
Abstract

Modern probe microphone systems offer a wide range of measurement options including a multiplicity of test signals. The signal of choice for any particular measurement is largely determined by the purpose in performing the measurement. For example, while a pure tone sweep would be fine for measuring a real-ear-to-coupler difference, the patient's own vocalizations would probably serve better for troubleshooting occlusion-related complaints. In this commentary, it assumed that the goal of the probe microphone measurement is to ensure speech audibility in fitting one of the current digital hearing aids, and the influence of advanced signal processing in choosing signal type for this purpose is discussed. Important considerations include compression characteristics in the hearing aid, the fitting rationale employed, and any special signal processing in the hearing aid (e.g. noise reduction).
Modern hearing aids, and digital hearing aids in particular, can provide input-level dependent amplification over a wide range of input levels. This implies that in verifying a fitting, it is important to choose a prescriptive method intended for fitting nonlinear amplification as well as to test the response of the hearing aid at different input levels. Concerning signal type, it should be borne in mind that non-speech signals will tend to underestimate gain for real speech when hearing aids are operating in a nonlinear fashion, with the greatest discrepancies occurring for swept pure tones. In a study comparing input signal types for obtaining frequency responses of hearing aids with AGC circuitry, Preves et al (1989) found lower output levels with swept pure tones than with broadband noise. They asserted that frequency response curves obtained using broadband noise inputs would be more representative of how “real world” sounds are processed by the hearing aid. Stelmachowicz et al (1996) used hearing aid gain for continuous discourse as the basis for comparison with different input signal types. Like Preves and his colleagues, they found lower hearing aid gain for swept pure tones than for broadband signals, particularly when the hearing aids were set to provide non-linear amplification. Compared to hearing aid gain for real speech, the gain observed for swept pure tones varied by up to 14 dB.
Another aspect of compression systems in modern hearing aids is that they often have two or more compression bands in which the compression characteristics can differ. Depending on the number of bands and degree of overlap between bands, dramatic differences can be observed in measurements performed with pure tone sweeps versus broadband test signals (Edwards et al, 1998).
Note that some prescriptive methods for nonlinear amplification define target gain values for a specified signal type. For example, the insertion gain targets generated by GN ReSound's proprietary rationale for its digital hearing aids are intended to be verified using swept pure tones. Target gain values have been adjusted to compensate for differences in the way this compression system amplifies sinusoidal signals relative to speech inputs. Conversely, the NAL-NL1 rationale assumes a broadband test signal with a speech-like spectrum for its default gain prescriptions (Byrne et al, 2001). The NAL-NL1 user must indicate in the software whether the intent is to verify the fitting with narrowband signals, in which case the prescriptions are altered to compensate for this (NAL-NL1 software, version 1.01, 1998). Generally speaking, broadband test signals will give the most accurate impression of gain for speech at various levels when fitting analog and digital multiband compression hearing aids, and should be preferred over narrowband signals unless otherwise specified by the fitting rationale employed.
Another aspect which should be considered when performing probe microphone measures on digital aids is how special sound processing schemes might interact with different types of test signals. In digital hearing aids currently on the market, special signal processing algorithms which can be expected to interfere with attempts to estimate gain for speech inputs via probe microphone measures are limited to noise reduction and feedback management.
Briefly, current noise reduction algorithms assume that large fluctuations in the levels of incoming sounds indicate that the sounds include speech. As the degree of level fluctuation in the input decreases, the incoming sound is assumed to include mostly noise, and gain is reduced. Because the type of broadband signals typically available in probe microphone equipment do not vary in level during the course of a measurement, noise reduction systems found in digital hearing aids will (correctly) identify them as noise. The noise reduction algorithm will reduce gain, and the results of the measurement will not be representative of how speech is amplified by the hearing aid. Fortunately, many digital hearing aids allow their noise reduction systems to be shut off for performing real ear and coupler measurements, permitting the audiologist to estimate the effects of the hearing aid's compression system on speech using random noise signals without interference by noise reduction.
