
Abstract
In many COVID-19 survivors, symptoms continue for a long time. This study aims to examine the relationship between the long-term effects of COVID-19, levels of anxiety and depression, and suicidal ideation with sociodemographic factors and symptoms. A cross-sectional study was conducted on patients who came for control at least 3 months after having COVID-19 disease, in the stable period, and still have symptoms after COVID-19. Demographic characteristics, symptoms, The Beck Depression Scale (BDS), The Beck Anxiety Scale (BAS), and suicidal ideation were assessed with face-to-face questionnaires. A total of 490 patients participated in the study. Thirty percent of patients scored positive on the BDS and 46% scored high on the BAS. Female sex was found to be a risk factor. Anxiety and depression were found to be significantly associated with long COVID symptoms. Both BAS and BDS scores were significantly higher in people with suicidality compared to others, and long-term symptoms were found to be statistically associated with this situation. Depression and anxiety are common in cases of long COVID. It is important for healthcare professionals to be aware of these potential mental health consequences, especially suicidality, and to provide appropriate support and interventions for individuals with long COVID.
Keywords
Introduction
It has been 3 years since severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2; COVID-19) infection was defined as a global epidemic. Although the disease has lost its impact, it continues to manifest itself from time to time with new mutations. 1 Approximately 80% of those affected individuals had mild to moderate disease, and 5% of those with severe disease developed critical illness. 2 Ongoing follow-up of patients who have recovered from COVID-19 has shown that in many cases one or more symptoms persist even weeks or months after the acute infection. 3
Post-acute sequelae of SARS-CoV-2, or long COVID, is a prevailing second pandemic with nearly 100 million affected individuals worldwide and growing.4,5 It has been reported to occur in at least 10% of SARS-CoV-2 infections. 5 The term “prolonged COVID” was first used on social media in Italy by Perego to describe the persistence of symptoms weeks or months after the initial SARS-CoV-2 infection. 6 It is also referred to as “post-COVID syndrome.” It is defined as the presence of symptoms 3 months after the onset of symptoms, lasting at least 2 months and unexplained by an alternative diagnosis, in people with a history of probable or confirmed SARS-CoV-2 infection. 7 Although prolonged COVID can occur in all age groups, it has been reported to be most common in the 35–50 age group 5 and associated with the severity of acute illness. 5
The literature demonstrates that long-term symptoms following COVID-19 and mental health issues are a serious concern and warrant further attention.
This study delves deeper into the relationship between long COVID-19 symptoms and anxiety, depression, and suicidal thoughts, presenting novel and significant findings.
Particularly noteworthy are the identified risk factors of the female gender and the strong associations found between anxiety, depression, and suicidal ideation.
In clinical practice, it can provide guidance on the evaluation of patients with long COVID-19 symptoms from a mental health perspective and on the provision of necessary support and interventions.
The clinical picture of this disease is independent of the viral status and it may present with the persistence of one or more symptoms of acute COVID-19 or the emergence of new symptoms. 8 More than 200 symptoms affecting multiple organ systems have been described. 7 According to a meta-analysis, a significant proportion of individuals experience persistent fatigue and/or cognitive impairment following recovery from acute COVID-19. 9 Fatigue and shortness of breath, which persist for months after acute COVID-19, are the most common symptoms. Other persistent symptoms include cognitive and mental impairment, chest and joint pain, heart palpitations, myalgia, dysesthesia, cough, headache, and gastrointestinal and cardiac problems.10,11
In particular, mental health problems have a significant impact on the quality of life. According to previous systematic reviews, depression and anxiety are the most reported psychiatric symptoms in the context of “long COVID-19.” 12 A prospective cohort study showed that anxiety level, which was reported in 29.6% of patients 1 month after the acute illness, persisted at 3 months (25.5%). 13 In another study of 478 patients, anxiety was found in 31.4% and depression in 20.6% of the patients. 14 A meta-analysis of studies of long COVID-19 found that 23% of people with long COVID-19 reported anxiety and 12% reported depression as symptoms. 15 In another study, the frequency of depressive symptoms +12 weeks following COVID-19 ranged from 11% to 28%. 16
These findings highlight the significant psychological distress experienced by individuals with long COVID-19. The first thing to be considered in a patient group that experiences such intense anxiety and depression is suicidality. The most important determinant of suicide is the presence of depression. It has been found that not only the effects of the disease but also social isolation, quarantine, and financial problems are risk factors for suicide and suicide attempts during the COVID-19 epidemic. 17 Due to both sociological factors and the psychological effects of the disease, survivors of COVID-19 survivors are considered to be at high risk of suicide.
