
Abstract
There is significant literature on the existence and adverse effects of social isolation and depression among the elderly, exacerbated by the recent COVID-19 pandemic. A literature review indicates no studies of how the Medicare home health benefit addresses social isolation and depression, including no studies of home care social workers’ perceptions of the nature and consequences of Medicare coverage. This article summarizes an initial, exploratory study to address the literature gap, based on interviews of a convenience sample of 44 home care social workers from 5 different home health agencies in the New York City metropolitan area between November 1, 2021 and May 31, 2022. Six themes emerged from the study. Social workers believe: (1) extensive social isolation and depression exist among Medicare home health beneficiaries; (2) Medicare home health policy provides no systematic measure to detect or monitor social isolation and a limited measure for depression among the homebound elderly; (3) Medicare home health policy provides no coverage to treat either depression or social isolation; (4) effective interventions are available to prevent and treat depression and social isolation. Social workers also believe that: (5) the lack of social isolation and depression coverage results in additional mental and physical health conditions; (6) lack of social isolation and depression coverage exacerbates existing mental and physical health conditions. Policymakers are urged to modify the Medicare home health benefit to improve detection and monitoring of social isolation and depression as well as coverage of appropriate evidence-based preventative and treatment interventions.
Keywords
Purpose
The purpose of this study was to explore Medicare home health social workers’ perceptions of the extent of social isolation and depression among Medicare home health beneficiaries; whether the Medicare home health benefit effectively addresses social isolation and depression as well as the consequences for not meeting patient needs.
Establishing Context
There is evidence of significant prevalence and adverse impacts of social isolation and depression on the elderly population.1,2 Extensive literature has established social isolation as a risk factor for depression and vice versa.1-4
A report from the National Academies of Sciences, Engineering, and Medicine (NASEM) points out that more than one-third of adults aged 45 and older feel lonely, and nearly one-fourth of adults aged 65 and older are socially isolated.1,2,5
As regards depression, Various studies have estimated the rate of depression among the elderly in the United States at anywhere between 5%, among all community dwelling elderly, with home-based setting estimated at 13.5%.6,7 For Medicare home health beneficiaries, Avalere Health reported that in 2015, 44% of all Medicare home health users had a Serious Mental Illness (SMI), “defined as having depression or other mental disorder, including bipolar disorder, schizophrenia, and other psychoses” 8 (p. 28). This rate compared to only 32% among all Medicare beneficiaries. 8 Of those Medicare home health users with SMI, 94% had depression and 31% had another mental disorder. 8 A review of 2021 Medicare data made similar findings. 9
Research also has established several types of interventions which are the most effective as a prevention or treatment to reduce elderly social isolation and depression, including group-based interventions, such as support groups and activity-based groups; interventions facilitating transportation to group activities; person-centered interventions, such as cognitive behavioral therapy; and increased access to and use of computers and other technologies.1,2,5
Medicare home health beneficiaries are required to be homebound to be eligible, thus increasing their likelihood of being socially isolated and depressed.10,11 Despite evidence of this situation and effective interventions, the Medicare home health benefit, under original Medicare, covers only limited individual therapy, no group therapy, and no transportation to outpatient sites where such therapy or social interaction might occur.11,12 The limited social work coverage contributes to social work historically being 1% or less of all national Medicare home health visits. 12
Literature Review and Study Rationale
The article addresses a gap in the literature and presents the results of an exploratory research study of 44 home care social workers from 5 different home health agencies in the New York City metropolitan area between November 1, 2021 and May 31, 2022. The study used interviews, averaging 45 minutes each, to explore Medicare home health social workers’ perceptions of the extent of social isolation and depression among Medicare home health beneficiaries; whether the Medicare home health benefit addresses social isolation; and the consequences for not meeting patient needs.
