
Abstract
We aimed to determine the hospitalization rate and average days spent at home in a population of assisted living (AL) residents served by a home-based primary care (HBPC) practice during the COVID-19 pandemic. We provided on-site HBPC to 1,699 AL residents and calculated hospitalization rate and days spent at home. The AL population had a mean age of 84 ± 10 years and 73% were female. The mean hospitalization rate was 449 admissions per 1,000 per year, and there was wide variation among AL communities. AL residents spent a mean of 358 days at home per year, and the average days spent at home varied during the COVID-19 pandemic. Use of these measures may help AL articulate its value proposition by enabling seniors with complex health needs to live in community settings for as many days as possible.
Keywords
Introduction
There are over 800,000 assisted living (AL) community residents in the U.S. 1 AL residents typically have multiple chronic conditions and dependencies on assistance with activities of daily living, and approximately three-fourths have dementia. 2 These individuals have difficulty accessing a physician’s office for care and experience high rates of emergency room and hospital utilization.1,3 Home-based primary care (HBPC) has been shown to reduce hospitalizations, rehospitalizations, and skilled nursing facility placements and improve patient and caregiver satisfaction.4-7 AL residents can benefit from on-site care provided by physicians and non-physician practitioners who are familiar with the assisted living setting.8,9
There is little research about which outcome measures are most meaningful for AL residents. Hospitalization rate is an outcome measure that is being used as an indicator of population-based acute care utilization in value-based payment models. Days spent at home is a person-centered outcome measure that can describe the time people with chronic and serious conditions spend in the community, outside of inpatient settings.10,11 Although the days spent at home measure was initially developed for use near the end of life, new models for population management, including the Centers for Medicare and Medicaid Innovation’s (CMMI) Primary Care First and Seriously Ill Population Models, have included it as outcome measures to align patient, provider and payer goals of producing quality, community-centered care at a lower cost. 12 Residents of AL communities typically have multiple chronic conditions, often need assistance with 1 or more activities of daily living, and experience falls at high rates, which together is associated with a higher risk of hospitalization. 1
In this study, we aimed to determine the hospitalization rate and average days spent at home in a population of AL residents served by HBPC, to evaluate for variability in these metrics between senior living communities, and to assess for change in these measures during the COVID-19 pandemic.
Methods
As recently described, our practice provides on-site HBPC to residents in 101 ALs in Ohio. 13 In the current study period of June 1, 2019 to May 31, 2020, we included 75 of these ALs where we had reliable, daily health information exchange (HIE) data coverage including hospitalization data, that was subsequently verified by AL staff. These ALs are owned by a variety of entities, including sole or family owners of a single home, local chains, regional operators and national AL organizations. HBPC visits were made to residents of Ohio AL communities by a team of physicians and advanced practice clinicians. Our practice’s model is to provide on-site access to care for AL residents by having a practitioner visit once or twice per week, depending on census. The practitioners are supported by nurse care managers who tracked census, the number of managed days (the number of days a patient was on our census), hospitalizations and inpatient skilled nursing admissions and lengths of stay using a HIE (CliniSync, Ohio Health Information Partnership). The inpatient list was distributed to medical practitioners on a daily basis, and the list was regularly reviewed to facilitate transitional care management.
Hospitalization rate per 1,000 was calculated as (admissions/managed months/1,000) × 12). 14 Inpatient days per 1,000 per patients served was calculated as (inpatient days /managed months) × 1000 patients × 12 months. Days spent at home was calculated as total managed days minus days spent in hospitals or nursing homes. For each of these 3 metrics, we performed standard descriptive statistics and box plots to assess for potential variation among AL communities. In addition, we evaluated trends in these metrics over the twelve month study period, including 4 months (January 20–May 31, 2020) during the COVID-19 pandemic.
