementation of home palliative care in both regions.
Methods
Design
This paper is a scoping review, which aims to systematically identify and map the available literature and clarify key concepts and characteristics across different sources of evidence related to a particular topic. 18 We followed the methodological framework for a scoping review published by Arksey and O’Malley 19 : identifying the research question, identifying relevant studies, selecting studies, data charting, and finalization. This review is reported according to PRISMA Scoping Review guidelines. 20 Because of the nature of scoping reviews, ethical approval is not required.
Search Strategy
We conducted a comprehensive search to gather relevant studies for this review. Our search strategy involved using specific terms related to palliative care, family caregivers, home care, and South and Southeast Asian countries. We employed truncation and Boolean logic to ensure accurate retrieval of relevant studies. There were no restrictions on the publication dates. The countries included in this review are Afghanistan, Bangladesh, Bhutan, India, Maldives, Nepal, Pakistan, Sri Lanka, Indonesia, Malaysia, Singapore, Thailand, Vietnam, Myanmar, Laos, Brunei, Philippines, East Timor, and Cambodia.
The search was completed on April 18, 2023, across 6 electronic databases: PubMed, Ovid MEDLINE, EMBASE, Web of Science, APA PsycINFO, and APA PsycArticles Full Text. Access was facilitated by the library of Amsterdam UMC location AMC. Supplemental File 1 provides more details on the search strategy.