An alternative way to obtain a reasonable estimate of hearing aid processing of speech without disabling noise reduction is to select a test signal which will “fool” the hearing aid into identifying and processing it as speech. Given that current noise reduction schemes discriminate between speech and noise on the basis of amplitude modulation, most digital hearing aids with noise reduction can also be tested utilizing a test signal which simply fluctuates in level, such as the modulated noise signals available in the Madsen Aurical (for a review of the Aurical, see Baer and Groth, 1998). These signals are created by essentially interrupting the white noise and speech-weighted random noise signals at random intervals. Stimulus equalization and measurement only take place during the random “on” time, which spans from 120 to 320 ms. The random “off” time for the signals ranges from 60 to 120 ms. In Figure 1, the coupler gain measured with the Aurical's speech-weighted noise and modulated speech-weighted noise signals are contrasted for a digital hearing aid with slow-acting noise reduction. As expected, the speech-weighted noise signal activates the noise reduction, causing the gain to be significantly reduced. As anticipated, the gain for the modulated speech-weighted noise signal is much greater. Note that for noise reduction systems with very fast time constants, an accurate impression of how the hearing aid processes speech inputs may not be obtained even with modulated test signals. This is a shortcoming of the method rather than the test signal, as information regarding gain variations over time are lost.
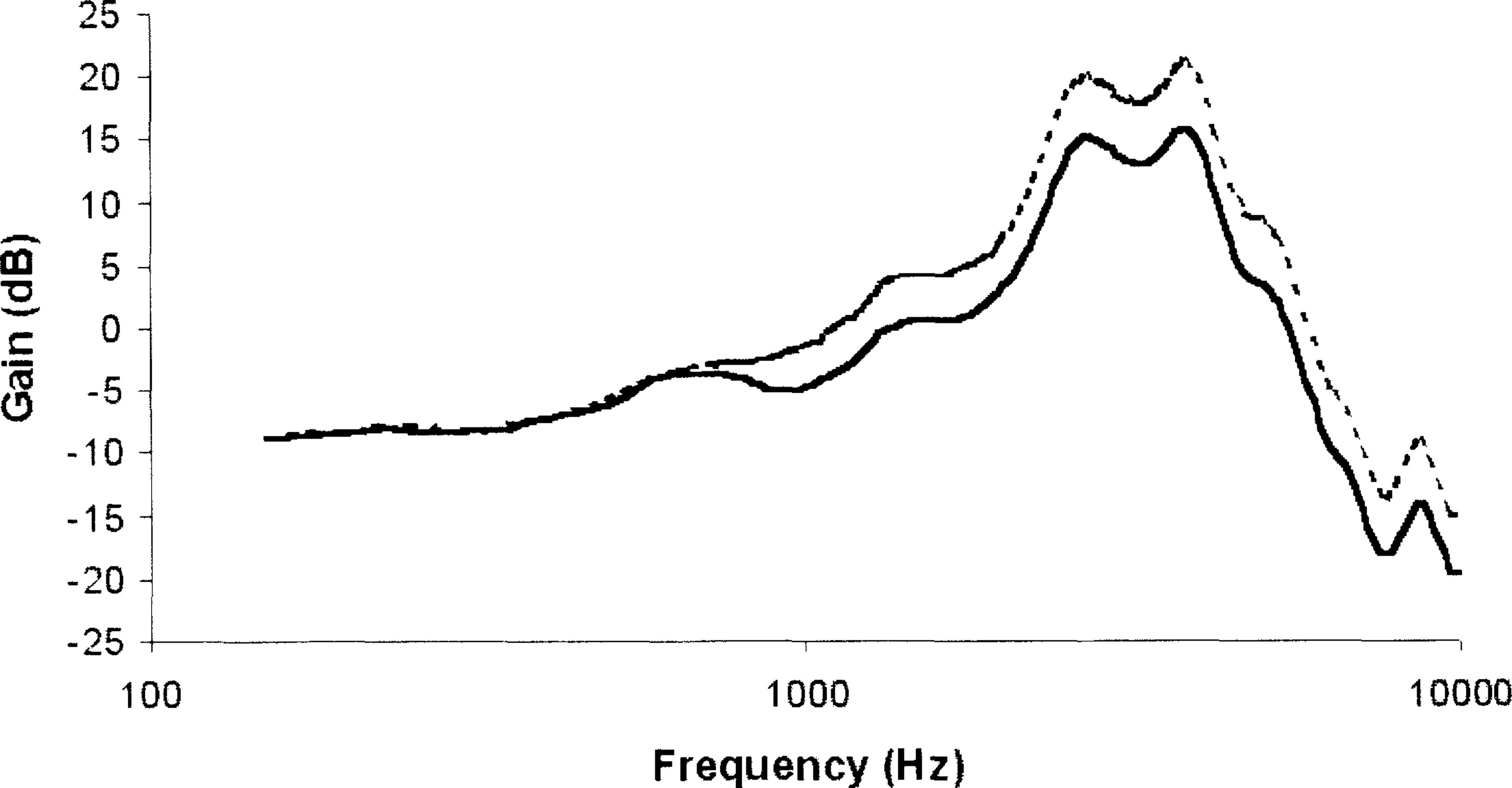
2cc coupler gain for a digital hearing aid with noise reduction activated. Both curves were obtained using test signals available in the Madsen Aurical. The upper dotted curve was measured with 70 dB SPL modulated speech-weighted noise and the lower solid curve with 70 dB SPL speech-weighted random noise. As expected, the random noise signal causes the hearing aid's noise reduction system to decrease gain.
