
Abstract
Cera, a homecare provider, uses digital care plans (DCP), to streamline the provision of home care. DCP rollout is part of a larger digitization initiative, including carer visit reports collected through a mobile app and branch actions recorded in a web application supported by a secure central database. This retrospective cohort study aimed to assess the association of a DCP rollout with service user hospitalization rates. his study utilized retrospective data from 2 groups of service users, those for whom their first 30 days of Cera membership occurred prior to DCP rollout (pre-DCP group) versus those whose first 30 days of Cera membership occurred after DCP rollout (post-DCP group). The 30-day hospitalization rate was the primary outcome measure and was determined through a combination of carer reports, reporting from service users or their families, and branch staff follow-up. There were 55 hospitalizations among 392 users in the pre-DCP group in the 30 days after joining Cera (14.0% hospitalization rate), compared to 23 hospitalizations among 297 users in the post-DCP group (7.7% hospitalization rate). This represented a significant reduction in hospitalizations in the post-DCP group (6.3% absolute difference in hospitalization rate; 45% relative reduction; P < .001). This result was robust to multiple sensitivity analyses. The implementation of a DCP was associated with a 45% relative reduction in the 30-day hospitalization rate for new service users when compared to pre-DCP enrollment. These benefits could be further amplified by combining the DCP with additional initiatives aimed at the prediction and prevention of avoidable hospitalizations.
Introduction
Healthcare systems around the world are seeing increasing strain from the combination of an aging population, rising demand, and spiraling care costs.1,2 One approach to addressing this in the UK has been to encourage a shift from hospital-based to community-based care for the large majority of patients that do not require inpatient services.3,4 This entails supporting people to manage their health and wellbeing by bringing community support to them. For those with significant support requirements, this might consist of a nursing or residential care placement with remote GP visits. However, many others can be cared for in their own home. Home (or domiciliary) care is important for providing people with support while allowing them to maintain independence and autonomy as they remain in a familiar environment.5,6 It might also be more cost-effective than institutionalized care though conclusive evidence is lacking. 4
While providing home care is a popular option, there are constraints in terms of staffing and logistical requirements. For example, the limited pool of carers means that there is a drive to ensure appointments with service users are as efficient as possible. 7 Every additional administrative task or activity not directly related to care can reduce the overall time available for carers to support service users as well as to spot any deteriorations in their underlying health.
The approach taken by Cera, a home care provider, is to digitize the provision of home care with 2 main aims. 8 First, it reduces the administrative burden of recording and managing care activities, through digital automation, thereby freeing up carers to spend more time on direct care activities with service users. Second, it facilitates more seamless and scalable data collection which can then be used for service improvement purposes. Eventually, this data may also help with tasks such as predicting and preventing downstream adverse events such as hospitalization. 9 If this proves possible, it would be helpful to ascertain what, if any, improvement there is in hospitalization rates purely arising after the rollout of the digital care plan but before any further “predict and prevent” programs are launched.
We aimed to assess the impact of the rollout of a digital care plan (DCP) among new service users on a set of branches that Cera acquired from alternative providers that had previously used a non-digitized care system. We hypothesized that the net effect of the rollout would lead to more time spent on direct care, smoother operating processes and that this could thereby reduce hospitalization rates.
Methods
Cera Care is a technology-enabled home care provider registered in the United Kingdom. 10 The people using home care services are referred to as “service users” rather than “patients” as they are not necessarily receiving support for a specific medical condition.
Home care is typically provided in the UK by a hub and spoke model in which a local branch operates as a base for carers to see service users in the nearby area. Appointment frequency and intensity vary according to the needs of the service user. As part of its expansion plans, Cera acquires branches from other providers from time to time. The operating protocols for these branches then switch to the Cera operating model encompassing a digital care platform (which incorporates many digital records including the digital care plan (DCP) for each service user). This occurs during the post-acquisition process. The DCP rollout date is distinct from the branch acquisition date.