Data Extraction and Analysis
The flow diagram illustrating the process of study identification, screening, and inclusion is presented in Figure 1. The eligibility criteria for the included studies in this review were as follows: (1) exploration of family experiences of palliative care; (2) conducted in a home setting; (3) conducted in South and Southeast Asian countries. Case reports, conference abstracts, reviews, and clinical trials were excluded. The screening and selection of studies were facilitated using EndNote 20. Following critical feedback from all authors on the search strategy, the first author conducted the search, selected relevant studies, and thoroughly read the full-text papers multiple times. The results were organized in data extraction tables and summarized using thematic analysis. 21 All authors participated in thematic analysis. The methodological quality of each article was not assessed as this study is not a systematic review.
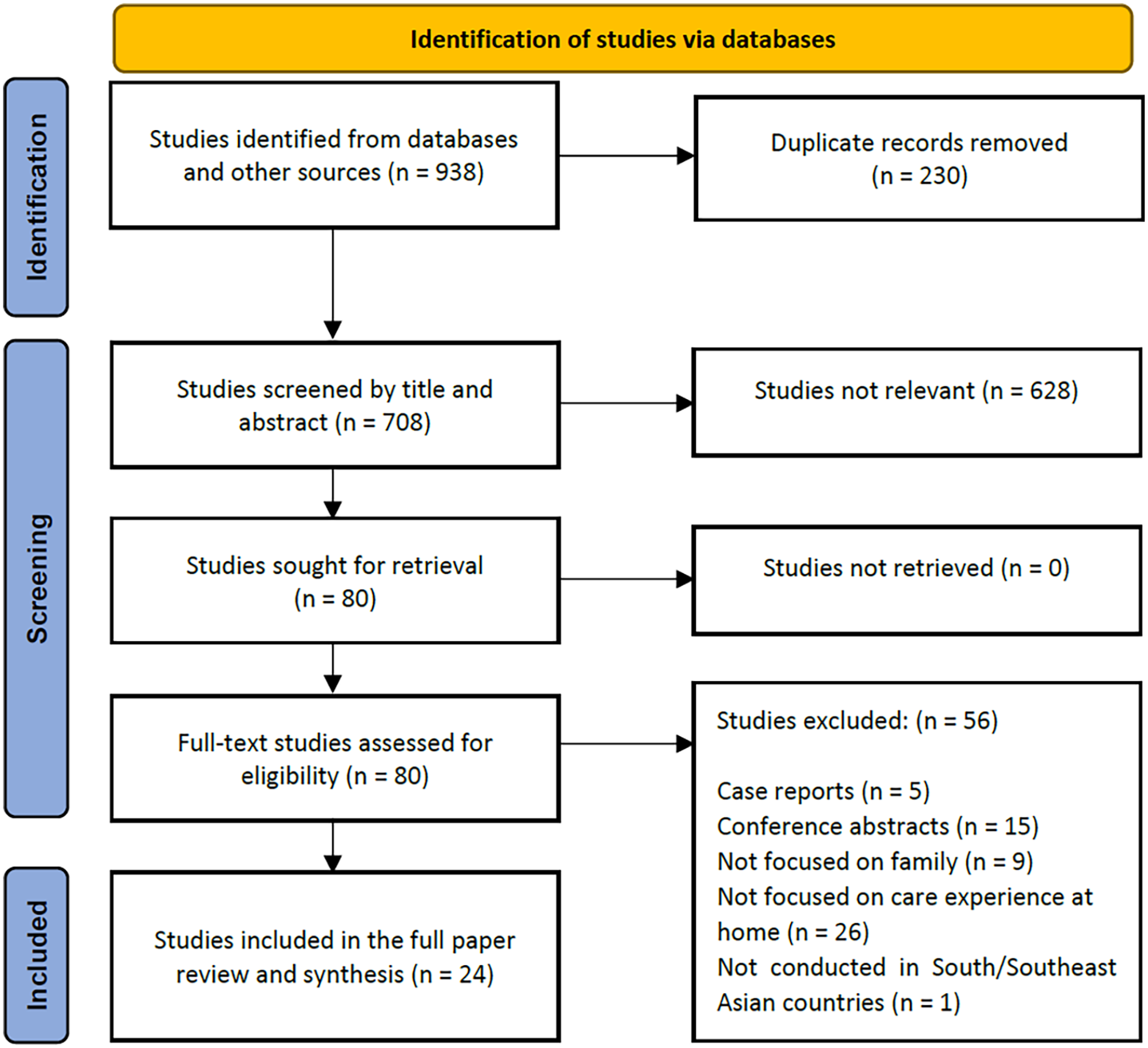
PRISMA flow diagram.
Results
Range of Studies
Out of 938 studies, 230 duplicates were identified and deleted. The first phase of the screening was through the title and abstract. In the second phase of the screening, the full text of 80 articles was retrieved to assess the eligibility. We included 24 studies in this review. A mapping of the studies based on their aims, methodology, and patient characteristics is presented in Table 1. Seventeen studies (71%) were from Southeast Asian countries and 7 studies (29%) from South Asian countries. There were seven Indonesian, two Malaysian, two Singaporean, 6 Thai, one Bangladeshi, and six Indian studies.
