
Abstract
Although asthma and anxiety are clinically associated, the genetic basis of their co-occurrence has not been established. This study investigates whether the two conditions share underlying genetic risk factors, providing a foundation for understanding their biological interplay. Pediatric patients diagnosed with anxiety or asthma (n = 2168; 1085 females and 1083 males) were compared to controls without either condition (n = 1960; 926 females and 1034 males). To account for potential sex differences, polygenic risk scores (PRS) were analyzed separately for females and males. Cross-examination revealed that asthma patients do not have increased anxiety PRS, nor do anxiety patients have increased asthma PRS. No significant correlation was found between PRS in the control samples for either females (r = 0.008, p = 0.797) or males (r = −0.026, p = 0.396). This study demonstrates that asthma and anxiety do not share significant genetic risk factors, suggesting their clinical association may be driven by environmental factors, psychosomatic interactions, or gene-environment interactions. Sex-specific genetic differences indicate distinct factors influencing the co-occurrence of these conditions in males and females.
Introduction
In the United States, over 4.5 million children under the age of 18, or ~6.5%, are diagnosed with asthma, 1 while 7.8% of children aged 3–17 are diagnosed with anxiety. 2 A bi-directional relationship between asthma and anxiety has been observed; that is, asthma, particularly in its severe and uncontrolled forms, increases the risk of lifetime anxiety disorders, while current anxiety increases the risk of developing asthma or asthma-like breathing conditions. 1 Supporting this, studies in school-aged children have demonstrated that the presence of anxiety and other mental health conditions can double the risk of contracting asthma compared to children without such conditions. 3
Neuroimaging studies of anxiety patients have shown heightened activity in brain regions such as the amygdala, dorsomedial prefrontal cortex, ventrolateral prefrontal cortex, and thalamus, along with reduced activity in the ventromedial prefrontal cortex and subgenual anterior cingulate cortex. 4 These findings suggest a complex interplay between psychological and physiological processes, while lung–brain crosstalk mechanisms have also been highlighted in asthma studies. 5 Genetic risk plays a significant role in the development of both asthma 6 and anxiety. 7 Genome-wide association studies (GWAS) have revealed asthma-related genetic variants linked to type-2 immune responses, inflammation, and cellular processes. 6 GWAS identified anxiety-associated genes involved in synaptic function (THBS2), RNA splicing and neural excitability (RBFOX1), and inhibitory neurotransmission (GLRB), 7 which could potentially relate to the lung–brain crosstalk in asthma.
Given the clinical association between asthma and anxiety, it is plausible that the two conditions may share underlying genetic risk factors. Identifying such shared risks could provide valuable insights into their co-occurrence and pave the way for personalized treatments targeting both conditions simultaneously. Polygenic risk scores (PRS), which aggregate the effects of multiple genetic variants associated with a given condition, offer a powerful tool to assess shared genetic susceptibility. 8 This study aims to investigate whether the clinical association between asthma and anxiety is underpinned by shared genetic risk. By leveraging the clinical and genetic resources at the Center for Applied Genomics (CAG) at Children’s Hospital of Philadelphia (CHOP), we analyze PRS for asthma and anxiety in pediatric populations.
Methods
Subjects
Pediatric patients (n = 2168, including 1085 females and 1083 males) with anxiety or asthma were compared to controls without anxiety or asthma (n = 1960, including 926 females and 1034 males). The age of the subjects ranged from 2582 to 8497 days, with a median age of 6271 days. Since the PRS models for anxiety and asthma were primarily developed based on European populations. Only samples with European ancestry were included in this study. Ancestries were confirmed using the Admixture 1.3 Software (UCLA, Los Angeles, CA) 9 based on genome-wide genotyping and imputation. Cases and controls were selected as unrelated based on identity-by-descent analysis (kinship coefficient <0.0442). All the patients were recruited by the CAG at the CHOP, which has established a large pediatric biobank coupled to a comprehensive electronic medical record.
Genotyping
The genotyping was done by the Illumina Genotyping BeadChips with at least 550,000 single-nucleotide polymorphisms (SNPs) genotyped. Genome-wide imputation was done with the TOPMed Imputation Server (https://imputation.biodatacatalyst.nhlbi.nih.gov/#!) using the TOPMed (Version R2 on GRC38) reference panel. Altogether, 44,673,317 autosomal SNPs with quality R 2 ≥ 0.3 and with <10% missing rate were imputed.
PRS scoring
The anxiety PRS score was based on PGS catalog ID: PGS004451, which includes 1,059,939 variants. 10 The asthma PRS score was based on PGS catalog ID: PGS002727, which includes 985,837 variants. 11 Considering the potential sex effects in anxiety 12 and asthma, 13 each sex was analyzed separately.
