2024 Western Medical Research Conference Award Winners
Edwin E. Osgood Award
Alina Ferguson, University of Washington School of Medicine
WAFMR Outstanding Investigator Award
Shan Luo, University of Southern California
WAFMR Trainee Research Award
Pritika Parmar, University of Colorado
Leah Thomas, Loma Linda University
Nozomi Yamashita, Children’s Hospital Los Angeles
WAFMR/WAP/WSCI Student Subspecialty Award
Reagan Badger, University of Washington School of Medicine, University of Idaho
Heather Berndt, Western University of Health Sciences
Nicolas Cevallos, University of California San Francisco
Shengying Chen, Loma Linda University
Salina Goff, The University of Colorado School of Medicine
Caleb Hoopes, University of Washington School of Medicine
Verena Lawrence, University of Washington School of Medicine
Justin Lo, University of Washington School of Medicine
Luis Pozo, Northeast Ohio Medical University
Perla Saldivar, University of California, Riverside
Sailesh Wignarajah, University of California Irvine
WAFMR/WAP/WSCI Outstanding Resident Award
Sophia Kim, University of British Columbia
WAP/WSCI Travel Award
Kendra Francis, Seattle Children’s Hospital, University of Washington
Tyler Goshia, University of California San Diego, MelioLabs, Inc.
Shamil Jugnundan, University of California San Francisco
Varunya Kattunga, Charles R. Drew University of Medicine and Science
Maria Martes Gomez, Los Angeles General Medical Center/Keck School of Medicine of USC/CHLA
Megan Parfait, Saint Joseph Hospital
Nitya Rajeshuni, Stanford University School of Medicine
Danielle Sharp, Stanford University
Wenxi Tang, University of California San Diego
Alicia White, University of Colorado
WSPR Abbott Nutrition David W. Smith Pediatric Trainee Research Award
Paula Dias Maia, University of Colorado
WSPR Abbott Nutrition Lowell Glasgow Student Research Award
Danielle Liu, Loma Linda University
WSPR Abbott Nutrition Outstanding Resident Research Award
Aimee Juan, University of Pennsylvania, Stanford University
WSPR Abbott Nutrition Subspecialty Award
Cheri Chambers, University of Washington, Seattle Children’s Hospital
Emily Dunn, Stanford University
Evan Giusto, University of California, University of California, Davis
Ahmed Moutwakil, University of Colorado
Sofia Pesantez, Stanford University
Crystal Tam, University of Washington, University of Washington
Jingshing Wu, University of California, San Francisco
WSPR Abbott Nutrition Young Investigator Research Award
Jane Stremming, University of Colorado
WSPR Reckitt/Mead Johnson Subspecialty Award
David Blair, University of California San Francisco, UCSF Benioff Children’s Hospital Oakland
Page Calvert, Santa Clara Valley Medical Center
Faith Myers, Stanford Medicine
Andrew Rebentisch, University of Utah
Cadence Seymour, UC San Diego
Desiree Starzyk, University of Colorado School of Medicine
Tasha Wainstein, University of British Columbia, BC Children’s Hospital Research Institute
WSPR Prolacta Bioscience Research Award
Arjun Anumula, Sharp Mary Birch
Shiyu Bai-Tong, Rady Children’s Hospital, University of California, San Diego
Alexandra Carl, Children’s Hospital of Colorado
Tessa Gillespie, David Geffen School of Medicine at UCLA
Mihai Puia-Dumitrescu, Seattle Children’s Main hospital
Juan Ramos, Stanford University
Frank Strnad, University of Utah
Jakob Van Boerum, University of Utah
Lan Weiss, University of California, Irvine
Sean Wickers, University of California, San Francisco
Lijun Zheng, University of Colorado School of Medicine
Adolescent Medicine and General Pediatrics I
Concurrent Session
12:45 PM
Thursday, January 18, 2024
# 1
IDENTIFYING MOLECULAR PATTERNS IN THE PERIPHERAL IMMUNE PROFILE OF PATIENTS WITH PEDIATRIC ACUTE LIVER FAILURE
Kim H1, Fourfouris T1, Bangerth S2, Barbetta A2, Ascher-Bartlett J3, Rocque B4, Kohli R3, Emamaullee J2. 1Keck School of Medicine of USC, Los Angeles, CA; 2Keck School of Medicine of USC, Los Angeles, CA; 3Children’s Hospital of Los Angeles, Los Angeles, CA and 4University of Rochester Medical Center, Rochester, NY
Purpose of Study: Pediatric acute liver failure (PALF) is a rapidly progressing disease that can result in spontaneous resolution, need for emergent liver transplant, or death. Most cases are cause-indeterminate, which has been associated with upregulated CD8+ T-cell infiltrates in liver tissue.1 In this study, we used mass cytometry (CyTOF) to identify cell types and markers in the blood of PALF patients that deviate from controls, which may provide insight to the molecular patterns and processes of PALF.
Methods Used: Blood samples were collected from healthy children or those with PALF between August 2021 and June 2022. A 32-marker panel of metal-ion tagged antibodies was used for each sample and processed using CyTOF. Single cell data were analyzed to identify 27 immune cell phenotypes in FlowJo and R.
Summary of Results: This study included 12 patients: 5 with PALF and 7 healthy controls. PALF patients showed a trend toward marginal depletion of CD4+ T cells (p=0.14) and a marginal elevation of monocytes (p=0.21, Table 1). Further study into CD4+ T cell subtypes revealed a decrease in regulatory T cells (Tregs, CD25+/CD127-) (p=0.21) and terminally differentiated effector memory T cells (CD4+ TEMRA, CD45RA+/CD197-) (p=0.21) in PALF. CD4+ TEMRA in PALF were associated with lower expression of CD27 and CD38 (p<0.01, Fig. 1). Among monocyte subtypes of PALF compared to controls, classical monocytes (CD14+/CD38+) and transitional monocytes (CD38lo/CD14int) were elevated (p=0.091). PALF transitional monocytes showed higher expression of CD11c and lower expression of CD45RA (p<0.01).
Conclusions: In this pilot study, we observed differences in cell types and their marker expression when comparing PALF and healthy patients. Our data suggest that PALF may be associated with peripheral expansion of monocytes and depletion of CD4+ T cells subtypes. Further investigation of the relative depletion of Tregs and CD4+ TEMRA, as well as the elevated levels of classical and transitional monocytes in blood may lead to valuable insights regarding the cause, molecular processes, and therapeutic targets for mitigating inflammatory responses during PALF.
References
1Ascher Bartlett JM, Yanni G, Kwon Y, Emamaullee J. Pediatric acute liver failure: Reexamining key clinical features, current management, and research prospects. Liver Transpl. 2022;28(11):1776-1784. doi:10.1002/lt.26500
Comparing the average percentage of cells per sample in controls versus pediatric acute liver failure (PALF) for various immune cell types.
Cell type
Mean % of cells per sample ± SD (Control)
Mean % of cells per sample ± SD (PALF)
P value
All CD4+ T cells
35.871 ± 16.634
13.530 ± 8.374
0.14*
All monocytes
3.173 ± 3.566
15.657 ± 12.141
0.21*
Activated CD4+ T
0.584 ± 0.397
0.414 ± 0.299
1.00
CD4+ central memory T
4.332 ± 4.942
2.125 ± 1.928
1.00
CD4+ effector T
2.565 ± 1.533
1.414 ± 2.066
0.60
CD4+ TEMRA
10.638 ± 10.577
1.134 ± 1.602
0.21*
CD4+ naive T
6.192 ± 7.094
6.359 ± 1.896
1.00
Tregs
1.964 ± 1.589
0.395 ± 0.225
0.21*
Th2
10.214 ± 10.081
1.690 ± 1.560
0.53
Classical monocytes
2.627 ± 3.158
13.244 ± 12.028
0.091*
Nonclassical monocytes
0.168 ± 0.184
0.573 ± 0.666
0.150
Transitional monocytes
0.377 ± 0.582
1.840 ± 1.721
0.091*
# 2
SEASONALITY TRENDS IN MENTAL-HEALTH RELATED PEDIATRIC EMERGENCY DEPARTMENT VISITS DURING COVID-19 IN BRITISH COLUMBIA
Fan M, Black T, Doan Q. University of British Columbia, Vancouver, BC, Canada
Purpose of Study: During the COVID-19 pandemic, there were concerns about the potential negative implications of school closures on mental health. A surge in mental health service utilization was speculated, including visits to pediatric emergency departments (PEDs).
It is essential to examine rates of mental health PED visits by type of school day (school day, non-school day, school break, COVID-19 closure). This information is crucial for informing policies regarding school delivery, school supports, and emergency resource allocation. Our primary aim was to examine the change in rate of mental health PED visits with respect to type of school day in the first 2.5 pandemic years, compared to expected values based on pre-pandemic trends. Our secondary aim was to examine changes in proportion and rate for specific mental health presentations.
Methods Used: We conducted a retrospective cross-sectional study at the British Columbia Children’s Hospital PED using electronic administrative data. We included visits by children aged 2 to 17 years between January 1st, 2014 to December 31st, 2022. Descriptive statistics were used to calculate relative rates. A generalized additive model was used to estimate values during COVID-19 based on data from 5-years prior to the pandemic onset.
Summary of Results: Between January 1, 2014 to December 31, 2022, there were 13,484 total mental health presentations to the PED. There were 580 fewer mental health PED visits (95% CI, -914 to -245 visits) than expected during the pandemic. Rates of mental health PED visits were below expected during the pandemic, apart from school year 2 (2020 to 2021) where rates met expected values.
During the pandemic, there was a higher proportion of eating disorder and suicidal ideation presentations, and a lower proportion of aggression or behavioural problem, anxiety, mood, “other”, and substance use presentations. The proportion of visits for overdose, psychotic, and self-harm presentations remained unchanged. The was no difference in rate of specific presentations compared to expected, except the “other” category.
Pre-pandemic, school days averaged 5.0 visits per day ([95% CI 4.7 to 5.4]), non-school days averaged 3.8 visits per day (-25%, [95% CI -28% to -20%]) and school breaks saw 3.2 visits per day (-38%, [95% CI -42% to -33%]). During the entire pandemic, the decreased visit rates during non-school days and school breaks were similar to the decreased visit rates during COVID restrictions.
Conclusions: We found that mental health related PED visits decreased from expected rates in three of the four school years of the pandemic, with no significant deviations from expected visit rates when grouped by presenting concern. Mental health related PED visits were consistently higher on school days than non-school days, including COVID-19 school closure days. This may help inform resource allocation for emergency mental health management and highlights opportunities to improve support for pediatric mental health during school periods.
# 3
Small Rescuers Cannot Generate Sufficient Chest Compression Depth Using Conventional Chest Compression Methods, but They Can Generate Sufficient Chest Compression Depth Using Alternative Chest Compression Techniques
Sato J1, Len K1, Tessmer E2, Yamamoto LG1. 1University of Hawaii John A. Burns School of Medicine, Honolulu, HI and 2LifeScience Resources, Honolulu, HI
Purpose of Study: Effective CPR requires rescuers to use their body weight to provide sufficiently deep chest compressions for a prolonged period of time. Young/small children are unable to perform effective chest compressions due to their weight. Currently, there is no alternative CPR method for those who are too small. The purpose of this study is to assess the effectiveness of conventional and alternate chest compression methods performed by small children.
Methods Used: This study enrolled subjects ages 5-15 years old and taught them to perform standard CPR chest compressions using a standardized instructional video plus personal training/coaching by the study investigators. Subjects’ gender, age, weight, and height were recorded. Chest compression rate, depth, and release on a manikin were measured electronically for 2 minutes using chest compression depth sensing defibrillator pads. Those unable to successfully perform conventional chest compressions were taught alternative methods of jumping and squat bouncing on the manikin’s chest.
Summary of Results: 33 subjects ages 5 to 15 years have been enrolled thus far. The results are graphed in figure 1. Subjects weighing 27 kg were unable to perform sufficient conventional chest compressions. However, all underweight subjects (17 to 27 kg) could perform sufficient chest compressions using the alternative methods of jumping and squat bouncing on the manikin.
Conclusions: Conventional chest compression efficacy declines significantly below 27 kg but those who could not provide sufficient conventional chest compressions could perform sufficient compressions using jumping and squat bouncing potentially providing these children with a means of chest compressions while awaiting ambulance arrival.
Chest compressions provided in 2 minutes (Y-axis) by small rescuers at different weights (X-axis). Green triangles are total 2 to 2.5 inch depth (optimal) compressions delivered in 2 minutes. X and O symbols graph total 1.5 to 3 inch depth and 1.5 to 3.5 inch depth compressions delivered in 2 minutes, respectively. The left image shows standard compressions which were insufficient when performed by rescuers below 27 kg. The center and right images show better compressions performed by these rescuers below 27 kg using alternate compression methods. The middle image shows sufficient compressions delivered by jumping on the chest. The right image shows sufficient compressions delivered by squat bouncing on the chest.
# 4
Does Vitamin D Supplementation Have Prophylactic Health Benefits among Healthy Pediatric Patients? A Systematic Review of Randomized Controlled Trials
Law S, Zhang H, Park H, Truong K, Arnott K, Hsu M, Maheta B, Goswami C, Sheffield M, Culler F. California Northstate University College of Medicine, Elk Grove, CA
Purpose of Study: Previous studies have demonstrated vitamin D’s efficacy in preventing and treating rickets in children as well as its role in preventing vitamin D deficiency in breastfed neonates. However, excessive vitamin D supplementation can result in toxicity. The benefits of prophylactic prescription in a healthier pediatric population remains unclear. Thus, the goal of this systematic review is to assess whether prophylactic vitamin D has a beneficial effect in particular disease processes in healthy children (e.g. shortening the duration of a disease).
Methods Used: Covidence was utilized to review 10,155 articles from the PubMed, EMBASE, and Scopus databases. These articles underwent title/abstract and full-text screening through a blinded, independent dual review based on the inclusion criteria. The inclusion criteria for articles that were selected were randomized control trials with healthy pediatric patients who were prescribed vitamin D as prophylaxis. This study defines healthy patients as children under 18 years old who do not have a pre-existing vitamin D deficiency, chronic illness, signs of end-organ damage, or conditions with a proven benefit of vitamin D supplementation. The exclusion criteria eliminated articles that were not peer reviewed, not published articles in English, or contained patients with a history of hypercalcemia, rickets, or vitamin D deficiency. The dosage of vitamin D taken, frequency, duration, outcomes, and complications were extracted, and the Cochrane Risk of Bias tool was used to assess risk of bias. This study protocol has been registered to PROSPERO: CRD42023446944.
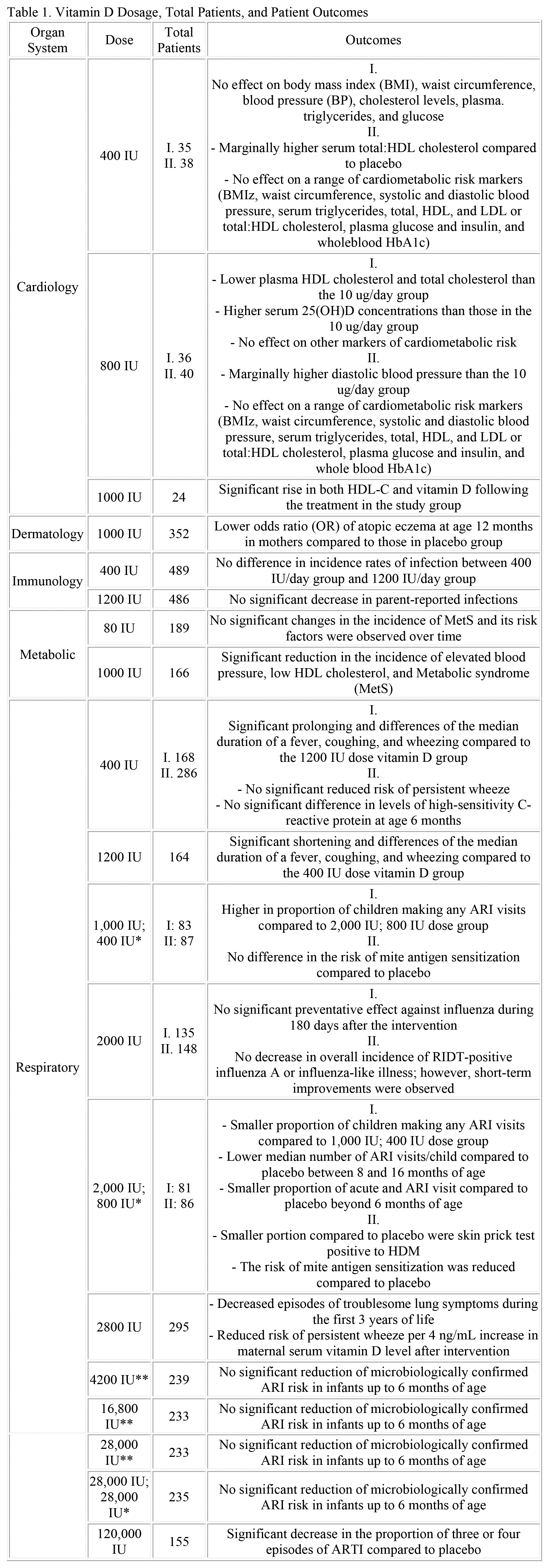
Summary of Results: A total of 14 articles, with 5,878 patients, and an overall low risk of bias were included. Eight studies observed the effects of prophylactic vitamin D on respiratory illnesses. For the prevention of acute respiratory infections and influenza, there was no significant reduction for supplementation doses between 2,000 IU/day and 28,000 IU/week. Interestingly, a 2,800 IU daily vitamin D supplement demonstrated a reduction in the risk of persistent wheeze and troublesome lung symptoms.
While three studies showed no statistically significant effect on cardiometabolic risk factors, including body mass index, waist circumference, and blood pressure when administering 400 or 800 IU daily, there were marginal increases in diastolic blood pressure and serum HDL cholesterol. Conversely, in a study administering vitamin D for metabolic syndrome prophylaxis, treated patients were less likely to have decreased HDL cholesterol levels and hypertension. Additionally, there were no significant decreases in incidence of parent-reported infections in patients given 1,200 IU daily.
Conclusions: Prophylactic vitamin D supplementation was generally not found to have statistically significant health benefits among healthy pediatric patients. Further investigation is necessary to determine the effects of prophylactic vitamin D on other organ systems and assess its potential harms.
Vitamin D Dosage, Total Patients, and Patient Outcomes.
Organ System
Dose
Total Patients
Outcomes
Cardiology
400 IU
I. 35 II. 38
I.
No effect on body mass index (BMI), waist circumference, blood pressure (BP), cholesterol levels, plasma. triglycerides, and glucose
II. - Marginally higher serum total:HDL cholesterol compared to placebo
- No effect on a range of cardiometabolic risk markers (BMIz, waist circumference, systolic and diastolic blood pressure, serum triglycerides, total, HDL, and LDL or total:HDL cholesterol, plasma glucose and insulin, and wholeblood HbA1c)
800 IU
I. 36
II. 40
I.
- Lower plasma HDL cholesterol and total cholesterol than the 10 ug/day group
- Higher serum 25(OH)D concentrations than those in the 10 ug/day group
- No effect on other markers of cardiometabolic risk
II.
- Marginally higher diastolic blood pressure than the 10 ug/day group
- No effect on a range of cardiometabolic risk markers (BMIz, waist circumference, systolic and diastolic blood pressure, serum triglycerides, total, HDL, and LDL or total:HDL cholesterol, plasma glucose and insulin, and whole blood HbA1c)
1000 IU
24
Significant rise in both HDL-C and vitamin D following the treatment in the study group
Dermatology
1000 IU
352
Lower odds ratio (OR) of atopic eczema at age 12 months in mothers compared to those in placebo group
Immunology
400 IU
489
No difference in incidence rates of infection between 400 IU/day group and 1200 IU/day group
1200 IU
486
No significant decrease in parent-reported infections
Metabolic
80 IU
189
No significant changes in the incidence of MetS and its risk factors were observed over time
1000 IU
166
Significant reduction in the incidence of elevated blood pressure, low HDL cholesterol, and Metabolic syndrome (MetS)
Respiratory
400 IU
I. 168
II. 286
I.Significant prolonging and differences of the median duration of a fever, coughing, and wheezing compared to the 1200 IU dose vitamin D group
II.
- No significant reduced risk of persistent wheeze
- No significant difference in levels of high-sensitivity C-reactive protein at age 6 months
1200 IU
164
Significant shortening and differences of the median duration of a fever, coughing, and wheezing compared to the 400 IU dose vitamin D group
1,000 IU; 400 IU*
I: 83
II: 87
I.
Higher in proportion of children making any ARI visits compared to 2,000 IU; 800 IU dose group
II.
No difference in the risk of mite antigen sensitization compared to placebo
2000 IU
I. 135
II. 148
I.
No significant preventative effect against influenza during 180 days after the intervention
II.
No decrease in overall incidence of RIDT-positive influenza A or influenza-like illness; however, short-term improvements were observed
2,000 IU; 800 IU*
I: 81
II: 86
I.
- Smaller proportion of children making any ARI visits compared to 1,000 IU; 400 IU dose group
- Lower median number of ARI visits/child compared to placebo between 8 and 16 months of age
- Smaller proportion of acute and ARI visit compared to placebo beyond 6 months of age
II.
- Smaller portion compared to placebo were skin prick test positive to HDM
- The risk of mite antigen sensitization was reduced compared to placebo
2800 IU
295
- Decreased episodes of troublesome lung symptoms during the first 3 years of life
- Reduced risk of persistent wheeze per 4 ng/mL increase in maternal serum vitamin D level after intervention
4200 IU**
239
No significant reduction of microbiologically confirmed ARI risk in infants up to 6 months of age
16,800 IU**
233
No significant reduction of microbiologically confirmed ARI risk in infants up to 6 months of age
28,000 IU**
233
No significant reduction of microbiologically confirmed ARI risk in infants up to 6 months of age
28,000 IU; 28,000 IU*
235
No significant reduction of microbiologically confirmed ARI risk in infants up to 6 months of age
120,000 IU
155
Significant decrease in the proportion of three or four episodes of ARTI compared to placebo
*Prenatal dosage to mother; Postpartum dosage to infant **Prenatal dosage to mother; Placebo to infant.
# 5
HIDDEN IN PLAIN SIGHT: LEARNING TO RECOGNIZE & RESPOND TO HUMAN TRAFFICKING IN OUR OWN COMMUNITY
Garza K1, Jackson Ruffin S1, Bertoldi A1, Colwell K1, Kinman R2. 1Fresno High School, Fresno, CA and 2UCSF Fresno, Fresno, CA
Purpose of Study: Human trafficking is a form of modern-day slavery; it is often described as being “hidden in plain sight” as victims of this crime may look “normal” and even interact with the community. Few of us are equipped to recognize its warning signs, while trauma and fear keep its victims from seeking help. Adolescents are especially susceptible to becoming human trafficking victims as traffickers often prey upon members of marginalized communities and other vulnerable individuals, while health care providers have generally not been trained to recognize victims of this crime. We chose to increase awareness of human trafficking by educating our high school peers, faculty, and staff, as well as local pediatric residents about the extent of human trafficking in the United States, how traffickers lure adolescents into this criminal activity, and the warning signs to be aware of.
Methods Used: A Kahoot survey was used to simultaneous survey and educate students about human trafficking. The national human trafficking hotline number was added to our school’s communication app, and red sand from the Red Sand Project was used to create an art installation project in the front of our school to raise awareness about this crime. We then went to UCSF Fresno to provide a didactic session for the UCSF Fresno pediatric residents on this topic and gave them badge cards containing the warning signs to watch for.
Summary of Results: Of the 154 high school students surveyed, only 70% were able to identify sex trafficking as the most common form of human trafficking in teens in the United States. Although 89% recognized that sex trafficking could happen to anyone, just 40% were able to identify those youth that are most likely to be trafficked. Eighty-seven percent identified gift-giving as a way in which human traffickers lure teens into human trafficking and 80% understood that human traffickers could be members of their own family, however only 57% were able to identify the warning signs that a teen was either being trafficked or being groomed for trafficking. Seventy-three percent correctly identified California as the state with the greatest number of teens being trafficked, 86% were able to state that the majority of human trafficking happens online, and 77% wanted to learn more about human trafficking.
Conclusions: Although human trafficking is the second largest and fastest growing criminal business in the world, if youth, adults working with youth, and adolescent health care providers cannot recognize the warning signs that someone in their own community is either at risk for or is actually being trafficked, then the human trafficking industry will continue to proliferate. Unfortunately, the average age of entry into human sex trafficking is just 12 years of age, with an average life expectancy of only 7 years after entering this criminal trade. As teen educators, we have the power to increase awareness and recognition of this crime that is robbing our fellow teens of their future and their lives.
# 6
Role of Physical Activity in Moderating the Relationship Between Cortisol Levels and Sleep Quality in Adolescents
Sankhala E2, Tan E2, Truong B2, Rao U1. 1University of California, Irvine, Irvine, CA and 2University of California, Irvine, Irvine, CA
Purpose of Study: Diurnal saliva cortisol levels can be used to measure stress levels on a day-to-day basis. This information can be analyzed and applied to key health factors such as sleep quality and daytime activity levels. Elevated night-time cortisol levels have been linked to poor sleep quality in adolescents. In particular, an increase in bedtime saliva cortisol levels is associated with reduced sleep quality, indicating sleep architecture changes. Daytime physical activity levels are also associated with sleep quality. Specifically, higher daytime activity levels, particularly soon after awakening, and increases in subjective sleep quality are positively correlated. However, we have limited information on the associations among nighttime cortisol, sleep, and activity levels. This analysis will examine the moderating effect of physical activity levels (analyzed via average daily steps) on the relationship between nighttime cortisol and sleep quality in adolescents.
Methods Used: 179 Adolescent females between ages 13-17 years (mean age 15.72) across three racial/ethnic groups (African American, Hispanic, and White) were recruited and interviewed for eligibility. Diurnal saliva cortisol samples were collected on two consecutive days at regular intervals (5 samples per day). Sleep and daily physical activity data were collected via daily diary and wrist ActiWatch (a watch-like monitor).
Summary of Results: A significant negative correlation between average daily steps and sleep onset latency was observed (r = -0.17, p = .021). Subsequent data analysis testing the moderating role of average daily steps on the relationship between nighttime cortisol levels and sleep onset latency revealed non-significant main effects of nighttime cortisol levels (b = 95.15, SE = 218.15, p = .66) and average daily steps (b = -0.00071, SE = 0.00071, p = .32) and a non-significant interaction effect (b = -0.0038, SE = 0.012, p = .75).
Conclusions: Although these results were not significant, they moved in the hypothesized direction. Possible modifications that may improve significance include using step count data from specific time periods; since physical activity fluctuates throughout the day, this data may provide a clearer trend. In addition, sleep onset latency was self-reported by participants and is subject to error.
# 7
ANALYSIS OF 3-DIMENSIONAL STEREOPHOTOGRAMMETRY TO TRACK FACIAL ATROPHY IN PATIENTS WITH PEDIATRIC JUVENILE LOCALIZED SCLERODERMA
Chambers CZ1, 2, Ringold S1, 3, Brandling-Bennett H1, 2. 1University of Washington, Seattle, WA; 2Seattle Children’s Hospital, Seattle, WA and 3Seattle Children’s Hospital, Seattle, WA
Purpose of Study: Juvenile localized scleroderma (JLS), or morphea, is a rare, chronic connective tissue disorder that causes excessive fibrosis and atrophy of the skin and subcutaneous tissues. Linear morphea is the most prevalent subtype of JLS. When it affects the head or face, it is known as en coup de sabre or progressive hemifacial atrophy/Parry-Romberg Syndrome. Currently, clinical assessment and 2-D photographs are primarily used to track response to treatment, as there are no standard laboratory tests that evaluate facial morphea activity. Therefore, there is an urgent need for an objective method to determine clinical response to treatment. We hypothesize that volumetric changes measured by 3-D surface images will correlate with clinical assessment of disease activity in pediatric facial morphea patients.
Methods Used: This retrospective study was conducted using a cohort of 11 patients, ages 3-18, seen at Seattle Children’s Hospital between January 2019 and June 2023 for facial morphea. Included patients had 2 or more appointments with a pediatric dermatologist and/or rheumatologist, over the time frame of 3 months to 4 years. Images were taken using the 5 pod 3dMD cranial system or handheld Canfield VECTRA H2 and were analyzed using Slicer 5.2.2 with extensions SlicerMorph and SlicerIGT.
Summary of Results: Volumetric analyses of 3-D images were completed in Slicer with a protocol developed to reduce error between patients and time points. First, images were aligned using standard landmarks: bilateral ear lobules, endocanthion, and exocanthion. Next, a bounding box for the region of interest (ROI) was created, using the hairline, chin, pronasale, and ear helices. Landmarks for the facial midline included bilateral endocanthion, exocanthion, and chelion, in addition to the nasion, subnasale, and pogonion. Growth was controlled for using midline symmetry, with the unaffected or less affected side for each patient serving as the control for normal growth. After each analysis, volume segmentations were adjusted for artifacts such as stray hairs covering the face. Volume measurements were found to be consistent with clinical assessments of disease activity characterized as improving, stable, or worsening for all 11 patients, who had images taken at 2-9 appointments each. This analysis was additionally helpful for monitoring facial asymmetry post-craniofacial surgery for facial morphea patients, with volumetric changes corresponding to physician perspective on surgery outcomes.
Conclusions: These results, from the largest pediatric facial morphea cohort in a 3-D imaging study, support the utility of 3-D imaging as an objective tool of disease activity to integrate into the clinical setting. Prompt treatment is important for preventing permanent atrophy from active morphea. Imaging as a method to track disease activity in facial morphea patients could help guide clinical decision making of treatment regimens, improving outcomes for patients.
# 8
MATERNAL THROMBOCYTOPENIA PRIOR TO DELIVERY WAS A POOR PREDICTOR OF NEONATAL THROMBOCYTOPENIA IN MOMS REGARDLESS OF MATERNAL PLATELET LEVEL OR MATERNAL ITP STATUS IN A RETROSPECTIVE REVIEW OF 4088 LATE-PRETERM AND TERM DELIVERIES FROM A DE-IDENTIFIED EHR DATABASE SPANNING 11 YEARS AT A TERTIARY ACADEMIC HOSPITAL
Wickers S1, Bokser S2. 1University of California, San Francisco, San Francisco, CA and 2University of California, San Francisco, San Francisco, CA
Purpose of Study: Providers do not use standard guidelines to screen newborns for thrombocytopenia (TP). Maternal Immune Thrombocytopenia Purpura (ITP) has been put forward as a risk factor for newborn TP. Some providers screen patients born to mothers with very low platelets regardless of maternal etiology. We did an analysis, leveraging large volume EHR data to better understand the predictive value of maternal platelet data and ITP on newborn TP.
Methods Used: We did a retrospective cohort study using de-identified EHR data. We included patients born at 36 weeks or later and associated maternal platelet data up to 5 days prior to delivery to infant platelet data up to 3 days following delivery. We assessed the predictive value of maternal platelet nadir prior to delivery for neonatal TP using linear regression and AUROC on all mothers as well as only mothers with the diagnosis of ITP.
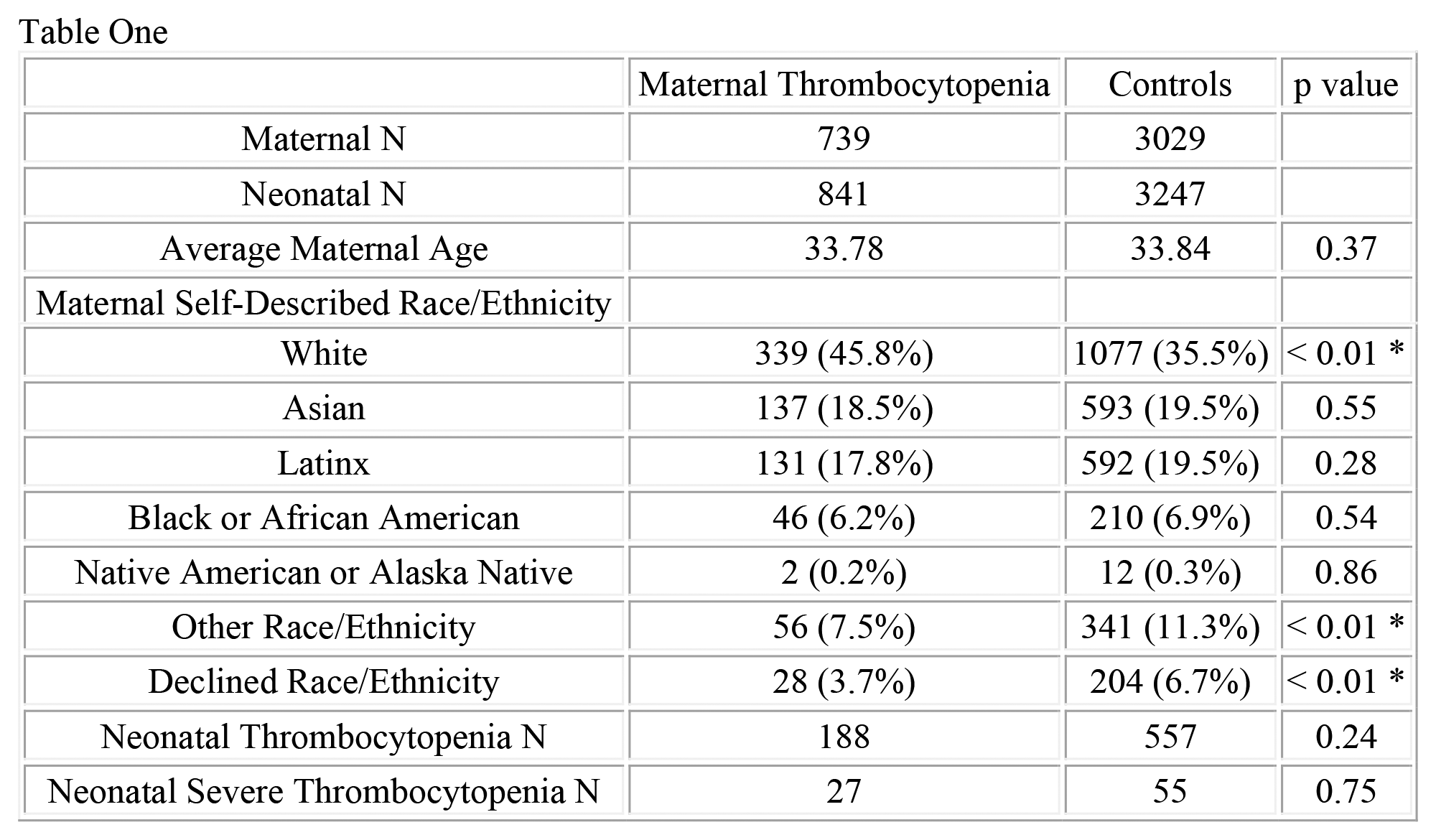
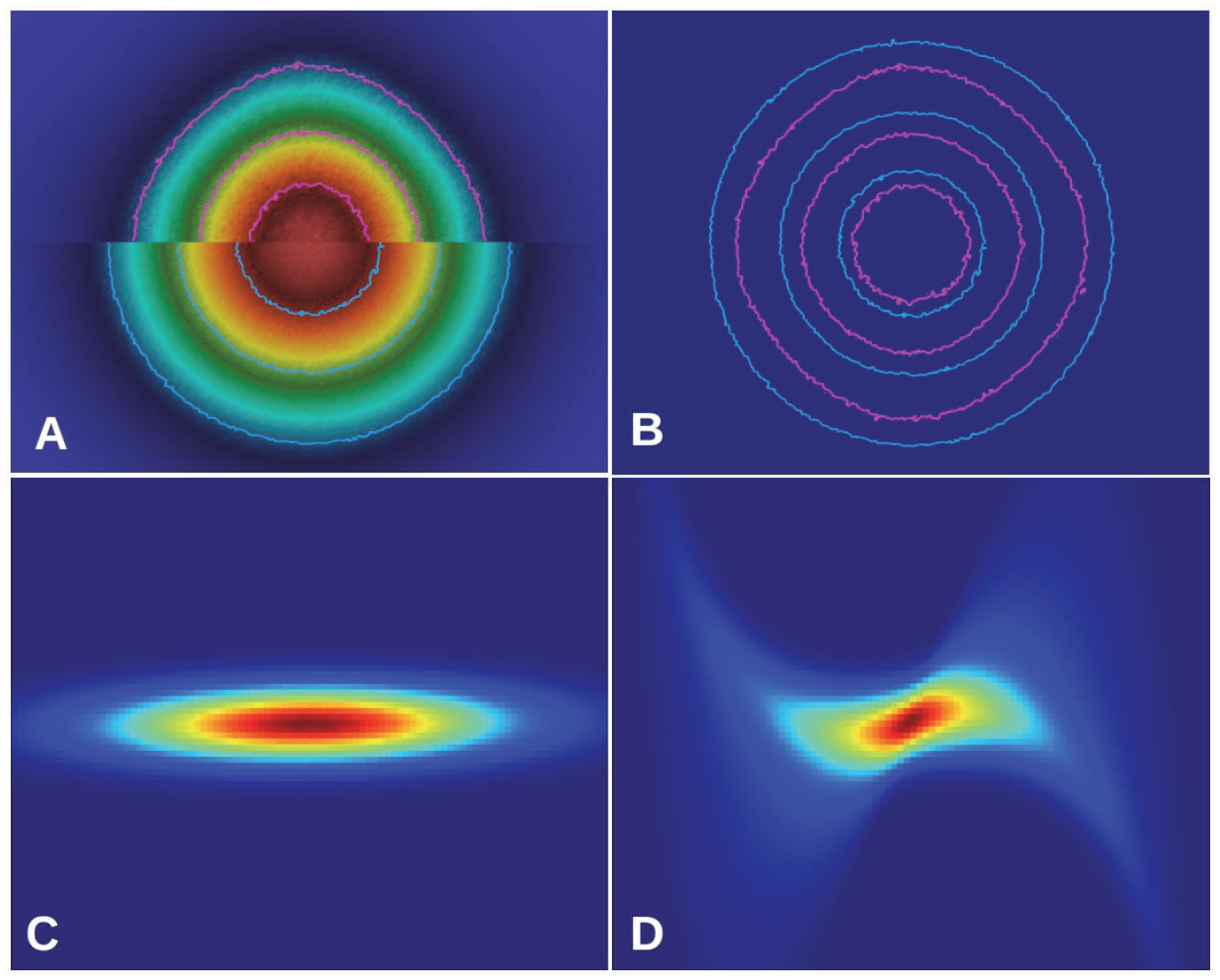
Summary of Results: We included 4088 deliveries, a cohort of 739 mothers with TP (841 newborns) and a control group of 3029 mothers (3247 newborns). 188 (22.4%) of neonates from the maternal TP cohort and 557 (17.2%) from the control group had TP (p = 0.24). Severe (< 50k) neonatal TP occurred in 27 (3.2%) and 61 (1.7%) respectively (p = 0.75). Maternal platelet nadir pre-delivery and infant platelet nadir data showed a statistically significant linear-regression correlation (slope = 0.097, p < 0.01*, R^2 = 0.007) (Fig Top Left). For the subgroup analysis of 94 infants born to 84 mothers with ITP, linear regression did not show a significant association (p < 0.59, R^2 = 0.003) (Fig Bottom Left). Analysis using AUROC for maternal platelet nadir level as a predictor of neonatal TP was 0.54 (Fig Top Right) and was 0.34 for moms with ITP (Fig Bottom Right).
Conclusions: This data suggests maternal platelet level does not have a clinically significant effect on neonatal platelets. Neither the linear regression or AUROC analysis support the previously reported association between maternal platelets of mothers with the diagnosis of ITP and neonatal TP. [Koyama et al]. Our analysis is limited by the EHR-data analysis retrospective design, nevertheless, our study suggests there is low value in routine platelets screening in neonates on the basis of maternal TP.
Maternal Thrombocytopenia
Controls
p value
Maternal N
739
3029
Neonatal N
841
3247
Average Maternal Age
33.78
33.84
0.37
Maternal Self-Described Race/Ethnicity
White
339 (45.8%)
1077 (35.5%)
< 0.01 *
Asian
137 (18.5%)
593 (19.5%)
0.55
Latinx
131 (17.8%)
592 (19.5%)
0.28
Black or African American
46 (6.2%)
210 (6.9%)
0.54
Native American or Alaska Native
2 (0.2%)
12 (0.3%)
0.86
Other Race/Ethnicity
56 (7.5%)
341 (11.3%)
< 0.01 *
Declined Race/Ethnicity
28 (3.7%)
204 (6.7%)
< 0.01 *
Neonatal Thrombocytopenia N
188
557
0.24
Neonatal Severe Thrombocytopenia N
27
55
0.75
Table 1. Maternal demographic information separated by cohort, as well as a comparison of the incidence of neonatal thrombocytopenia and severe (< 50k) neonatal thrombocytopenia by cohort.
# 9
Promoting healthy behaviors among adolescents in under-resourced schools through building successful partnerships with medical residency programs: An implementation study in four US states
Gefter L1, Srivastava A1, Jiang C1, Morioka-Douglas N1, Rodriguez E2. 1Stanford University, Stanford, CA and 2Stanford University, Stanford, CA
Purpose of Study: To describe the implementation of successful and sustainable partnerships of medical residency programs and high schools in low-income communities. Case studies of implementing health prevention in four different geographical areas are presented to better understand factors that facilitate successful program implementation and practices to overcome implementation challenges.
Methods Used: Stanford Youth Diabetes Coaches Program (SYDCP) is an 8-week program in which medical residency programs partner with local underserved high schools. Instructors (medical residents or other healthcare trainees) train high school students to become health coaches for family members with diabetes, with the goal of improving health knowledge, psycho-social assets, family communication about health, and healthy behavior among youth. SYDCP has been rigorously evaluated and proven to be beneficial both for medical residents and youth (see Table 1 for list of references). In these case studies, adolescent participants (grades 9-12) from under-resourced high schools in Alabama, California, Hawaii, and Washington DC were offered the program either in-person or remotely during Spring 2022- Spring 2023. Online pre-post surveys of youth participants were analyzed to assess program effectiveness. Online post-surveys of community partners including program administrators, schoolteachers and program instructors were analyzed to assess program acceptability and adoption and assess facilitators and barriers of program implementation.
Summary of Results: A total of 167 adolescents (78% female; mean age 15.4 years; 19% Asian; 28% Black or African American; 13% White; and 30% Hispanic) completed pre and post surveys. Significant improvements (p<.01) were reported in health knowledge, psychosocial assets (self-esteem, self-efficacy, problem solving), health behaviors (physical activity, nutrition, stress reduction), and family communication about health. 94% of youth participants reported making a health behavior change after program completion. Program administrators and schoolteachers expressed that the coaching program was applicable, implementable, easy to use, relevant to their community and aligned with curriculum needs at their schools. Medical residents found the program useful to grow their skills as physicians and manageable with other responsibilities. Barriers to implementation and expansion included limited resources and personnel, and scheduling conflicts with instructors.
Conclusions: Building partnerships between medical residency programs, community organizations, and local underserved schools can be an effective strategy to promote healthy behavior in youth from low-income communities in limited resource settings. Community partner organizations were able to successfully implement the program in coordination with medical residency programs.
Table of Abstract References
1. Gefter, L., et al., Training at-risk youth to become diabetes self-management coaches for family members: partnering family medicine residents with underserved schools. Diabetes Educ, 2014. 40(6): p. 786-96.
2. Gefter, L., et al., Service-Based Learning for Residents: A Success for Communities and Medical Education. Fam Med, 2015. 47(10): p. 803-6.
3. Gefter, L., et al., Supporting At-Risk Youth and Their Families to Manage and Prevent Diabetes: Developing a National Partnership of Medical Residency Programs and High Schools. PloS one, 2016. 11(7): p. e0158477.
4. Gefter, L., et al., Addressing Health Disparities and Increasing Cultural Competency of Medical Trainees with Community Engagement. J Community Med Health Educ, 2019. 9(647): p. 2161-0711.1000647.
5. Gefter, L.R., et al., Increasing patient activation scores of vulnerable youth by partnering medical residency programs with public high schools. Patient education and counseling, 2021. 104(4): p. 927-931.
6. Gefter, L., et al., Remote Implementation of a School-Based Health Promotion and Health Coaching Program in Low-Income Urban and Rural Sites: Program Impact during the COVID-19 Pandemic. International Journal of Environmental Research and Public Health, 2023. 20(2): p. 1044.
Cardiovascular I
Concurrent Session
12:45 PM
Thursday, January 18, 2024
# 10
CHARACTERIZING RIGHT VENTRICLE FUNCTION IN PHYSIOLOGICALLY AGED MALE MICE
Hoopes CR1, McNair BD2, Thornburg J2, Bruns DR2, 1. 1University of Washington School of Medicine, Seattle, WA and 2University of Wyoming, Laramie, WY
Purpose of Study: Age is the primary risk factor for heart disease, which is the leading cause of mortality in the United States. The aging process in the left ventricle (LV) is well characterized. Many clinical interventions rely on this understanding of LV aging to treat heart disease. However, little is known about the aging right ventricle (RV), even though in multiple clinical conditions, RV function is the primary predictor of patient survival. If the aging process of the RV differs from the LV, then drugs can potentially be tailored to preserve RV function, improving mortality for several conditions. The purpose of this study was to identify age-related changes in RV function and understand how the aging mechanisms differ from those previously established in the LV.
Methods Used: We quantified RV function in a cross-sectional cohort of young adult (8-10 weeks) and aged (19-22 months) C57BL6 male mice using pressure volume (PV) loops and echocardiography. RV PV loops were collected by an open chest apical approach using a conductance catheter inserted into the RV free wall. Following quantification of RV function, tissue was harvested for histology and RNA-sequencing. Results with a p-value below 0.05 were considered statistically significant.
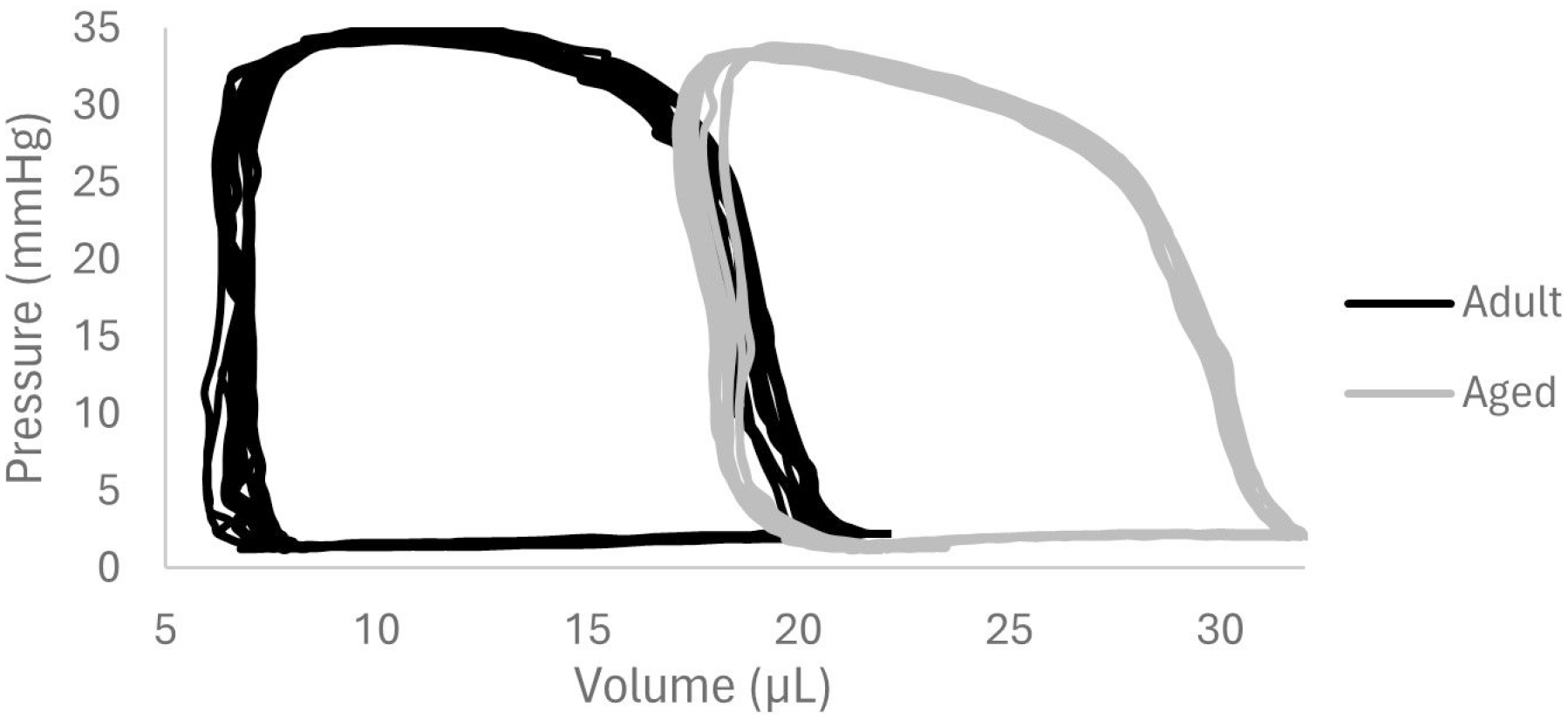
Summary of Results: The aged RV showed evidence of eccentric remodeling. The chamber was dilated in PV loop studies (Image 1), and echocardiography demonstrated increased RV area (p=0.03) and decreased thickness of the anterior RV free wall compared to young adult mice (p<0.001). Ejection fraction (p=0.003) and fractional area change (p=0.005) decreased with age. The evidence for eccentric remodeling was supported by histology that demonstrated RV wall thinning and chamber dilation. RNA-sequencing demonstrated distinct genetic signatures in the aging RV compared to those in the LV.
Conclusions: While the LV undergoes concentric remodeling and diastolic dysfunction with aging, the RV follows a pattern of eccentric remodeling with systolic impairment, clearly demonstrating ventricle-specific consequences of aging. Moreover, genetic analysis suggested that the two ventricles are molecularly different, an encouraging finding for the identification of RV specific drug targets. Ongoing studies aim to understand sex differences in RV aging given the reports of significant sex differences in the aging LV. The path forward to better treating heart disease involves identifying therapies that are specific to improving RV function- an unmet clinical need.
Representative RV PV loops in young adult and aged male C57BL6 mice.
# 11
Outcomes of Biopsy Negative but MMDx-Positive Biopsies After Heart Transplant: What Does This Mean?
Deckerman P, Singer-Englar T, Kanungo A, Bhatnagar N, Hamilton M, Kobashigawa J. Cedars-Sinai Smidt Institute, Los Angeles, CA
Purpose of Study: The endomyocardial biopsy after heart transplantation (HTx) has been the gold standard to detect rejection. However, in multi-center studies it has been demonstrated that the concordance rate of pathology-read biopsy positive rejection is only 67% and may be much less for antibody-mediated rejection (AMR). We now have the ability to assess mechanistic pathways through the use of intragraft mRNA transcripts (in the heart biopsy) called the molecular microscope (MMDx). This uses microarrays to assess gene-related pathways that reflect ACR, AMR and quiescence. In some cases, there have been reports of discordant biopsies with the MMDx; this is a biopsy read as normal but yet the MMDx reveals rejection. It is not known whether the outcome for these patients results in cardiac dysfunction and/or increased morbidity or mortality.
Methods Used: Between 2010 and 2022, we assessed 6 HTx patients who had a normal biopsy but positive MMDx for rejection and 11 Htx patients who had a normal biopsy and normal MMDx. Subsequent 1-year outcomes included survival, freedom from ACR/AMR, freedom from CAV, freedom from cardiac dysfunction (LVD defined as LVEF ≤40%), freedom from non-fatal major adverse cardiac events (NF-MACE: myocardial infarction, new congestive heart failure, percutaneous coronary intervention, pacemaker/implantable cardioverter defibrillator placement, stroke).
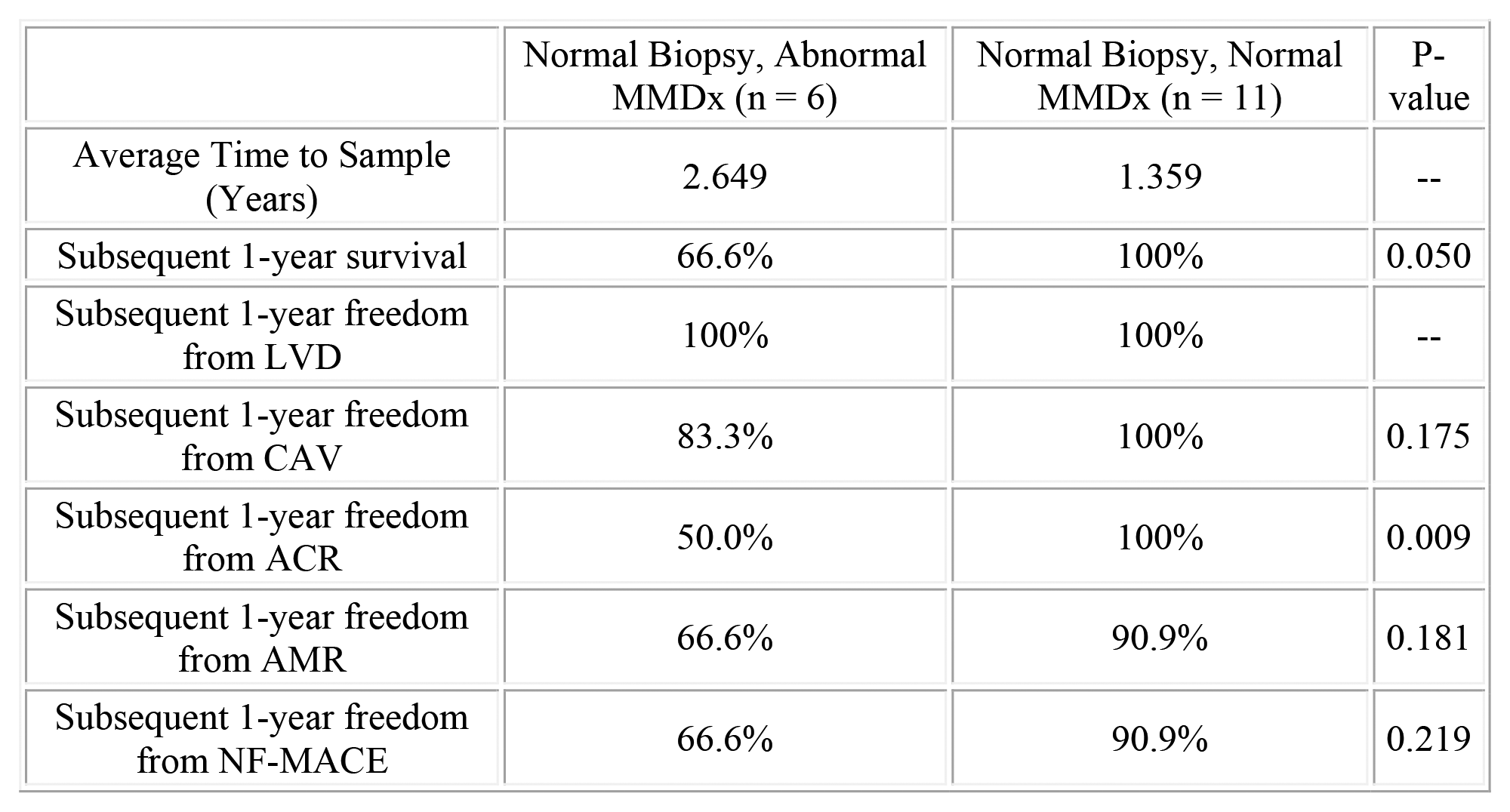
Summary of Results: Patients with normal biopsy but positive MMDx developed significantly less subsequent 1-year survival, 1-year freedom from ACR particularly if the MMDx was positive for cellular rejection. There were no significant differences between study groups on subsequent 1-year freedom from LVD, freedom from CAV, freedom from NF-MACE and freedom from AMR.
Conclusions: The MMDx may have clinical relevance in that untreated rejection may have serious consequences, especially if there is T-cell mediated rejection missed by endomyocardial biopsy read by pathology. Larger studies will be needed to confirm these findings.
Normal Biopsy, Abnormal MMDx (n = 6)
Normal Biopsy, Normal MMDx (n = 11)
P-value
Average Time to Sample (Years)
2.649
1.359
–
Subsequent 1-year survival
66.6%
100%
0.050
Subsequent 1-year freedom from LVD
100%
100%
–
Subsequent 1-year freedom from CAV
83.3%
100%
0.175
Subsequent 1-year freedom from ACR
50.0%
100%
0.009
Subsequent 1-year freedom from AMR
66.6%
90.9%
0.181
Subsequent 1-year freedom from NF-MACE
66.6%
90.9%
0.219
# 12
ACTION OF SECRETED FRIZZLED RECEPTOR PROTEIN 1 IN PEDIATRIC DILATED CARDIOMYOPATHY
Rausch E1, 2, Nyarko O4, Stauffer B2, Miyamoto S3, Sucharov C2. 1University of Denver, Denver, CO; 2University of Colorado Anschutz Medical Campus, Aurora, CO; 3University of Colorado Anschutz Medical Campus, Aurora, CO and 4University of Colorado Anschutz Medical Campus, Aurora, CO
Purpose of Study: Dilated cardiomyopathy (DCM) is the leading cause for heart transplantation in children over the age of 1. Treatment options are limited in pediatrics as children respond differently than adults to the disease at a cellular level, limiting traditional adult treatments from being effective in children. We previously showed that circulating proteins in the serum of children with DCM are important for cardiomyocyte remodeling in response to DCM. We previously found that secreted frizzled receptor protein 1 (sFRP-1), a protein upregulated in the serum of children with DCM, promotes cardiomyocyte stiffness and reactivate the fetal gene program (FGP), which is a key characteristic of pathologic cardiac remodeling in neonatal rat ventricular myocytes (NRVMs). Our preliminary results also show that sFRP-1 can cause cardiac dysfunction in neonatal rats. We hypothesized that this protein works through inhibition of the WNT signaling pathway similarly to its action in colorectal and prostate tumor suppression models. The purpose of this project was to determine if sFRP-1 acted as a WNT inhibitor as hypothesized.
Methods Used: NRVMs were treated with combinations of sFRP-1, WNT-C59 (a known WNT inhibitor), and CHIR-99021 (a known WNT activator). Cellular RNA was extracted using TRizol (Invitrogen) and reverse transcribed into cDNA using the Superscript IV synthesis kit (Thermofisher), as previously described by our group, and RT-qPCR was performed to assess FGP expression. The data was analyzed using ANOVA.
Summary of Results: Activation of the FGP is indicative of cardiomyocyte remodeling and heart failure and is characterized by upregulation of atrial natriuretic factor (ANF), b-type natriuretic peptide (BNP), and a decrease in the α-myosin heavy chain (α-MHC) to β-myosin heavy chain (β-MHC) ratio. We found that treatment of cells with sFRP-1 caused a similar activation of the FGP compared to treatment of the cells with WNT-C59, a known WNT inhibitor. Furthermore, a combination of WNT-C59 and sFRP-1 did not further increase the activation of the FGP. The lack of an additive or multiplicative effect indicated that WNT-C59 and sFRP-1 most likely worked through the same pathway. Cells treated with CHIR-99021 showed no activation of the FGP, regardless of co-treatment with WNT-C59 or sFRP-1. Cells treated with only CHIR-99201 showed significant decreases to ANF and BNP expression, and a large increase to the α-MHC/β-MHC ratio. These two results showed that activation of the WNT pathway entirely prevented the effects of WNT inhibition on the cells.
Conclusions: The findings of this project indicate that inhibition of the WNT pathway plays a role in cardiac remodeling in cases of pediatric DCM. This information will be used in the development of an animal model examining the effects of sFRP-1, WNT-C59 and CHIR-99021 in-vivo. Furthermore, these results show that the WNT pathway and sFRP-1 may be used as targets for potential DCM treatments in the future.
# 13
BODY COMPOSITION AND CARDIOVASCULAR OUTCOMES: FINDINGS FROM THE MULTI-ETHNIC STUDY OF ATHEROSCLEROSIS
Weene E1, Kronmal R2, Srikanthan p1, Allison M3, Watson K1, Horwich T1. 1UCLA, Los Angeles, CA; 2University of Washington, Seattle, WA and 3UC San Diego, San Diego, CA
Purpose of Study: This analysis aims to examine the associations between estimated fat mass and fat-free/ lean mass with incident CAD events. Although obesity is associated with an increased risk of coronary artery disease (CAD), it has been debated how body composition (fat and lean mass) contributes to CAD.
Methods Used: The study population included 6,814 participants in the Multi-Ethnic Study of Atherosclerosis (MESA) without clinically apparent cardiovascular disease. Using data from Exam 5 bioelectrical impedance analysis, equations were derived in order to estimate participants’ fat-free mass (ffm); equations were 93% and 95% accurate in predicting bioelectrical impedance outputs of ffm for men and women, respectively. [Female: ffm = 8.6682593*(age^-.2484878)*(weight(kg)^.4990013) * (1.026077*height(m)); Male: ffm = 6.6901882*(age^ -.1800577)*(weight(kg)^.4912168) * (1.397042* height(m))]. These equations were then used to estimate participants’ ffm at Exam 1, using age, weight, and height from Exam 1. Subsequently, participants’ fat mass was calculated using the equation fat mass = weight(kg) - ffm. Multivariable Cox regression models with cubic splines to allow for non-linear associations were used to determine the associations between fat mass, fat-free mass, and incident CAD events, defined as CAD-related death, myocardial infarction, angioplasty, or coronary bypass for angina. The MESA risk score, a single, composite covariate for cardiovascular risk was added to regression equations.
Summary of Results: After baseline, the median follow-up time was approximately 19 years. During that time, 559 CAD events occurred. In the multivariable regression model, both fat-free mass and MESA risk score had significant associations (P<0.001 and P<.0001, respectively) with CAD events. Fat mass was not significantly associated (P=0.744) with CAD events. The log relative hazard for fat-free mass (kg) is depicted in the figure below; there is a significant incremental increase in risk as fat-free mass descends below 40 kg.
Conclusions: Low fat-free mass is independently associated with a higher risk of incident CAD. These results suggest that effective lifestyle strategies that focus on maintaining healthy levels of muscle mass may be more relevant to CAD risk than strategies that focus on weight management.
# 14
OPTIMIZING SYSTEMIC TO PULMONARY ARTERY SHUNT DIAMETER IN DIGITALLY MODELED PATIENT GROWTH
Dion NR3, Tu Y1, Greene C4, 1, Bohuta L4, 5, Nigam V4, 1, del Alamo J1, 2. 1University of Washington, Seattle, WA; 2University of Washington, Seattle, WA; 3University of Washington, Seattle, WA; 4Seattle Children’s Research Institute, Seattle, WA and 5University of Washington, Seattle, WA
Purpose of Study: Hypoplastic left heart syndrome (HLHS) is a fatal congenital heart defect requiring treatment soon after birth. HLHS palliation involves a 3-part Norwood surgery to reconfigure the right ventricle to supply both the systemic and pulmonary vasculatures. The first step is achieved with a systemic-to-pulmonary artery shunt (S2PAS). Current Gore-Tex shunts have a fixed diameter and, therefore, vary in hemodynamic resistance as patients grow, posing a significant clinical problem. Eventually, patients outgrow the shunt leading to cyanosis from insufficient pulmonary blood flow. Conversely, if the implanted shunt is too large, the child will develop pulmonary over-circulation leading to systemic hypoxia. The goal of this study is to simulate the circulation post S2PAS implantation in digitally growing patients. We hypothesize these simulations will guide the design of smart shunts that optimally adjust their diameter in concert with patient growth.
Methods Used: A lumped-parameter model was used to simulate the Norwood circulation based on the well-established electrical circuit analogy, including time-dependent elastance models for the cardiac chambers. The model comprised the pulmonary loop, systemic loop, and hypoplastic heart, yielding a system of 25 differential equations that were solved with MATLAB. Model parameters at birth were selected from similar models in the literature and fitted to newborn patient hemodynamic data. Using the method of allometric scaling, these parameters were "grown" as a function of body mass, which was tabulated to patient age using standardized growth curves. For each patient’s age, multiple simulations were run to determine the optimal shunt diameter that would result in equal pulmonary and systemic vascular flow rates.
Summary of Results: Our model successfully generates time-dependent waveforms for systemic and pulmonary flow rates and pressures comparable to previous studies, in addition to matching pressure-volume curves for the right ventricle. The use of allometric scaling for longitudinal predictions of pulmonary flow demonstrates success in extrapolating the desired parameters. Our simulations, using digitally grown patient models, reveal that the optimal SPAS diameter varies significantly over the first 6 months of age, in contrast with the current constant-diameter clinically used shunts.
Conclusions: Prior research in this field has focused on optimizing shunt geometry and placement at the time of implantation, but this fails to account for the rapidly changing requirements of pulmonary flow as the infant develops. Modeling the Norwood circulation in digitally growing patients could lay the foundation for new smart shunts that change geometry in vivo to meet the dynamic needs of growing infants. The simplicity of lumped-parameter and allometric scaling models makes computing time short enough to avoid interference with clinical workflows.
# 15
TRANSIENT RECEPTOR POTENTIAL VANILLOID CHANNEL EXPRESSION IN MALE AND FEMALE MOUSE RESISTANCE-SIZED ARTERIES
Yeganyan S1, Ahmed SM2, Choi YD2, Bulley S2. 1Western University of Health Sciences, Pomona, CA and 2Western University of Health Sciences, Pomona, CA
Purpose of Study: Transient receptor potential vanilloid (TRPV) channels 1-4, activated by numerous ligands, temperature, osmotic imbalance, and mechanical stretch, are sensory channels expressed in smooth muscle and endothelial cells within the vasculature. Studies have shown that upon activation, these channels have the potential to modulate vascular diameter, leading to vasoconstriction or vasodilation, and therefore they are integral regulators of arterial tone and therefore blood pressure regulation. However, it is largely unclear whether differences exist in the expression and function of TRPV channels in resistance-sized systemic arteries between females and males, and due to their importance in vascular function, they could potentially be potential pharmaceutical targets for sex-specific treatment of numerous cardiovascular diseases, including hypertension.
Methods Used: Resistance-sized mesenteric and hindlimb arteries were isolated from 12–14-week-old C57BL/6J male and female mice. RT-qPCR and Simple Western were used to compare message and protein expression, respectively, of TRPV1-4 channels in isolated arteries. Immunofluorescence was utilized to determine the cellular expression and distribution of TRPV1-4 channels in systemic arteries. To determine whether TRPV1-4 expression is altered in hypertensive mice, osmotic pumps containing either angiotensin II (25mg/kg/day) or saline (controls) were implanted subcutaneously on the back in C57BL/6J male and female mice 14 days before tissue harvesting.
Summary of Results: Protein expression of TRPV1 channels is significantly reduced in female mouse mesenteric arteries compared to male mesenteric arteries (0.18-fold, p<0.05), whereas the expression of TRPV2 channels is elevated in mesenteric arteries isolated from females when compared to males (2.50-fold, p<0.05). In contrast, TRPV3 and TRPV4 expression is comparable in female and male mesenteric arteries (0.79-fold and 0.92-fold, respectively). TRPV channels are expressed in mesenteric smooth muscle and endothelial cells, as indicated by immunofluorescence.
Conclusions: These results suggest that TRPV channel expression is not equivalent in males and females, indicating that mechanisms for regulating arterial contractility in systemic vessels may have sex-dependent variation. Further studies are necessary to determine whether changes in TRPV expression correspond to changes in TRPV function in resistance-sized arteries, as well as determine whether there are sex-specific differences in the expression of TRPV channels in hypertensive female and male mice.
# 16
Monotherapy in Heart Transplantation Proves to be Safe While Followed By T-cell Immune Function Testing
Jeong E, Singer-Englar T, Kanungo A, Bhatnagar N, Hamilton M, Kobashigawa J. Cedars-Sinai Smidt Institute, Los Angeles, CA
Purpose of Study: Tacrolimus monotherapy immunosuppression (TMI) in heart transplantation occurs due to adverse effects from concurrent drugs. It has been found to be safe as noted by the TICTAC trial (2011). However, tacrolimus levels in that study were maintained in the 8-12 ng/ml range resulting in higher serum creatinine levels at 1-year post-transplant. The T-cell immune function blood test (TCIF) is used to assess the immunosuppressive state of heart transplant patients. It is not known if tacrolimus levels in the 4-8 ng/ml range provides adequate immunosuppression on TMI using the TCIF.
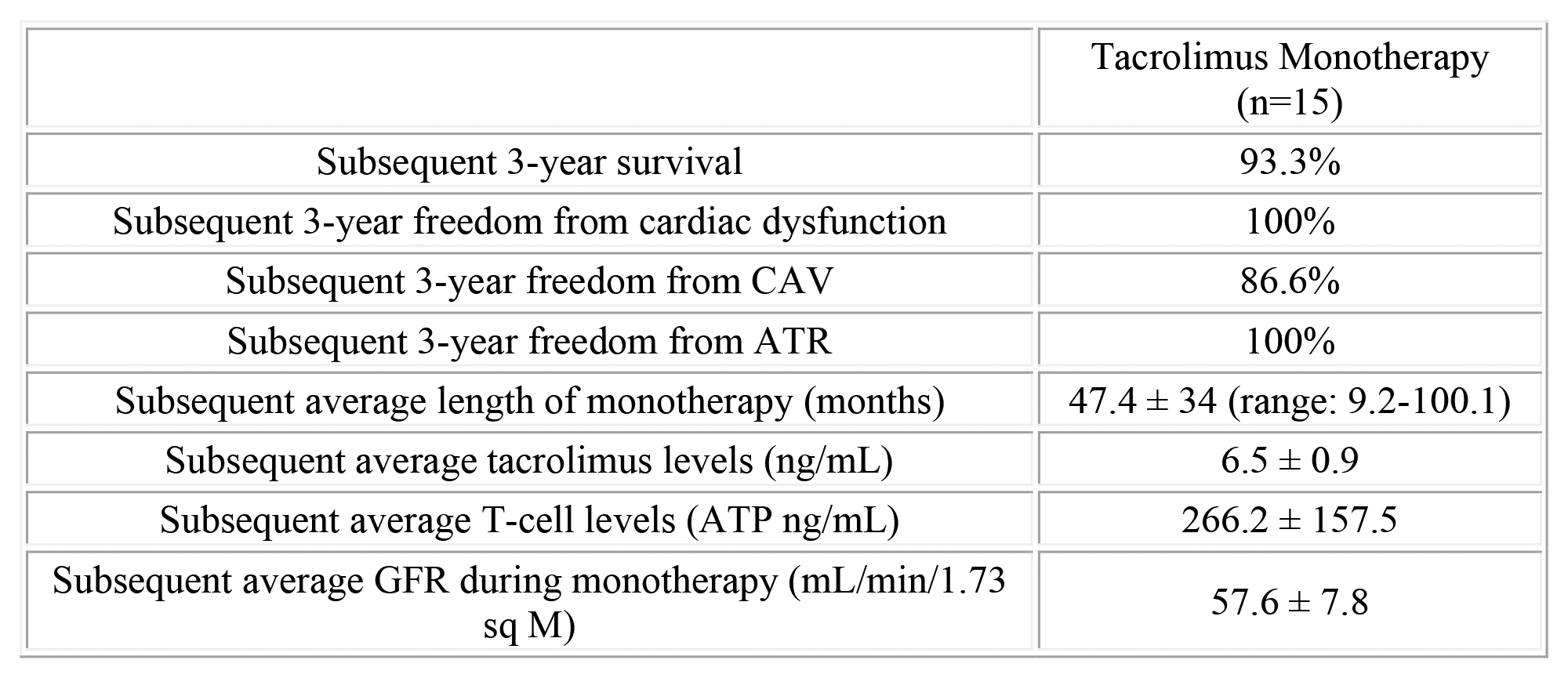
Methods Used: Between 2010 and 2021 we assessed 15 heart transplant patients who were maintained on TMI for at least 9 months. During this period of monotherapy, tacrolimus levels, along with TCIF were recorded. The tacrolimus level and TCIF results (≥2 tests) were averaged during this period of time. Subsequent 3-year (actuarial) survival, development of rejection, cardiac dysfunction, cardiac allograft vasculopathy, and renal dysfunction (GFR) were recorded.
Summary of Results: Of the patients on TMI, the average tacrolimus level was 6.5 ± 0.9ng/ml and the TCIF test was 266.2 ± 157.5 (therapeutic 200-550). There were no episodes of cardiac rejection within 3 years of starting monotherapy. Furthermore, cardiac function remained normal, and 86.6% had no development of cardiac allograft vasculopathy (CAV) and survival was 93.3% within 3 years of monotherapy. GFR remained in acceptable range. (see Table)
Conclusions: Tacrolimus monotherapy in heart transplant patients maintained at a therapeutic TCIF range appears to be safe and efficacious. With this lower level of tacrolimus, there does not appear to be risk for rejection and/or renal dysfunction.
Tacrolimus Monotherapy (n=15)
Subsequent 3-year survival
93.3%
Subsequent 3-year freedom from cardiac dysfunction
100%
Subsequent 3-year freedom from CAV
86.6%
Subsequent 3-year freedom from ATR
100%
Subsequent average length of monotherapy (months)
47.4 ± 34 (range: 9.2-100.1)
Subsequent average tacrolimus levels (ng/mL)
6.5 ± 0.9
Subsequent average T-cell levels (ATP ng/mL)
266.2 ± 157.5
Subsequent average GFR during monotherapy (mL/min/1.73 sq M)
57.6 ± 7.8
# 17
Does Crossing DSA and Its Binding Levels at the Time of Transplant Lead to Post-Op Complications?
Ivey B, Singer-Englar T, Kanungo A, Bhatnagar N, Hamilton M, Kobashigawa J. Cedars-Sinai Smidt Institute, Los Angeles, CA
Purpose of Study: Sensitization prior to heart transplantation (HTx) is seen in approximately 30% of transplant recipients. Sensitization may be caused by previous blood transfusion, multiparous pregnancies, and prior organ transplantation. As donor hearts are scarce, we find ourselves crossing donor specific antibodies (DSA) at the time of HTx. It has not been established whether crossing DSA and its strength (binding levels) at the time of HTx lead to more post-operative complications including antibody-mediated rejection (AMR) or graft dysfunction.
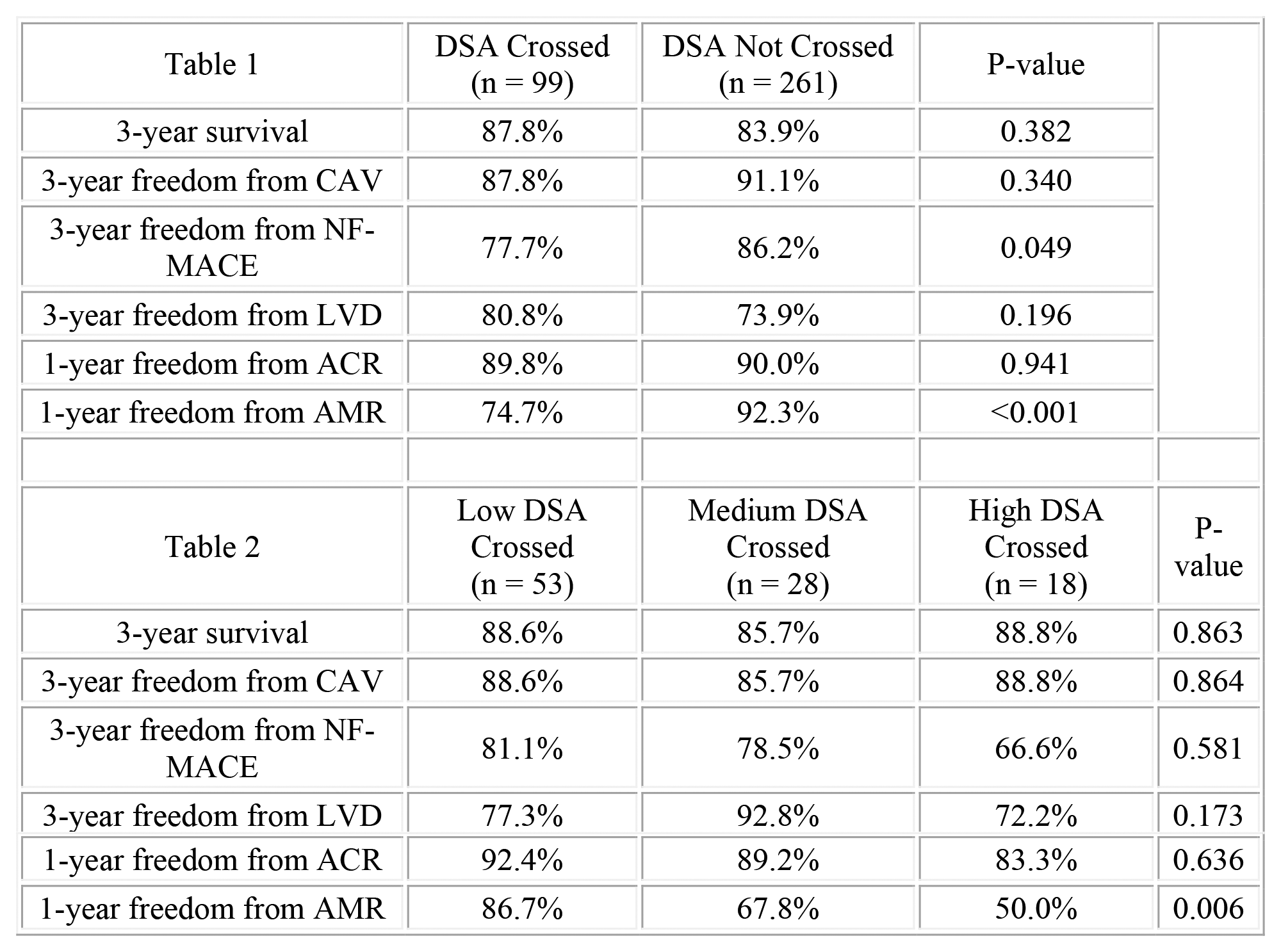
Methods Used: Between 2010 and 2020, we assessed 360 patients awaiting HTx who developed circulating antibodies. Patients were identified at the time of transplant if we crossed any DSA. Patients were then sub-grouped into those patients with low (<5K MFI), medium (5-10K MFI) and high (>10K MFI) binding levels of DSA in the undiluted specimen. A negative prospective crossmatch was mandated if crossing high DSA levels. All patients were given ATG followed by IVIG immediate post-op. When crossing high DSA levels, then eculizumab peri-op is added. Endpoints included 1-year acute cellular rejection (ACR) and AMR. 3-year outcomes included survival, freedom from cardiac allograft vasculopathy (CAV: ≥30% stenosis by angiography), freedom from non-fatal major adverse cardiac events (NF-MACE: myocardial infarction, new congestive heart failure, percutaneous coronary intervention, pacemaker/implantable cardioverter defibrillator placement, stroke), and freedom from cardiac dysfunction (left ventricular ejection fraction ≤40%).
Summary of Results: Crossing DSA of any binding strength resulted in significantly lower freedom from AMR and NF-MACE in the first year after HTx, however these antibodies did not cause graft dysfunction and survival was equivalent at 3 years. The high binding level (> 10K MFI) group compared to the lower DSA level groups had even lower freedom from 1-year AMR but 3-year outcome was similar.
Conclusions: Crossing DSA at the time of heart transplant can be done safely (with customized immunosuppression) but is it associated with an increased risk for first-year AMR. However, this did not impact 3-year survival or other outcomes.
Table 1
DSA Crossed
(n = 99)
DSA Not Crossed
(n = 261)
P-value
3-year survival
87.8%
83.9%
0.382
3-year freedom from CAV
87.8%
91.1%
0.340
3-year freedom from NF-MACE
77.7%
86.2%
0.049
3-year freedom from LVD
80.8%
73.9%
0.196
1-year freedom from ACR
89.8%
90.0%
0.941
1-year freedom from AMR
74.7%
92.3%
<0.001
Table 2
Low DSA Crossed
(n = 53)
Medium DSA Crossed
(n = 28)
High DSA Crossed
(n = 18)
P-value
3-year survival
88.6%
85.7%
88.8%
0.863
3-year freedom from CAV
88.6%
85.7%
88.8%
0.864
3-year freedom from NF-MACE
81.1%
78.5%
66.6%
0.581
3-year freedom from LVD
77.3%
92.8%
72.2%
0.173
1-year freedom from ACR
92.4%
89.2%
83.3%
0.636
1-year freedom from AMR
86.7%
67.8%
50.0%
0.006
# 18
Comparison of the Rate of Heart Transplant Rejection in Clinical Trials vs. Registries vs. Single Center: Which is More Reliable for Real World Experience?
Ng M, Singer-Englar T, Kanungo A, Bhatnagar N, Hamilton M, Kobashigawa J. Cedars-Sinai Smidt Institute, Los Angeles, CA
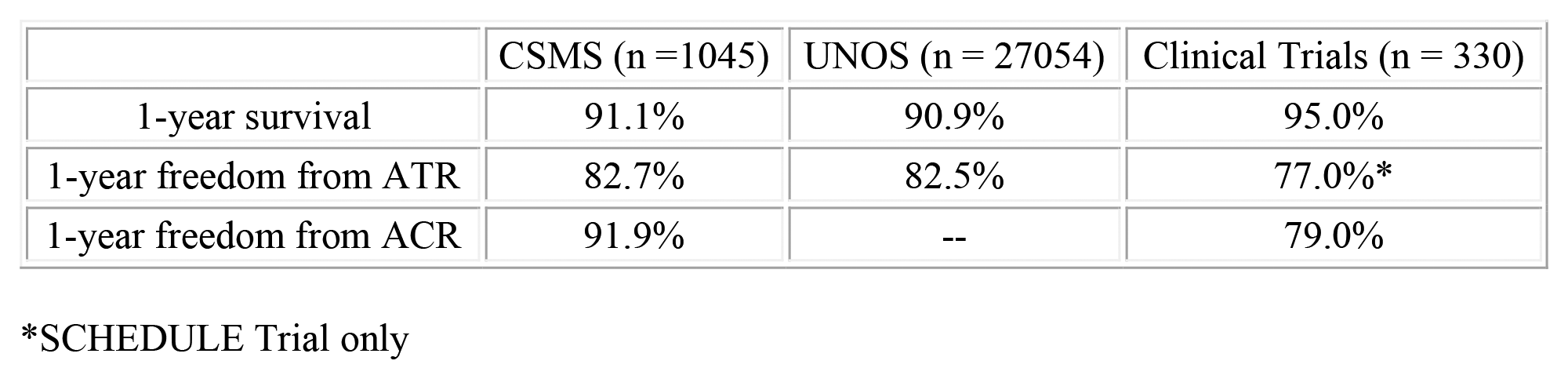
Purpose of Study: The incidence of rejection after heart transplantation (HTx) has been variable depending on what source is used (clinical trials, registries or single center reports). In general, rejection is defined as any-treated rejection (ATR) and sub-grouped into acute cellular rejection (ACR) in the first year after HTx. We assessed the incidence of 1 year rejection by reviewing randomized clinical trials (control arm), national registry (United Network for Organ Sharing (UNOS), and a large clinical transplant program (Cedars-Sinai) to demonstrate real world reliability of data.
Methods Used: We assessed clinical trial data, registry data (UNOS database 2014) and Cedars-Sinai data (2014) which were evaluated during the first-year post-transplant. Control arm data from two large heart transplant clinical trials are included which are the Everolimus vs Mycophenolate Trial (2013, n=271, DOI: 10.1111/ajt.12181) and the SCHEDULE Trial (2014, n = 59, https://doi.org/10.1111/ajt.12809). Rejection was determined as ATR and ACR.
Summary of Results: The registry and CSMC survival and freedom from ATR were similar. However, there was more first-year rejection in the clinical trials group compared to the registry and CSMC groups.
Conclusions: Registry and single center survival and rejection data appears most reliable for real world experience. Clinical trial data (control arm) appeared to have better 1-year survival which may be due in part to lower risk patients as those patients who were unstable at time of HTx were not included in the trials. The greater rejection rate in clinical trials may be due to a pathology core group over-reading the biopsies.
THE RELATIONSHIP BETWEEN SERUM ALKALINE PHOSPHATASE AND GROWTH VELOCITY IN CHILDREN WITH SHORT STATURE
Pedram Y1, Hernandez A1, Ryabets-Lienhard A2, 1, Bakhtiani P2, 1. 1Keck School of Medicine, Los Angeles, CA and 2Children’s Hospital of Los Angeles, Los Angeles, CA
Purpose of Study: Growth velocity (GV) is one of the key components that determines decision to start recombinant growth hormone (rhGH) therapy in a child with short stature. Serum ALP activity is higher during periods of rapid growth in childhood and adolescence as compared to adults.1 Bone-specific ALP activity rises after growth hormone replacement in children with Growth Hormone Deficiency (GHD). This increase is believed to be associated with increased bone turnover. The purpose of the study is to identify if ALP has the potential to be an adjunct surrogate marker for growth velocity when evaluating candidates for rhGH therapy.
Methods Used: We conducted a retrospective chart review of prepubertal children aged 2 years and above [N= 66] with significant short stature (height less than -2SD for age) and a diagnosis of GHD [N= 34, 17 females, 14 Latinx, mean age 9.4+/-3.8 years] or ISS [N= 32, 11 females, 13 Latinx, mean age 6.9+/-3 years] who had a baseline ALP activity drawn at the Childrens Hospital Los Angeles laboratory. Children with chronic medical problems, Vitamin D deficiency, fractures or liver disease were excluded. ALP standard deviation scores (ALP SDS) and growth velocity standard deviation scores (GV SDS) were calculated for patients’ bone age. Correlation analysis was used to identify a relationship between ALP SDS and GV SDS, and paired t-test to assess change in ALP activity before and after treatment with rhGH.
Summary of Results: Our pilot data showed mean ALP activity of 175.7U/L (SD 54.3) in patients with GHD and 178.9U/L (SD 49) in patients with ISS. We found a significant correlation between baseline ALP SDS and GV SDS (r=0.5, p=0.018) in patients with GHD, but not in patients with ISS (r=-0.17, p=0.38).
We found improvement in ALP activity in response to treatment with rhGH treatment in patients with GHD (N=13, p=0.014, two-tailed) and ISS (N=11, p=0.04, two-tailed). The mean ALP increased from 179.4U/L (SD 50.3) at presentation to 240U/L (SD 62.2) measured within a year of starting rhGH therapy in our study population.
Conclusions: In children with GHD, baseline activity of ALP has potential to be an adjunct indicator of growth velocity.
The improvement in ALP upon treatment with recombinant human growth hormone also points towards a direct effect of growth hormone on serum ALP levels. Analysis of a larger subject pool is underway to establish validity and determine clinical utility of this possible correlation.
# 20
CASE SERIES OF IATROGENIC CUSHING’S SYNDROME DUE TO OVER-THE-COUNTER SUPPLEMENT
Sharma R1, 2, Aranguri C1, TRANG NC1, 2, Khamlong M1, Clarke M1, 2, Singh S1, 2, Chandramahanti S1, 2. 1Kern Medical Center, Bakersfield, CA and 2David Geffen School of Medicine, Bakersfield, CA
Purpose of Study: Cushing’s syndrome (CS) is a complex disorder marked by the excessive production of cortisol, a hormone vital for regulating various bodily functions. It can result from inappropriate production of either CRH, ACTH or cortisol. This condition can also manifest from prolonged exposure to corticosteroid medications, leading to iatrogenic Cushing’s syndrome. Accurate diagnosis and appropriate management are crucial to mitigate the overall health impact of this syndrome. A growing number of cases of iatrogenic CS secondary to adulterated supplements are being reported. Herein we describe five cases of patients developing iatrogenic Cushing’s syndrome due to accidental ingestion of glucocorticoids while taking over the counter medication, “Artri King”.
Methods Used: A retrospective chart review of five patients who took the herbal supplement “Artri King” and presented to Kern Medical were reviewed. All patients who were found to take over the counter herbal supplement “Artri King” were included in this study.
Summary of Results: Case 1: A 44-year-old woman with multiple nonhealing bilateral lower extremity ulcers up to 6 cm referred for uncontrolled diabetes who presented with Cushingoid appearance.
Case 2: 47-year-old well appearing male with a morning cortisol level of 1.7 mcg/dL obtained as part of a weight loss consult.
Case 3: A 70-year-old woman with random cortisol 0.8 mcg/dL as ordered for workup of resistant hypertension.
Case 4: A 68-year-old female with history of morbid obesity found to have an AM cortisol of less than 0.5 mcg/dL (Ref. range 4.32 to 22.4) with a ACTH less than 5 pg/mL (Ref. range 6 to 50)
Case 5: 43-year-old male with acute respiratory failure requiring intubation, once extubated experienced post intubation complications and found to have adrenal insufficiency.
Conclusions: These cases show the wide range of presentation of patients who may be taking exogenous glucocorticoids. In all cases the patients were unaware of the deleterious effects of the “Artri King” supplement and, as such, did not initially disclose the use of the supplement since it is marketed as anti-inflammatory supplement. For patients using these supplements chronically a steroid taper was warranted to avoid adrenal insufficiency from abrupt discontinuation. In conclusion, these cases reinforce the value of a detailed medication reconciliation including over-the-counter, complementary and alternative medications at a patient’s presentation. In any case of iatrogenic Cushing’s syndrome, a safe steroid taper and discontinuation of supplemental health products including herbal supplements is essential, as many may include hidden ingredients including undeclared glucocorticoids. Healthcare practitioners should be aware of the growing use of “Artri King” and seek resources to safely wean patients from these agents.
# 21
COMPARATIVE ANALYSIS OF FETAL FERRET PANCREAS DEVELOPMENT
Branscomb R1, Engelhardt J2, Sussel L1, 3. 1University of Colorado, Aurora, CO; 2University of Iowa, Iowa City, IA and 3Barbara Davis Center for Childhood Diabetes, Aurora, CO
Purpose of Study: Cystic fibrosis (CF) is a progressive, multisystemic disease that affects more than 30,000 individuals in the US. Cystic fibrosis-related diabetes (CFRD) is the most significant co-morbidity, impacting >50% of adult patients. Studies in young children with CF indicate that defects in islet function is an early clinical feature of CF, but the cause of this dysfunction remains controversial. To begin to understand the potential origins of CFRD, it would be optimal to model CFRD in an animal model; however, CFRD is not well-modeled in mice. Alternatively, CFRD occurs spontaneously in the ferret model of CF, suggesting this would be a useful model to characterize whether there is a developmental origin of pancreas dysfunction in CF patients. Because the development of the fetal ferret pancreas has not yet been characterized, the purpose of this project is twofold: 1) to characterize wild type ferret pancreas development as a baseline for comparison with a CF ferret model, and 2) determine whether pancreatic developmental defects contribute to CFRD in adults.
Methods Used: Fetal ferret pancreatic tissues were collected at time points throughout gestation (embryonic days 21, 22, 23, 33, and 38) and then embedded in OCT and sectioned. Immunohistochemistry was employed to identify key markers of development including insulin, glucagon, pdx1, nkx6.1, and nkx2.2.
Summary of Results: In humans, islet-like structures appear at approximately week 12 of gestation and are primarily formed by the aggregation of insulin- and glucagon-producing cells with the adult islet containing intermixed insulin and glucagon expression. In the mouse model, pancreatic development takes on a distinctly different conformation in which glucagon-producing cells surround a mass of insulin-producing cells by adulthood. In the ferret, insulin- and glucagon-producing cells were noted to begin aggregating around day 33 of gestation, with a more similar conformation to that of the human than the mouse.
Conclusions: In this study we demonstrate that the ferret, mouse, and human pancreas appear similar in early development, but as development progresses, ferret pancreatic islet formation appears more similar to humans. Future studies will use similar analyses to determine whether CF ferrets display altered pancreatic islet development. Additionally, ongoing studies are employing RNA-seq to quantitatively define key endocrine markers and transcription factors spatially and temporally.
# 22
Inflammatory exposure to the adult mouse pancreas and isolated islets results in NFκB activation and changes in targeted gene expression
White A, Solar M, Rozance P, Wright CJ. University of Colorado, Aurora, CO
Purpose of Study: Islet failure in both type 1 and type 2 diabetes involves an inflammatory insult to the pancreas. One mediator of inflammation in the islet that impacts gene transcription is NFκB. We therefore hypothesized that inflammatory exposure to the adult mouse pancreas and isolated islets would activate NFκB resulting in changes in targeted gene expression that favor sustained inflammation and apoptosis.
Methods Used: Adult B6 (C57BL/6) mice (n=8/timepoint) or pooled isolated islets from 8-10 mice (n=6 sets) were exposed to lipopolysaccharide (LPS; 5 mg/kg IP) or a cytokine mixture (IFNγ 1ng/μL, TNFα 0.1 ng/μL, and IL1β 0.01 ng/μL), respectively. Male and female mice were used in equal numbers with data combined for analysis. NFκB activation was determined by phosphorylation and nuclear translocation of the NFκB proteins, p50 and p65, expression and localization of the NFκB inhibitors, IκBα and IκBβ, and the expression of NFκB target genes, Cxcl10, Tnf, Nos2, and Nfkbia, and the pro-apoptotic gene, Bax, at various timepoints. Student’s t-test was used to compare differences between groups.
Summary of Results: In the whole pancreas, there was no significant difference in cytosolic IκBα or IκBβ after LPS exposure as compared to control. However, there were increases in nuclear p50 (P=0.0147) and p65 (P=0.0018) measured 1 hr after LPS exposure. The increased nuclear p50 persisted 5 hr after LPS exposure (P=0.0107), whereas nuclear p65 returned to levels similar to control. In isolated islets, the phosphorylated p65 to total p65 ratio significantly increased 15 min after cytokine exposure (P=0.0003) then returned to values similar to control by 30 min. Gene expression for known NFκB target genes, Cxcl10 and Tnf, increased by 30 min after cytokine exposure and remained elevated at 5hr after exposure (P<0.01). Nfkbia, the gene for the NFκB inhibitor IκBα and a known NFκB target gene, also increased by 30 min (P=0.0003) after cytokine exposure and remained elevated at 5 hr (P<0.0001) after exposure. Gene expression for Nos2 and Bax increased 5 hr after cytokine exposure (P<0.01).
Conclusions: Inflammatory exposure to the adult mouse pancreas and isolated islets results in pancreatic NFκB activation with persistent elevation of target genes regulating inflammation and apoptosis. We speculate that these transcriptional changes yielding a sustained pro-inflammatory cytokine profile regulated by NFκB result in β-cell dysfunction and cell death thereby increasing the risk of both type 1 and type 2 diabetes. Therefore, targeting β-cell-specific NFκB signaling may be a strategy to prevent or slow the progression of diabetes.
# 23
HOW MUCH DO THEY TRULY UNDERSTAND? ASSESSING HEALTH LITERACY, NUMERACY, AND LEARNING STYLES IN A PEDIATRIC DIABETES CLINIC
Nguyen N1,2, Sathi S3,2, Kinman R4. 1El Capitan High School, Merced, CA; 2UCSF Fresno, Fresno, CA; 3Clovis North High School, Fresno, CA and 4UCSF Fresno, Fresno, CA
Purpose of Study: Effective self-management of Type 1 diabetes necessitates comprehensive education tailored to individual needs. However, low health literacy affects 88% of adults in the United States while numeracy skills are also subpar with only 9% of those aged 16-65 considered proficient in math. Diabetes education typically follows a one-size-fits-all approach, which may not suit diverse learning styles. We aimed to evaluate the health literacy and numeracy skills of Type 1 diabetes patients ≥ 14 years of age and/or diabetes caregivers while identifying their preferred learning styles to tailor education accordingly.
Methods Used: We utilized the "Newest Vital Sign" quiz to assess health literacy and modified the Diabetes Numeracy Test to align with current pediatric/young adult Type 1 diabetes practice. A learning styles survey was administered to determine preferred learning methods. Participants were questioned about their ability to comprehend written health information, understand verbal instructions, and fill out medical forms.
Summary of Results: Among the 48 adult patients (ages ≥18) and caregivers surveyed, educational backgrounds varied: 8% had not completed high school, 1/3 held a high school diploma or GED, 25% had some college education, 6% had an associate’s or technical degree, 17% had a bachelor’s degree, and 10% held master’s degrees. All respondents ages 14 and above reported varying needs for help with health-related reading and understanding of diabetes education with responses ranging from "always" to "never." When learning something new, most respondents felt that they learned best by listening to someone explain or teach the material followed by looking at pictures or diagrams. Health literacy and numeracy quizzes were administered to 20 patients (ages ≥14; average score 4 out of 6, range 0-6) and 12 adult caregivers (average score 5 out of 6, range 0-6). Scores of 0-2 indicate high likelihood of low literacy while scores of 4-6 suggest adequate health literacy. Most struggled more with numeracy than literacy with many scoring 5 or less out of a total of 8 assessed numeracy questions.
Conclusions: Effective diabetes self-management hinges on comprehensive education. Although education is provided individually, it often follows a uniform format. Our findings advocate for a multi-modal, personalized approach to diabetes education that aligns with individual learning styles. For Type 1 diabetes management, health literacy and numeracy skills are essential, even in those using "smart pumps" with continuous glucose monitoring systems. Inadequate literacy and numeracy skills may underlie poor glycemic control, emphasizing the importance of addressing these foundational skills. Rather than labeling patients as "non-compliant," it is vital to recognize the impact of health literacy and numeracy on diabetes management. Customized education strategies could be one key to improving patient outcomes and long-term diabetes complications.
# 24
Case Series of thyrotoxicosis: unique presentations and challenges of Thyroid Storm Management
Inga Jaco E, Clarke M, Chandramahanti S, Singh S, Garcia-Pacheco R, Joolhar F, Sukkar M, Kulasingam R. Kern Medical, Bakersfield, CA
Case Report: Hyperthyroidism is defined as inappropriately high production and release of thyroid hormones. The development of symptoms is called thyrotoxicosis while thyroid storm (thyroid crisis) is the acute and life-threatening state of exacerbated hyperthyroidism. The presentation of thyrotoxicosis and thyroid storm is wide and the resultant complications are unpredictable. The mortality of thyroid storm is estimated at 8 to 25% despite early recognition and appropriate treatment. In this three-patient case series, presentations such as cardiogenic shock during thyroid storm, as well as stroke and cardiac arrest as a result of thyroid storm are discussed.
A 37 year old Hispanic male with no known medical history presented to the hospital with shortness of breath and abdominal pain. During acute presentation, patient was found to be in thyroid storm manifested by thyroid stimulating hormone (TSH) < 0.008 mlU/mL (normal 0.554 - 4.780 mlU/mL ), free thyroxine (T4) > 7.6 ng/dL (normal 0.9-1.8 ng/dL ) and a Burch-Wartofsky point scale (BWPS) of 100. Incidentally, left ventricular ejection fraction was found to be < 10% making treatment for heart failure and thyroid storm antagonistic to one another. Patient was placed on mechanical ventilation for acute respiratory failure secondary to acute cardiogenic shock exacerbated by thyroid storm.
A 31 year old Korean male with no known medical history presented with hoarseness, neck mass, and left sided hemiplegia. CT brain without contrast showed right middle cerebral occlusion. Patient underwent thrombectomy which was complicated by post thrombectomy bleeding and development of new right anterior cerebral thrombosis. Thyroid function testing during admission showed TSH <0.008 mlU/mL and free T4 8.5 ng/dL and a BWPS of 75. Coagulopathy was likely a result of thyroid storm. The hypercoagulable state resulted in repeated ischemic strokes, making treatment challenging for both medicine and neurosurgery.
A 19 year old female with recent diagnosis of Grave’s disease who developed cardiac arrest and achieved ROSC. Presented to the hospital with tachycardia, agranulocytosis and acute respiratory infection. Thyroid storm was suspected by BWS score of 75 and TSH level of < 0.017 mlU/mL and free T4 of 4 ng/dL. Given that patient presented with agranulocytosis on thyroid storm, traditional therapy for Grave’s disease were held and Lithium was used.
Thyroid storm is a medical emergency with multisystem involvement that carries a high mortality rate. It is important to consider diagnosis of severe thyrotoxicosis in the young population as atypical presentations such as cardiogenic shock, stroke, and even cardiac arrest are possible with no prior history of hyperthyroidism. In this case series, we discuss cardiovascular complications of thyroid storm and treatment challenges in atypical cases.
# 25
Factors Associated with Osteoporosis, Fragility Fractures, and Osteopenia: A Population-Level Analysis utilizing the United Kingdom Biobank
O’Neill CK1, Duckworth E2, Shah R2, Jayakumar P2, Truumees E2. 1University of Washington, Seattle, WA and 2University of Texas at Austin, Austin, TX
Purpose of Study: Osteopenia, osteoporosis, and fragility fractures pose a major public health concern. Population-level clinical and biopsychosocial data may uncover modifiable risk factors. We aimed to identify demographic, clinical, mental, social, behavioral, and lifestyle factors associated with osteoporosis from the United Kingdom Biobank (UKB) – a population-level database. Secondarily, we aimed to identify factors associated with a diagnosis of fragility fracture and osteopenia.
Methods Used: We performed a cross sectional study on UKB patients evaluating the association of 39 explanatory variables with osteopenia, osteoporosis, and fragility fracture. Bivariate analysis was performed followed by multivariable logistic regression adjusting for multicollinearity using covariance testing.
Summary of Results: Of 502,507 patients in the UKB study, 40,657 had complete bone mineral density information from DEXA scans, and 32,193 had sustained a fragility fracture in the previous five years. In multivariable regression, increased time spent on TV (OR 1.15) and living in an area with a high index of deprivation (OR 1.14) were associated with increased risk of osteoporosis. Decreased exercise frequency (OR 1.27), living in an area with a high index of deprivation (OR 1.11), and decreased salary (OR 1.10) were associated with increased risk of fragility fracture. Symptoms of anxiety (OR 1.15) and living in an area with a high index of deprivation (OR 1.13) were associated with increased risk of osteopenia. (all p<0.05).
Conclusions: Population-level analysis revealed modifiable behavioral and social health risk factors associated with increased risk of osteoporosis, fragility fracture, and osteopenia.
# 26
NEURODEVELOPMENTAL OUTCOME OF TERM AND NEAR-TERM INFANTS WITH SEVERE HYPOGLYCEMIA
Bai-Tong SS1, 2, Golembeski D1, 2. 1Rady Children’s Hospital, San Diego, CA and 2University of California, San Diego, San Diego, CA
Purpose of Study: Hypoglycemia in term or near-term newborns is a frequent transitional complication in nursery. The implications of hypoglycemia on neurodevelopmental outcomes in this patient population remain unclear. At Rady Children’s Hospital San Diego (RCHSD) Neonatal Intensive Care Units (NICUs), infants who were admitted from the well-baby nursery with severe hypoglycemia were referred to the Neurodevelopmental Clinic at discharge for follow up. We aimed to evaluate the developmental outcomes of these otherwise healthy term and near-term infants.
Methods Used: In this retrospective chart review, medical records of hypoglycemic infants admitted to RCHSD NICUs from nursery or delivery room between February 2008 and April 2019 were reviewed. Infants were included if born at ≥ 35-week gestational age, had blood glucose level < 20 mg/dL or < 30 mg/dL twice, and had at least one Neurodevelopmental Clinic visit. Exclusions included major congenital abnormalities, neurologic complications (e.g. hypoxic ischemic encephalopathy or meningitis), critical illness requiring intubation or inhaled nitric oxide, or any other complication that may impact developmental outcomes.
Summary of Results: Seventy-three infants were included in the study. Patients’ demographics, prenatal/birth history, NICU courses, and Neurodevelopmental Clinic notes were reviewed. Average gestational age was 37 3/7 weeks. Average lowest glucose during admission was 16.1 mg/dL (median 18, range 0 – 29). Seventy infants completed the Bayley-III Screening Test. Among them, infants deemed not competent included 14 (19.2%) in cognition, 18 (24.7%) in receptive language, 26 (35.6%) in expressive language, 20 (27.4%) in fine motor and 22 (30.1%) in gross motor. Average age at first follow-up visit was 8 months (median 7, range 4 – 17). Eighteen infants had a second follow up at average 16 months (median 15, range 11 – 23) and completed Bayley-III Scales with average cognitive composite score 101 (median 100, range 85 – 110), average language composite score 88 (median 89, range 74 – 100) and average motor composite score 96 (median 95.5, range 76 – 121). Twelve infants had a third follow-up at average age 26 months (median 25, range 24 – 33). Average cognitive composite score was 90 (median 92.5, range 75 – 105), average language composite score was 89 (median 94, range 56 – 112) and average motor composite score was 99 (median 103, range 76 – 110).
Conclusions: In this study, although up to one third of infants were not competent in one area of development on Bayley Screening Test during initial follow-up visit, subsequent Bayley Scales from these infants did not show significant impairment with average composite score > 85 in all categories. However, given the limitations of Bayley Scales in predicting long term neurodevelopmental outcomes, small sample size and high attrition after initial clinic visit, further studies are needed to better delineate the impact of transient severe hypoglycemia on neurodevelopmental outcomes in this group of infants.
# 27
DIABETES SUPPORT GROUPS IN RURAL SETTINGS
Crowley B1, Keys T2. 1University of Washington School of Medicine, Seattle, WA and 2University of Washington School of Medicine, Seattle, WA
Purpose of Study: Lewistown, the county seat of Fergus County in Montana, has a population of Type 2 diabetics similar to the national average for rural prevalence. Rural citizens have a 16% higher prevalence of Type 2 diabetes mellitus (T2DM) and 20% higher T2DM related mortality compared to urban populations. Studies have shown that telehealth and in-person group interventions improved outcomes such as decreased HbA1c in adults with T2DM in rural areas. Implementation of diabetes support groups will act as a care resource for T2DM management and prevention in Fergus County.
Methods Used: The Community Health Needs Assessment (CHNA) performed by the local hospital showed a strong need for increased health and wellness opportunities. Conversations ensued with providers and the local dietician of Fergus County. Diabetes management was recognized as an ongoing challenge facing their patients. With the help, guidance, and project partnership of the local dietician, it was decided to reinstate the diabetic support group that was cancelled during the COVID-19 pandemic. This group initial meeting was advertised on KXLO, the local radio. The group is designed to create a sense of community, support, and accountability for locals with diabetes.
Summary of Results: A twenty-minute presentation was given to the newly formed diabetic support group discussing the importance of diabetes management and approaches to general wellness. The goal was to discuss management strategies in the local community that follow national guidelines. This presentation was in an open format, allowing group members to actively interject with any questions that they had. Although the group turnout was three members, the presentation was positively received. This group will continue to meet monthly while both the members and the dietician leading the group will work to increase attendance through conversations and advertisements.
Conclusions: The next step for this project is to actively discover ways to increase attendance of the monthly support group in order to create a larger sense of community. A limitation that the success of this group faces is the great distances that residents of farming communities like Fergus County must travel to attend meetings in town.
Healthcare Delivery Research I - Community Health Projects
Concurrent Session
12:45 PM
Thursday, January 18, 2024
# 28
BARRIERS AND FACILITATORS TO THE UPTAKE OF POST-VIOLENCE CARE SERVICES AND ORAL HIV TESTING AMONG YOUNG WOMEN ENROLLED IN PAMOJA COMMUNITY BASED ORGANIZATION, SEME SUB COUNTY, KENYA
Mourad N1, Gangji A1, Lai S1, Song J1, Mbullo P2, 3, Kapoor V1. 1University of British Columbia, Vancouver, BC, Canada; 2Wayne State University, Detroit, MI and 3Pamoja Community Based Organization, Kisumu West, , Kenya
Purpose of Study: Gender-based violence is prevalent in Kenya, with the 2022 Demographic and Health Survey revealing high rates of physical (34%) and sexual (13%) violence among women. Pamoja Community-Based Organization (CBO), a Kenyan grassroots organization, is dedicated to HIV prevention interventions in Kisumu County. Their DREAMS Initiative (Determined, Resilient, Empowered, AIDS-free, Mentored, and Safe) has equipped over 13,000 adolescent girls and young women (AGYW) with social skills to combat the high HIV vulnerability and advanced utilization of essential health services, among 15-24-year-olds in Kisumu County. Despite Pamoja’s comprehensive interventions, AGYW’s utilization of post-violence care remains low.
This mixed-methods study explores barriers and facilitators to post-violence care service uptake and oral HIV testing among DREAMS program participants. It employs in-depth interviews and focus group discussions (FGDs) to understand AGYW’s reproductive health experiences and inform service improvements.
Methods Used: Three FGDs (n=31) were conducted with women aged 18-38 (mean = 22.4) who were enrolled in the DREAMS program at Pamoja CBO. Additionally, two-parent FGDs (n=10) were held with both male and female caregivers of the participants. Finally, in-depth (n=5) and key informants (n=5) interviews were conducted with caregivers and healthcare providers respectively. Discussion guides were developed with questions regarding knowledge, attitudes, and availability of post-violence care, including HIV testing and contraceptive use. The interviews were conducted by two research assistants and were digitally recorded, transcribed, and translated into English where applicable. Using NVivo software, researchers sorted and coded key themes for analysis.
Summary of Results: Major facilitators to seeking post-violence care include the availability of safe spaces (girls-only meeting venues), teachers and mentors, and access to various services including police, legal, and counselling. Conversely, major barriers include stigma, access to services, concerns around confidentiality, and persistent myths in the community. The uptake of oral HIV testing was facilitated by a strong background knowledge about HIV and parents noted that knowing their HIV status was important to receive timely care. However, free rapid testing kits at clinics are not always in stock, so young people need to purchase them from local shops instead. Moreover, some users feel they provide inaccurate results because the tests require some skill to use correctly.
Conclusions: This study identified major facilitators and barriers to the uptake and use of post-violence care and rapid HIV testing in this community. To increase the use of post-violence care, the program should look to address concerns around access, privacy and confidentiality, and general perceptions of these services to remove cultural and religious stigma. Better access and education regarding the use of rapid oral HIV testing kits would also help to increase their use.
# 29
INCREASING HEALTHY HABIT AWARENESS IN GALENA, ALASKA
Chapman C1, Keys T2. 1University of Washington School of Medicine, Seattle, WA and 2University of Washington, Seattle, WA
Purpose of Study: Galena (population 462) is a remote Alaskan village located along the Yukon River, only accessible by air or water. Compared to Alaska at large, residents of Galena are more likely to experience poor health outcomes, including decreased length and quality of life; this is in part due to limited access to resources and a decrease in the availability of the subsistence foods that this population has long relied on. To address these health disparities, community organizers developed a 3-day health fair that promotes healthy habits. This event intertwines community engagement and health education. Developing further didactic materials to integrate into this event will aid in increasing awareness and promotion of sustainable healthy living habits within this community.
Methods Used: Research through the Census, VizHub, and Robert Wood Johnson County Health Rankings was conducted to assess demographics, epidemiology, and community assets in Galena. To understand resident and leader priorities of prevalent health issues, community conversations were initiated. Key areas identified were: substance use, physical activity, healthy eating, injury prevention, and mental health education. To determine effective strategies of health promotion in rural settings, a literature review was conducted. Research indicated that simple, focused lessons with interactive activities lead to enhanced understanding and retention of knowledge and community collaboration is crucial. A partnership was established with Tanana Chiefs Conference Wellness and Prevention Coordinator at Edgar Nollner Health Center to distinguish gaps in educational health content for existing activities; modified educational materials were then developed for the 2nd Annual Mind, Body, & Soul Event (2023).
Summary of Results: Organizers connected with around 50 community members through the 2nd Annual Mind, Body, & Soul Event (2023) in Galena, AK. The event included interactive activities highlighting bicycle helmet utilization, proper life jacket use, and identifying self-care activities. A scavenger hunt and a safety presentation were also created to emphasize the various health topics. Participant engagement was greatest in the scavenger hunt and triathlon. Individuals reported that involvement in these workshops was helpful, informative, and enjoyable. It is a goal that continued participation in and development of these events will allow for greater community awareness of safe recreation practices and provide a baseline for sustainable healthy living.
Conclusions: Early interpretation of health education delivery via community events in Galena, AK indicate that it is likely an effective method to increase awareness of healthy living habits. The success of this scholarship was based upon the ability to collaborate with community partners and use community input to guide this intervention. Moving forward, a study utilizing incident reports and reported participant learning could increase understanding of the effectiveness of this intervention.
# 30
Qualitative Study of QuitNow (Smoking Cessation Website) User Experiences
Salaheddin T1, Struik L2. 1University of British Columbia, Vancouver, BC, Canada and 2University of British Columbia, Kelowna, BC, Canada
Purpose of Study: Attempting to quit smoking is a challenging endeavor. On average, it takes 30 attempts for an individual to quit smoking for 1 year or more. Studies have demonstrated that the combination of behavioral support and pharmacotherapy is more effective than either approach in isolation. British Columbia residents have access to a service called QuitNow that provides information and support to smokers. Our qualitative study seeks to delve into users’ utilization and experiences of QuitNow, aiming to inform strategies for enhancing its impact, and share insights gained with other online cessation programs to address user needs effectively.
Methods Used: We interviewed 80 participants, of which 10 were frequent QuitNow users. These 10 interviews were transcribed, and inductive thematic analysis was performed using NVivo software to extract common themes about user experiences.
Summary of Results: Thematic analysis yielded five major themes. The first theme was that minimizing barriers to information promoted action in relation to quitting. This involved using infographics to replace lengthy text and allowing users to interact with the website anonymously to protect their privacy. The second theme related to a lack of clarity around accessing Nicotine Replacement Therapy (NRT), suggesting a need for improved messaging. For the third theme, users expressed a desire for connection with fellow smokers, personal networks, and professionals, highlighting opportunities for the website to facilitate such connections. The fourth theme related to incentives to quit. We found that participants would appreciate rewards as incentives, but that these do not have to be monetary. Finally, for theme five, participants recognized the role of personal agency in the quitting process, with websites providing support.
Conclusions: Given increases in digital literacy, websites must innovate content delivery to meet user expectations effectively. Collaboration between government, website developers, and pharmacies is essential for improving the delivery of free NRT to the community. Recognizing that online cessation websites cannot tackle this challenge in isolation, multi-sector engagement is key to enhance systemic approaches to addressing nicotine addiction, such as partnering with gyms to provide discounted memberships as quitting incentives.
# 31
IMPROVED DIABETES & CARDIOVASCULAR EDUCATION OUTCOMES AMONG COMMUNITY HEALTH PROMOTERS IN MAI MAHIU, KENYA
Pham CB1, Bosibori D3, 2. 1University of Washington School of Medicine, Seattle, WA; 2University of Washington School of Pharmacy, Seattle, WA and 3Naivasha Country Referral Hospital, Naivasha, Kenya
Purpose of Study: In Kenya, the prevalence of non-communicable diseases (NCDs), notably diabetes, has surged due to urbanization and unhealthy lifestyles, contributing to cardiovascular disease (CVD) burden. Prioritized resource allocation for infectious diseases has left Kenya’s strained healthcare system inadequately equipped to manage the diabetes epidemic. In low-resource settings, community health promoters (CHPs) play an essential role in community education and disease management. However, there is limited training among CHPs on uncontrolled diabetes and its comorbidity with CVD. This study aims to implement an educational program for CHPs in Mai Mahiu, improving their knowledge about uncontrolled diabetes, management, and its relation to CVD risk. We hypothesize that implementing this targeted educational intervention will lead to a statistically significant increase in knowledge scores among CHPs.
Methods Used: This community-based project employed a quasi-experimental design including registered CHPs in Mai Mahiu. Participants completed a pre-test and post-test survey based on the study objectives, with an educational intervention conducted in between. Responses were recorded using a Likert scale and converted into numerical values (1-5) that represented knowledge scores for assessment of post-intervention outcomes.
Summary of Results: A total of twenty-five CHPs participated. After a diabetes and CVD educational program, post-test scores (M = 4.77) significantly increased from pre-test scores (M = 3.29), indicating statistically significant improved knowledge (paired t-test: t = -15.81, df = 6, p = 4.06 E-06). Qualitative feedback included increased confidence in CHPs’ ability to educate, detect, and manage diabetes and CVD. Educational brochures were distributed to CHPs to aid local health campaigns.
Conclusions: This project increased awareness and knowledge of uncontrolled diabetes and comorbid CVD risk among CHPs in Mai Mahiu, demonstrating the effectiveness of targeted education. It also established a foundation for future training sessions, enhancing CHPs’ role in diabetes care and the prevalence reduction of CVD complications. Further training and increased funding from the Government of Kenya are essential to sustain CHPs’ community outreach efforts. Future steps would involve expanding the project’s sample size and studying specific knowledge gaps among CHPs to provide individualized training. Empowering the community through education remains valuable for decreasing the prevalence of uncontrolled diabetes, reducing CVD risk, and improving overall quality of life.
# 32
ASSESSING ABORTION CARE BARRIERS—DESIGNING SUPPORT FOR INTEGRATION OF SERVICES INTO THE PRIMARY CARE SETTING
Fine KE2, Zhang Y1, Fiastro A1, Shih G1, Aldrich D1, Godfrey E1, Bennett I1. 1University of Washington, Seattle, WA and 2University of Washington, Spokane, WA
Purpose of Study: Access to abortion care across the Washington, Wyoming, Alaska, Montana, and Idaho (WWAMI) region is more critical now than ever following the Dobbs v. Jackson Women’s Health Organization U.S. Supreme Court decision eliminating federal protection for abortion access. Our goal was to convene clinic champions across WWAMI who were interested in developing a regional learning collaborative for first trimester abortion services and understand barriers to help formulate strategies for future support.
Methods Used: Clinic champions interested in enhancing abortion care at their site were identified from a prior needs assessment survey shared with WWAMI Family Medicine Residency Network Program Directors (n=45), WWAMI Practice Based Research Network (WPRN) clinic champions (n=95), and Title X Washington clinics (n=16) from Dec. 2022-Feb. 2023. Following the survey, all interested providers were invited to attend a convening via Zoom to understand barriers and determine future steps for support. A semi-structured interview guide was used to conduct interviews and field notes were generated by two team members. Questions asked included: what is the current status of incorporating abortion services into your practice, what barriers are you facing and what support would be most helpful? A transcript of each convening was recorded with participant consent to support field notes. Debriefs took place after each meeting, field notes were compiled and results were discussed with the team to rule out individual bias and confirm overall themes to enhance creation of an abortion learning collaborative.
Summary of Results: Fifteen individuals were identified as clinic champions, with six clinicians participating in four online convenings. Most of the clinicians were from Washington (n=5), with one clinician from Idaho. Most sites were at the beginning stages of incorporating abortion services into their practice. Identified barriers included: obtaining mifepristone, understanding protocol, federal funding concerns, and navigating anti-abortion views. Significantly, barriers were observed in non-restricted and restricted states. A proposed solution included a learning collaborative comprised of: (1) trainings on integration and delivery of abortion services; (2) support for Federally Qualified Health Centers (FQHC) with funding concerns; and (3) referral to telemedicine abortion services at University of Washington.
Conclusions: Clinic champions across different state-level abortion restrictions faced barriers including: logistical, legal and ideological challenges. These obstacles can facilitate the creation of an abortion learning collaborative and regional networks with the potential to provide seamless, high-quality abortion care despite federal and state restrictions.
# 33
DEVELOPING A COMMUNITY-CENTERED HEALTH FAIR THROUGH A PIPELINE COLLABORATIVE APPROACH WITH LEARNERS IN TRAINING
Morton M1, Kuo P1, Casilang C2. 1UC Irvine School of Medicine/CHOC Children’s Hospital of Orange County, Orange, CA and 2CHOC Children’s Hospital of Orange County, Orange, CA
Purpose of Study: Building healthy communities involves placing local stakeholders at the heart of public health and reducing health inequities by addressing unique barriers faced by those in need. Community health fairs have been used in this practice as a way of offering health promotion, education, and screening services directly to underserved populations. The aim of this study is to highlight how a pipeline collaborative approach with medical trainees can alleviate barriers faced by vulnerable and under-resourced populations in the community.
Methods Used: Most residency programs in medicine provide opportunities to address social determinants of health to train learners on how to provide systemic and environmental change in the community. UC Irvine School of Medicine/CHOC Children’s Hospital of Orange County (UCI-CHOC) offers an advocacy track, through which, pediatric residents were inspired to organize and execute a community-based health fair to address gaps in healthcare. With the guidance of physicians in community medicine, American Academy of Pediatrics Orange County (AAP-OC), and Wellness on Wheels, pediatric residents recruited local organizations that were committed to providing resources and education to the community. Residents mentored medical students from various training sites to provide health education, and medical students in turn helped undergraduate students conduct outreach activities in the local communities. This pipeline approach was overseen by local organizations that pinpointed the needs of the community, and the trainers in various stages of learning addressed these gaps through the emphasis on 8 designated pillars of wellness, such as physical, mental, occupational, environmental, emotional, nutritional, financial, and social.
Summary of Results: The health fair not only increased learner awareness of the barriers that underserved communities experience, but it also promoted access to care and purposeful, culturally appropriate education in the areas of health that address the psychosocial aspects of wellbeing. The development of the health fair provided meaningful learning experiences for the health professions students.
Conclusions: It is imperative for communities to work collaboratively with local stakeholders and partners such as community physicians to help reduce health inequities and address the specific needs of families in a systemic way. This makes it even more important for physicians to mentor and collaborate with learners of different stages of training in engaging in community-based activities and programs, so the encouragement and opportunities to address health inequities can begin early on in training and continually cultivate leaders who are equipped to create solutions that bridge the gaps in healthcare.
A pipeline approach provides a platform for trainees to educate other learners in subsequent stages of training in a sustainable manner, which in turn enhances capabilities in medical practice and community leadership.
# 34
INCREASING OPIOID USE DISORDER AWARENESS ON THE BLACKFEET RESERVATION IN BROWNING, MONTANA
Kray CE, Keys T. University of Washington School of Medicine, Seattle, WA
Purpose of Study: Browning sits in the heart of Glacier County, MT on the Blackfeet Reservation and is home to 13,681 residents of which 64.6% identify as American Indian/Alaska Native (AI/AN). Substance use disorder (SUD), primarily opioids (e.g., fentanyl, oxycodone, and morphine), was identified as a top community health priority after a 2017 Indian Health Services (IHS) survey identified that 71% of 479 residents know of a close family member using opioids. It was hypothesized that providing community health education materials in addition to planning a public health forum would increase opioid use disorder awareness on the Reservation.
Methods Used: SUD on the Blackfeet Reservation is a complex issue and therefore requires a tailored approach to solutions. AI/AN traditional medicine/healing (TM/H) has been identified by the National Institute of Health (NIH) as a whole medical system that encompasses a range of holistic treatment requiring a bio-psycho-social-spiritual approach. Furthermore, to foster early screening and intervention in high risk individuals (e.g., pregnant women, adolescents, and elders) requires community efforts and education. From meetings with community members, it was determined that strengthened partnership coupled with a focus on TM/H remains an area of strong interest. After participating in a traditional medicine sweat ceremony on the sacred lands of Heart Butte, MT with Blackfeet elders, we were asked to share this experience and to further ground traditional culture in SUD treatment on the Reservation.
Summary of Results: Community partnership was cultivated with the Crystal Creek Lodge (CCL), an out-patient SUD treatment facility in Browning. A plan was developed with CCL to host a public forum for community stakeholders, including the Blackfeet Community Hospital, Browning Public Schools, and Community Corrections. Ideal outcomes outlined were strengthened partnership, collective education on SUD, and strategy implementation. A presentation was crafted, highlighting the epidemiology and physiology of SUD, in addition to traditional and allopathic medicine available on the Blackfeet Reservation. Flyers were made along with handouts that could be given to attendees focused on SUD facts/myths and available resources in the community. The forum would also include open discussion and personal stories from residents who have/are experiencing SUD.
Conclusions: Community deliverables were well received by CCL with the intent to pilot their first public forum and to continue like events. Limitations remain based on completion of the event and if the stakeholders find value from the discussion. Attendance by stakeholders and community members may also remain a challenge. Despite these barriers, the community relationships developed from partnership with CCL and our participation in sweat ceremonies with tribal elders has started the discussion on one of Browning’s top community priorities and has emphasized the need for addressing SUD and revitalizing AI/AN culture along with TM/H.
Opioid Use in Browning, MT Public Schools vs. Montana State Public Schools.
2012 Lifetime
2012 Last 30 Days
2014 Lifetime
2014 Last 30 Days
2016 Lifetime
2016 Last 30 Days
Browning 10th Grade
10%
5%
11%
2%
6%
3%
Montana 10th Grade
11%
4%
9%
3%
6%
2%
Browning 8th Grade
1%
1%
2%
2%
3%
1%
Montana 8th Grade
4%
2%
2%
1%
2%
2%
Indian Health Services Community Health Assessment (2017)
# 35
Evaluating Outcomes of Community Health Promoter’s COPD Diagnosis and Management Education in Karagita, Naivasha, Kenya. A Quasi Experimental Study
Anderson M1, Bosibori D2. 1University of Washington, Seattle, WA and 2Naivasha Sub-County Referral Hospital, Naivasha, Kenya
Purpose of Study: Chronic obstructive pulmonary disease (COPD) is the 3rd leading cause of death worldwide, with 90% of those deaths occurring in low- and middle-income countries. COPD accounted for up to 10% of male ward hospitalizations in Naivasha Sub-County hospital in 2022. The aim of this study was to educate community health promotors (CHP) within the Naivasha Sub-County community about COPD, with a focus on prevention, signs and symptoms, and treatment. The CHPs will be able to confer this knowledge to those in the community with the goal of decreasing the prevalence of COPD, decreasing COPD exacerbations, and increasing quality of life for those COPD.
Methods Used: Local health care workers were consulted to assess the prevalence of COPD and gain an understanding of the CHPs understanding of COPD. A literature review was then conducted, using articles from PubMed and Google Scholar. Educational materials were developed, and an education session was held to teach CHPs in Karagita about COPD. CHP participants were given an 8-question pretest survey to assess their confidence in knowledge about COPD and comfort in educating others about COPD. These were measured using a 5-point Likert scale. They were then given an educational presentation covering the learning objectives. After, they were given an identical 8-question post-test survey, to evaluate their knowledge and comfort in educating others about COPD. The results of the pre- and post-survey were collected anonymously, and averages compared at the group level. The CHPs were then given an educational pamphlet covering the information taught for their own use at home.
Summary of Results: A total of 18 CHPs participated. Their pretest surveys had an average confidence score of 2.7/5. They then engaged in the learning, demonstrating an understanding of each of the learning goals by their correct completion of the practice cases provided during the learning session. After the educational presentation those same 18 CHPs took the same survey, this time averaging a confidence score of 4.6/5.
Conclusions: This education session was able to increase the CHP’s understanding of COPD, as well as their confidence in their ability to teach vulnerable populations within their community about COPD. Thus, CHPs will be able to continue to educate those in the community about COPD risk factors and prevention, which may lead to a decrease in COPD, and COPD-related hospitalizations. Ongoing education for CHPs about COPD is needed, and will have an impact on the community.
# 36
ENHANCING HEALTH LITERACY AND PROMOTING PREVENTIVE MEDICINE AMONG THE GERIATRIC COMMUNITY IN BUFFALO, WYOMING
Bauer S1, Keys T2. 1University of Washington School of Medicine, Seattle, WA and 2University of Washington, Seattle, WA
Purpose of Study: Buffalo, Wyoming has a population of 4,485 with 20% being adults aged 65+. The 2021 health needs assessment by the community hospital identified the aging demographic as a major concern, emphasizing the necessity for education regarding Medicare benefits and heightened awareness of preventive medicine within the geriatric community. Local nurses and physicians noted the underutilization of Medicare’s preventive services, explaining the community’s limited access to healthcare literacy resources. Research shows that annual exams and preventive services lead to a 45% lower hazard of all-cause mortality. This project aimed to enhance health literacy about preventive medicine and raise awareness of Medicare-covered services, ultimately increasing utilization of these services and reducing the disease burden among Buffalo’s geriatric population.
Methods Used: This project adopted an asset-based approach, which guided investigation of the identified public health concern. This process involved analyzing the 2021 health needs assessment where the concern was identified, followed by conversations with the community hospital’s social worker and nursing director, who were key contributors to the assessment. These conversations aimed to gauge the community’s current stance on the issue and identify existing community organizations addressing the concern, in which the Buffalo Senior Center was identified as a pivotal community asset. Engagements were made with the Senior Center to discuss potential health education materials and distribution plans.
Summary of Results: In collaboration with the Buffalo Senior Center, a health education pamphlet was created regarding preventive medicine and its significance in reducing disease burden. The pamphlet highlighted Medicare-covered services for this patient demographic and guided seniors on navigating the process through annual wellness visits with primary care providers. A comprehensive presentation of this information was delivered at the Senior Center, along with pamphlet distribution during the event. Pamphlets were also distributed to residents’ homes via the Meals-on-Wheels delivery service.
Conclusions: The asset-based approach employed in this project emphasized the value of utilizing established community organizations in executing impactful public health education initiatives. The early and meaningful community engagement ensured that the developed health education materials were relevant to the current issues within Buffalo’s community, making it more likely to resonate with the target audience, and increasing the chances of successful engagement. Notably, the project highlighted the effectiveness of a strength-based framework for tailoring public health education to specific communities. Next steps include, devising a follow up evaluation on the comprehension of delivered pamphlets through conversations with local healthcare professionals and consider staffing limitations to an influx of annual exams.
Immunology and Rheumatology I
Concurrent Session
12:45 PM
Thursday, January 18, 2024
# 37
TESTING OF MULTIPLE AUTOANTIBODIES IDENTIFIES EXPANSION OF TARGETED ANTIGENS AND A METHOD TO IDENTIFY IMMINENT ONSET OF CLINICAL RHEUMATOID ARTHRITIS
Goff SH1, Bergstedt d4, Feser ML2, Moss L2, Mikuls T3, Edison JD5, Holers V2, Mahler M6, Deane K2. 1The University of Colorado School of Medicine, Aurora, CO; 2The University of Colorado School of Medicine, Aurora, CO; 3University of Nebraska Medical Center, Omaha, NE; 4St Joseph’s Hospital/Intermountain Health, Denver, CO; 5Walter Reed National Military Medical Center, Bethesda, MD and 6Werfen, San Diego, CA
Purpose of Study: Rheumatoid arthritis (RA) has a period termed ‘pre-RA’ during which there are autoantibody elevations prior to the onset of clinically-apparent inflammatory arthritis (i.e. clinical RA). Multiple autoantibody systems including antibodies to citrullinated proteins (ACPA), rheumatoid factor (RF), anti-peptidyl arginine deiminase (anti-PAD) and anti-carbamylated proteins (anti-CarP) have been described in pre-RA; however, few studies have tested all antibodies in a single pre-RA cohort. The objective of this study was to test multiple autoantibody systems in pre-RA, and evaluate the role of these autoantibodies in potentially identifying a signature in the pre-RA period that indicates imminent onset of clinical RA.
Methods Used: We evaluated 148 individuals with two pre- and one post-RA diagnosis serum samples available from the Department of Defense Serum Repository (DoDSR), and matched controls. Samples were tested for anti-CCP3, five ACPA fine specificities, anti-PAD, anti-CarP and RFIgA and IgM (Werfen). Positive levels for autoantibodies were determined using levels present in <=1% in a separate set of DoDSR controls. Analyses included comparison of positivity of autoantibodies over time in pre-RA and post-RA, and comparisons between RA and controls.
Summary of Results: The individuals with RA had a mean age at diagnosis of RA of ~37 years, were ~55% female and had post-RA positivity of anti-CCP3 of 60.8%, RFIgA of 45.9% and RFIgM of 45.9%. Positivity of anti-CCP3, RFIgA and IgM, anti-PAD1 and PAD4, anti-vimentin 2, anti-fibrinogen and anti-histone 1 increased over time in pre-RA and were significantly different than controls; however, positivity rates were overall similar in immediate pre-RA samples compared to post-RA samples. Counts of autoantibodies also increased over time in pre-RA, and within anti-CCP3 positive samples, a higher total autoantibody count was significantly associated with a time period <=3 years prior to RA diagnosis.
Conclusions: Multiple autoantibodies including anti-CCP3, RFIgA and M, ACPA fine specificities and anti-PAD antibodies are present in pre-RA, although anti-CCP3 and RFs have the highest positivity rates. This confirms prior findings, however also expands upon them by demonstrating the rates of these antibodies in a single cohort. In addition, in anti-CCP3 positive samples, an increasing total antibody count indicates a sample is <=3 years prior to RA diagnosis; when further validated, that could serve as a model to predict imminent RA.
# 38
HUMAN CD4 T CELL RESPONSES TO CHLAMYDIA TRACHOMATIS METABOLIC ENZYMES
Herko K, Campbell VL, McClurkan CL, Craig J, Hybiske K, Johnston C, Koelle DM. University of Washington, Seattle, WA
Purpose of Study:Chlamydia trachomatis (Ct) is an obligate intracellular bacterium and the leading cause of bacterial sexually transmitted infection in humans. Untreated infections can cause pelvic inflammatory disease and lead to infertility. Repeat infections are common and thought to be associated with limited antigen exposure due to conventional antibiotic therapy, suggesting a role for a Ct vaccine. Although the full significance is uncertain, studies in both humans and murine models suggest a protective role for CD4 T cells, mediated via interferon gamma (IFNγ). Our aim was to identify antigen specificity of Ct-reactive CD4 T cells within a subsection of the Ct open reading frame (ORF)eome.
Methods Used: We obtained blood from consented persons with prior Ct infections and positive Ct-specific serum antibodies. Because Ct-specific T cells are rare in blood, we selected and functionally enriched CD4 T cells reactive to whole killed Ct using Activation Induced Marker (AIM)-based sorting. Ct-reactivity of CD4 T cells was confirmed by intracellular cytokine staining assays, focusing on IFNγ. After expansion, resultant T cell lines (TCLs) were probed with a panel of Ct proteins, representing approximately one tenth of the total Ct proteome (91/920 annotated ORFs). Candidate antigens were selected due to their potential as drug targets. T cell reactivity was measured by IFNγ secretion using ELISA and lymphoproliferation using a 3H-thymidine incorporation assay.
Summary of Results: We observed specific reactivity to antigens containing the Ct proteins GAPDH and Lysine-tRNA synthetase. These T cell targets are metabolic enzymes, rather than secreted effectors or membrane components, likely due to our antigen panel being weighted toward drug targets. To validate these findings, we used overlapping peptides covering the top target GAPDH to discover single specific short linear peptides capable of eliciting IFNγ secretion for each of the two GAPDH-responsive TCLs. Interestingly, each GAPDH-responsive TCL recognized a different region of the protein. T cell responses to Lysine-tRNA synthetase were not assessed beyond whole protein antigenicity.
Conclusions: In conclusion, Ct-reactive CD4 T cells are detectable at low levels in the peripheral blood of persons with prior Ct infection. Further research is required to understand the significance of T cell responses to Ct and specifically Lysine tRNA synthetase and GAPDH. Well known for its role in glycolysis, GAPDH also interacts with host proteins at the cell surface, increasing virulence and possibly contributing to its antigenicity through increased extracellular exposure. As humans are colonized by many bacterial species containing conserved metabolic enzymes, it is relevant to discern whether these responses are unique to Ct or common across the human bacteriome. Further, determining the prevalence of responses to these proteins in symptomatic vs. asymptomatic and reinfected vs. uninfected cohorts would aid in exploring these Ct enzymes as potential vaccine antigens.
# 39
GLUTATHIONE MODULATES THE HOST IMMUNE RESPONSE BY ALLEVIATING ADVERSE EFFECTS OF SARS COV-2 SPIKE PROTEIN
Norris BJ, Chorbajian A, Dawi J, Mohan A, Ochsner J, Misakyan Y, Kiriaki A, Venketaraman V. Western University of Health Sciences College of Osteopathic Medicine of the Pacific, Pomona, CA
Purpose of Study: Researchers have identified immunothrombosis as a dominant mechanism for increased mortality and morbidity in coronavirus 2019 disease (COVID-19). Patients with severe COVID-19 enter a hypercoagulable state that can lead to clot formation within the pulmonary vasculature causing acute respiratory distress and worsened disease prognosis. Inflammation, endothelial cell damage, and a dysregulated immune system are all contributing factors to this more severe disease presentation. The dysregulation of the immune system, also termed a cytokine storm, is mediated by an increase in immune mediators including interleukin-6 (IL-6) and transforming growth factor-beta (TGF-β) among others. Glutathione (GSH) has been suggested by previous studies as a defense mechanism against this more severe COVID-19. Decreased levels of GSH have been associated with increased viral replication, inflammatory cytokine levels, and thrombosis, suggesting that GSH supplementation may be therapeutic for COVID-19. In this study, the effectiveness of GSH as an adjunctive therapy for preventing the development of COVID-19 was tested by performing in vitro studies using peripheral blood mononuclear cells (PBMC) treated with spike protein of SARS-CoV2.
Methods Used: Peripheral blood was drawn from nine participants, and the PBMCs were isolated using Histopaque-1077 and cultured in RPMI containing 20% autologous plasma on 96-well plates. PBMCs were treated with spike protein at 5 and 10ng/ml concentrations. Liposomal GSH (L-GSH Readisorb) was added at 40 and 80mM concentrations to PBMCs that were cultured in the presence and absence of spike-protein. ELISA was performed to measure amounts of IL-6, TGF-β, and TNF-α. GSH and malondialdehyde (MDA) levels were also determined in the cell lysates. Cell culture supernatants were also analyzed for microclot formation using thioflavin T stain and fluorescence microscopy.
Summary of Results: L-GSH treatment caused a statistically significant decrease in the levels of IL-6, TGF- β, and TNF-α levels at 3 hours, 3 days, and 7 days post-treatment. L-GSH treatment also resulted in a significant decrease in the levels of MDA (end product of lipid peroxidation) at 3-hour and 7-day time points. A significant increase in the levels of total form GSH was observed at 3 hours and 7-day post-LGSH treatment. Microthrombosis imaging with thioflavin T results also indicated a decrease in clot formation in the presence of L-GSH.
Conclusions: The results show a decrease in the levels of IL-6, TNF-α, MDA, and microclots when PBMCs were treated with L-GSH. These findings indicate that GSH may be effective in reducing the cytokine dysregulation, clot formation, and inflammation associated with COVID-19 spike protein exposure. Our study findings indicate that GSH supplementation should be explored as a means of lowering morbidity and mortality caused by severe COVID-19 infection.
# 40
ANALYSIS OF BIOLOGIC THERAPIES IN PREGNANCY WITH MATERNAL RHEUMATOLOGIC DISEASE
Bronnenberg T, Kachikis A, McCartney S. University of Washington, Seattle, WA
Purpose of Study: Rheumatologic diseases are commonly diagnosed in women of reproductive age. The onset of these diseases can cause significant strain in mental wellbeing, overall health, and family planning decisions. Inflammatory and autoimmune disorders are associated with adverse pregnancy outcomes, such as preterm delivery, pre-eclampsia, and fetal growth restriction, as well as maternal disease flares. Recent development of biologic therapeutics, which are small molecules or antibodies that target the immune system, have advanced the ability to treat autoimmune diseases. However, there is minimal data on the safety of these biologic therapies during pregnancy and whether they are superior to non-biologic treatments. Due to the unknowns of treating autoimmune disease during pregnancy, we sought to determine whether the use of biologic therapeutics were associated with altered risks of autoimmune flares or postpartum infections compared to non-biologic treatments in pregnant patients.
Methods Used: Utilizing electronic health records from University of Washington (UW), we identified patients of any age who delivered at UW between 2003-2023 whose pregnancy was complicated by autoimmune disease, with and without treatment using biologic therapeutics. We abstracted maternal and offspring clinical characteristics including medical, surgical, obstetric and gynecologic history, demographic parameters, medication usage and timing of administration, disease activity, labor and delivery characteristics, and pregnancy outcomes. Statistical significance was determined using Chi squared testing performed using Stata software.
Summary of Results: We identified 102 pregnancies with diagnosis of autoimmune disease (AID), specifically including rheumatoid arthritis (55), psoriatic arthritis (24), inflammatory arthritis (15), ankylosing spondylitis (5), multiple sclerosis (4), Sjogren’s syndrome (3), Still’s disease (3), hidradenitis (2), and systemic lupus erythematosus (1). The maternal age ranged from 18-47. A total of 59% of AID patients were treated with biologic therapeutics, in which the targets included TNF-alpha, IL-6, CD20, IL12/23, IL-5/IgE, IL-1, and integrins. Patients on biologics had an increased risk for flares during pregnancy when compared to those who were not treated with biologics (26% vs 7% respectively, p = 0.012), primarily occurring in the late 2nd and 3rd trimesters. There were no significant differences in postpartum flares, antepartum infections, or postpartum infections between patients treated with or without biologics.
Conclusions: Despite the potential benefits of biologic treatments in pregnancy, these data demonstrate increased antepartum flares patients on biologics compared to patients on alternative treatment. This may represent a more severe disease phenotype in patients receiving biologics. We did not detect increased risk of postpartum infections or readmissions in patients receiving biologics, suggesting safety of these medications despite potential for immunosuppression.
Rate of antepartum and postpartum flares across all groups.
Biologics (n=60, 58.8%)
No-biologics (n=42, 41.2%)
P-value
Any Antepartum Flare
16 (26%)
3 (7%)
0.012
Timing of Flare
1st tri (<14w)
5
3
0.34
Early 2nd tri (14-21w)
1
1
Late 2nd tri (22-28w)
6
0
3rd tri (>28w)
3
0
Any Postpartum Flare
16 (26%)
6 (14%)
0.13
# 41
INTERLEUKIN-22, INTERLEUKIN-17 AND, FORKHEAD BOX P3 IS SUPPRESSED IN STIMULATED PERIPHERAL BLOOD MONONUCLEAR CELLS OF MULTIPLE SCLEROSIS PATIENTS
Gezahegn B1, Wagner DH1, 2. 1University of Colorado School of Medicine, Aurora, CO and 2Webb-Warring Center, Denver, CO
Purpose of Study: Multiple Sclerosis is an autoimmune demyelinating disease of the central nervous system. The immune system goes haywire and attacks the myelin, an insulating sheath of the nerves utilized to increase the speed and efficiency of electrical impulses. Several predisposing factors including genetics are correlated but a clear association has not been identified. Once identified, the course of multiple sclerosis can vary depending on underlying inflammation, influenced by the balance of regulatory and inflammatory cytokines. Clinically, tracking the cytokine levels and transcription factors can potentially help identify response to therapy and progress of disease course. Our lab measured biomarkers such as Interleukin-22 (IL-22), a regulatory cytokine, Forkhead Box P3 (Foxp3), a regulatory transcription factor, and Interleukin-17 (IL-17), an inflammatory cytokine.
Methods Used: Samples were collected from Multiple Sclerosis patients receiving care at the Neurology Department at The University of Colorado Hospital. Lymphocytes were isolated by Ficol-Hypaque and stimulated. Cells were stained for CD3, CD4, IL-17, IL-22, and Foxp3. Flow cytometry was conducted using a MACSQuant Analyzer. The gates were set such that the upper left/right and lower right quadrants had less than 1% of events. Data was analyzed using GraphPad Prism from GraphPad Software, Inc.
Summary of Results: Samples collected from MS patients had a baseline lower level of IL-22 and Foxp3 levels compared to control (P<0.05). IL-17 levels were also lower in unstimulated MS samples but without statistical significance. IL-22, IL-17, and Foxp3 levels in MS samples remained relatively low compared to control after stimulation (P<0.05).
Conclusions: IL-22 and Foxp3 were downregulated in stimulated and unstimulated MS samples relative to control samples consistent with the imbalance of anti-inflammatory activity in the immune system. IL-17 levels were also lower in stimulated MS samples relative to control. This finding is not consistent with the inflammatory activity of IL-17. A likely explanation can be that an increased sample size and higher concentration stimulation of MS samples might be necessary to understand the relative IL-17 concentration in MS relative to control.
# 42
DRUG RASH WITH EOSINOPHILIA AND SYSTEMIC SYMPTOMS (DRESS) CAUSED BY AMIODARONE
Chaudhry A, Fox K, Chiu C, Mishra S. Kern Medical Center, Bakersfield, CA
Purpose of Study: Drug rash with eosinophilia and systemic symptoms (DRESS syndrome) is a serious idiosyncratic drug reaction. Cutaneous manifestations and other organ involvement is common. We present a unique case where a patient developed DRESS syndrome after the initiation of amiodarone. Currently, there is no literature that describes DRESS syndrome caused by amiodarone.
Methods Used: A single patient case report was conducted after IRB approval.
Summary of Results: 61 year old male with history of hypertension, dyslipidemia, and benign prostatic hyperplasia presented with five days of fever, cough, and shortness of breath. He was hypoxemic with oxygen saturation of 84% on room air and diagnosed with COVID-19. He completed a 10 day course of Dexamethasone but remained hypoxic requiring high flow oxygen after 2 weeks. His clinical condition deteriorated with development of atrial fibrillation (AF) with rapid ventricular response (RVR) requiring amiodarone drip. He required intubation and failed to improve, eventually requiring tracheostomy. AF with RVR required frequent boluses of amiodarone before successfully converting to sinus rhythm after cardioversion. While on amiodarone, he developed eosinophilia up to 3.1 x 10^3 cells/μL. Initially, eosinophilic pneumonitis secondary to amiodarone was suspected and patient was switched to sotalol and started on prednisone. Bronchoalveolar lavage was negative for eosinophilic pneumonitis. Due to continued AF with RVR, amiodarone was restarted. Several days later, he developed maculopapular rash on his abdomen, forearms and thighs, with worsening eosinophilia. Given persistent AF with RVR, he received another external cardioversion with successful conversion to sinus rhythm which was maintained with increased dosage of amiodarone. His rash worsened, became more confluent and extended to involve the majority of his body. Skin punch biopsy showed focal chronic inflammation and focal spongiosis. DRESS syndrome due to Amiodarone was suspected due to a score of six on the Registry of Severe Cutaneous Adverse Reactions (RegiSCAR) Scoring System. Amiodarone was stopped and switched to sotalol. Given the severity of DRESS syndrome, he was treated with intravenous methylprednisolone 250 mg daily for two days and followed by oral prednisone 1 mg/kg with tapering over twelve weeks. Eosinophilia resolved and the skin rash improved after discontinuation of amiodarone.
Conclusions: DRESS syndrome can be caused by many different medications. Although there is no literature describing DRESS syndrome caused by amiodarone, it can be caused by any medication as seen in our patient. The RegiSCAR Scoring System is most commonly used to confirm diagnosis. Despite treatment with steroids, the offending agent must be discontinued for resolution of disease. Even after resolution, recurrent flares are commonly seen in patients with DRESS syndrome.
# 43
GRANULOMA ANNULARE ONSET FOLLOWING COVID-19 VACCINATION
McIntyre ER1, 2, Lamb P2, Fung MA2, Kiuru M2, Chan LS2. 1California Northstate University, Sacramento, CA and 2UC Davis, Sacramento, CA
Case Report: Infection with SARS-COV-2 has shown the ability to damage many organ systems via immune-mediated reactions, including the largest organ - the skin. Granuloma annulare (GA) is a rare rash with unclear etiology that presents as annular, erythematous papules or plaques with central clearing. To our knowledge, there has only been one reported case of GA associated with COVID-19 vaccination published thus far. We present the cases of a 54-year-old female and a 66-year-old male who developed generalized GA and localized GA, respectively, following the administration of a COVID-19 vaccine, which worsened with subsequent boosters. A skin biopsy performed in the 54-year-old female after her first booster revealed the following histological findings: a multifocal, palisaded and interstitial histiocytic infiltrate with central degenerated collagen in the dermis, consistent with a diagnosis of GA. A shave biopsy performed in the 66-year-old male on his dorsal thumb revealed the upper portion of an interstitial mononuclear cell infiltrate with few multinucleated cells associated with thickened collagen fibers, compatible with a diagnosis of interstitial GA. The 54-year-old female underwent multiple treatments for GA associated pruritus over a period of two years, including Minocycline, Intralesional Kenalog, triamcinolone cream, Kenalog injections, and Methotrexate. Following these treatments, and at her most recent office visit, the patient had all lesions flattened, and most without erythema. The 66-year-old male patient received one dose of intralesional triamcinolone (10 mg/cc) and topical corticosteroid betamethasone for treatment, which improved his pruritic symptom.
This paper reviews the existing literature on GA associated with COVID-19 infection and vaccination, as well as the possible immunological mechanisms underlying the development of GA following vaccination. We especially note the striking similarities in disease morphology and temporal association with COVID-19 vaccination between our 54-year-old female and the first reported case of GA following COVID-19 vaccination . Despite the temporal association between COVID-19 vaccination and the development of GA, the exact causative relationship remains unclear. Further studies are needed to elucidate the underlying mechanisms and determine the true incidence and risk factors for GA associated with COVID-19 vaccination.
Infectious Diseases I
Concurrent Session
12:45 PM
Thursday, January 18, 2024
# 44
ADMINISTRATION OF BIOMIMETIC HUMAN CELL MEMBRANE-COATED NANOSPONGES GREATLY IMPROVES SURVIVAL IN A MURINE MODEL OF NEONATAL PERITONITIS WITH OR WITHOUT CONCURRENT EXPOSURE TO TARGETED ANTIBIOTICS
Yu B1, Gao W2, Zhang L2, Nizet V3, Lawrence SM1. 1The University of Utah, Salt Lake City, UT; 2UCSD, La Jolla, CA and 3UCSD, La Jolla, CA
Purpose of Study: Human cell-membrane-coated nanoparticles (NPs), or “nanosponges,” are non-specific biomimetic “decoys” engineered to maintain the same assortment of cell membrane receptors as the host cell. This property enables them to irreversibly sequester and neutralize a wide array of bacterial virulence and host pro-inflammatory mediators. Here, we demonstrate the ability of macrophage (MΦ) and red blood cell (RBC) NPs to significantly improve survival in CD1 murine pups using a cecal slurry (CS) peritonitis model.
Methods Used: CD1 murine pups were exposed to cecal slurry to achieve LD70 (70% mortality; CS dose of 2.0 mg/g) by intraperitoneal (IP) injection on postnatal day five. Pups were dosed with imipenem + cilastatin at 25 mg/kg IP one hour after CS injection, then received either 40 mg/kg of MΦNPs or RBCNPs IP one hour later and monitored for five days. Control mice were also exposed to CS at 2.0 mg/g IP, then received equal volume of PBS (imipenem control) and D10W (NPs control). Moribund mice were humanely euthanized during this period (IACUC-approved #1944). Serum cytokines and bacterial counts of the blood, liver, and spleen were collected at 6, 12, and 24 hours after CS injection and histopathology of end organs (liver, lungs, spleen, and kidneys) are being investigated.
Summary of Results: Administration of nanosponges significantly improved survival (nearly 30% compared to imipenem alone and 93% when combined with imipenem, p<0.0001) in a CS murine model of neonatal sepsis. Moreover, a single dose of RBCNPs has been shown to decrease mortality compared to either a solitary dose of imipenem or MΦNPs when administered 4h after the induction of CS peritonitis at LD70.
Conclusions: Nanosponges are a first-in-class therapeutic with proven efficacy to greatly improve survival, with or without concurrent exposure to targeted antibiotics, using the gold-standard murine model of neonatal sepsis.
Kaplan-Meier Survival Curve demonstrates a greatly reduced risk of mortality when red blood cell- or macrophage- coated nanoparticles are administered as adjunct therapy to targeted antibiotics in a cecal slurry murine model of neonatal sepsis at LD70 (2.0 mg/g).
# 45
CLINICAL AND EPIDEMIOLOGICAL CHARACTERISTICS OF MYCOPLASMA AND UREAPLASMA INFECTIONS DETECTED BY MOLECULAR DIAGNOSTICS
Hansen DM, Bourassa L, Leiberman J, Truong T. University of Washington School of Medicine, Seattle, WA
Purpose of Study: The bacterial genera Mycoplasma and Ureaplasma are the most clinically significant pathogens in the class Mollicutes; however, infections are difficult to diagnose as most species do not grow under standard culture conditions. The goal of this study is to describe the demographic and microbiological characteristics of a large study population of individuals positive for Mycoplasma or Ureaplasma by molecular methods.
Methods Used: Our reference laboratory provides identification of Mollicutes from clinical specimens through broad-range bacterial and organism-specific PCR-sequencing assays. We retrospectively reviewed testing data from 938 patients with specimens positive for Mycoplasma and Ureaplasma submitted from 33 states from 10/19/2020-5/31/2023. We performed additional chart review of 50 internal patients with available medical records.
Summary of Results: 15 Mycoplasma and Ureaplasma species were detected, with an additional 4 bone and tissue specimens containing under-described, unnamed species within genus Mycoplasma associated with zoonotic transmission. The most frequently detected species from respiratory sites were M. salivarium (70%), Ureaplasma (13%), and M. hominis (4.5%). While many specimens were polybacterial, 8% were monobacterial, suggesting likely cause of infection. Pleural fluid samples most often contained M. salivarium (30%), M. hominis (26%), and Ureaplasma (26%). 35% of these samples were monobacterial. Of the 40 cases of Mycoplasma or Ureaplasma infection in respiratory sites with available chart notes, 67% had recent (<3 months) solid organ transplantation and 12.5% had a hematologic malignancy. There were 2 cases of disseminated M. hominis infection after major traumatic injuries. In 503 positive urogenital cases, 83% contained Ureaplasma, 79% of which were in young adults aged 19-40. Ureaplasma was also detected in invasively-collected samples, including uterine, placental, kidney, and bladder tissues. One placental tissue sample contained M. hominis. Cerebrospinal fluid and brain tissue specimens were frequently positive for Ureaplasma (83%), with the remainder comprising M. faucium (11%) and M. salivarium (5.5%). 56% of CNS samples were monobacterial. Ureaplasma was the most common Mollicutes species in bone and joint sites (35%), followed by M. hominis (28%), and M. salivarium (22%). Uncommon species, including M. indiense and M. arginini, with one infection from a domestic cat bite, were also detected in bone and joint samples. 77% of samples from these sites were monobacterial. Other monobacterial samples were isolated from cardiac tissue, splenic tissue, abscesses, and surgical wounds.
Conclusions: Our results implicate many Mycoplasma and Ureaplasma species in infections involving a variety of patient populations and body sites, including monobacterial sterile site infections. These findings warrant reconsideration for several members of this group, especially uncommon species and species previously regarded as commensals, as underappreciated pathogens.
# 46
IMMUNE PATHWAYS ASSOCIATED WITH TUBERCULOSIS TREATMENT OUTCOMES
Hsieh A1, 2, Darboe F1, Walzl G3, Suliman S1. 1UCSF, San Francisco, CA; 2Western University of Health Sciences, Pomona, CA and 3Stellenbosch University, Cape Town, South Africa
Purpose of Study: Tuberculosis (TB) is the leading cause of death from a single infectious agent worldwide, with 1.5 million deaths annually. While standard-of-care 6-month TB treatment cures most patients, treatment may not fully clear Mycobacterium tuberculosis, increasing risk of relapse. A better understanding of underlying immunological pathways can help predict treatment response. In this study, we analyzed whole blood transcriptomes of patients with pulmonary TB undergoing treatment to define biological pathways associated with different treatment outcomes: cure, failure, or relapse.
Methods Used: We used a publicly available bulk blood RNA-seq dataset from the Catalysis treatment response cohort (PMID: 27595324). Samples were collected from TB patients undergoing treatment at diagnosis, week 4, and end of treatment (EOT). Participants were monitored for two years after EOT for relapse. Gene counts were obtained from Gene Expression Omnibus (GSE89403), and analysis was conducted using R (version 4.6.1). Differentially expressed genes (DEGs) were identified with DESeq2 (version 1.40.2), and gene set enrichment analysis was done using FGSEA (version 1.26.0) with Gene Ontology Biological Process terms. DEGs and related pathways were compared between patients with TB and other lung diseases, as well as among patients with different treatment outcomes, both at diagnosis and EOT.
Summary of Results: Ninety-six (59M and 37F) HIV-negative, nondiabetic, patients from Cape Town, South Africa, were diagnosed with drug-susceptible pulmonary TB and received standard-of-care treatment. Based on EOT sputum GeneXpert cycle thresholds, 76 patients cured, 8 failed treatment, and 12 had recurrent TB within 2 years.
We identified transcriptomic profiles associated with TB disease compared to other lung diseases, with the most significant DEGs being GBP5 (log2FC=2.06, padj=6.2e-9) and RSAD2 (log2FC=2.52, padj=3.6e-6). The top pathway at time of diagnosis associated with treatment failure ranked by normalized enrichment score (NES) was granulocyte activation (NES=2.75, padj=8.7e-18). The top pathway at EOT for patients who redevelop TB ranked by NES was glutathione metabolic process (NES=2.30, padj=1.9e-4).
Conclusions: We show here that gene expression can differentiate TB from other lung diseases with similar clinical presentations, offering potential for novel point-of-care tests. We observed that DEGs can predict treatment outcomes, even before starting treatment. Importantly, differentially expressed genes and pathways can identify patients more likely to redevelop TB within two years, despite clinical and microbiological cure at EOT. These results may justify extended treatment protocols for individuals predicted to be at a higher risk of treatment failure or recurrence. Our study seeks to deepen our understanding of underlying biological processes involved in successful completion of TB treatments, while also highlighting differentially expressed pathways as potential avenues for adjunct host-directed treatment regimens.
# 47
BACTERIAL ANTI-VIRAL IMMUNITY IN PSEUDOMONAS AERUGINOSA
Scheel A3, 1, Maderia M2, Faith D2, Secor PR2. 1Montana State University, Bozeman, MT; 2University of Montana, Missoula, MT and 3University of Washington School of Medicine, Seattle, WA
Purpose of Study:Pseudomonas aeruginosa is a human pathogen frequently associated with nosocomial infections that is rapidly becoming resistant to antibiotics. The demand for new antibacterial agents has rekindled interest in the use of viruses that infect bacteria (bacteriophages/phages) to destroy antibiotic-resistant pathogens. The use of phages to kill pathogenic bacteria is known as phage therapy. However, similar to antibiotics, bacteria often evolve resistance to phage infection, hindering the therapeutic use of phages. Bacteria have evolved diverse immune systems to defend themselves from phage infections. Understanding bacterial defense mechanisms is of utmost importance for the development of phage therapy as a viable weapon in the fight against antibiotic-resistant bacteria.
Interestingly, central components of antiviral immune systems in vertebrates have evolutionary roots that stem from bacterial phage defense mechanisms. The rapid discovery of novel antiviral immune systems in bacteria is now being leveraged through comparative immunology to discover homologous immune genes in eukaryotes. Through studying antiviral immune systems in P. aeruginosa, we can gain greater understanding of eukaryotic immune systems as well as gain insights into developing efficient phage therapy agents that can overcome bacterial phage defense systems.
Methods Used: To study the role of these systems in phage defense, we will evaluate phage susceptibility when the systems are genetically inactivated and when they are overexpressed. Deletion mutants of the entire Rtc or Pnc systems have been engineered and additional point mutations that inactivate specific domains in the Rtc or Pnc systems are being constructed. The Rtc and Pnc P. aeruginosa mutants will be challenged with different phage species to assess the role of these systems in phage defense.
Summary of Results: Our preliminary data indicate that two putative phage defense systems (Rtc and Pnc) are significantly upregulated in P. aeruginosa 10 minutes post-phage infection, suggesting that they play a role in phage defense. Furthermore, the Rtc system is conserved in eukaryotes and is implicated in numerous cellular processes related to stress response. The Pnc system is involved NAD+ biosynthesis. NAD+ depletion is a conserved anti-viral response, starving the cell of an essential co-enzyme and reducing viral replication.
Conclusions: We hypothesize that Rtc and Pnc are phage defense systems in P. aeruginosa. Understanding how Rtc and Pnc protect P. aeruginosa from viral infection may reveal analogous systems in eukaryotes that may be involved in antiviral immunity. Additionally, this study will have implications that influence our understanding of how pathogenic bacteria persist in the environment, and how they may be treated using phage therapy.
# 48
High Dose Amoxicillin in Pneumococcal Infections: Are teen doses too low or are toddler doses too high?
Stenger KS2, Yamamoto LG2, 1. 1John A. Burns School of Medicine, Honolulu, HI and 2Hawaii Pacific Health, Honolulu, HI
Purpose of Study: Because of increasing pneumococcal Penicillin resistance, The American Academy of Pediatrics Red Book recommended physicians treat patients with pneumococcal infections with high-dose amoxicillin (80-90 mg/kg/day) rather than the standard dose (20-40 mg/kg/day). High dose amoxicillin in children approaches previously typical adult doses beginning at age 4 years which can make clinicians reluctant to exceed “adult doses” in young children.This study aims to examine the disparity of amoxicillin dosing between the ages of children.
Methods Used: A retrospective chart review of patients under 19 years of age prescribed amoxicillin from 2021-2023 from a metropolitan hospital system that includes a pediatric tertiary care center was conducted using a smart query of its data base. The data set started with 5,504 patient encounters consisting of children prescribed Amoxicillin regardless of diagnosis. 369 patient encounters were excluded due to not having weight, dose, or frequency in their chart. We excluded 1,518 patient encouters that had diagnoses that reccomended a low dose. This left 3,617 patients encounters who were diagnosed with either otitis media, sinusitis, or pneumonia which are all infections that align with recommendations of high-dose amoxicillin.
Summary of Results: The 3,617 patient encounters had a mean age of 3.9 years, where 2,562 (71%) were ER patient encounters, and 2,197 (61%) were 1-4-year-old patient encounters. The age distribution is described in Table 1. Of the 13-18-year-olds, 89 (86%) were prescribed a LOW dose of amoxicillin (<40 mg/kg/day). 395 (46%) 5-12-year-olds were prescribed a HIGH dose (>75 mg/kg/day), and for both 1-12 months old and 1-4-year-olds 90% of patients, 416 and 1974 patients respectively received a HIGH dose of amoxicillin. Linear regression demonstrated a significant negative correlation between age/dose (mg/kg/day), and weight/dose (mg/kg/day) as shown in figure 1. There was a significant difference in the mg/kg/day dosing of amoxicillin between the four age groups (Kruskal-Wallis).
Conclusions: Older children are receiving a significantly lower than recommended dose per kilogram of amoxicillin compared to younger age groups for conditions that require high dose amoxicillin. There is a disparity in the dosing of Amoxicillin between age/weight categories.
Frequency of otitis media, sinusitis, and pneumonia, the diagnoses of the high dose condition.
Age
Otitis Media
Sinusitis
Pneumonia
0-12 mos
349
5
122
1-4 y/o
1607
52
611
5-12 y/o
674
49
145
13-18 y/o
78
11
15
Total
2708
117
893
The total number of patient encounters in this data set (3,718) exceeds the grand total (3,617) because some patients had more than one diagnosis.
# 49
Improving Screening for Viral Infectious Disease in the Emergency Department
Hood O1, Buresh C1, 2. 1University of Washington, Seattle, WA and 2Seattle Children’s Hospital, Seattle, WA
Purpose of Study: King County, WA has high rates of HIV and Hepatitis C infection. Many people belong to groups that do not interact with healthcare in usual ways. The University of Washington (UW) is part of the Frontlines of Communities in the United States (FOCUS) Program, an initiative to decrease the stigma of testing and increase screening and linkage to care. In the Emergency Department (ED) setting, we capture vulnerable people who do not receive care elsewhere. Screening this group allows for diagnoses of HIV and HCV that may be missed. The FOCUS Program was implemented across 3 EDs in Oct 2021. Since then, 3 interventions occurred as a means of improving screening: provider education, the implementation of a Best Practice Alert (BPA) in the electronic health record, and ongoing training and updates conducted by email. We evaluate the overall effectiveness of this program, and the utility of these changes in improving screening.
Methods Used: Provider education was initially provided at meetings and by email. The BPA was developed with our IT team. Further education and follow up consisted of presentations at meetings, monthly updates with statistics, encouraging stories, and focusing on educating residents in the ED. Screening among eligible patients during each phase of the implementation process are presented to understand each intervention’s added value.
Summary of Results: Since October of 2021, 14,595 patients were screened for HIV and 6,965 for HCV. 151 HIV+ (1.0%) and 407 HCV+ (5.8%) patients were identified. Prior to the program, 1.3% of eligible patients were screened for HIV and 0.8% eligible patients for HCV. After implementing provider education, screening increased to 3.3% of HIV eligible patients and 2.9% of HCV eligible patients. After optimizing the BPA, screening rates increased to 5.5% for HIV and 5.0% for HCV. Once regular reminders, feedback, and training were implemented by email, screening rates rose to 6.9% for HIV and 10.4% for HCV. We note a 530% increase in HIV screening rate and 1,300% increase in HCV screening rate from baseline. From the onset, 151 individuals have been diagnosed with HIV and 1,032 people have been identified with active HCV. When people test positive for HIV the ED and county health department work to link to care. They have a 95% rate of linking people to care within 12 months of their diagnosis. People with Hepatitis C are contacted by the ED study team and assisted with obtaining treatment if they would like. The overall rate of linkage to care for HCV is 24.2%, comparable to the ranges presented in other studies
Conclusions: Increases in HIV and HCV screening occurred with focused provider education, BPA development, and futher trainings and updates. This has allowed us to find individuals who were previously undiagnosed or out of care and get them linked.
However, screening rates remain between 7-10% of eligible patients. While this compares favorably with national estimates of screening there is room to improve.
# 50
THE ASSOCIATION BETWEEN REGULAR CANNABIS SMOKING AND ORAL HUMAN PAPILLOMAVIRUS INFECTION IN YOUNG ADULTS: A CROSS-SECTIONAL STUDY USING NATIONAL HEALTH AND NUTRITION EXAMINATION SURVEY DATA, 2011-2016
Haynes B1,2, Dipietro J1,2, Ray M1,2, Janetos E1, Marshall L1,2, Andrea S1,2. 1Oregon Health and Science University School of Medicine, Portland, OR and 2OHSU-PSU School of Public Health, Portland, OR
Purpose of Study: Human papillomavirus (HPV) infection is the most common sexually transmitted infection in the U.S. and the incidence rates of HPV-related oropharyngeal cancers in the U.S. have doubled in the last 20 years. While cigarette smoking is a known risk factor for oral HPV infection, it is unknown if smoking cannabis is associated with greater occurrence of oral HPV infections. The objective of this study was to estimate the association between cannabis smoking status and oral HPV infection in U.S. young adults ages 18-30 years and examine whether this association differs by HPV vaccination status.
Methods Used: This cross-sectional study used data from the 2011-2016 cycles of the National Health and Nutrition Examination Survey (NHANES). The analytic sample included 2,696 young adults aged 18-30 years with complete data on all key study variables. Cannabis smoking status was derived from questionnaire and categorized as never (reference), irregular, and regular. Oral HPV status was a laboratory-based binary variable. Multivariable logistic regression models, stratified by HPV vaccination status, were used to test the association between cannabis smoking status and oral HPV infection. Odds ratios (OR) and 95% confidence intervals (CI) were estimated as the measure of association after adjusting for gender and cigarette smoking status.
Summary of Results: The final analytic sample had a mean age of 24.4 (standard error: 0.1) years and most participants were female (50.9%), Non-Hispanic White (59.2%) and unvaccinated against HPV (74.7%). The overall unadjusted prevalence of oral HPV infection was 5.2% (95% CI: 4.1%, 6.5%). Oral HPV infection prevalence was greater among unvaccinated participants (5.8%) than among vaccinated participants (3.4%). Among vaccinated young adults, and compared to those who did not smoke cannabis, those who regularly smoked cannabis had 30% lower odds of oral HPV infection (AOR: 0.7; 95% CI: 0.2, 2.5), and those who irregularly smoked cannabis had 20% lower odds of oral HPV infection (AOR: 0.8, 95% CI: 0.2, 2.7). Among unvaccinated young adults, and compared to those who do not smoke cannabis, those who regularly smoke cannabis had 3.2 times the odds of oral HPV infection (AOR: 3.2; 95% CI: 1.6, 6.3) and those who irregularly smoke cannabis had 1.6 times the odds of oral HPV infection (AOR: 1.6; 95% CI: 0.8, 3.2).
Conclusions: Unvaccinated young adults who regularly smoke cannabis have higher odds of oral HPV infection compared to unvaccinated young adults who do not smoke cannabis. Limited conclusions can be made about associations observed among vaccinated participants due to lack of statistical precision. These findings suggest that smoking cannabis should be further examined in prospective studies as a risk factor for oral HPV infection.
# 51
CHILDHOOD VACCINATION TRENDS IN ZIGUINCHOR, SENEGAL
Stash NI1, Manga N2. 1University of Washington, Seattle, WA and 2Universite Assane Seck, Ziguinchor, Senegal
Purpose of Study: While Senegal has one of the highest rates of early childhood vaccination, they are lacking in later vaccinations. BCG, a vaccine for tuberculosis given in the first week of life, has a 96% vaccination rate in Senegal, while fully vaccinated children only reaches 70%1. Currently, rotavirus, a vaccine-preventable virus that is virtually absent in developed countries, accounts for 5% of childhood fatalities in the country2. Hepatitis B, a virus that increases risk for the often-fatal hepatocellular carcinoma, has a prevalence of 7% in Senegal3. Nema Health Post in Ziguinchor, Senegal, was identified as a clinic with poor late childhood vaccination rates, that needed deeper analysis of their vaccination trends to educate potential improvements.
Methods Used: The head nurse and vaccination coordinator at this health post were consulted in the need for digitization and analysis of their childhood vaccine records. Vaccination records from January 2021 to June 2023 were entered into Excel and analyzed for rates of vaccines completed on time vs at any point for each vaccine as well as rates of partial or full completion of the WHO-advised childhood series. Results were presented to the local team and improvements were discussed.
Summary of Results: 2021 and 2022 had early, on time vaccine rates (polio, TB, Hep B) at 82% and later vaccines (Rubella, Measles and Yellow Fever) at 22%. When adjusted for recording lapses and transfers to other health posts, rates were 94% for early vaccines and 54% for late vaccines given on time. These numbers were slightly higher at 96% and 62%, respectively, when vaccines given late were included.
Conclusions: Several vaccine rates were lower than the 2019 WHO national average and can mainly be attributed to barriers that arose over the past two years, such as the government halt on the rotavirus vaccine, and recording errors. When adjusting for the several reasons that caused reduced real and/or recorded vaccination rates, Nema Health Post in Ziguinchor had comparable rates to the national average. Consistency in recording methods was a major barrier for copying over accurate records into excel, and likely caused some rates to appear lower than their actual level. Going forward, this area would benefit from all medical centers having digitized vaccination records so that vaccines can be more efficiently provided and accurately analyzed.
# 52
EPIDEMIOLOGY AND RISK STRATIFICATION OF YOUNG INFANTS PRESENTING TO THE EMERGENCY DEPARTMENT WITH HYPOTHERMIA
Wang M1, Trehan I2. 1University of Washington, Seattle, WA and 2University of Washington, Seattle, WA
Purpose of Study: Hypothermia in infants can indicate a serious bacterial infection (SBI) (i.e., urinary tract infection (UTI), bacteremia, bacterial meningitis) or herpes simplex virus (HSV) infection, which can be fatal if left undiagnosed and untreated. However, no national guidelines exist regarding the management of hypothermic infants in the emergency department (ED), resulting in considerable variation in care across providers and centers. We aimed to investigate factors associated with the level of diagnostic workup performed for infants ≤90 days of age experiencing hypothermia (rectal temperature ≤36.5° C) in the ED. We also attempted to investigate risk factors for SBIs and/or HSV infection in these patients.
Methods Used: We conducted a single-center study over a 10-year period involving infants ≤90 days of age with hypothermia in the ED, excluding patients who were febrile during their ED visit. The primary outcome was the type of diagnostic testing ordered in the ED. Secondary outcomes were the occurrence of SBI and/or HSV infection. We used Fisher’s exact test to identify clinical and demographic factors associated with the primary and secondary outcomes, reporting odds ratios with 95% confidence intervals (OR, 95% CI).
Summary of Results: Of the 1,095 patients identified, 402/1,095 (36.7%) underwent testing for a SBI and/or HSV infection. A minimum temperature in the ED below 36° C (2.775, 2.156 – 3.582; p = <0.0001) compared to 36 – 36.5° C, as well as hospital / ICU admission (6.181, 4.436 – 8.567; p = <0.0001) compared to discharge home were associated with increased testing. Among the patients who underwent SBI and/or HSV testing, 34/402 (8.46%) had a SBI and/or HSV infection. Specifically, 4/107 (3.74%) of patients with HSV testing tested positive, 7/326 (2.15%) of patients with a blood culture had bacteremia, and 27/326 (8.28%) of patients with a urine culture had a UTI. 0/193 (0.00%) of patients with a cerebrospinal fluid culture had bacterial meningitis. 4 patients had concurrent UTI and bacteremia. No specific risk factors were identified for positive infectious studies.
Conclusions: Hypothermic infants appear to have slightly lower rates of SBI and HSV than febrile infants, for whom infectious studies are widely recommended. Nevertheless, the rates of infection in hypothermic infants are arguably still higher than the threshold needed to warrant widescale testing. Further research is required to risk stratify hypothermic infants in the ED to standardize care and improve outcomes while minimizing excessive testing.
Neonatology General I
Concurrent Session
12:45 PM
Thursday, January 18, 2024
# 53
AIRWAY COLONIZATION AND RISK FACTORS FOR DEVELOPMENT OF BRONCHOPULMONARY DYSPLASIA IN INTUBATED VERY LOW BIRTH WEIGHT INFANTS
Huang J1, 2, Cielo M3, 2, Ramanathan R1, 2, CAYABYAB R1, 2. 1Los Angeles General Medical Center, Los Angeles, CA; 2Keck School of Medicine of University of Southern California, Los Angeles, CA and 3Los Angeles General Medical Center, Los Angeles, CA
Purpose of Study: Bronchopulmonary dysplasia (BPD) is commonly seen in very low birth weight (VLBW) infants. Pathogenesis of BPD is multifactorial. Bacterial airway colonization and infection of lower respiratory tract have been suggested as important factors in the pathogenesis of BPD. The objectives of this study were to characterize patterns of airway colonization of intubated VLBW infants from routine tracheal aspirate (TA) cultures and to identify risk factors, including the type of bacterial colonization associated with BPD.
Methods Used: A retrospective study of all VLBW infants with gestational age (GA) less than 32 weeks on invasive mechanical ventilation (IMV) for ≥ 1 week admitted to Los Angeles General Medical Center NICU from July 2015 to July 2021 who had routine TA cultures were included in this study. Neonatal and maternal demographics, clinical course, antibiotic use, radiology reports, laboratory results, and TA culture results were collected from electronic health record. Clinical outcomes collected included diagnosis of ventilator associated pneumonia (VAP) and BPD, which was defined as the need for positive respiratory support at 36 weeks postmenstrual age regardless of supplemental oxygen use. We used the following definitions for BPD severity: Grade 1: Nasal Cannula Flow ≤2 L/min; Grade 2: Nasal Cannula Flow >2 L/min or non-invasive ventilation; Grade 3: IMV. Neonates were classified into 2 groups: no BPD/Grade 1 BPD, and Grade 2/Grade 3 BPD.
Summary of Results: A total of 62 intubated VLBW infants met inclusion criteria with a mean GA of 25.8 ± 1.8 weeks and a mean BW of 748 ± 248 grams. Majority of infants 39 (63%) were intubated at birth and mean duration of IMV was 33.5 ± 16 days. The first positive culture occurred with gram positive bacteria (GPB) in majority of the infants at median day 9 post-intubation followed by gram negative bacteria (GNB) at median day 13 post-intubation. There were 35 infants with no BPD/Grade 1 BPD and 27 infants with Grade 2/Grade 3 BPD. Infants with Grade 2/Grade 3 BPD were more likely to be male, had lower 5 minute APGAR, received repeat doses of surfactant, exposed to longer duration of antibiotics, higher rate of VAP, dexamethasone use, acetaminophen use for medical management of hemodynamically significant patent ductus arteriosus (hsPDA), surgical ligation of hsPDA, longer duration of IMV, and longer length of stay (LOS). There was no significant difference in bacterial airway colonization between the two groups (Table).
Conclusions: Majority of intubated VLBW infants were initially colonized with GPB followed by GNB at two weeks post-intubation. Development of Grade 2/Grade 3 BPD was associated with longer exposure to antibiotic use likely related to treatment of underlying infection, longer duration of presence of hsPDA, prolonged duration of IMV, and longer LOS. There was no difference in airway colonization pattern observed in infants who developed more severe form of BPD versus absent or mild BPD.
Neonatal characteristics, risk factors and outcomes of the study population.
No BPD/Grade 1 BPD (n=35)
Grade 2/Grade 3 BPD (n=27
P-value
Gestational age (weeks) *
26.0 (24.6-26.7)
25.3 (24.1-26.6)
0.22
Birth weight (g)*
760 (644-910)
630 (525-840)
0.06
Male, n (%)
12 (34.3)
18 (66.7)
0.01
Cesarian section, n (%)
32 (91.4)
21 (77.8)
0.16
Apgar at 1 minute*
4 (1-5)
2 (1-4)
0.11
Apgar at 5 minute*
7 (5-7)
5 (2-7)
0.02
Number of surfactant dose received*
2 (1-2)
3 (2-3)
<0.01
Postnatal use of dexamethasone, n (%)
18 (51.4)
22 (81.5)
0.01
Total antibiotic days during NICU stay*
20 (15-34)
30 (20-45)
0.01
Patent ductus arteriosus, n (%)
33 (94.3)
24 (88.9)
0.65
Indomethacin treatment for hsPDA, n (%)
21 (60.0)
17 (63.0)
0.81
Indomethacin treatment for hsPDA (≥ 2 courses), n (%)
8 (22.9)
9 (33.3)
0.36
Acetaminophen treatment for hsPDA, n (%)
15 (42.9)
17 (63.0)
0.12
Acetaminophen treatment for hsPDA (≥ 2 courses), n (%)
1 (2.9)
8 (29.6)
<0.01
Patent ductus arteriosus ligation, n (%)
6 (17.1)
14 (51.9)
<0.01
Ventilator associated pneumonia , n (%)
5 (14.3)
9 (33.3)
0.045
Length of intubation (days)*
27 (13-35)
43 (35-53)
<0.01
Number of reintubations*
2 (2-2)
3 (2-3)
0.04
Tracheal aspirate growth
0.65
No growth, n (%)
3 (8.6)
3 (11.1)
Gram positive, n (%)
16 (45.7)
10 (37.0)
Gram negative, n (%)
2 (5.7)
0 (0)
Mixed gram positive and negative, n (%)
10 (28.6)
8 (29.6)
Other bacteria or fungi, n (%)
4 (11.4)
6 (22.2)
Length of NICU stay (days)*
106 (84-114)
128 (113-149)
<0.01
Disposition
0.11
Discharge, n (%)
33 (94.3)
21 (77.8)
Expired, n (%)
0 (0)
2 (7.4)
Transferred out, n (%)
2 (5.7)
4 (14.8)
hsPDA, hemodynamically significant patent ductus arteriosus. *Data reported as median (interquartile range).
# 54
PRESSURE TRANSMISSION ON BI-NASAL (RAM) CANNULA WITH T-PIECE RESUSCITATOR
Kim S1, 2, Ramanathan R1, 2, Biniwale M1, 2. 1Los Angeles General Medical Center, Los Angeles, CA and 2Keck School of Medicine of USC, Los Angeles, CA
Purpose of Study: There are various nasal interfaces for positive-pressure ventilation in the delivery room for neonates, including face masks, bi-nasal cannulas, and laryngeal masks, but pressures delivered at the level of the infant is unclear with these interfaces. In an institution that uses Ram (bi-nasal) cannulas as first-line for resuscitation, the objective of this study was to measure the difference in pressures set on the t-piece resuscitator versus the pressures generated at the level of the prongs.
Methods Used: A physiologic model of neonatal patient nares and lungs with a digital manometer was used to measure the pressure at the level of the Ram cannula prongs with varying cannula sizes. Pressures read by the manometer were recorded at various pressures and flow set on the panda resuscitator. Difference in pressures and correlation between the pressures set and actual pressures delivered at nares were assessed.
Summary of Results: Pressure testing was performed in 300 observations with peak inspiratory pressures (PIP) set at various intervals from 20-40 cm H20 and positive end expiratory pressures (PEEP) set from 5 to 8 cm H20. Mean difference between set PIP and measured PIP was similar at various pressure levels (mean diff 0.02, SD 0.84, P= 0.69). Correlation coefficient between the measured and set PIP was 0.99. While measured PEEP read significantly lower than set PEEP (mean diff 1.96, SD 0.4, P<0.01), there was a strong correlation (0.94) between the measured and set PEEP indicating consistent difference at various PEEP levels. figure 1 shows similar differences in observed PEEP compared to set PEEP at difference sizes of RAM cannula.
Conclusions: While PIP at the level of the prongs is close to set PIP, PEEP may be lower than PEEP set on the resuscitator. However, pressures at the level of the prongs consistently correlated with pressures set on the resuscitator for all cannula sizes, pressures, and flow rates. Clinicians may need to take this into consideration when applying nasal cannula for performing resuscitation in newborn infants.
# 55
Low sodium maternal diet impairs the effective immune response to neonatal sepsis in a murine model
Jones J1, Cera A2, Bautista G2, Grobe J3, Segar J3, McElroy S2. 1UC Davis, Sacramento, CA; 2UC Davis, Sacramento, CA and 3Medical College of Wisconsin, Milwaukee, WI
Purpose of Study: Premature infants are at increased risk of hyponatremia due to underdeveloped kidney function. Limited clinical studies to date suggest that oral sodium supplementation leads to improved growth in premature infants. Additionally, oral sodium supplementation may decrease the incidence of sepsis and necrotizing enterocolitis (NEC). In vitro studies found that sodium plays a regulatory role within the immune system, with high sodium levels promoting a pro-inflammatory response. Whether sodium levels alter the immune response in neonatal sepsis is not understood. Our objective was to determine if reducing total body sodium increased the mortality rate and severity of gut injury in a murine model of neonatal sepsis.
Methods Used: Pregnant dams were given regular chow or low sodium chow starting at e18 (0.15% and 0.04% Na, respectively). Naturally delivered pups were nursed until P7, when neonatal sepsis was induced using a previously validated model. Pups were injected with 10 x 10^7 CFU/ml NECteria (enteric bacteria derived from an infant that died of NEC totalis) or sterile normal saline and followed for survival. Upon death or at 12 hours, pups were sacrificed, and serum and intestinal samples were obtained. Intestinal cytokine levels were quantified, and gut injury score was determined using a validated 3-point injury scale.
Summary of Results: While not statistically significant, there was a trend (p=0.10) towards decreased survival among sepsis-exposed pups fed a low sodium diet versus sepsis-exposed pups fed a regular diet. Sepsis-exposed pups fed a low sodium diet showed a similar injury score to sepsis-exposed pups fed a regular diet (median score 2 and 2). Low sodium sepsis pups had statistically significant lower expression of, IFNγ (11.2pg/ml vs 5.7pg/ml, p=0.01), IL-1a (37.2pg/ml vs 16.44mg/ml, p=0.03),IL-3 (2.0pg/ml vs 0.7pg/ml, p< 0.01), , IL-9 (12.3pg/ml vs 4.3pg/ml, p<0.03), IL-10 (19.0pg/ml vs 5.6pg/ml, p=0.04), , IL-13 (15.9pg/ml vs 0.9 pg/ml, p<0.05), RANTES (138.1pg/ml vs 61.5pg/ml, p=0.05), and TNF (14.2pg/ml vs 7.7pg/ml, p=0.03) compared to sepsis-exposed pups on a regular diet.
Conclusions: Sepsis-exposed pups receiving low sodium dam milk had decreased survival rates with a depressed cytokine response compared to pups nursed on a regular diet. These results suggest that sodium may be critical in mounting an appropriate inflammatory response in neonatal sepsis. Future studies are needed to understand these mechanisms.
# 56
PARENTAL PERCEPTIONS OF DISCHARGE READINESS FOR INFANTS WITH SEVERE BRONCHOPULMONARY DYSPLASIA: NICU SUPPORT, INFANT AND PARENT WELL-BEING, AND PARENTAL COMFORT
Hannan KE, Bourque SL, Sherlock L, Wymore E, Kinsella J, Mandell E, Houin S. University of Colorado, Aurora, CO
Purpose of Study: The clinical courses of extremely premature infants who develop severe bronchopulmonary dysplasia (BPD) consist of complex medical care and prolonged NICU stays. Both consistent provider teams and parental engagement are seen as key elements of their ongoing care and thus dedicated BPD clinical teams have been created. However, despite the perceived benefits of this model of coordinated care, little is known about the short and long-term outcomes. We seek to longitudinally assess medical and sociobehavioral outcomes, including discharge readiness and parental wellbeing, among these high-risk infants and their families.
Methods Used: This prospective cohort study, beginning in 2022, includes infants born at <29 weeks requiring high respiratory support at 4-6 weeks of age, cared for on the BPD clinical team in a Level IV regional children’s hospital NICU. We assessed demographic and clinical data from the electronic medical record and through surveys during and after birth hospitalization. Surveys prior to NICU discharge include the Fragile Infant Parental Readiness Evaluation (FIPRE), a validated quality measure of parent outcomes and perceptions of NICU-discharge readiness. Scores are converted to a standard 0-100 metric, with scores <75 representing unfavorable outcomes.
Summary of Results: To date, 18 families have completed the NICU survey. Average gestational age was 25 weeks, all infants required discharge respiratory support (nasal cannula to chronic mechanical ventilation), and 94% required a home feeding tube. Families indicated overall positive NICU experiences and receipt of support while in the NICU with 11% of scores <75 for FIPRE NICU Support questions (Table 1). Mean score for feelings of infant well-being was 74.1. Parental well-being scores and comfort scores were low (mean scores 57.9 and 56.8 respectively, Table 1). Additionally, 89% of families reported that caring for their baby at home would limit the time they have for themselves, their families, and their friends.
Conclusions: Our cohort of infants with severe BPD have ongoing medical needs and technology dependence including high prevalence of home mechanical ventilation and tube feeding at discharge. Despite the medical complexity of these infants, families indicated positive experiences in the NICU and overall readiness for discharge. However, parental comfort and emotional readiness for NICU discharge was low. Further analyses of this high-risk population is crucial to inform pre-discharge care practices and interventions to improve outcomes and assess effects on long-term healthcare utilization. Specific focus on programs supporting parental comfort and well-being as they prepare for discharge are indicated.
# 57
EVALUATING PRACTICE CONSISTENCY: COMPLYING WITH THE DIRECTIVE TO OBTAIN UMBILICAL CORD ARTERIAL AND VENOUS BLOOD GASSES, AND HEMOGLOBIN VALUES AT HIGH-RISK DELIVERIES
Tweddell SM1, Bahr TM1, 2, Ohls RK1, Christensen RD1. 1University of Utah, Salt Lake City, UT and 2Intermountain Health, Salt Lake City, UT
Purpose of Study: Using Intermountain Health multi-hospital data, we quantified compliance with the American College of Obstetricians and Gynecologists directive to obtain umbilical cord arterial and venous blood gasses at high-risk deliveries. We also quantified compliance with our local directive to obtain a hemoglobin with the cord gasses as an early screen for anemia.
Methods Used: Retrospective 24-month analysis of Intermountain Health deliveries.
Summary of Results: One-thousand-fifty births had ‘placental abruption’ mentioned in the peripartum notes. These constituted our high-risk delivery cohort. Of these, 726 (69%) had both a cord arterial and venous sample reported; 707 (67%) also had hemoglobins reported. In 86 (8%) only one (arterial or venous) was reported, and 293 (23%) had neither gasses nor hemoglobins. One-hundred-seven of the 726 had acidosis (cord arterial pH <7.13) and 619 did not (pH ≥7.13). Among those with acidosis, 82 had abruption confirmed after birth; in 25 abruption was not confirmed. Paired umbilical arterial vs. venous hemoglobin levels revealed the novel observation that umbilical venous hemoglobins are slightly lower than arterial (p<0.0001), perhaps due to maternal-to-fetal acellular fluid transfer. Among the 707 that had a cord hemoglobin reported, fetal/neonatal anemia was diagnosed in 83 (12%) neonates (defined as a hemoglobin below the 5th percentile lower reference interval for gestational age).
Conclusions: We see an opportunity to improve compliance with the directives to obtain cord arterial and venous blood gas and hemoglobin at high-risk births. Doing so will allow rapid evaluation of about 30% more high-risk infants for the presence of acidosis and anemia at birth.
Table 1. Umbilical cord arterial and venous blood gas determinations and hemoglobin levels from n=1050 births where placental abruption was suspected before birth. Success in obtaining these laboratory tests is compared between the group where abruption wa.
Umbilical cord blood gas and Hgb measurements (n and % of total)
Neonates where abruption was suspected, but not confirmed at birth (n=372)
Neonates born after confirmed placental abruption.
(n=678)
P value
Both arterial and venous cord gas
226 (60.8%)
500 (73.7%)
<0.001
Arterial gas only
13 (3.5%)
19 (2.8%)
<0.001
Venous gas only
12 (3.2%)
42 (6.2%)
<0.001
Neither arterial or venous gas
121 (32.5%)
172 (17.3%)
<0.001
Both arterial and venous hgb
222 (59.6%)
485 (71.5%)
<0.001
Arterial hgb only
8 (2.2%)
19 (2.8%)
<0.001
Venous hgb only
10 (2.7%)
43 (6.3%)
<0.001
Neither arterial or venous hgb
132 (35.5%)
131 (19.3%)
<0.001
hgb, blood hemoglobin concentration.
# 58
NEONATAL INPATIENT STAYS LONGER THAN 1 YEAR: WHO WAS ADMITTED, WHAT HAPPENED, AND HOW MUCH DID IT COST?
Shah ND, Dapaah-Siakwan F. Valley Children’s Healthcare, Madera, CA
Purpose of Study: Anecdotal evidence exists that some preterm infants remain hospitalized for more than a year in the Neonatal Intensive Care Unit (NICU) but no study has formally examined this population. Our primary objective was to describe the characteristics and hospital course for preterm hospitalizations requiring length of stay (LOS) ≥365 days. The secondary objective was to determine the inflation-adjusted hospital cost and predictors for NICU LOS ≥ 365 days.
Methods Used: This was a retrospective, cross-sectional analysis of the 2016 and 2019 Kids Inpatient Database (KID). The KID is the largest publicly available all-payer pediatric inpatient care database in the United States and it contains about 7 million weighted hospitalizations each year. ICD-10 codes were used to identify preterm infants, their comorbidities and surgical interventions. Transfers were excluded to avoid double counting. The study population was dichotomized into LOS ≤364 days (PT364) and LOS ≥365 days (PT365) and compared using Chi-square or Wilcoxon ranked sum test as appropriate. The exposure variable was PT365 and the outcomes of interest were the characteristics, co-morbidities, discharge disposition, and inflation-adjusted hospital costs. Multivariable linear regression was performed to identify the predictors of LOS ≥365 days. P=value <0.05 was considered significant.
Summary of Results: Among 688,995 preterm neonates, 688,884 had LOS < 364 days and 111 had LOS > 365 days (0.016%). Compared to PT364, PT365 were more likely to be males (74.6% vs 53.2%), have gestational age (GA) < 27 weeks (71.5% vs 4.7%), be born via vaginal delivery (78.5% vs 54.1%), have birthweight < 1000 g (64.2% vs 4.0%), have Medicaid 75.2% vs 51.5%), and be cared for in urban teaching hospitals (98.5$ vs 79.8%). Similarly, PT365 were more likely to have a higher prevalence of comorbidities in each organ system (Table 1), surgical and procedural interventions, and neonatal complex chronic conditions (872% vs 13.3%). PT365 were less likely to be discharged home (45.7% vs 93.4%) and more likely to be discharged to home health care (28.0% vs 5.7%) or to skilled nursing facility (16.0% vs 0.8%). In multiple linear regression, tracheostomy placement (odds ratio (OR) 98.3, 95% confidence interval (CI) 38.47-251.16), neonatal chronic complex conditions (OR 4.86, 95% CI: 1.74 – 3.55), and bowel resection (OR 2.80, 95% CI: 1.02 – 7.65) were the predictors of LOS ≥365 days. The mortality rate was 10.3% for PT365. The median hospital cost per surviving PT365 was $1,616,336 as opposed to only $9,868 per surviving PT364.
Conclusions: PT365 was rare but was associated with complex chronic conditions, increased morbidity and surgical burden, and inflation-adjusted hospital cost. The predictors of LOS ≥ 365 days can serve as targets for quality improvement efforts to decrease LOS. The data on hospital cost can serve as the basis for the payment of the cost of inpatient care for these infants.
Bivariate Commparison of the Hospital Course and Morbidities between preterm infants with LOS ≤ 364 days and LOS ≥ 365 days.
+Chronic complex condition was as any medical condition expected to last at least 12 months, involving either several organ systems or one organ system with sufficient severity to require special pediatric care and, probably, some period of hospitalization in a tertiary care center. The neonatal version define by Feudtner et al was used (Feudtner, C., Feinstein, J.A., Zhong, W. et al. Pediatric complex chronic conditions classification system version 2: updated for ICD-10 and complex medical technology dependence and transplantation. BMC Pediatr 14, 199 (2014). https://doi.org/10.1186/1471-2431-14-199.
# 59
Incidence of Gastroschisis in the United States from 2015-2021
Cera A, Bautista G. UC Davis, Sacramento, CA
Purpose of Study: Gastroschisis is a complex and costly birth defect in which the fetal intestine, without any protective membrane or sac, herniates through the abdominal wall, resulting in free floating intestine surrounded by amniotic fluid in the uterine cavity. Prognosis depends on the status of the bowel at the time of delivery which can become significantly inflamed or matted. Infants with gastroschisis require prolonged hospital stays, often have feeding difficulties, may encounter growth failure, or require long term parenteral nutrition. Previous research shows an overall increasing incidence of gastroschisis in the United States and Canada over the past decade with unclear etiology. The goal of this project was to determine the trend in gastroschisis incidence in the United States (US).
Methods Used: This is a retrospective review of the incidence of gastroschisis in the US from 2015-2021 using publicly available birth data via the CDC WONDER public health database. This database is derived from birth certificate data for births to US residents occurring in the US.
Summary of Results: The overall incidence (cases per 10,000 live births) of gastroschisis decreased during the study period from 2015 (2.70) through 2021 (1.88). Gastroschisis incidence was higher amongst mother’s with Medicaid (3.23) vs those with private insurance (1.38) or those who self paid (1.37). Gastroschisis incidence was also higher amongst mothers living in nonmetro areas (3.40 cases) vs mothers living in metro areas (2.04). Finally, the incidence of gastroschisis was greatest in the Midwest, followed by the West (2.36), the North East (1.94) and the South (1.86).
Conclusions: The incidence of gastroschisis is down trending in the US over the study period 2015-2021. The higher incidence of gastroschisis amongst mother’s with Medicaid, and those living in nonmetro areas prompts further consideration of whether socioeconomic factors, including environmental factors, may be contributing to variation in gastroschisis incidence.
# 60
ASSESSMENT OF ANTIBIOTICS USAGE TRENDS IN NICU PATIENTS WITH HYPOXIC-ISCHEMIC ENCEPHALOPATHY: OPPORTUNITIES FOR QUALITY IMPROVEMENT
Manjunath C1, Manjunatha H2, Ngo L1. 1Loma Linda University Children’s Hospital, Loma Linda, CA and 2Georgia Institute of Technology, Atlanta, GA
Purpose of Study: Assessment of antibiotic stewardship opportunities for NICU patients with hypoxic-ischemic encephalopathy (HIE) who received therapeutic hypothermia (TH) treatment at Loma Linda University Hospital (LLUH). The study subtasks are: 1) Identify the demographics and characterization of HIE infants. 2) Assess the utilization of antimicrobial therapy in newborns with HIE who underwent TH.
Methods Used: The subjects include newborns admitted to LLUH with the diagnosis of HIE and who received TH therapy. Retrospective data is obtained from our TH quality improvement database. We evaluated demographics, delivery room information, antibiotic treatment duration, and associated morbidities. Antibiotic usage pattern was stratified into four groups. Negative sepsis (NS): infants with sepsis rule out with antibiotics use for ≤ 2 days. Culture negative sepsis- limited antibiotic (CNS-L): infants treated with antibiotics for 3 - 6 days with negative cultures. Culture negative sepsis-empiric antibiotic (CNS-E): infants treated with antibiotics for > 7 days with negative cultures. Culture positive sepsis (CPS): infants with positive blood cultures who received a treatment course of antibiotics.
Summary of Results: A total of 98 (31 inborn and 67 outborn) patients underwent TH from Jan 2021 to Dec 2022. (2021 n= 51 and 2022 n= 47). Patient stratification resulted in the following number of patients, NS n=38, CNS-L n=18 CNS-E n=41, and CPS n=1. Statistical analysis was between the NS, CNS-L, and CNS-E groups. There were no significant differences between gestational age, gender, race, birth weight, birth location, delivery method, Apgar scores at 5 and 10 minutes, HIE severities, need for ECMO, or death. There were significant differences with the CNS-E group having a higher number of patients with hemodynamic instability (p <0.05) and a lower 1-minute APGAR score in comparison to the other groups. None of the groups for NS, CNS-L, and CNS-E needed to resume antibiotics following discontinuation.
Conclusions: The median duration of antibiotics usage in HIE infants with TH in our patient population was approximately 5 days; however, the highest number of patients were in the empiric group who were treated for > 7 days. There was no significant variation in antibiotic usage between 2021 and 2022 indicating a need for quality improvement studies. In our population, there was no re-initiation of antibiotics in the limited antibiotics and sepsis ruled out groups. These findings suggest an opportunity for antibiotic stewardship among infants who undergo TH for HIE.
Demographics and characteristics of HIE population who underwent therapeutic hypothermia.
Factors
All
Culture Positive Sepsis
Negative Sepsis
Culture negative sepsis - Limited Antibiotic
Culture Negative Sepsis - Empiric Antibiotics
p-value
N
98
1
38
18
41
-
Antibiotic Duration Median [IQR]
4.5 [2,7]
40
2 [2,2]
4 [3,6]
7 [7,9]
-
Gestational Age Median [IQR]
39 [37,40]
35
39 [37,39]
39 [37,40]
40 [39,40]
0.06
Birth Weight in grams, Median [IQR]
3404 [3015,3779]
2255
3388 [3063,3849]
3273 [2940,3890]
3440 [2985,3660]
0.92
Gender (n, %)
-
-
-
-
-
0.10
Female
38 (38.8)
1 (100)
15 (39.5)
3 (16.7)
19 (46.3)
Male
60 (61.2)
0
23 (60.5)
15 (83.3)
22 (53.7)
Maternal Race (n, %)
-
-
-
-
-
0.70
Asian
6 (6.1)
0
2 (5.3)
2 (11.1)
2 (4.9)
Black
11 (11.2)
1 (100)
4 (10.5)
4 (22.2)
2 (4.9)
Hispanic
60 (61.2)
0
25 (65.8)
7 (38.9)
28 (68.3)
While
14 (14.3)
0
5 (13.2)
2 (11.1)
7 (17.1)
Other/unknown
7 (7.1)
0
2 (5.3)
3 (16.7)
2 (4.9)
Birth Location (n, %)
-
-
-
-
-
0.62
Inborn
31 (31.6)
0
10 (26.3)
6 (33.3)
15 (36.6)
Outborn
67 (68.4)
1 (100)
28 (73.7)
12 (66.7)
26 (63.4)
Delivery Method (n, %)
-
-
-
-
-
0.35
C-section
64 (65.3)
0
26 (68.4)
14 (77.8)
24 (58.5)
Vaginal
20 (20.4)
1 (100)
9 (23.7)
1 (5.6)
9 (22)
Vaginal Assisted
14 (14)
0
3 (3)
3 (3)
8 (8)
Apgar Score [IQR]
-
-
-
-
-
<0.05
1 Minute
1 [1,2; N= 95]
0
2 [1,2; N= 37]
2 [1,2; N= 18]
1 [1,2; N= 40]
0.24
5 Minute
4 [2,5; N= 94]
0
4 [2,5; N= 37]
3 [2,5; N= 17]
4 [3,6; N= 40]
0.37
10 Minute
5 [3,7; N= 88]
0
5 [2,6; N= 36]
6 [3,6; N= 16]
5 [3,7; N= 36]
Encephalopathy Severity (n, %)
-
-
-
-
-
0.86
Mild
11 (11.2)
0
5 (13.2)
1 (5.6)
5 (12.2)
Moderate
67 (68.4)
1 (100)
26 (68.4)
13 (72.2)
27 (65.9)
Severe
17 (17.3)
0
6 (15.8)
3 (16.7)
8 (19.5)
Unknown
1 (1)
0
1 (2.6)
0 (0)
0 (0)
Morbidities
-
-
-
-
-
<0.05
Hemodynamic Instability (n, %)
30 (30.6)
1 (100)
6 (15.8)
6 (33.3)
17 (41.5)
ECMO (n, %)
6 (6.1)
0
0 (0)
1 (5.6)
5 (12.2)
0.08
Death (n, %)
6 (6.1)
1 (100)
3 (7.9)
1 (5.6)
1 (2.4)
0.55
Antibiotics resumed with 7 days of discontinuation (n, %)
1 (1)
1(100)
0 (0)
0 (0)
0 (0)
-
Antibiotic usage pattern in year 2021 and 2022 respectively.
# 61
LESSONS LEARNED FROM ROUTINE PERINATAL MENTAL HEALTH SCREENING IN A NEONATAL INTENSIVE CARE UNIT
Swenson SA1, Wilton DA1, Skalland B1, Kroupina M1, Osterholm EA1, 2, Paulsen M1, 2, Lampland AL3, 1, Downey AG3. 1University of Minnesota Medical School, Minneapolis, MN; 2M Health Fairview Masonic Children’s Hospital, Minneapolis, MN and 3Children’s Minnesota, Saint Paul, MN
Purpose of Study: The 2023 American Academy of Pediatrics (AAP) standards of neonatal care include screening parents of infants in neonatal intensive care units (NICU) for depression. Gaps regarding optimal screening practices remain. We implemented perinatal mental health (MH) screening as part of a quality improvement project with the goal of achieving at least 70% completion for parents whose infants remained hospitalized at 1, 2, 4 and 6 months, consistent with the AAP-recommended intervals for postpartum depression (PPD) screening at well visits. Here, we highlight lessons from 6 months of screening compared to baseline.