A literature review was conducted to determine the nature and extent of existing literature on the impact of the Medicare home health benefit eligibility and coverage on beneficiary social isolation and depression. The literature review used CINAHL, PubMed, Medline, Cochrane Library, Campbell Collaboration, PsycINFO, Sociological Abstracts, and Social Science Abstracts databases with a search period of January 1, 1965 through August 31, 2021, followed by an updated search after the study was conducted covering September 1, 2021 through August 31, 2022. Multiple keywords were used by applying Boolean search strategies, including: social isolation and home care; depression and home care; homebound older adults; home care social work; elderly social isolation; elderly depression; social determinants of health; and Medicare home health.
The literature review found no studies on home care social workers or other home care service providers’ perceptions of the nature, extent, and impact of social isolation or depression on Medicare home health beneficiaries. However the literature review found 3 studies on how home care nurses perceive the Medicare home health benefit addresses depression, asserting both assessment and treatment are inadequate.13-15
Bao et al 13 conducted semi-structured interviews with 6 directors, 5 supervisors and 9 nurses from 5 home health agencies using the CAREPATH nurse-delivered depression care management home health intervention in 5 states. Among their findings, they concluded that several Medicare home health policies, including Medicare’s homebound eligibility requirement and the lack of mandated treatment for patients with assessed with depression, were “misaligned with evidence-based depression care for home health patients” 13 (p. 905).
Liebel and Powers 14 conducted 2 focus groups and 16 semi-structured interviews with home care nurses and followed nurses on 25 visits to patients. The results focused on nurses’ experience with depression assessment and treatment and did not focus on patients’ outcomes. Among the results were nurse confusion and variation of interpretation of the depression screen in the nationally mandated Outcome and Assessment Information Set-C (OASIS-C) and limited nurse knowledge about managing depression.
Liebel et al 15 did a retrospective chart review of 100 new Medicare home health admissions. Their results focused on nurse compliance with evidence-based depression care management (DCM). They concluded that despite existing evidence of DCM with patient improvement “inadequate compliance to evidence-based DCM was found” and that Medicare and home health agencies “must ensure compliance to DCM, including follow-up depression assessment for patients with positive screens” 15 (p. 794).
Study Method
The study used a grounded theory approach. 16 Grounded theory is the research methodology of choice because it was developed for interpreting qualitative data in the absence of a pre-existing theory. The present study addresses a gap in the existing literature which does not provide insight into home care social workers’ perceptions of the nature, extent, and impact of social isolation and depression on Medicare home health beneficiaries. Data were collected through interviews of 44 home care social workers, selected from 5 different home health agencies in the New York City metropolitan area from November 1, 2021 to May 31, 2022.
Participants were selected using a snowball convenience sampling technique, whereby home care social workers known to the author constituted the initial interviewees and then identified other potential interviewees to the author. In-person interviews averaging 45 minutes each were conducted at locations convenient to participants and off-site from where they worked. Interviews were audio recorded and transcribed verbatim. No payments or other incentives were given to the interviewees. Social workers were selected as the study focus because the Medicare home health social work benefit is the only one of the covered services in Medicare home health designed to address psychosocial care, including issues related to assessing and treating social isolation, depression, and other social needs.11,12
A semi-structured interview guide was used to help standardize the data collection. The interview guide was developed by the author and reviewed by 2 other PhD-level home care researchers. All participants were assured of anonymity and confidentiality through an informed consent they signed. Interviews were audio recorded and transcribed verbatim. Qualitative analysis began shortly after the initial data were collected and resulted in additional questions and probes that were applied to subsequent interviews, in an ongoing iterative process. Analysis followed the grounded theory 3-stage coding of interview data: open, axial, and selective coding.
Open coding was used to fracture the data to “identify some categories, their properties, and dimensional locations” 16 (p. 97). The coding and classification generated a list of 317 codes. Code and category labels were created, systematically sorted, compared, and contrasted until they were complete, with no new codes or categories produced and all data accounted for. Through axial coding, multiple phenomena were identified from the connected categories and subcategories. These phenomena included the Medicare decision-making framework; social workers’ perceptions of the nature and extent of social isolation among Medicare home health beneficiaries; social worker perceptions of the impact of Medicare home health benefit in detecting and treating social isolation among Medicare home health beneficiaries; and social worker perceptions of policy changes necessary to improve detecting and treating of social isolation among Medicare home health beneficiaries. Finally, using selective coding, a “story line” was identified and a “story” written that integrated the axial coding phenomena. 16 The story that emerged was home care social workers’ perceptions that the Medicare home health benefit ignores the significance of social isolation and depression among home health beneficiaries, thus creating additional adverse consequences and fails to prioritize the detection and treatment of social isolation and depression by not covering evidence-based interventions and assessment measures.