The digital care platform itself encompasses an end-to-end system for the planning, recording and monitoring of all care activities taking place in Cera branches. The focus of these analyses are on the digital care plan (DCP) which is one component of the overall digital care platform. Carers have a secure app on their phone containing service user details as well as a list of questions to ask and tasks to carry out during the visit. These are recorded and transmitted to a secure central database where the data can be used for auditing, planning, and service improvement purposes. This compares to the traditional paper-based model of carers filling in paper reports of their visits to service users and then submitting these to be filed with the local branch office.
When a new service user joins a Cera branch that has transitioned to the DCP, their care records are processed through the digital care platform from the very start of their membership. However, existing users require their old paper records to first be transitioned over to the new system. Therefore existing service users experience a delay before the full benefits, if any, of the DCP can be realized. For this reason, we chose to concentrate our analysis on new service users joining a branch and proceeding straight onto the DCP. A new service user is defined as one who has (i) joined after branch acquisition, (ii) within the 90 days pre- or post-DCP rollout, and (iii) remains a member of Cera for at least 30 days.
Hospitalization of service users is ascertained from a combination of carer reports, direct reporting from service users or their families and follow-up from branch staff. This data is also recorded centrally by Cera (or prior to acquisition by the previous care provider).
We compared hospitalization rates for 2 groups of new service users, those for whom their first 30 days of Cera membership occurred prior to DCP rollout (pre-DCP group) versus those whose first 30 days of Cera membership occurred after DCP rollout (post-DCP group). Cera has a range of quality assurance processes for data collection that ensure, for example, a minimal likelihood of data leakage between pre- and post-DCP groups by verifying the date of hospitalization from at least 2 sources (where possible).
To ensure the robustness of this comparison, we also assessed as a sensitivity analysis the comparison between the post-DCP group and an empirically constructed distribution (to act as another form of control) using a stratified bootstrap method. The empirical distribution was constructed by drawing 1000 samples with replacement (of identical size to the post-DCP group) and measuring the hospitalization rate. This process was conducted at 2 levels (once at the branch level and once at the level of all branches). This sensitivity analysis will tend toward underestimating the impact of the DCP as the samples encompassing the empirical distribution are drawn from all new service users (ie, those pre- and post-DCP rollout). Therefore if there is truly a reduced hospitalization rate in the post-DCP group, it will be seen less often in the bootstrapped samples.
Another sensitivity analysis was conducted by looking at service user hospitalization among 24 branches that did not transition. The comparison to the control branches was conducted by extending the bootstrap analysis. To create a synthetic example, branches were sampled from those that did not deploy DCPs and assigned a date sampled from the rollout dates in the branches that did deploy DCPs. This was repeated 100 times and in each case, the bootstrap analysis was performed.
We also furthered this analysis using a difference-in-differences approach by directly comparing the change in user hospitalizations in branches that did and did not deploy DCPs. Three dates were identified when branches had transitioned to DCPs. On each date, the branches rolling out DCPs were selected and the hospitalization rate before and after rollout was compared with the hospitalization rate before and after the transition date in the 24 branches that did not transition. The difference observed was then compared against an empirically constructed distribution constructed by drawing 1000 samples with replacement from both the transitioning and non-transitioning branches and calculating the differences. This analysis takes into account any secular trends over time that may contribute to the impact on hospitalization rates following the rollout of DCP.
The analyses in this manuscript were conducted using retrospective anonymized data from Cera and therefore formal ethical approval was not sought. All service users sign an agreement upon joining Cera including clauses on how their data will be processed and used. This work aligns fully with the provisions of those clauses and falls under the remit of service improvement efforts at Cera.
Results
Sixteen branches representing a range of geographical regions in the UK transitioned to the DCP between 30th March 2021 and 5th July 2021. Seven hundred sixteen service users formed the pre-DCP group and 604 users formed the post-DCP group.
The hospitalization analysis was conducted for only users who had 30 days of post-joining data that did not overlap with the DCP rollout date. Their demographics are displayed in Table 1.
Comparison of Service User Characteristics in New Joiners Before and After the Rollout of Digital Care Plans (DCPs).
