
Abstract
The current study examined the relationship between home visiting nurses’ job stress and error incidents to provide a better understanding of risk management for home visiting nursing services. Home visiting nurses often perform patient care alone, under great mental and physical stress, increasing the risk of human error when executing tasks. A mail survey was distributed to 437 home visiting nurses working at agencies in 71 locations in Japan. The questionnaires were anonymously completed and included items on career history, experiences of job stress, and experiences of incidents. Answers were collected from 230 participants. After eliminating incomplete responses, 146 questionnaires were included in the analyses. Participants’ average age was 48.5 ± 9.3 years, and they had an average of 7.2 ± 5.6 years of experience in home visiting nursing services. In total, 21 (14.4%) were administrators, and 125 (85.6%) were staff nurses. Administrators experienced more no-harm incidents in which an error occurred but did not result in client injury than did staff nurses (p < .05) and scored higher on three items of job stress (quantitative overload, fit to the job, and supervisor support) (p < .05). Harmful incidents were positively associated with quantitative overload (p < .05) and work environment (p < .01). These results suggest that there is a limit to the extent to which an administrator can offer safe care. A less stressful working environment and active information exchange rooted in a culture of medical safety should reduce the number of incidents.
Introduction
Japan is an aging nation, more so than in the rest of the world, with an average life expectancy of 80.75 years for men and 86.98 years for women as of 2015. 1 Enhanced home-based health care will allow older adults to continue living in their homes, even when medical issues begin to arise. Home-based care can also reduce the length of hospital stays and associated costs by enabling earlier discharge. A national policy to promote home-based care would enable progress in establishing a sustainable social security system to improve the quality of medical care in Japan. 2 In short, the country’s demand for home visiting nursing is on the rise.
Home visiting nursing was implemented in Japan in 1983 as an insurance-based system in which hospital nurses visited patients’ homes. Home visiting nursing agencies could be run by nurses and were not affiliated with hospitals, and became possible through a change in regulations in 1992. 3 As of 2017, there were 8,613 home visiting nursing agencies in Japan, 4 averaging 4.8 nurses per facility with about 60% of all facilities employing fewer than five people. Around 70% of home visiting nurses (HVNs) are above the age of 40; 73.8% are employed full-time and 23.5% part-time. 5 Nurses have been at the forefront of promoting home care, taking leadership roles in this process. 6
As the current emphasis on early discharge from hospitals shifts the locus of care to homes, the need for HVNs is increasing among patients with severe conditions. Risk management is necessary to reduce the legal risks involved with home visiting nursing. 7
Nursing is a stressful occupation, and stress negatively affects workers’ health and safety, as well as the health and effectiveness of the organizations for which they work. 8 HVNs are often isolated and are required to provide care without the resources that would be available in a hospital environment. 9 We argue that being an HVN likely increases job-related stress because the mental and physical loads are higher when compared with those of hospital nurses. This is because HVNs provide care, alone, in complex environments. Higher stress levels increase the risk of human error, which highlights the importance of a risk management strategy. This is in line with previous research demonstrating high levels of job stress in home visiting nursing environments. 10 To the best of our knowledge, no research to date has explored the relationship between job stress and risk management. The following issues are central to the discussion of risk management in home visiting nursing practices: the close relationships and communication between the client/family and nurse/provider; the management of unregulated or uncontrolled situations; autonomy and isolation; multidimensionality of safety (physical, emotional, social, and functional); harm prevention; promotion of health and care for chronic conditions; issues with human resources; and maintaining competence. 11 We hypothesized that HVNs’ stressful work conditions would be related to error incidents. Our objective of this study was to clarify the relationship between HVN job stress and incidents experienced by HVNs to consider appropriate risk management for home visiting nursing.
Research Method
Terminological Definitions
Heinrich’s law, widely used in the industrial world, holds that for every major injury, there are 29 minor injuries and 300 noninjuries/near misses. 12 Near misses present strong warnings about dangers in the system, and they can serve as reminders to be prudent. 13 For this reason, it is important for HVNs to obtain as much information as possible, not only on cases resulting in actual injuries but also on those resulting in no injuries—in other words, near misses. For the purposes of the current study, incidents were divided into “harmful” and “no-harm” categories.