In keeping with the grounded theory approach, the data analysis and interpretation were facilitated by analytical and self-reflective memo writing, which helped move empirical data to a conceptual level; expanded and refined the data and codes; developed core categories and interrelationships; and integrated the experiences, interactions, and processes embodied in the data. 16 All initial abstraction, analysis, and interpretation were done by the author of this article. After the initial process, all abstraction, analysis, and interpretations were reviewed by 2 additional experienced qualitative researchers. Any differences were discussed by the 2 external reviewers and the author to reach final decisions used for the study results. All analyses were done using ATLAS.ti software.
Study Participants
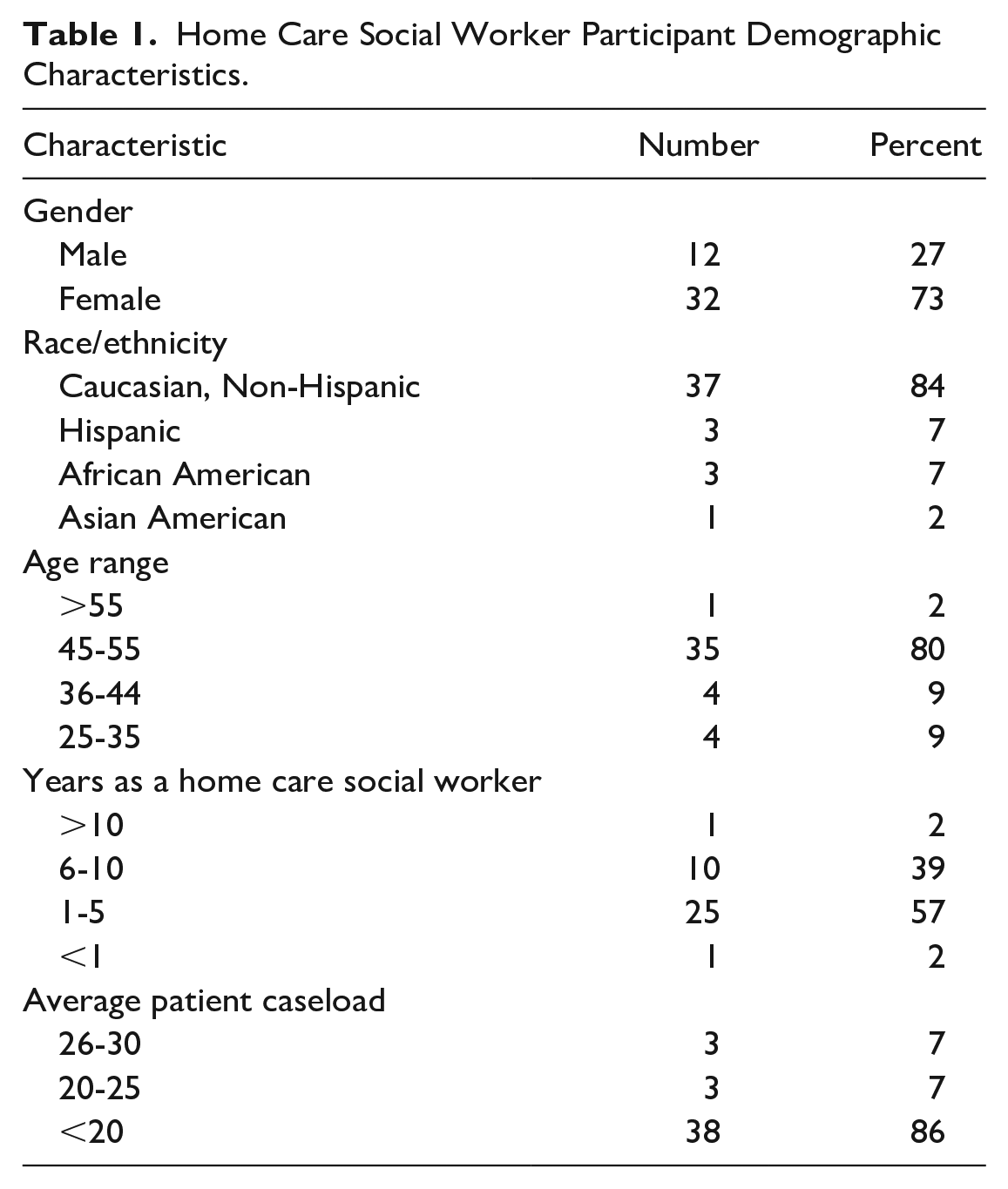
Limited demographic data were collected from study participants using a short survey. The results appear in Table 1. Overall, the social workers were 45 to 55 years old (80%); female (73%); Caucasian, non-Hispanic (84%); had 1 to 5 years of home care experience (57%); and had an average caseload of less than 20 patients (86%). Statistical analysis of the demographic variables’ impact on study outcomes was not done due to the qualitative nature of the study.
Home Care Social Worker Participant Demographic Characteristics.
Study Results
Six themes emerged from the study. Social workers believe: (1) extensive social isolation and depression exists among Medicare home health beneficiaries; (2) Medicare home health policy provides no effective systematic measure to detect or monitor social isolation or depression among the homebound elderly; (3) Medicare home health policy provides no coverage to treat either social isolation or depression; (4) effective interventions are available to prevent and treat both depression and social isolation; (5) the lack of social isolation and depression coverage results in additional mental and physical health conditions; and (6) the lack of social isolation and depression coverage exacerbates existing mental and physical health conditions. The social isolation and depression results from the interviews are presented below in separate sections.
Results of Interviews on Social Isolation
Social Isolation is an Extensive Unmet Need for Medicare Home Health Beneficiaries
All social workers interviewed agreed that social isolation is a major issue among Medicare home health beneficiaries. As Social Worker TL said, “They live in an isolation chamber.” She continued, noting: Most of our patients live alone or with someone who also has significant limitations. They have no interaction with anyone but themselves. Yes, they are isolated.