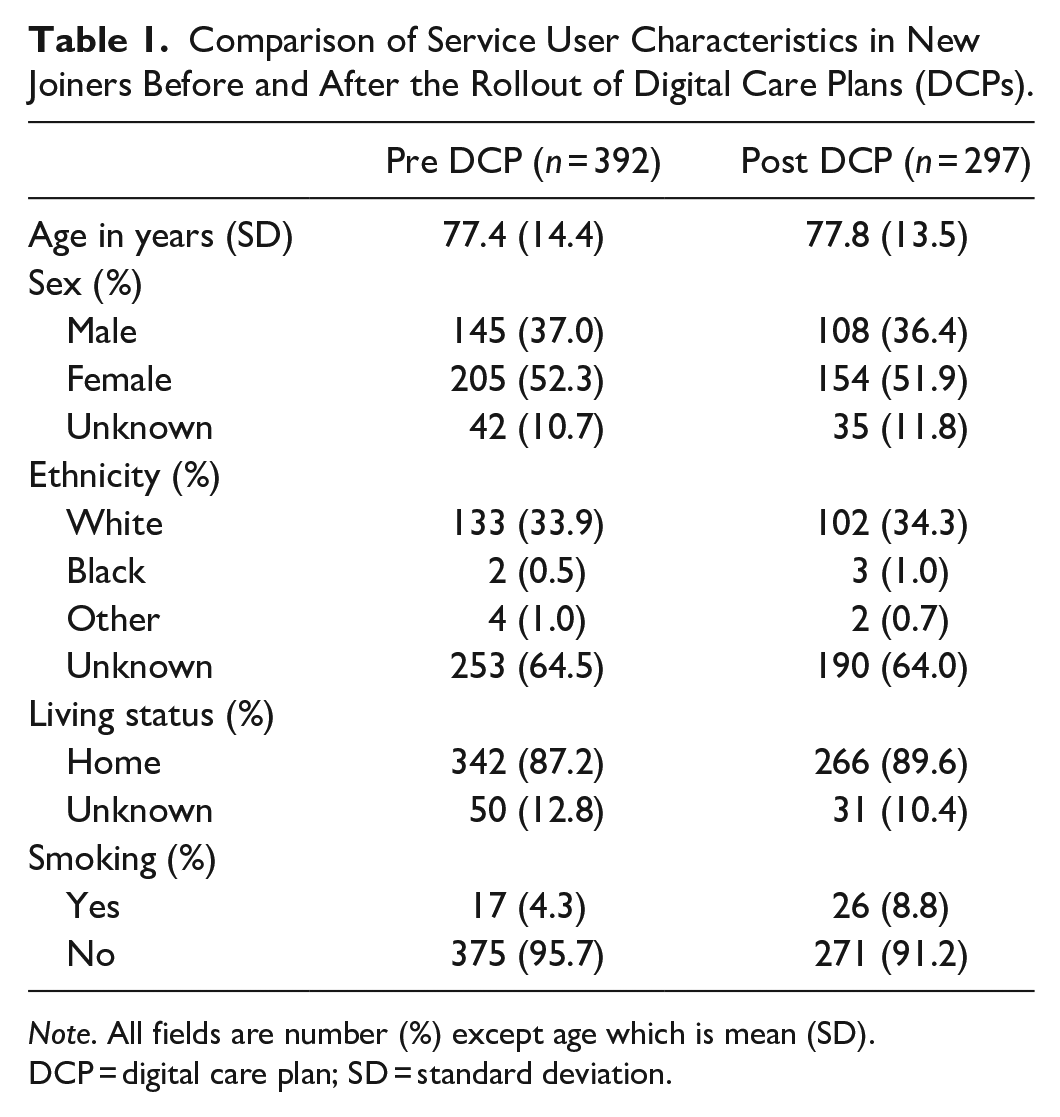
Note. All fields are number (%) except age which is mean (SD). DCP = digital care plan; SD = standard deviation.
There were 55 hospitalizations among 392 users in the 30 days after joining Cera for the pre-DCP group representing a 14.0% hospitalization rate compared to 23 hospitalizations among 297 users in the 30 days after joining Cera for the post-DCP group representing a 7.7% hospitalization rate. This 6.3% absolute difference in hospitalization rate (45% relative reduction) was significant at the P < .001 level when analyzed under the bootstrap sampled sensitivity analysis (Figure 1).
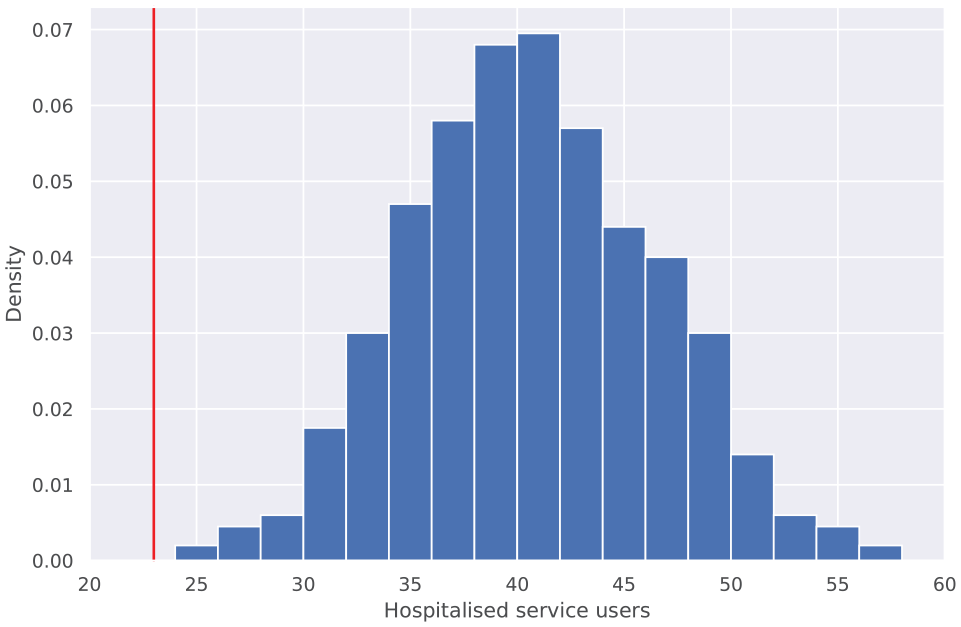
Distribution in the number of service users joining after the rollout of digital care plans predicted by bootstrap analysis to be hospitalized in their first 30 days. The solid vertical line indicates the number of newly joined service users actually observed to be hospitalized in their first 30 days following the rollout of digital care plans. In none of the 1000 trials was the actual number of post-digital care plan hospitalizations observed.
Among control branches, there were no instances among the 100 bootstrapped samples of a statistically significant difference in hospitalization (Figure 2). In the difference-in-differences analysis, there was an increase in hospitalizations from 3.9% in the before period to 5.7% in the after period among non-transitioning control branches (Figure 3). The reduction in hospitalizations attributable to the rollout of DCP in this sensitivity analysis, therefore, increased to 52% (up from the 45% unadjusted relative reduction) and was significant at the P < .01 level.
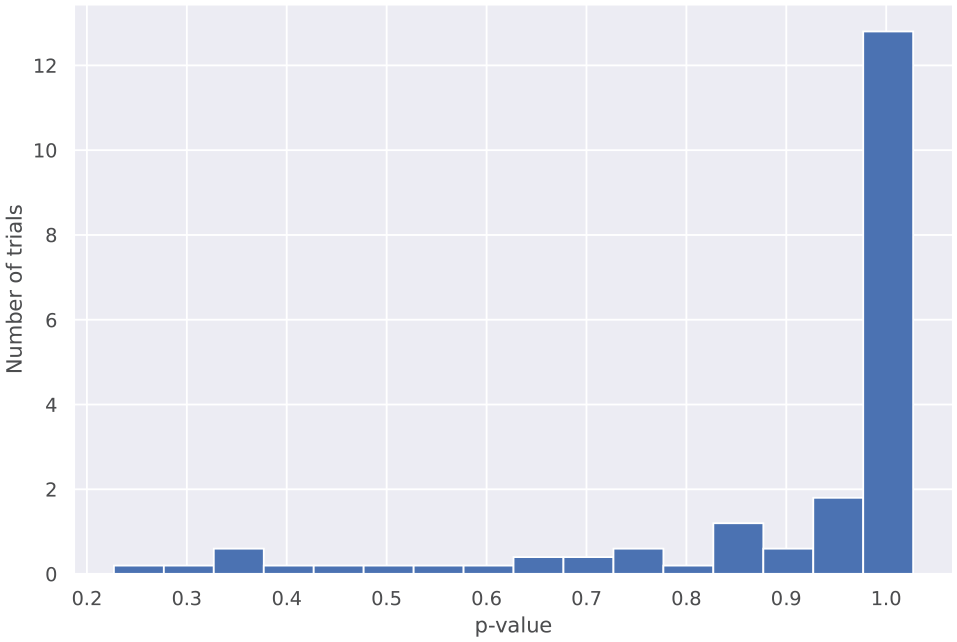
Observed P-values from bootstrap analysis conducted on a random resampling from branches that did not deploy digital care plans (DCPs). The lowest P-value observed in 100 trials was .223.