Although the acute phase of the disease has been well characterized and is now known, the long-term consequences are not well defined. There are no clear data on what constitutes prolonged COVID-19, which patients will develop prolonged COVID-19, what the phenotypes are, and how this condition can be predicted. Amid this uncertainty, long COVID patients should be asked about symptoms of anxiety and depression, and suicidality should be attempted to be identified.
Our primary hypothesis is to show that the rates of depression, anxiety, and suicidality are high in the long COVID patients and secondarily, these psychiatric conditions are associated with long COVID symptoms. With these hypotheses, our study will contribute to the literature on what aspects should be considered in the follow-up of long COVID patients.
This study aims to examine the relationship between the long-term effects of COVID-19, levels of anxiety and depression, and suicidal ideation with sociodemographic factors and symptoms.
Materials and methods
Study design, setting, and population
This is a cross-sectional study conducted on patients who applied to our chest diseases clinic, who came for control at least 3 months after having COVID-19 disease, in the stable period, and still have symptoms after COVID-19. After obtaining informed consent from the patients, demographic characteristics, anxiety, and depression status scales were assessed with face-to-face questionnaires.
Study measurements
Patients were asked about their age, sex, smoking and alcohol use, marital status, number of children, chronic diseases, the type of treatment during the COVID period, symptoms in the post-COVID period, and whether they had a sleep disorder/psychiatric illness before the pandemic. The Beck Depression Scale (BDS) and the BAS were administered to the patients. Patients were asked about suicidal ideation in the Beck Depression Questionnaire.
Inclusion criteria: Male and female patients who had COVID-19 at least 3 months ago, >18 years of age, who came for follow-up in the stable post-treatment period, and who still have symptoms after COVID.
Exclusion criteria: Patients who did not agree to participate in the study, whose level of consciousness was not suitable for answering the survey questions, and those with a known history of psychiatric disorders prior to the pandemic were not included in the study.
The Beck Depression Scale (BDS): It was developed by Aaron Beck and colleagues.18,19 The original version consists of 21 questions about how the person has felt in the last 1 week. No special training is required for the use of the scale. The person to whom the scale is administered is asked to choose the sentence that best expresses how he/she has felt in the last week, including the day of administration. The scale contains a total of 21 self-assessment sentences that provide a four-point Likert-type measurement by numbering 0, 1, 2, and 3. The sentence numbered “0” indicates that the depressive feeling or state specified in that item is absent, and the higher the number, the more intensely it is experienced. The validity and reliability study of the Turkish form of the depression scale in Turkey was conducted by Hisli. 20 BDS internal consistency for the reliability of the study Cronbach’s alpha reliability coefficient was found as 0.921. A total Beck depression score of 0–16 is considered normal and 17–63 is considered pathological.
The suicide-related questions in the BDS were grouped as follows: “I have no thoughts of killing myself,”“I have no suicidal tendencies,”“I sometimes think about killing myself, but I do not do it,”“I would like to kill myself,”“I would kill myself if I had the opportunity,” and “I have suicidal tendencies.”
The Beck Anxiety Scale (BAS): It was developed by Beck et al. 21 Turkish validity and reliability study conducted by Ulusoy et al. 22 It evaluates the frequency of anxiety symptoms experienced by the individual. It is a self-assessment scale consisting of 21 items and scored between 0 and 3. The patient is asked how much the feeling of distress has bothered him/her in the last week. A high score indicates high levels of anxiety. BAS internal consistency for the reliability of the study Cronbach’s alpha reliability coefficient was found to be 0.942. A Beck Anxiety Score of 0–7 is considered normal and 8–63 is considered pathological.
Statistical analysis
Statistical analyses were performed using the IBM-SPSS program (SPSS version 21; SPSS Inc., Chicago, IL, USA). The compatibility of continuous variables with normal distribution was analyzed by Kolmogorov–Smirnov test. Continuous variables were expressed as mean ± standard deviation and categorical variables were expressed as percentages. Student’s t-test was used for continuous variables and the chi-squared test was used for categorical variables to compare two groups. Factors affecting depression were determined by univariate logistic regression analysis. The level of statistical significance was accepted as p < 0.05 in all analyses.
Informed consent
This study was conducted ethically in accordance with the World Medical Association Declaration of Helsinki as revised in 2000. Written informed consent was obtained from the patient or the next of kin for publication.