Summary of Study Characteristics.
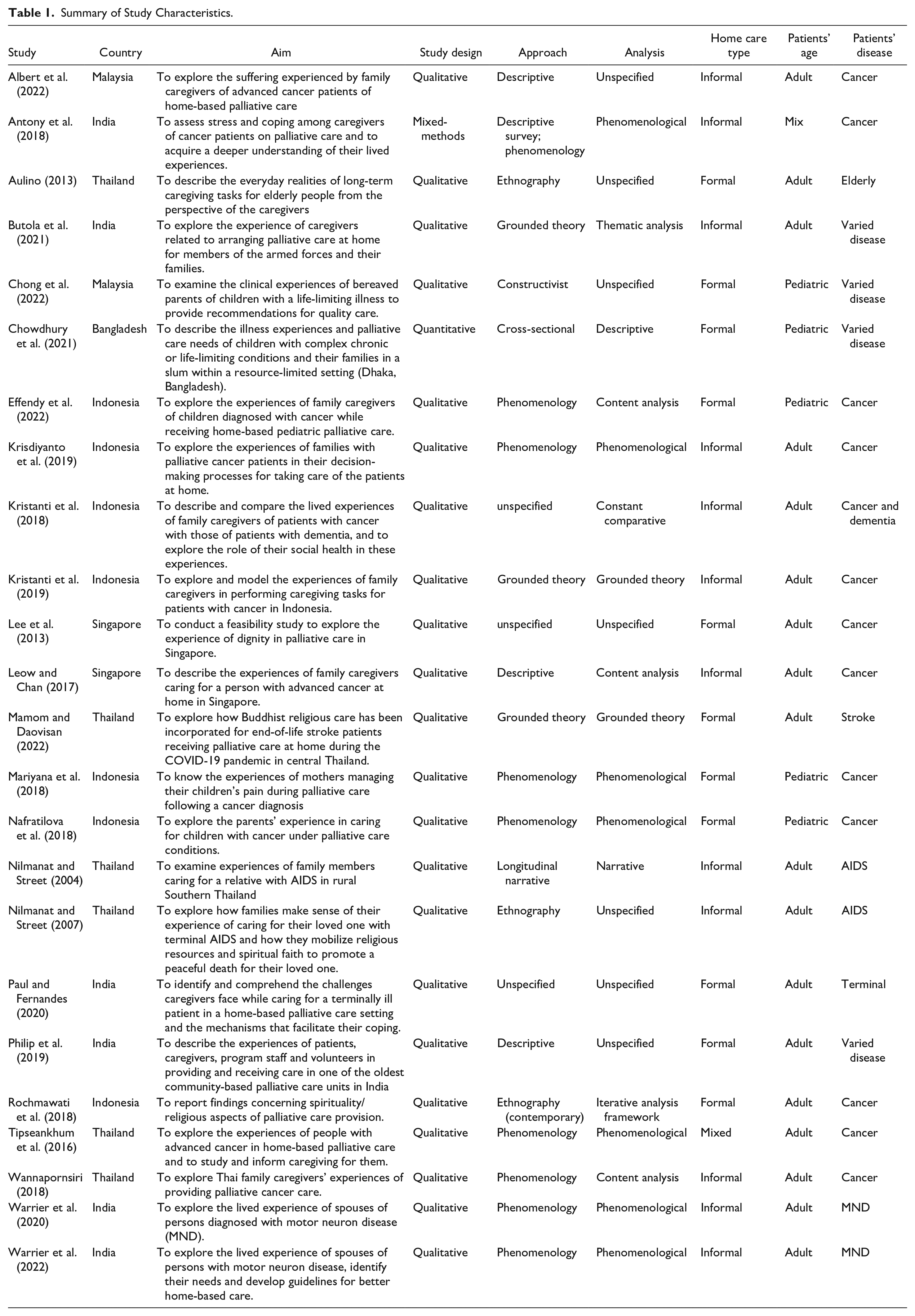
All the studies aim to explore family caregivers’ experiences while providing home palliative care. Eleven studies (44%) involved families of patients who received formal home palliative care, while the rest (56%) explored informal care provided solely by the family caregiver. Twelve studies involved the families of patients with cancer, 2 studies with a patient with AIDS, and 4 studies with patients with a neurology disorder. The rest of the studies involved families of terminal patients with various diseases. Qualitative research methods with different approaches were used by 23 studies (96%) in this scoping review. One mixed-method study used both a quantitative descriptive-survey study and qualitative phenomenology.
Study Settings
The reviewed studies were conducted in various locations. Indonesian studies were primarily based in the capital cities such as Jakarta, Surabaya, and Yogyakarta. Studies on other countries were also conducted in metropolitan areas such as Bangkok, Thailand, and Kuala Lumpur, Malaysia. In India, studies were conducted in Kerala, Mumbai, and Bangalore. Thai studies covered various regions. One study from Bangladesh focused on a resource-limited area in the capital city of Dhaka. The remaining studies’ location were not specified.