Other useful test signals for estimation of amplification for speech in cases where digital noise reduction cannot be disabled are the artificial speech signals developed for the International Collegium of Rehabilitative Audiology (ICRA). These signals are produced by digitizing running speech, randomizing the polarity and filtering to match the long term average speech spectrum for normal vocal effort (Dreschler et al, in press). The resultant signal has the same modulation properties as the original speech sample, and is consequently more speech-like than the modulated speech-weighted noise previously described. ICRA artificial speech signals are presently available in some probe microphone systems, as well as on compact disc. 1
Feedback management schemes may also impact the selection of signal type. Most forms of feedback management in digital hearing aids involve gain reduction in the high frequencies, gain limiting for low input levels, or notch filtering. All of these affect the frequency response of the hearing aid in use in ways which are important for the audiologist to be aware of. Thus it would be advantageous not to disable these functions during probe microphone measurements, and the test signal of choice would be determined by other hearing aid characteristics such as compression and noise reduction.
Some digital hearing aids, however, cancel feedback by adding a signal identical to, but opposite in phase from, the feedback signal. In order for such systems to function appropriately, a measurement of the feedback path is performed during the fitting. Performing probe microphone measurements with the feedback cancellation algorithm active is problematic in itself, as insertion of the probe tube changes the feedback path. This increases the likelihood of feedback occurring as well as the likelihood of measurement artifacts as the system works to cancel the feedback. The problem of measurement artifacts will be exacerbated if sinusoidal test signals are used. This type of signal may be identified by feedback cancellation systems as acoustic feedback, and the resultant attempt at cancellation of the signal can show up as spikes on a frequency response curve. This is illustrated in Figure 2. Since this situation is not representative of the way most real-life sounds, such as speech, are processed by the hearing aid, it is crucial either to disable the feedback cancellation algorithm, or to use a broadband signal for probe microphone measurements.

2cc coupler gain for a digital hearing aid with feedback cancellation. Both measurements were made with a pure tone sweep at 60 dB SPL. The solid curve was obtained with the feedback cancellation disabled, and the dotted curve with the feedback cancellation active. The feedback cancellation algorithm attempts to adapt to the tonal stimulus, resulting in measurement artifacts.
The need for more complex test signals for performing real ear measurements in the future hinges on at least three factors. One is that some feature or combination of features of speech apart from audibility may be identified as determining success with amplification. For example, Bentler and Dittberner (1998) speculated that a strategy involving acoustic analysis of easily confused phonemes might serve as a way of evaluating effects of signal processing on speech perception. Another emerging trend in hearing aid fitting which may lead to alternative signal types entails recording and analysis of sound in actual listening environments selected by the hearing aid user (Köbler and Leijon, 1999; Gatehouse et al, 2000). Test signals generated on the basis of recordings made by the hearing aid user in his customary listening environments might then be used as the basis for prescription and verification of hearing aid characteristics. A final factor which will certainly call for more advanced, speech-like test signals is related to the increasing sophistication of digital signal processing algorithms. In contrast to current noise reduction schemes, which basically shut down in the presence of running speech, future algorithms may work more in concert with the compression system to enhance certain speech characteristics either in the frequency or temporal domain, or both. More speech-like inputs will be required in order to capture the effects of such processing. Even with existing hearing instrument technology, currently available test signals and methods provide an inadequate means to objectively evaluate time-varying effects of nonlinear processing (Dyrlund et al, 1994; Stelmachowicz, 1995). Ultimately, real or synthesized speech samples combined with alternative methods of acoustic analysis involving temporal as well as frequency and amplitude characteristics will be necessary to observe the real ear effects of amplification. The challenge will be to refine them in such a way that real ear measurements remain clinically feasible and useful.
Footnotes
1
The International Collegium of Rehabilitative Audiology promotes the use of these signals by researchers, clinicians and manufacturers providing appropriate reference is given. Contact Wouter Dreschler (email: