
Abstract
Early identification and follow-up of sub-acute and acute functional decline in older persons living with multimorbidity at home require integrated and proactive care by interdisciplinary health personnel. Yet, in the context of the task-oriented and fragmented home healthcare services, early identification is challenging. Therefore, the aim of this study was to identify preconditions for the success of a proactive and interdisciplinary follow-up of older recipients of home healthcare. We conducted a qualitative secondary analysis of data from 6 focus group interviews with registered nurses and nurse leaders. In addition, we performed and analyzed data from 2 new focus group interviews with general practitioners and RNs who had a role as super users in a developmental project which introduced a clinical instrument for early identification of sub-acute and acute functional decline (sub-acute functional decline in the elderly—SAFE). Their experiences with using SAFE constituted the backdrop for the study. In total, 41 representatives of the interprofessional primary care staff of 3 city districts participated. Having a common goal, sharing tasks and having reciprocal understanding of each health profession’s contribution, systems and tools and clinical leadership were all seen as important factors for succeeding in the proactive and interdisciplinary follow-up of older recipients of home healthcare. Clinical leadership was deemed the strongest precondition, and clear leadership which promotes integrative and proactive care by facilitating interdisciplinary collaboration appears to be the main key for success.
Keywords
Introduction
Frail older people frequently experience having to travel repeatedly between their home and acute-care facilities. 1 This phenomenon is a great burden on the patient and places stress on healthcare capacity, and its overall costs are likely to be considerable. To meet these challenges, attention to the early identification of functional decline and interprofessional follow-up are necessary. 2 Intervention in home-based healthcare tends to be reactive, that is, it is in response to manifest care needs or acute events rather than a proactive strategy based on the early identification of symptoms and signs of functional decline.2,3 Because such symptoms and signs can easily be misinterpreted as simply an increased need for care, functional decline can pass unnoticed for an extended period of time and, thus, a chance for early intervention, that is proactive care, might be lost. The speed at which a patient loses functional capacity in everyday activities is important in selecting measures for early detection. 4 Acute (over hours or a few days) functional decline can often lead to hospitalization, because it is likely due to acute illness, while patients with chronic (over months or years) functional decline require optimized rehabilitation and necessary healthcare to maintain a good quality of life. Subacute (days or weeks) functional decline should be investigated immediately, hopefully enabling health personnel to intervene before the condition becomes too severe. 4
The concept of frailty has, during the last few decades, proven its usefulness in providing health care for older people. Frailty is the consequence of a cumulative decline in many physiological systems and implies increased vulnerability due to the poor resolution of homeostasis after a stressor event. 5 Addressing frailty is therefore of importance to home-dwelling older persons living with multimorbidity and functional decline. Frail people benefit from targeted healthcare and have an increased risk of functional decline during the course of acute illness. Two main tenets exist regarding the traditional identification of frailty. The frailty phenotype, as first defined by Fried et al, 6 is based predominantly on the assessment of physical performance. As well as this, the cumulative model of frailty, as defined by Rockwood et al, 7 is based on a comprehensive geriatric assessment in which various deficits are added together. Both concepts can predict an increased risk of an illness trajectory emerging, and in this text, we use them interchangeably.