Study approval statement: The ethics committee approval of our study was obtained from Recep Tayyip Erdogan University Clinical Research Ethics Committee (Ethics Committee Approval No: 2021/165).
Data availability statement
The data of this study were obtained from the patient database of Recep Tayyip Erdogan University Training and Research Hospital. The data can be shared if the corresponding author is reached via e-mail.
Results
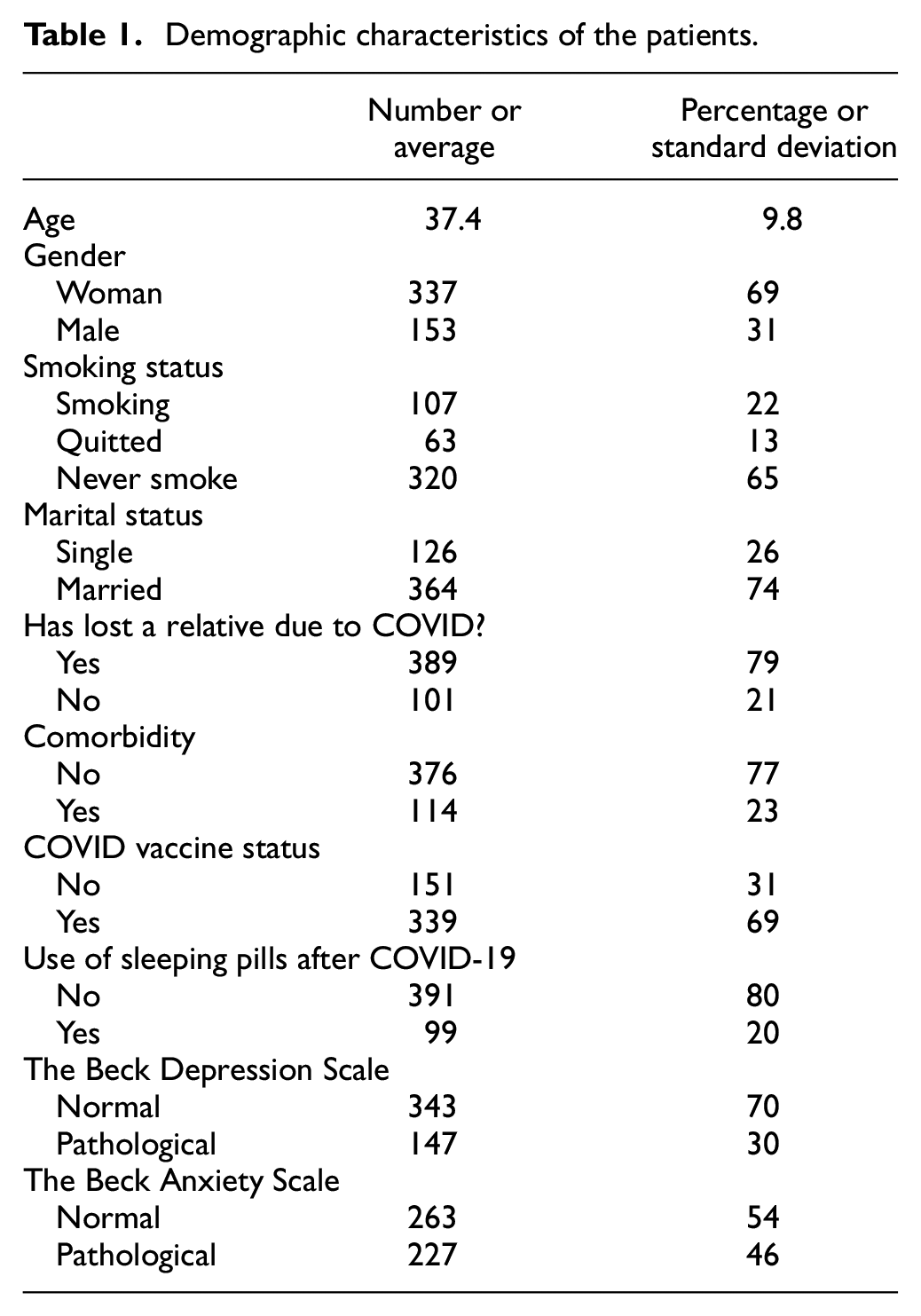
A total of 490 survivors of COVID-19 disease voluntarily participated in the study. The mean age of the participants was 37.4 ± 9.8 years, 31% (153) were males and 69% (337) were females. The sociodemographic characteristics of the participants are shown in Table 1.
Demographic characteristics of the patients.
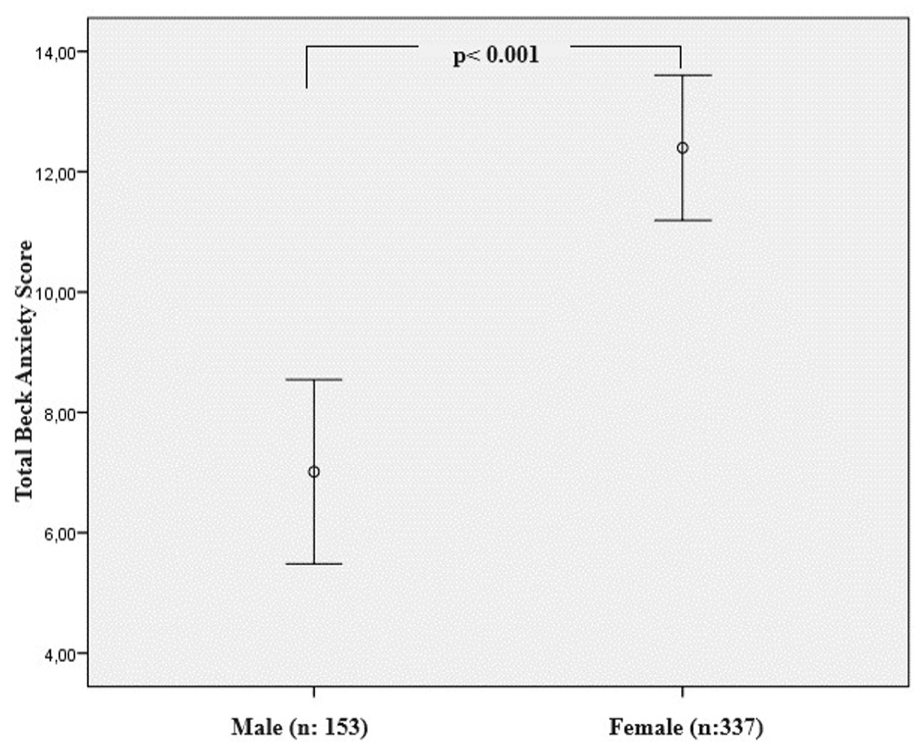
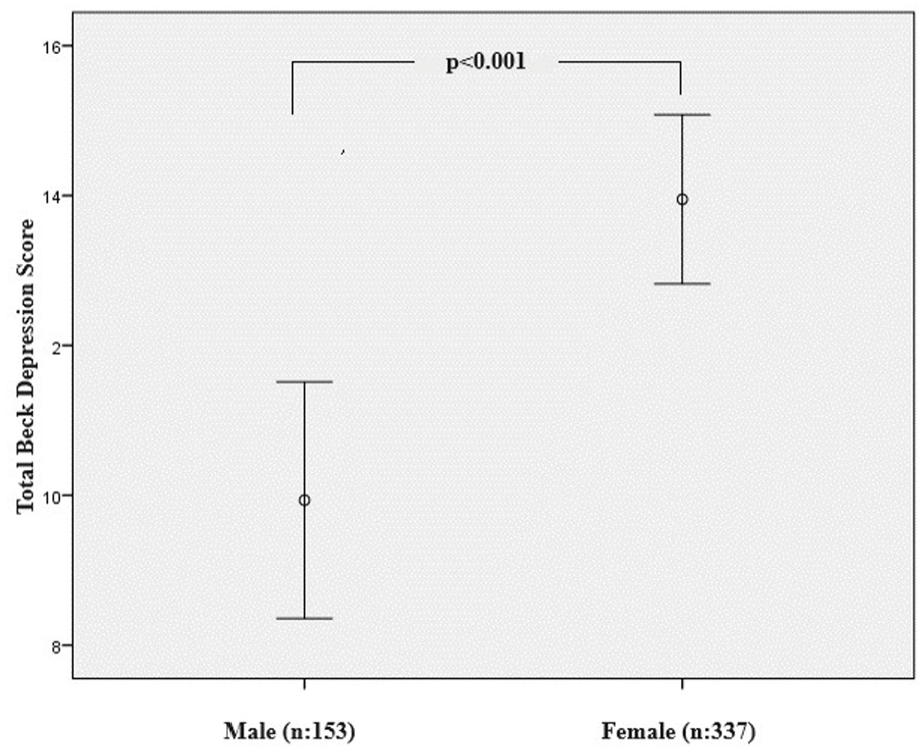
The depression scale was found to be positive in 30% of the patients and the anxiety scale was found to be high in 46% of the patients. Depression and anxiety were found to be significantly higher in females (p = 0.011, p < 0.001, respectively) (Figures 1 and 2). In addition, anxiety scales were significantly higher in patients with chronic diseases (p = 0.001). The most common symptoms in patients during the prolonged COVID period were weakness–fatigue, cough, and shortness of breath (Table 2). Anxiety and depression were found to be statistically significantly associated with symptoms (Table 2). For depression, weakness–fatigue, cough, shortness of breath, loss of taste and smell, headache, decreased appetite, feeling of exhaustion, fear of death, and palpitations were found to be significant symptoms, whereas anxiety, shortness of breath, headache, decreased appetite, feeling of exhaustion, loss of concentration and palpitations were found to be significant symptoms (Tables 2 and 3). Comorbidity was noted in 114 (23%) cases. The most common comorbidity was hypertension in 38 (7.7%) cases, asthma in 20 (4.1%) cases, and diabetes mellitus in 12 (2.4%) cases.
The Beck Depression score is higher in women.
The Beck Anxiety score is higher in women.
Comparison of depression and anxiety status with symptom rates.
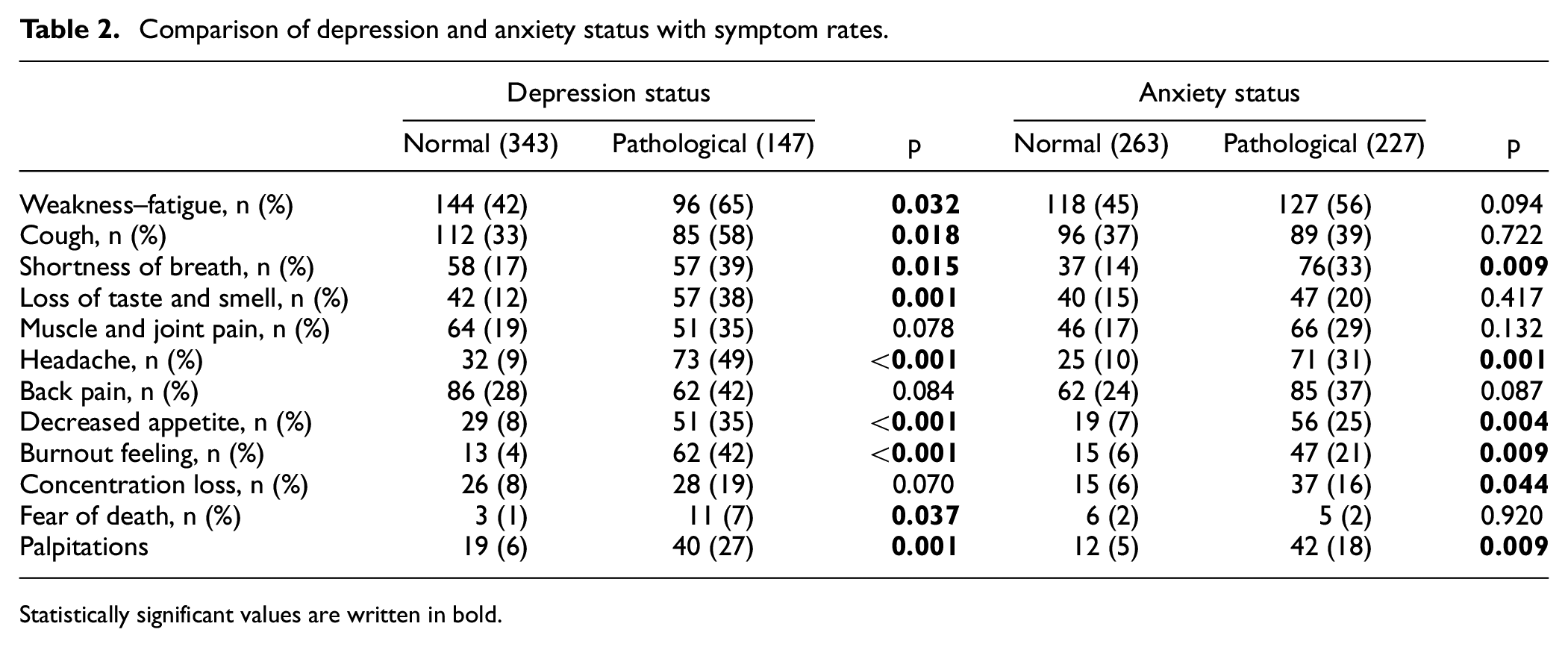
Statistically significant values are written in bold.
Univariate logistic regression analysis of factors associated with depression status.
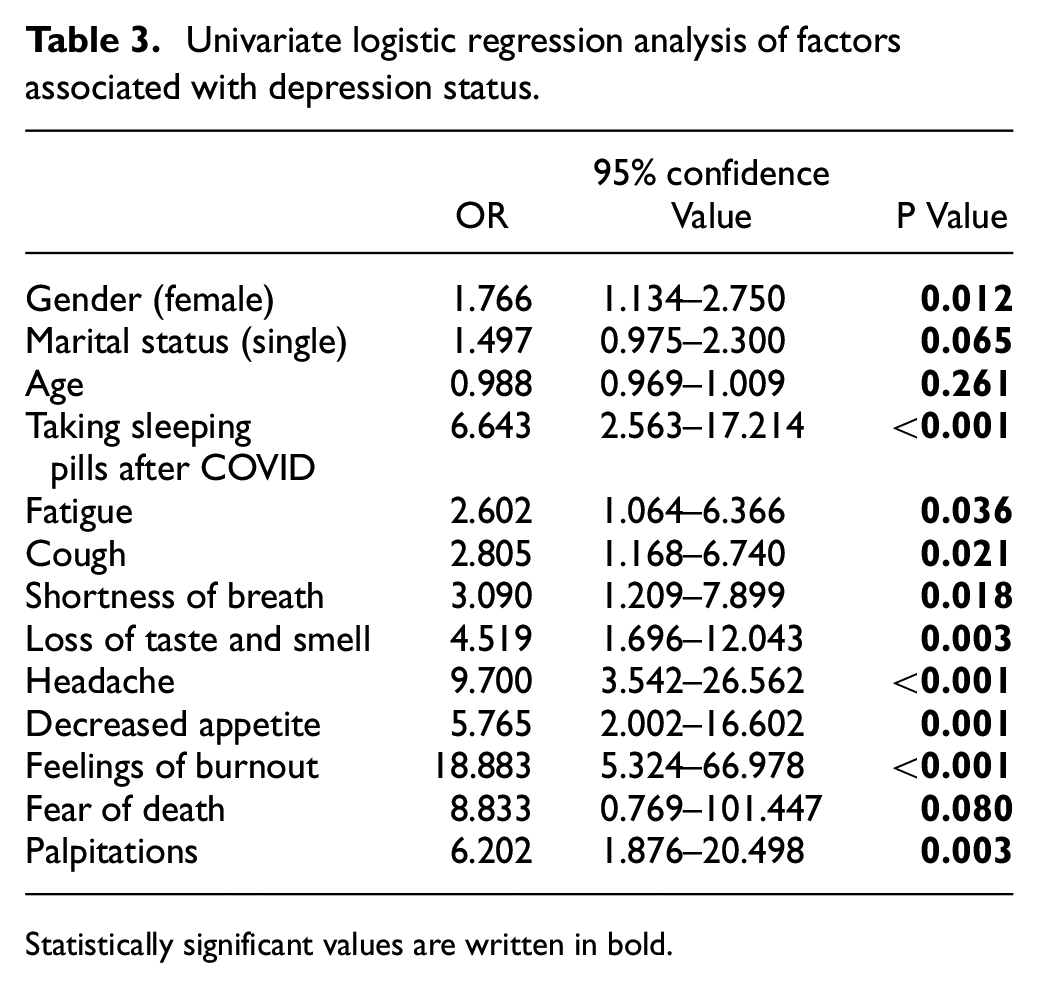
Statistically significant values are written in bold.
When all patients were analyzed, 34 (6.9%) were found to have suicidal tendencies. The mean age of these patients was 37 years, 11 (32%) were males and 23 (68%) were females. No statistical difference was found between those with and without suicidality in terms of gender, age, smoking, chronic diseases, marital status, and number of children. No statistical difference was found when the status of having lost a relative to COVID-19 and the status of having been vaccinated against COVID-19 were asked. Suicidality was statistically higher only among those who started to use sleeping pills during the long COVID-19 period (p = 0.024). Among the long-term symptoms, weakness–fatigue, cough, shortness of breath, loss of taste and smell, headache, decreased appetite, feeling of exhaustion, fear of death, palpitations, and increased appetite were found to be significantly higher in patients with suicidality. In addition, both the BAS and the BDS scores were found to be significantly higher in patients with suicidality than in other people (Table 4).