Social worker UH supported this view, stating: Of course, there is social isolation and it is extensive. They are homebound. That is an eligibility requirement to receive Medicare home health. That makes you de facto isolated. You can rarely get out of the home on your own and Medicare [home health] does not cover any assistance to get you out of your house to socially engage with others. Talk about being socially isolated.
According to 2020 Medicare data, Medicare home health beneficiaries are more prone to live alone (36.6%) than all Medicare beneficiaries (29.7%). 9
Medicare Home Health Policy Provides No Systematic Measure to Detect or Monitor Social Isolation Among the Homebound Elderly
All social workers interviewed also agreed that Medicare does not require an initial, ongoing, or at-discharge assessment of a beneficiary’s social isolation status. As one social worker noted: We know most of our patients are socially isolated if we get to see them. Even the ones we do not get to see are socially isolated-just ask any nurse. But these are not professional assessments. These are based on our professional knowledge and interaction with the patient. Medicare does not see this [social isolation] as an important enough issue for us to assess, monitor and treat. It’s not like wound care or diabetes. It’s not medical so, to them [Medicare], it doesn’t exist, but to us, and the patient, it does exist. Social Worker NR It’s not like there are not any measures out there to measure social isolation. There are, so why don’t they [Medicare] require us to use them, like as part of the OASIS? Social Worker FG
Social workers NR and FG were historically correct. In fact, until January 2023, the national Medicare home health mandatory home health Outcome Assessment and Information Set (OASIS) assessment measure did not contain any scale or other measure of social isolation, with the only psycho-social measure required within the OASIS being the Patient Health Questionnaire-2 (PHQ-2) for depression, though there is no requirement to treat a patient’s depression based on their score on the PHQ-2. 17 However, the new OASIS-E, which takes effect January 2023, includes a new item (D-0700. Social Isolation) which asks “How often do you feel lonely or isolated from those around you?” with 6 patient self-reported options: never, rarely, sometimes, often, always, and patient unable to respond. 18 The D-0700 item is not based on an evidence-based scale and does not require any clinician follow-up action based on the score. The federal Agency for Healthcare Research has identified multiple evidence-based measures to assess social isolation. 19
Medicare Home Health Provides No Coverage to Treat Social Isolation
Virtually all home care social workers interviewed (43 of 44, or 98%) agreed that Medicare home health provides no coverage of social isolation. Most agreed that social isolation was either created or exacerbated by Medicare’s lack of coverage of resources to facilitate social interaction outside the home.