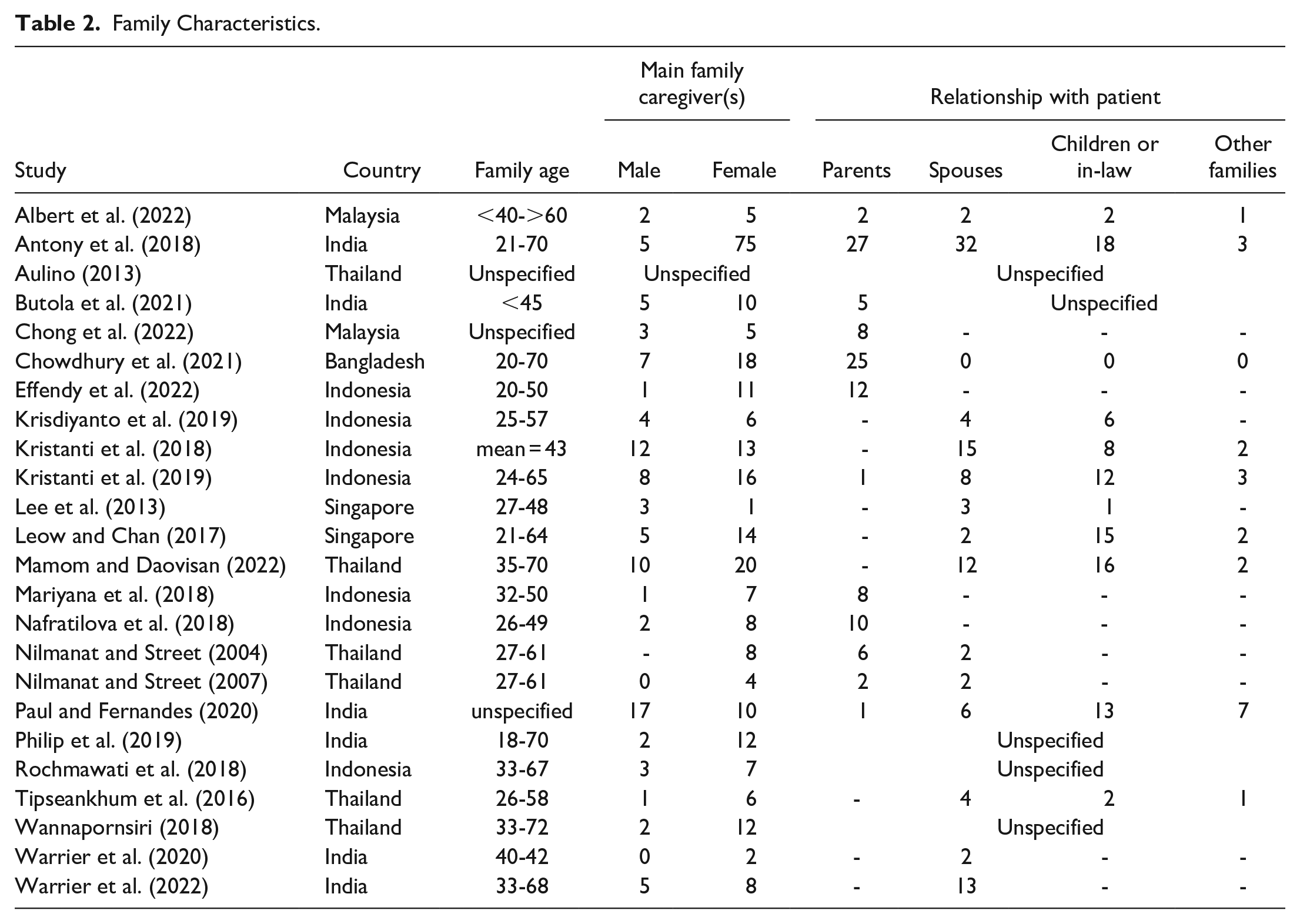
Family Characteristics
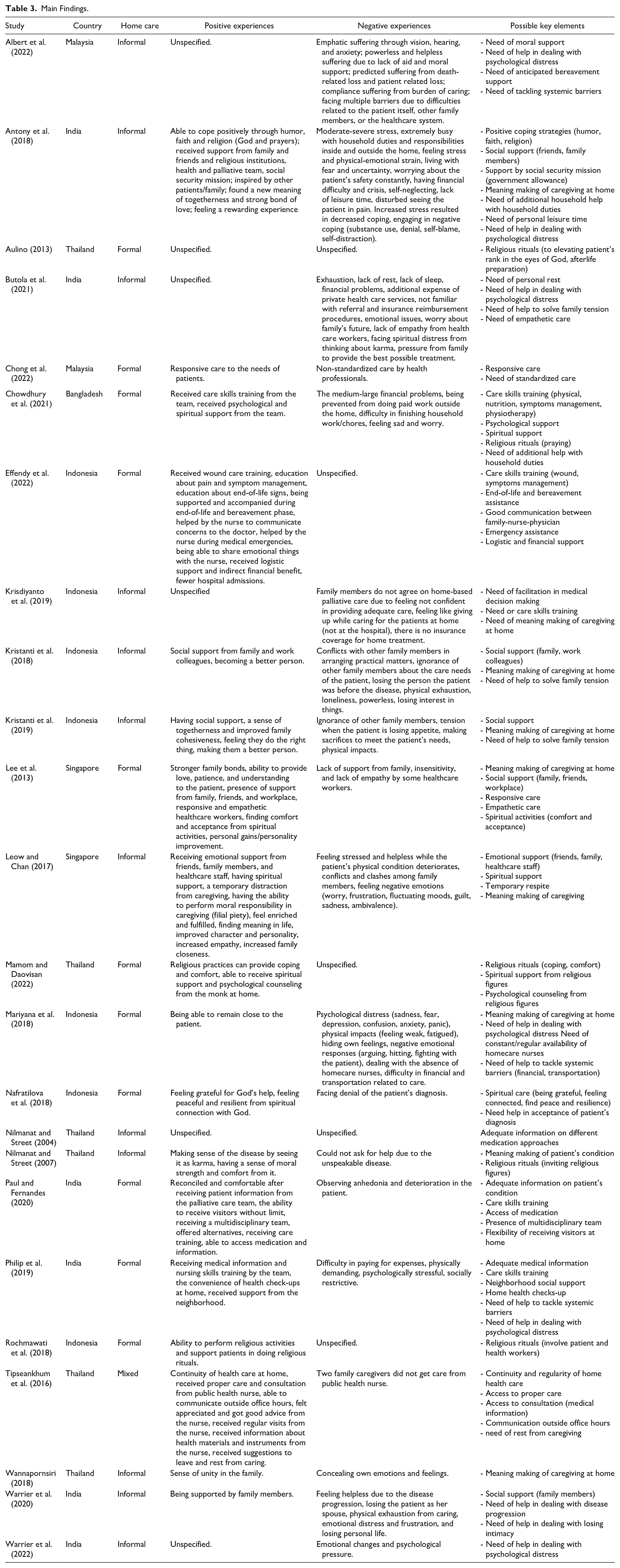
Table 2 provides information on family characteristics in the included studies. Caregivers’ ages ranged from 18 to 72, with a majority being female. This gender disparity can be attributed to socio-cultural norms that assign caregiving roles to women within families. However, 2 studies from Singapore and India reported a higher proportion of male caregivers,22,23 possibly due to caring for female patients. Spouses were the primary caregivers, followed by children or children-in-law. In elderly patients, if the spouse was deceased or unable to care, the responsibility fell upon the children. Table 3 describes the family caregivers’ roles and activities, positive experiences, and negative experiences reported by the studies in this review. A concept map to summarize the findings of this scoping review is presented in Figure 2.
Family Characteristics.
Main Findings.
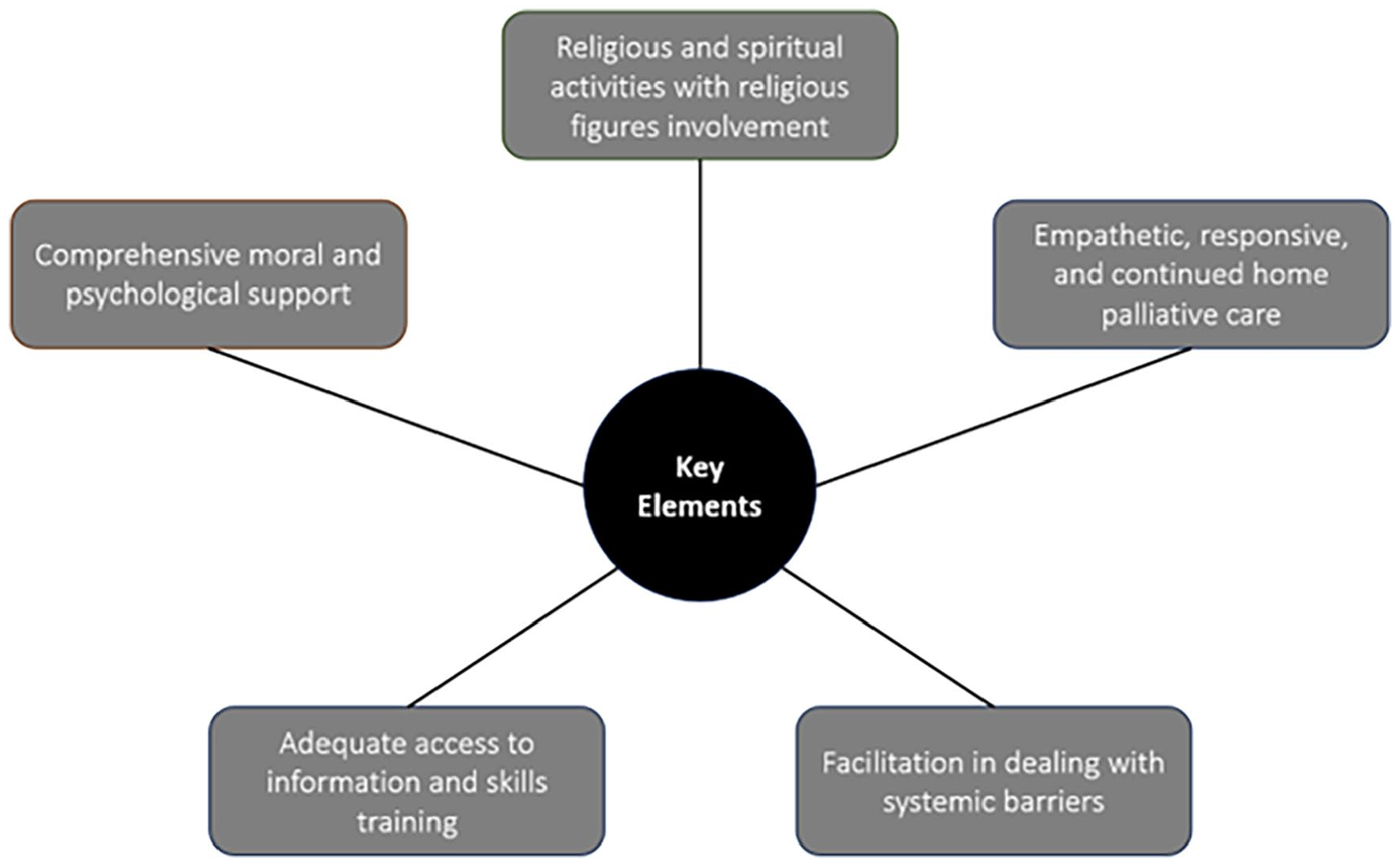
Concept map of the findings.
Comprehensive Moral and Psychological Support
Family caregivers felt positive experiences from receiving moral and psychological support that comprehensively covered their needs. Since families were dealing with various psychological distress and suffering,24-34 they needed help to access positive coping strategies facilitated by the formal home palliative care team. 25 One of the appreciated strategies was by helping families make a positive meaning of the patient’s condition and the caregiving activities, such as increased family cohesiveness, bond, and unity.22,25,29,32,34 This phenomenon emerged from the collaboration of family when providing emotional support for one another. Another positive meaning of the caregiving activities that can be pointed out by home palliative care team was the achievement of personal gain. Family caregivers felt that they were doing the right thing by caring for the patient, as they were able to provide love, patience, and understanding to the patient. Being able to stay close to the patient made the caregiving process rewarding for them.22,25,30 As families were anticipating the loss of the patient, an anticipated bereavement support by home palliative care would be helpful. 24 Support during end-of-life and bereavement phase had been helpful for families, particularly when they can share their emotional concerns with the home care nurses. 35 Sometimes, different perception of care and lack of support created social tensions among family members.24,26,27,29,36 Thus, home palliative care team could try to facilitate solving family tensions and moderating discussion between family members.26,28,36