Depression and anxiety status of patients with and without suicidality.
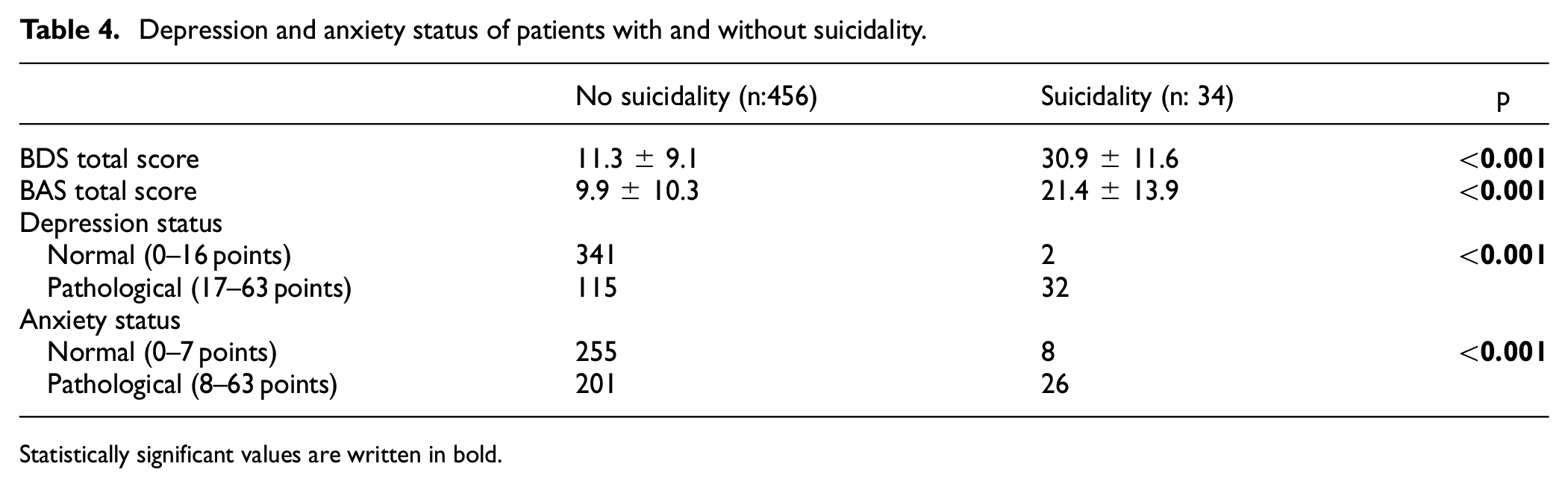
Statistically significant values are written in bold.
Discussion
As a result of our study, 30% of patients with long COVID scored positive on the BDS and 46% scored high on the BAS. In particular, female sex was found to be a risk factor for this condition. Anxiety and depression were found to be significantly associated with long COVID symptoms. When the patients were asked about their suicidality, it was found that 6.9% of the patients had suicide ideation, which was higher in females. Both BAS and BDS scores were significantly higher in people with suicidality compared to others, and long-term symptoms were found to be statistically associated with this situation.
A recognized aspect of long-term COVID is that similar post-viral syndromes have been observed in previous human coronavirus diseases. For example, fatigue, myalgia, and psychiatric disorders have been shown to affect survivors of Middle East respiratory syndrome and severe acute respiratory syndrome (SARS) for a period of up to 4 years. Even at 7-year and 15-year follow-ups, pulmonary complications were still evident in a proportion of SARS survivors, most of whom were under the age of 40. This is very disturbing for long COVID because it means that similarly with other viral infections long COVID can last from just a few months to many years. 23
In the literature, risk factors associated with COVID-19 survivors who develop persistent symptoms include female gender and a history of psychiatric disorder.24,25 Another study found that COVID-19 survivors who developed persistent fatigue 10 weeks after discharge were more likely to be female and to have a diagnosis of anxiety or depression or a history of antidepressant use. 26 In our study, similar to the literature, female gender was found to be a risk factor for anxiety and depression. And female gender was found to be more prevalent in individuals with suicidality. Another strength of our study is that, unlike these studies, it did not include people with a history of psychiatric disorders or antidepressant use. If these people had been included, the rates of anxiety, depression, and suicidality would have been much higher. We can show as evidence for this; in the study of Ho et al., COVID-19 and psychiatric patients had higher levels of depression, anxiety, and stress than healthy controls. 27
The prevalence of anxiety and depression among COVID-19 survivors has been investigated in various studies. One study found that COVID-19 patients with comorbidities were at a higher risk of depression and anxiety compared to those without comorbidities. 28 In our study, comorbidities were not found to be a risk factor for these conditions.