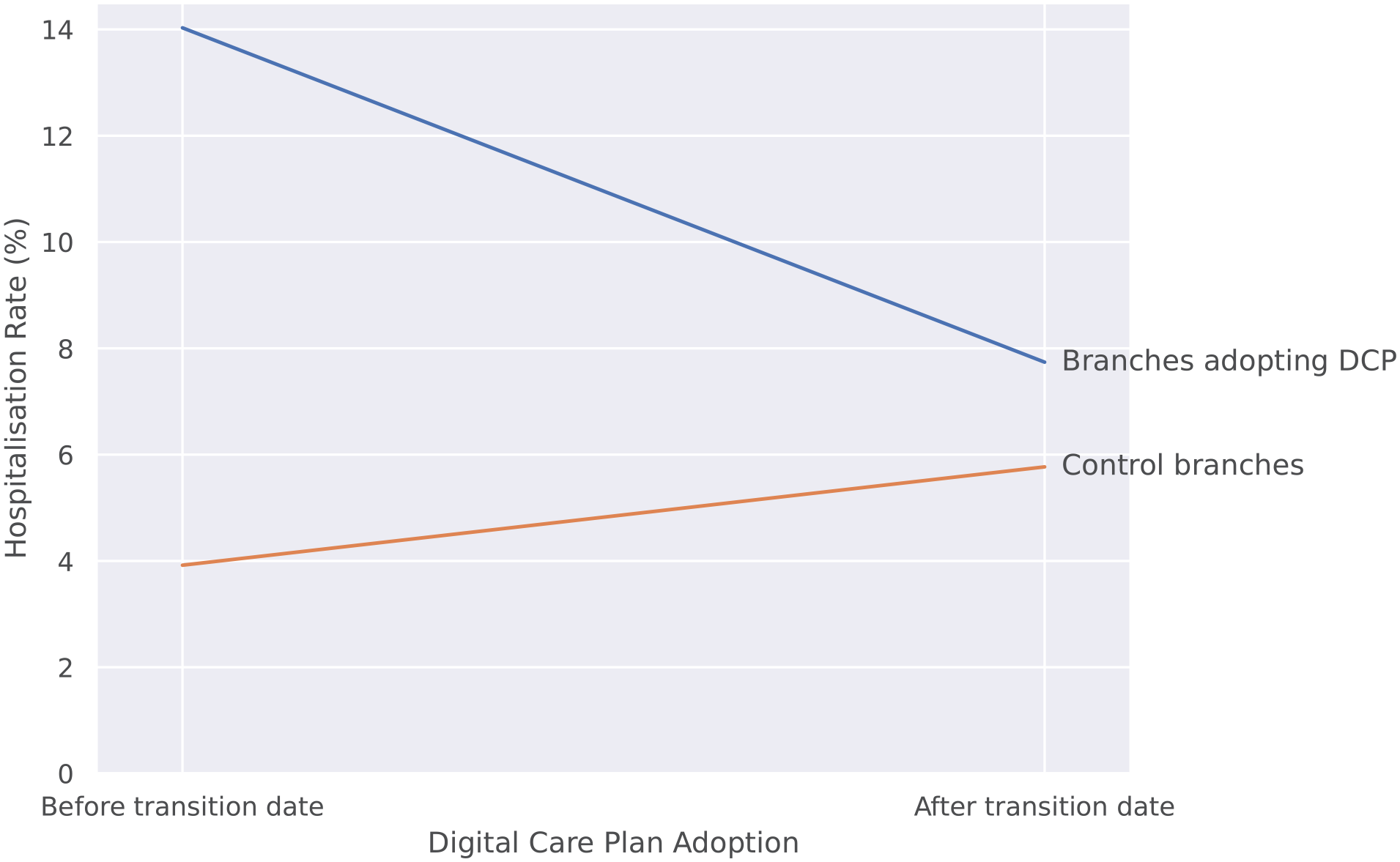
Comparison of hospitalization rates before and after the adoption of digital care plans with the hospitalization rates in control branches. Hospitalizations fell from 14% to 7.7% in branches adopting digital care plans compared to an increase from 3.9% to 5.8% in branches not adopting digital care plans during the same period.
Discussion
The key finding from this study is the reduction in the rate of hospitalizations of approximately 45% for new service users who joined Cera and were managed after the rollout of the DCP compared to those managed before. We performed sensitivity analyses which confirmed the robustness of these findings. These findings are likely to become more robust over time as more branches are acquired by Cera and rolled onto the DCP and thereby become available for inclusion within the current analyses.
Findings in Context
There is a paucity of existing literature on digital technology rollouts in the home care sector. Even in the secondary care sectors of advanced health systems such as the US, the speed of digital rollouts has typically been slower and of variable utility than in other non-health sectors.11,12 It is therefore unsurprising that the community care sector has lagged behind in this respect. The reasons for this are well documented but typically include the lack of investment in the social care sector, the fractured nature of the provider supply network and a lack of standardization in community digital health records and digital software.13,14 Despite this, efforts are now underway to prioritize digitization of both residential and home care in line with a renewed strategic focus by the NHS on digitization of health services in general, and accelerated in part by the need for remote consultations and monitoring during the COVID-19 pandemic. 15
The findings from our study should be viewed in the light of other initiatives such as the Care City testbed which is funded by NHS England and aims to bring the right stakeholders together to make the implementation of digital technologies in the community a reality. One of their first pilots involved measuring the vital signs of service users with appropriate triage if abnormalities were detected.13,16 An important prerequisite for the sustainable success of such initiatives is a robust underlying digital infrastructure to record and relay health data of service users as well as having their care plans seamlessly updated. In short, the right infrastructure needs to be in place to store incoming data and show it to the right stakeholders. This is the first step that Cera Care has taken with the launch of digital care plans and it lays the foundation for future prediction and prevention initiatives. The purpose of this analysis was to assess if this rollout alone might be associated with a reduced hospitalization rate which seems to be the case.
Implications
Acknowledging the limitation that the findings between DCP rollout and reduced hospitalization are not necessarily causally related, there are nonetheless major implications that arise from this study. The care sector is under significant strain and therefore any efforts to improve either accessibility, quality, efficiency or some combination thereof while containing costs is an extremely attractive proposition. 17 Even prior to this study, there is strong plausibility for the DCP having positive impacts on all 4 of accessibility, quality, efficiency and cost containment. From the perspective of accessibility, the DCP allows a greater ratio of care to non-care activities per visit. This might allow for shorter visits and therefore more service users to receive care from the limited pool of carers. In terms of quality, the data gleaned from the DCP can be used to target possible “predict and prevent” initiatives that aim to further reduce the risk of hospitalization or adverse events. 16 Alternatively, service users can be targeted to community healthcare providers such as GPs or district nurses before their condition becomes serious enough to warrant hospitalization. 18 Where hospitalization is inevitable, interventions could reduce the overall length of admission by treating patients earlier in their disease course before they are in extremis. 19
Efficiency and cost-containment could be improved by the DCP as it allows centralization of the back-end management of providing care and reduced waste (eg, cancelled appointments not being phoned through to branches and carers still making the journeys to the service user’s house). In addition, there are also equally important second-order benefits such as the potential improvement in morale and retention of carers as well as upskilling their digital skills. 20
It is tempting to speculate on what the mechanisms behind the large reduction in hospitalizations in our study might have been caused by. Given the size of the reduction, the impact of DCP on improving efficiency alone seems unlikely to be the sole cause. It is probable that there was a more direct effect on service users at risk of hospitalization being spotted at an earlier point in their deterioration and informally triaged to extra support. Furthermore, the DCP allows key information to be highlighted and updated instantly, including up-to-date allergy and medical dosage instructions, reducing the risk of incorrect medication administration and improving medication compliance. This would also explain a more direct plausible route to reduced hospitalizations. Finally, DCPs are instantly accessible and updates can be shared with all parties simultaneously, resulting in more responsive care and the ability for carers to more effectively action changes, such as removing a falls hazard or providing additional equipment, to reduce the likelihood of a preventable hospitalization.
Limitations
The findings from this study should be considered in the context of several limitations. First, the rollout of the DCP encompassed many changes from the digitization of care plans to streamlining of databases and information stores on which branches access service user information. Therefore pinpointing the specific component that might be most beneficial to reducing hospitalizations is not possible from the existing data.
Second, the data in this study is observational and we cannot, therefore, make a statement about whether or not the DCP is fully causally related to the reduced hospitalization rate in new service users post-DCP rollout. By assessing the extent to which control branches experienced any improvement in hospitalization rates, we can to some extent negate the effect of secular trends but it is still very much possible that unmeasured confounders are responsible for some or all of the results seen.
Third, this analysis considers only a single downstream outcome: hospitalization rate. While this is a severe adverse event and one of major importance to both service users and the wider health and social care system, it is nonetheless only one facet of providing safe and effective home care. Therefore, there may be other second-order benefits (or harms) from the DCP rollout that we were not able to identify here. One example that has already been discussed in the section on implications above is that the data generated through the DCP may be useful for directing “predict and prevent” initiatives that allow targeted interventions for reducing hospitalization rates. 21 Alternatively, service user satisfaction with their care may have risen as a result of carers being free to spend more of the available appointment time with them. Furthermore, while our ascertainment of the outcome (hospitalization) attempted to use as many sources of truth as possible to verify data, it nonetheless falls short of the gold standard in verification which would be to use official records of hospitalization linked to NHS number (which we do not have currently access to).
Fourth, the limited granularity and current sample size of the data make performing subgroup analyses difficult. It could be that specific service users are more likely to benefit disproportionately from the DCP. This might include users who have underlying conditions that are more sensitive to picking up deteriorations when carers are able to spend more time with them. For example, new-onset confusion can be a symptom of infection. 22 However, this is harder to detect in service users with some element of pre-existing mild cognitive impairment/dementia. 23 However, such subtle differences might be easier to detect if the carer can maximize direct contact time with the service user and minimize the burden of administrative activities. On a similar note, there could also be subgroups of carers that are less comfortable with using the DCP. Targeting training and resources to these carers might therefore amplify any beneficial effect of the DCP on a potential reduction in hospitalization rates.
Conclusions
The implementation of a digital care plan in newly acquired branches was associated with an approximately 45% reduction in the 30-day hospitalization rate for new service users as compared to service users enrolled pre-DCP. Notwithstanding the limitations of an observational analysis, these findings suggest that the DCP in and of itself may help reduce hospitalizations. This effect could be compounded if combined with interventions to predict hospitalizations in advance and use targeted interventions to prevent them where possible.
Footnotes
Acknowledgements
We thank Myura Nagendran for his advice on the project.
Declaration of Conflicting Interests
NW, AA, HP are employees at Cera Care Ltd, in receipt of company shares. MM is the founder and CEO of Cera Care Ltd. JS, ML, TF are employees at Faculty Science Ltd, receiving consulting fees as external consultants for Cera Care Ltd.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors. This work falls under the remit of service improvement efforts at Cera.