Results
Samples
Among the 1085 female patients, 628 have anxiety, and 576 have asthma. A total of 119 patients have both anxiety and asthma, accounting for 19% of those with anxiety and 21% of those with asthma. Among the 1083 male patients, 499 have anxiety and 696 have asthma. A total of 112 patients have both anxiety and asthma, accounting for 22% of those with anxiety and 16% of those with asthma. These comorbid rates are significantly higher than the rates expected by chance. According to the literature, the prevalence of anxiety is 4.7% in U.S. children, 14 and the prevalence of asthma is 9.3% in U.S. children. 15 Therefore, the clinical correlation between the two diseases is supported.
Genetic correlations of the two diseases
To test whether the two diseases share common genetic risk, we cross-examined the PRS scores of patients in each group (Table 1). As shown by our results, both females and males with anxiety have increased anxiety PRS, while those with asthma have increased asthma PRS. Among individuals with both anxiety and asthma, females have only increased asthma PRS, whereas males have only increased anxiety PRS. Cross-examination revealed that asthma patients do not have increased anxiety PRS, nor do anxiety patients have increased asthma PRS. Furthermore, in the control samples, we found no correlation in either females (r = 0.008, p = 0.797) or males (r = −0.026, p = 0.396).
Comparisons of anxiety PRS and asthma PRS with respective controls.
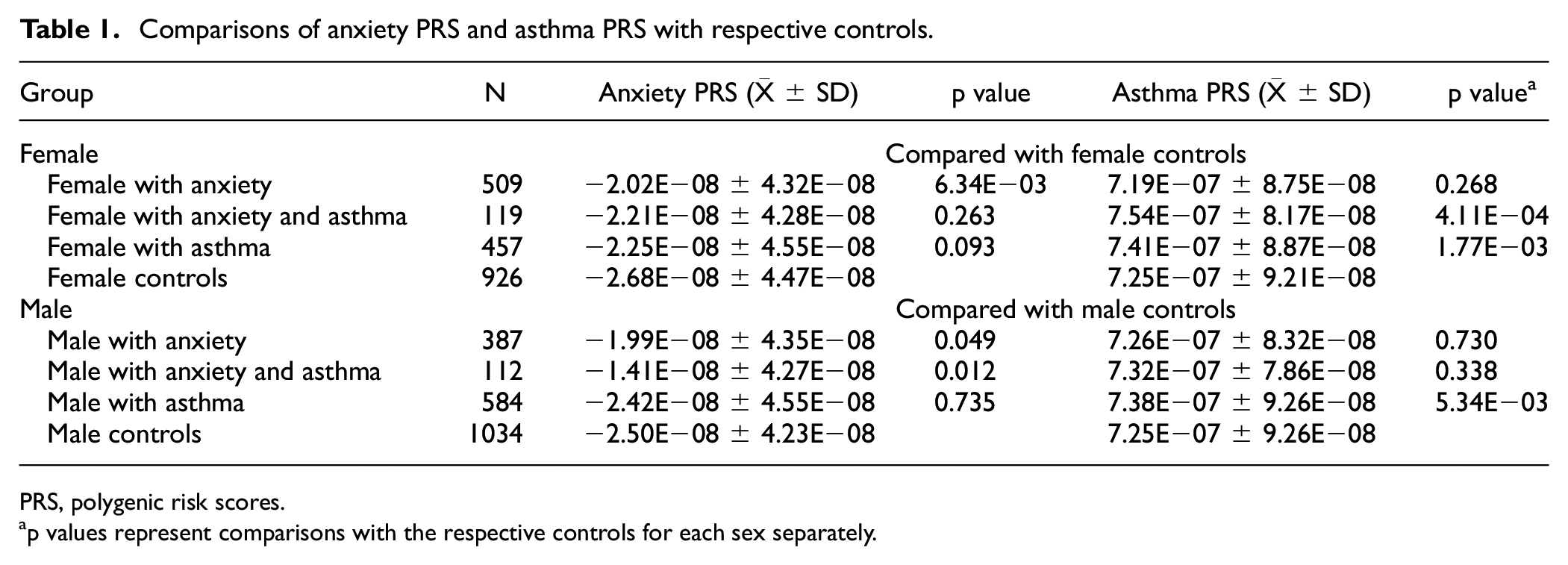
PRS, polygenic risk scores.
p values represent comparisons with the respective controls for each sex separately.
Discussion
In this study, we analyzed genetic risk scores from 2168 pediatric patients diagnosed with asthma, anxiety, or both at CHOP. Our findings revealed no significant genetic association between asthma and anxiety, as evidenced by the absence of increased anxiety PRS in asthma patients or increased asthma PRS in anxiety patients. This contrasts with the well-documented clinical association between both conditions, 1 challenging the assumption of a shared genetic basis for these conditions16,17 and highlighting the need to explore other biological or environmental mechanisms driving their clinical co-occurrence. Our findings provide important insights into the relationship between asthma and anxiety, specifically disputing the hypothesis that their clinical co-occurrence arises from shared genetic mechanisms.16,17 This hypothesis may oversimplify the relationship between these two conditions. While they often co-occur clinically, our results suggest that asthma and anxiety are likely to arise from distinct genetic pathways.