Health professionals, such as registered nurses (RNs) and general practitioners (GPs), normally meet the recipients of home healthcare (HHC) for only brief periods, leaving them with a limited possibility of detecting and identifying early symptoms or indicators of decline. HHC staff perform daily tasks in sequence, following a working list containing the patients’ names, addresses, and specific tasks or interventions, with estimates of the time they will take to complete, for each patient. 8 During a working day, HHC staff typically spend approximately 50% of their time caring for patients, 20% for transportation, and 30% on other tasks, such as preparing documentation and reports or attending meetings. 9 Most GPs in Norway are self-employed, and only a few are employed by the municipality in which they work. On average, a GP’s patient list consists of about 1100 patients. 10 HHC personnel and GPs are organized separately and not necessarily in geographic proximity to each other. Therefore, their collaboration is mainly conducted through digital communication such as e-messaging, although integrated care was one of the main goals of the Norwegian Coordination Reform. 11
Investing in a coordinated and integrated care is a global political issue.12,13 However, there is no universally established term to denote this type of care. “Integrated care” is the most commonly used term and is used synonymously with “coordinated care” or “seamless care,” all of which indicate a contrast to care fragmentation. 14 Integrated care, therefore, can be described as the seamless delivery of care for patients with complex long-term problems that span multiple services, professions, and levels of services. It covers care processes that take place on the micro- (clinical integration), meso- (professional and organizational integration), and macro- (system integration) levels. 14 A review of reviews by Briggs et al 12 found evidence that elements of integrated care for older people seem to focus particularly on micro clinical integration processes, and they seldom focus on care integration strategies on the meso-organizational and macro-system levels. Accordingly, there is missing evidence on care integration on meso- and macrosystem levels. Integrated care requires interdisciplinary teamwork, collaboration and coordination, and an integrated and proactive approach through interdisciplinary collaboration is crucial in dealing with the complexity of frail older patients’ health care needs. 13
Several screening and assessment tools are used in HHC, but to our knowledge, they are mainly employed reactively when symptoms of decline have become pronounced through nutritional status and assessments of acute illness.15,16 Although designed and validated for acute hospital settings, early warning scores are recommended as a clinical decision-making tool in outpatient settings in Norway15,16 Jeppestøl et al 16 found that RNs and GPs considered modified early warning scores as potentially useful in HHC settings, but this tool had not been adapted for use in HHC settings or for the older patients. Therefore, in 2013, a group of RNs, GPs and researchers developed a new tool for the context of older patients receiving HHC. The tool was designed as a checklist and was named sub-acute functional decline in the elderly (SAFE). 17 This development was part of a quality improvement project and was based on domain knowledge and experience-based assumptions to improve the proactive follow-up of potentially frail older people. SAFE is currently in use in several municipalities in Norway and is being developed further as a tool which is more than a checklist, although it is yet to be validated. SAFE facilitates the structured observation and assessment of personal hygiene, medical self-care, general self-care, nutrition, respiration, circulation, skin, elimination, mobility, cognition, mood, alertness, communication, vision, hearing and pain. The items within these areas have 3 response categories which reflect the degree of change: no change (green status), moderate change (yellow status) and severe change (red status). Potential or manifest functional decline is assessed systematically based on a baseline screening. Changes from the baseline outcome (yellow and red status) indicate sub-acute or acute functional decline, in which case, SAFE provides decision support on when to consult the patient’s GP. See Figure 1 for an illustration of the SAFE process.
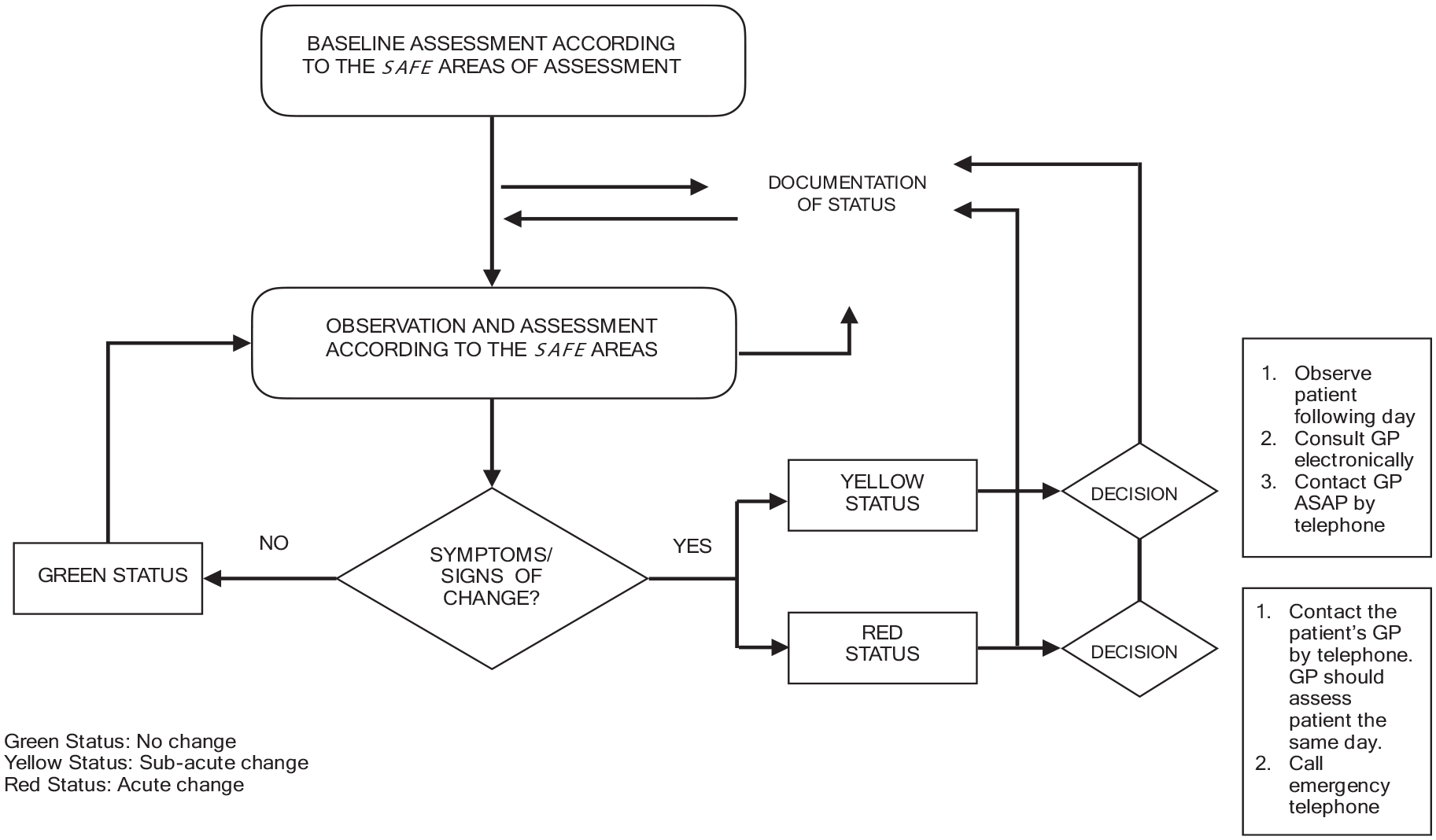
Illustration of the structured SAFE process.