They can get there [to activities outside the home], but not alone. They are homebound. That means the transportation and personal care assistant necessary to get to the group activities, and the group activities themselves, need to be covered [by Medicare]. They are not. Social Worker TD We can’t even promote social interaction in the home. They [Medicare] barely allow us [social workers] to do any individual therapy with the patient. We can do dyad therapy with the patient and their spouse or significant other in the home. And then they [Medicare] won’t provide personal care assistance and transportation to get them [the patients] to a group setting outside the home. Even if the patient manages to get to an activity outside the home, Medicare [home health] will not cover any cost involved, so it has to be free, like a senior center, if they [the patent] qualifies and can get there. It is so frustrating. Social Worker HJ
The social workers’ perceptions are correct. Medicare home health only covers psychosocial care by social workers, which is limited to in home individual therapy, no group therapy, and limited other supports by social workers, resulting in Medicare social work being 1% or less of all national home health visits.11,12
Effective Interventions Are Available to Prevent and Treat Social Isolation
All social workers interviewed agreed that Medicare home health could do more to prevent and treat social isolation.
Of course, Medicare could do more. They could cover transportation services for these people and personal care assistants to accompany them. Then they could cover going to senior centers or adult day care or community centers or group therapy. They could do that, but it would mean more money. Social Worker LT All I ever hear about is the home health industry worrying about how much they get pad. They are always mobilizing us providers whenever Medicare proposes [payment] cuts. Well, what are they spending the money on. That should be their concern. The money does not cover a lot of what needs to be covered so what’s the point if the care we give does not address underlying patient needs. Why are we providing care? Social Worker SD
Lack of Coverage of Social Isolation Results in Additional Mental and Physical Health Conditions
Virtually all (42 of 44, or 95%) agreed that failure to identify and address social isolation results in additional mental and physical health conditions.
They are homebound so they are isolated. Because they are isolated, they get depressed. Then because they are depressed, they get more isolated. It is a vicious cycle. Social Worker SG Imagine this. You sit around most of the day seeing the same four walls. What do you think will happen? You have no human contact, or you have an elderly spouse who also is in bad shape so then you get anxious about every little thing that happens. I see this all the time. I’m convinced if these patients could get out more, yes with assistance, they would not get so anxious and depressed. Social Worker RE Here is a scenario I often see. You have these homebound patients who get so frustrated sitting around at home and not being able to get out–the poor ones don’t even have a TV or computer–that they just push themselves to get up and go out, alone, with no help. They fall and there they are with a medical problem they didn’t have before. Social Worker FB
Multiple studies have associated social isolation with increased occurrence of mental health and physical health conditions, particularly falls, depression, and anxiety.2,20,21
Lack of Coverage of Social Isolation Exacerbates Existing Mental and Physical Health Conditions
All social workers interviewed agreed that failure to identify and address social isolation exacerbates existing mental and physical health conditions.