Runciman et al 14 specified important concepts regarding the International Classification for Patient Safety and defined them as follows:
Near miss: an incident that did not reach the patient;
No-harm incident: an incident that reached the patient but did not result in any discernible harm;
Harmful incident: an incident that harmed the patient.
Some studies on home visiting nursing limit the definition of the subject of incidents to the clients, whereas others include incidents befalling the nurses themselves. Thus, the term “incident” is not clearly defined across studies. For this reason, the current study defined the terminology as follows, based on prior work:12,14-16
Risk management: Individuals’ or organizations’ engagement in preventing medical incidents;
No-harm incident: An incident in which an error occurred but did not result in client injury;
Harmful incident: An incident in which an error resulted in client injury;
Incident: An event that caused or could have potentially caused unnecessary harm to a client. This includes both no-harm incidents and harmful incidents.
Participants and Data Collection
Data were collected from HVNs in one prefecture in the western part of Japan. The prefecture contains coastal areas, mountain areas, and remote islands. This diversity of regional features made it an appropriate site for the current study. A questionnaire was mailed to 437 HVNs who worked at agencies in 71 locations in the prefecture. The questionnaires were anonymously completed and returned by participants. The instrument assessed job experience, employment position, employment pattern, job stress, and experiences of no-harm and harmful incidents. Job stress was evaluated with the Brief Job Stress Questionnaire, used in industrial health research in Japan.17-20 The scale comprises 57 items related to job stressors, psychosomatic complaints, and support for workers. Based on prior research,21,22 we also investigated the types of incidents involving clients or clients’ families that tend to occur when receiving home visiting nursing. This section of the measure comprised 16 items: nine were nursing-care-related and seven were medical-care-related. The development of the questionnaire involved a pretest with 10 nurses who had more than 5 years of home visiting nursing experience and resulted in appropriate revisions.
Analyses
The relationships between job stress, nurses’ basic attributes, and experiences of no-harm/harmful incidents were examined using Mann–Whitney U-tests. The relationship between experiences of no-harm/harmful incidents and basic attributes was further examined using chi-square tests (Fisher’s exact test). Statistical analyses were performed using a significance level of p < .05, and all values are expressed as mean ± SD throughout our article. All analyses were performed using IBM® SPSS® Statistics for Windows™ version 23 (IBM, New York, USA).
Ethical Considerations
We obtained ethical clearance from the Independent Ethics Committee of the University of Shimane, Japan (Authorization Number 137). Before participants received the questionnaires, they were informed that the study followed all ethical guidelines, and that handing in a completed questionnaire would be equivalent to providing informed consent to participate.
Results
With 230 participants submitting their responses, the response rate was 52.6%. After excluding questionnaires with missing items on basic attributes or the job stress measure as well as those with more than half of the answers regarding incidents missing, 146 questionnaires were included in the analyses (valid response rate: 73.5%).
Nurses’ Characteristics
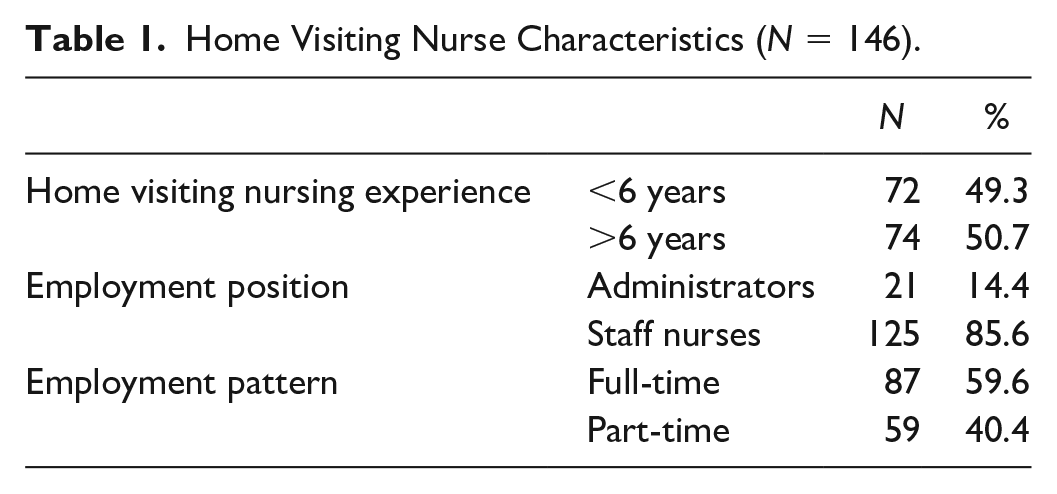
Participants’ average age was 48.5 ± 9.3 years, and they had an average of 7.2 ± 5.6 years of experience in home visiting nursing services, which ranged from 2 months to 21.5 years. A total of 72 participants (49.3%) had less than 6 years of experience, and 74 (50.7%) had 6 years or more of experience. As for employment positions, 21 participants (14.4%) were administrators, and 125 (85.6%) were staff nurses. A total of 87 (59.6%) were employed full-time, and 59 (40.4%) were employed part-time (Table 1).
Home Visiting Nurse Characteristics (N = 146).
Job Stress
Table 2 presents an overview of results related to job stress. Among job stressors, quantitative overload had a mean score of 8.7 ± 2.3 points, mental demand 9.7 ± 1.6 points, and physical workload 3.0 ± 0.8 points. There was no significant difference between years of experience in home visiting nursing and job stress. However, there was a significant difference between quantitative overload, fit to the job, and supervisor support and employment position. Administrators exhibited higher levels of job stress than did staff nurses. Quantitative overload was 10.0 ± 1.6 for administrators and 8.4 ± 2.3 for staff nurses (U = 804, p < .01), fit to the job was 2.2 ± 0.8 for administrators and 1.8 ± 0.6 for staff nurses (U = 955, p < .05), and supervisor support was 7.6 ± 2.2 for administrators and 6.3 ± 2.0 for staff nurses (U = 830, p < .01). There were significant differences between quantitative overload, interpersonal relations, fit to the job, irritability, fatigue, anxiety, depressed mood, and supervisor support and employment pattern. In terms of job stressors, quantitative overload averaged 9.4 ± 2.0 for full-timers and 7.6 ± 2.2 for part-timers (U = 1,384, p < .0001) and interpersonal relations averaged 5.7 ± 1.7 for full-timers and 4.9 ± 1.7 for part-timers (U = 1,829, p < .01). In terms of psychosomatic complaints: irritability was 5.8 ± 2.0 for full-timers and 4.9 ± 2.0 for part-timers (U = 1,868, p < .01), fatigue was 6.9 ± 2.3 for full-timers and 5.8 ± 2.2 for part-timers (U = 1,885, p < .01), and anxiety was 6.4 ± 2.0 for full-timers and 5.3 ± 1.7 for part-timers (U = 1,788, p < .01). In terms of support for workers, supervisor support averaged 6.8 ± 2.1 for full-timers and 6.1 ± 2.0 for part-timers (U = 2,036, p < .05), and full-time employees exhibited higher levels of stress than did part-timers in all related items.
Job Stress (N = 146).
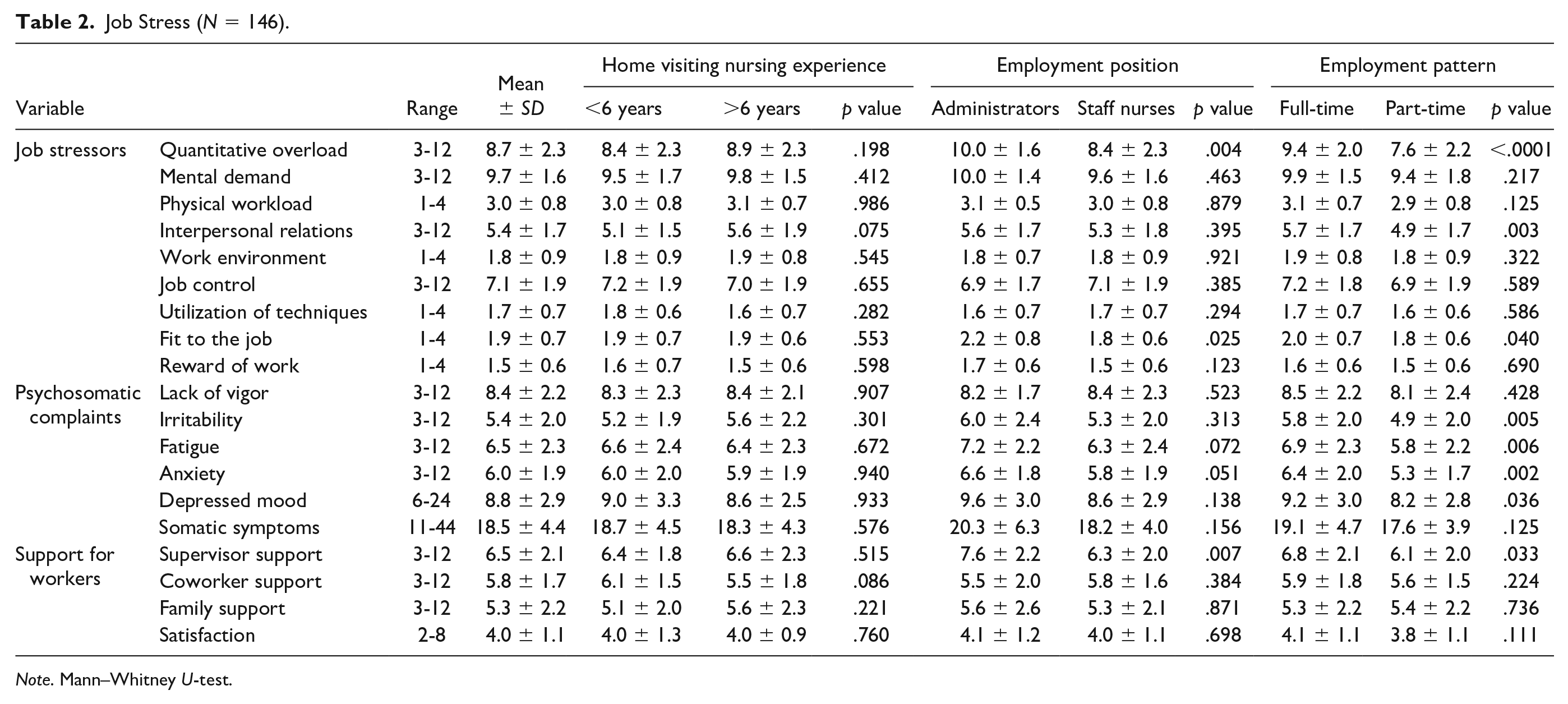
Note. Mann–Whitney U-test.
Figure 1 shows experiences of no-harm/harmful incidents. Experiences of no-harm incidents averaged 2.1 ± 2.3 across selected items (0-11 items); 102 participants (69.9%) had experienced no-harm incidents, whereas 44 (30.1%) had not. Among these, incidents related to scheduling daily life support ranked the highest, with 44 respondents (31.0%) indicating that they had experienced this. Other no-harm incidents were related to goods breaking (34, 23.3%), types of medication (27, 18.8%), treatment procedures (25, 17.5%), and support for client transfers (23, 15.9%). Experiences of harmful incidents averaged 0.7 ± 1.2 across selected items (0-5 items); 48 participants (32.9%) answered that they had experienced harmful incidents, whereas 98 (67.1%) answered that they had not. Goods breaking was most common (16 participants, 11.3%), followed by falling (10, 6.8%) and treatment procedures (9, 6.3%).