A previous study, on which the present study is based, identified RNs’ and their leaders’ experiences and opinions about the need for more structured follow-up and identified potential benefits and barriers to the use of SAFE when caring for frail home-dwelling older people. 18 The study provided some indications of the importance of achieving more proactive care which includes interdisciplinary collaboration. We found, in line with Jeppestøl et al 16 that a more structured working mode regarding observations and decision making was recognized as being important by the informants. However, both organizational and individual-level factors impeded such a structured working mode being developed. Individual-level barriers during direct patient care were insufficient geriatric care competence, limited time or a shortfall in available information. Organizational-level barriers included a deficient common strategy for collaboration between health professionals (RNs and GPs) and a shortage of time allocated for indirect patient care follow-up and documentation. These results prompted the need for further investigation of the above-mentioned issues to expand our understanding of structured follow-up in HHC. 18 SAFE is used as a backdrop to this study, as it is an example of a means of developing a structured, proactive, and interdisciplinary follow-up for frail older persons.
Aim
The aim of the present study was to identify preconditions for succeeding in the establishment of the interdisciplinary, structured, and proactive follow-up of older recipients of HHC who are at risk of functional decline. We posed the following research question:
As a result of using a structured assessment tool, which preconditions will, according to key health personnel and leaders, enable and consolidate an interdisciplinary, structured, and proactive follow-up of older recipients of HHC?
Material and Methods
This study had a qualitative descriptive design. The data material consisted of text transcribed from a total of 8 focus group interviews. Data from 6 of the interviews, of which results from the original analysis have been reported elsewhere, 18 were subject to re-analysis through qualitative secondary analysis (QSA). QSA allowed us to answer a greater variety of questions than the original analysis, to explore and expand on the analysis from the original project and to analyze the dataset alongside newly gathered data.19,20
Setting
The study took place in HHC settings in 3 districts in a large Norwegian city. Older people commonly receive HHC frequently, that is, on a weekly basis or one or several times per day and over an extended period of time.18,21 The RNs in this study are so-called “patient-responsible RNs,” which means that they have a limited number of patients (maximum 20) for whom they have a dedicated responsibility for following up. GPs have the overall medical responsibility for patients living at home. Super users (SUs) are RNs who have a special role in promoting the use of SAFE. Leaders manage on an intermediate level, and they have formal responsibility for home care on different levels, from group leaders to district leaders.
Participants
We applied a purposive sampling strategy to recruit eligible participants who were RNs (the SUs) and GPs collaborating in interdisciplinary teams. In addition, we included RNs (clinical nurses and leaders) participating in a former study. 18 All clinical nurses, their leaders and GPs in the 3 districts used SAFE in their follow-up of home-dwelling older people aged 75 and over. In addition, RNs who had earlier had positions as SUs participated in a separate group. The sample consisted of 41 participants: 17 clinical nurses, 3 SUs, 16 nursing leaders and 5 GPs from 3 districts.
Ethics
Participants were provided with written and oral information about the study. They were informed that they could withdraw at any time. All participants then signed an informed consent document before participating in the interviews. The study followed the ethical guidelines outlined in the revised Declaration of Helsinki. 22 The Regional Committee for Medical and Health Research Ethics in Norway (REK) approved the study (number 2012/1891).
Data Collection
The data material was collected by means of focus group interviews in line with Liamputtong’s 23 recommendations. In total, 8 focus groups were conducted in 2014. Three groups comprised clinical nurses and 1 was made up of SUs. Three groups consisted of nurse leaders, and 1 group was comprised of only GPs (see Table 1).
Overview of Focus Groups.