Results
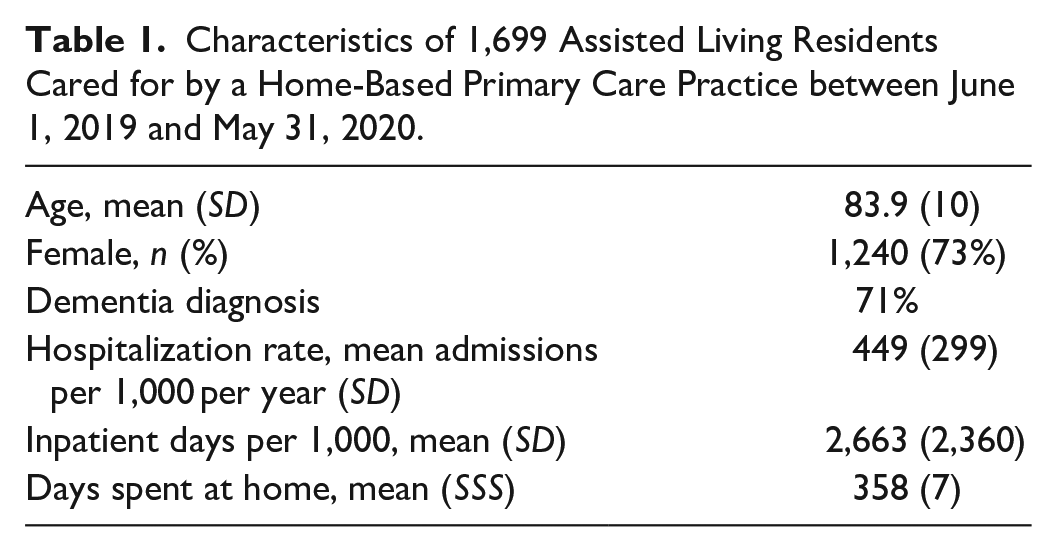
HBPC care was provided to 1,699 residents of 75 AL communities in the one year period between June 1, 2019 and May 31, 2020 (20,669 patient months). The patient panel had a mean age of 84 ± 10 years and 73% were female (Table 1). Our group’s average census in these communities was 23, and ranged from 2 to 94. 774 hospital admissions occurred, corresponding to a total length of stay of 4,586 inpatient hospital days. The mean practice hospitalization rate for senior living residents was 449 admissions per 1,000 managed months per year. There was wide variation in hospitalization rates among AL communities (Median 459, Range 0–1578, Interquartile Range 310–611, Figure 1). Patients experienced 2,663 inpatient hospital days per 1,000, and significant variation was observed among senior communities (Median 2,654, Range 0–13,220, Interquartile Range 1,716–3,804). This population also utilized 6,927 inpatient skilled nursing facility days in the 1 year study period. Overall, AL residents receiving HBPC from our group spent a total of 11,513 inpatient days in hospitals or nursing homes (1.9%) and a total of 608,560 days at home in the AL (98.1%) during the study period. On an annual basis, this cohort spent a mean of 358 days at home in the community, outside of hospitals and nursing homes. There was significant variation among AL communities in the number of days spent at home (Median 359, Range 325–365, Interquartile Range 356–361, Figure 2). In addition, we found that the percentage of days spent at home reached a nadir of 97.4% in February 2020, shortly after the onset of the COVID-19 pandemic in the U.S., and climbed to 98% in April and May, 2020 (Figure 3), generally correlating with Ohio’s Stay at Home order on issued on March 22 (expired on May 29, 2020).
Characteristics of 1,699 Assisted Living Residents Cared for by a Home-Based Primary Care Practice between June 1, 2019 and May 31, 2020.
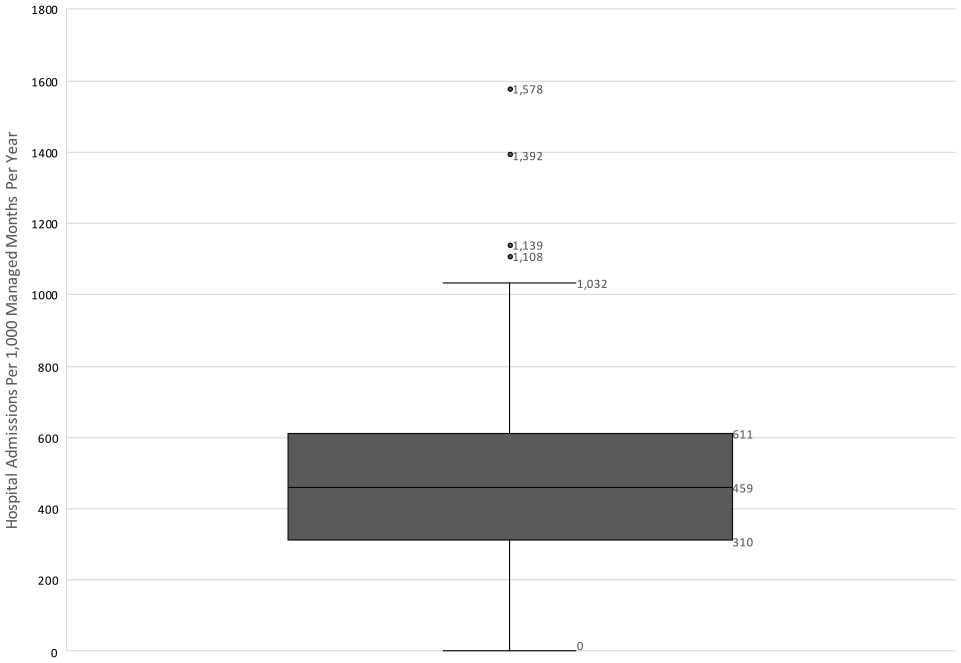
Distribution of hospitalization rates by senior living community.
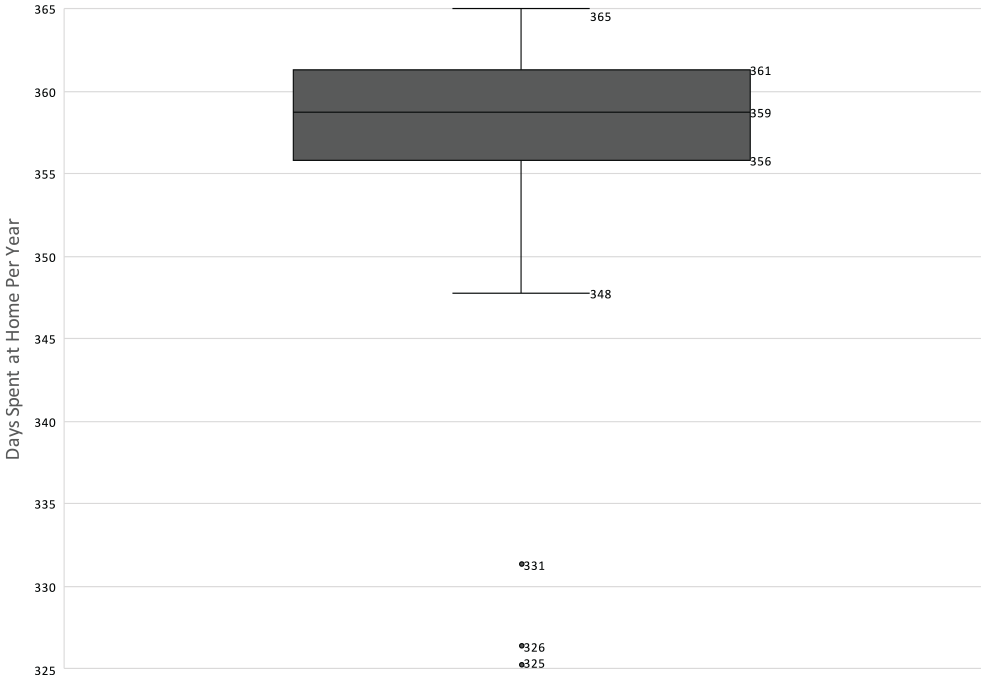
Distribution of days spent at home by senior living community.
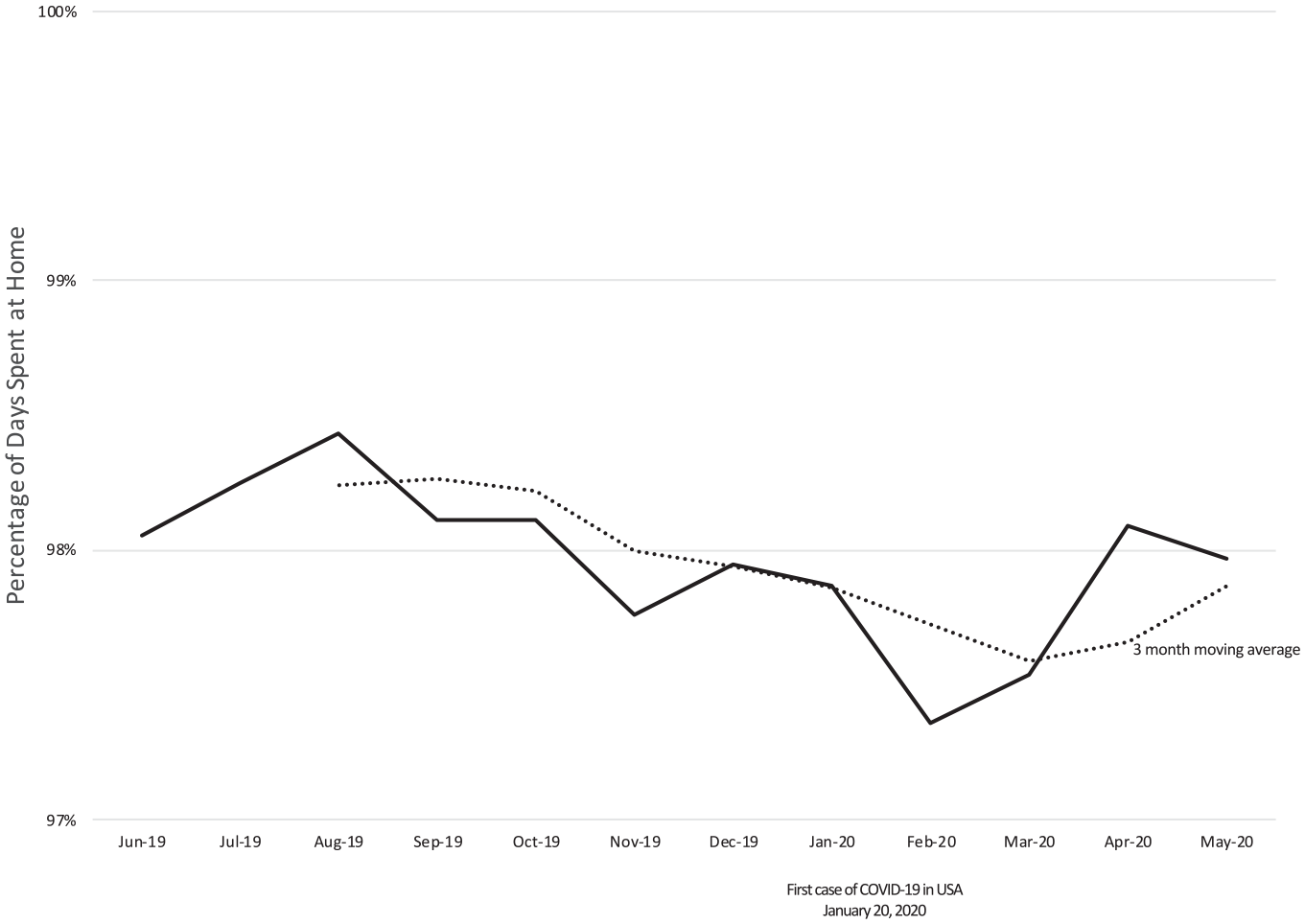
Percentage of days spent at home by month by senior living residents served by home-based primary care before and during COVID-19.
Discussion
Establishing quality and utilization metrics for AL residents is essential. Use of a HIE and daily patient tracking, as we performed in this study, can be enablers of gathering useful utilization data for this population. Hospitalization rate is increasingly being used as a means of measuring acute care utilization by value-based care initiatives. There is limited published hospitalization rate data currently available for AL residents in the U.S. In a population in Alberta, Canada, the cumulative annual incidence of hospitalization in AL residents with dementia was found to be 38.6%. 15 The authors reported a significantly increased risk for hospitalization in AL residents aged 90+ years, as well as those with poor social relationships, less severe cognitive impairment, greater health instability, fatigue, high medication use (11+ medications), and 2+ hospitalizations in the preceding year. Interestingly, the authors also reported that ALs with a smaller number of spaces, no chain affiliation, and those in specific health regions showed a higher risk of hospitalization. Whether similar tends exist in the U.S. is unclear. However, tracking hospitalizations and building programs to help reduce ambulatory-sensitive hospitalizations can be a worthy goal for senior living communities, provider organizations, and payers. In this study, AL residents were hospitalized at a rate of 449 hospitalizations per 1,000 per year. A subset of this population was risk stratified by way of the practice’s participation in CMMI’s Comprehensive Primary Care Plus program. The 702 attributed patients had a mean hierarchical condition category (HCC) score of 1.95, and 594 (85%) of these patients were in CMS’ complex risk tier, which included an HCC range between 2.2 and 15.0. Patients with a dementia diagnosis are also included in the complex risk category due to the