Another study reported a high prevalence of depression and anxiety among COVID-19 survivors in the city of Dhaka. 28 In addition, long COVID has been associated with neuropsychiatric manifestations such as depression, anxiety, post-traumatic stress disorder, sleep disturbance, fatigue, and cognitive deficits. 12 In our study, it was found that those who started using sleeping pills during the long COVID period had higher anxiety, depression, and suicidality. It can be considered that there is a cause-and-effect relationship between the higher incidence of sleep disturbance and poor sleep quality in patients with anxiety and depression. While people experiencing depression and anxiety as a result of the pandemic may lead to poor sleep quality and insomnia, poor sleep quality may lead to worsening depression and anxiety.
In particular, patients with COVID-19 have reported suicidal ideation during the acute phase of the disease. 29 The symptoms of psychiatric, neurological, and physical illness, as well as inflammatory damage to the brain, in patients with post-COVID syndrome, may increase the risk of suicidal tendencies in this population. 12
The COVID-19 pandemic has had a significant impact on mental health, with increased rates of depression, anxiety, and substance use reported. A survey conducted by the US Centers for Disease Control and Prevention (CDC) found that 10.7% of respondents reported suicidal ideation in the past 30 days during the COVID period. 30 The psychological impact of the pandemic, including social isolation, decreased physical activity, and pandemic-related social and economic insecurity, may contribute to the development of physical and psychological symptoms in individuals with long COVID. 31 Similarly, we found higher suicidal tendencies in patients with long COVID, and this was statistically significant in patients with long COVID symptoms.
Proposed solutions
It is important to address the mental health needs of individuals with long COVID to prevent and manage suicidal ideation. Psychological interventions can be formulated based on factors associated with a lower level of psychological impact and better mental health status, such as social support, access to health care, and coping strategies.32,33 And may be medical interventions should be suitable for these patients. Overall, studies have observed that vortioxetine significantly improved depressive symptoms among post-COVID participants in the adjusted model. 34 Or, Internet-based behavioral cognitive therapies may be considered for these patients who may be in isolation.35,36 Such digital therapies have been previously tried and found successful in the treatment of insomnia. 36 Suicide prevention measures should also be implemented, including improved access to mental health services, crisis hotlines, and support networks.
Limitations
The major limitation of our study is that it was a single-center study. The fact that only self-report scales measuring anxiety and symptom levels were used in the study and that examinations for psychiatric diagnoses of the subjects were not performed is a limitation. In addition, the fact that only the BDS questionnaire was used in the questioning of suicidal ideation of the subjects and a scale evaluating suicidal ideation was not used can also be considered as a limitation. However, despite all limitations, it is important to evaluate the psychosocial effects of COVID-19 in the long term. Therefore, we think that our study will shed light on future studies.
Conclusions
Depression and anxiety are common in cases of long COVID. Women are more likely to be affected. In addition, depression and anxiety should be considered in patients with more predominant symptoms of weakness–fatigue, cough, shortness of breath, loss of taste and smell, headache, decreased appetite, feeling of exhaustion, fear of death, and palpitations. These symptoms may persist even after recovery from the acute phase of the illness and can have a significant impact on an individual’s well-being. It is important for healthcare professionals to be aware of these potential mental health consequences, especially suicidality, and to provide appropriate support and interventions for individuals with long COVID.
Footnotes
Authors’ note
The article has not been presented elsewhere and has not been reviewed by any other journal. All the authors are aware of and approve the manuscript as submitted to this journal.
Author contributions
NÖ, SÖ, EST, and AG have given substantial contributions to the literature search, data collection, study design, analysis of data, manuscript preparation, and review of the manuscript. ÇH and ÜŞ analyze the interpretation of the data and review of the manuscript. All authors have participated in drafting the manuscript. NÖ, SÖ, EST, and AG revised it critically. All authors read and approved the final version of the manuscript. All authors contributed equally to the manuscript and read and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.