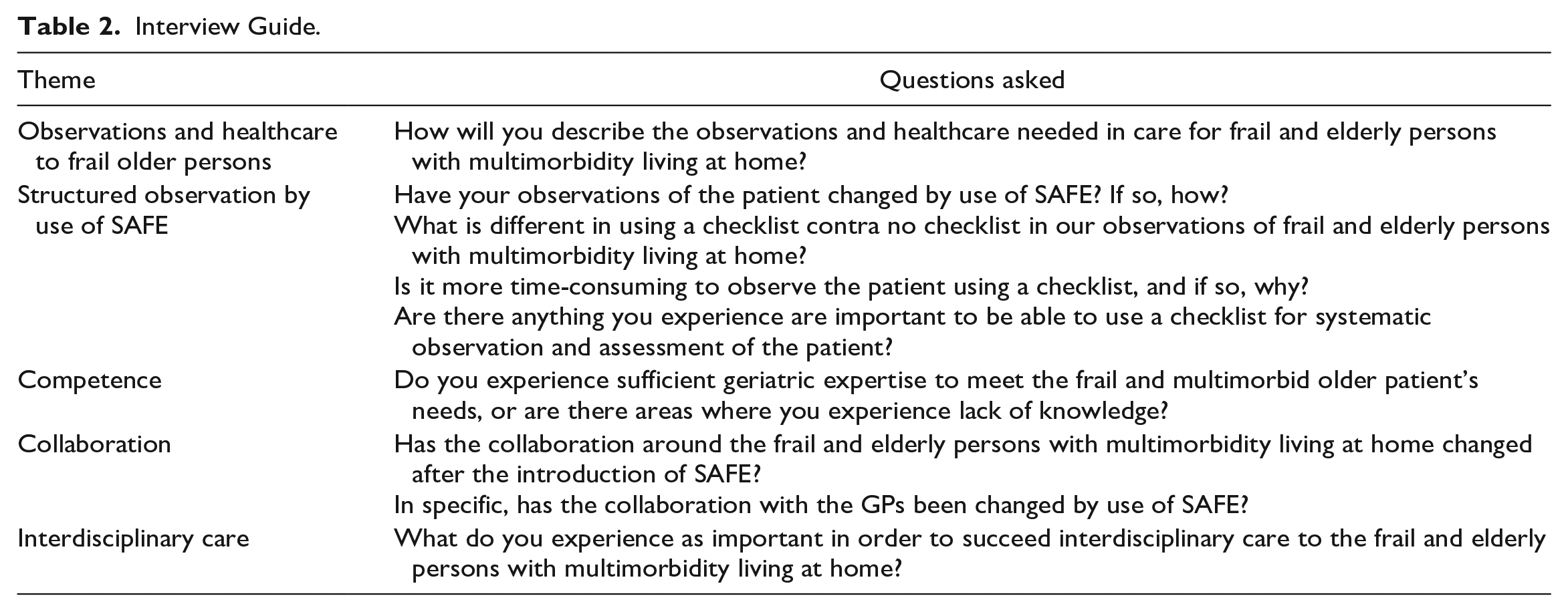
Two researchers conducted 4 focus group interviews. The first author (GN) was the moderator, and a colleague was co-moderator. Unforeseen events hindered one of the researchers from attending 4 interviews as planned. Therefore, GN conducted the interviews alone. All interviews took place at the participants’ workplace and lasted, on average, 71 minutes (minimum 54 minutes and maximum 88 minutes). An interview guide consisting of 5 main themes was used to stimulate and guide the discussion:
The guide, see Table 2, was based on existing knowledge, the researchers’ clinical experience and pre-understanding. The structure of the SAFE instrument and participants’ attitudes toward and experience with using SAFE served as a framework for the discussion for all the interviews. 23 Depending on the replies, the aspects and ideas raised by the informants led to probes—further questions to obtain additional information. The interviews were audiotaped and transcribed verbatim by an RN with substantial knowledge and clinical experience regarding treatment and care for older persons in both community and specialized care. GN checked and corrected the audio files prior to the analysis. The data collection yielded, in total, 158 pages of transcribed text.
Interview Guide.
Data Analysis
The transcribed text from all 8 interviews was subject to thematic analysis. 23
Two researchers read the interviews from the GPs and SUs (Groups 1 and 2) to obtain a condensed overview of the data. The next analytical step (initial coding) was conducted by GN, who read the interviews and identified codes. The codes referred to words, phrases, expression of emotions, reactions, actions, and reflections related to the study aim and research questions. The researchers searched for codes within and across the focus groups to find repeated patterns and links between them. Based on the initial coding, the codes were connected to form sub-categories and categories (axial coding). At this stage of the analysis, an agreement on final themes was reached through discussions and reflection among the authors. During the analysis of the data, we found that the informants repeatedly discussed preconditions for succeeding in interdisciplinary, structured, and proactive follow-up, although this was not within the scope of the initial interviews. Hence, we found it feasible to re-analyze data from the interviews with RNs and nurse leaders to conduct further investigation. GN and ERG performed the secondary analyses (QSA) of the interviews from the RNs and leaders (Groups 3-8) to explore new perspectives on proactivity and preconditions by using the same analytic approach as described above. GN, ERG, and TBW then discussed the findings and finalized the analyses.