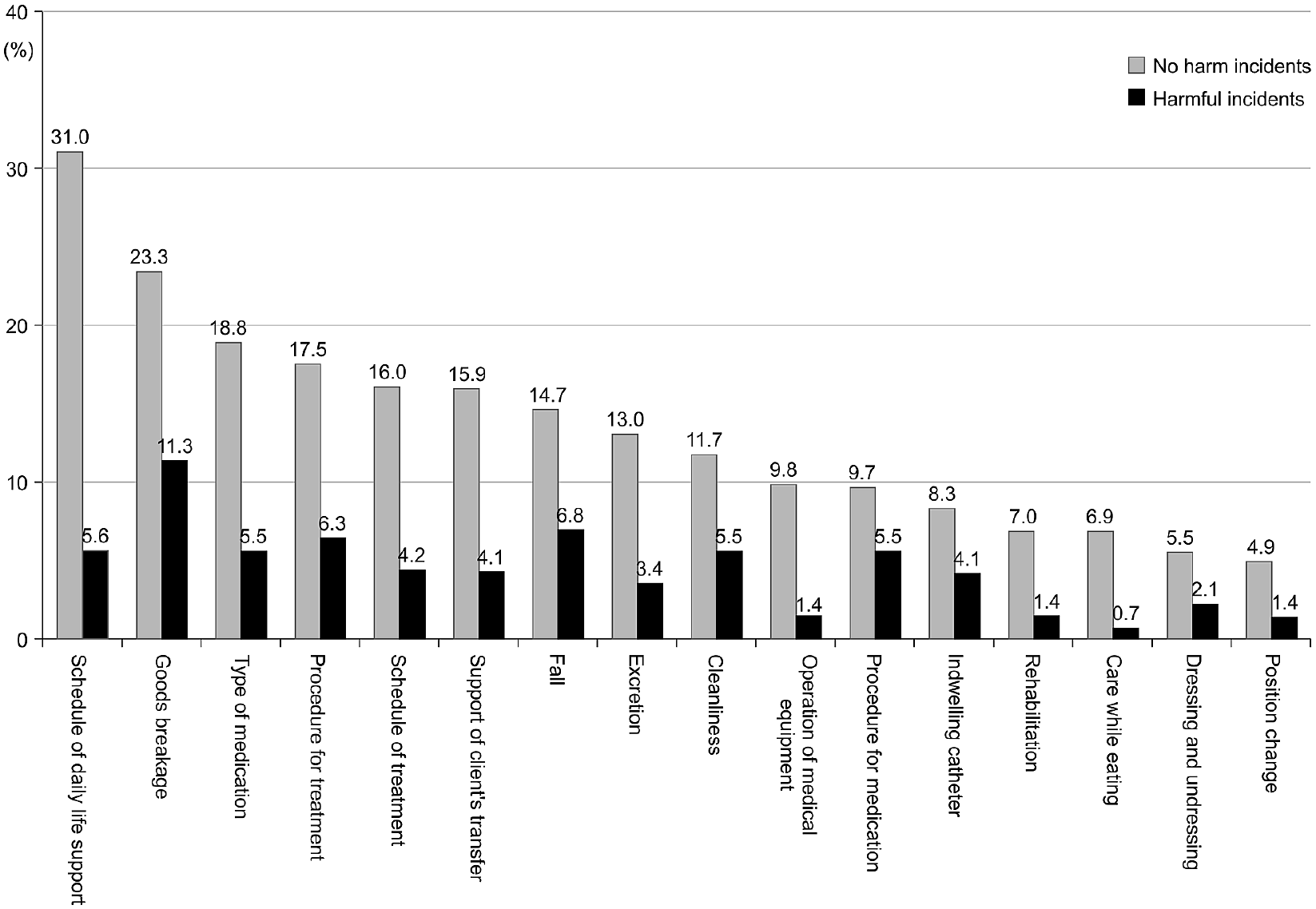
“No-harm incidents” and “harmful incidents” (N = 146).
Table 3 shows the relationship between experiences of no-harm incidents/harmful incidents and basic attributes. No significant differences were found regarding relationships between years of experience, χ2(1) = 1.768, p = .209, and employment pattern, χ2(1) = 1.390, p = .272, on the experience of no-harm incidents. Moreover, no significant differences were found regarding relationships between years of experience, χ2(1) = 1.662, p = .220, employment position, χ2(1) = 0.301, p = .620, and employment pattern, χ2(1) = 2.475, p = .151, on the experience of harmful incidents. Administrators had more experiences with no-harm incidents than did staff nurses, χ2(1) = 4.916, p = .037.
Relationships Between “No-Harm Incidents” and “Harmful Incidents” With HVN Experience and Characteristics (N = 146).
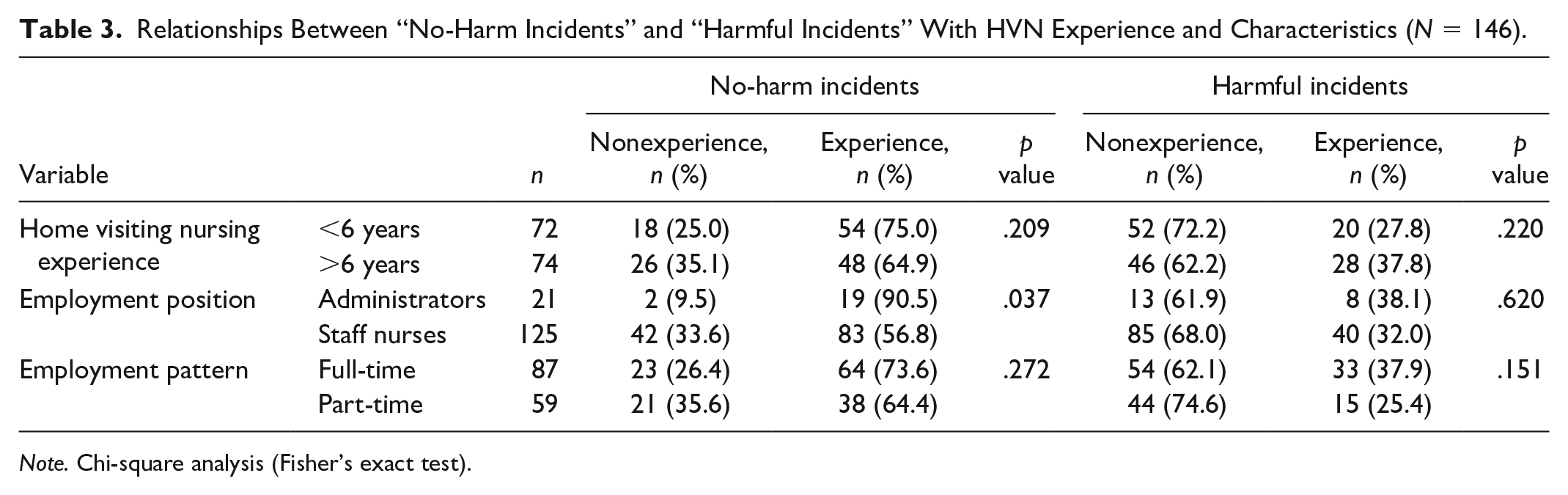
Note. Chi-square analysis (Fisher’s exact test).