Yes, of course [not addressing social isolation] makes things worse. I see it all the time. I had a patient who was really depressed. He had a high score on the PHQ-2 part of the OASIS. Well, all he did was sit around all day with no contact from anyone except when I or the nurse or [home health] aide came to visit. We were his social life. So, yes, of course, he got more depressed, even tried suicide. This is not unusual. Social Worker KP It is so ridiculous that they [Medicare] does not let us address social isolation. They make it as though it has nothing to do with physical health, which is bogus. We all know the two [physical and mental health] are inter-related. So you stay at home, homebound no less, and that further limits your mobility, you get no exercise, and then that increases your risk of falls, so then you get a broken arm, leg, hip or badly bruised. I can’t tell you how many patents I see where this happens as and the [home care] nurses tell me the same thing. Social Worker TY
Results of Interviews on Depression
Extensive Depression Exists Among Medicare Home Health Beneficiaries
All social workers interviewed agreed that depression is a major issue among Medicare home health beneficiaries. As Social Worker GK said, noting: “Of course they are depressed. Wouldn’t you be if you were homebound and elderly?”
Social worker TW supported this view, stating: It is the norm. All the patients we get, which are not many, are depressed and most are very depressed. We only get patients if the nurses refer them to us. They don’t refer many to us because they focus on physical health and that is where the money is. But I talk to the nurses. They [also] say virtually all their patients are depressed and need help, regardless of how they score on the OASIS.
Medicare Home Health’s Mandatory Assessment for Depression is Limited Because It is Done by Nurses, Not Social Workers
All social workers interviewed also agreed that Medicare home health’s mandatory assessment for depression is limited because it is done by nurses, not social workers. As one social worker noted: This is ridiculous. Your average nurse is not trained to do psychosocial assessments or interventions. That’s at the core of social working training. Why are they doing that? What was Medicare thinking? Social Worker ER
Another social worker echoed her view: The nurses hate doing it [the PHQ-2 assessment in the OASIS]. They hate doing anything that is behavioral, you know, mental health related. That is not their focus. They don’t get trained in it. They are focused on short-term physical health issues, and legitimately so. This mental health stuff they see as a burden, taking up valuable real patient care time. Social Worker SL
Another social worker, Social Worker MS, added, “Are they [Medicare] kidding us. We are trained to do psychosocial assessments, nurses aren’t, so why are nurses doing them?”
The social workers views are supported by the Bao and 2 Liebel et al studies of nurse perceptions cited earlier in this article.13-15
The national Medicare home health mandatory home health Outcome Assessment and Information Set (OASIS) assessment measure did not contain any depression measure until the OASIS-C in 2009.22,23 The OASIS-C added the Patient Health Questionnaire-2 (PHQ-2) for depression, though there is no requirement to treat a patient’s depression based on their score on the PHQ-2. 19 The new OASIS-E, which takes effect January 2023, revised the PHQ-2 in Section D, but still does not require treatment of a patient’s depression based on the revised measure score. 19
The Section D change replaces the previous M1730 item, which assessed mood based on the Patient Health Questionnaire-2 (PHQ-2), an evidence-based measure, with a new D0150 item titled “Patient Mood Interview” and a resulting D0160 item titled “Total Severity Score.” The new items combine the PHQ-2, which focus on symptom presence and frequency, with the Patient Health Questionnaire-9 (PHQ-9), another evidence-based measure, which focuses on severity. There are no instructions on what the assessing clinician should do in terms of further assessment, plan of care development, or treatment based on the patient’s score.
Medicare Home Health Does Not Require Treatment of Assessed Depression and Provides No Coverage for Treatments, Despite Existence of Evidence-Based Interventions
Virtually all home care social workers interviewed (43 of 44, or 98%) agreed that Medicare home health does not require treatment of assessed depression and provides no coverage for treatments, despite existence of evidence-based interventions.
It’s a debacle. Here we are with all these depressed homebound patients, the nurses assess for the depression, and then treatment is voluntary for the home health agency. There is no requirement the agency must treat what we’ve assessed as a clinical need. Is that fair, ethical, legal? Sometimes I wish some patients, or an advocacy group would sue [the Centers for Medicare and Medicaid Services] to get them to cover depression treatments that have been assessed as a need. Social Worker PL Now, they [Medicare] would never do this if it were wound care, diabetes, or some orthopedic or hear or respiratory condition. Those get assessed and they get treated. So, tell me, how is a mental health condition like depression any different? I’ll tell you why. It is because this whole Medicare home health benefit and the payment is driven by physical health. That’s it. Mental health is the patient’s problem. They barely cover any social work for us to help the patient at all. It’s not right. Social Worker HJ
The social workers’ perceptions are correct. As noted earlier, OASIS never has required the home health agency to treat a patient based on their depression assessment score.19,22 Furthermore, social workers have a limited ability to provide the care. Medicare home health only covers psychosocial care by social workers, which is limited to in home individual therapy, no group therapy, and limited other supports by social workers.
The Lack of Coverage for Assessed Depressed Patients Results in Additional New and Exacerbates Existing Mental and Physical Health Conditions
All social workers interviewed agreed that the lack of coverage for assessed depressed patients results in additional new and exacerbates existing mental and physical health conditions.
Of course, there are negative consequences. I know from my social work education and taking to the nurses that these [physical health and mental health] conditions are inter-related. They affect the other so when one gets worse the other gets worse or if one occurs, like being homebound because of diabetes or bad wounds, it increases the likelihood you will feel isolated, depressed, or worse. We all know suicide is tied into isolation and depression. Social Worker AL It happens all the time. I have seen it with y patients and the nurses tell me the same. A patient comes in because of a physical problem, you know they need that to be [Medicare home health] eligible, right? So, they come in with this physical issue and are homebound. They become depressed. It’s even worse if they come in depressed already and have the physical problem. Ugh. I feel so helpless just sitting there and watching it get worse. The nurses feel the same way, but they are not required to deal with the depression and don’t have the skills, so it doesn’t get done and he patients get worse. Social Worker TN
Multiple studies have associated depression with increased occurrence of mental health and physical health conditions, particularly falls, depression, and anxiety.12,17,20,24
Limitations
The study was a qualitative, exploratory study. As such it does not address causality and has several limitations including: small sample size; lack of random sampling for sample selection; use of a sample of home care social workers only from 5 agencies in the New York City metropolitan area; and lack of a randomized controlled trial experimental design to test specific interventions against a control group.
Discussion and Policy Options
Despite its limitations, the study does begin to address a gap in the literature and policy by Medicare home health social workers’ perceptions of the extent of social isolation and depression; whether the Medicare home health benefit addresses social isolation and depression; and the consequences for meeting patient needs. The social workers’ perceptions revealed through the interviews are supported by significant professional literature on the topic. Two national reports have recognized the inter-related nature of physical and mental health conditions and recommended that both Medicare and Medicaid expand integrated assessment and coverage of social and medical needs in multiple settings, including in the home and including social isolation and depression.2,5 Medicare data from 2020 indicates the health conditions of Medicare home health beneficiaries are substantially worse than all Medicare beneficiaries. There are several possible policy routes to achieve such policy reform.
Based on the study results, there are 6 policy actions recommended:
(1) The United States Department of Health and Human Services (USDHHS) should propose revision of the OASIS forms to include an evidence-based measure of social isolation. The current D-0700 item is not evidence-based and does not require any action by a clinician based on the item score. 18
(2) The USDHHS should establish an evidence-based score threshold that would require the home health agency to take affirmative action on social isolation and likewise on depression assessed by the PHQ-2/9.
(3) Medicare should allow social workers to administer the social isolation and depression assessments in OASIS, and possibly other psychosocial assessment, with or separate from nurse assessments.
(4) USDHHS should publish a list of evidence-based social isolation and depression interventions and cover payment for any intervention on the list.
(5) USDHHS should cover transportation and personal care assistance to improve access to interventions and programs outside the home which are useful in decreasing depression and social isolation.
(6) Expand the scope of therapy permissible by Medicare home health social workers so they could implement evidence-based social isolation and depression interventions.
Conclusion
Given these data it seems policymakers should immediately consider improving both patient care and reducing costs in Medicare by: requiring initial and ongoing assessment of social isolation; allowing social workers to administer depression and social isolation assessments in OASIS; and expanding Medicare home health social work coverage of interventions proven to effectively address social isolation and depression, both of which are already available to enrollees in Medicare Advantage plans.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.