Results
The participants described both professional and administrative challenges regarding interdisciplinary and proactive healthcare for older recipients of HHC. The use of the assessment tool SAFE contributed, according to the participants, to an improvement in structure, information exchange, and interdisciplinary collaboration. In the light of these experiences, the participants articulated what they saw as preconditions for enabling interdisciplinary and proactive healthcare for older recipients of HHC, summarized in the following 4 themes: (1) a common goal of a more proactive healthcare; (2) the clear interdisciplinary sharing of tasks and knowledge and awareness of each other’s work; (3) administrative systems and tools that support proactive practice and interdisciplinary care; and (4) leaders must facilitate and ask for proactive follow-up.
A Common Goal of a More Proactive Healthcare
Overall, the participants appreciated the idea of a more proactive practice. They experienced a new and more common proactive practice when using SAFE. Structured follow-up had now become a common and visible goal through the employment of SAFE and the new routines of communication between RNs and GPs. There was an overall agreement that this change of goal, that is, more proactive care, was needed, even though there were some differences in opinion over the need for new routines.
Some leaders said that the original practice mainly focused on “firefighting” and reactive actions, and because of this, they saw a need for change. Other leaders and RNs described a former system where little or no attention was paid to structured patient observations which would reveal small changes, and they saw the need for a more proactive approach with more coordinated observations. With SAFE, they explained that RNs’ observations were now more precise. The GPs confirmed their experience of the previous “firefighting” strategy of care, which, to a great extent, required them to carry out rapid and reactive intervention.
I do not have the opportunity to conduct a type of outreach activity, or the type of observation and assessment over time. I act when someone says, when something has happened, that the patient needs medical help. (GP1)
The participants confirmed that practice lacked structure and attention to the promotion of proactive healthcare. The interdisciplinary health personnel agreed that a more proactive healthcare was needed.
Clear Interdisciplinary Sharing of Tasks and Knowledge and Awareness of Each Other’s Work
Increasing the level of interdisciplinary collaboration is, according to the participants, dependent on a mutual knowledge and understanding of each other’s responsibility and work. All participants described a lack of clarity regarding RNs’ and GPs’ responsibilities with regards to healthcare to home-dwelling older patients prior to SAFE. They aspired to increase interprofessional teamwork in following up with home-dwelling elderly, as illustrated by the following excerpt.
Another important issue was the experience of shared responsibility and not being alone in following up. (GP3)
This sentiment was shared by most of the RNs and their leaders and related to a lack of clarity about their responsibility in relation to the follow-up of medical treatment for older home-dwelling patients.
With SAFE, participants experienced an overall understanding of what to expect from each other and how to complement each other in the care of the patient. One GP viewed the benefit of SAFE as the possibility of gaining specific information about patients on a daily basis. This had been difficult to achieve under the previous system. In the words of 1 participant:
That there are people out there working and that we can really get more out of it, because they [home care personnel] can follow up the patient every day, and they see them all the time. (GP2)
According to the leaders in this study, SAFE contributed to disclosing who was responsible for what in the follow-up of patients and made it easier for the RNs to carry out their professional responsibilities.
Then I feel that responsibility is placed where it belongs. That it is written and clear, and that we have done what we can do. (Leader1)
The participants appreciated the overall more frequent collaboration between RNs and GPs. Structured assessment and the sharing of information by using SAFE led to an increased trust and confidence felt by GPs toward RNs.
I have been given a little more faith in their work and that we can get a great help from them, if we use the resources that exist and the opportunities for such cooperation with them. (GP2)
The RNs mentioned there were more rapid and precise responses to their inquiries about patients. Prior to SAFE, collaboration with GPs was somewhat difficult and affected by gaps in their knowledge about each other. Previously, common goals, knowledge or expressed expectations concerning other parties’ contributions in healthcare were lacking. After the introduction of SAFE, GPs stated that they had gained more insight and awareness in these areas:
Since I have been involved in this project, I have gained a little more insight into how home healthcare is working, and it is very good to know. What can I expect from home healthcare, how can they contribute? (GP1) I think that awareness is valuable, and maybe we can collaborate a bit on a little more professional level. (GP2)
Several other RNs indicated that SAFE had contributed to increased awareness and, thus, more proactive care.