fact that the HCC algorithm does not include dementia, despite the utilization risk it carries. This subset was representative of the full population described in this study. Compared to AL residents managed by our HBPC group, we found that a simultaneously-managed private home patient population had a higher hospitalization rate (660 admits per 1,000 per year), more hospital inpatient days per 1,000 (4,340) and spent fewer days at home per year (352). Factors that may have contributed to these differences include the availability of nursing and caregiver assistance in ALs, increased ability to coordinate urgent diagnostics such as x-ray and lab, and the ability to administer medications promptly. Days spent at home is a simple outcome measure that may help to align AL residents and other high risk primary care recipients around the goal of enabling spending more time in the community and less time in hospitals and nursing homes. We noted substantial variation in hospitalization rates and days spent at home among AL communities receiving HBPC. Whether differences in the way that AL communities are staffed or other factors led to this variation needs to be further studied. As a goal of senior living communities is to enable a higher number of meaningful days spent in the resident’s chosen community, days spent at home per year may be a simple metric for AL communities to follow as a gauge of operational success and resource provisioning, as well as a metric to follow for emerging AL value-based care models including special needs plans. Finally, we found mild monthly fluctuations in days spent at home among this population of AL residents, and we observed an increase in days spent at home during the first 4 months of the U.S. COVID-19 pandemic.
Footnotes
Authors’ Note
An abstract of this paper was accepted to the 2020 meeting of the American Geriatrics Society (cancelled).
Brief Summary
We determined the hospitalization rate and annual days spent at home in a population of assisted living residents served by a home-based primary care practice during the COVID-19 pandemic.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.