Religious and Spiritual Activities With Religious Figures Involvement
Home palliative care could provide additional space for family caregivers and the patient to engage in religious activities together, thereby strengthening their spiritual connection with God and helping them cultivate feelings of gratitude, peace, and resilience.37,38 Furthermore, the presence of religious figures at home also brought comfort and facilitate acceptance of patient’s diagnosis and disease progression to the family.22,25,29,39,40 Religious rituals such as daily prayers and reading holy books performed could provide spiritual support for both patients and families, as these rituals can be seen as a way to increase patient’s good deeds and elevate patient’s rank in the eyes of God.38,40,41 It was appreciated by the family when healthcare workers were supportive of their religious needs, even getting involved in performing the religious rituals together. 38 By doing these activities, family caregivers aimed to provide calmness and mind clarity for patients, especially during their end-of-life phases.32,39,40,42,43
Empathetic, Responsive, and Continued Home Palliative Care
The families of patients who were receiving formal home palliative care appreciated the empathetic, responsive, and proper care provided by professional team that cater to the patient’s needs.22,42,44 The empathetic care included appreciation of family caregiving activities and helpful suggestion related to care-life balance from the healthcare workers. 42 On the contrary, insensitive health care workers contributed to negative experience of families. 22 Responsiveness to the individual needs of the patients and families were greatly appreciated, such as during difficult symptoms management and patient emergency conditions.22,35,44 Families also appreciated when they experience continuity and regularity of care at home. 42 Dealing with the absence of home care nurses was reported as a negative experience by families. 30 The availability of home care team could provide some personal time for caregivers, allowing families to have their rest from the physically and emotionally exhausting caregiving activities.25,26,29 However, standardization of care was also important for families. Negative experience was reported when families encountered different quality of care provided by different health care workers, particularly those lack of palliative care training. 44
Adequate Access to Information and Skills Training
Lack of knowledge and skills in caregiving raised concerns among family caregivers about care quality at home.28,36,45 Thus, it was appreciated when families could receive helpful information and training on patient’s disease and condition, basic nursing skills, wound care, symptom management, and end-of-life signs from the home palliative care team.23,27,31,35 Some families were trying to incorporate different approaches, such as modern medicine, traditional medicine, and supernatural healing rites. Adequate information from healthcare workers on these different approaches can be helpful for families to navigate their concerns related to patient’s physical condition. 43 Moreover, palliative nurses were able to help communicate families’ concerns to the doctor. 35 The ability to contact home care team outside office hours and received additional information addressing their concerns contributed to families’ positive experience of home palliative care. 42
Facilitation in Dealing With Systemic Barriers
As participants in the studies were residing in a low-middle income countries, some prominent systemic barriers were identified, such as financial difficulties, transportation challenges, complicated insurance procedure, and complex healthcare system. Some studies reported financial crises,25,27 making it difficult to afford healthcare equipment.36,42 Families also had difficulties in handling patient emergencies, transportation, and administrative papers related to referral and health insurance.26,28,30,33,36 Facilitation for families in dealing with these systemic barriers might be very helpful for them. Some instances included assisting families to receive social security support, 25 logistic support, 35 and neighborhood support. 31 Other social supports from family members, friends, work colleagues, were also greatly appreciated by families.22,25,28,34,36
Discussion
In this review, we synthesized 5 key elements contributing to good home palliative care in South and Southeast Asia from familial stand point. The multiple caregiving roles performed by family were described as challenging and burdensome, particularly when formalized home palliative care is unavailable, contributing to the exhaustion of family caregivers from taking most caring responsibilities.25,26,28,29,31,34,36 Physical and psychological distress experienced by families require comprehensive moral and psychological support. Otherwise, family caregivers might not receive adequate palliative care even though they are also eligible for a holistic care based on WHO definition of the palliative care. Our finding is supported by previous literatures showing psychological interventions for family caregivers were effective in improving their competence and preparedness in dealing with psychological distress.46,47
Our study also emphasizes how crucial role of religious and spiritual activities in providing positive experience during home palliative care specifically in South and Southeast Asia. This finding reflects the strong influence of religion, although these countries have different religious majorities.38,39 These shared experiences highlight how families utilize religious and spiritual practices to provide comfort while caring for the patient.22,36,39,40,43 The importance of spiritual care is also supported by previous studies in European countries, emphasizing religion’s ability to relieve suffering.48,49
Empathetic, responsive, and continued care was reported as an important element in our study. This finding aligned with previous review showing the importance of having responsive team that prepares and helps family caregivers during times of crisis, such as exacerbations of symptoms. 7 The importance of incorporating empathy in care, including home palliative care, had been described by previous study as an important component of clinical competence by building sustainable relationship with patients and families. 50 Moreover, continuity of care had also been reported as one of important elements of integrated palliative care, which can be enhanced by involving small numbers of healthcare professionals for each patients and regularly transfer information among healthcare providers. 51 A meta-ethnography study of home palliative care in high-income countries shows that 24-hour available professional care was one of the critical components to improve care experience, which aligned with our findings that support the important presence of competent, communicative, and supportive health professionals to support families in dealing with caregiving’s challenges. 52
Care-related positive experiences such as helpful healthcare professionals who provide information and skills training were more often found in family of patients receiving formal home palliative care.22,23,27,31,35,42,44 However, the availability and accessibility of formal home palliative care are still limited.26,30,36 Previous systematic review from high-income countries reveals that formal multidisciplinary team is essential to provide holistic care for the whole family. 7 By providing education and guidance to the family caregivers, home palliative care team can increase the patient and family preparedness in facing home caregiving situations. 7 These findings strengthen the idea that providing home palliative care with professional support is crucial for improving the care quality by providing adequate access to medical information and basic nursing skills training for patients’ families.
Some studies in our review described the limited availability of government allowance or free home care from charity organizations.25,35 The responsibility of family caregivers to pay some or all of the home palliative care costs had led to family financial crisis.25-28,31,33,36,41,44 Similar findings of family burden and limited funding was also reported in African countries, related to existing system-level barriers. 53 Our findings support an earlier review that emphasized family caregivers’ need for help to coordinate and arrange care, especially in a resource-limited setting. 54
Finally, this scoping review offers 5 key elements of good home palliative care from family perspectives across South and Southeast Asia, including Indonesia, India, Malaysia, Singapore, and Thailand. It is the first review of the topic in this region that encompasses both adult and pediatric patients with various illnesses. The similarities among these countries enhance our understanding of the topic. However, it is important to note that the number of studies on this topic is limited, and they were conducted within specific regions of each country. Therefore, a careful consideration is needed to generalize results to different settings. Further research is needed to explore integration of professionals into home palliative care within highly religious societies and improvement of palliative care provision from a healthcare system perspective.
Conclusion
Key elements of good home palliative care from family perspectives in South and Southeast Asia include comprehensive moral and psychological support; religious and spiritual activities with religious figures involvement; empathetic, responsive, and continued home palliative care; adequate access to information and skills training; and facilitation in dealing with systemic barriers. Specific findings from South and Southeast Asia regions were the crucial role of religious and spiritual activities and the need of facilitation in facing systemic barriers. Both findings came from the specific context of these regions which emphasizes the importance of religion and spirituality, and the systemic barriers related to the countries’ low-middle income with limited provision of formal palliative care. In these regions, palliative care was mainly provided by families at home, particularly in rural areas. The presence of formal home palliative care with emphasis on the 5 key elements in our review could improve the quality of care. The availability of formal home palliative care in combination with sufficient financial support to afford it, seems most influential for the patients’ quality of care and the family caregivers’ well-being and survival.
Supplemental Material
sj-docx-1-hhc-10.1177_10848223231224779 – Supplemental material for Family Perspectives on Key Elements of Good Home Palliative Care in South and Southeast Asia: A Scoping Review
Supplemental material, sj-docx-1-hhc-10.1177_10848223231224779 for Family Perspectives on Key Elements of Good Home Palliative Care in South and Southeast Asia: A Scoping Review by Raditya Bagas Wicaksono, Amalia Muhaimin, Dick L. Willems and Jeannette Pols in Home Health Care Management & Practice
Supplemental Material
sj-docx-2-hhc-10.1177_10848223231224779 – Supplemental material for Family Perspectives on Key Elements of Good Home Palliative Care in South and Southeast Asia: A Scoping Review
Supplemental material, sj-docx-2-hhc-10.1177_10848223231224779 for Family Perspectives on Key Elements of Good Home Palliative Care in South and Southeast Asia: A Scoping Review by Raditya Bagas Wicaksono, Amalia Muhaimin, Dick L. Willems and Jeannette Pols in Home Health Care Management & Practice
Footnotes
Acknowledgements
We thank Faridi Jamaludin from Amsterdam UMC library, who provided initial insights for the database search.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This scoping review is part of a PhD scholarship funded by the Indonesian Endowment Fund for Education (LPDP), grant number 202112220808210. The funding source has no influence on this review.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.