So that checklist, I think it is great with a kind of follow-up every other week, I think it is very useful. You get to pick up the little things, which you may not see in the stressful everyday life as it often is. (RN1)
Using a structured assessment tool was found to be useful for the collaboration between RNs and GPs with an increased awareness and knowledge of each other’s responsibilities and work regarding older HHC recipients. However, the participants clearly stated that increased mutual insight and awareness is necessary but not enough to change practice.
Administrative Systems and Tools That Support Proactive Practice
The participants expressed a united opinion on the need for new routines supported by administrative systems and tools. We found that most of the participants considered systems for assessing and sharing vital patient information as important, although insufficient, prior to SAFE. One leader expressed this view:
Previously, you may have made a summary of the patient, called the doctor, and talked about this and that and that in a way, but it would be your experience of the conversation. While now, it will be in a different way, now that the doctor writes back on your assessments and questions. (Leader2)
All RNs and the SUs reported that transferring data from SAFE to the electronic patient record (EPR) was difficult and should be improved. The introduction of SAFE had revealed a major problem with the inadequate documentation of patient information in all 3 districts. An understanding of how and why this documentation should be maintained was, according to the participants, missing. The participants outlined the need for systems for sharing information.
One GP said,
There is no system of information. (GP4)
Similarly, 1 leader expressed the following:
About documentation in EPR, to convey the information we possess about the patient, there we perform poorly. There is a big gap between what is actually done and what should be done. (Leader3)
The SUs also spoke about difficulties in including patients in the SAFE routine because of missing documentation in the EPR.
There was something that stopped here in the district, and we went more into the Electronic Patient Journal (EPJ), and we then saw that it might be due to basic documentation, and we had to start that process to somehow make them understand, why one should document and use SAFE. Then I had a lot of training, eh, which in a way then really went a little beyond SAFE, but which they had to have in order for them to get on. (SU1)
To facilitate more proactive healthcare, the participants also highlighted the need for individual care plans.
We have not had any care plans either. We have only had work lists, who said you should do it and that when you are with the patient. Not why, or what is the goal with the healthcare. (RN2)
A leader expressed the following opinion:
Because we have worked for many years now based on formal decisions on healthcare. That is, we have had a list of tasks that the RN gets on the work list every day, right? Still, it is a bit like that; really, the work lists should have come out of the patient’s individual care plans and not from formal decisions. Then it had become quite clear what to do and why by the patient. Then we would really have something that pushes us to secure that the care plans are good. (Leader4)
There was a change in how GPs and RNs collaborated, illustrated here by examples of utilizing a universal messaging system when sharing information about a patient, in this regard, by using SAFE as a clinical tool.
Response to the RN’s messages is, in a sense, part of the running patient record. When I formulate an answer, I think that answer must be written in a way that allows them (RNs) to see what I mean. So that it becomes even clearer that way. Working this way has been very structuring and very good. (GP4) You discover new things that actually make the patient come to the hospital, less out of control than it often appears. (RN3)
The SUs stated that the most important influence from SAFE regarding interdisciplinary collaboration was that RNs had become more aware of what it meant to be an RN with patient responsibility. The SUs explained that the RNs, by using SAFE, had become aware of what it meant to have an overview of the patient’s situation. This included realizing that the RN had to update the care plan regularly with patient information from SAFE, as well as communicating with the GPs, relatives and hospitals.
Leaders Must Facilitate and Ask for a Proactive Follow-up
The RNs stated that their own participation in the introduction of SAFE and new routines was directly influenced by their leaders’ ability to motivate and lead, illustrated by the following excerpt.
Approximately fifty percent of people in the leadership team are not motivated for project SAFE. The mentality one has among the leaders has a lot to say about the mentality in the group. (RN4)
To motivate and demand efforts to achieve new goals, the participants suggested that leaders must understand and agree on the need for change. A leader said,
Although SAFE is not something I should be doing, it is important to know what my employees are doing. To know the tool and value of it and understand what they are talking about when they are talking about it. (Leader6)
The leaders appreciated that there were difficulties with documenting observations from SAFE, but they highlighted other elements as being more influential when explaining why the new routines were not being fully implemented. The factors were both at the individual (i.e., employee) and system levels. Some of the leaders discussed their own responsibility in contributing to facilitating new, more proactive care. One leader explained it like this,
However, I think there are many in my district, at least as I see it, who may have lacked a person that acts as “an engine that sees and conveys that SAFE is, after all, an important tool.” (Leader7)
The SUs questioned whether the leaders could see the benefits of SAFE in terms of documentation and interprofessional collaboration.
About documenting in EPR, I think they (the leaders) also look at this at the expense of something else, they do not see that this helps to improve communication with the GP, the hospital and the client’s office, I think. I think it increases the quality of what one writes in EPR in general. However, you do not have the capacity to see this when running the way they (the leaders) do. (SU2)
The interviews revealed both professional and administrative challenges to succeeding in creating a more proactive follow-up of older HHC recipients. The leaders expressed ambivalence toward the SAFE tool and revealed that leaders’ motivation and knowledge regarding proactive and structured follow-up is of importance to its success.
Discussion
The aim of the present study was to identify preconditions for succeeding in establishing interdisciplinary, structured, and proactive follow-up of older recipients of HHC at risk of functional decline.
Our results demonstrated that RNs and GPs maximized their efforts to work systematically and proactively for the benefit of patients, and they recognized and appreciated each other’s contributions and roles within healthcare provision. However, they also described some challenges and put forward some suggestions that indicate that the preconditions for succeeding in the interdisciplinary and structured proactive follow-up of patients are predominantly connected to the organizational level. The findings span the topics of sharing a common goal, sharing tasks, gaining a reciprocal understanding of each health profession’s contribution, developing appropriate systems and tools, and leadership. Our main finding was that clear clinical leadership was considered an important precondition to the success of interdisciplinary proactive care.
Leadership can be widely defined as the relationship between the individuals who lead and those who take the choice to follow. It also involves directing and coordinating the activities of a team toward a common goal.24,25 Clinical leadership is a relatively new term, and it still requires a clear definition. 25 Bondas 26 suggested in a grounded theory study that nurse leaders have a “double focus,” which is likely to lead to management paradoxes stemming from having potentially competing responsibilities. For example, as described by Gjevjon et al 27 quality and continuity of care may compete with monetary issues and human resources. 27 The clinical leader (CL) has the overall responsibility for care quality, systems, staff, and resources. The CL in the context of this study was commonly a registered nurse. According to Jeon et al 28 a CL provides the link between governance, operational management, care, and service delivery. Additionally, they monitor business operations, maintain standards of care, manage personnel and budgets, and facilitate organizational or necessary changes in care. The CLs in our study were middle managers, supervising the nurses on the front-line but at the same time, being supervised by senior managers in the municipality. These middle managers have an important, but often overlooked, role in introducing new working modes, such as the SAFE instrument. Jeon et al 28 (p. 1000) claim that “middle managers are critical intermediaries in the interface between strategy development and implementation within the challenging contemporary aged care environment.” Jordal et al 29 found a knowledge gap concerning first-line nurse managers’ leadership and their management role in home care in their scoping review, and they claim this indicates a need to improve knowledge on leadership in HHC.
Leadership and a Proactive Interdisciplinary Care
Valentijn et al 14 found that insufficient shared language and divergent healing paradigms could hamper professional integration in health care. Clarity about factors such as roles, responsibilities, respect, and communication seems to be crucial in succeeding in promoting interdisciplinary care. This is supported in a study by Beijer et al 30 who found clear boundaries between the principal areas of responsibility and professions’ areas of responsibility, respectively, as necessary for effective cooperation among professionals. In our study, all the participants mentioned the same preconditions to succeed in interdisciplinary care, but the most important precondition to facilitating a change toward more proactive and interdisciplinary care was strong leadership. In line with this, González-García et al 31 claim that developing competent nurse managers is a key to success for health care organizations.
Despite their experience, our informants agreed that their own efforts were important for introducing change. This is supported in a systematic review by Schot et al 32 which describes how healthcare professionals contribute to interprofessional collaboration. Our participants’ experiences are in line with Daniels et al’s 33 findings, underlining some of the challenges and emphasizing the need for proactivity and interdisciplinary collaboration. Daniels et al assumed that the implementation of complex interventions could be hampered by a fragmented and reactive approach and a lack of intense collaboration between healthcare professionals.
In the Netherlands, an interdisciplinary primary care approach has recently been developed. This approach to more integrated care involves individualized assessment and tailor-made interventions, case management, and long-term follow-up. 34 Achieving integrated care is a complex process, and it often requires a reorganization of an established healthcare system. CLs must then facilitate changes in the healthcare system, which are crucial for the implementation of integrated primary healthcare in the context of the present study. Research on clinical leadership in integrated primary care is unfortunately scarce. 35
Common elements of integrated care models include interdisciplinary team care, comprehensive assessment, and case management, with many interventions focusing on micro-level service changes, 36 as in SAFE. Our study confirms this need for support for professionals (e.g. training and decision support), structured collaborative care processes and integrated care. Threapleton et al 36 found that small, focused teams of RNs and GPs may potentially facilitate the implementation of integrated care, as well as the shared values, goals, policy, and governance that enable integration. Their study supports our findings.
Clinical Leadership and the Need for Common Goals of Care and Knowledge of Each Other’s Responsibilities
RNs and GPs in our study revealed a dearth of coordination toward a common goal at the higher administrative level. They did not feel that their CL enhanced or requested common goals. In view of this, it is important to understand how to leverage middle managers’ influence and how they influence the innovation and implementation of new routines. This is in line with Leigh et al 37 who suggest that a CL is a clinical expert who leads their personnel toward better health care by providing a vision to their colleagues and through this, empowering them. It is necessary for an organization to be supportive of information sharing, good collaborative relationships, and the practical framework conditions for integrated collaboration with patients and between professionals. Teams having an awareness of each other’s responsibilities and tasks across organizational boundaries enhances interdisciplinary collaboration, as experienced and suggested by our participants. To achieve this, a CL who takes a coordinating role and acts as a mediator between different organizations, such as GPs and HHC, is crucial. We found this element to be missing in the context of our study.
Clinical Leadership and Competence to Succeed in Interdisciplinary Proactive Geriatric Care
To be able to initiate changes in a health care system and enhance new outcomes, CLs need to develop certain competencies.38,39 In our view, CLs should have the clinical skills to be able to provide mentorship and coaching, encourage clinical and ethical decision-making and provide necessary consultation and constructive feedback.
Geriatric nursing is considered a specialized and complex area of healthcare,39,40 and advanced and comprehensive competence is essential in meeting the needs of older people; yet our study indicates that practicing nurses and GPs sometimes fail to meet these complex needs of the aging population. Based on our study, we might suggest that inadequate support from CLs might be a factor contributing to shortfalls in care. A systematic literature review found no studies on the effectiveness of clinical leadership on integrated primary healthcare and results at the patient level, emphasizing the need for more research into the relationship between clinical leadership and quality of care. 35 It is however safe to assume that a leadership support program can help prepare leaders for the implementation of integrated primary healthcare. Moreover, leaders’ relational and organizational skills, in addition to process management and change management, were considered important in contributing to achieving integrated health services. In line with Pizzerani et al, 41 we found that clinical leadership programs could potentially contribute positively to nurses’ leadership roles and outcomes, patients’ outcomes, and in turn, organizational outcomes in terms of a more proactive interdisciplinary care of frail older home-dwelling older persons. Further study into results from clinical leadership development programs is therefore necessary.
Methodological Strengths and Limitations
This was a qualitative study, and the findings may not represent the views and experiences of all personnel in HHC units and district GPs. The 2 authors of this paper have held a range of different posts within HHC over the course of their careers, including that of unit manager and teacher and researcher in geriatric healthcare. These experiences have inevitably influenced the design of the study, the development of the interview guide, the focus groups, and the analysis. 23 Rather than attempting to separate the researcher from the research, continuous reflection on the preconceptions and pre-understanding regarding assessment and HHC practice was actively used in the research process. One author was a physician and a geriatrician. Familiarity with the field under study may provide unique insight, making it possible to identify patterns and complexities less visible to an “outsider.” 42 Over a period of time, and in several meetings, the authors discussed the initial findings that emerged from the analysis and reached agreement on the final findings presented in this paper.
Four of the focus group interviews were held by GN alone due to practical issues or sudden changes in schedule. GN has undertaken a number of focus groups and therefore has extensive experience in the role of moderator. Having only 1 moderator may have possibly lowered levels of stress and allowed the participants to speak more freely. However, some aspects, such as body language and inferred communication possibly containing vital information, may have been lost due to there not being a co-moderator.
Data were collected in 2014. However, studies in the proceeding years up to the present day have documented a constant increase in the number of older people living at home with multimorbidity, functional decline, and polypharmacy.3,16 At the same time, there has been little change in the organization of HHC. 43 There has been an increase in the number of employees, but there is still a lack of geriatric care competence. Accordingly, a reactive approach to meeting the need of healthcare seems to be the predominant style, and interdisciplinary and proactive care overall is still inadequate.21,43
Conclusion
It is likely that interventions targeting factors of functional decline are most promising for successfully providing proactive follow-up of older people. However, clear clinical leadership based on common goals and effective systems for sharing information seem to be the most important preconceptions to succeed in achieving interdisciplinary proactive healthcare for home-dwelling elderly living with frailty and multimorbidity.
Implications of Findings
There is a need to develop a greater understanding of clinical leadership in HHC to enhance integrated and proactive care. The content of the leadership role and the competence required—both geriatric and leadership competence—must be the target of future research. Our results lead us to suggest that clinical leadership in nursing should be emphasized in both undergraduate and graduate nursing education. In addition, and supported by our results, programs focused on clinical leadership and interdisciplinary health team management are of great importance to strengthen and enable nurses in their role as CL.
Footnotes
Acknowledgements
We want to send a great thank you to all our participants for sharing their experiences.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Disclosure
In addition, we want to thank Professor Marit Kirkevold for her valuable contribution to the analyses and reflections in the early phase of this study.