Relationship Between Job Stress and No-Harm Incidents/Harmful Incidents
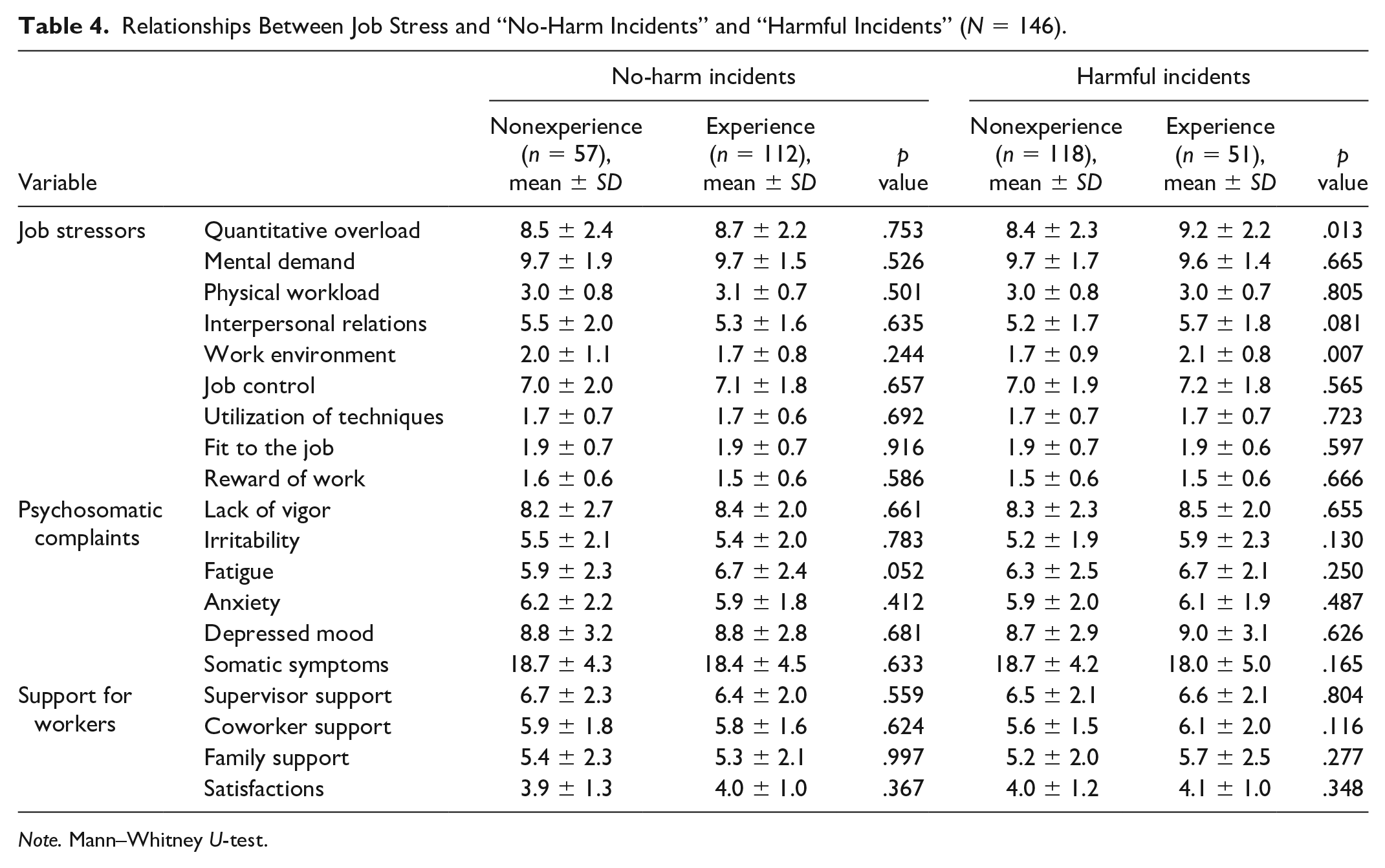
Table 4 shows the relationship between job stress and no-harm incidents/harmful incidents. No significant difference was found regarding job stress in relation to experience of no-harm incidents. Participants who reported high levels of stress on the quantitative overload and work environment items had more experiences of harmful incidents. Scores for quantitative overload averaged 8.4 ± 2.3 for those who had no experience of harmful incidents and 9.2 ± 2.2 for those who had such experience (U = 2,941, p < .05). Work environment scores averaged 1.7 ± 0.9 for those with no experience of harmful incidents and 2.1 ± 0.8 for those who had such experience (U = 2,954, p < .01).
Relationships Between Job Stress and “No-Harm Incidents” and “Harmful Incidents” (N = 146).
Note. Mann–Whitney U-test.
Discussion
This study investigated the relationship between HVNs’ job stress and experience of no-harm/harmful incidents. It is interesting to note that there were differences in incident experiences and job stress depending on employment position and employment pattern. Moreover, the incidents were unique to home visiting nursing. The inability to perform care on the scheduled visit date and time, and possible damage to goods at clients’ homes are examples of incidents that are unique to home visiting nursing practices and would not occur in hospitals. This indicates the importance of understanding home visiting nursing job stress features and typical incidents when developing risk management strategies.
Seventy percent of the respondents had experienced no-harm incidents, with scheduling daily life care and goods breakage being the most common. Thirty percent had experienced harmful incidents, with goods breakage being the most common category. HVNs follow nursing plans during their visits and often perform care using goods that belong to the clients.
When care takes longer than expected, HVNs are under pressure to complete a job within an allotted time frame, as determined by the contract. Time pressure significantly contributes to fatigue and depersonalization, and adjustments to interpersonal relationships with nurse administrators can have notable alleviating effects in relation to burnout caused by time pressure. 23 Harmful incidents and quantitative burdens were also related. Thus, in addition to general nursing skills, HVNs are required to be mindful of the time and environment where they are performing care. There is a possibility that HVNs experience incidents as stressful and, therefore, hesitate to share those experiences with colleagues. For many staff nurses, it is difficult to report suspicion of wrongdoing within specialized contexts, but the promotion of discussions about incidents, and good communication among those who serve in the medical field, is an appropriate strategy for reducing such errors. 24 It is necessary for the entire sector, and not just individuals, to engage with improvement to convert HVNs’ incident experiences into preventive safety. Home visiting nursing agencies need to establish workplace systems rooted in a culture of safety, in which HVNs can share information and hold discussions.
Many agencies perform emergency care by telephone or visits 24 hours per day. Full-time nurses may experience more stress related to time management than part-time nurses, as they are required to be prepared for emergency care. Full-time nurses reported more psychosomatic complaints than part-time nurses in this study. It has been reported that full-time nurses suffer emotional fatigue and poor health, causing them to miss work. 25 Moreover, Harrad and Sulla reported that job stress is one of the factors leading to burnout among home care workers, which, in turn, influences the quality of patient care. 26 Thus, our results suggest that reducing HVNs’ job stress can have a positive impact on both clients and HVNs: through the promotion of quality care and prevention of error incidents in the former and by preventing burnout and absenteeism in the latter. The subsequent quality assurance and employment stability at home visiting nursing agencies can ultimately lead to an increase in business revenue.
Many home visiting nursing agencies operate on a small scale, and administrators may be taking charge of risk management work. Whether a nurse would recognize an error that did not result in an injury as a no-harm incident depends on the individual nurse’s point of view. Our inference is that administrators recognize more no-harm incidents because they are engaged in risk management on a daily basis. According to our findings, incident occurrence is related to job stress, implying that stress management is an important consideration when developing a risk management strategy. One study suggests that a culture of safety is impaired by a lack of leadership and accountability. 27 While administrators might be more aware of incident occurrences, their workload was found to be high and they lacked support. This suggests a limit to administrator-centered approaches in providing safe care. In this regard, we recommend that both administrators and staff need to reduce their levels of job stress and create workplace environments that can facilitate active information exchange rooted in a medical safety culture.
In home care, teamwork plays a big role in patient safety, and managers are required to build teams rooted in trust and cooperation. 28 Depending on the case, the home care team consists of various members such as visiting nurses, doctors, pharmacists, rehabilitation and day service staff, and volunteers, with client and family forming the core. Therefore, to ensure safety, it is important to cooperate with clients and their families. Although client participation is required to determine the scope of quality and safety improvement work, in reality, it is difficult for them to participate. 29 In home care, when a problem occurs, the clients engage in an initial response by themselves or with their families. Therefore, HVNs need to support clients and their families in participating in risk management activities. Thus, we suggest that collaboration between clients, families, and HVNs can lead to the establishment of home care teams rooted in safety culture.
The present findings need to be interpreted in the context of certain limitations to our study. First, data were collected from one prefecture in the western part of Japan, and locally specific factors may limit the possibility of generalization. In addition, self-administered questionnaires allow the possibility that only nurses with an interest in risk management responded, which would introduce a selection bias. Related to this limitation, we recommend an intervention that would improve consciousness regarding medical safety among all HVNs.
Footnotes
Acknowledgements
The authors thank the home visiting nurses for contributing to this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by an individual research allowance from the University of Shimane. The funding agency had no role in the study design, collection, analysis, or interpretation of data; the writing of the report; or the decision to submit the article for publication.