Several explanations may account for the lack of genetic correlation between asthma and anxiety. One possible explanation is that asthma is a chronic respiratory disease that can impose significant emotional stress, particularly in children and adolescents, as they may perceive the condition as a barrier to their development. 18 This emotional burden may lead to overthinking, hypervigilance, and anxiety. Furthermore, behavioral patterns, such as excessive preparation for asthma attacks, may create heightened worry, reinforcing anxiety. 19 This psychosomatic interaction may explain the observed clinical association between asthma and anxiety despite the absence of shared genetic risk.
In addition, the relationship between asthma and anxiety may be explained through gene-environment interactions. Children with asthma may encounter environmental stressors that trigger anxiety, creating a feedback loop that does not necessarily involve direct genetic overlap. 20 For example, children genetically predisposed to anxiety may be more sensitive to environmental stressors, such as allergens, pollution, or social challenges, which exacerbate asthma symptoms. These environmental factors may also contribute to the development of anxiety. For instance, exposure to air pollution has been associated with both asthma exacerbations and the development of anxiety. 21 Similarly, childhood adversities, such as stressful life events or chronic stress, may act as environmental stressors that complement genetic risks to increase the likelihood of developing both asthma and anxiety. 22 Altogether, these findings suggest that shared environmental triggers, rather than a shared genetic basis, may underlie the co-occurrence of these conditions.
While we found no significant genetic overlap from our analysis, another study involving a large-scale genome-wide cross-trait analysis identified one locus significantly associated with both asthma and anxiety, tagged by the SNP rs1709393. 17 This SNP is located in the long noncoding RNA known as RIG-I Dependent Antiviral Response Regulator RNA, which is implicated in the regulation of antiviral immune responses. 23 These findings, along with our results, suggest the possibility of a subtle genetic correlation between asthma and anxiety. However, the weak effect size associated with rs1709393 highlights that such overlap, if present, is likely minimal and insufficient to explain the clinical association between the two conditions. This reinforces the importance of environmental factors and gene-environment interactions in driving their co-occurrence.
The insignificant genetic overlap we observed aligns with some previous research, further indicating that while asthma and anxiety share clinical associations, the genetic predisposition leading to the development of both conditions is independent. 24 This is supported by studies examining the heritability of asthma and anxiety, which suggest that both conditions have complex polygenic structures with different genetic risk factors. 25 The absence of significant genetic overlap does not eliminate the possibility of small genetic influences but suggests that genetic predispositions alone are unlikely to explain the concurrence of the two conditions. Instead, environmental factors, psychological stressors, and gene-environment interactions may play a more substantial role in the co-occurrence of the two conditions.
Our findings revealed sex-specific differences in the genetic contributions to asthma and anxiety. Females with both conditions exhibited increased asthma PRS but not anxiety PRS, whereas males showed increased anxiety PRS but not asthma PRS. This suggests that the genetic predisposition to asthma may play a more prominent role in the co-occurrence of these conditions in females, while the genetic predisposition to anxiety may be more influential in males. These differences may reflect underlying biological or hormonal differences, such as the influence of estrogen on immune responses in females 26 and the role of stress-driven pathways in males. 27 These results emphasize the importance of considering sex-specific genetic pathways when investigating the mechanisms underlying the relationship between asthma and anxiety. 28
Our findings have important clinical implications given the lack of genetic association between asthma and anxiety. This emphasizes the importance of a comprehensive approach to treating patients suffering from both conditions. Moreover, environmental factors such as air quality or family stress should be emphasized more when treating pediatric patients with both or either condition. While our study provides new insights, there are limitations to consider. The study population was limited to pediatric patients, which may restrict the generalizability of our findings to other age groups. The sample size, while robust, may still lack the statistical power needed to detect subtle genetic effects, for example, in patients with comorbid asthma and anxiety. Future research should incorporate larger, more diverse populations and longitudinal designs to examine the dynamic relationship between these conditions.
In conclusion, although our study found no significant genetic overlap between asthma and anxiety, it is still necessary to understand the complexities of the relationship between the two conditions. The clinical association of the two conditions may arise because of psychosomatic interactions, gene-environment interactions, and shared environmental factors. By deepening our understanding of the relationship between the two conditions, we can develop more effective treatment plans that address both conditions altogether.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by the Institutional Development Funds from the Children’s Hospital of Philadelphia to the Center for Applied Genomics, and the Children’s Hospital of Philadelphia Endowed Chair in Genomic Research to HH.
Ethics approval and consent to participate
The study was approved by the Institutional Review Board (IRB) of the Children’s Hospital of Philadelphia (CHOP). Informed consent was obtained from all subjects. If subjects are under 18, consent was also obtained from a parent and/or legal guardian, with assent from the child if 7 years or older.