Methods Used: A multidisciplinary team at a level IV NICU developed a driver diagram and screening algorithm. Referrals based on clinical interactions alone were tracked for 6 months prior to screening. In the screening period (October 2022-April 2023), the social work team used the Edinburgh Postpartum Depression Scale (EPDS) and anxiety subscale (EPDS-3A) with an EPDS threshold of 10 for gestational parents (GP) and 8 for non-gestational parents (NGP) and an EPDS-3A threshold of 4. Scores above threshold prompted referrals to MH or primary care providers. Measures included rate of parents undergoing screening, rate of parents above screening threshold, and perceptions of screening.
Summary of Results: In the pre-screening period, 58 referrals were made (GP 95% v. NGP 5%), with the majority (73%) occurring during the first week after admission to parents that did not have established MH providers (78%). In 6 months, 192 parents were screened (105 GP, 87 NGP) of 257 eligible parents (133 GP, 124 NGP). The median screening completion rate per week was 78% (80% GP, 75% NGP). 58 parents were referred due to positive screen (GP 70% v. NGP 30%). Positive screen rates were 34%, 28%, 55%, and 67% at 1, 2, 4, and 6 months. 77% of parents referred did not have established MH providers. An average of 27 parents were screened each month (average 8 screens due per week; average unit census 60). 30% of screens were positive (range 20-47% per month) with the highest percent positive in January. The average EDPS score was 6.5 (7.3 GP, 5.2 NGP, range 0-22). The average EDPS-3A score was 2.9 (3.3 GP, 2.1 NGP, range 0-9 GP, 0-7 NGP). Anxiety screening detected additional MH concerns in GP (NNT = 9) but not NGP. Screening was identified as valuable by 92% of parents and 100% of physicians and social workers.
Conclusions: Lessons learned through routine perinatal MH screening in the NICU are multiple. First, NGP have MH concerns that are better detected through screening than clinical interactions. Second, clinical interactions most often detect MH concerns within 1 week of admission but may miss concerns that develop later in the stay. Third, parents of infants with NICU stays ≥4 months are at highest risk for MH symptoms and may be missed if screening only occurs shortly after admission. Last, it is important to screen for symptoms beyond PPD.
Neonatology Pulmonary I
Concurrent Session
12:45 PM
Thursday, January 18, 2024
# 62
Postnatal Growth Restriction and DHA Supplementation Reduce Lung Perilipin Expression in Association Sex-Divergent Changes in PPARγ Activity
Chidester W1, Bitsui CT1, Parikh A1, Maschek A2, Cox J2, Joss-Moore L1. 1University of Utah, Salt Lake City, UT and 2University of Utah, Salt Lake City, UT
Purpose of Study: Determining the appropriate complement of lipid supplementation for preterm neonates is challenging. The incidence and severity of bronchopulmonary dysplasia (BPD) increases in preterm neonates deficient in the fatty acid docosahexaenoic acid (DHA). However, at least in some subgroups, DHA supplementation appears to worsen BPD. One way intrapulmonary lipids affect outcomes in the developing lung is via activation of PPARγ, which governs the expression of downstream target genes critical for lung development, such as perilipin2 (Plin2). We previously showed in a rat model that postnatal growth restriction (PGR) produces lung structure/function changes similar to BPD in both male and female pups and decreased circulating DHA in male pups. We also showed that PPARγΔ5, a dominant-negative isoform of canonical PPARγ (cPPARγ), is expressed in the lung. However, how PGR and DHA affect rat lung cPPARγ, PPARγΔ5, and target gene Plin2 mRNA expression is unknown.
We hypothesize that PGR and DHA will reduce levels of Plin2 and alter the relative expression of cPPARγ and PPARγΔ5 in rat lung.
Methods Used: PGR was induced by randomizing newborn rat pups into litters of 8 (control) or 16 (PGR). Each PGR litter was randomized to receive diets supplemented with DHA at 0.0% (regular diet), 0.01% (LoDHA), or 0.1% (HiDHA). At postnatal day 21, rat pups were euthanized and lung collected. Levels of Plin2, cPparγ, and PparγΔ5 mRNA measured. Differences were assessed using ANOVA with Fishers LSD.
Summary of Results: Rat pups in the PGR group weighed significantly less than control by postnatal d5 and continued to weigh less through d21 on all diets. In males, PGR with regular diet did not alter Plin2 mRNA. However, PGR with both does of DHA decreased Plin2 mRNA by 30% in PGR+LoDHA and 50% in PGR+HiDHA groups. In male rat lung, cPparγ mRNA was unaffected by PGR or PGR+LoDHA, but was decreased 35% by PGR+Hi DHA. PparγΔ5 was increased 66% by PGR and PGR with both DHA doses. In female rat lungs, PGR also decreased Plin2 mRNA in females by 27%, and DHA further decreased levels. In female rat lung, PGR and PGR+HiDHA decreased Pparγ mRNA by 20%, while PGR+LoDHA further decreased cPparγ mRNA by an additional 40%. In female lungs, PGR and PGR with both doses of DHA decreased PparγΔ5 mRNA by 40%.
Conclusions: We conclude that PGR and DHA reduce levels of Plin2 in male and female rat lung in association with sex-divergent relative expression of cPparγ and PparγΔ5 in rat lung. In male rat lungs, decreased Plin2 is associated with increased expression of the dominant-negative variant PparγΔ5. In contrast, in female rat lungs, decreased Plin2 is associated with decreased expression of cPPARγ. Ongoing work is examining fatty acid profiles and cPparγ and PparγΔ5 expression in isolated lung fibroblasts to determine cause-and-effect relationships.
# 63
PERINATAL ACETAMINOPHEN TOXICITY IS MEDIATED BY CYTOCHROME P450 2E1 (CYP2E1) IN A TIME AND CELL TYPE SPECIFIC MANNER
Golden E1, Zheng L1, Grayck MR1, Li Z2, Talaba N2, McCulley D2, Wright CJ1. 1University of Colorado School of Medicine, Aurora, CO and 2University of California San Diego, San Diego, CA
Purpose of Study: Acetaminophen (APAP) exposures occur in 50-60% of pregnancies in the US1 and is concerningly associated with childhood respiratory morbidity2–23 . The mechanism behind this remains unknown. Toxicity occurs from cell-specific expression of Cyp2e1, the enzyme responsible for metabolizing APAP into the mitochondrial toxin N-acetyl-para-benzo-quinone (NAPQI). In the developing murine lung, prenatal pulmonary Cyp2e1 expression peaks during the saccular stage (E17.5-P4) and is limited to the myofibroblast. We hypothesize this peak in Cyp2e1 expression predicts susceptibility to APAP-induced lung injury during this critical developmental period.
Methods Used: To confirm dynamic Cyp2e1 expression in the developing murine lung, RNA was isolated from lungs of wild-type mice from E12-P7 and assessed for Cyp2e1 expression. CYP2E1 protein was characterized by western blot. To determine a cell-specific pattern, Cyp2e1 expression in Pdgfra-GFP labeled pulmonary myofibroblasts was compared to Cyp2e1 expression in all other lung cell types.
C57BL/6 murine dams (n= 8-16 per condition) were exposed to APAP (250mg/kg IP; 6h) on embryonic day 17 (E17) or 18 (E18). We interrogated a pulmonary transcriptional response in inflammatory (Il6 and mmp9), oxidative stress (Gclc, Hmox1, Nqo1) and apoptotic related factors (Trp53, Puma, Noxa) by qPCR.
Summary of Results: In the time interval we analyzed, Cyp2e1 expression was low in the developing mouse lung[DM1] until E18 when it abruptly peaks (Fig.1). CYP2E1 protein was detected by western blot at both e17 and e18. Cyp2e1 expression at E18 was enriched in Pdgfraa-GFP positive lung myofibroblast cells (Fig.2). Following APAP treatment of pregnant dams at E17 and E18, Cyp2e1 expression is increased (p<0.05). In E18 APAP exposed embryos we observed increased expression of oxidative stress genes: Gclc, Hmox1 and Nqo1 and induction in p53 mediated apoptotic genes: Puma and Noxa, and in the inflammatory response gene Mmp9 (p<0.05).
Conclusions: Using a murine model we demonstrated that pulmonary Cyp2e1 expression is timing and cell type-specific, peaking at E18 and limited to the mesenchymal myofibroblast. We also found that a non-lethal dose of APAP resulted in upregulation of expression of genes associated with antioxidant response elements, apoptosis, and inflammation. Continued work is needed to determine whether perinatal APAP exposure has detrimental effects on the developing lung, its function, and the role of pulmonary Cyp2e1 in this mechanism of lung injury.
# 64
Neonatal hyperoxia exposure derails the normal development and the physiological aging of the lung
Seymour C1, Jansky S1, Glass C2, Sajti E1. 1UC San Diego, San Diego, CA and 2UC San Diego, San Diego, CA
Purpose of Study: A large proportion of premature infants develop significant complications and face life-long health problems. Especially those adult preterm birth survivors who have developed bronchopulmonary dysplasia (BPD) are at risk for chronic respiratory dysfunction. Accumulating evidence suggests that these health problems are a consequence of disrupted organ development and accelerated decline in organ function. Exposure to high levels of oxygen (hyperoxia) in the neonatal period plays a central role in the pathogenesis of BPD. However, the cellular and molecular processes that underlie the accelerated loss of healthy lung physiology in ex-preterm infants are poorly understood.
Methods Used: Newborn C57BL/6 mice were exposed to 75% oxygen for 2 weeks. Lungs were harvested immediately after the hyperoxia exposure at 2 weeks or at 8 weeks, 6 months, and 18 months of age following recovery in room air. To quantify the severity of lung injury at these time points, we measured alveolar simplification by calculating mean linear intercept (MLI) score on paraffin-embedded H&E stained slides. Gene expression was measured by RNAseq.
Summary of Results: Exposure of the developing lung to hyperoxia resulted in permanent changes in tissue architecture. Neonatal hyperoxia resulted in a significant increase in MLI with a corresponding decrease in internal surface area in the acute phase. At 8 weeks and 6 months of age, we found an interval decrease in MLI, however, the difference between hyperoxia-exposed and control mice remained significant. We measured changes in gene expression to understand the molecular mechanisms underlying these morphometric findings. The pulmonary transcriptome revealed distinct hyperoxia-induced changes in young and aging mice. Strikingly, the genes modulated by hyperoxia in the 2-week-old mice were downregulated in adult and aging mice. In young mice, hyperoxia-induced genes were related to apoptosis while in adult and aging animals vascular smooth muscle development and extracellular matrix organization. Importantly, aging-induced gene programs were altered by hyperoxia. Compared to normal aging lungs, neonatal hyperoxia-exposed lungs showed a more pronounced activation of the NFkB pathway and inflammatory processes.
Conclusions: We provide novel molecular insights into the long-term effects of neonatal hyperoxia on the lung and highlight that hyperoxia-induced gene programs are age and lung-development-specific. Of note, vasculature development-related genes were downregulated in the adult and old mice suggesting that neonatal hyperoxia exposure results in a sustained suppression of these gene programs. Importantly, in addition to derailing normal lung development in the neonatal period, hyperoxia exposure resulted in altered aging. Aging hyperoxia-exposed mice showed a heightened inflammatory profile.
A better understanding of the aging-related changes induced by neonatal hyperoxia will aid in the development of therapeutic strategies for the long-term complications of BPD.
# 65
PLATELETS ARE ACTIVATED AND INCREASED IN THE LUNGS OF HYPOXIC NEONATAL MICE
Archambault J, Posey JN, Jordan M, Nozik E, Delaney C. University of Colorado, Aurora, CO
Purpose of Study: Pulmonary hypertension (PH) is a life-threatening condition characterized by vasoconstriction, pulmonary vascular remodeling, and thrombosis. Platelets are mediators of both systemic and pulmonary vascular inflammation, which plays a critical role in the development of PH. We recently reported that platelets are activated and increased in the lungs of adult mice with hypoxia-induced PH and neonatal mice with bleomycin-induced PH. While these data support the premise that platelets promote the development of PH, whether platelets are activated and contribute to hypoxia-induced inflammation and pulmonary vascular remodeling in neonates is unknown. We now seek to determine if platelets are activated and recruited to the lungs of hypoxic neonatal mice, a second and potentially more clinically relevant model of neonatal PH.
Methods Used: C57BL/6 neonatal mice were placed in hypobaric hypoxia to simulate FiO2 12% at day of life (DOL 1) or remained in normoxia until DOL 15. Whole blood was collected via right ventricle cardiac puncture. Platelets and platelet poor plasma were isolated. We quantified cell surface markers of platelet activation by flow cytometry. Lungs were homogenized for ELISA or inflated and fixed for future use. Data were analyzed using unpaired t test and reported as mean +/- SE with significance defined as p<0.05.
Summary of Results: We found that platelets were activated in hypoxia compared to normoxia, demonstrated by increased expression of platelet p-selectin (11.7 +/- 1.9 vs 3.3 +/-1.0 [%], p<0.005) and activation of the transmembrane integrin α2βB3 (14.0 +/- 2.6 vs. 4.2 +/- 0.7 [%], p<0.01). Platelets were increased in the lungs of hypoxic mice, demonstrated by an increase in the platelet specific protein PF4 isolated from lung homogenates (3331 +/- 474 vs 1256 +/- 248 [ng/mL], p<0.005).
Conclusions: Our findings suggest that platelets may contribute to inflammation underlying neonatal PH. Neonatal platelets are activated in response to hypoxia and increased in the hypoxic lung. Future investigation will measure platelet-leukocyte aggregates, platelet-derived proteins in platelet poor plasma, and quantify lung platelet accumulation in response to hypoxia. There are a lack of convincing data to support the use of antiplatelet therapies in neonatal PH but given the high morbidity and mortality of this disease, investigation into novel therapeutic targets is warranted. These findings have potential to lead to a paradigm shift our understanding of neonatal PH, laying the foundation for prospective clinical studies that generate new evidence-based strategies to improve pulmonary outcomes in neonates with PH.
# 66
HYPEROXIA INDUCES AGE-DEPENDENT TRANSCRIPTOMIC CHANGES IN THE LUNG
Jansky S1, Glass C2, Sajti E1. 1UC San Diego and Rady Children’s Hospital, San Diego, CA and 2UC San Diego, La Jolla, CA
Purpose of Study: Supplemental oxygen therapy is one of the most widely used interventions in the ICU. While it can be lifesaving, inhalation of high concentrations of oxygen can lead to severe hyperoxic acute lung injury (HALI) in both neonatal and adult patients. The developing neonatal lung responds in a different way to hyperoxia than the adult lung. However, the molecular and cellular mechanisms directing this age-dependent response are not known. In addition, not every patient is equally sensitive to development of hyperoxia-induced lung injury. Our aim in this study was to investigate the impact of age and natural genetic variation on HALI severity by assessing the extent and nature of gene expression variability between young and adult mice in two strains that show differences in susceptibility to oxidant stress.
Methods Used: Newborn (postnatal 0) and adult (8 weeks) C57BL/6J (B6) sensitive and DBA/2J (DBA) mice resistant to HALI were exposed to 75% oxygen for 48 hours. Littermates raised in room air served as controls. Lungs were harvested immediately after the hyperoxia exposure and used for downstream analysis. Gene expression was measured by RNAseq. Data were analyzed with HOMER.
Summary of Results: Exposure of the neonatal lung to hyperoxia resulted in a qualitatively different response as compared to adult lungs. HALI in the neonatal lung was associated with the upregulation of genes related to cell division and cell cytokinesis while in adult mice to amino acid metabolic processes, apoptosis, and ferroptosis. Only 13 genes including Cdkn1a, Bax, Zmat3 involved in the p53-dependent growth regulatory pathway were commonly upregulated by hyperoxia in the two age groups. Hyperoxia exposure resulted in divergent transcriptomic changes in the two strains. Sensitive B6 mice showed significant upregulation of genes associated with apoptosis such as Nupr1 and Cdkn1a, whereas resistant DBA mice upregulated inflammation and chemotaxis related genes like Cxcl5 and Ccl9.
Conclusions: Unbiased genomic assessment reveals a divergent gene expression program in HALI in the lungs of neonatal and adult mice. Even brief exposure of the neonatal lung to hyperoxia in the postnatal saccular and alveologenesis periods resulted in marked alteration of cell division related gene programs. Adult HALI was characterized by apoptosis and cell death. The finding that activation of the p53 pathway occurred in both age groups and strains underscores the central role of this transcription factor in mediating the effects of hyperoxia. Importantly, activation of p53 resulted in different outcomes in neonatal vs adult and in sensitive vs resistant strains, suggesting that the timing and the magnitude of p53 activation drive different injury phenotypes. Understanding the discrepant responses between pediatric and adult patients, as well as interstrain variability in gene expression, to acute lung injury paves the way for future age-appropriate and personalized therapeutic interventions.
# 67
Nintedanib, an Anti-Fibrotic Drug, Preserves Lung Alveolar and Vascular Growth and Prevents Pulmonary Hypertension in an Experimental Model of Hyperoxia-Induced Lung Injury
Ding KL1, Smith C1, Abman SH2, Seedorf G2. 1University of Colorado, School of Medicine, Aurora, CO and 2University of Colorado, School of Medicine, Aurora, CO
Purpose of Study: Bronchopulmonary dysplasia (BPD), the chronic lung disease associated with prematurity, is characterized by poor alveolar and vascular growth, interstitial fibrosis, and associated comorbidities, including pulmonary hypertension (PH). Although multifactorial in origin, the pathophysiology of BPD is partly attributed to hyperoxia-induced postnatal injury, resulting in impaired distal lung growth and lung fibrosis. Despite marked improvements in the survival of premature newborns, the incidence of BPD has been increasing and it remains the most frequent complication associated with severe preterm birth. Recent work has shown that anti-fibrotic agents, including Nintedanib (NTD), can preserve lung function in adults with idiopathic pulmonary fibrosis. However, NTD is a non-specific tyrosine kinase receptor inhibitor that can potentially have adverse effects on the developing lung, and whether NTD treatment can prevent or worsen the risk for BPD and PH is unknown. The objective is to determine the effects of NTD treatment on the normal developing lung and whether NTD can preserve lung growth and function and prevent PH in an experimental model of hyperoxia-induced BPD in rats.
Methods Used: Newborn rats were exposed to either hyperoxia (90%) or room air (RA) conditions and received daily treatment of NTD or saline (control) by intraperitoneal (IP) injections (1 mg/kg) for 14 days, beginning on postnatal day 1. At day 14, lung mechanics were measured prior to harvesting lung and cardiac tissue. Lung mechanics, including total respiratory resistance and compliance, were measured using a flexiVent system. Lung tissue was evaluated for radial alveolar counts (RAC), mean linear intercept (MLI), and pulmonary vessel density (PVD). Right ventricular hypertrophy (RVH) was quantified with cardiac weights using Fulton’s index (ratio of right ventricle to the left ventricle plus septum).
Summary of Results: When compared with RA controls, hyperoxia exposure reduced RAC by 64% (p<0.01) and PVD by 65% (p<0.01) and increased MLI by 108% (p<0.01). and RVH by 118% (p<0.01). Hyperoxia increased total respiratory resistance by 94% and reduced lung compliance by 75% (p<0.01 for each). NTD administration restored RAC, MLI, RVH, and total respiratory resistance to control values and improved PVD and total lung compliance in the hyperoxia-exposed rats. NTD treatment of control animals did not have adverse effects on lung structure or function at the dose used in this study. When administered at very high doses (50 mg/kg), NTD reduced alveolar growth significantly in RA controls, suggesting dose-related effects on normal lung structure.
Conclusions: We found that NTD treatment preserved lung alveolar and vascular growth, improved lung function and reduced RVH in experimental BPD in infant rats without apparent adverse effects in control animals. We speculate that although potentially harmful at high doses, NTD may provide a novel therapeutic strategy for prevention of BPD and PH.
# 68
The Timing of Growth Restriction in the Rat Affects Intrapulmonary Lipid Profiles and PPARγ Expression
Bitsui CT1, Bartholomew A1, Chidester W1, Kindred C1, Cohen A1, Borton M1, Maschek A2, Cox J2, Joss-Moore L1. 1University of Utah, Salt Lake City, UT and 2University of Utah, Salt Lake City, UT
Purpose of Study: Bronchopulmonary dysplasia is characterized by impaired alveolar formation. Drivers of alveolar formation are incompletely understood. However, a well-appreciated impediment to alveolar formation is inadequate growth and nutrition. Long-chain ω-3 fatty acids contribute to signaling pathways driving the epithelial-mesenchymal transition, promoting lung development, in part, via activation of PPARγ. In order to elucidate mechanisms by which fetal growth restriction (FGR) and postnatal growth restriction (PGR) contribute to lung outcomes, we utilize a rat model. We previously demonstrated that both FGR with normal postnatal growth, PGR, and the combination of FGR+PGR differentially affect lung function at postnatal day 12, a timepoint corresponding to the saccular-alveolar transition in the rat. However, intrapulmonary ω-3 profiles and associated expression of a dominant negative isoform of PPARγ, PPARγΔ5, are unknown.
We hypothesize that the effects of growth restriction on intrapulmonary ω-3 fatty acids and PPARγΔ5 expression differ depending on the timing of growth restriction.
Methods Used: FGR was induced by bilateral uterine artery ligation at E19 of gestation, while PGR was generated by variation in litter size (pups/litter: control-8, PGR-16). Pups were raised by respective dams to postnatal day 12 when lung tissue was collected. GC/MS was used to measure lung lipid classes containing ω-3 fatty acids, and real-time RT PCR was used to measure PPARγΔ5 mRNA. Differences were assessed by one-way ANOVA and fishers post hoc test.
Summary of Results: In female rat lungs, intrapulmonary lipids were differentially affected by FGR and PGR. In female lung, FGR with normal postnatal nutrition resulted in increased lung docosahexaenoic acid (DHA) and docosapentaenoic acid (DPA) compared to control across all lipid classes. In contrast, female PGR lungs had decreased DHA and DPA across all lipid classes. In female FGR+PGR lungs, fewer lipid classes were affected with an overall increase in eicosapentaenoic acid (EPA), DHA, and DPA. PPARγΔ5was also differentially affected in female lungs by FGR and PGR. PPARγΔ5 increased by 54% in FGR lungs, with no changes in other groups. In male rat lungs, neither FGR, PGR, nor FGR+PGR significantly affected lung w-3 profiles or expression of lung PPARγΔ5.
Conclusions: We conclude that the effects of growth restriction on intrapulmonary ω-3 fatty acids and PPARγΔ5 expression are sex and timing-dependent. Given that PPARγΔ5 is a dominant negative isoform, which is increased under conditions of PPARγ activation, we speculate that poor lung outcomes in female FGR rats may be due to ω-3 activation of PPARγ. These data highlight the importance of considering lung developmental timing when evaluating nutritional options in preterm neonates.
Surgery I - Orthopedics
Concurrent Session
12:45 PM
Thursday, January 18, 2024
# 69
Angiotensin Converting Enzyme Inhibition as a Potential Risk Factor for Total Knee Arthoplasty Infection
Cevallos NA1, Trikha R2, Zhang A1, Stavrakis A2, Photopoulos C3, Bernthal N2. 1UCSF, San Francisco, CA; 2UCLA, Los Angeles, CA and 3Kerlan-Jobe Institute, Los Angeles, CA
Purpose of Study: There is growing evidence suggesting angiotensin-converting enzyme (ACE) has an immunomodulatory role. Prior in-vitro studies and in-vivo surgical animal models show ACE inhibitors may have an immunosuppressive effect. ACE inhibition (ACEi) may be a risk factor for surgical site infection. Given ACEis and angiotensin receptor blockers (ARB) have similar clinical indications, this study aims to determine whether a difference in infectious burden exists in patients taking ACEis versus ARBs prior to a total knee arthroplasty (TKA).
Methods Used: A retrospective review utilized PearlDiver database to query patients undergoing TKA. Patients were divided into two groups of taking ACEi or an ARB for at least 1 year prior to primary TKA. Current Procedural Terminology codes were used to identify which patients underwent an irrigation and debridement, and removal of prosthesis procedure following surgery at 6 months, 1 year, 2 year, 5 year, and 10 years. Propensity score matching was used to control for age, gender, insurance plan, Charlson Comorbidity Index (CCI), and comorbidities. Kaplan Meier survival (KMS) curves and log rank test calculated survival differences. Odds ratios (ORs) and 95% confidence interval (CI) were analyzed to compare infection rates with significance defined as p-value of <0.05.
Summary of Results: 77831 patients were identified in the ACEi group, 39105 in ARB. After propensity score matching, 39105 patients were included in each group. ACEi had statistically significant higher rates of infection in the KMS curve for 10 years from index surgery, p <.0001. At 6 months ACEi had a 95% CI of 4.39 [2.40, 8.02], 1 year 4.82 [2.81, 8.26], 2 year 4.41 [2.71, 7.16], and 5 year 3.94 [2.60, 5.96] with all p values <.0001.
Conclusions: Periprosthetic joint infection is a devastating complication. After controlling for various demographic factors and comorbidities, the ACEi group had significantly higher rates of infection. While recent techniques emphasize implant coatings or antibiotic elution, this study focuses on immune optimization. Patients on ACEi may benefit from switching to an ARB to decrease their infectious risk.
95% Confidence Interval Odds Ratio of ACEi relative to ARB periprosthetic joint infection.
Time from Index Surgery
Odds Ratio [95% CI]
P Value
6 months
ACEi
4.39 [2.40, 8.02]
<.0001
1 year
ACEi
4.82 [2.81, 8.26]
<.0001
2 year
ACEi
4.41 [2.71, 7.16]
<.0001
5 year
ACEi
3.94 [2.60, 5.96]
<.0001
Kaplan Meier Survival curve after propensity score matching with 39105 patients in each group tracked for 10 years. ACEi had statistically significant higher rates of infection.
# 70
EVALUATION OF BONE INGROWTH USING A SCAFFOLD MATRIX IN A RAT MODEL
Childers RV1, Nunez Romero A1, Figueroa G1, Gonzales D1, Loy D2, Muralidharan K2, Potter B2, Szivek J1, Margolis D1. 1University of Arizona College of Medicine Tucson, Tucson, AZ and 2University of Arizona, Tucson, AZ
Purpose of Study: Current treatment regimens for large critical bone defects do not provide reliable healing, often resulting in revision surgeries and complications. Prior work in our laboratory has been able to use 3D printed polybutylene terephthalate (PBT) scaffolds coated with beta-tricalcium phosphate (TCP) and loaded with autologous adipose derived stem cells to support bone growth, bridging a 4.2cm defect in a sheep in 3 months. However, PBT is a non-resorbable polymer and may be prone to late fracture or infection. Our lab engineered a resorbable material that is conducive for free form fabrication of 3D scaffolds using a blend of polylactic acid (PLA) and TCP, a known osteoconductive material. This study’s goal is to use quantitative histology and bone histomorphometry to evaluate bone formation with scaffolds in vivo.
Methods Used: 24 Sprague-Dawley rats were utilized in this IACUC approved study. Four scaffolds with differing materials were 3D printed and trimmed: TCP coated PBT, pure PLA, composite 75:25 PLA:TCP, and composite 50:50 PLA:TCP scaffolds. Strain gauges were attached to the scaffolds, which were implanted on a rat femur for 3 months. The rats were injected with Calcein twice before explant of the femora, one week in between both injections. The bones were embedded in polymethylmethacrylate (PMMA) for histology preparation. Quantitative histology and histomorphometry measurements were performed using Image J. Measurements included: total cortical bone area (mm2), bone volume (BV/TV, %), marrow cavity volume (MaV/TV, %), osteoid volume (OV/TV, %), and the scaffold pore space occupied by bone tissue (%), mineralized apposition rate (MAR, μm/day), and bone formation rate (BFR, μm3/μm2/day). The values were normalized by comparing the average differences between the experimental and contralateral control. All data was analyzed with SPSS using ANOVA with a Tukey HSD post-hoc test.
Summary of Results: 23 of the 24 scaffolds were securely attached to bone after explantation. Table 1 shows the average differences between the experimental and control. The pore space occupied by bone (bone ingrowth %, Table 1) was significantly higher in 50:50 PLA:TCP scaffolds compared to PBT scaffolds (p<0.05). OV/TV was significantly increased in experimental femora compared to control femora (p<0.005). There was no statistical significance found in MAR and BFR between the groups.
Conclusions: The results illustrate that 50:50 PLA:TCP scaffolds support accelerated bone ingrowth compared to PBT scaffolds. The 50:50 PLA:TCP scaffolds showed significantly more bone ingrowth than PBT scaffolds. The lower MAR and BFR in 50:50 PLA:TCP scaffolds indicate that the increased bone growth into scaffold pores was slowing down compared to PBT scaffolds. Overall, the composite 50:50 PLA:TCP scaffolds have shown improved bone growth with similar mechanical coupling to TCP coated PBT scaffolds. This in vivo rat study has indicated that 50:50 PLA:TCP scaffolds support more rapid bone ingrowth compared to PBT scaffolds.
Material
Cortical Bone Area (mm2)
Bone Ingrowth (%)
BV/TV (%)
MaV/TV (%)
OV/TV (%)
MAR (μm/day)
BFR (μm3/μm2/day)
PBT
1.49 ± 2.18
6.37 ± 2.04
-1.03 ± 5.29
-0.39 ± 2.21
-0.39 ± 2.21
0.84 ± 0.67
0.15 ± 0.98
PLA
1.07 ± 1.37
8.96 ± 2.44
-1.51 ± 4.52
-0.02 ± 4.59
0.71 ± 1.60
0.91 ± 0.42
-0.46 ± 0.31
75:25 PLA:TCP
1.09 ± 1.9
8.30 ± 3.19
-3.01 ± 2.18
1.50 ± 2.36
0.91 ± 1.27
0.98 ± 1.17
-0.37 ± 1.49
50:50 PLA:TCP
2.33 ± 2.18
10.80 ± 0.85
1.40 ± 8.10
-2.95 ± 7.88
0.92 ± 1.57
-0.06 ± 1.24
-0.75 ± 1.68
Average differences of quantitative histology and histomorphometry measurements.
# 72
INTRA-OPERATIVE SKIN TRACTION IN POSTERIOR SPINE FUSION FOR NON-AMBULATORY PEDIATRIC SCOLIOSIS
Coughlin G 1, Shah SA3, Bauer JM2, 1. 1University of Washington, Seattle, WA; 2Seattle Children’s Hospital, Seattle, WA and 3Nemours/Alfred I. duPont Hospital for Children, Wilmington, DE
Purpose of Study: Intraoperative traction (IOT) has been demonstrated to improve scoliotic deformity and pelvic obliquity (POB) during posterior spinal fusion (PSF). This is commonly done with invasive distal femoral traction pins or traction boots. Skin-based traction offers a novel surgical technique for IOT that may ameliorate risks associated with skeletal traction without loss of deformity correction effectiveness. The aim of this study is to assess the safety and efficacy of skin-based IOT for coronal plane correction and pelvic imbalance in non-ambulatory scoliosis.
Methods Used: We performed a retrospective study during 2017-2023 for scoliosis patients aged 5-21 YO, who were surgically treated with a T2-pelvis instrumented PSF and skin-based IOT by a single surgeon at a pediatric hospital. We reviewed charts for demographics and intraoperative data to assess safety of skin traction, and radiographs for pre-and post-operative (preop and postop) coronal and sagittal measurements. We used a published historical cohort that used distal femoral skeletal traction for statistical comparison (two-sample t-tests and Cohen’s d effect size) of IOT techniques.
Summary of Results: We reviewed 51 non-ambulatory pediatric scoliosis patients with majority having cerebral palsy (CP), CP-like pathology, or other myopathy or metabolic disease. 53% (n=27) were female, mean age at surgery was 12.8±3 years, and average follow-up was 1.5±1.3 years. Skin traction was applied setting a cranial attachment (6, 12% with halo ring and 45, 88% with Mayfield attachment) and attaching an average of 12% body weight to the pelvis using medical tape-rope-weight system with Trendelenburg assistance. The published skeletal traction cohort included 41 patients with no difference in collected demographics. The preop major scoliotic curve averaged 91°±20° in the skin traction cohort and 91°±17° in the skeletal traction cohort (p= 0.019; d=0.02). Preop pelvic obliquity averaged 22°±10° in the skin traction group and 34°±14° in the published cohort. Postop major curve decreased to 24°±14° (75% correction) at final follow-up in skin traction group vs mean 43°±15° (53% correction) in the published cohort (p<0.0001; d=1.29). Average POB at final follow-up was 5°±5° in skin traction group (77% correction) and 12°±8° (65% correction) in published cohort (p= <0.0001; d=1.04). No intraoperative or postoperative skin traction-related complications occurred (pressure sores at bony prominences, skin tears related to skull pins or tape traction).
Conclusions: In non-ambulatory neuromuscular pediatric scoliosis patients, intraoperative use of skin-based traction during surgical posterior fusion treatment to the pelvis is a safe and effective intra-operative technique for deformity correction. There were no associated perioperative complications and no loss of corrective strength for skin IOT compared to a published cohort using invasive skeletal traction IOT. This technique should be considered for assistance of T2-pelvis PSF for pediatric scoliosis.
# 73
TITLE: WHAT IS OCCURING AT THE OTHER DISC SPACES IN THE EARLY POSTOPERATIVE PERIOD FOLLOWING A CERVICAL DISC REPLACEMENT AT A SINGLE LEVEL? PRELIMINARY DATA
Basner L2, 1, Louie PK1, Bansal A1, Kumar R1. 1Virginia Mason Medical Center, Seattle, WA and 2University of Washington, Seattle, WA
Purpose of Study: Adjacent segment degeneration (ASD) is a well-described complication following cervical fusion surgery. Given the recent growth of cervical disc replacements(CDR), aimed to maintain motion at the operative level, less has been established regarding the changes that are occurring at the adjacent levels. We aim to characterize these changes, identify predictive radiographic factors, and compare adjacent segment changes between anterior cervical discectomy and fusion (ACDF) and CDR.
Methods Used: This is a single center retrospective study of patients who underwent single-level CDR whose lateral cervical X-rays were collected 1-12 months post-op. Data from April 2016 to July 2023 was included. Patients with multi-level CDR, without post-op X-ray, or those with prior cervical surgeries, were excluded. Segmental lordosis was measured at the operative level and both adjacent levels (cephalad and caudal). Measured parameters included pre-op and post-op C2-C7 lordosis, T1-Slope, Occiput-C2 angle (O-C2), and C2-C7 Sagittal vertical axis (SVA). Measurements were compared to patients who had single-level ACDF. Patients were stratified by operation spinal level, with primary emphasis on the C5-C6 subgroup due to its larger sample size. Both univariate and multivariate analyses were performed for this subgroup.
Summary of Results: 50 patients were included: 23 in the CDR group and 27 in the ACDF group. No significant differences were observed in the measurements between CDR and ACDF (Table 1). Greater pre-op T1 slope showed a weak correlation with a reduction of lordosis at the C5-C6 level (r=-0.24, p=0.09). Increased C5-C6 lordosis was associated with reduced cephalad (C4-5) lordosis (r=-0.27, p=0.06). Multivariate regression evaluated the combined influence of the O-C2 and C5-C6 angle changes on the cephalad C4-C5 angle change (R2 =0.15, p<0.05), showing that a larger pre-op O-C2, combined with an increase in the C5-C6 lordotic angle change, exerted a stronger influence on the reduction of lordosis at the cephalad C4-C5 level.
Conclusions: Our preliminary analysis revealed no significant differences between the measured parameters of CDR and ACDF groups. Furthermore, our key finding demonstrated that a greater pre-op O-C2, combined with an increase in C5-C6 segmental lordosis after surgery, is associated with reduced lordosis at the cephalad C4-5 level. While the effect is present, the effect size is small, as indicated by an R2 value of .15, which may not be clinically relevant. Additionally, our study was underpowered. Further studies, with an increased sample size, may expand upon these insights that could enhance pre-op surgical planning and identify patients who are potentially at risk for cephalad ASD.
Radiographic Measurements, CDR vs ACDF.
Total
CDR
ACDF
Change in Segmental Angle
N
M
SD
N
M
SD
N
M
SD
p
C5-C6
50
1.12
6.82
23
1.39
5.87
27
1.01
7.65
.85
C4-C5
50
1.04
4.77
23
0.70
4.59
27
1.32
5.00
.65
C6-C7
50
1.11
7.05
23
0.31
6.97
27
1.80
7.19
.46
T1 Slope
50
2.14
9.98
23
1.36
10.41
27
2.81
9.74
.61
C0-C2
42
0.12
7.22
20
-0.30
7.06
22
0.50
7.50
.72
Note. All p-values are for comparisons between CDR and ACDF groups. Unpaired t-tests were used for all comparisons of continuous variables.
# 74
COMPARATIVE ANALYSIS OF OUTCOMES FROM MENISCECTOMY WITH OR WITHOUT CONCURRENT SYNOVECTOMY
Williams K1, Constantine E1, Whitney K2, Fry SA1, McCarrick-Walmsley R2, Mayer B2, McCarty E2, Genuario J2, Boublik M2, Frank R2, Noonan T2, Dragoo J2. 1University of Colorado School of Medicine, Aurora, CO and 2UCHealth Inverness Orthopedics and Spine Surgery Center, Englewood, CO
Purpose of Study: Meniscectomy is the most performed procedure for meniscal injury due to its cost-effectiveness and faster rehabilitation. Synovitis is linked to knee joint dysfunction and the progression of knee osteoarthritis (OA), which have been associated with poor post-operative outcomes. Concurrent synovectomy with meniscectomy may help prevent cartilage damage and alleviate pain and dysfunction.
The purpose of this study is to determine whether patients who underwent an arthroscopic meniscectomy with concurrent synovectomy exhibited similar outcome scores compared to patients who underwent arthroscopic meniscectomy alone for up to 2 years of follow-up.
Methods Used: Patient-reported outcomes (PROs), including the Knee Injury and Osteoarthritis Outcome Score (KOOS) subscales, were collected pre-operatively and up to 2-years post-operation from patients who received a meniscectomy (M) or meniscectomy and synovectomy (M+S). Of 132 cases from seven physicians, 68 (51.5%) received meniscectomy alone and 64 (48.5%) had both meniscectomy and concurrent synovectomy. Medical record chart reviews were performed to record demographic and injury details, including age, gender, BMI, smoking history, comorbidities, and Kellgren Lawrence (KL) OA grade. Failures were defined as patients who had a subsequent procedure on the same knee.
Summary of Results: Patient demographics, injury details, and failure information are described in Table 1. While all PRO metrics were found to improve between baseline and all time points, KOOS subscale scores were not statistically significant between cohorts except for 6-month KOOS Pain (Mann-Whitney p=0.024) and 6-month KOOS Symptoms (Mann-Whitney p=0.047) (figure 1). Follow-up Kolmogorov-Smirnov tests were not statistically significant and in line with other KOOS subscales (KOOS Pain: p=0.13, KOOS Symptoms: p=0.14). We observed a higher proportion of severe OA in the meniscectomy + synovectomy group (M+S=34%, M=15%; p=0.06). Over the period surveyed (3.5 years), 7 cases were considered failures; 2 cases were in the meniscectomy cohort and 5 from the meniscectomy + synovectomy group. In failures, the average BMI trended higher (31.3 vs. 27.8 in non-failures, p=0.1205), the average KL OA grade trended higher (3.1 vs. 2.69 in non-failures, p=0.22), and we observed a higher proportion of subjects with a smoking history (28.6% vs. 21.1% in non-failures), but no comparison was statistically significant. There was no observed difference in BMI (p=0.23), OA grade (p=0.94), or age (p=0.89) between the failure and non-failure group. The failures observed occurred between 210 and 1,281 days after surgery.
Conclusions: PROs from patients without synovitis who underwent surgical meniscectomy were no different from those patients who had synovitis and underwent a meniscectomy and concurrent synovectomy, despite the larger proportion of high-grade OA in the latter. Further sample collection over a longer period than our 3.5-year period is needed to determine predictive factors of failures.
Patient demographics, injury details, and post-operative failures.
Meniscectomy + Synovectomy
(N=64)
Meniscectomy Alone
(N=68)
P-value
Age
Mean (SD)
58.0 (±12.0)
61.0 (±10.8)
0.196
Median [IQR]
60 [51 - 68]
62 [54 - 70]
Range
[29 - 80]
[29 - 80]
BMI
Mean (SD)
28.7 (±8.34)
27.5 (±6.12)
0.336
Median [IQR]
26.7 [23.7 - 31.8]
26.5 [24.8 - 31.7]
Range
[18.57 - 54.9]
[18.95 - 41.0]
Gender
Female
31 (48%)
30 (44%)
0.727
Male
33 (52%)
38 (56%)
OA Grade
0
4 (6%)
2 (3%)
0.06
1
2 (3%)
2 (3%)
2
17 (27%)
26 (38%)
3
19 (30%)
28 (41%)
4
22 (34%)
10 (15%)
Medial Meniscus Tear Type
Bucket Handle
3 (5%)
4 (6%)
0.896
Complex
43 (67%)
36 (57%)
Free Edge
1 (2%)
0 (0%)
Unknown
7 (11%)
6 (9%)
Oblique
0 (0%)
1 (1%)
Lateral Meniscus Tear Type
Complex
8 (12%)
13 (19%)
0.599
Free Edge
40 (62%)
39 (57%)
Oblique
16 (25%)
16 (24%)
Failures
Failure
5 (8%)
2 (3%)
0.264
Non-Failure
59 (92%)
66 (97%)
# 75
AN ANALYSIS OF RISKS AS A PREDICTOR OF THE OUTCOME OF ANKLE ARTHRODESIS
Nocek M, Zhu M, Huo D, Singh N, Lei M, Li S, Myerson M. University of Colorado School of Medicine, Aurora, CO
Purpose of Study: There are well recognized risk factors for the outcome of bone healing and ankle arthrodesis which include bone quality, deformity, and various patient co-morbidities. The presumption is that if arthrodesis of the ankle is performed in a high risk patient, the rate of arthrodesis would be lower. If the surgery is however performed according to an established protocol, the rate of fusion and complications should be comparable with treatment in patients with low risk.
Methods Used: We analyzed 22 non unions of the ankle joint specifically for bone risk factors which have been previously established. The scoring system used included deformity, avascular necrosis, bone defect, fracture with sclerosis and predisposing conditions). Each of these five risk categories was weighted according to severity (1-5) such that the worst score attainable would be 25 and a patient with no risk factors a score of 0. In the category of predisposing conditions, the weighted scores included osteoarthritis (1), rheumatoid arthritis (2), complex fracture with significant deformity (3), subtalar arthrodesis or ankle nonunion (4), prior sepsis or osteomyelitis (5). The rates of arthrodesis were evaluated with osseous union being defined as radiographic evidence of bony trabeculae across the ankle.
Summary of Results: We classified the patients as low risk (1-4), medium risk (5-10) and high risk (>10). Plate fixation was used for the arthrodesis in 8 ankles, and cannulated compression screws in the remaining 14. The mean preoperative risk score of the 22 patients was 3.9 (range, 1-15). There were 16 feet in the low-risk group, in 5 of which a plate was used for fixation, 3 in the medium risk (1 plate and 2 screw fixation), and 3 in the high risk group (2 plates, 1 screw fixation).
Conclusions: The assumption that patients with higher grades of deformity, bone loss and avascular necrosis would pose a higher risk of nonunion, was not supported in this study. Because of the small sample size, it was not possible to extrapolate the technical aspects of the surgery and fixation with the outcome.
Pre and postoperative images of a patient with post traumatic arthritis of the ankle. The risk (15) was graded accordingly as bone loss (4), post traumatic arthritis with deformity of the articular surface (5), avascular necrosis of the tibia (2), osteopenia (2), complex fracture with significant deformity (2).
# 76
Incidence of ACL Injuries in Females by Selective Use of Oral Contraceptive Pills
Fry SA, Keeter C, McCarrick-Walmsley R, Constantine E, Williams K, Whitney K, Dragoo J. University of Colorado School of Medicine, Aurora, CO
Purpose of Study: Females are more likely to experience anterior cruciate ligament (ACL) injuries compared to males. Relaxin, a collagenolytic hormone, among other biomechanical factors play a role in weakening the ACL, consequently increasing the risk of ACL tears in females. Oral contraceptive pills (OCPs) have been found to significantly decrease relaxin in serum and increase ACL strength. The purpose of this study is to investigate the incidence of ACL injuries among females that use four different formulations of OCPs.
Methods Used: In this retrospective cohort study, de-identified data were obtained from 14,664,162 female patients from 15 to 34 years of age between 2011-2023 from the Colorado Health Data Compass database. A total of 15,570 females who sustained an ACL injury, treated by arthroscopic ACL reconstruction, and 12,878,504 females without a history of ACL injury were included. Among these groups, non-OCP users and OCP users, including formulations norethindrone (NE) only, drospirenone (DS) + ethinyl estradiol (EE), etyodiol diacetate (ED) + EE, NE + EE, norgestimate (NG) + EE, were included in the analysis. Statistical analysis was completed using RStudio.
Summary of Results: Comparing ACL injury incidence with and without OCP use, the proportion of ACL injury incidence with OCP use (0.086%; CI: [0.08, 0.093]) was less than the proportion of ACL injury incidence with no OCP use (0.123%; CI: [0.12, 0.125]) (Table 1). When separated by five-year intervals, females aged 15 to 19 had no difference in proportion of ACL injury incidence with OCP use (0.117%; CI: [0.95,0.143]) compared no OCP use (0125%; CI: [0.121, 0.129]). All other age groups showed a lower proportion of ACL injury incidence in the OCP user group, suggesting age may be a factor in the effects of OCP use on ACL injury incidence. Additionally, different OCP formulations showed different ACL injury incidences, with a lower proportion of ACL injuries in the NE only group (0.029%; CI: [0.019, 0.043]) compared to NE+EE (0.093%; CI: [0.082, 0.104]) and NG+EE (0.094%; CI: [0.083, 0.106]) groups. No difference in ACL injury incidence in the DS+EE (0.104%; CI: [0.083, 0.13]) group compared to no OCP use (0.123%; CI: [0.121, 0.125]) was found. The progestin only formulation (NE only) showed a lower incidence of injury compared to the estrogen/progestin formulations, suggesting a role of progesterone in ACL injury prevention.
Conclusions: OCP use may be associated with lower ACL injury incidence compared to no OCP use in females. Further research is warranted to explore variables impacting the association between OCP use and ACL injury, such as contraceptive formulation and method, mechanism of injury, and demographics. This is an initial evaluation of OCP use and ACL injury associations and whether OCPs could serve protective effects against ACL injuries in females.
# 77
Spinal Tumor Surgery for Metastatic Cancer: Complete Resection Versus Partial Resection and Adjuvant Treatment
Quinn A1, Crooks SJ1, Pang H1, Kelly K2, Amin A2. 1University of Washington, Laramie, WY and 2University of Washington, Seattle, WA
Purpose of Study: The authors seek to determine if minimally invasive or shorter duration of surgical resection for spinal metastases paired with post-operative adjuvant therapy to metastases compared to traditional full surgical resections results in lower morbidity, mortality, operative and post-operative complications.
Methods Used: 119 patients who underwent spinal surgical resection for metastases were identified from multiple centers. Patient demographics, comorbidities, operative details, and outcomes were collected. Patients with primary bone tumors or intradural spinal cord tumors were excluded, as treatment for these entities differ from metastases. Complications measured include wound dehiscence, spinal infection, CSF leak, hardware failure, PE/DVT, epidural hematoma, UTI, readmission within 30 days, neurological decline, and mortality.
Summary of Results: Of the 119 patients, 58% (69) were male and 42% (50) were female, ages ranged from 31 to 90 with a median age of 62 years. These patients underwent either complete spinal tumor resection or spinal separation surgery and targeted radiation. For those who underwent complete tumor resection (76.5% of the cohort (91)): the average estimated blood loss was 519.1 mL with mean surgical duration of 234 minutes. Titanium implanted screws were placed in 40.7% (37) of patients, and mean postoperative hospital stay was 18.9 days. Decompression was performed in 92.3% (84) of patients. Complications were seen in 41.8% of patients (38), and 21.1% (8) experienced hospital readmission. Median survival to last follow up date was 54.9% (50) with median follow up of 187 days. In contrast, 23.5% of patients underwent minimally invasive spinal tumor separation with postsurgical targeted therapy. For these patients, the average estimated blood loss was 194.6 mLs and average surgical time was 228 minutes. Titanium implanted screws were used in 89.3% (25) of patients, and mean postoperative hospital stay was 6.6 days. Decompression was performed in 60.7% (17) of patients. Complications occurred in 14.3% of patients (4), with none requiring readmission related to the procedure. Median survival from last follow up was 78.8% (22) and median follow up time was 145 days.
Conclusions: We expect that less invasive surgery will provide patients with fewer inpatient complications, shorter hospital stays and expedite the ability of patients to receive subsequent adjuvant therapies, overall enabling better quality of life. While this study offers valuable insights, there are limitations. Multiple patients were lost to follow-up, primarily due to multimodal care at different facilities. Additionally, the limited number of minimally invasive surgical procedures and trained surgeons may lead to lessened understanding of the true merit of the procedure. Future studies should incorporate multi-institutional data to enable better understanding of the use of minimally invasive surgeries and enable more robust patient follow-up.
Cardiovascular II
Concurrent Session
3:15 PM
Thursday, January 18, 2024
# 78
Natural Outcome of Isolated Right Ventricular Dysfunction Immediately After Heart Transplantation
Chow E, Bhatnagar N, Kanungo A, Hamilton M, Kobashigawa J. Cedars-Sinai Smidt Institute, Los Angeles, CA
Purpose of Study: Right ventricular (RV) failure after heart transplantation (HTx) is not uncommon and may be due to an increase in pulmonary artery pressures. However, at certain times, RV failure occurs without pulmonary hypertension (PH) and may be due to insufficient preservation. The natural history of isolated RV failure without PH has not been well described. Therefore, we evaluated patients with isolated RV failure after HTx and assessed outcomes.
Methods Used: Between 2010 and 2020, we identified 30 HTx patients who developed isolated RV failure (described as moderate-severe by echocardiography within three days of transplant without the presence of PH. These patients were followed for the first year after HTx and compared to a case control group (n=30) without RV failure. Study endpoints included 1-year survival, 1-year freedom from acute cellular rejection (ACR) and antibody-mediated rejection (AMR), freedom from development of cardiac allograft vasculopathy (CAV: ≥30% stenosis by angiography), and freedom from non-fatal major adverse cardiac events (NF-MACE: myocardial infarction, new congestive heart failure, percutaneous coronary intervention, pacemaker/implantable cardioverter defibrillator placement, stroke).
Summary of Results: In the RV failure group, 3 patients necessitated a right ventricular assist device and overall, there were 3 deaths. Only 7 patients require sildenafil treatment. Between the RV failure group and control group, there were no significant differences between 1-year survival, 1-year freedom from ACR and AMR, freedom CAV, and freedom from NF-MACE.
Conclusions: Isolated moderate-severe RV failure immediately after HTx is well tolerated and resolves in almost all cases. Rarely is mechanical RV assist device needed.
RV Failure (n = 30)
Control (n = 30)
p-value
1-year survival
93.3%
100%
0.154
1-year freedom from ACR
96.7%
100%
0.317
1-year freedom from AMR
93.3%
100%
0.142
1-year freedom from CAV
96.7%
100%
0.325
1-year freedom from NF-MACE
80.0%
83.3%
0.671
# 79
TEMPORAL VALIDATION OF PEDIATRIC MYOCARDITIS MORTALITY PREDICTION WITH MACHINE LEARNING MODEL
Yu T1, Leigh RM4, Ghimire L3, Chou F2. 1College of Osteopathic Medicine of the Pacific, Pomona, CA; 2Kaiser Permanente Riverside Medical Center, Riverside, CA; 3UC San Francisco School of Medicine, Fresno, CA and 4Loma Linda School of Medicine, Loma Linda, CA
Purpose of Study: Pediatric myocarditis is characterized by infection/inflammation of the myocardium with a mortality rate of 4.9%. A recently developed machine learning (ML) based prediction has demonstrated a significant enhancement over traditional logistic regression models by achieving high sensitivity and specificity in predicting pediatric myocarditis mortality. This model was curated and internally and externally validated using the 2003, ‘06, ‘09, ‘12, and ‘16 Kids’ Inpatient Database (KID) datasets. We aim to further assess the performance of this ML model with the 2019 KID and the 2020 National Inpatient Sample (NIS) dataset.
Methods Used: Diagnosis codes for myocarditis were identified from the 2019 KID (N=1362) and 2020 NIS (N=399) dataset. The de-identified datasets negate the need for IRB approval. The NIS dataset allowed myocarditis patients with (N=124) and without COVID-19 (N=275) to be analyzed separately. Risk factor data were applied to the ML model. Descriptive statistics with median (interquartile range) for continuous variables and with count (percentage) for categorical variables are shown. To evaluate how well the prediction model performs, Receiver Operating Characteristic Area Under the Curve (ROC AUC) with 95% confidence interval was calculated based on the probability of mortality and the actual outcome for each patient.
Summary of Results: Demographic summary is provided. 2019 KID dataset’s ROC AUC was 0.915 (95% CI: 0.889-0.942). In the NIS dataset without COVID, ROC AUC was 0.954 (95% CI:0.925-0.982). There was only 1 patient who died from myocarditis with COVID-19; the patient was correctly predicted by the model. The model performance continued to suffer from a low positive prediction rate (predicting death but survived), but with a high negative prediction rate (correctly predicting survival).
Conclusions: Temporal validation of the ML-based myocarditis prediction model using more recent datasets has yielded promising results, suggesting that the model remains current and reliable. The study is limited by the small dataset of those with myocarditis and COVID and without COVID; a larger sample size would be more beneficial in challenging the ML model.
Prediction Model Performance.
Dataset
ROC AUC (95% CI)
Sensitivity
Specificity
Pos Predictive Value
Neg Predictive Value
Accuracy
Temporal validation(2019 KID)
0.9154(0.8892-0.9415)
81.1%
84.9%
17.8%
99.1%
84.7%
Temporal validation(2020 NIS w/o COVID)
0.9537(0.9254-0.982)
100%
86.7%
25.5%
100%
87.3%
Temporal validation(2020 NIS w/ COVID)
1(N/A-N/A)
100%
87.8%
6.3%
100%
87.9%
Testing(previously published)
0.94
89.9%
85.8%
26.7%
99.3%
86.0%
Demographic summary.
# 80
SIRTUIN 3, OXIDATIVE STRESS, AND INFLAMMATION IN ATHEROSCLEROTIC PLAQUE RUPTURE
Velpuri P2, Rai V1, Agrawal DK1. 1Western University, Pomona, CA and 2College of Osteopathic Medicine of the Pacific, Western University of Health Sciences, Pomona, CA
Purpose of Study: Atherosclerosis is a leading cause of morbidity and mortality in cardiovascular diseases. The atheromatous plaques along the intimal layer of arteries consist of calcium deposits, fatty cell droplets, and accumulation of immune cells leading to arterial stenosis, resistance to blood flow, ischemia, and fatal incidents such as myocardial infarctions, transient ischemic attack (TIA), and stroke. Although statins reduce hyperlipidemia and slow down the progression of atherosclerosis, inflammation within the plaque may predispose to plaque rupture and thrombosis precipitating ischemic events. The underlying molecular mechanisms are unclear. Intimal injury during angioplasty or invasive surgery can lead to the activation of renin-angiotensin system (RAS) leading to multitude downstream regulatory pathways increasing oxidative stress. In acute inflammation, cellular stress upregulates Sirtuin 3 (SIRT 3) that regulates oxidative stress through its downstream effect of activating Forkhead Box O3 (FOXO3) and increases the expression of antioxidant genes that suppress the production of oxygen radicals, a major contributor in atherosclerosis development and progression. However, the role of SIRT3 in plaque instability is not known. We examined the molecular mechanisms and differential expression of angiotensin II, SIRT3, FOXO3, and reactive oxygen species (ROS) in carotid arteries with angioplasty with and without exposure to minimally oxidized low-density lipoproteins (ox-LDL) from hyperlipidemic Yucatan microswine.
Methods Used: Carotid artery tissues were collected from female hyperlipidemic Yucatan microswine (blood cholesterol 450-600 mg/dL) that have undergone angioplasty in the carotid artery to denude endothelium and accelerate plaque formation and administration of oxLDL to the injured site (WesternU IACUC approval # R22IACUC014). Hematoxylin and eosin staining, immunohistochemistry, and quantitative PCR for SIRT3, FoxO3a, HIF-1α, HSP90, and AngIIType2R were performed with statistical analysis of the data using GraphPad Prism 9 and p value of < 0.05 was considered significant.
Summary of Results: We found that hyperlipidemia, intimal injury followed by plaque formation, and chronic inflammation were positively correlated to decreased expression of SIRT3 and FoxO3a, with a rise of ROS markers such as HIF-1α, HSP90, inflammatory markers, and AngIIType2R (activated RAS). Arteries without angioplasty and with no or minimal neointimal hyperplasia showed lower expression of HIF-1α, HSP90, and inflammatory markers.
Conclusions: These results suggest the role of ROS, SIRT3, and FOXO3a in plaque formation after intimal injury and sirtuins may be potential therapeutic targets to attenuate development and progression of atherosclerosis and enhance plaque stabilization. These novel findings warrant further investigation to establish the role of SIRT3 in the stability of atherosclerotic plaques.
# 81
Revisiting CMV Prophylaxis in Heart Transplantation in the Current Era: Does It Make Sense?
Kanungo A, Singer-Englar T, Bhatnagar N, Hamilton M, Kobashigawa J. Cedars-Sinai Heart Institute, Los Angeles, CA
Purpose of Study: Cytomegalovirus (CMV), is present in more than 50% of patients waiting for heart transplantation. Post-transplant, CMV is a potential infection, and if the donor is CMV positive and the recipient is CMV seronegative, there is a likelihood of the heart transplant recipient developing CMV infection. CMV infection after heart transplantation has been associated with a development of cardiac allograph vasculopathy (CAV). Therefore, recipients who are CMV positive, or those receiving a CMV positive donor heart are at risk for developing CMV post-transplant. Therefore, antibiotic (anti-viral) prophylaxis has been used to decrease the risk of developing this infectious complication. We reviewed a large single-center study to assess whether CMV prophylaxis is of value to prevent CMV infections in our current era.
Methods Used: Between 2010 and 2021, we assessed 1201 heart transplant patients who received CMV prophylaxis. Patients were divided into those who were donor/recipient CMV D-/R-, D+/R-, D-/R+, and D+/R+. The mismatch group D+/R- was at high risk with these patients usually having a prolonged course of antiviral prophylaxis. The D-/R+ and D+/R+ groups were combined as they were felt to be at similar risk. Outcomes of this study included the development of CMV infection (positive serology), CMV syndrome (symptoms) and CMV disease (CMV organ involvement) within the first-year post-transplantation. Prophylaxis for patients who were D-/R- included acyclovir for 3 months. Those patients who were D-/R+ or D+/R+ were treated with valganciclovir for 6 months, and the high-risk D+/R- group was treated with valganciclovir for 1 year. Other endpoints included first year rejection, which we sub-grouped into acute cellular rejection (ACR) and antibody-mediated rejection (AMR), in the first-year post-transplant, survival, graft dysfunction (LVEF < 40%), non-fatal adverse cardiac events, and development of CAV by angiography 1 year post transplant.
Summary of Results: The D+/R- group had significantly lower freedom from CMV infection (by positive serology) and a trend for a lower freedom from CMV syndrome compared to the other study groups. Among the 3 study groups, there was no difference in 1-year survival, 1-year freedom from ACR/AMR, freedom from graft dysfunction, freedom from CAV and freedom from NF-MACE. (see table)
Conclusions: Although CMV anti-viral prophylaxis appeared to be less efficacious in the high-risk D+/R- group, clinical outcome was similar to the other study groups. Antiviral prophylaxis for specific risk groups in the current era appears to be clinically useful. CMV prophylaxis for the high-risk group continues to be a challenge.
CMV D+/R-(n = 254)
CMV D-/R+, D+/R+
(n = 802)
CMV D-/R-
(n = 145)
p-value
1-year survival
90.9%
91.0%
93.7%
0.545
1-year freedom from CAV
95.6%
96.6%
96.5%
0.790
1-year freedom from ATR
81.8%
83.0%
83.4%
0.944
1-year freedom from ACR
88.5%
92.8%
91.7%
0.112
1-year freedom from AMR
93.7%
93.7%
92.4%
0.844
1-year freedom from NF-MACE
85.4%
86.7%
90.3%
0.387
1-year freedom from LVD
92.1%
93.8%
92.4%
0.581
1-year freedom from CMV serology
84.2%
88.2%
95.8%
0.003
1-year freedom from CMV syndrome
95.2%
97.7%
98.6%
0.068
1-year freedom from CMV disease (organ involvement)
98.4%
99.2%
99.3%
0.487
# 82
Does Neupogen Increase the Risk of Rejection After Heart Transplant?
Bhatnagar N, Kanungo A, Hamilton M, Kobashigawa J. Cedars-Sinai Heart Institute, Los Angeles, CA
Purpose of Study: Immunosuppression after heart transplantation (HTx) includes the use of a calcineurin inhibitor, antiproliferative agent, and corticosteroids. Antiproliferative agents are known to decrease white blood cell (WBC) counts after HTx. Even though these agents may be held, leukopenia is commonly seen. If the WBC count should be less than 2.0 x 103/L, administering granulocyte colony-stimulating factor (G-CSF known as Neupogen) may be considered. Stimulating the bone marrow with Neupogen does increase the WBC but there is concern that this stimulation may cause rejection. There are confounding studies in the literature in regard to the rejection risk with Neupogen. Therefore, we assessed our large program to assess if the use of Neupogen is a risk for rejection after HTx.
Methods Used: Between 2010 and 2020, we assessed 150 HTx patients who developed leukopenia after HTx. This was despite lowering or stopping the antiproliferative agents. These patients who received Neupogen were then followed for 6 months to determine if they did develop rejection (ACR ≥ 2R, AMR≥1R) The Neupogen dose was also included in the results, as well as the rise in WBC count. These patients were compared to a contemporaneous matched control cohort who were not treated with Neupogen.
Summary of Results: The administration of Neupogen increased WBC from an average pre-treatment level of 1.49 ± 0.5 103/L to a post-treatment level of 5.5 ± 2.3 x 103/L. The median time from transplant to leukopenia was 88 days [range: 1:912] and the average Neupogen dose was 321 ± 60 mcg/ml. In these patients, there was no increased risk of rejection during the 6 months following the Neupogen administration. This was compared to the contemporaneous control group. Subdividing rejection into acute cellular rejection and antibody-mediated rejection, there was no significant increase compared to controls. (see table)
Conclusions: The development of leukopenia and subsequent administration of Neupogen does not appear to increase the risk of rejection after HTx. Therefore, use of this drug does not appear to be a contraindication for treatment of leukopenia post-HTx.
Leukopenia treated with Neupogen (n=150)
No Leukopenia (n=150)
P=value:
Subsequent 6-month freedom from any rejection
90.7%
92.7%
0.676
___ Subsequent 6-monthfreedom from ACR (ISHLTgrade ≥2R)
92.7%
96.7%
0.116
___Subsequent 6-monthfreedom from AMR
98%
96.0%
0.324
# 83
MRA Use in ATTR Patients: Is It Effective?
Ivey B, Bhatnagar N, Kanungo A, Hamilton M, Kobashigawa J. Cedars-Sinai Heart Institute, Los Angeles, CA
Purpose of Study: Transthyretin amyloid (ATTR) is a disease state where the heart can be infiltrated by amyloid tetramers resulting in restrictive cardiac physiology. We now have medications to treat these patients to prevent progression of heart disease. The use of mineralocorticoid receptor antagonists (MRA) has been found to be helpful in patients with congestive heart failure. It has been used in patients with ATTR, but the benefits have not been established. Therefore, we reviewed our large amyloid program to determine the effect of the use of MRA.
Methods Used: Between 2012 and 2022, we assessed 96 patients with ATTR and divided into those treated with MRA and those that were not. RNA stabilizing therapy with tafamidis was administered in both groups. Endpoints included subsequent (after the start of MRA) survival and hospitalizations for heart failure.
Summary of Results: ATTR patients who were treated with MRAs compared to those without appeared to have similar subsequent 3-year survival and freedom from heart failure hospitalization. (see table)
Conclusions: MRA therapy does not appear to be beneficial in ATTR patients. This would suggest that a large, randomized trial may not be indicated.
MRA (n =48)
No MRA (n=48)
P-value
3-year survival
85.4%
95.8%
0.095
3-year freedom from subsequent hospitalizations for heart failure
77.0%
87.5%
0.201
# 84
SEX DIFFERENCES IN THE PATTERN OF NEWLY DIAGNOSED TREATABLE SEVERE AORTIC STENOSIS IN BRITISH COLUMBIA, CANADA: AORTIC STENOSIS IN B.C. DATA STUDY
Lakhani S1, Roshan A1, Yim J2, Sidhu A1, Sathananthan J2, Wood D2, Tsang MY2, Yeung DF2, Luong C2, Nair P2, Jue J2, Gin K2, Tsang TS2. 1University of British Columbia, Vancouver, BC, Canada and 2University of British Columbia, Vancouver, BC, Canada
Purpose of Study: Aortic valve stenosis (AVS) is the most common cause of valvular heart disease in North America, and despite recent medical advancements, symptomatic AVS has a high mortality rate. The invention of transcatheter aortic valve replacement (TAVR) has revolutionized treatment for this disease and has allowed treatment for patients previously unable to tolerate surgical aortic valve replacement (SAVR). As a pioneering faciliity in AVS treatment, we evaluated the relative penetration of each valvular replacement modality and effects on cardiovascular outcomes. This study aims to analyze the pattern of diagnosis and management of this disease, and to explore the effect of demographic characteristics delivery of each resource.
Methods Used: Following institutional review board approval, a retrospective chart review was performed of all echocardiograms of inpatient and outpatients with severe aortic stenosis diagnosed at the Vancouver General Hospital and University of British Columbia (UBC) Hospital from 2012 to 2022. Demographic, clinical, and echocardiographic data were extracted by chart review through divisional and provincial electronic medical records. We evaluated effects of these characteristics on provision of cardiology assessment, SAVR and TAVR eligibility, receipt of AVR, and 1-year cardiovascular outcomes.
Summary of Results: In the last 10 years, the echocardiography team at Vancouver General and UBC Hospital has diagnosed severe aortic stenosis (AS) in 5842 patients. In this preliminary analysis, 700 studies were identified to have severe AS for the first time, which included both inpatients and outpatients. Out of the 700 studies, 301 were female, 398 were male, and 1 was unclassified.
Significant sex differences existed in the provision and delivery of specialist care and AVR. Females were significantly less likely to be evaluated by either TAVR or SAVR services compared to males (60.20% versus 69.19%, p-value 0.018), and significantly less likely to receive AVR (either TAVR or SAVR) compared to males (49.82% versus 63.07%, p-value 0.001).
When comparing cardiovascular outcomes, females have higher rates of 1-year mortality (OR 1.094 [0.789, 1.517]) and heart failure hospitalization (OR 1.085 [0.741, 1.585]) compared to males, although not statistically significant.
Conclusions: From the data, specialist evaluation and AVR procedures are associated with reduced mortality and morbidity in patients diagnosed with severe AVS. The data also reveals several sex-based discrepancies, with females being significantly less likely to be evaluated for AVR despite not having a significantly higher burden of comorbidities. Our research also reveals that females are more likely to incur cardiovascular outcomes, including mortality and heart failure hospitalization. Further research is required to determine whether the lack of specialist evaluation and intervention on female patients has an independent effect on cardiovascular outcomes.
# 85
EXTRACELLULAR RIBOSOMAL PROTEINS IN ISCHEMIC MYOCARDIAL PATHOLOGY
Doescher CI1, Thai AV1, Agrawal DK2, Thankam FG2. 1Western University of Health Sciences, Pomona, CA and 2Western University of Health Sciences, Pomona, CA
Purpose of Study: Myocardial infarction (MI) is the leading cause of death worldwide and in survivors results in adverse myocardial remodeling that impedes contractile function. Unfortunately, current treatments, such as coronary artery bypass grafts (CABG), are associated with the persistence of ischemia and inflammation resulting in suboptimal recovery for the damaged myocardium. Additionally, the common comorbidity of hyperlipidemia in the setting of MI further complicates the recovery process. Our previous research identified extracellular exosomal secretion of ribosomal proteins from epicardial adipose tissue-derived stem cells (EATDS) following ischemia. This study aimed to establish an association between the EATDS-derived exosomal ribosomal proteins and beneficial cardiac remodeling via cardiac fibroblasts (CF). Herein, we aimed to assess the functional role of ribosomal proteins in the ischemia-challenged EATDS and CF cells. We expanded on previously presented research with additional data and analysis that provides a better understanding of the functional role of ribosomal proteins post-MI when compared to hyperlipidemic models.
Methods Used: Mass spectrometry analysis of previously presented samples revealed increased secretion of the ribosomal proteins including RPL10A, RPS30, RPL30, Laminin Receptor (LR), RPS18, and RPL14 in the secretory vesicles of EATDS. The expression level of these mediators was assessed in the EAT and LV tissues harvested from MI and CABG models as reported in our previous discussion. Also, the level of these ribosomal proteins was assessed in vitro cultured EATDS and CF under ischemia using qRT-PCR, Western Blot, and immunofluorescence as we reported previously. We report the expression of the aforementioned extracellular ribosomal proteins in hyperlipidemic porcine models (HL) as compared to our control, MI, and CABG groups and include an analysis via single cell RNA Sequencing (scRNA-seq) for these proteins in all reported models.
Summary of Results: Histologic analysis of the myocardial tissue from the post-MI swine revealed significant inflammation, extracellular matrix (ECM) disorganization, and increased fibrosis suggesting the similar clinical pathology of MI. The expression levels of RPL10A, RPL14, RPL30, RPS18, RPS30, and LR were significantly elevated in the LV tissues of CABG and HL swine but reduced in the MI group. RPS30 showed a similar expression in EAT tissues, whereas all other proteins failed to show a significant difference to the control group in EAT tissues. RPS18, RPL30, and LR of EATDS and CF favored ischemia and revealed anti-inflammatory and regenerative sub-phenotypes reflecting the protective/survival mechanism.
Conclusions: The results highlight the association of extracellular ribosomal proteins with phenotypic and functional changes within the damaged myocardium, suggesting an immense translational potential in the management of ischemic cardiac complications.
# 86
Prevalence of Preexisting Cardiac Disease in Cases of Sudden Cardiac Death After Energy Drink Consumption
Howard BC1, 2, Keyvan N3, Fung A2, Joe T2, Patel AB1, Spak V2, Lee BK2. 1University of California, Davis, School of Medicine, Sacramento, CA; 2UCSF, San Francisco, CA and 3University of Southern California, Los Angeles, CA
Purpose of Study: Over the past 20 years, the popularity of energy drinks has been on the rise. These drinks contain high doses of caffeine and other stimulants which have unclear effects on the heart. There has been accumulating reports of sudden cardiac death (SCD) following energy drink consumption. We sought to examine these SCD cases to better understand the mechanism.
The primary goal of this retrospective cohort study was to identify clinical factors associated with cases of SCD following energy drink consumption.
Methods Used: Using Google Search, cases of sudden cardiac death following energy drink consumption from November 2000 to May 2022 were identified. Searches were performed using phrases “energy drink consumption and sudden cardiac death”, “SCD and energy drinks”, and “death after energy drink consumption”. Once cases of SCD following energy drink consumption were identified, social networking sites were used to find relatives of the victims. They were queried by phone, email, or websites to obtain information about the death. For each case, we sought demographics, descriptions of preexisting cardiac disease, details surrounding the incident, and autopsy results. The data was compiled in an Excel and analyzed using GraphPad Software.
Summary of Results: Forty-five cases of SCD after energy drink consumption were identified. 37/45 (82.6%) of these cases involved males. Of the 42 cases where patient age was known, mean and median age was 27.2 ± 9.6 and 26 years, respectively. 36/42 (85.7%) of the patients were younger than 40 years old. Medical history and autopsy reports were available for 31/45 (68.8%) and 19/45 (42.2%) cases, respectively. Of the 31 cases with available medical records, 14/31 (45.1%) cases had known cardiac disease prior to SCD. 11/19 (57.9%) cases with available autopsy reports had no previously known cardiac disease. Among these 11 cases, 8/11 (72.7%) were found on autopsy to have a newly discovered heart disease. Among all patients with medical records, autopsy, or both, 22/42 (52.4%) had pre-existing cardiac disease at time of SCD.
Conclusions: In cases of SCD after energy drink consumption, the victims are more likely to be a male, young, and have preexisting cardiac disease that can cause SCD. This suggests that the energy drink is not likely to be the primary cause of SCD in most cases, although it still can be a contributing factor.
Clinical Factors Associated with Suddent Cardiac Death.
# 87
COMPARING THE SOCIAL DETERMINANTS OF HEALTH OF PATIENTS WITH SEVERE AORTIC STENOSIS OR MITRAL REGURGITATION THAT RECEIVE OR DO NOT RECEIVE PROCEDURAL INTERVENTION
Nguyen-Khoa JN1, Huang T2, Botting P2, Ebinger J2. 1Touro University California, Vallejo, CA and 2Cedars-Sinai, Los Angeles, CA
Purpose of Study: Social determinants of health (SDoH) are associated with disparities in the treatment and outcomes of cardiovascular diseases. While the association between economic factors and the receipt of valvular heart disease treatment has been examined, less is known about the association with SDoH more broadly. As such, we examined the association between a broad SDoH metric and the receipt of surgical therapy for patients with severe aortic stenosis (AS) or mitral regurgitation (MR).
Methods Used: We identified patients from a large academic medical center meeting criteria for either severe AS or MR by transthoracic echocardiogram between January 2017 and July 2023; from the electronic health record, we then identified which patients received a procedure for their respective valve disease. Next, we extracted patient demographics, comorbidities, and zip codes, the latter of which was linked to the California’s Healthy People Index 3.0 (HPI), a composite score of neighborhood-level SDoH. For analysis, R was used for mean comparison of the procedure and non-procedure AS and MR groups and logistic regression models, with receiving a procedure as the dependent variable.
Summary of Results: Of 2441 patients with AS, 863 (35%) received an aortic valve procedure. Compared to those who did not undergo AS treatment, those who did were generally younger (74.8 vs. 78.22; p<0.001), male (63.73% vs. 54.37%; p<0.001), with fewer comorbid conditions, and similar HPI scores (0.65 vs. 0.64; p=0.077). In multivariable regression analysis, increasing age, Black race, and renal dysfunction were associated with lower odds of receiving AS treatment, while no association was appreciated for HPI (OR 1.31, 0.93-1.86).
Of 1642 patients with MR, 46 (2.8%) received a procedure. Compared to those who did not undergo MR treatment, those who did had fewer comorbid conditions, but similar age (64.44 vs. 68.14; p=0.11), gender (73.91% vs. 60.15% male; p=0.084), and HPI scores (0.66 vs. 0.65; p=0.34). In multivariable regression analysis, increasing heart failure was associated with lower odds of receiving MR treatment, and increasing peripheral vascular disease was associated with greater odds of receiving MR treatment, while no association was appreciated for HPI (OR 1.13, 0.31-4.4).
While no clear association with treatment was found with HPI, certain subdomains were associated with AS treatment, including automobile access, census response, voting, and homeownership (Table 1).
Mean comparison of SDoH percentiles for AS and MR groups.
Aortic Stenosis (AS)
Mitral Regurgitation (MR)
Severe AS
With Procedure
No Procedure
p-value*
Severe MR
With Procedure
No Procedure
p-value*
N
2441
863
1578
N
1642
46
1596
Male, n(%)
1408 (57.68%)
550 (63.73%)
858 (54.37%)
<0.001*
Male, n(%)
994 (60.54%)
34 (73.91%)
960 (60.15%)
0.084
Age,mean (SD)
76.76 (12.6)
74.08 (12.2)
78.22 (12.5)
<0.001*
Age, mean (SD)
68.03 (15.4)
64.44 (15.1)
68.14 (15.4)
0.11
SDoH percentile, mean (SD)
SDoH percentile, mean (SD)
HPI
0.65 (0.43)
0.65 (0.42)
0.64 (0.45)
0.077
HPI
0.65 (0.46)
0.66 (0.38)
0.65 (0.46)
0.34
Above Poverty
0.64 (0.42)
0.64 (0.40)
0.64 (0.43)
0.086
Above Poverty
0.65 (0.43)
0.65 (0.38)
0.65 (0.44)
0.25
Employed
0.57 (0.48)
0.58 (0.48)
0.57 (0.49)
0.68
Employed
0.57 (0.47)
0.60 (0.43)
0.57 (0.47)
0.91
Per Capita Income
0.72 (0.46)
0.72 (0.46)
0.72 (0.47)
0.46
Per Capita Income
0.70 (0.46)
0.73 (0.45)
0.70 (0.46)
0.71
Bachelor
0.72 (0.41)
0.71 (0.40)
0.72 (0.41)
0.59
Bachelor
0.70 (0.42)
0.76 (0.44)
0.70 (0.42)
0.99
High School Enrollment
0.63 (0)
0.63 (0)
0.63 (0)
1
High School Enrollment
0.63 (0)
0.63 (0)
0.63 (0)
0.41
Preschool Enrollment
0.65 (0.51)
0.64 (0.51)
0.66 (0.50)
0.15
Preschool Enrollment
0.63 (0.5)
0.65 (0.42)
0.63 (0.51)
0.63
Active Commuting
0.49 (0.49)
0.43 (0.48)
0.52 (0.49)
<0.001*
Active Commuting
0.46 (0.5)
0.35 (0.47)
0.46 (0.50)
0.092
Automobile Access
0.46 (0.50)
0.51 (0.49)
0.43 (0.48)
<0.001*
Automobile Access
0.51 (0.51)
0.61 (0.47)
0.50 (0.52)
0.07
2020 Census Response Rate
0.43 (0.47)
0.49 (0.47)
0.39 (0.48)
<0.001*
2020 Census Response Rate
0.47 (0.5)
0.60 (0.55)
0.47 (0.50)
0.43
Voting
0.52 (0.40)
0.55 (0.39)
0.51 (0.39)
<0.001*
Voting
0.54 (0.42)
0.64 (0.46)
0.54 (0.42)
0.1
Low-Income RenterSevere Housing Cost Burden
0.5 (0.47)
0.51 (0.48)
0.49 (0.47)
0.37
Low-Income RenterSevere Housing Cost Burden
0.50 (0.49)
0.59 (0.49)
0.50 (0.49)
0.11
Low-Income HomeownerSevere Housing Cost Burden
0.44 (0.50)
0.43 (0.48)
0.45 (0.50)
0.92
Low-Income HomeownerSevere Housing Cost Burden
0.44 (0.49)
0.56 (0.51)
0.44 (0.48)
0.089
Housing Habitability
0.42 (0.62)
0.43 (0.61)
0.41 (0.63)
0.36
Housing Habitability
0.45 (0.6)
0.56 (0.57)
0.45 (0.60)
0.37
Uncrowded Housing
0.67 (0.46)
0.68 (0.46)
0.66 (0.46)
0.2
Uncrowded Housing
0.67 (0.49)
0.79 (0.45)
0.67 (0.49)
0.23
Homeownership
0.5 (0.56)
0.54 (0.55)
0.47 (0.55)
<0.001*
Homeownership
0.53 (0.55)
0.63 (0.49)
0.53 (0.55)
0.12
Insured Adults
0.59 (0.46)
0.60 (0.43)
0.59 (0.46)
0.14
Insured Adults
0.57 (0.47)
0.61 (0.59)
0.57 (0.47)
0.71
Diesel PM
0.51 (0.45)
0.55 (0.44)
0.49 (0.47)
<0.001*
Diesel PM
0.51 (0.47)
0.56 (0.45)
0.51 (0.47)
0.26
Drinking Water Contaminants
0.29 (0.29)
0.30 (0.29)
0.27 (0.32)
0.0028*
Drinking Water Contaminants
0.31 (0.34)
0.35 (0.32)
0.30 (0.34)
0.64
Ozone
0.37 (0.38)
0.34 (0.42)
0.38 (0.35)
0.16
Ozone
0.41 (0.40)
0.46 (0.51)
0.41 (0.40)
0.46
PM 2.5
0.34 (0.2)
0.36 (0.24)
0.33 (0.19)
0.071
PM 2.5
0.34 (0.24)
0.40 (0.38)
0.34 (0.24)
0.2
Park Access
0.42 (0.61)
0.42 (0.59)
0.42 (0.61)
0.47
Park Access
0.45 (0.59)
0.47 (0.59)
0.45 (0.59)
0.79
Retail Density
0.61 (0.53)
0.57 (0.53)
0.64 (0.51)
<0.001*
Retail Density
0.62 (0.53)
0.51 (0.56)
0.62 (0.53)
0.14
Tree Canopy
0.56 (0.37)
0.55 (0.38)
0.56 (0.37)
0.78
Tree Canopy
0.52 (0.41)
0.44 (0.44)
0.52 (0.41)
0.58
Study groups, baseline characteristics, and simple comparison of the mean percentiles of various SDoH subdomains between procedure and non-procedure AS and MR groups. **Significant at the 5% level.
Conclusions: Patients who received an aortic procedure had a more favorable SDoH with greater mean percentiles in automobile access, census response, voting, and homeownership, but not overall HPI. There were no significant differences between the MR groups. HPI was not independently predictive of receiving an aortic or mitral procedure. Importantly, a large portion of patients with severe valve disease were lost to follow-up, indicating both a potential bias, as well as a clear opportunity for improvement in care delivery.
Diversity, Equity, Inclusion Research I
Concurrent Session
3:15 PM
Thursday, January 18, 2024
# 88
Trends in Plastic Surgery Residents by Gender and Race – Are Our Efforts at Reducing Disparities Enough?
Petersen G1, Kadakia N2, Brandt Z1, Chung JH3, Myint J2, Wongworawat MD2, Kim H2. 1Loma Linda University, Loma Linda, CA; 2Loma Linda University Health, Loma Linda, CA and 3Loma Linda University Health, Loma Linda, CA
Purpose of Study: Although the diversity in surgery has improved, the number of women and underrepresented populations remains low in plastic surgery compared to other surgical subspecialties (Reghunathan 2021). There is a need for more data on the intersectionality of gender and race in the field. Our research aims to analyze the relative risk of going unmatched based gender and ethnicity. This study aims to contribute to the ongoing discussion on diversity in medicine and to promote equality and access to plastic surgery training.
Methods Used: To obtain demographic information on integrated plastic surgery residents during the academic years from 2016-2017 to 2021-2022, the authors acquired ACGME data books. Corresponding applicants for each academic year were then determined using publicly available ERAS statistics from the AAMC website. These corresponding applicants were comprised of residents in training from the preceding six years. By comparing the race and gender composition of the applicant pool to that of the enrolled residents, the relative risk of not matching was calculated for women compared to men, and for underrepresented populations (Blacks, Hispanics, Asians, Native Americans) compared to White applicants.
Summary of Results: Overall, there was an increase in the total number of applicants from 328 in 2011 (32.0% female) to 420 in 2022 (46% female) [ p< 0.001]. With a reciprocal decrease in the percentage of male applicants from 68% to 54% (p< 0.001). There was also an increase in the percentage of total female residents from 41% in 2016 to 43% in 2022 (p< 0.001 ). For integrated plastic surgery applicants in 2011-2016, when compared to the gender make-up of residents in training during the 2016-2017 year, women were more likely to match when compared to men (RR 0.87 [0.95% CI 0.83 to 0.91]; p < 0.001). This trend was persistent among residents in training in 2021-2022, when women had a further lower risk of not matching (RR 0.85 [0.79 to 0.92]; p < 0.001). However, for underrepresented populations, applicants consistently had a higher risk of not matching when compared to White applicants. In the past 11 years, Black, Hispanic, and Native American applicants experienced an increase in relative risk of not matching from 2016-2017 to 2021-2022. The exception being Asian applicants with an opposite trend from a significantly elevated relative risk in 2016-2017 (RR 1.10 [0.95% CI 1.05 to 1.15]; p < 0.001) to a nonsignificant elevated relative risk in 2021-2022 (RR 1.07 [0.95% CI 0.99 to 1.17]; p =0.11)
Conclusions: Over the last 11 years, female applicants have experienced an increased success rate in the plastic surgery match. This is a step in the right direction for diversifying gender in plastic surgery. Underrepresented populations have experienced less success in matching into plastic surgery as compared White applicants. Active efforts are needed to combat ethnic disparities in the plastic surgery match in the future.
Relative Risk of not matching for underrepresented populations and women when compared to White applicants and men, respectively. [p value 0.05].
Relative Risk of Not Matching
Residency Year
Black (95% CI)
Hispanic (95% CI)
Asian (95% CI)
Native (95% CI)
Women (95% CI)
2016-2017
1.19 (1.14-1.25)
1.20 (1.15-1.25)
1.10 (1.05-1.15)
1.11 (0.97-1.29)
0.87 (0.83-0.91)
2017-2018
1.19 (1.13-1.25)
1.22 (1.17-1.27)
1.10 (1.06-1.15)
1.14 (0.99-1.31)
0.86 (0.82-0.90)
2018-2019
1.24 (1.17-1.31)
1.28 (1.22-1.34)
1.14 (1.08-1.20)
1.28 (1.15-1.42)
0.84 (0.79-0.89)
2019-2020
1.24 (1.16-1.33)
1.30 (1.23-1.37)
1.14 (1.07-1.20)
1.32 (1.19-1.47
0.84 (0.79-0.89)
2020-2021
1.33 (1.24-1.42)
1.34 (1.26-1.42)
1.13 (1.06-1.17)
1.41 (1.27-1.56)
0.84 (0.79-0.89)
2021-2022
1.49 (1.38-1.62)
1.58 (1.48-1.69)
*1.07 (0.99-1.17)
1.78 (1.70-1.87)
0.85 (0.79-0.92)
# 89
TRENDS IN THE EMERGENCY MEDICINE MATCH RATES BY GENDER AND RACE: POTENTIAL IMPACTS OF VIRTUAL INTERVIEWS
Brandt Z1, Lorson R1, Oliinik M1, Yankee E1, Chung JH2, Wongworawat MD2. 1Loma Linda University School of Medicine, Loma Linda, CA and 2Loma Linda University, Loma Linda, CA
Purpose of Study: The authors examined the match rates of underrepresented populations: Black, Hispanic, Asian, and Native applicants versus White applicants; and separately examined the match rates of male versus female applicants in Emergency Medicine. Using data from residency years 2015-2022 authors investigated the current state of diversity in Emergency Medicine including data on how virtual interviews changed match trends.
Methods Used: Data on applicants who matched was obtained from Accreditation Council of Graduate Medical Education data books spanning from 2015-2016 to 2021-2022. To determine the corresponding applicants who applied to each academic year, the authors used Electronic Residency Application Service statistics. To account for the difference in the length of programs, the ratio of 3- and 4-year programs was used to calculate a weighted average of relative risks of not matching for each demographic group in each academic year. The authors subsequently compared the relative risk of not matching for both women compared to men, as well as for underrepresented populations compared to White applicants.
Summary of Results: Underrepresented populations had a consistently higher relative risk of going unmatched across all years studied (p <0.001). Contrarily, for the duration of years examined, female applicants had a lower relative risk of going unmatched (p<0.05). In the year when applicants first interviewed online, there was a drop in the relative risk of going unmatched in all groups studied.
Conclusions: Significant differences were observed between White applicants’ match rates and those of underrepresented populations. These discrepancies were seen to worsen over the years studied while an opposite trend was observed for female applicants. Notably, in the academic year in which applicants were first interviewed online, there was a drop in the relative risk of not matching in every group. Although there are limited sample years to make this claim, a compilation of future applicant and matriculant comparisons would elucidate the effect of virtual interviews on match equity.
Residency Years
Black (95% CI)
Hispanic (95% CI)
Asian (95% CI)
Native (95% CI)
Women (95% CI)
2015-2016
1.35 (1.27 to 1.43)
1.46 (1.39 to 1.53)
1.42 (1.37 to 1.48)
1.82 (1.69 to 1.97)
0.92 (0.88 to 0.95)
2016-2017
1.56 (1.47 to 1.65)
1.60 (1.52 to 1.69)
1.58 (1.52 to 1.65)
2.07 (1.90 to 2.25)
0.95 (0.91 to 0.99)
2017-2018
1.67 (1.56 to 1.78)
1.73 (1.64 to 1.83)
1.67 (1.59 to 1.75)
2.30 (2.11 to 2.51)
0.91 (0.86 to 0.95)
2018-2019
1.78 (1.67 to 1.90)
1.81 (1.71 to 1.91)
1.71 (1.63 to 1.80)
2.42 (2.22 to 2.64)
0.89 (0.84 to 0.94)
2019-2020
2.05 (1.92 to 2.19)
2.15 (2.03 to 2.33)
1.86 (1.76 to 1.96)
2.60 (2.34 to 2.89)
0.84 (0.80 to 0.89)
2020-2021
1.89 (1.77 to 2.02)
2.21 (2.09 to 2.33)
1.47 (1.39 to 1.56)
3.04 (2.86 to 3.24)
0.86 (0.81 to 0.90)
2021-2022
1.83 (1.72 to 1.94)
1.26 (1.17 to 1.35)
1.42 (1.34 to 1.50)
2.91 (2.74 to 3.09)
0.79 (0.75 to 0.83)
Table 1. Relative Risk of going unmatched for underrepresented populations when compared to White applicants along with women compared to male applicants. For all years and all groups p.
Trends in relative risks of not matching, underrepresented populations compared to White applicants, Women compared to Men from 2015-2022.
(Listed years (x-axis) indicates start of residency, not year of interview).
# 90
ENHANCING EMPATHY TOWARDS INDIVIDUALS WITH SUBSTANCE USE DISORDER
Alnaser M, Kim H, Luna-Valdez D, Butler A, Morauske R, Hayton A. Loma Linda University, Loma Linda, CA
Purpose of Study: In 2019, 20.4 million Americans in the U.S. suffered from substance use disorder (SUD). In 2021, the number increased to 61.2 million. As the number continues to rise and the opioid epidemic continues to spread, the healthcare system must adapt to face this crisis. One of the most important aspects of treating and healing patients with SUD is empathy. This project focused on evaluating the level of stigma among third-year medical students toward individuals with SUD. We aim to analyze the relationship between empathy and students’ prior exposure, feelings, and perceptions of individuals with SUD. and correlate it to their exposure level (family members, personal struggle, in the hospital).
Methods Used: Data from third-year medical students at Loma Linda University was collected using a modified version of The Opening Minds Stigma Scale for Health Care Providers (OMS-HC) to assess for stigma amongst medical students against individuals with SUD. Non-scored questions were included to assess and compare self-perception versus actual perception based on the scored questions.
Summary of Results: Results show that out of 87 students (1/2 of the third-year class), 38% had stigma against SUD while the average stigma score of the combined results leaned toward “no bias” against SUD. The analysis also shows that among the students who said they would treat an individual with SUD the same as any other patient, 70.6% were biased according to their overall survey scores.
Conclusions: Our study identifies gaps in medical school education where the stigma against SUD is not addressed. It found that students at Loma Linda as a whole expressed empathy toward the SUD population. The survey pointed out areas of potential bias among the students and how one’s qualitative perceptions don’t always equate the objective results. This study informs specific interventions around stigma to be added to the curriculum in the future.
# 91
COMPARISON OF THE SOCIAL DETERMINANTS OF HEALTH IN SURGICAL AORTIC VALVE REPLACEMENT VS. TRANSCATHETER AORTIC VALVE REPLACEMENT PATIENTS FOR THE TREATMENT OF AORTIC STENOSIS
Saldivar P1, Ebinger J2, Huang T2. 1University of California, Riverside, Riverside, CA and 2Cedars-Sinai Medical Center, Los Angeles, CA
Purpose of Study: The impact of social determinants of health (SDoH) on the decision to pursue surgical aortic valve replacement (SAVR) or transcatheter aortic valve replacement (TAVR) for the treatment of severe aortic stenosis (AS) is poorly understood. This study compared patient-level characteristics and neighborhood-level SDoH in a real-world cohort of patients who underwent SAVR and TAVR in a large health system.
Methods Used: This retrospective cohort analysis used data from an electronic health record, Society of Thoracic Surgeons (STS), and Transcatheter Valve Therapy (TVT) registries to evaluate differences in demographic, clinical, and SDoH (using the California Healthy Patient Index [HPI]) of 3728 adult patients who underwent SAVR or TAVR at a large academic medical center. Patient and clinical characteristics were analyzed using two-sample t-tests. Multivariable logistic regression analysis was performed, controlling for demographic and clinical characteristics, to evaluate the association between HPI and treatment modality for AS.
Summary of Results: Between December 2014 and May 2023, 486 patients underwent SAVR and 3242 underwent TAVR. On average, SAVR patients were younger (64 v. 79; p<0.001). No differences in the racial composition were appreciated between the groups, however, a higher proportion of the SAVR population identified as Hispanic (14.2% v. 9.7%; p<0.01). In a fully adjusted model, patients who underwent TAVR were more likely to have a history of diabetes mellitus (OR 1.55; 95% CI 1.20-2.03) and heart failure (9.45; 6.1-15.11), while were less likely to have a history of prior myocardial infarction (0.6; 0.42-0.84) compared with SAVR patients. Finally, a lower HPI (indicative of a less healthy living environment) was associated with a decreased likelihood of undergoing TAVR compared with SAVR (0.57; 0.35-0.92).
Conclusions: In the treatment of AS, patients living in less healthy neighborhoods with a lower SDoH score were less likely to undergo TAVR than SAVR, even when controlling for traditional demographic and clinical characteristics. Further work is required to understand individual, community, and health system variables that may be contributing to disparities in the utilization of novel treatment modalities for valvular heart disease.
Patient Characteristics
Total (n=3728)
SAVR Patients (n=486)
TAVR Patients (n=3242)
p-value*
Male, n (%)
2303 (61.78)
356 (73.25)
1947(60.06)
< 0.001
Age, mean (SD)
76.88 (12)
63.81 (12.2)
78.84 (10.6)
< 0.001
Age Category, n (%)
< 0.001
18-50
120 (3.21)
71 (14.6)
49 (1.51)
51-65
437 (11.72)
163 (33.5)
274 (8.45)
66-75
924 (24.79)
176 (36.2)
748 (23.07)
>75
2247 (60.27)
76 (15.6)
2171 (66.96)
Race, n (%)
0.25
White
3011 (80.8)
382 (78.6)
2629 (81.1)
Black
153 (4.1)
19 (3.9)
134 (4.1)
Asian
213 (5.7)
38 (7.8)
175 (5.4)
Other
292 (7.8)
41 (8.4)
251 (7.7)
Unknown
59 (1.6)
6 (1.2)
53 (1.6)
Hispanic, n (%)
382 (10.25)
69 (14.2)
313 (9.7)
<0.01
Post-Procedure Outcome, n (%)
Outcomes Combined**
598 (16)
152 (31)
446 (14)
< 0.001
Cardiac Arrest
12 (0.32)
7 (1.4)
5 (0.15)
< 0.001
Stroke/Transient Ischemic Attack
39 (1)
6 (1.2)
33 (1)
0.84
Aortic Complications
8 (0.21)
0 (0)
8 (0.25)
0.57
Unplanned Aortic Intervention
92 (2.5)
0 (0)
92 (2.8)
< 0.001
Unplanned Return to OR for Other Cardiac Reasons
39 (1)
6 (1.2)
33 (1)
0.84
Coronary Artery Complications
49 (1.3)
1 (0.21)
48 (1.5)
0.037
New Atrial Fibrillation/Flutter
146 (3.9)
118 (24)
28 (0.86)
< 0.001
New Dysrhythmia Requiring Pacemaker
209 (5.6)
12 (2.5)
197 (6.1)
0.002
Major Vascular Complication
51 (1.4)
0 (0)
51 (1.6)
0.01
Post-Op Bleeding
52 (1.4)
22 (4.5)
30 (0.93)
< 0.001
Pericardium Complications
7 (0.19)
3 (0.62)
4 (0.12)
0.074
Gastrointestinal Event
7 (0.19)
3 (0.62)
4 (0.12)
0.074
Renal Complications
18 (0.48)
3 (0.62)
15 (0.46)
0.91
*Comparing patients who underwent SAVR vs patients who underwent TAVR, p values between means for SDoH variables calculated using two-sample t-test. p-value < 0.05 notes a significant difference. ** Outcomes combined indicates if any other outcome presents for the patients.
# 92
QUALITATIVE HISTORICAL ANALYSIS ON DECOLONIAL AND ANTI-OPPRESSIVE FORMS OF PRACTICING PSYCHIATRY IN NORTH AND WEST AFRICA DURING POSTCOLONIAL TRANSITIONS (1950S) WITH CASE STUDIES COMPOSED OF THE CLINICAL PRACTICE OF DR. FRANTZ FANON AND DR. THOMAS ADEOYE LAMBO
Olivas-Blanco JM. UC Davis, Sacramento, CA
Purpose of Study: The purpose of this research is to advance the conversation regarding incorporating anti-oppressive and decolonial ideas and methods of medical practice into Psychiatry and medicine at large. The aims were to find the specific methodologies advanced by Dr. Lambo and Dr. Fanon in the transition period from colonial to post-colonial times in Northern and Western Africa, with the intention of applying these concepts to the modern landscape of medicine.
Methods Used: This was a qualitative historical analysis in which records were found (primary sources when possible) to unearth the practices of Dr. Fanon and Dr. Lambo.
Summary of Results: The qualitative historical analysis of decolonial and anti-oppressive psychiatric practices in Northern Africa, exemplified by Dr. Frantz Fanon’s work in Blida-Joinville and The Neuropsychiatric Day Centre of Tunis, along with Dr. Thomas Adeoye Lambo’s Aro Village System in Nigeria, underscores the transformative shift from colonial pathologization to culturally sensitive, patient-centered care. Fanon’s recognition of colonialism’s psychic effects and his emphasis on social aspects, cultural humility, and intersectionality offer essential lessons for equitable mental healthcare. Additionally, Fanon’s advocacy for integrating psychiatric services with general healthcare promotes destigmatization and patient agency. Dr. Lambo’s pioneering approach in Nigeria, incorporating traditional healing methods, proto-epidemiological studies, and cultural competence, highlights the importance of adapting psychiatric practices to local contexts and respecting patients’ cultural beliefs, reinforcing the need for culturally sensitive and contextually aware psychiatric care.
Conclusions: Dr. Lambo’s and Dr. Fanon’s work to advance a more humanistic and historically informed psychiatry has valuable lessons for the practicing psychiatrist in the 21st century. Their lessons in incorporating patients’ culture, changing hospital practices, and having an oppression-informed method of care are all valuable lessons for us now.
# 93
Perceived Stress in Female Medical Students Pursuing Male-Dominated vs. Female-Dominated Surgical Specialties
Hakel J, Gasbeck T, Gerriets V. California Northstate University, Elk Grove, CA
Purpose of Study: Surgical specialties are consistently amongst those with the greatest proportion of male physicians. Current literature has demonstrated poorer mental health outcomes and job satisfaction in female resident physicians working within male-dominated surgical specialties (MDSS) compared to those in female-dominated surgical specialties (FDSS). This disparity has largely been attributed to workplace gender discrimination, and prior publications demonstrate that female medical students experience similar discrimination. Therefore, the purpose of this study was to investigate whether female medical students pursuing MDSS (F-MDSS) experience similar adverse mental health outcomes as those observed in female residents in these fields. We hypothesized that F-MDSS experience higher levels of stress compared to those pursuing FDSS, similar to what is reported in female surgical residents.
Methods Used: A cross-sectional study was performed using results from voluntary surveys of medical students at California Northstate University College of Medicine that collected information on measures of mental wellness and preferred speciality. Stress was quantified on a scale from 0 to 40 using the Perceived Stress Scale (PSS-10) questionnaire. Students were grouped according to gender and preferred specialty, and mean PSS-10 scores were compared between these groups using a two-tailed t-test.
Summary of Results: Among the 251 survey participants, the 18 F-MDSS responses had a mean PSS-10 score of 18.39, the highest score of any of the studied groups. However, they were marginally separated from F-FDSS by difference of +0.08, which was not determined to be statistically significant (p=0.985).
Respondents with a preference for a surgical specialty demonstrated an average +1.73 increase in stress scores relative to nonsurgical respondents (p=0.0296) and females demonstrated an average +3.14 increase when compared to males (p=0.0002). Compared to males pursuing any surgical specialty, females pursuing surgery demonstrated a +3.98 increase in stress scores (p=0.001), the largest difference between any two groups.
Conclusions: While prior publications have demonstrated that female surgical residents in MDSS experience higher levels of stress than their male counterparts, this effect was not replicated for our surveyed students. Our analysis yielded minimal differences in stress levels between female subjects pursuing MDSS or FDSS, suggesting that gendered differences in mental health for female trainees in MDSS are not present prior to the onset of surgical training. This raises the question of whether the reported burnout and depression experienced by female surgical residents is due to environmental factors specific to male-dominated specialties. Moreover, both female gender and surgical specialties were associated with higher stress levels and should therefore be considered as contributors to poorer mental health in female surgical residents.
Difference in Mean Stress.
Group 1
PSS-10 (x1)
Group 2
PSS-10 (x2)
ΔX (x1 – x2 )
p-value
Females
17.007
Males
13.872
3.135
0.0002*
Students pursuing surgical specialties
17.221
Students pursuing non-surgical specialties
15.447
1.774
0.0296*
Females pursuing surgical specialties
18.333
Males pursuing surgical specialties
14.353
3.980
0.0001*
Females pursuing FDSS (F-FDSS)
18.310
Females pursuing surgical specialties
18.333
-0.023
0.9853
Females pursuing FDSS (F-FDSS)
18.310
Females pursuing MDSS (F-MDSS)
18.389
-0.079
0.9603
Females pursuing FDSS (F-FDSS)
18.310
Females
17.007
1.303
0.1791
# 94
RACIAL AND ETHNIC DISPARITIES IN ADHERENCE TO ANTI-SEIZURE MEDICATIONS AMONG PATIENTS WITH EPILEPSY
Jian Y1, Borhade A1, Choi L1, Lee B1, Lee G1, Shabbak R1, Wategaonkar A1, Afghani B1, 2. 1UC Irvine School of Medicine, Irvine, CA and 2CHOC Hospital of Orange County, Orange, CA
Purpose of Study: Because of advances in treatment, antiseizure medications play an important role in improving seizure control. Nonadherence to antiseizure medications is a significant problem that is linked to increased morbidity and increased healthcare costs. The purpose of this study is to assess the extent of racial disparities in adherence to antiseizure medication among patients with epilepsy.
Methods Used: A literature review was performed on PubMed and Google Scholar databases and searching the bibliograph of relevant articles for any additional studies. We used key terms: “epilepsy”, “racial disparity”, ethnic disparity”, “management”, “anti-seizure medication” and “adherence”. We included studies of pediatric or adult patients with epilepsy published after year 2000 which compared the difference in medication adherence rates among populations from different racial backgrounds.
Summary of Results: Of the 13 articles found, only 5 met our inclusion criteria (see Table 1). The vast majority of patients in different studies were on multiple seizure medications. Although the studies used different measurements of outcome, all studies found that people of color (Black, Asian, Hispanic, Native Hawaiian/Pacific Islanders, and multiracial groups) were less likely to adhere to anti-seizure medication compared to Whites. The non-adherence was more prominent in African-Americans. The limitations included heterogeneity among the studies in definition of nonadherence and adjusting for different variables. For example, severity of seizures, the number of anti-seizure medications, distance from the neurology subspecialty, and other demographic factors such as education income, or insurance type were not taken into account by some studies.
Conclusions: Our literature review suggests that patients belonging to minority populations, especially African-Americans, have significantly poorer antiseizure medication adherence. As multiple variables play a role in medication non-compliance, randomized controlled trials are needed to confirm our findings. Additionally, targeted interventions will be needed to remove barriers and improve antiseizure medication adherence and existing disparities that impact minority groups.
Studies of Antiseizure Medications Adherence among Patients from Different Racial Backgrounds.
First author last name, year published
Age group studied
Number (%) in each ethnic group
Outcome measured
Comparison or Odds ratio and p-value or Confidence Interval
Adherence to antiseizure medications (ASM), and proportion of days covered (PDC)* for 3rd generation ASMs
Odds of being on newer generation ASMs with Whites used as reference:Black: OR = 0.71 [95% CI: 0.68–0.75]
Hispanic: OR = 0.93 [95% CI: 0.88–0.99]NHOPI individual: OR = 0.77[95% CI: 0.67–0.88])Adherence odds ratio with Whites used as reference:Black: OR = 0.62 [CL = 0.6-0.65]
Asian: OR= 0.81 [Cl= 0.72-0.92]
Hispanic: OR = 0.78 [Cl = 0.74-0.82]"
Adherence to antiseizure medication with the following definition:High adherence = adherence of > 95% and did not require any intervention.Suboptimal adherence = Adherence
Odds ratio of being the suboptimal adherence group:
Children of color (i.e., Black, Asian, or multiracial): OR = 3.26 [p = .009]Black children: OR = 2.90 [p = .002]"
Proportion of days covered (PDC) for antiseizure medication, divided to groups based on adherence:
Early adherent group = PDCs re-mained above approximately 80% throughout
Early nonadherent group = PDCs dropped toward 0 within the first several quarters
Odds ratio of early nonadherent vs early adherence group:
Black OR=1.7 [CI=1.5-1.8 p< 0.01]Asian OR = 1.9 [Cl = 1.4 - 2.5 p< 0.01]Hispanic OR = 1.7[ Cl = 1.4-2.0 p< 0.01]
Gutierrez-Colina, 2021
Pediatrics; 2-17 y/o
White: n= 185 (81.9%)
Black: n= 41 (18.1%)
Barriers to adherence Pediatric Epilepsy Medication Self-Management Questionnaire:Higher sub-scale scores = greater endorsement of adherence barriers
Adherence rates:Black vs White 71.35% vs 85.23% [p=0.02]
Main barriers after controlling for socioeconomic status score (Black vs. White):
Running out of medications [F= 10.68, P=0.002],Competing demands [F=7.81, P=0.008]
Difficulty getting medications from the pharmacy [F=7.88, P=0.008]
Bautista, 2011
Adults; mean age = 42 y/o
White = 59 (54.6%)Black= 49 (46.4%)
Medication possession ratio(MPR) = the number of days between prescription refills (30 days) divided by the actual number of days between prescription refills.
Adherence as measured by MPR:White vs Black: 0.872 vs 0.796 (p = 0.02)
PDC: The PDC represents the days’ supply of medication that was dispensed divided by the total number of days in that calendar period, OR=Odds Ratio, CI=Confidence Interval.
# 95
RACIAL DISPARITIES IN SURVIVAL OF FEMALES WITH LATE-STAGE BREAST CANCER: A REVIEW OF THE LITERATURE
Rauf M1, Chai D1, Chao J1, Daza N1, Dharnidharka A1, Ly B1, Megid K1, Afghani B1, 2. 1UC Irvine School of Medicine, Irvine, CA and 2CHOC Hospital of Orange County, Orange, CA
Purpose of Study: Breast cancer is the second leading cause of cancer deaths in the United States. Although overall mortality has been declining, there has been a suggestion of possible disparities in survival among different ethnic groups with breast cancer. The purpose of this study was to compile the literature to determine whether disparities in survival exist in late-stage disease among different ethnic groups.
Methods Used: A literature review was conducted in PubMed and Google Scholar using the keywords: “breast cancer”, “survival”, “mortality”, “late stage”, “racial disparity” and “stage III-IV”. We included studies that were performed in the USA and published after 2015. Only studies that classified the breast cancer survival or mortality rate according to late-stage III-IV across different ethnicities were included in our review. Studies that only included early stages and did not compare survival across different races were excluded.
Summary of Results: Five studies satisfied our inclusion criteria (see table). All studies found that Black patients had higher mortality than their White counterparts. However, for Hispanic patients, three studies found inconsistent relationships between the survival when compared to White patients. One study found no difference in survival, and two studies found lower mortality in Hispanics compared to Whites. Other confounding variables that could play a role in survival, such as age, tumor characteristics (stage, receptor positivity, size, genetics), socioeconomic status, income, residence, marital status, and type of treatment were included in some of the studies. The observational-population-based nature of the studies poses some limitations as the reviewed studies were not consistent in adjusting for the same variables that could play a role in disparities. Additionally, most of the studies did not consider other comorbidities that could contribute to mortality.
Conclusions: This literature review suggests Black patients with late-stage breast cancer have lower survival rates compared to White patients. Our study highlights the need for future studies that evaluate the variables that could lead to racial disparities and examine the effectiveness of interventional programs to improve survival in those impacted by such disparities.
Studies comparing racial/ethnic disparities in patients with late-stage breast cancer.
First author and year published
Source of data and years included
Total number of subjects + definition of subjects
Definition of outcome
Comparison of survival or mortality rates (percentages) of different ethnic groups
Other variables adjusted for
Primm, 2022
Surveillance, Epidemiology, and End Results (SEER) Program of national Cancer Institute, 2000 to 2017
Total N=841,975; White: N=592,874; Black: N=89,297; American Indian: N=4,360; East Asian: N=24964; South Asian: N=6178; Southeast Asian: N=22206; other Asian: N=8623; Pacific Islander: N=5202; Hispanic: N=88271
5-year cancer-specific death rate for late stage
White: 1.00 (Reference)
Hazard Ratio
Blacks: 1.39 (95% CI: 1.15-1.21), p<0.001
American indian: 0.9 (95% CI: 0.79-1.03), p=0.13
East Asian: 0.85(95% CI, 0.79-0.9), p<0.001
South Asian: 0.82 (95% CI: 0.73-0.92), p=0.001
Hispanic: 0.95 (95% CI: 0.92-0.98), p<0.001
Age at diagnosis, pathology, receptor positivity, income, surgery, marital status
Miller, 2017
CDC National Program for Cancer, 2001-2009
Regional breast cancer total: Whites=343,830, Blacks=50,385
Distant breast cancer: Whites= 54,535, Blacks=10,730
Net 5-year survival for late stage
Survival: Whites vs Blacks
a) Regional (local spread):
2001-2003: 82.3% vs. 69.9%, p<0.05
2004-2009: 83.5% vs.71.8%, p<0.05
b) Distant Breast Cancer
2001-2003: 22.5% vs 15.2%, p<0.05
2004-2009: 25.7% vs 17.1%, p<0.05
Age at diagnosis, state of residence
Akinyemiju, 2016
Surveillance, Epidemiology, and End Results (SEER) Program of national Cancer Institute, 2000 to 2010
Breast Cancer Specific Deaths:
White: 40.8%
Black: 46.5%
Hazard Ratio:
Overall: 1.20 (95% CI:1.06-1.36)
Age, stage at diagnosis, subtype, SES, region of residence, insurance status
Ren, 2018
Surveillance, Epidemiology, and End Results database, 2010-2014
Non-Hispanic White (NHW), N=8503, Non-Hispanic Black (NHB), N=2204, Hispanic, N=1410, Non-Hispanic Asian
or Pacific Islander/American Indian/Alaskan Native (NHA), N=949
Age at diagnosis, SES (individual-level insurance and marital status, together with area-level neighborhood SES), tumor characteristics (histological type, grade, tumor size, number of positive regional lymph nodes, and molecular subtype) and metastatic patterns (number and site of distant metastases)
CI=Confidence Interval.
# 96
RACIAL DISPARITIES IN BONE MARROW UTILIZATION FOR THE TREATMENT OF ACUTE MYELOGENOUS LEUKEMIA IN THE ADULT POPULATION: A LITERATURE REVIEW
Sabour R1, Guillory M1, Koh M1, Labatia N1, Sunkara S1, Vishwarupe M1, Zettersten-Mansour F1, Afghani B1, 2. 1UC Irvine School of Medicine, Irvine, CA and 2CHOC Hospital of Orange County, Orange, CA
Purpose of Study: Hematopoietic stem cell transplant (HSCT) has been shown to improve the survival of many patients suffering from acute myelogenous leukemia (AML). However, timely access and other variables are critical to a successful outcome. As the utilization and indications for HSCT expands, there is a continued need to understand the multifactorial barriers which lead to inequalities in transplant utilization and survival. The objective of this literature review is to summarize findings of studies that tried to evaluate the impact of racial disparities on utilization of HSCT in adult patients with AML.
Methods Used: We conducted a systematic literature search in PubMed, Google Scholar, and Medline to better understand the effects of race on access to HSCT among AML patients. A combination of the following keywords was utilized in our search: “bone marrow transplant”, “acute myelogenous leukemia”, “Hematopoietic stem cell transplant”, “AML”, “racial disparities”, and “ethnicity”. We included studies performed in the USA of adult patients with AML which compared HSCT utilization/receipt rates among different ethnicities after adjusting for different confounding variables.
Summary of Results: A total of 4 studies satisfied our inclusion criteria (see Table). All 4 studies found that minority populations, such as Blacks and non-White Hispanic patients with AML were less likely to receive HSCT compared to White patients. The source of data and methodologies for reporting the outcome were different among the studies. Majority of the studies adjusted for sex, age, socioeconomic and insurance status. However, the limitations of the studies include lack of homogeneity in considering other confounding variables, such as cytogenetics, comorbidities, stage of AML, referral patterns, donor availability, household income, and access to transplant centers.
Conclusions: Our literature review suggests that in the US, minority population with AML, such as Blacks and Hispanics are less likely to receive HSCT. However, the reasons behind this finding are most likely multifactorial. Further large prospective studies are warranted to evaluate the reasons behind the persistence of the racial disparities in bone marrow utilization. Interventional programs tailored to address the reasons behind the lower rate of transplants in Hispanics and Blacks are warranted.
Studies of hematopoietic cell transplantation (HCT) in patients with AML according to their race/ethnicity.
First Author and Year Published
Location and Data Source
Age, Groups Compared with AML
Comparison of Outcome(HCT Likelihood)
What Other Covariates Were Accounted For
Joshua, 2010
Surveillance, Epidemiology, and End Results (SEER) Cancer Registry (1997 to 2002)
Age group> 15 years of age AML cases Ntotal=10,029 HCT recipients N=1106 Non-Hispanic (NH)-Whites=671 Hispanics=229 NH-Blacks=34 Asians/other=172
Hispanics vs NH-Whites: 20.7% vs 60.7% RR=0.86 (95% CI: 0.75-0.99)NH-Blacks vs NH-Whites: 3.1% vs 60.7%; RR=0.60 (CI: 0.44-0.83)
Adjusted for marital status, SES, distance from transplant center
Patel, 2014
California Cancer Registry (1998 to 2008)
All ages, Nt=11,084 White N=7,381, Black N=603, Hispanic N=1936, Pacific-Islander=1164
Blacks vs Whites: 51 (8%) vs 660 (9%)
OR=0.64, (95% CI; 0.46-0.87)
Hispanic vs. White: 235 vs 660
OR=0.74 (95% CI: 0.62-0.89)
Pacific-Islander, 153 (13%) vs 660 (9%)
OR=0.99 (95% CI: 0.81-1.22)
Adjusted for age, cytogenetic profiles, gender, comorbidities, year of diagnosis
Mock, 2021
Virginia Cancer Registry and CIBMTR data (2013 to 2017)
Age Group: 18-74 years old, Ntotal=818, HCT(N)=168
White N=132 African-American N=21 Other N=15
Region with a greater than 25% African-American population were 42% less likely to undergo HCTOR=0.58 (95% CI: 0.38 to 0.89)
Adjusted for age, sex, marital status, insurance, geographic location
CIBMTR=Center for International Blood and Marrow Transplant Research NH=non-Hispanic CI=Confidence Interval OR=Odds Ratio RR=Relative Risk.
# 97
Surveillance of Healthcare Equality and Implicit Bias through Incident Reports
Le FT1, 2, Greene N1, Langston S1, Payton K1, Nguyen J1. 1Cedars- Sinai Medical Center, Los Angeles, CA and 2Harbor- UCLA Medical Center, Torrance, CA
Purpose of Study: Implicit bias is a prominent factor contributing to healthcare disparities and substandard quality of care. However, the extent of racial and ethnic disparities within healthcare systems remains inadequately characterized. Hospitals frequently employ voluntary incident reporting systems to monitor adverse events, which, while valuable, are susceptible to biases. This study investigates a voluntary incident reporting database to evaluate healthcare disparities within a Level IV Neonatal Intensive Care Unit (NICU).
Methods Used: We conducted a retrospective review at a single site, examining all NICU incident reports submitted to the Cedars-Sinai Safety Event Reporting System (CS-SAFE) between January 2020 and June 2023. The study included infants with comprehensive data on mother-baby dyads who were admitted to the NICU. We compared the characteristics of infants with reported adverse events to those without. We collected demographic variables, including maternal age, gestational age (GA), birth weight (BW), and maternal body mass index (BMI) at delivery. Additionally, we recorded the infant’s race/ethnicity, length of newborn stay, and insurance status (public vs. private). To account for confounding factors, we conducted multivariable logistic regression analysis.
Summary of Results: Our analysis encompassed 3,340 infants, including 173 with adverse events and 2,867 without. Black, Asian, and Hispanic infants were overrepresented in the group with adverse events compared to White infants (p=0.03). However, this difference was mitigated and no longer statistically significant (p = 0.78) in the multivariable logistic regression model, which accounted for gestational age at birth. No significant differences were observed between the two groups concerning maternal age, BMI, and insurance status.
Conclusions: Our examination of the voluntary incident reporting database did not uncover statistically significant differences in the incidence of adverse events in our NICU during the reviewed timeframe. Gestational age at birth emerged as the sole independent predictor of adverse events. NICUs routinely collect incident reports, presenting an accessible tool for evaluating and enhancing care equity. Subsequent studies should explore whether voluntary reporting aligns with its intended purpose of accurately assessing equitable incident occurrence and reporting.
Healthcare Delivery Research II
Concurrent Session
3:15 PM
Thursday, January 18, 2024
# 98
PROTECTING CHILDREN FROM FIREARM VIOLENCE- ONE GUN LOCK AT A TIME
Agrawal A, Sun J. University of Nevada, Las Vegas, Las Vegas, NV
Purpose of Study: Firearm violence is the leading cause of death for all children under 18 years old, and Nevada has the 10th highest rate of gun violence in the US. The UNLV Health Pediatric Clinic located in downtown Las Vegas, NV serves an extremely diverse and underserved patient group; 70% of our patients are covered by Medicaid and the minority populations of the city include 11.5% Black or African American, 34.1% Hispanic or Latino, 11.1% 2 or more races, and 6.8% Asian. CDC data of firearm-related deaths between 1990-2017 found that the race/ethnicities most affected by gun violence were Blacks at 65% followed by Hispanics at 37% - the 2 largest minority populations in Las Vegas. With my roles as a pediatrician and as the Gun Violence Prevention Advocate for the Nevada Chapter of the American Academy of Pediatrics (AAP), I conducted a Quality Improvement project with the purpose of improving both knowledge of firearm safety and access to safe firearm storage.
Methods Used: Surveys were conducted by pediatric residents at the UNLV Health Pediatric Clinic to assess patient families’ baseline knowledge on AAP firearm safety recommendations. For perceived confidence, participants rated their knowledge level on a scale 1-5. For objective knowledge, participants answered questions on gun storage, ammunition, and overall safety of having a gun in the home. After the survey was completed, they were given a free cable-style gun lock with educational handouts, then re-assessed for any improvements in answers. My aim for this intervention was to increase both perceived confidence and objective knowledge on firearm safety by 25%.
Summary of Results: Data was collected from a total of 25 participants. Results were analyzed in two categories: perceived confidence and objective knowledge. Value was assigned to questions such that a higher number indicated either increased confidence or increased knowledge. The average pretest response for perceived confidence was 3.04 and posttest was 4.04, showing a 24.7% increase and statistically significant with a p-value of 0.001. The average pretest response for objective knowledge was 5.04 and posttest was 5.64, showing a 22% increase and statistically significant with a p-value of 0.000.
Conclusions: Overall, my findings showed statistical significance in increasing patient families’ perceived confidence and objective knowledge of firearm safety, even though increasing them by 25% was not achieved. Feedback from parents was positive regarding the free gun lock and many were eager to share this resource with gun-owning family members. Meaningful conversations were held and strong connections were formed, uniting on our common goal of safety for all children. One challenge with the project was sustainability with access to gun locks as the limiting factor. The Nevada Office of Suicide Prevention graciously donated a small amount of gun locks and provided educational materials. However, without a continual supply of locks, this intervention would be difficult to replicate.
# 99
ASSOCIATIONS BETWEEN ELEVATED BLOOD LEAD LEVELS AND CHILD OPPORTUNITY INDEX SCORES REVEAL DISPARITIES IN NEIGHBORHOODS
Kim C, Wilson L, Lee V. Loma Linda University School of Medicine, Loma Linda, CA
Purpose of Study: Lead poisoning damages the nervous system, leading to developmental delays, cognitive impairments, adverse educational outcomes, and other devastating health complications. There is no safe level of lead exposure. Although the Flint water crisis called attention to the ways in which lead exposure disproportionately affects children from low-income neighborhoods, exposures more devastating beyond Flint have been brought to the public eye. The Child Opportunity Index (COI) is a unified measure of social determinants of health (SDOH) that integrates 29 indicators of neighborhood opportunity that are relevant to a child’s health and development with specificity at the census tract level. We hypothesized that disparities in elevated blood lead level (EBLL) among pediatric populations in Michigan would be reflected by the COI.
Methods Used: We examined data for blood lead levels in 2017 among patients under 18 years of age in Michigan, exploring associations with SDOH as determined by the COI for each census tract. An EBLL was defined by blood lead levels above 4.5 micrograms of lead per deciliter of blood (μg/dL), following the CDC reference level at that time. After excluding 74 census tracts that are either water-only or special land-use areas with little or no residential population, there remained 2,739 tracts in the state of Michigan. EBLL data was available for 2,696 tracts (98%; data for another 29 tracts had been suppressed due to having 5 or fewer tests), encompassing 158,510 tests of blood lead level.
Summary of Results: Of the 158,510 tests in pediatric patients, 8,878 tests (5.6%) demonstrated elevated lead levels. EBLL results were unequally distributed among neighborhoods, even after adjusting for the size of pediatric populations within each census tract, showing a significant inverse correlation with opportunity levels. This disparity was best fitted by a power model, y = 25.7 × x(-0.54). On the low end of the opportunity axis, a 1-point improvement in COI score was associated with a decrease of 8 EBLL results per 1,000 children, whereas in the middle of the axis, a 10-point increase in COI score only decreases the risk of EBLL by 0.3 per 1,000 children.
Conclusions: These data show that EBLL in pediatric populations varies by SDOH on a local level, with lower-opportunity neighborhoods being significantly more vulnerable to lead poisoning and its irreversible, chronic complications. It is vital to address sources such as lead-based paints, industrial processes, and contaminated soil and water. The COI offers a comprehensive tool to examine SDOH, with validity in content, predictive value, and measure of equity. Given the serious harm that lead exposure has on the health, development, and future success of children in high-risk, low-opportunity neighborhoods, such sociological methods can offer valuable insight to both physicians and policymakers to combat lead exposure.
# 100
Hepatitis C Care Delivery Practices Among Primary Care Providers Who Do and Do Not Prescribe Buprenorphine
Mohabir AM2, James JR1, Simon CB3, Cole AM3, Tsui JI1. 1University of Washington, Seattle, WA; 2University of Washington, Seattle, WA and 3University of Washington, Seattle, WA
Purpose of Study: Elimination of Hepatitis C Virus (HCV) by 2030 is a global, national, and state goal. Primary care providers (PCPs)–particularly those who care for people who inject drugs–play a key role in HCV elimination. Yet, little is known on the PCPs’ perspectives on and practices for providing HCV treatment. We compared HCV screening and treatment among PCPs who do and do not prescribe buprenorphine in Washington (WA) State.
Methods Used: We conducted a cross-sectional survey of PCPs in WA State identified through professional societies and networks to assess provider characteristics and HCV care delivery practices. The independent variable was self-report of prescribing buprenorphine, and the dependent/outcome variables were: (1) guideline-concordant HCV screening and (2) directly providing treatment for HCV. Descriptive statistics were used for the descriptive variable distributions. Chi square tests were used to compare outcomes amongst independent variable groups. Multivariable logistic regression was used to predict guideline- concordant HCV screening and directly treating HCV. Analyses were conducted with Stata. A threshold of p <0.05 was used for hypothesis testing.
Summary of Results: Our sample included 79 PCPs from 15 counties in Washington State and was mainly female (63%), white (72%), non-Hispanic/Latino (84%), physicians (72%), and practicing in an urban area (66%). Most participants (71%) estimated that 25% or less of their patients inject drugs. In total, 76% of participants screen for HCV in all adults and only 18% directly provide HCV treatment. We found a nearly 4x greater relative odds that buprenorphine prescribers compared to non-prescribers correctly screen for HCV in all adults (OR=3.92; 95% CI: 1.24-12.38, p=0.020) and a nearly 3x greater relative odds that buprenorphine prescribers compared to non-prescribers directly treat HCV (2.92; 0.82-10.34; p=0.097), although the latter finding did not reach statistical significance.
Conclusions: Among PCPs in WA state, buprenorphine prescribers appear to be more likely to screen for and treat HCV compared to buprenorphine non-prescribers. Still, less than a fifth of all PCPs reported treating HCV. Interventions are needed to increase the number of PCPs who practice HCV guideline-concordant screening and treatment, including for people who use drugs.
Research reported was supported by the National Institute on Drug Abuse of the National Institutes of Health Award Number R25DA050985. The content is the responsibility of the authors and does not represent the official views of the National Institutes of Health.
# 101
Prevalence of common outcomes from randomized controlled trials in systematic reviews as a measure of publication bias: A meta-regression
Le P1, Qi S1, Luong P2, Caplan L1. 1University of Colorado School of Medicine, Aurora, CO and 2Ross University School of Medicine, St. Michael, Barbados
Purpose of Study: Treatment guidelines depend on the conclusions drawn from systematic reviews (SRs) and meta-analyses, which, in turn, typically depend on randomized controlled trial (RCT) data. However, the degree to which RCTs employ consistent outcomes and report the results sufficiently to allow for aggregation remains unknown. We assessed the completeness of common intervention outcomes across medical disciplines as a measure of publication bias.
Methods Used: To ensure all specialties were represented, a convenience sample of SRs from the Cochrane Database of Systematic Reviews were drawn from 21 medical specialties. Data were pooled using a random-effects model. SRs unable to perform meta-analyses due to heterogeneity, SRs evaluating the performance of diagnostic approaches, and SRs within Cochrane topics that did not pertain to a specific medical specialty were excluded.The primary outcome was the proportion of SRs comprised of RCTs with a common outcome. We evaluated SR characteristics associated with this proportion, including the number of included RCTs, the total number of study subjects, the duration of the SR period, and the number of outcomes in each SR.
Summary of Results: Only 14.3% of 105 SRs (encompassing 2308 RCTs) included an outcome common to all included studies. The likelihood of reporting a common outcome varied according to the number of included RCTs within SRs (61% [C.I. 52-70%] for reviews with less than 15 trials and 14% [5-27%] for reviews with >50 trials, p<0.001) and according to the time interval covered by a SR (p=0.01).
Conclusions: The prevalence of SRs reporting uniform outcomes across RCTs is small. Our findings likely overstate the occurrence of common outcomes, as data that could not be aggregated were excluded. Efforts to allow comparisons of studies and aggregation of results from trials must be improved.Without sufficient reporting of uniform outcomes, the precision for effect sizes may be severely compromised, identification of outlying results becomes difficult, and individual studies remain difficult to interpret.
List of included Cochrane topics, corresponding medical specialties, and the mean proportion of reported common outcomes (PORCO).*
Cochrane Topic
Medical Specialties
Mean PORCO
Specialty Category
Allergy & intolerance
Allergy
0.217
Internal Medicine
Blood disorders
Hematology
0.433
Internal Medicine
Cancer
Oncology
0.440
Internal Medicine
Child health
Pediatrics
0.312
Other
Ear, nose, & throat
Otorhinolaryngology
0.289
Surgical
Endocrine & metabolic
Endocrinology
0.202
Internal Medicine
Eyes & vision
Ophthalmology
0.517
Surgical
Gastroenterology & hepatology
Gastroenterology & hepatology
0.579
Internal Medicine
Genetic disorders
Medical Genetics
0.393
Internal Medicine
Gynecology
Gynecology
0.136
Other
Heart & circulation
Cardiology
0.423
Internal Medicine
Infectious disease
Infectious Disease
0.453
Internal Medicine
Kidney disease
Nephrology
0.307
Internal Medicine
Lungs & airways
Pulmonology
0.323
Internal Medicine
Neurology
Neurology
0.411
Other
Orthopedics & trauma
Orthopedics & trauma
0.438
Surgical
Pain & anesthesia
Anesthesiology
0.410
Other
Pregnancy & childbirth
Obstetrics
0.675
Surgical
Rheumatology
Rheumatology
0.387
Internal Medicine
Skin Disorders
Dermatology
0.082
Surgical
Urology
Urology
0.655
Surgical
List of excluded topics: complementary and alternative medicine; consumer and communication strategies; dentistry and oral health; developmental, psychosocial and learning problems; diagnostics; effective practice and health systems; health and safety at work; health professional education; methodology; public health; tobacco, drugs, & alcohol; wounds.
Forest Plot Showing Proportion of Reported Common Outcomes Stratified by Number of Included RCTs.
*Error bars represent 95% confidence intervals
# 102
Eliminating Barriers to Contraception Through Continuing Education and Implementation of Subcutaneous DMPA for At-Home Use
Rangel P, Clark C, Karlin J. UC Davis School of Medicine, Sacramento, CA
Purpose of Study: This project explores factors that affected clinics expanding user directed DMPA-SC with the goal of understanding how to increase awareness, education and access to DMPA-SC.
Methods Used: This mixed-method approach employed a large quantitative survey and qualitative in-depth interviews with providers across the country about their use of DMPA and their perceptions of interest and demand of DMPA. The survey questions were sent out via a Qualtrics survey, using convenience sampling from organizations that target providers of sexual and reproductive health. We obtained a sample size of 422, including MDs, PharmDs, and nurses who work in sexual and reproductive health. The survey contained a consent script to explain the purpose of the study and ensure anonymity. This survey included questions regarding barriers amd accelerators to prescribing DMPA-SC for user-administration. From this survey, people opted into a 1 hour interview to discuss these topics further and assess attitudes about DMPA-SC.
Summary of Results: There are challenges on patient, provider, and institutional levels that prevent the widespread rollout of DMPA for home-administration. On the patient level, there are logistical challenges, such as transportation barriers, fear of needles, and lack of awareness that prevent patients from seeking out DMPA. On a provider level, there is a lack of awareness that DMPA can be prescribed for at home use. Those that are aware appear to be biased against DMPA or do not have an established workflow to provide DMPA for home administration. On an institutional level, there are legal barriers, bereaucratic challenges, and problems with pharmacy supply.
We found, however, that those who do provide DMPA for self-administration elucidated solutions that facilitate the expansion of DMPA for self-administration that mirror the tiered challenges. On a patient level, DMPA for self-administration decreases logistical barriers. Folks can receive a year’s supply of DMPA from the pharmacy and give themselves their shots every 3 months rather than traveling to and from the clinic. On the provider level, increased advertising and provider education made the option available to patients. Having an established protocol for DMPA-SC, such as designating an MA or nurse to teach the injection, also facilitated DMPA for self-administration expansion. Institutional solutions included increased pharmacy supply and expanded insurance coverage.
Conclusions: Barriers and facilitators to SI of DMPA-SC traverse patient, provider, and institutional domains; each impact each other. DMPA-SC has a similar safety and efficacy profile as DMPA-IM and would allow more patient flexibility and autonomy by eliminating office visits, unnecessary transportation challenges, and granting patients more control over their reproductive decisions.
# 103
INCREASING EMERGENCY CONTRACEPTION COUNSELING AND PROVISION THROUGH RESIDENT EDUCATION AND ELECTRONIC HEALTH RECORD SUPPORT
Lutz J2, Chambers-Kersh L1, 3. 1Kettering Health, Beavercreek, OH; 2Loma Linda University, Loma Linda, CA and 3Loma Linda University, Loma Linda, CA
Purpose of Study: Emergency contraception (EC) remains underutilized in the United States for a variety of reasons, including inadequate training in counseling and prescribing. Education in emergency contraception should be routine in family medicine residency, however our initial data search done in July 2022 showed that, in the preceding year, no EC pills were prescribed, and no IUDs were placed as EC by Soin Family Medicine residents. The aim of this study was to evaluate whether a multi-faceted intervention to increase resident education and electronic heath record resources about emergency contraception improved the quantity and outcomes of EC counseling sessions.
Methods Used: This was a single-center retrospective cohort study of annual wellness visits (AWV) of reproductive age (18-45) patients between May 2022 and July 2023. Implementation of the intervention began July 2022 and included didactics reviewing emergency contraception, the provision of relevant templates and dotphrases to include in visit notes and patient handouts, and the creation of a same-day IUD insertion workflow. We reviewed 634 charts May 2022 through July 2023, evaluating how often resident physicians included EC counseling in their AWV’s, inserted EC dotphrases in the visit note, and gave EC information in the after-visit summary (AVS). We also tracked emergency contraception prescriptions throughout the period of implementation.
Summary of Results: The combined male and female percentage of AWV’s with EC counseling sessions was initially 0% and rose to 40% by the final month of the study. After updating male AWV templates to include EC, male counseling sessions jumped to 33% in February 2023 and continued to rise until its peak of 56% July 2023. Female counseling sessions also began to rise after updating female AWV templates in October 2022, with a peak of 33% July 2023. After the introduction of dotphrases in December 2022, utilization rose from 0% December 2022 to 7% July 2023. Provision of EC information in the AVS remained inconsistent with none in the first or final month of the study and a peak of 4% March 2023. Finally, throughout the period of implementation, six Ella and one Plan B prescriptions were written, but there were no IUDs as EC placed.
Conclusions: Implementation of the multi-faceted intervention was associated with an increase in EC counseling sessions during AWV’s. This increase was most significant after AWV templates were updated to include emergency contraception, with a greater effect size seen with male patients than female patients. There was an increase in EC pills prescribed compared to pre-implementation, but overall prescriptions remained low during implementation. Further studies are needed to see if the upward trajectory of EC counseling will continue months after this intervention as well as to explore persistent barriers that cause low rates of EC prescriptions after counseling sessions, particularly regarding IUD’s.
# 104
DECREASED NEED FOR SURGICAL INTERVENTION AMONG CHILDREN FROM AREAS OF HIGHER NEIGHBORHOOD DISADVANTAGE FOLLOWING TRAUMATIC INJURY
Orehova JE, Myers E, Eyal K, Pickett-Nairne K, Malham M, Hill L, Adelgais K, Acker SN. Aurora, CO
Purpose of Study: Area deprivation index (ADI) is a validated composite measure of neighborhood level disadvantage. We previously examined the relationship between ADI and pediatric trauma mechanism, severity, and outcomes and found higher injury severity among patients from neighborhoods of greater deprivation. Despite lower injury severity, the frequency of surgical intervention was higher for children from neighborhoods with lower socioeconomic disadvantage. We hypothesized that there would be differences in both the frequency and type of operative procedures among ADI quintiles related to underlying factors of injury mechanism and injury severity.
Methods Used: A cross-sectional analysis of pediatric trauma patients aged 0-18 years presenting to our Level I Pediatric Trauma Center between January 1, 2016 and December 31, 2021 was performed. Clinical data were obtained from the Children’s Hospital Colorado (CHCO) Trauma Registry and abstraction of the electronic health record (EHR). Patients were excluded if their home address was missing or incomplete. Patients were grouped into quintile using the 2020 version of ADI. Higher ADI quintile corresponded to greater neighborhood disadvantage. Operations were categorized into neurosurgical, orthopedic, general surgery, and other operations. Relationship between ADI quintile and volume and type of operative intervention, body region, and injury severity were evaluated. Descriptive statistics were summarized for continuous variables with medians and interquartile ranges, and for categorical variables with frequencies and proportions. Group differences are tested via t-test or Kruskal-Wallis test for continuous variables and Chi Squared test or Fisher’s Exact tests for categorical variables.
Summary of Results: A total of 5,655 pediatric patients suffered traumatic injuries, 3378 (59.7%) of whom underwent an operation including 48 neurosurgery (1.4%), 2253 orthopedic (66.7%), 88 general surgery (2.6%), and 989 other operations (29.3%). The percentage of operations varied by ADI quintile (p<0.001). Orthopedic procedures made up 70.2% of operations in the 1st quintile and 63.1% of operations in the 5th quintile, corralating with a higher rate of extremity injury in children from areas of lower deprivation (56.2% of 1st quintile vs 44.1% of 5th quintile, p<0.001). Patients who underwent orthopedic operations had a significantly lower mean Injury Severity Score (mean = 6.2, SD= 4.7, p<0.001) compared to neurosurgical operations (mean = 21.7, SD = 9.8, p<0.001) and general surgery operations (mean = 16.0, SD = 15.0, p<0.001).
Conclusions: Among children who suffered traumatic injury and required an operation, rate of operative intervention was higher among children with lower neighborhood level deprivation. Orthopedic procedures made up the majority of operations for all quintiles, with rate of orthopedic procedures decreasing with increasing deprivation, similar to the variation in rate of extremity injury by ADI quintile.
Percentage of operations performed by ADI quintile for children suffering traumatic injury.
Total Patients (N=5655)
Total operations (N=3378)
Neurosurgery (N=48)
Orthopedic (N=2253)
General Surgery (N=88)
Other Surgery (N=989)
p value
ADI quintile
< 0.001
1st
1222 (21.6%)
779 (63.7%)
9 (1.2%)
547 (70.2%)
22 (2.8%)
201 (25.8%)
2nd
1067 (18.9%)
675 (63.2%)
11 (3.3%)
480 (71.1%)
16 (2.4%)
168 (24.9%)
3rd
1162 (20.5%)
690 (59.4%)
12 (1.7%)
448 (64.9%)
13 (1.9%)
217 (31.4%)
4th
1072 (19.0%)
594 (55.4%)
6 (1.0%)
374 (63.0%)
19 (3.2%)
195 (32.8%)
5th
1132 (20.0%)
640 (56.5%)
10 (1.6%)
404 (63.1%)
18 (2.8%)
208 (32.5%)
ADI - area deprivation index.
# 105
EFFECT OF HIGH HEAT RUNNING ENVIRONMENT ON ACHILLES TENDON MORPHOLOGY IN RUNNERS
Jones E1, Lewis M1, 2, Crissey J2, Garbuz C2, Zhang-Lea J2. 1University of Washington School of Medicine, Spokane, WA and 2Gonzaga University, Spokane, WA
Purpose of Study: Global warming has posed an increasing challenge on human health. Increased heat has been shown to alter tendon structure by disrupting cell metabolism of extracellular matrix components, which could lead to development of musculoskeletal injuries in endurance runners. Tendon hyperthermia has been proposed to degenerate the tendon’s central core and precede tendon rupture, but the effect of heat on human Achilles tendon (AT) morphology and mechanical properties are not yet fully understood. This study investigated how high heat affects AT morphology in distance runners.
Methods Used: Six active distance runners performed two 30-minute running sessions, distributed with at least a one-week washout period, in heat (30°C) or temperate (20°C) conditions. We collected ultrasound images (Logiq e, GE, Boston, MA), before and after each run, as well as during a 24–72-hour follow-up period. We first labeled 2cm and 5cm location of the AT length measured from the tendon-calcaneus interface, and measured AT thickness and cross-sectional area (CSA) from ultrasound images scanned at both locations. Additionally, we obtained tendon stiffness using a myotonometry device (Myoton, Tallinn, Estonia). Linear mixed models were constructed to assess the effect of heat on AT geometry and stiffness, with a level of significance set at 0.05.
Summary of Results: Although the effect of heat did not reach significance for AT thickness (F=1.78, p=0.20) and CSA (F=3.51, p=0.08) at 2 cm location, heat showed medium effect size on these two variables (Cohen’s f = 0.277 and 0.373, respectively). After running in the heat condition, AT thickness was reduced by 3.88% and CSA was increased by 1.38% compared to pre-running. After running in the temperate condition, AT thickness was reduced by 1.63% and CSA was increased by 5.91% compared to pre-running. Heat did not show significant effect on AT thickness (F=0.06, p=0.81) and CSA (F=0.08, p=0.78) at 5cm position, with trivial effect size (Cohen’s f < 0.1). Heat had significant main effect on AT stiffness (F = 6.657, p = 0.019), with a medium effect size (Cohen’s f = 0.392). Specifically, compared to pre-running measurement, participants reduced AT stiffness by 3.4% after 30-minute running in the 30°C condition, and increased AT stiffness by 3.99% after 30-minute running in the 20°C condition.
Conclusions: Hot ambient running temperature decreased AT stiffness, which could be explained by the decreased AT thickness and CSA at 2cm location observed in this study. Although the difference in AT thickness and CSA at 2cm location did not reach significance, our post-hoc sample size estimation suggests that our current study with 6 participants is under-powered (Power=0.22), and a sample size of 34 participants will reach Power >0.8. The tendon geometry changes we noticed in this pilot study may contribute to the formation of degenerative lesions in the AT over time in distance runners.
# 106
MENTAL HEALTHCARE PROVIDER WORK ORIENTATIONS AND MENTAL HEALTH OUTCOMES
Zielinski OC1, Kennedy S2. 1University of Colorado School of Medicine, Aurora, CO and 2University of Colorado School of Medicine, Aurora, CO
Purpose of Study: Burnout and stress are common among mental healthcare professionals (O’Conner et al. 2018) and are associated with lower quality of life (Tawfik et al. 2019). Work orientations, how individuals conceptualize their relationship with work, have not been studied in relation to the mental health field (Wrzesniewski 2003; Wrzesniewski et al. 1997). This research aims to characterize work orientation in mental healthcare professionals and investigate its relationship to mental health outcomes and attitudes toward evidence-based practices.
Methods Used: Data were collected from 75 mental healthcare workers from a children’s hospital in the Mountain West who provide youth psychiatric inpatient or partial hospitalization services. Participants were 88% female (n = 66), 91% white (n = 68), and 83% not Hispanic/Latinx (n = 62). They completed survey measures of work orientation (University of Pennsylvania Work-Life Questionnaire; Wrzesniewski et al. 1997), openness to evidence-based practices (Evidence-Based Practice Attitudes Scale-15; Aarons 2004), emotional exhaustion (Maslach Burnout Inventory Emotional Exhaustion Subscale; Maslach et al. 1997), burnout (Professional Quality of Life Burnout Subscale; Stamm 2010), and stress (Perceived Stress Scale; Lee 2012). Participants strongly identifying with each work orientation were selected via purposive sampling for a qualitative interview. Descriptive statistics identified proportions of the sample identifying most strongly with each work orientation. Pearson bivariate correlations and one-way ANOVAS were used to examine relationships between work orientation and other variables, and linear regression determined whether certain orientations were associated with professional quality of life over and above the impact of burnout and stress.
Summary of Results: Overall, 30.7% of this sample endorsed a calling orientation; 45.3% a career orientation; and 5.3% a job orientation, in contrast with work in other populations showing equal endorsement of all three orientations (Wrzesniewski 2003; Wrzesniewski et al. 1997). A calling orientation was significantly and positively correlated with professional quality of life (r = .561, p<.001) and openness to evidence-based practices (r = .320, p = .006), and significantly and negatively correlated with emotional exhaustion (r = -.575, p<.001). This pattern was consistent with ANOVA results evaluating whether levels of these constructs differed by individuals’ predominant work orientations. Controlling for perceived stress, regressions indicated that stronger agreement with calling orientation remained significantly associated with professional quality of life (B = 5.5, p<.001) and with emotional exhaustion (B = -3.0, p<.001).
Conclusions: Findings reveal a significant relationship between calling work orientation, lower levels of negative mental-health outcomes, and higher openness to evidence-based practice. Qualitative analysis of interviews will also be presented to explore possible mechanisms.
# 107
LOWER CHILD OPPORTUNITY IS ASSOCIATED WITH MORE ASTHMA EMERGENCY DEPARTMENT VISITS ON A NEIGHBORHOOD LEVEL
Wilson L, Kim C, Lee V. Loma Linda University School of Medicine, Loma Linda, CA
Purpose of Study: Social determinants of health (SDOH) have a significant influence on health outcomes, even greater than the impact of clinical care. Despite the immense potential for early intervention in the prevention of chronic disease, fewer studies have assessed SDOH associations among pediatric populations. The Child Opportunity Index (COI) is a composite measure of SDOH, combining neighborhood resources and conditions that are relevant to children’s health and development into a single metric. The COI allows comparison of SDOH across communities and can be used to explore inequities in health outcomes. We hypothesized that differences in pediatric asthma emergency department (ED) visits would be associated with disparities in local opportunity levels. In addition, we speculated that greater warehousing in lower-opportunity neighborhoods may mediate an increase in pediatric ED visits.
Methods Used: We examined data from the California Health and Human Services (CalHHS) Open Data Portal for ED visits in 2019 among patients 0-17 years of age in California, exploring relationships with SDOH as determined by the COI for each zip code. Nationally-normed COI ratings as of 2015 were available for 2,420 zip codes in California. ED visit data was available for 882 zip codes (data for areas with 5 or fewer visits were suppressed), encompassing 55,581 pediatric visits. We further used data from Radical Research LLC detailing warehouse count and facility square footage by zip code to explore potential relationships of warehouses with asthma ED visits and SDOH.
Summary of Results: Of the 55,581 asthma ED visits by pediatric patients in California for which COI data was available, there was a significant inverse correlation with neighborhood opportunity. On average, a 10-point increase in COI score, indicating better childhood opportunity, was associated with a decrease of 0.9 visits per 1,000 children (95% confidence interval -0.8 to -1.0; R2 = 0.39). Additionally, there was an inverse correlation found between warehouse square footage and neighborhood opportunity by zip code.
Conclusions: These data support the idea that there is a greater frequency of asthma ED visits in areas with lower child opportunity, possibly due to disparities in accessing preventative care. Interventions to improve respiratory health may yield greater impact if directed at these higher-risk communities. There is also a significantly larger footprint occupied by warehouses in lower-opportunity neighborhoods. The consequences that such industrialization will have on residents’ health have yet to be fully examined. In light of the adverse health effects that these warehouse hubs may have on pediatric populations, further research is needed to protect these vulnerable communities.
Hematology and Oncology I
Concurrent Session
3:15 PM
Thursday, January 18, 2024
# 108
The mucosal melanoma tumor microbiome is distinct from cutaneous with unfavorable proportions of immune-associated species
Parmar P, MacBeth M, Witty P, Robinson W, Lozupone C, Couts K. University of Colorado, Aurora, CO
Purpose of Study: Immune checkpoint blockade (ICB) is effective in cutaneous melanoma (CM), but mucosal melanoma (MM) has poor ICB response and anti-tumor immunity. We discovered the microbial composition of MM tumors is unique, with a higher proportion of Gram-positive bacteria Firmicutes compared to CM. Firmicutes does not contain lipopolysaccharides (LPS) which are predominantly found within Gram-negative cell walls and trigger type I interferon (T1IFN) and inflammatory pathways via Toll-like receptor 4 (TLR4) signaling in immune and melanoma cells. In addition to lacking LPS, Firmicutes produces the immunosuppressive metabolite butyrate, which inhibits LPS and TLR4 signaling. Based on these data, we hypothesize the Firmicutes rich MM tumor microbiome contributes to immune evasion and ICB resistance by suppressing LPS-TLR4 mediated T1IFN signaling and inflammation (figure 1).
Methods Used: We performed 16S rRNA sequencing to analyze bacterial compositions in 75 tumors and 72 stool samples from CM or MM patients. We then evaluated immune gene expression by qRT-PCR in MM cell lines treated in vitro to analyze the impacts of LPS, CD14-independent TLR4 agonist CRX-527, TLR4 inhibitor CLI-095, and butyrate.
Summary of Results: 16S rRNA analyses on tumors showed that the ratio of Proteobacteria to Firmicutes (P:F), a metric commonly used to compare tissue types, was low in MM tumors (0.03) and stool (0.07) compared to CM (1.1). Overall, Firmicutes was found in greater proportions in MM than CM. In vitro studies with MM cell lines showed increased expression of T1IFN response genes (IFIH1, OAS1, IFI44) following treatment with LPS or CRX-527, and decreased expression with CLI-095. Inflammatory cytokines (IL-1β, IL-8) also significantly increased with CRX-527 treatment, with variable response to direct LPS agonist
Conclusions: Overall, the tumor microbiomes of CM and MM are significantly different and may be a critical factor underlying the “cold” tumor microenvironment and poor ICB response of MM. Furthermore, these effects may be partly mediated through interactions of LPS with the TLR4 signaling cascade directly on tumor cells. Unlike LPS, CRX-527 is a synthetic lipid A mimetic that does not require the cofactor CD14 to activate TLR4 signaling, likely explaining its ability to better activate T1IFN and inflammatory signaling than standard LPS. CRX-527, used clinically as a vaccine adjuvant, may be an effective treatment modality in combination with ICB to improve anti-tumor immune responses in MM.
# 109
IDENTIFYING MALIGNANT SMALL RENAL MASSES WITH RE-VASC, A NOVEL RETROPERITONEAL NEOVASCULARITY SCORING SYSTEM
Fateri C1, Roth B1, Rao S1, Ho E1, Peta A1, Limfueco L1, Bui T2, Kar N1, Glavis-Bloom J1, Landman J1, Houshyar R1. 1UC Irvine, Irvine, CA and 2University of Washington, Seattle, WA
Purpose of Study: Identifying small (T1a, < 4 cm) renal masses as either benign or malignant is critical for patient care and appropriate treatment. Renal biopsy is a sensitive and specific procedure that can accurately differentiate small renal masses as malignant or benign. However, it is an invasive procedure with a non-negligible complication rate and is not performed routinely at most institutions. The Re-VASC score is a previously established scoring system used to grade renal masses based on the measurement of neovascularity detected on CT imaging. In this study, we sought to apply the Re-VASC scoring system to T1a renal masses and analyzed whether it could differentiate these masses as benign or malignant.
Methods Used: We obtained Institutional Review Board approval to retrospectively examine the records of all patients who presented to our single, urban academic referral center for surgical treatment of renal cell carcinoma (RCC) between January 13, 2014 and February 4, 2020. The inclusion criteria consisted of pathology confirmed T1a RCC masses, history of simple or radical nephrectomy, and pre-operative CT imaging. The T1a benign comparison group consisted of non-malignant renal masses (fat-poor angiomyolipoma or oncocytoma) diagnosed via histopathology. Pre-biopsy or pre-operative CT imaging of all patients was blindly reviewed and assessed for Re-VASC score by a board-certified radiologist.
Summary of Results: This study includes 57 benign and 69 malignant T1a renal tumors. Average size for benign and malignant masses were 2.47 and 2.63 respectively (p=0.267). Analysis demonstrated no significant difference between both groups in terms of sex, laterality, or size. The average Re-VASC score of benign tumors was 0.175 and malignant masses was 0.784 (p<0.001). Comparison of Re-VASC scores of contralateral non-tumor bearing kidneys between RCC and benign group was showed no significant difference (p<0.508) (Table 1). The total range of Re-VASC scores for benign and malignant tumors was 0-2 and 0-4 respectively. Additionally, the Re-VASC score was independently associated with malignancy, with an odds ratio of 2.223 (p=0.0109).
Conclusions: There is a significant difference in Re-VASC score between malignant and benign T1a renal masses. The Re-VASC score may be utilized as an adjunctive tool in characterizing renal masses and improving clinical decision-making. Future efforts to assess the true efficacy of the Re-VASC score as a diagnostic marker will include prospective evaluation of a larger multicenter population.
Patient Demographics and Re-VASC Scoring.
Benign (N=57)
Malignant (N=69)
P-value
Sex (n(%))
0.280
Male
31 (54%)
45 (65%)
Female
26 (46%)
24 (35%)
Laterality
0.724
Right-Sided
28 (49%)
31 (45%)
Left-Sided
29 (51%)
38 (55%)
Tumor Size (cm)
0.267
Mean +/- SD
2.47 +/- 0.858
2.627 +/- 0.706
Re-VASC Tumor Score
<0.001
Mean +/- SD
0.175 +/- 0.428
0.784 +/- 1.296
Re-VASC Benign Score
0.214
Mean +/- SD
0.035 +/- 0.186
0.108 +/- 0.455
# 110
Radiotherapy Dose Maps Improve Radiologists’ Confidence and Accuracy in Interpreting Post-Treatment Thoracic CTs
Ferguson-Steele Z1, Newell K1, Shin D3, Noh M4, Pipavath S4, Tsai J2, Gutschenritter T2, Kang J2. 1University of Washington School of Medicine, Seattle, WA; 2University of Washington Medical Center, Seattle, WA; 3University of Washington, Seattle, WA and 4University of Washington Medical Center, Seattle, WA
Purpose of Study: For diagnostic radiologists, interpretation of surveillance imaging of patients previously treated with radiation therapy can be challenging because the indication for imaging may not adequately describe the radiation fields, and because radiation treatment effect and lesion progression can appear similar. Volumetric visualization of the radiation dose created by radiation oncologists is often inaccessible to radiologists. A semi-automated workflow can create an image series of the dose information overlaid on CT images and then transfer these images to PACS. We aim to clarify the utility of incorporating dose maps into radiologists’ work-flow.
Methods Used: CT imaging of 32 patients who received thoracic irradiation to 1-5 lesion(s) for a primary (24) or metastatic (8) thoracic malignancy were reviewed by a board-certified thoracic radiologist and a diagnostic radiology resident. A brief clinical history was provided for each case. The readers interpreted pre-treatment, treatment planning, and post-treatment images in anonymized sessions first without, and then with access to radiation dose information, with at least one month separating each read. Readers were asked to identify the treated lesion(s), and radiation treatment effect(s), and then complete a survey utilizing both Likert scale and yes/no questions to assess qualitative data points including their confidence in interpretation.
Summary of Results: There were 19 patients with 1 lesion and 13 patients with >1 lesion. Correct identification of all treated lesions significantly increased with the addition of dose maps (61% to 81%; McNemar test, p=0.00079), with the largest increase for cases with >1 lesion (15% to 54%; McNemar test, p=0.0039). This correlates with a decrease in false negatives (unlabeled lesions that had received radiation) from 39% to 19%. False positives, or the labeling of lesions and treatment effects in areas that had not been irradiated, also fell from 11% to 2% and 13% to 0%, respectively. Confidence in correctly identifying treated lesion(s) significantly increased from a rating of 4.1 to 4.8 on a scale of 1-5 (Paired two-tail t test; p=0.000005), while readers’ response to whether they would search the patient’s chart for more radiotherapy plan information decreased from 3.63 to 3.28 (Paired two-tail t test; p=0.0051).
Conclusions: Correct identification of irradiated lesions and treatment effect as well as confidence in identification significantly improved when radiologists had access to radiotherapy dose maps. The improvement in identification accuracy, especially in cases with multiple lesions, reflects a potentially meaningful reduction in misdiagnosed tumor progression or treatment failure. The increase in confidence and decreased need for additional EMR information points towards a benefit to radiologists’ work-flow and efficiency. These results demonstrate that adding radiation dose maps to imaging could improve quality of surveillance care for patients with irradiated thoracic malignancies.
Correct Identification Rate of All Treated Lesions.
All Cases
Simple Cases(1 treated lesion)
Complex Cases
(>1 treated lesion)
No Radiation Dose Overlay
61% (39/64 cases)
92% (35/38 cases)
15% (4/26 cases)
With Radiation Dose Overlay
81% (52/64 cases)
100% (38/38 cases)
54% (14/26 cases)
p-value
(McNemar Test)
p=0.00079*
p=0.083
p=0.0039*
For a complex case, all targets needed to be labeled to count as correct. * denotes statistical significance at significance level α=0.05.
# 111
THE PHYSIOLOGICAL ROLE OF RELT FAMILY MEMBERS IN HUMAN CANCER AND CELLULAR APOPTOSIS
Chou E, Chang E, Yanumula A, Wang W, Zhou J, Cusick G, Shi Y, Mohamed E, Cusick J. California Northstate University, Elk Grove, CA
Purpose of Study: Receptor Expressed in Lymphoid Tissues (RELT) is a Tumor Necrosis Factor Receptor family member implicated in several cancers. RELL1 and RELL2 (RELT-Like 1 and 2) are RELT homologs that bind RELT; they are collectively referred to as RELT family members (RELTfms). All three can be phosphorylated by the OXSR1 kinase. We sought to test whether RELTfm expression causes death and sensitizes breast cancer cells to chemotherapeutic agents and if RELT-induced death is dependent on OXSR1 binding. Furthermore, we assessed if RELT expression is altered in human tumor biopsies.
Methods Used: Empty vector or expression plasmids for RELTfms were transiently transfected into MDA-MB-231 (231) breast cancer cells with Lipofectamine. A Caspase-Glo 3/7 luciferase assay was used to quantify Caspase-3 cleavage in 231s. Flow cytometry (FC) was used to quantify apoptotic markers AnnexinV/PI expression in 231s treated with Doxorubicin or Paclitaxel. An X-Gal morphology assay was used to assess whether mutating the OXSR1 kinase binding site (RARA) inhibited RELT’s ability to induce apoptosis. Immunohistochemistry (IHC) was used to assess RELT expression in human breast and lung cancer biopsies.
Summary of Results: RELTfms overexpression induced apoptosis in 231s based on FC and X-gal assays, yet RELT overexpression did not result in Caspase-3 cleavage in 231 cells. FC showed increased apoptosis and necrosis with chemotherapy treatment in 231s overexpressing RELL2 versus vector. X-Gal staining revealed RELT and RARA had similar apoptosis enhancement versus vector. IHC results showed increased RELT expression in malignant breast cancer biopsies compared to patient-matched benign tissue. Interestingly, RELT was localized in the nucleus of malignant lung cancer cells, versus the cytoplasm of benign cells.
Conclusions: RELT and RELL2 induce apoptosis in breast cancer cells and RELL2 enhances the sensitivity of these cells to doxorubicin. RELT phosphorylation by OXSR1 may not be required to induce death in 231s. Interestingly, RELT expression and cellular localization is altered in lung cancer biopsies compared to benign tissue, indicating a potential role for RELT in cancer that warrants further investigation.
Effect of RELL2 expression on Annexin V/PI Staining in MDA-MB-231 cells treated with Doxorubin or Paclitaxel.
-AV/-PI
+AV/-PI
+AV/+PI
-AV/+PI
RELL2 + Doxorubicin
77.8%
12.5%
7.36%
2.31%
Vector + Doxorubicin
85.5%
5.29%
2.78%
6.40%
RELL2 + Paclitaxel
37.9%
60.5%
1.18%
0.38%
Vector + Paclitaxel
38.5%
59.6%
1.4%
0.48%
RELT IHC of Breast Cancer Biopsies.
# 112
MASTECTOMY RATES IN BREAST CANCER PATIENTS WITH PATHOGENIC VARIANTS IN THE ATAXIA TELANGIECTASIA MUTATED GENE
Kwan M1, Culver J1, Comeaux J1, Ricker C1, Tao M1, Woodworth A1, Okabe A2, Ye J1. 1University of Southern California, Los Angeles, CA and 2California Northstate University, Elk Grove, CA
Purpose of Study: Patients who are heterozygous for germline pathogenic variants (PVs) in ataxia telangiectasia (ATM) gene have a higher risk of developing several cancers, including breast cancer (BC). NCCN Guidelines do not consider heterozygous ATM PVs to be a contraindication for breast conservation or radiation therapy. Uncertainties regarding the risk of a second primary BC in ATM PV carriers might drive more aggressive treatment options, especially for younger patients. The patterns of care for these BC patients, as well as other characteristics of this patient group, are not well-defined.
Methods Used: We identified BC patients who underwent multigene panel testing from 2013 to 2023. We conducted a chart review of patients with ATM PVs and assessed their pathology, demographics, and surgical management.
Summary of Results: Out of the 1461 BC patients, 18 were ATM carriers. The mean age at BC diagnosis was 49 years in patients with an ATM PV. Of these patients, 83% (n=15) had mastectomies, and 17% (n=3) had segmental mastectomies or lumpectomies. In comparison to the general population, the ATM group was younger and had a higher rate of mastectomy. Among 16 of the 18 patients with available data, most (69%, n=11) of the patients had T0-2 N0 disease, and of those 73% (n=8) underwent mastectomies and 27% (n=3) underwent lumpectomies. Some (31%, n=5) had node-positive disease, and all received mastectomies.
Ten of 18 patients received radiation oncology consultations before surgery, including the three patients who underwent breast-conserving surgery.
Among 16 of the 18 patients with available data, 94% (n=15) were ER positive, 68% (n=11) were PR positive, and 36% (n=6) were HER2 positive. Additionally, of the 18 patients, 22% (n=4, mean age 48) had synchronous bilateral BC and 5% (n=1, age 74) had metachronous bilateral BC.
We identified 12 patients for whom genetic testing was a factor in their surgical decision-making, as inferred by provider notes. In 83% (n=10) of these cases, genetic testing was inferred to have played a role in the surgical decision while for 17% (n=2) of patients, genetic testing did not impact the surgical decision.
Two of the more recent genetic counseling notes included risk analysis for remaining lifetime second primary BC risk.
Conclusions: Our study highlights patterns in the surgical management of BC in ATM-positive patients, including a higher rate of mastectomy as the chosen surgical treatment. Given the rarity of patients with ATM pathogenic variants, further research with larger sample sizes is needed to confirm these findings. The influence of remaining lifetime BC risk found in the genetic counseling notes, a relatively new metric, on decision-making remains unclear. Notably, our study revealed discrepancies and missing information in patient documentation, particularly regarding the rationale behind treatment decision-making. This presents an important subject for further exploration.
# 113
A rare case of Intravenous immunoglobulin (IVIG) induced thrombocytopenia in a patient presenting in myasthenia gravis crisis
Ipalawatte H, Ahmed N, Durrani M, Takher J. HCA Los Robles Regional, Thousand Oaks, CA
Background: Intravenous immunoglobulin (IVIG) has known efficacy in the treatment of myasthenia crisis. Study design and methods: We present the clinical course of a patient with known myasthenia gravis, who developed acute thrombocytopenia and leukopenia upon administration of IVIG for acute myasthenic crisis. Patient developed thrombocytopenia and leukopenia on day 3 of IVIG administration. The patient’s platelet count progressed as follows: 136 x 10 3 , 105 x 10 3 , 99 x 10 3 , 84 x 10 3 , 80 x 10 3 /uL. White blood cell count was noted to progress as follows: 8 x 10 3 , 4.6 x 10 3 , 3.2 x 10 3 /uL. After day three of IVIG administration, the decision was made to discontinue treatment, especially as the patient’s myasthenic crisis and clinical symptoms resolved. Outpatient follow up was recommend for continuity of care.
Results: As the patient’s cell count abnormalities presented shortly after the administration of IVIG, thrombocytopenia and leukopenia should be considered a possible adverse effect of this treatment in myasthenia crisis.
Conclusions: This is one of the rare cases of acute thrombocytopenia and leukopenia occurring likely as a result of myasthenic crisis treatment with IVIG.
# 114
CREATION OF NARROW DIAMETER PROTON PENCIL BEAMS USING OCTUPOLE MAGNETS
Kim S1, Park J1, Slater J2, McAuley G2. 1Loma Linda University, Loma Linda, CA and 2Loma Linda University, Loma Linda, CA
Purpose of Study: Scanning pencil beam delivery, a combination of narrow proton beams (ie, pencil beams) magnetically steered to create a dose distribution, is the state-of-the-art technology in most proton treatments. In general, pencil beams of small diameter with sharp boundaries lead to more conformal tumor coverage and sparing of normal tissue. The purpose of this project was to employ computer simulations to investigate the use of octupole magnets to shape pencil beams with small diameters and sharp margins.
Methods Used: Monte Carlo simulations were performed of 127 and 157 MeV pencil beams (Gaussian profiles, 3 mm STD). Protons traveled through two octupole Halbach cylinder magnets to a water tank at isocenter (1 m downstream of the last magnet). The magnets had a 15 mm diameter, 50 mm length, a magnetic field gradient of 233 T/m, and were rotated 45° with respect to each other. Beam diameter and margins were quantified by the full-width-at-half-maxima (FWHM) and the 80/20 penumbra of the dose distribution measured in the water tank. FWHM and penumbra were compared with those of otherwise identical but unshaped pencil beams. Additional properties of the beams were determined by plots of particle angular direction vs. position (ie, phase space plots).
Summary of Results: For both energies, magnetically shaped pencil beams showed ~2 mm smaller FWHMs and ~0.5 mm smaller penumbras at isocenter compared to the unshaped beams. The 127 MeV (157 MeV) magnetically shaped beam had a 16% (15%) smaller FWHM and 9% (11%) smaller penumbra than the unshaped beam at isocenter (Table 1 and Figure 1A & B). The phase space plots illustrated the expected mechanism of beam diameter reduction (the bending of the tails of the beam towards the beam center) (Figure 1C & D).
- A) Dose distribution and contour lines of shaped (top) and unshaped (bottom) beam at isocenter. B) Dose contours (outter to inner) of 20%, 50%, and 80% of maximum dose for shaped (pink) and unshaped (cyan), C) Phase space taken downstream of first octupole magnet of unshaped, and D) shaped beams.
Conclusions: These results suggest the use of octupole magnets could potentially be useful in clinical pencil scanning beam nozzles, as well as in a technology under development called minibeam proton therapy, where smaller FWHM and penumbras are even more essential.
Transverse dose properties at isocenter.
Energy (MeV)
uFWHM (mm)
sFWHM (mm)
FWHM difference (%)
uPenumbra (mm)
sPenumbra (mm)
Penumbra difference (%)
127
11.6
9.7
16
5.7
5.2
9
157
11.3
9.6
15
5.7
5.1
11
uFWHM – full width at half maxima of the unshaped beam sFWHM – full width at half maxima of the magnetically shaped beam uPenumbra – 80/20 transverse penumbra of the unshaped beam sPenumbra – 80/20 transverse penumbra of the magnetically shaped beam.
# 115
IDENTIFYING PATIENTS WITH LUNG CANCER FROM ELECTRONIC HEALTH RECORDS: A SYSTEMATIC EVIDENCE REVIEW TO BRIDGE THE GAP BETWEEN RESEARCH AND REAL-WORLD IMPACT
Stevens AR1, Malinowski JR2, Levinson RT3, Chapman M4, Manemann SM5, Wilson MP6, Bielinski SJ5, Rasmussen LV7, Wiley LK6. 1University of Colorado Anschutz Medical Campus, Aurora, CO; 2Write InScite LLC, South Salem, NY; 3Heidelberg University Hospital, Heidelberg, Germany; 4King’s College London, London, United Kingdom; 5Mayo Clinic, Rochester, MN; 6University of Colorado Anschutz Medical Campus, Aurora, CO and 7Northwestern University Feinberg School of Medicine, Chicago, IL
Purpose of Study: Lung cancer is the leading cause of cancer-related deaths in the United States. Nevertheless, current lung cancer guidelines are not always developed on diverse populations. Researchers increasingly use electronic health record (EHR) data to inform strategies for disease prevention, treatment, and monitoring. These studies require phenotyping algorithms to identify patients with lung cancer, but it is unclear how well these algorithm-identified populations align with the known prevalence of the disease. Our study aims to address this knowledge gap, which currently poses a potential source of bias and misrepresentation of lung cancer identification that may propagate healthcare inequities in research and policy.
Methods Used: We conducted a sub-analysis of all lung cancer phenotyping algorithms identified by a systematic evidence review (SER) of US-based EHR phenotyping algorithms. The larger study searched PubMed for articles published through August 10, 2022 that mentioned both EHRs and one or more terms for automated cohort identification methods. All studies were reviewed in duplicate with a standardized protocol to assess inclusion/exclusion and extract key variables related to algorithm quality. In this study, a single reviewer performed additional extraction of demographic variables for lung cancer algorithms including: age, sex/gender, and race/ethnicity/ancestry.
Summary of Results: A total of 11,913 studies were identified with 856 studies included after review. This analysis extracted data from 29 studies that identified one or more lung cancer related phenotypes, representing 30 distinct phenotype-study pairs. Of these, 12 (40%) reported any demographics of their algorithm-identified lung cancer population. Sex was the most frequently reported demographic variable (n = 10), followed by age (n = 9), and race/ethnicity (n = 8). No algorithms reported gender identity and two algorithms reported genetic ancestry. Where reported, race/ethnicity had the most unique data labels (n = 23), while age had the greatest variability in reporting techniques. We are in the process of analyzing whether each algorithm included additional study specific filters that may influence the representativeness of the algorithm-identified population.
Conclusions: This study provides insights into the current state of demographic reporting for algorithm-identified lung cancer populations. While many studies acknowledge the importance of demographic data (e.g., age, sex, race), these same features are often omitted when describing the specific populations algorithms identify. Consequently, current reporting practices make it difficult to understand the generalizability of study results. These findings prompt a compelling need for standardized demographic reporting, which will amplify research impact through transparency and a greater ability to combat bias in lung cancer research and the clinical guidelines they inform.
# 116
Narrative Review of Strategies for Blood Product Shelf-Life Extension
Akaraphanth M1, 2, Oudakker J1, 2, Paulson M2, 3, Getz T2, 4. 1University of Colorado School of Medicine, Aurora, CO; 2University of Colorado Center for COMBAT Research, University of Colorado School of Medicine, Aurora, CO; 3Denver Health Medical Center, Aurora, CO and 4University of Colorado School of Medicine, Aurora, CO
Purpose of Study: Over 90% of potentially survivable United States (US) battlefield fatalities were associated with severe hemorrhage from 2001 to 2011, making prehospital blood transfusion vital to success in medical military operations. However, near-future conflicts with pronounced casualties and trauma in a resource-limited setting may increase a more sustained demand for blood. Thus, finding innovative ways to prolong the shelf-life of blood products is crucial in the future of trauma care. We reviewed various methods to extend the shelf-life durations of blood products and their possible effectiveness/implementations within an austere environment setting.
Methods Used: We performed a literature review by searching PubMed with a combination of several keywords. Additional pertinent studies were identified by cross-referencing primary articles. Clinical experience of each author was also considered.
Summary of Results: We identified several effective methodologies that can be utilized to prolong blood product storage durations within an austere medicine setting: Additive Solution 7 (AS-7, SOLX), extension of storage with current anticoagulants, supplementation with nicotinic acid or ascorbic acid to anticoagulant solutions, dilution of fresh whole blood with longer stored whole blood, deoxygenation/anaerobic storage during red blood cell (RBC) cold storage, improvements in the cryopreservation of RBC, trehalose use in lyophilization of RBC, thermal holding of whole blood, and the effects of variable temperature cycling on whole blood.
Conclusions: Several studies reveal promising combinations of methods that would allow for shelf-life extension during the storage of blood products and introduce new possibilities that could logistically improve infrastructure to support an extended blood duration supply if needed. Current practices for blood storage can be feasibly manipulated to extend a blood bank; however, more novel implementation that requires massive changes to existing infrastructure may be too expensive for rapid, widespread, and sustained use. More research would be necessary to elucidate the specific implementation of these combined practices to weigh out the estimated risk of transfusing extended stored blood products within resource-limited environments.
# 117
Coronary artery dilation in EBV induced HLH
Bhangal DK, Snider J, Razzaqi F. Valley Children’s Healthcare, Madera, CA
Case Report: A 3 yo female with a history of repaired congenital vaginal atresia and congenital bilateral cataracts status post surgery was transferred to our hospital with anterior neck mass, lymphadenopathy and splenomegaly. She was admitted at an outside hospital for respiratory distress, fever and an enlarging neck mass for 5 days. CT imaging was done, which showed diffuse cervical, submental and axillary lymphadenopathy. She was treated with vancomycin and ceftriaxone. She tested EBV IgM positive. She was transferred to our hospital for further workup. Upon arrival to our hospital she was only responsive to painful stimuli with cool mottled extremities and delayed capillary refill. The patient was transferred to the PICU for closer monitoring. In the PICU she remained febrile with significant cervical lymphadenopathy, splenomegaly, and she also developed cracked lips. Labs were significant for elevated inflammatory markers, mild anemia and thrombocytopenia. An echocardiogram was ordered which showed coronary artery dilation. Given this finding she was immediately treated with IVIG for presumed Kawasaki disease. Her response to IVIG was limited. Rheumatology, cardiology, hematology and oncology were consulted. Additional labs were ordered including HLH, SLE, vasculitis, sarcoidosis, MAS and MIS-C workup was done. Her Ferritin, LDH, and triglycerides were found to be elevated. She was started on Anakinra. After one night her fevers defervesced, lymphadenopathy improved and her periorbital edema decreased. Inflammatory markers began to down trend. She was transferred to the acute care floor. On the acute floor her echocardiogram was repeated which showed decreased coronary artery dilation. Her HLH labs showed elevated CXCL9 and sIL2r. Her EBV PCR titer came back markedly elevated 358,000. She was weaned off of Anakinra. Her other rheumatic disease work up was negative. Hereditary HLH genetic testing was negative. She had resolution of symptoms prior to discharge. She no longer had a neck mass, lymphadenopathy, fevers, or rash.
Conclusion: Kawasaki disease presents with bilateral conjunctivitis, mucositis and coronary artery aneurysms which are rare in HLH. HLH is associated with cytopenias and liver abnormalities. In EBV HLH, the viral infection causes a hyperinflammatory interaction with T cells and macrophages, resulting in excessive production of IFNy, TNFa, IL-1 and other cytokines. Cardiovascular involvement is a rare but very severe complication of EBV infection caused by direct damage and immune injury. Although most children with EBV are asymptomatic and some adolescents will have self limiting mononucleosis., pediatricians should consider these rarer complications, especially in the setting of complex presentation which is not fitting another disease process.
Neonatology General II
Concurrent Session
3:15 PM
Thursday, January 18, 2024
# 118
EFFECT OF A MULTIDISCIPLINARY CARE TEAM ON ACHIEVEMENT OF DISCHARGE MILESTONES IN PATIENTS WITH SEVERE BRONCHOPULMONARY DYSPLASIA: A SINGLE-CENTER STUDY
Gravley W, Kinsey G, Lusk LA, Wai S. UCSF Benioff Children’s Hospital - Oakland, Oakland, CA
Purpose of Study: Hospitalized premature infants must meet several milestones prior to discharge. Among these are absence of bradycardia or apnea episodes, ability to adequately regulate temperature, minimal oxygen requirement, and ability to tolerate full enteral feeds (preferably oral feeds). Infants with bronchopulmonary dysplasia (BPD) reach these milestones two to five weeks later than infants without BPD. Prior studies have demonstrated that the use of multidisciplinary teams (MDTs) in the care of neonates with severe BPD (sBPD) have led to decreased length of stay (LOS), decreased post-menstrual age (PMA) at discharge, increased weight z-score at discharge, and decreased likelihood of feeding difficulties or discharge on home oxygen. The purpose of our study is to examine the effect of a MDT on LOS, PMA at discharge, and time to reach low flow oxygen support (LFS) and full oral feeds (FOF) at our institution.
Methods Used: We performed a retrospective review of all infants born <32 weeks’ gestation who required invasive ventilation or high noninvasive support at 36 weeks PMA born during 2015-2023. Our MDT to treat patients with sBPD was established in January 2019. We compared baseline characteristics, LOS, PMA at discharge, and day of life and PMA where the infant reached FOF and LFS (defined as ≤ 2L nasal cannula) before and after initiation of our MDT. The first year after initiation was treated as a washout period and not included in statistical analysis. Patients who passed away or underwent tracheostomy were not included in LFS analysis. Patients who passed away, underwent tracheostomy, or were discharged on nasogastric or gastrostomy feeds were not included in FOF analysis.
Summary of Results: Birth weight and PMA at birth were similar between the two groups. LFS was reached at a significantly later PMA (43.0 vs. 48.3 weeks, p = 0.003) and later day of life (122 vs. 160 days, p = 0.001) in MDT infants compared to pre-MDT infants. FOF was reached at a significantly later PMA (42.1 vs. 45.5 weeks, p = 0.01) in MDT infants, but there was no significant difference in days of life to reach FOF (122 vs. 139 days, p = 0.08). PMA at discharge was greater (47.9 vs. 51.9 weeks, p = 0.03) and LOS was longer (159 vs. 184 days, p = 0.04) in MDT infants. The number of gastrostomy tube placements decreased serially in the years following initiation of the MDT, but this change was not significant (χ2= 4.42, p = 0.22).
Conclusions: Contrary to findings in other studies, establishment of an MDT at our facility for the treatment of patients with sBPD has resulted in delayed achievement of discharge milestones. The factors contributing to our longer LOS are unclear but possibly related to slower respiratory support weaning and/or delayed initiation of oral feeding. However, practice changes may have yielded potential benefits such as decreases in pulmonary hypertension, neurodevelopmental delay, or postnatal growth failure.
Characteristics
Pre-MDT
MDT
p-value
Birth weight, g
745 (664 - 826)
737 (664 - 810)
0.88
PMA, weeks
25.2 (24.6 - 25.8)
25.6 (25.0 - 26.2)
0.31
Male, %
64
71
0.60
PMA at LFS, weeks
43.0 (40.1 - 45.1)
48.2 (45.8 - 50.9)
0.003
DOL at LFS, days
122 (111 - 134)
160 (143 – 178)
0.001
PMA at FOF, weeks
42.1 (40.4 - 43.9)
45.5 (43.5 - 47.5)
0.01
DOL at FOF, days
122 (108 – 137)
140 (125 – 155)
0.08
PMA at discharge, weeks
47.9 (45.1 - 50.7)
51.9 (49.5 - 54.3)
0.03
LOS, days
159 (141 – 177)
184 (167 – 185)
0.04
Mean birth weight, PMA, time to LFS and FOF with means and 95% confidence intervals. n = 62 for discharge/LOS analysis, n = 59 for LFS analysis, n = 38 for FOF analysis. PMA, post-menstrual age; LFS, low-flow support; DOL, day of life; FOF, full oral feeds; LOS, length of stay.
# 119
ASSOCIATION OF TREATMENTS FOR PATENT DUCTUS ARTERIOSUS WITH SPONTANEOUS INTESTINAL PERFORATION IN PRETERM INFANTS
Cautivar KM1, Cacho BJ2, Jennings H1, Chun P3, Marshall A3, Deming D2. 1Loma Linda University School of Medicine, Loma Linda, CA; 2Loma Linda University Medical Center, Loma Linda, CA and 3Loma Linda University Medical Center, Loma Linda, CA
Purpose of Study: We examined the association of different treatment options for patent ductus arteriosus (PDA) in preterm infants born at < 30 weeks gestation with the development of spontaneous intestinal perforation (SIP).
Methods Used: We reviewed medical records of neonates born in Loma Linda University Children’s Hospital with gestational age < 30 weeks between October 2017 through July 2023. The various PDA treatment protocols included: no treatment, pharmacological therapy (ibuprofen, acetaminophen, or indomethacin), surgical ligation, and catheter occlusion. We assessed the association of each management type with the development of SIP. Data were analyzed using descriptive statistics, Chi-square analysis, and logistic regression (SPSS v28, IBM).
Summary of Results: We identified 370 infants out of which received: 185 no treatment, 145 pharmacologic treatment, 16 surgical ligation, and 24 catheter occlusion. There was no significant difference between the incidence of SIP and any of the various management types (Table 1).
Conclusions: In our population SIP was not associated with any of the treatment types. With the relatively limited sample size for SIP patients, continuing data collection for further longitudinal study is encouraged to increase the power of this study.
SIP
Model Variables
β
OR (95% CI)
p
No Treatment (Referent)
Pharmacologic Treatment
1.097
2.994 (0.903–9.928)
0.073
Surgical Ligation
1.104
3.017 (0.317–28.727)
0.337
Catheter Occlusion
1.414
4.114 (0.7–23.770)
0.114
# 120
OUTCOMES OF INFANTS SCREENED FOR HYPOGLYCEMIA IN THE MOTHER BABY UNIT AND RISK FACTORS ASSOCIATED WITH ADMISSION TO THE NEONATAL INTENSIVE CARE UNIT
Massoumi JY1, Siddiqui S1, Becerra V2, Wertheimer FB1, Ramanathan R1, Cayabyab R1. 1University of Southern California/Los Angeles General Medical Center, Los Angeles, CA and 2Los Angeles General Medical Center, Los Angeles, CA
Purpose of Study: Risk factors for hypoglycemia include preterm gestation, low birth weight, small and large for gestational age, and infants of diabetic mothers. Glucose monitoring is initiated soon after birth in these at-risk infants. The use of 40% oral glucose gel has been reported to be an effective, non-invasive treatment for transient neonatal hypoglycemia in late preterm and term infants within the first 48 hours of life and has been shown to prevent admission to the Neonatal Intensive Care Unit (NICU) and separation of mother and baby. This study aims to characterize the outcomes of infants undergoing screening for hypoglycemia in the mother baby unit (MBU) and to determine risk factors associated with NICU admission.
Methods Used: This is a retrospective (2017-2019) cohort study of infants admitted to the MBU at risk for hypoglycemia and enrolled in the hypoglycemia protocol at LAC+USC Medical Center. Oral glucose gel dose was administered to infants with hypoglycemia defined as blood glucose level below 45 mg/dL. Oral glucose gel dose was based on birth weight. Demographics and outcomes were collected from the electronic medical record, paper records and the Neonatal Information System newborn database.
Summary of Results: There were 410 infants included in this study, 186/410 (45%) of these patients developed hypoglycemia managed in the MBU while 35/410 (8.5%) developed hypoglycemia requiring NICU admission. Neonatal demographics was not different between groups however hypoglycemic infants requiring NICU admission had a higher rate of exposure to maternal preeclampsia and use of antenatal steroids, longer normalization of blood glucose levels and longest hospital stay. Rates of exclusive breastfeeding were highest in infants with normoglycemia. (Table)
Conclusions: Our preliminary data showed that exposure to maternal preeclampsia and antenatal steroids were risk factors associated with NICU admission. Despite no differences in gestational age or birth weight, these infants had longer time to normalize glucose and longer length of stay. Frequent breastfeeding should be encouraged in infants at risk for hypoglycemia. Collection of data is ongoing to verify these results in a larger sample size.
Demographics and Outcomes of the Study Population.
EXTENDED FOLLOW-UP TRENDS IN EXTREMELY PRETERM INFANTS ENROLLED IN THE PRETERM ERYTHROPOIETIN NEUROPROTECTION (PENUT) TRIAL
Patel K1, Horner D2, Puia-Dumitrescu M2, German K2, 3, Perez K2, Valentine GC2, Law J2, Wood TR2, 3, Comstock B2, Mayock D2, Heagerty P2, Juul S2, 3, Kolnik S2. 1University of Washington School of Medicine, Seattle, WA; 2University of Washington/Seattle Children’s Hospital, Seattle, WA and 3Center on Human Development and Disability, University of Washington, Seattle, WA
Purpose of Study: Existing studies have revealed a discrepancy in healthcare utilization between term and preterm infants, with increased utilization in preterm infants up to two years of life. Many infants with significant comorbidities have greater needs as outpatients; however, studies evaluating long-term utilization are limited and suggest that not all follow-up differences can be attributed to in-hospital comorbidities, making the prediction of long-term utilization challenging. This descriptive analysis aims to better understand hospital and medication use after discharge in infants born extremely preterm (EP) at 30-60 months corrected age (CA), and to compare emergency room (ER)/urgent care utilization and rate of hospitalizations to the general population.
Methods Used: This is a post hoc analysis of EP infants born between 24 0/7 and 27 6/7 weeks’ gestation enrolled in the Preterm Erythropoietin Neuroprotection (PENUT) Trial. Infants with at least one phone questionnaire follow-up between 30-60 months CA were included. In addition to maternal, neonatal, and NICU stay information from the PENUT database, questionnaires collected information on ER/urgent care visits, hospitalizations, and medication use. The cohort that survived to discharge was compared to the follow-up cohort using the Mann-Whitney U test, with significance indicated by p < 0.05. General population data for children ages 2-4 years were collected from the National Center for Health Statistics National Health and Nutrition Examination Survey and the Agency for Healthcare Quality and Research via the Healthcare Cost and Utilization Project.
Summary of Results: 569 EP infants were included in this analysis. Maternal, infant, and NICU stay data were similar for the PENUT infants who survived to discharge and for those with follow-up, except infants with follow-up were less likely to have a mother who identified as black (p<0.0001). The most common reason for ER/urgent care visits, hospitalizations, and medication use was for respiratory issues. Compared to the general population, EP infants had fewer ER/urgent care visits but more hospitalizations.
Conclusions: EP infants’ lower rate of ER visits may be indicative of greater access to alternative healthcare resources, while the greater incidence of hospitalization may be secondary to greater baseline severity of illness or need for procedures. Further analysis is needed to direct future efforts to improve overall healthcare and medication utilization among EP infants.
Total number of encounters for ER/urgent care visits and hospitalizations by cause and medication usage by type for PENUT infants with follow-up between 30 and 60 months CA.
PENUT Cohort 30-60 mo CA % (n)
ER/Urgent Care Visits
Hospitalizations
Medications
% of Total Encounters
27.6% (n= 402/1455)
10.0% (n=146/1455)
21.5% (n=313/1455)
Respiratory
35.3% (142)
37.7% (55)
36.7% (115)
Gastrointestinal
5.0% (20)
9.6% (14)
9.3% (29)
Neurologic
7.2% (29)
6.2% (9)
7.7% (24)
Allergy
2.7% (11)
0.7% (1)
24.2% (76)
Infectious
21.6% (87)
2.7% (4)
NA
Accidental Trauma/Ingestion
18.2% (73)
3.4% (5)
NA
Procedures
7.0% (28)
35.6% (52)
NA
Other
3.0% (12)
4.1% (6)
22.0% (69)
Incidence of ER/urgent care visits and hospitalizations in the PENUT cohort and general population per 100 encounters.
# 122
OUTCOMES OF PREGNANCIES AFFECTED BY ALLOIMMUNIZATION IN A LARGE U.S. HEALTHCARE SYSTEM OVER SIX YEARS
Bahr TM1, 2, Tweddell SM1, Zalla JM2, Dizon-Townson D3, Henry ER2, Ilstrup SJ4, Ling C1, Lindgren PC2, O’Brien E2, 1, Christensen RD1, 2. 1University of Utah, Salt Lake City, UT; 2Intermountain Health, Salt Lake City, UT; 3Intermountain Health, Murray, UT and 4Intermountain Health, Murray, UT
Purpose of Study: Advances in the prevention and treatment of Rh(D) alloimmunization have been one of the great success stories of modern obstetric, fetal, and neonatal medicine. Nonetheless, alloantibodies to Rh(D) and non-Rh(D) red blood cell antigens are reported in as many as 4% of pregnancies and can result in hemolytic disease of the fetus and newborn (HDFN). The purpose of this study was to review all deliveries in Intermountain Health hospitals during a six-year period in which the mother had a positive antibody screen; and then summarize neonatal outcomes.
Methods Used: From our data warehouse, we identified all deliveries between January 1, 2017, and December 30, 2022, where the mother had a positive antibody screen anytime during the pregnancy. A member of the research team reviewed the electronic medical record of each pregnancy (mother and baby), not relying on coded information or on data tables. We verified whether the diagnosis of alloimmunization was correct and collected other pertinent information and outcomes. We then summarized these data using summary statistics and hypothesis tests.
Summary of Results: 707 neonates were born to 705 mothers with positive antibody screens during the pregnancy (incidence 3.0 per 1000 live births or 0.3%; two twin gestations). We excluded 31 neonatal cases (4.4%) where the mother’s positive antibody screen was positive due to RhIG and no other antibodies. Three of these had a positive DAT that could not be explained by a cause other than RhIG, but none of the 3 required phototherapy or developed anemia. Of the 676 neonates remaining, 464 (69%) had a DAT performed; 171 of those (25%) were positive. 174 of the 676 (26%) were antigen-positive for at least one antibody identified in the mother’s screen. HDFN was most severe in cases of alloimmunization due to Rh group antibodies (c, C, D, e, E). NICU admission for hyperbilirubinemia was most common in Anti-D cases (64.3% of antigen-positive neonates born to mothers with anti-D). The risk of at least one RBC transfusion or exchange transfusion in neonates born to mothers with positive antibody screens was 4.1%. All were Rh group alloimmunization. No neonates born to mothers with anti-M, anti-S, anti-Duffy, anti-Kidd A, or anti-Lewis required NICU admission for hyperbilirubinemia, RBC transfusion, or exchange transfusion. None of the 676 neonates were later diagnosed with kernicterus.
Conclusions: Approximately 26% of neonates born to mothers with positive antibody screens were antigen positive. Antigen-positive neonates born to mothers with Rh-group antibodies were at highest risk of hyperbilirubinemia, NICU admission for hyperbilirubinemia, and other complications. Though the risk of severe complications (transfusion or exchange transfusion) was low, diligent surveillance and management of these neonates is required to identify those with complications and avoid kernicterus.
# 123
PROCALCITONIN LEVELS IN NON-INFECTED NEONATES IN THE PRESENCE OF RESPIRATORY DISTRESS WITHIN THE FIRST 48 HOURS OF POSTNATAL LIFE
Lorusso Vivas GA1, Vachhani A2, Ramanathan R1, CAYABYAB R1. 1Los Angeles General Medical Center, Los Angeles, CA and 2Children’s Hospital of Orange County, Orange, CA
Purpose of Study: Procalcitonin is a biomarker for bacterial infections. Physiologic elevations of procalcitonin have been reported in the neonatal population in the first 72 hours of life (HOL). Association of procalcitonin levels with severity of respiratory distress in preterm infants has been reported.
The objective of this study is to determine the association of procalcitonin levels in non-infected neonates with respiratory distress within the first 48 hours of postnatal life.
Methods Used: Retrospective cohort study of all infants admitted to the neonatal intensive care unit (NICU) at Los Angeles General Medical Center who underwent early onset sepsis (EOS) work up consisting of procalcitonin, C-reactive protein, complete blood count and blood culture between August 2018 and February 2021. Procalcitonin levels were collected at 0-12 HOL (Time 1), 12-24 HOL (Time 2) and 24-48 HOL (Time 3). Infants with culture positive sepsis and those who were treated for more than 72 hours with antibiotics were excluded from the study. Neonatal and maternal demographics, clinical course, laboratory results were collected. Neonates were divided into 2 groups, presence (PRD), or absence of respiratory distress (ARD). Data was analyzed with Fisher-exact test or Chi Square and Wilcoxon rank sum where appropriate.
Summary of Results: There were 205 non-infected patients included in the study. Infants with respiratory distress were more likely to be born by cesarean section, infant of diabetic mothers, exposed to intrauterine infection and inflammation and less likely to be small for gestational age. There was no difference in birth weight or gestational age. Procalcitonin levels in infants with respiratory distress were significantly higher at Time 2 and Time 3. (Table 1)
Conclusions: Our preliminary data showed that procalcitonin levels are higher in non-infected neonates with respiratory distress within the first 48 HOL. Reference range of procalcitonin levels need to be established in non-infected neonates within the first 48 HOL. Data collection is ongoing to verify these findings.
Neonatal and Maternal Demographics and PCT Levels in the Study Population.
Variable
Absence of Respiratory Distress (ARD)
Presence of Respiratory Distress (PRD)
p value
Birth Weight (grams)
2852.5 (2130, 3345)
2090 (1585, 2975)
0.73
Gestational Age (weeks)
36.715 (34.57, 39)
33.57 (32, 35.43)
0.41
Male Gender
36 (51.43%)
76 (56.3%)
0.3
Hispanic Ethnicity
47 (74.6%)
81 (61.83%)
0.05
Small for Gestational Age
12 (17.14%
8 (5.93%)
0.01
Cesarean Section Delivery
35 (50%)
100 (74.07%)
<0.01
Maternal Gestational Diabetes Mellitus
11 (15.71%)
37 (27.41%)
0.04
Maternal Intrauterine Inflammation and Infection
12 (17.14%)
3 (2.22%)
<0.01
Time 1. PCT values (ng/mL) from 0-12 HOL
0.18 (0.14, 0.33)
0.19 (0.12, 0.3)
0.78
Time 2. PCT values (ng/mL) from 12-24 HOL
2.09 (0.88, 5.98)
3.05 (1.06, 10.7)
0.03
Time 3. PCT values (ng/mL) from 24-48 HOL
1.84 (0.79, 4.5)
3.09 (1.28, 11.4)
0.01
PCT - procalcitonin. HOL - Hours of life.
# 124
NEONATAL HYPOTHERMIA PREVALENCE IN A TERTIARY REFERRAL BIRTHING CENTER IN NEPAL
Tomlin BD2, Mahato A1, Bohara N1, Bajracharya A1, Fassl B3, Judkins A2, Dongol S1. 1Dhulikhel Hospital, Dhulikhel, Nepal; 2University of Utah, Salt Lake City, UT and 3Northeast Ohio Medical University, Rootstown, OH
Purpose of Study: Neonatal hypothermia is a massive worldwide health burden with a global incidence ranging from 32-85% in hospitals and 11-92% in home births. It has been well-studied that neonatal hypothermia is associated with increased morbidity and mortality. While limited studies are available on the prevalence of neonatal hypothermia in Nepal, the cold climate places newborns at an elevated risk. The World Health Organization recommends various practices that have been shown to prevent hypothermia, including Kangaroo Mother Care (KMC), immediate drying of the infant, early skin-to-skin, and early breastfeeding. Unfortunately, their adoption has not been universal, with one study estimating that only 10% of community births receive proper thermal management, and few studies have been done to assess rates of thermal management and their effect on hypothermia in higher-resource hospital settings in Nepal. The purpose of this study is to quantify the prevalence of neonatal hypothermia and assess the impact of standard thermoregulatory practices in the resuscitation period.
Methods Used: This was a prospective cohort study that was based at Dhulikhel Hospital in Nepal, an affiliate of Kathmandu University. A convenience sampling of babies > 35 weeks gestational age who were admitted to the newborn nursery between January and June of 2023 was included in this study. Any thermoregulatory practices were recorded, and an axillary temperature was measured at 1 hour of life as well as complications and discharge information. Our primary outcome was hypothermia at 1 hour of life.
Summary of Results: 193 infants were included in this study. 13 infants (6.7%) were preterm and 21 infants (10.8%) were less than 2500g. At 1 hour of life, 69 (35.8%) of infants were normothermic, 110 (57.0%) had mild hypothermia, and 14 (7.3%) had moderate hypothermia. Those born via C-section had less hypothermia than those born via vaginal delivery (48.3% vs. 79.8%, p = <0.005). All infants were dried after delivery, 50.2% had early skin-to-skin, 21.2% had Kangaroo Mother Care, and 11.9% had early breastfeeding. Infants who received early skin-to-skin were more likely to be hypothermic (78.4% vs. 50.0%, p < 0.005) and those who received KMC were also more likely to be hypothermic (78.0% vs. 60.5%, p = 0.044). Early breastfeeding appeared to have no impact on 1-hour hypothermia (60.9% vs 64.7%, p = 0.817).
Conclusions: A high prevalence of neonatal hypothermia at one hour of life exists in a tertiary referral hospital setting in Nepal. Vaginal delivery, KMC, and early skin-to-skin are all associated with higher rates of hypothermia.
# 125
BODY COMPOSITION ASSESSMENT USING POINT-OF-CARE ULTRASOUND FOR INFANTS ADMITTED TO THE NEONATAL INTENSIVE CARE UNIT
Yeager S1, Hendrixson D1, Cunha GM2, Valentine GC1, Wood TR1, Strobel KM1. 1University of Washington, Seattle, WA and 2University of Washington, Seattle, WA
Purpose of Study: Fat-free mass has been associated with improved neurodevelopment and metabolic health in preterm infants. However, current body composition techniques are not feasible in unstable infants admitted to the neonatal intensive care unit (NICU). This study aims to assess if ultrasound measurements of rectus femoris and biceps muscle area in infants in the NICU are feasible, safe, and reliable.
Methods Used: This is a pilot, prospective observational study recruiting infants from 24-46 weeks admitted to the NICU. Infants have ultrasound measurements, foot length, mid-upper arm, mid-thigh and abdominal circumference measured every other week. Parental anthropometrics are collected at enrollment. Nutritional prescription and standard anthropometrics are collected weekly. During each ultrasound session, three static cross-sectional images of each muscle are obtained using a linear probe with depth adjusted to visualize the muscle and bone. For the first twelve subjects, a second neonatologist obtains a single image of each muscle for assessment of inter-rater reliability using intraclass correlation. Images are reviewed by an ultrasound radiologist to ensure accuracy in identifying the appropriate muscle. Quantitative muscle cross-sectional area measurements are obtained using the polygon tool on Horos medical image software (horosproject.org).
Summary of Results: Prior to study launch, pilot scans were conducted with parent permission on infants of various gestational ages. All study procedures took approximately 30 minutes. To date, six participants have been enrolled and a total of ten sets of measurements have been obtained.
Figure 1
demonstrates offline processing of the biceps and rectus femoris muscle area in a 2-week-old ex-29-week infant who weighed 1.7 kg at the time of the scan. Mean area was found to be 43.7 mm2 for left biceps and 41.6 mm2 for left rectus femoris. Study procedures were well tolerated by all subjects without any reported adverse safety events (hypothermia, apnea, bradycardia, or desaturations).
Muscle area measurements in a 2-week-old, ex 29-week infant. Left outline represents a biceps muscle, right outline represents a rectus femoris muscle.
Conclusions: Overall, early results indicate the methods presented in this study for ultrasound measurements of infant muscle mass are feasible, safe, and identify anatomy accurately. Images obtained are adequate to measure biceps and rectus femoris muscle area. Following further subject recruitment, we will assess inter-rater reliability of these measurements and the association of muscle area with other growth metrics and protein prescription.
Neonatology Pulmonary II
Concurrent Session
3:15 PM
Thursday, January 18, 2024
# 126
Continuous Chest Compressions with High Frequency Jet Ventilation Improves Gas Exchange in Asphyxiated Cardiac Arrested Preterm Lambs
Giusto E1, 2, Riley E3, 1, Sankaran D1, Lesneski A4, Valdez R1, Hardie M1, Hammitt VL4, Lakshminrusimha S1, Vali P1. 1University of California, Davis, Sacramento, CA; 2University of California, San Francisco, San Francisco, CA; 3REACH Air, Redding, CA and 4University of California, Davis, Davis, CA
Purpose of Study: Gas exchange is severely impaired during cardiopulmonary resuscitation (CPR) in neonatal cardiac arrested. Optimizing gas exchange during neonatal CPR may improve cerebral oxygen delivery (cDO2) and prevent fluctuations in PaCO2.
We hypothesize that asynchronous continuous chest compressions (CCC) with high frequency jet ventilation (HFJV) in extremely preterm lambs in cardiac arrest will result in improved gas exchange and cDO2 compared to 3:1 compression-to-ventilation (C:V) resuscitation and continuous chest compressions with asynchronous ventilation via a T-piece resuscitator (CCaV).
Methods Used: Time-dated extremely preterm (124-126 days gestation; equivalent human ~25 weeks) fetal lambs were intubated and instrumented. Lambs were asphyxiated by umbilical cord occlusion until asystole and delivered. Initial resuscitation commenced with positive pressure ventilation via T-piece device at an FiO2 of 0.3 for 30 seconds. If heart rate did not improve, chest compressions (cc) were started and FiO2 was increased to 1.0. Lambs were assigned to standard 3:1 C:V resuscitation following the Neonatal Resuscitation Program algorithm (3:1 C:V group), CCC (120cc/min) with asynchronous ventilation (CCaV group), or CCC (120cc/min) with HFJV (CCC + HFJV group). First dose of epi (epinephrine) was given at 3 minutes and repeated every 3 min until return of spontaneous circulation (ROSC). Lambs in the 3:1 C:V and CCaV groups that achieved ROSC were managed on conventional ventilation and lambs in the CCC + HFJV group were maintained on HFJV. Ventilation parameters and FiO2 were adjusted to maintain SpO2 at 88-95% and PaCO2 between 45-60 mmHg.
Summary of Results: 23 lambs were studied. Baseline characteristics were similar and all lambs achieved ROSC. 22 lambs achieved ROSC after just one epi; one of the lambs in the CCaV group achieved ROSC after a second dose of epi. The CCC + HFJV group had quicker time to ROSC than the CCaV group but similar to the 3:1 C:V group (Table).
PaCO2 was lower in the CCC + HFJV group at time of ROSC and post-ROSC compared to the 3:1 C:V and CCaV groups (Figure). PaO2 was higher during CPR and at time of ROSC in the CCC + HFJV group compared to the other groups (Table). There was no difference in carotid flow between groups, however cDO2 was higher in CCC + HFJV group compared to 3:1 C:V group during CPR and at time of ROSC (Table). cDO2 was higher in the CCC + HFJV group compared to the CCaV group at time of ROSC (Table).
Conclusions: Resuscitation using CCC during HFJV is feasible with similar success of ROSC and improved gas exchange and cDO2 during CC and at ROSC in asphyxiated cardiac arrested preterm lambs. Further studies are required to validate our results and to assess biomarkers and lung injury by histology.
Oxygenation, Carotid Flow during Resuscitation, and Time to ROSC. Values are median (interquartile range).
CaO2 = oxygen content of carotid arterial blood. Mean Qca = mean carotid blood flow. cDO2 = cerebral oxygen delivery. *p-value < 0.05 via Kruskal-Wallis H Test ap-value < 0.05 via post-hoc Dunn test comparing CCC + HFJV to 3:1 C:V bp-value < 0.05 via post-hoc Dunn test comparing CCC + HFJV to CCaV.
# 127
Randomized trial of effectiveness of peripheral venous vs. umbilical venous routes in an ovine model of perinatal asphyxial arrest
Valdez R, Giusto E, Lesneski A, Hammitt VL, Tully KC, Vali P, Lakshminrusimha S, Sankaran D. University of California, Davis, Davis, CA
Purpose of Study: Current guidelines recommend umbilical venous route for epinephrine administration in neonatal cardiac arrest not responding to ventilation and chest compressions. However, an umbilical venous catheter (UVC) placement can take 5.4 ± 2.2 min (Halling et al 2017) and requires expertise and specialized material that may be a challenge for emergency medical personnel and non-neonatal providers. Our objective was to compare the incidence of return of spontaneous circulation (ROSC) between low-lying UVC and peripheral venous (PIV) routes of epinephrine during ovine perinatal asphyxial arrest.
Methods Used: Term fetal lambs were intubated and instrumented. Asphyxia was induced by cord occlusion until cardiac arrest. Based on randomization, UVC and/or PIV were placed. Following resuscitation with ventilation and chest compressions, lambs were randomized to receive epinephrine at 0.02-0.03 mg/kg via UVC or PIV. Intravenous epinephrine was followed by a 3mL normal saline flush in both the groups. Hemodynamics weremonitored.
Summary of Results: Gestational age and birth weightwere similar between the study groups (table). All lambs achieved ROSC with the first dose of epinephrine in theUVC and PIV groups, except for 1 lamb in the PIV groupthat did not achieve ROSC despite 4 doses of epinephrine, table). Incidence and time to achieve ROSC were not different between lambs that received UVC vs PIV epinephrine (table). Carotid blood flow and mean blood pressures were similar after ROSC (figure).
Conclusions: Incidence of ROSC and time to ROSC were similar between PIV and low-UVC routes of epinephrine. We plan to compare plasma epinephrine concentrations from the lambs. Further studies are warranted to study the feasibility, timing, and effectiveness of the PIV route of epinephrine in newborns not responding to chest compressions. This simple technique may benefit newborns globally especially when the resuscitator is an emergency medical personnel lacking expertise in UVC placement or in low resource settings without access to a UVC.
Table 1: Comparison of baseline characteristics, ROSC outcomes and hemodynamics at ROSC between low UVC and PIV routes.
Parameters
UVC(n=5)
PIV
(n=8)
p-value
Gestational age (days)
140.2 (1.1)
140.2 (1.2)
0.94
Birth Weight (kg)
3.15 (0.7)
3.31 (1.4)
0.82
Sex
3F, 2M
5F, 3M
0.93
Incidence of ROSC n (%)
5 (100%)
7 (87.5%)
0.83
Time to Asystole (minutes)
14.3 (3.1)
15.3 (2.3)
0.50
pH at Asystole
6.9 (0.1)
6.9 (0.1)
0.91
Median time to ROSC from PPV (seconds) and interquartile ranges
214 (210-219)
215 (206-221)
0.81
Median time to ROSC from Epi dose (seconds) and interquartile ranges
29 (25-36)
30 (26.5-39)
0.80
Data presented as mean (standard deviation) or median (interquartile range) as specified. Categorical data compared by Fishers Exact test. Continuous data compared by unpaired t-test. Data not different between the two study groups. UVC, umbilical venous catheter. PIV, peripheral intravenous catheter, ROSC, return of spontaneous circulation. PPV, positive pressure ventilation.
Data not differnt by repeated measures ANOVA.
CPR- Cardiopulmonary Resuscitation, ROSC- Return of Spontaneous Circulation.
# 128
USE OF LONG TERM VENTILATION FOR PRETERM INFANTS WITH SEVERE BRONCHOPULMONARY DYSPLASIA IN BRITISH COLUMBIA: A RETROSPECTIVE COHORT STUDY
Mundi K1, Kieran E1, 2, Van Dyk J1, 3, Wright M1, 4. 1University of British Columbia, Vancouver, BC, Canada; 2BC Children’s Hospital, Vancouver, BC, Canada; 3BC Women’s Hospital and Health Centre, Vancouver, BC, Canada and 4BC Children’s Hospital, Vancouver, BC, Canada
Purpose of Study: With improved survival of infants born at increasingly low gestations, a growing number of infants with bronchopulmonary dysplasia (BPD) are being discharged from neonatal intensive care units (NICU). Some infants with severe disease require ongoing respiratory support after discharge, which can include low-flow oxygen (LFO2), non-invasive ventilation (NIV), or invasive ventilation via tracheostomy (trach/vent).
This study characterizes the population of infants with BPD who require respiratory support after NICU discharge, and addresses knowledge gaps about their trajectory (duration of respiratory support, long-term respiratory and non-respiratory outcomes, differences in outcomes according to type of respiratory support).
Methods Used: We conducted a retrospective review of infants ≤28 weeks gestational age (GA), diagnosed with BPD, and discharged from a level 3 NICU in British Columbia in a 10-year period (2013–2022) with need for respiratory support at discharge. Data were also collected for infants with BPD requiring respiratory support who died in NICU.
Cases were identified from hospital coding and databases of provincial NICU follow-up and pediatric home ventilation programs.
Data collected included demographics, antenatal background, medical comorbidities, postnatal management, serial growth and neurodevelopmental assessments.
Summary of Results: In a 10-year period, 104 infants with BPD were discharged on home respiratory support: 65% male and 23% multiple births. Median GA was 25 weeks (IQR 3) and birth weight (BW) was 730g (IQR 175). 24 children with BPD receiving ventilatory support died before NICU discharge at median 47 days old (IQR 63). There was no difference in GA or BW between infants who died and survived to discharge.
Of surviving infants, 9% (n=9) were managed with trach/vent, 40% (n=42) with NIV (55% BiPAP, 45% CPAP), and 51% (n=53) with LFO2. Infants with trach/vent were significantly older at NICU discharge (median 386 vs 216 days, p<0.001) and stopping ventilation (median 4.6 vs 1.7 years, p<0.001) than those discharged on NIV. In LFO2 treated children, median age at stopping O2 was 9 months (IQR 6).
Characteristics of children managed with NIV and trach/vent were similar, apart from a higher prevalence of medically managed pulmonary hypertension (PH) and older age at initial successful extubation in the trach/vent group (Table 1).
In the 2 years after NICU discharge, 62% of children (n=64) were readmitted to hospital, more frequently in children with trach/vent than NIV (89% vs 61%, NS). 74% of admissions were for acute illness. All children discharged on NIV and trach/vent were alive at median 4.5 years follow-up.
Conclusions: NIV can be used to support infants with severe BPD after NICU discharge, irrespective of GA at birth, and is associated with shorter NICU admission and ventilation duration than trach/vent. PH is a significant predictor for tracheostomy. Further analyses will compare clinical outcomes including longitudinal measures of growth and neurodevelopment.
Differences in patient characteristics and management between children discharged on NIV and trach/vent support (n=51).
PPROM: preterm prolonged rupture of membranes. HFOV: high frequency oscillatory ventilation *Statistically significant, p<0.05.
# 129
ANALYSIS OF SIGNALING PATHWAYS THAT CONTROL PROGENITOR EPITHELIAL CELL PROLIFERATION & DIFFERENTIATION USING HUMAN LUNG ORGANOIDS
Kibe R1, 2, Li C3, 4, Smith SM5, 6, Minoo P5, 3. 1LAGMC, Los Angeles, CA; 2University of Southern California, Los Angeles, CA; 3Keck School of Medicine, USC, Los Angeles, CA; 4Hastings Institute of Pulmonary Research, Los Angeles, CA; 5Hastings Institute for Pulmonary Research, Los Angeles, CA and 6USC School of Dentistry, Los Angeles, CA
Purpose of Study: Bronchopulmonary Dysplasia (BPD) is a known complication of prematurity as a result of unrepaired alveolar injury. A potential cause in BPD pathogenesis may be either lack of or unresponsiveness of regenerative alveolar type 2 (AT2) stem cells secondary to interruption of their communication with the surrounding niche mesenchyme due to immaturity and/or injury. In a mouse genetic model, we recently identified signaling pathways including Hepatocyte Growth factor (HGF) and Insulin-Like Growth Factor 1 (IGF1) which appeared to be interrupted in the cross-communication between the niche mesenchyme and the progenitor AT2s during alveologenesis, resulting in a BPD-like phenotype. Information on progenitor AT1 and AT2 cells, and their cross-communication with the surrounding niche mesenchyme during human fetal lung development is limited. Our aim was to elucidate the role of signaling pathways in the development and differentiation of alveolar epithelial progenitor cells using an organoid model of human pluripotent stem cells obtained from distal human fetal lung tissue
Methods Used: Lung Organoids were prepared from the distal tip of lung tissue isolated from 11-week gestational-age human fetal lungs. The lung tips have been shown to contain functional pluripotent alveolar epithelial progenitors by several studies. We used both stimulation and inhibition of the IGF1 and HGF signaling pathways using recombinant protein or targeted small molecule inhibitors respectively. We examined the impact on the growth of organoids, alveolar epithelial cell proliferation, and differentiation. Quantitative RT-PCR was used to quantify gene expression for proliferation and alveolar epithelial cell differentiation markers. Immunostaining was performed to assess the organoid structure and spatial localization and distribution of the specific cell markers
Summary of Results: Isolated distal tips of human 11-week gestation fetal lung formed multiple organoids composed of distal lung epithelial progenitors which express high levels of SOX9 and low levels of SOX2. Treatment of organoids with recombinant IGF1 had a measurable impact on cell proliferation, represented by an increase of proliferation marker Ki67. Consistent with the latter findings, inhibition of IGF1R by picropodophyllin (PPP) reduced cell proliferation. In contrast to IGF1, blocking HGF signaling by capmatinib affected both cell proliferation and AT1 lineage gene expression as evidenced by robust increased expression of HOPX.
Conclusions: The studies using the distal lung tips that contain pluripotent progenitor cells demonstrate that at least some of the functional findings regarding the role of IGF1 and HGF signaling pathways in niche-epithelial cell cross-communication may be conserved between mouse and human. Current studies are underway to elucidate the function of this cross-communication in more detail.
# 130
Lamellar Body Formation in LRRK2 -/- Distal Lung Organoids
Smith E1, 2, McVicar R1, Leibel SL2. 1Sanford Burnham Prebys, La Jolla, CA and 2University of California San Diego, La Jolla, CA
Purpose of Study: Neonatal respiratory distress syndrome (RDS) occurs in over 50% of infants born less than 28 gestational weeks, making it a leading cause of neonatal morbidity and mortality. RDS occurs due to a gestational quantitative deficiency of surfactant, a molecule that is made and stored within lamellar bodies (LBs) of alveolar type two cells (AT2) that functions to reduce surface tension in the lung. Currently the only treatment for RDS is invasive intubation and exogenous surfactant therapy, as well as supportive therapy through positive pressure ventilation. Exposure to invasive ventilation and oxygen may lead to chronic lung disease. Recent studies have discovered that inhibition of the leucine-rich repeat kinase 2 (LRRK2) kinase gene increased the production and size of the surfactant-containing LBs. This may be a novel therapy against RDS that is safer and longer lasting than exogenous surfactant and mechanical ventilation.
Methods Used: We used LRRK2 KO induced pluripotent stem cell derived distal lung organoids (LO) to elucidate the mechanism of LB growth and surfactant secretion. The LRRK2 KO line was generated by deleting 5 bp at the G2019S site within the LRRK2 gene with CRISPR/Cas9. We generated 3 different model systems of wild type and LRRK2 KO iPSC derived distal LOs including 1) 3D matrigel embedded; 2) 3D dissociated into monolayers and 3) 3D dissociated onto transwells in air-liquid-interface (ALI) format. We evaluated the gene and protein expression of alveolar type II markers including HTII-280 and pro-SPC along with the LB marker, LAMP3.
Summary of Results: Nile red, a stain that targets LBs, had higher expression in 3D distal LOs compared to dissociated 3D monolayers. In addition, flow cytometry analysis for alveolar type 2 markers revealed that 3D organoids in an ALI format had higher yields of AT2’s compared to the 3D matrigel embedded organoids. Finally, measurement of LB size showed that they were larger in the LRRK2 KO LOs vs wild type LOs.
Conclusions: We found that LRRK2 KO iPSC derived distal LOs had increased AT2 cells when modelled as ALI cultures and that LBs from the KO lines were larger than those from WT lines. These findings will promote the understanding of LB development and potentially be translated into a therapeutic intervention for babies born premature.
# 131
Impact of Early Postnatal TBX4 Insufficiency on Lung Development and Pulmonary Hypertension in Infant Mice
Smith C1, Ding KL1, Seedorf G2, Abman SH2, 1. 1University of Colorado School of Medicine, Aurora, CO and 2Pediatric Heart Lung Center, Aurora, CO
Purpose of Study: T-box transcription factor 4 (TBX4) mutations represent a rare disorder that presents with severe respiratory failure with pediatric pulmonary hypertension (PH). PH in these patients is often poorly responsive to therapy and is associated with abnormal lung development. However, there is a significant degree of clinical heterogeneity in presentation of TBX4 mutations regarding the age of disease onset, and the severity of lung disease and PH. It is known that TBX4 deficiency is embryonic lethal in genetic mouse models. Whether partial or late disruption of TBX4 signaling allows for neonatal survival or if there is impaired lung growth is uncertain. Therefore, we hypothesized that disruption of TBX4 expression in the early postnatal period impairs lung development as indicated by disruptions in the distal lung airspace as well as vascular growth.
Methods Used: In this study, a mouse model of genetic TBX4 deficiency is used in which the TBX4 gene is inactivated by an inducible Cre-loxP system. Cre is temporally induced by subcutaneous tamoxifen injection on day of life (DOL) 1. On DOL 21, lung function is measured using a Scireq Felxivent and lungs are collected and inflated with 4% PFA and held at 20 cm H2O inflation pressure for 1 hour. Lung tissues are then sent for histologic analysis. Mice are genotyped by PCR for both TBX4 and Cre. For subsequent analysis, subjects are genotypically grouped as: TBX4 KO/Cre- (TBX4), TBX4 KO/Cre+ (TBX4Cre), TBX4 WT/ Cre- (HET), or TBX4 WT/Cre+ (HETCre). Lung histologic samples are evaluated by morphometric analysis by measuring radial alveolar counts (RAC) and mean linear intercept (MLI). Samples are further analyzed for vessel density. Right ventricular hypertrophy (RVH) is additionally measured by Fulton’s index.
Summary of Results: We found that RAC was reduced in the TBX4Cre group when compared with the HET group (p < 0.05), which indicates impaired lung complexity. Similar findings were seen with MLI, which showed increased MLI in the TBX4Cre group in comparison with the TBX4 group (p < 0.05). The total respiratory system resistance was greater in the TBX4Cre group when compared with other groups (p < 0.05). Total lung compliance in the TBX4Cre group was lower than the HET group (p <0.005). Decreased pulmonary vessel density was found in TBX4Cre mice when compared with the HET group (p<0.05). TBX4Cre neonates exhibited significant RVH when compared with the HET group (p<0.05).
Conclusions: Inactivation of TBX4 signaling in the early postnatal period was sufficient to impair lung growth and development, leading to impaired alveolar and vascular growth with abnormal lung function and RVH. We speculate that postnatal TBX4 is essential for healthy lung development, and that the timing and degree of TBX4 disruption contributes to clinical heterogeneity of phenotypes associated with TBX4-related disease.
# 132
TEMPORAL VALIDATION OF A MACHINE LEARNING-BASED PREDICTION TOOL FOR SURVIVAL WITHOUT BRONCHOPULMONARY DYSPLASIA
Vu V1, Sakhamuru S1, Chou F2, Vora F1. 1Loma Linda University, Loma Linda, CA and 2Kaiser Riverside, Riverside, CA
Purpose of Study: Bronchopulmonary dysplasia (BPD) is speculated to have a developmental origin and is influenced by antenatal, perinatal, and postnatal factors. We first developed a machine learning (ML) based prediction model with data from 552 infants born between 2013 and 2020. The model was tested using data from 137 infants from the same cohort. In this study, we aim to validate the BPD predictability of the model with 2021-2023 infant data.
Methods Used: Infants born at gestational age (GA) of 30 3/7 weeks or less who survived till 36 weeks postmenstrual age (PMA) were included. We collected perinatal factors including GA, sex, race/ethnicity, birth weight (BW), maternal smoking and respiratory support mode in the first 14 days of life. BPD was defined based on the 2019 NICHD Neonatal Research Network criteria. The data table was then applied to the prediction model (https://neostat.shinyapps.io/Resp_Mode_ML/). Of note, the model was developed to predict no BPD vs. BPD regardless of grade. Descriptive statistics with mean±sd or median (interquartile range) for continuous variables and count (percentage) for categorical variables are presented. To assess prediction performance, the receiver’s operating characteristics area under the curve (ROC AUC) with 95% confidence interval was calculated based on the probability of no BPD and the actual BPD diagnosis. Paired ROC AUC were compared statistically with DeLong method.
Summary of Results: We screened 365 infants, included 234 infants and excluded 131 due to missing data. Of those, 85 infants did not have BPD, while 149 infants did. Infants with BPD were more likely to be male, with lower GA and BW. ROC AUC was 0.867 (95% CI: 0.820-0.914), compared to 0.921 (0.899-0.943) and 0.899 (0.848-0.949) from the training and testing datasets, with p-values of 0.041 and 0.361, respectively. In subgroup analyses, there were no differences in the prediction performance between birth years, infant sex, or small for GA status.
Conclusions: Temporal validation of the prediction model showed overall satisfying performance but slightly worse compared to the internal validation, likely due to evolving respiratory practice over time. Study limitations include the inability to predict BPD grade and data from single-center study. The ability to predict BPD in early life confirms a developmental origin and an opportunity for postnatal intervention to alter its trajectory.
Demographic summary
BPD
No BPD
P-value
Number
149
85
Birth year, n (%)
2021
55 (36.9)
28 (32.9)
0.746
2022
66 (44.3)
42 (49.4)
2023
28 (18.8)
15 (17.6)
Gestational Age (wk), median (IQR)
26 3/7 (24 6/7, 27 6/7)
29 3/7 (27 4/7, 30 0/7)
< 0.001
Birth Weight (g), mean±sd
824±240
1118±246
<0.001
Male, n (%)
81 (54.4)
31 (36.5)
0.012
Race/Ethnicity, n (%)
Asian
3 (2.0)
5 (5.9)
0.287
Black
21 (14.1)
15 (17.6)
Hispanic
83 (55.7)
48 (56.5)
Other
2 (1.3)
0 (0.0)
White
40 (26.8)
17 (20.0)
Maternal smoking, n (%)
6 (4.0)
2 (2.4)
0.761
# 133
OUTCOMES OF INFANTS REQUIRING SURFACTANT ADMINISTRATION THROUGH TWO DIFFERENT TECHNIQUES: LESS INVASIVE SURFACTANT ADMINISTRATION VS INTUBATION-SURFACTANT-EXTUBATION
Sandhu JK1, Siddiqui S1, Feliz Sala E1, Ramanathan R2, Biniwale M2. 1Los Angeles General Medical Center, Los Angeles, CA and 2Los Angeles General Medical Center, Los Angeles, CA
Purpose of Study: Surfactant administration decreased mortality and complications associated with respiratory distress syndrome (RDS) in premature infants. The most common administration technique such as the INtubation-SURfactant-Extubation (INSURE) method, requires intubation, giving surfactant through an endotracheal tube and a brief period of invasive mechanical ventilation. More recently, we changed our practice of surfactant administration using a thin catheter known as Less Invasive Surfactant Administration (LISA) which does not require endotracheal intubation. The purpose of our study was to compare the adverse events and outcomes after changing the practice of surfactant administration from INSURE to LISA in our patient population.
Methods Used: This is a retrospective (2016 to 2022) cohort study of neonates admitted to a Level III Neonatal Intensive Care Unit at Los Angeles General Medical Center who received surfactant administration through either LISA or INSURE. Data was abstracted from the NICU database and electronic health records, and analyzed using SPSS version 29.
Summary of Results: There were 119 infants included in this study. 69/119 (58%) received surfactant administration via INSURE; 50/119 (42%) received surfactant administration via LISA. Infant characteristics were similar in both groups. Of the infants that received LISA, it was successful in 90%; it failed requiring INSURE in 2%; and in 8% it was successful but intubation and mechanical ventilation was needed for continued respiratory distress. The rates of procedure related adverse events were 4.3% for InSURE compared to 12.2% (p=0.106) for LISA. The percentage of infants requiring mechanical ventilation after surfactant administration were similar for both LISA and INSURE (32.7% vs 27.1%, p=0.516). Bronchopulmonary dysplasia (BPD) was observed in significantly higher number of infants who received surfactant using INSURE compared to infants who received surfactant via LISA (43.5% vs 10.4%, p=<0.001). There was no significant difference between groups for grade of BPD however majority of the infants diagnosed with BPD were classified as moderate BPD (52.8%), defined as requiring oxygen supplementation <30% FiO2 at 36 weeks postmenstrual age, per the NICHD classification. The number of days spent on invasive or non-invasive ventilation between the two groups was not significantly different.
Conclusions: Our preliminary data showed that after introducing Less Invasive Surfactant Administration, significantly less number of infants were diagnosed with bronchopulmonary dysplasia when compared to the INtubation-SURfactant-Extubation technique. Collection of data is ongoing to determine other factors of significance and to verify these results in a larger sample size.
Demographics and outcomes of the study population.
INTRANASAL ADMINISTRATION OF NA-112, A SELECTIVE CALPAIN-2 INHIBITOR, PREVENTS SEIZURE-INDUCED HIPPOCAMPAL CALPAIN ACTIVATION
Berndt HN1, Pogue A1, Braga M1, Reece T1, Su W1, Penna E1, Bi X1, Baudry M2. 1Western University of Health Sciences, Pomona, CA and 2Western University of Health Sciences, Pomona, CA
Purpose of Study: Calpain-2 is a calcium-dependent protease that is activated by seizure activity and triggers neuronal damage. When calpain-2 is activated, it cleaves the cytoskeletal protein spectrin, resulting in the formation of spectrin breakdown products (SBDPs), which can be quantitatively analyzed with Western Blots. In this study, the first experiment aimed to determine whether intranasal (IN) administration of NA-112 could inhibit calpain-2 activity, and the second aimed to determine the effectiveness of IN NA-112 if given 4 hours, 8 hours, or 12 hours after seizure induction.
Methods Used: Animal experiments were conducted in accordance with the NIH Guide for the Care and Use of Laboratory Animals. All protocols were approved by the local IACUC of Western University of Health Sciences. Fifteen 3-month-old C57BL/6J male mice were acclimated to their cages for one week, which was followed by 5 days of rewarded habituation for intranasal administration. The first day of habituation involved placing the mice in the researcher’s palm for 3 minutes, with an additional minute for head-stroking. The second day involved holding the mice while head-stroking for 3 minutes, then suspending them in the IN hold without inversion for 15 seconds. On the third day, the mice were suspended and inverted in the IN hold for 15 seconds. A pipette was suspended in front of each nostril for 15 seconds while in the IN hold on the fourth day. The final day involved administering 1.5 µL of vehicle per nostril, then continuing to hold for 15 seconds after each dose. Kainic acid (5 mg/kg) was administered ip 3 times, 20 minutes apart, to induce seizure activity. Two hours after kainic acid (KA) injection, all groups received 1.5 µL IN dose per nostril, with a total dose of 3 µL per mouse. Each treatment group consisted of 3 mice: control (vehicle only), KA only (vehicle only), KA + NA-112 0.1 mg/kg, KA + NA-112 0.3 mg/kg, and KA + NA-112 1.0 mg/kg. Twenty-four hours after KA injection, hippocampi were harvested and processed for spectrin analysis with Western Blots. The procedure was repeated with fifteen same-strain mice for the second experiment, except the treatment groups were as follows: control (vehicle only), KA only (vehicle only), KA + NA-112 0.3 mg/kg dosed 4 hours, 8 hours, and 12 hours after seizure induction.
Summary of Results: There was a significant increase in the ratio of SBDP (150 kDa)/full-length spectrin (p-value<0.0001 for the first experiment, p-value = 0.0001 for the second experiment) for the KA only group as compared to control. As NA-112 dose increased, the ratio of SBDP (150 kDa)/full-length spectrin decreased significantly as compared to the KA only group (p-value<0.0001 for all 3 NA-112 treatment groups in both experiments).
Conclusions: These results demonstrate that IN administration of NA-112 is very effective to inhibit seizure-induced calpain-2 activation, even dosed 12 hours after seizure induction, showing the potential use of IN NA-112 to therapeutically treat seizures.
# 135
EFFECTS OF PERIPHERAL OR CENTRAL INSULIN RECEPTOR INHIBITION ON BLOOD-BRAIN BARRIER PERMEABILITY
Bandarupalli T1, Noonan C2, Weaver R2, Hansen K2, Banks W2, Erickson M2, Rhea E2. 1University of Central Florida College of Medicine, Orlando, FL and 2University of Washington, Seattle, WA
Purpose of Study: Existing associations between insulin resistance and pro-inflammatory states, particularly with endothelial cells, have been shown to influence the function of the Blood-Brain Barrier (BBB) and its associated cells in the neurovascular unit. Given this relatively unexplored link between insulin resistance and neuroinflammation, the objective of this study is to investigate whether inhibition of the insulin receptor, either peripherally or centrally, increases the susceptibility to BBB disruption. We hypothesize that insulin signaling, both peripherally and centrally, can affect the susceptibility of the BBB to a pro-inflammatory state. Additionally, acquiring a comprehensive range of physiological and biochemical data enables us to assess how peripheral/central insulin inhibition and inflammatory states affect neurally mediated metabolic schematics such as weight and satiety.
Methods Used: We induced peripheral/central receptor inhibition using an insulin receptor antagonist, S961, in mice with and without a lipopolysaccharide (LPS) inflammatory stimulus. Mice were treated first with S961 (+/-) and 30 minutes later, with LPS (+/-). S961 was administered intraperitoneally for peripheral insulin pathway targeting and intranasally for the central insulin pathway. Twenty-eight hours following the administration of LPS treatment to four experimental groups (Veh/Veh, Veh/LPS, S961/Veh, S961/LPS), physiological data was collected, and BBB permeability was evaluated using a radioactive tracer [99mTc-DTPA]. Body weight, food and water intake, and blood glucose levels were also measured before and after treatment. Serum amyloid A (SAA) levels were measured in serum as a pro-inflammatory marker.
Summary of Results: LPS injection (the inflammatory stimulus) resulted in a significant increase in BBB permeability compared to saline-treated mice. Peripheral insulin receptor inhibition with S961 did not affect BBB permeability following LPS treatment. Interestingly, central insulin receptor inhibition prevented the LPS-induced increase in BBB permeability and suppressed the LPS-induced rise in SAA.
Conclusions: Our data suggests that acute central insulin receptor inhibition provokes a neuroprotective effect both at the BBB and peripherally during inflammatory conditions. These observations have implications for treatment choice to protect against neurological damage during acute disruption of the BBB.
# 136
ETHNIC AND RACIAL DISPARITIES IN PROGRESSION OF MULTIPLE SCLEROSIS IN THE UNITED STATES: A LITERATURE REVIEW
Gerges M1, Cao R1, Desai K1, Hiranandani A1, Jin C1, Kang S1, Lee S1, Afghani B1, 2. 1UC Irvine School of Medicine, Irvine, CA and 2CHOC Hospital of Orange County, Orange, CA
Purpose of Study: There are conflicting reports on outcome or progression of multiple sclerosis (MS) in terms of disability among different races. In addition, it is unclear how other social determinants of health contribute to the racial/ethnic disparities. The objective of the study is to compile the existing literature to determine whether there are ethnic or racial disparities in the progression of MS.
Methods Used: PubMed and Google Scholar were used to conduct the systematic literature review using keywords: “Multiple Sclerosis”, “disability”, “progression”, “minority”, “racial”, “ethnic”, and “outcome”. We included studies done in the US and published after 2010 that evaluated disease progression of MS based on disability and/or cognition and included comparisons of different races/ethnicities. Studies that only measured difference in diagnosis or mortality only were excluded.
Summary of Results: A total of six studies satisfied our inclusion criteria (see table below). Most studies showed a significantly worse MS disability progression, outcomes, and self-rated health in African-American and Hispanic patients compared to their White counterparts. Follow-up period was variable and ranged from 1-10 years. In general, the severity at the initial presentation was an important factor but minority populations tended to reach advanced disability stages faster compared to non-minority patients. Some limitations of the studies included small sample size, possible sampling bias, and possible error in race/ethnicity classification. Additionally, there were inconsistencies in adjusting for all the variables that could play a role in disparities among the studies. For example, most of the studies did not consider, genetics, the time to initial diagnosis, or other co-morbidities that could contribute to disease progression and disability. Finally, a causal relationship could not be assessed because all studies were observational, retrospective, or cohort studies.
Conclusions: Our literature review shows that, compared to non-Hispanic Whites, African-American, and Hispanic/Latino patients with multiple sclerosis are at higher risk of disease progression and moderate to severe disability even after accounting for some of the other confounding variables. Larger prospective studies that consider social determinants of health, co-morbidities, genetics, access to medication, as well as symptoms at the time of initial diagnosis are warranted.
Ethnic and racial disparities in progression of multiple sclerosis: literture review table.
Author & year published
Type of Study (survey, prospective, cohort, retrospective, etc)
Number of patients in each group
Definition of outcome
Comparison of outcome (percentages) based on management of different ethnicities/groups
Summary of findings
Other factors taken into account that contribute to worsening
Pérez et al., 2021
Retrospective cohort study, Review of medical records
N total= 300, African Americans (N)=100 Whites (N)=100 Hispanics (N)=100
Survival Time Ratio (STR) or time to ambulatory disabilty
STR, Hispanic vs. White=0.17 (0.08–0.36), p=0.004 STR, African American vs. White=0.14 (0.05–0.27), p=0.002 STR, African Americans vs. Hispanic 0.92 (0.89–1.08), p=0.93
After adjustment for baseline characteristics, Hispanic and African American patients had higher overall ambulatory disability 5 years from diagnosis
Clinical characteristics at baseline, gender, age, income, and insurance
Gray-Roncal et al., 2021
Observational comparative, cross-sectional study
N total = 8,744, African Americans N = 1,214, Whites N = 7,530
Cognitive performance, walking and manual dexterity speed
African American vs. Whites Cognitive performance, -5.06 (-5.72 to -4.41), p<0.001
African Americans performed more poorly on cognition tests and had higher disability scores, walking and manual dexterity
Type of MS, age, gender, duration of symptoms, employment, and education level
Perez et al., 2020
Retrospective cohort study
N total = 188, Hispanics N=94, Whites N=94
Disability patterns of brain MRI, and its correlation to disability progression on the Expanded Disability
Status Scale (EDSS) scores and ambulatory assistance
Hispanics vs. Whites, Hispanic EDSS interquartile range [IQR] = 2.0; (1.0-3.5)
Caucasians median [IQR] =1.0 (0.0-2.0)), Hispanics had higher risk for ambulatory assistant (hazard ratio [HR] = 9.7; 95%
confidence interval [CI], (2.8-32.5)). Thalamic volume and correlation to EDSS scores (rs = −.42, P
Hispanic patients had a higher baseline median EDSS score, higher risk for ambulatory assistance with an association with disability to their measured MRI thalamic volume
Age, gender, insurance, disease phenotype, EDSS score at diagnosis, smoking status, comorbidities (Hypertension, Hyperlipidemia, Diabetes mellitus, Malignancy), BMI, and Vitamin D level
Petracca et al., 2022
Cross-sectional study
N total = 202 African Americans N= 103, Whites N=99
Expanded Disability Status Scale (EDSS), mobility and leg function (Timed 25 Foot Walk Test-T25FWT), finger
dexterity (9-Hole Peg Test-9HPT), cognitive efficiency and speed performance (Symbol Digit Modalities TestSDMT)
African Americans vs White, In 9HPT scores: African American coeff. 5.52, 95% (3.55 to 7.48) White coeff. 3.24, 95% (1.55, 4.92). In SDMT scores, African American coeff. -7.99, 95% (-11.58 to -4.38) va White coeff. -5.87, 95% (8.86 to -2.87)
African-American vs White, African American MS patients showed significantly worse manual dexterity and cognition than their white counterparts, with African Americans having lower SDMT and 9HPT scores
Age, gender, total income, total years of education, BMI, and comorbidities
Self-rated health (SRH), Patient-Determined Disability Steps (PDDS) to rate disability and SymptoMScreen (SyMS), a
validated battery for assessing symptom severity in 12 domains
African Americans vs Hispanic vs White, Mean PDDS for African Americans and Hispanics were higher than Whites (p < 0.0001). SyMS scores were higher in African Americans and Hispanics compared to Whites (p < 0.0001)
African American and Hispanic patients had higher mean PDSS scores, significantly worse SyMS scores than whites in walking, dexterity, spasticity, pain, sensory, bladder function, fatigue, vision, dizziness, cognition, depression, and anxiety
Age, gender, and MS subtype
Kister et al., 2018
Observational retrospective cohort study
N total= 1740, Whites N=1046, African Americans N=346, Hispanics N=219, Other N=129
Disability was assessed via Patient Determined Disease Steps (PDDS) and yielded a rank on the Patient-derived Multiple Sclerosis Severity Score (PMSSS)
The single most important predictor of final PMSSS in this study was the initial PMSSS (p
African-Americans had the highest initial baseline severity scores, followed by Hispanics but after multivariate analysis, race/ethnicity did not affect final severity score
Initial disease duration, Initial PDDS, Ambulatory assist, and Initial PMSSS
Elevated Alanine on Magnetic Resonance Spectroscopy is associated with death in pediatric patients with hypoxic ischemic injury
Cole C, Dopp M, Bartnik-Olsen B, Kim P. Loma Linda University, Loma Linda, CA
Purpose of Study: Magnetic Resonance Spectroscopy (MRS) is an important imaging adjunct for the diagnosis of hypoxic ischemic injury. As the concentration of adenosine triphosphate is depleted, the cell switches from oxidative phosphorylation to anaerobic glycolysis. The byproduct of this metabolic pathway is the creation of lactate from pyruvate. This leads to lactic acidosis, which can be detected with MRS. The presence of a lactate peak on MRS is not specific to the degree of hypoxic injury. In hypoxic conditions, other metabolites are detectable by MRS such as Alanine (Ala). Ala is a product of the glucose-alanine cycle, where pyruvate is converted to Ala. We hypothesize that the elevated level of Ala is seen in severe hypoxia and may be a more specific marker for poor outcomes/death.
Methods Used: We retrospectively reviewed pediatric patients with the diagnosis of hypoxic ischemic brain injury from 2019 to 2023. Inclusion criteria were age 0-18years, hypoxic ischemic brain injury, and MRS. The exclusion criteria was neonatal hypoxic ischemic brain injury. Clinical values were obtained including age, gender, mechanism of injury, and Glasgow Coma Score. The Ala value on MRS was also recorded. The correlation of elevated Ala metabolite of > 2 mol/L and poor outcomes (death) was studied using odds ratio, statical significant (p < 0.05).
Summary of Results: Our study included 31 patients with ages of 1-month to 14 years. There were 18 males and 13 females. Patients with a diagnosis of hypoxic ischemic injury and elevated Ala concentration of >2 mol/L are 9.5 times more likely to die (95% CI 1.4, 64.3).
Conclusions: There is a statistically significant increased concentration of alanine in patients with a diagnosis of hypoxic ischemic brain injury and poor outcomes/death. This study was an appropriate first step in confirming the presence and specificity of an alanine peak in this patient population. This pilot study gives us enough data to move forward with a larger goal: stratifying the severity of HIE based on Alanine concentration.
# 138
RESTORING CORNEAL SENSATION IN CHILDREN WITH NEUROTROPHIC KERATOPATHY: A SYSTEMATIC REVIEW
Cardey R1, Yin V1, 2, Courtemanche R1, 2, Tuen Y1, 2, Shayan S1, 2, Kwan-Wong T1, 2. 1University of British Columbia, Vancouver, BC, Canada and 2BC Children’s Hospital, Vancouver, BC, Canada
Purpose of Study: Neurotrophic Keratopathy (NK) is a rare degenerative eye disease characterized by loss of sensation to the cornea as a result of congenital or acquired dysfunction of the afferent nerves. This study aims to summarize the evidence regarding treatment options for pediatric patients with NK. This may assist in providing information on the efficacy of current and novel treatments used for pediatric NK to help in clinical decision making.
Methods Used: A systematic review of the literature was conducted to identify studies relating to the treatment of pediatric NK. Six databases were searched with the assistance of a medical librarian using a variety of relevant MeSH terms. Studies identified in this search were subsequently screened for inclusion by two reviewers. Data was collected including patient demographics, etiology, pre / post treatment corneal sensation, treatments received, surface pathology, and visual acuity.
Summary of Results: 44 total studies were eligible for inclusion in the systematic review (40 case studies, 1 retrospective review, 1 retrospective interventional case series, 1 cohort study and 1 abstract). In total, data was available for 80 pediatric patients (totalling 95 eyes) affected by NK. Pre-treatment corneal sensation was measured in 71 participants, with 44 demonstrating absent sensation and 27 demonstrating reduced sensation. Cochet-Bonnet aesthesiometry (CBA) was used to measure pre-treatment corneal sensation in 32 participants with an average of 4.1 mm. Post-treatment corneal sensation was measured in 46 participants, 43 of which had sensation present and 3 had sensation absent. CBA was measured in 29 patients post-treatment and averaged 39.1 mm, representing a significant improvement in corneal sensation. Surface pathology improvement was seen in 55 participants following treatment while 2 had no visible improvement.
Corneal neurotization (CN) was the treatment most frequently reported in the literature, followed by medicated eye drops. The majority of patients who received CN had absent corneal sensation pre-treatment and present sensation post-treatment. Where reported, improvement in surface pathology was observed in patients who underwent CN.
Conclusions: Overall, the literature suggests that pediatric NK responds well to a variety of treatments. Newer treatment options such as CN may demonstrate utility as a treatment option for cases refractory to medical therapy or more traditional surgical treatments.
This review identifies significant heterogeneity in the measurement and reporting of pre- and post-treatment outcomes in pediatric NK. The literature is also heavily skewed towards individual case reports, with a relative absence of higher levels of evidence supporting different modalities of treatment in NK. This suggests that additional work should be done to create more uniformity in outcome measure and reporting in pediatric NK, as well as the need for high-level studies comparing the effectiveness and indications of different treatment modalities.
# 139
Effects of Cardiac Arrhythmias on The Mortality and Morbidity in Pediatric Patients with Seizure Disorders
Cong CY, Ghimire L, El Rahi H, Torabyan Z. UCSF Fresno, Fresno, CA
Purpose of Study: Seizures, which are caused by abnormal electrical activities in the brain, can lead to significant brain damage and even death in children, especially when they are long-lasting or recurrent. Cardiac arrhythmias have a similar mechanism of action as they are also secondary to irregular electrical activities. Arrhythmias are a recognized cause of sudden unexpected death in epilepsy (SUDEP), which is an unexpected death in otherwise healthy patients with epilepsy. However, the relationship between cardiac arrhythmias and seizures in pediatric patients is not well established, and there is limited information about the burden of arrhythmias in seizure disorders. This study aims to determine whether cardiac arrhythmias increase the mortality and morbidity of children with seizure disorders.
Methods Used: We used the nationally representative dataset National Inpatient Sample(NIS) from the years 2016 to 2020. We included patients <21 years of age admitted with seizure disorders and excluded those transferred in and out of the hospital. We used a logistic regression model to calculate the mortality in children with tachyarrhythmias in those with underlying seizure disorders. The data is further stratified by patients’ age, gender, and median household income for the patients’ ZIP Code as well as the regions, urban/rural locations, teaching status, ownership, and bedsize of the hospital.
Summary of Results: Out of 28,816,668 admitted children, excluding those transferred in and out of the hospital, 820,975 had seizure disorders, of which 12,030 had tachyarrhythmias. Of the children with seizure disorders, 11.5%(n=94,400) had central nervous system disorders, 5.8%(n=47,240) had congenital heart disease, and 5.9%(n=48,155) had genetic anomalies (Table 1). In-hospital mortality was 1.6%. The rate of mortality was much higher in children with seizures with concomitant arrhythmias vs. those without arrhythmias, 8.8%(n=12,030) vs. 1.5%(n=12320), P<0.001. The length of stay was longer in the children with seizures with coexisting arrhythmias vs. those without arrhythmias, 5 (IQR 2-12) vs. 3 (IQR 1-5), P<0.001. In the logistic regression model, even after adjusting for confounding factors, the presence of tachyarrhythmias in seizure disorders was associated with significantly higher mortality risks, aOR=2.60 (CI 2.20-3.07), P<0.001. In this model, younger age, aOR=0.95 (Cl 0.947-0.96), P<0.001, and the presence of congenital heart disease, aOR=1.78 (Cl 1.60-1.97), P<0.001, were associated with worse outcomes.
Conclusions: Children with seizure disorders with concomitant cardiac arrhythmias have higher in-hospital mortality rates and increased morbidities such as prolonged hospitalization.
Variables
Presence of tachyarrhythmia
P-value
No
Yes
Total numbers
809,165
12,030
In-hospital mortality (%)
12,320 (1.5)
1,055 (8.8)
<0.001
LOS (median (IQR))
3 (1-5)
5 (2-15)
<0.001
Congenital heart disease (%)
44,800 (5.5)
2,440 (20.3)
<0.001
Central nervous system disorders (%)
93,315 (11.5)
1,085 (9.0)
<0.001
Genetic anomalies (%)
47,290 (5.8)
865 (7.2)
0.008
Heart block (%)
7,055 (0.9)
1,385 (11.5)
<0.001
Female (%)
378,375 (46.8)
5,495 (45.7)
0.312
Median household income for patient
0-25th percentile
244,745 (30.7)
3,540 (29.8)
0.808
26th to 50th percentile
20,6355 (25.8)
3,095 (26.0)
51st to 75th percentile
186,325 (23.3)
2,855 (24.0)
76th to 100th percentile
160,865 (20.2)
2,405 (20.2)
Year (%)
2016
164,135 (20.3)
2,270 (18.9)
0.009
2017
169,395 (20.9)
2,360 (19.6)
2018
170,245 (21.0)
2,585 (21.5)
2019
169,445 (20.9)
2,405 (20.0)
2020
135,945 (16.8)
2,410 (20.0)
Bed size of hospital (%)
Small
144,230 (17.8)
1,975 (16.4)
0.033
Medium
186,267 (23.0)
3,085 (25.6)
Large
478,665 (59.2)
6,970 (57.9)
Location/teaching status of hospital (%)
Rural
15,990 (2.0)
160 (1.3)
0.084
Urban non-teaching
44,995 (5.6)
625 (5.2)
Urban teaching
748,180 (92.5)
11,245 (93.5)
LOS=length of stay.
# 140
A review on the diabetic lumbrosacral plexopathy based on a 50 year old patient, a case report
Dao KT1, Johar L1, Abraham J1, Aranguri C1, Clarke M1, Veedu HK2, Ly B2. 1Kern Medical Center, Bakersfield, CA and 2Kern Medical Center, Bakersfield, CA
Case Report: Diabetic lumbosacral radiculoplexus neuropathy (DLSRPN) is a rare disease of exclusion that is difficult to diagnose due to its non-specific clinical presentation of neuropathy, autonomic symptoms, and possible weight loss. Due to this, many differential diagnoses are raised before making a diagnosis of such an uncommon disease. However, once the diagnosis is made, the management of this disease can vary quite heavily. Here, we would like to discuss the etiology, pathophysiology, diagnosis, and management of this disease as well as present a rare case of diabetic lumbosacral radiculoplexus neuropathy in a 50-year-old male.
Patients bilateral lower extremities on admission
# 141
Validation of Calpain-2-Mediated Truncation Sites in Human PTPN13
Pogue A1, Su W3, Penna E3, Reece T3, Braga M3, Berndt HN1, Bi X1, Baudry M2. 1Western University of Health Sciences, Pomona, CA; 2Western University of Health Sciences, Pomona, CA and 3Western University of Health Sciences, Pomona, CA
Purpose of Study: In the US, traumatic brain injury (TBI) and the resulting neurodegenerative effect on patients have become a serious public health concern. Recent studies have shown the calcium-dependent protease, calpain-2, plays a significant role in the long-term damage to neurons after TBI. When activated, calpain-2 cleaves a number of proteins, including the tyrosine phosphatase, PTPN13. This cleavage produces a fragment known as P13BP, which has been proposed to represent a novel blood biomarker for TBI. In order to use this biomarker for determining both the progression of the disease and the efficacy of future treatments, the cutting site(s) of PTPN13 by calpain-2 must first be identified.
Methods Used: A previous proteomic study suggested the existence of two cutting sites at amino acids 366-367 and amino acids 1517-1518. Two peptides with sequences overlapping these potential truncation sites were used as potential decoys to validate these cutting sites. Both cell lysates from HEK cells lacking calpain-1 and brain homogenates were incubated in the absence or presence of human calpain-2 and calcium, as well as the peptides alone or in combination. Western blots were then performed with an antibody against the N-terminal domain of PTPN13.
Summary of Results: Although results with the HEK cell lysates were not reproducible, they did show that both peptides reduced the formation of the truncation fragment with a molecular weight (MW) of 130 kDa. This suggests that calpain-2 may cut PTPN13 at both amino acids 366-367 and 1517-1518 to generate this fragment. Results with brain homogenates showed some evidence of reduced truncation of PTPN13 when the peptides were present, although this result was less specific due to the high level of cutting by calcium under the experimental conditions.
Conclusions: In order to validate these results, more experiments will be performed before an antibody specifically recognizing the C- or N-terminals of P13BP is prepared.
# 142
UNCOVERING THE REAL NON-PSYCHIATRIC DIAGNOSIS: A RARE NEUROLOGICAL DISORDER
Zahid A, Thukral J, Kaur H, Patel AA, Dargan KK, Hernandez EW, Lim AM, Oberndorf JK, Hambartzhumian R, Macwan S, Robinson J. Eisenhower Medical Center, Palm Desert, CA
Case Report: A 34-year-old woman presented with 4 months of progressive difficulty walking and falls. She had some vertiginous dizziness for 2 weeks, lower back pain, occasional urinary incontinence, numbness and tingling in extremities. Within 2 months, she started using a walker. She had no family history of movement disorders, demyelinating diseases, or autoimmune diseases. She never smoked or had alcohol. Initial exam showed power 4/5 with spasticity in lower extremities, reflexes 2+ in upper extremities, 3+ in lower extremities; plantar reflexes were equivocal bilaterally; coordination exam was normal in upper extremities, but there was difficulty with heel-shin testing and gait exam revealed difficulty standing up from the chair.
Investigations, management: MRI brain, C-spine and T-spine MRI with contrast showed no signs of demyelinating disorder. There was mild non-specific degenerative joint disease. Nerve conduction studies and electromyography were normal. The patient went to a psychiatrist and was diagnosed with somatic symptom disorder, bipolar affective disorder, and anxiety, and started on alprazolam. Treatment continued for 4 years, during which she saw multiple neurologists. She re-presented to a fourth neurologist with ongoing walking difficulties and falls; Stiff-Person Syndrome was suspected.
Additional tests, including antinuclear antibody screen, rheumatoid factor, C3/C4 complement antigen, creatine kinase, multiple sclerosis kappa free light chain (serum, CSF), venereal disease laboratory syphilis test (CSF), paraneoplastic antibodies in CSF (ampiphysin, AGNA-1, ANNA-1, ANNA-2, ANNA-3, CRMP-5-IgG, PCA-Tr, PCA-1, PCA-2) were negative. Lumbar puncture showed normal CSF cell count, unremarkable CSF IgG at 2.2 mg/dL (normal: 0.8-7.7mg/dL) and elevated CSF GAD-65 antibody at 0.88 nmol/L (normal range <= 0.02nmol/L).
Thus, after 5 years, the patient was diagnosed with Stiff-Person Syndrome.
She was started on clonazepam 1.5 mg three times daily and baclofen 10 mg twice daily. Steroid therapy and IVIG were later added. 9 months after diagnosis, rituximab 1000 mg every 2 weeks, was added. Overall, since her diagnosis of Stiff-Person Syndrome, she has had major symptom improvement and is able to walk longer distances.
Discussion: Neurological assessment and disorders are complex, with a wide range of differentials. Due to the subjective nature of history and exams, some patients may be misdiagnosed with a psychiatric disorder. Such patients should be re-evaluated, and other somewhat common neurological disorders should be ruled out, e.g. multiple sclerosis. More advanced work-up with specialized CSF biomarkers may be required such as in our patient - lumbar puncture and CSF analysis finally showed elevated GAD-65 antibody levels. Ultimately, somatic symptom disorder/functional psychiatric illnesses should be a diagnosis of exclusion; one must always have even a remote suspicion for rare disorders like Stiff-Person Syndrome.
# 143
UNCOVERING DRY BERI BERI IN A PATIENT WITH CATATONIA
Davtyan E, Sharma R, Fox K. Kern Medical, Bakersfield, CA
Case Report
Purpose: Dry Beri-Beri involves severely decreased thiamine levels and can lead to issues affecting the central and peripheral nervous systems. Catatonia is a neuropsychiatric syndrome characterized by motor and behavioral abnormalities, such as immobility, stupor and mutism. There can be diagnostic confusion when uncovering a neuromuscular condition such as Dry Beri-Beri in the setting of a patient with catatonia.
Methods: A retrospective review following IRB approval
Summary of Results: A 43-year-old woman with medical history of schizoaffective disorder and methamphetamine use presented to the emergency department from a local community behavioral health hospital due to poor oral intake for two days and severe catatonia. On arrival, the patient was mute, stuporous, immobile, and resistant to instructions, meeting DSM-5 criteria of catatonia. Initial labs were unremarkable. Extensive imaging was all of which were unremarkable. LP demonstrated elevated protein of 110 and normal white blood cell count suggesting diagnosis of Guillain-Barre. Patient received IVIG x5 days with no resolution of symptoms. Nerve conduction study was then conducted which demonstrated normal F waves, making Guillain-Barre less likely. Nerve conduction was also significant for diffuse sensory neuropathy, severe in lower limbs and moderate in upper limbs and moderate bilateral tibial motor axonal and mild bilateral peroneal motor demyelinating neuropathy. Thiamine level resulted <7. At this time 2nd look of the initial MRI brain was requested and clinical case debriefed; MRI findings of FLAIR bilateral thalami hyperintensities and overall clinical findings supported our hypothesis of Dry beri-beri. Patient was subsequently initiated on thiamine therapy. At present, patient continues to work with physical therapy with improvement noted in motor strength of lower extremities bilaterally.
Conclusion: Thiamine deficiency leads to beriberi, further classified as dry or wet beriberi. Dry Beri-Beri is characterized by sensory and motor neuropathy with the duration and magnitude of the thiamine deficiency correlating to the severity of its presentation. The presenting symptoms of both Dry Beri-Beri and Catatonia are so similar making it difficult in distinguishing the diagnosis between the two. In our case, patient initially presented with signs and symptoms of severe catatonia leading to extensive workup including LP which was initially misleading for GBS due to elevated protein levels in the CSF. Patient was initiated on IVIG, however given no improvement in patient’s clinical status, further studies were warranted including pending thiamine levels (which resulted severely low) and nerve conduction studies going against GBS and favoring the diagnosis of Dry beri-beri. This particular case of Dry Beri-Beri is remarkable as the patient presented with catatonia obscuring the patient’s significant neuromuscular deficits and ultimately delaying appropriate treatment.
Pulmonary and Critical Care I
Concurrent Session
3:15 PM
Thursday, January 18, 2024
# 144
COMPLEMENT CONTRIBUTES TO HYPOXIA-INDUCED PLATELET ACTIVATION AND PULMONARY HYPERTENSION
Posey JN1, Jordan M1, Nozik E3, 2, Delaney C1, 2. 1University of Colorado, Anschutz Medical Campus, Aurora, CO; 2Children’s Hospital Colorado, Aurora, CO and 3University of Colorado, Anschutz Medical Campus, Aurora, CO
Purpose of Study: Pulmonary hypertension (PH) is a progressive vasculopathic disease driven by inflammation. Platelets are increasingly recognized as immune cells that contribute to both local and systemic inflammation. Platelets are activated, and platelet-derived proteins are increased in the circulation of patients with PH and in experimental models of PH. Similarly, complement protein deposition is increased in the lungs of hypoxic animals and patients with end-stage PH. Disorders of complement hyperactivation result in uncontrolled platelet activation. We hypothesized that complement promotes hypoxia-induced platelet activation and hypoxic PH.
Methods Used: 7–8-week-old C57BL/6 and global C3 -/- mice were exposed to 10% hypobaric hypoxia for 3 or 21 days or remained in normoxia. Whole blood was collected via RV cardiac puncture. Whole blood was used to measure platelet-leukocyte aggregation by flow cytometry. Whole blood was processed to obtain isolated platelets for flow cytometry or platelet-poor plasma for ELISA. Flow cytometry was used to measure surface markers of platelet activation and complement protein expression. RVSPs were obtained by closed-chest RV puncture. Hearts were dissected to determine RV hypertrophy (Fulton’s index=RV/LV+S).
Summary of Results: Following 3 days of hypoxia, plasma C3a is increased and platelets are activated, demonstrated by an increase in platelet P-selectin, plasma PF4, activation of transmembrane integrin a2BB3, and increased platelet-leukocyte aggregation. Platelet expression of the central complement pathway proteins C3 and C3d, the classical complement pathway protein C1q, and the negative regulatory complement protein DAF (CD55) are increased in hypoxic WT mice. Platelet complement anaphylatoxin receptor C3aR and C5aR expression is increased in hypoxic WT mice. Ex vivo stimulation of platelets with the complement anaphylatoxins C3a and C5a resulted in a dose dependent increase in platelet activation, evidenced by increased P-selectin expression. C3 -/- mice were protected from hypoxia-induced platelet activation, demonstrated by prevention of platelet P-selectin and a2BB3 activation in C3 -/- vs. WT -/- mice. Hypoxia-induced increase in RVSP and RV hypertrophy were attenuated in C3 -/- vs. WT controls following 21 days of hypoxia.
Conclusions: Overall, our findings show that platelets and complement are activated following acute, 3-day hypoxia exposure and complement anaphylatoxins C3a and C5a directly activate platelets. Mice lacking C3 were protected from hypoxia-induced platelet activation and hypoxic PH. We demonstrate that one of the mechanisms by which platelets are activated by hypoxia involves complement-mediated platelet activation. Our findings provide evidence that platelet-complement interaction plays a role in the peak inflammatory stage of hypoxic PH and that the complement system plays a role in the development of hypoxic PH. Future studies will examine the mechanisms by which platelet-complement crosstalk contributes to the pathogenesis of PH.
# 145
EFFECTS OF COUGH SUPPRESSION THERAPY IN PATIENTS WITH CONCURRENT CHRONIC REFRACTORY COUGH AND OROPHARYNGEAL DYSPHAGIA
Chen SA1, Kim JF1, Krishna P2, Crawley B2, Murry T2. 1Loma Linda University, Loma Linda, CA and 2Loma Linda Health, Loma Linda, CA
Purpose of Study: Chronic refractory cough (CRC), a cough lasting longer than 6 months despite medical intervention, occurs in 9-30% of the population. Dysphagia (DYS) is found in up to 67-88% of patients with CRC, thus failure to treat CRC can increase risk for malnutrition and aspiration. Previous research has shown that cough suppression therapy (CST) is a promising treatment for CRC. However, little is known about effects of CST in CRC patients with comorbid oropharyngeal DYS – swallowing problems in the mouth or throat. The purpose of this study is to assess if CST contributes to improved self-assessment of DYS in patients with oropharyngeal DYS and CRC.
Methods Used: The charts of 106 patients referred to the Loma Linda Voice and Swallowing Center with a primary diagnosis of CRC were reviewed. Inclusion criteria included patients unresponsive to standard medical treatment, past participation in CST without DYS-specific treatment, diagnosis of oropharyngeal DYS, an onset of CRC prior to or along with DYS, and valid pre- and post-treatment self-assessment scores of the Cough Suppression Index (CSI) and Eating Assessment Tool-10 (EAT-10). Patients 18 years or younger, with central nervous system disturbances, or with a history of head or neck surgery during the study period were excluded. Two groups matched for age and gender were created: 15 with CRC+DYS and 15 with CRC only. Statistical analyses were conducted to compare pre- and post-treatment symptom severity, treatment quantity, demographics, and comorbidities.
Summary of Results: CST was effective in reducing the self-reported severity of DYS (p=0.0001) in CRC patients with comorbid oropharyngeal DYS. figure 1 summarizes the findings. Both the CRC+DYS and CRC only group reported significant reductions in cough severity (p=0.005, 0.001). EAT-10 scores decreased in all CRC+DYS patients, and their post-treatment EAT-10 average was similar to that of patients without DYS. Both groups had comparable pre-treatment cough severity, treatment quantity, comorbidities, age, and gender. Following CST, there was no significant difference in mean CSI and EAT-10 scores between groups (p=0.68, 0.05).
Conclusions: This is the first study to examine the effectiveness of CST in patients with concurrent CRC and oropharyngeal DYS. Our findings suggest that these conditions share an overlapping neurophysiological pathway. Strengthening the muscles in this pathway using CST improves both cough and swallowing. CST is thus supported as a treatment option for patients with CRC and oropharyngeal DYS to address the two simultaneously. Future studies could expand to a larger matched group and patients with CNS and other DYS disorders.
TB or not TB: A Rare Presentation of Hydropneumothorax Secondary to Coccidioidomycosis
Espinoza VE2, Mishra S1, Fox K2. 1Kern Medical, Bakersfield, CA and 2Kern Medical, Bakersfield, CA
Case Report: The patient is a 47-year-old homeless female with poorly controlled diabetes and a social history significant for tobacco use and methamphetamine use. The patient presented with a chief complaint of perianal pain. Physical exam was significant for perianal fluctuance with noted tenderness. In the emergency department, incision and drainage was performed with the evacuation of purulent discharge. A computed tomography (CT) scan abdomen and pelvis showed a perianal fluid collection concerning for abscess measuring 3.7 x 3.2 x 3.5 cm. CT also incidentally showed a large loculated left hydropneumothorax with segmental left lower lobe airspace disease, scarring, and left lower lobe bronchiectasis. The patient was admitted to Internal Medicine for intravenous antibiotics for treatment of the perianal abscess with noted improvement. Given the incidental pulmonary findings seen on CT abdomen and pelvis, a CT chest was ordered which showed a large left lung cavitary lesion along with multiple additional cavitary lesions within the right upper lobe with scattered micronodular densities also present. The patient continued to be clinically stable with normal vitals on room air and elicited no respiratory complaints. She denied a history of tuberculosis or coccidioidomycosis. She also denied subjective fever, rigors, pleuritic chest pain, cough, hemoptysis, and unintentional weight loss. A review of records showed prior imaging during hospitalization for trauma-related injuries in 2020. At that time, CT chest showed a 6.5 mm noncalcified nodule in the right upper lobe with minimal surrounding airspace opacity, and a 12 mm cavitating nodule in the left lower lobe posteriorly. There is no demonstrable pleural effusion or significant adenopathy.
Evaluation for tuberculosis, which included QuantiFERON and three acid-fast bacteria smears, was negative. Further evaluation of (1-3) B-D Glucan Assay was negative. Sputum culture grew rare fungus resembling Coccidioides species. Coccidioides serology was significant for positive IgG and IgM with complement fixation titers of 1:8. While the patient was clinically stable, given the progressive changes seen on lung imaging, a multidisciplinary approach was initiated with Pulmonology, Infectious Disease, and Cardiothoracic Surgery. Ultimately thoracentesis and surgical interventions were deemed unsafe given the risk of bronchopleural fistula and possible permanent air leak. The patient remained clinically stable without respiratory complaints. She was started on fluconazole 400 mg daily and scheduled with Infectious Disease for further outpatient management.
This case demonstrates the rare occurrence of hydropneumothorax secondary to coccidioidomycosis.
# 147
Analysis of Respiratory Injuries in California firefighters, 2000-2020
Murray M, Blanc P, Harrison R, Gandhi SA. UCSF, San Francisco, CA
Purpose of Study: Firefighting in California (CA) is a hazardous occupation with exposure to fine particulates (PM2.5). Excessive lung function decline in firefighters has been associated with cumulative exposure to PM2.5 over an occupational lifetime. Compared to the general population, firefighters have higher rates of COPD and asthma.
Since 2000 the number of CA wildfires has increased and is considered a manifestation of climate change. Firefighters are frequently exposed to the wildland-urban interface, resulting in a cumulative higher level of exposure to PM2.5. Respiratory protection for wildland firefighting is considered impractical due to its physically demanding nature. As wildland fires rise in CA, firefighters will continue to be exposed to higher levels PM2.5.
The objective of this study is to analyze the respiratory injuries in CA firefighter worker’s compensation claims (WCC) in efforts to understand the impact of climate change from 2000 to 2020. The hypothesis is the number of respiratory injuries in CA firefighter WCC has increased from 2000 to 2020 due to the rise in wildland fires.
Methods Used: We identified respiratory WCC by firefighters from 2000-2020 in the CA Workers’ Compensation Information System (WCIS) using International Classification of Diseases Ninth and Tenth Revision codes, WCIS recorded respiratory nature and cause of injury codes, and respiratory keywords in the injury description. All claims with date of injury from January 1, 2000 – December 31, 2020, meeting these criteria were extracted from WCIS in August, 2023. We calculated respiratory injury rates by sex, age group, county and date of injury compared to the total injuries using descriptive and relative statistics. A chi-square test was performed comparing the number of respiratory cases in Inland Northern, Coastal, and Southern regions in 2000-2009 vs 2010-2020.
Summary of Results: We identified 3,771 respiratory cases during 2000-2020. Male workers (3557) had a higher number of respiratory injuries than women (191). The Los Angeles region had the highest number of respiratory injuries (889), followed by the San Francisco Bay Area (775). The total number of respiratory claims decreased from 2010-2020 compared to 2000-2009. The geographic distribution, however, shifted toward inland northern California (p<0.01).
Conclusions: The Southern CA region had the highest number of respiratory claims. Our analysis demonstrated no temporal trend in respiratory injuries from 2000-2020. The rise in respiratory claims in the inland northern CA region may reflect the growing number of wildfires in that region in 2010-2020. This ongoing project will focus on the temporal and geographic trends of respiratory WCC in firefighters with the aim of identifying clusters that could reflect potential occupational exposures.
# 148
From Disgust to Discovery: A Rare Case of Oropharyngeal Myiasis in a Californian ICU
Uddin S1, Ghadiya K1, 2, Abraham J1, Espinoza VE1, Garcia-Pacheco I1. 1Kern Medical Center, Bakersfield, CA and 2Ross University School of Medicine, Saint Michael, Barbados
Introduction: Myiasis is a condition describing the infestation of fly larvae in human tissues. Cases typically occur in poor socioeconomic and tropical regions of the world. Myiasis rarely presents in the first world, even rarer for an infestation to present in a patient’s Nasopharynx. This report describes a case of nasopharyngeal myiasis in an elderly male admitted to a California intensive care unit after Cardiac Arrest.
Case Report: A 70-year-old male with a prior medical history of coronary artery disease status post Coronary Artery Bypass Graft surgery five years ago, past CVA with residual bilateral blindness, Diabetes Mellitus, hypothyroidism, and Adrenal Insufficiency presented for ICU admission after Cardiac Arrest at his place of residence. The patient was eating dinner at home when his caretaker noticed he turned pale and apneic, eventually falling over and becoming unresponsive. CPR was performed by EMS for 20 minutes and a return of spontaneous circulation (ROSC) was achieved. Upon arrival at the Emergency Department, the patient fell into cardiac arrest; ROSC came after four rounds of CPR. The patient underwent intubation with 20 mL of food suctioned from his oral cavity. Admission evaluation with Chest X-ray revealed aspiration findings in the Right Lower Lobe. Nasogastric and Orogastric tubes couldn’t be passed into the Stomach during the ICU stay, X-rays revealed coiling in the distal Esophagus with possible food bolus obstruction. He remained comatose with a Glasgow Coma Scale of 3 without chemical sedation during the hospitalization. An early electroencephalogram was done and revealed evidence of post-anoxic myoclonus. On day three of hospitalization, while assessing the gag reflex, copious insect larvae crawled out of his nares and oral cavity. Persistent suctioning proved futile as Larva continued to exit his orifices. Larvae samples sent for laboratory speciation revealed Blow Fly larvae (Calliphoridae family). The following day the patient had a positive apnea test with absent brainstem reflexes, and brain death was diagnosed. The patient’s family was informed and after agreement to proceed with terminal extubation, the patient expired within 2 hours.
Discussion/ Conclusion: Myiasis is a rarity in the developed world, usually coinciding with soft tissue or wound infections. This case details an atypical presentation of Larval infestation in a patient’s nasopharynx, a body cavity known for its mucociliary elevator, an innate human function to eliminate foreign pathogens from the airway. Further efforts into ICU hygiene, including insect extermination, should be performed to prevent this disturbing pathology.
# 149
HYPEROXIA SURVIVAL IDENTIFIES NOVEL LONG-LIVED, OBESITY, FATTY LIVER DISEASE, AND DIABETES-RESISTANT RAT STRAIN
Allen AG1, Long Z1, 3, Santoso S1, 2, Post MD1, Smith EE1, Wilson PV1, Repine JE1. 1University of Colorado Anschutz Medical Campus, Aurora, CO; 2University of Notre Dame, South Bend, IN and 3Northwestern University, Evanston, IL
Purpose of Study: Achieving healthy longevity that encompasses the TRIAD of longer lifespan, reduced disease, and increased biological function is the “holy grail” of biomedical research. For unknown reasons, life expectancy is declining, aging-related diseases (such as obesity, fatty liver disease, type-2 diabetes) are increasing, and aging-related dysfunction is escalating. These trends are occurring in both the United States and worldwide. While investigating the pathogenesis of pure (100%) oxygen-(“hyperoxia”)-induced acute lung injury (a.k.a., acute respiratory distress syndrome, ARDS), we serendipitously discovered a unique strain of “resistant” rats with prolonged survival and less lung inflammation and oxidative stress following hyperoxia exposure. Because of resistant rats’ reduced inflammation and oxidative stress responses, we next evaluated their longevity, weight gain, fatty liver disease, and stress hyperglycemia (“prediabetes”) responses linked to increases in inflammation and oxidative stress.
Methods Used: Longevity (average survival days), weight gain (g), abdominal girth (cm), fatty liver disease (Oil Red O staining), and stress hyperglycemia (blood glucose levels {mg/dL} following IL-1/LPS insufflation) were measured in matched cohorts of young (3-4-month-old) and old (12-18-month-old) male Sprague-Dawley resistant and control rats.
Summary of Results: Hyperoxia-resistant male rats have longer lifespans, gain less weight, have smaller abdominal girths, less fatty liver disease, and decreased stress hyperglycemia than male control rats. Differences between the two groups become more pronounced during aging. Consistent with their reduced weight gain during aging, male resistant rats naturally consume less food per week, demonstrate greater total activity (ambulatory and non-ambulatory), and manifest increased exercise capacity compared to control rats.
Conclusions: Discovered unexpectedly by their prolonged survival in hyperoxia, resistant rats represent a remarkable "experiment of nature" because of their innately longer lifespans, less disease, and increased function. Understanding the mechanisms responsible for the remarkable phenotype of the unique resistant rats holds promise for improving healthy longevity and aging-related disease and function in humans.
Shay R, Weikel B, Barry J, Grover T. University of Colorado Hospital, Aurora, CO
Purpose of Study: We sought to improve compliance with best practice for non-emergent neonatal tracheal intubations in our 82-bed level IV academic NICU.
NICU infants are at high risk for adverse events during tracheal intubation (TI) which become greater when a patient requires multiple intubation attempts. Literature demonstrates that neonatal TI can be performed more safely with use of specific premedication, paralysis and video laryngoscopy (VL).
Baseline data obtained from our institution demonstrated wide variability in premedication choices, infrequent paralytic and VL use for non-emergent neonatal TI, and increased number of attempts to intubate when compared to national benchmarks.
Methods Used: Quality improvement methodology and implementation science
Phase 1: The first aim was to improve compliance with evidence-based intubation premedication by 40% from baseline between July and December 2019 and sustain for ≥ six months.
Phase 2: The second aim was to utilize paralytic and VL in ≥25% of non-emergent neonatal TI by January 2022 and sustain for ≥ six months.
Summary of Results: 646 non-emergent neontal TIs have been reviewed over six acadmic years. We have increased utilization of evidence-based premedication, paralysis and VL. We have improved our ability to successfully intubate on the first attempt and within two attempts. We have decreased the frequency of physiologic instability associated with the procedure.
The combination of VL and a premedication regimen with paralysis, when adjusted for other patient and practice variables, is associated with intubation success on the first attempt in our unit (AOR 4.07, 95 CI [2.09, 7.92]).
Conclusions: With increased utilization of non-invasive ventilation, intubation has become a relatively low-frequency, high-risk procedure that lends itself to a standardized approach to improve outcomes. Our study demonstrates feasibility of practice and procedural outcome improvement in a large, academic NICU with multidisciplinary team involvement.
Despite statistically significant improvements in our care provision, our rates of desaturation during the procedure remain high. Next steps of this study will include continued montioring of outcomes related to increased VL use, assessing feasibility of utilizing oxygen during the procedure to reduce the frequency and severity of hypoxemia, and leveraging technology to reduce manual data extraction/entry and improve project transparency.
Practice and Outcome Variables by AY.
Academic Year
2017-2018
2018-2019
2019-2020
2020-2021
2021-2022
2022-2023
Intubations, n
80
88
116
84
115
163
Direct laryngoscope, n (%)
80 (100%)
88 (100%)
110 (95%)
73 (87%)
63 (55%)
43 (28%)
Video laryngoscope, n (%)
-
-
6 (5%)
11 (13%)
52 (45%)
110 (72%)
Premedication use, n (%)
21 (26%)
44 (50%)
83 (72%)
72 (86%)
98 (85%)
143 (88%)
Paralytic use, n (%)
11 (14%)
12 (14%)
29 (25%)
31 (37%)
45 (39%)
62 (41%)
First attempt success, n (%)
25 (31%)
31 (35%)
63 (54%)
34 (40%)
63 (55%)
95 (62%)
Bradycardia HR < 100, n (%)
40 (50%)
34 (39%)
20 (17%)
26 (31%)
19 (17%)
17 (11%)
Desaturation SaO2 < 80, n (%)
67 (84%)
64 (73%)
68 (59%)
58 (69%)
62 (54%)
94 (61%)
# 151
Technical Assessment of Simulated Neonatal Intubation Using Multi-angle Video
Gu H1, Cranshaw M1, Galindo R2, Alade T3, Pineda L2, McWilliam P4, Powell D2, Kent N5, Fuerch J1, Yamada N1, Halamek L1. 1Stanford, Palo Alto, CA; 2Center for Perinatal and Pediatric Education, Palo Alto, CA; 3Georgetown School of Medicine, Washington, D.C.; 4Labourne College of Healthcare, Milton, MA and 5Franklin Pierce University, Rindge, NH
Purpose of Study: Neonatal intubation is a life-saving intervention, though few objective markers of procedural proficiency exist. Characterizing differences in novice and expert intubation technique is necessary to optimize training. We aim to use multi-angle video technology to quantify differences in intubation technique between novice and expert intubators.
Methods Used: Study subjects included attending neonatologists, neonatal hospitalists, neonatology fellows, pediatric residents, and neonatal nurse practitioners. Experts were defined having >1 intubations and >1 year NICU experience. All others were novices. Each subject performed three intubation attempts using a video laryngoscope on both term and preterm neonatal mannequins. Subjects were blinded to the video view and used direct laryngoscopy. Intubation success was determined by intraoral visualization of endotracheal tube (ETT) passage through vocal cords and auscultation. Overhead and intraoral video were recorded. We divided the intubation procedure into temporal phases (Figure A). Cormack-Lehane view grade was also recorded (Figure B). Statistical analyses included Mann-Whitney U tests, and Fischer Exact tests.
Summary of Results: 38 study subjects were recruited. 20 were experts, and 18 were novices. 228 intubation trials were analyzed, 12 of which were unsuccessful (4 expert, 8 novice). The median time to intubate the preterm mannequin for an expert was 15.7sec compared to 17.9sec for a novice (p=0.121). The median time to intubate the term mannequin for an expert was 12.5sec compared to 15.8sec for a novice (p<0.001). In the preterm mannequin, experts were able to view the cords significantly faster than novices. In the term mannequin, experts were able to advance the ETT into the intra-oral view significantly faster than novices (Table). In the preterm mannequin, 7/54 (13%) novices obtained a grade I view, 40/54 (74.1%) novices obtained a grade IIa view, and 7/54 (13%) novices did not view the cords. In contrast, 4/60 (6.7%) experts obtained a grade 1 view, 55/60 (92.7%) experts obtained a grade IIa view, and 2/60 (3.4%) experts did not view the cords (p=0.022). The Cormack-Lehane views did not differ between novices and experts in the term mannequin.
Conclusions: Experts intubated the term, but not preterm, mannequin faster than novices. Expert and novice intubators differed in intraoral views of the preterm mannequin, but not the term mannequin. Experiential definitions of novice and expert may be inadequate to characterize procedural skill in simulated intubation.
Time Spent in Different Intubation Phases.
Novice
Median (IQR), seconds
Expert
Median (IQR), seconds
P-value
Mann-Whitney U Test
Preterm: total time to intubate
17.9 (13.7 - 22.4)
15.7 (11.6 - 21)
0.121
Preterm: blade in mouth → First view of cords
5 (2.9 - 7.2)
3.6 (2.6 - 5.9)
0.040
Preterm: first view of cords → call "cords"
2.2 (1.8 - 3.5)
1.9 (1.4 - 3.3)
0.12
Preterm: call "cords" → ETT in intraoral view
3.1 (2.4 - 3.9)
3.5 (2.8 - 4.3)
0.103
Preterm: ETT in intraoral view → ETT through cords
0.88 (0.33 - 1.7)
0.79 (0.46 - 1.42)
0.851
Preterm: ETT through cords → blade out of mouth
2 (1.5 - 3.2)
1.31 (1.1 - 1.9)
< 0.001
Term: total time to intubate
15.8 (13.3 - 23.3)
12.5 (10.5 - 16.0)
< 0.001
Term: blade in mouth → first view of cords
2.1 (1.7 - 3.1)
2.0 (1.7 - 3.6)
0.718
Term: first view of cords → call "cords"
2.5 (1.8 - 5.8)
2.5 (1.7 - 3.6)
0.193
Term: call "cords" → ETT in intraoral view
3.8 (2.6 - 4.7)
2.9 (2.1 - 3.9)
0.003
Term: ETT in intraoral view → ETT through cords
1.5 (0.56 - 3.5)
0.96 (0.58 - 1.7)
0.056
Term: ETT through cords → blade out of mouth
2.3 (1.3 - 3.2)
1.33 (1.0 - 1.9)
<0.001
ETT: endotracheal tube.
# 152
Effect of Stewardship on Inhaled Nitric Oxide use in a Preterm Infant Population
Thompson SL1, Mullen N2, Gross J3, Love J1, Maxwell J2. 1University of New Mexico, Albuquerque, NM; 2University of New Mexico Hospital, Albuquerque, NM and 3University of New Mexico Hospital, Albuquerque, NM
Purpose of Study: Persistent pulmonary hypertension of the newborn (PPHN) occurs due to an abnormal transition from fetal to extrauterine circulation. Inhaled Nitric Oxide (iNO) is a treatment modality approved by the Food and Drug Administration (FDA) for treatment of PPHN in term and near-term infants, but not in early preterm infants. The purpose of this study is to evaluate if an iNO guideline leads to improved practice changes in both initiation and duration of iNO in the early preterm population.
Methods Used: A prospective, interrupted time-series study of infants born ≤ 33 6/7 admitted to the Neonatal Intensive Care Unit (NICU) at the University of New Mexico Hospital is being completed. Use of iNO in this patient population was reviewed (January 1, 2015 – December 31, 2020) and an internal institutional baseline was established. Primary measures of interest in the population included indication for initiation of iNO, patient response to therapy, and overall duration of iNO therapy. Guidelines for iNO use were developed with implementation October 1, 2022. Prospective data collection is ongoing. Additional data included illness severity information (Critical Risk Index for Babies (CRIB II) and patient mortality.
Summary of Results: Baseline assessment showed significantly higher mortality rates among participants that received iNO compared to controls (those that did not receive iNO) as well as lower gestational age, lower birth weight, and higher CRIB II score in cases compared to controls (all p<0.05). Data collection continues in the prospective cohort, however preliminary analysis has been completed on data collected thus far. Following implementation of the iNO use guideline, those receiving iNO are similar in gestational age but are significantly smaller in birthweight (1395 grams in controls vs 507 grams in cases, p<0.05). There continues to be a significant difference in mortality (p<0.05), although overall utilization of iNO is not decreased based on preliminary prospective data (12% of retrospective cohort and 7% of prospective cohort p=0.41). In the retrospective cohort, 63% of cases had an echocardiogram completed prior to initiation of iNO, while in the initial prospective cohort data 100% of cases had an echocardiogram completed prior to initiation of iNO.
Conclusions: Significant differences including disease severity have been noted in infants receiving iNO prior to utilization of a guideline, with some differences no longer significant after the introduction of the guideline. This suggests that with stronger stewardship and implementation of evidence-based iNO utilization we can reduce patient exposure and potential harm while reducing medical expense.
# 153
HEMODYNAMICALLY SIGNIFICANT PATENT DUCTUS ARTERIOSUS AND MODERATE TO SEVERE BRONCHOPULMONARY DYSPLASIA
Fyfe AM2, Love J1, Markee S3. 1University of New Mexico, Albuquerque, NM; 2University of New Mexico, Albuquerque, NM and 3University of New Mexico, Albuquerque, NM
Purpose of Study: The patent ductus arteriosus (PDA) is a common problem in extremely preterm neonates with 80% of infants born from 25-28 weeks gestation and 90% of those born at 24 weeks gestation having a PDA at 4 days of life.1 The left-to-right shunting that occurs through the ductus causes pulmonary over circulation and decreased systemic perfusion. The persistence of the PDA has been associated with increased rates of interventricular hemorrhage (IVH), bronchopulmonary dysplasia (BPD), necrotizing enterocolitis, and cerebral palsy in epidemiological studies. 1-3 However, numerous clinical trials have demonstrated no reduction in these outcomes with medical treatment of the PDA.2-4 This has called into question whether the hemodynamic effects of the PDA are the cause of the increased rates of adverse outcomes. However, the majority of these studies lack reliability due to methodological errors, namely the lack of standardized echocardiography criteria to determine hemodynamic significance and reliance on size alone to determine hemodynamic significance.2, 5
Using Targeted Neonatal Echocardiography to evaluate hemodynamic significance and guide treatment has been shown to improve outcomes in micro-preemies, however targeted neonatal echo with evaluation by neonatal hemodynamic specialists is not available in every center. In this study we evaluate whether determining hemodynamic significance with parameters available on cardiac echocardiography is associated with moderate-severe BPD or death.
Methods Used: A retrospective cohort study was conducted. We plan to evaluate the cardiac echocardiograms performed on a total of 220 babies born at less than 28 weeks. We will exclude babies who are outborn, have multiple congenital malformations, had no echocardiograms performed, or who died before 3 days of life. We will determine if there was an increased risk of moderate to severe BPD or death in babies who were determined to have hemodynamically significant PDAs by cardiac echocardiogram. We will also evaluate whether that risk was increased with longer duration of shunt exposure. To determine hemodynamic significance, we will score echoes based on the PDA size indexed to weight, velocity of flow through the PDA, mitral valve E wave, Left atrium: aorta ratio, and left ventricle size.
Summary of Results: Preliminary results showed a non-statistically significant increase in risk of moderate to severe BPD or death in babies who were determined to have a hemodynamically significant PDA by cardiac echo. The risk ratio was 1.32 with a 95% confidence interval of 0.859-2.02 with a p-value of 0.42
Conclusions: With data analyzed from only 11 babies, more data is needed to determine whether using cardiac echocardiography to determine hemodynamic significance is useful in predicting which babies are at increased risk of adverse outcomes.
Surgery II - Plastic Surgery
Concurrent Session
3:15 PM
Thursday, January 18, 2024
# 154
AN ASSESSMENT OF BIOFILM FORMATION ON ACELLULAR DERMAL MATRIX IN BREAST IMPLANTS
Thomas LE1, Small EA1, Carlson PF1, Gupta S2. 1Loma Linda University, Loma Linda, CA and 2Loma Linda University, Loma Linda, CA
Purpose of Study: The use of acellular dermal matrix (ADM) in tissue repair and reconstruction procedures has become very common but may contribute to increased biofilm formation due to its porous nature and as a substrate for microbial attachment. Additionally, potential for compromised blood supply in the implanted ADM may create localized hypoxia, favoring bacterial growth. The purpose of this study is to understand how the application of acellular dermal matrix into biofilm formation may serve as a better model to study the prophylactic use of antibiotics during surgery.
Methods Used: Petri dishes with portions of breast implant shells wrapped in ADM were assigned to four experimental groups of ten specimens with and without bacteria and rinsed with saline or antibiotics (figure 1).
After inoculation with bacteria and time for culture growth, the specimens were irrigated, and biofilm quantified with absorbance spectrophotometry.
Summary of Results: In the absence of bacteria, the average absorbance was 0.0113 with saline and 0.0113 with antibiotics, yielding a non-significant p-value of 1. In the presence of bacteria, the average absorbance was 0.442 with saline and 0.386 with antibiotics, resulting in a non-significant p-value of 0.6362. Comparing the no bacteria and saline group to the bacteria and saline group yielded a statistically significant p-value of 0.0011, indicating sterile technique maintenance and adequate microbial growth.
Conclusions: We aimed to design a model similar to the environment of the breast pocket during breast reconstruction to assess biofilm formation using acellular dermal matrix (ADM). There was no statistical difference between using saline and antibiotics on the sterile ADM model to prevent biofilm formation. This suggests that prophylactic use of antibiotics to irrigate the breast pocket may be unnecessary and may contribute to the growing concern of antibiotic resistance with overuse. There was also no statistical difference using saline and antibiotics on the cultured ADM model to eliminate biofilm formation. This indicates that the current protocol for breast implant removal after suspected infection remains appropriate. Surgeons and healthcare professionals must prioritize infection prevention, including proper sterilization and aseptic procedures, to reduce excessive antibiotic use and safeguard the public against antibiotic-resistant infections.
Absorbance of Biofilm Under Various Conditions.
Group 1: No bacteria + saline solution
Group 2: No bacteria + antibiotic solution
Group 3: Bacteria + saline solution
Group 4: Bacteria + antibiotic solution
1
0.002
0.006
0.957
0.583
2
0.002
0.022
0.918
0.152
3
0.001
0.005
0.424
0.259
4
0
0.003
0.252
0.893
5
0.032
0.006
0.394
0.310
6
0.002
0.036
0.128
0.162
7
0
0.008
0.339
0.198
8
0.041
0.025
0.176
0.299
9
0.002
0.002
0.504
0.599
10
0.031
0
0.328
0.402
Average
0.0113
0.0113
0.442
0.386
# 155
ENHANCING TRIAGE EFFICIENCY IN PLASTIC SURGERY: VALIDATION OF AN ARTIFICIAL INTELLIGENCE-DRIVEN DIALOGUE PROMPT FOR COMPLEX WOUND REFERRALS
Small EA1, McMath K2, Thomas LE1, Carlson PF1, Gupta S2. 1Loma Linda University, Loma Linda, CA and 2Loma Linda University, Loma Linda, CA
Purpose of Study: In this study, we propose the development and validation of a specialized tool utilizing artificial intelligence (AI) to effectively triage patients with complex wound referrals to plastic surgeons. The aim is to provide medical assistants at a wound clinic with an AI-driven prompt that can guide their interactions with patients during phone calls, enabling them to better understand the urgency of a patient’s wound and appropriately schedule appointments. By leveraging the capabilities of AI, we seek to improve the accuracy and efficiency of triaging complex wound patients, ultimately leading to improved patient care and outcomes.
Methods Used: This study was conducted at a tertiary wound care center, involving a prospective design to assess the effectiveness and validity of the AI-based triage tool. We collaborated closely with plastic surgeons to develop a comprehensive dialogue prompt for Chat GPT, an AI language model. The prompt was created based on questions that are essential to accurately triage the urgency of patients with complex wounds. Eight patient vignettes were developed by an experienced clinician at the wound care center based on common scenarios referred to the Loma Linda University Medical Center Advanced Wound Care Center. The vignettes were rated as urgent (needing an appointment scheduled within a week) or non-urgent (appointment could be scheduled in greater than a week). The vignettes were then submitted into Chat GPT along with the prompt that we developed, and Chat GPT’s response was recorded.
Summary of Results: In total, eight different patient vignettes were analyzed. Four of the vignettes were designated as “urgent patients” and four were designated as “non-urgent patients.” Of the urgent patients, we provided a clinical scenario for dehisced abdominal panniculectomy, infected pressure injury, infected diabetic foot ulcer, and acute burn. The non-urgent patients represented clinical scenarios for chronic non-infected pressure injury, chronic non-infected diabetic foot ulcer, dry adherent eschar, and non-infected venous leg ulcer. Chat GPT accurately triaged all 8 patients as a correct urgent or non-urgent diagnosis.
Conclusions: The use of an AI-driven dialogue prompt, integrated with the Chat GPT language model appears to be a promising approach in assisting the triage process for patients with complex wound referrals. The patients within this study represent a wide range of patient wound scenarios both urgent and non-urgent. The use of AI can aid in preventing suboptimal scheduling times and potential delays in care. Implementation of AI into triage tools in outpatient clinics has the potential to improve efficiency and resource allocation by reducing the risk of complications in urgent patients and avoiding unnecessary overcrowding in clinics. Our research demonstrates the initial steps toward enhancing patient care with AI and contributing to more effective patient-centered care.
# 156
NERVE WRAP FOR LOCAL DELIVERY OF TACROLIMUS ACCELERATES NERVE REGENERATION BY MODULATION OF SCHWANN CELL ACTIVITY WITHOUT CONCOMITANT SYSTEMIC LOADINGError! Hyperlink reference not valid.
Jabbari K5, Su AA1, 5, Xiao B1, Feturi F1, van der Merwe Y2, Barnett JM1, Khatter NJ5, Katzel E1, Venkataramanan R4, Solari MG1, Wagner W3, Simons DJ6, Steketee MB2, 3, Washington K1, 5. 1University of Pittsburgh School of Medicine and Veterans Administration Healthcare System, Pittsburgh, PA; 2University of California, San Diego, San Diego, CA; 3McGowan Institute for Regenerative Medicine, Pittsburgh, PA; 4University of Pittsburgh School of Pharmacy, Pittsburgh, PA; 5University of Colorado School of Medicine, Aurora, CO and 6University of Pittsburgh School of Medicine, Pittsburgh, PA
Purpose of Study: Peripheral nerve injuries (PNI) frequently result in functional disabilities. We previously demonstrated improved functional recovery using a novel Tacrolimus/FK506-impregnated Polyester urethane urea (PEUU) nerve wrap to treat PNI in a validated rat infraorbital nerve (ION) transection and repair model. With PEUU-FK506 treatment, FK506 blood levels measured nearly at the limit of quantification. This study investigates the neurotrophic properties of PEUU-FK506 upon myelin and axonal neurofilament dynamics in our sensory nerve model.
Methods Used: Twenty-four 8–10-week-old Lewis rats underwent surgical PNI and repair, before assessing ION afferent function. Immunolabelling of histological samples was performed for treatment-groups: cut & repair only, intraperitoneally (IP) injected 2.2 mg/kg/day FK506, or 5 mm x 1.5 mm section of 10 mg PEUU-FK506 wrap (n=2-4/group). Animals were euthanized and IONs were dissected at four and six weeks postoperatively. ION samples of naïve rats served as controls. Each ION sample was immunolabelled with anti-neurofilament medium chain (NFM-FITC), anti-myelin (myelin-TRITC), and nuclei were stained with DAPI. Samples were imaged with confocal microscopy and fluorescence intensity was measured using ImageJ software.
Summary of Results: In the ION of naïve animals, myelin expression was greater compared to NFM (P<0.01). Both cut & repair and IP-FK506 groups exhibited greater NFM expression compared to myelin (P<0.01) and reduced myelin signal as compared to the naïve controls (P<0.01). Conversely, PEUU-FK506 treatment increased the ratio of myelin:NFM in the ION, albeit not significantly. With PEUU-FK506 treatment, Schwann cell myelin expression was higher compared against both cut & repair and IP-FK506 treatments (P<0.01), but this increase was not significant when compared to naïve (P=0.55).
Conclusions: Myelination in the proximal stump was greater in PEUU-FK506 treated IONs compared to IP-FK506 treatment up to 6-weeks following transection and immediate neurorrhaphy. Site-specific delivery of Tacrolimus to PNI sites with a PEUU-FK506 wrap increases differentiated Schwann cell myelination, accelerating functional outcomes. This modality holds promise for nerve regeneration as well as local immunosuppression in composite tissue allotransplantation.
# 157
DIFFERENCES BETWEEN POSTERIOR INTEROSSEOUS ARTERY FLAP OUTCOMES ACROSS VARIOUS SOFT TISSUE DEFECT ETIOLOGIES
Lascar E1, Friedrich J2. 1University of Washington School of Medicine, Seattle, WA and 2University of Washington, Seattle, WA
Purpose of Study: The purpose of this study was to evaluate if there are differences in the occurrence of major and/or minor postoperative complications between different injury etiologies following posterior interosseous artery (PIA) flap reconstruction. The results can help inform postoperative care on an individual level, with the goal of reducing postsurgical morbidity.
Methods Used: A cohort of thirty-four adult patients who underwent soft tissue reconstruction with PIA flaps between the years 2012 and 2023 at Harborview Medical Center were retrospectively identified from Epic and LKArchive. Demographic, operative, and flap characteristic data including soft tissue defect site, flap dimensions, time interval from injury to flap transfer, and operation time were examined. Postoperative complications were classified as major, which included life-threatening complications such as deep vein thrombosis, pulmonary embolism, septicemia, or death, or minor, including infection, necrosis, wound dehiscence, and incidence of subsequent revisions. The soft tissue defect etiology categories used for comparison were crush, burn, blast, infection/necrosis, degloving/avulsion, amputation, and soft tissue reconstruction following contracture release. Only categories with more than five patients were included in comparisons and an ANOVA was used to compare operative characteristics between groups.
Summary of Results: Of all 34 patients in the study, none had major postoperative complications. Twenty-three (68%) had minor postoperative complications and twelve (35%) had more than one complication. Amongst defect etiology categories with more than five patients, those who required a PIA flap due to chronic infection and/or tissue necrosis reported the highest rate of complications (87.5%), followed by those with avulsion injury (80%), and blast injury (69.2%). Additionally, those who required PIA flaps following avulsion injury experienced more than one complication more frequently (60%) than those with blast injury (38.5%) or those with infection/tissue necrosis (37.5%). Of these three defect etiologies, avulsion injury reconstruction had the highest rates of flap loss or necrosis (40%), infection (60%), and surgical revisions (80%). The highest rate of wound dehiscence was seen in PIA reconstruction following infection/necrosis, at 62.5%. Among these three groups, no statistically significant differences were observed between the operative characteristics (time interval between injury and flap transfer, P= 0.773; flap dimensions, P = 0.804; and operation time, P = 0.334).
Conclusions: These results indicate that soft tissue defects due to degloving or avulsion injuries may be more prone to minor postoperative complications following PIA flap reconstruction. While the absence of statistically significant differences among operative and flap characteristics indicates that these factors may not be associated with postoperative outcomes, due to the small sample size, further investigation is needed to confirm these findings.
# 158
COMPARISON OF CELL VIABILITY OF AUTOLOGOUS FAT GRAFTS OBTAINED WITH OPEN VERSUS CLOSED SYSTEMS
Carlson PF2, Small EA1, Thomas LE1, Gupta S3. 1Loma Linda University School of Medicine, Loma Linda, CA; 2Loma Linda University School of Medicine, Loma Linda, CA and 3Loma Linda University, Loma Linda, CA
Purpose of Study: Autologous fat grafting has emerged as a revolutionary technique in regenerative medicine and plastic surgery, offering promising solutions for soft tissue reconstruction and aesthetic enhancements. Processing of adipose tissue relies on several extraction methods within a closed or open system, such as enzymatic isolation, centrifugation, and filtration, to separate adipocyte-derived stem cells (ASCS) and mesenchymal stem cells (MSCs) from blood, oil, and debris. An open system processing design, characterized by intermittent open-air transfers, has traditionally been used because of cost-effectiveness and familiarity. However, a growing number of biomanufacturers have designed closed systems, believed to mitigate contamination risk and uphold graft integrity. With increasing importance placed on maximizing the viability of transferred fat, this study works to uncover whether a substantial disparity exists between open and closed processing systems.
Methods Used: The Pubmed and Food and Drug Administration (FDA) databases were used to review papers and documents pertaining to the certification of adipose graft processing systems and performance testing. Six papers with open system processing and five papers with closed system processing were located that listed the percentages of nucleated cell viability, cell yield, and an explanation on how the system isolates adipocytes. A T-test analysis for cell yield and percent cell viability between the two tests were performed with a significance value of p<0.05.
Summary of Results: The null hypothesis stated that there was no significant difference between the nucleated cell percent or the cellular yield in an open or closed system. The p-values for nucleated cell percentage and cell yield were 0.689 and 0.112, respectively (p<0.05).
Conclusions: According to the results of the T-test, the author failed to reject the null hypothesis therefore there is no evidence to support a difference in cell yield or percent of nucleated cells between open and closed systems. The primary objective of this experiment was to ascertain whether a notable distinction exists between open air transfers conducted within a controlled environment and transfers carried out within aseptic closed systems. That said, although there was no significant difference, it did not take into account the different methods of isolation that were used in each system. This could suggest that the methods of extraction may play a more important role in adipocyte viability than the type of system used for extraction. In future work, there should be an emphasis on comparing closed and open systems with identical extraction and processing methods.
# 160
ESTABLISHING A RETROSPECTIVE GENITAL GENDER AFFIRMING SURGERY DATABASE
Kalaf NC1, Lin JS2, Awada O1, Skokan A1, 2. 1University of Washington, Seattle, WA and 2University of Washington, Seattle, WA
Purpose of Study: Genital gender-affirming surgery (gGAS) has not been well studied and existing outcomes data come from retrospective, single-center studies. The gGAS program at the University of Washington (UW) is in its second year and there is need for analysis. The goal of this study was to evaluate trends in data and compare gGAS outcomes at UW to existing literature. This is anticipated to provide value to the patients we directly care for through surgical improvements and to potentially contribute insights to the broader professional community in refining best practices in surgical care.
Methods Used: A retrospective cohort study of 41 patients at UW who consulted for gGAS between February 2022 and August 2023 was completed and organized into a database. Patients were classified as seeking masculinization (phalloplasty or metoidioplasty) or feminization (vaginoplasty) surgery, and data on demographics, medical history, post-operative outcomes, and complications was collected. Complications were followed 90 days out from the date of surgery. Inclusion criteria were based on an ICD-10 diagnosis of gender dysphoria and CPT code for vaginoplasty, phalloplasty, or metoidioplasty. Individuals who received gGAS at another institution but sought follow-up care at UW were excluded.
Summary of Results: Of the cohort, 28 (68.3%) sought feminization surgery (vaginoplasty) and 13 (31.7%) sought masculinization surgery (phalloplasty or metoidioplasty). There were 29 patients (70.1% of cohort) who completed gGAS at UW between February 2022 and August 2023. The majority (82.8%, n=24) underwent vaginoplasty, for which patients elected to receive either limited depth (66.7%, n=16) or full depth (33.3%, n=8). Patients who received masculinization surgery had either phalloplasty (6.9%, n=2) or metoidioplasty (10.3%, n=3). The remaining 12 patients in the cohort anticipated but had not yet completed gGAS.
The focus of the results was on outcomes for vaginoplasty, which is performed primarily through penile inversion at UW (95.6%, n=23). The most common vaginoplasty complication was wound dehiscence (33.3%, n=8). Other complications included urinary tract infection (UTI) (25.0%, n=6), urinary retention (16.7%, n=4), tissue necrosis (16.7%, n=4), introital stenosis (4.2%, n=1), pelvic pain (4.2%, n=1), and vaginal prolapse (4.2%, n=1). No patients reported dissatisfaction following surgery.
Conclusions: The most common complications of vaginoplasty in this cohort were wound dehiscence, UTI, urinary retention, and tissue necrosis. Compared to the literature, the incidence of these complications was reasonable aside from tissue necrosis, possibly an artifact of a small sample size. Phalloplasty and metoidioplasty outcomes and other measures of post-operative care, such as the use of a wound VAC, will be assessed when a larger sample size is collected. Ultimately, a gGAS database at UW has been established and may provide insights into improving care for patients receiving gGAS as additional data is collected.
University of Washington Vaginoplasty Cohort,n = 24 (# of limited depth + # of full depth)
Wound dehiscence
5 - 33%
33.3%
n = 8 (5 + 3)
Urinary tract infection
2 - 32%
25.0%
n = 6 (4 + 2)
Urinary retention
< 32%
16.7%
n = 4 (2 + 2)
Pelvic pain
< 20%
4.2%
n = 1 (1 + 0)
Introital stenosis
4 - 15%
4.2%
n = 1 (0 + 1)
Meatal stenosis
< 14%
0.0%
n = 0
Tissue necrosis
1 - 4%
16.7%
n = 4 (3 + 1)
Clitoral necrosis
1 - 3%
0.0%
n = 0
Vaginal prolapse
1 - 2%
4.2%
n = 1 (0 +1)
Rectal injury
0.5 - 4.5%
0.0%
n = 0
Rectovaginal fistula
1 - 2%
0.0%
n = 0
# 161
Surgical Approaches for Carpometacarpal-1Osteoarthritis: A Meta-analysis of Delta Pain Scores and Clinical Implications
Sarli NM, Golovachev N, Xavier J, Ghayyad K, Kachooei A. Adventhealth, Rothman Orthopaedic Institute, Orlando, FL
Purpose of Study: Arthroscopic debridement(AD), trapeziectomy(T), and joint replacement(JR) are treatments adopted for patients with carpometacarpal-1 (CMC 1) osteoarthritis to alleviate pain and improve quality of life. However, doubts remain regarding the selection of the most effective intervention in terms of pain relief. This meta-analysis compares the impact of AD, T, and JR on the delta pain scores and evaluates their clinical significance in patients with CMC 1 osteoarthritis.
Methods Used: We conducted a systematic search of PubMed, Cochrane, Embase, and Medline databases for studies investigating pain outcomes associated with interventions for CMC-1 osteoarthritis. Delta pain scores, reported with the Visual Analog Scale (VAS), were compared with a predefined threshold (1.65) for Minimal Clinically Important Difference (MCID). Studies published in journals ranked within the first and second quartiles and those with a minimum follow-up duration > 6 months were included.
Summary of Results: Eighteen studies with 763 patients were included in this meta-analysis. Patients were treated with AD (n=76, 10%), T (n=442, 58%), and JR (n=245, 32%) between 2010 and 2023 with a mean follow-up period of 38 ± 28 months. 25 groups were included, 4 of which received AD, 14 of which received T, and 7 of which received JR. The mean delta VAS among all groups was 4.9 ± 2.
This meta-analysis showed a mean delta pain score of 4.3 (95%CI, 3-5.6, P<0.01) for AD, 4.8 (95%CI, 3.7-5.8, P<0.01) for T, and 5.9 (95%CI, 4.2-7.6, P<0.01) for JR. The difference in delta pain scores did not reach statistical significance(P=0.36). All surgical interventions were associated with a clinically significant improvement in pain scores, surpassing the MCID threshold. Specifically, the mean delta pain score was 2.6 times the MCID for AD, 2.9 times for T, and 3.6 times for JR (P=0.41).
Conclusions: The findings of this study indicate that AD, T, and JR, are associated with substantial improvements in pain scores, surpassing the MCID threshold, with no statistically significant difference between the groups. These results show that AD, T, and JR are all effective treatments for mitigating pain and enhancing the quality of life in individuals suffering from CMC-1 osteoarthritis.
Forest Plot of Delta VAS.
# 162
Validation of ChatGPT as a Tool to Optimize Readability of Patient-Facing Plastic Surgery Education Materials
Vallurupalli M1, 2, Shah ND2, Vyas R2. 1Keck School of Medicine of USC, Los Angeles, CA and 2University of California, Irvine, Orange, CA
Purpose of Study: To address low rates of patient health literacy, the American Medical Association (AMA) recommends that readability of patient education materials should not exceed a 6th grade reading level; and the National Institutes of Health recommend no greater than an 8th grade reading level. However, patient-facing materials in plastic surgery often remain above the recommended averages. Limited health literacy plays a detrimental role in patient understanding of health information, and hinders active patient involvement in care and shared decision making. The purpose of this study is to evaluate ChatGPT 3.5, an artificial intelligence interface, as a tool for analysis and simplification of patient-facing plastic surgery education materials.
Methods Used: 48 patient-facing plastic surgery education materials were evaluated for readability by a traditional calculator and ChatGPT 3.5. These excerpts included patient education information regarding craniofacial surgery, hand surgery, aesthetic surgery, and breast surgery. The resulting scores were compared. The original excerpts were then inputted to ChatGPT 3.5 and simplified by the artificial intelligence tool. The simplified excerpts were scored by the calculators.
Summary of Results: For the original excerpts, the difference in scores between the traditional calculator and ChatGPT 3.5 were not significant (p > 0.05). Additionally, the simplified excerpts’ readability scores were significantly lower than the original readability scores (p < 0.05), while the mean of the simplified excerpts was 7.60, less than the maximum recommended 8. Furthermore, ChatGPT 3.5 provided detailed, excerpt-specific feedback distinguishing it from the traditional readability calculator, which provided only numerical grade level analyses.
Conclusions: The use of ChatGPT 3.5 for the purpose of simplification and readability analysis of patient-facing craniofacial materials is efficient and may help facilitate the conveyance of important health information. ChatGPT 3.5 rendered readability scores comparable to traditional readability calculators, in addition to excerpt-specific feedback. It was also able to simplify materials to the recommended grade levels. After simplification by the AI, the mean grade level of the revised excerpts was not only significantly lower than the originals, but also below the national 8th grade recommendation. Additionally, author review of the generated excerpts did not necessitate any changes to maintain accuracy. With human oversight, we validate this tool for readability analysis and simplification within the field of plastic surgery..
# 163
Successful Extension of Vascularized Composite Allograft Perfusion Cold Storage to 24 Hours in a Rat Hind Limb Transplant Model
Huang J1, Ng P1, Yoeli D1, Luo Y1, Wang Y1, Li B1, Lu L1, Wang Z1, Arrowsmith P2, Jain S1, Mathes DW1, Washington K1, Farkash E2, Jani A1, Huang CA1. 1University of Colorado School of Medicine, Aurora, CO and 2University of Michigan School of Medicine, Ann Arbor, MI
Purpose of Study: Vascular composite allograft (VCA) transplantation is a treatment for reconstruction of complex tissue injuries but is limited by an allograft storage time of <6 hours. Ischemic reperfusion injury (IRI) often leads to both short and long-term complications. Hypothermic machine perfusion (HMP) preservation of grafts could mitigate IRI and extend storage times. In kidney grafts, HMP storage with University of Wisconsin (UW) Kidney Preservation Solution (KPS-1®) has been shown to significantly decrease IRI. However, HMP storage has not been evaluated in VCA transplantation. This study evaluates the preservation effects of KPS-1®, compared to normal saline (NS) in rat hind limbs subjected to 24-hour perfusion cold storage.
Methods Used:Perfusion – Hind limbs (n=12) from male Brown Norway rats (14-18 weeks old) were surgically procured. The femoral arteries were cannulated with a 25G blunt needle cannula for 24 hours of HMP cold storage. 6 donor limbs were perfused with KPS-1®, and the other 6 were perfused with NS. A peristaltic pump was used.
Tissue Analysis – Western blot was used to analyze RIP3, TLR4, and cleaved caspase-3 levels. TUNEL & cleaved caspase-3 staining was quantified using the percent of positive cells in 5 10x and 20x fields. Edema was quantified in 5 random 10x and 20x fields using the intercellular and interfascicular space.
Summary of Results: KPS-1® perfused hind limb muscles showed significantly less edema than limbs perfused with NS in both area (p=7.294E-05) and linear approaches (p=0.0003). Muscles in the KPS-1® group showed significantly less apoptosis, measured by percent positive cells in TUNEL and cleaved caspase-3 staining (p=0.0063 and p=0.0449). Western blot analysis showed significantly greater expression in RIP3 (13.76x, p=0.0022), and TLR-4 (8.54x, p=0.0022) for the NS group. While not significant, cleaved caspase-3 protein expression was 3.73x greater in the NS group compared with KPS-1® (figure 1).
Conclusions: HMP cold storage of rat hind limbs with KPS-1® solution significantly reduces edema and markers of inflammation and cell death compared to NS. In addition to survival applications post-transplant, future studies will investigate optimization of the perfusion solution through addition of inhibitors of apoptosis and necrosis.
TUNEL and Cleaved caspase-3 analysis of (A,D) naive muscle, (B,E) NS perfused muscle, (C,F) KPS-1® perfusion. Quantification of TUNEL (G), caspase staining (H) and Western Blot (I).
Poster Session I
Concurrent Session
6:00 PM
Thursday, January 18, 2024
#164
Evaluating the impact of an adolescent sexual and reproductive health education program in indigenous Tharu communities of rural Nepal
Bondy SK, Ho A, Kong P, Nakajima L, Chambers A, Cunningham J, Loughton S, Kapoor V. University of British Columbia, Vancouver, BC, Canada
Purpose of Study: The University of British Columbia’s Nepal Sexual and Reproductive Health (SRH) Project is a student-led global health initiative created in collaboration with local non-profit organization Creating Possibilities (CP) Nepal to provide essential SRH education to vulnerable youth in rural Dang, Nepal. In Dang, indigenous Tharu communities are recovering from a long history of bonded labor, which has had immeasurable impacts on women and children. In 2020, the Adolescent Health Program, a 10-session education series, was created to bridge gaps in SRH knowledge among Tharu youth. Our aim is to evaluate the effectiveness of the program by assessing its impact on SRH knowledge, self-esteem, gender-equitable attitudes, and use of SRH services.
Methods Used: Evaluation of our SRH education program involves three components: 1) Creation of the Training-of-Trainers (ToT) manual, 2) Survey development, and 3) Data collection and analysis. 1) The Training-of-Trainers (ToT) manual, developed in 2023, serves as a comprehensive resource for instructors. Aligned with key objectives from the International Technical Guidance on Sexuality Education (ITGSE), it ensures standardized, evidence-based, and culturally adapted program delivery. 2) Pre and post-program surveys were created using established evaluation tools and validated scales to gather data on demographics, SRH knowledge, self-esteem, gender-equitable attitudes, and use of SRH services. Both short answer and Likert scale multiple choice questions were included. All questions were reviewed and translated into Nepali by CP Nepal Staff. 3) We aim to include 90 students between ages 12 to 18 in the study. Participant recruitment and consenting will be done by CP Nepal staff via community outreach. Surveys will be administered before and after participating in the SRH education program. Quantitative data will be analyzed using paired t-tests to compare pre and post-survey scores for each participant. Qualitative data will be coded according to the Theoretical Domains Framework to identify themes and determine which areas of the program need improvement.
Summary of Results: Student feedback regarding the ToT manual has been very positive thus far, with 84% of students rating their educational experience as very good on preliminary feedback forms distributed to our initial trial group of 34 students. Instructors report increased confidence in course content and greater student engagement. Now that ethics approval has been obtained, survey distribution and data collection can begin. All surveys will be completed by January 2024 and data analysis will be conducted in early Spring 2024.
Conclusions: Consistent engagement and collaboration with CP Nepal and other Tharu community members has been integral to the success of this project so far. As interest in our SRH program continues to grow, formal evaluation is essential to establish two-way communication with students, assess program impact, and ensure community needs are being met.
#165
A Pediatric Dermatology Case: Persistent Lesions of the Lower Extremity in a 13-Year-Old Boy
Cherepakhin OS2, Gupta D1. 1University of Washington, Seattle, WA and 2University of Washington School of Medicine, Seattle, WA
Case Report: We present the case of a 13-year-old male with poorly controlled type 1 diabetes mellitus, who sought evaluation for chronic, non-healing plaques on his bilateral lower extremities persisting for over five years. Initially, tender, red and purple papules had appeared in an annular distribution, subsequently evolving into atrophic plaques. He had not had any similar rash previously or in other locations. No specific treatments had been trialed. Physical examination revealed bilateral lower extremity annular erythematous and yellow plaques. The plaques had scaly, atrophic, red and yellow centers with fine telangiectasias and hyperpigmented, violaceous and red borders. There were also three scaly, red papules arranged in a linear array present on the right shin. A 4 mm punch biopsy of the left leg’s largest annular plaque was performed. Histopathologic analysis confirmed the diagnosis of Necrobiosis Lipoidica, characterized by epidermal rete ridge atrophy without epidermal layer attenuation, dense dermal fibrosis, perivascular inflammatory cell aggregates in the superficial to mid-dermis, and degenerating collagen without mucin deposition. We treated our patient with a regimen of clobetasol 0.05% ointment nightly with occlusion and one month later, there was an improvement in the appearance of his plaques. Complete resolution in our patient remains to be seen.
Necrobiosis Lipoidica (NL) is a rare granulomatous skin disorder that has been associated with diabetes mellitus (DM). The pathogenesis of NL remains unclear but is thought to be related to vascular disturbances involving immune complex deposition or microangiopathic changes secondary to glycoprotein deposition, leading to collagen degeneration. This may explain its association with DM. NL is often specifically associated with type 1 DM, as in our pediatric patient, though cases in type 2 DM and non-diabetic individuals have been reported. It predominantly occurs in middle-aged females and presentation in pediatric patients, especially pediatric male patients, is very rare. NL typically manifests as red-pink and yellow annular plaques with red-violaceous borders and atrophic, telangiectatic centers on the extremities. This entity in pediatric patients can be mistaken for granuloma annulare, a more common condition in children, and this occurred in our patient’s case. One of our case’s unique features was the scaly red papules in a linear array, which could possibly indicate Koebnerization.
No standardized guidelines exist for NL management, but topical and intralesional corticosteroids are common initial treatments. Whether NL is associated with prognosis or severity of DM remains unclear, though some studies have demonstrated that NL may be associated with increased diabetic complications. Some studies have also shown that improved glycemic control can lead to improvement in NL. Further research is needed to establish optimal management protocols for this rare pediatric manifestation of NL.
#166
Ski and snowboard injury patterns in the United States from 2010 to 2020 in pediatric patients
Dea M, Zapata I. Rocky Vista University, Parker, CO
Purpose of Study: The objective of this study is to perform a nationwide analysis of pediatric skiing and snowboarding injuries to identify patterns regarding patient demographics, type of injuries, outcomes, and admission rates.
Methods Used: This was a retrospective cohort study of publicly available data. Cases were sourced from the National Electronic Injury Surveillance System (NEISS) from 2010 to 2020 and included 6421 incidents.
Summary of Results: Even when the highest percentage of injuries was the head at 19.30%; the diagnosis of concussion was placed third while fractures were the most common diagnosis at 38.20%. The proportion of pediatric incidents by hospital type is changing with children’s hospitals currently managing the majority of cases.
Conclusions: These findings can assist clinicians in the ED across different hospital types in understanding the patterns of injury to be better prepared for new cases.
#167
Assessment of Food Skills for Families with Children with Chronic Kidney Disease: A Novel Approach
Cushing M2, 1, Gibson K1, Walch A1. 1University of British Columbia, Vancouver, BC, Canada and 2BC Children’s Hospital, Vancouver, BC, Canada
Purpose of Study: This study aims to determine if a series of 3 virtual cooking classes for families with children with Chronic Kidney Disease (CKD) improves their food skills. This is important because in children with CKD, optimal nutrition usually requires strict control of sodium, potassium, and phosphorus. However, these nutrients are found in high amounts in processed foods, which families increasingly rely on for reasons including convenience, cost of fresh ingredients, taste, time, and lack of cooking abilities. Excessive consumption of sodium, potassium, and phosphorus can cause high blood pressure, heart and muscle problems, bone and mineral disorders, and progression of kidney disease.
Interventions aimed at strengthening cooking skills have been shown to result in higher consumption of fruits and vegetables, as well as reduced reliance on highly processed foods. Virtual cooking classes may help families provide a more suitable diet for their child with CKD, improving disease management and quality of life.
Methods Used: Eligible participants are families of patients aged 1-20 who attend the Chronic Kidney Care Clinic (CKCC) at British Columbia’s Children’s Hospital. Participants were recruited via email using the CKCC clinic database. Once consented, participants were invited to attend 3 Zoom sessions, each 2 hours long, that demonstrate approachable, kidney friendly recipes which families can cook alongside at home.
Participants complete the Food Skills Questionnaire (FSQ) before and after the cooking classes. The FSQ is a comprehensive tool for assessing food skills in individuals or groups with basic food skills. It has been shown to have strong content validity, face validity, and test-retest reliability. Pre- and post- intervention scores will be compared using a paired t-test to determine if there is a significant difference in food skills.
Summary of Results: It is anticipated that virtual education is an acceptable, and sometimes even preferred, mode of delivery. It is hypothesized that cooking sessions will result in significant improvements in food skills for families with children with CKD.
Conclusions: Given the significant dietary modifications needed for a child with CKD, home cooking skills are paramount. However, the challenges associated with food planning, preparation, and kidney-friendly diet modifications can be daunting and time consuming for families.
If this approach demonstrates that virtual cooking sessions are well received and produce a meaningful difference in the food skills of families, additional cooking demonstrations could be created. Future videos could cover a broader range of dietary needs in the CKD community, such as individuals who have received a kidney transplant or are starting home blenderized tube feeds.
To our knowledge, the use of virtual cooking classes is a novel approach to CKD management in the pediatric population. This represents an important advancement in empowering families with more autonomy and food skills to help manage their child’s CKD.
#168
BUILDING SUSTAINABILITY IN GLOBAL HEALTH EDUCATION PROGRAMS: DEVELOPMENT AND IMPLEMENTATION OF A TRAINING-OF-TRAINERS MANUAL IN RURAL NEPAL
Ho A, Bondy S, Kong P, Cunningham J, Chambers A, Loughton S, Nakajima L, Kapoor V. University of British Columbia, Vancouver, BC, Canada
Purpose of Study: The Tharu people are an indigenous group located in the Terai region of rural Nepal with a long history of bonded labour and persistent health inequities. Since 2020, the Nepal Sexual and Reproductive Health (SRH) Project has partnered with local non-profit organization, Creating Possibilities (CP) Nepal, to develop the Adolescent Health Program. Taught by local educators, the program is a 10-session curriculum encompassing topics ranging from puberty, menstruation, and reproduction to child marriage and gender equality. The program was initially piloted in a subset of 65 girls and optimized to facilitate expansion. To date, over 600 girls have completed the Adolescent Health Program. It has been well-received, with interest from nearby governments and communities for further expansion. To ensure consistent and sustainable delivery of the program as it continues to grow, a Training-of-Trainers (ToT) manual was created in collaboration with CP Nepal to serve as a teaching guide for new and current educators.
Methods Used: Similar to the development of our initial curriculum, topics included in the ToT manual are based on learning objectives outlined in the International Technical Guidance on Sexuality Education (ITGSE) commissioned by UNESCO. References used to further guide content include YUWA Nepal Comprehensive Sexuality Education Booklet, KidsHealth, and United Nations Population Fund (UNFPA). To ensure comprehensibility and cultural appropriateness, the manual was reviewed in its entirety with our Lead Educator during an on-site visit in Nepal this year. The finalized manual has been translated into Nepali by CP Nepal staff and is currently being piloted with new groups of students in the program. Initial feedback on the ToT manual has been gathered through discussions with educators.
Summary of Results: The ToT manual has been popular amongst educators, viewed as a helpful content and organizational tool in the classroom. Features such as a suggested schedule for each lesson, key diagrams, and recommended learning activities have been found to be particularly helpful. Feedback from educators and students continues to be gathered, with plans to update the manual on a biennial or triennial basis. The ToT manual ensures standardized program delivery, which will allow future studies to assess its impact.
Conclusions: Collaboration with community members and local organizations is crucial in establishing a successful global education program. Tools such as a ToT manual are key in ensuring consistency and sustainability of programs, particularly as they expand. Optimization of the program based on feedback from educators and students ensures that community needs continue to be addressed in a culturally-appropriate manner. Future directions of the project involve implementation of a mixed-methods study to formally investigate the impact of the program and areas of further development.
#169
DEVELOPMENT OF AN ADOLESCENT MENTAL HEALTH LITERACY NEEDS ASSESSMENT IN RURAL NEPAL
Kong P, Bondy S, Ho A, Cunningham J, Chambers A, Loughton S, Nakajima L, Kapoor V. The University of British Columbia, Vancouver, BC, Canada
Purpose of Study: Nepal currently grapples with a severe mental health crisis, marked by the second-highest adolescent suicide rate in South East Asia and limited mental health infrastructure (only 2.1 physicians per 10,000 people). This crisis disproportionately impacts rural adolescents, particularly young girls who face gender-based inequities. In partnership with Creating Possibilities (CP) Nepal, we launched an Adolescent Health Program (AHP) with the initial goal of delivering sexual and reproductive health education to Indigenous Tharu communities in rural Nepal. CP Nepal has since identified a pressing need for mental health education within these communities. In response, we are conducting a needs assessment among program participants to 1) assess the current level of mental health literacy (MHL) and 2) inform the development of a culturally-sensitive mental health module.
Methods Used: The needs assessment survey was developed through a review of the literature to understand the mental health landscape in Nepal and build upon validated measures assessing adolescent MHL in similar populations. We followed a Community-Based Participatory Research (CBPR) approach, tailored to actively engage community members, stakeholders, and researchers throughout the needs assessment process. We collaborated closely with CP Nepal and consulted over 100 girls from 5 school groups in the Dang district during our on-site visit this year. This informed the creation of an initial draft survey, which we further refined iteratively with input from our local partners to ensure its relevance and effectiveness in addressing the community’s mental health needs. The finalized survey was translated into Nepali by CP staff.
Summary of Results: We based our survey on a review of 9 relevant studies, especially drawing from Campos et al.’s Adolescent MHL Questionnaire. Local partner feedback fell into five categories: ’Self-help strategies,’ ’Alcohol-use disorder,’ ’Mental healthcare infrastructure,’ ’Suicide and self-harm,’ and ’Traditional perceptions towards mental health,’ guiding cultural adjustments as summarized in Table 1. The final survey consisted of two parts: one gathering socio-demographic data and the other containing 64 items rated on a three-point Likert response scale (1=disagree, 2= neither agree nor disagree, 3=agree). These items covered five sections: [1] mental health knowledge (including specific disorders), [2] beliefs and stereotypes, [3] first aid skills and help-seeking behaviors, [4] self-help strategies, and [5] curriculum delivery preferences. Local AHP facilitators are currently adminstering the survey among two classes of girls grades 6 to 12.
Conclusions: The CBPR approach fosters culturally sensitive research, empowers communities, and promotes sustainable, community-driven solutions to mental health challenges. Ongoing collaboration with local partners is vital to address mental health literacy gaps and rising suicide rates, guided by formal needs assessments for program development.
Outcomes of Partner Engagement.
Categories
Examples
Self-help strategiesDuring conversations about resilience and self-help strategies, cultural traditions like music and dance were frequently mentioned as common strategies.
We included the following survey items:•“Doing something enjoyable helps to improve mental health.”•“Engaging in hobbies or creative activities helps to improve mental health.”•“Writing in a journal or expressing my thoughts and feelings through creative outlets (such as art or music) can be a helpful coping strategy for me.”
Alcohol-use disorderHighlighted by our partners as a significant concern within the community, especially in conversations about domestic violence.
We included the following survey items•“Drug addiction (e.g. alcohol or opiates) may cause mental disorders.”•“Drinking alcohol, especially in large quantities, can worsen pre-existing mental disorders.”•“When someone is unable to sleep, drinking alcohol can help them to sleep better.”
Mental healthcare infrastructureIn Dang, healthcare is primarily provided through local health posts and community-based organizations/NGOs, with limited access to psychiatrists and counselors. Mental healthcare infrastructure, including counselors, psychiatrists, and psychologists, is notably lacking.
We included the following survey items:•“If I had a mental disorder, I would seek help from the local health post.”
•“If I had a mental disorder, I would seek help from a community based organization (CBO) or non-government organization (NGO).”
•“The number of people with mental disorders is low in our country.”
•“If I had a mental disorder, I would seek help from a spiritual doctor.”
Suicide and self-harmDuring our on-site visits, some girls mentioned that they might consider suicide as a potential option if they were to become pregnant before marriage, citing feelings of shame and concern about social stigma.
We included the following survey items:•“If I were to become pregnant before marriage, I would consider suicide as an option.”•“Self-harm is a behavior people engage in for attention-seeking purposes.”
Traditional perceptions towards mental healthThere are prevalent traditional beliefs attributing mental illnesses to supernatural powers or being cursed by evil spirits.
We included the following survey items:•“Mental disorders are caused by a supernatural power and are the result of a curse by evil spirits.”•“Marriage can heal mental disorders.”•“Mental disorders, once acquired, are life long.”•“There is no effective treatment available for people with mental disorders.”
#170
TRANSITION OF CARE FROM INPATIENT TO OUTPATIENT SETTING: PERSPECTIVES OF PARENTS ABOUT ASTHMA ACTION PLAN
Mazloom K1, 2, Chin D1, 2, Nguyen-Tang H1, 2, Afghani B1, 2. 1UC Irvine School of Medicine, Orange, CA and 2Children’s Hospital of Orange County, Orange, CA
Purpose of Study: Asthma action plans are used to help families manage a child’s asthma and prevent admission to the hospital. However, the details of the asthma action plan and how it is presented to the families differ among providers. This lack of standardization may result in inadequate asthma education which can result in readmissions to the hospital. The goal of this study was to review the parent’s understanding of their child’s diagnosis of asthma and their perspective on how the asthma action plan can be improved.
Methods Used: An anonymous survey via REDCap was distributed to parents at Children’s Hospital of Orange County on the day of discharge from the hospital after the asthma action plan was reviewed. This survey asked questions to gauge a parent’s understanding of their child’s asthma diagnosis, tested parent’s knowledge on what to do during an acute exacerbation, and asked what barriers prevent parents from providing adequate asthma care for their child at home. Parents were also asked how they would improve the asthma action plan to make it easier to understand.
Summary of Results: Of the 18 parents approached, all responded to our survey. More than half (56%) of the parents belonged to a minority ethnic background and half of the parents had a college or more advanced degrees. Of the respondents, 17%, 17%, and 11% reported that their child had intermittent, mild persistent, or moderate asthma, respectively, and 28% said it was their child’s first time being diagnosed with asthma. Despite of severity documentation on asthma action plan, 28% were unsure of their child’s level of asthma severity. Surprisingly, 60% of those who were unsure reported that their child had been admitted to the hospital previously for asthma. When parents asked if they had a thorough understanding of the green, yellow, and red zones on the asthma action plan, 33% of parents strongly disagreed. Of the 11 patients who required a daily inhaled corticosteroid, 45% of parents reported that they would not use the controller on a daily basis. When given a severe asthma exacerbation clinical scenario, 33% of parents answered that they would not take their child to the emergency room. Parents opinions on what could be done to enhance the asthma action plan included: making it easier to understand, incorporating more detailed steps, simplifying it, adding pictures, and having a less complicated version for the child. Barriers to caring for the child’s asthma at home included: difficulty obtaining medication and the cost of medication. Limitations of this study include small sample size and the lack of its generalizability since it was done in a single institution.
Conclusions: Our preliminary study suggests that significant gaps exist in caregiver’s understanding of management of their child’s asthma. Larger multicenter studies that consider various social determinants of health are needed to evaluate specific barriers. Patient-centered approach that recognizes individual barriers are needed when reviewing asthma action plans.
#171
HARNESSING COMMUNITY STRENGTHS: STRATEGIES FOR SUICIDE PREVENTION IN ANACONDA, MONTANA
Beach KT, Keys T. University of Washington School of Medicine, Seattle, WA
Purpose of Study: Anaconda, Montana, county seat of Anaconda-Deer Lodge County (population 9,421), is a rural town in southwest Montana with a rich history. Once a booming town with thousands of jobs at the smelter, Anaconda now has an aging population without work and a small adolescent population without much to do. Suicide prevention surfaced as a pressing concern after discussion with local mental health providers and local health department staff. The number of deaths by suicide in the county is 4.9 per 10,000 people, which dwarfs the national average of 1.4 and is almost double the statewide average of 2.6 deaths per 10,000 people.
Methods Used: Conversations with the county health department revealed that the national 988 lifeline resource was underutilized and undermarketed in the county. People in crisis have few options, namely going to the emergency department or to the state-run mental health hospital. Since the wait to see a psychiatrist is months long, it was important to leverage other resources. A review of literature highlighted how effective suicide prevention involves intervening at both the individual and community level. Studies also show that more than three-quarters of individuals who die by suicide visited their primary care provider in the past year; thus, utilizing relationships with providers would be key in any intervention.
Summary of Results: In partnership with local psychiatrists, the researcher created two brochures that detailed options for people in crisis, both for adult and adolescent audiences. Following local printing, the brochures will be delivered in September 2023 to clinics, the health department, schools, and other community organizations. Both brochures have a safety plan template on the back to be completed with a physician, family member or close friend. Having physical documentation to turn to helps with one’s mental processing in crisis and may offer legal protection for care providers. The front of the adult brochure has the 988 lifeline and Montana Warmline contact information. These resources are staffed by Montanans, an important factor as Anaconda residents strongly associate with their rural community. The adolescent brochure has information for the 988 lifeline and the Trevor Project, which is crisis support tailored to LGBTQ+ youth. The brochures reference the Anaconda Suicide Prevention Taskforce on Facebook, where one can access additional mental health resources.
Conclusions: By incorporating stunning nature photos taken by a local photographer on the brochures and the Anaconda Suicide Prevention Taskforce Facebook page, this intervention builds on existing strengths of the Anaconda community. Physicians and local community members can easily access the brochures in multiple locations around town. The brochures list established national and statewide crisis support organizations, reducing the need for frequent updates. Providing resources for people in crisis aligns with the broader health department goal to expand mental health support in the county.
#172
The Effect of Reflective Writing and Breastfeeding on Self-Efficacy Scores
Estafanous M, Lorson R, Son S, Maidan A, Thomas A, Hart E. Loma Linda University, Loma Linda, CA
Purpose of Study: - The purpose of this study is to analyze the impact of a qualitative writing intervention on self-efficacy scores of mothers in the immediate postpartum period and how this relates to breastfeeding.
- Breastfeeding is known to have a multitude of physical and psychological health benefits to both the mother and baby, such as lower risk of diabetes and obesity as well as better mood and stress reactivity in mothers (Section on Breastfeeding, Eidelman et al., 2012; Krol & Grossmann, 2018).
- Engaging in reflective writing, as compared to writing about superficial or mundane topics, has been associated with lower scores of depression, anxiety, and stress scales (Epstein et al., 2005).
- To the authors’ knowledge, no study has yet examined the role that reflective writing may have on new mothers’ self-efficacy.
Methods Used: - This was a randomized control trial that implemented a reflective writing exercise on postpartum day 1.
- Prompt: “Consider a time when you struggled to accomplish something and succeeded in the end. This could be a goal you set for yourself or one that was assigned to you or expected of you. What was difficult about the circumstance? What did you tell yourself to help you get through it? What actions did you take to help yourself overcome it? How did it make you feel to overcome the challenge?”
- On postpartum day 1 and week 6, all participants in the intervention and control groups completed three questionnaires assessing self-efficacy and growth mindset.
- Participants were assessed for rates of breastfeeding at postpartum week 6.
Summary of Results: - There was a statistically significant increase in self-efficacy survey scores from postpartum day 1 and postpartum week 6 for both the intervention and control groups (p < 0.05).
- This effect was the greatest in mothers who were exclusively breastfeeding at week 6 (p < 0.05). Within this subset, the effect was even greater for those in the intervention group (p < 0.01).
*Higher scores equate to higher levels of self-efficacy
Conclusions: - Self-efficacy scores increased in mothers from postpartum day 1 to week 6.
- This impact was more pronounced in mothers who were exclusively breastfeeding at week 6 and, even more so, those who engaged in reflective writing.
- The findings of this study suggest that mothers’ self-efficacy is malleable in the immediate postpartum period.
- Further research is needed to elucidate additional methods to bolster new mothers’ self-efficacy.
#173
Perspectives of Local Experts and Students on the Mental Health of Bhutanese Youth and Young Adults
Siu C1, Hsiao H1, Lam G2, 1, Kapoor V1. 1University of British Columbia, Vancouver, BC, Canada and 2BC Children’s Hospital, Vancouver, BC, Canada
Purpose of Study: Bhutan is known for implementing Gross National Happiness in place of GDP as a guiding philosophy, representing the collective wellbeing of its population. However, mental health issues persist as an increasing public health concern in Bhutan, with suicide as the sixth leading cause of death and a significant proportion occurring in youth and young adults (YYA). The COVID-19 pandemic has introduced additional challenges to mental health, such as isolation and unemployment. A qualitative assessment of local perspectives on mental health may help inform the development of resources and programs that are relevant and effective.
Methods Used: Four focus groups were conducted, involving six mental health experts and two university students, aged 18-25, in Thimphu, Bhutan. Participants were recruited via email and WhatsApp. Focus group questions were developed in collaboration between Bhutanese and Canadian stakeholders to ensure cultural sensitivity. Discussion topics included perspectives on mental health and wellbeing, strategies and resources used for resilience building, and the impacts of familial dynamics, domestic and gender-based violence, and COVID-19 on mental health. Focus group dialogue was transcribed and analyzed for common themes.
Summary of Results: Common influences on mental health identified by local experts and students alike included familial relationships and support, openness of family and peers to discuss mental health, and childhood experiences. Gender-based violence and stigma were recognized as rising issues that negatively affect YYA in the LGBTQ+ community. The majority of interview participants also identified stigma against mental illness as prevalent in their society. Discrimination and neglect from society and family were recurrently recognized as attitudes towards individuals with mental illness. These attitudes were seen as more predominant in older populations. Interview participants shared perceived causes of suicidal ideation, which included lack of familial support, economic difficulty, and insufficient mental health resources. Multiple participants emphasized the latter in rural settings. Participants described significant effects of the COVID-19 pandemic affecting mental health by inducing isolation, unemployment, and anxiety. Strong agreement was noted over the need for education and awareness surrounding mental health and increased access to resources, such as counselling.
Conclusions: Perceptions shared by local experts and university students highlighted common factors affecting mental health in YYA, including familial support and openness. Societal stigma was recurrently identified as a challenge to YYA with mental illness. The compounding effects of COVID-19 on mental health were also highlighted. There is an identified need to improve access to education and resources to support those with mental illness in both rural and urban settings.
#174
INTERVENTIONS IN THE NICU FOR FATHERS/PARENTING PARTNERS COPING AND BONDING WITH BABY: A SCOPING REVIEW
Solness C, Huber K, Casler C, Starzyk D, Dempsey AG. University of Colorado, Denver, CO
Purpose of Study: Parents are an important part of a NICU admitted infant’s care team with research showing that parent psychosocial well-being is linked to both short and long term infant developmental outcomes and parent-infant attachment. Research has documented the stressful and sometimes traumatic nature of the NICU as well as the need for interventions addressing parent well-being, however, there is a paucity of intervention research focused on fathers. The majority of studies focus solely on the mother, others focus on parents more generally, often with fathers under-represented. Therefore, the purpose of this scoping review is to map the breadth of literature addressing psychosocial and attachment-related interventions for fathers in the NICU. This review will provide a comprehensive overview of how well fathers are included in the literature, what methodologies are most prevalent, what types of interventions have been documented, what outcomes are being prioritized, and where there are gaps and needs still to be addressed for this population.
Methods Used: Methodology for this scoping review is following the Johanna Briggs Institute Manual for Evidence Synthesis. A team of three coders working in pairs independently coded citations for inclusion/exclusion before meeting to come to consensus. Data is being managed in EndNote and Excel
Summary of Results: A comprehensive literature review was conducted across Cinahl, PsychInfo, Embase, and PubMed, producing an initial list of 1722 citations. After removing duplicates, books, non-primary/secondary research, methodological articles, and non-NICU samples, 899 remaining titles/abstracts were coded based on the following criteria: fathers sample, presence of an intervention or father-focused without an intervention, and adult-focused outcomes (qualitative or quantitative), generating 41 father-only articles. Within these, 30 were non-intervention research and 11 were interventions consisting of 7 quasi-experimental, 2 reviews, 1 experimental, and 1 unclear design. Within the intervention category, outcomes measured included: fathering ability, attachment, support of the mother, and paternal mental health with stress and attachment being the most commonly named outcomes. Coding for this project continues as an additional 1239 citations have been pulled from the reviews and meta-analyses for coding. By the time of the conference we expect to have completed this coding and anticipate being able to report preliminary results of the data extraction process
Conclusions: Given the impact of fathers on child outcomes, future intervention research should focus on outcomes beyond stress to address depression, anxiety, trauma and attachment. This scoping review is a call to action to NICU providers and researchers to address the needs of the fathers which ultimately addresses the needs of the infants and families.
#175
Psychological interventions of virtual gamification within academic intrinsic motivation: A systematic review
Xu J2, Dhaliwal H1. 1McMaster University, Hamilton, ON, Canada and 2David Geffen School of Medicine, Los Angeles, CA
Purpose of Study: The purpose of this systematic review was to assess the effectiveness of virtual gamification methods in enhancing student intrinsic motivation and engagement in independent cognitive tasks. Rather than assessing all gamification techniques, this systematic review focused on the efficacy of virtual techniques, which can be integrated into a virtual application for greater global accessibility.
Methods Used: A systematic review was performed to determine the influence of virtual gamification integration on student motivation within academia. The objective of this systematic review was to search available literature to identify effective gamification techniques. Chosen interventions from this systematic review will yield potential features on the Felicity app after screening, extraction, and quality appraisal of data in present literature.
Summary of Results: This review provides a comprehensive examination of current literature regarding the effect of gamification on student intrinsic motivation in an academic setting. Generally, gamification is associated with increases in intrinsic motivation, which was recorded by observational, self-report, data analysis, or systematic review measures. The literature demonstrated this relationship, although there was variation in the presence and level of motivational improvement. Gamification methods reinforced extrinsic motivation through the implementation of points, badges, and leaderboards, to strengthen individual intrinsic motivation.
Conclusions: Points, badges, and leaderboards were found to be the most effective media for using gamification to grow intrinsic motivation. 35 studies used points, leaderboards, and badges in cumulation to reinforce motivation and enhance self-efficacy. These interventions also foster positive competition and acknowledge individual achievements, which collectively inspires students to participate in and complete more activities. The level of student engagement with respect to task completion rate was also higher when utilizing gamified platforms, compared to the non-gamified condition.
Structural diagram of the screening and study selection processes completed.
#176
EFFECTS OF HEAD TRAUMA FREQUENCY AND INTENSITY ON FOOTBALL PLAYERS IN HIGH, MODERATE, AND LOW CONTACT POSITIONS
Tsushima W1, Yamamoto H2. 1Straub Medical Center, Honolulu, HI and 2UCLA, Los Angeles, CA
Purpose of Study: Research suggests a possible link between the intensity of head impacts and repetitive high-intensity head injuries in young football players and decreased cognitive capacity and increased symptoms. This study investigated the effects of head impact intensity and frequency on the neuropsychological test results of high school football players.
Methods Used: Based on the biomechanical measures of head impact frequency reported in high school football, a High-Frequency, Low-Intensity group (n = 403) consisting of offensive and defensive linemen, a Moderate-Frequency, Moderate-Intensity group (n = 236) consisting of linebackers, running backs, and tight-ends, and a Low-Frequency, High-Intensity group (n = 414) consisting of cornerbacks, quarterbacks, defensive backs, safeties, and receivers, were compared[SA1] . The three groups were compared in terms of their scores on the Immediate Post-Concussion Assessment and Cognitive Testing (ImPACT) using linear analysis and a Kruskal-Wallis test.
Summary of Results: The results showed that the Low-Frequency High-Intensity group performed worse than the Moderate-Frequency Moderate-Intensity, and High-Frequency Low-Intensity groups on the ImPACT on two Composite scores (Visual Motor Speed, Reaction Time). No differences were found across the three groups in the other Composite scores of the ImPACT.
Conclusions: The current study is the first to date to report differences in athletes’ performance on neuropsychological tests when engaging in various contact positions. These findings may suggest that frequency findings could suggest that intensity is more impactful than frequency when looking at the effects of head trauma.
#177
Frequency of Negative Adult Spectator Behavior at Youth (11-14 y/o) Sporting Events
Yung MY, Rooks EA, Chen R, Maarat S, Doyle R, Yamamoto LG. University of Hawaii John A. Burns School of Medicine, Honolulu, HI
Purpose of Study: This study aims to determine the frequency of negative adult spectator behavior at youth sporting games for 11-14 year-olds and compare the frequency of different negative behaviors across four sports. This study is an extension of previous research in 6-10 year-olds.
Methods Used: Investigators attended 27 youth sporting events in Central Oahu, Hawaii from January 2022 through September 2023. Participants were between the ages of 11 to 14 years old and were of both sexes. Investigators observed baseball, basketball, soccer, and flag football games for 45 minutes each. The frequencies of negative adult spectator behavior events such as alcohol use, smoking, swearing, and negative language, were recorded. The number of spectators and players was recorded as well. Observed events were discussed between researchers and then recorded on a standardized data sheet. A one-way ANOVA was performed to compare the mean incidence of negative adult spectator behavior at different sports games.
Summary of Results: We found baseball had the highest mean incidence of total negative adult spectator behavior with a mean of 5.2 incidences, 95% CI [8.25, 2.14] per game. Basketball had 2.6 incidences, 95% CI [4.79, 0.41], football had 0.9 incidences, 95% CI [1.33, 0.47], and soccer had 0.5, 95% CI [1.19, -0.19] as shown in figure 1. The error bars on the graph indicate 95% CIM. There was a significant difference between the total mean incidence of negative behavior at baseball games compared to football and soccer (p-value = 0.035). There was no significant difference between baseball and basketball. Alcohol consumption was only observed at baseball games (mean incidence = 2.2), and smoking and vaping were only observed at baseball (mean incidence = 0.6) and football (mean incidence = 0.5) games. There was no significant difference between the incidences of swearing or negative language behavior across all sports.
Conclusions: Our study found that children are exposed to varying amounts of undesirable adult behavior at youth sporting events. These preliminary results indicate that more negative behavior occurs at youth baseball and basketball games. There may be significant differences in the type of negative behavior displayed at different forms of youth sporting events, but a larger sample size is needed to clarify preliminary trends. This ongoing investigation may indicate a need for adult behavior regulation at youth sporting events.
#178
Constipation-Induced Delirium
Deemer, E2, Zahid M2, Quillatupa N1. 1Kern Medical Center, Bakersfield, CA and 2Kern Medical Center, Bakersfield, CA
Case Report: Delirium affects approximated 30% of inpatient geriatric patients. Delirium increases likelihood of institutionalization, higher mortality, longer hospital stays, and complications.1,3 One known preventable causes of delirium in older patients is constipation. The prevalence of constipation in the geriatric population is estimated at 50%.2 Constipation can result in delirium and manifests as dehydration or nausea, with eventual progression to fecal impaction.2 In the inpatient setting, early diagnosis and treatment of constipation can decrease duration and incidence of preventable delirium.
Patient is a 79-year-old male with history of Parkinson’s dementia, hypertension, and type 2 diabetes mellitus, who presented to clinic for “being disoriented.” Patient suddenly required diapers and occasionally forgetting how to dress himself. Also, patient endorse urinary retention so, urinalysis and retroperitoneal ultrasound were ordered and negative. Upon follow-up, patient having worsening symptoms, such as walking into walls. Patient eventually taken to the emergency department but, imaging and labs are within normal limits. Patient was discharged with diagnosis of new onset dementia. Daughter reports patient is still confused. Physician ordered labs, MRI, and abdominal radiographs. MRI brain with and without contrast and labs are within normal limits. Abdominal radiographs show moderate constipation with no sign of bowel obstruction. Daughter reports patient has not had a bowel movement for 3 days, despite using suppositories. Increased bowel regimen to senna and Miralax twice a day, with goal to achieve at least 2 bowel movements per day for 3-4 days. Follow-up revealed patient’s mentation returned to baseline.
Constipation-induced delirium is a common diagnosis seen within geriatric medicine, but it is not well known amongst general physicians. Due to the COVID-19 pandemic, the patient was unable to attend in-clinic geriatric medicine appointments. As seen in this case, misdiagnosis in the emergency department delayed this patient’s treatment. Patients with delirium have been found to have twice the 30-day mortality rate, and 1.2-fold higher 30-day readmission rate as compared to patients without delirium.4 Misdiagnosis of delirium with dementia in elderly patients can be avoided by using the CAM screening tool.5 The diagnosis and treatment of constipation is low-cost with relatively swift results. Constipation can be managed with pharmacological or non-pharmacological methods, depending on what is most suitable to the individual patient, and should be considered in all delirious patients. Adequate training to diagnose delirium for all physicians could improve patient outcomes.3
Ultimately, this patient case illustrates the importance of prompt diagnosis and treatment of constipation in the setting of delirium. Since prompt treatment can lead to decrease hospital stays, unnecessary diagnostic tests, and even mortality.
Bowel regimen: senna and Miralax with goal for 2 bowel movements every day for 3-4 days
06/19/2020
Telephone visit
Patient at baseline.
#179
AIR POLLUTION AS AN ENVIRONMENTAL STRESSOR IN THE PATHOGENESIS OF CARDIOVASCULAR DISEASES: A REVIEW OF THE UNDERLYING PATHOPHYSIOLOGICAL MECHANISMS
Ahmed Z, Agrawal DK. College of Osteopathic Medicine of the Pacific, Western University of Health Sciences, Pomona, CA
Purpose of Study: Outdoor air pollution is a major public health concern and a significant contributor to the morbidity and mortality in cardiovascular diseases (CVDs). The World Health Organization reported that 99% of the global population resides in locations with sub-optimal air
quality. We critically reviewed the effects of air pollution as an environmental stressor in the underlying pathogenesis of CVDs with an emphasis on mitigation measures.
Methods Used: A literature search following PRISMA guidelines was conducted using PubMed and Google Scholar to critically review the 110 selected peer-reviewed full-length articles in the English language, based on the keywords, published in the last 15 years.
Summary of Results: Air pollutants contain ultrafine (<0.1 μm in diameter particulate matter (PM)), fine (2.5 μm PM), and coarse (10 μm PM) particles loaded with transition metals, pyrogens that induce oxidative stress, vapor-phase compounds, ozone, nitric oxide, benzene, carbon monoxide, and other gases. Ultrafine particles and gases are the most toxic to the cardiovascular system due to their enhanced alveolar penetration, reaching systemic circulation, causing oxidant/antioxidant imbalance inducing oxidative stress and inflammation, activation of central sympathetic mechanisms, stress hormone signaling, abnormal calcium signaling, reduction in vascular nitric oxide leading to endothelial dysfunction, pro-thrombotic events, enhancing atherosclerotic plaques, to develop hypertension, ischemic heart disease with increased plaque vulnerability and acute coronary syndrome, arrhythmia, heart failure, and cerebrovascular disease. Short-term and long-term exposure to air pollutants increases all-cause mortality and cardiovascular mortality. Climate change modifies the degree of air pollution and contributes to global warming to adversely affects cardiovascular health. Air pollution particles alter circadian gene expression, including BMAL1, CLOCK, periods, cryptochromes, altering lipid metabolism and triggering CVDs. The recommended mitigation strategy of using face masks and N95 respirators reduces health risks but might engender a false sense of security to certain populations. However, outdoor physical activity has clear benefits even when exposed to low and moderate PM concentrations. Indeed, the lowering of allowed emission levels and thus improving air quality will be the most promising mitigation strategy.
Conclusions: Air pollution confounded with factors, such as climate change, noise, smoking, and sedentary life, triggers a chain of cellular and molecular events in the pathophysiology of cardiovascular diseases to aggravate the disease burden. We, as health professionals, have the responsibility to increase awareness of environmental stressors, and develop better and more effective preventive and treatment measures by creating guidelines, advocating for enhanced resources in the teaching, education, and research of the adverse effects, to reduce morbidity and mortality in cardiovascular diseases.
#180
Long Term Outcome of Isolated First-Year C1q Positive Donor Specific Antibodies After Heart Transplantation
Wakefield Z, Bhatnagar N, Kanungo A, Hamilton M, Kobashigawa J. Cedars-Sinai Smidt Institute, Los Angeles, CA
Purpose of Study: Detection of donor specific antibodies (DSA) after heart transplantation (HTx) has been associated with poor outcome in the long term. DSA have been associated with decreased survival, increased incidence of cardiac allograft vasculopathy (CAV), increase in cardiac dysfunction, and increase in non-fatal major adverse cardiac events (NF-MACE). DSA are heterogeneous and can be detected by the Luminex assay. Functional studies indicate whether the DSA can cause killing by the ability to bind complement. It has not been established whether these complement-binding (C1q+) antibodies have increased risk for poor outcome after HTx.
Methods Used: Between 2010 and 2018, we identified 18 HTx patients who were found to have DSA C1q+ antibodies (with normal LV function, LVEF>50%) in the first year after transplant. These patients were compared to a control (case matched) group (n=18 patients) who were DSA C1q-.Study endpoints included 5-year survival, freedom from CAV (≥30% stenosis by angiography), freedom from NF-MACE (myocardial infarction, new congestive heart failure, percutaneous coronary intervention, pacemaker/implantable cardioverter defibrillator placement, stroke), freedom from cardiac dysfunction (left ventricular ejection fraction ≤40%) and 1-year freedom from acute cellular rejection (ACR) and antibody-mediated rejection (AMR).
Summary of Results: The patients who developed DSA C1q+ compared to DSA C1q- had significantly lower subsequent 1-year freedom from AMR and lower 5-year freedom from CAV. Between study groups, there were no significant differences in subsequent 1-year freedom from ACR, 5-year survival and freedom from NF-MACE.
Conclusions: The development of C1q+ donor-specific antibodies after HTx is associated with more subsequent 1-year AMR and more 5-year CAV. Treatment of DSA C1q+ may be warranted to prevent these downstream complications.
DSA C1q+(n = 18)
DSA C1q-
(n = 18)
P-value:
Subsequent 1-year freedom from ACR (ISHLT ACR ≥ 2R)
94.4%
100%
0.317
Subsequent 1-year freedom from AMR (ISHLT pAMR ≥ 2)
50.0%
88.8%
0.004
Subsequent 5-year survival
77.8%
83.3%
0.494
Subsequent 5-year freedom from CAV
77.8%
100%
0.019
Subsequent 5-year freedom from NF-MACE
77.8%
83.3%
0.462
#181
Does Targeting Lower Levels of Tacrolimus Make a Difference After Heart Transplantation?
Bhatnagar N, Kanungo A, Hamilton M, Kobashigawa J. Cedars-Sinai Heart Institute, Los Angeles, CA
Purpose of Study: Immunosuppression after heart transplantation is not standardized. The use of calcineurin inhibitors (CNI) such as tacrolimus is the cornerstone of immunosuppression with an additional antiproliferative agent and corticosteroids added. Tacrolimus is by far the most common calcineurin inhibitor medication used by heart transplant programs. In most heart transplant programs, the target tacrolimus trough level is between 10 to 15 ng/ml for the first three months up to the first six months after heart transplantation. In our large single center program, we target for lower tacrolimus levels, which would include level 10-15 ng/ml in the first month, decreasing to 8-12 ng/ml in the second month, and after the third month, to 5-10 ng/ml. It is not known if targeting this lower tacrolimus level is safe and whether it does actually decrease adverse effects in the first six months after transplantation.
Methods Used: Between 2010 and 2019 we assessed 88 Hx patients in our program who had these lower target levels of Tacrolimus as noted above. These patients were compared to the TAC/MMF group in the recent multicentered trial, Tacrolimus with Mycophenolate Mofetil or Sirolimus vs. Cyclosporine with MMF (*Am J Transplant. 2006;6(6):1377-1386). In the standard of care arm of this randomized trial, patients were targeted for a tacrolimus level of 10-20 ng/ml for the three months, and 5-15 ng/mL after three months. Study endpoints included 1 year survival and 1-year freedom from acute cellular rejection (ACR) and any treated rejection (ATR), freedom from 1-year post-transplant diabetes as well kidney function, determined by serum creatinine obtained at baseline and the end of one year.
Summary of Results: The lower tacrolimus target range group compared to a higher tacrolimus target range group resulted in similar freedom from 1-year rejection (ACR and ATR) and with a numerical improved median serum creatinine level. Tacrolimus levels were higher at 1-year in the higher target range group. Between study groups, there were similar 1-year survival, freedom from 1-year diabetes. (see Table)
Conclusions: Managing lower tacrolimus levels in the first-year after heart transplantation appears safe and efficacious having similar anti-rejection properties to higher target levels.
Cedars-Sinai TAC/MMF(n = 88)
*Standard of Care Arm TAC/MMF(n = 107)
P-value
1-year survival
93.2%
95.0%
0.738
1-year freedom from ATR
72.8%
57.9%
0.954
1-year freedom from ACR ≥ 2R
89.8%
77.6%
0.052
1-year median TAC levels (ng/mL)
5.7
8.8
–
1-year freedom from post-transplant diabetes
83.3%
87.0%
0.732
Baseline median serum creatinine, mg/dL (n)
1.1
1.1
n.s.
1-year median serum creatinine levels, mg/dL
1.1
1.3
n.s.
Change from baseline to 1-year in creatinine levels, mg/dL
0.0
0.2
n.s.
#182
Is Crossing DSA Detected in the Dilution Assay Safe for Patients Undergoing Heart Transplant?
Kanungo A, Bhatnagar N, Hamilton M, Kobashigawa J. Cedars-Sinai Smidt Institute, Los Angeles, CA
Purpose of Study: Patients awaiting heart transplant who are highly sensitized may have high binding levels detected in the undilution assay. However, these antibodies are only found to be significantly elevated if they are also detected in the dilution assay (1:8 dilution assay). It has not been established whether crossing DSA detected in the dilution assay at the time of HTx is safe or leads to more post-operative antibody-mediated rejection (AMR) or graft dysfunction.
Methods Used: Between 2010 and 2020, we assessed 315 sensitized patients (PRA>10%) who underwent HTx. 54 patients were identified at the time of transplant if we crossed any DSA in the undilution assay. Of these 54 patients, 6 had DSA detected in the 1:8 dilution assay and the remaining 48 patients had DSA detected only in the undilution assay. The remaining 261 sensitized patients with no DSA crossed was the control group. A negative prospective crossmatch was mandated if crossing high DSA levels (> 10K MFI) and those DSA detected in the 1:8 dilution assay. All patients were given ATG followed by IVIG immediate postop. When crossing high DSA levels (MFI>10K), eculizumab periop is added. Endpoints include 3-year survival, freedom from cardiac allograft vasculopathy (CAV: ≥30% stenosis by angiography), freedom from non-fatal major adverse cardiac events (NF-MACE: myocardial infarction, new congestive heart failure, percutaneous coronary intervention, pacemaker/implantable cardioverter defibrillator placement, stroke), and freedom from left ventricular dysfunction (LVD, defined as left ventricular ejection fraction ≤40%) and 1-year freedom from any-treated rejection (ATR), acute cellular rejection (ACR) and antibody-mediated rejection (AMR).
Summary of Results: Crossing any DSA compared to not crossing DSA has significantly lower freedom from ATR and AMR. Crossing DSA detected in the dilution assay compared to those DSA detected in the undilution assay showed a lower freedom from ATR and AMR but the numbers are small. There were no significant differences among the 3 study groups in 3-year survival, freedom from CAV, freedom from NF-MACE, and LVD.
Conclusions: Crossing DSA at the time of heart transplant appears safe with customized immunosuppression and has acceptable clinical outcomes. DSA detected in the dilution assay at the time of heart transplant may lead to more AMR which does not impact clinical outcome.
p=0.07 for Dilution DSA vs Undilution DSA **p-0.02 for Dilution DSA vs Undilution DSA.
#183
AN UNEXPECTED LARGE RIGHT ATRIAL THROMBUS DURING PATENT FORAMEN OVALE CLOSURE
Kim J1, Kar S2. 1Los Robles Medical Center, Thousand Oaks, CA and 2Los Robles Medical Center, Thousand Oaks, CA
Case Report: Right atrial thrombus is rare but possibly underdiagnosed condition with a high mortality rate, and there is currently no standard management established. (1) We herein present a case of a patient with a large right interatrial thrombus detected during a patent foramen ovale (PFO) closure.
Clinical Case: A 68-year-old male with past medical history of hypertension, hypothyroidism and hyperlipidemia presented to the emergency department (ED) for worsening right-sided weakness for 5 days. Numbness started on the right hand which with time progressed to right foot, face and chest. This was the first-time patient experienced these symptoms prior to presenting to the hospital. On ED presentation, his vitals were temperature 96.5, heart rate 68, respiratory rate 18, blood pressure 179/87, O2 saturation 96% on room air. Computed Tomography (CT) head without contrast did not show any acute abnormalities. MRI brain showed small acute left thalamic infarct which explained the patient’s presentation. Transthoracic Echocardiogram (TTE) with bubble study showed significant right-to-left shunt concerning for paradoxical embolic stroke. His symptoms improved and made full recovery to baseline with anticoagulation with IV Heparin that was bridged to Apixaban 5mg BID.
2 months later, the patient undergone scheduled PFO closure with intracardiac echocardiography (ICE) guidance. The procedure started uneventfully but intra-operative ICE showed large pedunculated right inferior interatrial septal thrombus measuring 1cm x 1cm. With cautious maneuver, circumventing the thrombus, 25mm Gore septal Occluder was placed successfully without getting in contact with the thrombus. After deployment of the PFO closure device, the thrombus was again confirmed in position. The patient was continued on Apixaban 5mg BID with close follow up with cardiology outpatient clinic.
The patient underwent repeat TEE for 2-month follow-up which showed no evidence of right interatrial septal thrombus. Gore Septal Occluder remained in satisfactory position and no bubble leak was seen with Valsalva maneuver.
Discussion: Differential diagnosis for right atrial mass includes primary or metastatic tumors, tricuspid valve vegetations, or thrombi. When right atrial thrombus is identified, 80-90% of the patients had pulmonary embolism (PE) that required immediate treatment. Burgos et al. concluded that the thrombolysis or surgical thrombectomy showed better outcome than anticoagulation alone in patients with PE. (2,4) PFO is a common condition with approximate incidence of >25% of adult population and increases risk of cryptogenic stroke. (3) Given that the patient did not have any symptoms or signs other than the first inciting ischemic stroke and that the right atrial mass had disappeared on follow-up TEE, the patient was successfully treated with oral anticoagulation and PFO closure.
#184
EFFECT OF INCREASED INTERHOSPITAL TRANSFER TIMES ON HEALTH OUTCOMES IN CRITICAL CARDIAC CARE IN BRITISH COLUMBIA AND THE YUKON IN CANADA
Lakhani S1, Taylor C2, Ramanathan K2. 1University of British Columbia, Vancouver, BC, Canada and 2University of British Columbia, Vancouver, BC, Canada
Purpose of Study: Cardiovascular disease is a highly prevalent condition among Canadians. However, many Canadians reside in communities without the necessary expertise or equipment to manage common cardiac emergencies and therefore require transportation to a specialized centre in a timely manner to receive treatment. Delays in treatment for acute cardiac conditions requiring hospitalization lead to unnecessary suffering and poorer outcomes. These delays in receiving the recommended treatments also lead to prolonged hospitalization, further burdening the healthcare system. This quality improvement study aims to examine transfer times between healthcare centers across British Columbia and the Yukon in Canada for acute cardiac conditions, to determine the effect of interhospital transfer times on survival.
Methods Used: Following institutional board approval, a retrospective chart review was conducted of consecutive patients admitted to the St. Paul’s Hospital Cardiac Intensive Care Unit (CICU) in Vancouver, British Columbia (BC) after interhospital transfer within the Canadian provinces of British Columbia or the Yukon from 2022 to 2023. St. Paul’s Hospital is one of 5 major cardiac centres in BC that regularly receives patients for acute cardiac condition management, needing expert care for acute cardiac conditions. Demographic and clinical data was abstracted using department admission records. Times of transfer to the CICU were measured, as well as patient priority times and adverse outcomes.
Summary of Results: Our cohort consisted of n = 575 patients transferred from a hospital or nursing station within British Columbia and the Yukon in Canada to the St. Paul’s hospital CICU in Vancouver for an acute cardiac condition. The primary diagnosis was Acute Coronary Syndrome (ACS) in 58% and ventricular tachycardia in 6%. Amongst the ACS patients, the ratio of ST segment elevation to non-ST segment elevation was 2:1.
A total of n = 255 (44%) patients were classified as “Life, Limb or Threatened Organ” (LLTO) critical condition. The LLTO patients had a shorter median transfer time of 3 hours and 15 mins compared to the non LLTO patients of 16 hours and 2 mins.
Transfer was cancelled in 14 (0.02%) patients, redirected to an alternative site in n =18 (0.03%). Death occurred in n = 7 (0.01%) before or during transfer.
Conclusions: The most common diagnosis for interfacility transfer was an Acute Coronary Syndrome with predominance for ST-segment elevation. The transfer times were shorter in emergent patients. The mortality of interfacility transfer patients was extremely low at 0.01%.
Our preliminary data supports the presence of an efficient and safe interhospital transfer system to St. Paul’s Hospital following hospitalization in BC or the Yukon. Further analysis is needed to determine the effect of time delays on longer-term adverse health outcomes and heath economic determinants.
#185
Effect of carvedilol and R-carvedilol on Nitrogen Mustard induced mRNA overexpression of pro-inflammatory genes in the skin of SKH-1 mice
Miwalian R, Shahid A, Huang Y. Western University of Health Sciences - College of Osteopathic Medicine of the Pacific, Pomona, CA
Purpose of Study: The chemical warfare agent sulfur mustard (SM) and its analog nitrogen mustard (NM) causes severe vesicating skin injuries due to its potent DNA alkylating properties. The pathologic mechanisms for skin injury following mustard exposure are poorly understood; therefore, no effective treatment is available. Previous reports demonstrated the protective activity of carvedilol, an FDA-approved β-blocker, and its enantiomer R-carvedilol, against ultraviolet radiation-induced skin damage. Besides having beta adrenergic and alpha 1 blocking properties, Carvedilol has direct anti-inflammatory and antioxidant properties. The effects of carvedilol on NM-induced skin injuries were evaluated in mice. In a pilot study, as assessed by RT2 Profiler™ PCR Arrays containing 84 genes in the NF-kB pathway, NM strongly induced several NF-kB-regulated pro-inflammatory genes in the skin of SKH-1 hairless mice. The current IACUC approved study aimed to accurately verify the mRNA gene expression changes of selected genes activated by NM and quantify the anti-inflammatory effects of 10 μM topical carvedilol (CAR) and R-carvedilol (R-CAR) on mRNA expression of these genes in mouse skin.
Methods Used: Qiagen’s RNeasy Kit was used to isolate RNA from previously collected skin tissue of SKH-1 mice following the manufacturer’s instruction. cDNA was synthesized using a high-capacity cDNA reverse transcriptase kit (Thermo Fisher Scientific, Waltham, MA, USA). The cDNA was amplified with Power SYBR™ green PCR master mix (Applied Biosystems) utilizing primers for mouse IL-1β, Csf3, Ccl2, Cox-2, and β-actin. PCR was performed on a CFX96 real-time thermal cycler detection system (Bio-Rad, Hercules, CA, USA). The data were analyzed using β-actin as the normalization gene based on the 2-ΔΔCt method. The mRNA expression was compared between 4 different treatment groups (Control, NM only, NM+CAR, NM+R-CAR) to determine the significant expression difference of the selected genes.
Summary of Results: NM statistically upregulated the four pro-inflammatory genes IL-1β, Cox-2, Ccl2, and Csf3. Carvedilol statistically reduced NM-induced IL-1β and Cox2; however, R-carvedilol appears to reduce more potently NM-induced IL-1β, Cox2, Ccl2, and Csf3 to levels that are not distinguishable from the controls.
Conclusions: The qRT-PCR studies demonstrate that carvedilol and R-carvedilol reduced inflammatory biomarkers induced by NM in the skin, which suggested the potential of this β-blocker and its R-enantiomer to be repurposed as a countermeasure against mustard-induced skin injuries. Since R-carvedilol is not a β-blocker, there is no indication that the effects of carvedilol are adrenergic receptor dependent. Carvedilol is an ROS-scavenging drug which may explain the underlying protective effect against NM. Furthermore, its anti-inflammatory properties may also promote a less stressful environment facilitating cutaneous recovery from vesicant exposure.
#186
ARTIFICIAL INTELLIGENCE IN THERAPEUTIC MANAGEMENT OF HYPERLIPIDEMIA AND OCULAR PATHOLOGY
Petrosyan A, Inouye K, Moskalensky L, Thankam FG. Western University of Health Sciences, College of Osteopathic Medicine of the Pacific, Pomona, CA
Purpose of Study: Retinal vascular occlusions (RVO) are characterized by the formation of thromboembolism in the blood vessels supplying the retina. Although the type of RVO varies in pathophysiology, it has been a common manifestation in patients with systemic vascular diseases including hyperlipidemia. Nonetheless, the increasing incidence of ocular manifestations in hyperlipidemic patients calls for a more effective way to diagnose and treat earlier. Artificial intelligence (AI) emerged as a novel platform to perform cognitive functions and is rapidly being implemented into the diagnosing and treatment of RVO. This study overviews the effectiveness of AI in RVO management based on the recent literature.
Methods Used: The study utilized Google Scholar and Pubmed databases, utilizing search functions including “RVO,” “AI,” and “dyslipidemia”. Articles included are experimental studies, meta-analyses, and systematic reviews. Exclusion criteria included works published earlier than 1980. A total of 55 sources were utilized in the construction of our literature review.
Summary of Results: Our findings indicate that the subset of AI known as Deep Learning (DL) has been trained to accurately detect RVO-associated lesions and ischemia presented in diagnostic imaging modalities. Also, AI’s ability to identify key RVO features translates into correctly distinguishing RVO from other oculopathies such as Diabetic retinopathy, and Sickle Cell retinopathy. Furthermore, AI promises predictions of RVO-patient responses to treatment such as intravitreal injections. These findings are suggestive of AI’s learning capabilities, and potential in-clinic applications.
Conclusions: AI display multifaceted applications in monitoring the disease progression of RVO. Specifically, AI aids in detection, diagnosis, and short-term prognosis. However, AI alone isn’t conclusive in more complicated cases such as the presence of multiple oculopathies, or in the prediction of long-term treatment patient outcomes. Providing AI with opportunities to learn in these areas may result in a comprehensive understanding of RVO.
#187
Pulmonary Embolism and Stroke: A Case Report of a Large Biatrial Thrombus saddling a PFO
Sharma R1, Ghadiya K3, Garcia J3, Kooner G2, Joolhar F3, 1. 1David Geffen School of Medicine, Bakersfield, CA; 2Rio Bravo Family Medicine, Bakersfield, CA and 3Kern Medical Center, Bakersfield, CA
Case Report: In the intricate realm of cardiovascular pathology, a compelling case emerges: a large biatrial thrombus boldly stradding a patient foramen ovale. This daring interplay between anatomy and pathology sets a case for medical thriller, a twist of the ominous threat of both pulmonary embolism and stroke. Here in unravled is a case of complexities of this clinical conundrum of a large biatrial thrombus saddling a patent foramen ovale.
A 67-year-old male patient presented to the emergency department for severely progressive dyspnea and lower leg pain. Upon presentation patient was hypoxic to 85’s, tachycardic to 112 and tachypneic to 23. Patient tested positive for COVID-19. CT pulmonary angiogram was immediately done which revealed large bilateral pulmonary emboli with evidence of right heart strain; tPA was given and the patient was taken for immediate mechanical thrombectomy and IVC filter placement. At admission the patient was alert and oriented to name, place, location, and situation without any other significant deficits. 2nd hospital day the patient developed acute encephalopathy with right-sided weakness. Stroke protocol was initiated and subsequent MRI revealed acute infarctions of the left frontal and occipital lobes along with the left basal ganglia. TTE was additionally done showing left atrial mass which was confirmed to be a large biatrial thrombus by TEE measuring 3cm x 1cm saddled on the interatrial shunt. During the next few days of hospitalization, the patient continued to show mental status deterioration with worsening aphasia and confusion. On Day 7, the patient developed new facial palsy and worsening right lower extremity weakness concerning for acute CVA. Imaging was not concerning for new cerebral infarction at that time. However, on Day 14 of hospitalization, the patient again developed worsening aphasia, right side weakness, and fine motor movement. Repeat MRI confirmed new infarctions in the left frontal lobe and occipital lobe. It was determined the patient was likely developing recurrent CVAs from paradoxical emboli originating from his biatrial thrombus. Therefore, the patient was transferred to a tertiary care facility for surgical removal of the thrombus.
In conclusion, the intricate interplay between a biatrial thrombus and a patent foramen ovale highlights the critical importance of early diagnosis and tailored treatment, ultimately safeguarding patients from the devastating consequences of pulmonary embolism and stroke.
#188
A CASE OF PERONEAL ARTERY PSEUDOANEURYSM: TREATMENT AND LONG-TERM FOLLOW-UP
Thayapran KG1, Rafie R2. 1University of Colorado School of Medicine, Aurora, CO and 2Adventist Health, Visalia, CA
Case Report: Introduction: Peroneal artery (PA) pseudoaneurysms are a rare complication of peripheral vascular interventions of the lower limb that may be asymptomatic or present with leg swelling, pain, bruising, or rupture. Here, we describe a case of a right PA pseudoaneurysm and arteriovenous fistula that arose following atherectomy of the PA, subsequent treatment of the pseudoaneurysm with a covered stent, and reintervention 8 years later following stent closure.
Case Presentation: A 71-year-old female with type 2 diabetes and hypertension presented with right leg claudication that significantly affected her daily activities. Ankle-brachial index testing, duplex ultrasound testing, and angiogram of the right leg confirmed the presence of severe peripheral artery disease (PAD) of the below-knee vessels, prompting further intervention. Directional atherectomy within the PA was successful; however, angiogram immediately after showed a perforation of the proximal PA, which prompted balloon tamponade until the perforation was successfully sealed. However, angiogram 2 days later revealed a proximal right PA pseudoaneurysm with an associated arteriovenous fistula, prompting deployment of a covered stent to treat the pseudoaneurysm. The patient subsequently reported complete resolution of symptoms. However, the patient developed right leg claudication refractory to conservative management 8 years later. Angiogram revealed occlusion of the covered stent in the proximal PA, prompting balloon angioplasty to achieve patency. The patient subsequently reported complete resolution of right leg symptoms once again.
Discussion: With the increasing number of peripheral vascular interventions being performed, identification of complications such as PA pseudoaneurysms is crucial. Indeed, most reported cases, such as the one described here, arise from iatrogenic injury. Treatment may be surgical or endovascular, depending on the size, location, and extent of soft tissue involvement. Prompt identification and treatment is required to prevent rupture, hemorrhage, compartment syndrome, and long-term morbidity.
PA pseudoaneurysm following directional atherectomy.
#189
A Broken Heart Familial Dilated Cardiomyopathy Presenting with Bilateral Intraventricular Thrombi and Multiple Arterial Thromboemboli
Uddin S, Aboaid S, Sharma R, Petersen G. Kern Medial Center, Bakersfield, CA
Case Report: Familial Dilated Cardiomyopathy is a relatively common autosomal dominant inherited disease often presenting with Biventricular Heart failure in its advanced stages, coinciding Biventricular thrombi causing sites of Arterial thromboembolism in major vessels is rare.
Case Presentation: A 36-year-old Hispanic male who had recently immigrated to the United States without prior medical history presented to the hospital with complaints of epigastric pain for one week and fatigue for two weeks. His epigastric pain and general fatigue occurred without provocation and had been persistent. The symptoms had limited his ability to function at his work in a construction yard. A review of systems revealed he had been suffering from right lower extremity swelling that had caused pain with ambulation. The patient stated he never indulged in recreational drugs or Alcohol use. A laboratory evaluation revealed mild transaminitis, mild renal impairment, lactic acidosis of 3.5 mmol/L, and a BNP of 1,097 pg/mL. Imaging results with CT Abdomen and Pelvis revealed cardiomegaly and significant biventricular dilation with biventricular thrombi which in the right ventricular apex measured 1.4 x 2.4 x 1.1 cm and in the left ventricular apex measured 2.5 x 1.3 x 1.3 cm, an enlarged liver 20 cm with periportal edema, regional area of loss of contrast-enhancement of the superior left renal pole involving a 2 x 1 cm segment of renal cortex concerning for renal infarct, and Large partially occlusive and occlusive emboli throughout the right common iliac, external iliac, and internal iliac artery. CT angiography of the Right Lower extremity revealed infra-popliteal occlusion as well. A complete Cardiac Echocardiogram confirmed imaging findings; the Left ventricle was severely dilated with an ejection fraction of less than 10% and a moderate apical mobile thrombus, a severely dilated right ventricle with global systolic dysfunction and a large apical mobile thrombus. Evaluation with Urine toxicology, HIV serology, Thyroid panel, Respiratory Viral panel, Trypanosoma Cruzi Antibody, and Antiphospholipid Antibody were negative. Further history from the patient revealed his mother and brother had passed away after similar presentations at ages 26 and 25, respectively. The patient was initiated on anticoagulation therapy with Heparin drip, Carvedilol 3.125 mg twice daily, and Losartan 25 mg daily. The patient required transfer to a Higher Level of Care for urgent right lower extremity thrombectomy and to address his Biventricular heart failure and thrombi.
Conclusion/Discussion: Familial Dilated Cardiomyopathy is a relatively common cause of biventricular heart failure however the presence of biventricular thrombi with shower emboli complicates the prognosis. A multidisciplinary approach between Cardiologists and Vascular surgeons is needed to optimize outcomes.
#190
Snorting, Shooting, or Swallowing Methamphetamine: Does Route Of Administration Affect Your Heart Health?
Yip SA1, Dulani S2, Narasimhan A1, Wieselthier K1, Brown J1, Saito S3, Fuchs S1. 1Western University of Health Sciences - College of Osteopathic Medicine of the Pacific, Pomona, CA; 2Western University of Health Sciences - College of Osteopathic Medicine of the Pacific - Northwest, Lebanon, OR and 3Kern Medical Center, Bakersfield, CA
Purpose of Study: Methamphetamine (meth) use is a predominant cause of numerous cardiovascular (CV) pathologies – such as arrhythmias, dilated cardiomyopathy, etc. – and has been linked to the reduction of the left ventricular ejection fraction (LVEF) and significant left ventricle dilation due to rapid and acute increases in heart rate and blood pressure. These associations therefore establish LVEF as an important measurement to evaluate meth usage consequences. This study’s purpose is to investigate the least harmful route of administration (ROA) for meth to develop a harm reduction approach for patients, as many patients, especially those who are unhoused, are unable to achieve immediate abstinence. Based on our literature review, we believe the intravenous ROA of meth currently results in the most harm as it contains more potent dosages and poses the highest risk for dependence.
Methods Used: In our IRB-approved study, we surveyed unhoused individuals in California’s meth usage epidemic areas on meth ROA (smoking, oral, intravenous, intranasal) and usage length. LVEF was measured in participants meeting inclusion criteria by measuring E-point septal separation (EPSS) on ultrasound. Unhoused individuals not using meth were included in our control group to study the prevalence of CV disease in this population.
Summary of Results: Participant recruitment is ongoing and we aim for a sample size of 100 patients by December 2023. Although prior studies have noted the common association of meth use with reduced LVEF, our results thus far have shown that despite significant years of meth usage, ejection fraction (EF) appears to be preserved in our preliminary cohort of four subjects. We believe this could be attributed to the modifying effects of exercise or prolonged periods of abstinence between usage (from unstable housing and lack of resources). Taking this into account, we expanded our survey to include exercise data to better understand how exercise modulates meth’s effect on EF. With the data, we aim to demonstrate how different ROAs of meth can affect CV structural changes and provide education for those with cardiac health issues.
Conclusions: Overall, recruiting more participants will allow us to evaluate the degree of CV risk associated with different meth ROAs and help identify the least harmful one. We utilize EPSS measurements to evaluate LVEF as studies have demonstrated EPSS efficacy in estimating patients’ CV function. We also provide unhoused patients a holistic education, such as identifying heart disease symptoms they may face, providing follow-up resources, and recommending lifestyle modifications that can attenuate their cardiac conditions. With our results and protocol, we plan to generate a harm-reduction approach to assist patients with eventual meth usage cessation.
#191
Association of Pediatric Post-Operative Outcomes with Gender, Race and Ethnicity in Canada
Zhang J1, 3, Boldut R1, 3, Duan A2, 3, Kwong A1, 3, Duffy D3, Afshar K4. 1University of British Columbia, Vancouver, BC, Canada; 2University of British Columbia, Vancouver, BC, Canada; 3BC Children’s Hospital, Vancouver, BC, Canada and 4BC Children’s Hospital, Vancouver, BC, Canada
Purpose of Study: Currently, little is known about healthcare disparities in pediatric populations, especially in Canada. While several American studies have pointed to the association between post-operative complications and the male gender as well as non-white patients in pediatric populations, we are unsure if this association is established in Canadian populations. Furthermore, the underlying factors leading to this association (including both biological and social factors) are complex, and require further investigation. By exploring the association of gender, race, and ethnicity with post-operative outcomes in pediatric populations, we can better understand the long-standing systematic health and social inequities in the context of Canadian institutions. Our research goal was to determine how race, ethnicity and gender affect pediatric postoperative outcomes in Canada through a literature review.
Methods Used: The research goal was addressed through a comprehensive search of Ovid Medline, with terms related to pediatric populations, Canadian institutions, post-operative outcomes, race, ethnicity and gender. Papers that were in English, included Canadian pediatric populations, and directly compared demographic information with post-operative outcomes were included for review.
Summary of Results: 75 records were initially identified. After title and abstract screening, 13 articles were included for full-text review. Only 4 met the criteria set for inclusion, though two additional studies were reviewed for their perceived relevance despite not meeting the exact inclusion criteria. Three articles reported that non-white patients had increased risk of post-surgical complications and/or increased need for more aggressive treatments upon follow-up. An article also reported that lower income patients were at increased risk for post-surgical complications when compared to higher income patients. Two articles reported that ethnicity itself can act as a risk factor rather than social factors that make ethnicity a risk factor. One article found that there was no correlation of patient demographic information collected and post-surgical outcome. Through this review, we found a lack of consensus on the relationship between post-operative outcomes with race as well as ethnicity, and no information was uncovered about the relationship between post-operative outcomes and gender. This review has served to identify the existing gaps in research in Canada, and highlights the need for research on factors impacting post-operative outcomes.
Conclusions: The conflicting results and the paucity of research highlight the need for further research on this topic. We have begun work on a follow up review that broadens the scope to include other developed nations’ pediatric populations, and other databases including EMBASE and CINAHL. Our preliminary findings indicate a significantly increased amount of research around the association between post-operative outcomes and gender along with race and ethnicity criteria in the United States.
#192
Reimagining heathcare for children - a pivot emphasizing justice and human dignity
Mowery A, Reiley J, Brunelli L. University of Utah, Salt Lake City, UT
Purpose of Study: The United States (U.S.) boasts many of the best children’s hospitals in the world and one of the largest and most knowledgeable workforces dedicated to the care of children. U.S. pediatric healthcare is a leader in research and innovation such as the increasing utilization of genome-wide technologies associated with the revolution of precision medicine. After several studies suggested the potential benefits of genetic testing in critically ill children in neonatal intensive care units, the recent proposals for genomic-based newborn screening (G-NBS) are among the most innovative approaches in pediatric healthcare. Despite these strengths, pediatric outcomes in the U.S. remain worse than any other industrialized nation, and pediatric healthcare costs per capita are substantially higher than comparable wealthy countries. Due to these challenges, in recent years there have been increasing calls for more equity and justice in U.S. pediatric healthcare. Consistent with these calls for justice, a published analysis of more than 130 million births in the U.S. between 1959 and 1995 showed that traditional NBS led to improvements in infant mortality and health equity only when it was implemented in association with measures to improve healthcare access for children.
Methods Used: Here, we analyzed why better integration of the concept of justice in U.S. pediatric healthcare necessitates a deeper analysis of the meaning of “justice” and we explored the ethical concepts upon which we can ground the concept of justice.
Summary of Results: Our analysis suggests that, for the well-being of society and people, justice cannot be just a partial, interpersonal concept. It is a fundamental concept; it needs to be objective and elevated above an exchange interest. Our analysis further indicates that justice needs to be grounded on the value of human dignity. Accepting the human dignity of every child implies the absolute responsibility of adults to respect the unique and embodied gift of each child by addressing their physical, mental, social, and emotional health needs and well-being. Applying these principles has several implications for the implementation of precision medicine. For example, the data on traditional NBS suggest that the new G-NBS could lead to better child health only if the same degree of attention devoted to genomic technologies is directed to the promotion of public health measures that facilitate providing high-quality healthcare to all children. Consistent with an objective concept of justice, significant efforts need to be made to ensure all children have access to providers for accurate interpretation of results and adequate follow up and specialty care.
Conclusions: A pivot to focus on human dignity can not only help ground the concept of healthcare justice but also provides a foundation to reimagine and improve children’s health in the U.S. In this way, G-NBS could become a vehicle to drive change for better equity and justice for all children to live a healthy life.
#193
Quality improvement initiative to reduce disparities in human donor milk utilization
Daly-Jensen K, Rodriguez J, Gievers L, Khaki S. Oregon Health and Science University, Portland, OR
Purpose of Study: Exclusive breastfeeding for the first 4-6 months of age has been associated with better long-term health outcomes for both infants and mothers. When nutritional supplementation is needed, many pediatricians recommend using human donor milk (HDM). Disparities exist regarding who receives HDM as supplementation. Non-white infants are less likely to receive HDM, especially if their families’ first language is not English or they are publicly insured. The purpose of this study was to improve utilization of HDM for all patients, particularly for non-white and publicly insured patients.
Methods Used: We evaluated HDM supplementation rates in the Mother Baby Unit (MBU) at a single quaternary academic medical center in the Pacific Northwest following multiple PDSA cycles. Baseline data was obtained from January to September 2021 and PDSA cycles were performed from September 2021 to February 2023. A HDM FAQ sheet was created to address previously determined concerns about HDM. PDSA cycles included distribution of the FAQ sheet to prenatal care providers and patients, a newsletter reminder to provide the FAQ sheet to patients prior to supplementation, and reminder notices on MBU formula bins.
Summary of Results: We did not find correlated changes in rates of HDM usage among publicly insured or non-white patients with any PDSA cycles. Most notably, the rate of HDM use among privately insured patients remained consistently above 60% while the rate of HDM use among publicly insured patients varied widely (35-55%).
Conclusions: These results confirm that a disparity in HDM utilization exists based on insurance type and race. Despite creating a FAQ sheet to address previously determined concerns about HDM, utilization of HDM did not increase in our study population. The lack of improvement is likely multifactorial and may include inconsistent use of the FAQ sheet due to frequent staff turnover and competing clinical priorities during the COVID-19 pandemic.
It is important to note that HDM utilization rates remained consistently higher for privately insured patients compared to publicly insured patients. This highlights a demographic worthy of future focus as we determine how to best provide messaging around the safety and utility of HDM. A better understanding of how and where this population prefers to receive their medical information could aid in this effort.
#194
COMMUNITY VOLUNTEERS IMPROVE MENTAL HEALTH OUTCOMES FOLLOWING DELIVERY OF A SCHOOL-BASED MENTAL HEALTH LITERACY PROGRAM TO YOUTH: ADVOCATES 4 ALL YOUTH (ALLY)
Izere M1, Wilson SN2, Mata C2, Simon S1, Kaar J1. 1University of Colorado Anschutz Medical Campus, Aurora, CO and 2University of Colorado Anschutz Medical Campus, Aurora, CO
Purpose of Study: Examine pre-post changes in key mental health constructs among community volunteers (ALLYs) who delivered a school-based mental health literacy program to youth.
Methods Used: ALLY is a universal, school-based mental health literacy intervention targeted to deliver equitable, supplementary mental health education through a student-centered, peer-to-peer design framework. Community volunteers (ALLYs) from diverse backgrounds completed an online training (i.e., 90 minutes) prior to administering the program to students through curated, six-weekly small group sessions using a bilingual interactive activity workbook. ALLYs taught students mental health-related terminology and provided hands-on practice for mindfulness strategies, positive self-talk, and healthy coping skills. ALLYs facilitated group discussions & activities on varying topics each week including emotions and moods, building healthy relationships, and problem-solving. ALLYs completed pre- and post-assessments including Social Connectedness, Geriatric Depression & Anxiety Scale, Self-Perceptions of Generativity; and Knowledge and Attitudes to Mental Health Scales (KAMHS).
Summary of Results: A total of 21 community volunteers were trained as ALLYs. ALLYs were a mean age of 59 years, with 90% identifying as female, 90% as non-Hispanic White, 76% as having attained post-graduate education, and 56% as being retirees. Of the 18 ALLYs who completed pre-post assessments; 56% reported an improvement in social connectedness, 60% improved in generative achievement (i.e., I feel like I make a difference in my community; I am giving back; I am doing things that will leave a legacy); and 67% improved in their understanding of mental disorders & 57% improved understanding of how to optimize and maintain good mental health via the KAMHS.
Conclusions: We conclude that community volunteers who serve as ALLYs to youth not only improve the mental health of those youth, but also key mental health constructs for themselves. ALLYs reported improvements in giving back to their community through their volunteering and improved their mental health in the process.
#195
EXPLORING RACIAL AND ETHNIC DISPARITIES IN THE EVALUATION OF CHILD ABUSE IN VERY YOUNG PEDIATRIC PATIENTS
Jiang M1, Bryant S1, Dao A1, Joshi K1, Krishnan A1, Vellanki K1, Yang Y1, Afghani B1, 2. 1UC Irvine School of Medicine, Irvine, CA and 2CHOC Hospital of Orange County, Orange, CA
Purpose of Study: Child abuse is a critical public health concern requiring prompt and accurate evaluation. According to the Children’s Bureau, nearly three-quarters of the children who died due to child abuse or neglect in 2019 were younger than three years old. Studies from the 1990s have highlighted the overrepresentation of Black patients in reporting and substantiating child abuse. Since then, several studies have been performed to evaluate factors that trigger the evaluation of child abuse. The purpose of our research is to compile the literature that examines racial disparities in assessing and diagnosing child abuse in young children.
Methods Used: A literature review was conducted through PubMed and Google Scholar databases using keywords such as "child abuse," "suspected," "non-accidental trauma," "disparity," "diagnosis," "racial," and "pediatric." Inclusion criteria consisted of studies published after 2000 that focused on a) patients under three years of age, b) involved suspected or diagnosed child abuse cases, and c) compared the evaluation for child abuse by race/ethnicity.
Summary of Results: Five studies met our inclusion criteria (see Table 1). Three studies showed that non-White patients were more likely to be evaluated for child abuse than White patients. In one of the three studies (Wood, 2010), the analysis showed that although child abuse was more likely to be assessed in Black patients than Whites patients, it was more likely to be substantiated in White patients after a full workup. Conversely, another study (Hymel, 2018) found that in two out of 18 participating sites, minority patients were more likely to be both evaluated and reported for child abuse and no statistical difference was found in the remaining 16/18 sites. One study of military health beneficiaries (Jones, 2022) where patients had universal health coverage and were evaluated through uniform guidelines showed no significant differences among races, even after adjusting for various variables. The limitations of this research included small sample sizes in some studies and a lack of uniformity in considering potential confounding variables.
Conclusions: Our review suggests there may be racial disparity in initiating child abuse investigations. However, contributing factors for initiation and substantiation are complex and require further elucidation. A better understanding of these factors will enable healthcare professionals to develop more equitable practices and promote a more inclusive and practical approach to safeguarding the well-being of pediatric patients.
Racial disparities in the evaluation and diagnosis of child abuse in children under three years old.
Author, Year Published
Source of Data
Age Group and Presentation
# Patients with Suspected Child Abuse
% White Patients Suspected or Diagnosed with Child Abuse or Obtained Further Evaluation
% Non-White Patients Suspected or Diagnosed with Child Abuse or Obtained Further Evaluation
Odds Ratio or P-Value
Henry, 2022
Pediatric Health Information Systems
N = 2585
Neuroimaging obtained = 668/1148 (58%)
Neuroimaging obtained: 487/748 (65%)
After adjusting for socioeconomic disadvantages, there was no association between race and ethnicity and neuroimaging use (p=0.48)
Jones, 2022
Military Health System Data Repository of Military Health System
N = 424
SCA = 294/33021 (0.9%)
SCA = 78/6556 (1.1%)
No significant differences in SCA by race were observed. Black patients to White patients – aOR: 1.11 (95% CI, 0.84-1.48)
Lane, 2002
Children
≥12 months to 3 years old with acute primary skull or long-bone fractures
Minority children were more likely to be reported for suspected child abuse than white children. Minority vs. non-minority: Medicaid or no insurance – RR: 3.08 (95% CI, 1.37-4.80); Private insurance – RR: 3.74 (95% CI, 1.46-6.01)
Hymel, 2018
Pediatric Brain Injury Research Network (18 participating sites)
N = 281
Abusive head trauma evaluation = 72%
Abusive head trauma diagnosis = 68%
Abusive head trauma evaluation = 86%
Abusive head trauma diagnosis = 81%
For 2/18 sites, minority race/ethnicity patients were more frequently evaluated (p
Wood, 2010
39 pediatric hospitals
N = 3063
Skeletal survey ordered = 67.8%
Full workup + diagnosed with child abuse = 61%
Skeletal survey ordered = 84%
Full workup + diagnosed with child abuse = 51%
More skeletal surveys were ordered in Black than White patients (p
Hereditary Angioedema: An acute exacerbation triggered by sun exposure
Abraham J, Al-Yousfi N, Mishra S. Kern Medical, Bakersfield, CA
Case Report: Hereditary angioedema (HAE) is a rare autosomal dominant disease. It occurs due to a deficiency in C1 esterase inhibitor which leads to excess production of bradykinin, resulting in recurrent attacks of angioedema. The genetic condition manifests as severe swelling in various parts of the body and may be potentially life-threatening in cases of laryngeal edema. HAE attacks may be triggered by various factors such as emotional stress, infection, environmental factors, physical exertion, and trauma.
Case presentation: A 34-year-old female with a history of hereditary angioedema presented to the emergency room complaining of diffuse facial swelling and right lower extremity swelling that started one day ago. The patient believed this attack was triggered by sun exposure while she was riding her bike the day prior. She stated that emotional stress has been a trigger in the past for facial swelling attacks. The patient had been unable to obtain her monthly maintenance medications (Firazyr and Takhzyro) for the last two months due to homelessness and social issues. The patient was diagnosed with HAE when she was ten years of age and has a family history of HAE with her sibling being affected. Prior acute attacks have required six intubations and a tracheostomy. The patient was given 0.3 mg of epinephrine intramuscularly by emergency medical services on route to the emergency department. In the emergency department, her vital signs were stable, and bloodwork was unremarkable. She denied symptoms of respiratory distress or airway compromise. The physical exam was remarkable for diffuse orbital and perioral edema, in addition to right lateral foot swelling. She was given another dose of epinephrine in the emergency department. C1 esterase inhibitors were not available in pharmacy formulary at the time of patient presentation. She was admitted to medicine and given 2 units of fresh frozen plasma, 10 mg of Decadron, and famotidine with noted improvement of symptoms. While awaiting monitoring for improvement, the patient eloped from the emergency department. The patient was scheduled for an outpatient visit the following week to establish care. Discussion: The management of hereditary angioedema primarily consists of the medical management of acute episodes and long-term prophylaxis therapy. In acute attacks, priority is given to securing the airway if signs and symptoms of airway compromise are present. The first line therapies for acute treatment include C1 inhibitor, kallikrein inhibitor, or bradykinin B2-receptor antagonist; in addition to fresh frozen plasma, if first-line therapies are unavailable as utilized in this case. This case highlights that, in addition to medical management, the identification of factors that trigger acute episodes in an individual can significantly improve long-term disease management, allowing for prompt treatment and prevention of acute attacks.
#197
THE SPECTRUM OF DISEASE EXPRESSION IN X-LINKED DISORDERS USING COFFIN LOWRY SYNDROME CASE
Barbour K, del Campo M. University of California San Diego, San Diego, CA
Case Report: We present a case of a 12 year old girl seen in genetics clinic for hypotonia, intellectual disability, and polydactyly. In addition, she had a history of short stature, obesity, febrile seizure, and myopia. Developmental delay was first noted at 9 months of age with no history of regression. She was born full term with no issues during pregnancy or perinatal period. Exam was notable for short stature (length 2%), obesity (weight 99%), epicanthal folds, hypertelorism, upturned nose, full lips, tapered fingers, polydactyly, hypotonia, and spinal lordosis. MRI, EEG, muscle biopsy, audiogram, and echo were normal. Metabolic testing with amino acids, urine organic acids, TSH, and lactate were normal. Chromosomes 46, XX. Microarray and Fragile X were normal. Rare obesity gene panel found a heterozygous pathogenic variant in RPS6KA3 associated with X-linked Coffin-Lowry syndrome (CLS). Follow up x-ray of the hand showed hypoplasia of distal phalanges bilaterally consistent with CLS. X-ray of the spine showed mild spine curvature and no kyphosis.
She was diagnosed with CLS. There is an association with obstructive sleep apnea and was referred for sleep study given presence of snoring and unrestful sleep. We suspect her sister and mother also have heterozygous variants and sent testing for them. Her sister has intellectual disability and suspected stimulus induced drop attacks, and both her sister and mother have short stature and facial features/ tapered fingers seen in CLS. She can participate in preconception planning in the future if she chooses.
Hemizygous males with CLS have a more severe phenotype and can have severe intellectual disability, stimulus induced drop attacks, progressive kyphoscoliosis, spastic paraparesis, seizures, short stature, hearing loss, and obstructive sleep apnea. Heterozygous women can have mild to moderate intellectual disability, less severe neurologic and spine abnormalities, and dysmorphic features (hypertelorism, short upturned nose, thick lips, and tapered fingers).
This case is an example of how heterozygous women often demonstrate less severe phenotypes and variable expression in X-linked conditions. This may be related to random versus skewed X-inactivation, genomic mosaicism, and whether the protein is cell autonomous (Shvetsova et al., 2019, Eur J Hum Genet; Dobyns, 2006, Acta Paediatr Suppl). Some have proposed shifting away from the terminology “carrier” and instead using “heterozygous” to prompt increased surveillance for disease symptoms in women (Wang et al., 2007, Genet Med; Pinto et al., 2010, Orphanet J Rare Dis). Some have even suggested using the terminology “X-linked” diseases rather than “X-linked dominant/recessive” (Dobyns, 2006; Acta Paediatr Suppl). One carrier of an X-linked disease started a nonprofit Remember the Girls to create community among affected women, raise awareness for disease surveillance in women, and advocate for women to be included in research (https://rememberthegirls.org).
#198
Establishing a Database to Reliably and Efficiently Identify Patients Eligible for Novel Gene Therapies
Boldut R1, 2, Kwong A1, 2, Armstrong L3, 4, Gardiner J5, 6, Prentice L3, Wokhloo P3, Duffy D2. 1University of British Columbia, Vancouver, BC, Canada; 2BC Children’s Hospital, Vancouver, BC, Canada; 3BC Women’s Hospital, Vancouver, BC, Canada; 4University of British Columbia, Vancouver, BC, Canada; 5BC Children’s Hospital, Vancouver, BC, Canada and 6University of British Columbia, Vancouver, BC, Canada
Purpose of Study: Inherited retinal dystrophies are a genetic form of visual impairment. RPE65 gene related Leber congenital amaurosis (LCA) is the first inherited retinal dystrophy (IRD) for which an ocular gene therapy has been approved for public use in Canada. In the British Columbia (BC) Women’s Medical Genetics Department, there is a lack of a multidisciplinary-informed genetic database which includes patients with IRD’s. Such a database would bring together the detailed clinical features and any available genetic test results of patients with IRD’s. This quality improvement (QI) project aimed to create an optimal care model pathway centred around a robust database system and related periodic review initiatives for IRD patient care. This quality improvement project would allow us to identify gaps in the current system in terms of the number of patients that may be eligible for research and clinical treatment options not identified through the previous system, and would furthermore inform us of what services are needed for optimal patient care. This project also aimed to identify information that would be helpful to include on new intake forms for the BC Women’s Medical Genetics program for future improvement.
Methods Used: A password-protected Microsoft Excel sheet was developed as a data collection tool. This included formatting and selecting data points for collection. The data collection tool was edited with feedback from key partners and subject matter experts. Charts of patients who had IRDs and were referred to the Medical Genetics program were reviewed. Data was collected, by the two QI assistants, from charts in the Medical Genetics clinic. Following data extraction of every ~20 charts, the team (made up of two research assistants, a genetic counsellor, a geneticist, an ophthalmologist, and a data project manager) reviewed the data collected for further optimization of data collection and for discussion of any problems encountered. Reviewing charts of those who have IRD, but no genetic testing referral could be reviewed at a later date as a compliment to this quality improvement project.
Summary of Results: So far, the QI assistants have added ~50 patients to the database. Selecting and defining data fields involved meticulous efforts to align nomenclature of data fields to relevant other initiatives. We are recognizing that the data regarding disease courses is from the time of consultation, so will need to explore ways of keeping that current if this approach to care is to be fully optimised.
Conclusions: Overall, this collaboration between the Medical Genetics and Ophthalmology departments is helping us identify the data requirements for and establishing a resource for ongoing quality improvement. This project highlights the need for collaboration between departments to provide optimal care.
#199
VASCULAR EHLERS-DANLOS SYNDROME AND VON WILLEBRAND DISEASE: CASE REPORT AND REVIEW OF LITERATURE
Gomes A, del Campo M. UCSD, San Diego, CA
Case Report: Vascular Ehlers-Danlos Syndrome (vEDS) is a severe subtype of EDS caused by mutations in the COL3A1 gene responsible for type III collagen synthesis. vEDS is characterized by arterial, intestinal, and/or uterine fragility, with an increased risk of arterial rupture, aneurism, dissection, and intestinal and uterine rupture. Patients with vEDS are also at higher risk of surgical damage, rupture of encapsulated organs, and hernias. Affected individuals present skin fragility and joint hypermobility with a higher risk of dislocations and subluxations.
Von Willebrand disease (VWD) is a common congenital bleeding disorder caused by deficiency or abnormality of von Willebrand factor, a large adhesive glycoprotein involved in hemostasis. VWD is a disorder of platelet aggregation that causes mucocutaneous bleeding, clinically presented with easy bruising, prolonged and recurrent nosebleeds, and prolonged bleeding following surgery, trauma, or childbirth.
Von Willebrand Factor (VWF) and platelets, the primary components of blood clotting, interact with collagen types I, III, and IV. The interaction with type III collagen is more clinically significant due to its higher content in the subendothelial matrix.
The co-occurrence of Von Willebrand Disease (VWD) and Ehlers-Danlos Syndrome (EDS) is rare. VWD is the most common inherited bleeding disorder, affecting 1% of the population; vEDS is a rare subtype of EDS and has an estimated prevalence of 1 in 90,000. The expected occurrence of both conditions together is one in 900,000.
In 2018, Hall et al. described the clinical presentation of five patients with co existing VWD and EDS (classical and cardiac-valvular subtypes) and 21 patients with VWD and joint hypermobility. To our knowledge, there have not been any reported cases of a combination of Von Willebrand disease and vEDS.
We report on a preterm male (ex 34 weeker) initially evaluated at the NICU due to arachnodactyly. PPROM and maternal gestational diabetes complicated pregnancy history. Delivered was via C-section, breech, with Apgar of 6 and 8. He was admitted to the NICU due to respiratory distress and hypoglycemia. Small skin tears along bilateral groin creases and bruising were noted at birth. Physical examination showed congenital plagiocephaly on the right, low-set ears, slender fingers and toes, and bilateral cryptorchidism. He had a normal echocardiogram, abdominal ultrasound, and microarray and was discharged in 12 days. At 9 months of age, his development was globally delayed. In addition, bilateral hip dysplasia and plagiocephaly have required surgery and helmet therapy.
Whole exome sequencing found two pathogenic variants in COL3A1 and VWF that have determined a combined diagnosis of vascular Ehlers-Danlos and von Willebrand disease.
We report the features of a child with VWD and vEDS; we present a literature review and the pathogenesis of both disorders. We discuss possible complications, clinical interventions, surveillance, and prognosis.
#200
FAMILIAL CASE OF APLASIA CUTIS CONGENITA AND ECTRODACTYLY SKELETAL SYNDROME - A CASE REPORT AND LITERATURE REVIEW
Parashar K1, 2, Wigby K4, Feigenbaum A1, del Campo M1, 3. 1University Of California at San Diego, San Diego, CA; 2Rady Children’s Hospital, San Diego, CA; 3Rady Children’s Hospital, San Diego, CA and 4UC Davis, Davis, CA
Case Report: Two-month-old baby boy was transferred to the hospital due to persistent metabolic acidosis, congenital microcephaly, Small for Gestational age with postnatal growth deficiency, renal dysgenesis and dysfunction, genital anomalies, and dysmorphic features.
He had elevated creatinine but no hypoglycemia, negative urinary ketones, normal electrolytes, and anion gap. Urine organic acids and plasma amino acids showed abnormalities that did not suggest a specific metabolic disorder.
Physical examination showed microcephaly, hypertelorism, upslanting palpebral fissures, ectrodactyly of the left hand with four fingers due to absent left middle finger, right foot second and third toe syndactyly left foot overriding toes, coronal hypospadias, and right undescended testes.
Imaging revealed significant cardiac Patent ductus arterioles, Patent Foramen Ovale, bilateral atrophic kidneys with a small complex cystic mass on the left lower pole, and hepatocellular disease.
New born screening and chromosomal microarray were normal.
Whole Genome sequencing revealed a paternally inherited UBA2 (ubiquitin-like modifier-activating enzyme 2) gene mutation, but the father’s phenotype was a single bald patch on the scalp and hypertelorism.
Aplasia cutis congenital and ectrodactyly skeletal (ACCES) syndrome is characterized by highly variable expressivity, even within the same family. Most patients exhibit scalp defects, whereas ectrodactyly is less common; however, more variable and less obvious digital and skeletal anomalies are often present. Early growth deficiency and neurodevelopmental delay are also commonly seen.
The most specific aspects of the UBA2-related phenotype are Aplasia Cutis Congenita and ectrodactyly, which is less common (37%). Early growth deficiency and neurodevelopmental delay are reported in 61% and 80% of affected individuals, respectively.
Other observed features included other ectodermal variations (~82%), ocular abnormalities (53%), cardiac (43%), genital (50%, in males) and renal (36%) abnormalities.
UBA2 plays a vital role in the post-translational modification of protein (sumoylation) by adding SUMO1 (small ubiquitin-like modifier) protein. UBA2 forms a heterodimer with SAE1 (sumo-activating enzyme subunit 1) and binds with SUMO1 in an ATP-dependent manner. Unlike ubiquitination, sumoylation does not only target proteins for degradation but is involved in cell cycle regulation, subcellular trafficking, signal transduction, stress responses, and chromatin structure dynamics. Sumoylation alters protein kinases and transcription factors to maintain transcriptional regulation of tissue-specific gene expression.
The highly variable expressivity of the human UBA2 phenotype, either via sequence alteration or contiguous gene deletion, even within the same family, remains unexplained; there are likely other modifiers yet to be identified.
#201
“15 years of muscle weakness”: A case of limb girdle muscular dystrophy
Patel AA, Thukral J, Kaur H, Zahid A, Dargan KK, Hernandez EW, Lim AM, Oberndorf JK, Hambartzhumian R, Macwan S. Eisenhower Medical Center, Rancho Mirage, CA
Case Report: A 44-year-old woman presented with 15 yrs of progressively worsening proximal upper and lower extremity weakness. She had experienced difficulties since childhood, struggling to keep up with peers. Left quadriceps biopsy 15 yrs ago indicated severe mixed myopathic and neurogenic changes, leading to a diagnosis of polymyositis. Myoglobin and creatine kinase (CK) levels were elevated. Prednisone was administered without relief, and electromyography results were unable to be obtained.
Weakness worsened after pregnancy at age 21, impacting activities like climbing stairs and lifting her child. She also reported dysphagia, and denied family history of similar symptoms. On examination, she had generalized cachexia and a waddling gait. Motor strength was diminished: 2/5 in bilateral hip flexors and adductors, 4/5 in bilateral deltoid and biceps, 3/5 in bilateral triceps, and 4/5 in neck flexors.
Initial tests, including a myomarker panel, CK, barium swallow, serum immunofixation electrophoresis, serum protein electrophoresis, aldolase, and vitamin B12, yielded unremarkable results. Lower extremity MRI revealed nonspecific marked intramuscular fatty atrophy in bilateral thighs, with relative sparing of the vastus intermedius and no significant intramuscular edema. She declined repeat muscle biopsy at this stage.
Due to the progressive decline in strength and dysphagia, a presumptive diagnosis of inflammatory myopathy led to IVIG treatment (2g/kg every 3 weeks for almost 1 year). Her muscle strength did not recover, prompting the discontinuation of IVIG. Further genetic testing was conducted to investigate the possibility of muscular dystrophy, specifically Limb Girdle Muscular Dystrophy (LGMD). Genetic testing confirmed FKRP (1 pathogenic mutation p.L276I c.826C>A and 1 likely pathogenic p.Q482X c.1444C>T) consistent with autosomal recessive fukutin-related protein (FKRP) LGMD. She was referred to a tertiary care center and is undergoing evaluation as a potential candidate for clinical trials.
Discussion: Muscle weakness in adults can have various etiologies, from infections, autoimmune disorders to underlying systemic diseases, including malignancies. In this case, family history and autoimmune biomarkers were negative. Genetic testing is often necessary but challenging to arrange outside tertiary centers. Muscle biopsy and electromyography remain valuable diagnostic tools. Currently, treatment remains supportive as no targeted genetic therapies are approved, which explains the limited effectiveness of prednisone and IVIG in our patient. In hindsight, childhood muscle weakness should prompt suspicion of an underlying genetic disorder. Patient’s reported dysphagia should have raised concerns about systemic muscle pathologies.
#202
NO OOCYTES IN SIGHT: BIALLELIC LHCGR VARIANTS LEADING TO EMPTY FOLLICLE SYNDROME
Verma K1, Waud K2, Sule AM1, Aghajanova L3, Tise CG1. 1Stanford University School of Medicine, Stanford, CA; 2Pacific Fertility Center, San Francisco, CA and 3Stanford University School of Medicine, Stanford, CA
Purpose of Study: The luteinizing hormone/choriogonadotropin receptor (LHCGR) plays a critical role in both male and female reproduction. Binding of luteinizing hormone (LH) or human chorionic gonadotropin (hCG) to the LHGCR leads to a cascade of events which facilitates male sexual differentiation and female oocyte development and ovulation. Biallelic loss-of-function variants in LHCGR can cause primary amenorrhea, delayed puberty, and infertility in women. Empty follicle syndrome (EFS) is defined as the failure to retrieve oocytes after ovarian stimulation for in vitro fertilization (IVF) despite normal follicular development. We describe the clinical features of a female found to have LHCGR deficiency after being diagnosed with EFS, as well as the personal and familial reproductive implications of this autosomal recessive condition.
Methods Used: Chart review, physical examination, and literature review.
Summary of Results: A 33-year-old G0 female initially presented to medical care for primary amenorrhea at 17 years of age and was diagnosed with hypogonadotropic hypogonadism. Her family history was notable for a younger sister who also had a history of primary amenorrhea. Years later, the proband and her partner were interested in embryo banking for fertility preservation and underwent one IVF cycle with good response to ovarian stimulation and adequate follicular growth. However, two oocyte retrievals during this cycle revealed only the presence of cumulus cells with no eggs, consistent with a diagnosis of EFS. Genetic testing demonstrated a likely pathogenic 2p16.3 deletion involving exon 1 of LHCGR in trans with two hemizygous likely pathogenic variants in LHCGR. The proband was counseled that subsequent IVF cycles would likely be unsuccessful and she was recommended to consider other family building options. Genetic testing was advised for her sister prior to fertility planning or any fertility treatment.
Conclusions: Only seven other females have been reported in the literature with EFS due to biallelic loss-of-function variants in LHCGR. Elucidation of this genetic etiology has profound reproductive and medical implications for individuals, their partners, and other family members, yet is inevitably underdiagnosed. This case demonstrates the importance of considering a genetic etiology in cases of primary amenorrhea, delayed puberty, and infertility, particularly for patients with a positive family history and/or EFS.
#203
Plasmablastic Lymphoma in a HIV Negative Patient
Zahid M, Deemer E, Mishra S, Mehta S, Mezinord A, Morales G. Kern Medical Center, Bakersfield, CA
Case Report: Plasmablastic lymphoma ("PBL") is a rare and highly aggressive subtype of diffuse large B-cell lymphoma typically affecting oral mucosa, gastrointestinal system, lymph nodes, and skin, often associated with immunosuppression, particularly in HIV patients. Interestingly, PBL tends to occur more frequently in HIV(+) males, or in HIV (-) females. We report a unique case of PBL diagnosed in a HIV-negative, immunocompetent male. These patients respond poorly to chemotherapy and compared to HIV(+) patients, survive 9 months versus 14 months. Early diagnosis and treatment are critical in improving prognosis for patients with PBL.
Case Description: Patient is a 57-year-old man presented to our hospital for increased swelling and redness of the left face post resection of a fungating mass at the left maxillary area, 1 month prior to admission.
His vitals were stable and examination revealed poor dentition and left upper mandible swelling around molars with pus-like drainage. Molar appeared split down middle. Labs showed leukocytosis 17.6, hemoglobin 6.3, uric acid 14, blood urea nitrogen 145 and creatinine 18.7. Started on intravenous ampicillin-sulbactam for cellulitis over the surgical area. MRI demonstrated opacification of left maxillary, ethmoid, sphenoid sinuses extending from left zygomatic arch to left mandible regions. Pathology was consistent with plasmablastic lymphoma and negative for CD20, CD56, BCL-1, HHV-8, EBV ISH and positive for CD138, MUM1, ALK, Ki-67, c-myc. HIV was negative. AKI was secondary to light chain deposition related to malignancy with SPEP showing m-spike of gamma globulin, uric acid resolved with rasburicase. The patient underwent successful placement of a right internal jugular Port-a-cath and was eventually transported to HLOC.
Discussion: PBL is a rare subtype of diffuse large B-cell lymphoma characterized by proliferation of large, abnormal plasma cells. Usually associated with immunosuppression, particularly in HIV(+) patients. PBL commonly affects oral cavity, gastrointestinal tract and lymph nodes but can involve other organs. PBL has also been found to cause kidney injury through multiple mechanisms, including paraproteinemia, hypercalcemia, immune mediated glomerulonephritis, and amyloidosis.
An HIV(-), immunocompetent male with PBL is a unique presentation, as this type of lymphoma is typically seen in patients with HIV or other forms of immunosuppression. However, there have been a few reported cases in HIV(-) patients, suggesting that other factors are involved in the development of this lymphoma. It’s been suggested that chronic inflammation and immune dysregulation may play a role in the pathogenesis of PBL in HIV(-) patients. Early diagnosis and treatment are critical in improving the prognosis for patients with PBL. The standard treatment for PBL is combination chemotherapy with regimens used for other types of non-Hodgkin lymphoma. Stem cell transplantation may also be considered in select cases.
#204
Hodgkin’s lymphoma presenting with pulmonary symptoms
Orogian A1, 2, Dhillon H1, 2, Abraham J1, 2, Mann B1, 2. 1Kern Medical Center, Bakersfield, CA and 2David Geffen School of Medicine, Los Angeles, CA
Case Report: Typical presenting clinical signs and symptoms of Hodgkin’s lymphoma include painless cervical lymphadenopathy, fever, night sweats and involuntary weight loss. Very rarely do patient’s present with an unusual presentation such as the case presented below. Herein presented is a case of a young male who presented with cough and dyspnea.
A 26-year-old male with no known past medical history presents to the emergency department with productive cough and dyspnea ongoing for three months. Patient was endorsing cough for 3 months, productive of yellowish, greenish sputum without blood. As patient’s symptoms progressed to dyspnea along with the cough patient was evaluated at an outside facility 2 weeks prior to his presentation. At the time patient was diagnosed with pneumonia and discharged with a 10 day course of levofloxacin which patient stated he completed. Despite completing the course of antibiotics patient’s symptoms continued to worsen prompting him to present to the ED. Upon initial evaluation, patient was tachycardic and tachypneic, febrile and saturating on RA. Physical exam was significant for coarse breath sounds bilaterally and palpable, non-tender left axillary lymph node. Initial labs were significant for anemia, thrombocytopenia, leukopenia, lymphopenia, hyponatremia and hypocalcemia. Additionally, LDH and ALP were elevated. Initial CT chest w/contrast revealed thoracic and upper abdominal adenopathy, along with splenomegaly, suggesting lymphoproliferative disease along with right perihilar mass/consolidation and post-obstructive pneumonia, worst in the right upper lobe with cystic bronchiectasis. Subsequently CT abdomen with contrast was obtained which demonstrated enlarged lymph nodes in the retrocrunal, gastrohepatic ligament, porta hepatis, portacaval, pericaval, periaortic and aortocaval regions with the largest node being portacaval and measuring 3.2 x 4.1cm. Additionally marked splenomegaly, hepatomegaly along with retroperitoneal and upper peritoneal adenopathy was noted supporting lymphoproliferative disease. Excisional biopsy of the left axillary lymph node was performed resulting in coexpression of CD15 and CD30 with PAX5, consistent with classic Hodgkin lymphoma, lymphocyte-depleted subtype. Upon further investigation, patient was noted to have unintentional weight loss of 40 pounds over 3 months along with disturbed sleep, fatigue and excessive nausea. Given patient’s clinical symptoms and significant laboratory and diagnostic findings, patient was ultimately discharged home in stable condition. Patient is scheduled to begin chemotherapy with doxorubicin, bleomycin, vinblastine and dacarbazine for atleast 2 cycles.
Hodgkin’s lymphoma presenting with subtle symptoms of cough and dyspnea is an atypical presentation and warrants close attention and further thorough evaluation by practitioners to maintain broad differential diagnoses including malignancies when the pretest probability of other etiologies is greater.
#205
HURTHLE CELL THYROID CARCINOMA METASTASIZING TO THE LUNGS AND LIVER DUE TO DELAYED CARE PURSUANT TO RELIGIOUS CONVICTIONS
Sahadevan S1, Ghai V2. 1Adventist Health Bakersfield, Bakersfield, CA and 2AIS Cancer Center/Adventist Health Bakersfield, Bakersfield, CA
Introduction: Hürthle cell thyroid carcinoma (HCTC) is a rare type of thyroid carcinoma that comprises about 3% of all thyroid malignancies. HCTC largely has a poor prognosis if not treated in comparison with other well-differentiated variants since these tumors are generally more aggressive in nature. We present to you a unique case of a patient who had a progressively worsening HCTC with a large thyroid tumor burden metastasized to the lungs and liver since the patient opted out of treatment due to religious reasons after an early diagnosis five years prior.
Case: A 64-year-old Indian female presented initially upon feeling a mass on her thyroid area. She subsequently underwent a biopsy and was diagnosed with Hurthle cell carcinoma. The patient opted not to undergo radioactive ablation iodine treatment citing personal religious tenets, nor did she follow up with an oncologist. Five years later, the patient presented with worsening neck mass along with right upper quadrant abdominal pain and shortness of breath. She had a CT of the chest which showed a large mass in the right lobe of the thyroid gland with an additional mass partially imaged, large mediastinal nodes, and bulky adenopathy in the anterior mediastinum, along with a large infra hilar mass. The largest thyroid mass was 6x4 cm in size. There were also numerous infra hilar masses consistent with extensive pulmonary metastasis. She was also noted to have a large mass in the right lobe of the liver consistent with hepatic metastasis which was confirmed with a liver biopsy. She later underwent I-131 thyroid ablation and showed some response demonstrated by dropping thyroglobulin numbers and decreasing the size of the masses. A liver biopsy performed later indicated metastatic Hürthle Cell Neoplasm. A second, I-131 thyroid ablation was performed after she had further progression. A PET/CT showed the overall progression of metastatic disease; cervical metastatic lymphadenopathy, intrathoracic lymphadenopathy, increase in size of the right thyroid lobe bed with further tracheal deviation, and innumerable metastatic pulmonary nodules.
Discussion: In patients with HCTC, early diagnosis with prompt treatment has been shown to have a good prognosis. Metastatic HCTC is quite uncommon since these are low-grade tumors that have a favorable prognosis at an early stage if treated Whereas, increasing tumor size in untreated patients has shown to have an unfavorable prognosis with reduced survival rates. There has been a very small number of cases that have been reported on metastasis to the colon, skin, and pleura.
This case illustrates the progression of HCTC in a patient who delayed care secondary to personal religious convictions. As this case demonstrates the patient ultimately decided to pursue treatment. This case also escalates the necessity for clear, compassionate communication in the context of an individual’s personal conviction.
#206
Uncommon Presentation of Coccidioides immitis-Induced Dermatitis in a Young Adult
Al-Yousfi N, Abraham J, Mann B, Donsanouphit H, Afolabi O, Ashrafi A. Kern Medical, Bakersfield, CA
Case Report: Coccidioidomycosis, also known as "San Joaquin Valley Fever," is an infectious systemic fungal diseases predominantly prevalent in the Western Hemisphere, primarily in regions of the Southwestern United States, northern Mexico, and parts of Central and South America. While pulmonary disease is the most common manifestation, it can affect various organs. Cutaneous involvement is of particular significance due to its diverse clinical presentations, often posing diagnostic challenges. We report a case of a 23-year-old male with an intriguing presentation of a telangiectatic erythematous lesion filled with fluid, situated on the right upper chest. The patient reported tenderness and localized swelling as the primary symptoms, with no systemic or pulmonary complaints other than localized discomfort. Notably, the patient’s residence in an endemic coccidioidomycosis region, coupled with occupational exposure through fruit-picking in agricultural fields and positive cocci titers, raised strong suspicion of cutaneous coccidioidomycosis. A biopsy and fluid aspiration were performed on the lesion located on the right upper chest, followed by a gram staining procedure, which ultimately yielded the growth of Coccidioides immitis. This conclusive outcome not only validated the diagnosis but also facilitated the commencement of antifungal treatment, with fluconazole selected as the therapeutic option. This case emphasizes the importance of recognizing uncommon expressions of coccidioidomycosis in providing thorough and personalized patient care. Raising awareness of such unique clinical scenarios fosters improved diagnostic accuracy and, subsequently, better patient outcomes.
#207
A case of coccidioidal meningitis presenting with severe hydrocephalus
Dulani S1, 2, Mishra S1, Fox K1. 1Kern Medical Center, Bakersfield, CA and 2Western University of Health Sciences, College of Osteopathic Medicine of The Pacific, Loso Angeles, CA
Case Report: Coccidioidomycosis, caused by the soil-dwelling fungus Coccidioides, predominantly affects regions in the southwestern United States, Mexico, and parts of Central and South America. While often asymptomatic, some patients present with primary pulmonary disease, with varying degrees of severity. Rarely, the fungus disseminates, leading to extrapulmonary manifestations, such as central nervous system (CNS) involvement and meningitis. This abstract outlines the diagnosis and treatment of a 62-year-old male with a complex clinical presentation of coccidioidal meningitis and severe hydrocephalus.
Methods: A single patient case report was conducted after IRB approval
Case Presentation: A 62 year old male with alcoholic cirrhosis, obesity, and pulmonary coccidioidomycosis on suboptimal isavuconazole presented to the ER with altered mental status. The patient was diagnosed with primary pulmonary coccidioidomycosis in November 2018, with complement fixation titer of 1:32 and was started on fluconazole. The patient did not tolerate fluconazole due to side effects and was transitioned to isavuconazole in June 2019. The patient was lost to follow up and was inadvertently taking a suboptimal dose of isavuconazole. During this visit, the patient presented with confusion, forgetfulness, and persistent headaches. Physical exam was significant for midline lumbar tenderness and ataxic gait but negative for nuchal rigidity. Lumbar puncture (LP) was significant for elevated white blood cell count with lymphocytic predominance. MRI with contrast revealed loculated collections in the left cerebellar pontine angle, extending into the upper cervical canal, and diffuse hydrocephalus with compression of the cauda equina. VP shunt was placed, resulting in rapid improvement of mental status. The patient reached his baseline function and was discharged home. Upon follow up, the patient was found to have VP shunt infection with Proteus Mirabilis one month later, necessitating the removal of the shunt, placement of an external ventricular drain (EVD), and treatment with antibiotics.The patient’s clinical status continued to deteriorate, leading to discussions with the family regarding hospice care, and ultimately, the patient was transitioned to home hospice care.
Discussion: This case underscores the complexities of coccidioidal meningitis, especially in patients with interrupted treatment courses and neurological involvement. LP with measured opening pressure is a helpful tool for diagnosis of increased intracranial pressure in the setting of CNS coccidioidomycosis. If opening pressure fails to improve after serial LPs, VP shunt is warranted to prevent worse neurological outcomes. Immediate neurosurgical consultation should be obtained for placement of VP shunt in these patients. Physicians and patients should be aware of the risk of infection in patients with VP shunts. Multidisciplinary care and vigilant follow-up are crucial to managing these challenging cases.
#208
The Cheerio Sign: An Atypical Presentation of Coccidioidomycosis Masquerading as Metastatic Thyroid Cancer
Ghadiya K, Aranguri C, Khamlong M, Kahlon J, Munoz A. UCLA-Kern Medical, Bakersfield, CA
Case Report: The Cheerio Sign is a rare pattern seen on chest imaging, appearing as scattered, uniform nodular lesions with lucent centers that resemble the famous breakfast cereal. Differential diagnoses include atypical adenocarcinoma, pulmonary Langerhans cell histiocytosis, and vasculitis. Fungal infections may also present with this pattern, but very few reported cases are in the literature. This case report studies one such patient with the Cheerio Sign; his presentation was initially concerning for cancer, but he was eventually diagnosed with coccidioidomycosis. Currently, no documented cases of the Cheerio Sign are associated with coccidioidomycosis; this is the first case presenting with this pattern.
A 73-year-old male presented to the ED complaining of dysphagia and weight loss. His physical exam revealed a large left neck mass. His chest x-ray showed evidence of mass effect in the neck causing tracheal deviation, a right upper lobe consolidation, and diffuse pulmonary nodules concerning metastasis. CT scans confirmed the neck mass but further detailed the lung nodules, showing small uniform lesions with lucent centers surrounded by normal pulmonary parenchyma, characteristic of the Cheerio Sign. The patient was then admitted for concern of metastatic thyroid cancer, but later his thyroid biopsy was negative. CT-guided lung biopsy of the right upper lobe consolidation was also negative for malignancy. Fungal pathology was then considered as the patient lived in the Central Valley of California; serological testing soon showed positive titer levels for coccidioidomycosis. After undergoing bronchoscopy, BAL cytology confirmed a large presence of spherules resembling coccidioidomycosis. The patient was discharged on antifungal therapy with fluconazole and given appropriate follow-up with ENT for his neck mass. Three months later, the patient had a repeat chest x-ray that showed resolving nodular densities and improved right upper lobe consolidation.
This case is interesting because although the patient had signs of malignancy, his biopsies were negative. After initiating antifungal therapy, his chest x-ray improved. Thus, this is a novel presentation of coccidioidomycosis and can contribute to the existing radiologic literature as a rare pattern of the fungal disease process.
CT scan of the lungs showing small nodular lesions with lucent centers surrounded by normal pulmonary parenchyma.
#209
Infectious etiology of generalized polyarthritis: a diagnostic challenge
Inga Jaco E, Mann B. Kern Medical, Bakersfield, CA
Case Report: Neisseria gonorrhea is known to cause STDs, proctitis and pharyngitis, and oligoarticular arthritis. In the case of arthritis, it can cause arthritis-dermatitis syndrome, and purulent gonococcal arthritis with involvement of up to 4 joints including knees, ankles and wrists. In this case we present an atypical disseminated purulent gonococcal arthritis with involvement of big and small joints in a diabetic patient.
This is a case of a 47-year-old Hispanic male who presented with generalized body pain, it started four days prior to presentation as bilateral leg swelling. Then, was unable to move lower extremities and walk given nonlocalizing excruciating pain. Later, pain and lack of motion covered upper extremities. Physical exam noted adequate sensation all throughout, no skin changes, profound weakness in all extremities, decreased mobility with severe excruciating pain that rendered further exams challenging. 2+ reflexes in upper extremities and areflexia of lower extremities were noted. Patient reported noncompliance with hypertension treatment, reported weekly heavy drinking. Patient denied allergies, surgeries, family diseases, STDs, drug abuse, recent infections, hospitalizations, headache, vision changes, fever, rigors, diaphoresis, cough, diarrhea, skin changes, dysuria, or purulent discharge. Laboratory work showed mild hyperglycemia, Mild leukocytosis 13.8 k/uL (normal 4.5 -11.0 k/uL) with neutrophils 85.0% (normal 50.0 to 75.0%), CRP 25.40 mg/dL (normal high ≤ 0.30 md/dL), ESR 89 mm/hr (normal high ≤ 15 mm/hr), A1c 11.6%, TSH 6.832 mcIntlUnit/mL (normal 0.550-4.780 mcIntlUnit/mL), free T4 1.0 ng/dL (normal 0.9-1.8 ng/dL), positive ANA screen with nuclear homogenous pattern, ANA titer 1: 40, complement C3c 207 mg/dL (normal 82-185 mg/dL). Patient had noncontributory levels of Centromere B Ab, complement C4c, CCP Ab IgG, DNA (ds) Ab, rheumatoid factor, SCL 70 Ab, Sjogre’s Ab (SS-A and SS-B), Smith Ab, Sm/RNP Ab, thyroid peroxidase Ab, folate RBC, CK, HIV, syphilis, urine toxicology, B9, B12, and hepatitis panel. As medical necessities were addressed, patient was able to localize pain in multiple bigger and small joints. Upon suspicion of polyarthropathy, patient reported a recent unprotected sexual encounter. Knee aspirate rendered rare Neisseria gonorrhoeae and patient was diagnosed with acute disseminated purulent gonococcal arthritis. Antibacterial treatment helped with slow regain of range of motion of all joints.
This presentation of acute disseminated purulent gonococcal arthritis in multiple small and big joints, associated with immobility, and masked with severe pain in all extremities could be explained by a rapid spread of the bacteria in an already immunocompromised body. The rapid and extraordinarily vast level of Neisseria gonorrhea infection in a newly diagnosed diabetic patient is an example of atypical presentations of diseases on the diabetic population, an idea that all clinicians need to keep in mind.
#210
ATYPICAL PRESENTATION OF COCCI MENINGITIS WITH HYDROCEPHALUS
Johar L, Davtyan E, Bhandohal J. Kern Medical, Bakersfield, CA
Case Report: Coccidioidomycosis is an infection caused by the fungus Coccidiodes imitis and C. poasadasii and is prominent in southwestern United States and Central and South America. This infection is transmitted via inhalation of fungal spores. In 2019, CDC reported that there were 20,300 Valley Fever cases, with most of them in Arizona or California. One of the most severe extrapulmonary coccidioidomycosis is coccidioidomycosis meningitis.
Typical presentation of coccidioidomycosis meningitis includes headaches that can be persistent, progressively worsen, or have unusual severity. Patients can also present with fever, nausea, vomiting, blurry vision, photophobia, altered mental status, hearing difficulties
Methods: A retrospective review following IRB approval
Summary of Results: A 60 year old hispanic female, agricultural worker presented to the emergency department with chief complaint of nausea associated with mild headaches and intermittent presyncopal symptoms for 10 days. Initial physical exam was unremarkable with no pertinent findings. Initial labs including cbc with differential and basic metabolic panel were unremarkable. Initial CT head without contrast demonstrated acute hydrocephalus with dilated lateral, third and fourth ventricles suggesting obstruction at the basal cisterns. Potential etiologies for hydrocephalus considered at the time were infectious versus chronic meningitis versus autoimmune versus metabolic vs idiopathic. Subsequently, MRI Brain with and without contrast was completedd revealing communicating hydrocephalus. Lumbar puncture was also completed showing CSF coccidioidomycosis IgM IgG positive, 1:128 titer. Serum IgM and IgG for coccidioidomycosis were also positive 1:32 titer. Patient was treated with fluconazole 1000 mg IV daily inpatient, which was switched to fluconazole 1200 mg PO daily after discharge. After hospital discharge, patient was followed at the Infectious Disease clinic with no further worseninng symptoms after initiation of antifungal treatment.
Conclusion: Majority of patients with meningitis have clear signs and symptoms and distinguishable features pointing towards the diagnosis. However, in this case given patient presented with atypical signs of hydrocephalus, meningitis was not amongst the initial differential. In addition, this patient’s symptoms started ten days ago, which is unconventional as coccidioidal meningitis typically presents weeks to months after initial infection. Anatomic shunt combined with Ommaya reservoir insertion is usually definitive for symptomatic relief in coccidioidal meningitis with hydrocephalus. Interestingly, our patient’s symptoms resolved with oral antifungal treatment without needing further intervention including an antomic shunt, which also contributes to the atypicality of her case.
#211
HIV-Associated Burkitt Lymphoma presented as Submandibular Infection
Kooner L1, D’Assumpcao C3, Heidari A2. 1Rio Bravo Family Medicine Residency Program at Clinica Sierra Vista, Bakersfield, CA; 2Dignity Health, Bakersfield, CA and 3Kern Medical, Bakersfield, CA
Case Report: A 39-year-old Caucasian male diagnosed with HIV seven months prior and non-compliant with combined antiretroviral therapy presented to the emergency room for right-sided jaw pain and swelling for one week. The patient had a history of multiple dental infections with multiple teeth removals due to decaying teeth. He endorsed chills, however denied fevers and night sweats. Vitals and labs were unremarkable. CT of the neck showed a 29 x 25 mm low-attenuation lesion in the right submandibular region. Differentials were branchial cleft cyst, infected cystic structure, and phlegmon. He was admitted and treated with IV Ampicillin/Sulbactam and discharged a day later with a 10-day course of Amoxicillin/Clavulanic Acid.
After one month, the patient presented to the infectious disease clinic with difficulty swallowing and elevated tongue. He denied headache, fever, chills and dyspnea. After ENT consult, patient was sent to the ED where CT of neck with contrast showed the mass had increased in size to 58 x 46mm in the right submandibular region with a necrotic center. There was downward displacement of the platysma muscle and lateral fascial plane between the mass and the right genioglossus muscle, lucency surrounding mandibular lateral incisors or premolar and the mass completely surrounded a branch of the right fascial artery. A 15 x 12 mm ovoid lymph node adjacent to the medial aspect of the mass.
Ultra sound guided right submandibular gland mass core biopsy was used to diagnosed high grade B-cell Lymphoma with malignant cells staining positive with CD20, BCL6, CD10 and nearly 100% with Ki61. FISH study demonstrated a MYC rearrangement t(8;14). Findings were consistent with Burkitt Lymphoma.
A month later the patient was admitted for treatment with dose-adjusted etoposide, prednisone, vincristine, cyclophosphamide, doxorubicin, and rituximab (DA-R-EPOCH). Rituximab was given first. There was increased swelling to his jaw over submandibular mass. He received Decadron and swelling improved. He received DA-EPOCH two days later. Perineal rash was noticed and he was started on clotrimazole and lidocaine creams which improved the pain. He then completed the rest of the chemotherapy cycle 48 hours later. Allopurinol 300mg was given daily, but no rasburicase was indicated because uric acid was not elevated.
Sagital view of submandibular Burkitts Lymphoma.
#212
EARLY RECOVERY FROM EPSTEIN BARR VIRUS-INDUCED PNEUMONITIS WITH EARLY CORTICOSTEROID ADMINISTRATION IN IMMUNOCOMPETENT ADOLESCENT
Morton M1, Purdie D2. 1UC Irvine School of Medicine/CHOC Children’s Hospital of Orange County, Orange, CA and 2MemorialCare Miller Children’s and Women’s Hospital, Long Beach, CA
Case Report: EBV-induced pneumonitis is rare in immunocompetent patients. While case reports recommend multimodal treatment with severe disease (i.e., ARDS), the authors present a case of an immunocompetent adolescent with EBV-induced pneumonitis and pARDS that was responsive to early administration of corticosteroids.
Case: A 15-year-old previously healthy female presented with a 1-day history of midsternal chest pain. Her symptoms began approximately 5-6 days prior to admission with mild sore throat, headache and fatigue. She denied vaping/illicit drug use or recent travel. There is a parrot that lives inside her home. Her initial labs showed mild hyponatremia (sodium = 132), mild transaminitis (ALT =171; AST =281), positive monospot and negative respiratory viral panel by PCR. Chest x-ray was clear. She was admitted for monitoring. Within a few hours, she developed shortness of breath. Her vitals were significant for fever to 101.3, tachycardia to 150s and hypotension to 80/50. Her tachycardia mildly improved with fluid resuscitation, but she developed hypoxemia to 80’s. Chest x-ray showed bilateral infiltrates with no cardiomegaly. Her cardiac work-up was negative. Repeat chest x-ray showed worsening bilateral infiltrates. There was concern for atypical pneumonia, viral pneumonia or psittacosis and she was started on Ceftriaxone and Doxycycline. During the next 24 hours, her work of breathing and hypoxemia progressed despite escalating HFNC and she was transitioned to bilevel positive airway pressure. Her acute respiratory failure with hypoxemia (SpO2/FiO2 ratio = 199) associated with bilateral infiltrates on chest x-ray suggested development of pediatric acute respiratory distress syndrome (pARDS).
On HD#3, her EBV VCA IgM resulted positive (117). The remainder of her infectious work-up was negative including testing for Covid-19, psittacosis and coccidiomycosis, which is endemic to our area. After discussion with infectious disease and pulmonology specialists, she was started on intravenous methylprednisolone 2 mg/kg/day for EBV-induced pneumonitis. Her oxygen requirement had improved (FiO2 40% on HFNC) in 24 hours. By HD#4, she was transitioned to low flow nasal cannula. She was transferred to the floor and discharged by HD#6 with a steroid taper over two weeks.
Summary/Conclusion: This case presents an immunocompetent patient with EBV-induced pneumonitis and rapid progression to pARDS. Proposed mechanisms for acute lung injury in EBV-induced pneumonitis include accumulation of the virus secondary to rapid viral replication, an autoimmune reaction to the underlying infection and/or both. Most cases reports describe patients successfully treated with combinations of antivirals, corticosteroids and/or immunoglobulins. Our patient’s early recovery without antivirals or immunoglobulins suggests that steroid monotherapy may be sufficient owing to the regulation of EBV-associated immunological reactions in lungs.
#213
FOURNIER’S GANGRENE IN A DIABETIC PATIENT: A CASE REPORT
Nguyen S1, Nguyen T2, Columbus J1. 1Trinity Health System, Steubenville, OH and 2Ben Taub Hospital, Houston, TX
Case Report: Necrotizing fasciitis (NF) or Fournier’s Grangrene is a rapidly progressive, life-threatening infection of the deep fascia and subcutaneous tissue. Comorbid conditions such as diabetes, obesity, immunosuppression, and disruption of skin integrity place patients at higher risk for NF. Mortality rates range from 25-42%, underscoring the need for early recognition and aggressive treatment for improving patient outcomes.
Case Presentation: A 68-year-old male with a history of diabetes, emphysema, and chronic obstructive pulmonary disease (COPD) presented with a left buttock abscess. The patient reported pain in the area for the past four days, which was aggravated with walking. He denied fever, chills, nausea, vomiting, tingling, numbness, shortness of breath, lower extremities weakness, or changes in urination. Vital signs were unremarkable. Physical examination revealed erythema radiating from the left anal verge to the base of the left scrotum along the left medial buttock, with no area of fluctuance. An open wound was discovered on the left medial buttock, accompanied by tenderness and a mass on digital rectal examination.
Discussion: A perianal abscess was suspected initially because of the patient’s diabetes history. A CT scan of the pelvis was ordered to determine the depth of the abscess. During the patient’s evaluation, he developed a fever of 102°F, met systemic inflammatory response syndrome (SIRS) criteria, and was started on sepsis workup and treatment, including IV fluids and IV antibiotics. The patient’s CBC showed an elevated white blood cell count, with elevated neutrophils, and the complete metabolic panel revealed evidence of acute kidney injury, which was likely his baseline.
A CT scan of the abdomen and pelvis revealed extensive gas within the subcutaneous tissues of the left perineum, extending into the left inguinal region, and moderate surrounding tissue edema and cellulitis. These findings were consistent with NF, and urgent surgical intervention was recommended.
Conclusion: This case illustrates the importance of diagnosing NF in patients with risk factors such as diabetes and the importance of early recognition and prompt treatment. NF is a rare but life-threatening infection that can rapidly progress to septic shock, with high mortality rates. Patients with a history of diabetes and perianal abscesses are at increased risk for developing NF. Prompt recognition and early surgical intervention are crucial for improving patient outcomes. A sepsis workup and treatment, including IV fluids and antibiotics, should be initiated in patients with suspected NF and signs of SIRS.
#214
Immune Reconstitution Inflammatory Syndrome from Fingolimod Withdrawal in a Patient with Cryptococcal Meningitis in s Multiple Sclerosis Patient
Okumoto L, Mishra S, Jestila T, Sharma R, Kuran R. Kern Medical, Bakersfield, CA
Case Report: Fingolimod, a medication that is used to treat patients with multiple sclerosis (MS), is a sphingosine-one-phosphate receptor modulator. It sequesters lymphocytes in lymph nodes, preventing them from contributing to an autoimmune reaction. Withdrawal of the medication can cause an immune system overreaction such as Immune Reconstitution Inflammatory Syndrome (IRIS). Because this medication suppresses the immune system, it is known to be associated in rare cases with progressive multifocal leukoencephalopathy (PML) and Cryptococcal Meningitis. Fingolimod induced cryptococcal meningitis occurs in 8/100,000 patients per year, while fingolimod induced IRIS happens in approximately 1/10 patients when this medication is stopped. This patient had a rare occurrence in which the patient had both IRIS and cryptococcal meningitis occurring simultaneously.
Case Description: The patient, a 60-year-old male with medical history of MS on Fingolimod, presented to the emergency department with concern of altered mentation and weakness. Initially patient was admitted to the critical care unit and underwent lumbar puncture (LP) which resulted positive for cryptococcus antigen and India ink stain. Subsequently, amphotericin and flucytosine therapy was initiated. During patient’s hospitalization it was determined that the patient had developed IRIS secondary to discontinuation of long-term MS therapy (Fingolimod) on admission, and therefore dexamethasone 20mg daily was added, which resulted in significant clinical improvement of the patient’s altered mentation. LP was repeated, cultures revealing rare cryptococcus. Amphotericin was discontinued after 1 week upon negative cultures and the patient was initiated on fluconazole 800mg for 4 weeks followed by 200mg daily life-long. Throughout hospitalization, the patient’s clinical signs and symptoms improved significantly and the patient was discharged to an acute rehab facility in stable condition.
Conclusion: This case illustrates the complications that can arise from the use and discontinuance of Fingolimod. Its use puts the patient at risk for Cryptococcal Meningitis, while it can cause IRIS when the medication is discontinued. Clinicians should be aware that a patient can develop both.
#215
SPIROCHETE INFECTION INDUCED BITEMPORAL LIMBIC ENCEPHALITIS IN AN ELDERLY MALE
Rodriguez A, Davtyan E, Mann B. Kern Medical, Bakersfield, CA
Case Report: Limbic encephalitis is a clinical syndrome characterized by acute or subacute changes to mood and behavior, short-term memory deficits, cognitive decline, and structural and functional changes to the mediotemporal regions of the brain. It has been often defined as a paraneoplastic syndrome most commonly associated with small cell lung carcinoma. Otherwise, when no underlying occult neoplasm is found, autoimmune etiology is frequently suspected and, in many cases, proven to be symptomatically responsive to immunotherapy. However, cases of limbic encephalitis are not solely exclusive to paraneoplastic and/or autoimmune etiologies, but also viral such as HSV. In rare cases, limbic encephalitis has also been associated with Treponema pallidum.
Methods: A Retrospective review following IRB approval
Summary of Results: A 73-year-old male with history of hypertension, HFrEF 25%, CKD and dementia presented to the emergency department with altered mental status and cognitive decline. Upon evaluation, MMSE 16/30 suggested cognitive impairment. Initial labs significant for positive syphilis RPR and FTS-ABS with 1:4 titer. MRI Brain without contrast showed T2 hyperintensity involving the bilateral medical temporal lobes, suggesting encephalitis. CSF revealed increased protein level of 49.7mg/dl. Initial physical exam significant for confusion as patient was oriented only to self and situation. Further extensive laboratory workup including hepatitis panel and pertinent altered mental status workup resulted negative. Given patient’s overall clinical status, initial lab finding of positive syphilis along with the MRI findings, patient was subsequently treated with penicillin G 3 million units every 4 hours IV daily for neurosyphilis for a total of two weeks. Throughout hospitalization, patient’s cognitive decline improved with the course of the treatment. As patient continued to remain altered to location and time, further collateral information was obtained from the patient’s family and it was found that patient endorsed history of dementia at baseline. Patient eventually was discharged to skilled nursing facility in stable condition.
Discussion: Limbic encephalitis is commonly associated with paraneoplastic syndromes and autoimmunity. However, it can also be due to other infectious etiologies such as HSV and in rare instances, Treponema pallidum. This particular case is noteworthy as our patient presented with acute-to-progressive cognitive changes, limbic symptoms, bilateral mediotemporal lesions on MRI suggesting encephalitis. Given patient’s lab resulted positive for RPR and FTS-ABS, patient was initiated on Penicillin G IV therapy for neurosyphilis and throughout his hospital course was able to return to his baseline mental status.
#216
PERONEUS TERTIUS VARIANTS AND THEIR DISTINCTNESS FROM EXTENSOR DIGITORUM LONGUS
Bas A, Kay K, Wedel M. Western University of Health Sciences, Pomona, CA
Purpose of Study: The peroneus tertius (PT) is a muscle of the anterior leg compartment that contributes to foot eversion and dorsiflexion. PT is highly variable and often blends with extensor digitorum longus (EDL) to some degree. This complicates the classification of the two muscles and their variants. Complete doubling of PT, including its tendon, has only been reported once before. Tripling of the tendon is also extremely rare, and neither variant has been described before in detail. The purpose of this study is twofold: 1) To document complete duplication and tendon tripling of peroneus tertius in two dissected cadaveric subjects 2) To offer more precise nomenclature regarding PT morphology.
Methods Used: The anatomic variations presented in this study involved two human cadavers donated through the willed body program at Western University of Health Sciences. The subjects described herein were identified through routine cadaveric dissection for first-year osteopathic medical students in the gross anatomy lab. We found these two subjects in a survey of 184 limbs of 92 donors. Standard surgical dissection tools were used to perform dissection.
Summary of Results: In Subject 1 we observed complete duplication of the PT muscle and its respective tendon. One PT muscle belly attached along the fibula more proximally than the other. Both PTs extended distally and each formed their own single tendon that attached to the base of the fourth and fifth metatarsal, respectively. In Subject 2 we identified two muscle bellies that gave rise to three peroneus tertius tendons. The proximal muscle belly, which is a blend of PT and EDL, formed a proximal tendon, while the distal muscle belly formed a distal tendon. Additionally, both muscle bellies contributed separate tendinous slips that coalesced to form a middle tendon. All three tendons inserted at the base of the fifth metatarsal.
Conclusions: Most tendons insert on a single bony feature, and are therefore less ambiguous to identify than muscle bellies, which often originate from multiple surfaces and may give rise to multiple tendons. PT and EDL develop from the same sheet of embryonic tissue, and their muscle bellies occasionally fail to differentiate completely. Nevertheless, we need a way to distinguish the components of these muscles that insert on the metatarsals (evertors) from those that insert on the phalanges (digital extensors). We propose that tendons from the anterior leg muscles that insert on the dorsal surfaces of metatarsals 4 and 5 should be identified as PT tendons, and tendons that insert on the digits should be identified as EDL tendons, regardless of which muscle bellies they originate from.
#217
TOPOGRAPHY AND MORPHOMETRICS OF THE CARTILAGE SURFACES IN THE PERITALAR JOINTS
Nocek M, Challapalli A, Kumar A, Zhu M, Oudakker J, Wittels S, Hunt KJ, Myerson M, Li S. University of Colorado, Aurora, CO
Purpose of Study: Recent studies highlight the important role of peritalar joint congruence in maintaining alignment of the hindfoot. Peritalar subluxation is associated with a variety of pathological deformities including flatfoot, cavovarus foot, and clubfoot, as well as stress fractures. To date, studies of peritalar joint congruence have all been performed using X-ray, Weightbearing Computed Tomography based direct measurements, or 3D segmentation and analysis. However, none of these techniques can demonstrate the cartilage location nor disruption, nor the exact location of the articulation on the bone surface. Data bias caused by these limitations is therefore inevitable. This study used 3D surface mapping to assess morphometrics of the cartilage surfaces of the peritalar joints.
Methods Used: 11 fresh-frozen cadaveric feet without trauma, surgery, nor significant deformities were dissected to expose the calcaneus, cuboid, talus, and navicular bones, and the articular surfaces. Surface mapping of the articular surfaces and the two bones was completed using an Artec Space Spider 3D scanner and Mimics. Further digital analysis was completed using GeoMagic Studio 10. T-test was used for statistical comparisons, with p<0.05 as statistically significantly different.
Summary of Results: Data on the articular surfaces is summarized in Table 1. The average articular area on both sides of the joint matched each other well in the posterior facet of the subtalar (ST) joint (4% difference) and calcaneocuboid joint (3% difference) without significant statistical difference, but not in the anterior & middle facets of the ST joint, nor the talonavicular (TN) joint. In the anterior & middle facets of the ST joint, the cartilage articular area on the talar side was 124% of that on the calcaneus (p<0.05), and in the TN joint the cartilage articular area on the talus was 138% of that on the navicular (p<0.05).
Conclusions: The cartilage articular surfaces in certain peritalar joints do not match its opposing surface in size. In the TN joint, it is easy to understand since area of the socket must be much smaller than that of the ball in order for the joint to glide and rotate. There must be functional reasons for this phenomenon to happen in the anterior and middle facets of the ST joint, which need further investigation. This study shows that the extent of subluxation of the peritalar joints may be physiological and not necessarily pathological.
Table 1. Cartilaginous articulation area of the peritalar joints. *, **: Statistically significant area difference between the two cartilaginous surfaces in the same joint.
3D modeling
#218
STANDARDIZING MANAGEMENT OF PATENT DUCTUS ARTERIOSUS IN A REGIONAL NEONATAL INTENSIVE CARE UNIT: A QUALITY IMPROVEMENT INITIATIVE
Adigwu YN1, 2, Joshi R1, 2, Danon S1, Tay C1, Kokhanov A3, Iacob A1. 1Miller Children’s & Women’s Hospital Long Beach, Long Beach, CA; 2University of California Irvine, Orange, CA and 3Paul L. Foster School of Medicine at Texas Tech University Health Science Center at El Paso, El Paso, TX
Purpose of Study: Management of hemodynamically significant patent ductus arteriosus (PDA) includes pharmacotherapy and invasive PDA closure by surgical ligation or transcatheter device closure. In our regional level IV neonatal intensive care unit, we observed variation in PDA treatment and a high rate of surgical PDA ligation in very low birth weight (VLBW) infants compared to other units in the statewide network (10% versus 1%). The goal of this project was to standardize PDA management within our unit with the overall aim of reducing the surgical PDA ligation rate by 25% in VLBW infants during a six-month period.
Methods Used: Through several PDSA cycles, we created and implemented a PDA management guideline. Baseline data was collected from one year prior to guideline introduction. All infants with birth weight below 1500 grams were screened for inclusion. Exclusion criteria were death prior to PDA evaluation, pulmonary hypertension as a contraindication to PDA closure, or transfer to our unit for PDA ligation. Adherence to the guideline was tracked by process measures. Balancing measures included rates of bronchopulmonary dysplasia, necrotizing enterocolitis, and transcatheter PDA closure.
Summary of Results: Since implementation of the PDA management guideline, 36 eligible infants received treatment for PDA. Of these, 35 met the guideline definition of hemodynamically significant PDA and 33 were treated pharmacologically with recommended medications. 7 infants underwent surgical ligation and 7 were treated with transcatheter closure. While we did not have 25% reduction in PDA ligation rate during the six-month intervention phase, we did meet our aim during the maintenance phase of the project. Rates of surgical PDA ligation, transcatheter PDA closure, and overall mechanical PDA closure in VLBW infants decreased by 40%, 25%, and 33% from baseline, respectively. In VLBW infants treated medically for PDA, rates of surgical ligation, transcatheter closure, and overall mechanical closure decreased by 38%, 16%, and 32% from baseline, respectively. There was no significant change in the rate of bronchopulmonary dysplasia. There was a slight increase in the rate of necrotizing enterocolitis, from 4.1% at baseline to 5.9% after guideline implementation, however this difference was not statistically significant.
Conclusions: Standardization of PDA management through guideline implementation was feasible in our unit. There was a decrease in the surgical PDA ligation rate, transcatheter PDA closure rate, and overall mechanical PDA closure rate in all VLBW infants and in VLBW infants treated medically for PDA. This decrease is potentially attributable to the efficacy of pharmacotherapy. Continued follow up is needed to see the trends in mechanical PDA closure and the effects of the PDA management guideline on neonatal outcomes.
#219
DIAGNOSES, TREATMENTS, AND OUTCOMES IN A RURAL NEONATAL INTENSIVE CARE UNIT IN INDIA
Arredondo D1, Butt MF1, Ruf AM1, Panchal H2, Pathak P2, Patel S2, Malkan H2, Yadav K2, Patel N2, Judkins A3, Fassl B1. 1Northeast Ohio Medical University, Rootstown, OH; 2Shakti Krupa Charitable Trust, Mota Fofalia, India and 3University of Utah, Salt Lake City, UT
Purpose of Study: The neonatal mortality rate in rural India is twice that in urban areas, where admission to a newborn intensive care unit is commonly not an option. As a pilot project in collaboration with the government, Mota Fofalia Community Health Center (MFCHC), located in a rural community in Gujarat, India, established a small NICU in 2016 to fill the gap of intensive care services in rural areas. The purpose of this study is to describe the patient, disease, treatment, and outcome characteristics of patients admitted to a rural Indian NICU.
Methods Used: The retrospective study took place at MFCHC in May 2023. A team of students from NEOMED abstracted medical record information of infants admitted to the NICU from 2016-2023 from the patient logbook, which documents basic demographic admission, diagnosis, treatment and medical outcomes.
Summary of Results: 922 patients (45% female) were admitted to the NICU from January 2016 through June 2023: 21% were preterm births, mean birth weight: 2.39kg, mean admission weight: 2.27kg, and mean age at admission: 5.19 days. Most common diagnoses: neonatal jaundice (457/50%), low birth weight (236/25.8%), and respiratory distress (80/8.8%). 7 patients (0.76%) died and 52 (5.64%) were referred to higher centers; most common diagnoses of deaths and referrals were low birth weight and respiratory distress syndrome.
Conclusions: Neonatal jaundice, treated with phototherapy, is the most common condition at MFCHC’s NICU. Rural NICU care in India is feasible and may help reduce overcrowding in urban centers.
#220
OPPORTUNITY TO PREVENT BILIRUBIN-INDUCED NEUROLOGICAL DYSFNCTION BY IDENTIFYING FEMALE CARRIERS OF A G6PD CLASS 1 MUTATION
Bahr TM1, 2, Prince WL2, Agarwal AM1, Bhutani VK3, Christensen RD1, 2. 1University of Utah, Salt Lake City, UT; 2Intermountain Health, Murray, UT and 3Stanford University, Palo Alto, CA
Purpose of Study: To prevent bilirubin-induced neurological dysfunction (BIND) from occurring in all future generations of a very large White North American kindred that carries a Class I Glucose-6-phosphate dehydrogenase (G6PD) mutation (637G>T) which has resulted in many early deaths from severe jaundice and at least five cases of BIND among survivors.
Methods Used: In 2021 we reported on a large kindred, of European ancestry, in which 35 males have been affected with Class I G6PD deficiency, over seven generations, with most family members currently living in the Western part of North America (PMID 34773909). Recently we were made aware of another large kindred, living predominantly in the Eastern part of North America, with at least seven severely affected males with G6PD deficiency over three generations.
Summary of Results: We determined that this kindred carries the same mutation as our original Western kindred (Class I, c. 637G>T). Moreover, our genealogical research has determined that the matriarch of our Western kindred and the matriarch of the Eastern kindred were first cousins. This family tree now extends to nine generations of severely affected individuals in the United States.
Conclusions: The family members who participated in this genealogical research believe that a great number of women in this large kindred who carry the G6PD Class I mutation are unaware. Thus these women are at substantial (50%) risk that male offspring will be affected. By identifying the carriers and providing education to them and their medical care teams, anticipatory guidance during the immediate newborn period can result in rapid identification of affected babies, with timely administration of mitigation strategies such as phototherapy, thus avoiding BIND in future generations. We have developed a research protocol to seek out possible carriers, offer carrier detection with studies run at the ARUP laboratories, and return the results with anticipatory guidance. Despite the costs, time, and resources required in this endeavor, we are compelled by the opportunity to prevent further cases of BIND in this large and vulnerable kindred.
#221
ASSOCIATION OF TREATMENTS FOR PATENT DUCTUS ARTERIOSUS WITH NECROTIZING ENTEROCOLITIS IN PRETERM INFANTS
Cautivar KM1, Cacho BJ2, Jennings H1, Chun P3, Marshall A3, Deming D2. 1Loma Linda University School of Medicine, Loma Linda, CA; 2Loma Linda University Medical Center, Loma Linda, CA and 3Loma Linda University Medical Center, Loma Linda, CA
Purpose of Study: We examined the association of different treatment options for patent ductus arteriosus (PDA) in preterm infants born at < 30 weeks gestation with the development of necrotizing enterocolitis (NEC).
Methods Used: We reviewed medical records of neonates born in Loma Linda University Children’s Hospital with gestational age < 30 weeks between October 2017 through July 2023. The various PDA treatment protocols included: no treatment, pharmacological therapy (ibuprofen, acetaminophen, or indomethacin), surgical ligation, and catheter occlusion. We assessed the association of each management type with the development of NEC. Data were analyzed using descriptive statistics, Chi-square analysis, and logistic regression (SPSS v28, IBM).
Summary of Results: We identified 368 infants out of which received: 183 no treatment, 145 pharmacologic treatment, 16 surgical ligation, and 24 catheter occlusion. There was no significant difference between the incidence of NEC and any of the various management types (Table 1).
Conclusions: In our population NEC was not associated with any of the treatment types. Considerations for the power of this study must be made as the relatively limited sample size for NEC patients encourages additional data collection for further longitudinal study on this topic.
NEC
Model Variables
β
OR (95% CI)
p
No Treatment (Referent)
Pharmacologic Treatment
0.644
1.904 (0.790–4.588)
0.151
Surgical Ligation
0.254
1.289 (0.153–10.870)
0.816
Catheter Occlusion
1.016
2.762 (0.693–11.010)
0.150
#222
Early Onset Sepsis Risk Evaluation and Management of Infants Born at 34 weeks: A QI Project
Cheung S1, Tay C2, Iacob A2. 1University of California Irvine, Orange, CA and 2MemorialCare Miller Children’s & Women’s Hospital Long Beach, Long Beach, CA
Purpose of Study: Infants born 34w0d-34w6d represent a significant portion of moderate preterm NICU admissions. AAP recommends using delivery indications and infant’s presentation to decide blood culture and empiric antibiotics. Conversely, the Kaiser Early Onset Sepsis (EOS) Calculator uses maternal risk factors and infant’s presentation to determine blood culture and empiric antibiotics. Our unit’s heterogenous approach to EOS evaluation, often with providers choosing the AAP or Kaiser management based on preferences, led to this QI project. Our objectives include: 1) Standardize EOS management among 34w0d-34w6d infants, 2) Assess adherence to unit guidelines, 3) Assess antibiotic use and blood culture management under new guidelines.
Methods Used: The QI work is set in a 96-bed level IV NICU in an urban hospital. Participants include NICU nurses, newborn hospitalists, and neonatologists. The first PDSA cycle included a chart review of all infants born at 34w0d-34w6d in 2022 to review the unit’s management of EOS and identify areas of improvement. The second PDSA cycle included literature review and development of a unified approach to EOS management. In the third PDSA cycle, the use of a managment guideline based on Kaiser EOS score was tested. The most recent PDSA cycle involved the education of NICU and L&D nurses on the new guideline.
Summary of Results: Chart review revealed a heterogenous EOS approach for infants born at 34w0d-34w6d in 2022 (n=76) in our unit with 42% managed per AAP guidelines, 36% per Kaiser guidelines, and 22% with no guidelines documented. Baseline antibiotic usage rate in 2022 was 46%. During PDSA cycle 2, 12 out of 15 physicians responded to our survey; the majority opted to use Kaiser EOS Calculator.
Since the introduction of the Kaiser EOS score in December 2022, 60 infants born at 34 weeks have been admitted. The EOS score was documented in 51 infants (85% adherence). Blood cultures were obtained in 45 infants, of which 17 were unnecessary per EOS scores. A total of 21 infants (35%) received antibiotics, 4 of which did not meet criteria per EOS score. Our overall antibiotic usage rates and obtaining blood culture rates are displayed in Fig 1 and 2. One infant had a positive blood culture, which was captured by an elevated EOS score. No infant required additional septic workup in the first 3 days of life.
Run chart of antibiotic usage rates bimonthly 2022-current.
Conclusions: Implementation of a standardized EOS management guideline for infants of 34w0d-34w6d gestation led to a decrease in usage of antibiotics from 46% to 35% across an 8-month timeline, without any adverse effects.
#223
Fat Loss After Infusion of Fortified Human Milk in a Polyurethrane Plastic Feeding System
Hamilton V1, Fusezy M3, Elliott M3, 2, Ramanathan R1, CAYABYAB R1. 1LA General Medical Center, Los Angeles, CA; 2Pediatrix Medical Group, Baltimore, MD and 3Prolacta Bioscience, Duarte, CA
Purpose of Study: Polyurethane plastic tubing is used in feeding premature infants which have lipophilic properties that decrease the delivery of fat in Human Milk (HM). The purpose of this study is to quantify fat losses over time with simulated HM fortification strategies at different feeding duration and to determine if there is a HM fortification delivery method that may minimize fat loss.
Methods Used: Fortified and unfortified HM were studied for fat loss using an in vitro model of simulated feedings. Unfortified HM were Mom’s own milk (MOM), and donor human milk (DHM). Fortified HM were MOM fortified to 26 cal/oz (MOM H2MF26) and Ready to Feed 26 cal/oz (RTF26). Cream (Prolact CR) was mixed to final caloric content of 28kcal/oz (MOM H2MF28), 30 kcal/oz (MOM H2MF30) and (RTF26 CR, RTF 26 CR2). To examine methods of cream delivery, Prolact CR was administered first as bolus before infusion of fortified milk (CR MOM H2MF26) and (CR2 MOM H2MF26). The milks were infused in triplicate through a polyurethane plastic feeding tube and microbore extension tube to deliver 45 mL of milk feeding in a 60 mL syringe via an infusion pump for 30, 60, 120, and 180 minutes with new tubing for each run. After infusion ended, the tubing was flushed with 5 ml of air. All milk feedings were analyzed for Fat content by Mojonnier method.
Summary of Results: There were 130 samples analyzed for fat content. There was significant decrease in fat content in all types of fortified HM at 30 minutes (6.46-43.02% loss) (Figure). All fortified human milk delivered a higher fat content compared to MOM and DHM. Milks with higher fat content; MOM H2MF26, MOM H2MF28 and MOM H2MF30 experienced the highest fat loss over time (Figure). CR MOM H2MF26 and CR2 MOM H2MF26 had the lowest fat loss. There was no significant difference in fat loss between CR MOM H2MF26 and CR2 MOM H2MF26 (Table).
Conclusions: Fortified and unfortified HM significantly loses fat in a polyurethane plastic feeding system at 30 minutes feeding duration. Fortified HM have higher fat loss, however, had a higher fat delivered despite losses. Administering HM cream before infusion of fortified HM resulted in the least fat loss.
#224
Right aortic arch with aberrant left subclavian artery: radiography and computed tomography findings
Holden N2, Wyers M1. 1Ann & Robert H. Lurie Children’s Hospital of Chicago, Chicago, IL and 2College of Osteopathic Medicine of the Pacific, Western University of Health Sciences, Pomona, CA
Case Report: A vascular ring is a rare congenital anomaly in which abnormal vessels or other structures encircle and compress the trachea and esophagus. Generally, a double aortic arch is a “tight” ring that presents in patients earlier in life, while a right aortic arch (RAA) with aberrant left subclavian artery is a “loose” ring that tends to present later. According to the Edwards classification scheme, two types of right aortic arches (RAAs) predominate: Type I (59% of RAAs): mirror image branching of the great vessels; and Type II (40% of RAAs): aberrant left subclavian artery from a diverticulum of Kommerell. In a Type II RAA, the first branch off the aorta is the left common carotid artery, followed by the right common carotid artery, right subclavian artery, and then the aberrant left subclavian artery. The vascular ring is completed by a left ligamentum arteriosum/ductus arteriosus. We herein report a Type II RAA in an 11-month-old female who presented to the emergency room (ER) with tachypnea and coughing. The radiography revealed a leftward deviated trachea, and computed tomography revealed a right aortic arch with aberrant left subclavian artery. Notably, upon admission to the ER this patient tested positive for adenovirus and rhinoenterovirus, which likely made her symptoms more pronounced. The patient underwent genetic testing for 22q11.2 deletion syndrome as the patient was exhibiting developmental delays, and is awaiting surgical correction. The presence of the thymus in young children makes visualization of the aortic arch difficult on a chest x-ray, which is why it is important to look at the tracheal position in a frontal chest x-ray. Barium swallows, bronchoscopy, and echocardiograms are widely used for looking at associated abnormalities; however, CT and MR are crucial for surgical intervention, as they provide detailed anatomic information that characterize the vascular anomaly, extent of tracheobronchomalacial compression, and presence/location of associated abnormalities such as Kommerell’s diverticulum. Clinical outcomes for patients who undergo surgical correction are excellent with very low post-operative morbidity and mortality in the absence of other cardiac anomalies.
#225
First Breaths: An exploratory study evaluating the potential to create personalized 3D-printed CPAP masks for preterm infants
Holden N, Son J, Tran T, Park J, Wisser G, Mitsouras K. College of Osteopathic Medicine of the Pacific, Western University of Health Sciences, Pomona, CA
Purpose of Study: The American Academy of Pediatrics (AAP) recommends Continuous Positive Airway Pressure (CPAP) therapy with selective surfactant administration for preterm infants who are at risk for neonatal respiratory distress. This presents an exciting opportunity for the application of 3D-printed CPAP masks in preterm neonatal care. 3D-printing of CPAP masks is already an emerging field in pediatric medicine, particularly for infants with craniofacial abnormalities and obstructive sleep apnea. Research assessing the application and establishing technical protocols for integrating 3D-printed CPAP masks into preterm neonatal care is currently very limited. While products created by Kamath et al. (2022) and Mirnia et al. (2021) present different existing approaches for 3D-printing neonatal breathing devices (CPAP masks and cannulae), they also raise the issue of the lack of standardization. To this end, our study aimed to: 1) extend the current literature evaluating the need for 3D-printed CPAP masks in preterm neonatal care and 2) describe protocols and discuss considerations for potential prototype workflows within the context of preterm neonatal care.
Methods Used: PubMed and Embase were searched using the following key terms: 3D-printed, 3D-printing, personalized, preterm, early term, prebirth, neonatal, CPAP, and mask.
Summary of Results: Our results suggest that pronged masks warrant a customizable approach, as numerous studies note there is a high risk of nasal injury resulting from ill-fitting CPAP masks. Pressure ulcers or nasal trauma is a frequent complication in very low birthweight preterm infants using CPAP masks/masks with nasal prongs for extended periods of time. Mask fit issues can also result in unwanted leakage that may prolong reliance on these masks, which in turn may delay initiation of oral feeds, prolong hospitalization, limit infant holding, and interfere with the effective and timely implementation of necessary developmental therapies. Image acquisition modalities for producing personalized CPAP masks range greatly; notably, phone applications provide an accessible approach to facial scanning that allows for quick image acquisition in a patient demographic characterized by frequent movement.
Conclusions: Recent advances demonstrate that 3D-printing of CPAP masks for preterm neonates is not only feasible, but also accessible and has the potential to be widely implemented. As medical devices shift more towards personalized care, it is important to acknowledge the demonstrable need and ability to improve CPAP masks for preterm neonates. As new 3D-printed CPAP masks for preterm neonates undergo prototype development, future comparative studies assessing efficacy and comfort are warranted.
#226
Central line insertion complications in neonates: a retrospective chart review
Lane E, Sollinger C. UC Davis, Sacramento, CA
Purpose of Study: Central lines are an essential tool in any NICU, providing a long-term means of administering medications and nutrition to critically ill neonates. Some central lines must be removed due to a complication, with an estimated 15-25% central lines requiring early removal. The complications that can develop from the insertion of central line include infection, thrombosis, breakage, and malposition. The likelihood of an individual neonate developing these complications likely rests on a variety of risk factors. Improved understanding of these factors may alter the management strategy for specific neonates. The goal of this study is to examine the incidence of complications in central lines, specifically PICC lines and umbilical venous catheters, in our NICU.
Methods Used: All UVCs and PICCs inserted in our NICU during January to June 2021 were contemporaneously tracked to obtain baseline data as part of a future nursing-led quality improvement process. With each PICC or UVC insertion, the provider wrote a procedure note documenting the date of placement, indication for insertion, and a narrative describing immediate complications. Patient and catheter characteristics within this data set were reviewed within Epic, including primary diagnosis, duration of each catheter, and reason for insertion. Each UVC and PICC was reviewed to determine whether a complication such as malposition, thrombosis, infection, breakage, or unsuccessful attempt occurred during the catheter duration.
Summary of Results: On average, approximately 50 central lines per month were inserted in the UC Davis NICU. UVCs and PICCs were placed in patients with a diverse range of diagnoses, with the most common diagnosis being prematurity (49%). The most common reason for insertion was for administration of TPN (49%). UVCs tended to have shorter durations than PICC lines (average 4 days compared to 13 days). 51% of all lines had a complication. The most common complication was malposition (30%).
Conclusions: We observed relatively high rates of complication in our review. Our findings, in particular complications related to malposition, provide a foundation for future QI efforts in our unit. A central line bundle will be developed to focus on education about line insertion, and systems-based confirmation and maintenance of placements. There are limitations in interpreting the results of our study. Our data relies on detection of any complication, so the rates are dependent on how symptomatic a complication is or on the completion of recommended screening X-ray to detect malposition. Additionally, our review is limited to one institution and our standard of comparison is based on literature review as opposed to direct comparison. Further analysis could include incorporation of chi-square analysis and multivariate models to further characterize the significance of risk factors.
#227
NEONATAL GASTRIC PERFORATION: CASE SERIES
Mladenov GD1, Sharafeddin F1, Edelbach B2, Vacaru A2, Moores D1, 2, Singh Y3, 2, Radulescu A1, 2. 1Loma Linda University Children’s Hospital, Loma Linda, CA; 2Loma Linda University School of Medicine, Loma Linda, CA and 3Loma Linda University Children’s Hospital, Loma Linda, CA
Case Report: Neonatal gastric perforation (NGP) is a life-threatening condition that is associated with high morbidity and mortality rates. Of all perforations of the gastrointestinal tract in newborns NGP represents 7%. It has been shown that as a result of an increase in number of premature and low birth weight neonates the number of NGP cases increased as well.
Methods Used: After retrospective chart review, we report our experience with neonatal patients with gastric perforation treated at Loma Linda University Children’s Hospital Neonatal Intensive Care Unit.
Summary of Results:A total of 15 patients were treated at our neonatal intensive care unit between 2000 and 2023 with the diagnosis of NGP. The median age at admission was 2 days old, with 10 (67%) patients admitted before or at age 2 days old. The median birth weight was 2.075 kg and the median age at surgery was 5.5 days old. There were 4 (26.67%) patients that had a birth weight below 1 kg. The gender distribution in our group was the following: 10 (67%) males and 5 (33%) females and the 30-day mortality rate was 26.67% (4 patients), out of which 75% (3 patients) were males and 25% (1 patient) were females.
Conclusions: Our study supports the tendency in published literature of the male sex being a poor prognostic factor for both prevalence as well as survival in NGP patients. However, our results did not reinforce the higher NGP mortality paradigm among neonates with low birth weight. We found that the median time between admission and surgery in our group was 1.5 days, which confirms the importance of early determination of neonatal gastric perforation. Timely verification of disease manifestations will allow for more appropriate decisions on treatment methodologies in addressing surgical aspects of the disease.
#228
NEURODEVELOPMENTAL OUTCOMES FOLLOWING EXTRACORPOREAL MEMBRANE OXYGENATION
Owens D, Roundy J, Winter S, Maslach-Hubbard A, Carr NR, Profsky M, Yost CC, DuPont T. University of Utah Neonatal Follow Up Program, Salt Lake City, UT
Purpose of Study: Describe neurodevelopmental testing for infants discharged after extracorporeal membrane oxygenation (ECMO).
Methods Used: A seven-year retrospective review of infants who received ECMO at Primary Children’s Hospital in Salt Lake City, Utah, who underwent developmental testing through the University of Utah’s Developmental Follow Up Clinic. Developmental delay was defined as follows: Bayley Scales of Infant Development 3rd Edition (Bayley-III) score < 70 in any domain at 18-36 months, Developmental Assessment of Young Children (DAY-C) score of <70, or a 9-month Hammersmith Infant Neurological Exam (HINE) at > 9 months with score less than 62.
Summary of Results: Of the 28 infants who received ECMO, 24 infants had any type of developmental testing completed through the developmental follow up clinic between (May 26, 2013 and November 5, 2020). Infants excluded from the study either had a loss to follow-up or died prior to discharge. Of the 24 patients with any developmental testing, 10 had Bayley-III testing at 2-3 years of age, 6 had DAY-C testing at 3 years of age, and 11 had a HINE between 9-12 months of age. Ten patients (42%) had a developmental test concerning for significant developmental delay. Of these ten infants that had a Bayley-III performed the median scores were 85 (IQR 65-95) cognitive, 71 (IQR 53-112) language, and 81 (IQR 59-100) motor. There was no correlation between the length of the ECMO run and Bayley-III scores in any domain. Of the six infants with DAY-C testing, scores less than 70 were noted in four infants for expressive language and two for receptive language. Fine and gross motor scores were noted to all be >70. HINE scores were <65 in three infants.
Conclusions: There is limited data on neurodevelopmental outcomes for infants who experience ECMO. While 42% showed significant developmental delay on testing, the majority of ECMO recipients had average to low average range neurodevelopmental outcomes. This study is limited by its small sample size and potential selection bias. This study highlights the needed larger data sets to describe neurodevelopmental outcomes of patients who receive ECMO therapy as they relate to length of ECMO run, indication for ECMO, neuroimaging, and neuromonitoring during ECMO. Given the small number of neonatal ECMO performed at individual centers, there is an urgent need for collaboration with defined developmental testing to inform families and care givers on the outcomes of ECMO.
Demographics.
Normal Development
Developmental Delay
Sample Population
14
10
Female
7
7
Premature
2
5
Term
11
6
Average Length of ECMO Run (days)
6
10
Ischemia on Brain Imaging
0
2
Hemorrhage on Brain Imaging
4
1
Bayley-III Assessment
6
4
DAY-C Assessment
2
4
HINE Assessment
8
3
ECMO: extracorporeal membrane oxygenation; Bayley-III: Bayley Scales of Infant Development 3rd Edition; DAY-C: Developmental Assessment of Young Children; HINE: Hammersmith Infant Neurological Exam.
#229
Incidence and Risk Factors for Acute Kidney Injury in Extremely Low Birth Weight Infants– Experience at a Single Center Level III Neonatal Intensive Care Unit
Patel S, Ramanathan R, Barton L, CAYABYAB R. LAC+USC Medical Center, Los Angeles, CA.
Purpose of Study: Neonatal acute kidney injury (AKI) has been previously poorly studied with different definitions used. The incidence of AKI varies significantly from 18% - 55% using the modified KDIGO criteria. Recent studies in both pediatric and neonatal AKI suggest that survivors of AKI in the neonatal period are at increased risk for chronic kidney disease and warrant long-term follow-up. Studies have shown that neonatal AKI is very common, is associated with poor outcomes and certain risk factors such as being born extremely low birth weight (ELBW) have been established. The aim of this study is to determine the incidence of AKI in ELBW and identify risk factors.
Methods Used: Retrospective study of all ELBW infants admitted to the neonatal intensive care unit at Los Angeles General Medical Center from July 2015 to July 2023. Neonatal and maternal demographics, maternal and neonatal medications, laboratory results, clinical course and survival outcomes were collected. To define AKI, we used the Modified KDIGO criteria (Stage 1:SCr rise ≥ 0.3 mg/dl within 48 h or SCr rise ≥ 1.5-1.9 X reference SCr within 7d, Stage 2: SCr rise ≥ 2.0-2.9 X reference SCr, Stage 3: SCr rise ≥ 3 X reference SCr or SCr ≥ 2.2 mg/dl or receipt of dialysis. (Reference Scr is defined as the lowest previous SCr Value). Infants were grouped into AKI absent, and AKI present. We opted not to use urine output due to limitations of data collection.
Summary of Results: A total of 79 ELBW infants were included in the study. The incidence of AKI was 56% (35/79). Only 32 infants had data for staging. Majority of infants 26/32 (81%) had Stage 1, 4/32 (12%) had Stage 2 and 2/32 (6%) had Stage 3. AKI occurred at a median postnatal day of life 11 (IQR 6, 27) and resolved at median day 7 (IQR 4,14). ELBW infants who had AKI were significantly younger, of lower BW, higher rate of hypotension requiring vasopressor use and higher rate of exposure to indomethacin, gentamicin and vancomycin. There was no significant difference in gender, apgar scores at 1 and 5 minutes, use of antenatal steroid, delivery room resuscitation and use of furosemide between the two groups. There was no significant difference in maternal illness and maternal use of non- steroidal anti-inflammatory drugs, angiotensin converting enzyme inhibitors and substance use. (Table)
Conclusions: Our preliminary data showed that the incidence of neonatal AKI in ELBW infants within the first 2 weeks of postnatal life is high and likely under reported. Nephrotoxic medications should be judiciously used in lower BW, and lower GA ELBW, and their kidney function should be closely monitored. Collection of data is ongoing to increase the sample size to verify these findings.
Neonatal and Maternal Characteristics of the Study Population (n=79).
Maternal Angiotensin Converting enzyme inhibitor use, n (%)
1 (2)
1 (3)
0.87
Maternal Non-steroidal anti-inflammatory drug use, n (%)
1 (2)
2 (6)
0.44
Survival at discharge, n (%)
1 (2.3)
0 (0)
1
Median (25th, 75th percentile).
#230
Effect of longer extracorporeal life support and early treprostinilon survival in infants with severe congenital diaphragmatic hernia
Rice-Townsend S1, Puia-Dumitrescu M3, Riehle K1, Dellinger M1, Yung D2, Jackson E2, Foster C1, Ashe J1, Stark R1, DiGeronimo R3. 1Seattle Children’s Hospital, Seattle, WA; 2Seattle Children’s Hospital, Seattle, WA and 3Seattle Children’s Hospital, Seattle, WA
Purpose of Study: To compare infants with severe congenital diaphragmatic hernia (CDH) who received extracorporeal life supprt (ECLS) and treprostinil before andafter implementing a new treatment approach strategy in 2021.
Methods Used: This is a retrospective analysis of data from a single-center. All infants born between 2015-2023 with severe CDH were included. Severe CDH defined as lung to head ratio (LHR) < 1 or observed to expected (O:E) total fetal lung volume (TFLV) by MRI < 25%. Patients born prior to 2019 did not have fetal MRIs done routinely, therefore O:E TFLV were not available. Infants who did not receive ECLS or treprostinil during their stay were excluded. A new protocol was implemented in 2021, and the cohort was split in pre-intervention and post-intervention. Demographic data and clinical outcomes were describeed.
Summary of Results: 15 infants met inclusion/exclusion criteria, with 9 infants treated with standard care before 2021 and 6 infants treated with the strategy of early repair on ECLS, longer ECLS, and early initiation of treprostinil therapy (post 2021change).
5 infants in each group were initiated on treprostinil for pulmonary hypertension (PH). Tricuspid regurgitation was not measurable on every patient.
The infants treated with newer strategy (after 2021) had fewer bleeding or thrombotic adverse events on ECLS, longer length of treprostinil therapy, longer length of hospital stay and increased survival.
Conclusions: In this single center, small cohort, survival and ECLS associated adverse events appear improved. Improved survival is presumed to be due to less severe PH, fewer bleeding complications and decreased ventilator induced lung injury. Longer length of treprostinil therapy and hospital stay are likely related to the improved survival. The change in treatment strategy appears promising, but requires further validation
#231
IMPROVING PSYCHOLOGICAL SAFETY IN THE NICU CLINICAL LEARNING ENVIRONMENT
Sanchez R, Pham B, Boriski A, Brock W, Marenco Y, Dexheimer L, Catalan L, Freeman S, Geolina T, Lim A, Iseri J, Glenn T, Marc-Aurele K. University of California San Diego, San Diego, CA
Purpose of Study: Psychological safety (PS) occurs when learners feel comfortable raising concerns, asking questions, seeking feedback, and admitting mistakes. The hierarchy and traditions in medicine present barriers to building an environment of PS. Lack of PS in the culture of medicine is not acceptable, especially for medical trainees. In 2021 and 2022, our Neonatal-Perinatal Medicine fellowship ACGME survey identified an area of vulnerability in interprofessional teamwork at our clinical site. Our goal for this QI project was to increase PS in the clinical learning environment.
Methods Used: Staff and learners were surveyed starting in August 2022. Our outcome measure of PS was from a validated survey utilizing Likert scale responses to, “Members of the clinical team of which I am a part are able to bring up problems and tough issues.” Our SMART aim was to increase the percentage of respondents who strongly agreed with the PS measure by 15% within 7 months.
Our process measure was from a validated survey of PS utilizing Likert scale responses to, “People in this unit trust each other.” Our balancing measure was the time needed to do interventions to increase PS. A free text field queried, “What can we do to improve the Speak Up culture?” and data from free text answers were analyzed for themes. In response, we implemented “Speak Up” team rounds in stepwise PDSA cycles after the collection of baseline data.
Summary of Results: During the baseline period, the median percentage of respondents who strongly agreed with the PS measure was 37%. The median percentage of respondents who strongly/somewhat agreed to the PS measure remained high (88%). Common themes highlighted a need to improve involvement of staff on rounds (21%). After implementation of Speak Up Team Rounds, we noted a special cause variation and median shift for the PS outcome measure to 55%. The process measure of trust tracked closely with the outcome measure.
Conclusions: A multidisciplinary QI approach led to an increase of PS in the clinical learning environment. Asking for input from staff and implementing changes based on their input resulted in effective PDSA cycles. In addition, surveying every 2 weeks maintained a focus on PS. Future directions include further assessment of the balancing measure, formalization of educational materials for families on Speak Up Rounds, and a debriefing tool based on themes identified from our survey data.
#232
MATERNAL AND NEONATAL RISK FACTORS FOR THE SURGICAL TREATMENT OF NECROTIZING ENTEROCOLITIS
Sandhu JK1, Barton L2, Biniwale M2, Ramanathan R2, Yeh A2. 1Los Angeles General Medical Center, Los Angeles, CA and 2Los Angeles General Medical Center, Los Angeles, CA
Purpose of Study: Necrotizing enterocolitis (NEC) is one of the leading causes of morbidity and mortality in neonates, with a multifactorial pathogenesis. More severe cases may need surgical intervention. The purpose of this study is to identify and compare maternal and neonatal factors that increase the probability of NEC requiring surgical treatment.
Methods Used: This is a retrospective (February 2009 to June 2023) cohort study of neonates admitted to a Level III Neonatal Intensive Care Unit at Los Angeles General Medical Center who were diagnosed with NEC. Those who received medical treatment for NEC were compared to those who needed surgical intervention. Data was abstracted from the NICU database and electronic medical records, and analyzed using SPSS version 29.
Summary of Results: There were 91 infants included in this study. 67/91 received medical treatment for NEC (73.6%). 21/91 received surgical treatment for NEC (23.1%). The other 3.3% were either transferred or expired prior to receiving treatment at LA General Medical Center. 52.7% of our population was male; 46.2% was female. The mean gestational age was 31+1 weeks ± 4.6. The mean birth weight was 1470 grams ± 886. More than 80% of our population was of Hispanic descent. There was an association between mothers who were given antenatal steroids prior to delivery and infants who developed surgical NEC (71.4%) compared to medical NEC (38.8%), p=0.009. There was an association between mothers who were given magnesium sulfate prior to delivery and infants who developed surgical NEC (71.4%) compared to medical NEC (38.8%), p=0.009. There was no difference in medical and surgical NEC cases when comparing mothers with pre-eclampsia, chronic hypertension, diabetes mellitus, intrauterine growth restriction or presenting in preterm labor (Table 1). Infants with surgical NEC had lower birth weight (p=0.001), lower gestational age (p=0.004), and longer length of stay (p=0.008). The presence of intraventricular hemorrhage (IVH) was associated with infants who had surgical NEC (71.4%) compared to medical NEC (23.9%), p<0.001. The presence of patent ductus arteriosus (PDA) was associated with infants with surgical NEC (57.1%) compared to medical NEC (28.4%), p=0.016. Logistic regression analysis revealed IVH to be the most significant factor in the surgical NEC cases.
Conclusions: Our preliminary data showed that maternal exposure of antenatal steroids or magnesium sulfate prior to delivery was associated with greater percentages of infants who developed surgical NEC compared to medical NEC. Maternal characteristics of preeclampsia, chronic hypertension, diabetes mellitus, intrauterine growth restriction or presenting in preterm labor revealed no association with either medical or surgical NEC. Infants with surgical NEC had lower birth weight and gestational age and longer length of stay. They were more likely to have IVH or PDA. Collection of data is ongoing to determine other factors of significance and to verify these results in a larger sample size.
Demographics and outcomes of the study population.
PREDICTORS OF BLOOD GLUCOSE LEVEL IN LATE PRETERM AND TERM INFANTS AT RISK FOR HYPOGLYCEMIA WITHIN THE FIRST HOUR OF LIFE
Siddiqui S, Massoumi JY, Becerra V, Wertheimer FB, Ramanathan R, CAYABYAB R. University of Southern California/Los Angeles General Medical Center, Los Angeles, CA
Purpose of Study: Risk factors for hypoglycemia include preterm gestation, low birth weight, small and large for gestational age, antenatal steroids, and infants of diabetic mothers. Glucose monitoring is initiated soon after birth in these at-risk infants. This study aims to determine the predictors of blood glucose (BG) level within the first hour of life (HOL) in infants undergoing screening for hypoglycemia.
Methods Used: This is a retrospective (2017-2019) cohort study of term and late preterm newborn infants born at Los Angeles General Medical Center at risk for hypoglycemia and managed with our hypoglycemia prevention bundle. Neonatal and maternal demographics, use of oral glucose gel administered to infants with hypoglycemia defined as BG level below 45 mg/dL and outcomes were collected from the electronic medical record, paper records and the Neonatal Information System newborn database. Infants were divided into 3 groups: Group 1 = infants with BG greater than 44 mg/dL, Group 2 = BG 26 - 44 mg/dL and Group 3 = BG less than 26 mg/dL. First feeding was initiated within first HOL.
Summary of Results: There were 334 late preterm and term infants screened for hypoglycemia within the first HOL included in the study. 128/334 (38%) of infants developed hypoglycemia within the first hour of life and 27/334 (8%) had BG level under 26 mg/dL. Mean BG within the first hour was 64 mg/dL, 37 mg/dL and 17 mg/dL in Group 1, 2, and 3 respectively. There was no significant difference in the maternal and neonatal demographics between the three groups. (Table) However, linear regression showed that birth weight (Coef -0.009, 95%CI: -0.013, - 0.005; p value <0.01) and late preterm (Coef -12.48, 95% CI: -19.45, -5.52; p value <0.01) and early term infants (Coef -8.68, 95%CI -15.3, -2.05 p value 0.01) compared to full term infants had a significant negative association with BG level within the first HOL.
Conclusions: Our preliminary data showed that late preterm and early term infants have lower BG levels one hour after birth compared to full term infants and as the birth weight increases, the infant is at higher risk for lower BG level. Collection of data is ongoing to verify these results in a larger sample size.
Maternal and Neonatal Demographics of the Study Population.
Group 1
Blood glucose level > 44 mg/dL
N = 206
Group 2Blood glucose level between 26-44 mg/dLN = 101
RISK FACTORS FOR VERY LOW BIRTH WEIGHT INFANTS WITH ABNORMAL NEURODEVELOPMENTAL PATTERN DETECTION IN THE FIRST YEAR OF LIFE AND ITS IMPACT ON FUTURE DEVELOPMENT
Thirumalai H1, Manickam S1, 2, Ramanathan R1, 2, Biniwale M1. 1Keck School of Medicine of USC, Los Angeles, CA and 2Keck School of Medicine of USC, Los Angeles, CA
Purpose of Study: Bayley Scales of Infant and Toddler Development is an extensive formal developmental assessment tool for diagnosing developmental delays in early childhood. Very low birth weight infants (VLBW) are at significant risk of developmental delays that can be diagnosed and monitored at ages 6-12 months, 18-24 months and 36 months. The purpose of this study was to characterize the etiologies and outcomes of abnormal neurodevelopment patterns as detected by Bayley Scales of Infant and Toddler Development scores performed at high-risk follow-up visits at age 6-12 months.
Methods Used: Infants with BW<1500g referred to high-risk follow-up premature infant clinic between 6/1/2008 - 03/20/2020 were included in the study. A retrospective review of medical records was performed to collect neonatal events, diagnoses, neurological examinations at discharge, maternal risk factors, follow-up clinic evaluations and Bayley scales of infant development scores at ages 6-12 months, 18-24 months and 36 months. Bayley score averages of 4 and above were classified as normal and scores that were less than 4 were classified as abnormal.
Summary of Results: A total of 369 babies were included in this study. The incidence of abnormal Bayley scores in this population was 53%. The mean birth weight and gestational age were lower in infants who had abnormal Bayley scores at age 6-12 months. Significant factors that were associated with higher rates of abnormal Bayley scores at age 6 -12 months were severe intraventricular hemorrhage (IVH), seizures, abnormal neurological examinations at the time of NICU discharge, ages 6-12 months, 18-24 months and 36 months. These infants with abnormal Bayley scores at 6-12 months showed a significantly higher risk of developmental delays with abnormal Bayley scores at age 18-24 months and 36 months with abnormal neurological examinations at age 6-12 months, 18-24 months and 36 months. Logistic regression analysis adjusted for all significant factors showed that the most significant factors predicting abnormal Bayley scores at 6-12 months were birth weight (p=0.006) and seizures (p=0.035).
Conclusions: VLBW infants with seizures and lower birth weight are likely to present with abnormal neurodevelopment patterns as detected by Bayley Scales of Infant and Toddler Development scores at 6-12 months of age. These infants may continue to have abnormal neurological examinations and abnormal scores and are at higher risk for developmental delay in the first 3 years of life.
Characteristics of VLBW infants presenting with Abnormal Bayley Scales of Infant and Toddler development scores at 6-12 months of age.
Factors
Infants with abnormal Bayley scores at 6-12 months
N=194
Infants with normal Bayley scores at 6-12 monthsN=175
P value
Birth weight(g), mean (SD)
1017 (291)
1127 (253.7)
<0.001
Gestational age(wks), mean (SD)
27.8 (2.7)
28.6 (2.6)
0.005
1 min Apgar score, median (1st quartile, 3rd quartile)
6 (4,8)
7 (4,8)
<0.05
5 min Apgar score, median (1st quartile, 3rd quartile)
8 (7,9)
8 (7,9)
<0.05
Severe IVH, N (%)
18 (9.1)
5 (2.8)
<0.05
Seizure, N (%)
19 (9.8)
3 (1.7)
<0.001
Abnormal Bayley scores at 18-24 months, N (%)
122 (91)
87 (67)
<0.001
Abnormal Bayley scores at 36 months N (%)
74 (89)
46 (63.9)
<0.001
Abnormal neurologic exam NICU N (%)
34 (20)
13 (9.3)
<0.05
Abnormal neurologic exam at 6-12 months, N (%)
75 (44)
2 (1.4)
<0.001
Abnormal neurologic exam at 18-24 months, N (%)
43 (39.4)
6 (5.4)
<0.001
Abnormal neurologic exam at 36 months, N (%)
31 (40.8)
11 (15.3)
<0.001
#235
Baseline Assessment of Prenatal, Perinatal, and Postnatal Care on Newborn Health Outcomes in Rural Nepal
Tran P1, Price N1, Lamichhane B2, Fassl B1. 1Northeast Ohio Medical University, Rootstown, OH and 2Global Envirotech Initiative, Kathmandu, Nepal
Purpose of Study: Insufficient access to peripartum care is a significant factor for newborn health disparities globally. Across rural Nepal, challenges due to geographic remoteness, limited healthcare infrastructure, socio-cultural and economic factors all play a role in the quality and accessibility of prenatal, delivery and postnatal care. The purpose of this study is to perform a baseline assessment survey in 2 remote districts (Accham, Bajura) of Nepal in preparation of an upcoming healthcare capacity building initiative. This study also aims to document baseline health service quality of prenatal, postnatal, and delivery care and to identify areas of needed improvement
Methods Used: The study took place in 18 rural villages in the two districts of Nepal, Accham and Bajura, from April until August 2023. Using a previously validated standardized household survey tool, a Nepali study team performed household interviews in recently delivered women (RDW) who gave birth within 2 years. Interviews were conducted in the local language. The survey tool assesses basic demographic characteristics, healthcare quality for prenatal, postnatal, delivery care and documents medical outcomes. Reporting is descriptive.
Summary of Results: 182 surveys were completed. Prenatal care: 81% of women had anemia screening and 55% had urine analysis checked. Postnatal care: Only 1.1% of newborns received antibiotics and 47.7% had a health care worker visit within 1 week. Delivery care: Only 30.67% of facilities carried oxygen. Health outcomes: 13% of newborns with low birth weight and 4% reported as sick/unwell. See summary outcome table for detailed report of the results.
Conclusions: Many elements of peripartum care require improvement to ensure safe motherhood and childbirth.
#236
A COMPARISON OF FIVE DEFINITIONS OF NECROTIZING ENTEROCOLITIS
Wei V1, McGill-Vargas L2, Underwood M3, 2. 1WSU Elson S. Floyd College of Medicine, Spokane, WA; 2Sacred Heart Children’s Hospital, Spokane, WA and 3UC Davis, Sacramento, CA.
Purpose of Study: The Bell staging system and its most popular revision remain the most common diagnostic criteria for necrotizing enterocolitis (NEC) for clinical and research purposes. Several deficiencies in this definition have prompted proposals for alternative definitions of NEC, however none of these is universally accepted. An optimum definition of NEC would improve clinical care and the validity and generalizability of observational and interventional studies. We aimed to analyze a series of NEC cases applying five definitions of NEC.
Methods Used: 50 cases of NEC were identified from discharge diagnoses from the neonatal intensive care unit at the Sacred Heart Children’s Hospital in Spokane WA. Each case is being reviewed to determine whether it meets the criteria for five different published definitions of NEC: modified Bell (Walsh 1986), VON database, two of three rule (Gordon 2017), gestational age specific NEC score (Battersby 2017) and NEC INC consensus group (Caplan 2019).
Summary of Results: To date we have reviewed 37 cases (analysis ongoing). The Table demonstrates the number of cases that meet each of the five definitions. The Figure presents Venn diagrams showing overlap between the four definitions of infants with Bell stage 2 and Bell stage 3 NEC.
Conclusions: Among 37 infants with a discharge diagnosis of NEC, 24 met criteria for either Bell’s stage 2 or 3, suggesting the possibility of overdiagnosis. There was significant variation among the five definitions with the 2 of 3 and INC definitions being the most restrictive and the VON and NEC by GA definitions the most similar to the Bell criteria. A restrictive definition of NEC may have particular advantages for research while an inclusive definition may be more valuable in a clinical setting. Upon completion of the 50 cases, we will update the analysis and include an analysis of inter-evaluator agreement using the kappa statistic.
Bell Stage
0
1
2
3
11
2
12
12
Other Definitions
VON
2 of 3
INC
Gest Age
22
13
8
24
#237
FACTORS ASSOCIATED WITH DONOR BREAST MILK RECEIPT IN THE NEONATAL INTENSIVE CARE UNIT IN AN ASIAN PACIFIC ISLANDER POPULATION
Wong N1, Siu A4, Wong Ramsey K3, 2. 1Hawai’i Pacific Health, Honolulu, HI; 2Hawai’i Pacific Health Kapi’olani Medical Center for Women & Children, Honolulu, HI; 3John A. Burns School of Medicine, Honolulu, HI and 4Hawai’i Pacific Health, Honolulu, HI
Purpose of Study: Despite the protective benefits of donor breast milk (DBM) against morbidities such as necrotizing enterocolitis (NEC) in preterm infants who are unable to receive maternal breast milk (MBM), previous studies have demonstrated racial disparities in the receipt of DBM among Black and Hispanic infants in comparison to Caucasian infants. Limited data exist regarding DBM use among Asian and Pacific Islander (API) infants. This study aims to evaluate a predominantly API neonatal intensive care unit (NICU) population for disparities in the provision of DBM among infants at lower risk of NEC (>1800 grams birth weight, >32 weeks gestational age) who are not routinely offered DBM per unit protocol and thus potentially more vulnerable to provider bias.
Methods Used: A retrospective chart review was conducted of infants admitted to the largest level 3 NICU in Honolulu, Hawaii from 2018-2022. A total of 1,814 mother-baby dyads were analyzed after excluding infants hospitalized less than a week, with medical contraindications to receiving enteral feeds, were transferred to an outside hospital, or were missing data on race. Multivariable logistic regression was performed to calculate adjusted odds ratios (aOR) for use of DBM while controlling for maternal age, race, primary language, multiple gestation, insurance, delivery method, maternal illicit drug use, and infant receipt of MBM.
Summary of Results: Distribution of mother’s race was 24.2% Filipino, 19.1% Pacific Islander, 21.8% Native Hawaiian, 15.2% Asian, 14.4% Caucasian, and 5.3% Other. Eleven percent did not speak English as the primary language and 16.6% of infants received DBM. Filipinos were more likely to receive donor breast milk when compared to Caucasian infants (aOR 1.94 [1.19, 3.15]). Mothers who did not speak English as their primary language were less likely to use donor milk (aOR 0.55 [0.33, 0.94]). Older maternal age, multiple gestation, and cesarean section delivery were also associated with a higher likelihood of receiving DBM.
Conclusions: A decreased likelihood of donor milk receipt did not exist among low risk Asian and Pacific Islander NICU infants in comparison to Caucasian infants. However, there are disparities in the receipt of donor milk for mothers who did not speak English as their primary language, which may represent insufficient patient education of the benefits of donor milk, cultural differences in the acceptance of DBM, or bias among providers in their likelihood of offering DBM for this population. Further research through targeted focused groups to interview both NICU staff and patients who primarily speak non-English languages and investigation into other social determinants of health are needed to address this disparity.
Adjusted Odds Ratio for maternal characteristics that predict the likelihood of DBM use for infants low at risk for NEC (≥1800 grams, birth weight ≥32 weeks gestational age) in the NICU.
Odds Ratio Estimates
aOR
95% CI
Maternal age (years)
1.04*
[1.02, 1.07]
Primary Race
Caucasian
ref
—
Native Hawaiian
1.42
[0.85, 2.35]
Filipino
1.94*
[1.19, 3.15]
Asian
1.11
[0.64, 1.93]
Pacific Islander
1.69
[0.97, 2.94]
Other
1.34
[0.63, 2.88]
Primary Language Not English
0.55*
[0.33, 0.94]
Multiples (twins, triplets)
2.28*
[1.53, 3.42]
Insurance
Commercial
ref
—
Government
1.12
[0.81, 1.56]
Military
0.51
[0.22, 1.17]
Self-pay/Other
3.21
[0.91, 11.38]
Delivery Method
Vaginal
ref
—
C/S
1.33*
[1.01, 1.76]
Illicit Drug Use
1.55
[0.87, 2.78]
MBM Receipt
0.92
[0.49, 1.75]
Controlled for maternal: age, race, primary language, multiples, insurance, delivery method, illicit drug use, MBM receipt. * p-value <0.05.
#238
PERCUTANEOUS TRANSCATHETER CLOSURE OF PATENT DUCTUS ARTERIOSUS IN PREMATURE NEONATES – THE ROLE OF ECHOCARDIOGRAPHY IN PREDICTION OF POST LIGATION SYNDROME
Yu CG1, Nageotte S2, Lee J2, Jodhka U2, Singh Y1. 1Loma Linda University, Loma Linda, CA and 2Loma Linda University, Loma Linda, CA
Purpose of Study: Patent ductus arteriosus (PDA) is the most common cardiovascular abnormality in extremely premature neonates. PDA can be closed by medications, surgical ligation, or transcatheter device closure. Surgical ligation for PDA is associated with substantial complications. Recently, transcatheter PDA (cath) closure is increasingly used. Cath closure has been demonstrated to have less complications with shorter recovery time.
Cardiorespiratory compromise in the first 24 hours after closure of PDA is known as post-ligation syndrome (PLS). It manifests as hypotension requiring inotropic support, and respiratory failure with escalation of ventilatory support and/or supplemental oxygen. PLS has immediate mortality risks. ~ 45% of surgical ligation patients developed PLS. Prophylactic inotropes have been used to minimize PLS. Cath closure PLS incidence is not well described. We aim to identify incidence and predictive factors using echocardiographic data in premature neonates who had cath closure.
Methods Used: This was a retrospective study of all preterm neonates with cath closure at our institution from August 2018 to December 2022. Demographic and echocardiographic data were obtained. Cardiac output was calculated from echo recordings. These parameters were reviewed to investigate the relationship between myocardial function and post-closure cardiorespiratory instability. We performed comparative evaluation between those with and without PLS.
Summary of Results: Of 59 cases, 3 (5%) had PLS. There was no significant difference in cardiac output before and after cath closure between the group of neonates with and without PLS.
Conclusions: Cath closure has low incidence of PLS. Contrary to previous studies, cardiac output did not predict those who developed PLS. Our data does not support prophylactic inotropes in neonates who had low cardiac output by echo after cath closure. We hypothesize there are other factors that lead to development of PLS that may warrant further study to prevent PLS
#239
Quantifying Fetal Reprogramming in Preeclampsia for Neonatal Outcome Correlation
Newton K. Loma Linda University Children’s Hospital, Loma Linda, CA
Purpose of Study: To determine if preeclampsia causes alterations in the global gene expression profile in fetal and placental tissue, which can be evidenced by differential expression in cell free fetal RNA (cffRNA)
To establish and to test a protocol for collection of maternal specimens prior to delivery from women diagnosed with prepreeclampsia.
To perform transcriptome analysis of cffRNA to quantify gene expression levels for clinical outcome correlation/time to delivery</div>
Methods Used: Mothers are concented upon admission to LLUCH labor and delivery unit. Upon consent, 10 mL of blood is collected into EDTA-coated vacutainer tubes and placed in a 4 degree celsius refridgerator until samples are processed within 2 hours.
Plasma is then separated from blood via centrifugation twice at 500g for 15 minutes at 4 degrees celcius using the supernatant for nucleic acid extraction. Plasma is then stored in -80oC freezer in an assigned slot.
Library prep and sequencing to be outsourced to NORGEN, whereas sequence analysis to be performed by Dr. Newton and Dr. Wilson using R. We will correct for confounders of prematurity control vs preeclampsia groups using Log2 ratios. Data visualization for differential gene expression will be visualized via a heatmap. QIAGEN Ingenuity Pathway Analysis (IPA) vs Cytoscape will be used to find the biological mechanism driving gene expression differences
Results to be correlated with time-to-birth and neonatal outcomes (ie weight z -score, hypoglycemia, and developmental outcomes).
Summary of Results: Results pending and will be ready by 12/1/2023.
Conclusions: Pending and will be ready by 12/1/2023
#240
Two Cases of Anterior Shoulder Dislocation and Fracture Secondary to Generalized Tonic-Clonic Seizure
Dao KT2, Veedu HK1, Ly B1, Ipe J1, Nguyen C1, Eagan M3. 1Kern Medical Center, Bakersfield, CA; 2Kern Medical Center, Bakersfield, CA and 3Kern Medical Center, Bakersfield, CA
Case Report: Dislocation of the glenohumeral joint secondary to generalized tonic-clonic seizures is well-documented in the medical literature, with posterior dislocation being most commonly described. Still, these occurrences tend to be rare and affect a minority of patients, and fractures associated with dislocations after seizure are even less common. As such, the management of these injuries tends to be quite varied and there is a paucity of documented cases in the literature. Here we would like to present two rare cases of anterior shoulder dislocation secondary to seizures, with one patient also sustaining a fracture of the proximal humerus. We would also like to discuss the management and outcomes that have been achieved since these cases tend to occur in a small number of epileptic patients.
AP right shoulder, pre-reduction (Case 1)
#241
Rare Case of Pontine bleed as an adverse effect of Acalabrutinib
Sabetian K. Kern Medical, Bakersfield, CA
Case Report: Acalabrutinib is a next-generation covalent Bruton Tyrosine Kinase (BTK) inhibitor which have has improved patient outcomes in Chronic Lymphocytic Leukemia (CLL). Acalabrutinib was approved by the FDA for the treatment of CLL in 2019. Some of the common side effects of the drug include anemia, infection, headache, neutropenia, thrombocytopenia, etc. Some of the more serious adverse reactions include severe hemorrhage, neutropenia, HBV/EBV/CMV reactivation, etc. In this case report, we present a case of a 62-year-old African American male with CLL treated with Acalabrutinib who presented with a pontine bleed.
Case Presentation: 62-year-old African American male with previous cocaine use (last 13 years ago), tachycardia on Metoprolol, Chronic Lymphocytic Leukemia (CLL) on Acalabrutinib 100 mg daily, and Obinutuzumab 1000 mg Intravenous monthly at cancer center (but not infused x 5 months due to insurance issues), and schizophrenia (on Olanzapine and Fluphenazine) who was brought into the emergency department (ED) from a Sober living facility, by his case manager for few days of sleeping more than normal, generalized weakness and requiring assistance getting out of bed and going up and down the stairs and one mechanical fall with no head trauma nor loss of consciousness 2 weeks prior.
On presentation, vitals were stable. Labs only revealed mild leukocytosis microcytic anemia. Coagulation studies were also within normal limits. Urine Toxicology Screen was negative. Comprehensive Chemistry panel was largely unremarkable. On ambulation in the ED patient was noted to have a slow gait. Hence a Computed Tomography of the brain without contrast was obtain which showed a linear focus of increased attenuation in the right side of the pons which may represent a small intra-axial hemorrhage. Subsequently a Magnetic Resonant Imaging of the brain without contrast was done which confirmed a sub centimeter recent hemorrhage in the right pons.
At this time, Neurology was consulted. His neurologic exam was normal except for mild to moderate abnormal involuntary movement of his mouth, restless movement of his right arm and leg, thought to be due to possible Tardive Dyskinesia and gait which was slow, but steady, with no movement of his arms and he would take an extra step to turn and was unable to do tandem gait. Patient was subsequently discharged back to his facility with instructions to discontinue Acalabrutinib and follow up with his cancer doctor.
Discussion: Although Acalabrutinib is a better tolerated BTK inhibitor with lower side effect profile compared to other BTK inhibitors, serious side effects such as serious hemorrhage may occur spontaneously. Acalabrutinib should be considered in any patient presenting with hemorrhage of any organ including the brain and medication should be discontinued swiftly. Further studies need to be considered to determine percentage of serious hemorrhage in patients treated with Acalabrutinib.
#242
NAVIGATING THE COMPLEXITY: A UNIQUE CASE OF AUTOIMMUNE ENCEPHALITIS
Reyes MP, Thiagarajan S. Sierra View Medical Center, Porterville, CA
Case Report: The patient, a previously healthy 32-year-old female, initially presented with psychiatric symptoms, including psychosis, agitation, and delusions. Subsequent neurological examination revealed the presence of seizures, abnormal movements, and autonomic dysfunction. Seronegative autoimmune encephalitis was diagnosed after a thorough diagnostic workup, including cerebrospinal fluid analysis and antibody testing.
The patient received prompt immunotherapy, including corticosteroids and intravenous immunoglobulin. However, antibodies were negative in the serum and CSF. Additionally, tumor screening was negative. Over the course of several weeks, the patient showed significant improvement in both neurological and psychiatric symptoms.
This case report highlights the importance of early recognition and treatment of seronegative autoimmune encephalitis. By sharing this case, we aim to contribute to the knowledge of autoimmune encephalitis and enhance awareness for timely diagnosis and appropriate management of this challenging and complex condition.
Methods: A comprehensive evaluation of the patient’s medical history, physical assessments, laboratory investigations, and neuroimaging studies was conducted. Diagnostic procedures included cerebrospinal fluid analysis, evaluation of serum antibody levels, electroencephalogram recordings, and brain magnetic resonance imaging.
Results: Following a thorough investigation and exclusion of other potential causes, a diagnosis of autoimmune encephalitis was established. There was no detection of specific antibodies in the serum or cerebrospinal fluid. Brain MRI was negative, and EEG was abnormal - consistent with encephalitis. Despite the absence of detectable antibodies in the CSF, the patient’s clinical presentation and EEG findings suggested an autoimmune etiology. Empirical immunotherapy was initiated, consisting of corticosteroids and intravenous immunoglobulin (IVIG). Supportive care and close monitoring of symptoms, vital signs, and neurological status were also provided. Remarkably, the patient demonstrated significant improvement in cognitive function and neurological deficits within weeks of treatment initiation, further supporting our evidence of autoimmune encephalitis.
Conclusion: Following the initiation of treatment, the patient exhibited improvement in psychiatric symptoms, resolution of seizures, and a return to baseline neurological functioning. This case highlights the importance of considering seronegative autoimmune encephalitis in patients with suggestive clinical features, even without detectable antibodies in the CSF. Negative CSF antibodies should not exclude the possibility of an autoimmune etiology, as the diagnostic sensitivity of current antibody panels is not absolute. This case further emphasizes the significance of early recognition and prompt treatment in effectively managing seronegative autoimmune encephalitis.
#243
Under Pressure: Pulmonary Arterial Hypertension Prevents Hemodynamic Collapse in Pericardial Tamponade
Uddin S, Nikolov N, Hajeh H, Jestila T, Petersen G. Kern Medical Center, Bakersfield, CA
Case Report: Cardiac tamponade is a life-threatening condition that causes extracardiac pressure on the heart due to an accumulation of excess fluid in the pericardial sac causing collapse of the Ventricles and circulatory compromise. Research of cases with concomitant pulmonary arterial hypertension and pericardial effusion are associated with increased morbidity and mortality. The case presented here suggests that pulmonary arterial hypertension prevented his hemodynamic collapse and death.
Case Presentation: A 55-year-old man with a history of Coronary Artery Disease, End-Stage Renal Disease, Heart Failure with Reduced Ejection Fraction of 15%, Hypertension, and WHO group two Severe Pulmonary Artery Hypertension (PAP) with Pulmonary Arterial Pressure of 65 mmHg presented for Heart Failure Exacerbation secondary to missed Hemodialysis sessions. His Arteriovenous Fistula (AVF) was thrombosed and non-functioning, requiring a thrombectomy and balloon angioplasty. The patient was bacteremic with cultures growing Methicillin-Sensitive Staphylococcus Aureus secondary to an infected AVF and was treated with IV antibiotics. While receiving hemodialysis several days later, the patient became hypotensive with a mean arterial pressure of 56. His blood pressure remained low despite fluid resuscitation, with his lactic acid persistently elevated at 13.7 mmol/L. He was transferred to the ICU for vasopressor support where adequate blood pressure management with Norepinephrine and Dobutamine did not resolve his Lactic Acidosis. A CT angiogram of the Abdomen and Pelvis obtained due to concern for possible bowel ischemia revealed a large complex pericardial effusion with tamponade. Echocardiogram revealed physiologic hypotension, however, the Right Atrium and Ventricle had not collapsed under duress from the pericardial effusion due to the patient’s severe Pulmonary Arterial Hypertension. Interestingly EKGs obtained during this time did not reveal low voltage QRS complexes or Electrical Alternans. Emergent pericardiocentesis with removal of 1.75 liters and placement of a pericardial drain was performed. The pericardial effusion was attributed to uremic pericarditis. Vasopressor requirements subsequently decreased and Lactic Acidosis resolved. He eventually returned to his baseline state of health and was discharged in stable condition after 26 days of hospitalization.
Discussion: This patient developed obstructive shock secondary to an acute massive pericardial effusion secondary to uremic pericarditis. The complete circulatory collapse in the patient was likely prevented due to his concomitant pathology of Severe Pulmonary Arterial Hypertension, which elevated the pressure within the right side of his heart allowing it to to overcome the extracardiac pressure of the tamponade. This case highlights an exception where PAP was of life-saving benefit.
Poster Session II
Concurrent Session
6:00 PM
Thursday, January 18, 2024
#245
Decreasing Orthopedic Pan Size Can Increase Cost-Effectiveness, Efficiency, and Sustainability
Boldut R1, 2, Duan A4, 2, Kwong A1, 2, Zhang J1, 2, Duffy D2, Cooper A3. 1University of British Columbia, Vancouver, BC, Canada; 2BC Children’s Hospital, Vancouver, BC, Canada; 3BC Children’s Hospital, Vancouver, BC, Canada and 4University of British Columbia, Vancouver, BC, Canada
Purpose of Study: Research assistants at the British Columbia Children’s Hospital (BCCH) were observing pediatric orthopedic surgeries to understand tools that are redundant or removable from pans to help minimize inefficiencies caused by large numbers of tools in pans. Major findings of this project include that only 71% (30/42) tools in the pan are used at all, and 38% (16/42) tools were used once or less in the 34 observed epiphysiodesis and hardware removal surgeries (<10% use rate). As this project progressed, a literature review to understand the potential benefits of such research was proposed. Therefore, the purpose of this review was to explore how decreasing the number of tools in a pan can lead to increased cost-effectiveness, efficiency and sustainability in the operating room (OR).
Methods Used: Research assistants conducted a literature review searching database MEDLINE to gain an understanding of the current state of literature. Results were summarized in a report presented to BCCH orthopedic surgeons.
Summary of Results: Cost-Effectiveness— A study by Toor et al. (2022) exploring the economic impacts of pan optimization found that a 42% reduction in pan size as determined through clinician review along with mathematical models represented $31,870 in annual savings for the Department of Orthopedic Surgery at the University of Toronto. When data was extrapolated to the institution, it was estimated that application of such tray optimization methodology would result in $205,000 of savings annually. A similar study conducted by Lonner et al. (2021) predicted that a 32-41% reduction in pan size can lead to average annual savings of $281,298.05 at the institutional level.
Efficiency— A study by Mhalaba and Stockert (2014), found that increasing the number of instruments per tray was associated with decreased use and an increased instrument error rate. Lonner et al. (2017) found that removing 32% of tools from a pan for knee arthroplasties led to a decrease in mean set up time from 20.7 to 14.2 minutes, along with 40-75 minutes saved during the sterilization process.
Sustainability— Operating rooms are a healthcare subsector that has high energy demands, waste volumes, and consumable throughput. Therefore, understanding how the carbon footprint of the operating room can be minimized is vital. As described above, many tools that are unused continue to be sterilized, which contributes to carbon emissions originating from the operating room.
Conclusions: Overall, this review provides insight into the potential benefits of streamlining surgical instrument pans from the perspectives of cost-effectiveness, efficiency and sustainability. Future research could include a formal scoping review of literature on this topic, and conducting cost as well as carbon emission audits at BCCH to better estimate the potential benefit of decreasing orthopedic pan size.
#246
Social, cultural, and economic factors contributing to iron-deficiency anemia in a rural district of Nepal
Brocker BJ1, Casteel J1, Raghavachari S1, Karki P1, Lamichhane B1, Fassl B1, 2. 1Northeast Ohio Medical University, Rootstown, OH and 2University of Utah, Salt Lake City, UT
Purpose of Study: Iron deficiency anemia is a severe public health problem in Nepal. The purpose of this project is to provide a description of the social, cultural, and economic factors that influence dietary iron deficiency in the highest risk groups: women of childbearing age and their children.
Methods Used: This study took place in Nuwakot, Nepal in May 2023 and was part of a healthcare quality improvement initiative of the Nepali government. A team of Nepali community health experts conducted a 28-question standardized nutrition survey in a convenience sample of 23 anemic women (HgB less than 10g/dl) identified during screening events. Survey responses were converted to categorical data and indexed themes. Descriptive statistics for these and any numerical responses were reported.
Summary of Results: The majority of household food supply is grown at home (average 60%). Rice and potato are the most popular crops, and products such as salt and oil are purchased. Travel times to markets averaged 40 minutes and ranged as high as 4 hours. 68% of reported meals consisted of a variation of “dal-bhat” (lentil soup with rice, with or without vegetables); only one report included meat. There were an average of 2.8 meals per day. 77% reported access to vitamins; only 53% of those reported taking iron. 4 of 9 women reporting breastfeeding were doing so less than 8 times per day. 76.5% of women believe they are receiving inadequate nutrition or experience food insecurity.
Conclusions: Food insecurity and lack of food diversity are serious problems contributing to nutritional deficiencies.
#247
PERINATAL CARE QUALITY REVIEW IN RURAL DISTRICT OF NEPAL
Brockwell M, Lamichhane B, Fassl B. Northeast Ohio Medical University, Rootstown, OH
Purpose of Study: The Sustained Development Goal 3.2 aims to reduce neonatal mortality below 12/1,000 live births globally, however as of 2021 Nepal’s infant mortality rate remains high at 23/1,000 with inaccessible facilities and poor infrastructure representing barriers to care. In rural Nepal, birthing centers are often the most accessible option for delivery, but staff training and access to equipment remains a challenge. This study investigates the infrastructure, equipment, and manpower needed for a rural birthing center and describes perinatal services provided by Madaanpur Health Post (MHP).
Methods Used: The study took place in Nuwakot, Nepal from June 2022 to June 2023. A team of Nepali community health specialists conducted standardized health facility surveys and household surveys in the catchment area of MHP, interviewing recently delivered women using validated survey tools. Survey data from medical records were transferred into an electronic database for analysis. Reporting of findings is descriptive. Surveys were approved by the NEOMED IRB and local authorities.
Summary of Results: One facility survey and 101 household surveys were completed. MHP had one Skilled Birthing Assistant and antenatal care, but lacked a staff doctor, delivery equipment, and postnatal equipment. Of women interviewed 99% received antenatal care at a health post. 44% delivered in a birthing center, 48% in a hospital, and 9% at home. 22% identified a health issue in the child. 16% of mothers faced complications during labor. 100% of children are alive and healthy, but only 38% saw healthcare workers within 6 weeks after birth, and none have been screened for anemia.
Conclusions: MHP has the equipment, facilities, and resources necessary to provide prenatal care, but does not have the equipment or resources to operate as a birthing center without intervention. Future projects should focus on upgrading MHP to function as a birthing center, and increasing follow up after birth with the aim to improve infant and maternal mortality in Nepal.
Madaanpur Health Post (MHP) Catchment Area Survey.
Perinatal Care Measures and Outcomes
Percentage
N
Mother received antenatal care
99.00%
100/101
Mother received antenatal care at healthpost
98.01%
99/101
Mother received antenatal care at hospital
0.99%
1/101
Mother received ultrasound
95.05%
96/101
Mother screened for anemia
35.64%
36/101
Established birth preparedness plan
89.11%
90/101
Maternal urine sample checked
87.13%
88/101
Delivered at home
8.91%
9/101
Delivered at birthing center
43.56%
44/101
Delivered at hospital
47.52%
48/101
Skilled Birthing Assistant (SBA) present for delivery
86.14%
87/101
Obstructed labor
9.90%
10/101
Postpartum hemorrhage
1.98%
2/101
Maternal seizure
5.94%
6/101
Mother reported "almost died"
4.95%
5/101
Healthcare worker visited infant within 6 weeks after delivery
37.62%
38/101
Newborn weighed at birth
76.24%
77/101
Health issue identified in newborn
21.78%
22/101
At time of survey, child alive and healthy
100%
101/101
Child ever screened for anemia
0%
0/101
#248
EVALUATING FAMILY-CENTERED CARE: PARENTS’/CAREGIVERS’, ADOLESCENT PATIENTS’, AND HEALTH CARE PROVIDERS’ PERSPECTIVES
Cook CB1, Study G1, Elliott A1, 2. 1University of British Columbia, Vancouver, BC, Canada and 2BC Children’s Hospital Research Institute, Vancouver, BC, Canada
Purpose of Study: Family-centered care (FCC) is a method of service delivery that emphasizes collaborative caregiving in which families are recognized as the experts on the child’s abilities and needs and therefore work with healthcare providers (HCP) to make informed decisions about the services the child receives. Although FCC is of significant benefit to both children and families, there is often a disconnect between the principles of FCC and the realities of clinical practice. Integration of genetic counsellors (GCs) into multidisciplinary clinics is one way in which FCC needs can be addressed. The purpose of this study was to evaluate perspectives of parents, adolescents, and HCP on the degree to which care is family centered.
Methods Used: Using a mixed methods approach, we explored the experiences of families seen in specialty clinics at BC Children’s Hospital that do not have a GC as part of the care team. By administering validated tools (MPOC-20, GYV-20, MPOC-SP, Peds-QL), we evaluated the perspectives of parents, adolescent patients, and HCP, respectively. Descriptive statistics were calculated to contextualize the sample and logistic regression was used to explore associations between MPOC scores and potential demographic variable predictors. Semi-structured interviews were conducted with a subset of parents and analyzed using an interpretive description approach with thematic analysis in order to develop a deeper understanding of families’ experiences.
Summary of Results: Analysis (n=118) showed parents rated the MPOC-20 domain “respectful and supportive care” the highest (occurs to greatest extent), and the domain “providing general information” the lowest. Linear regression analysis showed having appointments >1/year and a hybrid service delivery model were positively associated with higher MPOC-20 scores. Urban area of residence was positively associated with PedsQL scores, whereas child’s older age, access to >1 additional service and living in an area of residence which makes access to care challenging were negatively associated with PedsQL scores. Themes from qualitative interviews (n=10) related to parents’ desire to be involved in discussions about their child’s care and plans for transition to adult care, having easier access to HCP outside of appointments, feeling heard by HCP, and receiving regular updates on their child’s condition.
Conclusions: Findings in this study demonstrate the need to improve the extent to which FCC is provided, particularly in terms of providing general and specific information about the child’s condition and encouraging partnership between parents and HCP. Recognizing the unique needs of families based on their demographic factors will help meet the specific needs of children living with a chronic condition and their families. Involving GCs in care teams can facilitate shared decision making, communication between care providers and families, and the provision of appropriate resources for support.
#249
HELPING YOUTH SELF-IDENTIFY MOTIVATIONS AND STRATEGIES TO INCREASE HELMET USE IN KOTZEBUE, ALASKA
Denney G, Keys T. University of Washington School of Medicine, Seattle, WA
Purpose of Study: Kotzebue, Alaska is a community of approximately 3,000 people located in the Northwest Arctic region. Due to a limited system of paved roads, citizens of the largely Iñupiat town rely on off-road vehicles such as ATVs and snow machines for transportation and access to subsistence foods. Low rates of helmet use while using off-road vehicles has led to a relatively large volume of head injuries among the population, including amongst the pediatric population. Developing effective methods to increase helmet use and reduce pediatric head injuries is a community health goal in Kotzebue.
Methods Used: An understanding of community health priorities and concerns was gained through conversations with community members and healthcare providers. Community members cited connecting youth to cultural practices like language and traditional foods as critical for the health of the town. Healthcare providers noted that accidental injuries, especially head injuries involving off-road vehicles, were a common presenting concern amongst patients. A community partnership was developed with the Maniilaq Association Environmental Health Department which voiced a desire to begin a series of presentations for youth to encourage helmet use. Off-road vehicles are an essential part of life and culture in Kotzebue and helmet use was identified as a strategy to prevent serious injuries while allowing youth to participate in off-road vehicle activities. A literature review was undertaken to assess current research on pediatric head trauma and behavior modification techniques. Key findings included research pointing to helmets as an effective tool to reduce the incidence of head trauma, the need for personalized strategies to increase helmet use, and motivational interviewing as an effective tool for youth behavior modification.
Summary of Results: Based around the principles of motivational interviewing, a curriculum for school-aged children called Protect your Brain! was developed. Along with providing basic information about the efficacy of helmets and functions of the brain, the curriculum focuses on questions such as “what makes it hard to wear a helmet?”, “what do you think would help?”, and “what do you think wearing a helmet can do for you?”. The curriculum was demonstrated to Environmental Health staff and includes detailed presenter notes to allow for use by multiple staff members.
Conclusions: Over the next year, the Environmental Health Department is planning to give the presentation through the school district or local Boys and Girls club. The goal of the curriculum is to aid youth in understanding their personal barriers to helmet use and provide an opportunity to identify personalized solutions. Additionally, the question-based approach to the curriculum is intended to provide the Environmental Health Department with an informal method of data collection to continue identifying Kotzebue-specific strategies to support helmet use.
#250
CW: Birth Trauma, a Reddit Analysis
Eaton N, Nelson A, White S. College of Osteopathic Medicine of the Pacific, Western University of Health Sciences, Pomona, CA
Purpose of Study: Birth trauma is emerging as a significant contributor to postpartum suffering; its definition is still evolving. Up to 30% of women categorize their hospital birth as traumatic, and 3-4% meet clinical diagnosis criteria for PTSD at 24 weeks postpartum, demonstrating the long-term impacts of a traumatic birth. This study extracted themes from Reddit posts and comments to describe what people spontaneously characterize as birth trauma in an unfiltered setting, and what conversations around the topic are occurring.
Methods Used: Reddit has 55.7 million daily active users primarily in the 16-49 age range. We used the search words “birth trauma” and “traumatic birth” to identify potentially relevant posts after 2017. Exclusion criteria included fewer than five upvotes or fewer than five comments. Reddit subgroups r/beyondthebump and r/babybumps were used along with the main search page to further narrow down results. Multiple themes were extracted from individual entries. Thematic saturation was achieved when no new themes were discovered in 5 consecutive entries.
Summary of Results: 296 posts and 1488 comments were evaluated for inclusion; 100 posts and 834 comments met criteria; ten thematic groups emerged. These 10 theme groups include – support for the content of the post, medical complications and poor communication, PTSD from delivery, birth stories, I had a similar story, mental health/long term effects, conversations around negligence, fear, specific advice, and healing. The most prevalent themes were “Support for the content of the post” (‘because it is NOT fair that our experiences as mothers are erased because our babies are fine’) (26% of themes), “medical complications and poor communication” (17%), and “fear” (‘The fear of death. The lingering guilt when something goes wrong. The constant questioning…’) (13%). Notably, 242 comments of 1095 comments explicitly supported the mother. “I have to send some serious gratitude and support to everyone in this subreddit because it has been SO therapeutic for me as I managed my pregnancy.”
Conclusions: While issues like fear of lack of control and unexpected medical complications led to hesitancy about future births and dissatisfaction with the medical system, this work highlighted support for mothers on social media. Commentors validate the posters experiences, explain unclear medical jargon and processes, advise them to talk to their doctor when warranted and ease concerns like those of this Reddit user. “It was the most traumatic and dehumanizing experience I’ve ever endured. I was treated so poorly by the male doctors." Understanding what birthing people are posting when discussing traumatic birth can better help define this phenomenon. Pairing trauma-informed care with patient education about pregnancy risks may help reduce people’s perceptions of birth trauma. Leveraging social media as a tool for working against misconceptions around birth can further support this.
#251
WHAT ISSUES DO AMERICAN WOMEN CARRYING BREECH BABIES DISCUSS ON SOCIAL MEDIA?
Fisher E, Nelson AL. College of Osteopathic Medicine of the Pacific, Western University of Health Sciences, Pomona, CA
Purpose of Study: Professional guidelines and management of singleton term frank breech pregnancies has been evolving, but little has been done to examine the American woman’s experience carrying and delivering a breech fetus. This study sought to investigate what opinions pregnant people express and what concerns they share in posts and comments in public subcommunities on Reddit. Social media provides insight into real and unfiltered reports and spontaneous dialogues, which can help identify areas of miscommunication or misunderstanding between providers and patients.
Methods Used: We used the search term “breech” within Reddit subcommunities r/pregnant (402,000 members) and r/babybumps (307,000 members) to screen for related posts. Inclusion criteria included posts with 10 or more upvotes and 10 or more comments. Any posts obviously from outside the United States were excluded. Comments were examined in the order of most upvotes to least until thematic saturation was reached, which was defined as 5 comments with no new themes. The purpose of each post was categorized, and all themes were collected from both the original post and comments. All posts were read twice to ensure objectivity and increase reliability.
Summary of Results: We evaluated 499 posts containing 7,210 comments for inclusion and analyzed the 58 posts containing 1,966 comments that met study criteria. We categorized the purpose of each post; 37.6% involved venting, 34.4% sought advice, and 23.0% shared experiences. A total of 10 themes were identified; the major themes were anxiety (60.7%), confidence in their medical team (31.1%), gratitude for a healthy baby regardless of delivery route (27.9%), frustration surrounding instability of the presentation (23.0%), and feeling relief over being advised to have a scheduled cesarean section (23.0%). For instance, one user hoping for an unmedicated vaginal birth described feeling “cheated” after discovering they were carrying a breech fetus and recounted how they “did everything right” (maneuvers at home to flip the fetus, ate a healthy diet, exercised, and attempted external cephalic version with their provider) but would still require a cesarean delivery. Several other users described their fetus’s breech positioning as a “blessing” and were thankful to avoid the pain and unpredictability of labor with a scheduled cesarean delivery.
Conclusions: Many patients turn to social media to ask questions, share their experiences, and find community. More than a third of the posts analyzed were categorized as “seeking advice,” which could indicate unmet educational needs. The high frequency of anxiety (60.7% of analyzed posts) shows one area needing improvement. Overall, the results of this study show a high reliance on social media, which providers should understand.
#252
Patient characteristics of those served by a telehealth medication abortion service in 5 U.S. territories
Gibbons S, Fiastro A, Godfrey E. University of Washington, Seattle, WA
Purpose of Study: United States territory residents face barriers to accessing abortion care due to geographic isolation, lack of healthcare services or trained abortion providers. Telemedicine medication abortion has the potential to fill this gap. This study aims to understand the preferences and characteristics of patients utilizing telehealth medication abortion in U.S. territories.
Methods Used: Using de-identified electronic medical health records, we examined all U.S. territory residents seeking medication abortion (n=243) or abortion medications for future use (n=26) from the telemedicine service Aid Access between June, 4 2020 and March 30, 2023 (n=269). We used descriptive statistics to describe patient characteristics and reasons for choosing the service in both groups. Patients were able to select multiple reasons for choosing Aid Access in the online form.
Summary of Results: Guam and Puerto Rico had the largest patient populations with 61% (n=149) and 24% (n=59) respectively. A majority of patients reported being 20-24 years old (34%, n=83) and 4-7 weeks gestational duration (67%, n=163). 31%(n=46) of patients in Guam reported being between 0-3 weeks gestational duration. Cost of alternative options, distance to nearest abortion provider, keeping procedure private, and interference with obligations were cited reasons for choosing Aid Access. A majority of Puerto Rican and US Virgin Island clients (59%, 51%) cited cost as a reason they chose to use Aid Access. Of advanced provision patients, a greater share of Guaman clients (87.5%) cited distance as reason for choosing Aid Access abortion medications for future use, while more Puerto Rican patients (58.3%) cited cost as their primary reason.
Conclusions: These findings suggest that U.S. territory residents face barriers to procedural and in-person medication abortion care primarily in distance to providers and cost of service. We recommend further federal investment in healthcare infrastructure within U.S. territories and expanding legislation that increases access to reproductive healthcare services for U.S. territory populations.
Pregnant U.S. Territory Patients Utilizing Aid Access Service.
Patients were able to choose all reasons that applied to them.
#253
THE EFFECT OF INTERVENTIONAL PROGRAMS TO INCREASE CERVICAL CANCER SCREENING IN MARGINALIZED POPULATIONS
Guarina S1, Borges J1, Kanchrakuntla M1, Myoung A1, Padhi I1, Pham C1, Velazquez V1, Afghani B1, 2. 1UC Irvine School of Medicine, Irvine, CA and 2Children’s Hospital of Orange County (CHOC), Orange, CA
Purpose of Study: Rates of cervical cancer have decreased in recent years due to robust Papanicolaou (Pap) vaccination and human papilloma virus (HPV) screening. Despite preventive measures, a disproportionate number of women from marginalized communities (poverty-stricken, Hispanic/Latina or Black communities) die from cervical cancer each year. The purpose of this study is to review interventional programs to increase cervical cancer screening in underserved or marginalized communities.
Methods Used: A literature review was conducted through PubMed and Google Scholar using key words: ‘cervical cancer screening,’ ‘intervention,’ ‘Pap smear’, ‘minority,’ and ‘marginalized.’ We also looked at the bibliography section of each article for additional studies. We included studies published after 2015 that were performed in marginalized communities in the United States, and used interventional programs with a primary endpoint of receipt of a Papanicolaou (Pap) smear.
Summary of Results: A total of 7 studies met our inclusion criteria (Table 1). Most of the intervention programs included education, navigation services, and/or at-home HPV screening tests. Many of the studies demonstrated an increase in receipt of Pap smear after the intervention. The baseline screening rate in the marginalized communities ranged from 6.4% to 48% (in the control groups). After the intervention, there was an increase in the rate of screening with a range of 17.6% to 83%. The studies that included multidimensional interventions, such as help with scheduling and an in-home screening kit seemed to be more effective in increasing the receipt of the Pap smear (83% for Pretsch 2023 and 77% Carrasquillo 2017). The limitations of some studies included selection bias due to loss to follow up of several participants, small sample size, focus on only one marginalized community, and heterogeneity in considering social determinants of health.
Conclusions: Our literature review indicates that interventional programs lead to an increase in cervical screening rates, with the at-home screening kits being the most effective. Although interventions increased the rate of screening, in some communities the rate remained low. Larger studies that include more diverse groups from different racial/ethnic that evaluate the impact of structural barriers such as cost, lack of childcare or transportation, language proficiency, and physician recommendation are needed. Partnership with community organizations is crucial to address disparities and targeted interventions for under-screened people.
First Author and Year Published
Location of Study and Subjects
Control and Intervention Groups
Study Length
Outcome Comparisons of Pap Smear Receipt
Other Variables Taken into Account
Pretsch et al, 2023
United States (North Carolina),
Population with income of 250% or less of the US Federal Poverty Level
Total (n=549)
Control Group:
Scheduling assistance only (n=185)
Intervention Group:
HPV self-collection with scheduling assistance (n=364)
United States (Baltimore, Maryland),
Black women recruited from inner-city HIV clinics, university-based HIV/AIDS research centers and community organizations dedicated to serving people with HIV
Total (n=58)
Control Group:
Cervical cancer brochure (n=32)
Intervention Group:
Cervical cancer brochure, 30-60 min health literacy-focused education, monthly phone counseling, and navigation services (n=26)
6 months
Control Group:
n=7 (21.9%)
Intervention Group:
n=13 (50%);
χ2=5.02, p=.025
Age,
Education,
Maritial status,
Employment status,
Income,
Type of residence,
Health insurance coverage,
Have PCP,
Own a smartphone,
Prior pap tests
Savas et al, 2021
United States (El Paso, Texas),
Latina/Hispanic population
Total (n=429)
Control Group:
Usual care (n=216)
Intervention Group:
Education program (n=213)
6 months
Control Group:
n=105 (48.6%)
Intervention Group:n=100 (46.9%);p=0.730
Only intervention group women 50 years and older were more likely to complete a Pap screening compared with control group women (PP: 64.5% vs. 43.5%, p =0.019).
Age,
Marital status,
Income,
Health insurance coverage,
Country of birth
Shokar et al, 2019
United States (El Paso, Texas),
Latina/Hispanic population
Total (n=460)
Control Group:
Usual care (n=203)
Intervention Group:
Education program, navigation services, and no-cost screening (n=257)
Age,
Race/ethnicity,
Education,
Marital status,
Health status,
Country of birth,
Primary language,
Employment status,
Annual income,
Years in the USA,
Have PCP,
Acculturation
Carrasquillo et al, 2017
United States (Florida)
Hispanic, Haitian, and Black populations
Total (n=601)
Group 1 - Outreach (n=182)
Group 2 - Navigation services (n=212)
Group 3 - Self-swab option (n=207)
6 months
Navigation vs Outreach (43% vs. 31%, OR=1.62, 95% CI: 1.07-2.45, p=0.02)
Self-swab vs Navigation (77% vs. 43%, OR=4.61, 95% CI: 3.02-7.05, p<0.01)
Age,
Income,
Education,
Health insurance coverage,
Race/ethnicity,
Immigration status,
Prior pap tests
Valdez et al, 2016
United States (Los Angeles, California; Fresno, California; San Jose, California),
Latina/Hispanic population
Total (n=727)
Control Group:
Usual care (n=344)
Intervention Group:
Cervical cancer education program (n=383)
6 months
Control Group:
n=164 (48%)
Intervention Group:
n=196 (51%);p=0.35
Age,
Primary language,
Birthplace,
Years in the USA,
Health insurance,
Years of formal education,
Maritial status,
Particular doctor,
Number of children
Thompson et al, 2016
United States (Washington, Lower Yakima Valley),Rural agricultural region where 67% of the population are of Latino origin
Total (n=443)
Control Group:
Usual care (n=147)
Intervention Groups:
Group 1 - Spanish-language educational video (n=146)
Group 2 - Spanish-language educational video and home visit (n=150)
7 months
Control Group:
n=50 (34.0%)
Intervention Groups:
Group 1 (n=78 (53.4%); p<0.001)
Group 2 n=58 (38.7%); p<0.01)
Age,
Education,
Maritial status,
Country of birth,
Primary language,
Health insurance coverage,
Acculturation,
Prior pap tests
ASSESSING NURSING PERSPECTIVES ON SURGICAL CO-MANAGEMENT IN PEDIATRICS
Gupta R1, 2, Lehman D3, 4, Zamkoff J1, 2, Brittan M1, 2, Ziniel S1, 2. 1Children’s Hospital Colorado, Aurora, CO; 2University of Colorado School of Medicine, Aurora, CO; 3Lucile Packard Children’s Hospital Stanford, Palo Alto, CA and 4Stanford Children’s Health, Palo Alto, CA
Purpose of Study: Surgical co-management (SCM), a practice in which hospitalists and surgeons share responsibility in caring for surgical patients, has been implemented at various pediatric institutions to optimize care for medically complex patients in the perioperative period. SCM has led to improved communication amongst providers as well as a reduction in postoperative complications, medical errors, and length of stay for patients. SCM began at our institution in 2004 for complex spine patients and has since expanded to additional patient subgroups. Nursing staff (RNs) play a crucial role in managing SCM patients, communicating with different providers to coordinate and consolidate care, thus impacting patient outcomes. The purpose of this study was to evaluate RN perspectives on SCM at a free-standing children’s hospital, as these data are lacking in the literature.
Methods Used: This study was approved by the hospital’s Organizational Research Risk and Quality Improvement Review Panel (ORRQIRP). With the assistance of a survey methodologist, a 16 question survey was designed to assess RN preferences and comfort with SCM. Since SCM patients are admitted to the medical-surgical floor of our institution, this REDCap survey was administered via an email link to all RNs who worked on that floor in November 2021. The survey remained open for 40 days with three follow-up reminder emails sent to non-responding RNs. Data were analyzed descriptively using frequencies and percentiles.
Summary of Results: Sixty of 134 RNs responded to the survey (44.8%). Most respondents (92%) had managed at least one SCM patient and were eligible to complete the rest of the survey. 94.4% of RNs said SCM was “pretty” or “very” beneficial for having additional medical expertise in creating a care plan (Table 1). 92.4% felt that SCM was “pretty” or “very” helpful for admission order reconciliation. 94.4% of RNs reported a “somewhat” or “strongly” positive impact of SCM on the patient/family experience as well as on the care team. 79.2% and 88.7% of RNs reported that SCM supports timely and safe/efficient discharge “pretty” or “very” well respectively. Open ended comments revealed that RNs felt more content with the faster response times, overnight availability of the primary providers, and improved communication with patients and care team members.
Conclusions: Overall, RNs reported high levels of satisfaction and benefits to patient safety, communication between providers and care team members, timeliness, care effectiveness, and patient/family experience with pediatric SCM. This study supported the development of a formal surgical co-management inpatient service, thus separating SCM patients from non-surgical patients on other inpatient teams, to optimize care for medically complex patients during the perioperative period. Further research is needed to assess whether the SCM model in pediatrics benefits specific patient outcomes such as clinical deterioration events, pain management, postoperative recovery, and readmission rates.
Percentage of Respondents Answering Survey Questions Positively.
Survey Questions
Percentage of Positive Answers
Helpfulness (Pretty and Very Helpful)
Helpfulness of SCM for admission order reconciliation
92.4%
Rating (Very Good and Excellent)
Rating of provider response
times on weekdays
84.9%
Rating of provider response
times on weekends
70.4%
Benefit (Pretty and Very Beneficial)
Benefit to care team of directly interacting with the surgical team for surgery specific questions
81.8%
Benefit to patient/family of directly interacting with the surgical team for surgery specific questions
80.0%
Benefit of having additional medical expertise through SCM in creating a care plan for medically complex patients
94.4%
Quality (Pretty and Very Well)
Quality of SCM addressing
non-surgical questions
87.3%
Quality of SCM supporting
timely discharge
79.2%
Quality of SCM promoting
safe and efficient discharge
88.7%
Impact (Somewhat and Strongly Positive Impact)
Impact of SCM and ability to interact with both surgical and medical teams on the patient/family experience
94.4%
Impact of SCM and ability to interact with both surgical and medical teams on the care team experience
94.4%
#255
MODERN DISCUSSIONS ON SOCIAL MEDIA SURROUNDING OOCYTE CRYOPRESERVATION
Hammi MC, Moskalensky L, Nelson AL, Fuchs S. Western University of Health Sciences, Pomona, CA
Purpose of Study: The purpose of this study was to assess the understanding, beliefs, and concerns people harbor about oocyte cryopreservation by conducting thematic analysis of the anonymous unfiltered discussions on social media platforms such as Reddit and Tiktok.
Methods Used: We selected Reddit, with its daily 56 million users, to represent the 18-49 year olds and TikTok, with its daily 1.6 billion users, to represent those under the age of 30. Search terms “Egg Freezing" and “Egg Freezing Support” as well as the subreddit thread “r/EggFreezing” were used on Reddit and the search functions of “egg freezing” and “egg freezing journey” were used on Tiktok to gather data. Exclusion criteria included posts having less than 10 relevant comments, posts coming from outside of the US, posts regarding embryo freezing, sponsored posts, and medical advice from non-patient medical professionals. Thematic saturation was achieved when 10 consecutive comments were reached with no new themes.
Summary of Results: A total of 4,021 entries were evaluated, 355 were excluded, and 189 posts and 3,477 comments were included in our analysis. The top five general themes on Reddit, with 1,440 entrees, included ‘Personal Experience’ (34%), ‘General Support’ (27%), ‘Advice’ (18%), ‘Side Effects’ (11%) and ’Age of Egg Freezing Experience’ (10%), while the top five general themes on TikTok, with 1,533 entries, were ‘General Support’ (56%), ‘Cost’ (14%), ‘Recommended Age Range for Egg Freezing’ (13%), ‘Personal Experience/Journey’ (9%), and Advice (8%).
Conclusions: Based on the data, the concerns that individuals share in regards to oocyte cryopreservation differ in that the majority of Tiktok users seek to provide general support for one another, while the majority of Reddit users tend to discuss their personal experience. This could be due to the different demographics on the two platforms as well as the platform set up, where Reddit serves more as a discussion forum and Tiktok as response to pre-recorded video streams. Despite the slight differences between the platforms, in general, social media can be used to demonstrate educational gaps in the realm of women’s health. We hope physicians can benefit from learning about unanswered questions that women have about the general concerns and behaviors needed to maximize success in oocyte cryopreservation.
#256
Enhancing Pain Management and Education in Dang, Nepal: Insights from a Community and Healthcare Worker Needs Assessment
Handra J1, Cunningham J1, Yu S1, Penner J1, Sapkota D2, Kapoor V1. 1University of British Columbia, Vancouver, BC, Canada and 2Creating Possibilities Nepal, Kathmandu, Nepal
Purpose of Study: The UBC Nepal Health Education Partnership has collaborated with Creating Possibilities (CP) Nepal since 2015 to improve healthcare outcomes in Dang, Nepal. During community engagement activities, critical gaps in pain education and management were identified. We conducted a needs assessment to identify gaps in education and management for pain in Dang, with the goal of informing community educational resource development.
Methods Used: Community input was obtained through a 16-question Pain Experience and Knowledge survey. The survey included five sections: participant demographics, experience of pain, personal pain management strategies, barriers to care, and educational needs. CP Nepal distributed the survey in paper form to adults during community events, including mothers’ group meetings and health education forums. Responses were later translated and electronically recorded for quantitative analysis.
Healthcare workers, including physicians and community health workers, participated in semi-structured interviews. Interview topics included common reasons for seeking pain management, current treatment methods, and care delivery challenges. Interview transcripts were coded and thematically analyzed.
Summary of Results: To date, 41 community questionnaires have been collected. 31 (75.6%) of participants are female and the average age is 37.59 years. 9 participants (22.0%) required assistance with reading or writing. Of respondents, 34 (82.9%) reported experiencing pain: 13 acute, 18 chronic, and 2 both. Average pain severity was rated at 3.47 for acute and 3.81 for chronic pain on a 0-10 scale. A majority (23/34, 67.7%) experienced daily or weekly pain and participants travelled an average of 1.10 hours for medical care. Participants primarily relied on traditional/herbal remedies (16/34) or rest and relaxation (14/34) for pain management. Common access barriers included limited nearby care or providers (15/34), lack of knowledge (9/34), and medication cost (6/34). Concerns about medication addiction or tolerance (14/34) and side effects (8/34) deterred pain care-seeking. Only 6/41 (14.6%) participants were aware of potential pain medication side effects. Topics desired for pain education included causes of pain (33/41), how to take medication (23/41), side effects (19/41), and non-pharmacological pain management strategies (22/41).
Expert interviews were conducted with 3 physicians and 12 community health workers. Preliminary thematic analysis revealed barriers such as low health literacy, strict government regulations on pain medications, and pharmaceutical scarcity in rural regions. Proposed solutions included creating community educational resources and expanding community health worker training.
Conclusions: Community and healthcare worker input highlights a high prevalence of pain in Dang, coupled with inadequate knowledge and resources to meet population care needs. Collaboration with community partners is crucial for developing pain education and management resources.
#257
Understanding the Barriers and Hesitancies toward the Covid-19 Vaccination in a Safety-Net Hospital in Phoenix, AZ
Winfield B, Sainz A, Hilton J, McElhinny M. Creighton University School of Medicine, Phoenix, AZ
Purpose of Study: Covid-19 created unprecedented turmoil in the United States. According to the World Health Organization, Covid-19 has caused over 1.1 million deaths in the United States as of 09/2023 [1]. While vaccination rates have slowly been growing as of July 2022 [1], the majority of people hospitalized for Covid were unvaccinated (85 percent of total Covid hospitalizations were unvaccinated) [1] [2]. This ultimately places strain on healthcare resources and acts as a barrier to care for the vaccinated. The average hospitalization for Covid costs approximately 20,000 dollars [3].
We aimed to identify common barriers to receiving the Covid-19 vaccine and general attitude towards receiving the vaccine amongst patients at a county hospital in Phoenix, Arizona.
Methods Used: Our data was gathered from patients in a single county hospital in Phoenix, Arizona between the dates of July 2022 and April 2023. Patients were offered an electronic-based mixed-survey combining multiple-choice and free-text answers. We utilized Redcap software to compile the data. We analyzed 33 responses looking at general attitudes towards Covid-19 vaccines based on education level and income level. Responses questioning attitudes towards receiving the Covid-19 vaccine were recorded as “positive” or “neutral/negative”.
Summary of Results: In regards to attitudes towards vaccines, 13 of 21 (62%) respondents that had a total household annual income less than 50,000 dollars had an overall positive attitude towards the vaccine. 8 out of 11 (73%) respondents that made more than 50,000 dollars had an overall positive attitude towards the vaccine. Those that identified as having received at least a Bachelor’s degree had a positive attitude towards the vaccine 9 out of 13 (69%) respondents. Those having less than a Bachelor’s degree had a positive attitude in 12 out of 19 (63%) respondents.
The most common barrier identified to receiving the vaccine amongst respondents was that it “seemed like an inconvenience” and they “did not think receiving another dose made a difference” (30 percent of total responses for each). There were 10 total responses.
Conclusions: In summary, our study looked at identifying barriers to those receiving the Covid-19 vaccine and aimed to further analyze attitudes towards receiving the vaccine based on income level and education level amongst patients of a county hospital. Our study had several limitations. One being that we had a very poor response rate leading to low overall study size. Many patients refused to fill out the survey and many that did agree to it only partially filled it out. Response bias was also possible given that it appeared those that felt strongly for or opposed to the topic of Covid-19 were the ones willing to fill out the survey. Unfortunately, not many definitive conclusions can be drawn from our data given the sample size, however, it can provide an insight to healthcare professionals to researching methods to better serve and understand our patients in future public health issues.
#258
Medical Students’ Attitudes Towards Medicolegal Risk in Obstetrics & Gynecology
Huynh KZ1, Thai AV3, Pickering TA2, Stohl H1. 1Harbor-UCLA Medical Center, Torrance, CA; 2University of Southern California, Los Angeles, CA and 3Western University of Health Sciences, Pomona, CA
Purpose of Study: Despite the rise in residency applications to obstetrics and gynecology (Ob/Gyn), no recent study has examined the factors that influence or deter medical students from this field including medicolegal risk. This study aims to explore medical students’ attitudes towards medicolegal risk in Ob/Gyn.
Methods Used: For this study, we conducted an electronic survey of 1200 medical students in District XI. The survey explored student demographics, exposure and understanding of medicolegal malpractice laws, expressed interest or disinterest in pursuing Ob/Gyn, factors that affect their interest and ranking these factors from most to least important. Fisher’s exact tests and Pearson’s Chi-squared tests were performed.
Summary of Results: Medical students who expressed interest in Ob/Gyn considered the prestige of the field, patient continuity, and the patient population. These medical students were less likely to consider medicolegal risk. Medicolegal risk was the third most common factor that deterred medical students from pursuing Ob/Gyn, with 37.5% ranking it as the most influential factor (p=0.006), and female medical students ranking it higher than male students (p=0.006). Males were more likely than females to know about malpractice laws, although their understanding was limited to “slight” or “some” knowledge (53.3% and 20.0% respectively, p<0.001).
Conclusions: Despite Ob/Gyn being a high-risk specialty for medicolegal liability, it was not an influential factor for those who chose to pursue Ob/Gyn in our study. However, of the medical students that were deterred from the field, medicolegal risk was one of the most influential factors and cited more frequently amongst female medical students. Knowledge about medicolegal risk also differed between genders which highlights the educational gap between genders in medical education.
Liability was the third most common factor that deterred medical students from pursuing Ob/Gyn.
#259
PROMOTING THE USE OF TRADITIONAL INGREDIENTS TO IMPROVE FOOD SECURITY AND HEALTH IN THE BRISTOL BAY AREA REGION
Kaden-Hoffmann MT, Keys T. University of Washington School of Medicine, Seattle, WA
Purpose of Study: Traditional ingredients in the Alaska Native diet have been shown to offer significant nutritional benefits, which are linked to improved health, while not having additives like trans fats and excess sugar. Unfortunately, studies have revealed that, on average, the portion of Alaska Natives’ diet that is traditional has been declining. The Bristol Bay Area in Southwest Alaska is home to 6,500 people (68% Alaska Native) and is served by the Bristol Bay Area Health Corporation (BBAHC) operating a hospital and 21 village clinics, is no exception to this trend. Mostly BBAHC messaging has focused on the downsides of Western-based diets, such as posters displaying the amount of fats and salts in microwavable meals. Currently, there is a need to emphasize the benefits of traditional ingredients and present them as a healthier alternative. This project aimed to bridge this gap, thereby promoting better health while also addressing food security and reducing costs.
Methods Used: During the summer of 2023, a month was spent with a physician at BBAHC’s Kanakanak hospital in Dillingham and in the village clinics in King Salmon, Naknek, and South Naknek. Prior to the trip, an analysis of BBAHC’s 2022 Health Needs Assessment was conducted to gain a deeper understanding of the community’s strengths and challenges. One challenge was the higher incidence rates for obesity (69%), diabetes (11.3%), and the mortality rate for heart disease (1.49/1000 person years) in the BBAHC service area compared to statewide (66, 7.9, and 1.16/1000, respectively). During clinical encounters, it was observed that physicians throughout the BBAHC system often dedicated time to counseling patients on diet and weight with a strong emphasis on transitioning to a traditional diet that avoids processed Western foods. Through discussions with patients, six traditional ingredients were selected. A partnership was established with the Diabetes Program at Kanakanak hospital to explore the nutritional benefits of these traditional ingredients.
Summary of Results: A poster was created to be displayed in exam rooms, highlighting the nutritional benefits of blueberries, red salmon, herring eggs, seal oil, fiddlehead ferns, and sour dock. The poster includes QR codes that lead to recipes for each ingredient. Furthermore, all ingredients are named in the four languages spoken in the region: English, Yup’ik, Supiak/Alutiiq, and Dena’ina. These posters have been distributed to each of the 21 clinics and Kanakanak Hospital.
Conclusions: Providers can utilize these posters as visual aids to discuss nutrition, emphasizing the significance of traditional foods in enhancing overall health and encouraging individuals to make healthier dietary choices. Providers can also assist patients in incorporating these ingredients into their diets using the recipes provided on the posters, thereby promoting a more holistic approach to healthcare. This may potentially lead to a reduction in the incidence of obesity, diabetes, and heart disease within the community.
#260
NAVIGATING BREECH: EXTERNAL CEPHALIC VERSION IN MEDICAL EDUCATION
Kaye M1, Nelson AL1, Dong F1, Stohl H2. 1Western University of Health Sciences, Pomona, CA and 2Harbor UCLA, Torrance, CA
Purpose of Study: With the skills and experience required to perform vaginal breech delivery declining, the American College of Obstetricians and Gynecologists (ACOG) recommends offering external cephalic version (ECV) as an alternative to planned cesarean for eligible patients. If ECV fails or is declined, the decision between vaginal delivery or cesarean section depends on patient preferences, provider experience, and hospital-specific protocols. This study examines clinical faculty intentions and medical student experiences of counseling and observing ECV for term breech presentation.
Methods Used: IRB approved surveys were distributed to clinical faculty and fourth-year osteopathic medical students from WesternU’s Pomona and Lebanon campuses. Three waves of invitations were sent to the students. A comparative analysis evaluated potential differences between faculty practices and student observations.
Summary of Results: The response rates were 17% (10/59) for clinical faculty and 11.6% (38/328) for students. All clinical faculty respondents expressed their willingness to offer ECV. However, only 29.7% of students observed ECV being recommended to patients, with 21.6% observing an ECV attempt. On the other hand, 67.6% reported witnessing a breech cesarean section.
Conclusions: There’s a discernible discrepancy between the intentions professed by clinical faculty and the actual practices observed by students, especially regarding ECV. This raises questions about the applicableness of ACOG’s guidelines in real-world scenarios. This also raises questions about patient counseling, and access to desired procedures and concerns about the impact those are having in the next generation of physicians.
#261
COMMUNITY AWARENESS AND INTERVENTION PROMPTS FOR HEMORRHAGE CONTROL IN POWELL, WYOMING
A Erickson and Keys T. University of Washington, Seattle, WA
Purpose of Study: Powell, WY is a rural agricultural community in Park County, WY 75 miles east of Yellowstone National Park with a population of 6,500 people. There are 2 critical care hospitals in the county and the nearest level II trauma center is 100 miles away in Billings, MT. Due to the large focus on agriculture, HIGH engagement in outdoor recreation, frequent inclement weather, and need to travel large distances frequently for everyday activities, trauma is one of the leading causes of death and disability in the community. Unfortunately, local EMS providers and the public outreach department of Powell Valley Community Hospital noted logistical issues related to timely EMS response and the rapid rate of deterioration of trauma victims. Many community members expressed concerns with the high frequency of traumas and death in the county.
Methods Used: Trauma deaths are the 5th leading cause of death in Park County and 40% of trauma deaths are secondary to excessive blood loss. With a large, sparsely populated area the importance of community members being able to provide basic lifesaving interventions increases. A literature review supported reaching a wide variety of community members might be more effective due to the erratic nature of trauma (i.e. not focusing specifically on one demographic such as a school). In communities where bleeding control was taught the self-reported likelihood of a person intervening rose from 44% to 81%. The value of this education was also useful for promoting health and raising awareness on personal safety by 89% of participants. A community partnership with the Powell Valley Hospital public outreach department was established with a common desire of addressing trauma deaths in the community.
Summary of Results: A handout was developed in basic rack card format with information relating to issues of trauma in the community on one side and basic steps to control bleeding including common pitfalls encountered on the other side. The public outreach department of Powell Valley Community Hospital distributed the rack cards in varied locations of their healthcare system to reach a wide array of people such as the emergency department, front desk, outpatient laboratory, outpatient clinic, and auxiliary outpatient buildings. As the healthcare system is a central hub for many in Big Horn and Park Counties, there is wide reach to the community.
Conclusions: The applicability of the learning outcomes highlighted on the handout to a multitude of demographics in the community would suggest a wide possibility of engagement in Powell. It would be reasonable to expect similar reported usefulness and increased likelihood of intervention. Increased community knowledge and intervention should have a positive impact in Park County trauma situations. Going forward, the addition of a hands-on component in workshop format with addition of tourniquets and subsequent resource distribution to community members (gauze, tourniquets, etc.) would be beneficial.
#262
UNLOCKING MEDICAL COMMUNICATION MASTERY: A CREATIVE PATH THROUGH THE MEDICAL IMPROVISATION ELECTIVE
Khan A1, Siddiqui SI2, Hayton A2. 1Loma Linda University Health, Loma Linda, CA and 2Loma Linda University Health, Loma Linda, CA
Purpose of Study: Effective communication is paramount in healthcare for patient-centered care and interprofessional collaboration. Clinical encounters often demand spontaneous communication in high-stress situations, leaving medical students feeling unprepared. This study introduces a novel approach—a medical improvisation elective designed to equip students with essential communication skills to enhance verbal and non-verbal communication, deep listening, boost confidence, promote empathy, and prepare students for the unexpected challenges of clinical practice. Our objective was to develop and evaluate the feasibility and outcomes of this innovative curriculum to better prepare students for communicating in clinical encounters in a low-stressed environment.
Methods Used: A two-week elective course in medical improvisation was developed specifically for pre-clinical medical students. Each session introduced the tenets of improv through exercises adapted to the medical context, followed by a debrief that connected these skills to clinical applications. A de-identified, self-reported survey, utilizing the validated Self-Perceived Communication Competence Scale (SPCCS), was employed both before and after the elective to assess participants’ communication skills. Additionally, a post-elective survey was administered to evaluate the course, with responses provided anonymously on a 5-point Likert scale, spanning from 1 (strongly disagree) to 5 (strongly agree). Paired t-tests were used to measure the differences in scaled responses.
Summary of Results: A total of 13 students participated in the medical improv elective held in Fall 2022, and the feedback was overwhelmingly positive (Image 1). Paired t-test analyses indicated that pre-test versus post-test SPCC scores were significantly different, implying that participation in the medical improvisation elective did improve communication skills (Table 1). The elective helped the students feel more fearless (mean=4.5±0.6) and increased their self-confidence (mean=4.6±0.6). The mean scores for students’ perceived improvement in listening, teamwork, and the ability to respond in the moment were 4.5±0.7, 4.7±0.6, and 4.7±0.6, respectively.
Conclusions: Medical improvisation curriculum can provide medical students with a safe space to develop and refine their communication skills, ultimately better preparing them for the challenges they will face in clinical practice. It’s an innovative approach to addressing a frequent problem in medical education.
Self-Perceived Communication Competence Scale
Measure
Pre- Mean ( SD)
Post- Mean (SD)
p value
Public
61.0 (22.99)
79.70 (18.40)
0.002
Meeting
54.70 (20.73)
79.30 (14.90)
<0.001
Group
65.40 (16.91)
83.40 (11.60)
<0.001
Dyad
72.20 (13.13)
88.50 (7.57)
0.002
Stranger
49.60 (19.90)
81.0 (13.0)
<0.001
Acquaintance
60.80 (20.30)
83.50 (12.40)
<0.001
Friend
79.70 (13.23)
88.70 (9.20)
0.042
SPCC Total
63.30 (15.1)
84.40(10.7)
<0.001
Self-perceived communication assessment in variable settings using self-perceived communication scale
Evaluation of Medical Improv Elective.
#263
Optimizing the Organization of Familial Genetic Testing Information in an Inherited Retinal Dystrophy Registry
Kwong A1, 2, Boldut R1, 2, Armstrong L3, 4, Gardiner J5, Prentice L3, Wokhloo P3, Duffy D2. 1University of British Columbia, Vancouver, BC, Canada; 2BC Children’s Hospital, Vancouver, BC, Canada; 3BC Children and Women’s Hospital, Vancouver, BC, Canada; 4University of British Columbia, Vancouver, BC, Canada and 5BC Children’s Hospital, Vancouver, BC, Canada
Purpose of Study: As gene sequencing technology becomes more accessible, genetic testing is increasingly common for patients with genetic diseases. Familial genetic testing provides insight into the inheritance pattern, risk factors, and cause of a genetic disease for affected and unaffected family members. Familial testing also allows for the identification of individuals at risk of genetic diseases, which allows for proactive preventative and/or interventional steps. However, familial testing poses an organizational challenge for creating registries for patients with inherited genetic diseases. As such, this project aimed to optimize the fashion in which familial genetic testing results are organized, analyzed, and transcribed into a genetic database for inherited retinal dystrophies (IRD’s) at BC Women’s Hospital (BCWH).
Methods Used: A data collection tool (password-protected excel sheet) was created to collect and organize patient data. This tool included basic information (IE identifying information, date of birth, age), patient histories, and genetic information. Medical genetics numbers (MGNs) are used by BCWH to group members of the same family, and patient documents grouped by their MGN to store multiple related patients in the same chart. Patients with a common MGN were sequentially inputted into the database, ensuring all family members would be grouped in the registry. Consult notes stored within charts were consulted to differentiate the proband from ancillary family members. Family members included in charts but lacking genetic information were excluded from the database if they did not have a medical history relevant to IRD. Charts were reviewed and inputted information was verified by two researchers.
Summary of Results: So far 45 patients and 35 families have been entered into the IRD database. A robust and efficient method for organizing family members to the genetic registry was established. This was achieved by efficient organization of charts and database design, paired chart reviews, and screening of patient family members with irrelevant medical histories. Maintaining this organization becomes increasingly challenging as the registry grows, and continuous optimization in patient organization is critical. The efficiency and organization of familial genetic testing data may allow physicians to be more proactive in the treatment of genetic diseases by identifying family members of patients who are at risk of genetic disease prior to consultation.
Conclusions: We have demonstrated an effective method of organizing family members in a genetic registry. This has the potential to optimize patient care by identifying individuals at risk for heritable diseases. This project illustrates the need for informed, organized, and collaborative approaches to clinical data management.
#264
BURNED OUT BY THE START OF A NEW YEAR? A CROSS-SECTIONAL ASSESSMENT OF RESIDENT-REPORTED BURNOUT SYMPTOMS AMONG RESIDENTS FROM MULTIPLE PROGRAMS AT A SINGLE INSTITUTION
Laguerre W, Taylor R, Tran M, Studer K, Schill-Depew A, Miller C. Loma Linda University, Loma Linda, CA
Purpose of Study: Studies on resident burnout have generated varying outcomes (Rodrigues et al, 2018). This may be attributed to reporting bias or inability of residents to identify burnout symptoms. Our research centers on the utilization of wellbeing programs at Loma Linda University Health Education Consortium (LLUHEC) to assess baseline burnout risk, residents’ confidence in detecting burnout, and the capacity to increase resilience through utilization of our proactive intervention tool, the personalized Plan of Action for Resilience (PAR), which utilizes specific, measurable, attainable, relevant, and timely (SMART) goals to prevent and alleviate burnout (Miller et al, 2021).
Methods Used: Our team engaged the chief wellness residents, program directors, or program coordinators for all 66 of LLUHEC’s residency and fellowship programs. We subsequently assisted with dissemination of the PAR wellbeing tool, a validated Physician Well Being Index (WBI), and PAR feedback survey to residents over 3 months. Categorical survey responses were analyzed as markers of point-in-time wellbeing or burnout.
Summary of Results: Between June 2023 and August 2023, we distributed the PAR to 48 programs (619 residents) and received 105 WBI responses which evaluated resident self-reported wellbeing over the previous month. While 87% of PAR survey respondents (n=48) expressed confidence in identifying burnout signs, 39% of WBI respondents felt burned out from their work. Notably, 51% experienced anxiety, irritability, or depression in the previous month, and 24% reported sadness or hopelessness. Emotional hardening due to work was reported by 43%, while 24% admitted to falling asleep in public spaces, and 23% perceived a work-life imbalance. Overall, 53 participants reported at least one symptom of burnout. On the positive side, 91% found their work to be meaningful. Among the PAR respondents, 61% planned to share the tool with colleagues, and 42% intended to use it themselves in the future.
Conclusions: Our findings highlight significant burnout risk among residents at LLUHEC, who experienced danger signs even at the beginning of the academic year in July. Baseline burnout rates were consistent with previous reports (25-75%, Yash and Tadi, 2023), with higher reported meaning in work compared to other studies. We acknowledge a low response rate and plan to address this in follow-up surveys, ensuring responses are linked to specific programs and PGY years. This research underscores the need for proactive interventions like PAR to support resident well-being and reduce burnout.
#266
Breathe Easy: Improving Smoking Cessation Services for Patients Experiencing Homelessness at the Willow Clinic
Luong BH1, Sujith J1, Lin C1, Richards K2. 1University of California, Davis, Davis, CA and 2University of California, Davis Health, Sacramento, CA
Purpose of Study: Within the large population of cigarette smokers in the United States, approximately 68-80% of the unhoused population are tobacco users (Baggett, et al. 2013). Given the living conditions and circumstances of those unhoused, it is more difficult for them to manage their tobacco usage than those housed. To address the lack of clinical attention for unhoused patients who smoke, the Willow Clinic, a UC Davis student-run free clinic, created its Smoking Cessation program in 2016. This program uses motivational interviewing and one-on-one consultations for patients experiencing homelessness in Sacramento to help them develop a smoke-free lifestyle catered to their values and needs. This Quality Improvement study aims to identify any gaps in our program and determine the best course of action to improve the care we provide to our unhoused patients who smoke. To guide our project, the Plan-Do-Study-Act (PDSA) framework is utilized. The program is in the ‘Plan’ phase, where we are performing a preliminary needs assessment to understand our patient demographics and evaluate patients who have been seen by our developing Smoking Cessation program.
Methods Used: A retrospective review was performed for Willow Clinic patients from June 2021 to October 2022. Data regarding patient demographics, past medical history, and smoking history were collected. From May 2022 onwards, surveys were distributed to patients who had expressed interest in Willow Clinic’s Smoking Cessation program.
Summary of Results: A total of 160 unhoused patients (52.5 ± 10.7 years; 62.3% male) were seen by the Willow Clinic between June 2021 and October 2022. Of these patients, a staggering 54.2% (84) of patients had identified as active smokers. Of those who actively smoke, 39.3% (33) were light cigarette smokers (1-9 cigs/day), 23.8% (20) were moderate cigarette smokers (10-19 cigs/day) and 17.9% (15) were heavy cigarette smokers (20-39 cigs/day). Since May 2022, 48 patients who were active smokers were surveyed and asked if they were interested in being seen by Willow Clinic’s Smoking Cessation program. Eleven patients have expressed interest in quitting, and 5 have expressed interest in reducing their tobacco usage.
Conclusions: Our findings reveal the importance of increasing patient engagement in our Smoking Cessation program. As we advance to the next stages of the PDSA framework, our project has two aims: 1) to introduce a clinical intervention to better assist our existing Smoking Cessation patients to transition to a smoke-free lifestyle, and 2) to increase awareness of our program among general Willow Clinic patients who smoke. For the first aim, we seek to combat the issue of patient retention via a new system that can better track patients’ progress over time and encourage continued program attendance. For the second aim, we plan to distribute flyers of our Smoking Cessation program during our outreach efforts, with the goal of increasing awareness and educating our unhoused community members about the services we provide.
#267
Title: Experience of Adolescents with Cerebral Palsy with the ExerciseRx App: Qualitative Feedback Regarding App Usability for Home Based Exercises
McCue J1, Grenard D2, Li T3, Reibold C1, Leibow C2, Lin C1. 1University of Washington, Seattle, WA; 2Seattle Children’s Hospital, Seattle, WA and 3University of Minnesota, Minneapolis, MN
Purpose of Study: Adolescents living with cerebral palsy (CP) often require lifelong physical therapy and exercise to maintain their health and function. However, challenges including time, transportation, and engagement during the adolescent years can impact therapy adherence, leading to suboptimal functional and physical outcomes. Recent research indicates that interventions using digital health and wearable activity trackers have the potential to boost physical activity levels; however, there are few apps designed to support adolescents with physical disabilities. This study aims to assess the patient-centered usability of ExerciseRx-CP, a mobile app integrated with electronic health records, designed at our university for supporting regular home based exercise.
Methods Used: Semi-structured virtual interviews via Zoom were conducted with five participants to gather insights on the feasibility of an in-home exercise app and to better understand patients’ experiences with exercise. Screenshots of the patient app were presented to participants for their feedback. Interview data underwent thematic coding and multistage affinity mapping to extract insights on app usability, design, and overall user experience. Feedback was categorized into themes such as exercise importance, exercise experiences, app intuitiveness, benefits and drawbacks of the app, motivation, and barriers to engagement.
Summary of Results: The interviewees, with a mean age of 15 years, included 20% females. All participants emphasized the significance of exercise for strengthening muscles in teens with CP. Specifically relating to CP, interviewees commented on the utility of exercise in relaxing muscle tone and the need to maintain functional movement for activities of daily living. Views on self-recording video during exercises varied; some were indifferent, others saw benefits in improving form, and a few considered it invasive. Participants were willing to use the app on average for three to six weeks for activity support. Common themes from the interviews included recommendations to improve motivation and goal setting by incorporating incentives or rewards into the ExerciseRx-CP interface.
Conclusions: Consistently, participants voiced the importance of exercise for strengthening muscles in teens with CP. Acknowledged challenges relating to exercise adherence included access to exercise equipment, having to remind selves to perform and perceived lack of motivation from phsyical therapists. Participants acknowledged the role of digital apps and media in their lives. While most understood the app’s information, some usability recommendations were raised. Future enhancements could involve incorporating gamification, setting reminders, displaying progress indicators, and involving families to improve proper exercise adherence. This study was important in identifying the barriers and facilitators in adolescents with CP to use of ExerciseRx-CP app to help improve the tailoring of digital health tools to support the unique needs of this population.
#268
CONTRACEPTION EDUCATION TO ADDRESS TEENAGE PREGNANCY IN TORRINGTON, WYOMING
Mills HS1, Keys T2. 1University of Washington School of Medicine, Seattle, WA and 2University of Washington, Seattle, WA
Purpose of Study: Torrington, Wyoming has a teen birth rate of 23.7 births compared to the national rate of 18.8 births per 1,000 women aged 15-19 years old. Although comprehensive support exists for teenage parents through Wyoming’s Hand in Hand and WIC Programs, there is no pregnancy prevention program, and the nearest Title X Family Planning Clinic is over 30 miles away. Therefore, providing education on birth control options to adolescents will increase contraception use and lead to reduced rates of unplanned teen pregnancy.
Methods Used: A review of the 2019 Torrington Community Needs Assessment identified a need for improved health literacy and access to care. Specifically, conversations with physicians and members of the community regarding the strengths and needs of the community were completed which highlighted teenage pregnancy as a current concern. Literature review revealed that despite having higher pregnancy rates, fewer programs exist for rural youth; however, school-based programs tend to have the greatest reach. Therefore, community partnerships were made with Torrington High School and Goshen County Public Health. The literature notes contraception use as a greater contributor than changes in sexual activity to the decline in adolescent pregnancy rates. One rural program that implemented a seminar with contraception pamphlets found that 100% of participants believed it increased their awareness and openness to other contraception methods as well as an increase of 2.3 points (on a 10-point scale) of their perceived education of long-acting reversible contraception.
Summary of Results: Infographic posters and pamphlets were developed and given to all community partners that provided contraception education on the methods and efficacy of birth control. Goshen County Public Health intends to disseminate the pamphlets to those who may be receiving STI/HIV or pregnancy testing and display posters in their waiting room. Additionally, Goshen County Public Health shared materials with Wellness Wagon, a mobile healthcare provider reaching individuals at home in areas surrounding Torrington. Torrington High School plans to display posters and distribute pamphlets if desired to students.
Conclusions: As Torrington has comprehensive support for teenage parents that has greatly assisted so many, the best avenue to addressing the prevention of unplanned teenage pregnancy was using infrastructure already in place to promote healthcare provider partnership in identifying the birth control method that best fits each individual’s lifestyle and circumstance. This partnership along with the educational materials should have a positive impact on contraception use and teenage pregnancy in the Torrington community. The next steps would involve education on social determinants of teen pregnancy, ensuring youth are able to access clinical services, increased referral of youth to clinic services, and engaging and motivating community members through public awareness campaigns.
#269
SHIFTING FROM PEER REVIEW TO PEER LEARNING IN THE DEPARTMENT OF RADIOLOGY
Nakashima K, Xu C, Park S, Aldoghmi M, Llauro N, Aguilar D, Shieh S, Anavim A, Houshyar R. University of California, Irvine, Orange, CA
Purpose of Study: Practicing radiologists must participate in ongoing performance evaluations in the form of a scored peer review system to maintain their professional competencies. The peer review system while in use for decades, poses some problems due to lack of anonymity and the possibility of being used as a punitive measure. To address these issues, shift towards individual and group teaching, building community within the department, and improving patient care, peer learning, a review process focused on feedback, learning, and improvement, was introduced at our academic institution. This study aims to assess peer learning between professional colleagues centered around studying errors as a group rather than as individuals, improving processes and systems, and creating a workplace environment that focuses on learning rather than punishment.
Methods Used: In this retrospective analysis, we reassessed the physician participation in the peer learning program over time since its implementation at our institution. This study was conducted in the Department of Radiology at UC Irvine Medical Center, an academic hospital. Implementation of peer learning began July 2019 and was established June 2020. This process has three stages: to solicit feedback, discuss learning opportunities, and execute improvement. The concept of feedback establishes learning opportunities for attendings and fellows to give and share reflections on the group’s performance issues. In the learning process, a quality and patient safety nurse leads and facilitates monthly peer learning meetings by scheduling presentations, assigning cases, and emphasizing learning points. The goal is to discuss potential pitfalls and develop strategies for preventing error, such as near misses, while maintaining a constructive tone with all participants. All attendees are responsible for process and system improvement by identifying problems, developing action plans, and following up on these items during the next conference to drive change. The attendance was tracked and analyzed retrospectively to determine the efficacy of the peer learning process at this institution.
Summary of Results: Following the complete implementation of the peer learning process in June 2020, attendance rates increased from 62% in 2020 to 75% in 2021 and further increased to 79% in 2022.
Conclusions: The transition from peer review to peer learning aims to reinforce a supportive learning environment by replacing score-based evaluations with collaborative constructive feedback amongst professional colleagues. It is important to highlight the significance of the Quality Nurse, given their leadership role in the development and oversight of the peer learning process. The removal of quantitative data raises potential questions on the efficacy of peer learning to grade a physician’s accuracy in diagnosis. However, further studies can remediate this limitation by comparing patient outcomes prior to peer learning.
#270
CHARACTERIZING THE NEONATAL INTENSIVE CARE UNIT MICROBIOME AND EVALUATING THE ASSOCIATION WITH POSITIVE BLOOD CULTURES
Nolan M1, Loc-Carrillo C2, Chan B1, Elkayssi M3, Ling C1, Drews F4, Grubb P1. 1University of Utah, Salt Lake City, UT; 2University of Utah, Salt Lake City, UT; 3University of Utah, Salt Lake City, UT and 4University of Utah, Salt Lake City, UT
Purpose of Study: After an extended period of nearly three years with zero central line-associated blood stream infection (CLABSI) events in the University of Utah neonatal intensive care unit (NICU), the CLABSI rate increased significantly and remains elevated. As part of a larger investigation and infection prevention effort, this study characterized the environmental microbiome in the NICU by sampling high-touch surfaces and equipment over a one-year period. The study also compared the microbes found in the environment to those responsible for positive blood cultures in patients in the unit over the same period. This study served as the baseline for our ongoing quality improvement effort to reduce CLABSIs and BSIs in the NICU.
Methods Used: Environmental samples were collected from various high-touch surfaces and equipment in the NICU, including isolette portal handles, stethoscopes, bedside computer workstations, and other items for 20 bedspaces in two high-turnover, high-acuity multi-occupancy rooms in fall 2022 and spring 2023. Samples were cultured and speciated using MALDI-TOF mass spectrometry at the Utah Public Health Laboratory. A third round of microbial sampling is planned for fall 2023. CLABSI and BSI data were extracted from reportable Centers for Disease Control National Healthcare Safety Network data for the period August 1, 2022, through August 31, 2023. The two data sets were compared for microorganisms common to both.
Summary of Results: A total of 461 environmental microbial samples were collected and 116 of those returned positive for one or more microorganisms (25% overall positivity rate). The most common microorganisms found in the NICU environment were coagulase-negative Staphylococcus, Micrococcus, and Bacillus species. Staphylococcus aureus, Enterococcus, Klebsiella, and Neisseria were also found. During the study period, there were a total of 29 positive blood cultures (3 CLABSIs and 26 non-CLABSI BSIs). There was overlap between the species of microorganisms found in the NICU environment and those responsible for 21 (72%) of the total positive blood cultures including all three of the CLABSIs.
Conclusions: It is understood that the NICU environment cannot reasonably be expected to be entirely sterile, yet the overall 25% positivity rate of environmental microbial samples suggests there is a relatively high microbial burden in the NICU. Microorganisms that grew from our environmental samples were a mixture of virulent, potentially infection-causing microorganisms and those that are known to commonly colonize the environment. Though a causative link was not investigated in this study and cannot be concluded from the data collected, the overlap between environmental and infection-causing microorganisms responsible for positive blood cultures indicates there is a positive association. A third round of environmental sampling is currently in progress, and those results will be compared against the prior data to evaluate for any potential patterns or inconsistencies.
#271
TEACHING MEDICAL STUDENTS HOW TO HAVE BRAVE CONVERSATIONS TO PROMOTE UNDERSTANDING
Nwankwo O1, Ongyiu A1, Sajdak G1, Hayton A1, ChenFeng J2. 1Loma Linda University, Loma Linda, CA and 2Fuller Theological Seminary, Pasadena, CA
Purpose of Study: Competencies woven into medical school curricula include the need to recognize and mitigate stigma and bias in various interactions, foster partnership with a diverse healthcare team and patient population, and build trust in patient-doctor relationships. Brave conversations, built on respect and civility despite controversy, can provide students and healthcare professionals with valuable opportunities to acknowledge and address social determinants of health in practice.
The purpose of the presentation was to educate first-year medical students on the importance of brave conversations, and to provide the prerequisite skills needed to practice having brave conversations.
Methods Used: A 3-question, anonymous Likert scale pre-survey was administered to gauge first-year medical students’ level of comfort in, and willingness to engage in brave conversations. A presentation by professors from the Schools of Medicine, Religion, and Office of Physician Vitality followed. The presentation focused on defining truth, understanding how to make spaces safer through skills to have brave conversations. The session ended with a linked post-survey using the same questions.
Summary of Results: The surveys were completed by 98 students. The pre-session survey showed 50% were somewhat or very comfortable working with groups of people with whom they disagreed, 37% were somewhat or very comfortable engaging in meaningful conversations about differences, and 56% were somewhat or very comfortable presenting differing opinions with others. The post-survey results showed 68%, 74% and 68% respectively.
Conclusions: The survey results were statistically significant (n = 98, p <0 .05) as more students reported a higher likelihood of engaging in brave conversations after the session.
#272
Evaluating Patient Perceptions of Smartphone Use for Active and Passive Collection of Health Data
O’Neill CK1, Duckworth E2, Shah R2, Jayakumar P2. 1University of Washington, Seattle, WA and 2University of Texas at Austin, Austin, TX
Purpose of Study: Limited evidence has been collected on patient perspectives of remote health data collection and health status monitoring. The primary objective of this study is to assess patient willingness to share smartphone generated health data with providers. A secondary objective is to characterize patient populations who express hesitation around providing these data to providers.
Methods Used: Patients were recruited from the Amazon Mechanical Turk online surveying tool. The survey probed patient comfort around various modes of data sharing with an orthopedic doctor: active perceptual data and image sharing, passive social data sharing (e.g. number of calls, texts), and passive physical activity transmission (e.g. time sitting, sleeping, walking). Bivariate analysis involved unpaired t-test or analysis of variance for comparing continuous variables. An alpha value of 0.05 was used. A multivariable regression to investigate demographic factors associated with comfort with sharing health data was performed. Odds ratios compared participants by age group, educational attainment, and race.
Summary of Results: A total of 485 participants completed the survey, with an average age of 38 years old. Respondents were 65% male and 73% Caucasian. The majority (70%) of participants were comfortable answering questions about their health on their phone, as well as sending pictures of their health problems or wounds. Over half of participants were comfortable with passive social and physical activity information being sent to their doctor and would allow their doctors to download a data tracking application on their smartphone (55% and 59%, respectively). Younger participants (OR 2.0, p<0.05) and participants with increased education (OR 2.5, p < 0.01) were more likely to be comfortable in sharing their data. Privacy concerns were cited as the most common reason patients desired to refrain from sharing data.
Conclusions: Most study participants were comfortable sharing smartphone generated health data.
#273
CHALLENGING TRADITION: COMPARING THE SAFETY AND EFFICACY OF ULTRASOUND-GUIDED PERCUTANEOUS NON-TARGETED LIVER BIOPSY IN THE PEDIATRIC POPULATION: RIGHT VERSUS LEFT LOBE APPROACHES
Overfield ID1, Turk A2, Parry X1, Lee H1, Liao M2, Smith J2, Chen R2, Cooper K2, Cho A2, Jin D2. 1Loma Linda University, Loma Linda, CA and 2Loma Linda University, Loma Linda, CA
Purpose of Study: Compare the safety and efficacy of right hepatic lobe (RHL) versus left hepatic lobe (LHL) approaches for ultrasound-guided percutaneous non-targeted liver biopsy in the pediatric population.
Methods Used: Retrospective review was conducted on 160 non-targeted percutaneous US-guided liver biopsies performed at a single tertiary care children’s hospital over a 13 year period (2010-2023), with direct comparison of RHL versus LHL approaches in pediatric patients. Demographics observed included patients’ age, gender, height, weight, BMI, inpatient/outpatient status, needle type (Supercore, Biopince, Temno) and gauges used, biopsy indication, underlying coagulopathy, anticoagulation medication status, complication rate, and laboratory studies (Platelets, PT, INR, PPT). Technical success was determined by histological diagnosis provided in the medical chart. Data analysis was performed with independent sample T-test, Fisher’s exact test, Chi Square Test, ANOVA, post-hoc tests, and Mann-Whitney U tests.
Summary of Results: Out of the 160 biopsies, 131 (81.9%) were RHL and 29 (18.1%) were LHL. Baseline patient characteristics undergoing RHL versus LHL approaches were not statistically significant (all P-values >0.23). Comparing RHL and LHL approaches, there was no difference in technical success with RHL (131/131 100%) and LHL (29/29 100%). Among the RHL approaches, 45/131 (34%) patients were inpatients and 13/29 (45%) were inpatient for the LHL cohort (P=0.29). Complications were observed in 2/131 (1.5%) RHL and 1/29 (3.4%) LHL, (P=0.43). One patient (aged 5.5 months) in the LHL cohort expired (Complication Class F) secondary to procedural related hemorrhage. In the RHL cohort, both patients had minor complications that required no therapy or hospital stay (Complication Class A).
Conclusions: Contrary to some traditional notions, with the advent of ultrasound, there may be no statistically significant difference in the technical success rate or complication rate in RHL versus LHL approaches to US-guided percutaneous non-targeted liver biopsy in the pediatric population. The approaches may come down to the operator’s preference and the patient’s anatomy.
Patient characteristics of LHL vs RHL approaches
LHL (n=29)
RHL (n=131)
p-value
Male
16/29 (55%)
80/131 (61%)
0.56
Mean Age ±SD
10.4±4.83
9.91±5.32
0.623
Mean BMI ±SD
23.8±8.3
24.2±8.0
0.825
Coagulopathy present
3/29 (10%)
26/131 (20%)
0.23
Anticoagulant/antiplatelet medication
0/29 (0%)
9/131 (6.9%)
0.37
Mean INR ±SD
1.2 ±0.1
1.2 ±1.1
0.772
Mean platelets (x109/L) ±SD
237.9 ±84.4
266.7 ±130.1
0.274
Mean PTT (sec)
36.1 ±16.5
41.3 ±45.2
0.670
#274
Pediatric Educational Discussion Scenarios: Empowering Residents to Cope with Difficult Patient Encounters and Adverse Medical Events
Payne C1, Zieve H1, 2, Taylor-Lucas C1, Shekarabi N1, Vasa M1, Reddy V1, Bauer K1, Afghani B1, 2. 1UC Irvine School of Medicine, Irvine, CA and 2Children’s Hospital of Orange County, Orange, CA
Purpose of Study: Medical residents and physicians commonly face challenging clinical situations such as dealing with adverse events and difficult patient encounters that may lead to burnout and anxiety. One way to process these distressing events is through debriefing, however training on how to debrief and hold debriefing sessions is not commonplace in residency training programs. The objective of this study was to determine the effectiveness of Pediatric Educational Discussion Scenarios - Reflect, Inspire, Support, and Empower (PEDS-RISE) workshops designed to teach coping strategies to first year pediatric residents.
Methods Used: All 25 participants completed the pre- and post- workshop surveys. Two workshops were designed to teach first year pediatric residents strategies to cope and care when 1) challenged by difficult patient encounters and 2) faced with an adverse event. The workshops were developed in collaboration among ambulatory and in-patient pediatricians, a psychologist, and a psychiatrist. Each workshop consisted of a short video scenario and reflection from a psychologist and psychiatrist, followed by a seminar discussion conducted via Zoom. The coping strategies taught included the Periodic Table for High Concern Communication Tool Box, 4Cs (Care, Communication, Compassion, Community) when dealing with an adverse event, and 4Ds (De-escalation, Deep listening, De-briefing, De-stressing) when dealing with difficult patient encounters. The facilitator gave the residents an opportunity to self-reflect after each case. Anonymous pre- and post- workshop surveys were administered to assess the residents’ comfort with processing and debriefing.
Summary of Results: Pre- and post- workshop surveys demonstrated statistically significant increases in residents’ comfort in identifying when a debriefing session is necessary for themselves or a colleague, holding a debriefing session for a junior colleague, and using tangible strategies to cope with adverse medical events or difficult patient encounters. Only 4% of residents reported familiarity with coping and communication strategies for handling difficult patients prior to the workshop, which increased to 100% after the training. Residents’ awareness of support systems for handling difficult patients and for coping with medical mistakes increased from 44% and 24%, respectively, to 100% in the post-workshop survey. The limitations of our study include social desirability/response bias, small sample size, and a single center study.
Conclusions: Our preliminary results show that facilitated reflection about difficult patient encounters, using video case scenarios, serves as a model to enhance resident training by teaching the skills needed to cope with distressing events in pediatric clinical learning environments. Such case scenarios may be further adapted and applied to other fields of medicine and levels of training within the medical profession to enhance physicians’ resilience and well-being.
Pre- and Post- Workshop Resident Survey Responses on the Effectiveness of Two Video Case Scenarios (n=25)
Table 1.1 “Coping and Caring when Challenged by Difficult Patient Encounters” Workshop.
Mean*
Survey Statement
Pre
Post
P-value
I am very comfortable communicating with a demanding or distressed patient/parent.
2.56
3.08
0.001
I recognize the symptoms of distress in myself when dealing with a difficult patient/parent.
3.12
3.48
0.005
I can identify when a debriefing session for myself is necessary after dealing with difficult patients.
2.76
3.28
<0.001
I can recognize symptoms of distress in my colleagues when dealing with difficult patients/parents.
3.00
3.24
0.026
I can identify when a debriefing session is necessary for one of my colleagues or junior team members.
2.60
3.12
0.001
I am comfortable with holding a debriefing session if one of my more junior team members is in need.
2.12
2.88
<0.001
I am aware of additional support systems available to help me when dealing with difficult/demanding patients or parents.
2.32
3.44
<0.001
I am familiar with the 4 Ds strategy when dealing with demanding or difficult patients/parents.
1.72
3.52
<0.001
I am familiar with the Tool Box: Periodic Table for High Concern Communication.
1.68
3.36
<0.001
Table 1.2 “Coping with Making a Medical Mistake or Adverse Event” Workshop.
Purpose of Study: In the remote regions of Bajura and Achham in Nepal, nutrition isn’t just a matter of personal choice; it’s a complex interplay of societal norms, economic constraints, and geographical challenges. Residents of these regions primarily rely on two methods for obtaining their daily food: growing it themselves or purchasing from local markets.
Even these seemingly straightforward methods are fraught with socioeconomic and logistical barriers. Income disparities and limited economic opportunities create substantial challenges for accessing an adequate and diverse diet. The seasonal ebbs and flows of crop cultivation, coupled with factors like inadequate irrigation and technological limitations, compound these difficulties. A common thread in these regions is the unsettling reality of running out of food.
In anticipation of launching a comprehensive health initiative in Achham and Bajura districts in collaboration with the Nepal government, a Nepali study team conducted a nutritional and economic survey to identify major nutrition related health challenges. The goal of this study is to describe prevalence of food insecurity, food procurement challenges and household economic means in 2 remote districts of Nepal.
Methods Used: A Nepali team of public and community health experts conducted a standardized economic and nutrition household survey in a convenience sample of households in Accham and Bajura districts over a span of six months in 2023. In this qualitative survey, answers to open-ended questions were grouped into indexed themes and transferred into an electronic format for de-identified descriptive analysis.
Summary of Results: A total of 364 surveys were completed. Respondents were 100% female reporting an average household income of 190,544 Nepali rupees. 73% of households reported running out of food; Food source: on average 37% of food is grown at home vs 62% of food is purchased at the market. Major obstacles to food procurement were reported to be lack of funds and lack of land/fields to grow crops.
Conclusions: Food scarcity and poverty are significant challenges in Accham and Bajura. Economic and nutritional programs need to be considered in future health strengthening interventions.
Average findings from each region.
Location
Percent of food grown at home
Percent of food purchased
Answered ’Yes’ to the question: Do you ever run out of food at home?
Average Annual Income (Nepali rupees)
Achham Chaupati
38.6%
62.8%
73.6%
229,411
Achham Dhakari
25.0%
75.0%
98.1%
205,405
Bajura
45.9%
51.8%
54.1%
136,818
Average
37.0%
62.0%
73.0%
190,544
#276
SALUD CON SABOR: CULTURALLY TAILORED NUTRITION EDUCATION MATERIAL TO EQUIP LATINOS WITH TYPE 2 DIABETES IN MOUNT VERNON, WASHINGTON
Reinhardt MI, Keys T. University of Washington School of Medicine, Seattle, WA
Purpose of Study: Mount Vernon, Washington is a charming coastal town of approximately 35,000 residents in Northwest Washington. Over one third of the population identifies as Latin, most of who are Spanish speaking. Evidence demonstrates Latinos in the U.S. are at increased risk of developing Type 2 Diabetes (T2D) and are disproportionately susceptible to low health literacy. These findings hold true in Mount Vernon, where the highest rates of both poverty and T2D are within the Latin community. This project will provide Latinos with a culturally appropriate resource to equip patients with knowledge and confidence to make healthy diet changes to help manage T2D and mitigate the associated risk of cardiovascular disease.
Methods Used: Conversations with local health educators and dieticians assisting Latinos with T2D indicate many patients are unable to access or afford appointments to discuss the role nutrition can play in self-managing their chronic disease. Even if patients secure initial consultations, discontinuity of care is common due to a language barrier. Typical diet-change materials might suggest patients “consume fewer pastas,” or “try Swiss instead of American cheese,” but Latinos do not typically eat pastas or American cheese. Reducing refined carbohydrates in a Latin diet would consist of eating less ‘masa,’ or the dough used for tortillas and tamales. A suitable low-fat cheese option is queso panela. Just as language is too complex to translate verbatim, so is nutrition. Fortunately, studies show culturally and linguistically appropriate services lead to better health outcomes.
Summary of Results: Using guidelines from the American Diabetes Association and the American Heart Association, a comprehensive educational handout was designed in Spanish with the intention of providing nutritional education tailored to a typical Latin diet in Mount Vernon. Local Registered Dietician Nora Burnfield graciously extended her expertise in which foods (considering local cost, availability, and popularity) were most applicable. The handout includes education on HbA1c levels, correct portion size, healthy versus unhealthy fats, and empty lines for patient notes/reflection. The language is simple, and many illustrations fill the page. Patient Oriented Evidence that Matters (POEMs) and the ‘good of the family’ are proven to be effective motivators in the target population and are present on the page for that purpose.
Conclusions: This handout is currently being sent to the Sea Mar Community Health Center in Mount Vernon for physicians, dieticians, nutritionists, and health educators to provide to Latin patients with T2D who can benefit from culturally appropriate nutrition recommendations to live longer and healthier lives. It has the potential to be used in other settings including offices, clinics, hospitals, and community centers in and outside of Mount Vernon.
#277
FIGHTING MEDIA WITH MEDIA: ADDRESSING THE YOUTH MENTAL HEALTH CRISIS IN GILLETTE, WYOMING BY MEETING THEM WHERE THEY’RE AT
Robitaille T1, Keys T2. 1University of Washington School of Medicine, Seattle, WA and 2University of Washington, Seattle, WA
Purpose of Study: In May 2023, the U.S. Surgeon General voiced concern that social media may be exacerbating the youth mental health crisis in a public address titled Social Media and Youth Mental Health. There is also concern amongst parents and young people alike, particularly in the small community of Gillette, Wyoming, which is younger on-average than the rest of the state and has a 40% higher suicide rate than the national rate. In fact, topics related to mental health and suicide are rated as three of the top five priorities of the 2022-2024 Campbell County Heath Needs Assessment. The purpose of this study was to deliver the people of Gillette the expert-driven strategies to safely use social media and reduce poor mental health secondary to social media use in the most widely accessible method of distribution possible. It was hypothesized that posting mental health education resources online and on social media sites may improve uptake and mental health among young people in Gillette, Wyoming.
Methods Used: An asset-based approach was first taken to elicit the programs already in place that had historically been working to improve mental health in Gillette and thus would continue working to improve it. A community partnership was established with Campbell County Memorial Hospital, who is strongly invested in the improvement of mental health for their community. The hospital publishes a health education blog on their website and social media sites that often includes resources and education concerning mental health. Next, a literature review was completed to compile the evidence surrounding social media and its effect on youth mental health, as well as the effectiveness of social media as a method of distributing resources and education about mental health.
Summary of Results: Based on a review of the current literature, social media may be at its best when helping with identity formation, peer support, and community building among kids of marginalized populations, such as sexual, gender, neurodiverse, and racial minorities. At its worst, it may be contributing to the youth mental health crisis, and frequent social media use may be altering the centers for emotional regulation, impulse control, and moderating social behavior in developing brains. Additionally, the use of social media sites to distribute mental health support and education have been found to be well received by young people, with high usability, engagement, and perceived support.
Conclusions: The health education blog about social media and youth mental health with information provided by the AAP and U.S. Surgeon General was distributed by Campbell County Memorial Hospital on its website and social media sites in September of 2023. While there is still much research that needs to be done to elicit the extent of social media’s effect on youth mental health, as well as the use of social media to deliver mental health education and resources, much can still be done to improve mental health among young people in the meantime.
#278
STEP 1 TO WELLNESS: A STUDENT-LED RESILIENCE INITIATIVE DURING USMLE STEP 1 STUDYING
Butoy J, Rotinsulu A, Tran D. Loma Linda University School of Medicine, Loma Linda, CA
Purpose of Study: Medical students face high levels of stress and burnout during their training.The Step 1 to Wellness program was developed at Loma Linda University School of Medicine to promote resilience by encouraging participation in seven categories of wellness activities during the USMLE Step 1 dedicated study period.
Methods Used: Participants documented their activities on Discord or by emailing the moderators of the initiative. They were entered into a weekly drawing for gift cards and a separate larger prize drawing for completing activities for four consecutive weeks.
A survey consisting of 15 questions was conducted to assess the involvement and self-reported effectiveness of the Step 1 to Wellness (S12W) program. The survey was emailed to the participating medical student cohort, with a total of 67 out of an estimated 160 students responding.
Summary of Results: 31 of the 67 students reported participating in the initiative, with 45.2% (14/31) of those students reporting engagement in wellness activities every day during the initiative. The top two categories that students participated in and posted about were “Physical Activity” and “Relationships/Social Connection”. 93.5% of students reported a positive impact on their stress levels in response to the program. The top reasons for non-participation were a lack of interest or forgetfulness, and a fear of publicly posting about the program. 47.8% of students reported an increased likelihood of participating in these activities when seeing their peers engage. Logistic regression was used to analyze the relationship between peer motivation and participation (coef. =1.43, p< 0.001 95% CI [0.68-2.17]) and monetary motivation and participation (coef. = 1.12, p= 0.002 95% CI [ 0.41 - 1.84]) respectively.
Conclusions: Students who engaged in these fulfilling activities every day prior to the program continued to do so during the program, while those who engaged in these activities less frequently decreased their frequency during the dedicated Step 1 study period. This decrease may have been due to the demands of boards preparation. However, most students reported that engaging in these activities had a positive effect on their stress levels during this time. Those that did participate in S12W were more likely to be influenced by peer participation compared to non-participants. The finding that peer engagement can be an encouraging factor in participation highlights the importance of social influence in promoting participation in resilience activities.
The Step 1 to Wellness program has the potential to promote resilience and decrease stress among medical students. Future directions for the program could include continued funding for future classes, integration into the medical school curriculum, providing alternative proof of participation, and implementing the program year-round. The results of this study also highlight the importance of promoting social connectedness and considering individual differences in spirituality in future wellness initiatives.
#279
A Fresh Take on Feminine Care: Describing Women’s Non-Menstrual Hygiene Practices and Perceptions
Skillman K, Nguyen J, Chen M, Nelson AL, Nguyen L. Western University of Health Sciences, College of Osteopathic Medicine of the Pacific, Pomona, CA
Purpose of Study: The use of feminine hygiene products beyond menstrual care is a common practice among women despite guidelines recommending against it. However, there is limited research on the types of products women use, their motivations, and any potential health implications of product use. This study surveyed women to learn about the habits and perceptions women have regarding non-menstrual feminine hygiene product use.
Methods Used: An IRB approved, beta-tested survey was administered on 2 Instagram accounts (HL 3,414 followers and VY 238,000 followers) and in-person (LN’s office) to examine women’s non-menstrual feminine hygiene product usage, motivations, and side effects with product use. The results of the survey were analyzed for the frequency of responses to each question. For comparisons we used chi squared testing to determine possible differences between groups. We set the p value to be less than 0.05 to establish statistical significance.
Summary of Results: Although 61 women responded to the survey, only the data from 51 women were eligible for analysis. Ages of respondents were 37% 18-25, 51% 26-35, 8% 36-50, and 2% >50. Respondents were predominantly caucasian (49%), with 31% asian, 12% hispanic, and 8% other ethnicities. For vaginal use, 46% of respondents reported use of vaginal soap cleansers, 36% used wipes, 7% used deodorants, and 3.6% used douches, over the counter creams, or perfumes inside their vaginas. The fact that over one third of women used wipes for vaginal use raises the issue of whether the respondents knew the difference between vaginal and vulvar products.
For vulvar products, 50% use wipes, 43% use soaps, and 3.6% use deodorants, perfumes, and over the counter creams. 18 women provided why they used products. The most common responses for use were odor (44%) and cleanliness (33%). 46% of the 24 respondents who responded experienced at least one adverse event from using products such as dryness (36%), burning (27%), itching (18%), and excess vaginal discharge (9%). Vulvar wipe use (n = 47) was similar across ethnicities with white women (32%), asian women (27%), and hispanic women (16%) [p = 0.127].
Conclusions: Non-menstrual feminine hygiene product use is a prevalent and complex phenomenon among women, with diverse motivations and reported adverse health outcomes. Understanding the factors driving this behavior is crucial for healthcare providers, educators, and policymakers to promote safe and informed feminine hygiene practices. There is a need for clinicians to educate their patients in avoidance of unnecessary product usage.
#280
AGE FRIENDLY HEALTHCARE IN RAWLINS, WYOMING
Stampfli M1, Keys T2. 1University of Washington School of Medicine, Seattle, WA and 2University of Washington, Seattle, WA
Purpose of Study: Rawlins, Wyoming is the largest town in Carbon County. In a 2020 Community Needs Assessment, Carbon County was ranked 22 out of 23 Wyoming counties in overall health outcomes, and 20 out of 23 in length of life, measured as premature death before the age of 75. The population of people 65+ is 18.9%, higher than the national average of 17.3%. The Age Friendly framework was created to improve healthcare experiences for older adults and bridge gaps in communication between transitions of care. The 4Ms of the framework stands for What Matters, Medications, Mentation, and Mobility. Providing information on the Age Friendly framework (4Ms) and community resources will improve health outcomes of older adults in Rawlins, Wyoming.
Methods Used: Through informal conversations with Rawlins healthcare staff and patients, public health concerns such as chronic disease management, lack of end-of-life planning, and lack of knowledge of available resources in the community were emphasized. A literature review was completed on the Age Friendly framework and advance care planning. Studies show when the Age Friendly framework is integrated into healthcare visits by physicians, there is more shared decision making, increased depression and dementia screening, increased deprescribing and avoidance of high-risk medications, and increased functional ability, all which improve health outcomes. Additionally, multiple studies on Physician Orders for Life Sustaining Treatment (POLST) documents show that individuals with a POLST completed within 6 months of death are less likely to have CPR or ICU care against their wishes.
Summary of Results: Carbon County Public Health (CCPH) offers low-cost healthcare, LT101 assessments, outreach programs like monthly blood pressure checks, and is a resource hub for the community. A partnership was formed with CCPH to develop and distribute an educational brochure outlining the Age Friendly framework with questions for patients to ask their providers about each of the 4Ms. The brochure details advance directives and POLST documents and when each should be completed and/or used. A flyer was created highlighting exercise, healthcare (home health, nursing home, and hospice), and community resources. Social media posts with snippets from the brochure and flyer were also created to reach a larger audience.
Conclusions: Working with an established and trusted provider in the community like CCPH made engaging with the community a natural process. The target audience for the project is older adults and caregivers in Rawlins. The brochure and flyer will be displayed at CCPH and distributed to outreach programs, senior centers, and other clinics. CCPH’s Facebook page will feature informational posts. Our expectation is that a patient population that is better informed on the Age Friendly framework in Carbon County should see similar positive health outcomes as noted when physicians initiate 4Ms discussions.
#281
THE PREVALENCE OF ANEMIA IN CHILDREN ADMITTED TO THE CHILD MALNUTRITION TREATMENT CENTER IN RURAL INDIA
Thumma M1, Patel N3, Judkins A2, Fassl B1. 1Northeast Ohio Medical University, Rootstown, OH; 2University of Utah, Salt Lake City, UT and 3Shakti Krupa Charitable Trust, Mota Fofalia, India
Purpose of Study: 52 million children below 5 years suffer from malnutrition worldwide. South Asia is home to more than 50% of children affected by severe malnutrition and wasting. Childhood anemia is an indicator of micronutrient deficiency and is associated with poor long-term cognitive, physical, emotional, and social functioning. Interventions commonly address caloric malnutrition but micronutrient deficiencies/anemia are not assessed routinely. Identifying anemia in malnourished children could guide treatment plans and lifelong dietary management. The study objective is to assess the prevalence of anemia in patients admitted for treatment of severe acute malnutrition (SAM) to a Child Malnutrition Treatment Center (CMTC) in Gujarat, India.
Methods Used: This retrospective chart review took place in Mota Fofalia Community Health Center in May 2023 and includes children with SAM treated between 2021-2023. As part of a quality improvement initiative, the medical team included routine hemoglobin measurements and anemia treatment if applicable in addition to providing high-caloric nutritional supplementation. We performed a retrospective analysis on these admission data points to determine anemia prevalence and used WHO diagnostic criteria to classify anemia severity.
Summary of Results: 121 children were admitted to the CMTC between 2021 and 2023. Mean age was 33.85 months (8 - 86mo) and 47% were female. Mean hemoglobin values were 9.80 (range from 2.2 to 14). 9 children were severely anemic (5 female), 59 moderately anemic (27 female), 24 mildly anemic (13 female), and 29 were not anemic (12 female).
Conclusions: Anemia and micronutrient deficiencies are highly prevalent in children with SAM. Routine assessments for micronutrient deficiencies would be beneficial.
#282
PROMOTING WOMEN’S HEALTH SCREENING ON THE BLACKFEET RESERVATION
Tiersma K1, Keys T2. 1University of Washington, School of Medicine, Seattle, WA and 2University of Washington, Seattle, WA
Purpose of Study: Browning, MT is the largest community on the Blackfeet Reservation (total population 7,000). Native Americans face disproportionately high rates of cancer incidence and mortality. On the Blackfeet Reservation, female breast is the second most common cancer. Priorities from a 2017 Blackfeet Community Health Assessment include increasing breast and cervical cancer screening. The aim of this project is to develop tailored health educational material in tandem with a same-day screening initiative to increase awareness and participation in breast and cervical cancer screening on the Blackfeet Reservation.
Methods Used: Community conversations with healthcare workers, organizations, and community members identified priorities for improving women’s health on the Reservation. Using an asset-based lens, existing community strengths and resources were identified to create structure for continuing education. A literature review on tailored health promotion for Native American communities informed the development of the breast and cervical cancer educational material.
Summary of Results: Community conversations identified lack of awareness of screening options, transportation difficulties, and low attendance at yearly women’s health exams as barriers to screening. Community partners include the Montana American Indian Women’s Health Coalition, Blackfeet Community Hospital Women’s Clinic, and Logan Health mobile mammography team. Deliverables to the community are a same-day, no appointment necessary screening pilot hosted at the community hospital in conjunction with community distribution of digital and print educational material on breast and cervical screening.
Conclusions: Incorporating an asset-based framework identified existing community initiatives that were able to be built upon for this project. Next steps include presenting the developed educational material at a community Bingo event for breast cancer awareness.
#283
EFFICACY OF EDUCATIONAL INTERVENTION STRATEGIES TO REDUCE RACIAL AND ETHNIC INEQUITIES IN RISK FACTOR CONTROL AFTER STROKE
Tsang C1, Batongbacal S1, Gulati T1, Lee C1, Li H1, Mitchell N1, Samiullah A1, Afghani B1, 2. 1UC Irvine School of Medicine, Irvine, CA and 2CHOC Hospital of Orange County, Orange, CA
Purpose of Study: Underserved populations, particularly African-American, Hispanic, and Native-American groups experience disproportionately higher morbidity and mortality from stroke. Given the debilitating nature of stroke as well as the racial and ethnic inequities in its prevalence, this literature review seeks to investigate the effectiveness of various interventional educational programs at reducing the risk factors for stroke in marginalized patients with history of stroke.
Methods Used: A literature review was conducted through PubMed, Google Scholar, and Sci-Hub databases using keywords: “disparity”, “stroke”, “education”, “intervention”, “underserved”, “disadvantaged”, “racial”, “ethnic”, and “minority”. Only prospective randomized controlled trials in the USA published after 2015 that measured the effectiveness of preventative stroke strategies among different racial/ethnic groups with a history of transient ischemic attack or mild stroke were included in our literature review.
Summary of Results: A total of six studies (see table) matched the inclusion criteria. Intervention participants typically received an interactive educational video or in-person session before discharge followed by additional appointments and access to health caseworkers to clarify questions about medications and general stroke prevention. The most common outcomes measured included change in systolic blood pressure (SBP) and lab values over the course of the study period. A majority of the studies did not show a significant decrease in SBP when comparing the intervention with the control cohorts 6-12 months after the intervention. In two studies, subgroup analyses of the Hispanic participants found greater reduction of SBP between intervention and standard care (control) groups. Although the primary endpoint of decrease in BP was not achieved in a majority of studies, some programs found improvements in secondary outcomes such as salt intake, and low-density lipoprotein levels. The studies were variable in evaluating the effects of environmental determinants such as economic stability, health insurance, neighborhood walkability safety, and healthy food options.
Conclusions: In summary, although a majority of the studies demonstrated that the systolic blood pressure was lower in both control and intervention groups on follow-up, the interventional strategies failed to show a significant decrease in blood pressure among different races/ethnicities when comparing the control and intervention groups. The studies were limited by the small sample size in the subgroups and the variability in considering in social determinants of health. As the management and prevention of stroke are multifactorial and complex, we believe that larger studies measuring the impact of strategies that address the determinants of health at both the community and individual levels are warranted in developing targeted interventions that are effective in reducing racial and ethnic inequities.
Interventional studies for reducing stroke risk among different ethnic groups.
First Author, Year Published
Age Group & Inclusion Criteria
Description of Study Intervention
Sample Size (n) & Description
Definition of Outcome
Study Results
Boden-Albala, 2018
-Presents with TIA, Ischemic stroke, or Intracerebral hemorrhage
-Age >18 years-New York area resident with phone-One or more vascular risk factors (Hyperlipidemia, Hypertension (HTN), Current smoker, Diabetes mellitus, type 2, Metabolic syndrome)
1) Intervention group: Interactive educational session, patient-paced workbook and video, and follow-up calls 72 hours, 1 month, and 3 months post-discharge
2) Control group: usual care and American Heart Association stroke pamphlets
Intervention group (N=237)
24.8% Non-Hispanic White,
35.6% Non-Hispanic Black,
34.4% Hispanic
Control group (N=241)
30.8% Non-Hispanic White,
31.9% Non-Hispanic Black,
31.9% Hispanic
Systolic blood pressure (SBP) reduction between baseline (at discharge) and 12 months post-discharge
a) In adjusted models, no significant differences in SBP between intervention and control group
b) Sub-analysis of Hispanic intervention vs control participants showed an almost 10 mm greater mean reduction in SBP for the intervention group (Beta of 9.9, 95% CI: 1.8-18.0)
Towfighi, 2021
-Age >40 years old
-Pts who had an ischemic stroke, TIA, or intracerebal hemorrhage within prior 90 days
-SBP >=130 mmHg or 120-130 mmHg if they had a history of HTN or antihypertensive medications prior to stroke or TIA
1) Intervention group: In addition to usual care, were offered 3 advanced practice clinic visits, 3 communtiy health worker home visits, telephone visits, electronic decision support for clincians, BP monitors. Disease Self-Management Program (CDSMP)19 workshops in English and Spanish
2) Control group: recieved usual care
Intervention group (N=241)
70.9% White,
19.0% Black,
6.3% Asian,
2.1% Native- American/Alaskan native, 1.7% Other race Hispanic = 70.5%
Control group (N=246)
69.9% White,
17.6% Black,
6.3% Asian,
1.7% Native American/Alaskan Native,
6.3% Other race Hispanic = 72%
Primary outcome was change in mean SBP at 12 months
Secondary outcomes: mean change in systolic BP, control of other vascular risk factors, and behaviors
-No differences in the mean SBP improvement nor in the proportion achieving SBP control across arms
-From baseline to 12 months, mean SBP improved from 143 mm Hg to 133 mm Hg among participants in the intervention group and from 146 mm Hg to 137 mm Hg among participants in the usual care group-Compared to the control, the intervention group had more improvements in self-reported salt intake (P=0.004) and serum CRP level (P=0.003)
Cheng, 2018
-English or Spanish speaking
-TIA or ischemic stroke within 90 days prior-Mean SBP >= 120 mmHg
1) Intervention group: Attend group clinics, 5 clinic visits during 10 month period and scheduled calls from case managers once a month
2) Control group: usual care
Primary outcome was change in SBP
The secondary outcomes were low-density lipoprotein reduction, antithrombotic medication use, smoking cessation, and physical activity. Outcomes were measured 3 months, 8 months (by phone), and 12 months
a) Overall, the between-arm difference was not significant (-3.6 mm; 95% confidence interval, −9.2 to 2.2)
b) Mean baseline SBP was 150 mm in both arms. SBP decreased by 17 mm in the intervention arm and 14 mm in the usual care arm
c) Among secondary outcomes, persons in the intervention arm were significantly more likely to lower their LDL
Boden-Albala, 2019
-At least one of the following diagnoses: TIA, ischemic stroke, or intracerebral hemorrhage
- Age >18
- Have at least one of the following vascular risk factors: HLD, HTN, current smoker, DM2, or metabolic syndrome.
1) Intervention group: interactive educational session with a community health coordinator prior to discharge; received a patient-paced workbook, and follow-up calls from a coordinator at 72 hours, 1 month (typically immediately prior to neurology appointment), and 3 months to enhance strategies for patient-physician communication, behavior change, clarify medication regimen
2) Control group: usual care and received standard stroke treatment as well as AHA stroke pamphlets in English or Spanish.
Intervention group (N=274)
24.8% Non-Hispanic White,
35.6% Non-Hispanic black,
34.4% Hispanic
Control group (N=278)
30.8% Non-Hispanic White,
31.9% Non-Hispanic Black,
31.9% Hispanic
Primary outcome was difference in SBP reduction between the intervention and usual care groups.
-No significant difference in systolic blood pressure reduction between the intervention and usual care groups following one year after the start of the study.
-Hispanic participants within the intervention group demonstrated a clinically and statistically significant mean systolic blood pressure reduction that was 9.9 mmHg greater than the usual care group, (P<0.05)
- There were no clear differences between individuals amongst non-Hispanic white (β = 3.3; 95% CI, -4.1 to 10.7) and non-Hispanic black participants (β = -1.6; 95% CI, -10.1 to 6.8).
Goldmann, 2020
-Presents with TIA, Ischemic stroke, or Intracerebral hemorrhage
-Age >18 years-New York area resident with phone-One or more vascular risk factors (Hyperlipidemia, Hypertension, Current smoker, Diabetes mellitus, type 2, Metabolic syndrome)
-Can participate in educational sessions in English or Spanish
1) Intervention group: interactive educational session with a community health coordinator prior to discharge; received a patient-paced workbook prior to discharge, and follow-up calls from a coordinator to enhance strategies for patient-physician communication, clarify medication regimen
2) Control group: usual care and received tandard stroke pamphlets in English or Spanish from the AHA
Intervention group (N=237)
24.8% Non-Hispanic White,
35.6% Non-Hispanic Black,
34.4% Hispanic
Control group (N=241)
30.8% Non-Hispanic White,
31.9% Non-Hispanic Black,
31.9% Hispanic
Primary outcome was the association between SBP reduction at 12 month follow up and self efficacy (perception of protecting themselves against stroke)
Mean SBP reduction was significantly greater among those with self efficacy versus those without (7.8 versus 1.2 mm Hg; P=0.015)-For all subgroups, mean SBP reduction was greater among those with self efficacy compared with those without. Stronger association between self efficacy and SBP reduction was found in the usual care versus intervention trial arm
Feldman, 2020
-First-time or recurrent stroke or transient ischemic attack at any point prior to enrollment
-Uncontrolled SBP at the time of enrollment
-Self-identification as Hispanic and/or Black
1) UHC group: physician-ordered plan of care
2) UHC + NP: UHC and 30-day transitional care program with 3 in-home visits and 3 patient/caregiver telephone contacts
3) UHC + NP + HC: UHC + NP + 60 days of coaching/self-management support from a home health aide specially trained to be a health coach. The HC protocol added 3 in-home visits and 3 telephone contacts beyond the 30-day NP intervention
Primary outcome was change in SBP from baseline to 3 and 12 months
The three groups were not significantly different at each time point
-Virtually all SBP reductions occurred between baseline and the 3-month follow-up but were sustained at the 12-month follow-up.
TIA=Transient Ischemic Attack, UHC=Usual Home Care, NP=Nurse Practitioner, HC=Health Coach, LDL=Low Density Lipoprotein, CI=Confidence Interval, CRP= C Reactive Protein.
#284
ASSESSING THE EFFECTIVENESS OF A DIABETES EDUCATIONAL PROGRAM ON COMMUNITY HEALTH PROMOTERS’ SELF-RATED UNDERSTANDING OF THE DISEASE IN NAIVASHA, KENYA
Yip K1, Bosibori D2, 3. 1University of Washington School of Medicine, Seattle, WA; 2Naivasha County Referral Hospital, Naivasha, Kenya and 3University of Washington School of Pharmacy, Seattle, WA
Purpose of Study: Kenya, and other low- and middle-income countries, are in the middle of the second epidemiological transition marked by a shift in the mortality rate and burden of disease from infectious diseases to non-communicable diseases (NCDs). Community Health Promoters (CHPs) are trained members of the community that are first-line in providing basic health services and linking community members with formal healthcare. They have a broad scope of practice and knowledge around factors influencing health, but lack training on specific NCDs, such as diabetes. As a result, limitations exist in their capacity to promote community understanding of the disease and improve its health outcomes. The aim of this study is to assess the effectiveness of a diabetes educational program given to CHPs to increase their capacity to both educate others and identify/refer suspected cases among community members. We hypothesize that there will be a significant difference between CHP self-rated knowledge after the intervention is given.
Methods Used: Participants were from a convenience sample of CHPs (N=17) that attended the planned educational meeting at the Naivasha County Referral Hospital (NCRH). CHPs were given a pre-test survey that consisted of seven questions asking them to evaluate their self-rated knowledge from “Strongly Disagree” coded as (1) to “Strongly Agree” coded as (5) on diabetes prevention, risk factors, signs and symptoms, complications, and a health center referral protocol that I created. Participants were then given an educational session on the above objectives. Afterwards, an identical post-test survey was administered to re-evaluate their self-rated knowledge on the same objectives. A paired sample t-test was used to compare the pre and post-test results. All educational materials including the PowerPoint presentation, pamphlets, and screening/referral checklists were given to the Nakuru County Department of Health Services for further distribution and future use in the community.
Summary of Results: Quantitative analysis indicated that the CHPs’ self-rated understanding of the diabetes objectives after receiving the educational session (M=4.91, SD=0.07) were significantly higher than before the educational session (M=4.07, SD=0.09) with t(6)=2.447, p=<0.001. Qualitatively, representatives from the NCRH board and Nakuru County Department of Health present at the meeting gave positive feedback and expressed a desire for similar educational programs for other diseases in the future.
Conclusions: This project increased CHPs’ understanding of diabetes, capacity to educate fellow community members, and how to identify/when to refer suspected cases. Further educational initiatives on specific disease conditions can be an effective way to increase community understanding of diseases and reduce their burden on healthcare systems by emphasizing prevention and avoiding complications.
#285
SOCIAL MEDIA AND ITS IMPACT ON KNOWLEDGE REGARDING ORAL CONTRACEPTION
Yu VJ, Southard R, Nelson A. Western University of Health Sciences, College of Osteopathic Medicine of the Pacific, Pomona, CA
Purpose of Study: Social media has made it easy to connect with not only friends and family, but also with influential figures and brands. Although it has become increasingly popular for medical professionals to be seen on social media doing their best to educate the public about health and medicine, it is not clear how effective it is in correcting the large amount of misinformation online. Online testimonials about the effectiveness, side effects, and safety of birth control pills from other women, especially celebrities, can greatly influence both the behavior and medical decisions they make. This study attempted to characterize social media platforms and usage for women’s reproductive health and any association with users’ knowledge about oral contraception.
Methods Used: This IRB-approved, anonymous study asked English-speaking, female followers of two of the authors’ (VY, RS) large platforms on Instagram and YouTube 14 questions about their social media usage and application, specifically the top three reasons they used it. We collected demographic information and personal experiences with hormonal contraception. It then asked for agreement on a 5-point Likert scale assessing women’s oral contraception knowledge and the sources of that knowledge with 4 factual and 4 nonfactual statements about pills. The sources of information were compared between subjects who got ≤ 2 questions correct, ≥ 2 and ≤ 5 correct, and ≥ 5 correct.
Summary of Results: 2054 women responded. The majority (72.3%) were 25 years old or younger; 57.6% were Caucasian; 67.5% had at least college degrees. Nearly 50% were students; the remainder were employed. Incomes were well distributed. The leading reason subjects used social media (26.2%) was to connect with friends and family; 25.1% to pass time by viewing funny articles, memes, or videos; 13.2% to follow up on trending news and gossip; 12.9% to connect with influential figures. Two-thirds had used oral contraceptives but nearly 80% reported they would search online prior to filling a prescription. The average correct score was 4 out of 8 questions. Most frequently missed questions were related to mood disorders, weight gain, and infertility. Comparing those who had ≤ 2 questions correct (42.3%), ≥ 2 and ≤ 5 correct (46.6%), and ≥ 5 correct (11.1%), 56.6% of low scorers acquired information from friends and social media; only 43.4% of medium and high scorers combined relied on those sources. Duration of daily social media exposure did not affect scores.
Conclusions: This survey of young, highly educated, frequent consumers of social media harbored many myths about oral contraceptive use, often originating from friends and social media sources. Understanding how these online platforms may influence women’s perceptions and attitudes toward their reproductive health may assist providers in addressing common online misconceptions with their patients.
#286
MODEL FOR INTEGRATING OPIOID USE DISORDER AND OVERDOSE PREVENTION TRAINING INTO MEDICAL SCHOOL EDUCATION
Yusuf F, Sharma A, Crosswhite B, Giuliani D, Abusham T, Dean A, Ibarra F. California Health Sciences College of Osteopathic Medicine, Clovis, CA
Purpose of Study: Due to increasing rates of opioid use disorder diagnoses and opioid overdose-related deaths, medical education must adapt to better treat these conditions. Integrating skill workshops and didactic lessons related to these disorders into medical school programs may facilitate the early development of these skills in future physicians. California Health Sciences University College of Osteopathic Medicine’s (CHSU-COM) Overdose Prevention Task Force (OPTF) proposes a model for managing opioid use disorder and leading community-centered initiatives as an educational reference for other institutions undergoing the creation or revision of their own substance use programs and curricula.
Methods Used: CHSU-COM’s OPTF was established in 2021 as part of a resolution passed in 2019 by the National Student Osteopathic Medical Association (SOMA). Once established, the chair recruited an assistant professor experienced in preventing and managing opioid use disorder and opioid-related overdoses to serve as their advisor and create interprofessional connections. OPTF contacted the county’s public health director and other local leaders to collaborate further and implement change. The organization then created the following subcommittees with their own respective chairs and focus areas: internal events/education, interprofessional programs, and research.
Summary of Results: OPTF’s first event was led by the county’s public health director and provided naloxone training to 80 CHSU medical students who voluntarily participated. The naloxone training event was followed by two high school outreach events that attracted over 300 students, where OPTF members provided naloxone training and information on medical careers. The OPTF chair collaborated with the CHSU school board to stock naloxone in campus first aid kits and created a policy for storing, administering, and tracking its usage. The internal events/education subcommittee organized substance use education discussions for students to learn from experts living with and treating opioid use disorder to supplement the school’s curriculum. Through an OPTF-led initiative, group members worked alongside the school’s basic life support curriculum to provide overdose response training to 167 first-year medical students. Following the removal of the X-Waiver, OPTF organized a continuing medical education event alongside the county’s medical society that was attended by over 200 prescribers to review medication assisted treatment options and substance use challenges encountered in the Central Valley.
Conclusions: CHSU COM’s student-led model exemplifies the expanded role of medical students in educating and managing opioid use disorder and opioid overdose-related deaths. OPTF’s initiatives provide an effective framework for other institutions to refer to when integrating overdose prevention, naloxone administration, and harm reduction into their school’s medical education.
#287
PUIPUIA LE OLA: COVID-19 DATA DISSEMINATION WITH PACIFIC ISLANDER COMMUNITIES IN HAWAI’I
Yuzon NO1, 2, Ching JN1, Sy A1, Nicholas C1, Tauasosi-Posiulai T1, Aoki J1, Yanagihara R1. 1John A. Burns School of Medicine, University of Hawai’i at Mānoa, Honolulu, HI and 2Western University of Health Sciences, College of Osteopathic Medicine of the Pacific-Northwest, Lebanon, OR
Purpose of Study: Pacific Islanders (PI) are overrepresented in COVID-19 cases, hospitalizations, and mortality in Hawai’i. Puipuia le Ola (Protecting Life) funded by the National Institutes of Health’s Rapid Acceleration of Diagnostics-Underserved Populations aimed to promote COVID-19 testing among PIs. This study aims to describe culturally and linguistically suitable dissemination of project results to convey and discuss study findings with PI communities in Hawai’i.
Methods Used: Community dissemination methods comprised of data walks, PowerPoints, infographics, contact cards, and audience incentives were reviewed to ensure data accuracy, cultural and linguistic suitability, and comprehension by the project’s PI staff. The field team worked with their communities to conduct dissemination at churches, academic institutions, or Zoom. Preparation for dissemination events involved collaboration with the staff to discuss event logistics, tailor PI audience-specific results, and rehearse scripted simulated presentations. Presentations concluded with a “talk story” enabling attendees to engage with the staff presenters about study findings.
Summary of Results: To date, >250 PIs attended 8 of the dissemination events. Attendees appreciated small gifts (tote bags, cosmetics, toys, pens, t-shirts). PowerPoints were cost-efficient and most effective for generating audience-specific data visualizations for all ages in a timely manner. Dissemination resulted in attendees recounting personal COVID-19 experiences and shared sentiments to protect their communities during the “talk story” of the PowerPoint presentations.
Conclusions: In-person and virtual scripted and rehearsed PowerPoint presentations to audience groups engaged PI participants in conveying study findings to their communities. Culturally and linguistically tailored dissemination fosters trust with hard-to-reach populations to likely continue beyond the COVID-19 pandemic.
Digital image of Puipuia le Ola RADx-UP data walk board for the Pacific Islander community at the Micronesia Festival and Republic of the Marshall Islands Constitution Day in O’ahu, HI May 2023.
#288
SEASONALITY OF SURGICAL SITE INFECTION RATES ACROSS A HEALTH SYSTEM
Anioke T2, Fei Y1, 2, Colborn K2, 1, Stuart CM2, Bronsert MR2, 3, Henderson W2, 3, Healy GL2, Dyas A2, Meguid R2, 3. 1University of Colorado Denver, Aurora, CO; 2University of Colorado Denver, Aurora, CO and 3University of Colorado Denver, Aurora, CO
Purpose of Study: Surgical Site Infections (SSIs) are one of the most frequent and costly post-operative complications. Although there are studies investigating the seasonality of SSIs, most use methods that do not adequately account for confounding factors or the non-parametric nature of seasonal trends. While some studies attribute this seasonality to the “July effect” of new resident house staff, others believe it is related to increased body flora at high temperatures during the summer months. This study aimed to explore SSI rates from various surgeries performed at different hospitals within the same system, varying in degree of trainee involvement using novel artificial intelligence methods on electronic health record (EHR) data.
Methods Used: We analyzed 352,074 surgeries performed across the University of Colorado Health System from 2014 to 2019 using the EHR. Individual preoperative risk and postoperative probabilities of SSIs were estimated using the Automated Surveillance of Postoperative Infections (ASPIN) models previously published by our team. We estimated complication rates, preoperative risk of complications, and observed/expected (O/E) ratios. These values were plotted by week, and cubic smoothing splines were used to visualize trends (figure 1). Seasonality was modeled using generalized linear mixed models with sine and cosine transformations of the week of the year or quadratic transformations as predictors, depending on the observed trends. Fitted values from these models were compared to the splines (figure 1).
Summary of Results: More SSIs were seen between July and August. Preoperative risk also increased around July but not significantly. The risk-adjusted O/E ratio and postoperative probabilities of SSIs showed a significant increase during the summer months compared to the winter (P <0.01).
Conclusions: Our study supports prior work suggesting a significant peak in SSIs during the summer but not a specific spike in July, which would be associated with a change in house staff. This study incorporated novel application of artificial intelligence methods to predict preoperative risk and postoperative probability of SSI, and showed that even after adjustment, the O/E ratios significantly increased between these months. Further research is needed to understand this increase beyond what would be expected, given the patient risk factors.
#289
DATA DISPLAYS: ASSESSING METHODS OF SHARING QUALITY OF LIFE CHANGES WITH BREAST CANCER PATIENTS
Annest G1, Helmkamp L2, Vemuru S3, Adams M2, Huey M3, Scherer L4, Baurle E5, Matlock D6, Kim S3, 7, Lee C8, Tevis S3. 1University of Colorado, Aurora, CO; 2University of Colorado Anschutz Medical Center, Aurora, CO; 3University of Colorado Anschutz Medical Center, Aurora, CO; 4University of Colorado Anschutz Medical Center, Aurora, CO; 5University of Colorado Anschutz Medical Center, Aurora, CO; 6University of Colorado Anschutz Medical Center, Aurora, CO; 7University of Colorado Anschutz Medical Center, Aurora, CO and 8University of North Carolina at Chapel Hill, Chapel Hill, NC
Purpose of Study: Patients with early-stage breast cancer have equivalent survival outcomes after mastectomy (MX) or lumpectomy (BCT). To aid in decision making, surgeons review oncologic outcomes, potential adjuvant therapies, immediate post-op recovery, and reconstruction. Notably, expected post-operative quality of life (QoL) is not routinely discussed, and little is known about how patients interpret QoL information. Patient reported outcomes (PROs) from survivors provide valuable insight on QoL changes over treatment. This study aims to determine the best method for sharing surgical outcome PROs with patients to maximize post-surgical QoL according to patient values.
Methods Used: We created six visual displays of QoL changes following BCT (figure 1) based on PRO data from the BREAST-Q survey. Of 285 eligible patients diagnosed with Stage 0-IIIV breast cancer seen in surgical consultation from June 2019-June 2022, 40 (mean age 54.6 years) consented to the study. Patients ranked PRO displays and provided open-ended comments on figure preferences. Demographic and cancer variables were accessed via EMR. Figure rankings were compared using means, standard deviations, and one-way ANOVA. Differences in rankings by demographic and cancer variables were assessed by generalized linear models with interaction between figure option and variable of interest. Theme analysis was conducted on open-ended responses.
Summary of Results: One way ANOVA revealed statistically significant differences in first choice ranking among the six figures with p < 0.0001. [AM1] Figures 2, 4, and 5 were ranked best; 1 and 6 were ranked worst. [HM2] There was noNo differences were found between rankings and demographic or cancer variables, including race, ethnicity, education, income, or surgery type. Patients favored figure simplicity, reading ease, and inclusion of timepoints over recovery. Patients disliked images for either not having enough detail or an overwhelming volume of information.
Conclusions: Preliminary findings show that no single display is best for counseling patients on QoL choices. Data displays that prioritize clarity and QoL changes over time are strongly preferred by patients. D, while displays with large amounts of information may be overwhelming and counterproductive. Future work aims to identify variation with a diverse population. Findings provide guidance for counseling patients on expected post-operative QoL, expectation setting, and improved shared decision making.
#290
Consequences of Increasing Border Wall Height: A Retrospective Study
Azad S2, 1, McCague A1, Henken-Siefken A1. 1Deser Regional Medical Center, Palm Springs, CA and 2Western University of Health Sciences College of Osteopathic Medicine - Pacific Northwest, Lebanon, OR
Purpose of Study: Our retrospective cohort study focuses on the differences in the severity of injuries sustained from border wall falls before and after wall height increase. Severity of injuries is categorized by injury severity score (ISS), length of stay in the hospital (LOS), ventilation, ICU and surgery. The purpose of this study is to underline the medical consequences of extending the US-Mexico border wall. Specifically, we focused on the severity of injuries that are seen in trauma centers near the US-Mexico border. We propose that the rise in trauma cases from the border wall is associated with the extension of the border wall.
Methods Used: In this IRB approved retrospective cohort study, patients were assigned to Pre-2020 or Post-2020 subgroups, based on time of admission. Total number of admissions, ISS, LOS, surgeries, ventilation and ICU services were compared. We defined the pre-wall and post-wall time frame as beginning of 2020, as December 2019 was when the border wall height had been fully extended. The patients were separated by admission date with 22 that were admitted before January 2020 and 86 admitted after January 2020. Data was collected on Injury Severity Score (ISS) from the deidentified data base. Statistical analysis was complete with Microsoft Excel™ (Seattle, WA). All tests were 2-sided with a = 0.05. The continuous variables were compared using the independent samples t-test. We analyzed the ISS score in patients admitted before 2020 and compared them to the patients admitted after 2020. We also assessed LOS, days spent in ICU and days on ventilation between the two groups and found a p-value. To assess the statistical significance to determine how many patients required surgery, we gave a numerical value of “0” to those who did not receive the service and “1” for those who received the service. We did all of the calculations from the data using Microsoft Excel™ (Seattle, WA).
Summary of Results: Injuries from border wall falls grew 1250% from 2016 to 2021 (4 vs 50 admissions). When comparing the two subgroups, hospital admissions (20 vs 84) and injury severity score (9 vs 15) have also risen dramatically. Of all the variables compared, the days spent in the ICU proved to be statistically significant at a p-value of 0.02. According to the US Customs and border protection, there was a 4-fold increase in the number of migrants that crossed the border from 2016 and 2021. This increase in the volume of migrants 2021 may also have led to an increase in falls, and is noted as a limitation of our study. Although the remaining data was not statistically significant, there still remains a trend of increasing injuries that are also more severe in presentation, requiring more interventions.
Conclusions: The increase in border height has led to a record high number of admissions and severity of injuries. This study shows that increasing the border wall height has led to a public health crisis and underlines the profound impact that political decisions have in the medical field.
#291
AN ANALYSIS OF PUBLICATION TRAJECTORY OF CANADIAN PLASTIC SURGEONS ACROSS DECADES OF PRACTICE
Buchel T1, Banyi N2, Tuen Y3, Shayan S3, Courtemanche R3, Arneja J3, 4. 1The University of British Columbia, Vancouver, BC, Canada; 2the University of British Columbia, Vancouver, BC, Canada; 3BC Children’s Hospital, Vancouver, BC, Canada and 4the University of British Columbia, Vancouver, BC, Canada
Purpose of Study: Academic surgeons’ publication trajectories may vary from the traditional curve, which showcases an initial surge in publications followed by a plateau, possibly due to the modern emphasis on rapid career development in competitive programs. Given this understanding, this study aims to identify trends in research productivity among Canadian academic plastic surgeons, grouped by their respective decades of practice. Secondary objectives include exploring authorship order, factors influencing productivity, and research impact by decade of practice.
Methods Used: A list of all Canadian academic plastic surgeons was gathered from university websites and confirmed with a contact from each center. Publications were searched in the Web of Science and PubMed databases in July 2023. A list of the articles was compiled, capturing the author’s name, year of medical school graduation, sex, position in the article, title, journal of publication, publication year, and citation count. The start of the educational decade was defined as 4 years prior to medical school graduation date. Accuracy was ensured by using two independent reviewers to cross-reference each article with the appropriate surgeon and affiliation. Descriptive statistics and appropriate parametric and nonparametric tests were used.
Summary of Results: 3498 publications were identified for 246 surgeons (72% male). The preliminary data considers 206 of the 246 plastic surgeons. The median current decade of practice was 2 (95% CI 0.9, 5.0) decades following the educational decade. The average total number of publications per surgeon was 15.5 (95% CI 0.0, 53.3), with a mean citation per paper count of 21.9 (95% CI 0.0, 64.2). The median number of publications in the educational decade, decade 1, decade 2, decade 3, decade 4, and decade 5 were 0 (IQR = 0), 0 (IQR = 2), 2 (IQR = 6.75), 1 (IQR = 6), 2 (IQR = 10), 2 (IQR = 6.25), respectively. The 206 surgeons were found to be in the following decades of practice: 1st decade (n=206), 2nd decade (n=206), 3rd decade (n=145), 4th decade (n=85), 5th decade (n=48). The average proportion of first authors in the educational decade, decade 1, decade 2, decade 3, decade 4, and decade 5 was 0.57, 0.43, 0.27, 0.11, 0.11, and 0.09, respectively. The average proportion of last authors in the educational decade, decade 1, decade 2, decade 3, decade 4, and decade 5 was 0.14, 0.05, 0.26, 0.43, 0.42, and 0.40, respectively.
Conclusions: As surgeons progress through their careers, an increase in variability in research productivity is seen, with the most pronounced variability occurring in the fourth decade of practice. Furthermore, the proportion of first authors tends to be higher in earlier decades of practice, with the highest proportion of first authors being in the educational decade. The proportion of last authors tends to be higher in the later decades of practice, peaking in the third decade and remaining relatively stable thereafter.
#292
Unveiling the Clinical Response to Platelet-Rich Plasma in Knee Osteoarthritis
Constantine E1, Williams K1, Whitney K2, McCarrick-Walmsley R2, Fry SA1, Dragoo J2, 1. 1University of Colorado School of Medicine, Aurora, CO and 2UC Health Steadman Hawkins Clinic, Denver, CO
Purpose of Study: Leukocyte-poor platelet-rich-plasma (LP-PRP) is an autologous biologic that decreases pain in knee osteoarthritis (KOA). Current PRP literature lacks power to drive clinical decisions, due to poor preparation standardization and mechanistic uncertainty. This study identifies demographic factors and molecular components of LP-PRP that influence better PROMIS Pain and Function outcomes.
Methods Used: This retrospective cohort study used de-identified data from 45 patients ages 30 - 85 with KOA (KL grades I - IV) and symptomatic knee pain treated with a single, intra-articular PRP injection. Of the 45 patients, there were 58 cases (n=58 knees), 34 of which had adequate PRP for molecular analysis. 13 patients bilateral injections (n=26 knees), 32 were unilateral. There were 18 cases with PROMIS Pain and Function scores collected at baseline and 3-months following LP-PRP. The delta change between baseline and 3-month PROMIS Pain and Function scores were calculated with an MCID threshold of 10-points, those with 10% difference from baseline were defined as responders. Multiplex Human XL Cytokine 46-plex Luminex assay measured protein concentrations. For each injection, blood from patient’s arm was spun down in a centrifuge, LP- PRP was injected into the supralateral aspect of knee. Statistics performed using Wilcoxon-Ranked Test and t-test. P<0.05 determined significance.
Summary of Results: Of the 58 cases, 27 had OA grades I-II, and 31 had III-IV. BMI ranged from 17 to 42 (mean 26.8). 38 cases reported chronic injuries, while 16 were acute. Of the 18 patients with follow-up scores, there was a significant difference in PROMIS Pain between baseline and 3-months post LP-PRP (baseline: 55.0 ± 6.3, 3-month: 61.6 ± 7.2, p<0.05). Of completed cases, 8 subjects were positive responders at 3-months post LP-PRP compared to baseline (mean: 12.9% ± 8.4), while 2 subjects responded negatively (mean: -6.7% ± 5.2) (Fig.1A). Molecular factors were detectable in 8 positive and 2 negative responders(Fig.1B), there was a significant increase in GCSF (mean = 37.8 ± 9.48, p = 0.03), IL-12 (mean = 24.5 ± 11.3, p = 0.03), and IL-1b (mean = 4.5± 1.55, p = 0.004) compared to non-responders (Fig.1C). GCSF positively correlated with RANTES (ρ=0.71) and PDGF AB/BB (ρ=0.74). IL-1b positively correlated with IL-13 (ρ=0.77).
Conclusions: Key findings were a significant reduction in PROMIS Pain following LP-PRP and the significant increase in GCSF, IL-1b, and IL-12 in positive responders. Further investigation can determine the association between these markers in KOA. Limitations include donor heterogeneity and limited follow-up. Analysis of the responder LP-PRP will further personalize and improve KOA treatment efficacy.
#293
RETURNING TO GOLF FOLLOWING SPINE SURGERY: PRELIMINARY RESULTS
Cooper K2, Bansal A1, Nemani V1, 3, Louie PK1, 3. 1Virginia Mason Franciscan Health, Seattle, WA; 2University of Washington School of Medicine, Seattle, WA and 3University of Washington, Seattle, WA
Purpose of Study: Despite the high prevalence of spinal injuries that occur within the golfing population, little information exists in the literature on when and how to safely return golfers to play following a spinal operation. The purpose of this study is to gain a deeper understanding of when players can return to golf across various levels following spine surgery. Secondarily, the data obtained in this study can help establish benchmarks related to ability to return to golf after these procedures.
Methods Used: All patients between 18-89 years old that played at least one 18-hole round of golf per year and underwent a cervical or lumbar laminectomy or microdiscectomy, 1-level lumbar fusion, cervical disc replacement, or anterior cervical discectomy and fusion between January 2019 and July 2023 were eligible for this study. They completed an electronic questionnaire that retrospectively assessed varying aspects of the patient’s golf game, such as club distances, handicaps, and symptomology during 9- and 18-hole rounds of golf, before and after their operation [PL1] . Paired two sample t-tests were used to evaluate the difference in average, self-reported, club distances (yards) between pre-injury and 6 months post-operation as well as between pre-injury and 12+ months post-operation distances for the wedge, 7 iron, 5 iron, and 3 wood golf clubs.
Summary of Results: To date, 8 patients have completed the study. 4 underwent lumbar fusions, 3 laminectomies, and 1 a microdiscectomy. The average age of enrollee was 64.25 years (range, 51-78). 7 were male and 1 was female. All respondents completed the survey 12 or more months post-operation. 75% (n=6) of golfers returned to golfing 9 holes on average between 5-7 months post-operation and 62.5% (n=5) of golfers returned to golfing 18 holes on average 5.8-7.8 months post-operation. 25% (n=2) of participants who were greater than 12 months post-operation had not returned to golfing on a course at all. Table 1 illustrates the average changes in club distances over time. General trends indicate a near complete recovery of ability to hit the golf ball by 12+ months post-operation, however, none of these changes were statistically significant.
Conclusions: Early results show that the majority of golfers, independent of spinal operation type, return to playing 18 holes between 5.8-7.8 months and regain near pre-injury levels of club distance performance at 12+ months post-operation. Low sample size is a limitation of this preliminary data. More time and data collection within this on-going investigation will help better discern whether the timing of this return to play is safe and how these golf-game metrics differ based on type of spinal operation the golfer had.
Average Club Distances.
Club Type
Pre-injury club distance (yards)
6-month post-operation club distance (yards)
12+ months post-operation club distance (yards)
Wedge (n=6)
90.83
87.5
93.3
7 iron (n=5)
145.6
139
144.6
3 iron (n=5)
167.4
158
165
3 wood (n=5)
209
192
207
#294
Missed Diagnosis of a Rare Retro-patellar Juxta-Articular Angioleiomyoma: A Case Report
Case Report: A 42-year-old female patient presented to our clinic with a history of chronic right anterior knee pain persisting for approximately 5 years. Initially, the pain was sporadic and non-specific. However, the patient reported having trouble while climbing stairs and kneeling due to pain. She localized the pain just above the tibial tubercle and described it as being aggravated by light touch. The patient denied any history of trauma. She mentioned that she had undergone arthroscopic knee surgery twice in 2019 and 2021 for the same chief complaint, without resolution of symptoms.
On physical examination, full extension of the knee joint was observed, but active flexion was limited (-30 degrees) due to pain. No noticeable swelling or redness was observed around the knee joint. Light touch palpation elicited tenderness in the area just above the tibial tuberosity. Furthermore, there were no signs of muscle atrophy, typical indications of meniscus lesions, or any evidence of ligament injuries.
The knee MRI image obtained prior to the patient’s initial knee arthroscopy surgery and the current knee MRI image were meticulously examined and compared. In both MRI scans, a distinct and well-circumscribed lesion was identified in the retro-patellar juxta-articular region. Plain orthogonal radiographs of the knee did not reveal any abnormalities in the bone or soft tissue (figure 1). The lesion appeared hyperintense on T2-weighted images and hypointense on T1-weighted images (Figure 2). Based on these diagnostic findings, the decision was made to proceed with surgery. Due to the previous unsuccessful arthroscopic surgeries and the challenges associated with completely excising the lesion using an arthroscopic approach, the patient underwent open surgery (Figure 3).
As revealed in the pathology report, macroscopically the specimen appeared as a medium-hard, nodular material with a smooth surface. It measured 2x1x0.5 cm and had a solid, off-white whorled appearance on the cross-sectional cut. Microscopically, the lesion was well-defined and characterized by intersecting fascicles of spindle cells with uniform cigar-shaped nuclei. Immunohistochemical analysis reveals positive staining of these cells for smooth muscle markers including Desmin, Sooth Muscle Actin, Caldesmon, and Calponin. Microscopic findings reveal that the tumor comprises numerous blood vessels (hematoxylin and eosin, x20, x40). The final diagnosis was a benign angioleiomyoma with clean margins free of cellular atypia.
#295
Effectiveness of Arthroscopic Debridement, Trapeziectomy, and Joint Replacement for Thumb Basal Joint Osteoarthritis: A Meta-analysis of Pre and Postoperative Pain Scores
Golovachev N, Sarli NM, Xavier J, Ghayyad K, Kachooei A. AdventHealth, Rothman Orthopaedic Institute, Orlando, FL
Purpose of Study: The landscape of surgical treatments for thumb basal joint osteoarthritis (TBJO) showcases three notable procedures: arthroscopic debridement (AD), trapeziectomy (TRAP), and joint replacement (JR). Beyond mere pain mitigation, these surgeries aim to uplift patients’ quality of life. While their individual efficacies are often debated, this study offers a meta-analysis diving into the pain management capabilities of AD, TRAP, and JR for those with TBJO.
Methods Used: In compliance with PRISMA guidelines, we conducted a thorough search across PubMed, Cochrane, Embase, and Medline databases. The endpoint was pain relief, measured via the visual analog scale (VAS) pre- and post-surgery. Selection criteria excluded studies from Q3 or Q4 journals and prioritized those with a follow-up period exceeding 6 months.
Summary of Results: Our comprehensive review resulted in 18 articles published between 2010 and 2023. 763 patients had undergone one of three procedures: AD, with 76 patients (10%); TRAP, with 442 patients (58%); or JR, with 245 patients (32%). The studies collectively had a follow-up duration averaging 38 ± 28 months and distinguished 25 distinct treatment groups: AD had 4, TRAP 14, and JR 7. Initial pain, measured using the VAS, averaged 6.7 ± 1.7, while postoperative scores significantly decreased to an average of 1.7 ± 1.3 across all groups (P<0.001).
Delving into the procedures individually, AD’s preoperative pain score averaged at 5.6 (95%CI, 3.5-7.8, P<0.01), TRAP’s at 6.6 (95%CI, 5.8-7.4, P<0.01), and JR’s at 7.7 (95%CI, 7.0-8.5, P<0.01). However, these differences were not statistically significant (P=0.09). Postoperatively, pain scores settled at 1.2 (95%CI, 0.1-2.3, P<0.01) for AD, 1.7 (95%CI, 1.1-2.3, P<0.01) for TRAP, and 1.7 (95%CI, 0.3-3.1, P<0.01) for JR, all showcasing comparable outcomes (P=0.73).
Conclusions: AD, TRAP, and JR demonstrated significant potential in alleviating pain for TBJO. Despite variations in initial pain levels, post-surgical relief was uniformly pronounced across the procedures.
Forest Plot of Pre-Op (Top) and Post-Op (Bottom) VAS Scores after Arthroscopic Debridement, Trapeziectomy, or Joint Replacement for Thumb Basal Joint Osteoarthritis.
#296
UNDERSTANDING RISK FACTORS FOR POSITIVE KIDNEY STONE CULTURES AND IMPLICATIONS UPON SURGICAL OUTCOMES
Hanessian KA, Crew R, Sajdak G, Farkouh A, Song S, Okhunov Z, Baldwin D. Loma Linda University, Loma Linda, CA
Purpose of Study: Positive kidney stone cultures are associated with risk of postoperative sepsis and infectious complications. There has been limited information predicting positive stone cultures and determining the effects of these cultures upon outcomes. The purpose of this study was to investigate factors associated with positive stone cultures and the effect upon outcomes.
Methods Used: A retrospective review was performed on 197 patients with stone cultures who underwent percutaneous nephrolithotomy (PCNL) at a single academic institution between 2017 and 2023. Data collection encompassed patient demographics, medical history, laboratory findings, operative details, and postoperative complications. A comparative analysis was performed between positive and negative stone cultures to detect potential associated variables and outcomes. Statistical methods used were Chi Square for categorical variables and Mann Whitney U test for continuous variables. Significance was defined as p<0.05.
Summary of Results: Of the 197 patients who obtained stone cultures, 111 were positive. Patients with positive stone cultures were more likely to be female (61% vs 42%; p=0.007) and have preoperative Foley catheters (12% vs 4%; p=0.036), ureteral stents (20% vs 7%; p=0.010), and nephrostomy tubes (26% vs 7%; p<0.001). Those who had stone cultures were more likely to have higher positive urinary tract infection indicators on preoperative urinalysis (UA), including urine white blood cell counts (WBC), higher pH, leukocytes, nitrites, and presence of bacteria (p<0.05 for all). Patients with positive stone cultures had increased preoperative urine cultures (56% vs 13%; p<0.001) and were more likely to have calcium phosphate (51% vs 20%) or struvite stone compositions (8% vs 1%; p<0.001). Positive stone cultures were also associated with grades 1-2 Clavien-Dindo complications (27% vs 15%; p=0.045), postoperative fever (11% vs 1%; p=0.007), readmission (22% vs 9%; p=0.020), and stone recurrence (23% vs 7%; p=0.002).
Conclusions: The results of this study demonstrated that female gender, indwelling catheters, UA markers of infection, positive urine cultures, and calcium phosphate or struvite stone compositions were all associated with positive stone cultures. Patients with positive stone cultures were at higher risk of grade 1-2 surgical complications, postoperative fever, readmission, and stone recurrence. Subsequently, patients with preoperative risk factors should undergo more aggressive preoperative prophylaxis and more aggressive prevention strategies to avoid complications and stone recurrence.
#297
Predicting Nasopharynx Distance in Children: A Pilot Study
He M1, Huang C1, Dorling M1, Tobia A2, Pauwels J2, Chadha NK2. 1University of British Columbia, Vancouver, BC, Canada and 2BC Children’s Hospital, Vancouver, BC, Canada
Purpose of Study: The nasopharynx (NP) swab test is a commonly performed procedure for diagnosis of viral upper respiratory infections. Previous studies predicting nasopharyngeal depth (ND) in children are unavailable. Current North American guidelines to obtain a viable NP swab are vague and impractical, potentially leading to inconclusive test results. This study aims to investigate whether a correlation exists between ND and patient’s surface landmark measurements or clinical data: age, sex, ethnicity, height, weight, finger length, and distance from tragus to alar rim of nose (TrAla). The secondary objective is to examine whether an accurate prediction of ND could be made through a simple predictive formula. This could then be used to guide healthcare professionals in obtaining reliable bedside NP sample collection.
Methods Used: We conducted a cross-sectional pilot study at the BC Children’s Hospital Pediatric Otolaryngology (ENT) Clinic from June to August 2022 and June to October 2023. Participants were children under the age of 17 years of age undergoing flexible nasal endoscopy as part of their standard care. ND was measured from nostril to the posterior NP wall during nasal endoscopy and compared to participant demographics and clinical measurements including height, weight, TrAla, and fingers lengths (index, middle, ring, and pinky). Statistical analyses were performed with R version 4.2.1 to develop a model predicting ND using stepwise linear regression.
Summary of Results: A convenience sample of 53 participants was recruited from June to August 2023 (30% female, age range 3 weeks–18 years). The mean ND ± standard deviation for participants between the ages of 0-4 years old (N = 23), 5-9 years old (N = 11), 10-14 years old (N = 11), and ≥ 15 years old (N = 2) were 5.89 ± 1.78 cm, 7.25 ± 1.80 cm, 8.91 ± 1.76 cm, and 9.03 ± 1.79 cm respectively. 4/53 had previous adenoidectomy. A linear relationship was found between seven continuous predictor variables and NP distance: age in months, age in years, height, weight, index length, middle finger length and small finger length. The seven multicollinear variables were analyzed separately within the test model that included non-collinear measures (TrAla, sex, history of adenoidectomy). Stepwise linear regression identified that each of the collinear variables resulted in a comparable adjusted R2 (0.75-0.80) for a predicting model. The pinky equation had the highest R2 for predicting ND. Rounding the equation to “ND=0.25TrAla+pinky+0.5,” presented the simplest and most accurate model to estimate NDin children (training RMSE 0.98, testing 0.80, adjusted R-square 0.70).
Conclusions: A simple and accessible bedside equation can potentially be used to predict the distance of the swab insertion for sampling the NP: ND=0.25TrAla+pinky+0.5. This formula offers an individualized NP sample collection guide to achieve reliable sampling while minimizing discomfort and complications.
#298
Association of Postoperative Complications with Attributable Increase in Postoperative Length of Stay in a Broad Surgical Population
Healy GL, Stuart CM, Dyas A, Bronsert MR, Meguid R, Anioke T, Schulick RD, Henderson W. University of Colorado School of Medicine, Aurora, CO
Purpose of Study: Postoperative complications occur in 15% of nonemergent inpatient surgeries. The impact of surgical complications on postoperative length of stay (PLOS) in a broad surgical population is relatively unstudied. The objective of this study was to determine the unadjusted and risk-adjusted changes in PLOS associated with specific types of postoperative complications in a broad inpatient surgical population. This information may be helpful to patients and providers to inform decision-making and provide insight into resource allocation.
Methods Used: This was a retrospective cohort study using the American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) participant use file, 2005-2018. The associations between PLOS, preoperative characteristics, and postoperative complications were tested using a t-test, one-factor ANOVA, or Pearson correlation, where appropriate. Multiple linear regression analysis was performed with PLOS as the dependent variable and the preoperative variables and postoperative complications as independent variables. Models estimating the association between postoperative complications alone and risk-adjusted with preoperative variables and PLOS were examined.
Summary of Results: Of 4,413,041 patients analyzed, the majority of patients were female (56.5%), white (67.1%), ASA class II-III (87.2%), and underwent general or orthopedic surgery procedures (70.0%). All 27 preoperative patient characteristics were significantly related to PLOS (p<0.0001) and all 18 postoperative complications were associated with significant increases in unadjusted PLOS, ranging between 2.1-12.8 days. A total of 733,500 patients (16.6%) had at least 1 postoperative complication, increasing their length of stay on average 6.1 days. The most common complication was bleeding requiring transfusion (7.1%), while the least common was cardiac arrest requiring CPR (0.1%). After adjusting for preoperative variables and multiple complications, PLOS remained increased for all postoperative complications, with attributable increases ranging from 1.6-9.6 days. The largest risk-adjusted individually attributable increases in PLOS were associated with ventilator use >48 hours (9.63, 95% Confidence Interval (CI) 9.58-9.68), acute renal failure (6.95, 95%CI 6.87-7.04), and organ/space surgical site infection (4.25, 95%CI 4.21-4.28). The lowest risk-adjusted increase in PLOS was associated with myocardial infarction (1.60, 95%CI 1.53-1.66).
Conclusions: Occurrence of any postoperative complication was associated with extended PLOS, even when adjusting for preoperative risk. The increase varied depending on the complication, with the greatest individually attributable impact resulting from prolonged ventilation, acute renal failure, and organ space SSI. These data can help inform patients about impact of postoperative complications, surgeons about targets for perioperative risk mitigation, and administration about resource allocation after postoperative complications.
Risk Adjusted Average Increase in Postoperative Length of Stay Associated with Postoperative Complications.
Risk-Adjusted Predictors
Average Increase in PLOS (days)
Lower 95% CI
Upper 95% CI
Ventilator Use > 48 hours
9.63
9.58
9.68
Acute Renal Failure
6.95
6.87
7.04
Organ Space SSI
4.25
4.21
4.28
Pneumonia
3.83
3.79
3.87
Septic Shock
3.61
3.56
3.67
Wound Disruption
3.29
3.23
3.35
Unplanned Intubation
3.14
3.09
3.20
Cardiovascular Accident/Stroke with Neurological Defecit
3.10
3.01
3.19
Progressive Renal Insufficiency
3.01
2.94
3.09
#299
The Use of a Percutaneous Radiolunate Screw in the Treatment of a Dumontier Group 1 Radiocarpal Dislocation
Irby M, Manoharan A, DeSilva G, Margolis D. University of Arizona College of Medicine Tucson, Tucson, AZ
Case Report: Treatment algorithms for radiocarpal dislocations remain unclear due to the rarity of the injury. Evidence in case series seems to suggest primary volar ligament repair with temporary radiolunate fixation yields acceptable results. However, in an effort to reduce surgical time and anesthesia alternative treatment options were explored for polytraumatized patients. Currently, there is no described literature on treatment of radiocarpal dislocations with a percutaneous radiolunate screw. We present the case of a 24-year-old male who presents with a Dumontier Group 1 radiocarpal dislocation after falling off his motorcycle. He was treated at that time with closed reduction and percutaneous radiolunate screw fixation. We describe a technique for percutaneous radiolunate screw fixation for 18 weeks, much like the technique used in stabilization of Lisfranc injuries, for the treatment of Dumontier Group 1 radiocarpal dislocations. Primary volar repair was not attempted. After removal of his screw at 18 weeks his wrist was stable with no evidence of ulnar translocation and near full active range of motion at 1 year.
#300
A Dedicated Outbound Scheduler Improves Clinic Utilization and Access to Care
Krewson C2, Taylor A1, Kieran K1. 1Seattle Childrens, Seattle, WA and 2Pacific Northwest University, Yakima, WA
Purpose of Study: Differential access to care for patients living in more disadvantaged areas has been well documented, though the specific factors underlying these disparities have not been well described. We undertook this study to describe how clinic utilization and patient demographics differed before and after the utilization of a dedicated scheduler making outcalls for scheduling.
Methods Used: We identified all new patients seen in a single pediatric urology outreach clinic in March and April 2021 (prior to the scheduler being hired) and July and October 2021 and April, July and October 2022, and April 2023 (after the scheduler was hired). We recorded the overall clinic utilization for each fiscal year and also demographic data (including Area Deprivation Index [ADI]) on the new patients seen in clinic. Data before and after the hiring of the dedicated scheduler were compared.
Summary of Results: Scheduled clinic utilization increased from 93.6% in FY 2021 to 95.2% in FY2022 and to 98.9% in FY2023. Missed appointments were relatively stable at 7.4% in FY2021, 7.8% in FY2022, and 6.8% in FY2023. The number of new patients scheduled per month increased by 59% (62 vs. 39) after the addition of scheduling outcalls. The proportion of new patients living in the most disadvantaged areas (ADI 9-10) increased from 35.9% before the scheduler was hired to 61.3% after the addition of the scheduler (p=0.009), while the proportion of new patients living in the least disadvantaged areas (ADI 1-2) remained stable (2.6% vs. 4.8%, p=0.56).
Conclusions: Addition of a dedicated clinic scheduler making outbound calls increased clinic utilization durably and facilitated access primarily for patients living in the most disadvantaged areas. Further research is needed to identify what aspects of outbound scheduling are most helpful to the most vulnerable patients.
#301
COMPARING THE TREATMENT OF BENIGN PROSTATIC HYPERPLASIA IN UNDERSERVED COMMUNITIES USING BIPOLAR TRANSURETHRAL ENUCLEATION OF THE PROSTATE VERSUS ROBOTIC-ASSISTED SIMPLE PROSTATECTOMY
Kim U1, Quines JF1, Farkouh A2, Amasyali AS2, Okhunov Z2, Baldwin D2. 1Loma Linda University School of Medicine, Loma Linda, CA and 2Loma Linda University Health, Loma Linda, CA
Purpose of Study: Benign prostatic hyperplasia (BPH) is a highly prevelant disease among elderly men that causes lower urinary tract symptoms (LUTS) due to excess prostatic tissue constricting the urethra. Simple prostatectomy (SP) has been the traditional surgical treatment for larger prostates (>80 g), but new surgical techniques have emerged that reduce complication rates and cost, while maintaining high efficacy. Among those innovations, Bipolar Transurethral Enucleation of the Prostate (B-TUEP) has been recognized in recent years as a reliable technique for treating BPH where high-power lasers are not available. However, there is limited information on how B-TUEP compares to robotic-assisted simple prostatectomy (RASP). This study assessed the effectiveness and safety of B-TUEP compared to RASP in the largest most ethnically-diverse patient population reported to date.
Methods Used: This study retrospectively reviewed 125 patients, 84 undergoing B-TUEP and 41 undergoing RASP, for the treatment of symptomatic BPH in a diverse underserved patient population within a single academic institution. Information sourced from the US Census Bureau was used to determine the percentage of participants residing below the poverty line based on their zip codes. Data collection encompassed medical history, transrectal ultrasound (TRUS), urinalysis, voiding trials, blood tests, PSA values, and surgical outcomes. Statistical analysis, which involed the two-tailed t-test, Wilcoxon signed-rank test, and Pearson Chi-square test (p<0.05 considered significant for all tests), compared outcomes based on surgery group, race, and residence in a low-income area.
Summary of Results: Significant baseline demographic differences between the surgery groups included a greater average prostate mass in the RASP group (163 g vs 114 g; p<0.001) and a higher percentage of catheter-dependent patients compared to the B-TUEP group (p=0.042). Furthermore, a significantly greater proportion of non-White individuals underwent B-TUEP, whereas more White individuals received RASP (p=0.026). Though both techniques were effective at removing prostate tissue and improving voiding symptoms, B-TUEP had shorter operation times (110 min vs 257 min; p<0.001), hospital stays (0.49 days vs 1.73 days; p<0.001), and catheterization durations (3.24 days vs 11.29 days; p<0.001) compared to RASP. Complications including catheter malfunction, erectile dysfunction, urinary incontinence, and blood transfusions were also more prevalent after RASP (p<0.05). There were no significant differences in outcomes when stratifying by race or poverty.
Conclusions: Our findings highlight both B-TUEP and RASP as effective surgical options for BPH patients belonging to a wide range of ethnicities and socioeconomic backgrounds. Thus, B-TUEP is a safe and effective approach for treating prostatic obstruction that provides equitable healthcare access at institutions that may not have high-power lasers and surgical robots.
#302
Consensus Guidelines For Infection Reduction In Deep Brain Stimulation Surgery: A Modified Delphi Study
Pardakhtim S, Marsans M, Farrokhi F. Virgina Mason, Seattle, WA
Purpose of Study: To establish consensus guidelines for minimizing infection in DBS surgery.
Methods Used: A modified Delphi technique was employed to establish consensus guidelines for perioperative infection reduction. After literature review on surgical site infection (SSI) prevention in Deep Brain Stimulation (DBS) surgery, an expert panel was employed to refine findings. This panel consisted of neurosurgeons in the state of Washington active in DBS surgery. A four step modified Delphi method was used including: literature review, initial survey of an expert panel, live discussion, and a final survey with ranking of recommendations.
Summary of Results: All nine surgeons performing DBS surgery in Washington participated. In the first round, the expert panel rated interventions based on current practice. This yielded separation of the 22 recommendations into: 11 unanimous or high consensus, 1 moderate, 7 low and 3 with no consensus. After refining the recommendations during live discussion, the final survey asked participants to weigh the value of 23 interventions. This yielded 1 unanimous or high consensus, 8 moderate, 11 low and 3 with no consensus.
Conclusions: Using a modified Delphi method, we established statewide consensus guidelines for infection prevention in DBS surgery. These guidelines may guide current practice toward decreasing infection rates.
#303
THE RADPAD: COMPARISON OF A NOVEL LEAD-FREE RADIATION PROTECTION DEVICE TO CONVENTIONAL LEAD APRON
Quines JF, Hanessian KA, Farkouh A, Crew R, Kim U, Sajdak G, Baldwin D, Amasyali A, Okhunov Z, Baldwin D. Loma Linda University Health, Loma Linda, CA
Purpose of Study: Complex kidney stone removal with percutaneous nephrolithotomy (PCNL) routinely requires fluoroscopy that exposes the surgeon to ionizing radiation. While the standard radiation protection for urologists involves a lead apron and thyroid shield, these routinely do not protect the head, arms, and legs. Recently, a non-lead device (RADPAD ®) that can be placed on the patient has been developed. The RADPAD® is a non-lead shielding device positioned directly in the surgical field to protect against scatter radiation. The objective of this study was to compare the effectiveness of the RADPAD® to conventional lead and the combination of the two.
Methods Used: To simulate a PCNL, a radiographic phantom patient and a mannequin surgeon were utilized (figure 1). Radiation doses were measured in μSv at seven distinct anatomical locations on the surgeon (head, neck, chest, abdomen, pelvis, forearm, leg). Three shielding devices were evaluated: a conventional lead apron with a thyroid shield (LA), a double-thickness RADPAD® (R2X), and a triple-thickness RADPAD® (R3X). The effectiveness of combining LA with R2X (LAR2X) and R3X (LAR3X) was also examined and compared to baseline (no lead). Five trials of five-second fluoroscopy were conducted for each site and shielding combination.
Summary of Results: The LA alone significantly reduced radiation exposure at all tested sites compared to the baseline, reaching reductions >98% (p<0.05), except for the head, leg, and forearm of the surgeon. Both R2X and R3X significantly reduced radiation at all tested sites, with the exception of the legs, and additionally reduced radiation to the head (up to 47.62%) and forearm (up to 84.16%; p<0.05). When comparing the performance of each shielding device, LA significantly outperformed R2X and R3X at the neck, chest, abdomen, and pelvis (p<0.05). LAR3X resulted in the greatest reduction in radiation, performing significantly better than LA alone at the head, pelvis, and forearm (p<0.05). No single shielding device or combination significantly reduced radiation exposure to the legs.
Conclusions: The LA alone reduced radiation >98% at shielded sites, but provided no protection to the head, leg, and forearm. The R2X and R3X alone were not sufficient to replace lead as they provided less protection for vital organs than the LA. However, additional use of either R2X or R3X resulted in significant radiation reduction (41-100%) to the head and forearm, without imposing increased weight burdens upon the surgeon.
#304
Radiation Exposure in Voiding Cystourethrograms and Intraoperative Cystograms in Children with Vesicoureteral Reflux
Roh D, Dwumfour S, Papaioannou P, Farkouh A, Pearce J, Cheng K, Kuang R, Song S, Chamberlin D, Chamberlin J. Loma Linda University, Loma Linda, CA
Purpose of Study: Voiding cystourethrogram (VCUG) is an imaging modality used to diagnose vesicoureteral reflux (VUR), monitor its progression, and assess for recurrence after treatment. However, it involves ionizing radiation, which confers the risk of cancer and tissue damage with each exposure. In select settings, such as after endoscopic VUR treatment with Dextranomer/hyaluronic acid, intraoperative cystograms have been utilized to assess immediate treatment response and may reduce the overall radiation burden for patients with VUR. There is controversy regarding the utilization of intraoperative cystograms for this indication due to their inability to detect reflux during the voiding phase and unclear radiation burden. The purpose of this study was to evaluate radiation exposure during VCUG compared to intraoperative cystograms for patients with VUR.
Methods Used: Retrospective review of a prospectively maintained database of patients with primary VUR at a single children’s hospital was performed. All patients who had endoscopic Dextranomer/hyaluronic acid treatments for VUR were included. VCUG data was evaluated for the reflux onset. Fluoroscopy data was collected from both VCUGs and intraoperative cystograms when available. Total fluoroscopy time was compared between the two imaging modalities. Independent samples t-test was conducted with a p-value of <0.05 deemed statistically significant.
Summary of Results: Forty-five patients met inclusion criteria, with 27 female (60%) and 18 male (40%) patients. At the time of initial presentation, low-grade VUR (grades 1-3) was noted in 27 patients (60%), and high-grade VUR (grades 4-5) was noted in 18 patients (40%). Of all 110 VCUGs conducted during initial and follow-up visits, 26 (23.6%) exhibited reflux during the voiding phase. Reflux was observed during the early filling phase in 49 VCUGs (44.5%) and during the late filling phase in 23 VCUGs (20.9%). In 18 of the VCUGs (16.4%), the onset of reflux was unable to be determined. The fluoroscopy times for VCUGs were 7.6 times higher than those for intraoperative cystograms (54 seconds vs. 7.2 seconds, respectively; p < 0.001).
Conclusions: VCUGs expose children to 7.6 times more radiation than intraoperative cystograms for the assessment of VUR. Intraoperative cystograms reduce radiation exposure and may be considered for evaluating VUR response in children with filling phase reflux after endoscopic treatment with Dextranomer/hyaluronic acid.
#305
The Impact of Social Vulnerability on Aortic Arch Surgery
Shah A1, Carroll AM2, Suarez-Pierre A2, Rove JY3, Velopulos C4, Aftab M3, Reece TB3. 1University of Colorado School of Medicine, Aurora, CO; 2University of Colorado School of Medicine, Aurora, CO; 3University of Colorado Anschutz Medical Campus, Aurora, CO and 4University of Colorado Denver, Anschutz Medical Campus, Aurora, CO
Purpose of Study: Socioeconomic status is a known factor influencing morbidity and mortality. The CDC’s social vulnerability index (SVI) quantifies neighborhood-level vulnerability. Although high SVI has been associated with adverse outcomes in trauma, CABG, and AAA repair, its impact on aortic arch surgery remains unknown. It is predicted that in total aortic arch (TAR) and hemiarch (HAR) replacement, higher SVI will correlate with increased comorbidities, surgical acuity, and post-operative morbidity and mortality.
Methods Used: This single-center retrospective study examined adult patients undergoing HAR and TAR performed for aortic aneurysm and/or dissection between 2010 and 2022. SVI was calculated by the patients’ residential ZIP codes. The cohort was stratified into three groups: SVI<0.33, SVI 0.33-0.66, and SVI≥0.66. The primary endpoint was postoperative mortality, with control for confounding bias through multivariable logistic regression.
Summary of Results: For 753 patients, higher SVI correlated with more baseline comorbidities and minority status. SVI was associated with dissection pathology (p=0.04) and urgent/emergent procedures (p=0.02). High SVI was associated with TAR (p=0.01), reflected by lower nadir bladder temperatures (p=0.01), longer cardiopulmonary bypass (p=0.02), longer circulatory arrest times(p=0.01), and more coagulation product usage.
High SVI patients had longer length of stay, higher rates of infection (p=0.01) and a trend towards increased stroke risk. SVI did not correlate with in-hospital or late mortality, confirmed by multivariable regression.
Conclusions: In socially vulnerable communities, patients who require aortic arch surgery have more comorbidities and present urgently or emergently with dissection pathology, requiring more extensive arch repair. Post-procedure, they have a higher risk of infection and a trend towards more stroke risk, but not higher rates of other adverse outcomes or increased mortality during or after hospital stay.
Summary of pre-operative and operative characteristics, and post-operative outcomes for patients undergoing hemiarch or total aortic arch replacement stratified by social vulnerability index (with higher SVI denoting increased social vulnerability). Additional variables were analyzed but not included in final table. All reported values are median [interquartile range]. Performed tests are Kruskal-Wallis rank sum for continuous variables and Chi-square test for categorical variables. * < 0.05.
SVI < 0.33 (n=275)
SVI 0.33-0.66 (n=331)
SVI ≧ 0.66 (n=147)
p-value
Pre-Operative Outcomes
Race
<0.01*
Comorbidities
Hypertension
185 (67.3)
213 (64.4)
112 (76.2)
0.04*
Diabetes
19 (6.9)
26 (7.9)
20 (13.6)
0.05*
Peripheral Vascular Disease
7 (2.5)
3 (0.9)
10 (6.8)
<0.01*
Etiology
0.04*
Aneurysm
190 (69.1)
208 (62.8)
86 (58.5)
Dissection
36 (13.1)
71 (21.5)
33 (22.4)
Aneurysm and Dissection
49 (17.8)
50 (15.1)
26 (17.7)
Operative Outcomes
Status
0.02*
Elective
197 (71.6)
198 (59.8)
85 (57.8)
Urgent
30 (10.9)
49 (14.8)
22 (15.0)
Emergent
48 (17.5)
84 (25.4)
40 (27.2)
Procedure
0.01*
TAR
63 (22.9)
82 (24.8)
53 (36.1)
HAR
212 (77.1)
249 (75.2)
94 (63.9)
Bladder Nadir Temperature, C
27.1 [25.6, 28.0]
26.8 [25.0, 27.9]
26.5 [24.0, 27.9]
0.01*
Cardiopulmonary Bypass Time, min
146 [119, 202]
154 [120, 212]
166 [133, 215]
0.02*
Circulatory Arrest Time, min
11 [7, 22]
12 [8, 22]
15 [10, 25]
0.01*
Post-Operative Outcomes
Unplanned Reoperation Needed
0.56
Cerebrovascular Injury
20 (7.3)
34 (10.3)
21 (14.3)
0.07
Infection
16 (5.8)
31 (9.4)
22 (15.0)
0.01*
Length of Stay, days
7 [6, 11]
8 [7, 13]
9 [7, 13]
<0.01*
ICU Length of Stay, days
3 [2, 5]
3 [2, 6]
4 [2, 6]
0.05*
Post-Operative In-hospital Mortality
16 (5.8)
29 (8.8)
11 (7.5)
0.39
Post-Discharge Death (within one year)
0.28
#306
Patients with Lumbar Degenerative Spine Disease Are Satisfied with Outcome Measure Surveys
Sheasley J1, Dohm M2. 1University of Washington School of Medicine, Seattle, WA and 2University of Minnesota, Minneapolis, MN
Purpose of Study: Patient-reported outcome measure (PROM) surveys help evaluate the effectiveness of medical interventions. It is important to evaluate patients’ reactions to these surveys to determine if they are perceived as worthwhile. The purpose of this study is to identify lumbar degenerative spine disease (DSD) patients’ perceptions of three commonly used PROM surveys: the Patient-Reported Outcomes Measurement Information System-10 (PROMIS-10), the Patient Health Questionnaire-9 (PHQ-9), and the Oswestry Disability Index (ODI).
Methods Used: A prospective cohort study was performed to examine patients with lumbar DSD at one practice between June 2014 and December 2016. Patients completed a survey online prior to their first appointment or on a tablet at the appointment. The following data were collected from patient records and survey results: patient demographics, pain level, social history, co-morbidities, patient-reported outcome measures (PROMIS-10, PHQ-9, and ODI), and patient perception of the surveys they completed.
Summary of Results: Two hundred and seventy-nine patients completed at least some portion of the surveys at their initial appointment. 96.4% of patients felt neutral, satisfied, or very satisfied with the types of questions. 94.9% of patients were satisfied with the number of questions. 95.2% were satisfied with the system used for answering questions. 98.4% of patients felt it was at least minimally important for the clinician to get the information. Of the 279 patients, 96.1% completed the PHQ-9, 96.1% completed the PROMIS-10, and 95.3% completed the ODI.
Conclusions: Satisfaction with the three surveys was high and the importance of obtaining this information was well-understood by patients. Completion rates for all three measures were greater than 95% each, indicating that the online or tablet format was very successful and is an effective survey administration method that can be used in the future.
#307
EMERGENT ABOVE-KNEE-AMPUTATION IN A VASCULOPATHIC PATIENT
Shen C, Soria C. University of California San Diego, San Diego, CA
Case Report: 57M with extensive vascular surgery history, CAD status-post 3 vessel CABG, and congestive heart failure (LVEF 29% with biventricular failure) was taken for an emergent right above-knee-amputation in the setting of a non-healing below-knee-amputation wound. The patient coded during emergence from general anesthesia and underwent a successful resuscitation with return of spontaneous circulation achieved in less than two minutes. Post-operative care was delayed due to a complex disposition, which included a stroke code called over two hours after emergence for a fixed, dilated right pupil. Ultimately the patient did not have a stroke, and his abnormal pupil exam was attributed to his pre-existing diabetic retinopathy and cataracts. The patient was later found to have reduced LVEF from 29% to 18% after the procedure. His code status was changed to DNR/DNI, and he was discharged on postoperative day 10 without new neurologic deficits or surgical complications.
#308
ANALYZING THE ASSOCIATION BETWEEN SOCIAL VULNERABILITY INDEXES AND SURGICALLY UNDERSERVED AREAS IN THE INLAND EMPIRE
Shin B, Wongworawat MD, Baum M. Loma Linda University, Loma Linda, CA
Purpose of Study: The United States lacks equitable surgical access, prompting us to investigate the relationship between social vulnerability and surgeon number using the Inland Empire as a model.
Methods Used: The Centers for Disease Control’s (CDC) SVI 2018 database was compared against the American Medical Association’s (AMA) Physician Masterfile. Analysis was performed via a Spearman’s bivariate and a multiple regression.
Summary of Results: Our work demonstrates that an inverse relationship exists between surgeon number and overall social vulnerability (ρ=-0.266 [95% CI -0.330 to -0.199], p<.001), and between surgeon number and each category of social vulnerability: Socioeconomic (ρ=-0.345 [95% CI -.0405 to -0.281], p<.001), Household Composition and Disability (ρ=-0.121 [95% CI -0.190 to -0.051], p<.001), Minority Status and Language (ρ=-0.0317 [95% CI -0.379 to -0.252], p<.001), and Housing Type and Transportation (ρ=-0.093 [95% CI -0.153 to -0.023], p=.005). Multiple regression analysis revealed that the following were associated with a higher number of surgeons: higher “Per Capita Income” (B=0.000151 [95% CI .000079 to .000223], t(820)=4.104, p<.001), larger Daytime Population (B=0.000143 [95% CI .000072 to .000214]; t(820)=3.956, p<.001), larger Total Population (B=-0.013 [95% CI -.022 to -.003]; t(820)=-2.672, p=.008), and smaller number of Persons aged 17 and younger (B=-0.005 [95% CI -.008 to -.001]; t(820)=-2.794, p=.005).
Conclusions: Thus, this study concludes that access to surgery is significantly linked to differences in social vulnerability and continues to advocate for future research into understanding the surgeon’s role in both individual and population health.
#309
ANATOMICAL VARIATIONS AND FUNCTIONAL CONSIDERATIONS OF QUADRATUS PLANTAE IN RECONSTRUCTIVE FOOT SURGERY
Sidhu SK, Atterholt J. Western University of Health Sciences, College of Osteopathic Medicine of the Pacific, Pomona, CA
Purpose of Study: This study aimed to contribute to the literature of anatomical variations as there are implications for surgical approaches and recovery time for patients.
Methods Used: During routine dissection at an osteopathic medical school, a quadratus plantae (QP) muscle variant was found which prompted a survey of all available cadaveric lower limbs. Variations of QP were carefully photo documented by a student-faculty pair.
Summary of Results: An ongoing survey of cadaveric lower limbs has found several variations of QP and its attachments to flexor digitorum longus (FDL) and flexor hallucis longus (FHL): A unilateral variation of QP dividing into superficial and deep layers around FDL, a bilateral trilaminar variation of QP contributing tendons to toes three and four with interconnections to FHL, and, finally, a novel unilateral variation involving complete QP attachment, as well as the origin of a lumbrical muscle, onto the second tendon of FHL (Fig. 1).
Conclusions: Given the variation of the second tendon of FHL harboring both the QP attachment and lumbrical origin, several surgeries are advised to reconsider their approach to preserve functionality and improve recovery.
For example, a surgeon using the FHL for transfer in chronic Achilles tendon ruptures will lead to increased complications for a patient with the described variation. The functionality of the QP may be compromised and result in decreased plantar flexion and foot eversion, thus affecting overall synergy of bipedal movement.
Additionally, in a hallux valgus or bunion surgery, the first tendon of the FHL may be released to reduce pull on the first phalanx. However, this release could distribute force onto the second tendon of FHL, which in this variant is connected to QP, and lead to increased pronation or plantar flexion. Such a patient will likely need prolonged physical therapy post-operatively to regain functional gait.
Thus, surgeries for posterior tibial tendon dysfunction, hammertoe deformity, flatfoot deformity, and plantar fasciitis would benefit from documentation of QP variations. Therefore, a classification system may be appropriate to aid surgeons in identifying and considering key landmarks.
QP attachment to FHL.
#310
Analysis of Risk-Adjusted Surgical Outcomes in the ACS-NSQIP Demonstrates Improvements Over Time
Thompson K, Stuart CM, Bronsert MR, Henderson W, Meguid R. University of Colorado School of Medicine, Aurora, CO
Purpose of Study: Prior publications have demonstrated that hospitals who participated in the American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) found no association between NSQIP participation and risk-adjusted outcomes over time. The purpose of this study was to re-examine the trend in postoperative complications over time using the full ACS-NSQIP dataset. We hypothesize that unadjusted and risk-adjusted outcomes improve over time for all operations.
Methods Used: We used the ACS-NSQIP database, 2006-2018, to analyze rates of adverse postoperative outcomes by year. Outcomes of interest included 30-day mortality, overall morbidity, pulmonary, infection, urinary tract infection, venous thromboembolism, cardiac, renal, stroke, and bleeding complications. Expected values were calculated using multiple logistic regression with the 28 non-laboratory preoperative ACS-NSQIP variables as the independent variables. Annual observed-to-expected (O/E) ratios for each outcome were used to risk-adjust outcomes over time.
Summary of Results: The analytic cohort included 7,474,298 operations across 9 surgical specialties. Total cases/year ranged from 117,512in 2006 to 1,003,238 in 2018. The unadjusted rate of post operative complications decreased over time in 9 of the 10 outcomes except for cardiac complications (figure 1). After risk adjustment, there was an overall downward trend in most outcomes with the exception of cardiac morbidity. While the O/E ratio for mortality remained around 1, the O/E ratio of overall morbidity decreased from 1.11 to 0.97. The greatest decrease in postoperative complications occurred for bleeding complications, decreasing from 1.34 to 0.79.
Conclusions: We found the hospitals participating in the ACS-NSQIP have experienced a risk-adjusted decrease in postoperative surgical outcomes over time in all areas except cardiac complications. This is contrary to prior analyses. This is possibly due to a combination of gradual improvement in patient care decreasing some postoperative adverse outcomes, and awareness of surgical outcomes guiding targeted intervention to decrease others. Future analysis of outcomes by surgical specialty may further elucidate trends.
#311
A Survey on Enhanced Recovery After Surgery Elements in Pediatric Orthognathic Surgery
Vallurupalli M1, 2, Fligor J2, Vyas R2, 3. 1Keck School of Medicine of USC, Los Angeles, CA; 2University of California, Irvine, Orange, CA and 3Children’s Hospital of Orange County, Orange, CA
Purpose of Study: Enhanced Recovery After Surgery (ERAS) protocols implement perioperative interventions to improve patient outcomes by limiting the surgical stress response, optimizing physiological function, and facilitating recovery. They have demonstrated success in adult surgical populations. We predict these benefits extend to the pediatric craniofacial population and can be particularly effective for orthognathic surgery. This study investigates current attitudes and use of ERAS protocols in orthognathic surgery.
Methods Used: An electronic survey was distributed to 102 craniofacial (CF) and oral and maxillofacial (OMF) surgeons in the United States. Responses were collected from April to July 2023. Surveys queried surgeons’ knowledge, use, and attitudes regarding specific ERAS elements in pediatric (patients under age 25) orthognathic surgery. Surgeons were specifically asked about their preoperative, intraoperative, and postoperative practices and beliefs. Survey responses were collated and analyzed.
Summary of Results: 41 (40.2%) of 102 surgeons completed the survey. 7 of 14 surveyed elements are employed by a majority of surgeons for all patients: hypothermia prevention (61.0%), standardized protocol for maintaining normovolemia (61.0%), bolus of intraoperative tranexamic acid (51.2%), multimodal approach to postoperative nausea (61.0%), minimized use of opioids for postoperative pain control (51.2%), postoperative antiemetics in the first 48 to 72 hours (53.7%), and postoperative bite stabilization (58.5%). Additionally, 21 (51.2%) of surgeons reported using short acting anesthetic agents, like Precedex, at time of extubation for all or most patients, but only 11 (26.9%) surgeons reported use for all or most patients early in the postoperative period. With regards to bite stabilization, 29 surgeons (70.7%) reported using just elastics. Liposomal bupivacaine was not commonly used: 37 surgeons (90.2%) reported never using this modality. Infusion dosing of intraoperative tranexamic acid was used for no or some patients by 24 surgeons (58.5%). Surveyed surgeons were least familiar with preoperative nutritional screenings or consultations (17.1%) and postoperative goal directed or zero fluid balance models (29.3%). Surgeons reported the most familiarity with bite stabilization (65.9%), minimizing use of opioids for postoperative pain control (48.8%), and administering a bolus of intraoperative tranexamic acid (43.9%).
Conclusions: Surveyed surgeons endorse and report using ERAS-type perioperative elements in pediatric orthognathic surgery. Most surgeons reported, at minimum, being somewhat knowledgeable about most surveyed ERAS elements. Further evidence and multidisciplinary cooperation is necessary to implement a formalized ERAS protocol for pediatric orthognathic surgery.
#312
ORTHOPEDIC INJURY AND INTIMATE PARTNER VIOLENCE; UPPER EXTREMITY FRACTURE PATTERNS: A LITERATURE REVIEW
Willson RE1, Martinson H2. 1University of Washington School of Medicine, Seattle, WA and 2University of Alaska Anchorage, Anchorage, AK
Purpose of Study: Intimate partner violence (IPV) is a prevalent issue in the U.S., causing both chronic health concerns and acute injuries such as fractures. After maxillofacial traumas, musculoskeletal injuries are the second most common injury seen in victims of IPV. The prevalence of musculoskeletal injuries in this population demonstrates the opportunity for orthopedic surgeons to identify IPV victims. Specific IPV injury patterns have been previously identified yet despite upper extremity fractures (UEF) being prevalent in this population, data on fracture patterns associated with IPV is limited. This literature review aims to determine patterns of orthopedic injury associated with IPV that physicians can utilize as an objective sign to identify IPV patients.
Methods Used: A comprehensive literature search was completed using PubMed, PsycINFO, and Web of Science. Zotero removed 42 duplicates from 316 resulting articles. Title and abstract screenings were completed by two independent researchers. Inclusion criteria consisted of retrospective cohort studies and literature reviews where patients presented to a medical facility with an orthopedic injury caused directly by IPV and where an orthopedic physician was involved or had reason to be involved with patient care. Excluded articles were case studies or perspective articles, materials published before 2003, studies with pediatric and elderly populations, and maxillofacial fractures. Screening identified 24 articles assessed for eligibility, of which 16 were included.
Summary of Results: The final 16 articles reflected a diverse study topic range; 5 radiology studies, 4 orthopedic studies and 2 trauma studies. The remaining 5 studies came from family medicine, violence, and open publication journals. Data supported historical findings of musculoskeletal injury as the 2nd most common injury in patients with IPV. In 4 of 6 studies with specified UEF location, minimally displaced fractures of the phalanges were most common (9.9-64%), while 2 studies identified isolated ulnar fractures as the most common UEF. Minimally displaced ulnar fractures were associated with an 8.5 – 12.8 relative risk of IPV. Four radiology studies found patients with acute and chronic fractures were more likely to be victims of IPV (sensitivity 25.2%, specificity 99.2%, PPV 96.2%). Location patterns of chronic fractures matched those of acute UEFs caused by IPV. Two studies demonstrated new findings in male IPV victims: a higher proportion of lower extremity fractures in men and significantly more pelvic fractures in a male cohort (p < 0.05).
Conclusions: This study synthesizes evidence of IPV-related orthopedic injuries, offering objective criteria for identifying victims. Despite limitations in fracture descriptions, the patterns of UEFs and other orthopedic injuries will aid orthopedic surgeons, radiologists, and emergency physicians in recognizing IPV victims. Considering ongoing IPV prevalence and screening challenges, further research on injury patterns is needed.
#313
An Innovative Way to Upgrade Patient and Provider Experiences: ONE-4-ALL
Wilson SN, Mata C, Izere M, Acker SN, Kaar J. University of Colorado Anschutz Medical Campus, Aurora, CO
Purpose of Study: Caregivers experience increased anxiety and stress when navigating medical procedures as a part of their child’s healthcare. Standardized education around medical procedures reduces anxiety and improves experiences with healthcare. However, education demands additional time and an increased workload for providers. We seek to reduce these burdens through the use of an innovative patient-facing app that provides comprehensive education about medical procedures, including what to expect during post-procedure care. This app will grant providers more time to focus on caregivers’ questions and more complex needs while expanding parent satisfaction with the quality of their child’s medical care.
Methods Used: We collaborated with a team to create a family self-service model of care enabled by customizable apps. We sought to test the feasibility of the model by designing an app with workflow for families of children needing gastrostomy tubes. We created a three-step module containing a total of 11 lessons, including three four-minute educational videos, organized in a modular workflow that can be assigned to families at time points before surgery, the day of surgery, and before their follow-up visit. The workflow includes prompts to write down important information, think about questions for providers, and schedule follow-up care. Families can then access the content at their convenience and indicate mastery of each assignment at the designated time points. Included in the design of this model is the capability to monitor patients’ progress on their workflow, allowing staff to target support to each patient’s needs. Participating families were asked to complete G-Tube Readiness and Parent Anxiety & Satisfaction surveys before and after completing the modules.
Summary of Results: Six families completed pre- and post-education surveys on G-Tube Readiness, Anxiety, and Satisfaction. These families were randomized into two education groups: 3 families received standard education and 3 families used the IOM App for their education. Families who received app education improved their G-Tube Readiness scores by 3.7% more than the standard education group, had 5.5% lower anxiety scores, and increased their satisfaction scores by 13.9% over the standard education group. As more families are enrolled in the study, we expect these trends to continue.
Conclusions: Self-service care empowers parents while enhancing healthcare team efficiency. A family-centered, app-based model leads to increased confidence from parents in their child’s care, decreased time for clinical staff, and an upgraded experience for families and providers.
#314
RATES OF NON-UNION FOLLOWING ARTHRODESIS OF FIRST METATARSOPHALANGEAL JOINT: A META-ANALYSIS
Xavier J1, 2, Miller C3, 2, Sarli NM1, 2, Golovachev N1, 2, Ghayyad K2, Kachooei A2. 1Loma Linda University, Loma Linda, CA; 2Rothman Orthopedics, Orlando, FL and 3Maimonides Medical Center, Brooklyn, NY
Purpose of Study: Non-union is a relatively common complication of first metatarsophalangeal (MTP) arthrodesis, with a sizeable portion of those patients experiencing symptoms across numerous fixation techniques. The aim of this study was to provide an update to the literature regarding non-union rates in first MTP arthrodesis and to analyze these rates by surgical approach, pathology, deformity, bone preparation method, and fixation type.
Methods Used: PubMed, Cochrane, Embase, and MEDLINE databases were queried according to the PRISMA guidelines to identify studies that reported non-union rates following first MTP arthrodesis. The inclusion criteria were for studies from 2000-2020 reporting non-union rates among patients who underwent first MTP arthrodesis for hallux valgus or hallux rigidus deformities, and inflammatory conditions such as osteoarthritis and rheumatoid arthritis. Only patients undergoing primary arthrodesis were retained. The mechanism of arthrodesis (plates and screws, screws, nails, and wires), incision site, and preparation method were recorded. Random effect models were utilized to assess for mean non-union rates.
Summary of Results: A total of 76 studies were included in the final analysis, with 5327 extremities identified, a mean age of 59 years old, and a standard deviation of 6.8. The rate of non-union across all identified studies was 0.04 (95% CI 0.4-0.5). There was no significant difference in non-union rates identified when stratified by surgical approach 0.035 (95% CI 0.028-0.043, p=0.45), pathology 0.06 (95% CI 0.04-0.07, p=0.72), deformity 0.05 (95% CI 0.04-0.06, p=0.08), bone preparation method 0.05 (95% CI 0.04-0.06, p=0.08), and fixation method 0.04 (95% CI 0.4-0.05, p=0.81).
Conclusions: The determination of the non-union rates for first MTP fixation provides clinically relevant data for clinician and patient awareness as it allows for improved benefits/risk analysis. The finding of no significant difference in non-union rates in the surgical approach, bone preparation, and fixation method sub-analysis demonstrates the need for future analysis that considers other factors such as clinical outcomes, necessity of revision operation, patient preference, or surgeon expertise.
#315
ADVERSE EVENTS ASSOCIATED WITH MALE ARTIFICIAL URINARY SPHINCTER: A REVIEW OF THE MANUFACTURER AND USER FACILITY DEVICE EXPERIENCE DATABASE
Yazditabar J, Wright E, Cohen A. Johns Hopkins University, Baltimore, MD
Purpose of Study: Artificial urinary sphincter (AUS) placement remains the gold standard for correcting male stress urinary incontinence (SUI). As a medical device, the AUS is subject to reporting to the MAUDE database. The FDA depends on Medical Device Reports (MDRs) to inform policy regarding medical devices, but it is unknown if the MAUDE contents are consistent with real-world complications.
Methods Used: MDRs from the MAUDE database were queried for Boston Scientific AMS 800 and AMS 800 with InhibiZone (antibiotic coating) from September 2020 to September 2021. This search generated an initial total of 514 reports. Application of exclusion criteria, including incomplete reports and duplicate entries, resulted in a final cohort of 452. MDR event types were classified based on narrative descriptors of the cause of the adverse event. Data was compared to a single-center, multi-surgeon registry of AUS placements and outcomes. Descriptive statistics were calculated using R with p <0.05 considered statistically significant.
Summary of Results: The most common problem was persistent SUI, 162 cases (36%). 417 (92%) cases lead to surgical re-intervention, with complete device replacement in 244 (54%) cases. There were no major differences in complications stratified by AMS product type except for tissue Injury (Table 1). Extrapolation from the MAUDE database to then assume 4,600 yearly AUS cases yields a 9.8% incidence rate of adverse events per year. In contrast, based on institutional series, we incur a 33% incidence rate.
Conclusions: The MAUDE database seemingly suffers from under-reporting of AUS complications. A key limitation is the possibility of a gap between event occurrence and reporting, affecting the totals. Per the MAUDE database, most devices with issues are completely replaced instead of
salvage procedures for individual components of failure. The AUS has been the gold standard implant following prostate surgery in males for many years; however, it is essential to understand its safety and efficacy. The majority of adverse events lead to surgical intervention. These issues are under-represented in a key database dictating healthcare policy regarding medical devices. Future experiments can ascertain the necessity of antibiotic coating (no significance shown here) for the AMS or other surgical implants, the accuracy of the MAUDE database for similar medical devices, and the efficacy of similar treatment options such as the male urinary sling.
Adverse events associated with each AMS 800.
Adverse Event
AMS 800 n (%)
AMS 800 with InhibiZone n (%)
P-Value
PATIENT RELATED
Incontinence
86 (19)
76(17)
0.16
Tissue Injury
22 (4.9)
58 (12.8)
<0.01
Erosion
28 (6.2)
35 (7.7)
0.47
Other1
15 (3.3)
15 (3.3)
0.88
Infection
8 (1.8)
6 (1.3)
0.52
DDEVICE RELATED
Mechanical
40 (8.8)
34 (7.5)
0.31
Fluid Leak
35 (7.7)
25 (5.5)
0.11
Puncture
30 (6.6)
25 (5.5)
0.35
Inadequate Size/Shape
15 (3.3)
21 (4.6)
0.38
Other2
17 (3.8)
14 (3.1)
0.48
1: adhesion, allergies, discomfort, fever, fluid discharge, foreign body in patient, hematoma, hematuria, hernia, obstruction/occlusion, pain, perforation, retention, scar tissue, sepsis, urethral stenosis/stricture. 2: device contamination, improper use of device, malposition of device, migration, unrelated.
Adolescent Medicine and General Pediatrics II
Concurrent Session
8:00 AM
Friday, January 19, 2024
# 316
Screening and intervention for adolescent opioid use disorder in the emergency department
Buresh C1, 2. 1Seattle Children’s Hospital, Seattle, WA and 2University of Washington, Seattle, WA
Purpose of Study: The United States is experiencing a large increase in overdose deaths amongst adults and teenagers, with adolescent deaths from overdose rising more than 200% since 2019. The majority of these overdose deaths are related to illicitly manufactured fentanyl. It has been shown that having more naloxone available within a community leads to lower rates of death from overdose and that starting people with opioid use disorder (OUD) on medications to treat opioid use disorder (MOUD), such as buprenorphine or methadone, can decrease the rates of death by 40-60%. This initiative was designed to increase screening for OUD amongst a population that uses the pediatric emergency department (ED) in order to identify adolescents who may benefit from further targeted intervention. Interventions that were studied were the provision of naloxone from the emergency department and prescriptions for buprenorphine.
Methods Used: This project took place at an academic pediatric emergency department that sees approximately 40,000 patients per year. In the initial phase a mandatory training was developed for all medical staff and deployed, accompanied by live education sessions at staff meetings and faculty meetings. In the second stage, we sought to screen adolescents by identifying presenting Chief Complaints (CC) that may be related to OUD. We then built an automated alert in the electronic medical record, a Best Practices Alert (BPA), that notified clinicians that the patient may require further screening based on their presenting CC. The BPA went live on October 27, 2022 and was used by clinical staff. In the background of these efforts, the state passed a law on January 1, 2022 that all patients at risk of harm from an opioid had to be discharged from emergency departments with naloxone in hand.
Summary of Results: At baseline naloxone was distributed an average of 0 times per quarter in the pediatric emergency department and no buprenorphine was prescribed. With the initiation of department wide required education on OUD and MOUD naloxone was distributed 7.4 times per quarter and buprenorphine was prescribed 1.4 times per quarter on average. With the implementation of the state law rates of naloxone dispensing went up to 22.7 times per quarter and buprenorphine prescriptions rose to 8 times per quarter. In phase 2 when the BPA went live rates of naloxone prescribing nearly doubled to 41.5 times per quarter while rates of buprenorphine prescribing dropped slightly to 5.8 times per quarter.
Conclusions: This study demonstrates that opioid use disorder is a significant problem among the adolescent population that was under-recognized in this department. Increasing education and screening using the electronic medical record can increase rates of recognition of OUD. Increased screening leads to higher rates of naloxone distribution and initiation of MOUD. Legislation that mandates the distribution of naloxone from the emergency department is very effective at increasing rates of dispensing.
# 317
Parents’ Perceptions of Social Needs Screening after Pediatric Hospital Discharge
Hollo A1, Mason N1, Gupta R1, Gambino J2, Thomas J3, Brittan M3. 1University of Colorado, Denver, CO; 2Childrens Hospital Colorado, Aurora, CO and 3University of Colorado, Aurora, CO
Purpose of Study: Social determinants of health (SDOH) have a significant impact on the health and development of children. Thus, hospitals should consider screening for SDOH and referring to community-based organizations to provide more comprehensive care. While several studies have evaluated screening outcomes during hospitalization, few have evaluated families’ perceptions of screening and connection to community resources following discharge. The purpose of this study is to examine patient and family perceptions of SDOH screening and factors associated with families’ connection to socio-economic resources after pediatric hospital discharge.
Methods Used: A post-discharge phone survey was conducted of families who had been screened during their child’s admission to a free-standing children’s hospital. Families were screened on six social needs (SN) categories: financial concerns, keeping appointments, filling prescriptions, food insecurity (FI), benefits, and housing insecurity. Screen-positive families were offered community-based referrals and resources during the hospitalization. Phone surveys were conducted two weeks post-discharge to assess parents’ perceptions of SN screening, connection to resources, and perceived helpfulness of these resources. Demographic and screening characteristics were compared between families who reported connecting or not connecting to resources using Pearson’s chi-square, Fishers Exact, or Wilcoxon Rank Sum tests.
Summary of Results: Out of 37 families surveyed post-discharge, 23 (62%) had a positive SDOH screen during the hospitalization. Of these, 13 (56%) reported connecting to community resources after discharge, while 8 (35%) did not connect, and 2 (9%) did not disclose. Twelve (92%) of the 13 families that reported connecting to resources found them to be helpful (Fig 1). Families reporting a connection to resources screened higher for positive SNs (3 vs. 1; p=0.01) and were more likely to screen for FI (54% vs. 0%; p=0.018) during hospitalization than families who reported not connecting to resources (Table 1).
Study Flow Diagram.
Conclusions: Despite a small sample size, our results indicate that most families find inpatient SDOH screening and resource referral to be acceptable and beneficial. Certain screening characteristics may correlate with post-discharge linkage to resources, though further study is needed to explore why families may not connect with offered resources.
Demographic and Screening Comparisons Between Groups.
Variable
Not Connected
n=8
Connected
n=13
P-value
Screening Characteristics
Positive Screen in SN or Barrier Categories, N=6 (Median, IQR)
1.0 (1.0-2.0)
3.0 (2.0-4.0)
0.010
1. In the last 3 months, did you ever feel stressed about making ends meet?Yes, n (% of total)
5 (63%)
11 (85%)
0.325
2. Do you have any concerns or problems that make it hard for you to keep your child
3 (38%)
6 (46%)
>0.999
3. Do you ever worry about not being able to fill your child
1 (12.5%)
1 (7.7%)
>0.999
4. In the last 3 months, did you ever worry that your food would run out before you had money to buy more?
0 (0%)
7 (54%)
0.018
5. Are you worried about your benefits right now? For example, have your benefits been denied, reduced, or eliminated or do you need help renewing your benefits?
3 (38%)
8 (62%)
0.387
6. Do you have concerns about your housing or becoming homeless?
0 (0%)
2 (15%)
0.687
Demographics
Child’s Sex: Female
2 (25%)
5 (39%)
0.656
Male
6 (75%)
8 (61%)
Home Zip Code: Urban
7 (88%)
11 (85%)
>0.999
Rural
1 (12%)
2 (15%)
Child’s Insurance: Public/Charity
4 (50%)
9 (69%)
0.646
Commercial
4 (50%)
4 (31%)
Education: High School Graduate or Less
1 (12%)
5 (39%)
0.1
Some College or Technical School
2 (25%)
6 (46%)
College Graduate or More
5 (63%)
2 (15%)
Parental status: One-parent home.
1 (12%)
5 (39%)
0.239
Two-parent home.
7 (88%)
6 (46%)
Not answered
0 (0%)
2 (15%)
# 318
DO SPORTS PREPARTICIPATION EVALUATIONS FOR PEDIATRIC PATIENTS FOLLOW RECOMMENDATIONS FROM THE AMERICAN ACADEMY OF PEDIATRICS
Ng T1, Magee-Gonzalez J2, Taylor S3, 4, Shaikh U1. 1UC Davis Health, Sacramento, CA; 2UC Davis School of Medicine, Sacramento, CA; 3UC Davis Clinical and Translational Science Center, Sacramento, CA and 4UC Davis, Sacramento, CA
Purpose of Study: Sports preparticipation evaluations (PPEs) are commonly conducted by primary care clinicians. The American Academy of Pediatrics (AAP) website provides free sports PPE resources, including a medical history form, which outlines questions that clinicians should ask to gather a thorough and relevant medical history for evaluating eligibility for sports participation. This study seeks to determine whether clinicians have been obtaining standard elements of the medical history as recommended by the AAP’s current clinical guidelines.
Methods Used: A retrospective chart review was performed on patients at an academic health center between the ages of 0-21 years who had a sports PPE performed between January 1, 2022 to December 31, 2022. Descriptive statistics were performed to analyze patient demographic and clinician characteristics. Compliance with documenting elements of the medical history was summarized across all patients, and the percentage of elements documented for each patient (i.e., overall compliance) was calculated and summarized as a mean. A robust covariance matrix was used to account for within-provider correlation in calculating standard error. A linear regression with robust covariance matrix was used to test for differences in overall compliance between clinicians in family medicine vs. pediatrics and between attending and resident physicians.
Summary of Results: 365 patients participating in 25 sports were included in this analysis. The mean age was 14.38 (SE=2.69). 62.7% of patients were male and 37.3% were female. Attendings physicians (79.5%) comprised the majority of clinicians, followed by resident physicians (18.6%) and nurse practitioners/physician assistants (1.9%). Sports PPE encounters were evenly distributed between family medicine clinicians (50.4%) and pediatric clinicians (49.6%). The mean percentage of elements documented across all patients was 28.6% (SE=0.74) with a range of 0% to 70.8%, and the median was 28% [IQR=16.7, 37.5]. The most documented element was past medical history (79.2%), and the least documented elements were special equipment (0.3%) and protective equipment (0.3%). There was no difference in overall compliance between attending and resident physicians (p = 0.12). However, family medicine clinicians (mean=30.1 [SE=1.1]) had slightly higher compliance (p=0.044) than pediatric clinicians (mean=27.1 [SE=0.9]).
Conclusions: Based on this dataset, clinicians are only documenting about one-third of the medical history elements recommended by current clinical guidelines. Future endeavors should focus on identifying barriers and facilitators to conducting sports PPEs that follow the AAP’s clinical guidelines.
Percentage of clinicians documenting each element of the medical history.
Overall (N=365)
Injury or illness
33 (9.0%)
Past medical history
289 (79.2%)
Medications
175 (47.9%)
Allergies
129 (35.3%)
Dizziness
49 (13.4%)
Sudden death
148 (40.5%)
Syncope during exercise
68 (18.6%)
Syncope after exercise
14 (3.8%)
Chest pain
149 (40.8%)
Palpitations
103 (28.2%)
Marfan syndrome
66 (18.1%)
Past restriction
14 (3.8%)
Skin problems
119 (32.6%)
Head trauma
175 (47.9%)
Nerve injury
25 (6.8%)
Heat illness
19 (5.2%)
Respiratory symptoms
194 (53.2%)
Special equipment
1 (0.3%)
Vision
148 (40.5%)
Musculoskeletal injury
179 (49.0%)
Weight concerns
17 (4.7%)
Stress
147 (40.3%)
Immunizations
235 (64.4%)
Menstrual history (Females)
50 (36.8%)
Protective equipment
1 (0.3%)
# 319
REVOLUTIONIZING ADOLESCENT HUMAN IMMUNODEFICIENCY VIRUS SCREENING: PAVING THE WAY FOR POINT OF CARE TESTING IN PEDIATRIC CLINICS
Abutouk M, Pina G, Davidge R. Loma Linda University, Loma Linda, CA
Purpose of Study: Pediatricians play a key role in preventing Human Immunodeficiency Virus (HIV) by offering routine HIV testing. While there has been great progress in treatment for patients with HIV and AIDS, many adolescents still believe they are not at risk for HIV and have never been tested. Recent studies have shown that almost half of adolescents who have HIV are undiagnosed. A key barrier to screening adolescents for HIV during clinic well child visits includes patient follow through with HIV screening lab work. Traditionally, this requires a visit to the lab, serum draw, followed by waiting hours to days for a result. We sought to eliminate this barrier by implementing a rapid point of care (POC) HIV oral swab during adolescent well child visits with anticipation of increasing our overall HIV screening rates.
Methods Used: All adolescent patients ages 15-18 who presented to clinic for well child check and had not yet tested once in their lifetime for HIV were eligible.
Interventionsincluded creating a website with educational curriculum for physicians and ancillary staff regarding HIV screening guidelines and functionality of the HIV POC swab and resources for families and providers. A multidisciplinary team was created to ensure efficiency of implementation of the screening test into the clinic workflow.
The primary outcome measure was the monthly percentage of adolescents ages 15-18 who were screened for HIV via the POC swab during their well child visit.
Summary of Results: We found a statistically significant difference between the proportion of patients screened for HIV before and after the availability of POC HIV swab testing in clinic with p=0.007.
Prior to implementation, the year-to-date percentage of those screened among eligible patients from January 2023 to July 2023 was 24% (64/267). Within one month of implementation of the HIV POC swab the percentage of adolescents screened increased to 45 % (17/38).
Conclusions: Improving HIV screening among adolescents is feasible and effective through the use of point of care rapid antibody testing. This type of testing is painless for patients, can be quickly performed during clinic visits, and improves patient confidentiality as results are available at time of visit instead of traditionally waiting for the results by phone or email. Furthermore, Medi-cal currently covers POC testing for HIV so this form of testing could be used in many clinics.
# 320
PARENT PERSPECTIVES ON PEDIATRIC INTERVENTIONS TO ADRESS ADVERSE CHILDHOOD EVENTS
Mangunsong J2, Marie-Mitchell A1. 1Loma Linda University, Loma Linda, CA and 2Loma Linda University, Loma Linda, CA
Purpose of Study: Adverse childhood experiences (ACEs), such as parental divorce, mental health problems, substance use problems and child maltreatment- are common and can have long term consequences over the lifespan. Pediatric practices have an opportunity to intervene by connecting families to community resources, supporting parent resilience, and providing information about child development. However, there is much that remains unknown about how to successfully design and implement interventions to support children with ACEs through pediatric practice. The purpose of this project was to solicit parent feedback about barriers to participation in support programs, best methods for sharing information with families, and any other feedback regarding interventions.
Methods Used: Our target population for this project was the parents of pediatric patients who had presented for recent well-child care visits at an urban federally qualified health center in southern California. Parents were recruited to participate in Family Voice group meetings or individual telephone interviews. Through either modality, parents were solicited for their input regarding the development and implementation of two types of programs: 1) Family mentors who provide 1:1 support and information about community resources; and 2) Family classes which provide group support and a curriculum about nurturing healthy relationships at home. A $5 gift card was offered to each participant as a thank you for participation. A total of four data collection periods took place between October 2021 and August 2023. This project was approved by our institution’s human subjects committee.
Summary of Results: A total of 46 parents participated in focus groups or interviews, most of whom were mothers. About 63% of participants were Hispanic and about 15% were Spanish-only speakers. Two main themes were identified as barriers to participation in interventions for ACEs: provider descriptions and parent availability. Regarding methods for sharing information, explanations by nurses and doctors in the clinic, posting fliers at the clinic, calling or texting families after their visits at the clinic, and posting on social media were considered effective strategies by most participants. Additional feedback regarding interventions was centered around the fact that most parents had "no prior knowledge of ACEs" (Table 1).
Conclusions: This qualitative study described parent perspectives on the design and implementation of pediatric interventions to support children with ACEs. We identified key themes related to strategies to overcome barriers to participation and optimizing methods for sharing information. We highlighted insights from parents, including the importance of addressing lack of understanding about ACEs, fears about health care interventions, and pragmatic details related to communication and incentives. This feedback from parents can be used by pediatric practices to optimize success in connecting families with ACEs to community resources.
Examples of Parent Responses to Open-ended Questions.
Question
Response
Thoughts regrading referrals to CHWs (Community Health Workers)?
“Parents may be afraid of working with CHWs due to fear of what they say being used to take their children away”
To help with this, the term “CHW” should be changed to “mentor”
Best time for family classes?
Weekends or weekdays, mornings or evenings
Virtual sessions to address lack of transportation of lack of childcare
Background info/understanding of ACEs?
Most parents did not have knowledge about what ACEs were
How to reach hard to reach families?
“Some parents don’t want to admit that there is an issue or that they are in need of help. When you show them statistics/ facts then they are more likely to listen”
Provide handouts summarizing helpful/important information
Emphasize that “it shows strength to ask for help”
“Make them feel listened to, comfortable and heard”
Small gift suggestions for children?
Toys, books, arts/crafts, chocolate
# 321
Navigating Identity Development and Psychological Adaptation in Adolescents with Genetic Conditions: Considerations for Genetic Counselling and Adolescent Medicine
Wainstein T2, 3, Austin J1, 2, Elliott A2, 3. 1University of British Columbia, Vancouver, BC, Canada; 2University of British Columbia, Vancouver, BC, Canada and 3BC Children’s Hospital Research Institute, Vancouver, BC, Canada
Purpose of Study: Existing literature indicates that genetic counselling for adolescents necessitates an approach distinct from that used with adults, consistent with adaptations made for this population in other health spheres. Developing best practices for adolescent genetic counselling is crucial, considering the growing number of disabled adolescents worldwide, the need to be mindful of their cognitive and emotional development, and increasing utilization of genetic/genomic testing early in life. We investigated the perceptions of adolescents (10-19 years) who had been diagnosed with a genetic disorder in terms of how they describe receiving, understanding, and living with a genetic condition.
Methods Used: We undertook a cross-sectional, qualitatively oriented mixed methods study in British Columbia, Canada. Eighteen participants (median age: 15.5y; 61% women; 56% White; 72% typical cognition; 44% de novo presentation) completed two quantitative survey measures (psychological adaptation scale (PAS) and illness identity questionnaire (IIQ)) and participated in semi-structured interviews.
Summary of Results: Participants had a mean PAS of 3.07 (SD=0.84) indicating adequate adaptation; their IIQ profiles indicated slightly better mean adaptive scores (3.10; SD=1.06) than mean maladaptive scores (2.85; SD=0.99). We developed a conceptual model that incorporates both identity as a person with a genetic condition and disability identity and consists of three interacting components: (i) an internalized process, (ii) variability arising from contextual factors, and (iii) external factors that impact the process. The internalized process generally followed a trajectory through four statuses (i.e., initiating, minimizing, exploring, and accepting), however movement across these statuses took place frequently because of contextual factors like location and type of disability. Communication and engagement with caregivers, family, peers, teachers, and healthcare providers; social interactions with others who have the same or a similar condition; and the impact of ableism constituted the main external factors with which adolescents engaged in the development of their disability identities. Statistically significant differences were identified among the four internalized statuses and the coping efficacy and social integration sub-scales of the PAS, and the engulfment sub-scale of the IIQ, reflecting their possible value in assessing adaptation to a genetic condition and targets for intervention.
Conclusions: Our findings present a foundation upon which to develop a genetic counselling process that is optimized for adolescents with genetic conditions. Enhancing access to clinical genetic services that includes genetic counselling as a means of facilitating positive identity development is an important goal. Our results underscore the need for the integration of genetic counsellors into the multidisciplinary teams who care for this population in adolescent medicine and other youth services to achieve this goal.
Cardiovascular III
Concurrent Session
8:00 AM
Friday, January 19, 2024
# 322
The Outcome of Biopsy Negative Rejection After Heart Transplantation: Does Severity of BNR Matter?
Hu J, Singer-Englar T, Kanungo A, Bhatnagar N, Hamilton M, Kobashigawa J. Cedars-Sinai Heart Institute, Los Angeles, CA
Purpose of Study: Biopsy negative rejection (BNR) after heart transplantation is described as the development of cardiac dysfunction (LVEF less than 40%) without evidence for rejection on the heart biopsy. BNR can be associated with hemodynamic compromise (HCR) characterized as a need for inotropic/presser support. It is not clear whether the severity of BNR compromises subsequent 1-year outcome. We compared heart transplant patients with BNR to a contemporaneous control group without BNR.
Methods Used: Between 2010 and 2018 we assessed 210 heart transplant patients who developed BNR. These patients were then divided into those that demonstrated HCR and those that did not. Both study groups were then compared to a contemporaneous control group without BNR. End points included subsequent 1-year survival, freedom from CAV, non-fatal adverse cardiac events (NF-MACE: myocardial infarction, new congestive heart failure, percutaneous coronary intervention, pacemaker/implantable cardioverter defibrillator placement, stroke), cardiac dysfunction, recurrence of BNR, newly developed ACR/AMR.
Summary of Results: Heart transplant patients who developed BNR with or without hemodynamic compromise had significantly poorer subsequent 1-year survival compared to the control group. Comparing the two BNR groups (with HCR and without HCR), there was no significant difference in subsequent 1-year survival, NF-MACE, cardiac dysfunction, freedom from ACR/AMR, or recurrent BNR.
Conclusions: BNR after heart transplantation, whether it is associated with hemodynamic compromise or not have poor outcome after this event. Further studies into the mechanisms of BNR and needed intervention are ongoing.
BNR with HCR(n = 24)
BNR without HCR (n = 46)
No BNR (n =140)
P-value
Subsequent 1-year survival
70.8%
60.8%
94.2%
<0.001
Subsequent 1-year freedom from CAV
95.8%
86.9%
95.7%
0.060
Subsequent 1-year freedom from ACR
91.6%
95.6%
94.2%
0.767
Subsequent 1-year freedom from AMR
100%
100%
96.4%
0.338
Subsequent 1-year freedom from NF-MACE
54.1%
73.9%
95.0%
<0.001
Subsequent 1-year freedom from cardiac dysfunction (LVEF <= 40%)
12.5%
50.0%
93.5%
<0.001
Subsequent 1-year freedom from BNR
70.8%
76.0%
100%
<0.001
# 323
Does Donor Diabetes Lead to Poor Outcome After Heart Transplant?
Patel R, Singer-Englar T, Kanungo A, Bhatnagar N, Hamilton M, Kobashigawa J. Cedars-Sinai Smidt Institute, Los Angeles, CA
Purpose of Study: Diabetes is a well-known risk factor for the development of atherosclerosis in non-transplant patients. Diabetes can lead to endothelial cell dysfunction in native coronary arteries which results in myocardial infarction and subsequent cardiac dysfunction. Outcome of donor hearts from diabetics has not been well established after heart transplantation (HTx). Furthermore, the impact of insulin-dependence vs. oral diabetic medications in the donor is not clear. Therefore, we elected to assess our large patient population to assess for diabetes in the donor and assess for outcomes after HTx.
Methods Used: Between 2010 and 2017, we assessed 776 HTx patients and queried the donor records as to the presence of diabetes. The diabetic donors were further divided into those on insulin or oral hypoglycemic agents, Endpoints included post-transplant 5-year survival, freedom from development of CAV (≥30% stenosis by angiography), freedom from non-fatal major adverse cardiac events (NF-MACE: myocardial infarction, new congestive heart failure, percutaneous coronary intervention, pacemaker/implantable cardioverter defibrillator placement, stroke), freedom from cardiac dysfunction (LVD defined as LVEF ≤40%), and freedom from development of restrictive physiology (suggestive of microvascular disease). 1-year outcomes included freedom from the development of acute cellular rejection (ACR) and antibody-mediated rejection (AMR).
Summary of Results: HTx patients receiving donor hearts from diabetics compared to those without diabetes had a significantly lower freedom from 5-year NF-MACE and a trend for a lower freedom from the development of restrictive physiology. There was a trend for diabetic donors on insulin (vs oral agents) to have a lower 5-year freedom from LVD. There were no significant differences between study groups for 5-year survival, freedom from CAV, and 1-year freedom from ACR/AMR. (see table)
Conclusions: HTx patients who received a donor with diabetes had increased risk to develop restrictive physiology suggestive of microvascular disease. Diabetic donors on insulin therapy may have additional risk for LVD. Further studies are needed to assess interventions to prevent these complications.
Table 1
Donor DM (n=43)
No Donor DM (n=733)
P-value
5-year survival
79.0%
80.2%
0.806
5-year freedom from CAV
97.6%
95.7%
0.564
5-year freedom from NF-MACE
62.7%
76.3%
0.048
5-year freedom from LVD
76.7%
74.4%
0.780
5-year freedom from restrictive physiology
79.0%
88.5%
0.059
1-year freedom from ACR
90.6%
91.8%
0.756
1-year freedom from AMR
93.0%
94.1%
0.745
Table 2
Insulin Dependent (n=18)
Not Insulin Dependent (n=25)
P-value
5-year survival
83.3%
76.0%
0.458
5-year freedom from CAV
94.4%
100%
0.288
5-year freedom from NF-MACE
66.6%
60.0%
0.391
5-year freedom from LVD
61.1%
88.0%
0.074
5-year freedom from restrictive physiology
77.7%
80.0%
0.892
1-year freedom from ACR
88.8%
92.0%
0.835
1-year freedom from AMR
88.8%
96.0%
0.405
# 324
5-year Outcome After Coronary Stent Placement in Heart Transplant Recipients
Cristobal C, Singer-Englar T, Bhatnagar N, Kanungo A, Hamilton M, Kobashigawa J. Cedars-Sinai Smidt Institute, Los Angeles, CA
Purpose of Study: Cardiac allograft vasculopathy (CAV) is one of the major causes of death long-term after heart transplantation (HTx). The incidence of CAV is reported in more than 30% of all patients within 5 years of HTx. CAV usually is a diffuse process within the donor coronary arteries but occasionally appears in a focal region which is amenable to percutaneous cardiac intervention (PCI) and stent placement. In recent times, drug-eluting stents have been placed which have been known to have increased patency in non-transplant patients. It is not known whether there is acceptable long-term outcome of stents placed 5 years ago and whether specific immunosuppression makes a difference in outcome. We sought to answer these questions in our large patient population.
Methods Used: We assessed 24 HTx patients who underwent drug-eluting coronary stent placement between 2010 and 2019. Endpoints included subsequent 5-year survival and 5-year freedom from repeat PCI intervention. The patients were also sub grouped into those being treated with everolimus/sirolimus (EVL/SIR) or mycophenolate (MMF) immunosuppression. These findings were compared to 428 contemporaneous non-transplant patients undergoing PCI for native coronary artery disease (*Zellweger MJ, J Am Coll Cardiol. 2012;59(9):793-799).
Summary of Results: The average time from heart transplant to the initial PCI was 3.9 ± 2.5 years. In the heart transplant patients compared to non- transplant patients, there was similar 5-year freedom from repeat PCI intervention however subsequent 5-year survival was significantly lower (see table). Heart transplant patients treated with EVR/SIR vs MMF had similar 5-year freedom from repeat PCI intervention and subsequent 5-year survival.
Conclusions: Heart transplant patients requiring drug-eluting stents appear to have acceptable patency of stents at 5 years, but subsequent survival is less due to the known outcome of CAV. The type of immunosuppression did not significantly impact outcome.
Table 1
HTx patients (n = 24)
Non-Transplant patients (n = 428)
P-value
5-year freedom from repeat PCI intervention
91.6%
88.0%
0.595
Subsequent 5-year survival
70.8%
89.9%
<0.001
Table 2
Treated with EVR/SIR (n = 13)
Treated with MMF (n = 11)
P-value
5-year freedom from repeat PCI intervention
92.3%
90.0%
0.900
Subsequent 5-year survival
84.6%
54.5%
0.134
# 325
Concomitant Cell-Free DNA and Donor Specific Antibodies: Do They Predict Outcomes After Heart Transplant?
Kermanshahchi J, Singer-Englar T, Bhatnagar N, Kanungo A, Hamilton M, Kobashigawa J. Cedars-Sinai Smidt Institute, Los Angeles, CA
Purpose of Study: The endomyocardial biopsy has remained the gold standard to detect rejection after heart transplant (HTx), but many non-invasive methods to detect rejection are now available. A recent Biomarkers Consensus Conference in 2022 suggested that donor-derived cell-free DNA (dd-cfDNA) and donor specific antibodies (DSA) are two biomarkers that best correlate to detect rejection. dd-cfDNA is representative of donor heart injury, whereas development of DSA is representative of the upregulation of the immune system. It has not been established whether these biomarkers when combined would have good prediction of rejection.
Methods Used: Between 2010 and 2020, we assessed 165 HTx patients who had both dd-cfDNA (positive is > 0.25%) and DSA (positive is any detection) drawn within 1 month of each other in the first year post-HTx. Patients were divided into subgroups which included dd-cfDNA+/DSA+, dd-cfDNA+/DSA-, dd-cfDNA-/DSA+, and all compared to dd-cfDNA-/DSA- (control group). These groups were compared for the following endpoints: 3-year survival, freedom from development of cardiac allograft vasculopathy (CAV: ≥30% stenosis by angiography), freedom from non-fatal major adverse cardiac events (NF-MACE: myocardial infarction, new congestive heart failure, percutaneous coronary intervention, pacemaker/implantable cardioverter defibrillator placement, stroke), and 1-year freedom from ACR and AMR.
Summary of Results: The detection of dd-cfDNA+ and DSA+ led to an increased risk of AMR in the first year after HTx, although there was no difference in 3-year outcomes (see table). dd-cfDNA+ alone but not DSA+ alone was significant to predict AMR compared to the control. The average time from transplant to the detection of a positive dd-cfDNA or positive DSA was 26.0 ± 14.1 weeks. The average time from cfDNA+/DSA+ to the detection of rejection (AMR) was 5.3 ± 4.9 weeks. The average time from cfDNA+/DSA- to the detection of rejection (AMR) was 12.1 ± 13.2 weeks.
Conclusions: Positive dd-cfDNA and DSA can best predict the development of rejection after HTx. More aggressive anti-rejection therapies should be pursued to alter outcome when both positive dd-cfDNA and DSA are detected.
dd-cfDNA+/DSA+ (n=10)
dd-cfDNA+/DSA- (n=26)
dd-cfDNA-/DSA+ (n=10)
dd-cfDNA-/DSA- (n=112)
1-year subsequent freedom from ACR (grade 2-3)
100%
(p=0.612)
96.1%
(p=0.753)
100%
(p=0.753)
97.3%
1-year subsequent freedom from AMR (pAMR 1-3)
80.0%
(p<0.001)
92.3%
(p=0.003)
100%
(p=1.00)
100%
3-year subsequent survival
100%
(p=0.481)
88.5%
(p=0.237)
100%
(p=0.448)
94.6%
3-year subsequent freedom from CAV
90.0%
(p=0.436)
88.4%
(p=0.159)
100%
(p=0.510)
94.5%
3-year subsequent freedom from NF-MACE
100%
(p=0.506)
87.5%
(p=0.102)
100%
(p=508)
95.3%
3-year subsequent freedom from cardiac dysfunction
90.0%
(p=0.968)
96.1%
(p=0.503)
100%
(p=0.448)
93.6%
p-value: compared to dd-cfDNA-/DSA- group.
# 326
IMPACT OF ANTHROPOMETRIC FACTORS AND PATHWAY GEOMETRY ON POSTOPERATIVE HEMODYNAMICS IN EXTERNAL PERICARDIAL LATERAL TUNNEL FONTAN SURGERY
Nguyen K1, Razzouk J1, Nageotte S2, Lee J2, Razzouk A3, Fortuna R3. 1Loma Linda University School of Medicine, Loma Linda, CA; 2Loma Linda University, Loma Linda, CA and 3Loma Linda University, Loma Linda, CA
Purpose of Study: The external pericardial lateral tunnel Fontan (EPLTF) is a variant of the Fontan operation for single ventricle palliation. Unlike other alternatives, the EPLTF is created using viable, autologous pericardium that is capable of undergoing changes in both size and shape as patient growth occurs. We investigated differences in the postoperative cardiovascular condition of patients who underwent EPLTF surgery with respect to time after surgery, patient anthropometric characteristics, and pathway geometry.
Methods Used: Retrospective review of cardiac catheterization studies following EPLTF surgery was conducted. Pathway dimensions were assessed using cardiac catheterization imaging. Minimum and maximum diameters were measured in both the anteroposterior and lateral views. These measurements were used to calculate minimum and maximum cross-sectional areas, with the maximum to minimum area ratio serving as an indicator of pathway uniformity. All measurements of pathway dimensions were indexed according to body surface area. For the analysis, cases were separated into “Optimal Fontan” and “Suboptimal Fontan” groups on the basis of hemodynamic criteria. “Optimal Fontan” cases were defined as ones having a Fontan pressure less than or equal to 12 mmHg and a cardiac index greater than or equal to 3 L/min/m2. The two groups were compared with respect to time after surgery, height, weight, body mass index (BMI)-for-age percentile, and pathway uniformity using an independent sample t-test with Levene’s test for equality of variances. A p-value less than 0.05 was deemed statistically significant.
Summary of Results: A total of 231 catheterization studies from 158 patients were reviewed. Significant differences were found between the study groups with respect to time after surgery (p = 0.004), height (p = 0.008), weight (p < 0.001), and BMI-for-age percentile (p = 0.011). Pathway uniformity did not differ significantly between the groups (p = 0.684).
Conclusions: For patients undergoing EPLTF surgery, time after surgery, height, weight, and BMI-for-age percentile may influence postoperative hemodynamic conditions. Pathway uniformity did not appear to influence postoperative hemodynamic conditions in this population. Long term follow-up and metabolic health should be prioritized in order to help preserve ideal hemodynamics in patients following Fontan surgery.
Comparison of Optimal and Suboptimal Fontan Groups.
Variable
Optimal Fontan
Suboptimal Fontan
Two-Sided p-value
Time after Surgery (y)
7.36 ± 3.60
8.92 ± 4.90
p = 0.004
Height (cm)
131.53 ± 19.39
139.53 ± 25.87
p = 0.008
Weight (kg)
31.26 ± 13.35
43.91 ± 25.09
p < 0.001
BMI-for-age Percentile (%)
47.60 ± 28.39
58.33 ± 32.44
p = 0.011
Ratio between Areas
2.80 ± 1.85
2.90 ± 1.64
p = 0.684
Data is presented as mean +/- standard deviation.
# 327
EFFECTS OF GENERAL ANESTHESIA ON LEFT VENTRICULAR SYSTOLIC FUNCTION
Arif H, Li F, Jelacic S, Mackensen B. University of Washington School of Medicine, Seattle, WA
Purpose of Study: The relationship between the induction of anesthesia and left ventricular systolic function remains poorly defined. While ejection fraction is a common metric for assessing left ventricular function, it may not capture subtle subclinical impairment. An alternative parameter, left ventricular global longitudinal strain (LV GLS), has demonstrated reproducible sensitivity to systolic function changes. In this study, we hypothesize that the induction of anesthesia leads to an immediate decrease in left ventricular function, as evidenced by a reduction in LV GLS. Understanding the immediate impact of anesthesia induction on left ventricular systolic function is crucial for patient care and surgical outcomes.
Methods Used: This ongoing prospective observational study at the University of Washington Medical Center focuses on eligible patients aged 18 and above undergoing the mitral transcatheter edge-to-edge repair (TEER) procedure. The study commenced in May 2020 and is ongoing, with 49 patients enrolled to date and a target of 75 patients for study completion. For each subject, an experienced sonographer performed peri-procedural transthoracic echocardiograms (TTE) immediately before and after induction of anesthesia. Left ventricular systolic function was assessed using LV GLS analysis through 2D speckle tracking (TomTec Arena, TOMTEC Imaging Systems, Germany). Additionally, we recorded mean arterial pressures, pressor use, and heart rate within 15 minutes before and after induction of anesthesia. Statistical analysis was performed using the R software.
Summary of Results: As of May 2020, 49 enrolled patients undergoing mitral TEER have had pre- and post-induction TTE studies performed. Prior to induction of anesthesia, the mean LV GLS was -12.09% ± 5.02%, which decreased to -11.23% ± 4.42% following induction (p-value = 0.02). In contrast, mean LVEF before anesthesia induction was 52.00% ± 15.11%, and post-induction, it was 51.56% ± 15.83% (p-value = 0.4673). The mean pre- and post-induction blood pressures were 94 ± 18 vs. 85 ± 18 mmHg (p-value < 0.001). Heart rates remained similar (80 ± 16 vs. 81 ± 18 bpm, p-value = 0.4). The observed decrease in LV GLS after anesthesia induction signifies an average reduction in left ventricular systolic function.
Conclusions: In this prospective observational study of patients undergoing mitral TEER, we aimed to elucidate the immediate effects of anesthesia induction on left ventricular systolic function utilizing LV GLS analysis. Previous studies have indicated a reduction in LV GLS following anesthesia induction in subjects without cardiac comorbidities. Our findings provide additional insight by demonstrating a statistically significant reduction in LV GLS after anesthesia induction in patients with cardiac comorbidities. The clinical significance of this decrease in LV GLS warrants further investigation to determine its impact on perioperative management and postoperative outcomes.
# 328
ASSOCIATION OF NEIGHBORHOOD-LEVEL SOCIAL DETERMINANTS OF HEALTH AND LOSS OF GLYCEMIC CONTROL DURING THE COVID-19 PANDEMIC
Sedaghat B1, Kwan A2, Huang T2, Ebinger J2. 1Rosalind Franklin University - Chicago Medical School, North Chicago, IL and 2Cedars-Sinai Medical Center, Los Angeles, CA
Purpose of Study: Chronic disease management was disrupted during the COVID-19 pandemic, and little is known about the differential effects across patient social determinants of health (SDoH). We evaluated the association of SDoH variables with changes in control of Type 2 Diabetes Mellitus (T2D) during the pandemic era.
Methods Used: We performed a retrospective study of adult patients continually followed at a large academic healthcare system in Southern California between 2018-2022. Using appropriate ICD-10 codes and A1C thresholds, we identified patients with a history of T2D, excluding Type 1 or Gestational Diabetes. We extracted basic demographic (age, sex, race, ethnicity) and clinical (comorbidities, BMI) data, as well as A1C values during the study period; next we classified patients as having controlled (A1C<7.0%) or uncontrolled (≥7.0%) T2D in the pre-pandemic (1/1/2018-3/20/2020) and post-pandemic (1/1/2022-12/31/2022) eras. Time thresholds were selected based on regional implementation of emergency health measures (3/20/2020) until the return of primarily in-person visits (1/1/2022). We also characterized glycemic control trajectories during the pandemic: remained controlled, gained control, remained uncontrolled, and lost control.
SDoH data was obtained by linking patients’ zip code to an open health equity database provided by the Public Health Alliance of Southern California, the Healthy Places Index mapping tool (HPI; version 3.0). The HPI is a validated compositive score of 23 social indicators of health across 8 SDOH domains. HPI served as our primary predictor variable of which the association with change in glycemic control was evaluated using multivariable logistic regression controlling for baseline patient characteristics.
Summary of Results: A total of 8,115 patients met inclusion criteria of whom 50.3% were male and 14.5% Hispanic. Overall, we observed an increase in mean A1C level for patients with pre-pandemic glycemic control. Nearly 20% of patients with glycemic control had lost control (A1C increased to ≥7%), and only 28.8% of patients had newly gained control. Among patients with pre-pandemic T2D control, factors associated with loss of glycemic control included male sex [1.33 OR, (1.14-1.56 95%CI)] and pre-pandemic A1C levels [10.04, (8.11-12.51)]. Conversely, factors associated with maintaining glycemic control included HPI [0.71, (0.52-0.98)], age [0.77, (0.72-0.82)], hypertension [0.78, (0.65-0.94)] hyperlipidemia [0.76, (0.61-0.95)], and stroke [0.5, (0.26-0.90)].
Conclusions: We identified unique associations and directional trends for T2D glycemic control during the COVID-19 pandemic using basic demographics, clinical characteristics, and zipcode-derived SDOH data. Our study significantly enhances the literature surrounding the pandemic’s impact on chronic disease management in Southern California, and our approach advocates for the integration of neighborhood-level risk and protective factors to improve individual patient care and to refine our public health interventions.
Characteristics of cohort (only those with SDoH data).
Comparing patients with controlled A1C levels (A1C < 7.0) to patients with uncontrolled A1C levels (A1C ≥ 7.0) before COVID-19 pandemic.
# 329
INFECTIVE ENDOCARDITIS AFTER TRANSCUTANEOUS AORTIC VALVE REPLACEMENT (TAVR): HIGHLIGHTING THE NEED FOR REVISED ANTIBIOTIC PROPHYLAXIS GUIDELINES
Hajeh H, Narang VK, Abraham J, Win T. Kern Medical, Bakersfield, CA
Case Report: Infective endocarditis is the infection of the endocardium lining the heart. It is characterized by fever, positive blood cultures and valvular vegetations in many cases and is complicated by septic emboli, valvular abnormalities, perivalvular abscesses and heart failure among other serious complications.
Due to the severity of this disease and its sequelae, prophylactic antibiotic treatment for preventing infective endocarditis is indicated in certain cases including the presence of a prosthetic valve.
Case Description: This is a 51-year-old female with medical history of severe aortic stenosis of bicuspid valve (replaced with a prosthetic valve via Transcutaneous Aortic Valve Replacement TAVR 4 years ago), heart failure with improved ejection fraction, complete heart block (with permanent pacemaker) and hypertension who presented to the hospital with shortness of breath. Her symptoms started 3 months ago where she noticed gradual progression of shortness of breath, lower extremity swelling and inability to lay flat.
During hospitalization, patient was diagnosed with acute on chronic heart failure. A transthoracic echocardiogram was performed and showed worsening of left ventricular ejection fraction (LVEF) from baseline of 55% to 25% in addition to severe stenosis and regurgitation of aortic valve with vegetations and valve dehiscence. It also demonstrated severe tricuspid regurgitation and possible vegetations on the atrial lead of the pacemaker. Blood cultures showed coagulase negative Staphylococcus. Antibiotics were started and patient was transferred for valve and pacemaker leads replacement.
Upon further questioning, patient endorsed that she underwent a dental procedure shortly before her symptoms started and she was prescribed antibiotics for infective endocarditis prophylaxis before the procedure.
Discussion: Infective endocarditis is a well-documented sequelae of dental procedures. The risk of developing this complication is high in patients with prosthetic valves and guidelines recommend antibiotic prophylaxis.
Aortic valve replacement has seen revolutionary advancements in the past years with the innovation of TAVR. Valves used in TAVR are usually bulkier than the valves placed surgically. In addition, TAVR leaves the native calcified valve that is usually resected in surgical aortic valve replacement SAVR. This theoretically creates a nidus for infections especially after dental procedures.
Revision of the infective endocarditis antibiotic prophylaxis guidelines is warranted after the introduction and wide use of TAVR in medical practice.
Conclusion: TAVR can theoretically create a nidus for infective endocarditis. Revision of the endocarditis antibiotic prophylaxis guidelines is warranted after the introduction and wide use of TAVR in medical practice.
Case Reports I
Concurrent Session
8:00 AM
Friday, January 19, 2024
# 330
SOFT TISSUE CALCIFICATIONS, END-ORGAN RESISTANCE TO MULTIPLE HORMONES, AND COMPLEX INHERITANCE PATTERNS IN A MULTIGENERATIONAL FAMILY
Hall A, Akay G, Viskochil D, Cole SL. University of Utah School of Medicine, Salt Lake City, UT
Case Report: An adolescent male presented to the medical genetics clinic with soft tissue calcifications, central obesity, round facies, short stature, and intellectual disability. His biochemical profile was notable for elevations in parathyroid hormone (PTH) and thyroid stimulating hormone (TSH). His current medications included calcitriol, cholecalciferol, and levothyroxine. The proband’s oldest brother had received both a clinical and a molecular diagnosis based on similar features. Another sibling displayed similar manifestations, but had not yet been formally diagnosed. Many affected family members reported a history of soft tissue calcifications, short stature, intellectual disability, and end-organ resistance to multiple hormones. Some members described osteodystrophy, brachydactyly, hypocalcemia and hyperphosphatemia. Within this multigenerational family, the constellation of clinical, biochemical, and phenotypic features were consistent with pseudohypoparathyroidism-1A (PHP1A) and pseudopseudohypoparathyroidism (PPHP). PHP1A and PPHP represent two of the six phenotypes associated with disorders of GNAS inactivation. Presented in this case is a proband with a previously unreported pathogenic GNAS variant, c.878del (p.Lys293Serfs*42), associated with the presentation of PHP1A. The family pedigree shows an observed pattern of inheritance that reflects a pattern of allele imprinting in affected individuals. A detailed pedigree was obtained from the proband’s mother, who, along with five of her seven siblings, exhibited manifestations of PPHP: soft tissue calcifications without evidence of end-organ hormone resistance. The proband’s maternal grandfather demonstrated features of PPHP due to soft tissue calcifications without evidence of end-organ hormone resistance. Genomic DNA from the proband, brother, and mother was sent for molecular testing for full gene sequencing and deletion/duplication analysis, and was performed per next-generation sequencing protocol. A novel pathogenic variant in GNAS resulting in p.Lys293Serfs*42 was identified in all three samples. The information provided with this family’s molecular testing confirmed a diagnosis of PHP1A in the proband and brother, and PPHP in his mother. The disorders of GNAS inactivation have characteristic clinical, biochemical, and phenotypic features that represent specific parent-of-origin modes of inheritance. The family in this case involved a proband who inherited PHP1A from a maternally-derived inactivating GNAS mutation. The proband’s mother inherited PPHP from a paternally-derived inactivating GNAS mutation. Whether the proband’s maternal grandfather inherited PPHP from his father, or from a novel mutation in GNAS, is unknown. There are reports in the literature that discuss the wide inter-familial and intra-familial phenotype variability that is observed in disorders of GNAS inactivation, even among individuals with the same inactivating GNAS mutation derived from the same parent-of-origin.
# 331
H3F3B-RELATED NEURODEGENERATIVE DISORDER: A NEW CASE REPORT
Chilakamarri L, Enns GM. Stanford University, Palo Alto, CA
Case Report: Purpose of Study: The purpose of this case report is to expand the genotypic and phenotypic data for the newly discovered H3F3B-related neurodegenerative disorder.
Methods Used: Chart review, physical examination, and medical literature review.
Summary of Results: A 13-year-old girl with intellectual delay, epilepsy, hypothyroidism, bilateral conductive hearing loss, hypotonia, and microcephaly was examined in clinic for suspected mitochondrial disease. She was born at term via uncomplicated spontaneous vaginal delivery to a healthy 33-year-old woman. She presented with developmental delays at 4 months of age and developed seizures at 20 months of age. Physical exam was notable for short stature, microbrachycephaly, prominent ears with superior notch, arched eyebrows, midfacial flattening, sparse hair, and small hands and feet. Exome sequencing identified a maternally inherited variant of uncertain significance in NDUFS1, associated with mitochondrial complex 1 deficiency. Muscle biopsy at 4 years of age revealed skeletal muscle with mitochondrial hyperplasia and hypertrophy, following which she received a diagnosis of mitochondrial encephalomyopathy. However, exome re-analysis at the age of 5 years revealed a de novo heterozygous likely pathogenic variant in H3F3B c.88G>C (p.A30P).
Discussion and Conclusions: Both H3F3A and H3F3B encode for Histone Family 3 (H3F3) histones (H3.3), which are replication-independent histones that play a crucial role in epigenetic memory and maintenance of heterochromatin. Somatic pathogenic variants in these genes have been implicated in a number of solid tumors. More recently, H3F3Bgermline heterozygous variants have been noted to cause a neurodegenerative disorder found in 52 patients thus far. These patients present with a core phenotype of progressive neurologic dysfunction, epilepsy, facial dysmorphism, and congenital anomalies. Initial functional studies have demonstrated enhanced binding of H3.3 with the chaperone protein DAXX, which is predicted to disrupt post-translational modifications and lead to aberrant transcription. The variant reported herein has also been identified in one patient in the literature who has similar clinical findings and was diagnosed with Bryant-Li-Bhoj Neurodevelopmental Syndrome 2. Investigation of mitochondrial function has not yet been reported; secondary mitochondrial dysfunction occurs in certain myopathies and neurodegenerative conditions and appears to be possible in H3F3B-related neurodegenerative disorder, but further studies are needed to determine the significance of this finding. Ultimately, the emerging understanding of this neurodegenerative disorder underscores the need for further investigation of molecular mechanisms of this disease process.
# 332
MENKE’S DISEASE: AN OVERVIEW OF THE PATHOPHYSIOLOGY, DIAGNOSIS AND MANAGEMENT
Eckert KL, Martin MM, Shen JJ. UC Davis, Sacramento, CA
Case Report: The patient presented at two weeks of age with hypothermia (93F), lethargy, jaundice and poor feeding and was diagnosed with E. coli meningitis. Physical exam revealed hypotonia and dry, kinky hair. The family history revealed multiple maternal uncles diagnosed with Menkes disease, all of whom had died at ~2 years of age. Molecular testing and clinical details of affected family was not available. A two-year-old brother was healthy and developmentally normal. Maternal prenatal and preconception testing had not been performed.
Labs: Serum Copper (nl 75-153) <10 ug/dL 12 days of age; 24 ug/dL 37 days of age
Serum ceruloplasmin (19-68) 2.6 mg/dL 12 days of age; 9.6 mg/dL 37 days of age
Molecular Testing: ATP7A, Exon 8, c.1933C>T (p:arg645*), hemizygous PATHOGENIC variant. This results in a premature translational stop signal and is expected to result in absent or disrupted protein product.
Background: Menkes disease is an X-linked disorder of copper metabolism resulting from severe loss of function variants in ATP7A, a copper transporting ATPase, and is characterized by early onset (6-8 weeks of age) of progressive neurodegenerative changes, seizures, hypotonia, failure to thrive, “kinky” hair, connective tissue abnormalities and early death. A broad range of severity in clinical manifestations may present; however, severely affected patients typically die before the third year of life. Previous estimates of prevalence ranged from 1/40,000 to 1/354,307, based on clinical ascertainment. However, more recent calculations based on the allelic frequency of deleterious ATP7A variants in a genomic database predicts prevalence as high as 1/8664 live male births with Menkes disease or ATP7A related disorders.
Conclusions: Early recognition and diagnosis, including prenatal diagnosis in families with known disease, is imperative as treatment initiated after the first month of life is associated with poor outcome. Postnatal diagnosis is supported by clinical features and biochemical markers; however, serum copper and ceruloplasmin should be interpreted cautiously as normal newborns may have low levels. Plasma catecholamine analysis, indicative of dopamine β -hydroxylase deficiency, offers a more reliable and expedient method of diagnosis, while awaiting molecular results. Currently, copper-histidine treatment is the only treatment available, but significant barriers exist in accessing treatment in a timely manner. We will discuss the pathophysiology, diagnosis, and management of this disorder and a summary of our patient’s progress to date.
# 333
EXPANDING THE PHENOTYPE OF FUMARATE HYDRATASE DEFICIENCY
Sule AM1, Calderwood L2, Matalon DR1. 1Stanford University, Palo Alto, CA and 2Lucile Packard Children’s Hospital, Palo Alto, CA
Purpose of study: Fumarate hydratase deficiency (FHD; MIM#606812) is a rare autosomal recessive inborn error of metabolism affecting the citric acid cycle due to biallelic pathogenic variants in the FH gene with around 50 cases reported. The clinical presentation includes severe early-onset encephalopathy characterized by failure to thrive, hypotonia, and refractory seizures. Most affected individuals have profound developmental delay and are nonverbal and non-ambulatory. There is a high mortality rate with death commonly occurring in infancy or early childhood, often due to respiratory complications. Here we report a 4 year old Hispanic male with global developmental delay and abnormal brain MRI diagnosed with FHD due to compound heterozygous variants in the FH gene. His lack of seizures, normal growth, and gradual developmental progression, highlights the variability within FHD and adds to the limited reports on milder presentations of FHD.
Methods Used: Chart review, clinical and physical examination, clinical genetic and biochemical testing, literature review.
Summary of Results: A 2-year-old Hispanic male was evaluated for global developmental delay. He smiled at 7 months, sat at 1 year, and rolled around 2 years. Physical exam was notable for a non-dysmorphic child with normal growth, axial hypotonia, appendicular hypertonia, and persistent primitive reflexes. Family history was remarkable for mother with history of right nephrectomy. A brain MRI at 25 months showed nonspecific abnormalities including paucity of the cerebral white matter, thin corpus callosum, delayed myelination, and possible, mild cerebellar hypoplasia. Microarray was negative. Trio exome sequencing revealed compound heterozygous pathogenic and likely pathogenic variants in the FH gene: c.1431_1433dup(p.K477dup) and c.817G>A (p.A273T). Urine organic acid analysis showed massive elevation of fumaric acid consistent with the diagnosis of FHD. He is now 4-years old, non-ambulatory but can take forward steps in a gait trainer and attends a special education classroom. He can say “mama” and “dada” but otherwise babbles and vocalizes to communicate. He continues to make gradual progress and is thus far seizure-free with normal growth parameters and no history of hospitalizations for illness.
Conclusion: FHD is a rare disorder characterized by profound developmental delay, refractory seizures, growth deficiency, and early mortality. Limited reports of individuals with a milder phenotype, later onset of diagnosis and prolonged survival exist in the literature. In the review article by Peetsold et al. 2020, only 10/51 individuals were diagnosed after the age of 1 year. This report highlights the variability associated with FHD and is notable for the lack of seizures, normal growth, and prolonged survival with no other medical or respiratory complications.
# 334
Navigating Sotos Syndrome: A Complex Case With Persistent Gastrointestinal And Endocrine Challenges
Basharkhah S1, Luz D2, Li M1. 1Rush Medical College, Chicago, IL and 2Stanford University, Stanford, CA
Case Report: Previous reports have noted hyperinsulinism in individuals with Sotos syndrome, although it is typically observed in infancy and tends not to persist beyond that stage. This case highlights the challenges and complexities in managing a ten-year-old female with Sotos syndrome, recently diagnosed enzyme deficiencies, and a history of various medical issues, including severe feeding difficulties, insufficient weight gain, and poor glycemic control.
Case Description: The patient, a ten-year-old ex-27-week female with molecularly confirmed Sotos syndrome, had a complex medical history comprising global developmental delay, hyperinsulinemia, severe oropharyngeal dysphagia, chronic constipation, pseudo-obstruction, bronchopulmonary dysplasia, and a history of aspiration pneumonia requiring a tracheostomy. The patient was admitted to the ICU due to failure to thrive. Her admission growth parameters were: weight 20.1 kg (0.02 percentile), length 127 cm (2.15 percentile), head circumference 56.6 cm (97 percentile).
Genetic investigations commenced at age two due to developmental delays. Initial workup with karyotype and chromosome SNP microarray analysis was normal. At the age of three, exome sequencing revealed the presence of a novel de novo pathogenic missense variant (c.5182 G>C, p.A1728P) in the NSD1 gene. Prior to her admission at age ten, endoscopic biopsies indicated the presence of deficiencies in lactase (LCT) and sucrase-isomaltase (CSID) enzymes, suggesting malabsorption issues in the gastrointestinal tract. The subsequent disaccharidase activity panel confirmed deficiencies in three intestinal enzymes. A re-analysis of exome sequencing did not identify any additional genetic alterations.
The goal during her admission was to optimize carbohydrate absorption through adjustments to the patient’s formula. The team continuously monitored her blood glucose levels. Despite adding dextrose fluids, her levels dropped as low as 55 mg/dL intermittently. The patient required Sucraid (sacrosidase) enzyme replacement medication, pending prior authorization. In the interim, she received formula supplemented with parenteral nutrition, allowing a smooth transition to a carbohydrate-free formula . The patient’s weight fluctuated as her formula and nutrition were medically adjusted and optimized, taking into account her enzyme deficiencies. The patient was discharged, awaiting approval while maintaining her weight at 20.8 kg.
Discussion: This case underscores the challenges in managing a ten-year-old with Sotos syndrome, emphasizing feeding, weight gain, and glycemic control difficulties. It also highlights novel enzyme deficiencies impacting gastrointestinal absorption in an older Sotos syndrome patient. These deficiencies likely contribute to severe gastrointestinal symptoms and exacerbate nutritional challenges. Multidisciplinary care remains crucial for Sotos syndrome patients, and research is needed to enhance diagnostics and interventions.
Disaccharidase Activity Panel.
Enzyme
Value
Status
Reference Range
Lactase
1.5
L
>=14.0 nmol/min/mg
Sucrase
10.2
L
>=19.0 nmol/min/mg
Maltase
74.5
>=70.0 nmol/min/mg
Palatinase
3.8
L
>=6.0 nmol/min/mg
Glucoamylase
8.0
>=8.0 nmol/min/mg
In this table: "Value" represents the measured value. "Reference Range" provides the acceptable range for each enzyme’s activity. "L" indicates that the value is lower than the reference range.
# 335
CARBONIC ANHYDRASE DEFICIENCY IN A NEONATE: A CASE REPORT
Null E, Keehan L, Forero Zapata L, Matalon DR, Enns GM. Stanford University, Palo Alto, CA
Case Report: Carbonic anhydrase VA (CA-VA) deficiency (OMIM 615751) is a rare autosomal recessive inborn error of metabolism due to biallelic pathogenic variants in CA5A, leading to aberrant bicarbonate production within the mitochondria due to decreased CAVA enzymatic activity. In 22 previously reported cases, presentation has been characterized by metabolic hyperammonemic encephalopathy, lactic acidosis, hypoglycemia, and ketonuria with generally good prognosis following medical intervention. However, the complete range of initial presentations and long-term prognoses are not fully understood. Here, we report a case of CA-VA presenting in a neonate, the first of Guatemalan descent.
A term female, the first child to nonconsanguineous parents, was born after an uncomplicated pregnancy and developed acute respiratory failure at 18 hours of life. Blood gas analysis showed pH 7.51 (ref 7.35-7.45), pCO2 25 mmHg (ref 35-45), HCO3- of 20 mmol/L (ref 22-26), and a base excess of -3 (ref -2 to +3) indicating a mixed respiratory alkalosis with metabolic acidosis. Blood lactate peaked at 12 mmol/L (<2) and ammonia peaked at 367 mmol/L (ref 56-107). Her presentation was initially concerning for a urea cycle disorder (UCD), organic acidemia (OA), or a mitochondrial disorder. Plasma amino acids showed increased glutamine (3024 nmol/L, ref 5-115) and decreased citrulline (3 nmol/mL, ref 32-143). Acylcarnitine profile showed evidence of mitochondrial dysfunction, and urine organic acids (UOA) showed marked lactate peak and ketones. Ammonia and lactate normalized with administration intravenous dextrose-containing fluids, as well as sodium phenylacetate and sodium benzoate and supplementation with carnitine, riboflavin, vitamin B12, and thiamine. Rapid trio genome sequencing revealed biallelic homozygous missense variants of uncertain significance in CA5A (c.475T>C, p.Trp159Arg). She was discharged on day of life 22 after advancement of enteral feeds without dietary restriction and has not had further attacks of hyperammonemic encephalopathy.
We report another case of neonatal metabolic encephalopathy due to CAVA deficiency who was diagnosed by genome sequencing and showed a typical course of disease with normal development at two months. Although rare, CA-VA may be underreported and should be considered in any child or neonate with marked hyperammonemia, lactic acidosis, hypoglycemia, and ketonuria. Findings on acylcarnitine profile, plasma amino acids, and UOA are non-specific, and absence of abnormalities should not exclude the diagnosis of CA-VA in a patient with a suggestive presentation. Additional cases are needed to better delineate the clinical and biochemical phenotype, provide prognostic information regarding growth, development, and risk for subsequent decompensation episodes, and to further inform optimal clinical management.
# 336
FAMILIAL PARTIAL DELETION WILLIAMS SYNDROME - A CASE REPORT
Parashar K1,2, Bird LM1,2, del Campo M1,2. 1UCSD, San Diego, CA and 2Rady Children’s Hospital, San Diego, CA
Background: Williams syndrome (WS) is a disorder characterized by developmental delay, mild intellectual disability, specific cognitive profile, unique personality characteristics, cardiovascular disease (supravalvular aortic stenosis (SVAS), peripheral pulmonary stenosis, hypertension), connective tissue abnormalities, growth deficiency, endocrine abnormalities (early puberty, hypercalcemia, hypercalciuria, hypothyroidism), and distinctive facies.
Typical Williams syndrome is caused by heterozygous 1.5-to 1.8-Mb deletion at chromosome 7q11.23 involving 26-28 genes. The identification of families with partial deletions of the interval, who only show some manifestations of the Williams syndrome phenotypes, has led to the conclusion that multiple genes (e.g., ELN) appear to be responsible for the phenotypic features of WS. For example, ELN is the only responsible for the cardiac phenotype and mutations in ELN are the cause of isolated SVAS.
Study: We evaluated a six-month-old boy born with mild SVAS. He had normal development till now without any feeding problems, growth delay, or endocrine abnormalities. He had a mild WS facial profile, including periorbital fullness, slightly down slanting palpebral fissures, and epicanthal folds. His chromosomal microarray showed a partial deletion of the 7q11.23 chromosome measuring only 548 KB.
He inherited this deletion from his affected mother, who shares it with her other son, her four sisters, one brother, her father, and one paternal half-sister.
Mom does not have any major neuro-cognitive challenges but she is very sociable and outgoing, a trait she shares with most of her affected family. She has trouble drawing and some visual-spatial problems. His affected half brother and maternal cousin both have some developmental delays and an outgoing personality.
Discussion: Partial deletion in this case involves the ELN gene, the primary gene associated with Williams syndrome, causing elastin arteriopathy, resulting in SVAS. Still, it does not include GTF2I and GTF2IRD1 (TFII-I family of genes), which are associated with the typical neurocognitive profile and some aspects of the gestalt phenotype of WBS.
Since none of the affected family members had calcium/parathyroid, thyroid, or insulin-related metabolic problems, we can conclude that none of the deleted genes are associated with these conditions. As reported earlier, the MLXIPL gene (which codes for carbohydrate response element binding protein) may be a good candidate for a diabetic metabolic profile.
To clearly identify the genes that contribute to each aspect of the Williams Syndrome phenotype, a thorough molecular analysis of all patients with partial deletions is needed. This analysis should include data on the expression of regional genes, as well as comprehensive and consistent clinical phenotyping.
Deleted Genes.
# 337
A CASE OF CONGENITAL GLAUCOMA: EXPANDING THE PHENOTYPE OF USP9X-ASSOCIATED NEURODEVELOPMENTAL DISORDER
Vieta-Ferrer ER1, 2, Huang Y2. 1UCLA, Los Angeles, and 2UCLA, Los Angeles, CA
Case Report: Glaucoma is a group of disorders that are the leading cause of permanent vision loss worldwide. It is characterized by progressive and irreversible optic neuropathy resulting from the death of retinal ganglion cells. Pediatric glaucoma has been estimated to affect between 1 in 10,000 to 1 in 100,000 children worldwide. Studies have found that up to about 13% of patients with childhood glaucoma have an associated systemic abnormality. Patients with congenital glaucoma and other ocular abnormalities have a threefold higher risk of an underlying systemic anomaly when compared to patients with isolated primary congenital glaucoma. To date, only a handful of genes associated with glaucoma have been identified.
In this case, a 2-year-old male presented with hypotonia, developmental delay, congenital glaucoma, iron deficiency anemia, and arachnoid cysts, for which he was evaluated by Ophthalmology and Medical Genetics. He was born at 36 weeks of gestation via cesarean section secondary to maternal hypertension that was unresponsive to medical management. The pregnancy was otherwise uncomplicated, without exposures to toxic substances or infections during the pregnancy. At the age of one month, he was found to have buphthalmos and severely elevated intraocular pressure unresponsive to topical medications, for which he underwent surgical repair. He was also found to have hypertelorism, sparse eyebrows, almond-shaped eyes, epicanthal folds, iris hypoplasia, and corectopia. Trio exome sequencing identified a hemizygous pathogenic variant in USP9X (c.539 C>T, p.P180L) confirming the diagnosis of USP9X-associated neurodevelopmental disorder.
The gene USP9X, located on the X chromosome, encodes a highly conserved deubiquitinase known to play a significant role in brain development and cancer. Pathogenic variants in USP9X have been associated with neurodevelopmental and dysmorphic findings. USP9X has not been previously associated with increased intraocular pressure or glaucoma. Interestingly, previous studies have provided in vitro and in vivo evidence supporting the potential role of USP9X in maintaining protein stability in retinal ganglion cells. Ye and colleagues found that TBK1 inhibited mTORC1 pathway by phosphorylating RAPTOR at a specific serine residue. This blocked the RAPTOR interaction with USP9X, leading to increased ubiquitination and reduced protein stability, specifically in retinal ganglion cells. While this study was designed to evaluate the role of TBK1 in glaucoma, it also provided evidence to suggest that USP9X plays a role in glaucoma. In this study, we report congenital glaucoma as a new phenotype associated with USP9X-related neurodevelopmental syndrome, expanding the phenotype spectrum for this very rare genetic condition, and underscoring the importance of screening such patients for ocular manifestations of the disease.
Endocrinology and Metabolism II
Concurrent Session
8:00 AM
Friday, January 19, 2024
# 338
LOOKING BEYOND BODY MASS INDEX: A PILOT STUDY EXAMINING THE IMPACT OF ADIPOSITY ON FEMALE HEALTH
Ward AM1, 2, Nunez L1, Aguiar Bonfim Cruz A3, Brown AF3, Fehrenkamp B1, 2. 1University of Idaho, Moscow, ID; 2University of Washington School of Medicine, Moscow, ID and 3University of Idaho, Moscow, ID
Purpose of Study: Obesity, defined as a body mass index (BMI) ≥30 kg/m2, is a significant health issue and recent research highlights potential links between obesity and the immune system. Adipocytes function as an endocrine organ, secreting proinflammatory adipokines, contributing to inflammatory conditions, further contributing to chronic inflammatory conditions associated with obesity.
BMI categorizes individuals based on height and weight as Underweight (<18.5 kg/m2), Normal (18.5-24.9 kg/m2), Overweight (25.0-29.9 kg/m2), or Obese (≥30 kg/m2). BMI fails to identify those with excess adiposity, creating a hidden population within the ’normal’ BMI range. This group, Normal Weight Obese (NWO), has a BMI of 18.5≤24.9 kg/m2 but fat mass (FM) ≥30%. Given our evolving comprehension of adiposity’s impact on health, it is crucial to acknowledge and study this hidden population and the chronic health consequences linked to adipose related inflammation.
Our hypothesis posits that females with excess adiposity will exhibit elevated inflammatory markers compared to their lean counterparts. This pilot study’s primary goal was to investigate how excess adiposity relates to inflammation in college-aged females.
Methods Used: Females aged 18-25 years old were recruited from a convenience sample in the U of I Human Performance Lab. Each participant had received a DXA (dual x-ray absorptiometry) scan in the last 5 months. Participants from these studies were classified as Underweight (UW: BMI <18.5 kg/m2), Normal Weight Lean (NWL: BMI 18.5≤24.9 kg/m2, FM <30%), NWO (BMI 18.5≤24.9 kg/m2, FM ≥30%), and Overweight/Obese (OV: BMI ≥25.0 kg/m2) using previously collected data. Data regarding participants’ chronic medical conditions, current medication use, any use of birth control, and a blood sample was collected. Plasma was used for quantification of the cytokines of interest (IL-6, IL-10, TNFα, and IL1β) by Enzyme linked immunosorbent assays (ELISA, R&D systems).
Summary of Results: Twenty-eight participants were recruited, including 1 UW, 11 NWL, 8 NWO, and 8 OV. Results of this study show that there is a higher percentage of adiposity in NWO and OV participants compared to BMI, p<0.0001. No significant difference existed for the NWL and UW ps. Indicating the presence of the NWO category missed by traditional metrics. Cytokine quantification showed no difference between groups; however, vast differences emerged at individual levels. Additional analyses evaluating chronic medical conditions, current medication use, association with menstrual cycle, and current or past use of birth control are in progress.
Conclusions: Our data suggests that BMI does not account for adiposity, especially for college-aged NWO females. However, results relating adiposity to inflammation are inconclusive. Additional studies comparing fluctuations in inflammatory markers throughout the menstrual cycle instead of a single unknown time point are warranted.
# 339
Analysis of Inflammatory Markers in Response to Induction of Reprometabolic Syndrome by a Eucaloric High Fat Diet in Normal Weight Women
Nguyen T1, Kuhn K1, Bolt M2, Bradford A1, Santoro N1. 1University of Colorado School of Medicine, Aurora, CO and 2Colorado School of Public Health, Aurora, CO
Purpose of Study: Obesity in women is associated with a spectrum of metabolic and reproductive endocrine disorders including decreased fertility, adverse pregnancy outcomes, and relative hypogonadotropic hypogonadism, which we term Reprometabolic Syndrome. We have shown that the decrease in LH and FSH levels and impaired response to GnRH observed in women with obesity can be recapitulated, in normal weight women, by administration of a one-month eucaloric high fat diet (HFD). To identify potential mediators of Reprometabolic Syndrome, we examined the impact of the HFD on serum levels of a panel of inflammatory markers and adipocytokines.
Methods Used: 18 healthy, eumenorrheic, women with BMI 18-24.9 kg/m2 were exposed to a one-month, eucaloric, prescribed HFD (48% calories from fat) and underwent a 6-hour frequent blood sampling study in the early follicular phase, before and after consumption of the diet. Serum samples were pooled and analyzed for a panel of inflammation markers using a multiplex immunoassay (Mesoscale Discovery, Rockville, MD). Differences between pre-diet and end of HFD were analyzed by paired t-test.
Summary of Results: A small but significant increase in the anti-inflammatory cytokine IL-10 (p=0.04) was observed in response to the HFD. Eotaxin (p=0.05), IL-6, MIP-1β and IL-1α exhibited similar increases in response to the HFD, which approached statistical significance (p = 0.07). There were no significant differences in levels of CRP or any other cytokines, interleukins, and chemokines tested (Table 1).
Conclusions: Induction of Reprometabolic Syndrome in normal weight women was associated with a significant elevation in the anti-inflammatory cytokine IL-10, which may represent a counterregulatory response to the HFD. Eotaxin, IL-6 and MIP-1β exhibited similar increases in response to the HFD, which approached statistical significance (p=0.07). These cytokines have been linked to obesity, impaired gonadotropin signaling, and infertility. These findings suggest that the chronic increase in multiple inflammatory markers, characteristic of obesity, is not a primary mediator of the relative hypogonadotropic hypogonadism of Reprometabolic Syndrome.
# 340
HYPOTHALAMIC GLIOSIS IS ASSOCIATED WITH MULTIPLE CARDIOVASCULAR DISEASE RISK FACTORS
Lo J1, Melhorn SJ2, 3, Huang A3, 5, Kee S3, Olerich K4, Schur E2, 3. 1University of Washington School of Medicine, Seattle, WA; 2University of Washington, Seattle, WA; 3UW Medicine Diabetes Institute, Seattle, WA; 4University of Washington, Seattle, WA and 5University of Washington, Seattle, WA
Purpose of Study: Hypothalamic gliosis has been linked to obesity and insulin resistance in both rodent models and humans. We tested associations between radiologic markers of hypothalamic gliosis and clinically relevant cardiovascular disease (CVD) risk factors and diagnoses, as well as prevalent coronary heart disease (CHD).
Methods Used: Brain MRIs in 867 adults from the Framingham Heart Study were analyzed. T2 signal intensities were extracted bilaterally from the mediobasal hypothalamus (MBH), amygdala (AMY), and putamen (PUT). T2 signal ratios were created for our primary exposure assessing hypothalamic gliosis (MBH:AMY ratio), a positive control (MBH:PUT ratio), and a negative control (PUT:AMY ratio). Risk factor outcomes included BMI, HDL-C, LDL-C, triglycerides, and hypertension (HTN); prevalent clinical diagnoses outcomes included diabetes mellitus (DM), metabolic syndrome (MetS), and CHD. T2 signal ratios were log-transformed to satisfy conditions of normality and used as predictors in multivariate linear regression or multivariate logistic regression as appropriate. Covariates in fully adjusted models included age, sex, smoking status, risk factor treatment status (e.g., lipids), and BMI (for outcomes except BMI and MetS).
Summary of Results: Mean age was 54.9±8.8 y; 54.9% were female. Greater MBH:AMY ratios were associated with higher BMI (figure 1, P<0.001) and higher triglycerides (P<0.001, without adjustment for BMI). MBH:AMY ratios were associated with presence of HTN and lower HDL-C, independent of BMI (figure 1, both P<0.05). Results were consistent for the MBH:PUT ratios (all P<0.05) but absent for the PUT:AMY ratios (all P≥0.05). MBH:AMY ratios were not associated with DM or CHD in the fully adjusted models (figure 1, both P≥0.05) but were positively associated with MetS (figure 1, P<0.001). The MBH:PUT ratios were associated with MetS (P<0.001), whereas the PUT:AMY ratios were unrelated to any clinical diagnosis (all P≥0.05).
Conclusions: Using a well-established study of CVD development, we found evidence linking hypothalamic gliosis to multiple CVD risk factors independent of BMI, as well as associations with MetS. Novel findings suggest that MBH gliosis is associated with hypertension and dyslipidemia through pathways independent of obesity. Our results highlight the need to consider neurologic mechanisms in efforts to understand and improve cardiovascular health.
MBH:AMY T2 signal ratio coefficients & 95% CIs from fully adjusted models by outcome.
# 341
"DIETARY SUPPLEMENT USE IN INFANTS AND TODDLERS IN THE EXTRAORDINARY BABIES STUDY"
Todd E, Davis S, Brown M, Tartaglia N. Children’s Hospital Colorado, Aurora, CO
Purpose of Study: Dietary supplements are frequently used in children with neurodevelopmental disabilities, with studies reporting 30-50% prevalence of dietary supplement usage. Children with sex chromosome aneuploidies (SCAs) are at risk for neurodevelopmental deficits but dietary supplement use within this population has not been studied. The aims of this study were to describe the prevalence of dietary supplement use for young children with SCA and parent perceptions of safety and efficacy of dietary supplements.
Methods Used: A cross-sectional survey on dietary supplement usage was administered to parents of participants in the eXtraordinarY Babies Study, a natural history study following 298 individuals who were prenatally identified to have an SCA. The survey assessed dietary supplement use for the child as well as maternal use during pregnancy and while breast feeding. Descriptive statistics were used to summarize results; logistic regression was used to determine predictors of supplement use, and the proportion of supplement use was compared to the literature using chi-squared test.
Summary of Results: The overall survey response rate was 88% (n=262) including XXY (n=156), XYY (n=33), XXX (n=60), XXYY (n=9), XXXY (n=2), XXXX (n=1) with the child’s mean age 27.5 +/- 18.5 months at the time of the survey. 173/262 (66.0%) of children with SCA were currently using or had used dietary supplements, significantly higher than previously reported for Trisomy 21 (49%; p=0.015), autism spectrum disorder (42%, p=0.0013) and developmental delays (30%, p<0.001)). Those using supplements had a higher family socioeconomic index (p=0.043), higher maternal supplement use during pregnancy (p<0.001) and breastfeeding (p<0.001), and infants were more likely to have been solely breastfed (p=0.034) than the group not using supplements, but there were no differences by current age, karyotype, race or ethnicity. Parents reported giving supplements to benefit the child’s neurodevelopment, immune health, digestive health, and general health overall. The most used supplements in addition to daily multivitamins vitamins and vitamin D were prebiotics/probiotics, essentially fatty acid supplements, iron, and zinc. No one perceived dietary supplements as unsafe for their child.
Conclusions: Dietary supplement use is common in infants and toddlers with SCAs. Dietary supplement use associated with other variables may be a factor contributing to individual variability in health and development in these conditions and use should be considered as a potential covariate in outcome models. Future research is needed on the objective effects of specific supplements as well as other complementary and alternative therapies in this population.
# 342
AgRP Neuron Inactivation Induces Sustained Amelioration of Hyperglycemia in Diabetic Lepob/ob mice
Gou Y2, Glat M2, Leung A2, Phan BA2, Bryan C2, Mathan SA2, Damian V2, Choi PP2, Watts CA2, Quah E2, Redford IK2, Scarlett J2, 1, Morton G2, Schwartz M2. 1Seattle Children’s Hospital, Seattle, WA and 2University of Washington Medicine Diabetes Institute, Seattle, WA
Purpose of Study: Type 2 diabetes (T2D) is among the most common and costly diseases worldwide. Current medical therapies can effectively lower the blood glucose (BG) level but do not restore the biologically defended BG level to normal. We have previously shown that in Lepob/ob mice and other rodent models of T2D, weeks-long remission of hyperglycemia can be achieved by a single intracerebroventricular (icv) injection of FGF1. Through a series of subsequent studies, AgRP neuron inhibition was identified as a potential mediator of this FGF1 effect. Located in the hypothalamic arcuate nucleus (ARC), AgRP neurons are known to be hyperactive in Lepob/ob mice and other rodent diabetes models. We therefore sought to determine whether the sustained antidiabetic action of icv FGF1 injection in Lepob/ob mice can be recapitulated by inactivation of AgRP neurons.
Methods Used: To permanently inactivate AgRP neurons in a mouse model of T2D, we generated Lepob/ob mice in which cre recombinase is expressed solely by AgRP neurons (Lepob/ob AgRP-cre mice). By microinjecting an adeno-associated virus (AAV) containing cre-inducible tetanus toxin (TetTox)-GFP cassette into the ARC, TetTox expression was induced specifically in AgRP neurons of these mice. Food intake, body weight, blood glucose, and glucose tolerance (intraperitoneal glucose tolerance test (IPGTT)) were monitored, and immunohistochemistry was used to validate viral targeting. Control Lepob/ob mice lacking cre recombinase underwent the same AAV microinjection and monitoring procedures.
Summary of Results: One week after AgRP neuron inactivation, the mean BG level of Lepob/ob AgRP-cre mice fell from 230 mg/dL to 120 mg/dL. Although food intake and body weight also decreased initially, the effect was transient and both parameters returned to baseline by the end of the first week. In contrast, euglycemia persisted for more than 2 months, and glucose tolerance was also normalized by AgRP neuron inactivation in these mice. Immunohistochemistry confirmed that all GFP-expressing cells (which marks cre-induced TetTox expression) colocalize with AgRP immunoreactivity. Data from control groups are pending.
Conclusions: AgRP neuron inactivation recapitulates the sustained antidiabetic effect of icv FGF1 injection in Lepob/ob mice.
# 343
A case of nodular cystic fat necrosis after Whipple procedure
Wittmann JL, Mannering I, Shackelton J. University of Nevada, Reno School of Medicine, Reno, NV
Introduction: Nodular cystic fat necrosis (NCFN) is a rare and distinctive form of encapsulated necrosis of subcutaneous fat. The pathogenesis underlying the formation of NCFN is not completely understood but is thought to be triggered by trauma leading to a sudden vascular insufficiency. The adipocytes become distressed and sequestered from blood supply leading to a fibrous encapsulation of ghost adipocytes and the resulting NCFN. Other authors propose that diabetes mellitus and systemic corticosteroid therapy could play a role in pathogenesis. They speculate that microangiopathy cause local ischemia and suggest that diagnosis of NCFN is suggested to be a dermadrome of Cushing’s syndrome.
Case Presentation: We present a case of a 60-year-old female who presented initially in 2011 with lower extremity swelling and painful bumps for several months occurring after removal of her pancreas in late 2010. Her past medical history is notable for Whipple procedure and removal of a pituitary tumor which subsequently led to the development of Cushing’s syndrome and diabetes mellitus. She was on pancreatic enzyme supplementation and hydrocortisone. Her physical exam revealed edematous lower extremities and evidence of extreme weight loss. Evaluation by vascular surgery determined her findings were inconsistent with lymphedema and venous disease.
A referral was made to dermatology for further evaluation however the patient was lost to follow-up and did not present to clinic until 2018. At this time, she continued to complain of painful bumps now increasing in number but no swelling or drainage. Physical exam showed several firm subcutaneous nodules distributed on the lower and upper extremities and abdomen. The differential diagnosis was broad and included angiolipomas, lipomas, malignancy, and panniculitis. Laboratory work-up showed CBC, CMP, lipase, amylase, and alpha-1-antitrypsin all within normal range. The only notable lab value was elevated glucose at 194 mg/dL and decreased lipase at <3 U/L. A biopsy was done and showed an encapsulated cystic structure with no communication with surrounding vasculature. Ghost adipocytes, lipomembranous changes, and dystrophic calcifications were also noted.
Based on these findings, a diagnosis of nodular cystic fat necrosis was made. The patient was again lost to follow up, returning to clinic 5 years later with the same complaint and findings, but with increased calcification and fibrosis of the nodules. Assessment was that disease is stable with no new lesions and surgical excision would be done for symptomatic lesions.
Discussion: This case demonstrates a unique time course of NCFN due to the extensive, long-lasting nature of the nodules. Two factors could have contributed to its pathophysiology. One being vascular compromise from the Whipple procedure, and the other being her systemic corticosteroid use resulting in diabetes mellitus and Cushing’s syndrome that has been speculated to play a role in the pathogenesis.
# 344
Role of IκBβ in the pancreatic inflammatory response to nutrient-induced stress
Solar M, White A, Wright CJ, Rozance P. University of Colorado Anschutz Medical Campus, Denver, CO
Purpose of Study: Inflammation has been implicated in both the development and the ongoing pathophysiology of diabetes. One of the key regulators of inflammation is the NFκB pathway. We have previously demonstrated that experimentally increasing NFκB activity by lowering the expression of an NFκB inhibitory protein, IκBβ, increased susceptibility to streptozotocin-induced diabetes in mice. However, it was unclear if the increased susceptibility to diabetes in the IκBβ-deficient animals was due solely to immediate injury of the islets by streptozotocin or if impaired glucose or insulin tolerance at baseline or further islet injury from exposure to hyperglycemia also contributed. Therefore, the goal of our study was to determine baseline glucose and insulin tolerance in these animals and determine the inflammatory and apoptotic response of the isolated islets to glucose, palmitate, or a combination of the two. We hypothesized that IκBβ-deficient animals would have normal baseline glucose and insulin tolerance, but their isolated islets would have higher inflammatory and apoptotic responses to nutrient stress.
Methods Used: Adult male B6 (WT) and IκBβ-/- mice were used for glucose tolerance and insulin tolerance tests (n=6/genotype). After a 6 h fast, glucose was measured (0/15/30/60/90/120 min) following injection of glucose (2g/kg) or insulin (0.75 IU/kg). Pooled islets (10 mice per pool; 3 experiments/genotype) were exposed to elevated glucose (16.7mM glucose), 0.5mM palmitate, or both for 24 h. mRNA expression of NFκB target genes, Nfkbia, Cxcl10, Tnf, as well as pro- (Bad, Bax) and anti- (Bcl2 and Bclxl) apoptotic factors were quantified via qPCR. All results were analyzed using ANOVA. Statistical significance was defined as (p<.05).
Summary of Results:In vivo, there was no significant difference between genotypes at any time point throughout the glucose tolerance test. However, the insulin tolerance test demonstrated a significantly greater decrease in glucose for the IκBβ-/- at 60 and 120 min compared to WT. In vitro, elevated glucose exposure resulted in no significant differences in gene expression between groups. In contrast, palmitate exposure resulted in significant upregulation of Nfkbia, Cxcl10, and Bcl2 only in IκBβ-/-. Combination exposure resulted in a significant increase in Nfkbia and Bclxl expression for WT and a significant decrease in Tnf expression for IκBβ-/-.
Conclusions: Our results demonstrate no difference between genotypes in their response to glucose in vivo or in vitro. However, proinflammatory NFκB target genes were increased in IκBβ-/- islets in response to palmitate. Contrary to our hypothesis, IκBβ-/- mice showed an increase in insulin sensitivity. Future studies aim to determine the mechanistic role of IκBβ in the β-cell’s response to palmitate exposure and IκBβ’s role in maintaining normal insulin sensitivity.
# 345
CAN THERMAL IMAGING ASSIST IN EARLY DETECTION OF DIABETIC SMALL FIBER NEUROPATHY?
Duran-Valdez E1, Soliz P2, Saint-Lot S2, Duro T1, Schade DS1. 1University of New Mexico, Albuquerque, NM and 2Vision Quest Biomedical, Albuquerque, NM
Purpose of Study: Early identification of small fiber peripheral neuropathy in individuals with diabetes has the potential to prevent diabetic foot ulcers which affect approximately 1.6 million per year in the United States. The Food and Drug Administration recommends Nerve Conduction Studies as the current gold standard for diagnosing neuropathy. However, it requires skilled medical personnel to conduct the studies and is unable to detect small nerve fiber neuropathy. In this study we compared the use of the Michigan Neuropathy Screening Instrument in addition to temperature changes from Thermal Imaging of the plantar foot vs standardized Nerve Conduction Studies.
Methods Used: 84 subjects diagnosed with type 1 or type 2 diabetes, non-smoking, and without a clinical diagnosis of neuropathy, were consented and enrolled. They were evaluated using Nerve Conduction Studies and scoring from the Michigan Neuropathy Screening Instrument plus Thermal Imaging of the ball of the plantar foot to evaluate sensitivity and specificity in early detection of peripheral neuropathy.Neuropathy was assumed to be present if any of the three tests were positive.
Summary of Results: An indication of large fiber neuropathy was made when Nerve Conduction Studies were positive. However, an indication of small nerve fiber neuropathy was made when Nerve Conduction studies were negative but both thermal imaging and Michigan Neuropathy Screening Instrument were positive. This yielded 80 % sensitivity and 83% specificity for these latter two testing modalities.
Conclusions: The combined results of Thermal Imaging and scores from the Michigan Neuropathy Screening Instrument were more sensitive and specific for detecting neuropathy when compared to Nerve Conduction. Early detection of small fiber neuropathy using thermal imaging and the Michigan Neuropathy Screening test is a new alternative in detecting small fiber neuropathy.
Nerve Conduction
Temperature Recovery + Michigan Neuropathy Screening Instrument
Sensitivity
0.73
0.80
Specificity
0.79
0.83
Accuracy
0.76
0.82
Gastroenterology
Concurrent Session
8:00 AM
Friday, January 19, 2024
# 346
Characterizing the intestinal chondroitin sulfate glycosaminoglycan sulfation code in inflammatory bowel disease
Francis K1, 2, Zheng H1, Suskind DL1, Phan BA2, Nuding M1, Morton G2, Schwartz M2, Alonge K2, 3, Scarlett J1, 2. 1Seattle Children’s Hospital, Seattle, WA; 2University of Washington, Seattle, WA and 3University of Washington, Seattle, WA
Purpose of Study: The current work was undertaken to test the hypothesis that inflammatory bowel disease (IBD) is associated with changes in the intestinal extracellular matrix (ECM) chondroitin sulfate glycosaminoglycan (CS-GAG) sulfation code. CS-GAGs consist of chains of repeating disaccharide isomers, each identified by a unique sulfation pattern that affects mucosal permeability and immune response. Certain CS-GAG isomers promote matrix stability (e.g., CS-A (4S) and dermatan sulfate (DS) (2S4S)), while others are implicated in inflammation and plasticity (e.g., CS-C (6S) and CS-E (4S6S)). Recent evidence linking changes of the ECM to IBD pathogenesis prompted us to determine if intestinal ECM composition, specifically the CS-GAG sulfation signature, is altered in patients with IBD, and if so, whether these changes are responsive to effective IBD therapy.
Methods Used: To decode the intestinal CS-GAG isomer profile, we employed liquid chromatography-tandem mass spectrometry to quantify the abundance of CS-GAG isomers isolated from banked intestinal colonic biopsy samples from 50 pediatric/young adult patients (n=13 control, n=37 IBD with colonic involvement; 38%(f)/62%(m); age range 7-23, age mean 14.1±3.3). Endoscopies on patients with IBD were performed at diagnosis before treatment was initiated and at follow up while in clinical remission (CR).
Summary of Results: In pediatric patients with active, untreated IBD with colonic involvement (IBD at Dx), the abundance of matrix stabilizing isomers in the colon was significantly decreased compared to healthy controls without IBD (Control (n=13) vs IBD at Dx (n=22); CS-A: 76.5 vs 70.2%, p<0.0001; DS: 1.2 vs 0.7%, p<0.0001), while the abundance of pro-inflammatory isomers was increased (CS-C: 18.1 vs 21.9%, p=0.002; CS-E: 1.5 vs 4.1%, p<0.0001). Furthermore, this pattern was largely reversed in those IBD patients in CR at follow up (IBD in CR). Specifically, these individuals exhibited an increase in stabilizing isomers in the colon (IBD at Dx (n=22) vs IBD in CR (n=22); CS-A: 70.3 vs 77.6%, p<0.0001; DS: 0.7 vs 1.0%, p=0.004) and a decrease in pro-inflammatory isomers (CS-C: 21.9 vs 16.6%, p<0.0001; CS-E: 4.1 vs 2.5%, p=0.001). Notably, there were no striking differences in the abundance of CS-GAG isomers between controls and patients with IBD in CR. Across the entire IBD cohort, the abundance of stabilizing CS-GAG isomers inversely correlated with clinical IBD disease activity index scores, and inflammatory isomers were positively correlated with disease severity scores.
Conclusions: These results show that in pediatric patients with active IBD, areas of inflamed bowel associate with a higher percentage of pro-inflammatory CS-GAG isomers and a decreased percentage of stabilizing CS-GAG isomers, an imbalance that is restored upon achieving CR. Ongoing studies seek to determine if pro-inflammatory changes in the intestinal CS-GAG sulfation code serve as a biomarker of IBD risk and/or play a role in IBD pathogenesis.
# 347
An Odd Presentation of Dysphagia Due to Pericardial Effusion
Ipalawatte H, Ahl A, Gower A, Takher J. HCA Los Robles Regional, Thousand Oaks, CA
Case Report: Motility disorders and intrinsic mechanical obstruction most commonly cause esophageal dysphagia. However, extrinsic obstruction, such as pericardial effusion, are rare cause of dysphagia. We present an 89-year-old Male with a history of Waldenstrom macroglobulinemia, Charcot-Marie-tooth syndrome, and basal cell carcinoma presenting with generalized weakness, productive cough, shortness of breath, and dysphagia to both solids and liquids. A chest x-ray obtained showed cardiomegaly with suggested central vascular congestion and pulmonary edema. Further imaging with CT of the abdomen and pelvis showed a moderate to large pericardial effusion. The patient later developed signs and symptoms of cardiac tamponade, requiring urgent pericardiocentesis with the removal of 1L of sanguineous fluid. Up to today, only 6 cases of dysphagia due to pericardial effusion have been described This case displays another rare case and highlights the importance of recognizing dysphagia as a critical symptom as well as non-GI causes of dysphagia.
Computed Tomography of the abdomen and pelvis without contrast showing a moderate-large pericardial effusion (yellow arrows) and small-moderate bilateral pleural effusions (red arrows).
# 348
A PILOT STUDY INVESTIGATING THE EFFECTS OF HUMAN MILK ON INTESTINAL IMMUNE DEVELOPMENT IN A NEONATAL PIGLET MODEL
Badger R1,2, Nunez L2, Fehrenkamp B2. 1University of Washington School of Medicine, Seattle, WA and 2University of Idaho, Moscow, ID
Purpose of Study: Human milk (HM) is considered to be the optimal nutrition source for newborns. It contains a variety of immune cells, beneficial bacteria, and bioactive agents that modify the function of the infant immune system as well as gastrointestinal tract. Like HM, infant formula (IF) provides nearly all essential macro- and micronutrients to support infant growth. However, IF lacks many of the non-nutritive components of HM known to play a role in immune development. In this study, we investigate the effects of feeding intervention on early immune development within a porcine model. Specifically, we are interested in the role of HM in regulating immune cells and promoting the appropriate growth and maturation of gastrointestinal associated lymphoid tissue (GALT). We hypothesized that HM-fed piglets would have more developed GALT than their IF-fed counterparts. We further hypothesized that HM feeding would support a more anti-inflammatory microenvironment within secondary lymphoid tissues.
Methods Used: Neonatal male piglet littermate pairs were assigned to feeding groups: HM-fed (n=6), IF-fed (n=6) and control (n=2). IF-fed piglets received commercially available preterm infant formula, while control piglets were reared on sow’s milk. Piglets were reared for 28 days; intestinal and splenic tissues were harvested and preserved at necropsy. Lymphocyte infiltration into intestines and spleens was then assessed by immunohistochemistry and immunofluorescence. Total T cells were quantified using a pan T-cell marker, while differential B cell staining was used to determine B cell activation status. Additionally, inflammatory cytokine profiles (TNF-alpha, IL-1beta, IL-6, IL-8, and IL-10) were quantified using protein-based techniques. Data analyses (including ANOVA and Tukey post-hoc testing) were carried out using R statistical analysis software.
Summary of Results: Compared to IF-fed and control piglets, HM-fed piglets had more robust lymphocyte populations in both intestinal and secondary lymphoid tissues, including proper T cell infiltration and higher levels of activated B cells. There were significantly higher concentrations of pro-inflammatory cytokines IL-1beta and IL-6 in the intestines of HM-fed and IF-fed piglets compared to control. However, there was no significant difference between HM and IF groups. There were no significant differences in IL-8, IL-10, or TNF-alpha across feeding groups.
Conclusions: These data suggest that HM helps to optimally stimulate the infant immune system and support the development of GALT. However, HM did not strongly influence inflammatory cytokine milieu of either porcine intestinal tissues or spleens compared to other feeding interventions. Together with ongoing transcriptomic and histologic analyses, our findings will help further elucidate the specific mechanisms by which breastfeeding exerts its protective effects and may inform future studies of feeding intervention in human infants.
# 349
Native Splenocaval Shunt in a Cirrhotic Patient
Oliinik M, Floresca J. Loma Linda University, Loma Linda, CA
Case Report: Splenocaval shunts are a portosystemic shunt and can present similarly to other spontaneous portosystemic shunts (SPSS) like splenorenal, splenogonadal, and inferior mesenteric-iliac vein. Splenocaval shunts are considered rare, and the literature on this topic is limited to a few case reports and splenocaval formation procedures. SPSS are not created intentionally, but rather are abnormal connections that occur between the portal vein and systemic circulation, bypassing the liver. Bypassing the liver causes increased toxins, proteins, and nutrients that were absorbed by the intestines to now flow into the systemic circulation. The formation of SPSS often means that the patient is at a higher risk of mortality, along with complications including portal vein thrombosis, hepatic encephalopathy, and gastrointestinal bleeding.
SPSS typically develop secondary to portal hypertension. Portal hypertension is usually caused by cirrhosis, which can precipitate from alcoholic liver disease, nonalcoholic fatty liver disease, hepatitis B or C, and many other causes. In our case, the patient was a 43-year-old male with alcoholic hepatitis with progression to liver cirrhosis. Other comorbidities included chronic cholecystitis, upper gastrointestinal bleeding, coagulopathy, and portal hypertension with ascites. The splenocaval shunt was noted during an abdominal and pelvis CT. In patients where there are no negative side effects from the shunt, it’s best to not provide any interventions. If shunting activity is increased, patients can experience encephalopathy. In these cases, embolization can stop the shunting and encephalopathy. BRTO, PARTO, and CARTO are specific techniques that can be used in portosystemic shunting.
This case highlights the rare and intriguing occurrence of a native splenocaval shunt. This unique vascular anomaly can provide us with valuable insights into both its clinical implications and management strategies. This shunt is thought to have helped with the patient’s portal hypertension. The side effects of a splenocaval shunt would present similar to those of any other portosystemic shunt. The assumed decrease in portal pressure would decrease the chances of variceal bleeding but increase the likelihood of encephalopathy. This case report serves as a reminder of the importance of continued research in the field of vascular anomalies to improve patient outcomes and enhance our understanding of these rare occurrences.
# 350
Body Composition and Pediatric Obesity and Metabolic Dysfunction-Associated Steatotic Liver Disease Using Magnetic Resonance Imaging and Elastography
Dong AM1, Adamos TR1, Kafali S2, Shih S2, Delgado-Esbenshade T2, Mohpatra S1, Li J1, Ghahremani S2, Wu HH2, Calkins KL1. 1UCLA, Los Angeles, CA and 2UCLA, Los Angeles, CA
Purpose of Study: Approximately 10% of children have metabolic dysfunction-associated steatotic liver disease (MASLD); all of whom are at risk for metabolic dysfunction-associated steatohepatitis (MASH). While obesity is a major risk factor for MASLD, it is unpredictable which children with MASLD will progress to MASH and fibrosis. Body composition may enhance our ability to better understand different metabolic phenotypes. This study’s purpose was to investigate associations between body composition and liver disease using quantitative magnetic resonance imaging (MRI) and elastography (MRE).
Methods Used: Children ages 6-17 years were recruited at the University of California Los Angeles. Subjects were divided into 3 cohorts: 1. Lean children (body mass index [BMI] <85th percentile) without liver disease, 2. Overweight children (BMI ≥85th percentile) without liver disease, and 3. Overweight children with hepatic steatosis consistent with MASLD. Free-breathing 3D MRI was used to measure hepatic (H)-proton density fat fraction (PDFF; 0-100%), a biomarker for hepatic steatosis, along with visceral adipose tissue (VAT) volume, VAT-PDFF, subcutaneous adipose tissue (SAT) volume, and SAT-PDFF. PDFF is a biomarker for adipose tissue fat content; a higher PDFF indicates white-like fat. Breath-holding 2D MRE was used to measure liver stiffness (kPa), a biomarker for fibrosis. Figure 1 depicts how these biomarkers were quantified.
Summary of Results: Fifty-two lean children (mean±SD age 13±2 years), 21 overweight children (mean age 14±3 years), and 26 children with hepatic steatosis consistent with MASLD (mean age 13±3 years) completed the study. Age, sex, and race were comparable across the 3 cohorts. As expected, BMI z-scores (p<0.0001) and anthropometric measurements, such as waist circumference (p<0.0001), were different between the cohorts. VAT volume, VAT-PDFF, SAT volume, and SAT-PDFF were also different between cohorts (
Table 1
). On post-hoc analysis, when compared to overweight children, overweight children with hepatic steatosis had a higher liver stiffness, VAT volume, VAT-PDFF, and SAT volume (p<0.05 for all). VAT-PDFF (r=0.53; p<0.0001), VAT volume (r=0.62; p<0.0001), and SAT volume (r=0.62; p<0.0001) were positively correlated with H-PDFF.
Clinical Characteristics and MRI/MRE Biomarkers.
Lean
(n=52)
Overweight(n=21)
MASLD
(n=26)
p-value
Age (years)
13.2 ± 2
14.1 ± 3
13.1 ± 3
0.41
Male sex
25 (48)
9 (43)
18 (69)
0.13
Hispanic
13 (25)
10 (48)
19 (73)
0.0002
Race
White
20 (38)
13 (62)
20 (77)
0.07
Black
2 (4)
1 (5)
2 (8)
0.07
Asian
5 (10)
2 (10)
1 (4)
0.07
Other
2 (4)
0
0
0.07
More than 1 race
23 (44)
5 (24)
3 (12)
0.07
BMI z-score
-0.01 ± 0.9
1.9 ± 0.5^a
2.1 ± 0.4^b
<0.0001
Waist circumference >75th percentile
5 (10)
16 (76)
26 (100)
<0.0001
Infant of diabetic mother
2 (4)
0
9 (36)
<0.0001
Maternal history of metabolic diseases during pregnancy
5 (10)
8 (4)
14 (56)
<0.0001
Family history of MASLD
0
5 (25)
5 (20)
0.002
Family history of metabolic diseases
24 (47)
13 (65)
22 (88)
0.003
Hepatic-PDFF (%)
2.1 ± 0.7
3.0 ± 1.2
18.8 ± 9.6
-
Liver stiffness (kPa)
2.1 ± 0.2
1.9 ± 0.2
2.2 ± 0.7^c
<0.0001
VAT volume (cm3)
163.8 ± 92.7
318.2 ± 161.7^a
467.6 ± 257.1^bc
<0.0001
VAT-PDFF (%)
55.4 ± 12.4
74.5 ± 11.1^a
82.7 ± 7.1^bc
<0.0001
SAT volume (cm3)
780.0 ± 396.3
2176 ± 997.4^a
2809 ± 795.4^bc
<0.0001
SAT-PDFF (%)
77.9 ± 18.9
94.4 ± 7.7^a
96.2 ± 2.5^b
<0.0001
Table 1. Clinical characteristics and MRI/MRE biomarkers. Data presented as mean±SD and n (%). ANOVA (followed by a post-hoc Tukey’s test) and Chi-squared analyses were conducted to assess for differences between the 3 groups. ap
Conclusions: Distribution and composition of adipose tissue in the body may play an important role in the development of MASLD/MASH. We speculate that VAT and white adipose tissue promote insulin resistance and hepatic steatosis and fibrosis.
# 351
Monomicrobial Non-Neutrocytic Bacterascites Caused by Atypical ESBL Escherichia coli and Spontaneous Bacterial Peritonitis Prophylaxis
Li W, Vongbunyong K, Park N. UC Irvine, Irvine, CA
Case Report: Monomicrobial non-neutrocytic bacterascities (MNB) is a subtype of spontaneous bacterial peritonitis (SBP), defined as a positive ascites culture and a polymorphonuclear neutrophil (PMN) count < 250/mm3. The prevalence of MNB compared to all other subtypes of SBP is between 11%-26%. Most cases of MNB are self-resolving, but a significant proportion of untreated cases of MNB progress to SBP. Although Escherichia coli (E. Coli) is commonly the cause of MNB, multidrug-resistant variations such as extended-spectrum beta-lactamase (ESBL) E. Coli can also rarely cause MNB. Such cases require more complex short-term and long-term treatment.
Herein we describe one such case of MNB caused by atypical ESBL E. Coli. A 68-year-old male with hypertension, hyperlipidemia, and Child-Pugh class B liver cirrhosis likely due to HBV was brought in for dull abdominal pain for the past week, associated general weakness, confusion, and constipation. Of note, the patient was admitted a month prior for acute metabolic encephalopathy secondary to hepatic encephalopathy. Examination was notable for a paraumbilical hernia and a distended abdomen with diffuse tenderness upon palpation. Diagnostic paracentesis obtained on admission showed a PMN count of 30.7/mm3. On day 5 of admission, ascitic fluid culture grew ESBL E. Coli, consistent with MNB.
Patient was started on ceftriaxone 1000 mg IV and metronidazole 500 mg IV to cover for intra-abdominal infection. He was broadened to meropenem 100 mg IV starting on day 5 after ESBL E. Coli was isolated. Patient showed clinical improvement of symptoms post-meropenem treatment. Repeat paracentesis on day 7 showed a PMN count of 0.69/mm3. Repeat culture was unobtainable as the sample was lost in lab and there was no fluid pocket to attempt subsequent paracentesis. As there is currently no available carbapenem PO formulation offered at our hospital, Infectious Disease was consulted to guide prophylactic antibiotic choice. Despite having intermediate sensitivity, ciprofloxacin 500 mg PO was recommended for future SBP prophylaxis, given there was no better oral option. Patient was discharged on day 11 and continues to take ciprofloxacin 500 mg PO every day for SBP prophylaxis.
MNB is usually considered a colonization phase of bacterial ascites, with most cases self-resolving. However, MNB is reported to have the potential to progress to SBP in only a few hours. As microbes continue to develop resistance at an alarming rate, physicians must practice antimicrobial stewardship. However, differentiating cases of asymptomatic MNB colonization from cases with likely SBP progression makes antimicrobial treatment decisions difficult. Our case highlights the importance of considering both the presence of symptoms in addition to the specific microbe isolated in guiding treatment decisions.
# 352
A Deadly Triad: Metastatic Esophageal Adenocarcinoma with Alpha-Fetoprotein Production, Liver Capsular Tear after Needle Biopsy, and Spontaneous Solid Tumor Lysis Syndrome
Uddin S, Guerrero L, Mann B, Jestila T. Kern Medical Center, Bakersfield, CA
Case Report: AFP-secreting esophageal adenocarcinomas are rare neoplasms with a poor long-term prognosis as the presentation is often insidious and advanced. Complications of large Capsular tear after Needle Liver Biopsy and Spontaneous Solid Tumor Lysis syndrome before initiation of Chemotherapeutic agents are rarer yet and may have devasting outcomes on mortality.
Case Presentation: A 43-year-old male with a prior diagnosis of Asthma presented for Hospitalization with progressive weakness, fatigue, and syncopal episodes in the prior three days. He had been experiencing progressing epigastric pain with intermittent dysphagia for the last three months and had repeatedly returned to the Emergency Department for symptom relief. He had been referred for outpatient follow-up with a primary care physician for further evaluation and scheduled for Gastroenterology evaluation. Due to the progression of his symptoms he returned to the Emergency Department. Evaluation revealed the patient to be anemic with a Hemoglobin level of 6.0, transaminitis, serum AFP levels of 1,118.3 ng/mL, and imaging results consistent with Gastroesophageal Malignancy with innumerable Hepatic masses. A follow-up EGD with biopsy confirmed a circumferential ulcerated fungating mass in the distal esophagus. Specimen pathology was consistent with invasive poorly differentiated Adenocarcinoma. An Ultrasound-guided Needle mass core biopsy of Hepatic segment II was completed in the following days without complication, with pathology confirming findings consistent with Metastatic Esophageal Adenocarcinoma. The patient had not tolerated any form of oral intake secondary to dysphagia from mass effect and thus underwent a Gastrostomy on Hospital Day Six. During the operation he was found to have a 4 cm capsular tear of the anterior left lobe of the liver left of the falciform ligament with 1.5 L old blood hemoperitoneum and surgical repair with Bovie cauterization was performed. On hospital Day Nine his laboratory findings were concerning for Tumor lysis syndrome even though he had not received any chemotherapeutic agents. The patient received treatment with Rasburicase and Allopurinol. The decision was made with the patient to begin palliative chemotherapy with Oxaliplatin, Leucovorin, and Fluorouracil despite his multiple complications. The following morning the patient became anuric with qSOFA findings consistent with Septic Shock. The patient was admitted to the ICU and placed on mechanical ventilation where he expired on Hospital Day 11 after his family agreed with comfort care measures.
Discussion/ Conclusion: Metastatic Esophageal Adenocarcinoma holds a relative 5-year survival rate of only 6%. AFP-producing Esophageal tumors are rare and warrant further oncologic investigation and research to provide appropriate and timely care to patients with early and rapidly progressing presentation.
# 353
DETERMINING LONG-TERM HEALTH AND NUTRITIONAL OUTCOMES OF CHILDREN WHO COMPLETED TREATMENT IN A CHILD MALNUTRITION CENTER FOR SEVERE ACUTE MALNUTRITION
Ruf AM1, Arredondo D1, Butt MF1, Panchal H2, Pathak P2, Patel S2, Malkan H2, Yadav K2, Patel N3, Judkins A4, Fassl B1. 1Northeast Ohio Medical University, Rootstown, OH; 2Dr. Kiran C. Patel Medical College & Research Institute, Bharuch, , India; 3Mota Fofalia Hospital, Mota Fofalia, , India and 4University of Utah, Salt Lake City, UT
Purpose of Study: 2.3 million children 6-60 months die due to severe acute malnutrition (SAM) each year in India; Mota Fofalia Hospital operates a child malnutrition treatment center (CMTC) to treat SAM and related morbidities. These inpatient programs for SAM often result in short term weight gain during the hospital treatment but long-term effectiveness on nutrition outcomes is not well documented.
Describe the long term weight outcomes of children who completed nutritional rehabilitation for SAM.
Methods Used: This study took place at Mota Fofalia Community Health Center, Gujarat, India, June 2023-Aug 2023, includes all children admitted to the CMTC from 2019-2021. We abstracted demographic and SAM treatment information from the CMTC record. As part of a local quality improvement initiative the local field team performed household visits in a convenience sample of children, performing anthropometric measurements. We calculated changes in the weight-for-age (WFA) z-score, expressed as standard deviations above/below the mean weight-for-age between CMTC discharge date and follow-up.
Summary of Results: 224 patients were admitted to the CMTC, 167 could be located/contacted during follow-up, 92 have a complete data record. Average patient age at discharge: 20 months (range 4-58); at follow-up: 67 months (range 46-111). 60 children (65%) showed a positive change in their WFA z-score: (mean:+0.55; range -4.41-3.87). Average CMTC WFA z-score at discharge: -2.93 (ranges -5.79-1.70), at follow-up -2.37 (range -5.98-1.63).
Conclusions: A structured follow-up program after CMTC discharge may increase the proportion of children who maintain weight gain.
Genetics I
Concurrent Session
8:00 AM
Friday, January 19, 2024
# 354
A multi-omics approach to the characterization of a novel repeat expansion in FAM193B in a family with oculopharyngodistal myopathy
Reuter C1, Fazal S2, Jensen T1, Gorzynski J1, Marwaha S1, Bonner D1, Kohler J1, Mendez R1, Voutos I1, Emami S1, Kravets E1, Smith K1, Goddard P1, Ungar R1, Network U1, Danzi MC2, Ashley E1, Sampson J1, Bernstein JA1, Zuchner S2, Montgomery S1, Wheeler M1. 1Stanford Center for Undiagnosed Diseases, Stanford, CA and 2University of Miami, Miami, FL
Background: Oculopharyngodistal myopathy (OPDM) is an autosomal dominant disorder characterized by facial and distal limb weakness, ptosis, and external ophthalmoplegia. Patients may have pharyngeal involvement or myopathic changes on skeletal muscle biopsy. Known molecular mechanisms of OPDMs include trinucleotide repeat expansions in LRP12, GIPC1, RILPL1, and NOTCH2NLC. The disease-causing motif is a 5’ UTR CGG expansion. Still, roughly 30% of OPDM patients remain genetically undiagnosed.
Case Report: At the Stanford Center for Undiagnosed Diseases, we evaluated a 68 year old female with significant weakness of facial muscles, bilateral distal upper and lower extremity weakness, respiratory muscle weakness, osteoporosis, dysphagia, dysarthria, double vision, and hypothyroidism. The patient’s sister is similarly affected. Clinical genetic workup including targeted testing for muscular dystrophies, exome sequencing, and short read genome sequencing (SR-GS) were nondiagnostic.
Suspecting a short tandem repeat expansion, the patient was nominated for evaluation using an ExpansionHunter Denovo (EHDn) pipeline through the Undiagnosed Diseases Network. No expansions were detected in genes associated with OPDM – LRP12, GIPC1, RILPL1, or NOTCH2NLC. EHDn identified a rare, heterozygous CGG expansion in the 5’ UTR of the FAM193B gene from SR-GS estimated at 72 repeats (range 71-121). The expansion is present in both affected sisters and the unaffected mother, but absent in father and other unrelated controls. To better characterize the true size of the expansion, nanopore long read genome sequencing (LR-GS) was performed. The patient (245 repeats), sister (225 repeats), unaffected mother (185 repeats) were outliers compared to typical <50 repeats at this locus in a cohort of 100 unrelated individuals with LR-GS. Blood RNA sequencing revealed that FAM193B was over-expressed in both affected sisters compared to 282 unrelated controls. The mother’s unaffected status despite carrying a smaller expansion may be explained if hers is a premutation allele.
Conclusions: The CGG 5’ UTR expansion in FAM193B may represent a novel molecular mechanism of OPDM. While SR-GS detected an expansion at this locus, LR-GS was superior in its ability to accurately characterize the expansion size. The integration of LR-GS and transcriptome analyses inform disease-causing potential of the FAM193B 5’UTR CGG repeat expansion. Further work is ongoing to characterize the functional impact of this expansion on RNA and protein and identify additional affected individuals.
# 355
Mechanisms of spiny mouse DNA methylation in kidney regeneration at the cellular level
Wessels ME1, Gere JB2, Suh K2, Okamura DM2, 3, Collins SJ2, Tsai A4, Majesky MW2, 3, Nguyen E2, 3. 1University of Washington School of Medicine, Seattle, WA; 2Seattle Children’s Research Institute, Seattle, WA; 3University of Washington, Seattle, WA and 4University of Washington, Seattle, WA
Purpose of Study: African spiny mice (Acomys cahirinus) have full restoration of kidney function after injury without fibrosis, as opposed to house mice (Mus musculus). Their genes are >90% similar in sequence identity but Acomys gene expression pattern is strikingly different after kidney injury, indicating that epigenetic regulation such as DNA methylation may play a role in the regenerative capability of Acomys. Notably, after Acomys experience kidney injury, genes with upregulated expression are primarily related to cell cycle regulation and DNA damage response as opposed to fibrosis in Mus. K(lysine) acetyltransferase 5 (Kat5) is an enzyme that repairs DNA and is involved in cell cycle progression, cell proliferation, and has been associated with proximal tubular repair in the kidney in prior studies. Our project characterizes the DNA methylation landscape of the Acomys as well as expression of Kat5 in Acomys versus Mus after kidney injury. We hypothesize DNA methylation is different between Mus and Acomys, and that Kat5 plays a role in kidney regeneration seen in Acomys after kidney injury.
Methods Used: Data Analysis: We characterized the DNA methylation landscape in the Acomys by analyzing long-read Nanopore sequencing data of CpG islands. We then compared the DNA methylation patterning, chromatin accessibility, and differential gene expression after day 3 ischemic reperfusion injury for both Mus and Acomys in several genes related to kidney repair after injury based on literature review.
Experimental Analysis:Western blots were used to characterize protein expression of Kat5 in Mus and Acomys. Samples used in our study included subcellular fractions (including chromatin, nuclear and cytoplasmic fractions) in normal kidneys as well as whole cell lysates of kidneys 3, 7 and 14 days after ischemic reperfusion injury. Protein quantification was performed with ImageJ and normalized against total protein expression stained by Ponceau S.
Summary of Results: 34% of CpG islands in Acomys overlap 5’ UTR promoter regions of genes and could potentially regulate gene expression. Kat5 expression from Western blot in normal Acomys kidneys is increased compared to Mus, and is increased at least 10 fold following ischemic injury. Other genes related to kidney repair such as Slc22a12 and Ifngr2 are also differentially expressed after kidney injury and may represent future targets to explore.
Conclusions: DNA methylation may play a significant role in kidney regeneration in Acomys, particularly through KAT5 regulation of DNA repair and cell cycle progression after kidney injury. Further experiments exploring these mechanisms may lead to improved treatment options for individuals with chronic kidney disease.
# 356
A SYNDROME OF TRAUMA-INDUCED HEMIPARESIS CAUSED BY R1349Q MUTATION OF CACNA1A
Brown SR, Willis M. Naval Medical Center San Diego, San Diego, CA
Case Report: CACNA1A encodes the pore-forming subunit of voltage-gated calcium channels found predominantly in the brain, and pathogenic variants in CACNA1A are responsible for a range of neurologic diseases including developmental and epileptic encephalopathy-42, episodic ataxia type 2, familial hemiplegic migraine, and spinocerebellar ataxia 6. In addition, many patients present with a variety of features that overlap with the above phenotypes. A few variant-specific genotype-phenotype correlations have been reported. We present here a case series of patients with R1349Q variant in CACNA1A demonstrating a consistent phenotype of developmental delay/intellectual disability, seizures, hemiparesis, altered mental status, and cerebral edema elicited by minor head trauma.
In addition to our index patient with R1349Q mutation, literature review of case reports of an additional 8 patients with R1349Q mutation were found. Case reports which did not detail specific symptoms of R1349Q patients were excluded from review.
Of the 9 patients identified with R1349Q mutation all were de novo. 100% of patients exhibited motor delay, 78% also exhibited speech delay. Our index patient and 75% of case reports (78% of all patients reviewed) reported episodic symptoms elicited by minor head trauma. The episodes included hemiplegia (100%), altered mental status (86%), migraine (71%), seizures (57%), and cerebral edema on head imaging (71%). Two case reports did not discuss trauma, but both patients experienced episodic hemiparesis and seizures without identified inciting factor. Additionally, the following symptoms were reported: seizures in absence of trauma (78%), cerebellar atrophy (78%), ataxia (56%), paroxysmal tonic upward gaze (33%), and hypotonia (33%). The episodes following minor head trauma characterized by hemiplegia and altered mental status with additional neurologic findings, may cause a prolonged period of neurologic dysfunction with slow or only partial return to baseline.
This case series suggests a consistent phenotype associated with the R1349Q variant in CACNA1A including features of developmental and epileptic encephalopathy-42 with the more unique feature of cerebral edema following minor head trauma. Recognition of the strong genotype-phenotype correlation for R1349Q informs prognosis for newly diagnosed patients and will enable preventive measures to avoid minor head trauma and earlier recognition of cerebral edema to potentially improve outcomes.
# 357
GENETIC TESTING FOR NEONATAL SEIZURES: A NECESSARY DIAGNOSTIC TOOL?
Heringman K1, Gold J2. 1University of California San Diego, San Diego, CA and 2University of California San Diego, San Diego, CA
Purpose of Study: Neonatal seizures are a devastating cause of mortality and morbidity, with an incidence of 1-5/1000 live births. 33% of infants with neonatal seizures die, and 40-60% of survivors have disability. Optimal treatment to seizures requires accurate and timely diagnosis of their cause. Neonates at our institution routinely receive rapid next-generation sequencing to look for genetic causes of disease through the Rady Children’s Institute for Genomic Medicine. We investigated the utilization and yield of genetic testing in a consecutive series of neonates with seizures form 2016-2022.
Methods Used: We performed a retrospective chart review from 2016 to 2022 of all newborns (any gestational age and birth weight) admitted to the NICU at Rady’s Children’s Hospital with seizures. We retrieved demographic, obstetrical and clinical information related to their hospital stay such as imaging, EEG results, genetic testing, seizure medication, and outcomes. Patterns of ordering and yield of genetic testing were identified. Descriptive statistics was used to characterize frequency, median, or means for data collected. Statistical analysis was performed with the Chi-square T-paired tests. Statistical significance was determined with a P value set at < 0.05.
Summary of Results: We identified 248 neonates with seizure. 4 were excluded due to incomplete information in their charts. 101 patients (41%) had genetic testing performed in the NICU and 43 (43%) had abnormal results. 90 newborns were diagnosed with hypoxic-ischemic encephalopathy (HIE); 18 (20%) had genetic testing, and 2 (11%) were abnormal. 154 patients had a diagnosis other than HIE; 83 (54%) had genetic testing done, and 41 (49%) of these results were abnormal. Patients with lower APGAR scores (0-4) at the 1 and 5 minute were significantly less likely to have genetic testing ordered than the neonates with higher scores (5-9), chi square p<0.05; Average APGAR at 1 and 5 minutes was significantly higher in infants who got genetic testing (3.9 vs 5.6 and 5.8 vs 7.2, P < 0.01). 70 of the 90 infants with HIE survived to discharge; 3 who did not receive genetic testing in the NICU subsequently had genetic testing as outpatients. 2 out of the 3 had abnormal results.
Conclusions: Genetic testing has a high yield in neonates with seizures, obtaining an abnormal result 41% of the time. At our institution, physicians appear to avoid genetic testing in neonates with low APGAR scores, likely because HIE is considered a contraindication for genetic testing. Our findings indicate this likely leads to missed genetic diagnoses, as we found abnormal genetic results in 11% of neonates diagnosed with HIE who obtained genetic testing in the NICU, and 2 of 3 patients diagnosed with HIE who had genetic testing after NICU discharge. Broader testing in the neonatal intensive care is likely to find more infants with genetic causes of seizures.
# 358
A NEW FAMILY WITH A NOVEL C.515DEL HSPB8-ASSOCIATED MYOPATHY WITH CARDIOMYOPATHY
Tan J1, Duong H1, Awad Y1, Kimonis V2. 1Western University of Health Sciences, Pomona, CA and 2University of California, Irvine, Irvine, CA
Purpose of Study: HSPB8, or heat shock protein family B (small) member 8, is a member of the chaperone-assisted selective autophagy (CASA), aiding in the recognition of misfolded proteins for refolding or degradation. Mutations in this gene have been associated with Charcot-Marie-Tooth type 2 L (CMT2L) disease, distal hereditary motor neuropathy type II (dHMNII), and recently a distal myopathy. Here, we report a family with autosomal dominant rimmed vacuolar myopathy (RVM) caused by a novel c.515del variant of the HSPB8 gene.
Methods Used: Using whole exome sequencing, we identified a novel variant c.515delC (p.Pro172Leufs*75) in HSPB8 in a family with autosomal dominant rimmed vacuolar myopathy. The mutant was confirmed with Sanger sequencing. Histological studies were done on muscle biopsies to assess the pathological features that may characterize this variant. The proband’s medical history including the cardiology, pulmonary, musculoskeletal, and family history were also assessed.
Summary of Results: The proband is a 38 y. old male with a history of muscle weakness, scoliosis, restrictive lung disease, pericardial effusion, elevated left diaphragm and eventration, hypertension, NAFLD, and hypercholesterolemia. He had a scapuloperoneal pattern of muscle weakness with proximal leg involvement. Histological analysis showed rimmed vacuoles, vacuolated fibers, internal nuclei, degenerative and regenerating ring fibers, and adipose tissue infiltration. MRI revealed severe atrophy in paraspinal muscle, marked atrophy in bilateral thighs with mild relative sparing of rectus femoris and vastus lateralis, and moderate atrophy in bilateral lower legs. His echocardiogram was normal. Family history revealed a similar pattern in the proband’s maternal side of the family. His mother had complained of muscle weakness and difficulty walking during her 40s with muscle biopsy showing evidence of myofibrillar disruption. The maternal grandmother reported proximal arm and leg weakness, and died in her 80s. His maternal uncle was diagnosed with ‘muscular dystrophy’ with rimmed vacuoles on biopsy. He used a cane for ambulation in his early 20s, and a wheelchair in his 30s. He was diagnosed with left ventricular hypertrophy in his early 50s, and died of concurrent cardiomyopathy at 54 y. The clinical manifestations of muscle weakness appear to be more severe in males compared to females in this family.
Whole exome sequencing analyses revealed a deletion of C at position 515, resulting in a translational frameshift expected to disrupt the last 25 AA of HSPB8 protein and extend protein by an additional 49 AA.
Conclusions: We report a new family with vacuolar myopathy associated with a novel frameshift mutation that resulted in an elongated protein structure that may contribute to rimmed vacuolar myopathy’s pathogenesis. Cardiomyopathy was identified in one individual, a feature previously reported in one patient. This family expands the phenotype and genotype correlations in a new HSPB8-associated vacuolar myopathy.
# 359
SOLAMEN SYNDROME: SEGMENTAL EXACERBATION OF PTEN HAMARTOMA SYNDROME IN A 2-YEAR-OLD MALE WITH A GERMLINE PTEN VARIANT AND A SECOND SOMATIC MOSAIC PTEN EVENT
Hoover A1, Chang V4, Bottomley S1, Grossman E2, Iqbal A3, Upadhyay S3, Martinez-Agosto J1, 5, Russell B1. 1UCLA, Los Angeles, CA; 2Cottage Health, Pismo Beach, CA; 3Cottage Health, Santa Barbara, CA; 4UCLA, Los Angeles, CA and 5UCLA, Los Angeles, CA
Case Report: PTEN hamartoma tumor syndrome (PHTS) is an autosomal dominant genetic condition that describes the spectrum of individuals with a pathogenic variant in PTEN. PHTS includes features such as macrocephaly and autism, and is associated with increased risks for certain cancers, typically adult onset. A 2-year-old boy presented to our multidisciplinary Pediatric Cancer Predisposition clinic with a large left lipomatous neck mass with extensive involvement into the chest and abdomen. Biopsy was consistent with a hibernoma. The patient was also found to have macrocephaly (Z score>6), epidermal nevi, bilateral 2,3 syndactyly, verrucous nevi on left side, and minor left leg length discrepancy. The initial mass on shoulders and spine was first noted prenatally on an 8-week ultrasound but was not visible at birth. The mass became noticeable to parents around 3 months of age. Imaging via MRI and CT indicated a large mass size extending into the chest cavity and under axilla. The mass was not restricting movement and was not associated with pain. A genetic panel analyzing genes associated with macrocephaly and overgrowth on blood tissue was completed which identified a pathogenic frameshift variant in PTEN. Shortly after, the patient underwent surgical excision of the left neck mass. Further genetic testing with a somatic overgrowth panel was pursued on biopsy of affected tissue given concerns for severity of the hibernoma. Results of testing revealed the previously identified germline variant in PTEN at 44% variant allele frequency along with a second hit with a 10% mosaic pathogenic variant in PTEN. The findings are consistent with an ultra-rare condition called SOLAMEN (segmental overgrowth, lipomatosis, arteriovenous malformation, and epidermal nevus) syndrome which explains the patient’s severe manifestation that mimic other genetic conditions such as Proteus Syndrome. This condition has only been described in 3 individuals to date.
The Happle Hypothesis has been used to describe exacerbation of autosomal dominant genetic disorders by way of a second somatic mosaic variant hit in the same gene. One such rare presentation of this disorder is through a novel condition with the proposed name SOLAMEN Syndrome. This case illustrates the possibility of individuals to harbor two distinct genetic variants in a germline and somatic state that would typically be considered incompatible with life in a purely homozygous state. Although rare, clinicians should consider these diagnostic possibilities in these patients who present with severe manifestations of otherwise relatively common genetic disorders as medical management considerations could be affected.
# 360
PARENT NARRATIVES PROVIDE PERSPECTIVES ON THE EXPERIENCE OF CARE IN TRISOMY 18
Bierer R1, Mladucky J2, Anderson R3, Carey JC1. 1University of Utah, Salt Lake City, UT; 2Intermountain Health, Murray, UT and 3University of Utah, Salt Lake City, UT
Purpose of Study: Trisomy 18 syndrome, also known as Edwards syndrome, is the second most common autosomal chromosome syndrome after Down syndrome. As is well known, trisomy 18 is a serious medical disorder due to the increased occurrence of structural defects, especially heart malformations, the high neonatal and infant mortality, and the cognitive and psychomotor disabilities observed in older children. Interventions, including cardiac surgery, remain controversial, and the conventional approach is usually to pursue pure comfort care. While cardiorespiratory difficulties and congenital defects have been characterized, there are scant data on the parental views and perspectives of rearing a child with these conditions. Knowledge of the parental viewpoints can inform care as clinicians guide and counsel families through decision-making. Our aim was to identify parents’ views and perspectives by analyzing a series of narratives.
Methods Used: In this qualitative research study we collected 46 parent narratives at the 2015 (Salt Lake City) and 2016 (Tacoma) annual Support Organization for Trisomy 18 & 13 (SOFT) conferences. The narratives were obtained as part of a web-based tool, Sensemaker, that the parents volunteered to take. (This tool, introduced to the Department of Pediatrics by Dr. Ron Bloom, has been used for various research questions and QI). The participants are asked to “Tell us a story about your experience”. The data presented here are on the analysis of the parent narratives. Inductive content analysis was used to identify themes from 46 submitted stories with consensus coding of two authors (RB and JCC). Dedoose, a web-based application to analyze qualitative data, was used to for coding themes more systematically.
Summary of Results: The narratives ranged from a few sentences to detailed stories of more than 300 words; the ages of the family member with trisomy 18 were not recorded but were often mentioned in the narrative and ranged from 4 months to the third decade. Of 80 total themes coded in stories, the most common included “Diagnosis impacts care” (n=14) and “Surpassing expectations” (n=12). Other common themes included “Support from professionals” (n=8) and “Support from faith/religion” (n=4), “Change in attitude” (n=4), “Postnatal diagnosis changes care” (n=4), “A child, not a diagnosis” (n=4), “Attitude impacting care” (n=5) and Trust/lack of trust (n=2). Feelings coded included avoidant (2), joy (3), negative (2), devastating (3), hopeful (3).
Conclusions: Our goal was to examine the voice, the perspectives, & the viewpoints of the parents in their challenges in rearing children with potentially life-limiting conditions. The recognition and exploration of the themes can ideally guide clinicians in their approach to the counseling and care of the child and parents.
# 361
MODELING HAILEY-HAILEY DISEASE IN HUMAN ORGANOTYPIC EPIDERMIS TO UNDERSTAND ITS PATHOGENESIS AND IDENTIFY NOVEL THERAPEUTIC STRATEGIES
Tam CJ1, 2, Ayers J1, 3, Tiwaa A1, Sarkar M4, Gudjonsson JE4, Simpson CL1. 1University of Washington, Seattle, WA; 2University of Washington, Seattle, WA; 3University of Washington, Seattle, WA and 4University of Michigan, Ann Arbor, MI
Purpose of Study: Hailey-Hailey Disease (HHD) is an autosomal dominant skin disorder caused by loss of adhesion between epidermal keratinocytes, resulting in recurrent blisters and reduced quality of life. Over 20 years ago, HHD was linked to ATP2C1 mutations that deplete its encoded protein SPCA1, a Golgi ATPase necessary for processing adhesive cadherins to form desmosomes. Currently, there are no FDA-approved treatments and no pre-clinical model for HHD since Atp2c1 knockout (KO) mice do not replicate the disease. We aimed to model HHD in vitro to understand its pathogenesis and identify therapeutic targets. We hypothesized that depleting SPCA1 in human keratinocytes would disrupt adhesion protein trafficking and assembly of cell-cell junctions.
Methods Used: We used CRISPR to ablate ATP2C1 in TERT-immortalized human epidermal keratinocytes and quantified adhesion protein levels by Western blot. Cell-cell adhesion was measured in a mechanical dissociation assay, in which stress was applied to cell sheets (monolayers) and fragments were counted. We performed RNA sequencing (RNAseq) to quantify global gene expression in SPCA1-deficient cells. Immunofluorescence was used to localize adhesion proteins while actin was visualized by live confocal microscopy. We used Golgicide-A (GCA) to induce Golgi stress in cells. To form organoid epidermis, keratinocytes were grown on collagen rafts at an air-liquid interface.
Summary of Results: SPCA1 depletion was confirmed by Western blot. Monolayers lacking SPCA1 exhibited more fragments after mechanical stress (p = 0.0092 for heterozygous [HET]; p = 0.0188 for KO), reflecting impaired cell-cell adhesion. Levels of intercellular junction proteins were not altered in HET cells, but cadherins were poorly localized to cell-cell contacts. RNAseq of HET cells showed altered regulators of actin and proteotoxic stress. Live microscopy revealed actin disorganization in KO cells. Treating control cells with GCA disrupted desmosomes and increased monolayer fragmentation, suggesting proteotoxic stress from Golgi dysfunction compromises cell-cell adhesion. In organoid epidermis, SPCA1-deficient cells replicated the key feature of HHD, splitting between keratinocytes, but also showed mis-localization of adhesive proteins and actin disorganization. These features were replicated by immunostaining HHD patient biopsies.
Conclusions: We ablated ATP2C1 in human keratinocytes to generate cellular and organoid models of HHD. Our studies showed adhesion proteins are not properly trafficked to intercellular junctions in SPCA1-deficient cells, explaining the loss of cell-cell adhesion in HHD. Validating RNAseq from SPCA1-deficient cells, we found potential therapeutic targets including regulators of actin and proteotoxic stress. We propose these could serve as drug targets to strengthen cell-cell adhesion and improve wound healing in patients with HHD. In sum, our in vitro models advance our understanding of HHD and provide a platform for testing potential treatments.
Neonatology General III
Concurrent Session
8:00 AM
Friday, January 19, 2024
# 362
CHARACTERISTICS OF VERY LOW BIRTH WEIGHT INFANTS PRESENTING WITH ABNORMAL NEUROLOGICAL EXAMINATION AT NICU DISCHARGE
Thirumalai H1, Manickam S2, Ramanathan R1, Biniwale M1. 1Keck School of Medicine of USC, Los Angeles, CA and 2Keck School of Medicine of USC, Los Angeles, CA
Purpose of Study: An integral part of monitoring infants in the neonatal intensive care unit (NICU) is performing thorough physical examination. Neurological examination may reveal underlying problems that may persist through the first years of life. Very low birth weight infants (VLBW) are at significant risk of developing neurological complications in the NICU that may be revealed through abnormal neurological findings at discharge.
The purpose of this study was to characterize the etiologies and outcomes of abnormal neurological examinations performed at the time of discharge from the NICU in VLBW infants.
Methods Used: Infants with BW<1500g referred to high-risk infant follow-up clinic between 6/1/2008 - 03/20/2020 were included in the study. A retrospective review of medical records was performed to collect neonatal events, diagnoses, neurological examinations at discharge, maternal risk factors, follow-up clinic evaluations, Bayley scales of Infant and Toddler development scores and neurological examination findings at age 6-12 months, 18-24 months and 3 years.
Summary of Results: A total of 412 babies were included in this study. The mean birth weight and gestational age were lower in infants who had abnormal neurological examinations. Significant factors during the NICU stay that were associated with higher rates of abnormal neurological examinations were intraventricular hemorrhage (IVH), severe IVH, bronchopulmonary dysplasia (BPD), necrotizing enterocolitis (NEC), seizures, retinopathy of prematurity (ROP), severe ROP and anemia of prematurity. In the follow-up clinic, these infants who had abnormal neurological examinations in the NICU showed a significantly higher association of developmental delays with abnormal Bayley scores at age 6-12 months and abnormal neurological examinations at age 6-12 months and 18-24 months. Logistic regression analysis adjusted for all significant factors showed that the most significant factors associated with abnormal neurological examinations were severe IVH (p=0.006) and seizures (p=0.006).
Conclusions: VLBW infants with IVH and seizures will likely present with abnormal neurological examination at discharge from NICU. These infants may continue to have abnormal neurological examinations and are at risk for developmental delay in the first 3 years of life.
Characteristics of VLBW infants presenting with abnormal neurological examinations.
Factors
Infants with abnormal neurological examination
(N%) (N=58)
Infants with normal neurological examination (N%) (N=354)
P value
Birth weight(g), mean (SD)
975.6 (296.1)
1078 (273.1)
<0.05
Gestational age(wks), mean (SD)
27.0 (2.8)
28.4 (2.8)
<0.001
1 min Apgar score, median (1st quartile, 3rd quartile)
6 (4,8)
6 (4,8)
<0.05
5 min Apgar score, median (1st quartile, 3rd quartile)
8 (7,9)
8 (7,9)
<0.05
10 min Apgar score, median (1st quartile, 3rd quartile
8 (7,8)
8 (7,8)
<0.05
Intraventricular Hemorrhage (IVH), N (%)
30 (51.7)
75 (21.2)
<0.001
Severe IVH, N (%)
17 (29.3)
8 (2.3)
<0.001
Bronchopulmonary Dysplasia (BPD), N (%)
27 (46.6)
78 (22.0)
<0.001
Necrotizing Enterocolitis (NEC)
4 (6.9)
6 (1.7)
<0.05
Seizure, N (%)
16 (27.6)
8 (2.3)
<0.001
Retinopathy of Prematurity (ROP), N (%)
42 (73.7)
207 (58.6)
<0.05
Severe ROP, N (%)
11 (19)
25 (7.1)
<0.05
Anemia of Prematurity, N (%)
48 (82.8)
237 (66.9)
<0.05
Abnormal Bayley Scores at 6-12 months, N (%)
34 (72.3)
138 (52.1)
<0.05
Abnormal neurologic exam at 6-12 months, N (%)
28 (62.2)
42 (18.0)
<0.05
Abnormal neurologic exam at 18-24 months, N (%)
17 (45.9)
31 (18.5)
<0.001
Abnormal neurologic exam at 36 months, N (%)
13 (52.3)
28 (25.0)
<0.05
# 363
Developing a modern model for assessing parent and infant stress response in the NICU through using biosphysical data collection through wearable devices
Garavatti E, Ondusko DS, McEvoy C, Mackiewicz-Seagate K. Oregon Health and Science, Portland, OR
Purpose of Study: Our objective was to develop a methodology for studying physiologic stress response in parents and infants in NICU environment during a family-centered intervention.
Methods Used: IRB oversight was obtained. Participants include parent-infant dyads currently admitted to the NICU. Written informed consent was obtained. Heart rate data was used as metric of physiologic stress response. To capture parents’ heart rate, parents wore a wearable wristband before, during and after intervention. For infants, physiologic data was collected off bedside monitors. Infant heart rate data was broken down into time periods of baseline, intervention and post-intervention, and means were calculated for each participant for those time periods. Box plots were used to demonstrate distribution of data with median, interquartile rant and range, given non-normal distribution. Heart rate data for parents was extracted from wearable device and then run through software for heart rate variability (HRV) analysis.
Summary of Results: 24 parent-infant dyads were enrolled and 21 completed the study. 76% of sessions had infant vital sign data collected, methodology was modified for increased data capture using smaller units of time for 61% of sessions. See Graph 1. Parent wore wristband for 100% of sessions. Of parent data collected, 66% had complete data sets, on further analysis, on 47% had data that was sufficient for HRV analysis. See Table 1.
Conclusions: We demonstrated the use of a wearable device for heart rate collection was acceptable to parents and that this methodology was feasible in the NICU environment. Several limitations were identified in our initial study design, including difficulty extracting data from wearable device, suboptimal device functioning and poor quality of data recordings. Pre-post anaylsis were done to explore outcomes, as this was a feasibility study, a larger study would need to be done to look at effects of intervention. Recommendations for future studies includes exploration of alternative devices, and consideration of devices that are compatible with analysis software. Additional considerations would be capturing infant data in continuous manner to allow for heart rate variability analysis for infant. The application of wearable device technology for monitoring biophysiological stress response to hospital-provided family-centered interventions in the NICU is promising and warrants further exploration.
EVIDENCE OF NEURONAL LOSS/DAMAGE AND ANAEROBIC METABOLISM IN THE BRAINS OF NEONATES WITH SEVERE HYPOXIC ISCHEMIC BRAIN INJURY
Batin B, Jalal R, Bartnik-Olson B, Barajas Terrones A, Oyoyo UE, Kim P. Loma Linda University, Loma Linda, CA
Purpose of Study: Hypoxic-ischemic encephalopathy (HIE) is a leading cause of neonatal mortality and long-term neurologic disability worldwide. While magnetic resonance imaging (MRI) and magnetic resonance spectroscopy (MRS) are both commonly used to predict adverse outcomes, some studies have found MRS measurements to outperform MRI findings. Lactate peaks and NAA attenuation are the most frequently reported MRS predictors of poor neurological outcomes. However, many other MRS values remain to be explored as biomarkers for HIE outcomes. We propose to study all the MRS findings with HIE clinical data including Sarnat score.
Methods Used: A retrospective cohort study of 102 total neonates with mild-to-severe HIE was performed. Inclusion criteria were neonates with diagnosis of HIE and MRI/MRS within 4-14 days of life. Exclusion criteria included poor images. Clinical data including age, APGAR, Sarnat score and time in minutes post-injury to cooling were collected. MRS values (lactate, NAA, choline, creatine, myo-inositol) were also recorded. Associations between clinical data and MRS values were studied using ANOVA, linear regression and logistic regression (p < 0.05).
Summary of Results: 61 males and 41 females with average gestational age of 38 weeks and 7 days (SD: 1.45). Neonates with worse Sarnat scores are associated with lower NAA/Cr (p=0.002). Neonates with low APGAR at 1-minute are 5.3 times more likely to have lactate presence on MRS (95% interval). There is no statistically significant associate of choline/Cr and myo-inositol/Cr ratios with the clinical data.
Conclusions: Our study showed there is an association of lower NAA/Cr with the worst Sarnat score. Since NAA/Cr is a marker of neuronal viability, our findings suggest neonates with worse Sarnat scores have neuronal loss/damage. Our study also showed that neonates with lower APGAR have elevated lactate metabolite in the brain, reflecting anaerobic metabolism in the brain. Choline is a marker of cellular membrane turnover. However, we did not find any association between elevated choline and the clinical data.
# 365
FULL-TIME, DEDICATED TELENEO CRITICAL CARE SERVICE REDUCES CONNECTION TIMES, REDUCES TRANSFERS, AND IMPROVES NEWBORN PATIENT CARE – FIRST YEAR RESULTS
Minton SD1, 2, Zinkhan E1, 2, Valencia R1, Halgren M1, Cox JC1, O’Brien E1, 2. 1Intermountain Health, Murray, UT and 2University of Utah, Salt Lake City, UT
Purpose of Study: Regionalization of neonatal care has decreased the number of sick newborns who are seen by a Neonatologist. Implementation of telehealth services can bring neonatal critical care to the bedside in level 1 and 2 nurseries that don’t have Neonatologist services available. Our first implementation of a TeleNeo Critical Care program in 2013 created additional burdens for Neonatologists during their regular in-unit shifts. Connection times to speak with a Neonatologist were long. Due to lack of time to spend on telehealth consultations, infants were frequently transferred to higher levels of care for further evaluation. Thus, Intermountain Health created a full-time telehealth neonatal critical care service with a Neonatologist whose sole responsibility was telehealth consultations, resuscitation guidance, hospital load balancing, and transport control. The purpose of this study was to determine whether our new TeleNeo Critical Care service would reduce the burden of telehealth consultations on the in-unit Neonatologist, decrease consultation connection time, reduce newborn patient transfers, and improve patient care of newborns and newborn provider satisfaction at level 1 and level 2 nurseries.
Methods Used: Starting September 12, 2022, the new TeleNeo Critical Care was implemented. Providers were able to call 801-321-BABY in a dedicated transfer center for rapid video and audio connection to the dedicated telehealth Neonatologist. Implementation of this process required hiring an additional 4.8 FTE of Neonatologists. Data on number of calls, reason for the call, connection time, time to final disposition, and number of transfers were collected. Feedback from the newborn provider community was encouraged.
Summary of Results: From 9/12/22 through 9/12/23, a total of 1,218 calls were made to TeleNeo Critical Care. Of these, 44% were for an emergent active resuscitation, 37% for urgent calls, and 19% for non-urgent consultation. A 50% reduction in connection time to a Neonatologist was achieved, with an average of 1 minute to phone connection and 3 minutes to video connection. A total of 220 transfers were initiated (20% of total calls). The average time spent on consultation was significantly longer. Further, an anticipated 118 fewer transports were required. Only 40 calls (3%) were sent to an in-unit Neonatologist due to tele-neonatologist unavailability. Feedback from the newborn provider community was overwhelmingly positive.
Conclusions: Implementation of the new dedicated Telehealth Neonatologist Critical Care service with a dedicated Neonatologist reduced the burden of telehealth consultation, reduced connection times, reduced transfers – keeping newborns closer to their mothers, and provided greater support to our newborn provider community. We speculate that implementation of a dedicated telehealth Neonatologist is feasible and may benefit other healthcare systems.
# 366
BANKED TERM UMBILICAL CORD BLOOD TO MEET THE RED BLOOD CELL TRANSFUSION NEEDS OF EXTREMELY-LOW GESTATIONAL-AGE NEONATES: A FEASIBILITY ANALYSIS
Christensen TR1, Bahr TM2, Ohls RK2, Krong J3, Carlson L3, Henry ER3, Sheffield M3, Gerday E3, Ilstrup SJ4, Kelley W5, Christensen RD2. 1Intermountain Healthcare, Murray, UT; 2University of Utah, Salt Lake City, UT; 3Intermountain Health, Murray, UT; 4Intermountain Healthcare, Murray, UT and 5American National Red Cross, Salt Lake City, UT
Purpose of Study: Neonates born <28 weeks gestation (ELGANs; extremely-low-gestational-age-neonates) are at risk for adverse outcomes like bronchopulmonary dysplasia, retinopathy of prematurity, intraventricular hemorrhage, and necrotizing enterocolitis. Several studies show associations between risk for these outcomes and number of red blood cell (RBC) transfusions received. If RBC transfusions are causally associated with adverse ELGANs outcomes, one mechanism might be transfusing adult hemoglobin into patients who physiologically should have fetal hemoglobin. Compared with fetal hemoglobin, adult hemoglobin releases oxygen to tissues liberally, and releasing “too much” oxygen could cause oxidative injury to developing tissues. It has been hypothesized that RBC from otherwise discarded cord blood, drawn after healthy term births, are a more appropriate transfusion product for ELGANs. However, before a definitive study can be proposed, feasibility information is needed regarding ELGAN transfusion needs, availability of cord blood, and barriers to implementation.
Methods Used: 1) Retrospective analysis of all ELGAN RBC transfusions over the past three years at three Intermountain Health Level 3 NICUs, 2) Data-based projections of the umbilical cord blood available for transfusion, if collected from those same hospitals, then processed by the Cord Blood Laboratory of the Red Cross Blood Center in Salt Lake City, 3) An on-line anonymous survey of 81 local providers and caregivers from the fields of transfusion medicine and perinatal/neonatal medicine. The survey assessed willingness to participate in, and perceived implementation barriers to, conducting a phase I trial to test the effect of processed and banked term umbilical cord blood (experimental treatment) vs. adult donor blood (standard treatment) to meet the RBC transfusions needs of all ELGANs in three Intermountain Health NICUs.
Summary of Results: In the past three years we cared for 266 ELGANs; 165 (62%) received ≥1 RBC transfusion. Our average annual number of RBC transfusions to ELGANs was 197 ± 76 (mean ± SD; 95% CI, 152 - 243). If only 10% of the 10,353 annual term births at the three target Intermountain hospitals had cord blood drawn and processed by the Red Cross, and only half of those were found acceptable for transfusion, collections would exceed the 95th% upper estimate for need by >four-fold. Forty% responded to the survey; 97% of respondents want their NICU to participate. Perceived implementation barriers included; training needed to collect and bank cord blood, infectious concerns, and consent fatigue of a heavily studied population.
Conclusions: Despite uncertainties in our projections, we judge it is feasible for our health system to begin a new experimental program to determine whether the RBC transfusion needs of ELGANs can be met using cord blood, collected, processed, safety-tested, and banked in a collaborative effort between Intermountain Health and the Red Cross.
# 367
Predictors and Neonatal Outcomes Associated with Prenatal Maternal Substance Use in Very Preterm Infants
Chang MA1, 2, Alag A2, 1, Biniwale M2, 1, Barton L2, 1, Ramanathan R2, 1, Cayabyab R2, 1. 1Los Angeles General Medical Center, Los Angeles, CA and 2University of Southern California, Los Angeles, CA
Purpose of Study: Maternal substance use (MSU) during pregnancy is associated with adverse neonatal outcomes, including preterm delivery. More research is needed to evaluate the effects of in-utero drug exposure among early preterm neonates. Our study objective was to identify neonatal characteristics and morbidities associated with prenatal exposure to MSU in preterm infants less than 32 weeks gestational age.
Methods Used: We performed a retrospective chart review of preterm infants less than 32 weeks gestational age (GA) admitted to a Level III neonatal intensive care unit (NICU) between 2017–2022. MSU of amphetamines, cocaine, opiates, cannabinoids, and benzodiazepines was determined by positive maternal or neonatal urine toxicology screens and/or self-report on admission.
Summary of Results: We identified 259 preterm neonates born less than 32 weeks gestational age, with 36/259 (14%) exposed to maternal substance use. Mothers with substance use had higher rates of psychiatric comorbidities, particularly mood disorders. Aside from increased HIV and syphilis diagnoses among mothers with substance use, there were no significant differences between the two cohorts in other maternal medical comorbidities, including diabetes mellitus and pre-eclampsia. Mothers with MSU were also less likely to receive antenatal steroids, magnesium sulfate , adequate prenatal care, and were more likely to be single, homeless, and unemployed. There were no significant differences in neonatal gestational age, birth parameters, delivery room resuscitation, and length of stay. While neonates with MSU were less likely to have respiratory distress syndrome and bronchopulmonary dysplasia, they had increased rates of seizure diagnosis, necrotizing enterocolitis (NEC), and retinopathy of prematurity (ROP) during their NICU admission. (Table)
Conclusions: Our study found that exposure to substance use among very preterm infants is associated with less respiratory comorbidities, but increased rates of NEC and ROP. More research is needed to guide appropriate care for preterm infants exposed to drugs prenatally.
Neonatology - Perinatal Biology I
Concurrent Session
8:00 AM
Friday, January 19, 2024
# 368
Mode of respiratory management of preterm lambs affects long-term neurobehavior outcomes and insulin-like growth factor-1 expression and epigenetic profile in the hippocampus
Simmons M1, Ke X2, Dawson E1, Headden D1, Bowen S1, Rebentisch A1, Van Boerum J1, Beachy J3, Null D1, Dahl MJ1, Lane RH2, Albertine K1. 1University of Utah, Salt Lake City, UT; 2Children’s Mercy Hospital, Kansas City, MO and 3Division of Newbron Medicine, Baystate Children’s Hospital, Springfield, MA
Purpose of Study: Preterm infants who receive invasive mechanical ventilation (IMV) suffer hippocampal dysfunction as evidence by impairment of learning, memory, and socialization. Hippocampal function depends on local expression of insulin-like-1 growth factor (IGF-1), a neurotrophin for which multiple variants are expressed and is under epigenetic miRNA regulation. We hypothesized that preterm lambs receinving NRS demonstrate better neurodevelopmental outcomes and normalized expression of hippocampal IGF-1.
Methods Used: Preterm lambs groups were (a) IMV ~7d (n=6), (b) IMV ~3h + noninvasive respiratory suport (NRS) ~7d (n=5), or (c) NRS resuscitation (face mask) + NRS ~7d (n=5). Neurobehavioral outcomes in the former preterm (FPT) lambs were tested at 2-months corrected postnatal age (cPNA; eq: 1-2y in humans) and 5-months cPNA (eq: ~6y in humans). Tests were non-reflective/reflective surface (socialization), maze (learning/memory), and novel object (curiosity). Hippocampi were analyzed at 5-months cPNA for IGF-1 mRNA and protein levels, and miRNA profiles related to cognitive impairment, The same analyses were made in unventilated term reference lambs (n=4).
Summary of Results: Outcomes are reported/lamb and by sex because of small sample size and large within-group variability. Lambs receiving NRS ~7d spent less time at the non-reflective surface, and finished the maze faster relative to the 2 IMV groups (Fig 1). Results for novel object assessment are not shown but provided similar outcomes. The 3 FPT groups had significantly lower abundance of endogenous IGF-1 protein than the term reference group (Fig 1). Concurrently, NRS retained expression of miR-23a whereas the IMV groups had low levels of miR-23a (Fig 1). Low expression of miR-23a is related to impaired cognition (Fig 1; Piscopo, Ageing Res Rev 2019).
Neurobehavioral results (top row) and hippocampal epigenetic results (bottom row).
Conclusions: Preterm lambs enduring NRS demonstrate better neurodevelopmental outcomes and normalized expression of hippocampal IGF-1 and IGF-1 miRNAs. We speculate that interventions that moderate the impact of IMV on hippocampal IGF-1 mRNA epigenetic profile will decrease the risk of learning, memory, and socialization impairments in individuals. Our next step is to determine the epigenetic regulation of the IGF-1 miRNAs.
# 369
Piezo1 In Smooth Muscle Cells Support Intestinal Epithelial Growth And Adaptation In A Murine Model Of Small Bowel Obstruction
Bautista G2, 1, Sweeney N1, McElroy S2, Martin MG1. 1University of California, Los Angeles, Los Angeles, CA and 2University of California, Davis, Sacramento, CA
Purpose of Study: Small bowel obstruction (SBO) is a common surgical emergency in neonates resulting from various pathological processes unique to the neonatal period. SBO leads to the dilatation or stretching of the bowel proximal to the site of obstruction, resulting in adaptive responses promoting growth. Piezo1 is a stretch-induced cation channel that modulates trophic effects in mechanosensitive tissues. Piezo1 is expressed throughout the intestine, including the smooth muscle cells (SMC) in the muscularis layer that contribute essential factors to the ISC niche critical for intestinal adaptation. However, the role of Piezo1 in mediating adaptive responses of the epithelium at homeostasis and following obstruction remains unknown. Here, we aimed to determine the potential role of SMCs Piezo1 on epithelial cell expansion and differentiation during homeostasis and following SBO. We hypothesized that loss of Piezo1 in the SMCs within muscularis layers will lead to an attenuated adaptive response to SBO.
Methods Used: Using the Piezo1/Myh11-ERT2/Cre-LoxP system, we generated mice with tamoxifen (Tam) inducible-Piezo1 knockout (Piezo1ΔSMC) in the SMCs of the small bowel muscularis. Mice at 28 days of age were given Tam or a vehicle, then subjected to either partial SBO surgery or sham surgery. The distal small bowel was resected for analysis. The crypt-villi axis was assessed for length and cellular composition. Immunofluorescence staining was performed to determine ISC expansion (Olmf4+) and proliferation (Ki67+), as well as specific populations of differentiated epithelial cell populations, including Paneth cells (PC, Lyz+) and goblet cells (GC, PAS). Statistics: Two-way ANOVA with posthoc analysis using FDR set to 5% was applied (n = 9-12 animals per group).
Summary of Results: Mortality rates were similar between Piezo1WT and Piezo1ΔSMC mice. Non-obstructed Piezo1ΔSMC mice had significantly deeper crypts and longer villi (p<0.0001). Furthermore,Piezo1ΔSMC mice had increased proliferation, ISC expansion, GCs (p<0.0001), but showed depletion of PCs (p<0.01) and EECs (p<0.0001) when compared to non-obstructed Piezo1WT. In response to prolonged partial SBO, Piezo1ΔSMC mice showed a 10% decrease in villi height compared to the 20% increase in obstructed WT mice. Additionally, obstructed Piezo1ΔSMC mice showed only a 30% increase in crypt depth with proliferation and ISC expansion, compared to the 80% increase in crypt depth and the expected increase in ISCs and proliferation in Piezo1WT mice (p<0.0001).
Conclusions: Piezo1 in SMCs may be integral in modulating the adaptive response to SBO within the epithelium. This data improves our understanding of how mechanosensitive channels may contribute towards epithelial homeostasis and adaptation, which may have implications for future therapies for patients with SBO and/or SBS.
# 370
L-ALANYL-L-GLUTAMINE INFUSION INTO FETAL SHEEP ACTIVATES REGULATORS OF SKELETAL MUSCLE PROTEIN SYNTHESIS
Stacey HE1, Chang EI1, Painter CS1, Eroglu EC1, Calero Herrera LM3, Wesolowski S1, Rozance P1, Barooni NB2, McCurdy CE2, Brown LD1. 1University of Colorado, Aurora, CO; 2University of Oregon, Eugene, OR and 3Animal Hospital, Los Fresnos, Peru
Purpose of Study: In fetuses with growth restriction (FGR) caused by placental insufficiency, skeletal muscle adapts to a low oxygen and nutrient environment by selectively releasing alanine and glutamine, presumably to support metabolic processes in vital organs. In critically ill adults and in rodent models of catabolism, L-alanyl-L-glutamine (AG) infusions have been shown to suppress muscle protein breakdown and stimulate protein synthesis. Thus, it is possible that AG infusions may similarly increase muscle protein synthesis in FGR fetuses. Before testing AG infusions in FGR fetuses, we aimed to determine the physiological impact of AG in normally growing fetuses.
Methods Used: Chronically catheterized fetal sheep (singleton and twins) were randomized to receive 0.5 g/kg/day AG (n=6) or saline (SAL, n=4) intravenously for 7 days at 90% gestation. Fetal arterial blood was sampled at baseline and every other day during the 7-day period to measure blood gases and plasma amino acid, glucose, lactate, cortisol, insulin, and IGF-1 concentrations. On day 6 of infusion, 10 g/kg 5-ethynyl-2’-deoxyuridine (EdU) was infused into the fetus to measure myoblast proliferation rates using flow cytometry. Fetal skeletal muscle was collected on day 7 to measure regulators of protein synthesis (phosphorylated and total mTORC1, Akt, p70S6 kinase, 4EBP1, and rpS6) and branched-chain amino acid (BCAA) catabolism (BCAT 1 and 2, BCKDH) by Western blot. Two-way ANOVA was performed to determine differences in plasma measurements between groups during the infusion period. Student’s t-tests were used to compare measurements made at the end of the study.
Summary of Results: AG resulted in 32%, 23%, and 150% higher fetal plasma glutamine, alanine, and cysteine concentrations, respectively, compared to SAL (group x time interaction; P≤0.06). Insulin, IGF-1, and cortisol concentrations did not differ between groups, nor did glucose, lactate, or oxygen. There were no differences in the expression of proteins within the BCAA catabolism pathway. However, the activated (phosphorylated:total) 4E-BP1 and rpS6 within muscle protein synthesis pathways were upregulated by 1.8-fold and 1.5-fold, respectively, in the AG group compared to SAL (P<0.05). There were no differences in rates of myoblast proliferation as measured by EdU incorporation into CD56+ myoblasts.
Conclusions: AG infusion into late gestation fetal sheep increased circulating plasma alanine and glutamine concentrations. The concentrations of other circulating amino acids were not affected except for cysteine, a likely consequence of upregulated glutamine metabolism. AG was well tolerated by the fetus with minimal effects on other hormones and substrates. Given the upregulation of key proteins that stimulate muscle protein synthesis in the AG group, we speculate the AG infusions may be effective in promoting muscle growth in FGR fetuses.
# 371
NET-INHIBITORY PEPTIDES INCREASE PLACENTAL AND FETAL GROWTH IN MOUSE MODEL OF HYPERTENSIVE DISEASE OF PREGNANCY
Strnad F, Tristao M, de Araujo C, Brown A, Wieben M, Cody M, Owen L, Fung C, Yost CC, University of Utah, Salt Lake City, UT.
Purpose of Study: Intrauterine growth restriction (IUGR) causes perinatal morbidity and mortality. In developed countries, IUGR most commonly results from uteroplacental insufficiency (UPI) caused by hypertensive disease of pregnancy (HDP). HDP increases placental neutrophil extracellular traps (NETs) in response to placental ischemia/reperfusion injury. The placenta regulates NET formation through expression of HTRA1, a serine protease, that cleaves the carboxy-terminus of alpha-1-antitrypsin to generate A1AT-CF, a NET-Inhibitory Peptide (NIP). Whether placental NETs contribute to UPI and IUGR in experimental HDP remains unknown.
Methods Used: We employed a well-established mouse model of HDP by infusing timed-pregnant C57BL/6 mouse dams with a continuous infusion of TXA2-analog via a micro-osmotic pump implanted on embryonic day (E) 12.5. Sham-operated dams with vehicle infusion acted as controls. To inhibit NET formation, we injected TXA2-or vehicle-exposed dams with either 10mg/kg A1AT-CF or a scramble peptide control (SCR) daily from E13-E18. Additionally, we treated TXA2-infused HTRA1+/- dams bred to HTRA+/- with A1AT-CF or SCR under the same conditions. We assessed placenta and pup weights. We used immunofluorescence to determine placental NET formation (citrullinated histone H3), neutrophils (myeloperoxidase), and platelets (CD41) on E19. For HTRA1+/- dams, pups and placentas were genotyped and analyzed according to genotype. We reported results as mean ± SEM and used the students t-test or the one way ANOVA with Tukey’s post hoc testing for comparisons of 2 or 3 groups respectively, with a p-value of <0.05 as significant.
Summary of Results: As expected, we demonstrated decreased placenta and pup weights in TXA2-exposed dams on E19. We found increased placental NETs and platelet levels in TXA2-exposed dams compared to vehicle controls but detected no difference in placental neutrophil levels. A1AT-CF decreased placental NETs and increased platelet levels in A1AT-CF treated dams compared to SCR treated dams with concomitant increases in placental and fetal weights at E19 compared to SCR treatment. Finally, HTRA1-/- pups demonstrated decreased weights, decreased placental weights, increased placental NETs, and decreased placental platelet levels compared to HTRA1+/- or HTRA1+/+ pups. A1AT-CF treatment of HTRA1+/- dams reversed these findings in HTRA1-/- pups as compared to HTRA1+/- or HTRA1+/+ pups of SCR-treated HTRA1+/- control dams.
Conclusions: NET inhibition with A1AT-CF, a NET inhibitory peptide, decreases placental NETs and IUGR in an experimental model of HDP. Global knock out of HTRA1 increases placental NETs and IUGR in this model, a phenotype reversed by dam treatment with A1AT-CF. These results suggest that placental NETs exacerbate UPI in this mouse model of HDP and that inhibiting placental NETs with HTRA1-dependent NIPs represents a novel therapeutic strategy to ameliorate IUGR in pregnancies affected by HDP.
# 372
ASSESSING THE EFFECTS OF BREASTMILK AND FORMULA ON NEONATAL IMMUNE DEVELOPMENT USING A PIGLET MODEL
Richter J1, Keele S2, Nunez L1, 2, Chen Y3, Fox M1, Childress A1, Fehrenkamp B1, 3. 1University of Washington School of Medicine, Moscow, ID; 2University of Idaho, Moscow, ID and 3University of Idaho, Moscow, ID
Purpose of Study: Breastfeeding is recommended for the first six months of life to provide optimal nutrition and immunological support. Breastfed infants have been observed to have lower rates of infection, allergies, and intestinal problems however, the mechanism of protection is currently unknown. Here we use a piglet model to study the effects breastmilk and formula have on the developing immune system specifically within the intestinal tract.
Methods Used: Neonatal littermate Yorkshire-Duroc piglet pairs were assigned to receive either human milk (HM, n=3) or infant formula (IF, n=3) and reared for 28 days. A pair that remained on the farm feeding on sow’s milk (n=2) was also obtained as controls. RNA was extracted from intestinal tissues and used for quantitative PCR (qPCR) to quantify gap junctional proteins of interest (zonula occludens (ZO)-1, ZO-2, and Claudin 1) as well as immune markers of interest including Interleukin 1 Beta (IL1B), along with white blood cell markers CD4, CD8A, and CD79b. Expression levels were normalized to GAPDH and B-actin.
Summary of Results: Expression levels of ZO1, ZO2, and Claudin 1 showed no statistically significant difference between the HM- and IF-fed groups showing no difference in the development of gap junctions. The lymphocyte markers CD4, CD8A, and CD79b were elevated in the HM-fed group compared to the IF-fed group. It is also noteworthy that through this study the gene specific primers (GSP) used were validated to be effective in the porcine model.
Conclusions: HM-feeding did not appear to affect gap junction expression of targets investigated, however HM-feeding does appear to promote proper lymphocyte infiltration into the gastrointestinal associated lymphoid tissue which may explain observed protective effects of breastfeeding compared to formula feeding in neonatal infants.
# 373
INCIDENCE OF PREGNANCY COMPLICATIONS WITH AND WITHOUT BIOLOGIC USE IN PATIENTS WITH INFLAMMATORY BOWEL DISEASE: A RETROSPECTIVE STUDY
Puri M, McCartney S. University of Washington, Seattle, WA
Purpose of Study: Biologic medications have become the standard of care for the treatment of Inflammatory Bowel Disease (IBD). However, data on the risks and benefits of continued use of biologics throughout pregnancy for patients with IBD is limited. Since biologics target the immune system, they may alter risks of pregnancy complications, which have been linked to inflammation. The purpose of this study is to assess the incidence of pregnancy complications in subjects with concurrent biologic therapy for IBD compared to no biologic therapies.
Methods Used: The population for this study includes patients from the University of Washington with IBD identified by retrospective chart review. Inclusion criteria were subjects who were pregnant, with a documented diagnosis of IBD prior to or during their pregnancy (Crohn’s Disease or Ulcerative Colitis, confirmed with a colonoscopy) with and without biologic use during pregnancy. Medical record abstraction was performed to identify demographic data, medications, and pregnancy characteristics. Statistical analysis was performed using Chi-squared test for categorical variables between subjects who received biologic therapies (monoclonal antibodies or small molecule inhibitors) and those who were treated with traditional disease modifying medications (mesalamine, steroids) during pregnancy. The primary outcome was composite risk of adverse pregnancy outcomes including preterm birth, preeclampsia, fetal growth restriction, and stillbirth/spontaneous abortion.
Summary of Results: 102 subjects with IBD during pregnancy were identified, 41 diagnosed with Ulcerative Colitis and 61 diagnosed with Crohn’s Disease. 40.2% (n=41) of patients were on Biologic therapies and 59.8% (n=61) were not on Biologic therapy during pregnancy. There was no significant difference in composite adverse pregnancy outcomes between subjects on biologics (34.1%, n=14) versus patients not on biologic therapy, (27.8%, n=17), p=0.82). Similarly, there were no significant differences in individual adverse pregnancy complications with and without use of biologics (Table 1).
Conclusions: These findings demonstrate no significant difference in adverse pregnancy outcomes in subjects with Inflammatory Bowel Disease exposed to biologic therapies. This provides evidence that the use of biologics in pregnancy for patients with IBD may be low risk, but requires further investigation in a larger cohort.
Instance of Pregnancy Complications Stratified by Complication.
IMPROVING READABILITY AND ACCESSIBILITY OF POST-OPERATIVE INSTRUCTIONS IN BREAST RECONSTRUCTION USING CHAT GPT
Small EA1, Carlson PF1, Thomas LE1, Gupta S2. 1Loma Linda University, Loma Linda, CA and 2Loma Linda University, Loma Linda, CA
Purpose of Study: After patients undergo breast reconstruction surgery, they are provided with post-operative instructions to guide them through the recovery process. However, these instructions may be challenging for patients to understand and hinder patients’ comprehension and adherence to the guidelines. This research project aims to investigate the potential use of artificial intelligence (AI) in enhancing the readability, comprehensiveness, and accuracy of post-operative instructions for breast reconstruction patients.
Methods Used: A selection of online resources was made based on a Google search of popular sources for breast reconstruction post-operative care. To assess the readability of the selected resources, we employed readable.com to analyze the text based on various established literacy formulas. The readability formulas used were Flesch-Kincaid (FK), Simple Measure of Gobbledygook (SMOG), Coleman Liau Index (CLI), and Gunning Fog (GF). These metrics allow us to quantify the readability of written materials by estimating the grade level required to comprehend the text. Subsequently, we utilized ChatGPT to develop post-operative breast reconstruction instructions at a 6th-grade level. The original instructions from the selected online resources were compared with the modified instructions generated by the AI model regarding readability, comprehensiveness, and accuracy. Similarly, the standard breast reconstruction postoperative instructions from Loma Linda University Hospital (LLUH) were analyzed in the same format.
Summary of Results: The average grade level of online resources according to FK, SMOG, CLI, and GF were 7.17, 10.66, 9.51, and 9.73, respectively. Therefore, the average grade level for online post-op resources across all indices used was 9.26. Chat GPT generated instructions at an average grade level of 7.76. The difference between resources found online and those generated by Chat GPT was a difference of 1.51 grade levels. The LLUH instructions resulted in FK: 5.16, SMOG: 8.41, CLI: 7.54, and GF: 6.63. The average grade level of LLUH post-operative instructions between the indices was 6.94.
Conclusions: Our research aimed to explore the utility of AI in enhancing post-operative instructions for breast reconstruction patients. Clearer instructions lead to better adherence from patients and overall improved recovery after surgery. Chat GPT demonstrated the ability to generate thorough and accurate instructions at a reading level almost one and a half grades lower than the average online resource. LLUH’s reading level of 6.94 demonstrates their efforts in addressing healthcare disparities within San Bernardino County. Our research hopes to demonstrate AI’s potential in reducing literacy barriers and improving healthcare disparities in underserved populations.
# 375
IS IT POSSIBLE TO IDENTIFY PATIENTS AT RISK FOR BREAST IMPLANT ILLNESS? A COMPREHENSIVE CHART REVIEW
Thomas LE1, Carlson PF1, Small EA1, Gupta S2. 1Loma Linda University, Loma Linda, CA and 2Loma Linda University, Loma Linda, CA
Purpose of Study: Breast implant illness (BII) refers to a collection of symptoms and health issues that some individuals with breast implants self-report. While breast implants have been widely used for cosmetic and reconstructive purposes, there has been growing concern over the potential association between these implants and various systemic symptoms. BII is not a medically recognized diagnosis but rather a term used to describe a range of symptoms that some people attribute to their breast implants including fatigue, cognitive difficulties, joint and muscle pain, hair loss, and sleep disturbances. A comprehensive study analyzing BII incidence and patient demographics could determine its prevalence, risk factors, and inform safer breast implant surgery guidelines.
Methods Used: A list of patients who have undergone breast implant surgery in Loma Linda University Department of Plastic Surgery was collected between the years 2018-2023. From this patient data, those who have undergone breast explant surgery were isolated. Patients with implant-related infections or dissatisfaction with appearance were excluded. Demographics of the remaining patients were assessed to identify possible risk factors associated with breast implant illness.
Summary of Results: Of the 29 patients that had undergone isolated breast explanation at Loma Linda University, 7 patients were identified as having symptoms of breast implant illness. These symptoms included back pain, difficulty breathing, joint pain, malaise, and fatigue. The demographic factors of age, BMI, implant size, history of radiation, diabetes, hypertension, dyslipidemia, and autoimmune disease were assessed between the patients with breast implant illness symptoms and those without symptoms. These variables were investigated as possible factors for unfavorable surgical outcomes. Our retrospective chart review fails to demonstrate any demographic or clinical factors that consistently correlate with patients undergoing an explant procedure and those who experience breast implant illness symptoms.
Conclusions: The absence of identifiable demographic predictors suggests no reliable basis for screening patients for susceptibility to breast implant illness (BII) before breast augmentation consultations. This also questions the credibility and scientific validity of BII, as no consistent demographic associations have been found. While some patients report symptoms linked to breast implants, the lack of clear markers makes it challenging to establish a cause-and-effect relationship. BII remains a subject of controversy, but healthcare professionals should acknowledge positive outcomes post-explantation and prioritize addressing patients’ health concerns. As such, healthcare professionals and patients should approach discussions of breast implant illness with a balanced and evidence-based approach. Further research is needed to better understand the causality of these symptoms and to better educate patients about what is known and unknown about this spectrum of symptoms.
Demographic Factors.
BII patients
Non-BII patients
History of Radiation
1
0
Type 2 Diabetes
2
3
Hypertension
0
5
Dyslipidemia
2
3
Autoimmune Disease
1
0
BMI>30
1
6
# 376
Evaluating the aging larynx in F344 Brown Norway rats
Adcock K1, Aboueisha M2, Jaleel Z2, Cvancara D1, Bhatt N2. 1University of Washington School of Medicine, Seattle, WA and 2University of Washington, Seattle, WA
Purpose of Study: In the aging larynx nerves and musculature atrophy, which can lead to alterations in voice quality, muscle coordination and strength while swallowing. This age-related vocal atrophy (ARVA) can lead to poor voice quality, diminished laryngeal sensation, and increased risk of aspiration. By coming to better understand the neurophysiologic changes that cause this laryngeal atrophy, the effectiveness of existing and future treatments could be better evaluated. To this end, we hope to establish a rat model in which we can evaluate these changes and analyze their effect on variables such as cough, aspiration and nerve injury.
Methods Used: 10 Fischer 344xBrown Norway (F344xBN) rats were used in this study (5 non-aged (4 months), 5 aged (21 months)). Under anesthesia, endoscopy was used to calculate the bowing index (BI), abduction angle, and normalized vocal fold width (NVFW), which were quantified by 3 blinded raters. Laryngeal motor evoked response studies were performed by stimulating the recurrent laryngeal nerve (RLN) with an active electrode inserted into the thyro-arytenoid muscle. The compound motor action potential (CMAP) was analyzed along with Latency, Amplitude, Neg. Duration, Neg. Area and Motor unit number estimation (MUNE). Finally, the RLN’s and larynx were removed, fixed, embedded and sectioned for analysis. Slides were prepared using toluidine blue stain and analyzed using the AxonDeepSeg plugin for axon diameter, % myelin and g-ratio.
Summary of Results: 10 non-aged (4-month) vs.10 aged (21-month) rat hemi-laryngeal preparations were included in this study. The mean BI was higher in the aged group compared to non-aged group, 5.02±1.05 vs. 4.12±1.05 units, respectively, and this difference approached statistical significance (mean difference 0.89 units, 95% CI: -0.10 – 1.80 units, p=0.07). There was no significant differences in abduction angle and NVFW. CMAP latency was significantly higher in the aged vs. non-aged group, 0.90 ± 0.05 ms compared to 0.84 ± 0.06 ms, respectively (mean difference 0.06 ms, 95%CI: 0.01–0.11 ms, p=0.02). Mean % myelin in the aged rats vs the non-aged rat was 70.70±15.76% and 75.79 ± 9.24%, respectively, mean difference 4.08% (95%CI: -4.83 – 13.02%, p=0.59).
Conclusions: The consistent successful quantification of several ARVA variables in this project is a success, and the data suggest that the aging rat larynx is a useful model in studying ARVA. We found a statistically significant increase in CMAP latency and an increase in BI that approached statistical significance in the aged rats. With this reliable methodology, we could repeat this experiment with an older and larger cohort, further investigating the strength of this model. Visible changes such as bowing are valuable markers of the aging process used clinically today, and if further analysis can establish the F344 BN rat as an effective aging model for the larynx, we could have a valuable tool for investigating significant causes of pathology such as aspiration in our increasingly aging population.
# 377
THE SYMPTOM SPECTRUM OF GLOTTIC INSUFFICIENCY AND LARYNGOPHARYNGEAL REFLUX IN THE AGING POPULATION
Vacaru A2, Feng M1, Adebowale A2, Bahjri K3, Krishna P1, Crawley B1. 1Loma Linda University Health, Loma Linda, CA; 2Loma Linda University School of Medicine, Loma Linda, CA and 3Loma Linda University School of Pharmacy, Loma Linda, CA
Purpose of Study: This study seeks to investigate the degree of symptom overlap and response to treatment in glottic insufficiency (GI) and laryngopharyngeal reflux (LPR) in the aging population. We hypothesize that patients diagnosed with both GI and LPR are often unnecessarily being prescribed acid-suppression therapy and can be successfully treated with voice interventions.
Methods Used: A retrospective review of patients over the age of 50 with a primary diagnosis of GI and LPR, determined by a reflux severity index (RSI) score of greater than 12 points, at a tertiary academic center between 2018-2022 was performed. Patient demographics, diagnosis, and symptoms of mucus, throat clearing, dysphonia, globus sensation, or dysphagia were recorded. Patients received either medical therapy—LPR medical therapy and/or voice therapy, or surgical intervention—vocal fold injection augmentation, thyroplasty, and/or transnasal esophagoscopy with esophageal dilation. All patients who received surgical intervention had previously received medical therapy. Voice handicap index (VHI), RSI, cough severity index (CSI), and eating assessment tool (EAT-10) scores were collected before and after surgical or medical intervention.
Summary of Results: Seventy-eight patients met inclusion criteria, with 52 patients (66.7%) in the surgical intervention group and 26 patients (33.3%) in the medical intervention group. The mean age was 72.3 ± 9.8 and 65.3 ± 10 in the surgical intervention group and medical intervention group, respectively. There was no statistically significant difference between the two groups for symptoms of throat clearing, mucus sensation, globus sensation, cough, and dysphagia (
Table 1
). Symptoms of dysphonia were statistically greater in the surgical intervention group (88.5%) compared to the medical intervention group (69.2%) (p=0.037). There was a statistically significant improvement in pre- and post-treatment RSI scores in both the surgical and medical intervention groups (p<0.001). There was no significant change in VHI scores in both groups (p=0.297), though the mean pre- and post-treatment scores were higher in the surgical intervention group (p<0.001). There was a statistically significant improvement in pre- and post-treatment EAT-10 scores in the surgical intervention group (-5.4 points, p=0.023), but not in the medical intervention group (+0.2 points).
Clinical characteristics.
Surgical
Medical
P-value
Throat clearing
20 (38.5%)
14 (53.8%)
0.196
Mucus sensation
19 (36.5%)
13 (50%)
0.255
Dysphonia
46 (88.5%)
18 (69.2%)
0.037*
Globus sensation
15 (28.8%)
12 (46.2%)
0.130
Cough
29 (55.8%)
13 (50%)
0.630
Dysphagia
32 (61.5%)
16 (61.5%)
0.999
Positive pH probe
0 (0%)
8 (30.8%)
<0.001*
All values represent count and percentage. * indicates significance at an alpha of 0.05.
Conclusions: Throat clearing, mucus sensation, globus sensation, cough, and dysphagia might result from underlying age-related voice changes and GI rather than solely LPR. This highlights that symptoms of reflux can be successfully treated with voice interventions, avoiding the need for prolonged acid-suppression therapy and their side effects.
# 378
NOVEL LATERAL TUNNEL FONTAN PROCEDURE IN CHILDREN PROMOTES CONTINUED PATHWAY GROWTH INTO ADULTHOOD
Marciniak M, Razzouk J, Tran J, Jutzy G, Fortuna R. Loma Linda University, Loma Linda, CA
Purpose of Study: The Fontan procedure for palliation of single ventricle congenital heart disease creates a direct blood flow pathway from the inferior vena cava to the pulmonary arteries early in childhood. The most commonly used technique utilizes a fixed-size Gore-Tex tube for the blood flow pathway. Our novel technique, the External Pericardial Lateral Tunnel Fontan (EPLTF), creates a pathway utilizing the patient’s pedicled pericardium and atrial wall. We hypothesize that viable, autologous tissue preserves growth potential of the pathway into adulthood and correlates with increasing body surface area (BSA).
Methods Used: A single-center retrospective review of serial echocardiographic images of the blood flow pathway following the EPLTF procedure. Echocardiographic measurements of the pathway diameter were recorded at two locations: the inferior vena cava junction with the Fontan and mid conduit, approximately 1 cm away from the junction. BSA was calculated at the time of each echocardiogram.
Summary of Results: 1155 echocardiographic images from 172 patients up to 24 years following the EPLTF procedure were identified. Average patient age at time of procedure was 2.9 years +/- 1.6 years. Significant enlargement of the pathway at the inferior vena cava junction and mid conduit is observed (p<0.001, p<0.001). There is significant correlation of increasing pathway size with increasing BSA (p<0.001).
Conclusions: The External Pericardial Lateral Tunnel Fontan surgical technique provides a viable, autologous option for creation of the Fontan blood pathway that is able to grow into adulthood. Correlation of pathway size with increasing BSA suggests that pathway growth may be a response to increasing physiologic demands of somatic growth. Further studies are needed to investigate the impact of this novel technique on patient outcomes.
# 379
Diving Deeper: Does Deep Learning Reconstruction Improve Subjective CT Image Quality in Patients with Metal Hardware?
Crew R1, Smith J4, Farkouh A1, Kassir M4, Escobar-Poni B2, Cheng K1, Chung JH3, Song S1, Kim U1, Quines JF1, Sajdak G1, Hanessian KA1, Okhunov Z1, Amasyali A1, Baldwin D1, Oberg K2, Baldwin D1. 1Loma Linda University Health, Loma Linda, CA; 2Loma Linda University School of Medicine, Loma Linda, CA; 3Loma Linda University Health, Loma Linda, CA and 4Loma Linda University Health, Loma Linda, CA
Purpose of Study: Performing and interpreting CT scans in patients with metal hardware may be challenging due to the metal artifact causing image distortion and obscuring visibility of anatomic structures, particularly when lower radiation doses are utilized. Those with metal prostheses presenting with signs and symptoms of urinary stones may therefore pose a diagnostic challenge and require a higher radiation dose for diagnosis. The purpose of this study was to compare image quality of CT scans with and without deep learning reconstruction (DLR) and metal artifact reduction at conventional, low, and ultra low dose radiation settings for the detection of distal ureteral stones in the presence of metal hip prostheses.
Methods Used: Ten different urinary system combinations were each separately implanted into a cadaver vehicle with a bilateral metal hip replacement. Each combination was scanned under three different radiation doses (Conventional Dose (CD)=141 mAs, Low Dose (LD)=30 mAs, and Ultra Low Dose (ULD)=7.0 mAs). For each radiation dose, two scans were obtained: one with single energy metal artifact reduction (SEMAR) and Advanced intelligence Clear IQ Engine (AiCE), which is a clinically validated DLR, and a second scan with no additional reconstruction. A total of 60 scans were collected. The CT scans were acquired using a Canon Aquilion One Genesis CT equipped with SEMAR and AiCE. Images were reconstructed with a 2.5 mm section width. Utilizing a modified 5 point Likert scale, a blinded radiologist ranked each image in terms of Artifact, Image Noise, Image Sharpness, Overall Quality, and Diagnostic Confidence, with lower scores indicating worse outcome and higher scores indicating better outcome. The t-test was used to compare image quality with and without the use of DLR and metal artifact reduction at each dose setting.
Summary of Results: Of the six treatment groups, ULD without AiCE and SEMAR subjectively had the worse image quality. ULD with AiCE and SEMAR resulted in significantly improved image quality in all 5 measured domains (p<0.05 for all). At LD, AiCE and SEMAR resulted in significant improvment in artifact and image noise (p<0.05 for both), but not in image sharpness, overall quality, and diagnostic confidence (p>0.05). At CD, use of AiCE and SEMAR did not result in significant improvement in any of the image quality domains (p>0.05 for all).
Conclusions: The incorporation of a DLR in Ultra Low Dose CT scans was demonstrated to outperform Normal Dose CT in every category measured by the Likert scale. These results are encouraging to the use of Ultra Low Dose CT with AiCE and SEMAR in clinical practice, which would reduce unnecessary radiation exposure to patients with metal hip replacements.
# 380
SUBCHONDRAL RAFTING WIRES MAY PREVENT TIBIAL PLATEAU FRACTURE SUBSIDENCE
Patterson JT, Rusu D, Duong A, Satish V, Yang M, Mayer L. Keck School of Medicine of USC, Los Angeles, CA
Purpose of Study: Tibial plateau fractures often require operative fixation to restore alignment and stability of the joint. Patients may experience post-operative articular subsidence of the tibial plateau after fixation, which may be associated with post-traumatic arthritis and poor functional outcomes. We hypothesized that the use of subchondral rafting wires is associated with a decreased incidence of post-operative subsidence.
Methods Used: Patients (18+ years) who underwent open reduction and internal fixation (ORIF) for tibial plateau fractures at a level 1 trauma center from 2018-2023 were identified and grouped based on retained subchondral rafting wire use. Potential confounding covariables were collected by chart review. Linear and angular subsidence were measured by comparing differences between immediate post-operative and follow-up tibial plateau radiographs (figure 1). Welch two sample t-tests were performed for normalized linear and angular subsidence between the groups with retained or removed rafting wires. Associations between subsidence and patient, injury, and treatment covariables were assessed through multivariable linear regression.
Summary of Results: 179 patients with mean follow-up time of 217 days were identified. Of those, 15 patients retained subchondral rafting wires as definitive implants while 164 patients did not retain subchondral rafting wires. Patients with retained rafting wires experienced less linear subsidence (-0.52 log[mm] vs –1.92 log[mm], 0.30 mm vs 0.012 mm, p<0.001) and less angular subsidence (-0.55° vs 0.93°, p=0.003) as represented by a positive difference in medial proximal tibial angle (MPTA). Linear regression demonstrated that retained rafting wires, sex, depressed plateau area, and active smoking had significant effects (p<0.05) on linear subsidence, while retained rafting wires, osteoporosis, Charleston Comorbidity Index (CCI), AO-OTA classification, and race had significant effects (p<0.05) on angular subsidence.
Conclusions: Use of retained subchondral rafting wires was significantly associated with less linear and angular subsidence. However, current literature suggests the difference in subsidence may be clinically insignificant (<2 mm). Known risk factors were confirmed to significantly contribute to the degree of articular subsidence. Further studies may be warranted to determine whether retained subchondral rafting wires improve functional outcomes after tibial plateau fracture as well as the degree of post-operative subsidence associated with complications.
Multivariable Linear Regression Analysis on Normalized Linear Subsidence and Angular Subsidence (Statistically Significant Covariates).
Log Linear Subsidence
Variable
Coefficient
T-Value
P-Value (<0.05)
Retained wires
-1.37
-4.67
<0.001
Sex (Male)
0.49
2.63
0.009
Depressed Area
0.001
2.16
0.032
Active Smoker
0.46
2.53
0.012
Angular Subsidence
Variable
Coefficient
T-Value
P-Value (<0.05)
Retained wires
1.52
2.15
0.033
AO-OTA Classification (41C3.2)
-6.28
-2.09
0.038
AO-OTA Classification (41C3.3)
-5.69
-2.04
0.043
AO-OTA Classification (41B1.3)
-8.02
-2.5
0.015
Race (Multiple)
-2.32
-2.32
0.022
Osteoporosis
13.65
2.51
0.013
CCI
-1.23
-2.12
0.036
Linear subsidence measured from joint line to most depressed part of articular surface.
# 381
SILICON MEETS SURGERY: THE AI-DRIVEN EVOLUTION OF PLASTIC SURGERY RESEARCH
McMath KR, Gupta S. Loma Linda University Health, Loma Linda, CA
Purpose of Study: The fusion of technology and medical science heralds a renaissance in research methodologies. We sought to examine the transformative potential of AI-powered research tools, particularly focusing on the literature review phase, and to determine how such tools can expedite and enrich every facet of the plastic surgery research process.
Methods Used: Our approach began with the integration of six AI-powered workflows, each requiring a mere 10 minutes to master, to accelerate the literature review process:
-Utilizing Elicit or Evidence Hunt to source papers and subsequently creating a "knowledge base" in Dante AI to facilitate queries about these documents (Elicit.org & evidencehunt.com).
-Employing Connected Papers to procure articles, which were then downloaded and incorporated into Zotero for detailed reading and note-taking (Connectedpapers.com).
-Leveraging Litmaps to search for relevant articles, with a subsequent strategic use of Litmaps-Zotero integration to bolster organization within Zotero (Litmaps.com).
-Deploying Iris’s "concept maps" to trace papers that align with the project’s theme (Iris.ai).
-Adopting R Discovery’s smartphone application to stay updated with the latest publications in the domain. These papers are then automatically synchronized with both Zotero and Mendeley (R Discovery phone app).
-Employing Inciteful to craft graphical representations highlighting relationships between a specific paper and its counterparts in the field (Inciteful.xyz).
Progressing from these workflows, we advanced to the experiment design and data analysis phases, leaning heavily on AI tools like "DeepLearning.ai" and "TensorFlow" for in-depth data exploration.
Summary of Results: Our study illuminated the multifaceted potential of AI in reshaping research dynamics. The literature review phase, fortified by the six workflows, showcased enhanced depth, breadth, and efficiency. Experimental designs and data analysis, amplified by AI, unraveled profound insights, ensuring surgical research that was both innovative and deeply relevant.
Conclusions: The convergence of AI tools and workflows, such as Elicit, Evidence Hunt, Dante AI, and TensorFlow, amongst others, is poised to revolutionize plastic surgery research. As these digital allies become integrated into the research landscape, we stand at the brink of an era characterized by enhanced depth, precision, and groundbreaking discoveries.
Translational Science
Concurrent Session
8:00 AM
Friday, January 19, 2024
# 382
A Pair of Conserved Fox/Sox Binding Sites Are Essential for GARR-Mediated Regulation of GDF5
Lee Y, Yeboah R, Phillips J, Pira C, Oberg K. Loma Linda University, Loma Linda, CA
Purpose of Study: Mutations in Gdf5, a secreted joint marker, are linked to multiple skeletal malformations and a higher risk for osteoarthritis, underscoring its importance in skeletal and joint development. The mechanisms that maintain Gdf5 expression during joint formation are still under investigation. We (and others) have previously identified a conserved Gdf5-associated regulatory region (GARR) that may provide a risk locus for osteoarthritis. Predicted binding sites for skeletal and joint-associated Fox, Sox, and Osr2 transcription factors (TFs) within GARR provide a mechanism for Gdf5 regulation and maintenance: In the murine model, there are two binding sites for both Fox and Sox TFs (Fox/Sox sites), two for only Sox TFs (Sox-only sites) and a single Osr2 binding site. We previously reported that the pair of Fox/Sox sites were necessary for murine GARR activity, while the Sox-only sites inhibited activity, and the Osr2 site did not contribute to the activity.
Methods Used: Several species have other predicted Fox/Sox, Sox-only, and Osr2 sites within GARR. Chicken GARR (cGARR) has three additional Fox/Sox sites and two predicted Osr2 binding sites. We hypothesized that the conserved pair of Fox/Sox sites were necessary for GARR activity across vertebrates. Thus, we created a GFP-reporter construct with the conserved cGARR sequence and mutated the predicted binding motifs for the conserved Fox/Sox sites, Osr2 sites, and the Sox9 sites. We assessed the enhancer activity of the mutated reporter constructs in an in ovo chicken wing bud bioassay and an in vitro cartilage micromass assay.
Summary of Results: Wildtype cGARR had normal enhancer activity in the developing joints of the chicken forelimb. Mutations of the two conserved Fox/Sox sites in cGARR were enough to markedly reduce enhancer activity despite three additional Fox/Sox sites. However, similar to the murine GARR, mutation of the two predicted Osr2 binding sites in cGARR did not alter activity.
Conclusions: Our results suggest that the two conserved Fox/Sox sites, present in most limb-having vertebrates, are essential for GARR-mediated regulation of Gdf5 and are not redundant with other fox/Sox sites. Further identification of the native Fox/Sox TF bound to these sites will help to establish their role in regulating GARR activity during development and joint maintenance.
Vyhmeister E2, 1, Britton J1, Pira C1, Oberg K1, 2. 1Loma Linda University, Loma Linda, CA and 2Loma Linda University, Loma Linda, CA
Purpose of Study: During limb development, fibroblast growth factors (FGFs) from the apical ectodermal ridge (AER) coordinate proximodistal outgrowth, while sonic hedgehog (SHH) secreted from the zone of polarizing activity (ZPA) directs anteroposterior patterning and expansion. SHH and FGF both regulate each other’s expression in a positive feedback loop. The pioneer transcription factor LIM homeodomain 2 (LHX2) is an intermediate the FGF-to-SHH loop and enhances wound healing and skin re-epithelization post injury. We have identified two LHX2-associated subAER cis-regulatory modules (LASARM1 and LASARM2) that are active within the LHX2 expression domain and contain binding sites for FGF-regulated ETS transcription factor proteins. These binding sites are necessary for LASARM activity. We hypothesize that ETS transcription factors are expressed in the LHX2 expression domain and bind to LASARM to regulate LHX2.
Methods Used: To determine whether ETS transcription factors are co-expressed with Lhx2, we analyzed the expression of ETS transcription factors in cell populations expressing LHX2 using published mouse forelimb single-cell RNA sequencing data (scRNA-seq) and performed whole mount in situ hybridization (WMISH) on chicken forelimbs. To investigate whether ETS proteins bind to LASARM1 and LASARM2, we performed chromatin immunoprecipitation (ChIP) on mouse limb buds using ETS antibodies followed by PCR to detect and quantify LASARM1 and 2 targets.
Summary of Results: scRNA-seq analysis revealed the co-localization of ETS transcription factors Ets2, Etv4 and Etv5 in Lhx2+ cells, and WMISH confirmed that these are expressed in the limb bud overlapping LHX2 expression distally. Investigation of the binding of ETS proteins to LASARM1 and 2 is in progress.
Conclusions: Our findings show that Ets2, Etv4 and Etv5 proteins are present in cells expressing Lhx2 and are likely to bind to ETS binding sites within LASARM1 and 2 to regulate activity. Moreover, this data provides a mechanism by which FGF, through ETS transcription factors, activates LASARM1 or 2 to regulate LHX2 expression. Further work is needed to confirm this connection.
# 384
LMX1B BOUND CIS-REGULATORY MODULES ASSOCIATED WITH GDF5 THAT LACK LMX1B BINDING SITES HAVE WEAK ENHANCER ACTIVITY
Phillips J, Yeboah R, Pira C, Lee Y, Oberg K. Loma Linda University, Loma Linda, CA
Purpose of Study: LIM homeobox transcription factor 1-beta (Lmx1b) is involved in dorso-ventral patterning of limbs. Haploinsufficiency of Lmx1b causes Nail-Patella syndrome (NPS), a condition characterized by hypoplastic or missing dorsal structures such as the patella. Patients with NPS also have an increased risk of accelerated osteoarthritis. To understand how Lmx1b regulates joint development, we identified that Growth Differentiation Factor 5 (Gdf5), a marker of developing synovial joints linked to joint maintenance, was upregulated by Lmx1b during limb development. Additionally, Lmx1b was found to bind to three potential cis-regulatory modules (PCRM1-3) in the Gdf5 locus during limb dorsalization. Previously we showed that CRM3, now known as Gdf5-associated regulatory region (GARR), has robust joint-associated activity overlapping Gdf5 expression. We hypothesized that PCRM1 and 2 would also exhibit activity coincident with Gdf5 expression.
Methods Used: To test our hypothesis, we examined the chromatin interaction between PCRM1 and 2 and the Gdf5 promoter to demonstrate their potential for Gdf5 regulation. Since PCRM1 and 2 were identified through Lmx1b binding, we evaluated their sequences for Lmx1b binding sites. We also tested PCRM activity in micromass cartilage culture and in the developing elbow of chicken embryos through targeted regional electroporation.
Summary of Results: PCRM1 and 2 were positive for active chromatin marks and were accessible during limb development. Chromatin conformation data revealed that both regions interact with the Gdf5 promoter, but with less frequency than GARR. Both PCRM1 and 2 exhibited weak enhancer activity in cartilage culture and in the developing chicken elbow. Interestingly, no Lmx1b binding sites were identified in either sequence.
Conclusions: Since CRM1 and 2 do not have predicted Lmx1b binding sites, our results suggest that they are likely not critical for direct Lmx1b-mediated regulation of Gdf5. However, CRM1 and 2 may contribute to Gdf5 regulation through an Lmx1b-associated regulatory complex. Further sequence evaluation is needed to assess for possible Lmx1b co-factor binding sites.
# 385
THE ROLE OF LIPASE MATURATION FACTOR 1 IN MULTIFACTORIAL CHYLOMICRONEMIA SYNDROME
Chen P, McCleary X, Peterfy M. Western University of Health Sciences College of Osteopathic Medicine of the Pacific, Pomona, CA
Purpose of Study: Hypertriglyceridemia (HTG) is a common clinical condition characterized by abnormal elevation of serum triglyceride levels. Severe HTG (> 885 mg/dl) is associated with pancreatitis, cardiovascular disease, hepatic steatosis and exhibits dual etiology. In a minority of patients, it is a monogenic disease (familial chylomicronemia syndrome, FCS) due to biallelic mutations in genes involved in TG catabolism. More commonly, severe HTG is polygenic and results from the presence of heterozygous variants interacting with non-genetic factors (multifactorial chylomicronemia syndrome, MCS). The genetic determinants of FCS and MCS overlap and include genes involved in the regulation of Lipoprotein Lipase (LPL)-mediated TG clearance. One of these genes is Lipase Maturation Factor 1 (LMF1), a chaperone required for the expression of active LPL. While LMF1 has been established as a canonical gene in FCS, its potential role in MCS remains poorly understood. Thus, in the present study we hypothesize that heterozygous loss-of-function mutations in LMF1 contribute to HTG in MCS. To investigate this hypothesis, we assess the impact of heterozygous LMF1 deficiency on plasma TG levels in the presence or absence of LPL-deficiency and high-fat (HF) diet feeding in mouse models. We anticipate that our study will provide insights into the genetic etiology of MCS.
Methods Used: To investigate the metabolic impact of LMF1 deficiency and the genetic interaction between LMF1 and LPL, heterozygous LMF1 knock-out (LMF1+/-) and double heterozygous (LMF1+/-;LPL+/-) mice were generated. Steady state plasma TG levels were assayed after 4 hours of fasting and the rate of TG clearance was assessed by measuring the time-course of plasma TG concentration after a bolus intravenous injection of Intralipid. To model the non-genetic component of MCS, mice were fed a 60% HF diet for 20 weeks. Body weight and composition was determined weekly by NMR analysis.
Summary of Results: Heterozygous LMF1 deficiency had no effect on fasting TG concentrations or the rate of TG clearance in male or female mice in the presence or absence of heterozygous LPL deficiency on either chow or HF diets. In contrast, heterozygous LPL deficient mice exhibited significantly elevated fasting TG and reduced TG clearance. Unexpectedly, LMF1 and LPL heterozygosity had opposite effects on body weight and composition in females on the HF diet.
Conclusions: Our results fail to demonstrate an effect of heterozygous LMF1 deficiency on plasma TG catabolism even when combined with LPL heterozygosity and the metabolic stress of HF diet feeding. We conclude that, at least in the mouse, LMF1 expression is not rate-limiting in TG catabolism and heterozygous mutations in LMF1 are unlikely genetic contributors to MCS in humans. However, our study unexpectedly revealed LMF1 haploinsufficiency in the regulation of body weight and composition, a novel aspect of LMF1 biology warranting further mechanistic investigations.
This work was supported by NIH grant HL154071.
# 386
FUNCTIONAL ANALYSIS OF MISSENSE MUTATIONS IN LIPASE MATURATION FACTOR 1 IN FAMILIAL CHYLOMICRONEMIA SYNDROME
Samara H, Peterfy M. Western University of Health Sciences, COMP, Pomona, CA
Purpose of Study: Familial chylomicronemia syndrome (FCS) is an autosomal recessive disease of aberrant chylomicron metabolism resulting in severely elevated plasma triglycerides (TG) and a high risk for acute pancreatitis. FCS is due to mutations affecting lipoprotein lipase (LPL) or other factors involved in LPL-mediated TG catabolism. Lipase maturation factor (LMF-1) is a chaperone in the endoplasmic reticulum critically required for the posttranslational maturation and enzymatic activity of LPL. Previous studies identified rare nonsense LMF-1 mutations and established LMF-1 as a canonical gene in FCS. In the present study, we functionally characterize four homozygous missense variants in LMF-1 associated with severe hypertriglyceridemia (HTG). Our objective is to gain novel insights into the LMF-1 structure-function relationship and the molecular etiology of FCS.
Methods Used: The potential functional impact of missense variants was predicted using in silico analyses. LMF-1 protein expression was analyzed by western blotting using lysates from transiently transfected cells. The lipase maturation activity of LMF-1 was assessed in a reconstitution assay based on LMF-1 deficient HEK293 cells co-transfected with LMF-1 and LPL. LPL activity in culture media served as a proxy for LMF-1 function. The interaction between LMF-1 and LPL was evaluated by co-immunoprecipitation from transfected cells.
Summary of Results: In silico analysis indicated that all four missense mutations analyzed in this study (p.N147K, p.P246R, p.R354W, p.R364Q) are likely to be deleterious to LMF-1 function. Indeed, immunoblot analysis revealed that p.N147K and p.R354W virtually abolished LMF-1 protein expression. While p.P246R and p.R364Q had no apparent impact on protein amount, both mutations reduced the lipase maturation activity of LMF-1. Co-immunoprecipitation experiments demonstrated that the interaction of p.P246R and p.R364Q with LPL was indistinguishable from that of wild-type LMF-1.
Conclusions: In the present study, we functionally characterized four novel HTG-associated missense mutations in LMF-1. Overall, our results demonstrate that all variants impair the LPL-maturation function of LMF-1 and establish these mutations as novel genetic determinants of FCS. Our data also indicate that the variants affect LMF-1 function through different mechanisms. p.N147K and p.R354W diminish protein expression, whereas p.N147K and p.R354W reduce the specific activity, but not the amount, of LMF-1. Interestingly, the interaction with LPL was unaffected by the p.N147K and p.R354W mutations suggesting a potential role for these residues in LPL folding or interaction with other proteins. Further studies are warranted to explore these possibilities.
This work was supported by NIH grant HL154071.
# 387
Effects Of N-acetylcysteine And Cyclic Peptide R4W4 Combination Treatment On Mycobacterium Avium Survival
Sasaninia KC1, Kelley M2, 3, Badaoui A1, Mohan A1, Tiwari R1, 4, Venketaraman V1. 1Western University of Health Sciences, Pomona, CA; 2Western University of Health Sciences, Pomona, CA; 3Kansas City University, Kansas City, MO and 4Chapman University, Harry ad Diane Rinker Health Science Campus, Irvine, CA
Purpose of Study:Mycobacterium avium (M. avium) is an opportunistic pathogen and a leading contributor to nontuberculous mycobacterial infections in immunocompromised individuals with HIV infection and type 2 diabetes (T2DM). M. avium is treated with a 12-month macrolide regimen. However, treatment duration and antibiotic toxicity present challenges in the management of M. avium infections. Furthermore, the emergence of antibiotic resistance prompts a need to develop novel treatment modalities. N-acetylcysteine (NAC) is a precursor to glutathione (GSH) and exhibits potent antimycobacterial effects. Antimicrobial peptides, such as novel cyclic R4W4, have also been shown to provide additive effects when administered along first-line antimycobacterial agents such as rifampin and azithromycin. We aim to elucidate the effects of NAC and R4W4 combination treatment on M. avium survival in culture and in an infected THP-cell derived macrophage cell line. The findings of this study may offer new insights into therapeutic strategies against mycobacterial antibiotic resistance.
Methods Used: To assess direct antimycobacterial effects of NAC and R4W4, M. avium (2x106 CFU/mL) was inoculated in 7H9 media and treated with varying concentrations of singular NAC, NAC with cyclic R4W4, or sham treatment. Treatment was applied to M. avium culture 1 hour, 3 days, and 6 days post-inoculation. Growth was terminated 3 hours, 4 days, and 8 days post inoculation. Harvested bacterial cultures were serially diluted, plated on 7H11 agar, and grown to enumerate colony forming units (CFU) to assess M. avium survival post-treatment.
To assess intracellular survival of M. avium post NAC and R4W4 treatment, THP-cell derived macrophages (6 × 105 cells/mL) were infected with M. avium with multiplicity of infection ratio of 1:10 (M. avium: macrophage) and treated with NAC or combination NAC and R4W4 treatment. Treatments were applied 1 hour, 3 days, and 6 days post-infection using either sham treatment or varying concentrations of singular or combination NAC and R4W4 treatment. Treated infected macrophages were incubated until termination 3 hours, 4 days, and 8 days post infection. M. avium CFUs from cell lysates of terminated macrophage infections were grown and enumerated to determine bacterial survival.
Summary of Results: Significant reductions in M. avium inoculum survival were observed 8 days post inoculation following 20 mM NAC + 8 μg/mL R4W4 treatment compared to single NAC treatment. Intracellular M. avium survival was significantly reduced 3 hours post-infection following 20 mM NAC + 2 mg/mL R4W4 treatment and 20 mM NAC + 8 μg/mL R4W4 treatment compared to single NAC treatment. NAC and R4W4 combination treatment significantly reduced intracellular M. avium survival in a dose-dependent response 4- and 8-days post-infection for all tested treatment concentrations compared to single NAC treatment and untreated controls.
Conclusions: Additive effects are observed with NAC and R4W4 combination treatment against M. avium infection in vitro.
# 388
FULLERENE GALLIUM PHOSPHONATE SHOWS ANTIMYCOBACTERIAL EFFECT AGAINST MYCOBACTERIUM AVIUM
Yoon S1, Sasaninia KC1, Kelley M3, Mohan A3, Bi X1, Baudry M2, Venketaraman V1, Butzloff P4. 1Western University of Health Sciences, Pomona, CA; 2Western University of Health Sciences, Pomona, CA; 3Western University of Health Sciences, Pomona, CA and 4Independent researcher, Irvine, CA
Purpose of Study: Mycobacterium-related infections have been a historically difficult problem and still pose great public health challenges due to the inherent antibiotic resistance. Thus, developing alternative treatment strategies is of paramount importance. In 2022, Dr. Peter Butzloff created a novel compound called Fullerene Gallium Phosphonate (FGP) that combines buckminsterfullerene – a spherically shaped 60 carbon molecule – with gallium phosphonate groups, which demonstrated antimicrobial effects against some viruses, fungi, and bacterial species. Although both fullerene and gallium had each demonstrated antimicrobial effects in the past, the synergistic effect between the two has never been explored, especially on Mycobacterium avium. This study has three aims: determine if FGP has antimycobacterial effect against M. avium, validate gallium as a core component of FGP by comparing with sham control Fullerene Disodium Phosphonate (FDSP), and assess FGP’s effect on M. avium-infected macrophage cell line. We hypothesized that FGP would show antimycobacterial effect and be superior to FDSP both in vitro and in vivo.
Methods Used: To test these hypotheses, M. avium was cultivated in a 96 well-plate (6 x 104 cells/well) with varying FGP and FDSP concentrations (1, 10, 100 ug/ml) given at three different timepoints (day 0, 3, 6) followed by terminations at timepoints: 3h, day 4 and 8.
Summary of Results: Our results showed dose dependent reductions of M. avium colony forming units (CFUs) with FGP in all three time points (3h, day 4, day 8). In comparison with FDSP (sham control), there was antimycobacterial effect in both FGP and FDSP, but only FGP showed clear dose-dependent reductions of CFUs in all three time points. Furthermore, FGP showed superior antimycobacterial effects to FDSP at all three time points with greater magnitude of CFU reductions in relation to the control (untreated). The in vivo experiment is currently ongoing.
Conclusions: Our study findings suggest the gallium in FGP, when combined with fullerene, shows superior antimycobacterial effects than fullerene alone. In addition, the clear dose-dependent reduction of CFUs suggests FGP’s potential as an alternative treatment for mycobacterium-related infections.
# 389
GSK3β/NF-κB dependent transcriptional regulation of homeostatic hepatocyte Tnf production
Grayck M, McCarthy WC, Solar M, Golden E, Zheng L, Bala N, Sherlock L, Wright CJ. CU Anschutz, Aurora, CO
Purpose of Study: Maintenance of hepatocyte homeostasis plays an important role in mediating the pathogenesis of many diseases. A growing body of literature has established a critical role played by TNFα in maintaining hepatocyte homeostasis; however, the transcriptional mechanisms underlying constitutive Tnf expression is unknown. Hepatocytes are known to express constitutive NF-κB, a transcription factor that directly targets Tnf, yet whether this is responsible for driving constitutive Tnf and hepatocyte homeostasis is unknown. One mechanism proposed to be responsible for constitutive NF-κB is GSK3β. We hypothesize that baseline NF-κB activity is regulated by GSK3β, and this is responsible for controlling constitutive Tnf expression and maintenance of hepatocyte homeostasis.
Methods Used: Whole liver fractions and isolated hepatocytes from adult control C57BL/6 mice (8-12 wk) and murine hepatocyte cell line, AML12, was assessed for constitutive Tnf expression through RT-PCR. We first assessed constitutive NF-κB and the effects of GSK3β inhibition (CHIR-99021 10μM; 24hr) on nuclear presence of subunits p65 and p50 through Western Blot. Following this, we interrogated efficacy of inhibition and constitutive Tnf expression following pharmacologic inhibition of GSK3β (CHIR-99021 1,3,10μM; 24hr, 7-28-42-day and LiCl 30mM; 24hr) and NF-κB (BAY 11-7085 20μΜ;30min). Chromatin immunoprecipitation (ChIP) was used to determine the role of GSK3β on transcription factor NF-κB in mediating constitutive Tnf expression in AML12 hepatocytes. Finally, the assessment of AML12 cell proliferation following GSK3β (CHIR-99021 1,3,10μM; 24hr and LiCl 30mM) and NF-κB (10μΜ;30min) inhibition was evaluated.
Summary of Results: Constitutive Tnf gene expression is present in whole liver, isolated hepatocytes and cultured AML12 hepatocytes (n=5-8, p<.05). GSK3β inhibition decreased nuclear levels of the NF-κB subunits p65 and p50 at baseline (n=8, p<.05). Pharmacologic inhibition of GSK3β resulted in a time- and dose-dependent inhibition of Tnf gene expression (n=6-9, p<.05). We determined that NF-κB transcription factor subunit p65 binds to consensus sequence elements present in the murine TNFα promoter and inhibition of GSK3β decreases binding and subsequent Tnf gene expression (n=8, p<.05). Finally, AML12 cell growth was significantly reduced following GSK3β and NF-κB inhibition.
Conclusions: We present constitutive Tnf expression in the murine whole liver, isolated and culture hepatocytes, AML12. We show that baseline NF-κB is driven by GSK3β, constitutive Tnf expression is directly impacted by NF-κB and GSK3β activity, and this results in a reduction of AML12 proliferation. Further studies are required to determine the relationship of these factors at homeostatic conditions and within chronic liver disease progression.
Behavior, Development and Psychology I
Concurrent Session
10:15 AM
Friday, January 19, 2024
# 390
HEALTHCARE INEQUITIES IN TREATMENT OF AUTISM SPECTRUM DISORDER: A LITERATURE REVIEW
Zhu J1, Chen J1, Law F1, Li K1, Nguyen C1, Sam D1, Vellanki S1, Afghani B1, 2. 1UC Irvine School of Medicine, Irvine, CA and 2CHOC Hospital of Orange County, Orange, CA
Purpose of Study: Although access to treatment for autism spectrum disorder (ASD) at an early age has been shown to improve outcome, various barriers can delay diagnosis and treatment in marginalized communities. Our review aims to identify disparities in treatment of ASD based on the distinction of race/ethnicity.
Methods Used: We performed a comprehensive literature review using several databases including PubMed and Google Scholar and cross checking of references. We used keywords: "autism", "autism spectrum disorder", "ethnicity", "race", "disparities", and "inequities". We only included articles that were published after 2015 and compared access to treatment for ASD among different races/ethnicities.
Summary of Results: Five studies satisfied our inclusion criteria. The studies included children with ASD up to 17 years old. After adjusting for factors, such as parental education, income, and insurance coverage, there were still significant differences in treatment access and satisfaction when comparing White and non-White families. Studies that focused on provider and parent interactions found that minority parents, especially Black families, were less satisfied and were less likely to feel like their needs were met by providers. In terms of utilization and access to services, Black and Asian families were less likely to use outpatient services through Medicaid but were more likely to access school services. Additionally, despite efforts to make insurance more accessible, non-White families had less access to family centered ASD treatment compared to White families. Our study was limited because of non-uniformity in considering different variables that could impact ASD care. For example, severity of autism, other comorbid conditions and parental beliefs were not controlled for in some of the studies.
Conclusions: Our literature review suggests that although there is variation by type of service, disparities in autism-related services continue to exist when comparing White and non-White children in the United States. Compared to Whites, non-Whites were less likely to use outpatient services but more likely to use school-based services. Further studies than consider all variables that could impact care are needed. In addition, studies with different interventional modalities that target groups based on socio-economic factors and ethnicity are warranted.
Summary of pediatric studies published after 2015 that examined access to ASD treatment across various races.
First author, year published
Age group studied
Study method
Number in each ethnic group
Outcome comparison, or Odds ratio (OR) and p-value
Other predictors of access taken into account
Zeleke, 2019
6 to 17 years
Survey of Pathways to Diagnosis and Services
Racial minority (Hispanics, African-Americans and others)=347 White=1368
White vs. minorityA) Parents satisfaction more in Whites: F=4.486, p=0.004B) Provider met the needs more in Whites: F=8.35, p=0.004
Parental education, poverty level, proxy indicator for the availability of services, insurance coverage
Bilaver, 2021
3 to 17 years
Medicaid Analytic Extract data 2012
Total N=117,848
Black = 20,907
Latinx = 16,966
Asian = 2154
Native American/ Pacific Islander = 1871
White = 75950
A) Outpatient services: Black less than Whites by 5.2%, p<0.001
Asians less than Whites by=3.2% p<0.01
Latinx more than Whites by 0.9% p
B) School based services Blacks more than Whites by 7%, p<0.001
Asian more than White by 8.6%, p<0.001
Comorbidities and age
Magana, 2015
Birth to 17 years
Cross-sectional telephone survey in 2005-2006 and 2009-2010
White children with ASD N=3772, Black children with ASD N=685, Latino children with ASD N=662
Black vs. WhiteA) Provider listened, OR=0.67, p<0.05
B) Provider provided information: OR=0.85, p>0.10C) Provider partnership: OR=0.62, p
D) Provider spent time: OR=0.57, p
E) Provider sensitivity: OR=0.64, p<0.01
Family income, parent eduction, family structure, insurance, condition severity
Doshi, 2017
Birth to 17 years
Cross-sectional telephone survey in 2005-2006 and 2009-2010
N= 2123 in 2005 without mandate and N= 3055 in 2009 with mandate*
Whites vs Non-WhitesA) 2005/06 wave, Access to family centered care: 879 (53.4%) vs 119 (38.5%), p<0.001
B) 2009/10 wave, Access to family centered care: 1261 (53.6%) vs 276 (41.9%), p<0.001
Family income and child health
Yingling, 2018
2 to 17 years
Cross sectional data from 2011-2012 national survey of children with special health care needs
Nt=1624
Non-Hispanic White = 827
Non-Hispanic Black = 149
Hispanic = 202
Multiracial/ other = 129
Non-Hispanic Blacks vs White entry to treatment at a later age:Age 3 yrs OR=1.18, p<0.05
Adjusted for age, gender, English as household language, education, poverty, and autism severity
Data taken in states before mandate that required private insurance companies to cover autism related services.
# 391
Changes in Cognition and Mood Following Sleep Extension in Adolescents with Habitually Insufficient Sleep
Schrage M3, Bernard A1, 2, Cooper E2, 1, Holtman S1, 2, Cree-Green M4, 2, Wright K5, Nadeau KJ6, 2, Simon S1, 2. 1Children’s Hospital Colorado, Aurora, CO; 2University of Colorado Medical Campus, Aurora, CO; 3Rocky Vista University, Parker, CO; 4Children’s Hospital Colorado, Aurora, CO; 5University of Colorado Boulder, Boulder, CO and 6Children’s Hospital Colorado, Aurora, CO
Purpose of Study: Insufficient sleep is common in adolescents which places them at risk for mood and cognitive impairments. Previous studies found that cognition and positive affect decline with sleep restriction (5-7 hours/night) and improve with sleep extension (8-10 hours/night) in healthy adolescents. Mixed findings have been reported for negative affect. This study aims to assess the impact of a one week at-home sleep extension manipulation on cognition and mood in adolescents with habitually insufficient sleep (≤7 hr/night).
Methods Used: This randomized crossover study assessed 17 short-sleeping adolescents ages 14-19 following one week of Typical Sleep (TS) and one week of Sleep Extension (EXT; +1 hour in bed) at home during the school year in counterbalanced order. Actigraphy assessed adherence to the sleep schedules. An overnight in-laboratory visit followed each sleep condition where participants completed cognitive and mood tasks every hour starting at 5:00 pm until bedtime. Tasks included: 1) Digit Symbol Substitution Test (DSST) with higher scores indicating better cognition; 2) Karolinska Sleepiness Scale (KSS) with higher scores indicating greater sleepiness; and 3) Positive Affect Negative Affect Scale (PANAS) with higher scores indicating greater positive/negative affect. Generalized linear mixed models, using Gaussian or Gamma distributions as appropriate, were used to evaluate the impact of EXT on task scores. The models included a random intercept by participant and covariates for week and number of completed tasks. Time-by-EXT and week-by-EXT interaction terms were evaluated for each model.
Summary of Results: During EXT, DSST scores were higher by an average of 4.4 points (p=0.04) compared to TS. DSST scores increased on average by 2.3 points/hour (p<0.001) and were higher in week 2 by 8.9 points (p<0.001). KSS, Positive Affect, and Negative Affect were not significantly different between TS and EXT. KSS scores increased by 0.7 points/hour (p<0.001) and lowered in week 2 by 0.7 points (p<0.001) compared to week 1. Positive and Negative Affect scores decreased by factors of 0.92 and 0.97 per hour, respectively (both p<0.001). Positive Affect scores lowered by a factor of 0.93 in week 2 compared to week 1 (p=0.048).
Conclusions: In this sample, cognition improved with EXT, while sleepiness and affect were not different between EXT and TS. This is consistent with previous studies that found improved cognition and no change in negative affect, but contrary to previous findings of improved positive affect with EXT. DSST scores increased with repeated testing during both conditions and on week 2, likely due to associative learning. KSS scores increased as the participants got closer to their bedtime and positive/negative affect decreased over each hour. Future research is needed to isolate the effects of EXT on cognition from associative learning and to parse out the relationship between sleep duration and mood. Increasing sleep duration in short-sleeping adolescents may improve cognition.
# 392
PROMOTING ACCESSIBILITY TO HEALTHCARE WITH PROCEDURES
Bregman TE1, 2, Ma VK1, 2, Owens KH2, Roseborough E2, Tuss V2, Akins RS1, 2. 1UC Davis, Sacramento, CA and 2UC Davis, Sacramento, CA
Purpose of Study: The PATH Program (Promoting Accessibility To Healthcare) at UC Davis is a health system wide initiative aimed at improving healthcare experiences for neurodivergent individuals and their families. Previous studies have shown that neurodivergent individuals have higher rates of health care utilization and costs, while also being significantly more likely to have unmet healthcare needs. Neurodivergent individuals have unique stressors in medical settings that often contribute to care refusals and challenging behaviors. Many healthcare providers report receiving minimal training in how to support neurodivergent individuals during medical visits.
There is a growing body of research endorsing healthcare provider training, sensory accommodations, and environmental adaptations to facilitate medical care of neurodivergent individuals, but there is limited research related to procedures such as venipuncture.
Methods Used: PATH Glassrock is a specialized phlebotomy clinic where neurodivergent patients will be scheduled for 30-minute appointments. A pre-appointment telephone intake with caregivers will be completed to create an individualized care plan. Patients will receive procedural support by a Certified Child Life Specialist during the appointment. The treatment room was also recently renovated to better meet the sensory needs of neurodivergent patients.
Phlebotomists working at PATH Glassrock will complete two, 2-hour in-person training sessions followed by asynchronous viewing of training videos. Training topics include Introduction to Neurodevelopmental Disabilities (NDDs) and The PATH Program, Environmental and Sensory Adaptations and Developmentally Appropriate Patient Communication and Comfort Positioning. Phlebotomists completed a pre-training survey and they will complete a post-training survey.
Summary of Results: 24 UCD Phlebotomists were surveyed. Pre-training survey results showed 96% of respondents cared for patients with NDDs. Only 2 of 24 respondents had received 5 or more hours of training related to NDD; 75% stated that they were interested in receiving additional training about caring for patients with NDDs. Respondents had rarely used social stories, visual supports or sensory accommodations (<11%), but 42% had used personalized patient information to prepare for visits. Phlebotomists listed lack of familiarity with neurodivergent children, environmental challenges, and time pressures in the work setting as the most significant barriers to caring for patients with NDDs. The support strategies phlebotomists rated as most helpful for additional training were strategies for sensitivities, patient safety skills and pediatric friendly patient communication.
Conclusions: Preliminary data from the pre-training survey of phlebotomists demonstrated knowledge gaps related to NDDs and interest in additional training on patient safety skills, strategies for sensitivities, environmental adaptations, and communication strategies.
# 393
EXtraordinarY Babies Study: Profile of early executive functioning skills in toddlers with sex chromosome trisomy
Janusz J1, 2, Lal G1, Thompson TG1, 2, Wilson R1, 2, Davis S1, 2, Ross J3, Tartaglia N1, 2. 1Children’s Hospital Colorado, Aurora, CO; 2University of Colorado School of Medicine, Aurora, CO and 3Nemours Hospital for Children, Wilmington, DE
Purpose of Study: Children and adults with sex chromosome trisomy (XXY, XXX, XYY) are at increased risk for deficits in executive functioning skills. Previous research with school-age children has shown weaknesses in multiple domains of executive functioning including working memory, cognitive flexibility, planning, and problem solving. However, little is known about emerging executive functioning skills in young children with sex chromosome trisomies (SCT). This study investigated early executive functioning skills at 24, 36, and 48 months of age to explore whether deficits seen in older children can be identified in the toddler years.
Methods Used: The study cohort consisted of children with XXX, XXY, and XYY enrolled in the eXtraordinarY Babies Study, a prospective study evaluating the health and development of children with prenatal diagnosis of SCT. Parents completed the Behavior Rating Inventory of Executive Function- Preschool (BRIEF-P) at the 24-month (n=142), 36-month (n=88), and 48-month (n=98) visits. The BRIEF-P provides scores for five subscales (Inhibition; Shift; Emotional Control; Working Memory; Plan/Organize) and three overarching indices: Inhibitory Self-Control Index (ISCI, consisting of the Inhibition and Emotional Control scales), Flexibility Index (FI, consisting of the Shift and Emotional Control scales), and Emergent Metacognition Index (EMI, consisting of the Working Memory and Plan/Organize scales). Mean T scores were calculated for each subscale and index. The percentage of scores falling in the clinically significant range (T score > 60) was also calculated.
Summary of Results: Mean scores for all subscales and indices were in the average range at all three timepoints (mean range 43.58-51.04). Percentage of scores falling in the clinically significant range were relatively low for the ISCI and FI at both the 24- and 36-month timepoints, ranging from 5% to 8% of the sample. In contrast, at the 48-month visit, 21 and 28% had scores in the clinically significant range on the ISCI and FI, respectively. For the Emergent Metacognition Index (EMI), a greater portion of the sample had scores in the clinically significant range at all three timepoints compared to the ISCI and the FI (19% at 24 months; 19% at 36 months; 28% at 48 months).
Conclusions: Findings suggest that for the majority of children with SCT, early deficits in executive functioning skills are not yet seen. However, for a portion of these children, deficits in working memory and planning/organization can be seen as early as 24 months. By 48 months, a larger percentage of the children are showing deficits across multiple domains of executive functioning skills. This provides information that can be used for early intervention in these areas. Future research will explore developmental patterns into school age.
# 394
The eXtraordinarY Babies Study: Parenting Stress in Families with a Prenatal Diagnosis of Sex Chromosome Trisomies, 36-month-old Follow-up
Wilson R, Davis S, Thompson TG, Peterson C, Howell S, Tartaglia N. University of Colorado School of Medicine, Aurora, CO
Purpose of Study: Prenatal identification of sex chromosome trisomies (XXY/Klinefelter syndrome, XYY, XXX) or SCTs has increased significantly with noninvasive prenatal screening. Such diagnoses often entail substantial parental stress with implications for parental well-being. Previous studies have reported negative impacts following a prenatal genetic diagnosis, the eXtraordinarY Babies study, a prospective evaluation of children with SCTs, surprisingly found lower parenting stress within the first year of life. This study aims to further assess parenting stress and associated factors in this cohort at the 36-month follow-up.
Methods Used: This is a cross-sectional analysis from the eXtraordinarY Babies Study 36 month visit (n=134; 92 XXY, 29 XXX; 13 XYY). Parents completed the Parenting Stress Index 4th edition (PSI-4), Social Responsiveness Scale (SRS-2), and a socioeconomic questionnaire to calculate Hollingshead index (HI). Children received developmental testing with the Bayley Scales of Infant and Toddler Development- 3rd edition (Bayley-3). T-scores for PSI-4 subdomains were compared to the normative sample using one-sample T-tests and among karyotypes using ANOVA. Pearson correlations were conducted between PSI-4 Child and Parent Domain scores and Bayley subdomains, SRS Total Score, and HI. Alpha was set at 0.05.
Summary of Results: The cohort includes 134 children with SCT with mean age of 37.4 ±1.7 months, ethnicity 86% non-Hispanic, and parents with upper-middle-class SES (HI 53.7±9.6). No significant differences in PSI-4 domain scores were observed among SCT karyotypes (XXY vs XYY vs XXX). Comparing T-scores to a normative sample (mean of 50 with SD 10), this cohort exhibited lower parent, child, and total stress levels (p<0.001 for all). Defensive responding, or a “look good bias” was identified in 25.1% of the group. Child-related stress negatively correlated with Bayley-3 receptive language (r=-0.39, p=0.002), gross motor (r=-0.36, p=0.006) and their corresponding composite scores. Additionally, a strong positive correlation was observed between child-related stress and the total T-score on the SRS-2 (r=0.69, p<0.001).
Conclusions: Parents of 3-year-old children with a prenatal diagnosis of a SCT participating in the eXtraordinarY Babies Study report lower stress levels on parent-reported measures, accompanied by a higher rate of defensive responding. These results are consistent with study findings at 2, 6 and 12 months, and provide important information about the parenting experience of young children with SCT identified prenatally. Compared to the first year of life, at 3 years of age there were stronger associations with impaired child development, particularly social communication, which prompts further exploration of interactive factors influencing parental stress and child development. Future research directions include examining individual changes over time and analyzing the interplay between child temperament, adaptive functioning, and social communication skills.
# 395
A multivariable analysis of psychosocial risk factors in pediatric renal transplant patients
Ashley S1, Chandnani A2, Arcona Z1, Christofferson E1, Monin K4, Sevick C1, Vemulakonda VM1, Bock M1, Walker J3, Buchanan C1. 1University of Colorado School of Medicine, Denver, CO; 2Barnes Jewish Hospital, St. Louis, MO; 3University of Tennessee Chattanooga College of Medicine, Chattanooga, TN and 4Nationwide Children’s Hospital, Columbus, OH
Purpose of Study: The Pediatric Transplant Rating Instrument (P-TRI) is a validated 17-item rating scale administered during pediatric pre-transplant evaluations to identify developmental, familial, and logistical barriers that may impact transplant success. This study evaluates the relationship between medical diagnostic factors and patient psychosocial risk factors as measured by the P-TRI.
Methods Used: Retrospective chart review of 177 pediatric kidney transplant candidates evaluated at Children’s Hospital Colorado between 2013 and 2021 was performed. Candidates were grouped into one of three diagnostic categories: CAKUT, primary renal, or syndromic neurogenic bladder. Differences in adherence and total risk were analyzed using cumulative logistic regression, with higher P-TRI totals and adherence subscale scores indicating less risk. The P-TRI and adherence scales were assessed for association with diagnostic category, catheterization and dialysis status. At risk status for transplant knowledge and psychiatric history were assessed for association with diagnostic category using binary logistic regression. The model for at risk status for transplant knowledge was further corrected for language, ethnicity, and insurance type. Analyses were conducted using SAS v.9.4 (Cary, NC).
Summary of Results: Patients who catheterize had lower adherence scores than patients who did not catheterized (OR 0.46, p=0.0206). Patients on dialysis trended towards higher adherence scores compared to those not on dialysis (OR 1.69, p=0.067). Each additional year of life was strongly associated with lower adherence scores (p=0.0011). Primary renal patients were more at risk for psychiatric concerns compared to CAKUT patients (OR 1.96; CI=1.06-3.66; p=0.046). Multivariable analysis was performed to compare language, ethnicity, and insurance type as risk factors in the “Knowledge About Transplant” category. There was moderate evidence indicating that Hispanic non-English speaking patients were more likely to score as “at risk” compared to non-Hispanic English-speaking patients (OR 3.4; p=0.03). There was moderate evidence that patients with public insurance were more likely to be at risk in this category compared to patients with private insurance (OR 3.8; p=0.011).
Conclusions: This study found that patients who catheterize, are not on dialysis, or are older in age are at increased risk of non-adherence and may benefit from additional support. Primary renal versus CAKUT diagnoses had more psychiatric risk factors which suggests a need for early psychiatric support in the renal setting. Finally, Hispanic non-English speaking patients and patients with public insurance may be more at risk of not having necessary knowledge about the transplant and additional educational supports may be beneficial.
# 396
Social Factors Predicting Pre-Linguistic Skills in Infants born Preterm
Pesantez S, Lazarus M, Marchman VA, Feldman HM. Stanford University, Stanford, CA
Purpose of Study: Infants born preterm (PT) are at risk for long-term delays in language development. These delays have been attributed to brain injuries and subsequent brain dysmaturity. Social factors contribute to individual differences in later language development in children born term and PT. It is unclear whether the child’s home environment contributes to individual differences in the earliest stages of communicative development among children born preterm. This study aims to determine whether developmentally stimulating features of the home environment and/or the amount of child-directed speech predict PT children’s gestures production at 9 months of age.
Methods Used: Participants (n=20, 10 M, 10 F) were recruited from the Lucile Packard Children’s Hospital NICU, and are all <32 weeks gestational age at birth. Predictor variables were (1) parent-reported results on the Cognitive Home Environment Questionnaire (STIMQ), (2) adult word count from a 16-hour recording with the Language Environment Analysis (LENA), which is a direct measure of the linguistic stimulation in the home. The primary outcome measure was the total number of late gestures from the MacArthur Bates Communicative Developmental Inventory (CDI) at 9 months of age. The strength of association between the two predictors and between the predictors and outcomes was determined with Pearson or Spearman correlations.
Summary of Results: PT children had a mean gestational age of 28.86 weeks. The total STIMQ score was weakly correlated with late gestures on the CDI at 9 months (R = 0.215, p-value = 0.362). The Adult word count was not correlated with later gestures on the CDI (R = -0.043, p-value = 0.866). Interestingly, parent’s scores on the STIMQ correlated significantly with Adult Word Count (AWC) on the LENA at 9 months of age (R = 0.577, p-value = 0.012).
Conclusions: Parent reports of the home environment and the objective measures of child-directed speech were significantly correlated, suggesting that these different measures may be assessing overlapping features of the social environment. However, neither measure was significantly correlated with gesture communication during infancy. The timing of gestures may be less tied to environmental stimulation than are other measures of language. We will increase the sample and continue to follow these children as they begin verbal communication.
Diversity, Equity, Inclusion Research II
Concurrent Session
10:15 AM
Friday, January 19, 2024
# 397
Neurodevelopmental outcomes in NICU graduates born to mothers with Non-English Language of Preference
Martes Gomez MP2, Vu M3, Nghiem N3, Mirzaian C1. 1CHLA, Los Angeles, CA; 2Los Angeles General Medical Center/Keck School of Medicine of USC/CHLA, Los Angeles, CA and 3CHLA, Los Angeles, CA
Purpose of Study: Research shows disparities in infant outcomes for families with a non-English language of preference (NELP). There is evidence that infants born to NELP mothers have worse neonatal outcomes than their peers. However, there are no studies at this point assessing neurodevelopmental outcomes in this group. There is evidence that other high-risk populations such as Autism Spectrum Disorder (ASD) patients, are negatively impacted and have more difficulty accessing resources, and received less therapies compared to their English speaking parents counterparts.
Methods Used: We reviewed a cohort 185 infants seen at Children’s Hospital Los Angeles (CHLA) high-risk infant follow-up (HRIF) clinic, which includes infants with gestational age <32 weeks, birth weight < 1500 grams or other HRIF-eligible medical conditions. Initial visit (at any age) occurred between July 2017 and June 2019 at 6-, 12- and 24-months corrected age. We utilized the Bayley’s standard scores (including cognitive, language, and motor components) at 6 (V1/Baseline), 12 (V2), 24 (V3) months to assess development progression. Outcomes were changes in scores from baseline. Analyses utilized linear mixed-effects models, adjusted for baseline score, gender, weight, and gestational age.
Summary of Results: Out of 185 infants, 134 were included for analysis. Out of 134, 98 were English Language of Preference (ELP) and 36 (32 Spanish) were Non-English Language of Preference (NELP). Majority were Hispanic in both groups, and no difference in gender. Majority were CCS insurance combined with public insurance status. About 45% of each cohort were connected to the regional center. Mean (SD) developmental scores for cognitive, language, and motor components were 94.5, 87.0, and 86.3.
While infants with NELP cognitive scores dropped by 4.4 at V2, and 8.9 at V3, compared to baseline, infants with ELP experienced a smaller decrease of 1.1 and 8.1, respectively. Language scores also decreased in larger magnitudes for NELP infants compared to the ELP infants (-6.9 vs. -2.8 at V2, and -13.5 vs. -5.6 at V3). Similarly, at V2, motor scores dropped by 6.1 for infants with NELP and 1.4 for ELP infants. Surprisingly, at V3, ELP infants experienced a larger decrease of 7 in their motor scores, compared to -1.8 in the NELP infants.
Conclusions: Although there was a downward trend in developmental progression for both groups, infants with NELP mothers experienced much larger decrease and are worse off in terms of their developmental progression, compared to the infants with ELP mothers, with the exception of motor development at 24 months. Few studies have examined disparities by maternal primary language, and these represent a key pathway by which to address racial and ethnic disparities in neurodevelopmental outcomes in former NICU patients. Addressing health inequity is an important goal for neonatal care, which does not end at discharge from the NICU. We hope our study helps understand this particular population better.
# 398
CHRONIC PAIN AND INTEGRATIVE MANAGEMENT EXPERIENCES AMONG ASIAN INDIVIDUALS: A QUALITATIVE STUDY
Tu K1, Johnson A2, Tong S2. 1University of Washington, Seattle, WA and 2University of Washington, Seattle, WA
Purpose of Study: An estimated 1 in 5 Americans experience chronic pain, making it more prevalent than chronic diagnoses like diabetes and hypertension. Among Asian populations, there is known potential for undertreatment of pain, contributing to inequitable burden. However, there is significant lack of engagement of the Asian/American diaspora in trying to understanding chronic pain experiences and management. These patients often seek options besides pain medication and surgery, largely outside engagement with a primary care provider. This study intentionally engages Asian individuals to (1) explore shared and geographic/identity-specific chronic pain experiences and (2) identify factors that influence an individual’s ability to engage in goal-concordant integrative pain management.
Methods Used: Asian individuals who currently experience chronic pain were recruited from primary care and community-based settings across Montana and Washington. Participants needed to be English, Mandarin or Cantonese-speaking unless they had family willing to serve as an interpreter. Semi-structured interviews were offered remotely or in-person. Questions focused on participants’ chronic pain experiences and management, with an emphasis on integrative approaches. Interviews were recorded, transcribed and then double-coded.
Summary of Results: 16 participants (MT=6, WA=10) completed the interview. The majority were female (n=12) and privately insured (n=12). The cohort included self-identified Iranian, Chinese, Taiwanese, Thai, Vietnamese, Indonesian, Japanese, and multiracial, with the most identifying as Vietnamese (n=5). Participants varied in age (25-76; IQR=34-51) and years of chronic pain experienced (.5-53; IQR=5-24).
Using thematic analysis, we identified key themes: (1) frequent patient initiative amidst lack of prioritization of chronic pain in primary care settings, (2) double invisibility due to nature of chronic pain and intersecting identities, particularly Asian, female, and proximal immigration narrative, (3) need for stability in chronic pain management facilitated by insurance coverage, regional accessibility, cultural exposure and access, varied perceptions of integrative approach among providers and communities, and consistency with primary care providers.
Conclusions: These exploratory findings serve to build primary care provider awareness of intersecting identities and potential barriers and facilitators to effective integrative pain management. By allowing participants to self-identify as Asian, this data provides specific context behind inconsistent numbers that suggest chronic pain is not a problem among certain groups when it is likely comparably prevalent and pressing. The study encourages critical engagement with patients who experience chronic pain, regardless of identity, in a way that seeks to improve life with chronic pain and minimize repetitive harm.
# 399
Is Bystander Intervention Training Effective in Mitigating Sexual Misconduct?
Kim E3, Jara Hidalgo K2, Dong F4, Silberger J1, Prasad C2. 1Kaiser Permanente, Portland, OR; 2Western University of Health Sciences, Pomona, CA; 3Western University of Health Sciences, Lebanon, OR and 4Western University of Health Sciences, Pomona, CA
Purpose of Study: Research on sexual harassment and assault in the medical community has been documented but lacks pro-active solutions to lessen these incidences. Our purpose was to determine if medical professionals have received Bystander Intervention Training (BIT) and to evaluate it as a method to implement in healthcare institutions.
Methods Used: In 2023, American College of Physicians (ACP) conducted a webinar series on sexual harassment in the medical profession. Registrants voluntarily completed a post-session online cross-sectional survey, which included prior BIT, level of confidence in intervening as a bystander, training effectiveness, methods, timing, and topics of effective training. Local and national resources were provided in the event of triggering effects. Consent was determined through survey completion and submission. De-identified data was analyzed using chi-square tests to assess the difference in the responses between categorical variables. Fisher’s exact tests were conducted as the expected cell count <5.
Summary of Results: 65 participants responded. 41.4% had received formal BIT. Within those who had received formal training, of which 87.5% agreed/strongly agreed that they were confident to intervene in the event of witnessing a sexual assault, as compared to 56.3% of those who did not receive formal training (p=0.0286). There was a statistically significant difference in the perception of BIT in the Caucasian versus non-Caucasian groups, as evident in the following questions: BIT addressed common barriers to intervention (100% versus 60%, P=0.0237), BIT was effective in making them feel confident to intervene (84.6% versus 30%, P=0.0253), they could safely intervene (91.2% versus 63.6%, P=0.0127). Furthermore, participants in the age 40+ group had a statistically significant higher percentage than those <40 years old, (1) in confidence to intervene (78.4% vs. 52.6%, P=0.0439), and (2) the ability of BIT to adequately address incidents involving faculty or persons of authority (84.6% versus 40%, P=0.0303). With reference to strategies and timing of effective BIT, the most preferred methods included small group sessions using vignettes and information on how to intervene safely. Participants considered BIT training at high school and undergraduate education to be most effective.
Conclusions: Our results indicate that BIT can be an effective tool in increasing confidence and ability to intervene safely in incidents of sexual misconduct. Effective BIT can include various modalities with clinical vignettes being the most effective. The responses highlight the need for development of informed policies and proactive education programs in healthcare institutions. Future research could include the differences in training among specific populations or the cultural factors that influence bystander behaviors and attitudes. Limitations of our study include the small sample size and the fact that healthcare trainees were not included.
# 400
Impact of cannabis legalization on maternal health disparities
Tamatam S1, 2, Becerra L2, Gould E2, Roble A2, Nguyen R2, Okemkpa C2, Laughter J3, Ceasar R2. 1Western University of Health Sciences, Pomona, CA; 2University of Southern California, Los Angeles, CA and 3California State University Fullerton, Fullerton, CA
Purpose of Study: Despite groups like the American College of Obstetricians and Gynecologists discouraging the use of cannabis while pregnant, cannabis is the most frequently used substance during pregnancy in the United States. Expanding legalization and increased cannabis use among women contributes to the perception that it may not be a significant risk to them or to their fetus. This lessened perception of risk and widespread use of cannabis coupled with limited safety guidance from healthcare professionals may lead to increased maternal health disparities for pregnant people who use cannabis. Therefore, this study seeks to investigate the experiences and challenges faced by people who disclosed their cannabis use during pregnancy to their healthcare providers.
We hypothesize that people who use cannabis during pregnancy may experience added burdens and disparities during pregnancy and postpartum due to variations in their healthcare providers’ approach.
Methods Used: Semi-structured, qualitative interviews were conducted with 19 participants who self-identified as BIPOC (Black, Indigenous, People of Color), were over 21 years of age, spoke English or Spanish, resided in California, and were currently pregnant or had given birth in the last 2 years. Each interview was approximately one hour and covered topics such as reasons for cannabis use, quality of care, and adverse consequences. Then, transcribed data was uploaded to Atlas.ti and analyzed by developing a codebook with categories for emerging themes.
Summary of Results: Three recurring key themes emerged from our analysis. Participants shared that they experienced 1) poor treatment from their healthcare providers such as being treated like “addicts” or “users,” 2) stress attributed to increased surveillance such as Child Protective Service (CPS) visits and undisclosed drug screens, and 3) withdrawal of care from their providers– which in one case resulted in a participant giving birth in an Emergency Room instead of with an OB-GYN capable of handling her high-risk pregnancy.
Conclusions: These preliminary findings underscore the challenges and negative encounters that pregnant BIPOC people experienced after disclosing their cannabis use to their healthcare providers. Further research should explore ways in which to address these maternal health disparities and how physicians can deliver equitable care for pregnant people who may use cannabis for various reasons.
# 401
EDUCATION LEVEL AND HEALTHCARE EXPERIENCES AMONG BLACK PATIENTS IN THE EMERGENCY DEPARTMENT: A CROSS SECTIONAL STUDY
Messele F2, Meller L1, Makar C2, Aijaz A2, Gebreyes M2, Okeke C2, Taylor-Lucas C3, Saadat S4. 1UC San Diego School of Medicine, La Jolla, CA; 2UC Irvine School of Medicine, Irvine, CA; 3UC Irvine Health, Irvine, CA and 4UC Irvine Health, Irvine, CA
Purpose of Study: Education is an important social determinant of health. Among all races/ethnicities, higher education is associated with improved quality of life and reduced morbidity. Little has been done to characterize the association between education level and healthcare experiences among Black patients. The aim of this study is to characterize the association between highest education level achieved, and Black patients’ perceptions about healthcare received as assessed the following: mistrust of Primary Care Provider (PCP), negative experience in the Emergency Department (ED), and experience of treatment with respect/dignity in the ED.
Methods Used: This is a cross sectional survey distributed to ED patients receiving care in a Southern California urban tertiary academic medical center from September 2021 to September 2023. Patient demographics (I.e., age, language, education, insurance, and PCP status) and patient perspectives of medical mistrust, negative experiences in the ED, and perception of being treated with respect/dignity were explored. Chi Square statistical test was used to analyze associations between highest education level and three measured parameters (medical mistrust, negative experience, and treatment with respect/dignity) with significance denoted as p<0.05.
Summary of Results: Among 73 Black patients, 42% (n=31) are female, 61% (n=45) prefer English language in household, 32% (n=23) less than high school (HS), 11% (n=8) un-insured, 61% (n=45) with PCP. Descriptive analysis revealed that all Black patients with an education level less than HS trusted their PCP and 1 out of 18 patients with education level greater than a bachelor’s degree (5.6%) did not trust their PCP (p =0.45). Out of 23 Black patients, 2 (8.7%) with education level less than HS reported a negative experience in ED. A higher proportion, 8 out 27 Black patients (29.6 %), with education level greater than a bachelor’s degree reported having a negative experience in ED (p=0.07). Out of 22 Black patients, 2 (9.1%) with education level less than HS reported not feeling respected while 2 out of 26 Black patients (7.7%) with more than bachelor’s degree reported not feeling respected (p=0.86).
Conclusions: Our study identified that Black patients have unique experiences with medical mistrust of PCPs, negative experiences in the ED, and perception of receiving care with dignity/respect. Although we did not identify statistically significant associations between education and perceptions about healthcare received, we identified a unique trend worth further exploration as higher education status appears to possibly not be protective of having a negative experience in the ED for Black patients. Further study is needed, with a larger sample size, to explore whether this is consistent with study populations in other geographic regions and time points.
# 402
FINDINGS FROM A PILOT STUDY ON COMBATTING SEXUAL HARASSMENT/GENDER DISCRIMINATION IN THE MEDICAL PROFESSION
Fuson OI1, Beatty B2, Dong F2, Silberger J3, Chiriboga K2, LaPlante M2, Prasad C2. 1Oregon Health & Science University, Portland, OR; 2Western University of Health Sciences, Pomona, CA and 3Kaiser Permanente, Portland, OR
Purpose of Study: Sexual harassment and gender discrimination (SH/GD) in the medical profession is a sensitive topic that requires systemic interventions. Research has shown that female medical students are 220% more likely to experience sexual harassment than non-science, engineering, or math students. Another study found that 58% of female academic faculty and staff experienced sexual harassment in the workplace. Prior research has focused on the epidemiology of SH/GD in the medical profession. Little work has been done to study quality improvement initiatives in this area. The Oregon Chapter of the American College of Physicians (ACP) conducted a lecture series on this topic. The goal of this study was to assess participant attitudes on SH/GD in the medical profession and perceptions of the educational materials presented after attending the lecture series.
Methods Used: National experts on the topic of SH/GD were recruited to participate in the lecture series. Participants in this speaker series, members of ACP, were invited to complete a voluntary survey at the end of the session from April 2023 through July 2023. Participants who registered for this lecture series received a follow up email with information on how to complete the survey. Completion and submission of the survey indicated consent. The de-identified data was analyzed with descriptive statistics.
Summary of Results: A total of 38 participants completed the survey. The majority (88.9%) of respondents were female and 66.7% were attending physicians. 73.1% of respondents felt the topic of these sessions was relevant to their daily practice. 88.5% of respondents felt the topic of these sessions was relevant to current events in the medical profession. 80.7% of respondents felt more confident discussing issues surrounding SH/GD after attending this series. 80.8% of respondents reported that diversity and intersectionality were effectively addressed, 78.6% of respondents would recommend this session’s topic to a colleague. 84.0% of respondents stated they were likely to attend another session with this format style. 80.8% of respondents stated they would attend future events on similar topics.
Conclusions: SH/GD is a relevant topic to both current events in the medical profession and the daily practice of both physicians and trainees. Educational events, including speaker series aimed at raising awareness about this important topic, have been demonstrated to increase participant confidence discussing issues surrounding SH/GD, as evident in our pilot study. The results of our study further demonstrate an interest in this topic among medical professionals and trainees. Further research should focus on best practices to develop and deliver high quality, accessible teaching resources on this topic.
# 403
Pioneering a Fresh Approach to Radiology Diversity and Inclusion
Park S, Aldoghmi M, Danza CN, Meraz J, Aguilar D, Ho E, Cortes G, Houshyar R. University of California, Irvine, Orange, CA
Purpose of Study: Diversity is a goal that is gaining increased recognition within medical and academic institutions. However, radiology is one of the least diverse non-surgical specialties in terms of gender and minority representation. While there has been progress in the diversity of medical school matriculants, the number of radiology applicants from these underrepresented groups has remained largely stagnant.
In response to this pressing concern, a student-driven grassroots taskforce called RODI (Radiology Outreach and Diversity Initiative) was established with the mission of promoting awareness and interest in radiology to underserved and underrepresented communities. Survey data was collected from RODI outreach events to assess effectiveness of our outreach efforts.
Methods Used: Since December 2022, RODI has hosted online presentation and question-and-answer sessions that introduce medicine, radiology, and research to over 170 high school and undergraduate students from underrepresented communities. Each session was advertised to career counsellors and educators at institutions at underserved areas.
Data was collected from consenting participants prior to and after each event. Online surveys were conducted through Qualtrics, and a Student’s t-test assuming unequal variances was used for statistical analysis. The pre-survey consisted of questions regarding demographics, career choices, obstacles in pursuing said careers, and basic understanding of radiology. The post-survey consisted of questions ascertaining changes in understanding and interest in radiology. A numerical value was assigned to each survey answer choice (5=very good; 4=good; 3=neutral; 2=low; 1=very low).
Summary of Results: Demographics of survey respondents were 73% female, 24% male, 3% other; 71% Hispanic, 44% other, 27% Asian, 22% White, 5% Black, 2% Pacific Islander, and <1% American Indian. There were statistically significant mean positive increases for all questions pertaining to interest and confidence for a career in radiology after participating in the RODI outreach event (Fig 1).
Conclusions: Our findings indicate that RODI’s outreach initiatives have the potential to foster interest in and understanding of both medicine and radiology, especially among demographic groups that are historically underrepresented in medicine. Notably, we observed smaller but still significant improvements in questions regarding whether students would consider careers in medicine and/or radiology. This may suggest that implementing longer term interventions, such as extended lectures or shadowing opportunities could further encourage students from these communities to pursue radiology by enhancing their exposure to the field and strengthening mentorship relationships. Additionally, it is essential to acknowledge limitations in RODI’s grassroots events, such as the necessity for additional funding to expand outreach efforts and to maintain ongoing follow-up with attendees to monitor impact on students’ career outcomes.
Summary of mean values (pre- and post-event) and p-values for each survey question.
Question
Mean (Pre)
(n=98)
Mean (Post)
(n=83)
P-Value
After today’s talk, how would you rate your overall understanding of applying to medical school?
3.191
3.747
p<0.001
After today’s talk, would you consider a career in medicine?
1.851
1.952
p=0.023
After today’s talk, would you consider a career in radiology?
1.745
1.867
p=0.038
After today’s talk, how would you rate your overall understanding of radiology?
2.681
4.084
p<0.001
After today’s talk, how would you rate your understanding of the educational pathway to become a radiologist?
2.670
4.145
p<0.001
After today’s talk, how would you rate your understanding of what radiologists do at work?
2.638
4.108
p<0.001
# 404
SOCIAL DETERMINANTS OF HEALTH SCREENING TOOL RESPONSES IN THE NEONATAL INTENSIVE CARE UNIT
Edwards S1, Khaki S2, Gievers L2. 1Oregon Health & Science University, Portland, OR and 2Oregon Health & Science University, Portland, OR
Purpose of Study: Social determinants of health (SDOH) screening tools can be used to identify patients and families who are at risk of potential negative health outcomes. Upon admission to the Neonatal Intensive Care Unit (NICU), a patient’s caretaker(s) receives a 10-item SDOH screening tool depending on needs, social workers help families connect with hospital, community, and legal resources. The purpose of this study is to determine what percentage of NICU families complete this screening tool and how they respond to the questions. Additionally, this study aims to determine the characteristics of families who fill out the screeners compared to those who do not.
Methods Used: A retrospective chart review from 6/1/20 to 6/1/23 was performed at a quaternary, academic medical center. Screening tool completion rates were obtained by comparing completed screeners to admission data. Frequency of positive responses (indicating a concern in that area) were obtained from completed screeners. Various sociodemographic characteristics (race, ethnicity, insurance status, mode of delivery, etc.) were compared when analyzing response rates.
Summary of Results: 381 families completed the screening tool, with a 19.2% completion rate. Of the 10 SDOH categories, the highest number of positive responses were need for food assistance (40.2%), concerns about job security (18.9%), and problems with childcare (12.1%). A majority of families had at least one SDOH concern (51.7%), and 12.1% of families had 3 or more concerns. 27.6% of the screening tools were completed by the non-gestational parent. [Table]
Based on preliminary data, the demographic data (sex, race, ethnicity, gestational age, etc.) for screening tool respondents was similar to all NICU admissions in the study period. Based on race, Black families had the lowest completion rate (17.0%), while American Indian/Alaskan Native families had the highest (25.9%), but this difference was not statistically significant (p=.36). Families with public insurance completed the screening tool at a slightly higher rate than families with private insurance (19.6% vs 18.6%, p=.82), although this was not statistically significant. There was a significant difference in completion rates based on gestational age at birth. Families with term neonates had the lowest completion rate at 15.3%, while families with very preterm neonates (28 to <32 weeks) had the highest completion rate at 26.4% (p=0.01). [Table]
Conclusions: The majority of families endorsed at least 1 social stressor on admission to the NICU and 12% of families reported 3 or more concerns. The completion rates also showed disparity among different groups. Given the growing literature surrounding SDOH and the negative impacts they impart on children’s growth and development, this work supports a tremendous need for holistic care in the NICU, not just medical interventions. A future direction will include a quality improvement project to increase the completion rates of the SDOH screening tool in the NICU within certain populations.
Responses and Response Rates for SDOH Screening Tools.
Responses to SDOH Questions (n=381)
Response Rates by Demographic Data
Yes
No
Q1 (childcare concerns)
12.1%
87.7%
Total Completion Rate
19.2%
Q2 (food insecurity)
8.1%
91.9%
Q3 (trouble paying utilities)
4.2%
95.8%
Race
White
21.7%
Q4 (unstable housing)
3.4%
96.6%
Black
17.0%
Q5 (environmental safety concerns)
3.7%
96.3%
Asian
18.5%
Q6 (transportation problems)
3.1%
96.9%
American Indian/Alaskan Native
25.9%
Q7 (personal safety concerns)
1.6%
98.4%
Pacific Islander
18.8%
Q8 (receiving/been denied food assistance)
40.2%
59.8%
Q9 (job insecurity)
18.9%
81.1%
Ethnicity
Non-Hispanic
20.7%
Q10 (caretaking for other family members)
2.6%
97.4%
Hispanic
24.7%
Other
13.8%
Positive Response to 1 SDOH
28.1%
Positive Response to 2 SDOH
11.5%
Insurance Type
Public (Medicaid)
19.3%
Positive Response to 3+ SDOH
12.1%
Private
18.7%
Negative Response to all SDOH
48.3%
Mode of Delivery
C-Section
19.6%
English Form Filled Out
95.0%
Vaginal
18.6%
Spanish Form Filled Out
5.0%
Gestational Age at Birth
Extremely Preterm (
21.8%
Gestational Parent Filled Out Form
66.9%
Very Preterm (28-
26.4%
Non-Gestational Parent Filled Out Form
27.6%
Moderate or Late Preterm (32-
21.5%
Both Parents Filled Out Form
5.5%
Term (37-42 weeks)
15.3%
# 405
EXPLORING DISPARITIES IN DERMATOLOGY MATCH RATES FOR WOMEN AND UNDERREPRESENTED POPULATIONS: AN ANALYSIS OF TRENDS BETWEEN 2015-2022
Small EA1, Brandt Z1, Kearns D2, Fay AB1, Wongworawat MD3. 1Loma Linda University, Loma Linda, CA; 2Loma Linda University, Loma Linda, CA and 3Loma Linda University, Loma Linda, CA
Purpose of Study: In this study, the authors aim to investigate the relative risk of not matching for women and underrepresented populations into dermatology residency programs and explore potential factors that may contribute to the observed disparities. In addition, conduct an investigation into the impact of virtual interviews on match rates.
Methods Used: Demographic information on dermatology residents was obtained from the Accreditation Council for Graduate Medical Education data books for the period of 2015-2016 to 2021-2022. The corresponding applicant pool was obtained by analyzing four years of Electronic Residency Application Service statistics, which were retrieved from the Association of American Medical Colleges website. The race and gender composition of the applicant pool was then compared to that of the enrolled residents to calculate the relative risk of not matching for women compared to men and for underrepresented populations (including Black, Hispanic, Asian, and Native individuals) compared to White applicants. The academic year 2021-2022 is the year in which transitions to virtual interviews are observed.
Summary of Results: The relative risk of going unmatched for women was less than men. Underrepresented populations consistently had a higher relative risk of going unmatched. In the academic year 2021-2022 there was a decrease in relative risk of going unmatched for all underrepresented populations and women. This shows a trend towards increased match rates with the transition to virtual interviews.
Conclusions: Our findings illustrate an interesting pattern for women applicants aspiring to secure a position in a dermatologic residency. Notably, women exhibit a considerably lower risk of going unmatched compared to their male counterparts. These findings suggest that women have a more favorable path in terms of securing residency positions within dermatology. Despite the lack of diversity within the field of dermatology as a whole, it seems as though residency programs are recognizing the disparities that exist within the field and are making strides toward a more equitable future in medicine.
Conversely, when examining the data pertaining to applicants identifying as Black, Hispanic, Asian or Native consistently face a higher relative risk of going unmatched compared to the White applicants. These findings highlight the issue of the underrepresentation of minority populations within dermatology. These disparities not only limit access to dermatologic care but also hinder the diversity and cultural competency within the field, all factors that contribute to improved patient outcomes.
Relative risk of going unmatched for underrepresented populations compared to white applicants and women compared to men.
Residency Years
Black
Hispanic
Asian
Native
Women
2015-2016
1.27(1.18 to 1.36)
1.34(1.26 to 1.42)
1.22(1.16 to 1.28)
1.51(1.40 to 1.64)
0.88(0.85 to 0.92
2016-2017
1.28(1.19 to 1.38)
1.39(1.32 to 1.47)
1.24(1.18 to 1.31)
1.53(1.40 to 1.67)
0.85(0.81 to 0.89)
2017-2018
1.34(1.25 to 1.45)
1.46(1.38 to 1.55)
1.24(1.18 to 1.31)
1.58(1.43 to 1.74)
0.83(0.79 to 0.87)
2018-2019
1.30(1.20 to 1.40)
1.43(1.36 to 1.51)
1.18(1.11 to 1.24)
1.56(1.42 to 1.70)
0.86(0.82 to 0.90)
2019-2020
1.26(1.17 to 1.35)
1.39(1.31 to 1.46)
1.18(1.13 to 1.25)
1.47(1.32 to 1.65)
0.86(0.83 to 0.90)
2020-2021
1.22(1.13 to 1.31)
1.37(1.30 to 1.45)
*1.09(1.03 to 1.15)
1.56(1.44 to 1.68)
0.87(0.84 to 0.91)
2021-2022
1.20(1.12 to 1.28)
1.15(1.08 to 1.22)
*1.07(1.02 to 1.12)
1.47(1.35 to 1.59)
0.84(0.81 to 0.87)
For all years and all populations p.
Healthcare Delivery Research III
Concurrent Session
10:15 AM
Friday, January 19, 2024
# 406
COST-EFFECTIVENESS ANALYSIS: EARLY LEAK DETECTION AFTER UPPER INTESTINAL OR GASTRIC SURGERY AT UNIVERSITY OF CALIFORNIA, IRVINE HEALTH
Hassani P, Wignarajah SR, Ho E, Shu C, Fateri C, Sabour R, Gerges M, Houshyar R. University of California Irvine, Orange, CA
Purpose of Study: The routine utilization of an upper gastrointestinal (UGI) series in the initial 24 hours following upper intestinal or gastric surgery has been regarded as a diagnostic technique for the early identification of postoperative complications, including gastrointestinal leaks. However, its efficacy has been questioned in several studies. The purpose of our study is to evaluate the fluoroscopically identified leak rate in a retrospective fashion and to assess the value of routine upper GI series in the immediate post operative setting. Additionally, we will explore alternative approaches for triaging post operative patients based on early signs and symptoms of sepsis.
Methods Used: We conducted a retrospective analysis of data derived from 2091 consecutive fluoroscopic studies for unique patients performed between January 2017 and June 2023. We included 1,458 patients who had undergone fluoroscopic evaluation within the initial 24 hours after their surgical procedures at our institution and excluded the rest. Demographics and surgical data were collected. Charts were reviewed to examine immediate clinical signs including heart and respiratory rate, temperature, type of surgery, blood pressure, and white blood cell count within the first 24 hours. Differences in the early clinical parameters were assessed for patients with gastrointestinal leak and those without using the Wilcoxon rank-sum test and Student t-test.
Summary of Results: 633 patients were excluded as they did not meet the inclusion criteria. 37 out of 1,458 individuals (2.54%) were diagnosed with post operative leak based on their gastrointestinal fluoroscopic imaging. Given a rate of 2.54%, and the average cost of a postoperative UGI contrast study of $300, it would require an expenditure of $11,811 to perform 39 routine UGI series in order to detect one leak. On average, Patients who experienced leaks exhibited higher pulse rates (89 vs. 80 beats per minute, P-value <0.01) and respiratory rates (18 vs. 16 breaths per minute, P-value <0.01).
Conclusions: This study indicates that a low percentage of post operative patients are positive for gastrointestinal leak in the immediate post operative setting when fluoroscopy is performed routinely. This highlights the inefficiency of reflexive fluoroscopic evaluation. Redirecting resources towards the early identification of septic symptoms may prove to be a more efficient and cost-effective strategy for identifying leaks following upper intestinal or gastric surgery.
# 407
IS BLOOD GLUCOSE RELATED TO THE OUTCOME OF TRAUMATIC BRAIN INJURY AT THE DISCHARGE OF INPATIENT REHABILITATION?
Tan A1, 2, Fanchiang S1, 2, Friedman T1, 2, Jordan B2. 1Charles R. Drew University, Los Angeles, CA and 2Rancho Los Amigos, Downey, CA
Purpose of Study: To explore the relationship between the blood glucose (BG) measured at the admission of an inpatient rehabilitation facility (IRF) and the outcomes at the discharge among patients with traumatic brain injury (TBI).
Methods Used: TBI Registry is a retrospective study using the electronic medical record (EMR) with patients admitted from 2018 to 2020 who met the inclusion criteria of TBI ICD-10 codes and were complicated mild and moderate/severe TBI. The outcome was reflected by the Disability Rating Scale (DRS) score, rated by three DRS-certified reviewers. The demographic variables, rehabilitation length of stay (LOS), injury mechanism, and comorbidities were included. The Glasgow Coma Scale (GCS) at the emergency room admission implied TBI severity. Two BG groupings were used: BG4 (Alhatemi et al., 2022) and BG2 (Tirosh et al., 2005). Exploratory analyses and stepwise linear regression analyses were used.
Summary of Results: With the complete data (N=278), significant relationships between DRS and GCS, LOS, age, and BG4 were found. Table 1 depicts the differences in DRS among the GB4 groups. The mean DRS did not exhibit a consistent increase when BG was > 110 mg/dL. DRS was significantly predicted by the combination of GCS, age, LOS, and the lowest level of BG4 (i.e., <110 mg/dL) (Table 2). The mean DRSs by BG2 with the cut point of 100 mg/dL were not significant (Table 3) but unequal variances were noted (F: 20.595, p .000). Hence, the similar stepwise regression model to replace BG4 with BG2 did not include BG2 as one of the significant independent variables.
Conclusions: The BG measured at the admission of an IRF was related to the discharge outcome of TBI. About 65% (181/278) of the patients with TBI were found to have BG < 110 mg/dL and within this group of patients, the lower the BG the worse the outcome. For patients with BG > 110 mg/dL, it seems the higher the BG, the worse the outcome; the data did not support the linear relationship between BG and DRS. Which may echo that both hyperglycemia and hypoglycemia will yield worse outcomes. A test that can capture BG during a longer period, e.g., from the onset of TBI to the admission of IRF, will be helpful. Further prospective studies are necessary to confirm the relationship between BG and the outcome of inpatient rehabilitation for patients with TBI.
# 408
IMPLEMENTATION OF AN ADAPTED DIALECTICAL BEHAVIOR THERAPY PROGRAM AND EFFECTS ON ACUTE SERVICE USE: A QUALITY IMPROVEMENT INITIATIVE
Ng P2, Zhang Y2, Kim S1, Smit M1, 3. 1University of British Columbia, Vancouver, BC, Canada; 2University of British Columbia, Vancouver, BC, Canada and 3Fraser Health Authority, Surrey, BC, Canada
Purpose of Study: Borderline personality disorder (BPD) is serious and affects 1-6% of the population, with 10% dying by suicide. Comprehensive Dialectical Behavior Therapy (DBT) is effective for BPD but is costly and difficult to implement. Emerging evidence supports the skills training component of DBT (DBT-ST) as standalone treatment. Fraser Health Authority (FHA) in Metro Vancouver, Canada is a publicly funded healthcare organization serving over 1.9 million people. FHA has implemented an adapted DBT program consisting mainly of DBT-ST groups. This quality improvement initiative studies the impact of this program on acute service use.
Methods Used: This retrospective chart review includes 214 adults in the DBT program from 2013-2020. Demographics, baseline BPD symptoms, and acute service use for one-year before and one-year after the start of treatment were recorded. Acute service use was defined as emergency department (ED) visits or inpatient unit (IPU) admission days and was divided into psychiatric or non-psychiatric. Differences between pre- and post-treatment acute service use were examined using exact McNemar’s tests and Wilcoxon signed-rank tests for non-normally distributed data.
Summary of Results: Total psychiatric ED visits and IPU days each decreased by >50% post-treatment. Non-psychiatric acute service use increased by about 20%. Exact McNemar’s test showed a significant increase in the proportion of clients with 0 psychiatric ED visits (p < 0.001) and 0 psychiatric IPU days (p = 0.002) post-treatment. The differences in non-psychiatric ED visits (p = 0.457) and IPU days (p > 0.999) were not significant. 64 clients made fewer psychiatric ED visits post-treatment while 20 made more. 48 clients had less psychiatric IPU days post-treatment while 21 had more. Wilcoxon signed-rank tests showed statistically significant fewer psychiatric ED visits (Z=-5.051, p<0.001) of medium effect size and fewer psychiatric IPU days (Z=-3.295, p=0.001) of small effect size.
Conclusions: The adapted DBT program in FHA consists mainly of skills training groups, allowing it to reach more patients in a resource-limited setting. Psychiatric ED visits and IPU days decreased significantly with meaningful cost savings. Further quality improvement may inform if an expansion of comprehensive DBT may be beneficial to a subset of patients.
Exact McNemar’s test on acute service use before and after treatment.
Psychiatric ED Visits
After
Psychiatric IPU Days
After
Before
0 ED Visits
≥1 ED Visits
Before
0 IPU Days
≥1 IPU Days
0 ED Visits
124
13
0 IPU Days
142
15
≥1 ED Visits
53
24
≥1 IPU Days
38
19
Non-Psychiatric ED Visits
After
Non-Psychiatric IPU Days
After
Before
0 ED Visits
≥1 ED Visits
Before
0 IPU Days
≥1 IPU Days
0 ED Visits
118
29
0 IPU Days
191
10
≥1 ED Visits
36
31
≥1 IPU Days
9
4
Acute service use pre and post treatment.
# 409
CHILD LIFE SPECIALISTS FOR PEDIATRIC BURN WOUND CARE
Kore Z1, Courtemanche R2, Tuen Y2, Nixon J3, Kwong G3, Shen Y4, Knight P5, Hynes S1, 2. 1University of British Columbia, Vancouver, BC, Canada; 2BC Children’s Hospital, Vancouver, BC, Canada; 3BC Children’s Hospital, Vancouver, BC, Canada; 4BC Children’s Hospital Research Institute, Vancouver, BC, Canada and 5University of British Columbia, Vancouver, BC, Canada
Purpose of Study: Acute burn wound care procedures can be painful and distressing for pediatric patients. Child Life Specialists (CLS) are healthcare professionals who apply evidence-based psychosocial interventions, including distraction and play therapy, to improve coping skills in children undergoing various medical procedures. This study aims to estimate the effect of CLS support on patient pain and anxiety for children receiving acute outpatient burn wound care.
Methods Used: This was an observational quality improvement study. Children undergoing acute burn wound care without sedation at our outpatient unit received different levels of CLS support: none, developmental toys, a preparatory booklet, and/or in-person support. Patients deemed to be at risk for procedural anxiety were selected for in-person CLS support. Surveys were administered to children, parents, and staff. Procedural pain was measured using the Wong-Baker FACES Pain Rating Scale. Procedural anxiety was assessed using the Venham Picture Test for children and Venham’s Anxiety Rating Scale for parents and staff. Demographic and burn characteristics were obtained from medical charts. Data were analyzed descriptively, and univariate analyses using a Generalized Estimating Equations model were employed to assess the impact of CLS support.
Summary of Results: To date, 45 patients (mean age=6.3 years) have been recruited. The majority of burns were scald injuries (57.8%) to the extremities (66.7%) with superficial partial-thickness depth (61.0%) and a mean total body surface area of 2.0%. Children who received in-person CLS support reported significantly lower pain (-3.69, p<0.001) than those with no support, while anxiety scores were not significantly different (+1.04, p=0.329). Children who received developmental toys and/or a preparatory booklet reported less pain than children with no support (-2.57, p=0.022), while anxiety scores were not significantly different (-0.89, p=0.196). Parent reports of patient pain and anxiety revealed no differences across levels of CLS support. Staff reports of patient pain showed no differences across levels of CLS support; however, reported anxiety was significantly higher for patients who received in-person CLS support (+0.86, p=0.029). Staff who perceived children as prepared for their burn wound care visit reported significantly lower patient pain and anxiety (p<0.001).
Conclusions: Preliminary results suggest CLS support can reduce a child’s perceived pain during outpatient burn wound care. The effect of CLS support on anxiety remains unclear. Our findings may be confounded by the CLS providing in-person support to children with a history of anxiety or showing signs of anxiety during the visit. Future data collection and analysis will account for these factors. This project has important implications for optimizing the quality of care at our outpatient burn unit.
# 410
Pharm2Home Initiative: Clinical Services at Your Home
Young C1, Wong S1, AJMAL A2. 1Touro University California, Vallejo, CA and 2Touro University California, Vallejo, CA
Purpose of Study: According to the CDC, 60% of American adults are living with a chronic disease. In 2016, Solano County, CA had higher than state average hospitalizations for diabetes, heart failure, and COPD/asthma. The Pharm2Home Initiative is a pharmacist-led intervention aiming to improve chronic disease management, self-efficacy, and preventative care through home visits and telehealth. This initiative aims to advance health equity in chronic disease management by providing interprofessional care coordination, education, and medication management. Pharm2Home co-manages the following conditions with the Solano County Family Health Services clinic system: diabetes, hyperlipidemia, hypertension, heart failure, chronic kidney disease, hypothyroidism, asthma, COPD.
Methods Used: Pharm2Home used a patient-centered approach. An initial home visit addressed participants’ challenges and medication quality/adherence. Subsequent telehealth/home visits occurred on a bi-weekly to monthly basis over a period of four to six months. Each appointment addressed medication adherence, education, and condition outcome measures.
The Pharm2Home Initiative’s evaluation focused on psychosocial (i.e., perceived self-efficacy through behavioral modifications), educational (i.e., understanding of chronic disease, measured through medication adherence as a proxy), and clinical outcomes. Outcomes were measured using validated survey tools and compared baseline and post-intervention data. Post-intervention data was collected after three and six months to monitor sustainable outcomes.
Summary of Results: 627 interventions were implemented between June 1st, 2020 to mid-May 2022. 59 patients completed an initial visit and 4 completed the program. 47 participants demonstrated behavioral modifications, such as lifestyle habits, monitoring habits, and self-efficacy. At baseline, 8 and 1 participants self-monitored blood glucose (SMBG) and blood pressure (SMBP), respectively. At the time of evaluation, 26 and 21 additional participants self-monitor SMBG and SMBP, respectively. HbA1c average dropped from 10.2% (baseline) to 9.4% (follow-up), with 23 participants exhibiting an improved HbA1c. 39 hypoglycemic episodes leading to hospital visits were prevented by Pharm2Home.
Conclusions: The Pharm2Home Initiative used pharmacist interventions to advance health equity in chronic disease management for Solano County’s underserved populations. In partnership with safety-net clinic systems, programs of this nature address polypharmacy management, self-efficacy, and education to empower patients in managing their conditions. Tertiary prevention, as measured by prevented hospitalizations/ER visits, was also addressed through home visits and telehealth.
Self-efficacy and lifestyle modification showed some improvement in the post-intervention period in comparison to baseline. However, sustained behavioral modification in chronic disease management beyond this period needs to be evaluated and factors that impact self-efficacy need to be further analyzed.
# 411
EVALUATING AFFORDABILITY OF TELEHEALTH MEDICATION ABORTION SERVICES IN CALIFORNIA, UNITED STATES
Ebadani L1, 2, Fiastro A2, Godfrey E2. 1University of Washington, Seattle, WA and 2University of Washington, Seattle, WA
Purpose of Study: California constitutes 20% of total abortions in the United States. Telehealth medication abortion is an alternative to expensive brick-and-mortar services, however limited information exists about its affordability in California. This study examines the use of sliding scale payment for Aid Access telehealth medication abortion service among California residents and assesses if sociodemographic factors are associated with payment.
Methods Used: This cross-sectional study analyzes California Aid Access questionnaires between March 2022 to December 2022 (n=2,236). Respondents with missing payment (n=1, 0.04%) and reshipment or failed shipment responses (n=6, 0.2%) were excluded yielding the analytic sample (n=2,229). Patient sociodemographic characteristics were described. The association between age, race and ethnicity, social vulnerability, and urbanicity and reduced payment was assessed using logistic univariable and multivariable regression.
Summary of Results: 22.7% of participants were unable to pay the full cost for medication abortion (M = $68.43). Patients younger than 20 years old were more likely to pay a reduced rate as compared to older patients (OR = 1.45, 95% CI: 1.07, 1.95). Patients who identified as Black/African (OR = 2.51, 95% CI: 1.68, 3.73), Hispanic/Latinx (OR = 1.76, 95% CI: 1.32, 2.35), multiracial/other (OR = 1.52, 95% CI: 1.02, 2.25), and preferred not to answer (OR = 1.57, 95% CI: 1.11, 2.21) had higher odds of paying less compared to White patients.
Conclusions: These findings suggest that medication abortion is expensive among California residents and certain groups are more likely to pay a reduced fee. We recommend including insurance coverage in these services to improve affordability.
# 412
EFFECTIVENESS OF A NOVEL SCHOOL-BASED DIABETES PREVENTION PROGRAM: A POST-IMPLEMENTATION ANALYSIS OF AROGYA WORLD HEALTHY SCHOOL PROGRAM, INDIA 2015-2022
Rajeshuni N1, Huynh M2, Mahajan S3, Bacong A1, Mukherji A1, Jaswal N4, Ramalingam S4, Ganesh N4, Pahwa S4, Saligram N4, Palaniappan L1. 1Stanford University School of Medicine, Stanford, CA; 2University of California Irvine, Irvine, CA; 3University of Rochester, Rochester, NY and 4Arogya World, Bengaluru, India
Purpose of Study: Non-communicable diseases (NCDs) pose significant challenges worldwide, particularly in low- and middle-income countries (LMIC). In India, NCDs like diabetes mellitus are on an alarming rise, especially amongst its youth. The Arogya World’s Healthy School Program (HSP), a two-year school-based initiative for 11-14-year-olds, targets diabetes prevention through health literacy and lifestyle modification. This study evaluates this intervention’s effectiveness in enhancing diabetes knowledge, attitudes, and practice.
Methods Used: Arogya World implemented HSP across 18 states and >7,500 schools, reaching nearly 450,000 students across rural and urban India. A sample of students was surveyed pre- and post- each year of intervention using Knowledge, Attitude, and Practice (KAP) questionnaires. This study presents a post-implementation quasi-experimental analysis of data from 2015-2022. Improvements in knowledge, dietary patterns, and physical activity levels were evaluated using descriptive statistics and mixed effects regression.
Summary of Results: The survey encompassed a sample of 6,616 students ages 11 to 15 years. Overall knowledge scores improved by 15.9% with gains in nutrition (14.6%), physical activity (13.1%), and diabetes awareness (24.5%) [p<0.01]. With respect to behavior change, healthy food consumption improved by 7.4% and physical activity by 10.1% (p<0.01). Outcomes varied by partner and intervention modality (in-person versus hybrid incorporating digital formats) but overall showed improvement.
Conclusions: This implementation of a low-cost, scalable health education program utilizing a school-based, peer-led model incorporating student leadership was highly effective in enhancing knowledge and behavior change relevant to diabetes prevention. Such programs hold tremendous potential in curbing the NCD crisis globally.
# 413
RADIOLOGY-DRIVEN PULMONARY NODULE CLINIC REFERRALS: WORKFLOW AND COST OF CLINICAL IMPLEMENTATION
Aldoghmi M, Nakashima K, Shu C, Gerges M, Aguilar D, Park S, Shieh S, O’Connell R, Houshyar R. University of California, Irvine, Irvine, CA
Purpose of Study: Lung cancer is the leading cause of cancer-related death in adults, with an estimated 234,000 cases and over 154,000 deaths yearly in the United States. With current advancements, the time of diagnosis and appropriate follow-ups are directly related to improving clinical outcomes—estimates of five-year survival rates average 18 percent in all patients with lung cancer. Multidisciplinary pulmonary nodule clinics have emerged as promising solutions for optimizing the efficiency of time to diagnosis. We aim to showcase how a lung nodule referral program was implemented at a single institution and its associated costs, with subsequent studies analyzing follow-up rates and TNM staging before and after the implementation of the referral program.
Methods Used: This study evaluated patient referrals to pulmonary nodule clinics using radiology reports exported from the Department of Radiology at UC Irvine Medical Center, an academic medical center. The program uses mPower, an algorithm that searches radiology reports to detect various items to index follow-up recommendations and collect a list of patients that meet the inclusion criteria. Inclusion criteria include lung nodule(s) ≥ 7mm, corresponding with a Lung-RADS score of 3 or 4, and referred to the pulmonology clinic for follow-up between October 2020 and April 2023. An interventional pulmonologist then uses Fleischner criteria to stratify patients by risk for management. Radiology reports were compared to pathology queries conducted at the pulmonary nodule clinic. From the lung biopsies conducted, the percentages of cancers and cancer subtypes were determined. Moreover, the cost-effectiveness was determined by comparing implantation of the noninvasive > 7mm tumor size biomarker to USPSTF guidelines of a diagnostic biomarker of at least 90% specificity and medium sensitivity that costs $250 or less.
Summary of Results: In total, 285 of 2096 referred patients (14%) underwent lung nodule biopsy. Among those biopsied, 98 of 285 (34%) had metastasis (non-primary), 86 of 285 (30%) had non-small cell carcinoma, 86 of 285 (30%) had benign nodules, 14 of 285 (5%) had infectious nodules, and 1 of 285 (0.4%) had small cell carcinoma (figure 1). Annually, the referral program’s gross total cost is $4,541, considering ancillary costs of mPower software and nursing salary. Implementing the diagnostic biomarker of >7mm criteria for referral indicates a cost-effective screening program per USPSTF.
Conclusions: In conclusion, we found that implementing a lung nodule referral program can contribute to developing similar referral programs in other healthcare settings by guiding patient selection criteria, referral processes, and cost considerations. Subsequent research includes determining TNM staging before and after implementation of this referral program with the hypothesis that tumors found after the program were caught earlier in the disease course to reduce patient mortality risk with a shorter time from diagnosis to treatment.
# 414
COMPARISON OF A NOVEL GENERALIZED DEEP LEARNING MODEL TO A TRADITIONAL SUPERVISED MODEL FOR LIVER AND SPLEEN SEGMENTATION ON ABDOMEN AND PELVIS COMPUTED TOMOGRAPHY
Danza CN1, Cortes G1, Chantaduly C1, 2, Wu AT1, Sabour R1, Jung J1, Shu C1, Ho E1, Law K1, Chang P1, 2, Houshyar R1. 1University of California, Irvine, Irvine, CA and 2University of California, Irvine, Irvine, CA
Purpose of Study: Computed tomography (CT) is commonly used in evaluation and diagnosis of hepatosplenomegaly. However, volume is often estimated using the largest single axis of the organ, a heuristic vulnerable to confounding factors such as patient sex and body size. Machine learning (ML) models offer promise for improved organ measurement. Supervised ML has been shown to have high accuracy at the cost of intense manual labeling and low generalizability. Unsupervised ML may offer benefits for decreased labeling burden while maintaining efficacy, but there is a current gap in the literature on comparing the performance and efficiency of supervised and unsupervised ML models for abdominal organ segmentation. This study aims to compare the performance and time-savings of an unsupervised deep learning algorithm to supervised 3D-2D U-Net convolutional neural networks (CNN) specialized for liver and spleen volume segmentation.
Methods Used: A new unsupervised ML model (ATLAS) trained on 14,366 unlabeled abdominal/pelvis CT scans was developed to segment structures in the abdominal cavity. Two 3D-2D U-Net CNNs trained on 500 manually labeled abdominal/pelvis CT scans for liver and spleen, respectively, were developed for comparison. All models were tested on a random 1% subset of 10,000 sequential single-institution abdominal/pelvis CT scans of adults without acute liver or spleen pathology. Ground truth was manually segmented by medical students with radiology resident or attending physician verification. Individuals self-reported time spent on manual annotation of each scan for the test cohort. Dice coefficients were calculated to compare model performance.
Summary of Results: The median Dice coefficient for ATLAS and ground truth liver segmentation was 0.930 (interquartile range 0.917-0.942), compared to 0.964 (0.959-0.967) for CNN and ground truth. The median Dice coefficient for ATLAS and ground truth spleen segmentation was 0.867 (0.829-0.890), compared to 0.939 (0.926-0.948) for CNN and ground truth. Total time spent segmenting the liver for the test cohort was 1064 minutes (mean 10.64 min/scan). Total time for spleen segmentation on the test cohort was 805 minutes (8.05 min/scan).
Conclusions: The performance of ATLAS was comparable to CNNs specialized for liver and spleen segmentation, demonstrating usefulness of a generalized, unsupervised ML model for organ measurement. Significant time was spent on manual image annotation, with about 31 person-hours required for the combined test set. Extrapolating the measured times for annotation to the 500 training scans annotated for CNN training yielded an estimated 155.75 person-hours, representing a notable relative time-savings of an unsupervised ML model over a supervised model. Comparable performance with extensive time-savings highlights a compelling benefit to the development of unsupervised ML models in radiology, which have an additional advantage of future application to other organ segmentations with minimal additional training.
Hematology and Oncology II
Concurrent Session
10:15 AM
Friday, January 19, 2024
# 415
Proposing A New Standard Hemoglobin Value Distribution Curve in Efforts to Improve Diagnosis and Treatment of Anemia in High Altitude Nepalese Populations
Pozo L1, Ghimire A2, Judkins A1, Fassl B1. 1northeast Ohio Medical University, Rootstown, OH and 2Mountain Medical Institute, Namche Bazaar, Nepal
Purpose of Study: In 2010, the World Health Organization (WHO) defined anemia as Hemoglobin (Hb) values <12 g/dL in premenopausal females and <13.0 g/dL in others. These values vary globally, with Andes Mountain populations having the highest incremental Hb increase (1 g/dL/1000 m). Tibetans at extreme altitudes have shown lower Hb concentrations than Andeans. Gender differences persist at altitude, but data for infants, children, and pregnant women are lacking. Research highlights the importance of distinguishing normal Hb distributions for high-altitude populations, impacting anemia diagnosis and related conditions. Recent Nepal data reveals varying anemia rates, notably lower in mountainous regions. Limited research in these areas necessitates efficient anemia detection to improve outcomes. Exposure to high altitude has a significant impact on blood hemoglobin concentrations but little is known about its effect in Nepal’s Sherpa population who are genetically uniquely adapted to life at high altitude and no universally accepted normal values exist for this patient population. We aim to describe the normal distribution of hemoglobin values in this population and describe rates of anemia using the WHO diagnostic criteria of anemia at altitude while comparing them to values calculated from our data set and discussing notable differences.
Methods Used: A Nepali medical team carried out a population anemia screening program in Pasang Lhamu Municipality in November 2022 using a validated point-of-care, handheld hemoglobin screening device. Screenings took place in nine villages and involved a convenience sample during screening events open to the public. We abstracted demographic, geographic and clinical information from the existing medical record.
Summary of Results: 830 screenings were performed, 54% female. The mean hemoglobin concentration ± 2SD among adults was 15.06 ± 4.58; for women 14.24 ± 3.64, men 16.22 ± 4.80, children aged 0-5 12.76 ± 3.64, women of childbearing age 14.35 ± 1.79; for children aged 5-17 14.09 ± 3.80. Using WHO altitude adjusted diagnostic criteria for anemia 34.51% of adult men, 54.56% of adult women; 68.85% of children under 5 and 22.65% of children 5-17 were anemic. Up to 31% of patients in certain groups met criteria for polycythemia.
Conclusions: Noting the high percentages of patients classifying as anemic under WHO criteria, unique diagnostic considerations need to be applied in the high altitude resident Sherpa population for diagnosing and managing anemia.
Outcome Summary Table
Ethnicity
Hb value interval (g/dL)
Average Hb value (g/dL)
% Polycythemic
% Anemic
% Anemic (WHO)
Rai Female (Age 5-17 sample size 63)
10.85 - 18.03 (95% CI)
14.43 ± 1.76
11.11%
3.17%
53.97%
Rai Male (Age 5-17 sample size 67)
10.86 - 18.49 (95% CI)
14.67 ± 1.91
1.49%
4.48%
70.15%
Sherpa Female (Age 5-17 sample size 75)
9.85 - 18.18 (95% CI)
14.02 ± 2.08
5.33%
5.33%
57.33%
Sherpa Female (Age 18+ sample size 128)
11.02 - 17.57 (95% CI)
14.29 ± 1.64
5.47%
2.34%
53.13%
Sherpa Male (Age 5-17 sample size 65)
10.14 - 18.65 (95% CI)
14.4 ± 2.13
0%
4.62%
67.69%
Sherpa Male (Age 18+ sample size 76)
10.79 - 21.11 (95% CI)
15.95 ± 2.58
9.21%
5.26%
39.47%
Age
Hb value (g/dL)
Average Hb value (g/dL)
% Polycythemic
% Anemic
% Anemic (WHO)
0-5 (sample size 61)
9.11 - 16.41 (95% CI)
12.76 ± 1.82
1.64%
6.56%
68.85%
65+ (sample size 54)
9.43 - 18.96 (95% CI)
14.2 ± 2.38
11.11%
3.70%
72.22%
Women of Childbearing Age (sample size 300)
10.76 - 17.93 (95% CI)
14.35 ± 1.79
9.33%
1.33%
53.33%
Gender
Hb value (g/dL)
Average Hb value (g/dL)
% Polycythemic
% Anemic
% Anemic (WHO)
Female (5-17 sample size 218)
10.26 - 17.71 (95% CI)
13.99 ± 1.86
5.96%
5.50%
62.84%
Female (18+ sample size 202)
10.61- 17.88 (95% CI)
14.24 ± 1.82
0.005%
2.48%
54.56%
Male (5-17 sample size 228)
10.31 - 18.08 (95% CI)
14.19 ± 1.94
0.004%
3.51%
77.19%
Male (18+ sample size 142)
11.42- 21.02 (95% CI)
16.22 ± 2.40
12.86%
4.23%
34.51%
Altitude
Hb value (g/dL)
Average Hb value (g/dL)
% Polycythemic
% Anemic
% Anemic (WHO)
3440m (Namche,F 5-17 sample size 85)
10.43 - 16.86 (95% CI)
13.65 ± 1.61
2.35%
4.71%
76.47%
3790m (Khumjung,F 5-17 sample size 121)
11.14 - 17.82 (95% CI)
14.48 ± 1.67
9.92%
4.96%
57.85%
3440m (Namche,M 5-17 sample size 106)
10.63 - 16.56 (95% CI)
13.6 ± 1.48
0%
2.83%
91.51%
3790m (Khumjung,M 5-17 sample size 120)
11.04 - 18.34 (95% CI)
14.7 ± 1.83
0%
6.67%
79.17%
3440m (Namche,F 18+ sample size 41)
10.32 - 18.11 (95% CI)
14.22 ± 1.95
9.76%
0%
58.54%
3790m-3840m (F 18+ sample size 88)
11.12 - 18.14 (95% CI)
14.63 ± 1.75
10.23%
4.55%
54.55%
3440m (Namche,M 18+ sample size 36)
11.61 - 20.40 (95% CI)
16 ± 2.2
13.89%
5.56%
38.89%
3790m-3840m (M 18+ sample size 59)
11.95 - 21.79 (95% CI)
16.87 ± 2.46
16.95%
1.70%
33.90%
# 416
CHARACTERIZING PSYCHOLOGICAL RESOURCES AND RESILIENCE IN PATIENTS WITH BLADDER CANCER: ASSOCIATIONS WITH FRAILTY, MENTAL HEALTH, AND QUALITY OF LIFE
Petersen E2, Holt S1, Browning A2, Jannat S1, Cavanaugh D3, Wright J1, Gore J1, Schade G1, Psutka S1. 1University of Washington, Seattle, WA; 2University of Washington, Seattle, WA and 3Icahn School of Medicine at Mount Sinai, New York, NY
Purpose of Study: Bladder cancer (BC) profoundly affects patients’ mental and physical well-being, with reports of reduced social function, increased depression and impaired daily activities. Understanding factors that influence patients’ responses to BC is crucial to tailored care. One such factor that has yet to be studied in BC patients is resilience, or the ability to maintain or restore baseline function following a stressor. Our objective was to demonstrate the feasibility of prospectively characterizing baseline resilience and frailty in patients with BC. We hypothesized that resilience and psychological resources (PsyResources) would be positively associated with improved quality of life (QOL) and mental health outcomes and inversely associated with frailty.
Methods Used: With IRB approval, we enrolled patients with BC (N=67) from a urology clinic (6/20-7/2021). Patients completed a comprehensive geriatric assessment incorporating validated assessments of frailty and PsyResources: University of Washington Resilience Survey (UWR), Psychological Capital (PsyCap), Brief Inventory of Thriving (BIT), and Self-Compassion Survey (SCS) which measure resilience, psychological capital, self-compassion, and mental health. Validated QOL surveys were completed at 2 weeks, 3 and 6 months post-treatment. Correlation matrices evaluated PsyResources’ links with baseline frailty and Spearman’s correlation coefficient (ρ) was reported. Associations between PsyResources, anxiety and depression symptoms, and QOL were evaluated with linear regression.
Summary of Results: Most of the cohort (median age 71, 83.6% male) had muscle-invasive BC (77.6%; cN+:20.9%, M1: 7.6%). PsyResource assessment completion rates ranged 96-100% and had strong inter-assessment associations (ρ=0.52-0.81, p< 0.0001 for all). Baseline PsyResources were strongly inversely correlated with the geriatric depression scale, (ρ=-0.50-0.65, p<0.0001). Negative correlations were found between functional status and self-compassion (ρ=-0.37, p=0.006). Higher baseline PsyResources were associated with improved global symptoms, emotional function, cognitive function (SCS only), and body image (BIT and SCS) over time (p<0.05 for all). Higher baseline PsyResources were also associated with decreased anxiety and depression over time (coefficient:-0.167-2.46; p<0.02 for all).
Conclusions: We present the first characterization of baseline PsyResources in a prospective cohort of patients with BC. PsyResources demonstrated positive correlations with mental health and across construct and inverse correlations with functional frailty. Interestingly, PsyResources were associated with improved QOL symptoms over time. Ongoing work is exploring the relationship between resilience and different domains of frailty and the potential role of functional recovery and decline following BC treatment. Future work will also evaluate associations with survival outcomes and the ability to modify resilience to facilitate recovery of functional status and quality of life after treatment.
# 417
THE EFFECT OF MCT4 INHIBITOR CB-2A ON PD-L1 EXPRESSION IN TRIPLE-NEGATIVE BREAST CANCER
Kattunga V, Wu Y, Wu K. Charles R. Drew University of Medicine and Science, Los Angeles, CA
Purpose of Study: The aim of this thesis is to investigate the effect of MCT4 inhibitor CB-2a in TNBC. Specifically, we will explore the role of MCT4 in regulating PD-L1 expression, and how this regulation affects TNBC cell growth, invasion, and immune evasion. The ultimate goal of the current study is to identify novel therapeutic targets for this subtype of breast cancer. As TNBC is more prevalent in African-American women, our research project will have a broad impact on cancer health disparities research by providing a deeper understanding of the mechanisms that play a role in the disproportionate burden of cancer between racial and ethnic groups.
Methods Used: MDA-MB-231 cells were cultured and subjected to various assays to study PD-L1/MCT4 related pathways, interactions, and expression in TNBC. STRING, cBioPortal, Metascape, and UALCN-TCGA databases aided in gene and protein enrichment analyses. Western blot measured PD-L1 expression under CB-2a and lactate treatments. A wound confluence assay observed cell migration using BioTek tools. Cytotoxic activity of activated CTLs on MDA-MB-231 cells was quantified using ELISpot, with spot count indicating T-cell activation and potential cytotoxicity. Analyses were statistically validated, with findings potentially elucidating immune response and cancer interplay.
Summary of Results: The study explored the relationship between MCT4, PD-L1, and TNBC, revealing their co-enrichment in cancer-related pathways through gene enrichment analysis. MCT4 and PD-L1 showed significantly higher expression in TNBC than in normal tissues. Treatment with CB-2a reduced PD-L1 expression and inhibited TNBC cell migration and wound healing, while lactate increased PD-L1 expression, highlighting their roles in modulating cancer pathways. CB-2a also restored CTL activity, suggesting its potential to counteract PD-L1-mediated immune suppression. These findings underscore the therapeutic potential of targeting MCT4 and PD-L1 interactions in TNBC.
Conclusions: The study demonstrated that CB-2a treatment decreased PD-L1 expression in TNBC cells, associated with increased tumor-infiltrating lymphocytes and enhanced antitumor immunity. This effect is likely due to the disruption of metabolic reprogramming caused by MCT4 inhibition, altering the cancer cells’ metabolic landscape. Western blot analysis revealed higher lactate levels correlated with increased PD-L1 expression.The findings align with previous studies indicating the potential of MCT4 as a target to overcome immune evasion in TNBC. The study has broader implications, especially for diabetes-associated breast cancer, due to the alteration of tumor metabolism in hyperglycemic conditions and the potential for CB-2a to address associated challenges.
The research lays groundwork for further investigation into the clinical applications of such combination therapies for TNBC and other cancers. However, in vivo studies and further exploration into CB-2a’s mechanism of inhibiting PD-L1 expression are required.
# 418
EVALUATING THE INCIDENCE OF FEVER FOLLOWING VINCRISTINE ADMINISTRATION IN PEDIATRIC PATIENTS
Lehman T, Uppala S, Jarman J, Bou Fakhreddine A, Al-Rahawan MM. Texas Tech University Health Sciences Center, Lubbock, TX
Purpose of Study: Vincristine is a commonly utilized chemotherapy agent for various types of pediatric
cancers. The FDA label for vincristine states that fever is a possible side effect. Fever in patients receiving chemotherapy always triggers a sepsis workup. Only a handful of vincristine-induced fevers have been reported in literature, but the true incidence is not known.
Methods Used: We compared the incidence of fever after vincristine administration to fever incidence following administration of all other chemotherapy agents. This study is an IRB-approved retrospective chart review of children 0-17 years old receiving chemotherapy from January 1, 2017 – January 1, 2022. Any temperature exceeding 100.4 F is considered a fever. Only fevers within 48 hours following the administration of chemotherapy with a negative infectious workup were included. Statistical analysis was conducted using binomial and multivariable logistic regression. An alpha of 0.05 was used as the statistical significance threshold. Fever scores were then calculated by using methods outlined by Ammann, RA. et al. (2010).
Summary of Results: We identified 61 patients who fit the inclusion criteria. The patient population was comprised of 31 males and 30 females with a mean age of 7.7 years. Leukemia was the most common cancer diagnosis seen in 50% of patients in the study. The patient cohort included children who received vincristine monotherapy or multidrug chemotherapy with or without vincristine. 73.8% of patients received vincristine once or several times. Of the patients that received vincristine, 6.6% experienced fever within 48 hours of administration, with a mean fever score of 11.5. Of the 26.2% of patients that did not receive any vincristine, only one developed a fever with a score of 7.
Conclusions: Data analysis determined no statistically significant difference in fever occurrence between patients who received vincristine compared to those who did not. In addition, no statistically significant association was found between fever and the independent variables such as cancer category, race/ethnicity, and gender. Fever score comparison was not conducted due to the small portion of patients that experienced a fever. Expansion of the patient cohort is required to allow comparisons between groups and comparison of the incidence of fevers following vincristine versus other chemotherapy agents. A larger number of patients may show a correlation between vincristine and fever and help better inform the management of fever in vincristine receiving children.
Ammann RA, Bodmer N, Hirt A, et al. Predicting adverse events in children with fever and chemotherapy-induced neutropenia: The prospective Multicenter SPOG 2003 FN study. Journal of Clinical Oncology. 2010;28(12):2008-2014. doi:10.1200/jco.2009.25.8988
# 419
RATE OF PEDIATRIC RED BLOOD CELL ALLOIMMUNIZATION IS COMPARABLE TO ADULTS
Bharani B1, Saifee N2, 1. 1University of Washington, Seattle, WA and 2Seattle Children’s Hospital, Seattle, WA
Purpose of Study: Red blood cell (RBC) alloantibodies may develop when an individual recipient is exposed to a non-self RBC antigen via transfusion or pregnancy. A range of factors from characteristics of the particular donor blood group antigens to whether the recipient’s HLA protein binding motif can bind the non-self antigen play a role in whether someone develops an RBC alloantibody. RBC alloimmunization can cause acute or delayed hemolytic reactions and hemolytic disease of the fetus and newborn and thus are associated with transfusion-related morbidity and mortality. There is limited data on the rates of alloimmunization in pediatric patients, necessitating research in this field. In this study we set out to evaluate the rate of alloimmunization in pediatric patients and identify populations that may be at higher risk of alloimmunization.
Methods Used: A single center retrospective data review of RBC antibodies in patients with RBC transfusion orders at Seattle Children’s Hospital, a large tertiary care pediatric facility with over 360 hospital beds, was performed for a 5-year period (from 6/8/2018 - 7/5/2023). Demographic and red cell antibody specificity data for 5812 unique patients with RBC transfusion orders was extracted from an enterprise data warehouse. Chart review was performed for the 175 patients with non-ABO RBC antibodies to determine primary diagnosis and age at antibody formation.
Summary of Results: Overall 3.01% (175/5812) of patients with transfusion testing during the study had RBC antibodies detected. 1.36% (79/5812) had clinically significant antibodies, which is similar to the rate of antibody formation seen in other adult and pediatric cohorts.
Previous cohort studies of pediatric patients showed no antibody formation at less than 4 months of age and only rare case reports of RBC alloimmunization during neonatal period. In our study, 2 patients less than 4 months were identified to have clinically significant antibodies. Both were being treated with emapalumab for hyperinflammatory disorders.
Our study found a variety of RBC antibodies similar to that demonstrated in adult European cohorts and more varied than the Japanese pediatric cohort. However the Japanese pediatric cohort likely shows less antibody formation and less variety of antibodies due to being more racially homogenous compared to our patients. Other antibodies observed in our pediatric cohort included warm autoantibodies (0.81%), passive antibodies (0.67%), cold antibodies (0.91%) and clinically insignificant antibodies (0.1%).
Conclusions: This work provides data to blood banks in the US primarily treating pediatric patients on the type of RBC antibodies to expect and reagents to keep for immunohematology testing. It also provides a foundation for further research into factors associated with alloimmunization in pediatric patients.
# 420
MIRNAS-LINKED TO ONCOGENES IN OVARIAN HIGH-GRADE VERSUS LOW-GRADE SEROUS CARCINOMA
Schiff S, Muinde J, Carter C, Khan S. Loma Linda University, Loma Linda, CA
Purpose of Study: Ovarian cancers as a whole are aggressive cancers for which there are currently no efficient screening methods such as those which have significantly decreased the risk of death from cervical cancer and colorectal cancers. Ovarian cancer comprises about 1% of cancers, and about half of these women succumb to death, in part due to lack of early detection. Therefore, our lab focuses on discovering early molecular biomarkers using gene mutations and miRNA profiling. Many studies have shown miRNAs are dysregulated in ovarian cancer, however, no data showed significant relationships between these miRNAs to the prognosis/overall survival of ovarian cancer patients. We hypothesize that several miRNAs linked to oncogenes are altered differentially in ovarian low-grade versus high-grade serous carcinoma. miRNAs can alter oncogenes, and tumor suppressor gene expression levels, therefore they may serve as early biomarkers.
Methods Used: To analyze the expressions of oncogenes and miRNAs, we utilized the TCGA database from the University of Alabama at Birmingham (UALCAN) software. We determined the oncogenes with higher statistical significance on survival rates, age, race, cancer stages, tumor grade, and TP53 mutation status and miRNAs linked to them.
Summary of Results: Of the genes analyzed, BRAF, CCNE1, and MYC showed statistically significant data on survival rates. BRAF/CCNE1 are amplified in ovarian high-grade serous cancer, whereas MYC is upregulated in ovarian low-grade serous cancer. One or more miRNAs-linked to these oncogenes were selected based on their significance in different age, race, and survival rate.
Conclusions: Successful identification of early molecular markers in ovarian cancer will potentially allow for earlier detection and decreased mortality rates. Analysis of the appearance and abundance of miRNAs in early and late ovarian cancer can aid in earlier diagnosis. In further study, we hope to verify our results by testing a larger cohort of samples.
# 421
ENIGMA/PDLIM7 INTERACTS DIFFERENTIALLY IN THYROID CANCER SIGNALING PATHWAYS
Robins C1, Rood K1, Laxa R1, Yamauchi C1, Gomez G1, Sanchez-Ruiz K1, Khan A1, Mirshahidi S2, Simental A3, Khan S1, 3. 1Loma Linda University School of Medicine, Loma Linda, CA; 2Loma Linda University Medical Center, Loma Linda, CA and 3Loma Linda University, Loma Linda, CA
Purpose of Study: Due to the prevalence of thyroid cancer, there is a growing demand for stage-specific diagnostic testing to facilitate accurate and personalized treatment approaches. Our previous studies have demonstrated an association between Enigma protein (PDLIM7 gene) overexpression and thyroid cancer, particularly at different stages. Additionally, researchers are exploring Enigma’s links to proteins including PI3/AKT, TERT, VDR, DBP and MDM2 pathways. However, the precise downstream interactions that contribute to cancer progression necessitate further investigation. This study aims to explore the expression of Enigma and its interactions with genes involved in signaling pathways that drive cancer progression.
Methods Used: To achieve this, we used UALCAN software analysis with TCGA database to explore the presence of PDLIM7 and its correlation with 9 other genes involved in signaling pathways that contribute to cancer progression in thyroid cancer patients with different ethnicities. We also utilized western blotting and immunoprecipitation techniques to analyze protein extracts from thyroid cancer tissue, allowing visualization of Enigma expression and its interactions with various cancer-promoting proteins.
Summary of Results: We found that PDLIM7 gene expression was correlated with BAX, PIK/AKT, RUNX, BCL2, MDM2, PARP, MAPK, and RAS and strongly correlated with TGF-B. Analysis of western blot density revealed differential levels of expression for Enigma, PI3/AKT, MDM2, BMP-1, VDR, and DBP proteins. Furthermore, immunoprecipitation demonstrated strong interactions between Enigma and PI3/AKT, MDM2, and VDR proteins, whereas mild interaction with BMP-1 through targeted antigen-antibody binding.
Conclusions: Our study highlights the presence of proteins associated with Enigma expression in thyroid cancer tissue, along with the identification of different interacting partners within the Enigma signaling pathway. These findings suggest the potential of Enigma as a biomarker or therapeutic target for thyroid cancer patients. Further research using in vitro manipulation of Enigma expression is necessary to determine the most significant pathways of interaction and their role in cancer progression. This knowledge can pave the way for more effective treatment strategies for thyroid cancer patients in the future.
# 422
CREATING A PICTURE BOOK TO INCREASE CANCER KNOWLEDGE IN UGANDA CANCER INSTITUTE’S PEDIATRIC POPULATION
Dank K1, 2. 1University of Washington, Seattle, WA and 2Uganda Cancer Institute - Fred Hutchinson, Kampala, Uganda
Purpose of Study: Uganda Cancer Institute (UCI) is the only public cancer treatment facility in Uganda, a country with one of the highest incidences of pediatric cancer in the world. UCI’s educational materials and outreach division are limited to text-heavy materials catered to adults. Providers at UCI experience a high patient burden, limiting physician-facilitated patient education. Thus, UCI’s pediatric population receives no formal educational outreach. The creation of an image-based educational tool not only addresses this unreached audience, but also increases accessibility among the country’s 52 distinct languages.
Methods Used: A 30-page children’s book was created to address key cancer-related issues identified through conversations with patients, parents, and providers at UCI. Topics covered included a cell-level definition of cancer, symptoms, rationale for early presentation, treatment overview, stigma-reduction, and risk prevention strategies. Illustrations were designed to reflect the local context with the primary analogy revolving around cells disobeying the roadside police checkpoints, a sight ubiquitous throughout Uganda. A quiz was included to reinforce readers’ knowledge. The book is written in English and Luganda, the primary language in central Uganda. Materials were presented to 40+ UCI staff at the weekly Research in Progress meeting which included a 30-minute question period and were revised to align with feedback. Final material effectiveness was gauged by having a focus group of primary students ages 6-10 read the book aloud and reflect on what they learned.
Summary of Results: Eighteen books were printed and distributed across 5 UCI-affiliated care settings. Opportunities for self-led education are provided by books in the inpatient ward, outpatient clinic, and 3 local hostels for visiting patients and caretakers. Weekly reading programs by ward, clinic, and outreach staff provide routine formal engagement opportunities. Cancer clubs in 238 secondary schools will conduct readings at primary schools to further expand community reach. Thus far, 8 schools and 50+ secondary students have been initiated into the program.
Conclusions: The children’s book makes key cancer topics accessible to audiences as young as 6 years old. The project received widespread support from stakeholders and numerous community members requested copies of the book. The book has been adopted into UCI processes to ensure sustainable outreach. Notably, the book provides the key material necessary to support the cancer club program’s existing goal of expanding into primary schools. A partnership has been established with Soleterre, a pediatric cancer-support nonprofit in northern Uganda. They will be translating the book into Swahili and Acholi, the dominant languages in the north, to expand outreach. Further funding is being pursued for an IRB-approved study on educational efficacy, additional prints of the book, and translation into 4 additional target languages to aid expansion to UCI’s 4 satellite campuses.
# 423
Stage IV nasal dedifferentiated Leiomyosarcoma with osteosarcoma component with metastasis to cavernous sinus and lungs: a rare case report
Sahadevan S1, TRANG NC2, Mehboob A3. 1Adventist Health Bakersfield, Bakersfield, CA; 2Kern Medical Center, Bakersfield, CA and 3AIS Cancer Center/Adventist Health Bakersfield, Bakersfield, CA
Introduction: Leiomyosarcomas are rare soft tissue sarcomas compromising around only 7% of all soft tissue tumors. Nasal leiomyosarcoma is an even more uncommon mesenchymal tumor and is generally aggressive. Our case is unique in that the pathology results confirmed dedifferentiated leiomyosarcoma with a focal osteosarcoma component and very few case reports have been documented with these findings
Case report: We present an 84 yo male who initially presented with ongoing headaches for 2 months and was diagnosed with migraines. Due to worsening symptoms, imaging studies were performed which showed a nasal mass concerning for possible malignancy. This mass was excised and the pathology results were positive for dedifferentiated leiomyosarcoma with focal osteosarcoma component, leiomyosarcoma component stains positive with caldesmon and focally positive for desmin, osteosarcoma component stain strongly with SATB2 and weakly with caldesmon, tumor up to 7 cm in dimension. A follow-up PET scan was performed for staging purposes and it showed a metabolically active soft tissue lesion centered along the left cavernous sinus region measuring approximately 1.7 X 1.3 cm in axial dimension. Maximum SUV 6.3 This was concerning for possible intracranial metastatic lesion related to the patient’s previously treated nasal sarcoma. Additionally, there were several metabolically active pulmonary nodules scattered throughout the lungs and metabolically active intrathoracic lymph nodes concerning for metastatic disease. The patient was then started on radiation therapy and subsequently underwent a biopsy of the lung nodule. The pathology report of the CT-guided biopsy of the right lung showed an atypical spindle cell lesion with histomorphology and immunophenotype compatible with the patient’s previous diagnosis of leiomyosarcoma. The patient was later started on liposomal doxorubicin chemotherapy for stage 4 nasal leiomyosarcoma with metastasis to cavernous sinus and lungs.
Discussion: This case presentation is to raise awareness of the aggression of nasal leiomyosarcoma as well as emphasize the pathology findings which showed dedifferentiated Leiomyosarcoma with an osteosarcoma component. Nasal leiomyosarcomas with pathology results showing an osteosarcoma component is rare and is not well documented in the literature. These tumors are extremely aggressive and have poor outcomes. Treatment for these tumors is limited and depends on the performance status of the patients including a combination of ifosfamide and liposomal doxorubicin versus liposomal doxorubicin alone.
Infectious Diseases II
Concurrent Session
10:15 AM
Friday, January 19, 2024
# 424
WALR PROTEIN-DNA INTERACTIONS AS A NEW ANTIMICROBIAL TARGET SUGGESTED BY CHARACTERIZATION OF DNA-BINDING SITE MUTANTS
Vainshtein J, Romero M, Szurmant H. Western University of Health Sciences, Pomona, CA
Purpose of Study: With a global rise in antibiotic resistances, there has been a growing need for drugs against new therapeutic bacterial targets. One such target without any antimicrobial drugs on the market is the bacterial two-component system (TCS), employed by nearly all bacteria to adapt to new environments. A TCS of particular interest is WalRK, which is essential for viability to most Gram-positive pathogens. The kinase WalK auto-phosphorylates and subsequently activates the response regulator protein WalR via phosphoryl group transfer. While several laboratories have focused on WalK as an antimicrobial target, the purpose of this study was to determine whether WalR might be the better therapeutic target. Here the isolation and characterization of genetic variants of WalR are described, with hypothesized constitutive activation in the absence of WalK or with diminished activity, leading to cell death.
Methods Used: Site directed mutagenesis was utilized to introduce DNA-binding helix mutations R203C, R204C and E207K in the walR gene of non-pathogenic model organism Bacillus subtilis. Mutant alleles with or without the neighboring walK gene were introduced ectopically in a previously engineered strain, where wildtype walRK genes can be inducibly excised. Strains were grown to test for viability upon excision of wildtype walRK genes. Differential expression of WalR-dependent genes was tested by RT-PCR for wildtype and mutant alleles. Expression plasmids were engineered for wildtype and WalR mutant proteins and proteins were expressed and purified to homogeneity. Isothermal titration calorimetry was applied to compare DNA-binding affinities of wildtype and mutant WalR proteins to a double-stranded DNA fragment with the WalR consensus binding sequence.
Summary of Results: A total of eight B. subtilis strains were engineered. Upon excision of the native walRK-copy, growth relied on the various ectopic walR alleles with or without the presence of walK. A strain with a wildtype walR-copy required a walK copy for proper growth. However, suppressor mutants in the absence of the walK gene show up after several days, suggesting that the absence of walK is easily overcome. One such suppressor mutant is E207K, suggesting constitutive activation. The R203C mutant also partially overcomes the absence of walK. Conversely, we found that strains with the R204C mutation were not viable, whether walK was present or not. DNA-binding affinity measurements and RT-PCR assays are underway to further support these results
Conclusions: Characterization of genetic variants in the DNA-binding helix of WalR revealed opposing effects, leading either to constitutive activation, and thus no longer requiring the presence of the WalK protein or killing the activity of WalR and thus leading to cell death. These results suggest that the WalR protein is a more suitable pharmacologic target in contrast to the WalK kinase, which becomes dispensable upon WalR constitutive activation.
# 425
CHANGES IN THE ANTIVIRAL ANTIBODY REPERTOIRE ASSOCIATED WITH SUBSEQUENT HIV ACQUISITION
Lawrence V1, Dasgupta S2, Stevens-Ayers T2, Joncas-Schronce L2, Basom R2, Lama J3, Duerr A1, 2, Bender Ignacio R1, 2. 1University of Washington School of Medicine, Seattle, WA; 2Fred Hutch Cancer Center, Seattle, WA and 3IMPACTA Salud y Educacion, Lima, Peru
Purpose of Study: Systemic immune responses, have been shown to increase risk of HIV acquisition, including as shown previously in the Sabes study. Determining what factors, specifically viral infections, contribute to systemic immune profiles is an important next question. Linkage between pre-existing viral infections and HIV has not been well elucidated, outside of Herpes simplex. We set out to determine which viral exposures may be associated with HIV acquisition.
Methods Used: The Sabes study followed 2,109 HIV-negative persons in Lima, Peru with monthly blood samples to detect incident HIV acquisition. A nested study matched 90 persons with incident HIV (cases) 3:1 with those who remained negative for HIV (controls). Cryopreserved plasma was analyzed with VirScan, a systematic viral serosurvey. Changes in individual epitope “Hits” for 110 viruses, excluding HIV, between enrollment and the last HIV negative sample for cases and controls were compared with a difference-in-difference analysis by t tests using a false discovery rate of 0.10 (Benjimini-Hochberg).
Summary of Results: VirScan data were available and interpretable for 43 cases and 246 controls (n=289). Of antibody responses to 110 geographically relevant viruses, changes in epitope recognition against 10 were found to be greater in those who subsequently acquired HIV as compared to controls (Table). The change in composite epitope hits across all 8 herpesviruses was greater in cases vs. controls, as was the combined score for adenoviruses A-F. The composite mean change in the antiviral repertoire of 110 viruses was +35 epitopes in cases vs controls (p=0.014). In addition to individual adenoviruses, other viruses with significant differential responses between cases and controls included alphapapillomaviruses, a polyomavirus, and a regional alphavirus.
Conclusions: Changes in the antiviral repertoire overall and in several unique viruses was greater in people who subsequently acquired HIV than matched controls. Further work will use machine learning to combine these viral antibody signals with biomarkers of immune activation to evaluate the joint effect of viral and immunologic exposures on HIV susceptibility.
Virus
Mean epitope change
Unadjusted p value
Adjusted p value
Human adenovirus B
1.9
0.0043
0.074
Alphapapillomavirus 9
0.71
0.0031
0.068
Human metapneumovirus
0.66
0.0078
0.090
WU Polyomavirus
0.27
0.0074
0.090
Alphapapillomavirus 1
0.22
0.00090
0.056
Mayaro virus
0.15
0.0082
0.090
Composite adenovirus score
8.5
0.00037
NA
Composite human herpesvirus score
12
0.014
NA
Composite total virome score
36
0.014
NA
# 426
Integrating Multiplexing into Digital High-Resolution Melt for Rapid and Accurate Universal Cross-Kingdom Pathogen Detection in Low Volume Whole Blood Samples
Goshia T1, 2, Sinha M2, Lawrence SM3, Fraley S1. 1UCSD, La Jolla, CA; 2MelioLabs, Inc, Santa Clara, CA and 3The University of Utah, Salt Lake City, UT
Purpose of Study: Most emerging pathogen detection technologies remain follow-on tests after a blood culture yields a positive result or have narrow adoption due to limited coverage of pathogen targets, low sensitivity, and high costs. Our digital high-resolution melt (d-HRM) platform is being developed for the rapid and comprehensive identification of all common pathogens in a single test from small volume patient blood samples within three hours. By combining universal molecular chemistry in a “digital” format with machine learning, d-HRM can identify 37 pathogens without a loss in sensitivity. The current study focuses on the platform’s ability to multiplex universal primers to accurately identify fungal, viral, and bacterial pathogens with high sensitivity and low cost directly from low volume (1mL) whole blood samples in a single test.
Methods Used: Using ten relevant pathogens for neonatal sepsis as samples, our dHRM platform incorporating universal cross-kingdom primers enabled digital pathogen melt curve analysis for untargeted or hypothesis-free identification of fungal, bacterial, and viral targets in blood (
Figure 1
).
Detection of Clinically Relevant Pathogens, including Bacterial, Fungal, and Viral, in a Single Test.
Summary of Results: dHRM universal pathogen identification technology enables broad pathogen discovery, including viral [human cytomegalovirus (HCMV), herpes virus simplex (HSV)-1, and HSV-2], fungal (Candida albicans, Candida glabatra, Candida auris, Candida parapsilopsis), and bacterial (Escherichia coli, Streptococcus agalactiae, and Staphylococcus aureus). We accurately identified all ten pathogens introduced into the reaction, demonstrating efficacy of extreme multiplexing with nine of the topmost relevant pathogens for neonatal sepsis, and one emerging pathogen in C. auris.
Conclusions: dHRM is a promising diagnostic for the accurate, rapid, and low-cost detection of a range of causative pathogens in neonatal bacteremia and sepsis. This innovative platform has the capacity to quickly expand to include > 50 pathogens.
# 427
ACTIVATION INDUCED MARKER SORTING OF TREPONEMA PALLIDUM SPECIFIC CD4+ T CELLS
Culver L1, Godornes CD2, Koelle DM1, 2, Reid TB1, 2. 1University of Washington Medical School, Seattle, WA and 2University of Washington Sexually Transmitted Infectious Cooperative Research Center, Seattle, WA
Purpose of Study:Treponema pallidum (Tp), cause of syphilis, is a sexually transmitted bacteria that causes morbidity and mortality in humans. Despite effective antibiotic treatments, diagnosis methods, and public health campaigns, rates of early syphilis continue to rise. Importantly, heterosexual populations and persons with pregnancy capability are more frequently infected with corresponding increases in congenital syphilis. Recent increased prevalence highlights the need for better understanding of the human immune response to Tp infection to aid vaccine development. We propose that CD4 T cells are key to produce IFNγ to activate macrophages and support the production of antibodies, both of which are needed for opsonophagocytosis of Tp. We sought to optimize our CD4 T cell antigen discovery by adding the CD4 activation markers CD134 and CD154 to our initial activation induced marker sorting panel including CD69 and CD137 (previously vetted CD4 T cell activation markers).
Methods Used: Peripheral blood mononuclear cells (PBMC) were previously collected from three syphilis positive patients (one patient had PBMC from 2 disease course time points). After incubation with Tp antigen preparation, Tp specific CD4 T cells were identified by either CD137/69+ or CD69/134/154+ markers staining and isolated by fluorescence-activated cell sorting and expanded in vitro. Intracellular cytokine staining was performed on each resultant T-cell line (TCL) to assess Tp specificity by stimulating with sonicated Tp and measuring CD4 T-cell activation by IL-2 and IFNγ production. TCL were also probed with a library of Tp recombinant proteins to assess for protein-level specificity in a CD4 T cell proliferation assay.
Summary of Results: All four samples demonstrated expansion of Tp specific CD4 T cells when comparing the CD69/137+ TCL to ex vivo PBMC. Excitingly, one sample also demonstrated Tp-specific CD4 T cell expansion in the CD69/134/154+ TCL. This TCL was further assessed for reactivity to individual Tp proteins. Preliminary results revealed Tp0621, Tp0792, Tp0574, Tp0315, and Tp0117 as Tp CD4 T cell antigens. The CD69/134/154+ TCL had 2 identifiable CD4 T cell antigens, Tp0769 and Tp0435. The biological significance of these antigens are as follows: Tp0621 (putative surface-exposed protein), Tp0792 (flagellar protein), Tp0315 (hypothetical protein), Tp0117 (outer membrane protein), additionally Tp0574, Tp0769, and Tp0435 (lipoproteins).
Conclusions: Seven Tp antigens were identified between the two TCL, six of which have been previously categorized in literature as recombinant Tp proteins with putative immune activation. Additionally, Tp0435 would not have been identified without the addition of the CD69/134/154+ TCL indicating the utility in incorporating the CD134/154+ activation marker in future sorts. Studies to confirm these results are ongoing. Continued work to elucidate CD4+ T cell reactivity to Tp specific antigens is critical for future syphilis vaccine design to provide protection from the disease.
# 428
ROLE OF THP-1 CELLS IN CONTROLLING M. AVIUM INFECTION
Badaoui A1, Kelley M2, 3, Sasaninia KC1, 3, Mohan A1, Tiwari R1, 4, Venketaraman V1. 1Western University of Health Sciences, Pomona, CA; 2Kansas City University, Kansas City, MO; 3Western University of Health Sciences, Pomona, CA and 4Chapman University School of Pharmacy, Harry and Diane Rinker Health Science Campus, Irvine, CA
Purpose of Study: Immunocompromised individuals, such as those who suffer from HIV or Diabetes, are especially susceptible to nontuberculosis mycobacteria infections. Mycobacterium avium is an opportunistic pathogen that is acquired mainly through soil exposure and water resources, and, in an otherwise healthy individual, is easily cleared by the immune system; however, it can lead to pulmonary infections, disseminated infections, and lymphadenitis in immunocompromised individuals. In our study, we aim to study the effects of cyclic peptide [R4W4] in inducing control of M. avium infection inside THP-1 macrophages. Antimicrobial peptides (AMPs) are emerging as a novel way to combat opportunistic multidrug resistant pathogens by utilizing their unique amphipathic and cationic properties to interact with the plasma membranes of bacterial cells. In a previous study, adjunct therapies of cyclic [R4W4]–azithromycin and cyclic [R4W4]–rifampicin at specific concentrations significantly reduced M. avium survival. In this study we determined the effects of different formulations of R4W4 and antibiotics (rifampicin or azithromycin) in altering the viability of M. avium inside macrophages.
Methods Used: THP-1 cells were grown, then treated with a 10 ng/ml solution of phorbol 12-myristate 13-acetate (PMA) allowing cells to differentiate into macrophages prior to Day 0. THP-1 cells were infected with M. avium at a ratio of 1:1 and treated with different concentration of free forms of R4W4 and antibiotics (rifampicin or azithromycin) and liposomal formulations of R4W4 and antibiotics (conjugated or non-conjugated). Macrophages were terminated on days 0, 4, & 8 while treatments were added at 3h, 3d, & 7d post infection and treatment. Macrophage lysates were then plated and incubated for 11 days for M. avium colonies.
Summary of Results: At 3 hours post-infection on Day 0, Cyclic Peptide [R4W4] was able to reduce the viability of M. avium in a dose-dependent manner, with 8 microg/ml being the most efficacious. At 4 days post-infection, Cyclic Peptide [R4W4] at all 3 concentrations was able to reduce the viability of M. avium by over half when compared to an untreated control. At 8 days post-infection, Cyclic Peptide [R4W4] had colony counts greater than the untreated control category and showed no efficacy against M. avium. Treatment of M. avium-infected macrophages with liposomal formulations containing unconjugated R4W4+rifampicin or R4W4+azithromycin resulted in a significant reduction in the intracellular bacterial burden when compared to treatment with liposomes containing either lone rifampicin or azithromycin.
Conclusions: A significant reduction in the intracellular viability of M. avium was observed when THP-1 cells were treated with liposomal formulations containing unconjugated R4W4+rifampicin and unconjugated R4W4+azithromycin. In conclusion, unconjugated R4W4 is a promising adjuvant to increase M. avium susceptibility to known antibiotics.
# 429
HEPATITIS C CARE CONTINUUM AMONG PEOPLE WHO INJECT DRUGS IN KING COUNTY, WA
Ebersberger J1, Tsui JI2, Corcorran M3, Glick S2. 1University of Washington School of Medicine, Seattle, WA; 2University of Washington School of Medicine, Seattle, WA and 3University of Washington School of Medicine, Seattle, WA
Purpose of Study: Hepatitis C virus (HCV) is a major cause of morbidity and mortality despite the availability of direct acting antiviral (DAA) medications for nearly a decade. Injection drug use is the most common risk factor for HCV, and prior research has found that many people who inject drugs (PWID) remain untreated for HCV infection. This study aims to update the HCV continuum of care and characterize the current prevalence of HCV among Seattle-area PWID. We hypothesized that the percent of PWID with HCV who had been treated for HCV would be higher in 2022 compared to 2018.
Methods Used: This study analyzed data from the 2022 Seattle-area National HIV Behavioral Surveillance (NHBS) survey of PWID, which is part of a CDC-funded multisite survey of populations at risk for HIV. Participants were recruited using respondent-driven sampling and completed both a primary and local survey focused on prior HCV testing, diagnosis, and treatment. All participants were offered HCV antibody rapid testing and HCV RNA laboratory testing to differentiate active HCV infection from prior infection. Among those who screened HCV antibody positive, we calculated proportions for steps along the HCV care continuum, including proportions of PWID who self-reported prior HCV diagnosis, treatment, and cure.
Summary of Results: The sample included 500 PWID, 303 (61%) of whom tested positive for antibodies to HCV. Just over one-half (54%, 272/500) of our sample received HCV RNA testing, and 21% (57/272) had evidence of current HCV infection. Among those who were HCV antibody positive, 92% reported any prior HCV test, and 71% reported a prior HCV diagnosis by a doctor or nurse. Of those ever told by a health care provider that they had HCV, 49% had received treatment and 35% reported being cured. When comparing 2022 Seattle-area NHBS-PWID survey data to a similar analysis using 2018 data, there was a 23 percentage-point increase in the proportion of PWID with HCV who had been treated as well as a 17 percentage-point increase in the proportion of PWID with HCV who reported being cured (figure 1).
Conclusions: Between 2018 and 2022, the proportion of PWID with HCV in the Seattle-area who were treated and cured nearly doubled. Nevertheless, approximately one-in-five PWID are currently viremic and in need of HCV treatment. To reach those still in need of treatment, researchers, clinicians, and policymakers must continue to develop and implement novel HCV treatment interventions and reduce barriers in accessing treatment.
# 430
CHARACTERISTICS OF PEDIATRIC COVID-19 INFECTIONS IN HAWAI’I
Tadaki S1, Len K1, 2, Siu A1, Kimata C1, Kosut J1, 2. 1Hawai’i Pacific Health, Honolulu, HI and 2University of Hawai’i John A. Burns School of Medicine, Honolulu, HI
Purpose of Study: The pandemic novel coronavirus disease 2019 (COVID-19) has been the subject of research globally since its identification at the end of December 2019. In Hawai’i, data between March 1, 2020 and February 28, 2021, revealed that the Pacific Islander community, which comprises 5% of the state’s population, disproportionately accounted for 22% of Hawai’i’s COVID-19 cases and deaths. These early statistics were primarily reflective of adult patients as the adult population was affected earlier in the pandemic. However, recent data shows a significant increase in pediatric cases. According to the American Academy of Pediatrics, pediatric cases now account for 17.9% of all cases since the onset of the pandemic. Data specific to the pediatric Hawai’i population has not been studied. This study aims to investigate hospitalized pediatric COVID-19 patients in Hawai’i’s only tertiary pediatric hospital, focusing on the unique characteristics of this population.
Methods Used: A retrospective chart review of children ages 0-18 years presenting to Hawai’i Pacific Health facilities with a final diagnosis of COVID-19 between April 2020 and June 2023 was conducted. Descriptive statistics were employed to describe the inpatient pediatric COVID-19 population. Univariate analysis and multivariable logistic regression were used to compare groups.
Summary of Results: Of the 307 COVID-19 encounters, 61.2% were male (n=188), 48.7% were Native Hawaiian or Pacific Islander (n=150) and the average length of stay was 5.8 days. The top 3 primary reasons for hospitalization were respiratory (45.3%), neurologic (14.0%), and gastrointestinal (12.7%). Males (p=0.0002), Native Hawaiians or Pacific Islanders (p<0.0001), and those with government insurance (p<0.0001) were more likely to be admitted to the hospital when compared to Hawai’i’s general pediatric population (see Table 1). Geographically, higher case concentrations were found in specific zip codes on Oahu, including Waianae, Waialua, metropolitan Honolulu, and Kaneohe. Of the pediatric hospitalized cases with COVID-19, 43.3% of patients had 0 comorbidities, 24.8% had 1 comorbidity, and 31.9% had 2 or more comorbidities.
Conclusions: This study reveals distinct patterns that could guide targeted interventions for pediatric patients with COVID-19 in Hawai’i. Certain groups such as males and Native Hawaiians or Pacific Islanders, as well as those with government insurance were more likely to be hospitalized, with particular geographic areas in Hawai’i exhibiting higher concentrations of cases. Understanding the characteristics of patients with COVID-19 can allow healthcare providers to intervene sooner with the appropriate therapeutics, potentially improving health outcomes for pediatric COVID-19 patients in Hawai’i.
Demographic comparison with Hawai’i’s general pediatric population.
Study Population
Hawai’i Population
p-value
Gender
Female
38.8
49.5
0.0002
Male
61.2
50.5
0.0002
Insurance Type
Government
73.6
45.8
<0.0001
Commercial
24.8
52.0
<0.0001
Other
1.6
2.3
0.4134
Primary Race
Native Hawaiian or Pacific Islander
48.7
13.8
<0.0000
Asian
31.6
49.4
<0.0001
White
15.6
33.4
<0.0002
Other
3.9
3.5
0.7031
General pediatric population data from Hawai’i’s Department of Business, Economic Development, and Tourism was used.
Shomento S1, Borgogna T2, Voyich J2. 1UW School of Medicine, Bozeman, MT and 2Montana State University, Bozeman, MT
Purpose of Study: Bacterial superinfections following influenza are especially precarious. These superinfections carry mortality rates 11-15 times higher than influenza alone. Staphylococcus aureus (S. aureus) can cause secondary pneumonia infections following influenza A virus (IAV). This species colonizes the nares of about 50% of the population and regularly contacts the lung environment via aspiration, yet seldom acts as a primary agent of community-acquired pneumonia (Borgogna, 2018).
It is hypothesized that S. aureus senses the vulnerable, post-IAV environment using its two-component gene regulatory system, SaeR/S, which responds by transcribing virulence genes critical to survival, neutrophil evasion, and tissue destruction (Borgogna, 2018 and Collins, 2020). In addition, previous research shows that IAV alters the composition of surfactant components, including the major lipid dipalmitoylphosphatidylcholine (Woods, 2016).
This study investigates the hypothesis that palmitate, a component of healthy surfactant, suppresses SaeR/S controlled virulent gene expression. Secondly, we explore if one commercially available surfactant, Infasurf®, does the same.
Methods Used: After harvesting S. aureus (USA300 strain LAC) at mid-exponential growth, cultures incubated for 1 hour at 37°C in the treatment. For the palmitate exploration, conditions included: DPBS, neutrophils (PMNs), 180 µM palmitate, and 18µM palmitate. For the second aim, conditions included: DPBS, PMNs, and 1% Infasurf®. RNA was extracted using a Qiagen kit and levels of transcription were measured using TaqMan qRT-PCR on targets: hla, hlgA, lukF, fakA, and essC. Transcripts were normalized to gyrB expression and calibrated to the DPBS condition to calculate log fold-change. A one-way ANOVA test with Tukey’s posttest determined significance. Three separate experiments were done for both aims.
Summary of Results: Data demonstrate that palmitate significantly suppresses the alpha-hemolysin (hla) gene, an SaeR/S modulated gene. This gene has been linked to pathogenesis in S. aureus lung infection (Bubeck, 2007). Palmitate caused statistically significant repression (-0.685 log-fold difference to DPBS, P<0.0049). While not statistically significant, hlgA was suppressed and essC, which is negatively regulated by SaeR/S, was increased in the palmitate treatment. Infasurf® did not show significant suppression among the probes tested.
Conclusions: The treatment of S. aureus with palmitate demonstrates a decrease in hla toxin expression. Because palmitate is a component of healthy surfactant, this data could explain why S. aureus is not a primary agent of community-acquired pneumonia. Instead, the pathogen strikes the post-IAV lung environment when surfactant has been disrupted. S. aureus treated with Infasurf ® does not decrease expression of the tested probes. Future work could include characterizing the components of commercially available surfactant and challenging S. aureus with other surfactant components to determine if those decrease toxin expression.
# 432
The Role of Jail Testing in the Public Health Response to Syphilis in King County, Washington
Buck T1, Herrera Perales L2, Berzkalns A2, Barash E2, Golden MR3, 4, Dombrowski JC3, 4. 1University of Washington School of Medicine, Seattle, WA; 2Department of Public Health - Seattle & King County, Seattle, WA; 3University of Washington, Seattle, WA and 4University of Washington, Seattle, WA
Purpose of Study: The incidence of syphilis in the U.S. has sharply increased over the last decade, particularly among heterosexual cisgender men and women, leading to a resurgence of congenital syphilis. In King County, Washington, the epidemic is disproportionately among people who are living homeless and people who use methamphetamine or inject drugs. The county health department implemented a jail testing program to improve screening outside of the healthcare system. The goal of this analysis was to evaluate the outcomes of the testing program.
Methods Used: Public Health Disease Intervention Specialists (DIS) conducted voluntary, opt-in syphilis testing four days per week in the South Correctional Entity (SCORE) Jail. This retrospective cohort study included all individuals who participated in the program during January 2022 - March 2023. Initial testing included a rapid (treponemal specific) test and our protocol was to empirically treat persons with a positive rapid test while awaiting confirmatory results from laboratory testing (treponemal EIA and RPR). DIS worked with medical providers at SCORE to coordinate confirmatory testing and treatment and made a final determination of syphilis diagnosis and stage through review of past test results and patient-reported symptoms. DIS conducted brief interviews to obtain demographic and risk factor data, including gender of sex partners, housing status, and limited substance use history. We categorized persons with positive rapid test results into confirmed, probable, possible, or no new case. We calculated test positivity; evaluated treatment initiation and completion; and compared characteristics of patients with confirmed syphilis to characteristics of all syphilis cases identified in King County during the same period using Pearson’s chi-squared test (statistical significance at a p-value of <0.05).
Summary of Results: 1,371 individuals opted into syphilis testing; 69 (5%) of whom had positive rapid results. 51 had confirmatory testing, which resulted in 33 confirmed new syphilis cases (prevalence of confirmed new syphilis = 2.4%). Of the 33 confirmed new cases, 29 (88%) initiated treatment and 18 (55%) completed treatment. Compared to all King County syphilis cases, persons diagnosed at SCORE were more often cisgender women (30% vs. 22%) or cisgender men with only women sex partners (67% vs. 21%) and more likely to report homelessness or unstable housing (67% vs. 24%), injection drug use (21% vs 5%), and methamphetamine use (91% vs. 20%) (p<0.001 for all comparisons). The proportions who reported exchanging sex for drugs or money were not statistically different (9% vs. 4%; p<0.18).
Conclusions: The SCORE jail testing program identified syphilis cases in high priority populations and captured a different demographic than that identified by syphilis testing in King County overall. The treatment outcomes emphasize the need for timely access to syphilis testing and treatment in the jail setting.
Morphogenesis and Malformations
Concurrent Session
10:15 AM
Friday, January 19, 2024
# 433
A PROMOTOR VARIANT IN WNT9B IS A CANDIDATE IN A CASE WITH FEMORAL FACIAL SYNDROME
Rope A1, Marvin C2, Chong J2, Buckingham K2, Shively k2, Bamshad M2. 1Genome Medical, South San Francisco, CA and 2University of Washington, Seattle, WA
Case Report: Femoral-Facial syndrome (FFS), also known as Femoral Hypoplasia-Unusual Facies syndrome (FHUFS), is a rare disorder currently characterized as an unsolved multiple malformation syndrome. The cardinal features include femoral hypoplasia and distinctive facial findings: upward-slanting palpebral fissures, a short nose with broad tip, a long philtrum, a thin vermillion border of the upper lip and micrognathia with or without cleft palate. (OMIM: 134780). The condition was probably first reported in 1961 by Franz & O’Rahilly, and formally delineated by Daentl et al. in 1975. To date, more than 100 individuals have been described in the literature as having the diagnosis, though their inclusion could be viewed as somewhat generous in some cases.
Though the precise etiology and mechanism of the condition remains a mystery, one of the intriguing observations is the frequent co-association of maternal diabetes (insulin-dependent, type 2 and gestational) with the overlapping features of caudal dysgenesis and pharyngeal arch anomalies. The overwhelming majority of cases have been sporadic, with only a single, well-characterized report of vertical transmission between a father and daughter. Consanguinity has been suggested as a possible factor in only two cases. Dizygotic twins of a diabetic mother were discordant for the diagnosis, as were monozygotic twins of a non-diabetic mother. One case has been possibly attributed to a duplication/deletion of chromosome 2q37.
We report a child with clinical features consistent with FFS presenting with bilateral femoral aplasia, cleft palate, micrognathia, talipes equinovarus, ventriculomegaly, absent septum pellucidum, and genitourinary abnormalities requiring right orchiectomy and left orchiopexy.
Short read genome sequencing of the proband identified a non-maternally inherited heterozygous c.-2C>G variant in the 5’UTR promoter of WNT9B. This variant is predicted to be damaging (CADD 18) and is not present in gnomADv2.1.1, gnomADv3.1.2, or TOPMed freeze 8. WNT9B is expressed in mouse craniofacial and hindlimb bud tissue. Homozygous variants in WNT9B have been reported in two consanguineous families to underlie renal agenesis and hypoplasia with reproductive tract abnormalities but to date no condition is known to result from heterozygous pathogenic variants in WNT9B.
The WNT family of genes encode highly conserved secreted signaling proteins expressed in embryonic and adult tissues. During embryonic development these genes regulate cell growth and differentiation through a canonical WNT/β-catenin pathway and non-canonical pathways without β-catenin. Pathogenic germline variants in WNT genes underlie a range of congenital disorders affecting the skeleton, limbs, genitourinary system, integument, dentition, and face. Expression studies are planned to confirm the pathogenicity of this variant in WNT9B and the mechanism by which it may result in FFS.
# 434
PALLISTER-HALL SYNDROME: A SEVERE NEONATAL TALE STEMMING FROM AN UNEXPECTED MOSAIC TRAIL
Ramos JP2, Schymick J1, Calvert P1, Matalon DR2. 1Santa Clara Valley Medical Center, San Jose, CA and 2Stanford University, Palo Alto, CA
Purpose of Study: Pallister Hall syndrome (PHS) is a rare autosomal dominant (AD) disorder due to pathogenic variants in GLI3 with range of congenital anomalies such as bifid epiglottis, mesoaxial or postaxial polydactyly, hypothalamic hamartoma (HH), genitourinary anomalies, and panhypopituitarism. High perinatal mortality is associated with PHS particularly when HH, panhypopituitarism, or severe anomalies (e.g. imperforate anus, laryngotracheal cleft) are present; however, the syndrome exhibits significant inter-individual variability. Pathogenic GLI3 variants are associated with other disorders including Greig-Cephalopolysyndactyly syndrome (GCPS), isolated polysyndactyly (IPD), and nonsyndromic HH. The same pathogenic GLI3 variants may cause GCPS or IPD but not PHS and brain-restricted somatic mosaicism is often found in nonsyndromic HH. Here we present a severely affected neonate with classic features of PHS found to be inherited from a mother with postaxial polydactyly of bilateral hands and feet and mosaic for the pathogenic GLI3 variant in blood. This represents the first confirmed case of inherited severe PHS from a mother with IPD due to a mosaic truncating pathogenic GLI3 variant.
Methods Used: The study employed chart review, physical examination, clinical genome sequencing, and literature analysis.
Summary of Results: A 2-month-old male, born at term, was prenatally diagnosed with cleft lip and palate, ambiguous genitalia, foot webbing, small kidneys, and shortened long bones. Prenatal microarray was negative. Postnatally, bilateral cleft lip and palate with bifid epiglottis, type II laryngeal cleft with submucous extension, subglottic narrowing, tracheomalacia, imperforate anus, hypothalamic hamartoma (HH) causing brainstem compression, panhypopituitarism, moderate atrial septal defect, ambiguous genitalia with prominent labioscrotal tissue with potential microphallic structure, ptosis, exotropia, oligodactyly, hypoplastic nails, and mesoaxial polydactyly were identified. Genetic analysis through genome sequencing showed a heterozygous pathogenic variant [NM_000168.5: c.2977 C>T (p.Gln993Ter)] in the GLI3 gene, consistent with PHS. Notably, the mildly affected mother was found to have the GLI3 pathogenic variant in approximately 15.5% of sequencing reads of blood derived DNA. Mother reports bilateral polydactyly of hands and feet and normal brain MRI. A clinical genetics evaluation is planned for her.
Conclusions: This is the first confirmed report of severe PHS inherited from a parent with history of IPD and a mosaic, truncating, GLI3 variant identified in blood. It is also the first report of an individual found to have blood-based somatic mosaicism with a relatively high variant allele fraction of a truncating variant known to cause a severe PHS phenotype. Overall, this case expands the spectrum of IPD and PHS genotype-phenotype correlation highlighting the importance of mosaicism detection and how prenatal counseling should be carefully performed for patients with IPD.
# 435
MYRF-RELATED CARDIAC-UROGENITAL SYNDROME
CASE REPORT AND REVIEW OF LITERATURE
Gomes A, Bird LM. UCSD, San Diego, CA
Case Report: MYRF-related cardiac-urogenital syndrome (MYRF-CUGS) is a recently described disorder caused by heterozygous mutations in the gene encoding the transcription factor Myelin Regulatory Factor (MYRF). CUGS is characterized by anomalies of the internal and external genitalia, heart, and eyes. In the nervous system, MYRF is necessary for oligodendrocyte differentiation and the expression of myelin-related genes. Recent evidence indicates that MYRF plays an essential role in the progenitor cells of the developing heart, lungs, diaphragm, and genitourinary tract. Less than 25 patients have been reported in the literature thus far, and the reported phenotypes consist of a combination of heart, lung, diaphragm, and genital and ophthalmic malformations. The clinical presentation overlaps with Meacham syndrome 4, Scimitar syndrome, and PAGOD syndrome 5.
We report on a 3-year-old child with a complex medical history, including congenital diaphragmatic hernia, ambiguous genitalia and hypospadias, anomalous circumflex coronary artery originating from the pulmonary artery, atrial septal defect, right ventricular enlargement, Wolff-Parkinson-White conduction abnormality, oral aversion, global developmental delays, concern for autism and high hyperopia.
As a newborn, chromosomal microarray revealed XY sex chromosomal constitution and no copy number variants. Rapid whole genome sequencing (WGS) was nondiagnostic. In 2022, a disorder of sexual development gene panel found a heterozygous c.1116-2A>G likely pathogenic variant in MYRF, affecting the canonical splice acceptor site of intron 7 and predicted to result in loss of normal protein function through either protein truncation or nonsense-mediated mRNA decay. Targeted re-analysis of the WGS showed the MYRF variant was present and de novo and classified as pathogenic. It had not been called on the initial analysis because the gene was first described as a cause of human disease earlier in the same year (2018).
We report the features of a child with a novel de novo pathogenic variant in MYRF and summarize the clinical features of published cases of MYRF-CUGS. This case illustrates the value in re-analysis of negative WGS when a genetic disorder is strongly suspected.
# 436
FRAGILE X SYNDROME DUE TO A RARE FMR1 SEQUENCE VARIANT
Keehan L1, Hale C2, Fisk DG2, Dykzeul N3, Scott SA2, 4, Tise CG1. 1Stanford University, Stanford, CA; 2Clinical Genomics Laboratory, Palo Alto, CA; 3Stanford Medicine Children’s Health, Palo Alto, CA and 4Stanford University, Stanford, CA
Purpose of Study: Fragile X syndrome (FXS) is an X-linked disorder characterized by developmental delay (DD), intellectual disability, characteristic facial features, and behavioral differences including ADHD, autism spectrum disorder (ASD), and anxiety. Over 99% of FXS cases are caused by pathogenic CGG triplet repeat expansions (TRE) in the 5’ untranslated region of the FMR1 gene, resulting in FMR1 promoter methylation and transcriptional silencing. However, recent case reports have described rare pathogenic FMR1 sequence variants in a small subset of patients with FXS. We describe the diagnostic journey of a male proband with ASD and neurodevelopmental concerns who was ultimately found to harbor a likely pathogenic three nucleotide deletion in the coding region of FRM1, consistent with a diagnosis of FXS.
Methods Used: Clinical genome-based exome sequencing (55.8X) was performed on DNA isolated from proband and parental blood specimens. Phenotypic data was collected from clinical evaluation and medical records.
Summary of Results: An 11-year-old male with ASD and neurodevelopmental concerns, including dyspraxia, executive functioning difficulties, and full-scale intelligence quotient of 76 (~5th percentile) was evaluated by Medical Genetics and noted to have non-dysmorphic features and two posterior hair whorls. Prior nondiagnostic evaluation included FXS TRE testing (32 CGG repeats), chromosomal microarray, and biochemical testing. After multiple insurance denials, trio exome sequencing was eventually approved and detected a maternally inherited, hemizygous, likely pathogenic, three nucleotide deletion in exon 15 of FMR1 (NM_002024.5:c.1599_1601del, p.Arg534del). This variant is absent from large population databases and eliminates an evolutionarily conserved arginine within the RGG box domain of the FMRP protein, which is involved in binding RNA transcripts for intracellular transport.
Conclusions: There is growing evidence underscoring the importance of FMR1 sequence variants as a rare cause of FXS, likely due to disruption of important regulatory or functional FMRP domains. While pathogenic FMR1 sequence variants can have phenotypic overlap with classical FXS, the associated testing modality and subsequent genetic counseling are considerably different. This case demonstrates the importance of sequence analysis of FMR1 in the diagnostic workup of individuals with ASD and the need for further research into the genotype-phenotype spectrum of rare FMR1 sequence variants.
# 437
MULTIPLE CONGENITAL ANOMALIES AND GENOTYPE-PHENOTYPE CORRELATIONS IN KAT6A SYNDROME: A CASE REPORT AND REVIEW OF THE LITERATURE
Calvert P1, Van Andel M1, Keehan L2, Matalon DR2, Schymick J1. 1Santa Clara Valley Medical Center, San Jose, CA and 2Stanford University, Stanford, CA
Purpose of Study: Heterozygous pathogenic variants in the KAT6A gene (lysine acetyltransferase 6A) have been identified as causing an autosomal dominant syndromic neurodevelopmental disorder known as KAT6A syndrome or Arboleda-Tham syndrome. The KAT6A gene codes for a lysine acetyltransferase enzyme that regulates gene expression by altering chromatin structure through histone acetylation. Late-truncating variants have been proposed to cause a more severe neurodevelopmental phenotype (Newbury-Ecob et al, 2019). Since this syndrome was reported in 2015, less than 100 individuals have been reported in the literature to date. KAT6A syndrome is typically characterized by intellectual disability, speech delay, microcephaly, cardiac anomalies, and gastrointestinal complications, although rare cases with multiple congenital anomalies have been described (Arboleda et al., 2015, Tham et al., 2015). Here we present a case with a unique phenotype including craniosynostosis, Chiari I malformation, and imperforate anus, not previously described. Furthermore, we evaluate genotype-phenotype correlations, and summarize the multiple congenital anomalies seen in this syndrome.
Methods Used: Chart review, clinical exam, whole exome sequencing and literature review.
Summary of Results: We present an 8-month-old male with multiple congenital anomalies including Chiari I malformation, sagittal craniosynostosis, imperforate anus, a large secundum ASD, cryptorchidism, inguinal hernia, rocker bottom feet, and dysmorphic facial features. His clinical course was complicated by the identification of low-lying cerebellar tonsils and acquired hydrocephalus concerning for tonsillar herniation necessitating an emergent ventriculoperitoneal shunt. He underwent whole exome sequencing and was found to have a novel likely pathogenic truncating variant in the KAT6A gene c.3562_3565dup, p.I1189Sfs*3.
Conclusions: In this study we present a severe KAT6A syndrome phenotype with multiple congenital anomalies due to a novel late-truncating variant located in the exon 17 of the KAT6A gene. We report the first case of imperforate anus, further expanding the gastrointestinal phenotype of this condition. In addition, we review the literature evidence correlating pathogenic late-truncating variants, including those located in exon 17, and a more severe clinical phenotype associated with multiple congenital anomalies including craniosynostosis and Chiari I malformation. Beyond the neurodevelopmental phenotype, this study highlights the importance of recognizing KAT6A syndrome and its associated life-threatening intracranial anomalies.
# 438
A RARE SYNDROME NOW PRENATALLY SEEN, DUE TO VARIANTS IN THE DPH1 GENE
Dunn E1, Smith CM2, Matalon DR1. 1Stanford University, Palo Alto, CA and 2Stanford Medicine: Children’s Health, Palo Alto, CA
Purpose of Study: Pathogenic variants in DPH1 are associated with a rare disorder: autosomal recessive developmental delay, short stature, dysmorphic facial features and sparse hair-1 (DEDSSH1; MIM# 616901). Limited prenatal findings have been published in association with this condition. The purpose of this case series of two unrelated patients is to describe the prenatal imaging findings and better delineate the prenatal and postnatal phenotype of DEDSSH1.
Methods Used: Medical literature and chart review, clinical physical examination and laboratory testing.
Summary of Results: Patient one had a prenatal presentation notable for a female fetus with growth restriction and MRI showing absence of the right globus, brachycephaly, ventricular septal defect (VSD), striking cerebellar vermian hypoplasia, clenched hands and hepatomegaly. Prenatal trio exome sequencing showed a homozygous, likely pathogenic variant in DPH1 NM_001383.4 (c.374T>C, p. Leu125Pro). Pregnancy termination was elected at 23 weeks. Patient two was a female born at 36 weeks via vaginal delivery. Prenatally, MRI showed VSD, hypotelorism, dolichocephaly, ventriculomegaly, and cerebellar vermian hypoplasia. Postnatally, metopic craniosynostosis, camptodactyly of the hands, and postaxial polydactyly of the left foot were noted, and she had severe respiratory distress requiring support. Trio genome sequencing showed a homozygous, likely pathogenic variant in DPH1 NM_001383.4 (c.374T>C p. Leu125Pro). She died of cardiac arrest at the age of 8 months.
Fewer than 20 cases of DEDSSH1 and less than ten missense variants have been published. The postnatal phenotype reported in the majority of these patients is consistent with this case series including brain malformations (commonly cerebellar vermian hypoplasia), skull differences, short stature, congenital heart disease, and hand/foot anomalies.
Conclusions: This case series presents two unrelated females with cerebellar vermian hypoplasia, congenital heart disease, fetal growth restriction, abnormalities of the skull, and minor anomalies of the hands/feet identified prenatally. Although no distinct prenatal phenotype has been described, these cases demonstrate that the prenatal findings correlate well with postnatal phenotype and are consistent with the previously reported postnatal cases of DEDSSH1. Thus, variants in DPH1 should be considered in patients with fetal growth restriction and multiple anomalies that include cerebellar anomalies. Overall, this case series expands the prenatal phenotype associated with pathogenic variants in DPH1.
# 439
DIFFERENTIAL DNA METHYLATION DRIVES ALLELIC EXPRESSION FOR IMPRINTED GRB10-DDC LOCUS IN THE DEVELOPING HEART
Juan A1, 2, Foong Y1, Thorvaldsen J1, Rosier C1, Krapp C1, Bartolomei M1. 1University of Pennsylvania, Philadelphia, PA and 2Stanford University, Palo Alto, CA
Purpose of Study: Imprinted genes are a unique subset of ~200 highly conserved genes that are expressed in a monoallelic, parent-of-origin specific manner. Although imprinted genes employ gametic differentially methylated regions known as imprinting control regions (ICRs) to regulate gene expression, the role of secondary differentially methylated regions (DMRs) that arise post-implantation are poorly understood. Here, we use the reciprocally imprinted Grb10-Ddc locus (maternal Grb10 suppresses growth, paternal Ddc stimulates heart development), a genomic region implicated in the imprinting disorder Silver-Russell syndrome, as a paradigm for how DNA methylation at secondary DMRs contributes to genomic architecture and mediates monoallelic gene expression.
Methods Used: We focus on a secondary DMR that functions as an insulator (CRB2.3) within the mouse Grb10 gene body that is orthologous in humans. CBR2.3 was previously identified as a novel regulatory element using allele-specific chromatin conformation technology (Juan et al., 2022). Here we used in vivo genetic mouse models (methyl-cytosine dioxigenase Tet1 KO and DNA maintenance methyltransferase Dnmt1 KO) that demonstrate DNA hyper- and hypomethylation at CBR2.3, respectively. Allele-specific bisulfite sequencing and quantitative RT-PCR revealed how aberrations in DNA methylation at CBR2.3 affect Grb10/Ddc expression in different tissues. Statistical analyses were performed using Prism9 GraphPad Software. Unpaired two-tailed t tests and ordinary one-way analysis of variance (ANOVA) followed by Tukey’s multiple comparison post-hoc test was used.
Summary of Results: Paternal Tet1 KO offspring exhibited paternal-specific hypermethylation at CBR2.3 (~5% in WT vs 70% in Tet+/-). These offspring adopted a maternal-like expression phenotype, illustrated by loss of Ddc 1a and activation of the normally silent paternal Grb10 1a promoter in heart and muscle tissues, recapitulating the previously published paternal CBR2.3 deletion (Juan et al., 2022). In contrast, E7.5 Dnmt1-/- embryos were ~5% methylated at CBR2.3 (compared to 50% in WT) and exhibited a paternal-like expression phenotype with increased Ddc 1a and loss of Grb10 1a expression.
Conclusions: Together, our results indicate that imprinted Grb10-Ddc expression depends on differential DNA methylation at a secondary DMR, CBR2.3 – a property previously thought to be unique to ICRs. The maternal-specific DNA methylation and paternal-specific DNA hypomethylation pattern at CBR2.3 contributes to the assembly of the architecture that restricts enhancer activity to target Grb10-Ddc promoters on each parental allele. Our work highlights that allele- and tissue-specific topology are not strictly required to be inherited by the germline like traditional imprinted loci. Given the genetic diversity and allelic skewing of many developmental and disease-related genes, we assert that this elegant regulatory framework is more prevalent in the genome than previously thought.
Neonatology General IV
Concurrent Session
10:15 AM
Friday, January 19, 2024
# 440
NEURODEVELOPMENTAL OUTCOMES IN INFANTS EXPOSED TO MATERNAL COVID-19 DURING PREGNANCY
Fajardo VM1, Ferreira F3, Fuller T2, Cambou M1, Mohole J1, Kerin T1, Paiola S1, Rao R1, Zhang D4, Marschik P4, Iyer S1, Kesavan K1, Britto J5, Moreira M5, Brasil P5, Nielsen-Saines K1. 1David Geffen UCLA School of Medicine, Los Angeles, CA; 2UCLA Institute for the Environment and Sustainability, Los Angeles, CA; 3Universidade do Rio de Janeiro, Rio De Janeiro, , Brazil; 4Heidelberg University Hospital, Heidelberg, Germany and 5Fundacao Oswaldo Cruz (Fiocruz), Rio De Janeiro, Brazil
Purpose of Study: Immune activation during pregnancy is associated with potential neurodevelopmental repercussions. Although vertical transmission of SARS CoV-2 is rare, the virus causes maternal immune activation. We evaluated neurodevelopmental outcomes in a cohort of infants exposed to maternal COVID-19.
Methods Used: Pregnant women with a positive SARS CoV-2 PCR result were enrolled in Los Angeles (LA), and Rio de Janeiro, Brazil, from 4/2020 to 8/2022 and followed prospectively. Infant neurodevelopment was evaluated by Ages and Stages Questionnaires (ASQ-3) and Bayley-3 Scales of Infant and Toddler Development for cognitive, language and motor domains, over time. Bayley-3 results were compared to that of pre-pandemic children of comparable age from the same institutions. Potential associations with maternal/birth parameters and COVID-19 severity and timing were explored. Risk factors (RF) for at risk of delay (<-1 to -2SD) and developmental delay (DD, <-2SD) were evaluated by logistic regression.
Summary of Results: 300 children (6-38 mo) were evaluated;none were infected at birth.Bayley-3s were evaluated in 53 exposed LA children 50 pre-pandemic LA controls 75 exposed Rio children and 78 pre-pandemic Rio controls ASQ-3s were evaluated in 44 additional exposed LA children. Median Bayley-3 scores for cognitive, language and motor domains in cases and controls respectively were 100 and 98, p=0.8, 83 and 89, p=0.01 and 97 and 94, p=0.21 in Rio and 110 and 120, p<0.001, 103 and 106, p=0.15 and 107 and 110, p=0.31 in LA. 12% and 6% of children in Rio and LA scored a -2SD on Bayley-3 (DD) compared to 3% and 0% of control children in Rio (p=0.029) and LA (p=0.24), (Figure). Language delay was the most affected domain driving lower scores.. More mothers had severe/critical COVID-19 in Rio (35%) as opposed to LA (9%), p<0.001 with more mothers vaccinated prior to infection in LA (30%) versus none in Rio (p<0.001). One RF for DD (<-2SD) in LA was maternal age >40 years [OR:8.2, 95%CI:1.5-43.7]. In Rio no RF were identified for DD. RF for below average performance (<-1SD and <-2SD) were prematurity [OR:4.2, 95%CI:1.2-14.5) and severe/critical COVID-19 [OR:5.5, 95%CI:1-29.3] in LA. Prematurity was a RF for below average performance at both sites [OR:2.6, 95%CI:1.1-6.4].
Conclusions: As compared to controls, children exposed to maternal COVID-19 in utero had a higher frequency of DD with no other RF identified beyond maternal COVID-19. Below average performance was associated with prematurity. Children exposed to COVID-19 in utero need long-term neurodevelopmental follow-up.
# 441
Clinical characteristics of neonates born less than 32 weeks gestational age to mothers with mental illness in an urban neonatal intensive care unit
Alag A1, Chang MA2, 1, Barton L1, 2, Ramanathan R1, 2, Biniwale M1, 2. 1University of Southern California, Los Angeles, CA and 2Los Angeles General Medical Center, Los Angeles, CA
Purpose of Study: Studies have shown that maternal psychiatric illness negatively affects neonatal outcomes, including increased risk for preterm birth and poor fetal growth. Less is known about neonatal outcomes among very preterm infants born to mothers with mental illness. Our objective was to evaluate maternal characteristics and outcomes of very preterm infants born to mothers with psychiatric conditions.
Methods Used: We conducted a retrospective review of neonates <32 weeks gestational age (GA) admitted to an urban and underserved Level III NICU between 2017-2022. Maternal psychiatric illnesses were identified through physician documented diagnoses and maternal self-report in behavioral health and social work evaluations.
Summary of Results: A total of 231 neonates were identified, with 70/231 (30%) born to mothers with documented psychiatric illness history and 161/231 (70%) without a psychiatric diagnosis. Of the identified mothers with psychiatric history, 90% had a mood disorder diagnosis and 5.7% were diagnosed with both mood disorders and schizophrenia (Table). Predictors of maternal mental illness included single mothers, housing insecurity, and lower educational attainment. Maternal self-identified race, inadequate prenatal care, low-income status, and unemployment were not significantly different. Maternal psychiatric history was associated with HIV diagnosis but not other medical comorbidities, such as hypertension, diabetes, obesity, and pre-eclampsia. Infants born to mothers with mental illness were not more likely to be small for GA or require delivery room resuscitation, mechanical ventilation, or surfactant administration during admission. The two cohorts had no significant differences in GA, birth weight, or length of stay.
Conclusions: Maternal HIV diagnosis, unpartnered status, housing insecurity, and lower educational attainment were associated with maternal psychiatric illness. Very preterm infants born to mothers with mental illness had no significant differences in GA, birth parameters, or length of stay. Long-term neurodevelopmental outcome studies are needed.
# 442
EFFECTS OF SURFACTANT ADMINISTRATION PROCEDURAL COMPLICATIONS ON OUTCOMES IN NEWBORN INFANTS
Feliz Sala EE1, Sandhu JK2, Siddiqui S2, Biniwale M3, Ramanathan R3. 1University of Southern California/ Los Angeles General Medical Center, Los Angeles, CA; 2University of Southern California/ Los Angeles General Medical Center, Los Angeles, CA and 3USC Keck School of Medicine, Los Angeles, CA
Purpose of Study: Respiratory distress syndrome is caused by a deficiency in surfactant and can lead to numerous complications, morbidity, and mortality. Surfactant therapy reduces the severity and complications of respiratory distress syndrome. Two common methods of surfactant administration include INtubation-SURfactant-Extubation (INSURE) as well as the more recent Less Invasive Surfactant Administration (LISA) method. Both methods have been associated with complications during the administration including bradycardia, hypoxemia, and trauma. The purpose of this study is to compare differences in outcomes in the presence or absence of these complications in infants who received LISA and INSURE.
Methods Used: The study design is a retrospective cohort study. Data was obtained via electronic medical records of neonates in Los Angeles General Medical Center Neonatal Intensive Care Unit, from 2016 to 2022. The presence or absence of complications associated with the administration of LISA and INSURE, including bradycardia and trauma, were cross referenced with infant outcomes using chi-squared and T-Test analyses. Outcomes variables included LOS, readmission to hospital, need for home O2, development of pneumothorax, diagnosis of BPD, days to room air, and need for intubation at day 3 and day 7 of life.
Summary of Results: Out of 119 infants included in the study 9 (7.5%) were noted to have procedural complications. Most common complications included airway trauma in 56% and need for manual positive pressure ventilation (PPV) in 33%. Complication rates for infants receiving INSURE was 4.3% compared to LISA 12.2% (P=0.15). INSURE procedure was most likely associated with trauma (100%) compared to LISA where most likely risk was need for PPV (50%). Risk of intubation requiring mechanical ventilation was 56% in infants after any complication in these infants. Chances of needing invasive mechanical ventilation at three days of life were significantly higher in infants having procedural complications (56% vs 15% P<0.01). These infants did not need higher respiratory support by 7 days after the procedure and did not contribute towards long term respiratory morbidities.
Conclusions: In conclusion, the presence of complications during the administration of surfactant, whether LISA or INSURE, was associated with increased risk of invasive mechanical ventilation in first 3 days after the procedure. While INSURE was most likely associated with trauma, LISA was most commonly associated with need for manual PPV. There were no additional long-term morbidities related to the surfactant administration procedural complications.
Comparison of outcomes in newborn infants with and without procedural complications associated with surfactant administration.
Mean +/- Standard Deviation; NCPAP-nasal continuous positive airway pressure; NIPPV-nasal intermittent positive pressure ventilation.
# 443
ACCURACY OF DOCUMENTED NEONATAL RESUSCITATION INTERVENTIONS PERFORMED ON PRETERM INFANTS USING DELIVERY ROOM VIDEO RECORDING
Anumula AR, Katheria A. Sharp Mary Birch, San Diego, CA
Purpose of Study: Neonatal resuscitation documentation is limited by relying on recollection of rapid events occurring within minutes of birth. Resuscitation personnel are not only tasked with performing the resuscitation, but they must remember the timing and frequency of these interventions. Missing information may contain critical information as to the acuity or difficulty of the resuscitation. Video capture of resuscitation interventions may provide a complete, objective assessment of changes in vitals combined with accurate reporting of interventions that occur in the delivery room. We sought to compare our video recordings with what was documented in the EMR during resuscitation of preterm infants.
Methods Used: Sharp Mary Birch Hospital for Women & Newborns routinely records all preterm deliveries in a high-risk neonatal resuscitation suite equipped with video and audio recordings of all deliveries. These video and audio recordings were compared to the documentation in the electronic medical record. These data were then compared to what was entered in the resuscitation notes in the EMR. Each variable was noted for accuracy (ie. number of intubation attempts, administration of surfactant) as well as whether the duration of each intervention was similar (i.e. duration of CPAP, time to successful intubation) to within plus or minus 30 seconds of what was documented in the EMR.
Summary of Results: A total of 233 pre-term births videos (23-32 weeks) were collected from 2019-2021 and reviewed as to the timing of interventions and how often they were performed. figure 1 demonstrates which interventions were then incorrectly reported in the EMR compared to video review. Timing of interventions (CPAP, intubation, surfactant administration) were the commonly misreported, followed by number of intubation attempts.
Conclusions: Traditional resuscitation documentation may omit crucial data, specifically ventilation information such as under-reporting of intubation attempts, and discrepancies such as total duration of PPV or time to successful intubation. Implementation and review of resuscitation videos into the EMR will likely improve documentation and provide a reliable resource for accurate delivery room reporting.
# 444
Patogens and in-hospital outcomes in neonates with sepsis requiring extracorporeal life support
Puia-Dumitrescu M1, Billimoria ZC1, Sullivan KM10, Rao R2, Chapman R11, Mahmood B3, Zaniletti I4, Rintoul N5, Seabrook R6, Hamrick S7, Keene S7, Gowda S8, Carr NR9, DiGeronimo R1. 1Seattle Children’s Main hospital, Seattle, WA; 2Washington University in St. Louis School of Medicine, St Louis, MO; 3UPMC Children’s Hospital of Pittsburgh, Pittsburgh, PA; 4Children’s Hospital Network, NA, CO; 5Children’s Hospital of Philadelphia, Philadelphia, PA; 6Nationwide, NA, OH; 7Emory University School of Medicine, Atlanta, GA; 8Baylor, NA, TX; 9Utah, Salt Lake City, UT; 10Thomas Jefferson University, Wilmington, DE and 11CHLA, NA, CA
Purpose of Study: To evaluate the incidence, pathogenesis, and in-hospital outcomes associated with sepsis among hospitalized neonates requiring extracorporeal life support (ECLS).
Methods Used: We conducted a retrospective review of the Children’s Hospital Neonatal Consortium database. All neonates supported with ECMO were identified. We created 3 groups: culture positive sepsis (CPS) (positive blood, tracheal, cerebrospinal fluid and/or urine culture), clinical sepsis (CS) (culture negative and treated with antibiotics for at least 7 days), and neonates treated with ECMO for other indications. All congenital diaphragmatic hernia patients were excluded from the cohort. Categorical variables were summarized with counts and percentages, while medians and interquartile ranges were used for continuous variables. Groups were compared using Chi-square, Fisher’s exact and Kruskal-Wallis as appropriate. All analyses were conducted in SAS Enterprise Guide v7.1 and significance was evaluated at a level of 0.05.
Summary of Results: From 2010-2016, we identified 818 neonates supported with ECMO, 108 with CPS, 176 with CS, and 534 for other non-sepsis etiologies. Most common pathogens were Escherichia coli (E. coli) (n=21; 19.4%), Group B Streptococcus (GBS) (n=20; 18.5%) and Herpes simplex virus (HSV) (n=8; 7.4%). Neonates with CPS were more likely to be supported with veno-arterial ECMO (69.4%) versus CS (44.3%). Mortality in neonates supported with ECMO for CPS was 50% versus 18.8% in neonates with CS. In addition, neonates with CPS required longer ECMO runs and had a longer hospital length of stay in survivors. A total of 41% of CPS neonates that survived post ECMO were discharged home with 34% of those needing gavage assisted feeding.
Conclusions: Many outcomes including survival in neonates with CPS following ECMO are worse compared with other clinical subgroups. GBS, E. coli and HSV were commonly identified pathogens. Neonates that survive to discharge home uncommonly require respiratory support other than oxygen but are at increased risk of needing gavage assisted feeding.
# 445
COMPARISON OF OUTCOMES OF INFANTS ADMITTED TO THE NEONATAL INTENSIVE CARE UNIT WHO NEEDED PHARMACOLOGIC INTERVENTION TO COMPLETE MAGNETIC RESONANCE IMAGING PROCEDURE COMPARED TO THOSE WHO REQUIRED ONLY NON-PHARMACOLOGIC MEASURES
Qamar H, Siddiqui S, Ramanathan R, Cayabyab R. University of Southern California/Los Angeles General Medical Center, Los Angeles, CA
Purpose of Study: Magnetic Resonance Imaging (MRI) is a widely utilized diagnostic modality in the Neonatal Intensive Care Unit (NICU). To achieve optimal imaging results, the use of non-pharmacologic intervention such as immobilization board, feeding prior to the procedure, non-nutritive sucking, and facilitated tucking are utilized. However, some neonates may require the use of pharmacologic intervention in the form of opioids or benzodiazepines. The use of sedation in neonates has potential risks and adverse effects, including progression to deep sedation and obtundation, death, increased respiratory support, and adverse neurodevelopmental outcomes. This study aims to assess the rate of infants requiring pharmacologic intervention to complete an MRI procedure and any adverse effects.
Methods Used: Retrospective cohort study of all neonates admitted to the NICU at Los Angeles General Medical Center who underwent MRI procedure between January 2021 and June 2023. Neonatal demographics, indication for MRI of the brain, duration of MRI procedure, respiratory support before and after imaging, feeding intolerance, and length of stay were obtained from electronic medical records and Neonatal Information System Database. Infants were divided into 2 groups whether they received or did not receive pharmacologic intervention prior to or during the MRI procedure. Chi Square and Wilcoxon rank sum was used for categorical and continuous variables as appropriate. McNemar test was used to determine the difference in respiratory support before and after MRI.
Summary of Results: There were 94 neonates who underwent MRI procedure during this study period. A majority of the neonates 66/94 (70%) received pharmacologic intervention in the form of midazolam 63/66 (95%), Fentaly 2/66 (3%) and morphine 1/66 (2%) to complete the MRI procedure. There was no significant difference in gender, gestational age, birthweight and indication for MRI between the two groups. However, the majority of neonates who required pharmacologic intervention were very low birth weight (VLBW) infants, had significantly higher post menstrual age, significantly higher rate of additional MR spectroscopy procedure in addition to MRI, significantly longer stay in the MRI suite (Table) and were more likely to need escalation of respiratory support after MRI (Difference 0.15, 95% CI: 0.04, 0.26 p value <0.01) There was no significant difference in tolerance of feeding nor occurrence of apnea, bradycardia, and oxygen desaturations after MRI between the two groups. (Table)
Conclusions: Our preliminary data showed that neonates requiring pharmacologic intervention to complete the MRI procedure were more likely to be VLBW, had additional imaging performed and stayed in the MRI suite longer. Pharmacologic intervention could have possibly led to the escalation of respiratory support. We need to limit the duration of the MRI procedure, avoid additional imaging and maximize non pharmacologic measures to prevent the use of sedation.
Median (25th, 75th percentile); CUS - cranial ultrasound; VLBW - very low birth weight; LBW - low birth weight.
# 446
RISK OF CEREBRAL PALSY IN VARIOUS TREATMENTS OF PATENT DUCTUS ARTERIOSUS
Cacho BJ, Jennings H, Deming D. Loma Linda University, Loma Linda, CA
Purpose of Study: We evaluated the development of cerebral palsy in very low birth weight infants with different management approaches for treatment of patent ductus arteriosus
Methods Used: We reviewed 204 neonates born at Loma Linda University Children’s Hospital with gestational age below 30 weeks between January 2018 through July 2023. We excluded infants with congenital malformations. Treatment pathways of patent ductus arteriosus was done per protocol and included no intervention, pharmacologic closure (indomethacin, ibuprofen, or acetaminophen), surgical ligation, or catheter occlusion. We then evaluated the prevalence of cerebral palsy at 24 months of age. We preformed descriptive statistics, Chi square analysis and multivariate logistic regression (no treatment was the referent) using SPSS (v28, IBM).
Summary of Results: There were 204 total patients who met the criteria for inclusion in this study. Out of 204, 22 were diagnosed at 24 months with cerebral palsy. Table 1 indicates the stratification of included patients by treatment type. The surgical ligation group had an increased odds of CP.
Conclusions: In our data set, surgical ligation was the only treatment modality associated with a significantly higher rate of preterm infants developing cerebral palsy
Treatment Type
OR (94%CI)
p
No Treatment (referent)
Pharmacologic
1.388 (0.523–3.683)
0.510
Surgical
6.200 (1.269–30.296)
0.024
Catheterization
0.608 (0.072–5.113)
0.647
Only surgical ligation was associated with a significantly increased odds of cerebral palsy.
Neonatology Perinatal Biology II
Concurrent Session
10:15 AM
Friday, January 19, 2024
# 447
Circulating and placental growth differentiation factor-15 are significantly altered in pregnancies complicated by obesity
Hermel JA1, Zeng F1, Flannery DD2, Mukhopadhyay S2, Barboza AZ2, Pfeifer M2, Lazar S1, Fisch K3, Cheung V4, Parast M4, Sajti E1. 1UC San Diego and Rady Children’s Hospital, San Diego, CA; 2The Children’s Hospital of Philadelphia and Perelman School of Medicine, University of Pennsylvania, Philadelphia, PA; 3UC San Diego, La Jolla, CA and 4UC San Diego, La Jolla, CA
Purpose of Study: Half of pregnant persons in the USA are overweight or obese. Obesity in pregnancy is associated with adverse outcomes for mothers and neonates. Chronic low-grade inflammation, characteristic of obesity, is thought to drive these complications. Growth differentiation factor-15 (GDF15), a cytokine with anorectic and immune-regulatory properties, counterbalances excessive energy intake and facilitates adaptation to inflammation. We hypothesized that placental GDF15 gene expression and serum GDF15 protein levels are altered in obese pregnant persons and their fetuses.
Methods Used: Gene expression was tested on the placenta and fetal membranes of 2 lean (pre-pregnancy BMI < 25 kg/m2) and 2 obese (pre-pregnancy BMI > 30 kg/m2) participants who had otherwise uncomplicated full-term births. We performed single-cell RNA sequencing (scRNAseq) on these tissues using the 10x Genomics platform and analyzed the data with the SEURAT pipeline. To validate these results at the protein level, we selected paired maternal and cord serum samples (18 lean, 18 obese) from a cohort established at Pennsylvania Hospital consisting of 4717 parturient patients and 4765 infants born full-term. Samples were chosen so that within each group, an equal number of neonates (n=6) were classified as either SGA, AGA, or LGA (Fenton’s 2013 growth charts). A balanced distribution of sexes was maintained. GDF15 levels were measured with ELISA and differences in mean GDF15 concentrations were estimated using a linear mixed model.
Summary of Results: ScRNAseq analysis revealed a substantial increase in GDF15 gene expression in placental and fetal membrane trophoblasts of obese participants compared to their lean counterparts. Protein measurements showed that maternal serum GDF15 levels were more than six-fold higher than their neonates irrespective of obesity status. We observed significantly higher GDF15 levels in the serum of lean mothers as compared to obese mothers (15388 pg/mL vs 13482 pg/mL, p < 0.05). Cord GDF15 levels did not vary with pre-pregnancy BMI or birthweight. However, among lean pregnant women, greater levels of maternal serum GDF15 levels were associated with LGA neonates.
Conclusions: Our study is the first to compare GDF15 protein levels in maternal-fetal dyads, and gene expression in placental samples. While placental GDF15 primarily originates from trophoblasts, we observed that maternal levels exceeded fetal levels by a factor greater than six. This suggests biochemical processes driving distinct GDF15 expression patterns in mothers and fetuses. Moreover, pre-pregnancy obesity was associated with altered maternal GDF15 levels in a manner strikingly different from that reported in non-pregnant men and women. Our findings suggest a significant role of GDF15 in regulating the effects of maternal obesity on neonatal development and may provide the basis for targeted therapeutics to prevent neonatal complications associated with obesity.
# 448
Inter-muscle differences in microvascular architecture within skeletal muscle of the growth restricted fetus
Dear T1, Chang EI1, Al-Juboori SI1, Strode D1, Jonker S2, Rozance P1, Stremming J1, Dobrinskikh E1, Brown LD1. 1University of Colorado School of Medicine, Aurora, CO and 2Oregon Health and Science University, Portland, OR
Purpose of Study: Skeletal muscle growth is reduced in the fetus affected by fetal growth restriction (FGR). We have previously shown that hindlimb blood flow is similar between late gestation control (CON) and FGR fetal sheep when normalized to hindlimb weight, yet oxygen delivery rates are reduced per gram of hindlimb. We also have shown reduced capillary density, lower vascular endothelial growth factor A (VEGFA) expression, and fewer oxidative fibers within the FGR tibialis anterior (TA) muscle, which is composed of both type I oxidative and type II glycolytic myofibers. Because oxidative fibers have increased capillary density compared to glycolytic fibers, it is unknown whether the reduced capillary density and VEGFA expression are the result of reduced oxidative myofiber composition. We hypothesized that in a muscle composed primarily of oxidative fibers, chronic hypoxemia associated with placental insufficiency would not impair capillary growth or angiogenic signaling pathways in the FGR fetus.
Methods Used: Soleus (SOL) muscle was harvested from CON (n=9) and FGR (n=6) late gestation fetal sheep (135±1 days of gestation, dGA; term=147 dGA). Protein was isolated and relative protein amounts of VEGFA and VEGF Receptor 2 (VEGFR2) were measured by Western blot. In frozen sections (5 µm) (CON, n=3; FGR, n=3), anti-dystrophin and anti-myosin heavy chain type I were used to identify myofibers and oxidative fiber type, respectively, and lectin agglutinin was used to identify vascular structures by immunofluorescence. Visiopharm® software was used to quantify myofiber number, fiber type proportions, vascular area, and capillary number. Student’s t-test was used to compare FGR versus CON and P<0.05 was designated as significant.
Summary of Results: SOL muscle was comprised of 99.7% oxidative myofibers, and 0.3% glycolytic fibers in both CON and FGR. Total vascular area, arteriole and venule area, capillary area, capillary density, and oxidative myofiber number did not differ between FGR SOL muscle compared to CON. Protein expression of VEGFA and VEGFR2 were similar between groups.
Conclusions: The proportion of oxidative myofibers and capillary growth are preserved in FGR SOL muscle compared to CON. There also were no differences in VEGFA or VEGFR2 protein expression, indicating that pathways regulating vascular development may be spared from chronic hypoxemia in primarily oxidative muscles such as the SOL. These data support our hypothesis that a reduction in oxidative myofibers as a result of chronic fetal hypoxemia contributes to reduced capillary development. Our results also show that SOL, a muscle composed predominantly of oxidative myofibers, does not account for the reduction in oxygen uptake of the hindlimb in the FGR fetus. We speculate that reduced oxygen uptake by the FGR hindlimb is driven by myofiber switching from oxidative to non-oxidative myofibers in muscle composed of mixed myofiber types.
# 449
EXPRESSION OF THE MECHANOSENSITIVE ION CHANNEL PROTEIN PIEZO1 IS DIRECTLY ASSOCIATED WITH THE DEVELOPMENT OF EXPERIMENTAL NEONATAL SEPSIS
Jain NJ, Cera A, Persiani M, Lopez V, Rudko A, McElroy S, Bautista G. University of California Davis School of Medicine, Sacramento, CA
Purpose of Study: Neonatal sepsis is the leading cause of infant mortality worldwide. Sepsis is an inflammation-mediated injury amplified by the intestine, resulting in impaired mucosal barriers, further immune system dysregulation, and subsequent organ failure. The novel mechanosensitive channel Piezo1 is a critical driver of inflammation and the innate immune system, and increased Piezo1 expression has been observed in adult inflammatory bowel diseases. However, its role in gut-specific inflammatory processes in the neonate remains largely unknown. Using a well-established murine sepsis model, we aimed to determine if Piezo1 expression in the gut is altered following exposure to experimental sepsis. We hypothesized that neonatal sepsis would significantly increase the expression of Piezo1.
Methods Used: To test this hypothesis, time-dated C57BL/6 mouse pups at postnatal age (P)7-8 were subjected to experimental sepsis. Pups were given 3.00x107 CFU/ml of NECteria (mixed enteric bacteria extracted from a neonate that died from NEC) or sterile normal saline (sham control) via intraperitoneal injection. Pups were monitored for up to 8 hours following inoculation, with distal ileal segments harvested at the time of demise. We analyzed mRNA levels of Piezo1 using droplet digital PCR and further localized Piezo1 expression using in situ hybridization (ISH) via RNA-scope.
Summary of Results: Sepsis-exposed pups died at an average of 5-6 hours post-inoculation, while sham control pups remained healthy and active for the entire protocol. Piezo1 levels were significantly elevated in the distal ileal segments of mouse pups with experimental sepsis (n=11) compared to sham controls (n=13) (9.15 vs 15.09 copies/ng; p=.0003). This was further correlated using ISH, suggesting an overall increase in Piezo1 expression across both the epithelial and muscularis layers of the gut.
Conclusions: Our data suggests that Piezo1 is critical to the signaling mechanisms involved in intestinal inflammation in neonatal pups. Further studies and experimental models are necessary to delineate the signaling mechanisms involved.
Piezo1 RNA expression via ISH depicted in red (black arrow) is dramatically increased across the epithelium and muscularis in distal intestinal segments of mice with experimental sepsis compared to controls where Piezo1 is primarily expressed along the lamina propria and submucosal muscularis. Images taken at 20x.
# 450
Insulin activates muscle protein synthesis regulators in isolated myofibers from fetal sheep
Painter CS, Stacey HE, Stremming J, Brown LD, Chang EI. University of Colorado, Aurora, CO
Purpose of Study: Increased insulin sensitivity for glucose utilization has been demonstrated in growth restricted fetal sheep (FGR) compared to normally growing control fetal sheep. Direct insulin infusion into FGR fetal sheep in vivo also has been shown to stimulate muscle protein synthesis regulators to a similar degree as controls. Yet, the FGR fetus has smaller skeletal muscles. In myofibers isolated from fetal skeletal muscle, we aimed to test the intrinsic capacity of FGR muscle to upregulate regulators of muscle protein synthesis in response to insulin ex vivo.
Methods Used: Pregnant sheep carrying singleton fetuses were randomly allocated to either environmental chambers with normal ambient temperatures for control (CON, n=7) or elevated ambient temperatures to produce placental insufficiency and FGR (n=7). Surgery was performed at 126±2 days of gestation (dGA; term 147 dGA) for placement of maternal and fetal catheters. At 133±1 dGA, fetal arterial blood was collected to measure blood gas, glucose, and insulin concentrations. Fetal biceps femoris (BF) muscle was collected at necropsy and placed into Krebs Henseleit Buffer (KHB) gassed with 95:5 O2:CO2. BF myofibers were dissected, placed in a clip to maintain natural distance (2-3 myofibers per clip), and equilibrated in gassed KHB for 30 min. Myofibers were incubated with and without 100nM insulin for 1 hr. Protein was isolated to measure total insulin receptor beta (IRβ), and both phosphorylated (activated) and total AKT, p70S6 kinase, 4E-BP1, rpS6, and ERK1/2. Student’s t-test was used to compare FGR vs. CON values, and two-way ANOVA was used to compare basal and insulin-stimulated conditions between FGR and CON.
Summary of Results: Fetal weights and summed hindlimb muscle weights were 50% and 54% smaller in FGR compared to CON, respectively (P<0.0001). Glucose concentrations were 37% lower (P<0.001), PaO2 was 32% lower (P<0.005), and insulin concentrations were 50% lower (P=0.05) in FGR compared to CON. In isolated myofibers, IRβ protein expression was greater at baseline and after insulin exposure in FGR compared to CON (P<0.05). Additionally, insulin increased the abundance of phosphorylated, total, and phosphorylated:total AKT in FGR compared to CON (P<0.05). Phosphorylated p70S6 kinase, rpS6, and ERK1/2 were higher in response to insulin compared to basal conditions in CON myofibers only, and there were no differences in 4E-BP1.
Conclusions: A 1 hr insulin incubation in isolated myofibers ex vivo increased AKT activation more significantly in FGR compared to CON. IRβ was also upregulated in FGR myofibers regardless of insulin stimulation, possibly the result of chronic exposure to lower insulin concentrations in vivo. Given that AKT regulates insulin-stimulated glucose uptake in addition to protein synthesis, we speculate that FGR muscle develops intrinsic mechanisms to activate AKT and stimulate glucose metabolism. However, limited activation of other regulators of protein synthesis may be a mechanism to slow skeletal muscle growth in FGR.
# 451
Maternal Tobacco Smoke Exposure Induces Placental Zone and Sex Dependent Changes in Epigenetic Mediators of LCPUFA Metabolism
Bartholomew A1, Chidester W1, Levaratto S1, Maschek A2, Cox J2, Joss-Moore L1. 1University of Utah, Salt Lake City, UT and 2University of Utah, Salt Lake City, UT
Purpose of Study: Appropriate organ development relies on adequate fetal acquisition of long-chain polyunsaturated fatty acids (LCPUFA). The placenta mediates maternal-fetal LCPUFA transfer. We recently identified a placental epigenetic pathway activated by hypoxia in the rat, which increases placental retention of LCPUFA at term gestation, the PPARγ-KMT5A-H4K20me pathway. Activation of this pathway results in placental LCPUFA accumulation at the expense of fetal LCPUFA acquisition and fetal growth. We have also shown, in the rat, that maternal tobacco smoke exposure (MTS) decreases fetal acquisition of the LCPUFAs docosahexaenoic acid (DHA) and arachidonic acid (AA) in male, but not female, fetuses. However, the effects of MTS on placental PPARγ-KMT5A-H4K20me and placental LCPUFA in our model are unknown.
We hypothesize that MTS causes sex-divergent changes in placental PPARγ-KMT5A-H4K20me in association with increased placental retention of DHA and ARA in the rat.
Methods Used: Pregnant rats were exposed to tobacco smoke (MTS) or room air (Control) from E11 to term (E21). Placenta were collected at term, and basal zone (BZ) and labyrinth zone (LZ) separated. Western blot was used to measure PPARγ, KMT5A, and global H4K20me, and GC/MS was used to quantify levels of LCPUFA, including DHA and ARA. Placenta supporting male and female pups were treated as separate groups, n=6-9 non-sibling placenta/group. One-way ANOVA with Fishers’ LSD post-hoc test was used to detect group differences.
Summary of Results: In the BZ of placenta supporting male pups, MTS increased levels of PPARγ (129±6%*), KMT5A (140±7%*), and H4K20me (199±40%*). In the BZ of placenta supporting female pups and in the LZ of placenta supporting either sex, MTS did not alter PPARγ, KMT5A, or H4K20me levels. MTS increased levels of lysophosphatidylcholine (LPC)-DHA (130±9%*) and LPC-ARA (151±12%*) in the BZ of male placenta. MTS did alter LPD-DHA or LPC-ARA in female BZ or LZ of either sex.
Conclusions: MTS causes zone and sex specific changes in the epigenetic PPARγ-KMT5A-H4K20me pathway in rat placenta. We speculate that MTS-induced upregulation of PPARγ-KMT5A-H4K20me and accumulation of LPC-DHA and LPC-ARA in the basal zone of male placenta contributes to our previous observation of less DHA and AA acquisition in male MTS fetuses.
# 452
INFLUENCE OF LONG-TERM, INTRAUTERINE HYPOXIA ON CALCIUM SPARKS IN MIDDLE CEREBRAL ARTERIAL MYOCYTES OF FETAL SHEEP
Nelapudi N1, Boskind M1, Zhang L1, Blood A1, Wilson CG1, Puglisi J2, Wilson S1. 1Loma Linda University School of Medicine, Loma Linda, CA and 2California Northstate University College of Medicine, Elk Grove, CA
Purpose of Study: The Ca2+ spark, generated by local activation of ryanodine receptors (RyRs) on the sarcoplasmic reticulum in vascular smooth muscle cells (VSMCs), is a significant participant in the autoregulation of vascular contractility and cerebral blood flow. As a known disruptor of such cerebrovascular processes, gestational hypoxia increases the risk of intracranial hemorrhage and stroke in the newborn. Due to RyR’s role in regulating cerebrovascular blood flow in the neonate, understanding intracellular Ca2+ release patterns offer insight into the pathophysiological disruptions taking place in hypoxia-related perinatal cerebrovascular disease. The central aim of this study is to further elucidate the pathophysiology of long-term, intrauterine hypoxia through examination of RyR activity in VSMCs of fetal ovine middle cerebral arteries (MCAs).
Methods Used: MCAs were isolated from term fetal sheep (~140 days of gestation) delivered from ewes held at low- (700 m) and high-altitude conditions (3801 m) for 100+ days of gestation. Arteries were bathed in a physiological buffer with 5 mm K+ (control) or were treated with either 30 mM K+ (30K), to depolarize myocytes and release Ca2+, in the presence or absence of 10 μM ryanodine, to block Ca2+ release. Ca2+ spark activity due to local activation of RyRs in myocytes were measured in situ with confocal microscopy fluorescence imaging techniques. Automated analysis of the recorded line scans as well as morphological characterization of Ca2+ sparks was conducted using SparkLab 5.8.
Summary of Results: Membrane depolarization with 30K increased the proportion of cells with Ca2+ sparks and their frequency of activation. Long term hypoxia, however, reduced spark activity and frequency in the 30K group. Ryanodine attenuated Ca2+ spark activity in myocytes from low and high altitude animals. Hypoxia’s influence on the spatial and temporal aspects of the Ca2+ sparks in fetal normoxic myocytes were found to be inconsistent and variable with regards to the amplitude and full-duration at half maximum, while the architecture of the sparks in relation to full-width at half maximum and tau were relatively preserved.
Conclusions: These findings corroborate previous evidence demonstrating that long-term hypoxia attenuates localized Ca2+ spark signaling, while also affecting spatial and temporal aspects to Ca2+ spark activity. The disruption in Ca2+ spark activity would then impact brain blood flow in the neonate, potentially increasing the likelihood of a traumatic event.
# 453
Piezo1 in the developing gut is inversely related to postnatal age in neonatal mice
Lopez V, Persiani M, Jain NJ, Rudko A, Cera A, McElroy S, Bautista G. University of California Davis Children’s Hospital, Sacramento, CA
Purpose of Study: Preterm birth remains the leading cause of mortality for children <5 years of age worldwide, with necrotizing enterocolitis (NEC) remaining the leading cause of mortality (20-50%). The impaired mucosal barrier and underdeveloped innate immunity in preterm infants make them particularly susceptible to intestinal injury. The signaling mechanisms that drive these pathways are central to the increased susceptibility of the premature gut to injury, but remain poorly characterized. Piezo1 is a mechanosensitive channel essential for maintaining the intestinal epithelial barrier and regulating innate immunity. Despite its broad expression across the numerous intestinal layers, its specific expression and role in the developing gut have yet to be elucidated. This project aimed to define Piezo1 gene expression and localization in the developing gut of mice from early embryonic age into adulthood. We hypothesized that Piezo1 is necessary for epithelial morphogenesis of the neonatal gut. Specifically, we hypothesized that Piezo1 expression would increase during epithelial reorganization, villous development (e14.5-E16.5), and crypt maturation which house stem cells essential for regeneration and Paneth cells critical for driving the innate immunity (E16.5-P15).
Methods Used: Time-dated C57BL/6 mouse pups were extracted at multiple embryological (e) and postnatal (P) ages (e14.5-P56). Distal ileal tissue was resected and isolated for subsequent RNA and tissue analyses. Piezo1 mRNA levels were quantified using droplet digital PCR and localized within the intestinal structures using in situ hybridization (RNAscope).
Summary of Results: Piezo1 mRNA expression (n = 6 m) was highest at e14.5 and then significantly decreased in an age-dependent manner until P56 (p <0.0001). We subsequently localized Piezo1 expression primarily within the muscularis layers during early gestational ages, with an increased presence throughout the developing villi and intervillous regions at P0 and gradually decreasing in the subsequent postnatal ages, with the lowest expression at adulthood (P56). Furthermore, we observed that at sites of maturing crypts, Piezo1 was abundantly expressed and further localized within Paneth cells.
Conclusions: These results suggest Piezo1 are associated with gut development and Paneth cell maturation. Additional studies are needed to elucidate the signaling mechanisms driving these processes to establish novel therapeutic targets in NEC.
# 454
THE PROTECTIVE USE OF CUTANEOUS VAGUS NERVE STIMULATION (VNS) IN AN EXPERIMENTAL NECROTIZING ENTEROCOLITIS (NEC) MODEL IN RAT PUPS
Baker ME1, 3, Mladenov GD2, Radulescu A2, Wilson CG3, 1. 1Loma Linda University Health, Loma Linda, CA; 2Loma Linda University Health, Loma Linda, CA and 3Loma Linda University Health, Loma Linda, CA
Purpose of Study: Necrotizing enterocolitis (NEC) is among the most common GI diseases in preterm neonates. Vagus nerve stimulation (VNS) is often used to treat adult inflammatory diseases. VNS also has the potential to attenuate the inflammation associated with NEC. However, VNS must first be studied pre-clinically to test its efficacy and safety. We hypothesize that non-invasive VNS can be used in a rat model of NEC to reduce the severity and incidence of NEC.
Methods Used: Rat pups from 10 full-term litters were divided at birth into 6 treatment groups: NEC induction with VNS, NEC induction with sham VNS, NEC induction with no VNS, no NEC induction with VNS, no NEC induction with sham VNS, and no NEC induction with no VNS.
NEC induction pups received a NEC induction protocol with hypertonic formula, lipopolysaccharide, and hypoxic/cooling stressing sessions. Non-NEC induction pups received normal newborn rat care. VNS was given via microvascular clips gently attached to the pups’ earlobes for 3, 30 minute sessions during the first 24 hours of life. Electrodes were epoxied to the clips, and 0.05 mA of current, with a 20 Hz frequency, was used to stimulate the auricular branch of the vagus nerve. Pups who received sham stimulation had identical sessions without electrical current.
Pups who died before 96 hours old had GI tract samples harvested immediately. All surviving pups were sacrificed and harvested at 96 hours old. Microscope slides were created from the GI tissue, and then were blindly analyzed and assigned a Bell NEC score of 0–4. The average NEC score for each treatment group was calculated. NEC incidence was defined as grades 2–4.
Summary of Results: There were 102 rat pups included from 6 litters. The average Bell NEC scores and NEC incidences were 1.33/43% for NEC induction + VNS (n=21), 1.38/33% for NEC induction + sham VNS (n=24), 1.56/44% for NEC induction - VNS (n=9), 0.55/0% with no NEC induction + VNS (n=11), 1.11/39% for no NEC induction + VNS (n=18), and 1.32/37% for no NEC induction - VNS (n=19) (see figure 1). These results were not significantly different between groups (p > 0.05).
Conclusions: Our study showed a possible protective effect of cutaneous VNS on NEC severity, but only in pups who do not receive NEC induction. It is unclear why some pups developed significant NEC without NEC induction. Future research should use more subjects, improved VNS methods, and intralitter controls to determine if VNS can help relieve NEC-related morbidity and mortality.
# 455
ALBUMIN-MEDIATED HYDROGEN SULFIDE SCAVENGING: MECHANISTIC INSIGHTS FORM IN VITRO INVESTIGATIONS
Duot A, Zhang M, Liu T, Blood A. Loma Linda University, Loma Linda, CA
Purpose of Study: Hydrogen sulfide (H2S ), a gaseous signaling molecule, has garnered considerable attention due to its versatile roles in physiology and pathophysiology. In our unintended exploration of H2S interactions, we observed that albumin, a multifunctional plasma protein, exhibits the capacity to scavenge H2S in vitro. By employing an amperometric H2S -specific probe, we conducted experiments involving the injection of H2S into buffer solutions, both with and without albumin. Intriguingly, our findings revealed that while H2S levels remained elevated in the absence of albumin, the presence of albumin led to an immediate decline in H2S concentrations. To elucidate the mechanistic underpinnings of this phenomenon, we formulated and tested several hypotheses.
Methods Used: Firstly, we postulated that the albumin-H2S interaction could be mediated through an enzymatic reaction. To probe this possibility, we subjected albumin to denaturation and compared its scavenging efficacy to that of native albumin. Denaturation did not significantly alter the H2S scavenging property of albumin, ruling out the involvement of enzymatic reaction in H2S scavenging.
Secondly, considering albumin’s role as heme carrier, we hypothesized that heme might contribute to the metabolism of H2S. The effects of azide and KCN, two well-known heme-blockers, were studied on albumin-H2S interactions. However, azide resulted in a steeper H2S decline, while KCN led to a lower peak and slower slope, hinting complicated reactions of these chemicals with H2S.
Thirdly, albumin is also a carrier of heavy metals such as iron and copper. Using respective chelators, we explored their involvement on the H2S scavenging property of albumin. While iron chelators including DTPA, EDTA, ferrozine, and DFO showed no pronounced effect, copper chelators tetrathiomolybdate and neocuproine demonstrated slope differences in scavenging profiles, underscoring the potential role of copper-mediated processes in H2S scavenging.
Lastly, we examined the participation of albumin’s free cysteine residues in the scavenging process. Albumin was treated with thiol blocker (NEM) and then filtered with ultracentrifuge tube (3kDa) to eliminate the NEM. NEM-treated albumin exhibited scavenging profiles akin to untreated albumin.
Summary of Results: While denaturation of albumin yielded trends similar to native albumin, heme-related azide reaction displayed a steeper H2S decline, whereas the KCN reaction exhibited a different pattern. Copper chelators exhibited observable slope differences in scavenging profiles. Notably, thiol blocking of albumin’s free cysteine residues did not impact the scavenging process.
Conclusions: Copper but not iron, enzymatic reaction, or free cysteine residues may be involved in albumin-mediated H2S scavenging. The complexities unveiled through this study warrant continued exploration of albumin’s potential role as a regulator of H2S dynamics and the associated implications for physiological processes.
Nephrology and Hypertension
Concurrent Session
10:15 AM
Friday, January 19, 2024
# 456
A Case of Primary Mutation Untreated Autosomal Dominant Polycystic Kidney Disease
Ike IS1, Okumoto L2, Petersen G2. 1Ross School of Medicine, Miramar, FL and 2Kern Medical, Bakersfield, CA
Case Report: Autosomal Dominant Polycystic Kidney Disease (ADPKD) is a multisystem disorder commonly caused by genetic mutations in either the PKD1 or PKD2 gene. It is typically characterized by bilateral renal cysts, liver cysts, and intracranial aneurysms. However, the manifestations of ADPKD can vary widely depending on the severity of the disease. Some studies have even shown that ADPKD can manifest differently depending on the presence or absence of a family history, with the latter suggesting a de novo mutation. In this particular case, we present a 56-year-old female with autosomal dominant polycystic kidney disease who has no known family history of the condition. She presented with extensive cysts in both the kidneys and liver, resulting in end-stage liver disease and end-stage renal disease. In this discussion, we explore the potential relationship between her disease status and lack of family history, as well as the importance of early intervention for treatment outcomes.
CT of the abdomen showed multiple large cysts in the liver and both kidneys.
There is a near complete replacement of the liver and kidneys with cysts.
# 457
Thrombospondin Type-1 Domain 7A (TSHD7A) Membranous Nephropathy: Rapid Remission After Obinutuzumab (Type II Anti-CD20) Treatment
Jordan SC1, Haas M2. 1Cedars-Sinai Medical Center, Los Angeles, CA and 2Cedars-Sinai Medical Center, Los Angeles, CA
Case Report: Patient is a 73 year old Russian female who had a history of hepatitis B (treated with Entecavir) and NAFLD . She had no history of malignancies or previous renal disease. She was in her usual state of good health until 12/22 when she noted onset of pedal edema and increasing abdominal girth. She rapidly progressed and was seen in ER for evaluation of SOB. On PE, she was noted to have severe anasarca without evidence of CHF. Her SCr was 2.0mg/dl Albumin 2.0gm/dl and urine protein/Cr 13gm. All autoantibody test were negative as was anti-PLA2R antibodies. A renal biopsy was performed and revealed TSHD7A MN. Patient was treated with IV diuretics and albumin without response. In our evaluation, we recommended treatment with obinutuzumab (obi) (type II anti-CD20). The patient received 1gm X 2 doses given 14 days apart. Within 5 days, she was dischared home . MMF 500mg bid was added after completion of Anti-CD20Rx. She continued to show improvement in clinical and biochemical features of NS (Fig 1). At 6M post-treatment, she has no significant proteinuria. Membranous nephropathy (MN) is a leading cause of NS in nondiabetic adults. Left untreated, two-thirds of patients with MN develop CKD. The recognition of MN as an autoimmune disease paved the way for the use of anti–B-cell therapy in management. Rituximab (Type 1 Anti-CD20) has been successfully used to treat MN and was shown to be noninferior to cyclosporine. However, 40% of patients with MN do not respond to rituximab . In addition, little is know about non-PLA2R+ responses to rituximab. We have reported that MN patients unresponsive to rituximab obtained good remissions with obi. Obi is a humanized and glycoengineered type II anti-CD20 monoclonal antibody that shows superior in vitro & in vivo B-cell depletion compared to rituximab. Obi is directed at a different epitope on CD20 than that recognized by rituximab and induces greater B-cell apoptotic response. Modification of the glycan tree structure at the Fc fragment of obi leads to an increased affinity to FcgRIII resulting in increased antibody dependent cellular cytotoxicity (ADCC) These B-cell depletional mechanisms contrast to the primarily complement-dependent cytotoxicity for rituximab. In summary, the advanced design of obi likely compensates for deficiencies of rituximab and results in better long-term remissions of MN. Here, TSHD7A+ MGN responded rapidly to obi treatment with complete remission.
Clinical Course of TSHD7A Membranous GN after Anti-CD20 Treatment.
# 458
CHALLENGES OF HYPONATREMIA IN A PATIENT WITH SIADH WITH RESET OSMOSTAT
Kamal N1, Davtyan E1, Eppanapally S2. 1Kern Medical, Bakersfield, CA and 2Kern Medical, Bakersfield, CA
Case Report: Reset Osmostat is a rare subtype of SIADH (syndrome of inappropriate antidiuretic hormone), characterized by a change in the normal plasma osmolality threshold for ADH secretion and can deplete sodium levels that remain chronically low. Sodium is an essential electrolyte that is responsible for regulating fluid balance, blood pressure, and nerve conduction to muscles and nerve cells. We present this case of SIADH complicated by Reset Osmostat with significant challenges in managing symptomatic hyponatremia.
Methods: Retrospective review following IRB approval
Summary of Results: A 62-year-old woman with medical history significant only for idiopathic SIADH not tolerating tolvaptan presents to the emergency department from a nephrology clinic with symptomatic severe hyponatremia. At arrival, patient is obtunded and weak with bilateral peripheral neuropathy of her lower extremities. Initial laboratory reports sodium 118 mmol/L, despite outpatient management with sodium tablet 2 g twice daily, furosemide 40 mg twice daily and 1L fluid restriction. Further workup while inpatient demonstrates normal adrenal and thyroid functions, serum plasma osmolality (258 mOsm/kg), urinary sodium (29 mmol/L) and elevated urine osmolality (632 mOsm/kg). Patient was initiated on home regimen with strict 1L fluid restriction and addition of Ure-Na 15g BID gradually increased to 30g in the a.m. and 15g in p.m. Despite optimal medical therapy, sodium never improved more than 126 mmol/L. Patient had symptomatic improvement and decrease in urine osmolality to 229 mOsm/kg with serum sodium levels ranging 122-126 mmol/L and serum osmolarities remained less 260mOsm/kg. Throughout the hospital course, serum uric acid levels remained low and patient was non-edematous. Based on labs and clinical presentation with chronic hyponatremia, diagnosis of SIADH with reset osmostat was given. At present, patient’s sodium levels range 122-123 mmol/L, remains asymptomatic, and is currently under investigation of autoimmune disorders as possible cause of reset osmostat.
Conclusion: SIADH can be subdivided into four subtypes (A, B, C, D). Subtype A is what is commonly referred to as the “classic” subtype. Subtype C is a unique hypoosmolar hypotonic condition and is called Reset Osmostat. Reset Osmostat hyponatremia results from an alteration in osmoreceptor cells’ metabolism, which induces ADH secretion at lower plasma osmolarities. Typically, patients are euvolemic with normal renal, adrenal and thyroid function. Most cases are difficult to diagnose because patients are asymptomatic and treatment of hyponatremia becomes a therapeutic dilemma. However, our patient did present with symptoms and symptomatic hyponatremia such as this case is challenging to treat as the osmostat is set at lower threshold. This case is noteworthy as the patient presented with symptoms of acute severe hyponatremia that obscured the underlying chronic illness and simultaneously presented challenges in treatment.
# 459
Turning the kidney into a lymphoid organ
Atwood D, He Z, Edelstein C. Univ Colorado, Aurora, CO
Purpose of Study: Pkd1RC mice (RC), a mouse model of autosomal dominant polycystic kidney disease (PKD), have suppressed autophagy in the polycystic kidney. The purpose of the study was to determine whether knocking out autophagy (ATG7) in the kidney in aged wild type mice would induce cyst growth.
Methods Used: ATG7-/- mice were generated using a renal tubule specific CreLox system.
Ischemic acute kidney injury (AKI) in the kidney in 6 month old mice was studied 45 days after a unilateral renal pedicle clamp, The contralateral kidney was used as the control
Summary of Results: No cysts were seen in ATG7-/- kidneys, but unexpectedly large tertiary lymphoid tissues (TLT) were seen in the ATG7-/- kidneys. TLTs are ectopic lymphoid tissues that develop de novo in nonlymphoid organs. There was increased TLT size, number, and index in 400 d old ATG7-/- kidneys (Table 1A). The phenotype of TLTs in ATG7-/- was confirmed by the presence of T and B cells and intense proliferation in the TLTs. There was intense staining for pS6 (mTORC1), an inducer of proliferation, in the TLTs. As autophagy knockout induced TLTs, we examined PKD kidneys, that have suppressed autophagy, for TLTs. There were increased TLT indices in 120 d old RC kidneys (Table 1B). Treating RC mice with the mTOR inhibitor Torin2 virtually eliminated TLTs. It is known that severe ischemic AKI in aged mice results in the formation of TLTs in the kidney. In ischemic AKI kidneys there was a large increase in the number, size and index (% of kidney) of TLTs compared to virtually no TLTs in the contralateral control kidney. The TLTs in ischemic AKI kidneys showed intense staining for pS6 (mTORC1). In future studies the effect of the mTOR inhibitor, Torin2, on TLTs in the ischemic AKI kidney will be determined.
Conclusions: There were numerous, large and discrete TLTs and intense pS6 (mTORC1) staining in the TLTs in aged tubule-specific ATG7-/- kidneys, RC kidneys and ischemic AKI kidneys. There was the virtual elimination of TLTs by treatment of RC mice with an mTOR inhibitor. Activation of mTORC1 in TLTs may drive formation and growth of TLTs.
# 460
RIDING THE WAVE OF GENETIC TEST ORDERING IN NEPHROLOGY: EXPERIENCES FROM A GENETIC COUNSELOR-LED RENAL GENETICS CLINIC
Dutra-Clarke M, Rome C, Russell B. UCLA Health, Los Angeles, CA
Purpose of Study: Monogenic disorders account for ~30% of adults and ~50% of children with nondiabetic chronic kidney disease. Identifying the underlying genetic cause of a patient’s kidney disease can help determine prognosis, guide treatment, identify at-risk relatives, and plan for kidney transplantation.
Recently there has been a surge in genomics uptake in the nephrology setting. Still, medical genetics clinics continue to have high volumes and long wait times to be seen by a geneticist, all while the population of geneticists continues to decline. To keep up with the demand, we established a renal genetics specialty clinic led by a genetic counselor (GC-only clinic) for patients with a variety of non-syndromic renal conditions.
We assessed the outcomes of the newly established GC-only renal genetics clinic, determined the diagnostic yield on genetic testing, and highlight the importance of the involvement of genetics providers in the counseling and interpretation of genetic test results when ordered by nephrologists.
Methods Used: We conducted a retrospective chart review of patients seen in the GC-only renal genetics clinic at UCLA over a two-year period. Patients received genetic counseling by a certified genetic counselor. In some cases, genetic testing was ordered. All visits were billed to patient insurance. Genetic testing in this cohort comprised of either a multi-gene panel specific to a renal disease subtype or a broad gene panel of several hundred genes associated with hereditary chronic kidney diseases.
Summary of Results: A total of 55 patients were seen in the GC-only renal genetics clinic, comprised of 10 children and 45 adults. In this cohort, 48 patients were referred for personal history of kidney disease and 7 were referred for only family history of kidney disease.
Of the total patients in this cohort, 47% (26/55) had prior genetic testing ordered by their nephrologist or other healthcare provider, of whom, 62% (16/26) had one or more variants of uncertain significance reported that benefited from genetic counselor expertise. For those whom genetic testing was not yet performed, or if further genetic testing was indicated, 17 patients completed genetic testing (n=24) with a positive diagnostic result in 76% (13/17).
Conclusions: In this cohort, there were instances of misinterpretation of genetic test results as well as ethical dilemmas when genetic testing was ordered and interpreted without a genetics provider prior to referral to the renal genetics clinic. Genetic specialty clinics for inherited kidney disorders, particularly GC-only clinics, increase access to care by avoiding long wait times to be seen by a geneticist and genetic counselor in a general genetics clinic and improves quality of patient care. Specialty clinics also advance professional growth of genetics providers by practicing at the top of their scope and developing expertise in a subspecialty.
# 461
Laser-guided Renal Access for Kidney Stone Surgery: A Comparison to Conventional Fluoroscopic Renal Access
Sajdak GM, Rotinsulu A, Farkouh A, Buell M, Amasyali AS, Leu R, Shete K, Ware C, Gentry V, Song S, De Guzman C, Baldwin D. Loma Linda University School of Medicine, Loma Linda, CA
Purpose of Study: Fluoroscopic-guided renal access exposes patients and staff to substantial radiation. The Laser Direct Alignment Radiation Reduction Technique (DARRT) is a hybrid technique utilizing fluoroscopy, ultrasound, endoscopic vision, and laser targeting to reduce fluoroscopy use and improve outcomes. The purpose of this study was to compare Laser DARRT to conventional fluoroscopic-guided kidney stone surgery.
Methods Used: A retrospective review was performed of all patients undergoing percutaneous nephrolithotomy (PCNL) for large kidney stones at a single academic institution from January 2017 to March 2023. Patients with pre-existing nephrostomy tubes used for access and only ultrasound-guided access were excluded. Renal access was categorized as either fluoroscopic or Laser DARRT access. The primary outcomes of interest were total fluoroscopy time and fluoroscopy time used for renal access. Secondary outcomes were stone-free rates (SFR), complication rates, procedure time, length of stay, and need for additional procedures. The independent samples t-test was used to compare continuous variables and the Chi-square test was used to compare categorical variables between groups, with p<0.05 considered significant.
Summary of Results: A total of 292 patients met inclusion criteria. Baseline patient characteristics were similar between groups. There was no significant difference in stone laterality, stone volume, and Hounsfield units, however there was a higher percentage of staghorn calculi in the Laser DARRT group (84.6% vs 67%; p=0.001). The Laser DARRT technique resulted in significantly lower total fluoroscopy time (21.8 vs 597.7 sec; p<0.001) and fluoroscopy time for access (10.8 vs 551.7 sec; p<0.001). There was no significant difference in total procedure times (178, 186 minutes; DARRT vs Fluoroscopy respectively p=0.4), length of stay (57.4, 62.4 hours; DARRT vs Fluoroscopy respectively p=0.4), blood loss (91.3, 87.3 mL; DARRT vs Fluoroscopy respectively p=0.7), or complication rates between groups. SFR was significantly higher for the Laser DARRT group (84.1% vs 64.1%; p<0.001).
Conclusions: Laser DARRT reduced mean renal access fluoroscopy time by 98% and total fluoroscopy time by 96.4% during PCNL. Despite reduced fluoroscopy time, laser DARRT had higher stone-free rates and similar operative times, estimated blood loss, and complication rates. The use of laser DARRT for renal access represents a promising option for surgical treatment of patients with large kidney stones.
# 462
Page Kidney, An Incidental Finding while Evaluating Perinephric Hematoma
Sharma R1,2, Yanni T1,2, Moosavi L1,2. 1Kern Medical Center, Bakersfield, CA and 2David Geffen School of Medicine, Los Angeles, CA
Case Report: Page kidney is a rare cause of secondary hypertension with 100 reported cases in the literature since 1991. Compression of the renal parenchyma by perirenal collagenous hulk results in a decrease in intrarenal arterial pressure leading to microvascular ischemia and decreased renal perfusion pressure. Herein presented is a patient who developed page kidney three years post a nephroureteral stent placement which was discovered incidentally during workup for a perinephric hematoma.
Middle-aged female with history of right ureteral stent 2/2 hydronephrosis presented to the ED with nausea, vomiting, and sudden right lower quadrant and right flank pain x1 day. CT abd/pelvis w/contrast revealed large right perinephric hematoma along with presence of right nephroureteral stent. The 11x7x13cm perinephric collection was heterogenous and hyperdense raising concern for perinephric hematoma versus perinephric absces. The patient was initiated on ceftriaxone and metronidazole given the possibility of an abscess. Imaging confirmed right perinephric hematoma with capsular distension of the fibrocollagenous hulk surrounding the kidney resulting in page phenomenon. Throughout the patient’s hospital course, she remained hemodynamically stable with preserved kidney function, without any notable bleed or low hemoglobin levels. On discharge, the patient’s hemoglobin and creatinine were within normal limits. Additionally, patient was found to be hypertensive with readings of SB>140 mmHg requiring intervention. The patient was discharged on lisinopril 10mg in stable condition.
It is postulated that the patient’s fibrous capsule formed due to chronic inflammatory changes due to her indwelling double-J catheter. They are usually removed within 6 weeks of placement however, this patient’s catheter was present for three years and resulted in significant calcification surrounding it. In this case, conservative symptomatic management with lisinopril combated the hyperreninemia and allowed her to return to a normotensive state. Further treatment decision will continue to evolve as the size of the hematoma and the compressive effects of it and the capsule are tracked.
# 462A
Renal Replacement Therapy Decreases Mortality in Alcohol-Associated Liver and Kidney Failure: A Bridge to Survival
Kulig CS1, Nadeau KJ2, Kulig CC3. 1George Washington High School, Denver, CO; 2University of Colorado, Aurora, CO and 3Presbyterian/St. Luke’s Medical Center, Denver, CO
Purpose of Study: Typically people with alcohol-associated liver failure complicated by kidney failure, who are not transplant candidates, have extremely high mortality. Renal Replacement Therapy (RRT) to address acute kidney injury (AKI) may allow time for alcohol-associated liver failure to improve to allow liver and kidney function to improve without transplant, thus decreasing mortality. However, the existing data are limited and lack a control group not receiving RRT. We hypothesized that RRT would improve survival in adults with co-existing alcohol-associated liver failure and AKI.
Methods Used: We performed a retrospective chart review of electronic medical records at a single transplant center to collect data on adults admitted to the hospital with both AKI with an indication for RRT, and alcohol-associated liver failure. Patients were stratified by those who did or did not receive dialysis. Group differences were compared with a Chi-squared or student’s T-test and Spearman’s correlation coefficients to look for factors that were associated with post-RRT survival.
Summary of Results: 41 patients were identified; 33 (80%) underwent RRT and 9 (20%) did not. Participant data is displayed in the Table. Survival was significantly higher in the group who received RRT (66%) vs. those not receiving RRT (0%) (p=0.0009). Of those who survived, 59% survived without needing a transplant and no longer needed RRT after discharge, 23% survived to receive a liver transplant and no longer needed RRT, and 18% survived without needing a transplant and were discharged from the hospital but continued to need RRT. The average length of follow-up in those still alive was 1.8+/ 2.2 years. Those who did not receive RRT were on average 51.5 +/- 10.2 years of age and had on average 2.8 +/- 3.4 months of sobriety prior to admission vs. an average age of 40.8 +/- 12.8 years of age and 1.0 +/- 1.8 months of sobriety in those who received RRT. The average model for end-stage liver disease (MELD, i.e. liver disease severity) score was almost identical in those who did not vs. did receive RRT (40.9 +/- 5.1 vs. 41.0 +/- 4.7, p=0.929). There were no associations between survival and age, sex, or liver disease severity, but length of sobriety (r=-0.36, p=0.040) was negatively associated with survival.
Conclusions: RRT appears to reduce mortality in patients with co-existing alcohol-associated liver and kidney failure who are not transplant candidates, regardless of age, sex or severity of liver disease, and thus could be widely implemented. Future studies should follow a larger group of patients prosepctively to further assess factors predictive of survival following RRT in this high-risk population.
Participant Characteristics.
Overall Cohort (n=41)
No RRT (n=8)
RRT (n=33)
P-value Comparing No RRT to RRT
Age (years)
42.9 +/- 13.0
51.5 +/- 10.2
40.8 +/- 12.8
0.033
Sex (% female)
22 (53.7%)
4 (50%)
18 (56%)
0.766
Sobriety Duration (months)
1.4 +/- 2.3
2.8 +/- 3.4
1.0 +/- 1.8
0.061
Length of Survival Since RRT (years)
n/a
1.8 +/- 2.2
0 +/- 0
0.00018
Maximal MELD Score
41.0 +/- 4.8
40.9 +/- 5.1
41.1 +/- 4.7
0.929
Survival (n,%)
22 (54%)
0 (0%)
22 (66%)
0.0009
RRT-free Survival to Discharge (n,%)
13 (32%)
0 (0%)
13 (59%)
0.0031
RRT-free Survival and Transplanted (n,%)
5 (12%)
0 (0%)
5 (23%)
0.138
Survival on RRT (n,%)
4 (19%)
0 (0%)
4 (18%)
0.200
Death (n,%)
19 (46%)
8 (100%)
11 (33%)
0.0008
Discharge to Hospice (n,%)
10 (24%)
5 (63%)
5 (45%)
0.367
Death in the Hospital (n,%)
9 (22%)
3 (37%)
6 (55%)
0.367
Table Key: Data are displayed as mean +/- SD or as n (percentage). P-value was determined by a t-test for continuous variables and by Chi-square test for categorical variables. Table abbreviations: MELD = model for end-stage liver disease, RRT = renal replacement therapy.
Shin BJ1,2, O’Neil SH2,3, Dhanani S2,4, Baron Nelson M2,5. 1Kansas City University, Joplin, MO; 2Children’s Hospital Los Angeles, Los Angeles, CA; 3Children’s Hospital Los Angeles, Los Angeles, CA; 4Lucile Packard Children’s Hospital Stanford, Palo Alto, CA and 5Keck School of Medicine at USC, Los Angeles, CA
Purpose of Study: Brain and spinal cord tumors are the most common childhood cancer - accounting for approximately 1 out of every 4 childhood cancers. Among these, 54 to 70% of all pediatric brain tumors are located in the posterior fossa. Previous studies have focused on the impact of treatment on children diagnosed with posterior fossa tumors, specifically from the combined effects of surgery, chemotherapy, and irradiation. In our research, we investigated changes in brain volume in the putamen, thalamus, and hippocampus amongst patients who received two levels of treatment - patients receiving only surgery and patients who were treated with surgery, chemotherapy, and cranial irradiation (CRT) and compared them to healthy sibling controls. In addition, we conducted neuropsychological assessments to determine cognitive abilities, memory, and attention outcomes associated with the different treatment modalities.
Methods Used: Thirty-six children, aged 6 to 17, with a history of posterior fossa tumor (17 treated with surgery; 19 with surgery, chemotherapy and CRT) underwent neuroimaging and neuropsychological assessment a minimum of 1 year after treatment, along with 15 healthy sibling controls who all had magnetic resonance imaging (MRI) with diffusion tensor imaging (DTI) done (n=51). The putamen, thalamus, and hippocampus were manually segmented on each participant’s MRI (Fig. 1) and in the radiation treatment group, the radiation dose for each structure was calculated. All subjects underwent neuropsychological evaluation.
Summary of Results: Block Design scores of both patient groups were lower than those of the controls, with the group who underwent surgery, chemotherapy, and CRT scoring lowest (p<0.001). Scores on Memory for Designs content were lower in the patient surgery group than the surgery, chemotherapy, and CRT group (p=0.03), and Symbol Search scores were lower in the surgery, chemotherapy, and CRT group than in the surgery group (p=0.01) (Table 1). Patients who underwent surgery, chemotherapy, and CRT had the lowest thalamic volumes of all groups when controlled for age (p=0.02). Diffusion tensor imaging values did not reflect microstructural brain injury in patient groups compared to controls.
Conclusions: Posterior fossa tumor treatment alters thalamic volume, with patients who received surgery, chemotherapy, and CRT having the greatest affected volume. Neuropsychological assessments also demonstrated decreased processing speed, visuoconstruction, and visual learning scores between patient groups and in all patients compared to healthy sibling controls.
THE RESPONSES OF MOTOR NEURON AND OLIGODENDROCYTE PROGENITORS AFTER SPINAL CORD INJURY
Zhou Y, Arena K, Appel B. University of Colorado School of Medicine, Aurora, CO
Purpose of Study: Near 300,000 people in the U.S. suffer from spinal cord injury (SCI) with an average age of 43, and the lifetime cost of SCI is $1.2-5.0 million per person. SCI causes death of motor neurons and oligodendrocytes, leading to various functional deficits. During development, these cells are both differentiated from pMN progenitors, which originate from neural progenitors. In this study, we investigated the responses of these progenitors after SCI. A better understanding of the regeneration process will help develop new treatments to promote recovery of patients with SCI.
Methods Used: We used zebrafish as the model organism because of their powerful regeneration ability and great similarities in its nervous system with humans. Transgenic lines and immunohistochemistry were used to label Sox2 and Olig2, which are genetic markers for neural progenitors and pMN progenitors, respectively. A complete spinal cord transection was performed in zebrafish at 5 days post-fertilization by making a dorsal-to-ventral incision perpendicular to the spinal cord up to the dorsal margin of the notochord. The injured fish were imaged immediately after injury (0 DPI), one day post-SCI (1 DPI), and two days post-SCI (2 DPI) using static and timelapse confocal microscopy.
Summary of Results: Soon after SCI, static imaging revealed a dramatic decrease in both Sox2 and Olig2 signals at the injury site (A), suggesting cell death of neural progenitors and pMN progenitors caused by the injury. Furthermore, timelapse imaging showed a 55.6% loss of Sox2+ neural progenitors happening progressively during 3-8 hours after the injury (B). At 2 DPI, increased Sox2 and Olig2 signals were observed at the injury site (C), which indicated a regeneration of these two progenitor populations, and this increased number of progenitors remained stable during 48-50 hours post-injury (D).
Conclusions: Spinal cord injury initially resulted in progressive cell death of neural progenitors and pMN progenitors after the injury. Such cell loss was then followed by a repopulation of these cells at the injury site, and the number of the replenished progenitors reached a steady point by two days after injury. Together, these findings indicate a potential post-injury repair mechanism driven by the regeneration of neural progenitors and pMN progenitors that can differentiate into motor neurons and oligodendrocytes.
Sox2 and Olig2 signals at 0 DPI (A) and 2 DPI (C) in static imaging. Number of Sox2+ cells at 0 DPI (B) and 2 DPI (D) in timelapse imaging. Dashed lines: injury site.
# 465
PHYSICAL REHABILITATIONS WITH EVIDENCE OF OUTPERFORMING STANDARD OF CARE FOR TREATING CHRONIC TRAUMATIC BRAIN INJURY SYMPTOMS – A SYSTEMATIC REVIEW
Rhodes M1, Wood TR2. 1University of Washington, Seattle, WA and 2University of Washington, Seattle, WA
Purpose of Study: There are over 250,000 hospitalizations for traumatic brain injuries (TBIs) annually in the United States. 43% of these patients will develop chronic sequelae and need long-term treatment. A lack of large-scale trials or guidelines detailing symptom-specific physical rehabilitation approaches can make clinical decisions difficult, particularly as each TBI patient can present with a unique spectrum of symptoms. The purpose of this systematic review was to investigate the symptom-specific effects of multiple physical rehabilitation techniques compared to standard physical therapy (PT) in treating each of the most common chronic TBI symptoms.
Methods Used: PubMed, CINAHL Complete, and Embase were systematically searched using PRISMA protocol to find full text randomized controlled trials (RCTs) from 2003 or later that included PT as the control and an alternative physical rehabilitation as an intervention. Studies included participants who were over 16 years old and had a previous TBI, with outcome data for at least one of the following chronic symptoms: cognitive deficits, balance deficits, fatigue, mood changes, and headaches or sleep disturbances. All included studies were assessed for Level of Evidence (LoE) using a standardized rubric.
Summary of Results: A total of 29 studies met full inclusion criteria. Physical rehabilitations with at least one included study were aerobics (running, walking, or aquatic), vestibular therapy, virtual reality with a stationary bike or treadmill (VR), tai chi, yoga, and weight supported treadmill walking (WSTW). Cognitive: Moderate evidence (at least one high LoE RCT) supports aerobic exercise outperforming PT in treating cognitive symptoms. Weak evidence (consistent results across multiple low LoE RCTs) supports the use of VR over PT. Balance: Moderate evidence supports the use of vestibular therapy over PT but no difference for either aerobics or VR. Two low LoE studies showed no difference between WSTW and PT, but in another low LoE trial the WSTW group was significantly worse. Fatigue: Moderate evidence supports the use of aerobics over PT. Mood: Weak evidence supports tai chi outperforming PT. Moderate evidence supports no difference between either aerobics or vestibular therapy compared to PT. Headaches: Moderate evidence supports no difference between either aerobics or vestibular therapy compared to PT. Sleep disturbances: Weak evidence supports no difference between either aerobics or yoga compared to PT.
Conclusions: There is evidence that for TBI patients with chronic cognitive, balance, fatigue or mood related symptoms, alternative physical rehabilitations are at least as effective as PT. These treatments warrant further evaluation and potential consideration for patients who cannot access or are not responding to standard PT. Overall, there remains a need for more randomized controlled trials in this field, particularly high LoE studies, to further develop targeted symptom-specific therapies for treating chronic symptoms in TBI populations.
# 466
RACIAL DISPARITIES IN THE TREATMENT OF CHILDREN WITH MODERATE TO SEVERE MIGRAINES
Dingle K1, Arumani R1, Bae E1, Ceja Ruiz L1, Kankanala P1, Leal M1, Saraf S1, Afghani B1, 2. 1UC Irvine School of Medicine, Irvine, CA and 2CHOC Hospital of Orange County, Orange, CA
Purpose of Study: Previous studies have demonstrated disparities in the care of pediatric patients for various illnesses, but few have investigated ethnic or racial disparities in the treatment of patients with moderate to severe migraines. This study aims to determine whether ethnic or racial disparities exist in the treatment of migraines in the pediatric population.
Methods Used: We conducted a literature review using the online databases of PubMed and Google Scholar, using keywords: “ethnic disparities”, “pediatrics”, “migraine”, and “treatment”. Only studies of pediatric patients who required an emergency department (ED) visit or hospitalization for migraine headaches and included a comparison of treatment among different races were included in our review.
Summary of Results: We found four studies that met our inclusion criteria. All children presented with moderate to severe migraine headaches. Three studies involved patients who were seen in the ED, while one involved patients who were hospitalized. Children of minority race or ethnicity (e.g. Black, Hispanic) had decreased odds of receiving IV medications, such as diphenhydramine, dopamine antagonists compared to non-minority children. The use of institutional guidelines was associated with decreased use of opiates and increased use of appropriate medication directed towards treatment of migraines, but disparities persisted even after using the guidelines. Interestingly, the study involving children who were hospitalized (Masonbrink et al) found that non-Hispanic Black and Hispanic children, particularly those who were older, showed greater odds of receiving opioid treatment which is typically not a part of migraine treatment guidelines. This unique finding may be due to inconsistencies in the use of migraine guidelines, parental demands, or adjustments for different variables. All studies were also retrospective, which raises some limitations as there is a risk for misclassification and unknown information about factors that affected providers’ decisions such as misclassification bias, previous associated diagnoses, or pain scores.
Conclusions: Our literature review demonstrates the potential presence of disparities in treatment of migraines among pediatric patients who require ED visit or are hospitalized. Following institutional guidelines is helpful but does not eliminate disparities. Further prospective studies, controlling for other factors that may lead to differences in treatment, such as education, language, age, parental factors and pain severity are warranted to determine the precise variables that contribute to the disparity.
Treatment of migraines based on ethnicity.
First author and year published
Source of Study Subjects
Subject Demographics (Race)
Definition of Outcome
Comparison of Outcome (Percentages) Based on Management of Different Ethnicities/Groups
Outcome
Variables Adjusted For
Hartford et al., 2022
ED visits, Electronic medical records, Children, 2016-2020
N total=833nH-White (N=423)
Black (N=69)
Asian (N=35)
Hispanic (N=18)
IV +/- PO Group N=546PO only Group N=287
Oral/Intranasal vs IV therapy for migraine
Comparison of each race odds to the "grand mean"nHWhite: aOR=1.45 (95% CI 1.08-1.93)
Black: aOR=0.55 (95% CI 0.35-0.87)
Asian: aOR=0.50 (95% CI 0.27-0.92)
Hispanic: aOR=0.57, (95% CI 0.41–0.79)
Compared to non-Hispanic Whites, all other races had significantly lower odds of receiving IV treatment
Pain severity, age, gender, insurance type
Genadry et al. 2023
ED visits, Electronic medical records, Pediatric Health Information System, 32 hospitals, 2009 to 2019
N total=112,077
White (N=70,726)
Black (N=24,064)Asian (N=1084)
Use of opiods, dopamine receptor antagonists, and diphenhydramine
Dopamine antagonist treatment:White = Reference
Black: aOR=0.92 (95% CI 0.87-0.97)
Asian: aOR=0.87 (95% CI 0.74-1.04)
Diphenhydramine administration:
White = Reference
Black: aOR=0.86 (95% CI 0.81-0.91)Asian: aOR=0.87 (95% CI 0.72-1.04)
Black children showed decreased odds of receiving dopamine and diphenhydramine compared to White children
Age,gender, income, insurance type
Kellier et al., 2023
ED visits, Electronic medical records, Pediatric Health Information System, 2016 to 2021
N total=142,250
nH-White (N=58465)nH-Black (N=34424)Hispanic/Latino (N=38977)
IV treatment between nH-White, nH-Black and Hispanic/Latino youth
Comparison of percentage of each race receiving IV treatmentnH-White 54.2% [50.2–58.1%] vs
nH-Black 44.2% [40.9–47.6%]
Hispanic/Latino 43.7% [39.0–48.5%]; p<.001)
Non-Hispanic White children received more IV medications compared to non-Hispanic Black and Hispanic/Latino children
Age,gender, insurance type
Masonbrink et al., 2020
Hospitalized Patients, Pediatric Health Information Systems, 2016 to 2018
N total=6632nH-White (N=4243)
nH-Black (N=922)
Hispanic (N=984)
Asian American (N=78)Opioid administrationN=448
Opioid administration rates amongst children who were hospitalized for migraine
Comparison of each race odds to nH-White childrennH-Black: aOR = 1.86 (p < 0.001)Hispanic: aOR = 1.54 (p = 0.005)
Non-Hispanic Black and Hispanic children showed increased odds of opioid administration
Association Between Type II Diabetes Mellitus and the Development of Parkinson’s Disease
Jugnundan S1, Weaver F2, Caroline T3, Gonzalez B2, Colletta K2, 4, Goldman S1, 5. 1UCSF, San Francisco, CA; 2Veterans Affairs, Hines, IL; 3UCSF, San F Francisco, CA; 4Loyola University, Chicago, IL and 5Veterans Affairs, San Francisco, CA
Purpose of Study: The etiology of Parkinson’s Disease (PD) is still unclear. Type II Diabetes Mellitus (T2DM) has been inconsistently associated with increased risk of PD in prior reports. A causal association is biologically plausible. Insulin has a diverse range of physiological effects on neurons and glial cells, and plays an important role in mitochondrial homeostasis. T2DM mice manifest a loss of mitochondrial Complex I activity, a pathological hallmark of PD1. Insulin resistance decreases expression of peroxisome proliferator-activated receptor-gamma coactivator one alpha (PPARGC1A)1, which can lead to mitochondrial dysfunction, creation of reactive oxygen species (ROS), and ultimately cell death. This mechanism is believed to contribute to dopaminergic cell damage seen in PD, as well as pancreatic beta cell damage seen in T2DM2.
Methods Used: The cohort utilized in our study was initially established by the Agency for Toxic Substances and Disease Registry (ATSDR). It was comprised of 172,128 marines stationed at Camp Lejeune, NC and 168,361 marines stationed at Camp Pendleton, CA between 1975-1985. PD was ascertained by identifying all individuals with ICD-9 (332.0) or ICD-10 (G20) codes in the Veterans Health Administration (VHA) Corporate Data Warehouse (CDW) or Medicare between 1999-2019. PD diagnoses and incidence dates were confirmed by chart review. The diagnosis of T2DM was defined as having any of 250.x0, 250.x2 (ICD-9) or E11.x (ICD-10) coded at least twice.
430 individuals with PD were identified from the 158,123 cohort members who ever utilized VHA or Medicare services. We utilized a nested case control study design that matched 10 controls to each PD case on age, sex, race, and military rank. We considered only T2DM diagnoses that occurred before the PD diagnosis date for cases or the same reference date for their matched controls. We used conditional logistic regression to derive odds ratios (OR) and 95% confidence intervals (CI) for T2DM and PD adjusted for Camp (Lejeune or Pendleton). In sensitivity analyses we explored models that included smoking and total duration of VHA usage, and that restricted the population to those who were active VHA users prior to their reference date.
Summary of Results: 71/430 (16.5%) cases and 544/4300 (12.7%) of controls had a T2DM diagnosis before the reference date. In adjusted analyses, T2DM was associated with a significantly higher risk of PD (OR 1.37, 95%CI 1.21-1.79, p < 0.0001). Inclusion of smoking or VHA usage duration had minimal impact on ORs, whereas ORs were modestly stronger when we restricted analyses to those who were active VHA users prior to reference date (OR 1.58, 95%CI 1.37-1.83, p<0.0001).
Conclusions: These results add to a growing body of evidence that implicates T2DM as a risk factor for PD. Given its high population prevalence and potential modifiability, further elucidation of the mechanisms underlying the association of T2DM and PD is essential.
# 468
Late Onset Cobalamin C Disease in an adolescent patient of Mixteco ancestry and response to treatment
Navea H1, Hoyt E1, Fraser S1, Ehrreich S2. 1Valley Children’ Healthcare, Madera, CA and 2Valley Children’s Hospital, Madera, CA
Case Report: Cobalamin C (CblC) Disease is an autosomal recessive disorder caused by mutations in the MMACHC gene, and is the most common inborn error of Vitamin B12 metabolism. Presentation and age of onset varies with the severity of the disorder. The late-onset subtype is often associated with psychiatric and cognitive symptoms.
An 11-year-old male of Mixteco inheritance presented with 3 weeks of upper extremity dysmetria, lower extremity weakness, ataxia and subacute cognitive decline. MRI brain and spine showed T2 hyperintensity in the periventricular white matter and dorsal columns. Laboratory work up suggested CblC Disease, showing elevated plasma homocysteine (110.2 µmol/L), elevated propionylcarnitine (C3), elevated methylmalonic acid, and normal methionine. Treatment was initially with cyanocobalamin 1mg IM daily, then transitioned to hydroxocobalamin 25mg IM daily on day 19; betaine, folinic acid, and levocarnitine were subsequently added. Genetic testing confirmed the diagnosis, detecting two pathogenic variants on the MMACHC gene confirmed to be in trans (c.328_331del (p.Asn110Aspfs*13) and c.482G>A (p.Arg161Gln)). Repeat neuropsychiatric evaluation showed improved processing speed and greater task persistence and effort. His lower extremity weakness and gait continued to improve, being able to ambulate with minimal assistance.
# 469
Successful Treatment of Chiari Idiopathic Intracranial Hypertension Syndrome With Dural Venous Sinus Stent After Ventriculoperitoneal Shunt: A Case Report
Rauser S1, 2, Lee E1, 2, Wilson M1, 2, Hawy E2. 1Loma Linda University, Loma Linda, CA and 2Loma Linda University, Loma Linda, CA
Case Report: A 32-year-old female presented to the neuro-ophthalmology clinic with a 1.5-year history of headaches, rare transient visual obscurations, rare pulsatile tinnitus, and blurred vision. Upon examination, severe papilledema was found, and the patient was sent to the emergency department (ED) for imaging and was started on 500 mg twice a day (BID) of acetazolamide. Imaging at the ED revealed a dual diagnosis of idiopathic intracranial hypertension and Chiari malformation type 1. The patient underwent ventriculoperitoneal (VP) shunt placement due to the intolerance the patient had to acetazolamide. The patient received the VP shunt without complication. At the 7-month follow-up with neuro-ophthalmology, the papilledema and blurry vision resolved, and the acetazolamide was discontinued. However, the papilledema had recurred, and the Humphrey Visual Field (HVF) test had worsened at 10-months post-shunt, so the patient resumed acetazolamide and was sent to neurosurgery for further evaluation. At 11-months post-shunt, the headaches had returned and were worsening. The patient underwent dural venous sinus stent (DVSS) placement due to the presence of a pressure gradient of 13 mmHg in the right transverse sinus, and an 8 mm x 21 mm stent was placed, subsequently reducing the pressure gradient. Two months after the stent placement, the patient reported resolution of headaches, papilledema was resolved, and HVFs were stable. The stent was confirmed to be patent 6 months post-operatively. At 19.5 months after the stent placement, the patient is completely off acetazolamide and symptoms remain resolved.
Chari malformation type 1 with a cerebellar tonsillar descent 1.68 cm below the level of the foramen magnum.
# 470
NEONATAL INFLAMMATION AND NEAR-TERM WHITE MATTER MICROSTRUCTURE IN INFANTS BORN PRETERM
Anderson K1, Lazarus M1, Bruckert L1, Poblaciones R1, Scala M2, Marchman VA3, Feldman HM1, Travis KE1. 1Stanford University School of Medicine, Palo Alto, CA; 2Stanford University School of Medicine, Palo Alto, CA and 3Stanford University, Palo Alto, CA
Purpose of Study: Infants born very preterm (VPT: <32 wks gestational age (GA)) are at increased risk of abnormal white matter (WM) development and associated long-term neurocognitive impairments. Inflammation during the early neonatal period may contribute to differences in WM pathway development in the vulnerable VPT brain. Comparing VPT children with and without a history of serious neonatal inflammation, differences in the corpus callosum (CC) microstructure at age 6 years were observed. Studies have yet to examine whether similar microstructural differences exist in the neonatal period.
Objective: To contrast WM microstructure of the CC in VPT infants who did and did not experience serious neonatal inflammation using near-term diffusion magnetic resonance imaging (dMRI).
Methods Used: A retrospective study of VPT infants (n=154) born at GA 22-32 wks between March 2016 to March 2020 was performed. Using medical chart review, the cohort was divided into two groups: VPT infants who experienced > 1 major neonatal inflammatory condition (bronchopulmonary dysplasia, necrotizing enterocolitis, or sepsis = I+) and VPT infants who did not (I-). Per standard of care, all infants underwent an MRI brain scan that included dMRI prior to hospital discharge (post-menstrual age (PMA) at scan 34-45 wks). The CC was segmented into 7 regions. Mean fractional anisotropy (FA) was calculated for each segment. We analyzed group differences and performed linear regressions to assess the unique contribution of neonatal inflammation to FA after controlling for GA and MRI PMA.
Summary of Results: Table 1 shows group characteristics. GA and birthweight are significantly lower for the I+ group, while MRI PMA is significantly higher. figure 1 presents a comparison of mean FA values across the CC segments between groups. Significant differences were found in the occipital and temporal segments. In regression models, GA was a significant predictor of FA in all CC segments after controlling for MRI PMA. When accounting for both MRI PMA and GA, inflammation did not uniquely predict variability in FA.
Conclusions: VPT infants who experienced neonatal inflammation had lower FA of the posterior segments of the CC than VPT infants who did not. However, this difference may be attributed to lower GA . On-going analysis will explore whether neonatal inflammation moderates relations between WM microstructure and early neurodevelopmental outcomes.
Comparisons of infant characteristics by group (n=154).
Note: Insurance type (public vs. private) was used as a proxy for socioeconomic status; IQR = Interquartile range, * p<0.001.
# 471
A RETROSPECTIVE CHART REVIEW ASSESSING THE OUTCOMES OF DURAL SINUS VENOUS STENTING IN IDIOPATHIC INTRACRANIAL HYPERTENSION PATIENTS
Lee E1, Rauser S1, Wilson M1, Hawy E2. 1Loma Linda University, Loma Linda, CA and 2Loma Linda University, Loma Linda, CA
Purpose of Study: Idiopathic Intracranial Hypertension (IIH) is a condition characterized by elevated intracranial pressure associated with symptoms such as papilledema, headache, migraine, pulsatile tinnitus, and transient visual obscurations (TVO) that affects women of childbearing age. Currently, treatment for IIH commonly includes acetazolamide usage and cerebrospinal fluid (CSF) shunt placement. Acetazolamide is contraindicated in pregnancy and associated with many unfavorable side effects and shunts are considered an undesired brain surgery by many patients due to risks and potential side effects. Dural venous sinus stenting (DVSS) is an alternative procedure that is being explored in the treatment of IIH. This study aims to analyze the post-operative effect of DVSS on quality of life of patients with IIH through assessment of symptoms and acetazolamide dosage and to add to the pool of existing literature on DVSS for IIH.
Methods Used: Charts of 15 patients who have undergone DVSS from April 2020 to April 2023 were retrospectively reviewed. Age, sex, lumbar puncture opening pressure, pressure gradient of the stenosis, and location of stenosis were recorded for each patient. Additionally, acetazolamide dosages in mg/day and retinal nerve fiber layer (RNFL) thickness in µm were recorded at baseline, pre-stent, and post-stent. RNFL thickness was obtained via Optical Coherence Tomography (OCT). Patient outcomes recorded include headaches, visual symptoms, papilledema, and pulsatile tinnitus, with these being recorded as either worsened, stable, or improved as compared to baseline if they were present then. The Wilcoxon signed-rank test was performed to determine the significance of acetazolamide dosages change and OCT RNFL thickness at post-stent compared to baseline and pre-stent.
Summary of Results: All 15 of the patients reviewed were women with a mean age of 37.7 and a median age of 36. There was a statistically significant difference in acetazolamide dosage between baseline and post-stent measurements (p=0.02) as well as between pre-stent and post-stent measurements (p=0.025). There was also a statistically significant difference in OCT RNFL right eye thickness between baseline and post-stent measurements (p=0.0069) as well as between pre-stent and post-stent measurements (p=0.028). The difference between baseline and post-stent OCT RNFL left eye thickness was significant (p=0.018), but the difference between pre-stent OCT RNFL left eye thickness was not significant (p=0.36). Post procedurally, headaches improved in 78.6%, migraines improved in 37.5%, papilledema improved in 100%, pulsatile tinnitus improved in 45.4% of patients, and TVOs improved in 100% of patients that had these symptoms prior to stenting.
Conclusions: This study supports the use of dural venous sinus stenting as a tool to improve quality of life of people with IIH, especially in women of childbearing age, through the decrease or cessation of acetazolamide therapy and the improvement in symptoms such as headache and papilledema.
Surgery IV
Concurrent Session
10:15 AM
Friday, January 19, 2024
# 472
THE IMPACT OF STERILIZING IRRIGANTS ON THE TENSILE STRENGTH OF SILICONE BREAST IMPLANTS: A COMPARATIVE STUDY FOR INTRAOPERATIVE USE
Thomas LE1, Carlson PF1, Small EA1, Gupta S2. 1Loma Linda University, Loma Linda, CA and 2Loma Linda University, Loma Linda, CA
Purpose of Study: Many solutions may be used in breast implant surgery as a part of the wound irrigation to the breast implant and surgical field to remove debris, bacteria, and other contaminants to reduce the risk of infection and promote healing. Currently, there is no conclusive study to assess breast implant strength after prolonged exposure to the various solutions used during a breast implant operation. The purpose of the study is to determine the impact of these solutions on breast implant shell integrity based on immersion time during operative techniques.
Methods Used: Silicone implants were divided into 21 equal pieces, each measuring 2 inches x 2 inches. As a standard control, one-third of the implant shell tensions were measured with saline solution immersed for 60 seconds. Another group of implants, the intraoperative control group, were rinsed for 60 seconds with a three-antibiotic containing solution typically used to irrigate the breast pocket. The remaining implants were immersed in a dilute chlorhexidine solution (Irrisept®) for the standard 60 seconds according to the manufacturer’s instructions. After rinsing, these implants were calibrated to the tensiometer. To measure the tension of each implant, a small slit was cut in the center of the implant square. One end of the implant was hooked through this slit, while the other end was clamped to the base. Tension was measured in Newtons over a displacement of 0.9 inches.
Summary of Results: The average tensions of the implant shells in saline solution, triple antibiotic solution, and chlorhexidine solution were 8.93 N, 8.24 N, and 7.89 N respectively. Using a two-tailed T-test, the p-value between the saline solution and triple antibiotic was 0.071. The p-value between the triple antibiotic and chlorhexidine solution was 0.217. The p-value between the saline solution and chlorhexidine solution was 0.013.
Conclusions: While the observed differences between the group of saline vs. triple antibiotic and triple antibiotic vs. chlorhexidine solution were not statistically significant, there was a statistically significant result between saline vs. chlorhexidine solution. We do not know the potential implications that chlorhexidine solution may have on the integrity of the silicone breast implant once placed in a patient. While chlorhexidine solution is effective at reducing the risk of infection in various surgical procedures, its use with silicone breast implants needs to be weighed against the triple antibiotic solution, due to the risk of decreased implant tensile strength. Further studies would increase the sample size of silicone implant shells. Antibiotic solutions designed specifically for surgical implant procedures may offer a safer alternative by targeting bacterial infections directly while minimizing the risk of harm to the implants themselves. Surgeons should exercise caution and consider alternative options when selecting irrigation solutions for breast implant surgeries to ensure the best possible outcomes for patients.
Tensions of Silicone Implants in Various Solutions.
60 seconds saline
60 seconds triple antibiotic
60 seconds chlorhexidine solution
Trial 1
8.3
9.1
7.7
Trial 2
8.6
8.4
8.3
Trial 3
9.4
8.1
8.0
Trial 4
9.7
7.9
7.3
Trial 5
8.4
7.5
7.6
Trial 6
9.2
8.4
9.0
Trial 7
8.9
8.3
7.3
Average
8.93
8.24
7.89
# 473
CHARACTERIZATION OF THE MICROBIAL POPULATION IN INFECTIONS PRODUCING FAILED BREAST CANCER RECONSTRUCTION
Carlson PF1, Thomas LE1, Small EA1, Gupta S2. 1Loma Linda University School of Medicine, Loma Linda, CA and 2Loma Linda University, Loma Linda, CA
Purpose of Study: Implant-related infections present a challenge for reconstructive surgery, often resulting in complications and suboptimal outcomes. Exploring the microbial diversity in unsuccessful breast reconstruction cases holds great promise, offering essential insights into implicated bacteria, their resistance patterns, and susceptibility to common antimicrobials. With the rise in antibiotic-resistant bacteria, this study aspires to analyze microbial populations in colonized breast reconstructions, their resistance to various antibiotics and the implications for future treatment strategies.
Methods Used: A review of records from the Loma Linda University Plastic Surgery Morbidity and Mortality between 2013-2022 identified 45 cases involving the removal of breast implants or tissue expanders linked to infections in breast reconstruction. Data was collected on infection site cultures and antibiotic resistance.
Summary of Results: There was a prevalence of Staphylococcus Aureus (40%) and Pseudomonas Aeruginosa (16%) positive cultures. A subset of cases (29%) exhibited no growth. The antibiotics with the most cases of resistance among the microbial strains tested were Penicillin, Cefazolin, Oxacillin, Erythromycin, and Amoxicillin/Clavulanate, exhibiting resistance rates of 35%, 20%, 18%, 16%, and 18%, respectively. Among evaluated antimicrobial agents, Trimethoprim/Sulfa, Gentamicin, Rifampin, and Linezolid displayed the highest sensitivities (36%, 33%, 33%, and 31%, respectively) to the microbial strains. Cefazolin and Oxacillin displayed mixed profiles of high resistance and high sensitivity. Cefazolin demonstrated a resistance rate of 20% alongside a sensitivity rate of 20%. Oxacillin exhibited an 18% resistance rate and a 25% sensitivity rate.
Conclusions: As fear of antibiotic resistance increases, selection of effective antibiotics for treatment is paramount. Among the antibiotics investigated, Linezolid and Rifampin exhibited optimal sensitivities, and displayed the lowest resistance percentages. Linezolid and Rifampin are helpful in the treatment of gram-positive microorganisms, with Rifampin becoming increasingly useful for treatment of MRSA forming biofilms. Vancomycin is one of the more frequently prescribed antibiotics for severe infections; however, it exhibited relatively modest sensitivity rates. Trimethoprim/Sulfa had high sensitivity but showed minor resistance to some strains. Antibiotics such as Penicillin, Amoxicillin/Clavulanate, Cefazolin, and Oxacillin may warrant caution among physicians, given their relatively higher resistance rates despite fewer sensitivities. Physicians must also assess the potential side effects of various antibiotics when making the final treatment decision. In the broader healthcare context, understanding microbial characterization can aid in the rapid treatment of infections by enhancing success rates, conserving resources, and streamlining treatment.
# 474
Which is the Most Accurate Method for Assessing Stone Volume: Enterprise Imaging, 3D-Slicer, or Scalene Ellipsoid Formula?
Sajdak G1, Baldwin D2, Farkouh A1, Hanessian KA1, Kim U1, Quines JF1, Crew R1, Okhunov Z1, Amasyali AS1, Baldwin D1. 1Loma Linda University Medical School, Loma Linda, CA and 2Southern Adventist University, Collegedale, TN
Purpose of Study: One in ten people will have a renal stone in their lifetime with a recurrence rate of 50%. Knowing renal stone volume is essential for treatment selection and predicting outcomes. It also is strongly associated with stone-free rates. Numerous methods for stone volume assessment exist in the literature including the scalene ellipsoid formula (SEF) and DICOM analysis software. However, the optimal method for assessing stone volume has not been determined. This study compared the accuracy, precision, and convenience of the novel Enterprise Imaging (EI) to the conventional SEF and the DICOM analysis software “3D slicer” (3DS).
Methods Used: Using a 3D printer, a silicone kidney was reconstructed from a patient’s CT scan. Five artificial BegoStones were then created (calcium oxalate density). Stones included one 12 mm diameter sphere (1.11 cm3), two 12 mm diameter spheres (2.14 cm3), 21 mm cylinder (0.91 cm3), one 25 mm irregular pyramid (8.5 cm3), and an 68 mm stagohorn stone (51.5 cm3). Gold standard volume determination was made via water displacement and was compared to EI, 3DS, and SEF volume measurement. Scans were performed on a GE Discovery CT750 HD 64 (120 KVP at 250 ma with a 0.7 rotation time and thickness of 1.25 mm). Ten subjects determined stone volume via EI, 3DS kidney stone volume extension, and SEF. Accuracy, validity, precision, and inter-rater reliability were compared for each method. Subjects also rated method convenience using a Likert scale of 1-10 with 10 indicating the most convenient.
Summary of Results: EI demonstrated the lowest mean relative error with 4.9% compared to 10.2% with 3DS and 43.8% for the SEF (p<0.001). All three methods were valid in assessing stone volumes (R2 = 0.982, 0.991, and 0.999 for SEF, 3DS, and EI, respectively). There was also high interrater reliability for all three methods (ICC= 0.986, 0.993, and 0.999 for SEF, 3DS, and EI, respectively). EI was significantly more precise compared to 3DS and SEF for all stone shapes (p<0.05 for all). EI was the most convenient (8.5) compared to SEF (6.6) and 3D Slicer (3.6; p<0.001).
Conclusions: Enterprise Imaging is significantly more accurate and precise for the assessment of kidney stone volume than 3D slicer and the scalene ellipsoid formula. This represents a significant advance in kidney stone burden assessment given its accuracy, precision, and ease of use. In addition, use of Enterprise Imaging during research studies could facilitate standardization of reporting and balanced comparisons.
# 475
Analyzing Supervised Machine Learning Models for Prediction of Endoleaks Following Endovascular Aortic Aneurysm Repair
Roh D, Cabrera AJ, Mezan R, Tomihama RT, Kiang SC. Loma Linda University, Loma Linda, CA
Purpose of Study: The purpose of this study was to evaluate the performance of various supervised machine learning algorithms to predict the occurrence of endoleaks following endovascular abdominal aortic aneurysm repair.
Methods Used: This IRB-approved retrospective study analyzed the demographic and clinical data of 72 patients with endoleak and 72 propensity-matched control patients with no endoleak. Seven machine learning models were selected: random forest, gradient boosting, decision tree, support vector machine, gaussian-naïve Bayes, multi-layer perceptron, and logistic regression. Sixty-four clinical and demographic variables were used as the feature matrix, which was standardized between a scale of 0 and 1 for continuous and categorical variables. The data was split 70:30 amongst the training and testing sets, respectively. The training data was inputted into each machine learning model with their respective preset hyperparameters. Then, the testing data was analyzed by each trained model, and the predictions of each of the models were compared with the ground truth. The sensitivities, specificities, confusion matrices, and AUC curves were then calculated.
Summary of Results: Initial results demonstrated that all seven models performed with AUCs ranging from 0.39 to 0.51. A permutation feature importance (PFI) was performed on the 64 clinical data points that significantly improved the AUC of the models. Smoking, ASA, and COPD had the highest average feature importance for all models, with an average improvement of 0.123. After PFI was implemented, the Random Forest Classifier was the best-performing model, with a sensitivity of 48%, a specificity of 74%, and an AUC improvement from 0.39 to 0.65.
Conclusions: Based on the clinical variables identified through the utilization of a PFI methodology, machine learning algorithms were able to further optimize predictive capacity in detecting endoleaks. Using PFI, we can identify the clinical data points that most significantly impact the performance of each model, leading us to optimize each model to identify the model that will best predict the occurrence of endoleaks after EVAR.
ROC curve of supervised machine learning models used to predict endoleaks after being optimized with permutation feature importance.
# 476
PRENATAL ULTRASOUND RISK FACTORS PREDICTIVE OF POSTERIOR URETHRAL VALVES
Cooper PA1, Lin S1, Farkouh A2, Kuang R2, Thaipejr T1, Pearce J2, Song S2, Cheng K2, Chamberlin D2, Chamberlin J2, 1. 1Loma Linda University School of Medicine, Loma Linda, CA and 2Loma Linda University Medical Center, Loma Linda, CA
Purpose of Study: Prenatal hydronephrosis (PNH) refers to dilation of the fetal renal pelvis and collecting system, and is found in up to 2% of pregnancies. While the majority of prenatal hydronephrosis cases resolve spontaneously postnatally, persistent PNH may be reflective of a serious obstructive etiology, such as posterior urethral valves (PUV). PUV can lead to significant complications including renal failure, dialysis, and kidney transplants. Therefore, early and accurate diagnosis of PUV is prudent. Current American Urology Association (AUA) guidelines recommend a screening voiding cystourethrogram (VCUG) in infants with high grade hydronephrosis to rule out obstruction due to PUV. Because VCUG can be invasive, uncomfortable and exposes children to ionizing radiation, we sought to optimize the utility of renal bladder ultrasound (RBUS) in aiding the diagnosis of PUV. We hypothesize that male infants with PUV have additional findings on renal bladder ultrasound (RBUS) that may be diagnostic for PUV.
Methods Used: We reviewed a prospectively maintained PNH database that included children diagnosed with PNH at a single institution. Inclusion criteria included the AUA screening guidelines for males with high grade hydronephrosis. We included all males with history of PNH, post-natal RBUS performed, unilateral high grade hydronephrosis (SFU 3-4), and VCUG to confirm or exclude diagnosis of PUV. Postnatal RBUS were evaluated for the following findings: highest SFU grade (grade 3 or 4), renal dysplasia, presence of bilateral hydronephrosis, hydroureter, or bladder trabeculations. The primary outcome of interest was diagnosis of PUV determined from VCUG. Secondary outcomes included presence of reflux and the grade of reflux on VCUG. Chi-square analysis compared findings between males with high grade PNH and PUV, to those without PUV.
Summary of Results: A total of 25 male infants with PUV were included and compared against 60 males without PUV, and with high grade hydronephrosis. Males with PUV were significantly more likely to have additional findings on RBUS compared to those without PUV. These findings included the highest SFU grade being 4 (96% vs 63.3%; p=0.002), presence of bilateral hydronephrosis (100% vs 41.7%; p<0.001), presence of hydroureter (92% vs 23.3%; p<0.001), renal dysplasia (88% vs 1.7%; p<0.001), bladder trabeculations (96% vs 5%; p<0.001). In addition, males with PUV were significantly more likely to have VUR (64% vs 15%; p<0.001) and were significantly more likely to have grades 4-5 reflux (48% vs 10%; p<0.001).
Conclusions: Compared to patients without PUV, patients with PUV were found to have significant additional findings on postnatal RBUS including bilateral high-grade hydronephrosis, hydroureter, renal dysplasia, and or bladder trabeculations. Utilization of these factors may be considered in the evaluation of patients with prenatal hydronephrosis and screening for VCUG.
# 477
INVESTIGATING PATIENT EXPECTATIONS, SATISFACTION, AND PATIENT-REPORTED OUTCOMES FOLLOWING SPINE SURGERY
Edalati K1, 2, Wilson PL1, 2, Bansal A1, Louie PK1. 1Virginia Mason Franciscan Health, Seattle, WA and 2University of Washington School of Medicine, Seattle, WA
Purpose of Study: Back pain is a pressing health issue, leading to significant healthcare use and reduced quality of life. With a surge in spine surgeries, evaluating safety and effectiveness is crucial. Patient-reported outcomes (PROs) like quality of life and disability provide valuable insights. Patient expectations about surgery outcomes often mismatch with reality, impacting satisfaction. This study explores the link between patient expectations, satisfaction, and PROs post-spine surgery. We analyzed standardized PROs, investigating preoperative expectations-outcomes correlation, the gap between expected and actual quality of life, and the interplay between satisfaction and reported quality of life.
Methods Used: This prospective cohort study gathered data from eligible patients at Virginia Mason Franciscan Health who underwent elective minimally invasive lumbar surgery, excluding those with specific conditions. Variables encompass pre- and post-operative aspects. Questionnaires captured demographics, expectations, Visual Analog scale (VAS) for leg and back pain, and Oswestry Disability Index (ODI) scores. MODEMS surveys assessed preop expectations and postop satisfaction. Statistical analysis using SPSS software involved multivariate Spearman ordinal correlation for preoperative expectations and overall health outcomes.
Summary of Results: The preliminary data collected from 13 patients indicate that pain relief is the primary expectation patients have from the surgery (mean Likert score 4.5). In contrast, the expectation to return to work is the least concern (mean Likert score 3.8). Correlation analysis revealed a significant relationship between sleep improvement and pain relief (r=0.815, p=0.001). Additionally, the expectation for sleep improvement was a strong predictor for expectation in daily activity improvement (r=0.655, p=0.021), return to exercise (r=0.739, p=0.006) and return to work (r=0.729, p=0.007). Among 6 patients with ODI, the mean ODI score was 48.1, indicating severe disability, while the mean VAS score for lower back and leg pain was reported to be 5.5 and 3.0, respectively, indicating moderate and mild pain severity.
Conclusions: The aim of this study was to explore the link between patient expectations, satisfaction, and PROs following spinal surgery. Our preliminary findings from 13 patients revealed a focus on pain relief over return to work. Severe disability (ODI score of 48.1), underscores the challenges patients face. Correlation analysis uncovers a strong link between sleep improvement and pain relief, suggesting that those expecting pain relief also anticipate enhanced sleep quality post-surgery. Furthermore, the expectation of improved sleep strongly predicts enhanced daily activity, exercise resumption, and return to work expectations. This study underscores the importance of clear preoperative expectations. Open discussions can refine patient preferences, boost satisfaction, and accelerate recovery.
# 478
Antegrade Pyeloperfusion for Percutaneous Thermal Ablation of Renal Masses
Oliinik M, Smith J. Loma Linda University, Loma Linda, CA
Purpose of Study: This abstract aims to present a case series highlighting the successful use of percutaneous antegrade pyeloperfusion with warm saline during cryoablation procedures. The educational goals are to demonstrate the technical feasibility of this approach, discuss its benefits in terms of procedural efficiency, and emphasize its role in protecting the renal collecting system. Percutaneous thermal ablation of renal masses is a standard treatment for renal masses. However, one rare complication unique to thermal ablation is injury to the ureter or renal pelvis. Pyeloperfusion with saline has been employed during percutaneous ablation to prevent thermal injuries. However, this technique requires added time, expense, and coordination between Urology and IR. We have a case series of successful pyeloperfusion from a purely percutaneous approach in C.T.
Methods Used: Out of a series of 313 patients who underwent percutaneous renal ablation over a 19.5 year period, 13 patients received warm saline pyeloperfusion to protect the collecting system during cryoablation of renal lesions averaging 3.7 cm (3.5-6.5 cm). Four patients underwent antegrade pyeloperfusion, and 9 underwent retrograde pyeloperfusion. Percutaneous access for perfusion took about 30 min on the CT table. Patients undergoing retrograde access had their access performed in either a cath lab before transporting to CT suite (n=2) or on a gurney in CT suite before transferring to the CT table (n=7).
Summary of Results: A self-limited urine leak occurred in one patient undergoing percutaneous perfusion, and one patient who underwent retrograde perfusion suffered a pulmonary embolus one day post ablation which was treated with anticoagulation. Two patients in the retrograde group had no imaging follow-up available in the EMR for review, one patient had recurrent and progressive disease on initial CT follow-up, while the remaining 10 patients had no evidence of recurrence on imaging with average follow up of 2.9 years (0.25-11.5).
Conclusions: In this study, percutaneous antegrade pyeloperfusion with warm saline is demonstrated to be a feasible and effective approach for protecting the renal collecting system during cryoablation of small renal masses. The technique not only offers a means to prevent damage to the renal collecting system but also avoids the need for collaboration with Urology for retrograde ureteral perfusion. This percutaneous approach, when coupled with its efficiency in terms of time and cost, showcases its potential as a valuable addition to the interventional radiologist’s toolkit.
# 479
DOES CHATGPT RECOMMEND THE APPROPRIATE TREATMENTS FOR SIMPLE AND COMPLEX UROLOGIC CONDITIONS?
Quines JF, Kim U, Crew R, Hanessian KA, Farkouh A, Song S, Cheng K, Amasyali A, Okhunov Z, Baldwin D. Loma Linda University Health, Loma Linda, CA
Purpose of Study: ChatGPT, developed by OpenAI (California, USA), is a publicly available large language model designed to engage in natural conversation with users. It has gained notable attention within the field of medicine, where its applications are being actively investigated. Despite its widespread use, the extent to which ChatGPT effectively responds to medical scenarios within endourology remains relatively unexplored. This study aims to evaluate ChatGPT’s knowledge and adherence to guidelines established by the American Urological Association (AUA) and the European Association of Urology (EAU) when presented with various endourologic vignettes.
Methods Used: Twenty hypothetical patient vignettes encompassing four endourologic conditions: benign prostatic hyperplasia, ureteral stones, prostate masses, and renal masses were created based on the AUA and EAU guidelines. These scenarios consisted of ten simple and ten complex vignettes. These vignettes were presented to ChatGPT Plus (July 20, 2023 Version). Five board-certified urologists assessed ChatGPT’s responses in four areas: tone (support of response and discussion of limitations rated 0-2), complementarity (support of patient-physician relationship rated 0-1), areas of uncertainty (rated 1-5), and accuracy (evaluated on a 10-point Likert scale; 0 is very inaccurate and 10 is very accurate). Additionally, “Readability” and “Ease of understanding” for ChatGPT’s answers were assessed using the Flesch Reading Ease and Flesch-Kincaid Grade Level formulas, respectively.
Summary of Results: No significant differences were found when comparing simple versus complex scenarios across all areas assessed (p>0.05). The average tone for simple scenarios was 1.14±0.7, and for complex scenarios, it was 1.16±0.7. These scores imply that ChatGPT’s responses generally lack discussions of limitations and exhibit some level of caution in the support provided. In terms of complementarity, simple scenarios scored 0.78±0.5, while complex scenarios scored 0.70±0.5, indicating that ChatGPT’s responses primarily support the patient-physician relationship. Areas of uncertainty scored 2.88±1.1 for simple scenarios and 2.90±1.1 for complex ones, indicating that ChatGPT exhibits partial uncertainty in the treatment options it suggests. The Likert scale scores were 6.76±1.9 for simple scenarios and 6.30±2.0 for complex scenarios, suggesting that ChatGPT’s responses demonstrate a moderate level of accuracy. Readability and Ease of understanding scores indicated a college-level response.
Conclusions: This study’s findings demonstrate that ChatGPT generates responses of consistent quality, regardless of the complexity of the clinical vignettes. However, ChatGPT’s scores for each area of assessment shows that improvement is needed in ChatGPT’s responses before it can be considered a reliable source of medical advice within endourology. Furthermore, ChatGPT recommended some treatments which were absolutely contraindicated in clinical practice.
# 480
RISK FACTORS ASSOCIATED WITH HOSPITAL READMISSION FOLLOWING KIDNEY STONE SURGERY
Hanessian KA, Crew R, Sajdak G, Farkouh A, Song S, Okhunov Z, Amasyali AS, Baldwin D. Loma Linda University School of Medicine, Loma Linda, CA
Purpose of Study: Urinary stones can harbor bacteria that are released during stone fragmentation, leading to deleterious surgical outcomes. Stone culture is highly predictive of infectious complications and postoperative sepsis. While there are several studies on risk factors for postoperative fever and sepsis, risks for readmission are poorly understood. The purpose of this study was to examine the risk factors for readmission after stone surgery.
Methods Used: A single center retrospective review was performed on patients who underwent percutaneous nephrolithotomy (PCNL) for treatment of large renal stones. Data collected included demographics, preoperative and intraoperative parameters, and postoperative outcomes including relative (<4mm fragments) and absolute (no fragments) stone free rates. Factors significantly associated with hospital readmissions within 30 days were determined. A univariate analysis to compare readmitted patients against non-readmitted patients was performed using Chi-Square for categorical variables and Mann Whitney U test for continuous variables. Significance was defined as p<0.05.
Summary of Results: Of the 290 patients examined, 48 patients were readmitted to the hospital within 30 days after PCNL, including 21 for infection, 4 for pain, 11 for indwelling catheter complications, and 12 for other complications. Patients who were readmitted were more likely to be male (67% vs 45%; p=0.007) and younger (mean: 52 vs 58 years old; p=0.011) compared to those not readmitted. Those who had postoperative readmission were associated with longer hospital stays (85 vs 54 hours; p=0.009), longer surgical time (208 vs 176 minutes; p=0.02), and higher estimated blood loss (128 vs 82 mL; p=0.003). Patients who were readmitted were more likely to have a preoperative nephrostomy tube (43% vs 27%; p=0.029). Those who had readmission had lower relative (56% vs 79%; p=0.001) and absolute (46% vs 62%; p=0.028) stone-free rates and more likely to need a second procedure (35% vs 9%; p<0.001). Patients who were readmitted were more likely to have positive stone cultures (50% vs 36%; p=0.007). They were also more likely to have surgical complications, scored by the Clavien-Dindo classification system grades 1-2 (36 vs 15%; p<0.001) and grades 3-4 complications (10% vs 3%; p=0.016). Multivariate analysis showed that younger age, male gender, grades 1-2 complications, and a positive stone culture were independent factors associated with readmission (p<0.05 for all).
Conclusions: Our findings show that male gender, younger age, positive stone culture, and grades 1-2 surgical complications were statistically associated with hospital readmissions within 30 days of surgery. Understanding these risk factors associated with hospital readmissions may provide valuable insight in preventing these readmissions in the future.
Joint Plenary Session
WAFMR, WAP, WSCI, AND WSPR
1:30 PM
Friday, January 19, 2024
# 481
INEQUITIES IN END-OF-LIFE HEALTHCARE UTILIZATION FOR PATIENTS WITH ADVANCED CANCER AND LIMITED ENGLISH PROFICIENCY
Ferguson A1, Sharma R1, 2. 1University of Washington School of Medicine, Seattle, WA and 2University of Washington Division of General Internal Medicine, Seattle, WA
Purpose of Study: Although patients with advanced cancer and limited English proficiency (LEP) are at high risk of receiving suboptimal end-of-life care due to cultural, language, and literacy barriers, few studies have examined the intensity of end-of-life care and use of palliative care in this population. Furthermore, given heterogeneity within the LEP population, it is necessary to compare individual LEP populations to identify those with the highest need for intervention. This study’s purpose was to evaluate inequities in the intensity of end-of-life care and palliative care use between advanced cancer decedents with and without LEP as well as between individual LEP populations at a large academic medical center.
Methods Used: We conducted a retrospective EHR analysis of adults with advanced cancer, identified by ICD codes, who received care at UW Medicine and died between 2019-2021. Outcomes based on the last year of life included ED visits, ICU admissions, palliative care consultation (PCC), documentation of advance care planning (ACP), and location of death. Descriptive statistics and chi-square tests were conducted.
Summary of Results: Among 9171 decedents with advanced cancer, 8578 patients (94%) had English proficiency (EP), and 593 patients (6%) had LEP. For patients with EP, the mean age was 69 +/- 14 years; 45% were female; 7226 (84%) identified as white, 458 (5%) as Black, 313 (4%) as Asian; and 226 (3%) identified as Hispanic. For patients with LEP, mean age was 71 +/- 15 years; 42% were female; 183 (31%) identified as white, 56 (9%) as Black, 301 (51%) as Asian; 110 (19%) identified as Hispanic; 117 (20%) had a preferred language of Spanish, 92 (16%) Cantonese/Mandarin, 75 (13%) Vietnamese, 62 (11%) Russian, 35 (6%) Korean, 29 (5%) Tagalog, 24 (4%) Somali, and 159 (27%) preferred other languages. Patients with LEP were more likely than those with EP to have Medicaid (24% vs. 11%, p<0.001) and less than 12th-grade education (30% vs. 7%). This population was more likely than those with EP to have an ED visit (72% vs. 58%; p<0.001), ICU admission (43% vs. 35%; p<0.001), and in-hospital death (51% vs. 39%; p<0.001). Patients with LEP also had higher rates of PCC than patients with EP (32% vs. 21%; p<0.001) but had similar rates of ACP as EP patients (82.2% vs. 82.3%; p=0.99). Within the LEP group, there were statistically significant differences in ED visits (p=0.005), ranging from 88% of Somali-speaking patients to only 49% of Korean-speaking patients. Additionally, while 60% of Korean-speaking patients died at home, only 28% of Cantonese/Mandarin-speaking patients did (p=0.02). PCC also ranged from 23% (Russian-speaking) to 46% (Somali-speaking) (p=0.06).
Conclusions: Adults with advanced cancer and LEP are more likely than those with EP to experience high-intensity end-of-life healthcare and receive PCC. However, significant variation in healthcare utilization exists between specific populations with LEP, suggesting tailored interventions are needed to improve care for these populations.
# 482
GLYCEMIC CONTROL, NEIGHBORHOOD SOCIOECONOMIC ENVIRONMENT AND THE DEVELOPING BRAIN
Luo SH, Hsu E, Belcher B, Kim MS. University of Southern California, Los Angeles, CA
Purpose of Study: To investigate associations between glycemic control and brain structure in youth and modulating effects of neighborhood socioeconomic environment.
Methods Used: This was a cross-sectional study of healthy, typically developing youth without diabetes, ages 10 - 13 years old, across 21 sites in the United States for the Adolescent Brain and Cognitive Development (ABCD) Study®. Brain structure was evaluated by magnetic resonance imaging and glycemic control was assessed with hemoglobin A1c (HbA1c). Neighborhood deprivation was assessed using Area Deprivation Index (ADI). Mixed effects models were used to examine relationships between brain structure, HbA1c, and ADI controlling for sociodemographic covariates. Stratified analysis was performed by tertiles of ADI.
Summary of Results: N=696 youth were studied (43.5% female; HbA1c 5.13 ± 0.27%; 16.5% Hispanic, 60.9% White, 10.2% Black, 1.3% Asian, and 11.1% Other). Higher HbA1c was associated with lower mean cortical thickness [β (95% CI) = -0.096 (-0.171, -0.021), P=0.030)] and smaller total cortical gray matter volume [β (95% CI) = -0.048 (-0.086, -0.011), P=0.030)]. Each 1% increase in HbA1c was associated with a -0.026 mm decrease in cortical thickness and 9,808 mm3 decrease in gray matter volume. There was a significant interaction of HbA1c and ADI on total gray matter volume (F2,642=34.477, P<0.001). Stratified analysis revealed that the high [β (95% CI) = -0.069 (-0.131, -0.007), P=0.028] and medium ADI group [β (95% CI) = -0.085 (-0.157, -0.013), P=0.041] but not the low ADI group [β (95% CI) = -0.006 (-0.070, 0.059), P=0.933] exhibited significant associations of HbA1c with total gray matter volume (
Figure 1
).
Relationships between HbA1c levels and adjusted total cortical gray matter volume in children from neighborhoods with low, medium, and high area deprivation index (ADI), with adjustment for family ID as random effects, and age, sex, pubertal status, race/ethnicity, family income, parental education, handedness, and intracranial volume as fixed effects. Lines represent interaction model regression fits and shaded areas around the fitted lines represent standard error of the fits.
Conclusions: Higher HbA1c levels are associated with smaller brain volumes, particularly in youth from disadvantaged neighborhoods. These findings provide preliminary evidence to support targeted diabetes interventions in these groups. Future studies are merited to assess if altered brain volumes are an early biomarker of diabetes.
# 483
BABE 2: BREASTFEEDING AND ANTENATAL BREAST MILK EXPRESSION VIA ELECTRIC BREAST PUMP VERSUS HAND EXPRESSION: RANDOMIZED CONTROL TRIAL
Liu D, Estafanous M, Richardson C, Choi Y, Son S, Louis M, Lorson R, Bello Adejugba O, Hart E. Loma Linda University, Loma Linda, CA
Purpose of Study: It is well established that breastfeeding confers significant health benefits for both mother and baby. However, the rates of exclusive breastfeeding in 2019 in the United States were only 62.6% at 0 months and 24.9% at 6 months postpartum, leaving room for improvement. This study evaluated the effect of antenatal breast milk expression on exclusive breastfeeding in mothers’ postpartum stay in the hospital and compared antenatal breast milk expression with electric pump versus hand expression.
Methods Used: A randomized control study was performed with 95 multiparous and nulliparous women enrolled at 2 clinics. Exclusion criteria included prior exclusive breastfeeding for 6 months or greater, contraindications to breastfeeding, multiple gestations, and history of preterm delivery. Participants were randomly assigned to pump or hand express, and were instructed to express breast milk for 20 minutes 3 times daily, starting at 37 weeks gestation. The primary outcome was formula use in the first 24-48 hours in the hospital, and secondary outcomes women’s quantitative rating for how helpful the study protocol was, amount of colostrum produced antenatally, and mean cervical dilation on admission. Data was collected from online Qualtrics survey responses and maternal electronic medical charts.
Summary of Results: There was no significant difference in the postpartum reports of hospital formula administration to babies with women in the pumping and hand expression groups, indicating similarly successful rates of exclusive breastfeeding (pumping: 80%; hand expression: 74.4%, p=0.52) in the first 24-48 hours postpartum. Women in both groups rated the study protocol as “very or extremely helpful” (pumping: 75%; hand expression: 63%, p=0.41) with no significant differences. The mean amounts of antenatal colostrum produced in the two intervention groups did not yield significant differences (pumping: 45.8 cc; hand expression: 26.6 cc, p=0.17). From 37 weeks to delivery, the amount of breast milk expressed ranged from 0 to 449 cc in the pumping group and 0 to 190 cc in the hand expression group. Although the difference in mean cervical dilation on admission was notable, it was not statistically significant (pumping: 2.6 cm; hand expression: 3.7 cm, p=0.067).
Conclusions: Antenatal expression of colostrum safely provides women the opportunity to become familiar with breastfeeding and potentially produce significant colostrum prior to delivery. As baseline exclusive breastfeeding rates in Loma Linda University Medical Center’s postpartum unit are 48%, both antenatal pumping and hand expression demonstrated improved rates of exclusive breastfeeding in the first 24-48 hours postpartum. This study suggests that both pumping and hand expression are similarly helpful and efficacious. Thus, prenatal care providers can consider recommending patients to implement either intervention.
# 484
SERIAL ECHOCARDIOGRAM ASSESSMENTS OF PULMONARY HEMODYNAMICS AND RIGHT VENTRICULAR HYPERTROPHY IN INFANT RATS WITH EXPERIMENTAL BRONCHOPULMONARY DYSPLASIA DUE TO ANTENATAL ENDOTOXIN
Dias Maia P, Seedorf G, Gonzalez T, Bye E, Frank BS, Mandell E, Abman SH. University of Colorado, Aurora, CO
Purpose of Study: Pulmonary hypertension (PH) and related pulmonary vascular disease (PVD) in premature infants present profound challenges to clinicians, including controversies and knowledge gaps related to its pathogenesis and non-invasive characterization by echocardiogram (ECHO). Disruption of angiogenesis and early changes in lung circulation due to antenatal stress have become increasingly recognized as major determinants of outcomes after preterm birth. We sought to define serial changes in ECHO metrics of PH that best characterize the presence and progression of cardiopulmonary disease in a well-established animal model of BPD-PH induced by chorioamnionitis, marked by disruption of alveolarization, reduced pulmonary vessel density, and development of right ventricular hypertrophy (RVH) from birth to 14 days of age.
Methods Used: Endotoxin (ETX, 10ug/sac) was administered to pregnant rats by intra-amniotic (IA) injection at embryonic day 20 (E20; term = E22) and pups were delivered by cesarean-section at E22. Transthoracic 2D and Doppler imaging were performed in spontaneously breathing rats using a VisualSonics Vevo 1100 ultrasound system. ECHO parameters, including pulmonary artery acceleration time (PAAT), pulmonary artery ejection time (PAET), PAAT adjusted by PAET (PAAT/PAET), left ventricular eccentricity index (LV EI) at the end of systole, and end-diastolic right ventricular wall thickness (RVWTd), were assessed on days 7 and 14. Comparisons were statistically analyzed according to study group (control (CTL) versus endotoxin-exposed pups (ETX)) at postnatal days 7 and 14.
Summary of Results: In comparison with the CTL group, the ETX group demonstrated an increase in LV EI by 32% (p<0.0001) at postnatal day 7. There were no significant differences in PAAT, PAET, PAAT/PAET, and RVWTd at day 7. At day 14, compared to CTL, antenatal endotoxin-exposed pups demonstrated an increase in PAET by 17.4 % (p<0.0001), LV EI by 33.3% (p<0.0001), and RVWTd by 34.7% (p=0.0311), and a decrease in PAAT/PET ratio by 15.1 % (p=0.0021). However, PAAT measurements were not different between study groups at day 14.
Conclusions: ETX exposure increased ECHO metrics of PH in infant rats during the first 2 postnatal weeks after antenatal exposure to ETX. Early changes in left ventricular EI but not PAAT, PAAT/PAET or RVWTd were identified at least as early as day 7, whereas each metric was abnormal in the ETX group by day 14. We speculate that ECHO is a valuable noninvasive tool to longitudinally study mechanisms underlying the temporal progression of cardiopulmonary disease and to phenotype pulmonary hemodynamics in experimental BPD-PH. These findings further suggest that LV EI precedes the increase in RVWT and may provide an early marker for PH among other traditional ECHO measurements and can characterize early changes to RV pressure load due to PVD in infant rats after antenatal inflammation.
# 485
Replacement insulin during IGF-1 infusion increases growth in fetal sheep
Stremming J1, Chang EI1, White A1, Barooni NB2, McCurdy CE2, Rozance P1, Brown LD1. 1University of Colorado, Aurora, CO and 2University of Oregon, Eugene, OR
Purpose of Study: Insulin-like growth factor-1 (IGF-1) is an essential fetal growth hormone that correlates with birth weight and is a potential therapeutic agent to mitigate fetal growth restriction (FGR). Infusion of IGF-1 to the normally grown sheep fetus increases the weight of some fetal organs but does not consistently increase body weight. However, IGF-1 infusion decreases fetal plasma insulin concentrations, which may limit fetal growth because insulin is another critical fetal growth hormone. We hypothesized that during a one-week fetal infusion of IGF-1, euinsulinemia must be maintained to support fetal growth.
Methods Used: Catheterized late gestation sheep fetuses received a one-week intravenous infusion of either IGF-1 (IGF, n=8), IGF-1 with insulin and dextrose infusions to maintain euinsulinemia and euglycemia (IGF+INS, n=8), or saline (SAL, n=8). Fetal blood gas and plasma glucose, lactate, amino acid, and insulin concentrations were measured prior to infusion start (baseline) and after the one-week infusion period (final). Baseline and final uterine and umbilical blood flow rates were measured, and uteroplacental and umbilical (net fetal) uptake rates of oxygen, glucose, lactate, and amino acids were calculated. Fetal body and organ weights were obtained. One-way or two-way (time, group, interaction) ANOVA was performed to compare differences among groups with Tukey’s post hoc test. P-values indicate post hoc test.
Summary of Results: Fetal weight was 21% heavier in IGF+INS compared to SAL (P<0.01). IGF fetuses were larger than SAL but smaller than IGF+INS; this was not statistically significant. IGF+INS had larger hearts, livers, and adrenal glands than IGF and SAL, and larger kidneys than SAL (P<0.01). Final glucose concentrations were similar among groups. IGF+INS had three-fold higher lactate and two-fold lower oxygen concentrations than IGF and SAL (P<0.0001) at the end of the study. Final amino acid concentrations in IGF+INS (n=7) were 32% lower than SAL (n=7) (P<0.05). Uterine (n=7 for all groups) and umbilical (n=7 for SAL) blood flow rates increased over time but were similar among groups. IGF+INS had 31% and 28% higher uterine oxygen uptake than IGF and SAL, respectively (P<0.05); IGF+INS had 39% and 50% higher umbilical oxygen uptake than IGF and SAL, respectively (P<0.001). Uterine and umbilical uptake rates of glucose, lactate, and amino acids were similar among groups.
Conclusions: Maintaining euinsulinemia during fetal IGF-1 infusion increased fetal body and organ growth, despite lower fetal oxygen, lower amino acid, and higher lactate concentrations. Both uterine and umbilical oxygen uptake rates were increased in IGF+INS; increased oxygen delivery to the fetus may be necessary to optimally promote oxidation of nutrients to support growth. More research is needed to determine whether IGF-1 and insulin infusions will promote growth in the FGR fetus after exposure to chronic placental insufficiency with limited oxygen and nutrient delivery. (Funding: Colorado NORC P30-DK048520)
Case Reports II
Concurrent Sessions
8:00 AM
Saturday, January 20, 2024
# 486
GASTROINTESTINAL VASCULAR MALFORMATIONS IN TURNER SYNDROME: A CASE TO CONSIDER SCREENING FOR RECTAL BLEEDING
Christensen TN, Akay G, Palumbos J, Viskochil D. University of Utah, Salt Lake City, UT
Case Report: Turner syndrome is a condition characterized by a partial or complete deletion of an X chromosome in females. Manifestations can include short stature, webbed neck, shield chest, and gonadal dysgenesis. Over 5% of individuals with Turner syndrome have gastrointestinal vascular malformations (Eroglu, Y, et. al., 2002, PMID: 12142816); however, present guidelines do not emphasize any screening recommendations for these individuals regarding possible gastrointestinal bleeds or iron deficiency anemia (Gravholt, CH, et. al., 2017 PMID: 28705803).
A young woman with non-mosaic Turner syndrome (45,X) presented to our clinic for follow-up after multiple episodes of gastrointestinal bleeding due to small bowel telangiectasias and/or venous malformations. She was diagnosed with Turner syndrome by karyotype at 18 months prompted by developmental delay, failure to thrive, and recurrent otitis media. Additionally, she has congenital nystagmus, a bicuspid aortic valve with a dilated aorta, ovarian failure, and bilateral renal cysts. At age 13, she presented with an isolated syncopal episode followed by 1 week of vomiting, lethargy, and hematochezia. Evaluation identified a hemoglobin of 3g/dL. She was life-flighted to a regional ICU where she received 8 blood transfusions. She was instructed to begin iron supplementation after discharge. Using an at-home hemoglobin monitor, she has had 3 subsequent episodes of a hemoglobin <7g/dL; one of which required hospital admission. Multiple exploratory laparotomies and a capsule endoscopy found several telangiectasias and possible arteriovenous malformations throughout the small and large bowel, but the source of bleeding could not be localized. She underwent a partial bowel resection at age 17 but has continued to have intermittent bleeds. At 18, she began sirolimus therapy with the hopes of preventing further bleeding episodes from telangiectasias.
As recurrent gastrointestinal bleeds can be life-threatening, individuals with Turner syndrome and their care providers may benefit from being informed of the association with vascular malformations. Furthermore, given that >5% of individuals with Turner syndrome have gastrointestinal vascular malformations, it may be worthwhile to consider the benefits of adding a complete blood count to the routine blood work recommended in the International Guidelines for Care of individuals with Turner syndrome.
# 487
A Severe Case of Reactive Infectious Mucocutaneous Eruption Associated with Two Possible Triggers: Coronavirus and Group A Streptococcus
Rodriguez I, Kwong A, Worswick S. Keck School of Medicine of USC, Los Angeles, CA
Introduction: Reactive infectious mucocutaneous eruption is a recently proposed disease group characterized by a mucocutaneous blistering eruption secondary to an upper respiratory infection. Here, we describe a severe case of RIME in a patient who tested positive for both coronavirus NL63 and group A streptococcus, which to our knowledge have not been reported as primary causative organisms thus far.
Case Presentation: A previously healthy 5-year-old girl presented with a one-week history of a progressively spreading rash that began on her arms and eventually involved her face, trunk, legs, and genital area. She had experienced a dry cough and a sore throat prior to rash onset. Initially diagnosed with chickenpox and provided valacyclovir, she later developed high fevers and severe mouth and throat pain with no improvement in the rash. Examination revealed extensive erythema with dusky violaceous pseudotargetoid plaques on the face, upper torso, and upper arms with small vesicles/bullae dispersed among the affected areas with body surface area involvement of 45%. Over time, affected areas began to desquamate. Infectious work-up revealed positive coronavirus NL63 via respiratory viral panel, positive mycoplasma IgG, and negative mycoplasma IgM with all other serologies being negative. A diagnosis of reactive infectious mucocutaneous eruption was made. Etanercept was given, and over several days BSA increased to 60% with progressive oropharyngeal involvement. The patient was intubated and transferred to the burn unit. She remained hemodynamically stable, although with persistent unexplained fevers. Labs notable for pancytopenia, and broad-spectrum antibiotics were started along with pancultures. Bronchoalveolar lavage was positive for group A streptococcus. With time and burn unit level supportive care, her condition improved, and by day 10 of hospitalization, her skin had largely re-epithelialized. The patient ultimately recovered and was discharged with clinic follow-up.
Conclusion: Although the most common pathogen associated with RIME is mycoplasma (MP), with MIRM being a well-documented predominantly mucosal disease with some cutaneous involvement, our patient’s negative IgM serology necessitated consideration of alternative causes. Whether our patient’s eruption was secondary to coronavirus NL63 and/or GAS is uncertain, given both infectious entities were found in close temporal proximity to one another. Further diagnosis complexity arises from overlapping clinical features with other severe mucocutaneous eruptions such as Stevens-Johnson Syndrome/Toxic Epidermal Necrolysis. In regard to treatment, currently, there are no evidence-based treatment recommendations for the management of RIME. Some recent studies have shown etanercept to be beneficial, with more robust studies needed. This case underscores the need for comprehensive infectious workups and drug exposure histories to evaluate for all possible causes of mucocutaneous eruptions.
# 488
PERSISTENT PULMONARY HYPERTENSION IN PREMATURE INFANT WITH PROLONGED PATENCY OF THE DUCTUS ARTERIOSUS
Lorusso Vivas GA1, Adie M2, Siassi B1, Ramanathan R1. 1Los Angeles General Medical Center, Los Angeles, CA and 2Adventist Health White Memorial Hospital, Los Angeles, CA
Case Report: Prolonged patent ductus arteriosus (PDA) in extremely low birth weight (ELBW) infants is associated with increased pulmonary blood flow (PBF) leading to pulmonary vascular changes and increased needs for respiratory support placing the infants at risk for bronchopulmonary dysplasia (BPD) and BPD associated pulmonary hypertension (PHN).
Premature infant born at 27.3 weeks via precipitous vaginal delivery to a 28-year-old G1P0 mother. Maternal history was relevant for well controlled asthma, obesity and occasional use of alcohol and THC during pregnancy. There was a positive triple screen with normal anatomy fetal ultrasound, negative serologies and unknown GBS status. No antenatal steroids or magnesium were given. APGAR scores were 7 and 8 at 1 and 5 minutes respectively, and the patient required Nasal Continuous Positive Airway Pressure (NCPAP) of 5 cmH2O, FiO2 0.25.
The patient was then transferred to the NICU, developed apnea with respiratory acidosis, requiring non-invasive positive pressure ventilation with FiO2 0.30-0.40. The chest X-ray showed ground glass appearance. Surfactant was given via INSURE technique. No steroids or vasopressors were given during the hospitalization. Serial echocardiograms (ECHO) were performed which persistently showed a large PDA (image 1) A summary of the findings is described on Table 1. No clinical or respiratory support changes occurred between DOL 3 to 34. When attempting to wean off NCPAP 7cmH2O to 2 LPM nasal cannula on DOL 51, significant pulmonary edema developed, requiring the use diuretics and re-initiation of respiratory support of NCPAP 7cmH2O. Repeat ECHO demonstrated findings consistent with worsening PHN. (Table 1)
Finally, on DOL 60 cardiac catheterization was performed and PDA was closed with an AmplatzerTM Piccolo occluder. The patient was weaned to room air within a week and then, discharged home on full oral feeds a week later.
High PBF through the PDA resulted in elevated pulmonary vascular resistance, though it remained sub-systemic throughout admission. PDA closure using Piccolo device led to immediate reversal of PHN and quick weaning off respiratory support. Earlier device closure of the large PDA even without other clinical signs of syatemic hypoperfusion could have prevented the development of BPD and PHN.
Echocardiogram summary findings on days of life (DOL) 3, 7, 29, 35, and 51.
DOL 3
DOL 7
DOL 29
DOL 35
DOL 51
PDA Diameter (mm)
2.5
2
3
3
3
BP, MAP (mm Hg)
56/31 (39)
62/30 (40)
70/32 (44)
71/35 (47)
75/33 (47)
PDA Flow Pattern
Bidirectional
Pulsatile Flow
Pulsatile Flow PG 2m/s
Not Done
Pulsatile Flow >1.2m/s
LA/Ao Ratio
2
1.8
2
2
2
PFO Shunt
Left-to-Right Shunt
Left-to-Right Shunt. PG 0.8m/s
Laminar flow. Left-to-Right Shunt
Left-to-Right Shunt
High Velocity Flow
TR Jet
None
Tiny to almost none
2.2m/s
4.2m/s
4.5m/s
Interventricular Septum
Normal
Normal
Normal
Normal
Normal
Patent ductus arteriosus (PDA), Pressure Gradient (PG), Blood Pressure (BP), Mean Arterial Pressure (MAP), Left Atrial to Aortic (LA/AO) Ratio, Patent Foramen Ovale (PFO), Tricuspid Regurgitation (TR) jet.
Parasternal short axis base view. Please note large PDA with bidirectional flow.
# 489
When Symptoms Deceive: A Case of Functional Neurologic Symptom Disorder Disguised as Stroke
Ghadiya K, Athwal P, Johar L, Bustamante IL, Nwebeh S, Yomi T, Covenas C, Civelli V, Uy J. Clinica Sierra Vista - Rio Bravo Family Medicine Residency Program, Bakersfield, CA
Case Report: Functional Neurological Symptom Disorder (FNSD) is a condition of clear, high-burden neurological symptoms, but workup typically does not reveal any clear etiology. Previous psychiatric history is a known risk factor. Some studies show a population prevalence of up to 5%, but this is largely unknown. Some common FNSD subtypes involve seizure-like symptoms, gait issues, and muscular dysfunction. This report studies a case of FNSD in a patient with stroke-like symptoms with no neuropathologic origin.
A 55-year-old female presented with left-side weakness and paraesthesia of her left face, arm, and leg - as well as dysphagia and dysarthria. Her last known baseline was the day before; her husband noticed her deficits this morning, and they came to the hospital. She has a self-reported history of hemiplegic migraines precipitated by panic attacks and stress but had inconsistent recollection of her episodes. She also deals with chronic back pain of unknown origin, for which she follows multiple specialists. At baseline, she was independent of all activities of daily living. In the emergency department, her vitals were stable. Physical examination showed absent movement and decreased sensation to pinprick in her left upper and lower extremities - no right side deficits. Her NIHSS score was 15. CT scans did not show evidence of acute intracranial process nor evidence of stenotic cerebrovascular disease. Due to her dysphagia, antiplatelet therapy was recommended rectally, but the patient was irritated and refused. Her symptoms were consistent with a CVA, and the patient was admitted. Examination by the primary team later revealed decreased sensation to light touch and pinprick below the knee but not in a stocking-glove distribution. She also endorsed decreased sensation to fine touch on the palmer aspect of her hands and had decreased position sensation of her great toes with mild sway on Romberg testing. Her MRI later confirmed no acute infarction, and her echocardiogram ruled out an interatrial shunt. Neurology’s examination the following day revealed marked discrepancies with her symptoms. During the interview, the patient denied left upper and lower extremity strength but had adequate strength when distracted. She intermittently used both hands to grab and move objects and had noticeable strength when the examiner initiated a handshake. Neurology had no more medical recommendations and requested that she follow up with psychiatry outpatient. She soon passed her swallow study and was discharged in two days.
Per neurology, the patient’s symptoms were a result of FNSD - likely due to underlying psychiatric issues that predisposed her presentation. This highlights the importance of proper examination when differentiating between organic and non-organic diseases. FNSD is largely underreported, and patients are more likely to have other psychiatric conditions; therefore, early psychiatric intervention can lead to a better prognosis and quality of life.
# 490
ORBITAL OSTEOMYELITIS AND PERIORBITAL ABSCESS DUE TO COCCIDIOIDOMYCOSIS FOLLOWING TRAUMA
Hayashi G1, Pardo N1, 2, Hirsh NM1, 2, Vijayan V1. 1Valley Childrens Healthcare, Madera, CA and 2Health Sciences University College of Osteopathic Medicine, Clovis, CA
Purpose: Coccidioidomycosis is a systemic fungal infection that is endemic to the Central Valley of California. Most infected individuals have asymptomatic/subclinical infections. Less than 2% of patients with coccidioidomycosis present as extra-pulmonary or disseminated disease. Common sites of dissemination include the skin, bone, joints, lymph nodes and central nervous system involvement being the most severe.Ocular involvement due to Coccidioides sp. is extremely rare.
We describe a 13-year-old Black male who presented with left orbital cellulitis following blunt trauma to the eye and found to have orbital osteomyelitis and periorbital abscess due to coccidioidomycosis. To our knowledge, this is the first case describing orbital osteomyelitis due to coccidioidomycosis following trauma.
Summary of Results: A previously healthy 13-year-old Black male presented to the ED with left eye pain, diplopia, and proptosis two weeks after being struck by a basketball. His initial CT scan showed a left lateral orbital wall fracture and he was discharged home on analgesics. However, due to increase in pain and swelling, he returned for further evaluation.
Examination of the eye demonstrated proptosis of the left eye with periorbital erythema and edema. He reported limited upward and lateral gaze due to pain. Vision was 20/20 bilaterally and pupils were equal and reactive. Remainder of examination was normal.
Imaging of the orbits revealed a left superior lateral periorbital rim-enhancing abscess, erosions of the superolateral orbital rim, and post-septal inflammation of the lateral and superior rectus muscles. He underwent incision and drainage of the abscess and surgical debridement of the left superior orbital rim and frontal bone. Fungal stain from the intraoperative specimen showed spherules with endosporulation and fungal culture revealed C. immitis. Histopathology of the frontal bone revealed fungal spherules and endospores consistent with coccidioidomycosis. The child was started on liposomal amphotericin B and fluconazole and antibiotics were discontinued. He underwent a workup for additional sites of dissemination. His nuclear medicine bone scintigraphy and cerebrospinal fluid studies were negative. CT scan of the chest demonstrated multiple small pulmonary nodules. His Coccidioides complement fixation (CF) titer was 1:32. The patient completed one month of treatment with liposomal amphotericin B and fluconazole. He was discharged on oral fluconazole and continues to do well with no signs of relapse.
Conclusions: Our case highlights the importance of considering coccidioidomycosis when evaluating patients with orbital disease. Delays in the diagnosis may result in the progression of disease, visual loss, and central nervous system involvement. In our patient, immediate surgical intervention, microbiological diagnosis, and prompt initiation of antifungal therapy were critical for diagnostic and therapeutic purposes and allowed for a favorable outcome.
# 491
A Case of Nasal Vestibulitis as Source of Septic Thrombophlebitis of Left Opthalmic Vein
Trang NC, Rahimi R, Mishra S. Kern Medical, Bakersfield, CA
Case Report: A 28-year-old African American female with history of obesity and DM2 presented to ED with two days of left-sided headaches. Patient was administered fluids for migraine/dehydration before being discharged. Two days later, she returned for worsening frontotemporal headache, with new onset diplopia, lightheadedness, fatigue, N/V and found to have DKA.ENT was consulted for left nasal vestibulitis, which initially started as a “pimple.” Patient mentioned tampering with her blemish before the onset of symptoms. Bedside I&D revealed purulent discharge and left eye ptosis, orbital edema, left lateral gaze palsy, and binocular diplopia suggesting cranial nerve VI palsy.
MRI revealed infected thrombophlebitis of her left upper ophthalmic vein. Blood and CSF culture show MSSA with suspected source arising from nasal vestibulitis. Thoracic/lumbar MRI showed no abscess. TEE showed no endocarditis. Serial LPs were done to monitor elevated OP. Patient was started on nafcillin for six weeks and Lovenox for infected thrombophlebitis but transitioned to dual oral anticoagulation therapy at discharge.
Prompt treatment of nasal vestibulitis aims at the prevention of seeding to surrounding vulnerable structures. To assess the nasal cavity,a flexible laryngoscopy helped identify purulent material. Sudden worsening of proptosis directly associated with extension of SOVT may occur. Orbital imaging is of pinnacle importance in identifying SOVT. Definitive diagnosis can be best made using iodinated MR venography to enhance the orbital venous system and accentuate location of the thrombus within the superior ophthalmic vein. Secondary to septic CSF, patients often demonstrate symptoms associated with elevated dural sinus pressures. Until anticoagulation and systemic antibiotic therapies begin to take effect, therapeutic LP may be required due to markedly elevated OP to relieve associated headaches.
In conclusion, the notorious “triangle of death” still poses a rather large threat. As seen in the patient above, a simple nasal vestibulitis spiraled into a suspected SOVT causing diplopia, lateral gaze palsy, and even possibly meningitis.
# 492
HYPERTENSIVE URGENCY IN A 4-YEAR-OLD GIRL
Chau J1, Khalessi Hosseini P2, 1, Nagle S1, Patel B1, Kim G1. 1Los Angeles General Medical Center, Los Angeles, CA and 2Children’s Hospital Los Angeles, Los Angeles, CA
Introduction: Up to 85% of pediatric hypertension cases are thought to be due to secondary causes, including renal artery stenosis (RAS). In adults, RAS is most commonly secondary to atherosclerotic diseases. However, in pediatric cases, RAS is thought to be most commonly secondary to congenital causes. Infectious causes of pediatric RAS are rare and can be difficult to identify and diagnose.
Case Description: A previously healthy 4-year-old female born in Mexico was sent to the emergency department for elevated blood pressures noted at her routine outpatient clinic visit. On arrival, her blood pressure was 161/126. The patient reported polydipsia, polyuria, and weight loss. Her initial physical exam was unremarkable and her vitals were otherwise within normal range for her age. She was admitted to the Pediatric Intensive Care Unit and oral antihypertensive therapy was initiated. The patient did not initially respond to antihypertensives, requiring multiple changes to medications and doses before her blood pressures started down-trending. Initial labs were unremarkable. Initial renal artery duplex showed unclear evidence of RAS; however, a renal bruit was noted on repeat physical exam so the imaging study was repeated. Renal artery duplex showed 60% stenosis of bilateral renal arteries. Because of concern for RAS and possible middle aortic syndrome, a computed tomography angiography (CTA) of the abdominal aorta and thorax was completed. It revealed a mediastinal mass, a circumferential mass around the abdominal aorta, and a mass encasing and segmentally narrowing the bilateral renal arteries. Tissue biopsy revealed that the masses were tuberculomas. The patient was started on anti-tuberculosis medications (rifampin, isoniazid, ethambutol, and vitamin B6) and continued on antihypertensive therapy. Repeat CT after 6 months of treatment demonstrated reduced mass burden.
Discussion: The initial differential for hypertensive urgency in a child this age was broad, including postinfectious glomerulonephritis, membranoproliferative glomerulonephritis, systemic lupus erythematosus, RAS, dysautonomia secondary to COVID-19 infection, pheochromocytoma, neuroblastoma, and adrenal adenoma. Normal laboratory findings were inconsistent with many of these diagnoses, making RAS most likely. The three soft tissue masses on imaging were most concerning for neuroblastoma, rhabdomyosarcoma, lymphoma, leukemia, or neuroendocrine neoplasm. Biopsy was critical in finalizing the diagnosis of extrapulmonary tuberculosis. It was later discovered that one of the patient’s parents had previously been treated for tuberculosis.
Conclusion: Tuberculomas are a very rare cause of RAS. Over 95% of renovascular hypertension cases are due to atherosclerosis or fibromuscular dysplasia, but it is important to be aware of other rare causes of renovascular hypertension. The purpose of this case study is to highlight one of these rare causes of renovasulcar hypertension.
# 493
A Case of Hemophagocytic Lymphohistiocytosis Secondary to Salmonella Typhi Infection
Sran-Samran P, Gandham S. Valley Children’s Hospital, Madera, CA
Case Report: An immunized, previously healthy 13 year old female presented for 12 days of fever, right upper quadrant (RUQ) abdominal (abd) pain, non-bloody/nonbilious emesis, and non-bloody diarrhea. She then developed fatigue, dizziness and tea-colored urine. Two months prior, she was exposed to Hepatitis A on a trip to Mexico.
Initially found to have scleral icterus, hepatosplenomegaly, and RUQ abd tenderness; no cardiac murmur or petechia. Labs in Table 1 show direct hyperbilirubinemia, transaminitis, anemia, thrombocytopenia and high inflammatory markers. CT abd showed hepatosplenomegaly & ileal wall thickening consistent with enterocolitis. Zosyn was empirically started. Hematology was consulted & further workup obtained for HLH, TTP. Rheumatology was consulted; a large workup for oncological & autoimmune causes was negative. Her stool pathogen panel was positive for Salmonella and her blood culture grew Salmonella. A normal ADAMS13 level ruled out TTP. Her bone marrow biopsy did not show leukemia cells or hemophagocytosis. Patient met HLH diagnosis criteria listed in Image 1. Her HLH labs continued to worsen. She was then started on 5 days of Dexamethasone with improvement in her symptoms and labs without any immunosuppression with a chemotherapeutic agent. She was discharged with hematology follow-up and Amoxicillin for Salmonella typhi bacteremia.
Conclusion: In a critically ill patient, if a single diagnosis does not fit all the labs, such as unexplained cytopenias, physicians must consider additional causes such as secondary HLH. Since it is a rare disease, it can go unrecognized and have fatal outcomes if left untreated. HLH is a rare hyperinflammatory condition with hemophagocytosis & abnormal natural killer cell activity. There is a primary hereditary form & secondary forms due to infection, autoimmune disease, or malignancy. Treatment guidelines consist of steroids (Dexamethasone) & a chemotherapeutic agent (Etoposide) for immunosuppression. Viruses are more associated with infectious HLH & there are less reports of bacterial causes, especially due to non-endemic organisms such as Salmonella Typhi. Although Typhoid fever is not endemic to the United States, one should consider it with a history of foreign travel. Although there are a few case reports of HLH with Typhoid fever, they are managed differently and without a chemotherapeutic agent. In this case, the patient received antibiotics and 5 days of steroids with significant improvement. She did not need further immunosuppression. This case supports that in cases of HLH associated with infection, patients may not need immunosuppression.
Diagnostic Lab Values.
Conjugated Bilirubin
2.20 mg/dL (H)
AST/ALT
398/118 U/L (H)
CRP
28.9 mg/dL (H)
Procalcitonin
7.98 ng/mL (H)
ESR
23 (H)
Ferritin
6934 ng/mL (H)
Creatine Kinase
357 U/L (H)
LDH
1478 U/L (H)
WBC
7400 mcL (normal)
Hemoglobin
9.9 g/dL (L)
MCV
82 fL (normal)
Platelets
66 10^3/mcL (L)
Lactate
0.5 mmol/L (normal)
COVID/Flu
Negative
EBV IgM
Negative
Hepatitis Panel
Normal (Negative Hep A IgM;HBsAg;Hep B Core IgM. Nonreactive Hep C)
ADAMS13 Activity
52 (normal)
Stool Bacterial Pathogen Panel
+Salmonella spp
Blood Culture
Salmonella Typhi
Triglycerides
612 (H)
Soluble IL-2R
1,834 U/mL (H)
(H)= High; (L)= Low.
Congenital Heart Disease
Concurrent Sessions
8:00 AM
Saturday, January 20, 2024
# 494
Neonates with Critical Congenital Heart Disease and Growth Failure
Newens J2, Tharayil J2, Desmond A1, Martinez G3, Afshar Y3, Calkins KL1. 1University of California Los Angeles, Los Angeles, CA; 2David Geffen School of Medicine at University of California Los Angeles, Los Angeles, CA and 3University of California Los Angeles, Los Angeles, CA
Purpose of Study: Neonates with critical congenital heart disease (cCHD) require prolonged hospital stays secondary to multiple surgeries and high rates of sepsis and necrotizing enterocolitis. These complications combined with suboptimal nutrition cause growth failure (GF) and have far-reaching consequences including neurodevelopmental delays. This retrospective, single-site study aimed to investigate the incidence of GF and characterize GF severity in hospitalized infants with cCHD.
Methods Used: Inclusion criteria included: cCHD, born between 2018-2022, neonatal intensive care at the University of California Los Angeles, and baseline anthropometric measurements. cCHD was defined by a postnatal echocardiogram (transposition of the great arteries, truncus arteriosus, hypoplastic left heart syndrome, single left ventricle, double inlet left ventricle, double outlet right ventricle, pulmonary atresia with intact pulmonary septum, Ebstein’s anomaly, atrioventricular canal, Tetralogy of Fallot, total and partial anomalous pulmonary venous return, Shone’s complex, coarctation of aorta). Weight and length z-scores were collected at birth and approximately 14, 21, and 30 days of age, and discharge and corrected for prematurity. The study’s primary outcome was GF at discharge, defined by a weight or length z-score decline ≥0.8. GF was further characterized by severity (none; mild, z-score decline of 0.8-1.2; moderate, decline >1.2-2; severe, decline ≥ 2).
Summary of Results: Sixty-two infants were included in this study. The mean (SD) gestational age was 38.1 (2) weeks; birth weight was 3.1 (0.6) kg; and length of stay was 31.5 (59) days. When compared to birth weight z-scores, weight z-scores at 21 days (-0.5 (1.2) vs. -1.2 (1.1), p<0.01) and 30 days (-0.3 (1) vs -1.3 (1), p<0.01) were significantly less (figure 1). A similar trend was noted for length. When compared to birth length z-scores, length z-scores at 21 days (0.1 (1.4) vs. -0.6 (1.5), p<0.05) and 30 days (0.1 (1.1) vs -0.9 (1.2), p<0.01) were significantly less. The severity of GF increased over time (Table 1).
Conclusions: In this study, weight and linear GF were common in neonates with cCHD and increasing rates of GF occurred during the hospitalization. This data suggests that nutritional support may be inadequate. It remains unclear how GF alters neurodevelopment in infants with cCHD.
Percentage of Infants with Growth Failure.
Percentage of infants with growth failure.
Weight Growth Failure
Mild Growth Failure
Moderate Growth Failure
Severe Growth Failure
14 days
31%
69%
0%
21 days
24%
65%
12%
30 days
23%
46%
32%
Discharge
27%
27%
38%
Length Growth Failure
Mild Growth Failure
Moderate Growth Failure
Severe Growth Failure
14 days
0%
63%
37%
21 days
36%
43%
25%
30 days
19%
63%
19%
Discharge
0%
70%
30%
Weight z-scores over time. *p
# 495
Successful Umbilical Line Placement in Newborns with Congenital Heart Disease at a Level IV NICU
Harding E, Weikel B, Grover T, Zenge J, Shay R. University of Colorado, Aurora, CO
Purpose of Study: Our institution’s fetal care center offers prenatal consultations, fetal interventions, and deliveries of infants with complex anomalies. The neonatal team provides delivery room resuscitation and secures vascular access as predetermined by the multidisciplinary delivery planning meeting or deemed necessary upon delivery. There is limited data regarding neonatal vascular access with cited rates of umbilical venous line malposition between 20-37%, and less is known for infants with cardiac defects. The primary aim of this analysis was to determine success rates of achieving the recommended umbilical vascular access plan for infants with cardiac diagnoses and planned admissions to the cardiac intensive care unit (CICU). Secondary aims were to determine any identifiable factors related to successful or unsuccessful vascular access placement and if these factors were dependent on the severity of cardiac defect.
Methods Used: This study was performed at a free-standing children’s hospital with a level IV NICU and CICU. Our retrospective chart review was performed on infants with cardiac diagnoses born between January 2020-December 2022 and admitted to the CICU. We described the cardiac lesions using four levels of care (LOC) proposed by Donofrio et al, which progress in severity of defect and anticipated need for resuscitation. Data was secured in RedCap following review of electronic medical record documentation, notes, comprehensive vital signs, and summary reports of vascular access.
Summary of Results: We reviewed 232 charts and performed an analysis on patients who had umbilical access recommended during delivery planning (n=187). Infants born at gestational age <=34 weeks was rare (1.6%). Infants in the LOC 2 category were the most numerous (n=137) and typically had ductal-dependent defects. In this cohort, our team achieved appropriate placement of both UAC and UVC only 42% of the time and UVC alone in 64% of cases. The median time to place lines was 47.5 minutes, and the lines were kept a median of 65.5 hours. The highest risk group, LOC 4, had the shortest time spent attempting line placement and the longest duration of the UVC (33 minutes and 79 hours, respectively). The lines in the LOC 4 group were more likely to be low-lying as the infants were the least stable and needed rapid admission to the CICU. The remainder of our analysis is summarized in Table 1.
Conclusions: Successful umbilical catheterization of infants with cardiac lesions is difficult. Our study findings are consistent with current literature citing rates of malposition between 20-37%. In patients with complex cardiac disease (LOC 2-4), successful central UVC placement rates were low despite significant time spent attempting the procedure. Next steps of our study are to compare umbilical line success rates in infants with and without cardiac defects and to develop internal quality improvement initiatives to optimize resource utilization, expedite admission, or increase maternal-infant bonding time.
Groups divided by anticipated level of care required at delivery, described by Donofrio et al. *LOC 1 is no anticipated instability in the delivery room or during first days of life. LOC 2 has minimal risk of instability in the delivery room but does require postnatal intervention. LOC 3 is likely to have delivery room instability needing subspecialty intervention. LOC 4 predicts instability upon separation from placenta needing immediate intervention.
# 496
A COMPARISON OF NEAR-INFRARED SPECTROSCOPY AND TRADITIONAL PARAMETERS FOR MONITORING OF INFANTS WITH PRENATAL DIAGNOSIS OF AORTIC COARCTATION
Sharp DP1, Phillips A2, Maskatia S2, Chock VY1. 1Stanford University, Palo Alto, CA and 2Stanford University, Palo Alto, CA
Purpose of Study: Prenatal diagnosis of aortic coarctation allows for early risk stratification, targeted monitoring, timely intervention, and improved outcomes in affected infants. Traditional non-invasive monitoring for neonatal aortic coarctation includes continuous pre- and post-ductal oxygen saturation monitoring. Patients with aortic coarctation demonstrate decreased end organ perfusion as a result of decreased aortic flow, and monitoring tissue oxygenation using near-infrared spectroscopy (NIRS) may provide valuable insights into regional cerebral (Csat) and renal (Rsat) oxygenation. We hypothesize that Csat and Rsat will decrease in patients who develop coarctation and require surgery in the neonatal period.
Methods Used: This single-center, retrospective cohort study included newborns greater than 34 weeks gestation with fetal echocardiographic diagnosis of a moderate or high risk of aortic coarctation admitted to the neonatal intensive care unit under an institutional arch watch protocol. All patients received NIRS monitoring in addition to traditional pre- and post-ductal saturation monitoring. Csat, Rsat, and systemic oxygen saturation data were collected for the first 7 days of life.
Summary of Results: A total of 50 patients met inclusion criteria, and 15 required surgical repair. Continuous PGE infusion was started in 86.7% of surgical patients and 34.3% of non-surgical patients. Univariate analysis showed no significant difference in pre-ductal saturations, post-ductal saturations, or Rsat values between the surgical and non-surgical patients in the first 7 days after birth. Csat values were significantly lower in the surgical group when compared to the non-surgical group on day of life three (75% vs 81%, p=0.01), four (76% vs 81%, p=0.01), and seven (73% vs 80%, p=0.01).
Conclusions: Csat values were significantly decreased in infants with prenatal diagnosis of aortic coarctation who required surgical repair. NIRS monitoring may provide valuable insights into tissue oxygenation and aid in identifying patients who require surgical intervention earlier than traditional pre- and post-ductal saturation monitoring.
# 497
CLINICAL OUTCOMES IN NEONATES WITH CONGENITAL HEART DISEASE WITH CONCURRENT CONGENITAL NEUROLOGICAL ANAOMALIES
Torabyan Z, El-Rahi H, Cong CY, Ghimire L. UCSF Fresno, Fresno, CA
Purpose of Study: Congenital heart disease (CHD) is one of the most prevalent birth defects. When coupled with major extracardiac anomalies neonates affected by CHD may encounter clinical challenges during both the fetal and neonatal periods. There is limited information on clinical courses of neonates with CHD born with congenital CNS (Central Nervous System) lesions. We hypothesized that neonates with CHD alongside concurrent CNS lesions experience worse clinical outcomes and increased mortality rates compared to those with isolated CHD. The primary objective of this study is to assess the risk factors and complications associated with significant CNS anomalies among neonates diagnosed with CHD.
Methods Used: We utilized the nationally representative National Inpatient Sample (NIS) database for the years 2016-2020 to examine the incidence of CHD and CNS lesions among neonates. We further categorized CHD into simple lesions, complex biventricular lesions, and single ventricle lesions. We used descriptive statistics to compare the characteristics of neonates with isolated CHD vs those with CNS anomalies. We then created logistic regression models accounting for important confounding factors to calculate the risk of CNS anomalies in outcomes in neonates with CHD. We used Stata version 15 and RStudio for data analysis.
Summary of Results: We retrieved 564,085 neonates diagnosed with CHD and out of those 22,065 had concomitant CNS lesions. In-hospital mortality rate for isolated CHD was 2.5%(n=13,710) vs 9.0%(n=1990) for those with combined CHD and CNS anomalies, P<0.001 . We discovered a remarkable correlation between the severity of CHD with presence of CNS anomalies for in-hospital mortality. Simple CHD with CNS anomalies had in-hospital mortality of 7.5% (n=1300), while it was 13% (n=550) for complex biventricular CHD with CNS and 25% (n=140) for single ventricle CHD with CNS, P<0.001. Regarding other serious complications, we found that risk of respiratory failure [0.6%(n=135) vs 0.3%(n=1885), p<0.004], acute kidney injury [4.8%(n=1050) vs 2.3%(n=12505), p<0.001] and sudden cardiac arrests [0.2%(n=45) vs 0.1%(n=530), p=0.025] were much higher in those with CHD with concomitant CNS lesions than the isolated CHD lesions. Moreover, our investigation found that the length of hospital stays was much longer in patients with CHD and CNS anomalies median 31 days (IQR 11-72) vs 7 days (IQR 2-30), p<0.001 in isolated CHD lesions. These findings provide critical insights into the intricate relationship between CHD severity, CNS anomalies, and clinical outcomes.
Conclusions: Neonates born with CHD and CNS anomalies experience higher morbidity and mortality compared to those with isolated CHD. These findings will help the clinicians, family members and payors in counseling and planning for optimal patient care.
Variables
CNS anomalies (n,%)
P- Value
No
Yes
Female
252905 (46.7)
10650 (48.3)
0.029
Prematurity
207265 (38.2)
12215 (55.4)
<0.001
CHD
Category 1
449375 (82.9)
17320 (78.5)
<0.001
Category 2
83025 (15.3)
4180 (18.9)
<0.001
Category 3
9260 (1.8)
565 (2.6)
<0.001
Bed size
Small
82990 (15.3)
3225 (14.6)
0.001
Medium
138780 (25.6)
4965 (22.5)
0.001
Large
320250 (59.1)
13875 (62.9)
0.001
Location/teaching status of hospital
Rural
11895 (2.2)
145 (0.7)
<0.001
Urban non-teaching
62110 (11.5)
1210 (5.5)
<0.001
Urban teaching
468015 (86.3)
20710 (93.9)
<0.001
Zip Quartile
0 -25th percentile
172220 (32.1)
7880 (36.1)
<0.001
26th - 50th percentile
137875 (25.7)
5650 (25.9)
<0.001
51st - 75th percentile
125440 (23.4)
4775 (21.9)
<0.001
76th - 100th percentile
101115 (18.8)
3520 (16.1)
<0.001
Resp failure
1885 (0.3)
135 (0.6)
0.004
Acute kidney injury
12505 (2.3)
1050 (4.8)
< 0.001
ECMO
1490 (0.3)
95 (0.4)
0.064
Tachyarrhythmias
11355 (2.1)
530 (2.4)
0.179
Heart block
3660 (0.7)
200 (0.9)
0.075
Sudden cardiac arrest
530 (0.1)
45 (0.2)
0.025
Length of stay(median, IQR)
7 (2-30)
31 (11-72)
<0.001
In-hospital mortality
13710 (2.5)
1990 (9.0)
<0.001
# 498
SLEEP AS A PREDICTOR FOR ANXIETY AND DEPRESSION IN CHILDREN AND YOUNG ADULTS WITH CONGENITAL HEART DISEASE
Maxfield KE1, Melcher L2, Bottrill K2, Combs D2, 3. 1University of Arizona College of Medicine Tucson, Tucson, AZ; 2University of Arizona, Tucson, AZ and 3University of Arizona College of Medicine Tucson, Tucson, AZ
Purpose of Study: Congenital heart disease (CHD) is the most frequently occurring congenital disorder and is the leading cause of mortality due to birth defects. However, many children with CHD now reach adulthood due to improved interventions. While many patients with CHD now survive to adulthood, these individuals are at increased risk of developing many comorbidities including sleep disorders, depression, and decreased health-related quality of life. We examined whether worse sleep predicts mood disorders in children and young adults with CHD.
Methods Used: We recruited individuals between the ages of 4-25 years with congenital heart disease and collected data on self-reported or parent-reported sleep, anxiety, and depression using the Tucson Children’s Assessment of Sleep Apnea (TuCASA) sleep habits questionnaire, Screen for Child Anxiety Related Disorders (SCARED), and Center for Epidemiological Studies Depression Scale for Children (CES-DC). T–tests were used to compare the mean differences in anxiety and depression scores in patients with CHD based on whether the individual reported consistently adequate or inadequate sleep.
Summary of Results: Participants who responded “yes” to the TuCASA question “Has this child ever been troubled by not enough sleep” demonstrated significantly higher depression scores on the CES-DC scale (p=0.006). Children with reported not enough sleep had a mean score of 17.2 ±11.4 on the CES-DC scale for depression, while those who reported obtaining enough sleep had a mean score of 4.0 ±3.8. Similarly, participants with self-reported inadequate sleep demonstrated significantly higher mean scores on the SCARED anxiety scale for total anxiety, 20.0 ± 15.6 vs 2.6 ± 3.5 (p=0.006); generalized anxiety, 5.2 ± 4.6 vs 0.4 ± 0.8 (p=0.009); separation anxiety, 4.8 ± 3.6 vs 1.0 ± 1.2 (p=0.009); and social anxiety, 4.8 ± 3.9 vs 0.7 ± 1.3, (p=0.019).
Conclusions: Inadequate sleep may be a contributing factor towards depression and anxiety in individuals with CHD. While further research is required to better elucidate the association between anxiety, depression, and sleep disorders in patients with CHD, these results could help to address and prevent some of the mood-related comorbidities often present in patients with CHD. Our findings demonstrating the association between sleep and mood-disorders in CHD patients may encourage both parents and clinicians to identify and treat sleep disorders in individuals with CHD.
# 499
In Utero Endothelial Cells Have Unique Gene Expression in Congenital Heart Disease
Desmond A1, Bhattacharya A2, Afshar Y3. 1UCLA, Los Angeles, CA; 2MD Anderson, Houston, TX and 3UCLA, Los Angeles, CA
Purpose of Study: Congenital heart disease (CHD) is the most common major birth defect and represents the leading cause of infant death due to a congenital anomaly. Etiologies and mechanism of CHD development are not well defined. The umbilical cord offers a unique platform to study in-utero vasculature. In this study, we aimed to identify differentially expressed genes (DEGs) in endothelial cells isolated from human umbilical veins in pregnancies affected by CHD and controls.
Methods Used: This was a prospective cohort study (IRB #19-001754) of pregnancies affected by fetal CHD (n=57) and controls (n=84). Umbilical cords were collected at delivery, processed, and exposed to collagenase to isolate venous endothelial cells. RNA was extracted using RNeasy Micro Kit (Qiagen, Germantown, MD) and library preparation was performed using TruSeq Total RNASeq Kit (Illumina, San Diego, CA). Sequencing was conducted at University of California Los Angeles (RNAseq). Benjamini-Hochberg false discovery rate (FDR) method was used with significance threshold of FDR <0.05. DESeq2 was used to interpret differential gene expression results. Clinical and demographic data was collected from electronic medical records. Pre-gestational diabetes, maternal CHD, gestational age, sex, and neonatal birthweight were incorporated into analysis. RStudio was used for statistics (t-test, chi-squared test). GO biological processes performed gene ontology term enrichment of identified DEGs.
Summary of Results: There were 30 cyanotic lesions and 19 lesions with single ventricle physiology. Mean gestational age was 37.29 weeks (SD 3.29) for CHD and 36.83 (SD 4.23) for controls (p=0.531). Mean birth weight was 2.993 kg (SD 0.740) for CHD and 2.801 kg (SD 0.763) for controls (p=0.148). There was no difference of fetal growth restriction (14.0% and 15.9%, p=0.957) or male sex (50.0% and 52.5%, p=0.914) between CHD and controls. Fetal CHD cases compared to controls had 418 DEGs, many involved in vasculature development, regulation of cell motility, heart development, and response to growth factor. Cyanotic lesions compared to controls had 95 DEGs with notable involvement in extracellular matrix organization, vasculature development, and regulation of smooth muscle cell migration. Single ventricle compared to controls had 75 DEGs and highlighted processes include tube morphogenesis, extracellular matrix organization, vasculature development, and smooth muscle cell migration. Specific DEGs are listed in Table 1.
Conclusions: Differentially expressed genes were identified in isolated umbilical cord endothelial cells across CHD and controls with controls having notably higher transcription of genes involved in development of vasculature, vascular smooth muscle cell function, and outflow tracts. Future studies include analyzing umbilical endothelial cell shape and response to shear stress to understand if and how hemodynamics during pregnancy influence gene expression and predisposition to fetal CHD.
Highlighted and Quantified Differentially Expressed Genes.
Gene
GO Biological Process
Log2FoldChange CHD vs. Controls
Log2FoldChange Single Ventricle vs. Controls
Log2FoldChange Cyanotic vs. Controls
HSPB6
Angiogenesis, vasculature development
-2.135
-2.352
-2.360
PDGFRA
Cell proliferation by VEGF-activated signaling pathway
Variation in Mechanical Ventilatory Support After Neonatal Cardiac Surgery
Barnes T1, Sharp DP2, Keller R1, Steurer M1. 1University of California, San Francisco, San Francisco, CA and 2Stanford University, Palo Alto, CA
Purpose of Study: High tidal volumes on mechanical ventilation can result in ventilator-associated lung injury (VALI) in post-operative populations. Neonates with congenital heart disease (CHD) are at risk for VALI, as hemodynamic concerns may lead to the use of high tidal volumes. Optimal post-operative ventilatory strategies have not been evaluated. We hypothesize that post-operative tidal volumes (Vt) vary in neonates with CHD after cardiac surgery.
Methods Used: This is a retrospective single-center cohort study. We combined data from the Pediatric Cardiac Critical Care Consortium (PC4) database with chart review. All neonates requiring cardiac surgery at the UCSF Benioff Children’s Hospital San Francisco between January 2016 and July 2021 were included. Clinical data were collected over the first 96 hours post-operatively.
Summary of Results: 473 patients met inclusion criteria; the first 100 neonates are presented. The most common ventilation mode at all time points was SIMV with pressure release volume control (PRVC). Mean Vt per kilogram at 24 hours post-op (24h Vt) was 10.3±3.6 mL/kg. Weight and gestational age were correlated with 24h Vt (Fig 1 and 2). Vt did not differ over the 96h post-operative period. Lactate did not correlate with 24h Vt (β=-0.002, p=.40 by linear regression). 24h Vt was not correlated with time to extubation (≤ 6 mL/kg, 5.8±0 d; 6-10 mL/kg, 8.0±0.9 d; ≥10 mL/kg 14.3±2.7 d; β=0.04, p=.67 by linear regression).
Lower weight was correlated with higher 24h Vt. Borderline significance via linear regression (p=.05). Fig 2. Polynomial regression demonstrated a significant non-linear relationship between 24h Vt and gestational age (p =.01).
Conclusions: In these data, mean Vt is 10.3 mL/kg in neonates with CHD s/p median sternotomy at 24h (normal 4-6 mL/kg) with the smallest patients receiving highest Vt, suggesting neonates with CHD may receive higher tidal volumes than physiologically necessary.
# 501
Cardiac and Aortic Surgery Outcomes in Patients with Turner Syndrome
Middleton A2, Prakash S1, Khanna A2, Howell S2, Carl A2, Davis S2. 1University of Texas Health Science Center at Houston, Houston, TX and 2Children’s Hospital of Colorado, Aurora, CO
Purpose of Study: Turner Syndrome (TS), the partial or complete absence of the second sex chromosome, occurs in 1 in ~2500 female live births. 30-50% of individuals with TS have congenital heart abnormalities, most often presenting in the left side of the heart and including coarctation of the aorta, bicuspid aortic valves, and aortic dilation. The aim of this study was to describe cardiac surgical outcomes in pediatric TS patients and compare commonalities between two groups of patients who had cardiac procedures.
Methods Used: This study included two cohorts of patients from Children’s Hospital Colorado: a retrospective cohort selected via electronic medical records, selective to TS and confirmed by chart review for cardiac malformations (n=341), and a cohort from the InsighTS Registry (n=152). For both cohorts, diagnostic and surgical data was pulled from EPIC, including information about cardiovascular malformations, other diagnoses, type and status of surgery, complications, and status following procedures. The cohorts were compared using Chi-squared tests for categorical variables and logistic regressions for continuous variables.
Summary of Results: There were 41 patients who had cardiac procedures in the retrospective cohort, and 38 patients in the InsighTS cohort, with a total of 83 procedures performed. The most common karyotype among these patients was 45, X (61%), and many patients had similar heart defects, with 77% of patients having coarctation of the aorta, and 66% having bicuspid aortic valves. 71% of procedures were urgent, 28% were elective, and the most common procedure in both cohorts was repairing an aortic coarctation (73%), followed by atrial septal defect closures in the InsighTS cohort, and endoscopic cardiac procedures in the retrospective cohort. Age at time of procedure was higher in the InsighTS cohort (3.04 years ± 5.43) than the retrospective cohort (1.29 years ± 3.74), but the difference was not statistically significant (p=0.6). The most common complications included ventilator requirement >24 hours post-op (14%), G tube placement post-op (6%), chylothorax (5%), ventricular tachycardia (5%), pulmonary edema (4%), and bleeding requiring transfusion (3.6%). There was one instance of complications resulting in death (1.2%). There was no correlation between history of coarctation (p>0.99), having previous cardiac surgery (p>0.99), or prematurity (p=0.64) on complications. Patients with 45,X were 2.2 (95% CI: 1.35-3.55) times more likely to have complications than other karyotypes (p=0.002).
Conclusions: This retrospective chart review showed low mortality associated with cardiac surgery in a pediatric sample of patients with TS, and similar cardiac procedures in both the retrospective and InsighTS cohorts. Future directions include looking at adult cardiovascular surgical complications in TS, and longer term follow up to identify and educate about TS specific complications.
Diversity, Equity and Inclusion Research III
Concurrent Sessions
8:00 AM
Saturday, January 20, 2024
# 502
REDUCING BIAS IN NEWBORN SUBSTANCE USE TESTING THROUGH A MULTIDISCIPLINARY TASKFORCE
Razdan S, Sharp DP, Bonifacio S. Stanford University School of Medicine, Palo Alto, CA
Purpose of Study: Disparities in substance use testing of birthing persons and newborns are well-documented. We aim to study current substance use testing patterns, evaluate and revise guidelines to reduce bias and address disparities, and determine the impact of changes up on testing patterns.
Methods Used: We performed a retrospective chart review to obtain baseline, pre-intervention data in a single hospital in Northern California. Infants born from 2006-2022 were included. Racial/ethnic, geographic, and language data were obtained for all infants. Infants with unknown race/ethnicity and language were excluded. A multi-disciplinary work group was created, including physicians from obstetrics, pediatrics, neonatology both attendings and fellows, social workers, and nurse practitioners. The hospital’s substance use screening and testing policy was updated to include more objective, less biased guidelines. We plan to compare the demographics of tested infants before and after implementing our revised guideline.
Summary of Results: The total baseline study population was 69,185 newborns, of which 1,235 (1.8%) underwent substance exposure testing before day of life 14. Testing by race/ethnicity was notable for over-representation of Black and Hispanic infants, who make up 4% and 11% of the total population, respectively, but 25% and 19% of infants tested (figure 1). Infants of Spanish-speaking families made up 7% of the total tested but only 3% of the total population (figure 1).
Conclusions: Racial/ethnic and language differences are present in substance use testing in newborns. We will measure if a new, less biased substance use guideline assists in reducing disparities in testing.
Proportion of infants in the population compared to proportion tested for substance exposure, displayed by race, ethnicity, and language preference.
# 503
SOCIO-ECONOMIC DISPARITIES IN UNPLANNED HOSPITAL ADMISSION AND IN-HOSPITAL OUTCOMES AMONG CHILDREN WITH CONGENITAL HEART DISEASE
El-Rahi H, Torabyan Z, Cong CY, Ghimire L. UCSF Fresno, Fresno, CA
Purpose of Study: Unplanned/non-elective admissions have been associated with worse clinical outcomes and increased use of hospital resources. We hypothesize that children with congenital heart disease (CHD) from lower socio-economic status backgrounds have higher rates of unplanned hospital admissions and increased hospital resource utilization.
Methods Used: We used Kids’ Inpatient Database (2016-2019). We included children <21 years of age with CHD, and excluded newborn hospitalization. We further categorized CHD into simple lesions, complex bi-ventricular lesions, and single ventricle lesions. We used a logistic regression model to calculate the risk of unplanned hospital admission, mortality, and hospital resources utilization in children with different socio-economic status backgrounds.
Summary of Results: Out of 4,722,684 admitted children, excluding those with newborn hospitalization, 199,757 had CHD and met study criteria. 121,626 had mild CHD, 61,639 complex bi-ventricular lesions, and 16,462 single ventricle lesions. In the CHD cohort, 27% had elective admissions while 73% had non-elective admissions. Mortality was higher in unplanned admissions vs elective admissions, 3.0% vs 0.93%, P<0.001. Unplanned admissions were more common in lowest income neighborhoods vs highest income neighborhoods, aOR=1.4(1.3-1.5), P<0.001. There were higher rates of unplanned admissions in lowest income neighborhoods for each category of CHD. Lengths of hospitalization were longer in the poorest neighborhood compared to their wealthiest counterparts, median 7 days (IQR 3-21) vs 6 (3-17), P<0.001.
Conclusions: In children with CHD, children who lived in lowest income neighborhoods have increased odds of unplanned hospitalization and have higher mortality and resource utilization.
Logistic regression of unplanned admissions in different zip codes (unadjusted and adjusted) in CHD (N= 199,656). Adjusted for age, sex and year.
Household zip codes
Emergent/Non-Elective
Unadjusted OR
P-value
Adjusted OR
P-value
0-24th
48564(76%)
1.5(1.4-1.6)
1.4(1.3-1.5)
<0.001
25-49th
36951(74%)
1.3(1.2-1.4)
<0.001
1.2(1.2-1.3)
<0.001
50-74th
34443(72%)
1.2(1.1-1.2)
1.1(1.1-1.2)
<0.001
75-100th
25724(68%)
Reference
-
Reference
-
# 504
REASONS FOR DECLINING WELL CHILD VISITS AND ROUTINE VACCINATIONS DURING THE COVID-19 PANDEMIC: PERSPECTIVES OF PARENTS FROM DIFFERENT BACKGROUNDS
Chang JS1, Afghani B2, 3. 1Western University of Health Sciences, College of Osteopathic Medicine of the Pacific, Pomona, CA; 2UC Irvine School of Medicine, Irvine, CA and 3CHOC Hospital of Orange County, Orange, CA
Purpose of Study: Literature reveals a drop in routine vaccinations and well-child visits during the COVID-19 pandemic. However, research on the reasons for this decline is limited. To mitigate similar declines in future pandemics, the goal of our study was to evaluate, from the parents’ perspective, the factors contributing to the decline in routine vaccination and well-child visits.
Methods Used: A survey was conducted at a Children’s Hospital and clinics in an inner-city academic center between September 2020 and February 2022. Parents completed an anonymous survey using REDCap regarding the barriers during the COVID-19 pandemic that influenced their decision regarding routine vaccinations and well-child visits for their child. Statistical analyses were conducted to assess the associations between those barriers and demographics.
Summary of Results: Of the 189 respondents, 64.6% self-identified as a minority (Hispanic, Black or Native-American) and 54.5% reported a family income of <$50K/year. The most common barriers chosen for well-child visits or routine vaccinations were fear of being exposed to COVID-19 (61.5%) and concern about mixing of healthy and sick patients in the waiting room (56.9%). Compared to those from non-minority backgrounds, minority respondents were more likely to choose fear of being exposed, fear of mixing healthy and sick children, lack of culturally sensitive material, lack of explanation of benefits/side effects of vaccines and inadequacy in reminders as barriers (figure 1). The same concerns (except for fear of being exposed) and transportation were more commonly chosen as barriers by the families with income of <$50K/yr compared to those with income of >$50K/yr.
Conclusions: The fear of COVID-19 exposure and mixing of healthy and sick children were the most common barriers chosen by the respondents for routine child visits and vaccinations. Overall, a higher percentage of parents from minority and poor backgrounds reported these and other barriers. To effectively mitigate these concerns during future pandemics, a holistic approach that considers the heightened challenges for those from minority and poor socioeconomic backgrounds is needed.
Barriers to routine visits during COVID-19 pandemic: Comparisons based on racial background and income.
# 505
SCHOOL-BASED MENTAL HEALTH LITERACY PROGRAM DELIVERED BY COMMUNITY VOLUNTEERS IMPROVES SELF-EFFICACY AND MOOD AMONG YOUTH: ADVOCATES 4 ALL YOUTH (ALLY)
Izere M1, Wilson SN2, Mata C2, Simon S1, Kaar J1, 2. 1University of Colorado Anschutz Medical Campus, Aurora, CO and 2University of Colorado Anschutz Medical Campus, Aurora, CO
Purpose of Study: Examine pre-post changes in self-efficacy, resilience, and mood among youth who receive a school-based mental health literacy program delivered by community volunteers compared to control group.
Methods Used: ALLY is a universal, school-based mental health literacy intervention targeted to deliver equitable, supplementary mental health education through a student-centered, peer-to-peer design framework. Community volunteers (ALLYs) from diverse backgrounds complete an online training (i.e., 90 minutes) prior to administering the program to students through curated, six-weekly small group sessions using a bilingual interactive activity workbook. Students learn mental health-related terminology and have hands-on practice including mindfulness strategies, positive self-talk, and healthy coping skills. Group discussions & activities are facilitated on varying topics including emotions and moods, building healthy relationships, and problem-solving. Students completed pre- and post-assessments for four mental health constructs: resilience, self-efficacy, and symptoms of depression and anxiety (i.e., mood) using validated, age-specific assessments.
Summary of Results: A total of 140, 5th and 6th graders (9-13 years, 53% free-reduced lunch, 39% non-Hispanic White) across three public schools in Colorado were randomized at the school level to receive ALLY (n=87) or wait-list-control (n=48). Students who received ALLY reported significant improvements in self-efficacy (9.9 vs. 1.9; p=0.05) and symptoms of depression (-2.2 vs. 0.2; p=0.04) compared to peers in the control group (figure 1). Improvements in resilience, symptoms of anxiety, and psychosocial stress were not significant by the treatment group.
Conclusions: We conclude that ALLY improves youth’s self-efficacy and mood after six weeks and promotes engagement and mentorship between students and local community members.
# 506
Prenatal Urologic Consultation for Antenatal Hydronephrosis: True Equity or Hidden Disparity?
Hoefer AB1, 2, Mendez M2, Nanizao G2, Kieran K1, 2. 1University of Washington School of Medicine, Spokane, WA and 2Seattle Children’s Hospital, Seattle, WA
Purpose of Study: Prenatal urologic evaluation (PUC) is now offered to many prospective parents for fetal antenatal hydronephrosis (AH). This study aims to describe patient- and community-level differences in prenatal and postnatal urologic care patterns for patients with AH and to identify potentially modifiable factors that would improve timely access to care.
Methods Used: We identified all patients with AH aged <6 months seen at a single freestanding children’s hospital from January 2021-December 2022. Data were collected on patient gender, race/ethnicity, characteristics of upper tract dilatation, timing of delivery, and socioeconomic status. Patients with and without PUC were compared.
Summary of Results: 250 patients met inclusion criteria. 179 (71.6%) were male, 122 (48.8%) were white, and 56 (22.4%) had PUC. The Figure shows level of neighborhood disadvantage (p=0.024). 8/56 patients with PUC (14.3%) and 23/194 (11.9%) patients without PUC experienced preterm birth (p=0.63). Patients with PUC had postnatal evaluation earlier than those without PUC (0.62 [0.2-5.0] vs. 2.1 [0.1-2.8] months (p<0.0001), but were equally likely to have bilateral AH (41.1% vs 41.2%, p=0.73). Patients speaking English (54/229; 23.6%) and those speaking other languages (LOE; 2/21; 9.5%) were equally likely to have PUC. Patients in less disadvantaged areas (ADI 1-2) were less likely to have PUC compared with those living in moderately disadvantaged areas (ADI 3-8; OR=0.51, 95% CI: 0.26-1.00), but equally likely to have PUC compared with patients living in most disadvantaged areas (ADI 9-10; OR= 1.52, 95% CI: 0.55-4.23). Of preterm infants, 25% of those living in ADI 1-2 had PUC, compared with 0% of those living in ADI 9-10 (OR=3.32, 95% CI: 0.57-11.4), and 24% of those speaking English had PUC, compared with 0% of those with LOE (OR=1.98, 95% CI; 0.09-45.6).
Conclusions: PUC is associated with earlier postnatal urologic evaluation, but—in our series—not with AH severity, language, race, or level of neighborhood disadvantage. However, among children living in ADI 9-10 with LOE, the proportion with PUC was notably low. Since access to general obstetric care is limited in these patient groups, our findings may not represent truly equitable care, but rather the exclusion of patients with limited or no prenatal care. Further research centering on patients living in disadvantaged areas and with LOE may identify patient- and community-level factors associated with differential access to care.
# 507
DID THE COVID-19 PANDEMIC CHANGE THE PREVALENCE OF SEXUAL ASSAULT AND HARASSMENT? AN ANALYSIS OF PHYSICIAN MEMBERS OF AMERICAN COLLEGE OF PHYSICIANS
Li P1, Fernandes C2, Prasad C2, Silberger J3, Dong F2. 1College of Osteopathic Medicine of the Pacific-Northwest Western University of Health Sciences, Lebanon, OR; 2College of Osteopathic Medicine of the Pacific, Western University of Health Sciences, Pomona, CA and 3Kaiser Permanente, Portland, OR
Purpose of Study: To determine prevalence of sexual assault and sexual harassment (SA and SH) among physician members of American College of Physicians (ACP). We also wished to determine the level of awareness of current policies and resources and determine sense of safety in online vs in person interactions during the pandemic.
Methods Used: In 2023, ACP conducted a webinar series on SA and SH in the medical profession. Registrants voluntarily completed a post-session online cross-sectional survey, which included physician members’ experiences with SA and SH during the COVID-19 Pandemic, perception of safety in online vs in-person interactions, relationship between years of experience and SA/SH, difference between male vs female experiences, and awareness of legislation regarding SA and SH. Local and national resources were provided in the event of triggering effects. Consent was determined through survey completion and submission. De-identified data was analyzed using chi-square tests to assess the difference in the responses between categorical variables. Fisher’s exact tests were conducted as the expected cell count <5.
Summary of Results: 49 participants responded. 66% were females, 60% had been practicing medicine for greater than 20 years. 9% had experienced SA and 12% experienced SH during the pandemic. 72% were aware of their institutional policy on SH and 61.5% on SA. 40.5% agreed/strongly agreed that they felt safer when engaging with others online during the pandemic. 87.2% agreed that a perpetrator should self-disclose on applications. Those who had practiced medicine for under 10 years had the highest probability of experiencing SA (p=0.0055) and SH (p=0.0012), as compared to their counterparts. Male physicians were more likely to experience SA (13.3% vs 7.1%, p=0.6018) and SH (20% vs. 7.7%, p=0.3365). Although not statistically significant, respondents facing financial stressors were more likely to experience SH (25% vs 4.2%, p=0.098).
Conclusions: Our study captured the prevalence and changes in SA and SH during the pandemic. Measures need to be undertaken to ensure remote interactions provide a safer environment and provide adequate resources and support to incoming junior physicians. On a positive note, a significant number of respondents were aware of their institution’s policies on SH and agreed that a perpetrator should self-disclose on job applications. Limitations of our study include the small sample size and the fact that healthcare trainees were not included.
# 509
CHILDHOOD OBESITY: DOES EFFICACY OF BEHAVIORAL INTERVENTIONS DIFFER BY RACE?
Pham C1, Estrada A1, Groner J1, Mei A1, Pande P1, Pang L1, Yu S1, Afghani B1, 2. 1UC Irvine School of Medicine, Irvine, CA and 2CHOC Hospital of Orange, Orange, CA
Purpose of Study: Obesity is a multifactorial disease and in the United States, it disproportionately affects Hispanic and Black children compared to White children. Family-based behavioral treatments are currently recommended for management of pediatric obesity. However, there are limited studies comparing the effectiveness of behavioral interventions among different races. The purpose of this study was to determine if there are racial disparities in the efficacy of behavioral interventions for pediatric obesity.
Methods Used: A literature search was performed through PubMed and Google Scholar using keywords “behavioral intervention”, “obesity,” “pediatric obesity,” and “racial disparities”. We also checked the bibliography of articles for additional studies. Only randomized controlled studies performed in the United States that included children <16 years of age and compared the effect of a behavioral intervention among different ethnic groups were included.
Summary of Results: The literature review yielded a total of four studies that fit the inclusion criteria (Table below). Components of the behavioral interventions included child and family involvement in group sessions about nutrition, physical activity, and goal setting. The primary outcome measured in all studies was change in body mass index (BMI) or percent change in overweight status. For all studies, the intervention group had greater decreases in BMI than the control group and the decrease was statistically significant in 3 of the studies. In two studies, White children had greater change in weight loss than Black children in the intervention groups and in the other two studies, no significant differences were found among different racial groups. The study that included interventions for the whole family (including parents and siblings) with goal setting had the highest sustained impact (Epstein et al). The programs required multiple sessions and some participants dropped out. There was also requirement for training of clinic staffing. The limitations of the studies included small sample size for subgroup analysis accounting for different variables that could contribute to obesity.
Conclusions: Our literature review suggests that although family-based behavioral interventions are effective in management of pediatric obesity, there may be racial disparities in the efficacy of these interventions. Larger family-based behavioral interventions studies that include diverse study populations and take into account other barriers, such as economic circumstances, access to healthy food options, and exercise facilities are warranted. To sustain family-based behavioral interventions, partnerships with local and national organizations are needed to address some of the challenges faced by patients and families as well as provide support and resources for staff training.
Summary of controlled studies comparing the efficacy of interventions for obesity among different races.
First Author’s Last Name, Publication Year
Population N, Age Range, BMI
Ethnic Groups N and %
Intervention and Control Definition
Outcomes Measured
% Comparison or Odds ratio and p-value or Confidence Interval
Summary of Findings
Savoye, 2011
N=174 obese children8-16 yearsBMI > 95th percentile of age range
White=36.7%, Hispanic=38.5%, Black=24.7%
Group 1: 12 months lifestyle intervention including exercise, nutrition, behavior modification
Control: Counseling every 6 months
BMI, percent body fat, total body fat mass, total cholesterol, LDL cholesterol, blood pressure, fasting plasma glucose and insulin
BMI of intervention vs control at 24 month follow-up: -0.16 (95% CI: -0.23 to -0.09), p<0.0001
There was a sustained treatment effect at 24 months. There were no statistical differences in dropout rates
among ethnic groups or in any other aspects.
Group 1: Parents and child attended 20 hours of education/treatment sessions about diet, physical activity and skills to change behaviorGroup 2: Only parents attended education/treatment sessions
Standardized BMI (BMIz) scores
BMIz Baseline vs 18 month follow-up: White: 1.99 to 1.78, Hispanic: 2.01 vs 1.83, NHNW: 2.0 to 1.88; Race/Ethnicity x Treatment interaction, p=0.719
The BMIz decreased in all ethnic groups, but there was neither a significant difference among different ethnic groups nor between the control and intervention groups.
Davison, 2021
N=179 parent/child dyads
7-11 yearsChildren BMI >= 85th percentile of age/sex range and had one parent with BMI >25
White=71.8%, Black=15.4%, Other=12.9% (Asian=0.8%, Native Hawaiian/Pacific Islander=0.4%, More than one Race=11.2%, Unknown=0.4%)
Group 1: 4 months of intense family-based behavioral weight-loss treatment (FBT) followed by weekly or biweekly sessions for 4-12 monthsControl: Education only
% change in overweight (OV) and child BMI
White vs Black vs other races % OV: 14.5% vs 10.8% vs 10.5%, p=0.018
White children had greater decreases in child %OV than children of other races, but all groups had significant relative weight loss. Children from households with higher income also had greater decrease in child %BMI.
Epstein, 2023
452 children and
parent dyads,6-12 years, children with BMI>85th percentile, also included 116 siblings with BMI>25
Group 1: 26 Individual family sessions with weight goals, activity plans, behavioral goal setting within 24 monthsControl: Usual primary care
% change above median BMI of child
White vs Black children in intervention group: −6.22% [95% CI, −8.02% to −4.42%]; p < 0.001)
In the intervention group, White children had greater % change above median BMI compared to Black children.
BMI=Body Mass Index, BMIz=Body Mass Index Score.
Endocrinology and Metabolism III
Concurrent Sessions
8:00 AM
Saturday, January 20, 2024
# 510
Pathophysiological role of ZADH2 in Brown and White Adipocytes
Kumar A2, Lodhi I1. 1Washington University School of Medicine, St. Louis, MO and 2Western University of Health Sciences, College of Osteopathic Medicine of the Pacific, Pomona, CA
Purpose of Study: Adipocyte differentiation can be regulated via several factors, however, Peroxisome proliferation-activated receptor γ (PPARγ) has been identified as the master regulator. Recent studies show that increased expression of prostaglandin-reductase-3 *(also known as PTGR3 or ZAHD2) affects the growth of preadipocytes. ZADH2 converts 15-keto-PGE2 (an endogenous ligand of PPARγ) into inactive 13, 14 dihydro-15-keto-PGE2, suppressing adipogenesis. The purpose of our study was to understand the role of ZADH2 during different time points in mature brown adipocytes and use such findings to predict the role of ZADH2 in the growth of white adipocytes.
Methods Used: To study the function of ZADH2 in brown adipocytes, we differentiated stromal vascular fraction (SVF) cells into brown adipocytes.
Cell Culture: The brown adipocytes were cultured in Dulbecco modified Eagle’s medium (DMEM) with 10% FBS, 1% penicillin–streptomycin solution and 1% glutamine. The cultivation dishes were incubated under a humidified atmosphere of 5% CO2 at 37 °C. Cultivated SV cells were harvested at 80–90% confluence following treatment with trypsin–EDTA solution. The trypsin–EDTA-treated SV cells were collected in a 15 mL tube before removing the medium by centrifugation at 1200g at 4 °C for 3 min. To induce brown adipocyte differentiation, 70-80% confluent cells were cultured with 5uM Dexamethasone, 0.02uM Insulin, 0.5uM Isobutyl methylxanthine, 1uM Rosiglitazone, 1nM T3, and 125 uM Indomethacin. Two days later, the cells were cultured with DMEM containing 0.02uM insulin and 1 nM T3 for 6 days. The RNA was collected at Day 0, Day 2, and Day 4 to measure ZADH2 mRNA expression levels.
Summary of Results: Although the mRNA expression of ZADH2 was not significant in different time points in brown adipocytes due to a low number of replicates, the trend does suggest that increased mRNA expression of ZADH2 could lead to increased adipogenesis in brown adipose tissue. More replicates of the time points and experiment would be necessary to confirm this trend.
Conclusions: Our experiment demonstrated no significant expression of ZADH2 in different time points. Due to a low number of replicates, further investigation would be needed. In the next steps, it would be beneficial to duplicate such results with additional time points and levels of mRNA expression of ZADH2 with a higher number of replicates. It would also be useful to understand the role of ZADH2 expression in mature white adipocytes. If the pathophysiological mechanism of the role of ZADH2 were to remain consistent in white adipocytes, we would predict that the silencing of ZAHD2 would lead to decreased white adipogenesis that could ultimately help in controlling metabolic diseases like obesity.
# 511
Decreased Executive Function and Fine Motor Skills in Pediatric Patients with Congenital Adrenal Hyperplasia
Yamashita NL1, Deras E1, O’Neil SH3, 4, Pickering TA2, Simon G1, Kim MS1. 1Children’s Hospital Los Angeles, Los Angeles, CA; 2University of Southern California, Los Angeles, CA; 3The Saban Research Institute of Children’s Hospital Los Angeles, Los Angeles, CA and 4Children’s Hospital Los Angeles, Los Angeles, CA
Purpose of Study: Congenital adrenal hyperplasia (CAH) is the most common cause of primary adrenal insufficiency in children and involves impaired cortisol synthesis and excess androgen production. Youth and adults with CAH exhibit affected brain morphology including smaller total intracranial, prefrontal cortex, and medial temporal lobe volumes. Additionally, older children are at risk for developmental delay and mental health concerns, with limited studies on developmental progression throughout childhood and adolescence. Therefore, we aimed to investigate neuropsychological development in pediatric patients with CAH at a large comprehensive care center.
Methods Used: Cross-sectional study of 42 pediatric patients (4-21 years old; 55% female) with classical CAH due to 21-hydroxylase deficiency. All participants completed age-appropriate assessments of cognitive function (NIH ToolBox Cognition Battery), gross motor (NIH ToolBox Grip Strength) and fine motor skills (Purdue Pegboard). Tanner staging for puberty was performed by a pediatric endocrinologist. Data presented as mean ± SD, with a population normative mean of 100.
Summary of Results: Executive function (inhibitory control, working memory) scores were lower in patients with CAH compared to the normative mean (NIH Toolbox Flanker Inhibitory Control 92.10 ± 15.06, 30th %ile, p = 0.02; and List Sort Working Memory 94.12 ± 11.71, 35th %ile, p = 0.04). Both inhibitory control (r = -0.68, p < 0.01) and cognitive flexibility (Dimensional Change Card Sort r = -0.38, p = 0.02) scores were inversely correlated with age. As well, similar correlations were noted for pubertal stage (Inhibitory control: Tanner I-II 100.58 ± 12.31, Tanner III-V 84.43 ± 13.25, p < 0.001; Dimensional Change Card Sort: Tanner I-II 101.68 ± 16.05, Tanner III-V 91.10 ± 15.17, p = 0.039). On the other hand, working memory was not associated with age (r = 0.2, p = 0.27) or puberty (p = 0.084) in patients with CAH. As well, overall cognitive flexibility scores were not different compared to the normative mean (Dimensional Change Card Sort 96.12 ± 16.30, 40th %ile, p = 0.25). Overall mean scores remained within ± 1SD for patients.
Fine motor scores were lower in patients with CAH (dominant hand 81.96 ± 18.45, 11th %ile, p < 0.001, non-dominant 84.64 ± 15.48, 15th %ile, p < 0.001, both hands 86.81 ± 17.67, 19th %ile, p < 0.001). However, there were no significant differences in gross motor skills in patients with CAH (all p’s > 0.3).
Conclusions: Our findings suggest decreased executive functioning (inhibitory control, working memory) with increasing age and puberty in pediatric patients with CAH compared to the population normative mean. Elucidating the relationships between brain and behavior in patients with CAH could help understand comorbidities such as obesity and affected mental health in this condition.
# 512
THE ROLE OF MITOGEN-ACTIVATED PROTEIN KINASE PHOSPHATASE IN REGULATING THE β3-ADRENERGIC PATHWAY IN ADIPOCYTES
Kurlagunda T1, Feng X1, Saltiel AR2. 1University of California, San Diego, La Jolla, CA and 2University of California, San Diego, La Jolla, CA
Purpose of Study: Adipocyte thermogenesis has been suggested as a therapeutic approach to increase energy expenditure, reduce weight, and fight insulin resistance. Browning of white adipocytes is characterized by the appearance of ‘beige’ adipocytes with enrichment of mitochondria, multilocular lipid droplets and expression of UCP1, promoting heat dissipation. The transcription of UCP1 in white fat is controlled by sympathetic activation via β3-adrenergic receptors (β3-AR). Extended cold exposure or repeated injection of β3-AR agonists lead to marked upregulation of UCP1 and browning of white adipose tissue (WAT). While the pathways controlling UCP1 expression are not completely understood, activation of both protein kinase A and p38 MAPK are involved. However, it remains unclear how adrenergic activation leads to p38 activation. Understanding the exact pathway of beiging can help us find a cure for diabetes.
Methods Used: To understand p38 pathway activation, we first looked at the expression pattern of MKP, mice were injected with CL-316243 for 7 days and the iWAT was collected. MKP mRNA levels were studied via RT-qPCR, and its protein levels were studied via western blotting. To further demonstrate MKP’s role in the p38 pathway, we overexpressed MKP in differentiated adipocyte cells and treated them with CL-316243. The UCP1 mRNA levels and the p38 protein activation were studied. We also conducted a siRNA-mediated MKP knockdown in differentiated adipocyte cells and treated the cells with CL-316243. The UCP1 mRNA levels and the p38 protein activation were studied.
Summary of Results: We showed that MKP is a potential regulator of p38 pathway during adipocyte thermogenesis. Brown adipocytes showed lower MKP expression when compared with those in white adipocyte tissues, demonstrating its potential role in inhibiting adipocyte thermogenesis. We further identified that lenti-virus mediated MKP overexpression leads to decreased p-p38 levels and lower UCP1 expression in response to CL-316243 treatment in differentiated adipocyte cells. On the contrary, siRNA-mediated MKP knockdown leads to increased p-p38 activity and higher UCP1 induction with CL-316243 treatment in differentiated adipocyte cells.
Conclusions: Our research shows that activating the β3 adrenergic pathway results in the decreased activity of MKP, allowing for the production of UCP1, as MKP blocks p38 activity. This further causes the browning or beiging of adipocytes, increasing energy expenditure. Thus, inhibiting MKP activity can be a therapeutic approach to activate adipocyte browning and treat diabetes.
# 513
UNCOVERING THE CONNECTION BETWEEN GENETIC RISK AND PHENOTYPIC OUTCOME IN POLYCYSTIC OVARIAN SYNDROME
Tidwell AJ1, Welt C1, 2. 1University of Utah School of Medicine, Salt Lake City, UT and 2University of Utah, Salt Lake City, UT
Purpose of Study: Polycystic ovarian syndrome (PCOS) affects 10% of reproductive-aged women worldwide, making it the most common endocrinopathy of this population. Despite the prevalence of PCOS, the etiology of the syndrome remains unclear. The genetic architecture of the disease is emerging, but there is little data exploring the effect of genetic risk on clinical presentation. The purpose of this study is to identify a connection between the genetic risk of women with PCOS and their variable phenotypic outcome, eventually leading to a better understanding of the underlying pathophysiology of the disease.
Methods Used: In this study, we analyzed the relationship between 29 genome-wide associated PCOS risk variants and the phenotypes of women with PCOS and controls. Women of European descent from Boston with PCOS (n=527) as diagnosed by the NIH Criteria matched with controls (n=426).
Subjects underwent physical examination, hormone sampling, ovarian ultrasound, and were genotyped for the 29 risk variants. Linear regression analysis was used to detect correlation between genotype and phenotypic traits with a p-value <0.0033 used for significance after Bonferroni correction.
Summary of Results: Of the 29 risk loci, 8 were significantly correlated with one of the hallmark traits of PCOS: irregular menses (gonadotropins), hyperandrogenism, polycystic ovarian ultrasound, and metabolic dysfunction. Three variants were associated with gonadotropin levels in loci containing the genes NEIL2/GATA4 (p=0.001), PRSS23 (p<0.001), and FSHB (p<0.001). Three variants were associated with polycystic ovarian morphology at loci containing SHBG (p<0.001), ZBTB16 (p=0.003), and CYP3 (p<0.001). Two variants were associated with androgen levels in loci containing NEIL2/GATA4 (p<0.001) and CYP3 (p<0.001). Two variants were associated with metabolic traits at loci containing INHBB (p<0.001) and FTO (p=0.002).
Conclusions: The genotype relationship to these fundamental PCOS traits confirms their underlying importance in PCOS etiology and pathophysiology. These results demonstrate that PCOS genetic risk variants may act through changing hormone levels and the development of ovarian follicles, along with increasing obesity risk. Interestingly, the genetic risk appears to drive traits that underly the classical clinical presentation of PCOS.
# 514
NLRP3 INFLAMMASOME AS A POTENTIAL LINK IN THE UNDERLYING PATHOGENESIS OF DIABETES AND CROHN’S DISEASE
Gargaloyan A, Agrawal DK, Rai V. Western University of Health Sciences, Pomona, CA
Purpose of Study: Recent studies suggest a link between type 2 diabetes and chronic intestinal inflammation with inflammatory bowel disease. Patients with IBD may develop diabetes. However, the underlying molecular mechanisms of the interplay between diabetes and Crohn’s disease are not well understood. Increased activity of inflammasomes and decreased activity of a regulatory phosphatase, protein tyrosine phosphatase non-receptor type 2 (PTPN2), could be the underlying causative factors in the pathogenesis of Crohn’s disease. This could result in the elevation of interleukin (IL)-12, IL-1β, toll-like receptor (TLR)-4, and decreased TLR-9. We examined the expression of these factors in the intestinal tissues of nondiabetic and diabetic rats to better understand the interaction between diabetes and Crohn’s disease. We hypothesized that attenuated expression and activity of PTPN2 in diabetes results in increased NLRP3 inflammasome assembly and upregulation of pro-inflammatory cytokines in the cells of the large intestine and colon. Increased inflammation can allude to a compounding effect of diabetes and inflammation on Crohn’s disease with synergistically increasing severity.
Methods Used: We used Sprague Dawley rats and induced type II diabetes with a low dose (25mg/kg) of Streptozotocin after feeding rats a high-cholesterol diet for two months (#R22IACUC020). After completion of ongoing experiments in the lab for other projects, we collected colons from nondiabetic and diabetic rats (N=5 in each group). Hematoxylin and eosin staining, immunohistochemistry, and quantitative PCR for PTPN2, NLRP3, TLR-9, IL-12, IL-18, IL-1β, and RelA were performed. The data analysis was done using GraphPad Prism 9 and a probability (p) value of < 0.05 was considered statistically significant.
Summary of Results: H&E staining showed diffusely enlarged crypts and an increased number of goblet cells with focal inflammation in lamina propria, muscularis mucosa, and submucosa in diabetic rats compared to nondiabetic rats. qPCR results showed significantly increased mRNA transcripts of PTPN2, NLRP3, IL-18, IL-1β, and RelA while decreased for IL-12 and TLR-9 in diabetic rats compared to nondiabetic rats. Immunohistochemistry imaging supported the finding of qPCR and immunopositivity for PTPN2, NLRP3, IL-18, IL-1β, and RelA.
Conclusions: An increased expression of inflammatory mediators in diabetic rats compared to nondiabetic rats suggests that diabetes-mediated inflammation is involved in the pathogenesis of Crohn’s disease and targeting NLRP3 inflammasome may have a therapeutic effect. The findings of this study may pave the way to develop better treatment strategies for patients with diabetes and Crohn’s disease using targeted therapy targeting NLRP3 inflammasome.
# 515
Ectopic Cushing’s Syndrome Presenting As Hypertensive Emergency and Psychosis
Jannareddy N, Lovato C. University of New Mexico School of Medicine, Albuquerque, NM
Introduction: Approximately 15% of endogenous Cushing’s syndrome cases have been attributed to ectopic ACTH-secreting tumors which are often occult. It is essential to detect and treat the signs and symptoms of ectopic Cushing’s syndrome as this condition can result in significant morbidity and mortality if untreated. Herein, we present a case of ectopic Cushing’s syndrome in a 64-year-old female who initially presented with hypertensive emergency and psychosis.
Case: A 64-year-old previously healthy Caucasian female presented to the ER with chest palpitations, weakness, elevated blood pressure and new onset confusion. She was diagnosed with hypertensive emergency, new onset atrial fibrillation, and hypokalemia. She was discharged on antihypertensive medication and potassium supplements after clinical improvement. She, however, returned to the ER a few days later for worsening confusion after the patient’s husband found the patient attempting to feed her medication to their dog. She had rapid weight gain of 20 pounds, excessive fatigue, decreased endurance, facial hair growth over the course of 6 weeks. On physical exam, the patient was noted to have moon facies, hirsutism, supraclavicular and dorsocervical fat pads, facial erythema, central obesity, and proximal myopathy. Midnight serum cortisol, 24 hour urine free cortisol and ACTH were elevated; 80.9 ug/dL (<7.5 ug/dL), 2,590 ug(<45 ug) 186 pg/mL (7-63 pg/mL). MRI of the brain was negative for a pituitary adenoma. CT scan of the chest, abdomen, and pelvis was negative for an ectopic source of ACTH. The patient was diagnosed with Cushing’s syndrome and was discharged on spironolactone and olanzapine with improvement in her blood pressure and psychosis. Inferior petrosal sinus sampling confirmed the source of ACTH was ectopic. Given no obvious tumor on initial imaging, the patient was started on ketoconazole 200 mg po bid after which she noticed improvement in fatigue, muscle weakness and psychosis. Her 24 hour urine cortisol level improved to 29.06 ug (<45 ug). A Cu-64 DOTATATE PET scan revealed multiple sclerotic osseous lesions suspicious for metastases and an 8 mm lesion in the right lower lobe of the lung. The patient was referred to the Mayo clinic for further evaluation after biopsy of one of the bone lesions was negative for malignancy and the lung lesion was less likely the ectopic source. Despite treatment with ketoconazole, her symptoms recurred and she underwent bilateral adrenalectomy. The search for the primary tumor continues and the patient is under active surveillance by oncology.
Conclusion: This case highlights the importance of recognizing the clinical presentation of Cushing’s syndrome, particularly those rare cases with an ectopic source of ACTH. As it can be challenging to localize these rare tumors on imaging, management of ectopic Cushing’s syndrome often involves addressing treatment of the hypercortisolism first and then, the malignancy once identified.
Genetics II
Concurrent Sessions
8:00 AM
Saturday, January 20, 2024
# 516
Trajectory of Project Baby Bear Rapid Genome Sequencing Project: A Review of Long-Term Follow Up at a Single Center
Chan R1, Wigby K2, Martin MM2, Shankar SP2. 1UC Davis School of Medicine, Sacramento, CA and 2University of California, Davis and UC Davis Children’s Hospital, Sacramento, CA
Purpose of Study: Project Baby Bear was a prospective quality improvement project which demonstrated the clinical utility and economic impact of ultrarapid or rapid whole genome sequencing (rWGS) in neonatal and pediatric intensive care units. This study found that rWGS provided a diagnosis for 40% and changed medical care for 32% of the infants. Given these positive outcomes, rapid genomic testing is becoming more feasible and efficient in the hospital setting. However, there is limited information on the long-term clinical outcomes and follow up of these individuals. We sought to evaluate the long-term outcome of rWGS among individuals who have had rWGS as part of Project Baby Bear.
Methods Used: A retrospective chart review of 53 participants was conducted using data from one large, tertiary academic center involved in Project Baby Bear. We evaluated follow-up among multiple sub-specialties, including genomic medicine, and we report on their current health.
Summary of Results: There were 39 males and 14 females in the study with a diverse ethnic distribution, including 26% White, 11% Black, 36% Hispanic/Latinx, 4% Asian, and 10% Other. Their ages ranged from 1 day to 18 months with 36% born preterm and 64% born at term. 8 participants are now deceased. WGS results were as follows: 20% pathogenic, 10% likely pathogenic, 10% variant of uncertain significance, and 59% with negative test results. Majority of patients had at least one follow-up, and the specialty distribution is shown in figure 1 below.
Conclusions: Over 95% of participants were seen by multiple specialties, representing their complexity of care irrespective of positive or non-diagnostic genomic test results. The most frequent follow-ups were with gastroenterologists and cardiologists given the high prevalence of feeding difficulties and congenital heart defects. Follow-up in genetics clinic helped with the overall management plan based on expected clinical features of a particular rare genetic condition with a positive genetic test result. As the clinical presentation of infants evolve with time, including these additional clinical phenotypes and re-analysis of genome sequence may help determine the underlying genetic etiology in additional patients and facilitate precision care. Contacting all individuals in a prospective manner with extended follow up would be helpful in studying the long term outcome of all individuals with rWGS and in re-analysis of the genome with expanded spectrum of clinical features.
# 517
EXTRAORDINARY BABIES STUDY: GENETIC COUNSELING IMPLICATIONS OF DISCORDANT PRENATAL NONINVASIVE SCREENING RESULTS IN SEX CHROMOSOME ANEUPLOIDIES
Howell S1, Davis S1, Ross J2, Tartaglia N1. 1University of Colorado Anschutz, Aurora, CO and 2Thomas Jefferson University, Philadelphia, PA
Purpose of Study: Sex chromosome aneuploidies (SCA) are chromosome abnormalities occurring in 1 in 500 live births with highly variable phenotypes. Tetrasomy SCAs are less common, manifesting more significant medical, developmental and psychological features compared to more common trisomy SCAs. Routine noninvasive prenatal screening (NIPS) has relatively poor positive predictive values (PPV) in SCAs, which often direct genetic counseling discussions towards false positive likelihood rather than thoroughly addressing various possible cytogenetic and phenotypic outcomes. Aims of this project are to illustrate cases of discordant NIPS vs. diagnostic results from participants in the eXtraordinarY Babies Study and explore genetic counseling implications.
Methods Used: The eXtraordinarY Babies study is a natural history study of children with prenatal diagnoses of SCA (current n=310). This analysis includes participants selected from the study cohort based on review of NIPS results in comparison to diagnostic cytogenetic results to identify discordance. A discordant result was determined if the NIPS result varied from the diagnostic cytogenetic result. Review was conducted by a board-certified genetic counselor. Participants were excluded if either report could not be obtained for review. Descriptive statistics were calculated to describe the sample and summarize the data.
Summary of Results: Of 201 infants, 11.4% (n=23) were discordant with confirmed diagnoses of XXYY (n=9), XXY (n=6), XXX (n=4), XYY (n=1), XXXY (n=2) and XXXX (n=1). Discordance categories included (in rank order): 1) NIPS trisomy result with tetrasomy diagnosed, 2) NIPS result inconclusive/atypical gender, 3) NIPS trisomy result with mosaicism diagnosed, 4) NIPS autosomal trisomy result with SCA trisomy diagnosed, 5) NIPS monosomy result with trisomy diagnosed, and 6) NIPS trisomy with different SCA trisomy diagnosed. Fifteen infants in this cohort (65.2%) had diagnostic testing deferred during pregnancy and confirmed postnatally.
Conclusions: Traditional genetic counseling for NIPS results demonstrating an increased risk for SCA is inadequate given a high degree of discordance that jeopardizes accuracy of the information discussed during counseling. Since more than half of parents of infants with SCA who experienced NIPS SCA+ results defer diagnostic testing until birth, discussions regarding discordant diagnostic outcomes, some with more significant phenotypes, must be addressed for true informed decision making.
Discordant Results Between NIPS and Diagnostic Karyotype.
NIPS Result
Fetal Fraction per NIPS report (%)
Maternal Age Range at Delivery (yrs)
Maternal Pre-Pregnancy BMI (kg/cm2)
Diagnostic Test Pursued
Diagnostic Test Result
45,X
NR
35-39
23.9
amnio
47,XXX
45,X
10.5
35-39
26.7
amnio
47,XXX
47,XXX
10.7
35-39
29.4
amnio
47,XXX[6] / 46,XX[9]
47,XXX
NR
20-24
28
postnatal
48,XXXX
47,XXY
6.9
30-34
21.5
amnio
47,XXY[91%] /46,XX [9%]
47,XXY
NR
30-34
22.4
amnio
48,XXYY
47,XXY
6
15-19
19.2
postnatal
48,XXXY
47,XXY
NR
25-29
39
postnatal
48,XXXY
47,XXY
11
30-34
20
postnatal
48,XXYY
47,XXY
13.1
30-34
28.3
postnatal
48,XXYY
47,XXY
NR
45-49
22.1
postnatal
48,XXYY
47,XXY
4
20-24
25.6
postnatal
48,XXYY
47,XXY
4
35-39
36.6
postnatal
48,XXYY
47,XXY
7
30-34
26.4
postnatal
48,XXYY
47,XYY
6.3
35-39
21.2
postnatal
47,XXY
47,XYY
7.1
30-34
24
postnatal
48,XXYY
47,XYY
6.1
30-34
30.2
postnatal
48,XXYY
Atypical result for sex chromosome
7
40-44
26.9
amnio
47,XXX
Atypical result for sex chromosome
5.6
30-34
19.8
amnio
47,XXY
Inconclusive
6
30-34
36.5
amnio
47,XXY
Inconclusive
11.3
35-39
25.5
postnatal
47,XXY
Increased risk for trisomy 13/18/triploidy
3.2
30-34
29.8
postnatal
47,XXY
Increased risk for trisomy 21
NR
35-39
18.6
postnatal
47,XYY
NR=not reported NIPS=noninvasive prenatal screening BMI=body mass index.
# 518
The eXtraordinarY Baby Study: Natural History of Infants Diagnosed with XXYY in the Prenatal Period
Nocon K, Howell S, Tartaglia N. University of Colorado School of Medicine, Aurora, CO
Purpose of Study: XXYY syndrome is a rare sex chromosome variation occurring in 1:18,000-1:40,000 males. Most literature focuses on males identified by genetic testing during childhood or later due to neurodevelopmental or medical problems. In the last 10 years, noninvasive prenatal screening has expanded, resulting in the increased numbers of infants identified with sex chromosome aneuploidy in the prenatal period. Individuals with XXYY share some phenotypic features with XXY/Klinefelter syndrome, however XXYY is associated with additional medical problems and more significant neurodevelopmental and psychological features. In this project, our aim was to describe clinical and developmental features in a group of XXYY infants identified in the prenatal period, describe medical and developmental features of an unselected cohort from birth in order to compare findings to what has been described in postnatally diagnosed patients.
Methods Used: Participants with XXYY were evaluated as part of the eXtraordinarY Baby Study, a natural history study following infants with a prenatal diagnosis of a SCA followed from birth to 3 years of age. Data was collected from study visit medical history interviews and medical record review. Adaptive skills were measured using the Vineland Adaptive Behavior Scales – 3rd edition. Descriptive statistics were calculated based off the information gathered to describe the sample.
Summary of Results: Ten infants were prenatally identified with a sex chromosome trisomy (SCT) via non-invasive prenatal screening (NIPS) and later confirmed XXYY postnatally. Of the 10 infants, 40% were born with congenital malformations: ear anomalies and cardiac septal defects being the most common. 90% of infants in this cohort have low muscle tone, 90% have food allergies, and 70% had early feeding problems. Developmental delays were identified in 80%, including both language and motor delays. 90% of participants were enrolled in early interventions, 60% received more than one intervention. Mean overall adaptive functioning at 2 years of age fell in the below average range, with strengths in motor skills and socialization domains, and weaknesses in communication skills.
Conclusions: The medical and developmental features found in the prenatally identified cohort are similar to those identified in previous literature, with high rates of hypotonia, early feeding problems, and food allergies. There were fewer congenital malformations in this cohort compared to previous cohorts diagnosed in the postnatal period. Longitudinal follow-up will allow for more comparisons of developmental and health outcomes to postnatally identified samples to help guide care and genetic counseling.
# 519
INITIAL DATA FROM THE GALAXY REGISTRY: GENERATING ADVANCEMENTS IN LONGITUDINAL ANALYSIS IN X & Y CHROMOSOME VARIATIONS
Molison K1, Howell S1, 2, Carl A1, Davis S1, 2. 1eXtraordinarY Kids Clinic, Children’s Hospital Colorado, Aurora, CO and 2University of Colorado School of Medicine, Aurora, CO
Purpose of Study: Sex chromosome aneuploidies (SCAs) are a group of genetic conditions characterized by an atypical number of sex chromosomes. Most SCA research has been limited by small sample sizes, negligible diversity, little SCA community involvement, and a non-longitudinal lens. To address these limitations, we developed the Generating Advancements in Longitudinal Analysis in X & Y Chromosome Variations (GALAXY) Registry, a multicenter clinical data registry that stores the medical data and biospecimens of individuals with SCAs. To better understand registry participant characteristics and to assess current recruitment strategies, we analyzed the demographic and diagnostic information of the participants enrolled within the first 15 months of the GALAXY Registry.
Methods Used: Within its first 15 months, a total of 272 participants enrolled in the GALAXY Registry. Of these 272 enrollees, 168 had complete demographic and diagnostic data (including an available genetic test) and were included in this analysis. Participants were categorized as underrepresented in research if they reported a minority race, ethnicity, gender, language, or payor status (a proxy for socioeconomic status). Diagnostic delay was calculated as the length of time between the date of symptom onset and the date of SCA diagnosis. Descriptive statistics were utilized to express key demographic and diagnostic information.
Summary of Results: The median age of enrollment is 11.5 years, with a range of 0 - 73 years. 71.4% of participants identify as Non-Hispanic White. 38.7% of participants are underrepresented in research, with payor status (19.6%), race (19.0%), and ethnicity (16.7%) being the primary sources of underrepresentation. 54.2% of participants were diagnosed postnatally, with a median diagnosis age of 7.9 years (range: 0 - 48 years) and a median diagnostic delay of 2.6 years (range: 0 - 14 years). Advanced maternal age was the most common reason for prenatal testing (54.7%), while developmental delay before age 3 (34.1%), learning and behavioral concerns (16.5%), and “other” (19.8%) were the most common reasons for postnatal testing. The majority of participants (73.6%) have non-mosaic 47,XXY (Klinefelter syndrome).
Conclusions: GALAXY Registry participants currently have diversity in age and timing of diagnosis, but not in race, ethnicity, or karyotype. Indications for postnatal genetic testing appear largely variable, emphasizing the irregularity of the clinical presentation of SCAs. Future work will focus on increasing enrollment of diverse participants, increasing the number of clinic sites participating in GALAXY, and analyzing how diagnostic and perinatal history vary by karyotype. We will also use the registry to examine the longitudinal course of SCA conditions.
# 520
AN EXTRA CHROMOSOME AMONG WOMEN IN THE MILLION VETERAN PROGRAM: A MORE BENIGN PERSPECTIVE OF TRISOMY X
Klamut N1, 2, Teerlink C3, 4, Lynch J3, 4, Ross J5, 6, Hauger R7, 8, Davis S1, 2. 1University of Colorado School of Medicine, Aurora, CO; 2Children’s Hospital Colorado, Aurora, CO; 3VA Salt Lake City Healthcare System, Salt Lake City, UT; 4University of Utah Health, Salt Lake City, UT; 5Nemours Children’s Hospital, Wilmington, DE; 6Thomas Jefferson University, Philadelphia, PA; 7University of California San Diego School of Medicine, La Jolla, CA and 8University of California San Diego, La Jolla, CA
Purpose of Study: Trisomy X syndrome (47,XXX) occurs in ~1 in 1000 females who have an additional X chromosome. Literature in Trisomy X has largely been limited by clinical ascertainment which may not be generalizable to all females with an additional X chromosome. The aims of this study were to establish the prevalence of females with 47,XXX in our military cohort and to compare sociodemographic, military service, medical morbidity, mortality, and participant-reported outcomes between females with 47,XXX and typical 46,XX controls.
Methods Used: The Veteran’s Health Administration (VA) Million Veteran Program (MVP) enrolled 73,759 females from across the United States and obtained SNP-based genotype, electronic health records, and survey data. Variables of interest were obtained from a combination of VA records and self-reported answers on the Baseline Survey and Lifestyle Survey. The Charleston Comorbidity Index (CCI) was used to estimate morbidity. Every female with 47,XXX in our cohort (n=61) was matched to five 46,XX controls (n=305) on age and genetic ancestry. Karyotype groups were compared using t-tests for continuous variables and chi-squared for categorical variables (exploratory α<0.05), with calculation of odds ratios (OR) and 95% confidence intervals (CI).
Summary of Results: We identified 61 females with an additional X chromosome, corresponding to a prevalence of 103 per 100,000 females. The prevalence of 47,XXX was significantly different between genetic ancestral groups. 27.9% had a clinical diagnosis of Trisomy X in their EHR. Females with 47,XXX were taller (170.7 ± 7.4cm vs 164.6 ± 6.9cm; p<0.001), however BMI was not different. Number of outpatient encounters were greater in the 47,XXX group (23.7/year) than in controls (19.0/year; p=0.026), but there were no differences in hospitalizations or emergency encounters. There was no difference in calculated Charlson Comorbidity Index. Self-reported prevalence of most medical diagnoses were similar between cases and controls with the exception of kidney disease (OR= 12.3; 95% CI 2.9-51.8), glaucoma (OR= 5.1; 95% CI 1.5-13.9), and congestive heart failure (OR=5.6; 95% CI 1.4-24.2). Military service metrics were similar between groups. Females with 47,XXX were less likely to be employed (p=0.008) and reported a lower annual income (p=0.023) at the time of survey completion, without differences in education level. Quality of life measures were not different.
Conclusions: The prevalence of Trisomy X among military veterans is similar to that reported in the general population, although may differ in genetic ancestry. In this predominately undiagnosed sample, 47,XXX conferred few differences in sociodemographic, lifestyle, and health variables when compared to matched controls. These results offer an opposing, but reassuring perspective to the previously endorsed Trisomy X narrative.
# 521
A novel non-coding deletion at Xq28 in a patient with X-linked primary immunodeficiency
Case Report: We evaluated a 2-year-old male with a personal and family history of immunodeficiency at the GREGoR Stanford Site, member of the GREGoR Consortium (Genomics Research to Elucidate the Genetics of Rare Diseases). He initially presented with low T cell receptor excision circle levels on newborn screening. Further testing revealed near absence of recent thymic emigrants, defects of T cell proliferation and decreased natural killer cell function. He underwent hematopoietic stem cell transplantation at 9 months old. Family history is significant for 7 maternal male relatives who died from infections in childhood in a pattern consistent with X-linked inheritance. Clinical genetic testing including microarray, exome and genome sequencing (GS) and transcriptome sequencing (RNA-seq) were non-diagnostic.
Trio GS data was re-analyzed with a structural variant calling and prioritization pipeline, and results were integrated with expression outliers from trio blood RNA-seq analysis. Re-analysis prioritized a novel hemizygous maternally inherited 2.8kb deletion at Xq28 encompassing a primarily intergenic region upstream of ARHGAP4 with partial overlap of the 3’UTR of NAA10. RNA-seq identified significantly reduced expression of ARHGAP4 (z-score -11.21) and slightly reduced expression of NAA10 (z-score -5.01) when compared to 282 controls. We considered this a promising diagnostic candidate as it was the only under-expression outlier that correlated with a rare variant on the X chromosome.
Patients reported with loss-of-function variants in NAA10 and ARHGAP4 do not demonstrate susceptibility to infection nor clinical immunodeficiency. A patient with a 34.4kb deletion overlapping with our patient’s deletion and a phenotype of immunodeficiency and nephrogenic diabetes insipidus is reported. The authors speculated that their patient’s immunodeficiency was caused by loss of the intergenic region between ARHGAP4 and NAA10 since it is highly conserved across species and involved in cellular response to hypoxemia. Recently, this intergenic region has also been described to have a regulatory role in chromatin accessibility and transcriptional regulation. We performed immunophenotyping mass cytometry on the patient’s peripheral blood mononuclear cells that showed an increase in gamma delta (γδ) T cells and decrease in double positive T cells, double negative T cells, CD4+ and CD8+ T cells. This suggests that the patient’s immunodeficiency may be caused by a disruption in the T cell maturation pathway.
Our patient is the second reported case with loss of the 2.8kb intergenic region between ARHGAP4 and NAA10 at Xq28 and primary immunodeficiency, providing further evidence for the locus-disease relationship. Research into the functional and epigenetic consequences of this deletion will clarify the mechanism of disease. Ongoing studies include segregation analysis, methylome sequencing and ATAC-sequencing.
# 522
MISCONCEPTIONS AND MISINFORMATION IN THE DIAGNOSTIC AND HEALTHCARE EXPERIENCES OF MALE RETT SYNDROME
Thompson TG1, 7, Gurfinkel D2, Klamut N1, Fu C3, Ferdinandsen K1, Ananth A4, Lane J4, Marsh E5, 6, Percy A4, Neul J3, Benke T1, 7. 1University of Colorado, Aurora, CO; 2University of Colorado, Aurora, CO; 3Vanderbilt University School of Medicine, Nashville, TN; 4University of Alabama at Birmingham, Birmingham, AL; 5University of Pennsylvania, Philadelphia, PA; 6Children’s Hospital of Philadelphia, Philadelphia, PA and 7Children’s Hospital Colorado, Aurora, CO
Purpose of Study: Rett syndrome (RTT), a neurogenetic disorder that results primarily from mutations in the transcriptional regulator Methyl-CpG-binding protein 2 (MECP2), is typically characterized by a period of relatively normal early development followed by regression of communication and motor skills and distinct hand stereotypies. A common misconception has been that, as an X-linked disorder, males with RTT do not survive gestation or have early-onset severe encephalopathy causing death in infancy. However, recent studies have revealed wider phenotypic heterogeneity. Despite frequent high disease severity, there are no clinical trials for male RTT, likely due to perceived low incidence and lack of awareness. The purpose of this study is to describe the diagnostic experience, parenting, and overall quality of life in male RTT through a mixed methods study design.
Methods Used: We are actively recruiting an international sample of parents of children with confirmed genetic diagnosis of male RTT (all ages, alive, deceased) to complete electronic surveys and in-depth, semi-structured interviews about their lived experiences. Descriptive statistics will summarize diagnostic experiences and child quality of life surveys (Quality of Life Inventory-Disability; QI) and Welch’s t-tests will compare to other genetic conditions. Qualitative themes will provide rich descriptions of diagnostic, healthcare, and parenting experiences. We plan to recruit N=40 parent participants by Jan. 2024.
Summary of Results: Preliminary quantitative results (n=14, 3 deceased) show age of diagnosis ranges from 1-16 years with a median (IQR) age of 3 years (4.92). Median time between onset of symptoms and RTT diagnosis is 1.75 years (3.88). Common diagnoses received prior to RTT include CP (29%), ASD (21%), and IDD (21%). Majority of RTT diagnoses were delivered by Geneticists (43%) or Neurologists (43%). QI results show quality of life for male RTT (Total score M=56.2±8.5 out of 100) is significantly lower than in female RTT (65.6±14.1, p<.01) and similar to CDKL5 deficiency disorder (58.9±16.1, p=0.36). Preliminary qualitative themes include an often difficult ‘Diagnostic Odyssey’ characterized by miscommunications and delayed care, ‘Provider Misconceptions’ including total unawareness of male RTT, and a ‘Significant Burden on Parents’ to act as advocates and assume the role of expert while providing constant monitoring and care for their sons. Illustrative quotes supporting these themes will be provided.
Conclusions: We demonstrate that a significant component of mis- and delayed diagnosis of male RTT is mediated by health-care systems biases, though influenced by low incidence, which negatively impacts patients and families. Medical providers and researchers require education about key issues and parent perspectives of male RTT in order to promote provision of specific medical care and therapies, accurate assessments of natural history and prognosis, participation and delivery of clinical trials, and to improve family quality of life.
# 523
NEW TECHNOLOGIES THAT INFORM PATHOGENIC MECHANISMS FOR BALANCED X;AUTOSOME TRANSLOCATIONS: WHAT’S OLD IS NEW AGAIN
Fernandez BA1, 2, Lee G1, Paredes Gonzalez K1, Schmidt R3, 5, Deardorff MA3, 5, Raca G3, 5, Gibson S4, Miller D4. 1Children’s Hospital Los Angeles, Los Angeles, CA; 2Keck School of Medicine of USC, Los Angeles, CA; 3Children’s Hospital Los Angeles, Los Angeles, CA; 4University of Washington, Seattle, WA and 5Keck School of Medicine of USC, Los Angeles, CA
Purpose of Study: Hypomelanosis of Ito (HMI) is a type of skin pigmentary dysplasia that is a sign of mosaicism. It appears as macular, hypopigmented whorls or streaks. Some HMI patients are females with balanced X;autosome translocations [t(X;A)] and skewed X-inactivation. The structurally normal X is preferentially inactivated in 75% of female t(X;A) carriers, so that no dosage imbalance exists for X or the translocated autosome. In 25% of cases, inactivation is skewed towards the translocated X that contains XIST (Xq13). This creates partial disomy for X on the other derivative (der) chromosome. Also on the der chromosome containing XIST, attenuated spreading of XIST non-coding RNA may occur into the attached autosomal region.
We used optical genome mapping (OGM) and long read DNA sequencing (LRS) to investigate the molecular mechanism leading to intellectual disability (ID) in a 7-year-old girl with HMI and her mother. They both carried a balanced t(X;A), 46,X,t(X;16)(q13;p11.2). Hypothesis: Their ID is due to inactivation of the translocated X on the der chromosome containing XIST, with more unfavorable skewing in the daughter who has HMI and more severe ID. This would result in partial disomy of chrX and potentially monosomy of part of chr16.
Methods Used: (1) Because one cytogenetic breakpoint was Xq13, it was unclear which der chromosome contained XIST. This was resolved by OGM. (2) To determine patterns of X-inactivation in the proband and mother, Nanopore LRS was performed which allows assessment of methylation.
Summary of Results: The proband had microcephaly and linear areas of skin hypopigmentation (HMI). She had had a normal microarray and exome sequencing. Her mother had less severe ID and did not have HMI. OMG results: a) To a resolution of 500 bp, the proband and mother’s translocation breakpoints were the same. b) XIST was on the der(16) chr. Its 3’ end was 2 Mb from the Xq13 breakpoint. XIST was not separated from its 5’ regulatory region. Hence der(16) would be capable of X-inactivation. LRS results: By analyzing differentially methylated CpG islands along chrX, we determined that X-inactivation in both individuals was 100% skewed and that the structurally normal chrX was inactivated. This favorable pattern of skewing is not predicted to lead to an abnormal phenotype.
Conclusions: (1) The proband’s HMI is due to skewed X-inactivation towards the structurally normal chrX. (2) ID in the mother and daughter does not seem to be due to preferential inactivation of the der(16) chr containing XIST. Their ID may be due to mutation in an X-linked recessive gene on one derivative chromosome not detected by exome or LRS. Short-read whole genome sequencing is underway to try to identify a mutation. Their phenotypes could also be due to differences in skewing in brain and other tissues, compared to blood. (3) This family highlights the importance of examining the skin for evidence of skewed X-inactivation and of then obtaining a karyotype. In the future, OGM or LRS may be used to identify similar events.
Healthcare Delivery Research IV - Medical Education
Concurrent Sessions
8:00 AM
Saturday, January 20, 2024
# 524
Outcomes of small group process work on medical student grit, resilience, and stress: A non-randomized pilot study
Sperling E. Western University of Health Sciences, Lebanon, OR
Purpose of Study: The incidence of high stress and mental ill-health begins very early in medical school. Chronic stress can lead to both physical and psychological issues as a student, resident, and physician. Chronic stress in medical students is not a new phenomenon, but recent research has highlighted the worsening mental health of medical students, with as high as three-quarters of students reporting mental ill-health. It is vital that we find ways to reduce stress and assist in improving the mental health of medical students.
Methods Used: This quasi-experimental study assessed the effects of a year-long small process group intervention, led by a psychiatrist, which aimed to improve self-awareness, mindfulness, and resilience in first and second-year medical students. Students self-selected into the process group, and eight agreed to participate in the research study. Eight students in the same cohorts who did not self-select into the group were randomly recruited as controls. The psychiatrist who led the groups was blinded to student participation in the study. Students in the process and control groups were surveyed with the Perceived Stress Scale, the Connor-Davidson Resilience Scale, and the Grit Scale prior to starting the sessions, and at the end of the year. Statistical analysis was done with R.
Summary of Results: The mean age of students in the process group was 28.63, with six females, six second-year students, six students identifying as white and two as Asian, and all identifying as heterosexual. In the control group the mean age was 25.38; three were females; three were second-year students; five identified as white, one as Hispanic, and two as multiracial; and one student identified as bisexual while the rest were heterosexual. The two groups did not differ at baseline on any of the outcome measures. At the end of the year, the process group has increased resilience, decreased stress, and maintained grit levels, while the control group had decreased resilience and grit and increased stress. The decrease in stress within the intervention group was significant (t(15) = -2.324, p = 0.053), as was the decreased resilience within the control group (t(13) = -2.912, p = 0.027). The intervention group also approached significantly better resilience than the control group (t(13) = -2.250, p = 0.065).
Conclusions: Alhough this was a pilot study with a small sample size, this study indicates that a small process group focused on self-awareness and resilience may result in better resilience, less stress, and maintained grit in preclinical medical students over the course of one academic year compared to controls.
# 525
THE EFFICACY OF FLIPPED CLASSROOMS OVER TRADITIONAL DIDACTIC LECTURES IN MEDICAL EDUCATION
Chang E, Zemeida S, Chou E, Gerriets V, Cusick J. California Northstate University, Elk Grove, CA
Purpose of Study: Flipped classroom instruction has been gaining popularity in higher education. Emerging evidence suggests this pedagogy may benefit students compared to traditional didactic lectures. In this study we aim to assess the efficacy and viability of implementing a flipped classroom modality in a medical school setting.
Methods Used: Medical students participated in a review game covering academic policies and took quizzes before and after to assess their understanding. In another study, students were randomly placed into groups that took quizzes on class material after exposure to either 1) a traditional didactic lecture or 2) a pre-recorded voiceover lecture followed by a review game. A third group served as a blind control and took the quiz prior to exposure to either pedagogy. Faculty and student feedback were also collected regarding flipped classroom instruction. A students’ t-test was used to determine statistical significance in quiz performance. Survey data was collected using a Likert scale.
Summary of Results: Academic policy quiz performance significantly improved (p = 0.048) from 51% (n = 14) to 67% (n = 19) after participating in a review game. In a cohort of second-year students, quiz performance after delivery of either pedagogy did not differ significantly (p = 0.20), as the voiceover and review game group averaged 65% (n = 10), lecture group averaged 71% (n = 14), and control group averaged 31% (n = 9). Faculty surveys indicated most agree that incorporation of active learning pedagogies would lead to better educational outcomes compared to traditional didactic lectures, and they would be more willing to create voiceovers if they had training, resources, and IT support (average Likert scores of 6.2 and 6.2 out of 7, respectively, n = 9). 89% of faculty also indicated they would be most incentivised to use voiceover lectures if it resulted in more positive student feedback (n = 9).
Conclusions: Students that participated in a review game covering academic policies on the first day of medical school scored significantly better in comparison to students that learned the information solely through orientation. Although neither flipped classroom nor traditional lecture resulted in significantly improved quiz performance on class material over the other, the combined use of voiceovers plus review games was positively received by both faculty and students. Furthermore, valuable insight from students regarding improvement of the delivery of this pedagogy was received.
Student and Faculty Survey Responses.
Student Questionnaire on Academic Progression Policy Review Game
Average Likert Score (out of 7)
The review game on the first day of medical school enhanced my understanding of academic progression policies.
6.2 (n=33)
I was overloaded with information during orientation, and I forgot a lot of the information that was presented to me during orientation regarding academic progression policies.
6.0 (n=33)
The review game on the first day of medical school was a fun ice breaker that helped me become acquainted with my classmates in a friendly competitive atmosphere.
6.1 (n=33)
Student Questionnaire on the combined use of Voiceover Lectures plus Review Games
I would like to see voice-overs used for more lectures.
5.4 (n=31)
I prefer short voice-over lectures that only focus on a single high-yield topic:
5.8 (n=10)
I like formative quizzes within the voiceover lectures.
6.1 (n=32)
I would come to more review games if there was a brief Q&A review before the game
5.5 (n=29)
Faculty Questionnaire on the combined use of Voiceover Lectures plus Review Games
Incorporation of active learning pedagogies would lead to better educational outcomes compared to traditional didactic lectures
6.2 (n=9)
Voiceovers coupled with review games were more beneficial than traditional didactic lectures.
5.6 (n=9)
I would be willing to try using voice-over lectures combined review games instead of traditional lectures
6.0 (n=9)
I would be more willing to try making voiceover lectures if I had access to training, resources, and additional IT support
6.2 (n=9)
I believe students that do not come to class are missing out on critical information that will help them be good physicians
6.0 (n=9)
The current generation of medical students (millennials and GenZ’s) are much more comfortable with technology than my generation
6.6 (n=9)
# 526
RESIDENT PERSPECTIVES ON INPATIENT ROUNDS LED BY SENIOR RESIDENT PHYSICIANS IN PEDIATRICS
Bauer K1, Borden L1, 2, Wang T1, 2, Payne C1, Afghani B1, 2. 1UC Irvine School of Medicine, Irvine, CA and 2CHOC Hospital of Orange County, Orange, CA
Purpose of Study: Balancing autonomy and supervision while maintaining optimal patient care is a crucial step in professional development of residents. Inpatient rounds led by senior residents have been shown to improve perceived autonomy, critical thinking, and comfort with independent decision making. However, evidence is lacking on how resident-led rounds in an inpatient pediatric setting impacts multiple components of resident education and development. The objective of this study was to assess residents’ perspectives on teaching, autonomy, supervision, and patient care when inpatient rounds were led by a senior resident, while the attending hospitalist took a more observational role.
Methods Used: Pediatric residents in their first (PL-1), second (PL-2) and third (PL-3) year of training at a high-volume children’s hospital were administered a survey using REDCap, to assess their perspectives on the quality of teaching, growth, autonomy, and supervision when a senior resident (PL-2 or PL-3) led inpatient rounds. The team performing rounds typically consisted of one senior resident (PL-2 or PL-3), two interns (PL-1s), two medical students and an attending hospitalist. Residents were asked to rate each parameter as poor, acceptable, good, excellent, or N/A.
Summary of Results: Of 81 residents, 74 (91%) completed the survey. Respondents consisted of 36% Interns and 64% senior residents. When senior residents led inpatient rounds, 51% of senior residents rated their attendings’ interest in teaching as “excellent” compared with 27% of interns (Figure1). Compared to the interns, senior residents were more likely to report increasing levels of independence, excellent self-confidence, and clearly defined roles. Senior residents had higher percentages of ‘excellent’ evaluations relative to interns after senior-led rounds with regards to quality of teaching, level of autonomy, level of supervision, quality of care and professional growth, however these differences were not statistically significant.
Conclusions: Our preliminary findings suggest that compared to the interns, senior residents were more likely to report excellent independence, self-confidence, clarity in their roles, and attendings’ interest in teaching when the rounds were led by them. There is room for improvement in clarity of roles and self-confidence of interns during senior resident-led rounds as very few interns rated these in the excellent category. To become competent practitioners, senior resident-led inpatient rounds are important in promoting resident development and eventual clinical autonomy and should be adapted in academic children’s hospitals.
# 527
Multi-Institutional and Multi-Disciplinary Collaboration for an Exceptional Neonatal Intensive Care Education (NICE) Quality Improvement Initiative
Arichai P1, 2, Sierra-Strum IE1, 2, Yeh A1, 2, Sardesai SR1, 2, Dixon M3, Ramanathan R1, 2. 1Los Angeles General Medical Center, Los Angeles, CA; 2Keck’s School of Medicine, University of Southern California, Los Angeles, CA and 3Children’s Hospital Los Angeles, Los Angeles, CA
Purpose of Study: The evolving landscape of graduate medical education and neonatology presents challenges to fellows’ clinical training including reduced procedural opportunities, more complex patient population, and concentrated specialized care. These issues jeopardize the readiness of future neonatologists. Our aims are to identify shortcomings in our Neonatal-Perinatal Medicine (NPM) fellowship program, restructure the core curriculum, and enhance fellowship education through quality improvement methods.
Methods Used: We conducted a needs assessment survey of NPM fellows in May 2023 via REDCap. We formed a Neonatal Intensive Care Education (NICE) quality improvement committee, involving multi-institutional and multi-disciplinary content experts and medical education mentors. In July 2023, we implemented the new core curriculum informed by the survey findings. We assessed education quality monthly via fellow survey for changes in attitude using 9-question 5-point Likert scale questionnaire, pre-/post- organ system block knowledge assessment, and quarterly Copenhagen Burnout Inventory (CBI). All surveys were anonymous, and gift cards were provided for survey completion. Data analysis used Microsoft Excel. This project is supported by the Committee of Interns and Residents quality improvement grant and approved by our IRB.
Summary of Results: 89% (16/18) fellows completed the needs assessment survey. 71% (10/16) felt that the mission of core curriculum should prioritize cultivating well rounded neonatologists over Board examination preparation. Curriculum goals, in order of importance, were: 1) Clinical application, 2) Neonatal Board preparation, 3) Research, 4) Wellness, 5) Career development, and 6) Equity and anti-racism. Fellows’ ratings of education quality improved from a baseline of 3.15 to 4.28 on 5-point Likert scale (figure 1). Clinical application received the highest rating and curriculum organization improved the most from baseline (Table 1). 83% (15/18) fellows completed the CBI survey. 60% (9/15) reported low or no symptoms of burnout, 33% (5/15) reported moderate burnout, and 7% (1/15) reported high level of burnout.
Conclusions: The new NPM fellowship curriculum structure improved fellows’ educational experience and demonstrated the feasibility of quantitative attitude change assessment for quality improvement. It is important to track symptoms of burnout throughout the academic year. Ultimately, our educational impact should be assessed for knowledge attainment and retention.
Mean average of education quality rating at various time points using quantitative questionnaire with 5-point level of agreement Likert scale.
Mean Quality Score
Survey Question
May 2023
July 2023
August 2023
Q1. The learning objectives of each CORE session are clear and the time is well utilized
3
4
4.5
Q2. The CORE educational activities are effective and engaging
3.5
4
4
Q3. Attending CORE helps me prepare for the NPM
3.5
4
4.5
Q4. Attending CORE helps me prepare for clinical situations that I may encounter
4
5
5
Q5. Attending CORE helps me reflect on my professional growth and future career goals
3
4
4
Q6. The CORE education promotes resilience, wellness, and a sense of community
3
4
4
Q7. The CORE education acknowledges and demonstrates the importance of diversity, equity and inclusion in patient care and health outcome
3
4
4
Q8. Overall, how satisfied are you with the CORE education?
3
4
4
Q9. Overall, how satisfied are you with the quality of education of the fellowship program in general?
3.5
4
4
# 528
Strengthening Personal and Team Resilience Through Emotional Intelligence on the Wards
Banner J1, Ivey A1, Tausinga T1, Brownson K1, 2. 1University of Utah School of Medicine, Salt Lake City, UT and 2Huntsman Cancer Institute, Salt Lake City, UT
Purpose of Study: For medical students, the transition from classroom learning to third year clinicals introduces a variety of new stressors. Some students have never held full-time, professional jobs and must learn to balance work expectations with educational endeavors. This may be the first time students have navigated ethical conflicts, witnessed a death, or are exposed to patient suffering and student mistreatment. Acknowledging these stressors, which can lead to depression, burnout, and decreased educational focus, and combating them is rarely discussed during clerkship education nor integrated into a formal curriculum. Our goal is to address the paucity of support and discussion regarding transitioning from the classroom to clerkships, collaborate with our Wellness Program to provide tools to manage emotional dysregulation, and strengthen students’ wellness self-awareness so they maintain an educational focus despite the stressors of the healthcare environment.
Methods Used: Data from a survey assessing the emotional intelligence, outward thinking, and mindfulness of preclinical students will be presented to advisors from the School of Medicine Wellness Center. Through collaboration with the Wellness Center on a student-driven initiative, online resources aimed at decreasing and managing emotional dysregulation will be disbursed to students via a canvas page; continuous data collection will help refine resources according to the student’s needs and perceived personal development as they progress through clinicals.
Summary of Results:
Preclinical students were given a survey before and after a 50-minute informational session about emotional intelligence and mindfulness. 100% of participants felt that clerkships would be stressful for them; 57% of respondents reported that it is difficult for them to learn when they feel stressed. Only 7% and 28% of respondents felt that UUSOM provides students adequate training on the subjects of emotional intelligence and stress management, respectively. After the informational session, there was a 20% increase in perceived ability to navigate stressful situations during clerkships. 100% of respondents felt that the informational session was helpful and wanted to learn more strategies for mitigating stressors on the wards.
Conclusions:
Emphasizing emotional intelligence, outward thinking, and mindfulness skills in medical students transitioning to the wards may not only facilitate emotional regulation and ability to maintain an educational focus during clinicals, but also provides tools which can be developed during their career as physicians to combat burnout.
# 529
PREDATORY AND OPEN ACCESS JOURNAL PUBLICATIONS AMONG CANADIAN PLASTIC SURGERY RESIDENCY APPLICANTS
Paiero Keeler A1, ElHawary H3, Tuen Y2, Courtemanche R2, Gilardino M3, Arneja JS2. 1University of British Columbia, Vancouver, BC, Canada; 2University of British Columbia, Vancouver, BC, Canada and 3McGill University, Montreal, QC, Canada
Purpose of Study: This study aimed to quantify the prevalence of publishing in predatory journals and open access journals among plastic surgery residency applicants. Characteristics of predatory publications and predictive factors associated with applicants publishing in predatory journals were also explored.
Methods Used: Study information was extracted from the curriculum vitae of applicants to the McGill University plastic surgery residency program from 2015 to 2018. Publications were reviewed in duplicate to confirm the existence of the article, publisher, year of publication, and impact factor. The journal or publisher of each article was cross-referenced to Beall’s list of potentially predatory publications which identifies predatory journals in different scientific domains as well as the Directory of Open Access Journals (DOAJ). Predatory publications underwent independent review to identify if they were open access, the length of time from submission to acceptance, alignment of article content with the journal topic, and if the article was on the subject of plastic surgery. A logistic regression model was used to examine applicant characteristics (gender, region of medical education, highest post-baccalaureate degree, and publication count) associated with publication in a predatory journal.
Summary of Results: 186 applicants published 388 journal articles. Overall, 63 articles published by 57 applicants were in open access journals. Simultaneously, 14 (3.6%) articles published by 14 (7.5%) applicants were published in predatory journals. The median impact factor for all applicants’ publications was 2.1 (25 - 75%ile = 0.7 - 3.5). Applicants publishing in a predatory journal differed from other applicants with at least one publication, reporting a higher average number of publications (6.57 vs. 2.87, p-value = 0.005) and a greater average number of publications in open access journals (3.29 vs.1.08, p-value = <0.001). A higher number of publications was the only applicant characteristic associated with publication in a predatory journal (OR 1.39, 95% CI 1.11 - 1.73). A review of predatory publications identified 14 publishers that advertised a continuous publishing model on their websites. Predatory publications time from acceptance to publication ranged from 0-214 days and research topics varied widely, with 3 (21.4%) publications on the subject of plastic surgery.
Conclusions: Canadian plastic surgery residency applicants had a higher rate of publication in predatory journals compared to their counterparts in other surgical residencies and academia. These findings highlight the need for further awareness amongst the plastic surgery community including medical students on the deceptive nature of predatory journals, the importance of integrity and professionalism in scientific publishing, and the fact that publication quality is more important than quantity.
# 530
"LET’S UNPACK MY FEEDBACK!" - AN APPROACH TO ENHANCE MEDICAL STUDENTS’ PEER FEEDBACK
Monasch EM1, Bhe A2. 1Stanford Health Care, Palo Alto, CA and 2UC Davis Health, Sacramento, CA
Purpose of Study: Peer feedback in medical education is a well-studied means of helping students promote self-reflection, identify knowledge gaps, and foster professionalism and communication skills. While multiple medical schools have documented positive outcomes from peer feedback instruction, it is not clear that the quality of peer feedback was specifically assessed during these interventions. Our study evaluates the impact of a “feedback on feedback” exercise on students’ confidence in delivering and receiving peer feedback. We also evaluate student perceptions of instruction on peer feedback and the “feedback on feedback” exercise.
Methods Used: We created a peer feedback session for first-year medical students at UC Davis for AY2022-23. To prepare for the session, students watched a pre-recorded video on delivering effective feedback that included two demonstration peer feedback scenarios. In class, students provided their peers with feedback following standardized patient encounters. Feedback providers subsequently received feedback on the quality of their feedback from a faculty or fourth-year medical student facilitator. We assessed students’ perceptions of this session and confidence surrounding peer feedback with pre- and post-session surveys and analyzed the data using a two-tailed t-test.
Summary of Results: Ninety-three percent (104/112) and 92% (98/107) of participating medical students responded to the pre- and post-session surveys, respectively. There was a significant difference in students’ self-reported confidence in their ability to provide their peers with effective feedback in a clinical setting before (M = 3.91, SD = 0.68) and after (M = 4.13, 0.60) the session; t(199) = -2.42, p = 0.02. There was also a significant difference in students’ self-reported confidence in their peers’ ability to provide them with effective feedback in a clinical setting before (M = 3.97, SD = 0.66) and after (M = 4.16, 0.58) the session; t(200) = -2.19, p = 0.03. Additionally, most students (33/41, 80%) agreed or strongly agreed that the “feedback on feedback” they received improved their ability to give effective feedback in the future (Table). Students frequently cited learning about different feedback frameworks as the most useful part of the module (19/64, 30%), followed by positive effects on their professional development (15/64, 23%).
Conclusions: Providing medical students with formal training in delivering effective peer feedback, including providing them with feedback on the quality of their feedback, can increase their confidence in their ability to deliver and receive feedback – a skill that is critical for their role as future physicians and educators.
Student Perceptions of Peer Feedback Session (N).
Strongly Disagree
Disagree
Neither Agreenor Disagree
Agree
Strongly Agree
Average
Giving peer feedback in class helped me apply the framework I learned in the pre-class video.
0%(0/41)
0%(0/41)
12%(5/41)
51%(21/41)
37%(15/41)
4.24
The "feedback on feedback" I received improved my ability to give effective feedback in the future.
0%(0/41)
0%(0/41)
17%(7/41)
39%(16/41)
41%(17/41)
4.20
Receiving peer feedback helped me understand the value of structured feedback in the clinical setting.
0%(0/52)
2%(1/52)
6%(3/52)
37%(19/52)
56%(29/52)
4.46
The "feedback on feedback" I observed improved my ability to give effective feedback in the future.
0%(0/50)
0%(0/50)
6%(3/50)
46%(23/50)
48%(24/50)
4.42
I will use feedback I have provided my peers to reflect on my own clinical skills and knowledge.
0%(0/98)
0%(0/98)
4%(4/98)
43%(42/98)
53%(52/98)
4.49
I will use peer feedback to implement self-improvement plans for my clinical skills.
0%(0/97)
0%(0/97)
3%(3/97)
44%(43/97)
53%(51/97)
4.49
# 531
Assessment of Adverse Mental Health Outcomes Among Traditional and Nontraditional Medical Students
Arief N, Jang E, Li A, Dang A, Gerriets V. California Northstate University College of Medicine, Elk Grove, CA
Purpose of Study: Despite institutional efforts to promote wellness amongst the student body, more than 80% of medical students continue to report some form of psychological distress. This study intends to examine whether being a non-traditional medical student (NTMS) entails higher levels of burnout, stress, depression, and anxiety than those of traditional medical students (TMS). In the context of U.S. medical students, “traditional” refers to students who went through an undergraduate pre-medical track and entered medical school immediately after getting their degree with two or fewer gap years in between. “Non-traditional” students are those who delay their application cycle or admission date for various reasons, such as starting a family or prior career. NTMS are predicted to express higher levels of the aforementioned adverse mental health outcomes than traditional students.
Methods Used: Participants were recruited from California Northstate University College of Medicine and asked to complete a survey with both basic demographic questions as well as questions from the Oldenburg Burnout Inventory (OLBI), Perceived Stress Scale (PSS), Patient Health Questionnaire-9 (PHQ-9), and Generalized Anxiety Disorder-7 (GAD-7) to measure burnout, stress, depression, and anxiety, respectively. Participants were categorized as a NTMS if they indicated at least one of the following: a) 26-33 years old as an MS1, b) 26-29 years old as an MS2, c) married, d) living with a spouse, or e) living with a minor. Participants that met none of the above criteria were categorized as a TMS. Responses were analyzed using Pearson’s chi-squared test. This study received approval by the California Northstate University IRB committee.
Summary of Results: With 95 unique responses from TMS and 52 unique responses from NTMS, there was no statistically significant difference between TMS and NTMS for scores in the OLBI, PSS, PHQ-9, and GAD-7. We observed a chi-squared value of 1.146 for burnout, 0.610 for stress, 0.749 for depression, and 0.621 for anxiety. 37% of TMS and 42% of NTMS scored at least 21/32 on the exhaustion dimension of OLBI. 66% of TMS and 71% of NTMS scored at least 14/40 on the PSS. 16% of TMS and 13% of NTMS scored at least 10/27 on the PHQ-9. 9% of TMS and 17% of NTMS scored at least 10/21 on the GAD-7.
Conclusions: Overall, 39% of survey participants indicated moderate exhaustion. 68% of survey participants experienced at least moderate stress, with 8% experiencing high perceived stress within this group. Lastly, 15% and 12% of survey participants may require further evaluation for clinically significant depression and anxiety, respectively. Although we did not observe a statistically significant difference in the levels of adverse mental health outcomes between TMS and NTMS, the overall percentages of each population are strikingly high and have important implications for addressing the culture of mental health amongst medical students.
Neonatology General V
Concurrent Sessions
8:00 AM
Saturday, January 20, 2024
# 532
EVALUATION OF SWALLING DYSFUNCTION IN PRETERM INFANTS WITH FIBEROPTIC ENDOSCOPIC EVALUATION OF SWALLOWING (FEES) IN THE NEONATAL UNIT
Ahn K1, Heston A2, Patel A1, Shipman B2, Graf K2, Muniraman H2. 1Creighton University, Phoenix, AZ and 2Phoenix Children’s Hospital, Phoenix, AZ
Purpose of Study: To describe the clinical findings of FEES evaluation and the changes in feeding and apnea/bradycardia/desaturation (ABD) episodes after implementing SLP recommendations.
Methods Used: Retrospective chart review of 90 infants born in 2018-2023 and who underwent FEES evaluation. Findings reported on FEES are described. The percentage of oral (PO) and number of ABD associated with PO feeds were calculated and compared for the seven days before and after FEES evaluation and SLP recommendation by Wilcoxon signed rank test.
Summary of Results: A total of 90 infants with a mean birth gestational age of 32.1 (+5.1) weeks were included in the study. FEES was performed at a mean age of 39.2(+2.5) weeks with a mean weight of 3045(+ 691) grams. Overall, 77 (85.5%) infants had an abnormal FEES exam, with 34 (37%) demonstrating aspiration below the vocal cords and 42 (46.6%) infants reported to have pharyngeal pooling (Table 1). Infants with aspiration noted on FEES showed improvement in PO feeding (82 vs. 54%, p=<0.01) and median ABD counts (p=0.01) following FEES evaluation and implementation of SLP recommendations. Similarly, specific SLP recommendations, including change of positioning, nipple, bottle, and thickening of feeds showed improvement in PO feeding and lower ABD events (p< 0.03) (Table 2&3). Infants with normal FEES and without SLP recommendations for feeding showed an improvement in PO feeding but were not associated with changes in ABD events.
Conclusions: Aspiration was noted in over a third of preterm infants evaluated by FEES. SLP recommendations based upon FEES evaluation resulted in clinically significant improvement in PO intake and the number of ABD episodes associated with feeding. Further large studies evaluating FEES on feeding, nutrition, and growth outcomes are required to demonstrate clinical effectiveness of FEES.
Patient characteristics, FEES findings, and recommendations.
Patient characteristics (n=90)
Birth gestational age (weeks, mean, SD)
32.3 (+/-5.1)
Birth weight (grams, mean, SD)
1998 (+/-1123)
Gender, Female n(%)
46 (52%)
Race/ethnicity n(%)
White
33(36.6)
Hispanic
37 (41)
Black
14 (15.5)
American Indian
3(3.3)
Asian
3(3.3)
Corrected gestational age at time of FEES (mean weeks, SD)
39.2 (+/-2.5)
Weight at FEES (grams, mean, SD)
3063 (+/-671)
Clinical findings on FEES Exam (n= 90)
Any abnormality on exam n(%)
77 (85.5%)
Aspiration below the vocal cords n(%)
34 (37.7%)
Pharyngeal pooling n(%)
42 (46.6%)
Penetration of the bolus into the laryngeal vestibule n(%)
31 (34.5%)
Residue in the hypopharynx n(%)
15 (16.6%)
Laryngomalacia n(%)
25 (27.7%)
Signs of gastroesophageal reflux (GER) n(%)
20 (22.2%)
Unexpected anatomic abnormalities n(%)
10 (11.1%)
SLP Recommendations after FEES (n=90)
No change n(%)
7 (7.7%)
Thickened feeds n(%)
34 (37. 7%)
Change feeding position n(%)
47 (52.2%)
Change to nipple or bottle n(%)
63 (70%)
Start antireflux medications n(%)
1 (1.1%)
Video fluoroscopic study n(%)
6 (6.6%)
# 533
Calcium and Phosphorus Losses After Infusion of Human Milk Based Feedings in a Plastic Feeding System
Hamilton V1, Fusezy M2, Elliott M2, 3, Ramanathan R1, Cayabyab R1. 1LA General Medical Center, Los Angeles, CA; 2Prolacta Bioscience, Duarte, CA and 3Pediatrix Medical Group, Balti, MD
Purpose of Study: Polyurethane plastic tubing is used in feeding premature infants which have lipophilic properties that bind fat-complexed nutrients such as Ca and Phos, decreasing the delivery of these nutrients in human milk (HM). The purpose of this study was to quantify Ca and Phos losses in different HM fortification strategies at different simulated feeding durations.
Methods Used: Fortified and unfortified HM were studied for Ca and Phos loss using an in vitro model of simulated feedings. Unfortified HM were Mom’s own milk (MOM), and donor human milk (DHM). Fortified HM were MOM fortified to 26 cal/oz (MOM H2MF26) and Ready to Feed 26 cal/oz (RTF26). Cream (Prolact CR) was mixed to final caloric content of 28kcal/oz (MOM H2MF28), 30 kcal/oz (MOM H2MF30) and (RTF26 CR, RTF 26 CR2). To examine methods of cream delivery, Prolact CR was administered first as bolus before infusion of fortified milk (CR MOM H2MF26) and (CR2 MOM H2MF26). The milks were infused in triplicate through a polyurethane plastic feeding tube and microbore extension tube to deliver 45 mL of milk feeding in a 60 mL syringe via an infusion pump for 30, 60, 120, and 180 minutes with new tubing for each run. After the infusion, the tubing was flushed with 5 ml of air. All milks were analyzed for Ca and Phos content by ICP Emission Spectrometry.
Summary of Results: There were 160 samples analyzed for Ca and Phos. There was a significant calcium loss in HM with high fat content at 30 minutes MOM H2MF28 (p=<0.01) and MOM H2MF26 (p=0.02). MOM H2MF30 had significant loss at 60 min (p=0.02). DHM and MOM with lower fat content did not have significant calcium loss. Fortified HM had higher calcium than unfortified HM. All RTF 26 products had minimal Ca and Phos losses over time regardless of fat loss. There was no consistent significant loss of phosphorus observed with the different types of milk at different durations. (figure 1)
Conclusions: Calcium loss was higher in HM with higher fat loss. Phosphorus loss was not associated with any type of HM feeding and duration. RTF 26 products combinations had minimal calcium loss over time.
Calcium and Phosphorus in Enteral Feedind Tube System overtime.
# 534
GABAPENTIN FOR SEDATION AND PAIN CONTROL FOR NEONATES AFTER MANDIBULAR DISTRACTION OSTEOGENESIS
Wahl MD1, Rdesinski R2, Nguyen T1, Go M1. 1Oregon Health & Science University, Portland, OR and 2Oregon Health & Science University, Portland, OR
Purpose of Study: Opioids are frequently the first-line choice for pain management in neonates, but are not without their side effects, most notably respiratory depression and decreased gastrointestinal motility. Gabapentin is emerging as a possible alternative medication, but there remains little data on its use or outcomes in neonates. We explored whether there was a difference in clinical outcomes among infants who received gabapentin instead of opioids as first-line pain management after undergoing a mandibular distraction osteogenesis (MDO). We hypothesize that patients on gabapentin will have less respiratory depression reflected by less ventilator days.
Methods Used: This was a single center retrospective cohort study of infants that underwent an MDO procedure between January 1, 2010 to December 31, 2021. Chart review was conducted, and infants were grouped according to use of gabapentin for pain management. Data was analyzed with SPSS statistical software. Primary outcome was post-operative time on a ventilator. Secondary outcomes included time on any respiratory support, cumulative opioid exposure, time to first enteral feed after surgery, time to full enteral feeds after surgery, and time on TPN.
Summary of Results: There were 30 infants who met inclusion criteria for our analysis. Demographic data and clinical outcomes are summarized in Table 1. Mean gestational age at birth was higher for the gabapentin group (39.34 + 1.01 weeks) versus those in the non-gabapentin group (37.70 + 2.24 weeks, p-value= 0.02). We found no difference for ventilator days between infants who received gabapentin versus those who did not (mean 9.29 + 3.9 days vs 6.98 + 4.5 days, p= 0.15), but those who were on gabapentin were fed sooner after surgery (0.4 + 0.35 days vs 0.8 + 0.48 days, p= 0.01). Also, the median time on a morphine infusion was 0 hours in the gabapentin group vs 33.5 hours in the no gabapentin group (p= 0.47).
Conclusions: Our primary outcome of time on a ventilator and most of our secondary outcomes did not reach statistical difference between the two groups. We think this is because our sample size was very small and likely not powered to detect such differences. However, some of our secondary outcomes show a trend that may favor the use of gabapentin as first-line pain control in post-operative neonatal patients. The significantly shorter time to first post-surgical feed suggests that using gabapentin as first-line pain management may avoid some of the adverse effects like delayed gastrointestinal motility or feeding intolerance associated with the use of opioids. A shortened time to feeding would be clinically relevant for promotion of infant growth and development. While cumulative opioid exposure may not have differed between the two groups, the shorter amount of time on infusions in the gabapentin group could be clinically relevant as an indicator of both neonatal comfort and cost reduction.
Demographics and clinical outcomes for infants who received gabapentin vs opioids for post-operative pain control
Purpose of Study: Lipids are critical for numerous biologic and physiologic processes in preterm neonates. Serum triglycerides are routinely measured in this vulnerable population as a proxy for lipid tolerance. It is often unclear how clinicians should interpret these values and whether they may have broad biological, translational, or clinical significance. We investigated serum triglyceride levels in age-specific cohorts of preterm infants and for repeated measured levels to describe potential variability in levels by age and time. To our knowledge, this is the largest longitudinal investigation of serum triglycerides in preterm infants.
Methods Used: This was a retrospective observational study of infants born at < 32 weeks’ gestational age admitted to the neonatal intensive care unit at Lucile Packard Children’s Hospital between April 2014 - December 2021. Clinical data were obtained utilizing the Stanford Research Repository (STARR). Descriptive analyses were conducted in R statistical computing framework, version 6.2. The study was approved by the Stanford University institutional review board.
Summary of Results: Included were 759 infants born < 32 weeks’ gestational age and admitted to the neonatal intensive care unit. 680 infants had available clinical data recorded and included in the descriptive analysis. All included infants received either Intralipid 20% or SMOFlipid 20% emulsions. Mean (SD) gestational age was 28.5 weeks (SD = 2.4). Triglycerides rose within the first postnatal week and subsequently plateaued by postnatal day 25. Infants born < 25 weeks’ gestational age had the highest triglyceride levels over the first 25 postnatal days compared to all other gestational age strata. By postnatal day 50 all gestational age strata demonstrated a similar triglyceride profile.
Conclusions: Longitudinal triglyceride profiling reveals age-dependent differences that are most pronounced in the first 3 postnatal weeks. These differences may reflect the spectrum of metabolic immaturity in circulating and tissue-specific lipases and associated transport proteins that govern lipid absorption and metabolism. This may have important translational and clinical implications for sequelae unique to preterm infants, such as glucose dysregulation, hyperbilirubinemia, bronchopulmonary dysplasia, and other acquired disorders of prematurity.
Maternal, Neonatal and Triglyceride Characteristics.
Neonatal Characteristics
No. (%, SD)
(n = 680)
Gestational Age (weeks), mean (SD)
28.5 (2.4)
Birthweight, (g), mean (SD)
1199 (468)
Sex
–-
Female
316 (46%)
Male
364 (54%)
Antenatal Characteristics
–-
PPROM
274 (40%)
Preterm Labor
303 (45%)
Pre-eclampsia
143 (21%)
Chorioamnionitis
118 (17%)
Exposure to Prenatal Steroids
661 (97%)
Fetal Growth Restriction
139 (20%)
Neonatal Outcomes
–-
Small for Gestational Age
60 (8.8%)
Necrotizing Enterocolitis
50 (7%)
Retinopathy of Prematurity (Stage ≥ 2)
91 (13%)
Intraventricular Hemorrhage (≥ Grade 3 or 4)
52 (8%)
Bronchopulmonary Dysplasia
276 (41%)
Suspected or Confirmed Genetic Malformation and/or Syndrome
32 (4%)
Triglyceride Data
–-
Mean (SD)
92.6 (69)
Median (IQR)
75.0 (64)
Mean No. Triglyceride Values per patient (SD)
9.3 (10)
Median No. of Triglyceride Values per Patient (IQR)
6 (4)
% of Total Triglycerides Obtained Between Postnatal Day 1-10
68.8%
% of Total Triglycerides Obtained Between Postnatal Day 11 – 49
24.8%
% of Total Triglycerides Obtained Between Postnatal Day 50 – 100
The antimicrobial peptide LL-37 improves experimental NEC survival and significantly improves intestinal epithelial wound healing
Leegwater AJ1, Boly T2, Bautista G1, Lueschow S2, McElroy S1. 1University of California, Davis, Sacramento, CA and 2University of Iowa, Iowa City, IA
Purpose of Study: Necrotizing enterocolitis (NEC) remains a leading cause of morbidity and mortality in premature infants. Antimicrobial peptides (AMP) are a vital component of intestinal defense through direct antimicrobial activity and regulation of epithelial homeostasis. The AMP LL-37 decreases experimental neonatal sepsis mortality; however, the mechanism is unclear, and studies in NEC are lacking. We hypothesize that LL-37 decreases NEC mortality and enhances epithelial wound closure.
Methods Used: NEC-like injury was induced using the well-described Paneth cell disruption model. 14-day-old mice were injected with 75 µg/kg dithizone followed by a gastric gavage of 10^8 CFU/g K. pneumoniae and compared to controls for mortality. Mice in the NEC-induction group were exposed to 100 µg/kg body weight LL-37 twice daily three days prior to NEC induction (pre-treatment) or once one hour after K. pneumoniae administration (post-treatment). Epithelial wounding was achieved by applying a rotating circular silicone disk to IEC-18 cell cultures. After wounding, cells were treated with LL-37 or epithelial growth factor (EGF) and compared to sham controls. Cell closure was quantified with Image J at 0h, 6h, 12h, and 24h and analyzed with GraphPad Prism.
Summary of Results: There were no significant differences in survival between LL-37-treated and non-treated groups. However, while NEC and pre-treatment group survival were similar (85% and 82%), there was a clinically relevant increase in survival in the post-treatment group (95%, n>19). LL-37 treatment (1ug/ml) significantly closed epithelial wounds faster than sham controls (79% vs. 51%, p<0.001) and was similar to EGF treatment (55.7 %). However, higher doses of LL-37 (12.5 and 25 ug/ml) significantly decreased rates of wound healing (43.1% and 10.9%, p<0.0001, n>18).
Conclusions: LL-37 treatment following but not before NEC induction improves survival in experimental NEC. While this improvement is not statistically significant, a three-fold decrease in mortality compared to non-treatment is clinically relevant. A possible mechanistic rationale for this is its impact on epithelial wound healing. Our cell culture data shows LL-37 significantly aids wound closure, similar to the impact of the growth hormone EGF. However, this is dose-dependent as administration of higher concentrations of LL-37 significantly worsened wound closure, likely secondary to LL-37 disruption of the cell wall of the epithelial cells. In conclusion, our data suggest that LL-37 may help reduce NEC mortality and improve gut healing, but dosing is critical to prevent further injury to the infant.
# 537
Cohort of Intestinal Perforations in Extremely Preterm Infants
Burgos M, Newman-Lindsay S. UC Davis School of Medicine, Sacramento, CA
Purpose of Study: There is increasing resuscitation and survival of infants less than 24-weeks gestational age (GA). In extremely premature infants (EPIs), the most common causes of intestinal perforation are spontaneous intestinal perforation (SIP) and necrotizing enterocolitis (NEC), with SIP overtaking NEC at lower GAs. This demographic of infants of <24w GA is poorly represented in literature regarding intestinal perforation (IP). The goal of our study is to describe the clinical presentation of EPIs with confirmed or suspected IPs and compare those born at <24 weeks GA to those born at 24-28 weeks.
Methods Used: This study is a retrospective cohort of inborn and transported infants admitted to our 49-bed level IV neonatal intensive care unit from 2020 through March 2023. We included all infants <28 weeks or <1000g at time of admission. Inclusion and exclusion criteria and categorization of patients are shown in figure 1. Infants were categorized as confirmed SIP by applying the Vermont Oxford Network (VON) definition (pneumoperitoneum and/or surgical confirmation) or suspected SIP if there was clinical concern without radiographic/surgical confirmation. Study is IRB exempt.
Summary of Results: Our cohort contains 145 infants. Characteristics of the cohort and prevalence of IPs are summarized in Table 1. Among the seven cases of suspected perforation, one patient recovered with supportive care and the remaining six died. In one case, an abdominal drain was placed with serosanguinous and meconium-colored fluid drained. In another, autopsy showed pigmentation consistent with meconium suggesting that a microscopic perforation occurred. Autopsy was declined or results are unavailable in the remaining four deaths.
Conclusions: This cohort is consistent with published trends on the increasing prevalence of SIP in the smallest infants. The heterogeneity of presentation in our cohort and high degree of co-morbidities, especially respiratory failure, shows the difficulty of categorizing some types of intestinal insult in EPIs. Many of the cases we present meet the 3/5 definition of SIP published by Gordon et al, but not the more commonly used definition by the VON and others, which requires surgical confirmation or pneumoperitoneum. We may be seeing abdominal discoloration and intestinal hypoperfusion as a final common step in systemic inflammatory response and metabolic acidosis interacting with immature fragile intestinal tissue. Our hope is that these cases will provide context to improving the management of these most immature infants.
Composition of Retrospective Cohort.
1a Prevalence of Surgical Abdominal Pathology
22-23w (n=17)
24w (n=28)
25-28w (n=100)
Total (N=145)
Inborn
10 (59%)
15 (54%)
65 (65%)
90 (62%)
Male
12 (70%)
17 (60%)
46 (46%)
75 (52%)
Early (
1
0
4
5
Survival to Discharge
10 (59%)
23 (82%)
80 (80%)
113 (78%)
Surgical NEC
0
2
8
10 (7%)
Other Perforation
1
incarcerated hernia
1
iatrogenic
3
incarcerated herniavolvulus (2)
5
Confirmed or Suspected SIP
8
8
14
30 (21%)
1b Clinical Characteristics of Confirmed and Suspected SIP
Pneumoperitoneum prior to surgery or drain placement
4 (50%)
5 (62.5%)
12 (86%)
21 (70%)
Clinical Suspicion: Treatment team concerned for intestinal perforation due to abdominal discoloration, abnormal bowel gas pattern, metabolic acidosis and/or hyperglycemia.
# 538
ASSESSING AND IMPROVING ACCESS TO LACTATION AND BEREAVEMENT SUPPORT FOR MOTHERS WHO EXPERIENCE PERINATAL LOSS AT A SINGLE REFERRAL HIGH-RISK ACADEMIC CENTER
Capossela E, Lehman S, Wolf A, Diaz A, Hammer R, Sanchez B, Stellwagen LM, Marc-Aurele K. University of California San Diego, San Diego, CA
Purpose of Study: The loss of a child is devastating, and those who experience miscarriage, termination, stillbirth, or death of an infant are no exception. In addition to the profound impact on their mental and emotional wellbeing, these mothers’ bodies will progress through lactogenesis, and they will have to navigate the extra challenge of having a milk supply but no longer having a baby to feed. It is important that health care providers support and educate mothers about this process.
The Cherry Blossom Family (CBF) program was created by the University of California Health Milk Bank with the goal of providing grieving mothers information about lactation and a free breast pump. After its launch in September 2022, we recognized we were missing many opportunities to help these mothers. The goal of our study is to determine what percentage of mothers with a perinatal loss at University of California San Diego (UCSD) Health are offered support from the CBF program and identify areas for improvement.
Methods Used: We created a multidisciplinary team in July 2022 and received IRB approval in February 2023. Our global aim is to improve lactation and bereavement support for mothers who experience a perinatal loss. Our SMART aim is to increase the percent of mothers who, after experiencing the loss of a fetus or infant, are offered support from the CBF program from 0% to 30% between July 1, 2023 and June 30, 2024. Our process measure is the percent of mothers with a documented lactation consult after a perinatal loss.
So far, we have collected baseline data of UCSD Health patients who have experienced a perinatal loss by reviewing their medical records, including if there was evidence of a lactation consult or mention of the CBF program.
Summary of Results: During our baseline period (January 1, 2023 to June 30, 2023), 34 patients had a perinatal loss. Of these, 82% had a fetal loss and 18% had an infant loss. The median percentage of women with documented CBF support offered was 0%. The median percentage of women with documented lactation consults was 8.5%. Our team has since used this data to start making key changes (see image).
Conclusions: We recognize the importance of providing mothers lactation and bereavement support after a perinatal loss. After initiation of the CBF program, unfortunately, the vast majority of the eligible mothers had no documentation of a lactation consult or offer of the CBF program. With a multidisciplinary team approach, we hope to improve the support of mothers during this sensitive time.
Key Driver Diagram.
# 539
IMPACT OF MATERNAL STRESS ON THEIR PARENT-INFANT INTERACTIONS: OBSERVATIONS WITH THE STILL FACE PARADIGM
Oyeku O1, Chao L1, Maxwell J2, 3, Lowe J2. 1University of New Mexico School of Medicine, Albuquerque, NM; 2Department of Pediatrics, University of New Mexico School of Medicine, Albuquerque, NM and 3Department of Neurosciences, University of New Mexico School of Medicine, Albuquerque, NM
Purpose of Study: During the early years of life, an infant’s brain undergoes significant changes, especially related to emotional regulation. Maternal interaction, specifically the use of contingent responding, is known to play a major part in the ability of an infant to positively regulate their emotions. Less is known about the impact of maternal stress on an infant’s ability to regulate emotions. Therefore, we investigated how maternal self-reported stress impacts the interaction with their infants. We hypothesized that higher maternal self-reported stress level would negatively impact an infant’s ability to regulate emotion.
Methods Used: 70 full term healthy infants at 3 to 4 months of age were included. Video tape analyses of the Still Face paradigm were used to create a maternal interaction and infant affect score. Contingent responding was defined by maternal response to their infant’s cues during their interaction. Infant’s recovery was measured by the increase in the infant’s positivity from the still face to the free-play episode. The short form Parent Stress Index (PSI) was completed at the visit. Two sets of Spearman’s correlation analyses examined the relationships between parental and infant stress (Episode 1 of the Still Face Paradigm), as well as between parental and infant response (Episode 3 of the Still Face Paradigm). Nested linear regression models investigated the relationship between infant stress (dependent variable) and a set of independent variables (sex, income, and parental stress).
Summary of Results: There was a weak positive correlation between parental and infant stress (PSI and Episode 1; p=0.79) and a weak negative correlation between parental and infant response (PSI and Episode 3; p=0.82). The results were similar after dichotomizing parental stress into high and low categories and conducting a point biserial correlation. We found a slightly stronger correlation between parental and infant stress (PSI and Episode 1; p=0.45), and a weak negative, non-significant correlation between parental and infant response (PSI and Episode 3; p=0.79). The independent variables did not contribute significantly to infant stress, and the overall model was not significant (p=0.81).
Conclusions: Reported stress of mothers as measured by the PSI was not significantly correlated with the amount of contingent responding in interactions with their infant. There was no significant association between infant recovery scores compared to reported maternal stress levels. Further studies can improve comparative power by increasing sample size as well as increasing child age range and deepening maternal stress indicators.
Neonatology - Perinatal Biology III
Concurrent Sessions
8:00 AM
Saturday, January 20, 2024
# 540
AVR-48 treatment improves respiratory system mechanics in former preterm lambs
Rebentisch A1, Borton M1, Major E1, Van Boerum J1, Dahl MJ1, Null D1, Riley D2, 3, Christensen D4, Bromley R2, Albertine K1, Acharya S2. 1University of Utah, Salt Lake City, UT; 2AyuVis Research Inc, Fort Worth, TX; 3Texas Christian University School of Medicine, Fort Worth, TX and 4Dale J. Christensen Consulting LLC, Cary, NC
Purpose of Study: AVR-48 is an immunomodulatory small molecule with TLR4 modulating activity in macrophages, shifting their phenotype from pro-inflammatory toward anti-inflammatory. AVR-48 has potential therapeutic benefits in preclinical models and is being developed to treat bronchopulmonary dysplasia (BPD) in at-risk preterm neonates. We showed improved indices of respiratory gas exchange and alveolar formation, with reduced TLR4 protein abundance in the lung, of preterm lambs (Hubbard, E-PAS2023:1120.1). Whether the benefits confer long-term improvements in respiratory system function is unknown.
Methods Used: Preterm lambs (~128d gestation; saccular stage of lung development; eq to ~28w gestation in humans) were mechanically ventilated for 7d. Either vehicle (saline; n=5) or AVR-48 (3.0 mg/Kg; n=5) was given iv 6h after delivery and every 12h for 7d. Lambs were weaned from respiratory support to become former preterm (FPT) lambs for 2-months corrected postnatal age (2moC PNA; weaning from milk; 90d of life). Unventilated term control (TC) lambs (n=5) were also studied. Respiratory system mechanics were dynamically assessed by oscillometry (Tremoflo N-100; Thorasys) at 2w, 1- and 2- moC PNA, using face mask, at baseline and during methacholine challenge (ATS 1999; Dahl 2021), followed by albuterol. During oscillometry, lambs breathed spontaneously while supported prone in a sling and lightly sedated (Lorazepam).
Summary of Results: Oscillometry results are presented as resistance/Kg (cmH2O/L*s-1/Kg) and reactance/Kg (cmH2O/L*s-1/Kg) because the AVR-48 FPT and TC lambs weighed more than the vehicle FPT lambs at 2w and 1-moc PNA (Fig 1). Results are pending for the vehicle group at 2-moc PNA. At 20Hz (Fig 2), the AVR-48 FPT lambs (4/5 survived, 92d) appeared to have lower resistance and less negative reactance at 1-moc PNA relative to the vehicle FPT lambs (2/5 survived >15d). Similar results were obtained for oscillometry at 7Hz and 41Hz (not shown).
Oscillometry at 20Hz (middle airways) revealed that the AVR-48 FPT lambs appeared to have lower respiratory system resistance (B) and less negative respiratory system reactance (E) to 2 mg of methacholine at 1-moc PNA relative to the vehicle treated FPT lambs.
Conclusions: AVR-48 appeared to improve overall body weight, survival, and indices of respiratory system mechanics in FPT lambs following methacholine challenge and equivalent to TC lambs. We suggest that AVR-48 is a promising molecule with potential therapeutic long-term benefit for preterm infants at risk of BPD.
Wt (Kg; mean±SD).
Age
TC
Vehicle FPT
AVR-48 FPT
2w
7.2±0.7
6.3±0.5
7.7±0.5
1 moC
13.0±1.0
8.8±0.3
12.7±0.5
2 moC
24.1±2.3
pending
25.7±1.8
# 541
FETAL BRAIN DHA CONTENT IN SHEEP IS PRESERVED IN FETAL GROWTH RESTRICTION, IN SPITE OF LOWER DHA CONCENTRATIONS IN MATERNAL AND FETAL PLASMA
Chassen SS1, Raymond-Whish S1, Zemski-Berry K2, Wesolowski S1, Brown LD1, Rozance P1, Powell T1. 1University of Colorado, Aurora, CO and 2University of Colorado, Aurora, CO
Purpose of Study: Docosahexaenoic acid (DHA), a long chain polyunsaturated fatty acid (LCPUFA), is critical for normal fetal brain development and must be transferred across the human placenta from mother to fetus. In human pregnancies complicated by fetal growth restriction (FGR), we demonstrated decreased cord blood DHA concentrations in lysophosphatidylcholine, the DHA form preferred for uptake by the brain. Whether this impacts fetal brain DHA content remains unknown. Using a sheep model of placental insufficiency and FGR, we tested the hypothesis that fetal plasma DHA concentrations are reduced, resulting in reduced DHA content of the fetal brain in FGR.
Methods Used: FGR was induced by exposing pregnant ewes to elevated ambient temperatures midgestation (term=147 days). Plasma samples (maternal uterine and fetal umbilical artery and vein) from catheterized control (CON;n=5) and FGR animals (n=6) were collected and necropsy performed for placenta and fetal brain (cortex, cerebellum) collection at 0.9 gestation. Fatty acids were extracted from plasma and placenta samples and targeted lipidomic analysis was performed to assess fatty acid content in total lipids, non-esterified fatty acids (NFEFA), triglycerides, and phospholipids using GC-MS. We also analyzed triglyceride and phospholipid species containing DHA in fetal brain using LC-MS/MS. Protein expression of fatty acid transporters and LCPUFA synthesis enzymes in placenta and brain were analyzed by Western blot. Statistical differences were assessed using student’s t test, correcting for multiple comparisons.
Summary of Results: FGR placental and fetal weights were 30% and 17% smaller than CON, respectively. Brain weights did not differ between groups. Maternal venous and arterial concentrations of DHA in NEFA and phospholipids were lower in FGR (p<0.05). Fetal arterial concentrations of total DHA and DHA in triglycerides were lower in FGR, as were fetal venous concentrations of DHA in phospholipid and triglyceride (p<0.05). Placental DHA content did not differ between groups. Placental protein expression of fatty acid binding and transport proteins, and of LCPUFA synthesis enzymes was reduced in FGR compared to CON (p<0.05). Fetal cortex and cerebellar DHA content in triglyceride and phospholipid subclasses was similar between groups. However, several phosphatidylcholine-DHA species were increased in FGR cortex (p<0.05). Protein expression of fatty acid transporter FATP4 was increased in the cortex of FGR brains compared to CON (p<0.01).
Conclusions: Placental insufficiency-induced FGR in sheep lowers DHA concentrations in both maternal and fetal plasma. Despite these reductions in DHA availability, placental DHA content was not different and fetal brain DHA levels in several phospholipid species were actually higher in FGR compared to CON fetuses. This suggests that compensatory mechanisms enhance DHA delivery to the fetal brain to support growth and development, possibly via upregulated fatty acid transport protein expression in the fetal brain cortex.
# 542
Continuous infusion of recombinant insulin-like growth factor 1 and binding protein 3 improves glomerular capillary growth in mechanically ventilated preterm lambs
Hansen C1, Carter L1, Rebentisch A1, Major E1, Vordos Z1, Van Boerum J1, Dawson E1, Yang H1, Dahl MJ1, Null D1, Barton N3, Carey G2, McHale M3, Niklas V3, Ward R1, Albertine K1. 1University of Utah, Salt Lake City, UT; 2Takeda, Lexington, MA and 3Oak Hii Bio Ltd, Altrincham, United Kingdom
Purpose of Study: Impaired vascular development underlies poor organ growth and development that contributes to diseases of prematurity, such as in the pathogenesis of bronchopulmonary dysplasia (BPD). Acute kidney dysfunction after preterm birth also occurs and results from poor glomerular capillary growth and development, with short and long-term impact on kidney function and disease. We showed that glomerular capillary growth is reduced in mechanically ventilated preterm lambs (Staub 2017), which may be related to the rapid decline of insulin-like growth factor-1 (IGF-1) that occurs after preterm birth and the persistent deficiency of IGF-1 that is characteristic of the early postnatal period of preterm neonates. We tested the hypothesis that the physiological replacement of IGF-1, using the complex of recombinant human (rh) IGF-1 bound to binding protein 3 (IGFBP3)) would increase glomerular capillary growth in mechanically ventilated preterm lambs.
Methods Used:
Ewes were given prenatal steroids and preterm lambs were delivered at ~128d; (term gestation ~150d; equivalent ~28w human gestation), resuscitated, intubated, and given surfactant, and continued on mechanical ventilation for 6-7d (Drager VN500, SIMV). Physiological targets were PaO2 60-90 mmHg, PaCO2 45-60 mmHg, O2 saturation 90-94%, pH 7.25-7.35. The control group received vehicle (diluent in saline; 10 mL iv; n=10; 5F/5M). The IGF-1 complex-treated group received an optimized physiological replacement dose of 1.5 mg/Kg/d (10 mL iv; n=10; 5F/5M). Treatment was started at 6h after preterm delivery and infused continuously iv. Lambs were euthanized and kidneys were prepared for stereology to quantify the glomerular capillary surface density, using immunohistochemically stained tissue sections (anti-CD34 antibody).
Summary of Results:
Glomerular capillary surface density was significantly greater in the IGF-1 complex-treated group (*p<0.05) compared to the control group (Fig 1A). Both groups had stable weight (Fig 1B) and urine output (Fig 1C). No differences were detected between females and males.
IGF-1 complex treatment led to significantly greater glomerular capillary surface density (A; *p.
Conclusions: Physiological replacement of IGF-1 increased glomerular capillary growth in mechanically ventilated preterm lambs. IGF-1 complex may be an effective therapy to promote capillary growth in the kidney, potentially reducing signs and symptoms of acute kidney injury along with BPD. Longer-term studies are likely necessary to differentiate the impact on kidney function and physiology.
# 543
A REDISTRIBUTION OF THE MICRONUTRIENT SELENIUM OCCURS AFTER CARDIOPULMONARY BYPASS WITH DEEP HYPOTHERMIC ARREST IN INFANT PIGLETS
Hernandez A, Khailova L, Suarez-Pierre A, Iguidbashian J, Lehmann T, Seedorf G, Mandell E, Nozik E, Davidson J, Sherlock L. University of Colorado Anschutz Medical Campus, Aurora, CO
Purpose of Study: Cardiopulmonary bypass with deep hypothermic cardiac arrest (CPB+DHCA) is frequently used babies with congenital heart disease, and post-operative complications contribute to high morbidity and hospital length of stay. Optimized levels of the micronutrient selenium (Se) improve outcomes in adult cardiac patients undergoing CPB. Adult animal data indicates Se is redistributed from the blood to the organs after CPB, where it can be incorporated into various Se-containing proteins that regulate oxidative stress, inflammation and metabolism. The role of Se in infants after CPB is poorly understood. We hypothesized that a redistribution of Se would occur in infant piglets after CPB.
Methods Used: Control (CON) infant piglets (5-10 kg; mixed sex) were anesthetized, mechanically ventilated, and received surgical lines for blood sampling. CPB piglets were placed on CPB, cooled to 18°C (DHCA) for 75 minutes, rewarmed, then separated from CPB and provided ICU care for 6 hours (h). Serum Se was measured at timepoint A (pre-CPB), timepoint B (2h post CPB) and timepoint C (6 h post CPB) for CPB piglets, and at corresponding timepoints from onset of anesthesia for CON piglets. After sacrifice (timepoint C), cardiac, hepatic, renal, and pulmonary Se levels were measured by ICP-MS. Cardiac, hepatic, renal, and pulmonary selenoproteins were assess by Western blot to measure protein content.
Summary of Results: Serum Se levels decreased after CPB from timepoint A (mean+/-SD 118.3ng/ul +/- 6.9) to timepoint B (107.1ng/ul+/-11.4) and C (98.11ng/ul+/- 8.8) and were unchanged in CON piglets across timepoints. Total Se levels were not significantly different between CON and CPB organs, but levels trended higher in the CPB group in the liver (CPB median[IQR] 5.2 pg Se/ug protein [4.75, 6.0] vs CON 4.55 pg Se/ug protein [3.95, 5.05]; p=0.12) and kidney CPB median[IQR] 13.2 pg Se/ug protein [10.19, 13.76] vs CON 9.9 pg Se/ug protein [3.95, 5.05]; p=0.14). Protein content for Se-containing antioxidant enzymes was unchanged between CON and CPB organs. Protein content for the endoplasmic reticulum selenoprotein O was increased in CPB livers (CPB mean 1.946 +/- SD 0.5166; CON mean 1+/-SD 0.1653, p<0.05) and kidneys (CPB mean 1.4+/- SD 0.5; CON mean 1.0+/-SD 0.23, p<0.05). Protein content for the endoplasmic reticulum selenoprotein S was higher in CPB livers compared to CON (CPB mean 1.8+/- SD 0.22, CON mean 1.0+/-SD 0.28, p<0.05).
Conclusions: Serum Se levels decrease after CPB in infant piglets. CPB livers and kidneys demonstrate an increase in the protein content of endoplasmic reticulum selenoproteins compared to CON livers and kidneys, indicating a redistribution of Se. As the organ-specific selenoprotein content is known to modulate inflammatory stress and metabolism after ischemia/reperfusion injury, this data provides mechanistic insight into the role and potential therapeutic benefit of Se in infants requiring CPB.
# 544
Mesenchymal stromal cell small extracellular vesicles improve capillary growth in the distal ileum of mechanically ventilated preterm lambs
Van Boerum J1, Salazar S1, Rebentisch A1, Major E1, Vordos Z1, Dawson E1, Yang H1, Dahl MJ1, Null D1, Delavogia E2, Mitsialis A2, Kourembanas S2, Albertine K1. 1University of Utah, Salt Lake City, UT and 2Boston Children’s Hospital, Harvard Medical School, Boston, MA
Purpose of Study: Necrotizing enterocolitis (NEC) occurs in 5-10% of preterm neonates with a birth weight of ≤1500 gm. NEC is associated with bronchopulmonary dysplasia (BPD). The pathogenesis of NEC is unknown, although ischemia, inflammation, apoptosis, and mucosal disruption are thought to be participants. Our preterm lamb model of BPD is associated with evidence of NEC when the preterm lambs are managed by invasive mechanical ventilation (IMV) but not noninvasive respiratory support. We showed that mesenchymal stromal cell small extracellular vesicles (MSC-sEVs) improve capillary growth and alveolar formation, and indices of respiratory gas exchange, in the lung of preterm lambs treated with MSC-sEVs versus vehicle control preterm lambs (Rebentisch J Invest Med 70 abstract 110, 2022). Most recently, we showed that MSC-sEV-treatment increased capillary growth in glomerular capillaries (Hansen J Invest Med 71 abstract 320, 2023). Increased capillary growth in both torgans raised the possibility that capillary growth in the distal ileum also may be increased, which was the tested hypothesis.
Methods Used: The distal ileum of preterm lambs (128d; term ~150d; ~28w human gestation) was analyzed. The preterm lambs were exposed to antenatal steroids, perinatal surfactant replacement, and resuscitated and supported by IMV for 6-7d (Drager VN500, SIMV). Physiological targets were PaO2 60-90 mmHg, PaCO2 45-60 mmHg, O2 saturation 88-92%, pH 7.25-7.35. The control group received vehicle (MSC-sEV diluent in saline; 10 mL; n=8; 4F 4M). The MSC-sEV-treated group received 2 x1011 NTA particles (10 mL; n=8; 4F 4M). Treatment was limited to hours of life 6 and 78 (iv). We used stereology to quantify surface density of capillaries in the lamina propria of the distal ileum, using immunohistochemically stained tissue sections (anti-CD34 antibody). We also measured villus height and width, and crypt depth and width.
Summary of Results: Capillary surface density in the lamina propria was significantly greater in the MSC-sEV-treated group compared to the control group (Table; n=6). MSC-sEV treatment was associated with stable weight and better enteral colostrum/milk feeding tolerance (Fig 1). Sex differences were not detected.
Daily weight and enteral milk tolerated volume. Preterm lambs treated with MSC-sEVs maintained body weight and tolerated larger volume of enteral colostrum/milk than vehicle control lambs (*p.
Conclusions: We conclude that MSC sEVs improved capillary growth in the lamina propria of the distal ileum in mechanically ventilated preterm lambs. We speculate that MSC sEVs may be an effective therapy to promote capillary growth in multiple organs in preterm infants at-risk of developing BPD.
Morphometry of distal ileum of preterm lambs.
Group
Capillary surface density (cm-1)
Villus height (um)
Villus width (um)
Crypt depth (um)
Crypt width (um)
Vehicle control (n=6)
53±10
287±132
64±26
56±23
37±14
MSC-sEVs (n=6)
92±17*
335±78
62±11
63±14
43± 6
# 545
CATECHOLAMINE METABOLITES ARE BIOMARKERS OF FETAL HYPOXEMIA AND GROWTH RESTRICTION DURING PLACENTAL INSUFFICIENCY
Moutwakil A, Brown L, Wesolowski S, Rozance P. University of Colorado, Aurora, CO
Purpose of Study: Fetal hypoxemia increases catecholamine secretion. A stable biomarker of elevated catecholamines would provide an opportunity to determine the presence and severity of chronic fetal hypoxemia. Homovanillic acid (HVA) and vanillylmandelic acid (VMA) are metabolites of catecholamines and are commonly used as biomarkers for catecholamine secreting pheochromocytoma tumors because of their stability. Our objective was to evaluate HVA and VMA as biomarkers for the severity of fetal hypoxemia. We hypothesized that HVA and VMA in both fetal blood and amniotic fluid would correlate with the degree of fetal growth restriction (FGR) in a sheep model of placental insufficiency.
Methods Used: Placental insufficiency and FGR were induced by exposing pregnant ewes to elevated temperatures throughout midgestation. Control (CON) ewes were kept at standard temperatures. After removal from experimental temperatures, fetal surgeries were performed in late gestation to place vascular catheters and collect amniotic fluid. Amniotic fluid (n=40 CON, n=17 FGR) and fetal arterial blood (n=12 CON, n=17 FGR) were analyzed for blood oxygen content by ABL Gas Analyzer and norepinephrine (NE), HVA, and VMA by GCMS. Student’s t test, the Mann Whitney test, and linear regression were used to test for differences between groups and relationships between measured parameters.
Summary of Results: : Compared to CON, FGR fetuses weighed less (1990±618 vs. 3117±560 grams, P<0.0001), had lower blood oxygen content (2.63±0.96 vs. 3.53±0.60 mmol/L, P<0.0001) and higher NE (3229±6259 vs. 688±680 pg/mL, P =0.0031), HVA (83.6±19.6 vs. 60.0±10.8 ng/mL, P =0.0003), and VMA (12.5±5.0 vs. 8.2±2.7 ng/mL, P =0.0031). Regression analysis demonstrated that for every 1 kg decrease in fetal weight there were increases in HVA (35.4 ng/mL, R2=0.4494, P<0.0001), VMA (9.3 ng/mL, R2=0.2818, P=0.0030), and NE (1080 pg/mL, R2=0.1399, P=0.0456) and decreases in oxygen content (1.7 mmol/L, R2=0.3733, P=0.0004). Regression analyses demonstrated a negative association of both HVA (R2=0.3199, P=0.0014) and VMA (R2=0.3766, P=0.0004) with oxygen content and a positive association of both HVA (R2=0.2831, P= 0.0030) and VMA (R2=0.3887, P=0.0003) with NE. Amniotic fluid samples from FGR fetuses had HVA concentrations 69.9±44.2 ng/mL higher than CON (P=0.0002) and VMA concentrations 9.5±7.1 ng/mL higher than CON (P=0.0283).
Conclusions: Fetal plasma HVA and VMA concentrations are higher in FGR fetuses compared to CON and were more highly correlated with fetal weight and fetal oxygen content than NE. This is the first study to demonstrate the association between HVA and VMA concentrations, fetal weight, blood oxygen, and experimental FGR, and the potential for HVA and VMA as biomarkers for chronic fetal hypoxemia. We speculate that HVA and VMA can be used in to stratify newborns following complicated pregnancies into those at higher or lower risk of complications related to fetal hypoxemia.
# 546
EFFECT OF CLEMASTINE ON NEUROPHYSIOLOGICAL OUTCOMES IN AN OVINE MODEL OF NEONATAL HYPOXIC-ISCHEMIC ENCEPHALOPATHY
Hawkins CC1, Mike J1, White Y1, Vento C1, Ha J1, Iranmahboub A1, Manzoor H1, Wang A4, Goudy B3, Lakshminrusimha S3, Ostrem B5, Fineman J1, 2, Ferriero DM1, 5, Maltepe E1, 2. 1University of California San Francisco, San Francisco, CA; 2Institute for Pediatric Drug and Device Development, San Francisco, CA; 3University of California Davis, Davis, CA; 4University of California Davis, Davis, CA and 5Weill Institute for Neurosciences, San Francisco, CA
Purpose of Study: Perinatal asphyxia that results in neonatal hypoxic-ischemic encephalopathy (HIE) can lead to significant myelin damage in the immediate perinatal period, as well as postnatally, resulting in long term impairment in motor function. Clemastine is an FDA-approved antihistamine with anti-muscarinic activity and H1 receptor antagonism that has emerged as a promising therapeutic agent for demyelinating diseases in adults. This study focused on defining the pharmacokinetics, safety and efficacy of clemastine administration in a large animal model of neonatal HIE.
Methods Used: Asphyxia was induced to near term lambs at 141-143 days gestation via umbilical cord occlusion. Lambs were randomly assigned to receive clemastine or placebo postnatally. A dose escalation study with pharmacokinetic analysis was conducted to determine the study dose and adverse effects. At various time points of the study, biochemical markers like serial complete blood counts and arterial blood gases were drawn. The lambs were also assessed over a 6-day period to determine neurodevelopmental outcomes before being euthanized. The researchers performing all the experiments, including the injury, post-injury care, biochemical, histological and neurological outcomes analysis were blinded to the group assignment until all measurements have been collected.
Summary of Results: Clemastine’s therapeutic range for neuroprotection in human neonates has not been defined. Based on allometric scaling of adult human doses, rodent stroke models, previous studies in neonatal lambs informing our dose escalation study, 2mg/kg IV Clemastine was chosen as the study dose. Some adverse events, primarily sedation, were seen following clemastine infusion at higher doses. Otherwise, there were no significant differences between the clemastine and placebo groups in vital signs, response to resuscitation, seizure activity, hypoglycemia, mortality or body and brain weight at explant.
The clemastine-treated group exhibited slightly higher absolute lymphocyte count at baseline compared to placebo lambs (p=0.01), but had lower absolute neutrophil count on day 5 after umbilical cord occlusion (p=0.006). Both peripheral blood cell indices, calculated systemic inflammatory indices were decreased in the clemastine-treated lambs on day 5. While clemastine treatment demonstrated a trend towards improvement in neurodevelopmental outcomes on day 1 after UCO, the overall outcomes were not different between the studied groups.
Conclusions: Clemastine improves select biochemical and inflammatory markers following hypoxic-ischemic injury in ovine models. However, we observed no improvements in neurodevelopmental outcomes in the clemastine-treated vs placebo animals.
# 547
THE PRO-INFLAMMATORY NF-κB AND HEPATOCYTE SPECIFIC RESPONSE TO STREPTOCOCCUS AGALACTIAE (GBS)
L Emmanuel, Wright CJ, Grayck MR, Solar M, Zheng L, Siegenthaler J, Doran K, Joyce L. University of Colorado Anschutz, Denver, CO
Purpose of Study: Streptococcus agalactiae (Group B Streptococcus; GBS) is a leading infectious cause of neonatal morbidity and mortality. The current paradigm suggests that GBS bacterial colonization of the gastrointestinal (GI) system leads to systemic spread. The liver is a frontline immunologic organ and plays an important role in innate immune defense. It does this through the prevention of systemic spread by pathogen eradication and through its anatomical position. However, the role of the liver in the innate immune defense against GBS is unknown. We hypothesize that an impaired neonatal hepatic innate immune response contributes to the risk of systemic spread of GBS in neonates.
Methods Used: Neonatal (P2 C57BL/6) mice were exposed to live GBS bacteria (1.5 x 106 CFU) through intragastric (IG) injection. Hepatic tissue was collected at 24 and 48 hours after exposure, and mRNA and nuclear extracts were isolated. The hepatic innate immune response was assessed through RT-qPCR for pro-inflammatory genes (Tnf, Cxcl10, Ccl2). Western Blot was used to test the nuclear translocation of NF-κB subunits p65 and p50 as evidence of NFκB activation. To assess the hepatocyte response in vitro, the AML12 murine hepatocyte cell line was exposed to LTA (GBS cell wall component and TLR2 agonist) at multiple doses (1/10μg/ml) for 1/5 hrs and RT-qPCR was performed for pro-inflammatory genes (Tnf, Cxcl10, Ccl2).
Summary of Results: Following exposure to IG GBS, hepatic expression of Tnf, Cxcl10, and Ccl2 significantly increased in P2 neonatal mice at 24 and 48 hours (n=3-5, p<.05). Upregulation of these pro-inflammatory mediators was temporally associated with significant increases in nuclear translocation of the NFκB subunits p65 and p50 (n=3-5, p<.05). In vitro, LTA exposure of AML12 cells induced significant induction of Tnf, Cxcl10, and Ccl2 (n=3-6, p<.05).
Conclusions: In neonatal mice, GBS exposed through intragastric injections results in hepatic NFκB activation and proinflammatory gene expression. Similarly, LTA exposure of AML12 hepatocytes resulted in significant induction of proinflammatory NFκB target genes. These results demonstrate that GBS induces an innate immune response in the neonatal liver and that the hepatocyte is responsive to these exposures. Future studies are needed to better understand the response to GBS in an adult murine liver. We would also like to better understand a time course and specific NFκB activation in hepatocytes following LTA exposure.
Pulmonary and Critical Care II
Concurrent Sessions
8:00 AM
Saturday, January 20, 2024
# 548
CAN THIS BE COCCI? A COMPLEX EMPYEMA
Patel J, Espinoza VE, Mendoza J, Mishra S, Fox K. Kern Medical Center, Bakersfield, CA
Purpose of Study: Pneumonia is a multifaceted condition with various underlying cases, the most prevalent of which are viral and bacterial. In cases of refractory pneumonia, it is important to consider atypical causes. Without prompt treatment, refractory pneumonia can lead to the formation of complicated parapneumonic effusions or empyema, posing a significant clinical challenge. A thorough history can further delineate atypical causes related to geographical regions, such as coccidioidomycosis, blastomycosis, and histoplasmosis, as well as atypical causes related to exposures in endemic areas such as tuberculosis. Diagnosis often includes use of septum samples, pleural fluid analysis, serologies, and imaging. Disease processes often have pathognomonic findings on imaging. In this case, we discuss a rare finding of calcifications in a complex empyema caused by coccidioidomycosis.
Methods Used: This study reports a case of a complex empyema due to a coccidioidomycosis infection. Information was obtained using the hospital’s electronic medical record system. This case was approved by our hospital’s Institutional Review Board, IRB # 23120
Summary of Results: A 79-year-old male with diabetes, hypertension, and coronary artery disease presented 2 months of fever and malaise with hemoptysis, night sweats and weight loss. On presentation, he was saturating 95% on room air with HR of 94. Chest X-ray revealed a left sided pleural effusion. Computed tomography (CT) scan showed scarring and calcification of the left pleura with significant volume loss of the left lung due to fibrotic changes. On hospital day 1, he had become tachycardic and hypoxic requiring 4L supplemental oxygen. Due to significant calcifications seen on imaging, a diagnosis of tuberculosis was suspected. Thoracentesis was performed and showed a brown, turbid specimen with cellular debris. Pleural fluid analysis was significant for LDH > 4,000 U/L and protein level of 6,100 mg/dL, suggesting an exudative pleural effusion due to infectious cause. Further testing revealed positive Coccidioides IgM antibodies with negative acid-fast bacilli stains of both sputum and pleural fluid. He was diagnosed with a severe empyema secondary to coccidioidomycosis. Unfortunately, he went into respiratory failure and succumbed to his disease.
Conclusions: The significance of obtaining a comprehensive patient history cannot be overstated when diagnosing cases of atypical pneumonia. Although imaging findings can serve as pathognomonic indicators for specific disease processes, such as tuberculosis or histoplasmosis, this unique case demonstrates the importance of broadening the differential diagnosis. The presence of calcifications within primary pulmonary coccidioidomycosis-related empyema is a rare occurrence. This observation highlights the complexity and diversity of atypical pneumonia presentations, emphasizing the need for vigilant clinical assessment to ensure accurate diagnosis and effective management.
# 549
A RARE CASE OF SEVERE EPISTAXIS FOLLOWING INTRAVITREAL BEVACIZUMAB INJECTION
Woods J1, 2, Patel J1, Dhillon A1, Garcia-Pacheco R1. 1Kern Medical Center, Bakersfield, CA and 2Ross University School of Medicine, Christ Church, Barbados
Purpose of Study: We describe the second known case of probable intravitreal bevacizumab (IVB) related severe epistaxis. This case underscores the potential systemic effects of IVB and challenges the assumption that the drug does not enter systemic circulation. We hope to highlight that further research is crucial to understand IVB’s adverse effect profile.
Methods: This is a report on a rare case in a county hospital in southern california. Review for this case was conducted on the hospital’s electronic medical record. The case was approved by our hospital’s Institutional Review Board, IRB# 23107.
Summary of Results: Our patient, a 72-year-old man with a history of hypertension, alcohol use, and age-related macular degeneration, had received his fifth monthly IVB injection for his AMD. Ten days after, he developed severe epistaxis which led to a near-syncopal episode due to hypovolemia supported by the finding of orthostatic hypotension upon arrival to the emergency department. There, he was intubated due to concerns for impending airway compromise. After two days in the hospital he was successfully extubated; however, 36 hours post-extubation, he experienced severe epistaxis requiring reintubation. Craniofacial angiography was obtained which showed mild hyperemia and telangiectasia in the Little’s area on left facial artery injection. Subsequently, embolization of the bilateral sphenopalatine arteries and the septal branch of the left superior labial artery was conducted. The patient was extubated in our intensive care unit without incident and was discharged without experiencing further episodes of epistaxis or mucocutaneous bleeding.
Conclusions: Our case of severe epistaxis resulting in major morbidity and complex interventions in a patient receiving IVB demonstrates the need for further investigation into potential adverse events related to IVB.
Tang W1, Lyu M5, Lee B4, Glass C2, Witztum JL1, Sajti E3. 1University of California San Diego, La Jolla, CA; 2University of California San Diego, La Jolla, CA; 3University of California San Diego, La Jolla, CA; 4University of California, San Diego, La Jolla, CA and 5University of Texas, Southwestern Medical Center, Dallas, TX
Purpose of Study: Increased production of OxPL has been shown to have deleterious effects in acute lung injury, but it’s role in lung fibrosis is not known. OxPL are recognized by the IgM natural antibody (Ab) E06 and binding neutralizes their pro-inflammatory effect. We have investigated the role of OxPL in bleomycin (BLM)-induced pulmonary fibrosis (PF) and whether neutralizing OxPL would ameliorate BLM-induced PF.
Methods Used: C57BL/6J(WT) and E06-scFv transgenic (E06-Tg) mice that overexpress the single-chain fragment of E06 were intratracheally instilled with BLM to induce lung fibrosis. We recorded weight change and survival rate after BLM instillation at serial time points. We measured OxPL and collagen content in the lungs by immunohistochemistry and ELISA. We measured gene expression in whole lung by RNA-seq. Data were analyzed with ImageJ, Prism Homer and Orbit Image.
Summary of Results: E06-Tg mice lost less weight after BLM instillation, and had significantly higher survival rate compared to WT mice. We observed an increased accumulation of OxPL in the lungs of WT mice compared to E06-Tg mice. In addition, we measured higher collagen content in the lung hydrolysates of WT compared to E06-Tg, suggesting more fibrosis in WT mice. To further explore the fibrotic process, we performed RNA-seq of whole lung tissue. After BLM instillation, transcripts that most up-regulated were pro-inflammatory genes and macrophage-related genes.
Conclusions: BLM instillation resulted in a significant accumulation of OxPL in the lungs of WT mice. Elevated OxPL levels were associated with upregulation of pro-inflammatory pathways, and lung macrophage activation. Neutralizing OxPL with E06 Ab resulted in marked improvement in the survival and significantly less lung fibrosis. These data together suggest that OxPL could be a potential target to ameliorate PF by reducing inflammatory responses and collagen deposition.
# 551
A CASE OF NECROBIOTIC PULMONARY NODULES PRESENTING AS AN EXTRAINTESTINAL MANIFESTATION OF INFLAMMATORY BOWEL DISEASE IN A 37-YEAR-OLD FEMALE
Thayapran KG1, Danch M2. 1University of Colorado School of Medicine, Aurora, CO and 2University of Colorado School of Medicine, Aurora, CO
Case Report: Introduction: Necrobiotic pulmonary nodules, defined as sterile lung nodules with cavitary potential, are a rare manifestation of inflammatory bowel disease (IBD). Reported in both ulcerative colitis (UC) and Crohn’s disease (CD), necrobiotic pulmonary nodules can resemble findings in infectious, autoimmune, and malignant etiologies. Here, we describe a case of pulmonary necrobiotic nodules in a patient with IBD initially characterized as UC but later as CD.
Case Presentation: A 37-year-old female with untreated UC presented to an outside hospital with 20 days of non-productive cough, abdominal pain, profuse diarrhea, hematochezia, weight loss, fevers, and fatigue. A chest CT showed numerous bilateral pulmonary nodules measuring up to 3.4cm that were larger 7 days later despite treatment with antibiotics for suspected colitis and pneumonia. After transfer to our facility 11 days later on antibiotics and IV solumedrol, extensive infectious and autoimmune work-up failed to reveal such etiologies, and antibiotics were discontinued. A CT chest 5 days after initial imaging and 1 day of steroids showed decreased size of the pulmonary nodules but with new central cavitations, reducing suspicion for infection or malignancy. Colonoscopy showed moderate UC causing friability from anal verge to cecum with normal terminal ileum and focal areas of ulceration in the sigmoid and descending colon. On day 7 after admission, all presenting symptoms had nearly resolved, and the patient was discharged on oral prednisone with a weekly taper. Given the negative work-up and effect of steroid therapy on her symptoms and pulmonary imaging, UC flare with necrobiotic pulmonary nodules was deemed the final diagnosis. However, the patient was admitted twice over the following 3 months for severe IBD flares despite oral and IV steroids, azathioprine, infliximab, dietary modifications, and close follow-up. Repeat colonoscopy revealed severe colitis from the sigmoid to transverse colon with rectal sparing consistent with CD. Three months after initial presentation, the patient underwent diverting lap loop ileostomy creation for medically refractory CD colitis. A chest CT 3 months after initial imaging showed significant improvement of the pulmonary nodules with cavitations, with many lesions resolving to bandlike opacities representing scarring.
Discussion: Necrobiotic pulmonary nodules are a noteworthy extraintestinal manifestation of IBD that has been reported since 2000. Previous reports have noted an increased occurrence in CD compared to UC, as well as responsiveness to steroid therapy. Here, we described a case of pulmonary necrobiotic nodules in a complex case of IBD that showed improvement and eventual resolution with steroids despite increasing severity of gastrointestinal disease, similar to previous reports. However, further protocoling of steroid therapy for necrobiotic pulmonary nodules has not been well-described, representing an avenue for further research.
# 552
CADAVERIC EXPLORATION OF LUNG ANATOMY VARIATIONS AND CLINICAL RELEVANCE
Navasardyan I, Delaney K, Wedel M. College of Osteopathic Medicine of the Pacific, Western University of Health Sciences, Pomona, CA
Purpose of Study: Variations in lung lobes, fissures, and hilar structures are potentially relevant to the functional and clinical anatomy of the lungs, and could inform diagnoses and treatment strategies. Our goal in this study was to investigate the relationship between variations in superficial features of the lungs, primarily the lobes and fissures, and variations in the bronchial tree in a cadaveric population. We also conducted a literature review of lung variations and their clinical implications. We hope to elucidate potential relationships among the gross anatomy, the functional anatomy, and the pathophysiology of the lungs. Documenting these variations could improve radiological interpretations and surgical outcomes, and hopefully enhance clinical practice and patient care.
Methods Used: Thirty pairs of embalmed lungs from human cadavers were obtained through the WesternU Willed Body Donation Program and preserved following established laboratory protocols. We examined 30 pairs of lungs to document variations in the hilum and in the lung lobes and the fissures that define them. We dissected lung specimens with substantially variant patterns of lobes and fissures to reveal the bronchial tree pattern.
Summary of Results: Eight right-sided and four left-sided superficially variant lungs were identified and underwent further dissection of their bronchial tree. Photographic documentation of each lung was undertaken before proceeding with the bronchial tree dissection. The most common variations were incomplete fissures (10 of 60 lungs, 17%) and accessory fissures (3 of 60, 5%). The continuation of either the horizontal or the oblique fissure past the other, to at least partially divide one of the three lobes, occurred in 2 lungs (3%). Despite the prevalence of superficial variations, the bronchial trees of all 12 superficially variant lungs showed normal branching patterns, and the hilar anatomy of all 12 was also typical.
Conclusions: Consistent with the published literature, our findings indicate that variations in the lung lobes and fissures are more common than those in the underlying bronchial tree branching patterns. This disparity between superficial and deep variations is likely due to the result of embryology. The primary and secondary bronchi form very early in lung development, and the early lung is much more superficially lobular than the late fetal lung. The numerous small lobes of the early lung fuse by obliteration of the fissures that separate them. This process continues until the typical 2-3 lobes and 1-2 fissures remain. This comparatively late process of lobar fusion explains how superficially variable lungs can be built on top of the typical and deeply conserved pattern of bronchial branching. Factors that promote or limit fissure obliteration are not well understood, and future work in this area will help elucidate the developmental and functional anatomy of the lungs.
# 553
A rare case of Valsartan induced angioedema
Ipalawatte H, Abadir S, Gower A, Takher J. HCA Los Robles Regional, Thousand Oaks, CA
Case Report: Angioedema is an uncommon but life-threatening condition that could progress to airway obstruction. It manifests as sudden, non-pitting, asymmetric swelling of deep layers of the skin or mucosal membranes. While angiotensin II receptor blockers (ARBs) were initially developed to avoid angioedema seen with angiotensin-converting enzyme (ACE) inhibitors, the increase in use of ARBs for heart failure and hypertension have lead to an increase of number of reported cases of ARBs induced angioedema.
Angioedemia of the face and neck is a rare and life-threatening condition seen with the use of angiotensin-converting enzyme (ACE) inhibitors [1]. The condition is characterized by spontaneous, asymmetric swelling of the deep layers of the skin or mucosal membranes [2]. While most cases of angioedema have been reported to be associated with ACE inhibitors, some patients have been found to develop the condition with angiotensin II receptor blockers (ARBs) [3]. While ARBs were developed to avoid the side effects of both the angioedema and cough seen with ACE inhibitors, the increase in angiotensin II levels causes inhibition of ACE activity and leads to the development of angioedema [4]. Here we present a case of ARBs induced angioedema in a hypertensive patient on valsartan
for years without prior episodes of angioedema.
# 554
Activation of Platelets and the Complement system in Schistosomiasis-induced Pulmonary Hypertension
Jordan M3, Posey JN3, Mickael C1, Nozik E2, 4, Delaney C3, 5. 1University of Colorado, Aurora, CO; 2University of Colorado, Aurora, CO; 3University of Colorado, Aurora, CO; 4Colorado Children’s Hospital, Aurora, CO and 5Colorado Children’s Hospital, Aurora, CO
Purpose of Study: Schistosomiasis infection may result in schistosoma-associated pulmonary arterial hypertension (sch-PAH) and is a major cause of morbidity and mortality worldwide. Schistosoma infection in mice leads to development of PH mediated via activation of the innate and adaptive immune system leading to a proinflammatory pulmonary response. Platelets are increasingly recognized as immune cells that contribute to both local and systemic inflammation. Our lab is interested in the role of platelets in inflammatory mediated PH. Disorders of complement hyperactivation result in uncontrolled platelet activation. In this study, we hypothesized that complement mediated platelet activation contributes to the development of schistosoma-induced PH.
Methods Used: C57BL/6 mice were intraperitoneally sensitized at 6 weeks of age with S. mansoni eggs and 2 weeks later intravenously treated with S. mansoni eggs. Blood and lung tissue were collected at 3- or 7-days post-infection. Whole blood was collected via RV cardiac puncture. Platelet activation and platelet expression of complement components were assessed by flow cytometry (FCS). Plasma complement anaphylatoxins C3a and C5a were measured by ELISA. Platelet localization in the lung was assessed by immunohistochemistry (IHC) by staining for CD41. To determine the effect of platelet depletion, selected mice were pre-treated with an anti-platelet rat IgG antibody (anti-GP1bα; 4μg/gm body weight delivered IP) one hour prior to IV egg treatment. Lung T cells and pulmonary interstitial macrophages (IM) were quantified by whole lung FCS. Lung IL-4 and IL-13 were measured using ELISA.
Summary of Results: We found that platelets were activated at 3 days post-infection demonstrated by increased expression of the alpha granule protein P-selectin, increase in activated α2βB3 and increased phosphatidylserine. Along with platelet activation, platelets expressing complement receptors increased and circulating complement components increased with infection. At 3 days, platelets were increased in the distal lung and the pulmonary arteries compared to controls. Both T cells and lung IMs were increased at 3 days, this increase was prevented in thrombocytopenic mice. IL-4 and IL-13 were both increased at 7 days, platelet depletion prevented lung IL-4 and attenuated IL-13 increase. RVSP and RVH were increased in schistosoma platelet replete mice, this increase was prevented in thrombocytopenic schistosoma mice.
Conclusions: Platelets are activated and increased in the lungs and pulmonary arteries of mice infected with S. mansoni. Circulating complement factors are increased in infection and expressed on activated platelets. Thrombocytopenia prevents the increase in lung T cells and IMs, and the pro-inflammatory cytokines IL-4 and IL-13, and prevents sch-PH. We speculate that platelet activation and complement crosstalk contributes to sch-PH via T cell activation and that targeting the platelet immune signaling may be a novel therapeutic strategy for this deadly disease.
# 555
OUTCOMES OF INFANTS IN THE NEONATAL INTENSIVE CARE UNIT UNDERGOING MULTIPLE ATTEMPTS OF INTRACHEAL SURFACTANT ADMINISTRATION
Siddiqui S, Feliz Sala EE, Sandhu JK, Ramanathan R, Biniwale M. University of Southern California/Los Angeles General Medical Center, Los Angeles, CA
Purpose of Study: Surfactant administration decreases mortality and complications associated with respiratory distress syndrome (RDS) in premature infants. The most common administration technique such as the INtubation-SURfactant-Extubation (INSURE) method, requires intubation, giving surfactant through an endotracheal tube and a brief period of invasive mechanical ventilation. More recently, we changed our practice of surfactant administration using a thin catheter known as Less Invasive Surfactant Administration (LISA) which does not require endotracheal intubation. This project aims to compare outcomes for infants who successfully received surfactant in a single attempt versus multiple attempts via INSURE and LISA methods.
Methods Used: This is a retrospective (2016 to 2022) cohort study of infants admitted to Neonatal Intensive Care Unit (NICU) at Los Angeles General Medical Center who received surfactant administration through either LISA or INSURE. Data was abstracted from the NICU database and electronic health records, and analyzed using SPSS version 29. Infants were divided into two groups based on one or more attempts during surfactant administration via INSURE or LISA.
Summary of Results: There were 119 infants included in this study. 69/119 (58%) received surfactant via INSURE and 50/119 (42%) received surfactant via LISA. There were 18/69 (26%) neonates who required multiple attempts of INSURE and 13/50 (26%) who required multiple attempts of LISA although the number of doses did not vary significantly. There was no significant difference based on infant demographics, mode of delivery, delivery interventions, or maternal antenatal steroids. There was a significantly higher rate of complications in infants with multiple attempts of INSURE (11%, p-value = 0.02). There were complications in 14% of LISA attempts, such as trauma or bradycardia. Infants requiring multiple attempts of surfactant via INSURE or LISA did not have a significantly higher need for intubation at 3 or 7 days of life though infants who received surfactant via multiple attempts of LISA did have increased duration of time requiring nasal cannula. About half (47%) of infants requiring multiple attempts of INSURE, whereas 8% of neonates requiring multiple attempts of LISA, had a diagnosis of bronchopulmonary dysplasia (BPD) at discharge. There was no significant differences in rates of intraventricular hemorrhage, patent ductus arteriosis, or pneumothorax across groups.
Conclusions: Our preliminary data shows that infants requiring multiple attempts of surfactant with INSURE had higher rates of procedural complications. Infants reuqiing multiple attempts for LISA procedure had increased requirement of nasal canuula. Multiple procedural attempts via INSIURE or LISA procedure did not translate into any long term morbidties. Collection of data is ongoing to determine other factors of significance and to verify these results in a larger sample size.
Comparison of Patient Demographics and Outcomes Between Neonates Who Received One Attempt at Surfactant Administration Versus Those Who Received Multiple Attempts.
Mean ± Standard Deviation; NCPAP - nasal continuous positive airway pressure; NIPPV - nasal intermittent positive pressure ventilation;
Behavior, Development and Psychology II
Concurrent Sessions
10:15 AM
Saturday, January 20, 2024
# 556
Leveraging Large Language Models to Assess Documentation of Medication Side Effects in Clinical Visits for Children with Attention-Deficit/Hyperactivity Disorder
Bannett Y, Gunturkun F, Pllai M, Herrmann JE, Huffman LC, Feldman HM. Stanford University School of Medicine, Stanford, CA
Purpose of Study: This study’s purpose was to assess the accuracy of artificial intelligence (AI) large language models (LLMs) in measuring the extent to which pediatricians inquire about and document ADHD medication side effects. If accurate, LLMs could be applied as quality metrics for primary care management of ADHD, a highly prevalent condition.
Methods Used: We identified 1249 children aged 6-11 years, seen >2 times in 2015-2022 in a community-based primary care network, who had >2 visits with an ADHD diagnosis and >2 ADHD medication prescriptions (stimulants or non-stimulants). We extracted clinical notes from all office/telehealth/telephone visits conducted after an ADHD medication was first prescribed (n=16,514 notes; 5,364 office/telehealth notes; 11,150 telephone notes). For model building, two clinicians annotated notes for a random sample of 120 patients (527 notes); inter-annotator agreement for clinician inquiry about medication side effects was 0.86. We used a subset of notes (n=419 notes, 80%) to train and tune the newly available open-source Large Language Model Meta AI trained on 13 billion parameters (LLaMA13B). In a holdout test set (n=108 notes, 20%), we assessed model performance compared to manual chart review. To validate our approach, we deployed the model on notes for the remaining 1,129 patients in the cohort. To assess model performance, we sampled and annotated 400 notes - deployment test set; inter-annotator agreement was 0.93.
Summary of Results: In classifying notes that contain side effects inquiry, the LLaMA13B model achieved a sensitivity of 89.9%, specificity of 86.4%, with an area under the curve (AUC) of 0.94 on the holdout test set, and a sensitivity of 89.2%, specificity of 95.7%, with an AUC of 0.98 on the deployment test set. Patient characteristics were similar across patients with and without documentation of side effects inquiry (Table). Based on model classifications, pediatricians inquired about side effects in 91% of patients prescribed stimulants but only in 75% of those prescribed non-stimulants (Figure). In 43% of patients, telephone visits were used for side effects inquiry.
Conclusions: Deploying a large language model on a vast and variable set of clinical notes, including notes for telephone visits, can enable scalable and continuous quality measurement of psychopharmacological medication management in primary care – leading to improved healthcare delivery and health outcomes.
Characteristics of study cohort: patients ages 6-11 years prescribed medications for ADHD by their primary care clinician.
Age in years at first visit with a diagnosis of attention-deficit/hyperactivity disorder. IQR=Inter-Quartile Range ^ASD=Absolute Standardized Difference; values of 0.2, 0.5, and 0.8 correspond to small, moderate, and large differences, respectively.
# 557
Comparison of Bayley Score Changes for High-Risk Infants after Release of Updated Norms
Starzyk D1, Dempsey J2, 3, Cooke DL1, Dempsey AG1. 1University of Colorado School of Medicine, Aurora, CO; 2Children’s Hospital Colorado, Aurora, CO and 3University of Colorado School of Medicine, Aurora, CO
Purpose of Study: To determine the potential impact of error in Bayley-IV norms for eligibility determination and anticipatory guidance among a population of children born with medical complications at ages 1 to 3 years.
Methods Used: This study involves secondary analyses of data gathered as part of a study to compare in-person developmental assessments (Bayley-IV scores) to two different developmental assessments conducted via telehealth. Bayley-IV scores were obtained for 30 children (ages 1-3 years) as part of the original study and scores were calculated based on the original Pearson norms for the Bayley IV. For the current proposal, we rescored the Bayley exams using the updated norms and will present the comparisons and implications for EI eligibility based on the score changes.
Summary of Results: The majority of children’s scores remained unchanged after rescoring with updated norms, particularly in the cognitive, receptive, expressive, and gross motor subscales (all with less than 10% of the children with changed scores each). In contrast, the fine motor subscale had a greater proportion of children with impacted scores, with scores impacted for just over 20% of the sample. The mean scores showed minimal differences between original and rescored data; the most notable change was in the Fine Motor Score (from 7.83 to 8.03), where the p-value was 0.01, indicating a statistically significant change. For other domains, the p-values ranged from 0.16 to 0.33, suggesting that the rescoring did not significantly alter the original data. Out of the re-scored data, 3 cases (10% of the sample) with standard scores ranging 51-79 were impacted. This was contradictory to Pearson’s indications that children who scored low average to extremely low range would not be impacted.
Conclusions: Although the majority of children with Bayley scores calculated from the original norms did not have changes with the new norms, there were still a significant proprotion of children whose scores were impacted (ranging from 10-20% based on subdomain. Notably, score changes involved both increases and decreases in scores and there were score changes for children whose original scores were in the low average range or below. Those engaging in research with the Bayley will need to consider recoding all data with the new norms to ensure accurate scores. The presentation will conclude with a discussion on whether EI eligibility would have potentially been impacted.
Changes in Bayley Subscale and Standard Scores.
Scale Scores (M=10, SD=3)
Standard Scores (M=100, SD=15)
Cognitive(N=30)
Receptive
(N=29)
Expressive
(N=30)
Fine Motor
(N=29)
Gross Motor
(N=29)
Cognitive
(N=30)
Communication
(N=28)
Motor
(N=28)
Number with No Changes in Score
28
28
29
23
28
28
21
16
Number with Changed Score
2
1
1
6
1
2
7
12
Mean (Original Norms)
6.93
6.31
6.03
7.83
6.17
84.67
78.04
83.26
Mean (Updated Norms)
7.00
6.34
6.10
8.03
6.2
85
78.46
83.56
Range of Differences
0-1
0-1
0-1
0-1
0-1
0-5
0-10
0-6
p-Value of Difference (Absolute)
0.16
0.33
0.16
0.01
0.33
0.16
0.32
0.27
# 558
The eXtraOrdinarY Babies Study: COMPARISON OF 3 DEVELOPMENTAL SCREENING MEASURES FOR IDENTIFYING DEVELOPMENTAL DELAYS IN YOUNG CHILDREN WITH PRENATAL DIAGNOSIS OF SEX CHROMOSOME TRISOMIES
Radunovic A1, 2, Bothwell S3, Thompson TG1, Davis S1, Ross J4, Tartaglia N1. 1University of Colorado School of Medicine, Children’s Hospital Colorado, Aurora, CO; 2Tilman J. Fertitta Family College of Medicine at the University of Houston, Houston, TX; 3University of Colorado, Anschutz Medical Campus, Aurora, CO and 4Nemours Children’s Hospital, Wilmington, DE
Purpose of Study: As non-invasive prenatal testing expands, increasing numbers of infants are being identified in the prenatal period with Sex Chromosome Trisomies (SCT), including XXX, XXY/Klinefelter syndrome, or XYY. Children with a SCT are at increased risk for developmental delays in both early language and motor domains. Developmental screening measures with optimal diagnostic accuracy, as measured by sensitivity and specificity, are necessary for the proper care and referral of children with SCT. The eXtraOrdinarY Babies study previously identified low sensitivity and specificity of the Ages and Stages Questionnaire (ASQ) at 6 and 12 months of age. In this project we aimed to: (1) build upon previous analyses with larger sample sizes and expanded age range up to 24 months, and (2) evaluate 2 additional screening measures including the Parents’ Evaluation of Development Status (PEDS) and the Infant Toddler Checklist (ITC) to determine their usefulness to detect developmental delays for this high-risk population.
Methods Used: The eXtraOrdinarY Babies Study is a natural history study of infants with a prenatal diagnosis of XXX, XXY, or XYY. Caretakers completed the ASQ, ITC, and PEDS prior to direct developmental evaluation using the Bayley Scales of Infant and Toddler Development (Bayley-3 or 4) at the 6 month (n=114), 12 month (n=132), and 24 month (n=79) visits. Developmental delay was defined as a Bayley scaled score of less than 7. Domains of each screening tool were matched with corresponding Bayley domains, and sensitivity/specificity analyses were conducted for the 3 screening measures at each timepoint. Desired sensitivity and specificity were 0.8 or above.
Summary of Results: There were no differences in developmental scores between the 3 SCT subtypes, thus all were combined for analysis. Overall, the ASQ, PEDS, and ITC sensitivities were below threshold for acceptability across almost all developmental domains at all timepoints, with sensitivity values ranging from 0.09 to 0.67. The exception was the ASQ at 12 and 24 months in the gross motor domain with sensitivities of 0.94 (12m) and 0.75 (24m). Specificity results were higher across all three measures ranging from 0.5 to 0.97.
Conclusions: All three developmental screening tools evaluated had low sensitivities in young children with SCT due to high false negative rates, and thus cannot be relied upon for identifying all cases with developmental delays. However, the higher specificity values indicate fewer false positives overall. Based on these results, direct developmental assessments are recommended for infants with SCT due to the heighted risk for delays and the lack of appropriate screening measures to ensure necessary referrals to early intervention therapy. Future directions include analyses of items most predictive of delays to determine if alternative scoring or new screening measure specific to the profile in children with SCT may be developed.
# 559
ANXIETY IN TURNER SYNDROME: ENGAGING COMMUNITY TO ADDRESS BARRIERS AND FACILITATORS TO DIAGNOSIS AND CARE
Carl A3, Good M2, Haag E2, Hutaff-Lee C4, 1, Swain D5, Tartaglia N5, 3, Davis S3, 6, Sakamoto C7, Thompson TG3, 7. 1University of Colorado School of Medicine, Aurora, CO; 2Turner Syndrome Colorado, Westminster, CO; 3Children’s Hospital of Colorado, Aurora, CO; 4Children’s Hospital Colorado, Aurora, CO; 5University of Colorado School of Medicine, Aurora, CO; 6University of Colorado School of Medicine, Aurora, CO and 7University of Colorado School of Medicine, Aurora, CO
Purpose of Study: Turner syndrome (TS), a genetic condition caused by complete or partial loss of the second sex chromosome, is associated with complex medical manifestations. The TS community identifies anxiety as a major contributor to reduced quality of life. This study aimed to improve our understanding of anxiety symptomatology in individuals with TS (IWTS) and to identify barriers and facilitators to diagnosis and care.
Methods Used: A mixed methods design integrated community engagement, including community leaders as decision-making co-Is and a collaborative community advisory board. The wider TS community was engaged through an online survey (N=135; Caregivers (CG)=61, IWTS=74) followed by in-depth interviews (CG=5, IWTS=5). Descriptive statistics, linear mixed models, logistic regression, and fisher’s exact tests were conducted for quantitative analysis and a rapid team-based approach was used for qualitative analysis.
Summary of Results: The sample ranged in age from 3-64 years (CG: 12y±6; IWTS: 26y±12). Majority of respondents said anxiety symptoms occur two or more days per week (CG=65%, IWTS=87%) and regularly impact activities of daily life, with IWTS reporting more frequent symptoms than CG (p=0.03). IWTS reported feeling anxious more often at school/work (71%), while both rater groups reported anxiety related behaviors were most likely to be expressed at home (CG 61%, IWTS 78%). Insomnia was the most common symptom of anxiety endorsed frequently across age and rater groups (>70% per group). Some symptoms showed significant (p<.05) linear relationships with age: physical aggression (CG OR: 0.91 95%: 0.83-0.99), crying/tantrums (CG OR: 0.90 95%CI: 0.83-0.97), clinging (IWTS OR: 0.96, 95%: 0.92-0.99), and diarrhea (IWTS OR: 1.07 95%:1.03 1.12) decreased with age, while body tension (IWTS OR: 1.04 95%: 1.01-1.08) increased with age. Some anxiety triggers increased significantly (p<.05) with age: ‘dealing with conflict’ (CG OR 1.09, 95%CI 1.00-1.18), ‘managing expectations’ (CG OR 1.16, 95%CI, 1.07-1.28; IWTS OR 1.05, 95%CI 1.01-1.10), and ‘recalling negative events’ (CG OR 1.08, 95%CI 1.00-1.18). Non-linear relationships with age included ‘dealing with organizational tasks’ as a frequent anxiety trigger in school-aged children (p=.037), and ‘new friendships’ in adolescence (p<.001). Therapy and medication for anxiety were reported as helpful by most respondents who had tried these strategies. Qualitative themes included: ‘Triggers for anxiety are related to TS’ (e.g., executive functioning deficits, medical procedures), ‘Anxiety impacts the whole family’ (e.g., high burden on mothers, separation anxiety), and ‘Opportunities for early identification and intervention’ (e.g., missed early signs, appreciation for early conversations).
Conclusions: Anxiety is common in TS; however, symptoms and triggers can change with age and may go undiagnosed or untreated during childhood. Families carry the burden of managing and accommodating for daily anxiety symptoms in the home.
# 560
Development and Evolution of a Psychology-Led Screening Program in a Level-3 Neonatal Intensive Care Unit
Cooke DL, Dempsey AG, Solness C, Kelleher J, Takamatsu S, Dempsey J. CU Anschutz Medical Campus, Denver, CO
Purpose of Study: Parents with infants admitted to the Neonatal Intensive Care Unit may be at a higher risk of perinatal mood and anxiety disorders. Forty percent of NICU mothers are estimated to experience postpartum depression. Increased interest has arisen in implementation of systematic NICU screening for depression, however most only occur at a single time point. The following data from program evaluation provides information on the development and implementation of a psychologist-led NICU screening protocol.
Methods Used: Institutional IRB was contacted and they confirmed no IRB approval was needed due to the results reflecting program development and evaluation project. Psychology providers developed a NICU screening protocol in December of 2020. Initial design was to screen at 2 weeks, 1 month, 2 months, 4 months, and within 2 weeks of discharge. Screening protocol was refined in January of 2021to reduce redundancy in screening, reduce provider/patient burden, and reduce disparities. The program followed the American Pediatric Association recommendations of screening at 1 month, 2 months, 4 months, and 6 months.
Summary of Results:Implementation: Psychologists approach mothers at designated timepoints to introduce the screening, explain why it is being administered, how the results will be used and stored in the mother’s electronic health record, and that scores will be reviewed and explained directly to the patient afterwards. The patient is then given the option to complete the screener or decline.
Inclusion: Screenings were provided in the respondent’s native language, when available. When parents are unable to be at bedside, screening was conducted over the phone, using a hospital-provided interpreter when needed.
Results: Screening is presented both in total percentage of eligible mother screened and a corrected percentage (Table 1). At one month, 64.38% (N=197/306) of eligible mothers were screened, 81.07% corrected (N=197/243). At two months, 53.19% (N=75/141) of eligible mothers were screened, 78.95% of corrected (N=75/95). At four months, 37.93% (N=11/29), 68.75% corrected (N=11/16). A mother declining screening occurred in only 2.3% of encounters. Reasons for missed screening are presented in Table 1 as percentage of missingness accounted for by that reason.
Conclusions: The screening appears acceptable to mothers in terms rates of declined screenings. Completion over the phone is a necessary component to catch mothers at risk for greater mental health concerns or who are experiencing psychosocial stressors that limit their ability to be at bedside. Limitations of this screening program to be addressed include 1) screening of non-birthing partners; 2) screening for anxiety as well as depression; 3) evaluate validity of screening in the case of verbal administration of an English screener through interpretation, and/or mothers with intellectual impairment; 4) tracking referrals and results of screening; and 5) quality improvement project to increase screening to 80% at all timepoints.
Percentage of Screened and Reasons for Failure to Screen by Month.
Family unable to be reached at bedside or via phone
3.92%
3.55%
3.45%
Already in treatment
2.29%
11.35%
6.90%
Declined
1.63%
2.84%
6.90%
Language
1.31%
0.71%
3.45%
Other^
0.98%
2.13%
3.45%
Screen given 2 weeks prior
0.00%
1.42%
0.00%
Indicates number has been corrected to reflect only percentage of failure to screen due to clinicians missing the mother ^Unable to be screened due to cognitive concerns, legal involvement, hospitalization, etc.
# 561
IMPROVING FAMILY ENGAGEMENT AND REDUCING DISPARITIES THROUGH TELEHEALTH IN THE NEONATAL INTENSIVE CARE UNIT
Kelleher J1, Santisteban A1, Dempsey J2, Cooke DL1, Solness C1, Huber K1, Dempsey AG1. 1University of Colorado School of Medicine, Aurora, CO and 2Children’s Hospital Colorado, Aurora, CO
Purpose of Study: This project’s primary aim was to increase frequency of parental participation in nursing care sessions by offering families the opportunity to participate virtually via iPads throughout an infant’s admission to the Neonatal Intensive Care Unit (NICU). Parental engagement is strongly linked to the infant’s overall health, development, and readiness for discharge. A critical component of engagement is parental presence at bedside, where they have opportunities to directly interact with their baby and to receive education about their baby’s care. Many NICU families experience challenges with regular visitation, particularly with long NICU stays. Common challenges include caregiving responsibilities for siblings, return to work, and transportation. Baseline data show that families with Medicaid often experience more of these barriers than families with commercial insurance.
Methods Used: The project team used the Institute for Health Care Improvement Model for Improvement (MFI) quality improvement approach, specifically Plan-Do-Study-Act cycles (PDSA) to create an iterative cycle of improvement and systematically test the technology and implementation processes. Visitation data (presence during care times on-site or virtually) was collected from the electronic medical record (EMR).
Summary of Results: Visitation and family engagement data was collected from the EMR to determine how often families were present for cares. The goal metric was set at 1 care session per day for 4 days per week, indicating families were present more days than not. During the project, a high of 15% of all care sessions were virtual. During the first 29 weeks of the project, the percentage of families meeting the metric dropped from 63% at 49 days of life (DOL) to 10% at 91 DOL. This is in stark contrast to families with commercial insurance, whose visitation improved (74% to 86%) over that same period. During the last 29 weeks of the project, the percentage of families with commercial insurance meeting the metric was 94% at 49 DOL and 90% at 91 DOL. For families with Medicaid, 58% met the goal at DOL 49 and 50% at DOL 91.
Conclusions: Families of premature and/or medically complex infants often experience stressors that limit their ability to be consistently present at bedside, particularly during lengthy NICU stays. Virtual cares are one way to address ongoing disparities that disproportionately affect families with lower socioeconomic status (as indicated by Medicaid coverage). By introducing telehealth, families had more opportunities to engage with their infant and receive important education. The percentage of families with Medicaid who met the goal stayed relatively stable instead of the sharp decline after DOL 49 as seen in the first part of the project. Despite this progress, the gap between commercially insured and publicly insured families remained. This clearly shows telehealth has significant benefits, and there is still work to be done to ensure all families can be present with their infant in the NICU.
# 562
LONGITUDINAL FOLLOW-UP OF METFORMIN TREATMENT IN FRAGILE X SYNDROME
Montanaro A1, Buldoc F2, Lippe S3, Hagerman RJ4. 1University of Bari Aldo Moro, Bari, Italy; 2University of Alberta, Edmonton, AB, Canada; 3University of Montreal, Montreal, QC, Canada and 4UC Davis MIND Institute, Sacramento, CA
Purpose of Study: Metformin targets Fragile X syndrome (FXS) by suppressing the mTOR pathway, elevated in both animal models and patients. Fragile X syndrome patients experience slower cognitive development, with IQ decline during childhood and adolescence. In this study, we are following the trajectory of IQ and adaptive behavior changes over one to three years in individuals with FXS who are clinically treated with metformin in an open label trial.
Methods Used: Twenty-six individuals with FXS ages 6 to 25 (13.15 ± 5.50) and nonverbal IQ of (57.69 ± 15.46) were treated with metformin (500mg – 1000mg) for 1-3 years (1.88±0.63). They all had a baseline IQ test using the Leiter-III non-verbal cognitive assessment and behavior assessment using the Vineland-III before the start of metformin. Repeat Leiter-III and Vineland-III were completed after at least one year of metformin therapy.
Summary of Results: Nonverbal IQ scores pre- and post- metformin were (pre: M = 57.69±15.46; post: M = 58.35±15.27) respectively; t-test was non-significant [t(26) = 0.65±6.78, p = 0.627]. Adaptive behavior among all participants also appears to remain the same over the duration of the study based on the VABS-3 assessment. The findings thus far indicate that both IQ and adaptive behavior are stable over time, and we did not see a significant decline in either measure.
Conclusions: Overall the small sample size and short follow-up duration limit the interpretation of the effects of metformin on cognitive development and adaptive functioning. However, it does begin to show stability of both non-verbal IQ and adaptive behavior. Further, longer-term investigations with a control group are needed for validation and therapeutic potential exploration.
Genetics III
Concurrent Sessions
10:15 AM
Saturday, January 20, 2024
# 563
Should We Consider Screening Newborns of California to Identify their Glucose-6-Phosphate Dehydrogenase (G6PD) Enzyme Status?
Bhutani VK1, Vidavalur R2. 1Stanford University School of Medicine, Palo Alto, CA and 2Cayuga Medical Center/Weill Cornell Medicine, Ithaca, NY
Purpose of Study: American Academy of Pediatrics has designated G6PD deficiency (G6PDd) as a key pre-discharge risk factor for bilirubin induced neurotoxicity to lower bilirubin thresholds and administer phototherapy. Thus far, this condition is not included in the mandated California Newborn Screening Program. Our primary objective is to empirically estimate the annual incidence of G6PDd among newborns in California, accounting for gender and racial diversity, thereby elucidating whether the implementation of newborn screening for this condition would be a judicious or onerous undertaking.
Methods Used: Data for California live births for the year 2021 was obtained from National Center for Health Statistics. Dataset included all birth data for California by race, based on maternal race and neonatal gender. We used US racial G6PDd prevalence data from published studies. Leveraging existing US racial prevalence data for G6PDd from published studies, we applied these race-specific prevalence estimates to extrapolate the anticipated incidence of G6PDd within the California birth cohort. Furthermore, we computed allele and carrier frequencies employing the principles of Hardy-Weinberg equilibrium.
Summary of Results: For 420,608 live-birth cohort in 2019 (Table 1), we derived an estimate of 5,811 newborns with G6PDd at birth (95% CI: 5,662, 5,962), equating to an overall incidence rate of 1,382 (95% CI: 1,346, 1,418) per 100,000 live births. When factoring in both sex and race, the prevalence rate stood at 1,081 (95% CI: 1,049, 1,112) per 100,000 live births. Notably, the incidence among non-Hispanic black males reached 11,211 per 100,000 live births, in stark contrast to 417 among non-Hispanic white males (Table). A similar pattern emerged among females, with rates of 4,674 and 263 for Black and White newborns, respectively, per 100,000 live births. Furthermore, our analysis revealed that approximately 4.5% of female births exhibited heterozygosity for G6PDd. These current annual estimates indicate that at least six newborns in California face an elevated risk of severe hyperbilirubinemia due to G6PDd.
Conclusions: These extrapolated prevalence estimates regarding G6PD deficiency in newborns, taking into account gender and racial disparities, underscore the potential benefits of integrating point-of-care enzyme identification and providing pre-newborn discharge counseling for both families and healthcare providers. This proactive approach could bridge the existing gaps in care and ensure a healthier start for California’s newborns.
# 564
Applying Data Science Methodologies to Clinical Genetic Data to Estimate Genetic Disorder Prevalence
Jackson S, Woods J. Valley Children’s Hospital, Madera, CA
Purpose of Study: Question: Can data from under-utilized clinical genetic testing data be leverage to gain population genetic insights?
Setting: Valley Children’s Healthcare (VCH) has a catchment area of 1.4 million pediatric patients and is the primary quaternary children’s hospital for the California’s Central Valley (CV) and also serves a substantial number of patients in the Central Coast.
Participants: All patients who had genetic testing at VCH during the study period.
Main Outcome and Measures: The main outcome was the estimation of genetic disorder prevalence in our catchment area. Secondary outcomes included mapping of genetic variants as a choropleth and identification of patients with genetic disorders lost to follow up.
Conclusions: Utilizing readily available software we developed a database and EDA methodology enabling us to estimate genetic disorder prevalence, localize geographies enriched for pathogenic variants and identify patients requiring further medical management.
Estimates of Minimum Genetic Disorder Prevalence.
AD Het
Gene
AD Het
Prevalence
AD Het
Total
AR Hom
Gene
AR Hom
Prevalence
AR Hom
Total
XL Hemi
Gene
XL Hemi
Prevalence
XL Hemi
Total
AR Het
Gene
AR Het
Prevalence
AR Het
Total
NF1
10.94
51
PEX6
1.5
7
ABCD1
1.72
8
CFTR
13.3
62
COL1A1
7.08
33
CFTR
1.29
6
DMD
1.72
8
PAH
10.3
48
FBN1
5.79
27
GALC
1.07
5
G6PD
0.64
3
ACADM
60.1
28
PTPN11
3.65
17
MCC2
1.07
5
GLA
0.43
2
HFE
3.65
17
HBA1
2.79
13
PAH
0.86
4
MID1
0.43
2
ARG1
2.36
11
XL Het
Gene
XL Het
Prevalence
XL Het
Total
SV
SVTotal
ABCD1
2.79
13
arr[GRCh37] 22q11.21(18919528_21460594)x1
5
DMD
2.79
13
arr[GRCh37] 17q12(34816424_36207539)x1
2
MECP2
1.5
7
arr[GRCh37] 1q21.1q21.2(145388977_147726541)x1
2
G6PD
0.64
0.64
arr[GRCh37] 21q11.2q22.3(15484314_48091215)x3
2
DDX3X
0.43
2
arr[GRCh37] 22q13.32q13.33(48540382_50951420)x1
2
Counts of the top five pathogenic and likely pathogenic (P/LP) variants by gene sorted by zygosity and inheritance pattern. P and LP variants were pooled for the calculation of variant counts. AD: autosomal dominant, AR: autosomal recessive, XL: X-linked, Het: heterozygous, Hom: homozygous, Hemi: hemizygous. Prevalence is per 100,000 individuals in our 466,011 patient VCH population during our five-year study period. AD het represents individuals expected to be affected with an autosomal dominant disorder, AR Hom affected with a recessive disorder, AR Het autosomal recessive disorder carriers, XL Hemi affected with an X-linked disorder and XL Het carriers for an X-linked disorder. The top ten P/LP structural variants are also listed.
# 565
FETAL DIAGNOSIS OF AUTOSOMAL DOMINANT ROBINOW SYNDROME DUE TO NOVEL DVL1 VARIANT: EXPANSION OF THE PHENOTYPE
Smith CM2, Guinon K1, Tise CG3, Bachir S3. 1Stanford Medicine: Children’s Health, Palo Alto, CA; 2Stanford Medicine: Children’s Health, Palo Alto, CA and 3Stanford University, Palo Alto, CA
Purpose of Study: Robinow syndrome is a skeletal dysplasia syndrome characterized by skeletal, genital, and craniofacial abnormalities. This syndrome demonstrates both autosomal dominant and autosomal recessive inheritance. Here we describe a fetal molecular and clinical diagnosis of autosomal dominant Robinow syndrome. We report prenatal and postnatal features to expand the phenotype of Robinow syndrome.
Methods Used: An amniocentesis was performed at approximately 15-weeks gestation at an institution in Venezuela due to ultrasound findings of reported femoral shortening and a flattened facial profile. Proband only exome sequencing was performed (xGen Exome Panel 2.0) with bioinformatic filtering for genes included in the lab’s extended skeletal dysplasia panel (522 genes - Instituto de Investigación Hospital 12 de Octubre, Madrid, Spain).
Summary of Results: Prenatal genetic testing identified a heterozygous, likely pathogenic variant in DVL1 NM_004421.2 (c.1500_1507dup; p.Pro503ArgfsTer149) resulting in a frameshift and premature stop codon. Variants in DVL1 are associated with autosomal dominant Robinow syndrome. To date, parental studies have not been performed to determine if the variant was inherited or occurred de novo.
Prenatal ultrasound findings included long bones measuring in the 1st percentile for gestational age, macrocephaly with frontal bossing and short, upturned nose with a wide nasal root, triangular mouth with chin cleft, low pedal arches concerning for rocker-bottom feet, and a moderate risk for coarctation of the aorta due to a hypoplastic aortic arch and left to right ventricle discrepancy.
A postnatal physical exam by Medical Genetics noted hypertelorism, brachydactyly with broad thumbs and halluces and clinodactyly of 2nd fingers, rigid gums with a frontal frenulum, ambiguous genitalia with no apparent phallus and rugated scrotum without palatable testicles, and a sacral dimple.
Conclusions: This case describes a novel variant in DVL1 identified prenatally in a fetus with phenotypic features consistent with autosomal dominant Robinow syndrome. To our knowledge this is the first case of a prenatal molecular diagnosis of autosomal dominant Robinow syndrome and only the third case to describe prenatal ultrasound findings in the literature. Given the prenatal diagnosis of autosomal dominant Robinow syndrome, our clinical teams were able to prepare for delivery and coordinate appropriate postnatal specialty services.
Patient at 29 weeks and 4 days gestation, 22 hours of life, and 7 months old.
# 566
RGX-121: AN INVESTIGATIONAL GENE THERAPY FOR THE TREATMENT OF NEURONOPATHIC MUCOPOLYSACCHARIDOSIS TYPE II (MPS II): INTERIM ANALYSIS OF DATA FROM THE FIRST-IN-HUMAN STUDY
Blair DR1, 2, Harmatz P2, Ficicioglu C3, Giugliani R4, Rajan DS5, Hagood J6, Fiscella M6, Yang L6, Gilmor M6, Cho Y6, Mulatya C6, Phillips D6, Falabella P6, Pisani L6. 1University of California San Francisco, San Francisco, CA; 2UCSF Benioff Children’s Hospital Oakland, Oakland, CA; 3Children’s Hospital of Philadelphia, Philadelphia, PA; 4HCPA, Porto Alegre, Brazil; 5The University of Pittsburgh, Pittsburgh, PA and 6REGENXBIO Inc., Rockville, MD
Purpose of Study: Mucopolysaccharidosis Type II (MPSII) is an x-linked lysosomal storage disease caused by deficiency of iduronate-2-sulfatase (I2S) leading to accumulation of glycosaminoglycans (GAGs). Neuronopathic MPS II (nMPS II) results in irreversible neurodevelopmental decline not addressed by intravenously administered enzyme replacement therapy. RGX-121, a recombinant adeno-associated virus serotype 9 capsid containing a human iduronate-2-sulfatase expression cassette (AAV9.CB7.hIDS), administered to the central nervous system (CNS) may provide a permanent source of secreted I2S, potentially correcting neurologic and systemic disease manifestations.
Methods Used: CAMPSIITE™ is a phase I/II/III, open-label, 104-week trial enrolling boys 4 months up to 5 years of age with nMPS II (NCT03566043) who receive one image-guided RGX-121 injection to the CNS. Assessments include safety and tolerability; CSF, plasma, and urine biomarkers; neurodevelopmental scales; and imaging. Participants are encouraged to enroll in a long-term follow-up study.
Summary of Results: As of January 3, 2023, 15 participants were enrolled in the phase I/II portion of CAMPSIITE in 3 dose cohorts (1.3x1010, 6.5x1010, and 2.9x1011 genome copies/gram brain mass). RGX-121 was reported to be well-tolerated with no drug-related serious adverse events. Longest post-administration follow-up was > 3 years. CSF GAGs showed dose-dependent reductions with D2S6 (neuronopathic MPSII biomarker) approaching normal levels in cohort 3 at 48 weeks. Interim neurodevelopmental assessments demonstrated CNS activity up to 3 years after RGX-121 administration. Evidence of systemic enzyme expression and biomarker activity was present after CNS RGX-121 administration.
Conclusions: RGX-121 has the potential to provide sustained CNS clinical outcomes and additional systemic effects in MPS II patients.
# 567
SUCCESFUL TREATMENT OF MULTIFOCAL ATRIAL TACHYCARDIA WITH TRAMETINIB IN COSTELLO PATIENT
Akay G, Taliercio V, Viskochil D. University of Utah, Salt Lake City, UT
Purpose of the Study: Costello syndrome is a rare disorder caused by germline mutations of the HRAS oncogene interfering in the RAS/mitogen-activated protein kinase (MAPK) signal transduction pathway. Manifestations of Costello syndrome is coarse facial appearance, intellectual disabilities, feeding difficulties, tumor predisposition, and cardiac anomalies that can range from hypertrophic cardiomyopathy to valvular defects to arrhythmias including chaotic multifocal atrial tachycardia (MAT). We describe a newborn infant who has de novo, heterozygous, pathogenic variant in HRAS gene (c.34G>A; p. Gly12Ser), presented with chaotic multifocal atrial tachycardia unresponsive to cardioversion and multiple antiarrhythmic medication, successfully treated with MEK inhibitor (trametinib).
Clinical Information: This term newborn was noted to have dysmorphic features including tall forehead and temporal narrowing, full lips with vertical creases, micrognathia, and deep palmar and plantar creases. During her time in the neonatal intensive care unit, she was diagnosed with tracheomalacia and left bronchomalacia, leading to a tracheostomy. She experienced an episode of necrotizing enterocolitis, which necessitated surgical intervention involving a small bowel resection and a right hemicolectomy. She also had atrial ectopy that progressed to persistent MAT. Despite receiving multiple antiarrhythmic drugs, she was unable to be weaned off the amiodarone drip and unresponsive to cardioversion.
Results: Trametinib was started at a dose of 0.025mg/kg/day with ongoing improvement in patient heart rate and rhythm. She has mild controllable side effects; initial diarrhea that resolved, eczema and dry skin that is under control with atopic dermatitis treatment, and mild elevation of liver function enzymes. Importantly, echocardiograms did not detect any reduction in her ejection fraction and hypertrophic cardiomyopathy did not found.
Conclusion: Multiple atrial tachycardia has been observed in Costello syndrome occurring independent of hypertrophic cardiomyopathy phenotype and demonstrating high rates of recurrence despite medical therapy alone. There is one report available on the use of MEK inhibitors to treat to hypertrophic cardiomyopathy five Costello patient. Among these patients one additionally happened to have MAT, and after a month of treatment with Trametinib the MAT resolved. The precise mechanism through which MEK inhibitors, such as trametinib, exert their antiarrhythmic effect is not fully elucidated. However, it is hypothesized that trametinib may reduce ryanodine receptor hyperphosphorylation and improve sarcoplasmic calcium release thereby reducing atrial susceptibility to non-reentrant tachyarrhythmias. Further research is warranted to determine the optimal dosage, treatment duration, and long-term safety profile of MEK inhibitors in patients with Costello syndrome
# 568
Adeno-Associated Virus (AAV) duo vector gene therapy strategies for HSPB8- related vacuolar myopathy
Weiss L1, Shmara A1, Pal P1, Zhang h2, Farahat P3, Boock V1, Villalta A3, Xu X2, Kimonis V1, 4. 1University of California, Irvine, Irvine, CA; 2University of California, Irvine, Irvine, CA; 3University of California, Irvine, Irvine, CA and 4University of California, Irvine, Irvine, CA
Purpose of Study: The use of adeno-associated viral (AAV) vectors for gene therapy treatments of inherited neuromuscular diseases has accelerated over the past decade. Recently an AAV9 variant called AAVMYO has emerged as a promising vector to deliver gene therapy to muscle tissue. HSPB8 associated autosomal dominant rimmed vacuolar myopathy is caused mainly by frameshift (fs) mutations in the HSPB8 gene. Patients develop a distal myopathy in their thirties, with progressive generalized weakness. Muscle biopsies show fatty replacement, fibrosis, rimmed vacuoles, and proteinaceous aggregates. We have shown that the mutant HSPB8 protein causes increased aggregation likely from a dominant negative effect on the functional HSPB8 protein. We propose that using an AAVMYO duo vector containing microRNAs against HSPB8 (which targets the mutation and normal HSPB8) in addition to replacement of normal HSPB8 is a logical therapeutic approach.
Methods Used: We have generated (1) stem cells from patient skin fibroblasts and transformed them into myoblasts to for translational studies and (2) a knock-in Hspb8 mouse model of the c.515dupC fs variant seen in our patients. The mice show muscle weakness starting at 6 months of age. Muscle pathology reveals central nuclei, muscle degeneration, fatty replacement, reduced HSPB8, increased TDP-43, autophagy pathology, and amyloid fibril aggregates recapitulating the clinical phenotypes.
For proof of principle gene therapy delivery studies, we (1) designed three micro-RNA against human HSPB8 and transfected HEK293T cells to check the knockdown efficiency; (2) dosed Hspb8 c515/+ mice with myotropic AAVMYO with muscle specific promoters (CK8 and MHCK7) to select the most potent constructs for muscle delivery and therapeutic effect.
Summary of Results: In vitro results showed the three micro-RNA can efficiently knockdown HSPB8 (50-70%) in HEK 293T cells. Our next step is (1) to determine whether the most efficient HSPB8 mi-RNA vector can rescue pathological features in patient iPSC-derived myoblasts. In addition, the in vivo mouse model of Hspb8 c515 studies showed strong muscle tropism concurrent with liver de-targeting with single doses of AAVMYO at 1 x 1012 vector genomes (vg) compared with AAV9, thus indicating that these vectors are likely safe and muscle specific. We plan to share results of treating the Hspb8 c515/+ mice with the AAVMYO construct that incorporates the normal Hspb8 versus micro-RNA and a combination of both.
Conclusions: We have shown that micro-RNAs can efficiently knockdown HSPB8. Treatment in animals will reveal the best combination of microRNA and/or normal Hspb8 constructs using AAVMYO with the best promoter in ameliorating muscle weakness and pathology. Results of our studies holds promise for treatment of HSPB8 associated myopathy as well as other related dominant diseases in patients.
# 569
MEK INHIBITION IN LYMPHATIC MALFORMATIONS CAUSED BY RASA1
Selvam P, Akay G, Taliercio V, Cole S, Viskochil D. University of Utah Health, Salt Lake City, UT
Purpose of the Study: RASopathies are a group of disorders caused by pathogenic mutations in the genes involved in either activation or regulation of RAS-MAPK pathway. Among those, RASA1 is a suppressor of activated RAS wherein it encodes for a GAP1 protein that enables the conversion of active RAS to inactive form. Loss of function mutations of RASA1 gene are associated with Capillary malformation-arteriovenous malformations (CM-AVM). Less commonly, lymphatic malformations and hydrops fetalis have been reported in several families with CM-AVM. MEK inhibitors including trametinib and selumetinib have been FDA-approved in cancers harboring RAS-RAF-MAPK pathway and plexiform neurofibromas. The purpose of this presentation is to describe the use the trametinib, a MEK inhibitor in effectively treating lymphatic malformations causing chylothorax in a newborn with a likely pathogenic mutation in RASA1.
Clinical Information: Genetics team was consulted to evaluate a preterm neonate born to a mom with di/di twin pregnancy who had bilateral pleural effusions that were identified antenatally. Postnatally, she was intubated due to respiratory compromise from chylothorax requiring bilateral chest tubes. Her MRI lymphangiogram found diffuse lymphatic leaking and reflux into intercostal and perihilar regions of the lungs. Genetic testing for hydrops and congenital chylothorax which identified a heterozygous maternally inherited splice region variant in RASA1 (c.693-5 A>G). On examination, in addition to the chylothorax, the proband had two small capillary malformations on her chest and head. Her mom and her brother also have multiple capillary malformations and as do many of the mom’s siblings. Her chylothorax was not responsive to medical management including octreotide and propranolol. We obtained consent from the parents for the compassionate off-label use of trametinib. Trametinib was started at the recommended initial dose of 0.025mg/kg/day.
Results: The proband’s chylothorax improved after 3-4 weeks on trametinib with reduced chest tube output from ~300ml/day on day 1 to less than 20ml/day on day 30 of trametinib. She responded better with an increased dosing range of 0.035-0.045mg/kg/day over the recommended initial dose. She was extubated and transitioned to high-flow oxygen respiratory support. Her chest x-ray obtained on day 30 showed significantly improved aeration in both lungs without pleural effusion. She did not develop any side effects that are commonly known with trametinib.
Conclusion: MEK inhibitors such as trametinib have been well studied from a safety and efficacy standpoint in the treatment of children and adults with cancers. Over the recent years, there have been case reports on its use in treating cardiac manifestations of RASopathies. We describe the use of trametinib in an infant with chylothorax due to a RASA1 mutation. This report expands the evidence of the use of MEK inhibitors on lymphatic malformations associated with RASopathies.
Healthcare Delivery Research V - Quality Improvement
Concurrent Sessions
10:15 AM
Saturday, January 20, 2024
# 570
A STUDY OF PATIENT OUTCOMES USING A HYBRID HUMAN AND ARTIFICIAL INTELLIGENCE WORKFLOW FOR FOLLOW-UP RECOMMENDATIONS FROM RADIOLOGY
Nakashima K, Shu C, Ho E, Lopez S, Wolf R, Hoang D, Shieh S, Houshyar R. University of California, Irvine, Orange, CA
Purpose of Study: Radiologists often put follow-up recommendations within their radiology reports; however, provider-adherence to these recommendations remains suboptimal. This low adherence dilemma can, and often do, lead to inadequate patient care and subsequent medical litigation. Our institution implemented a hybrid system consisting of using a natural language processing (NLP) software, to detect missed follow-ups in conjunction with a quality and patient safety nurse to coordinate care with providers and patients. The revenue created from completion of recommended imaging outweighed the operating costs thus demonstrating the potential profitability of the hybrid system. In the current study, we examine the hybrid system’s impact on patient health outcomes of proper and timely follow-ups.
Methods Used: A total of 318 radiology examinations were assessed resulting in 197 exams that required this hybrid system. Clinical diagnoses for these radiology examinations were established by reviewing the encounter history, imaging history, and lab analysis for each patient. Lastly, patient diagnosis was categorized into excluded cancer/stable benign nodule(s), exclude vascular disease, exclude infection, exclude inflammation, de novo malignancy, and exclude pulmonary embolism.
Summary of Results: As shown in Table 1, the included cases (n = 197) were sorted, analyzed, and organized according to a carefully chosen combination of exam outcome, count, and percentage. At nearly 86% of our data, exclusion of cancer or detection of stable cancer was the most common exam outcome. Additionally, potentially life-threatening screenings such as to exclude a vascular disease (ex. dissection, etc.) or a pulmonary embolism were also present. It is also worth pointing out the incidence of a de novo malignancy as a result of the follow up scan.
Conclusions: Because of this hybrid system, providers improved patient communication and adherence to radiologist follow-up. Such follow-up imaging improves timely notification of critical diagnoses as demonstrated by the 1.5% de novo malignancy rate. Early detection and treatment ensure enhanced patient outcomes. The ability to detect early-stage malignancy improves clinical outcomes and increases treatment options, additionally affording patients time to assess treatment options and make relevant life decisions. Similarly, exclusion of diagnoses, including the nearly 86% exclusion of malignancy, affords patients information related to quality of life and significantly decreases patient anxiety. Given the significance of early detection and improved outcomes, systematic follow-up and proactive communication have the potential to positively impact overall patient satisfaction.
Limitations of this study include lack of patient feedback on the significance of follow-up communication, lack of data on provider rationale to decline radiologist follow-up imaging recommendations, and no comparative analysis of a patient population for which our follow-up system was not employed.
Exam Outcomes, Case Count, and Percentage.
Exam Outcome
Case Count
Percentage
Exclude Cancer/Stable Benign Nodule(s)
170
86%
Exclude Vascular Disease
9
4.5%
Exclude Infection
7
3.5%
Exclude Inflammation
5
2.5%
De Novo Malignancy
3
1.5%
Exclude Pulmonary Embolism
3
1.5%
Total
197
100%
# 571
Optimizing Pregnancy and Infant Outcomes in substance use Disorder and Neonatal Abstinence Syndrome – A novel curriculum to improve the care of dyads impacted by opioid use disorder in rural northern California
Kuhn-Riordon K1, Connor S3, Marcin JP1, Yang S1, Htway E1, Sanders A1, Clark S2. 1UC Davis, Sacramento, CA; 2UC Davis, Sacramento, CA and 3UC Davis, Sacramento, CA
Purpose of Study: Opioid use in pregnancy and the impact on neonates is a public health crisis. Many mothers and/or infants were transferred to our academic hospital for advanced care given history of opioid use disorder (OUD) – taking them from much needed support systems, exacerbating transportation difficulties and financial hardships for many. We describe the development and implementation of a novel curriculum titled Optimizing Pregnancy and Infant Outcomes in substance use Disorder (OPIOID) and Neonatal Abstinence Syndrome (NAS) to improve the care of pregnant and parenting women with OUD and their exposed infants living in rural Northern California.
Methods Used: Utilizing the framework of Kern’s six step curriculum design, we first identified a gap in the knowledge, skills, and confidence of rural healthcare providers to care for dyads impacted by OUD. First, we performed a needs assessment of rural healthcare providers via focused discussions to identify knowledge gaps. Second, we surveyed parenting women with OUD in a medication assisted treatment (MAT) program to understand their lived experiences with the healthcare system and identify barriers to care.
Our goals and objectives were to enhance the competency of rural healthcare providers to care for dyads impacted by OUD in the domains of prevention, treatment, and recovery.
We developed a consortium of rural health systems in northern California and utilized the ECHO (Extension for Community Healthcare Outcomes) model of care to educate a multidisciplinary group of healthcare providers – physicians, nurses, lactation consultants, and midwives. This model utilizes telehealth services to leverage regionalized expertise, share evidence-based practices to reduce healthcare disparities, use case-based learning to help master complex patients, and offer the ability to evaluate and monitor community needs and outcomes. We held monthly ECHO clinics at which time our novel curriculum was implemented utilizing case presentations from consortium sites which helped solidify care of these complex dyads, and didactic presentations in which evidence-based care was taught. Uniquely, our consortium utilized a patient advocate, a mother with history of OUD in sustained remission on MAT, to provide a patient’s perspective and openly address the stigma and bias many patients face when interacting with the healthcare system.
Summary of Results: Providers reported improved comfort when caring for dyads impacted by OUD. We saw fewer transfers to a higher level of care as rural providers demonstrated the knowledge, skills, and confidence to care for these mothers and babies in their home communities.
Additional feedback from case and didactic presentations, as well as curbside clinical questions, provided new topics for discussion to further refine our curriculum.
Conclusions: We report the development, implementation, and outcomes of the novel OPIOID and NAS curriculum with improvement in health care delivery to dyads impacted by OUD in rural northern California.
# 572
Optimizing Healthcare Delivery for Sacramento’s Underserved: A Multi-Part Study of Willow Clinic’s Patients Demographics, Primary Health Concerns, and Quality Improvement Protocols (Part I)
Shah S, Nangia D, Richards K, Malhotra K. University of California, Davis School of Medicine, Sacramento, CA
Purpose of Study: The 2022 Annual Homelessness Assessment Report (AHAR) from the U.S. Department of HUD revealed that Sacramento County has the 5th largest percent of people experiencing homelessness of 48 major U.S. cities. The 2022 Point-in-Time (PIT) Report found that 3 out 4 individuals reported forceful relocation by law enforcement within the last month – yielding loss of connection to healthcare, social work aid, and personal items such as medications.
The student-run Willow Clinic is a vital bridge to healthcare. Established in 2009 in conjunction with the Salvation Army and the County of Sacramento, the Willow Clinic functions directly out of an emergency shelter and aims to provide free, acute healthcare to the unhoused population.
This project focuses on improving care for the unhoused in Sacramento County by improving the services offered at a free student clinic, informed by an understanding current patient demographics, medical needs and social influencers of health. This data will inform subsequent studies that will focus on modifying current protocols to enhance both the efficiency and quality of care at Willow Clinic.
Methods Used: Researchers performed retrospective chart reviews for patients with visits between 8/07/2021 - 08/07/2023. Demographic information collected included gender, race/ethnicity, insurance status, and social history. Health information collected included previous medical history, current/historical medications, and current/ historical chief complaints.
Summary of Results: Chart reviews prior to data validation, showed the following preliminary findings from 300 total patients:
Demographic: A majority are between the ages of 55-64 (30%), identify as men (60%), and identify as African American (27%) or Caucasian (21%).
Insurance: A majority are on government funded insurance plans (62%) or are uninsured (20%). Regardless of insurance status, 37% had >1 visit at Willow.
Housing: A majority are unhoused (81%) of which 90% are in a shelter and 10% are living outside.
History: The top 3 diagnoses include hypertension, diabetes, and psychiatric conditions (e.g, depression, anxiety, PTSD, etc.). Additionally, 58% of patients use tobacco products.
Medications: The top 3 OTC meds were acetaminophen, ibuprofen, and lidocaine patches. The top 3 prescription meds were Lisinopril, Amlodipine, and Atorvastatin.
Chief Complaints: The top 5 chief complaints included medication refill, low mood/depression, musculoskeletal pain, dermatological issues, and concerns of general infection.
Conclusions: Through the study, we identified the most significant medical needs of the unhoused patients and learned ways of effectively using our limited resources, such as purchasing essential medications for our patients. We also found ways of improving data collection to better inform our future efforts. Future QI projects will focus on addressing these issues via improved EMR and student training, and streamlining how to best manage the most prevalent health conditions and patient needs discovered in this study.
# 573
Hand Hygiene Heroes Initiative Implementation Improves Hand Hygiene
Purpose of Study: Hand hygiene is crucial to preventing spread of infectious disease in hospital settings, with hand hygiene promotion reducing health-care associated infections. During the COVID-19 pandemic, increasing compliance of hand hygiene measures for staff of healthcare facilities became even more important to maintaining a safe environment. A systematic literature review conducted by the project team prior to the work done revealed that goal setting, reward incentives, and monitoring led to improvements in hand hygiene compliance. During the COVID-19 pandemic and following, the Hand Hygiene Heroes initiative was piloted in the Operating Room and the Pre-Anesthesia Clinic at BC Children’s Hospital. The goal of the initiative was to first identify areas for improvement among staff and patient hygiene practices, then to find a way to use motivational and positive tactics to create a campaign in support of increasing hand hygiene compliance.
Methods Used: BC Children’s Hospital’s Operating Room and Anesthetic Care Unit piloted a Hand Hygiene Heroes campaign which included hand hygiene observations, staff, patient and family engagement, hero costumes with capes and t-shirts with theme branding, and a staff hand-washing competition to strengthen and maintain awareness.
Summary of Results: Hand hygiene was captured at four moments (before and after contact with patient or patient environment, before aseptic procedure, and after contact with bodily fluids) before and after implementation of the Hand Hygiene Heroes initiative. Baseline hand hygiene compliance was 20/39 (51%) in the Anesthetic Care Unit and 42/58 (72%) in the Operating Room over a 4-week period. There was an improvement of hand hygiene moments in the Anesthetic Care Unit 20/28 (71%) and in the Operating Room 40/44 (91%). Overall hand hygiene moments improved from 61% to 83%. A chi-squared goodness-of-fit test was done to determine whether or not the results were statistically significant. The overall improvement was significant: X^2(1, N= 199) = 5.63, p<0.5. Hand Hygiene Heroes were piloted with children and families with success. To strengthen patient and family hand hygiene, a three-prong improvement approach was developed, including waiting room TV messaging, hand hygiene heroes in the unit, and family education upon discharge.
Conclusions: Through awareness, education, and engagement incentives, hand hygiene improved greatly within the operating room and anesthetic care unit settings. The success of the hand hygiene heroes pilot campaign has become a scalable model for hand hygiene improvement across BC Children’s and Women’s Hospitals. Hand Hygiene Health Promotion activities can and should engage patients, families, and all members of the surgical team. Goal setting and monitoring hand hygiene performance helps maintain hand hygiene as a measurable organizational priority. Implementing Hand Hygiene Heroes and fun patient and staff engagement incentives builds awareness and supports compliance.
# 574
Grassroots Approach to Improving COVID-19 Vaccination Rates in the Hospital Setting: A Quality Improvement Intiative
Yu N1, Punatar N2, Shaikh U2, Agrawal G2. 1University of California, Davis School of Medicine, Sacramento, CA and 2University of California, Davis, Sacramento, CA
Purpose of Study: COVID-19 continues to persist and vaccination remains a challenge to the healthcare system. Prior to this QI intervention, weekly COVID-19 case averages peaked over 170. The aims of the project were to take a Hospitalist-driven approach to reduce COVID-transmission in the community and reduce COVID-19 related hospitalizations by improving vaccination rates prior to discharge for patients admitted to the Hospital Medicine service and improving documentation of vaccination status.
Methods Used: A root cause analysis was conducted to identify key reasons underlying low vaccination rates. After review, three interventions were implemented in the Division of Hospital Medicine. Intervention 1 utilized the functionality of our electronic medical record (EMR), Epic, to create a column, “COVID-19 Vaccine Series Status” on patient lists utilized by hospitalists with their vaccine status. Intervention 2 targeted improved COVID-19 vaccine status documentation with the addition of Smart Phrases in Epic. Intervention 3 involved partnering with the Transitions of Care (TOC) Navigators who help transition patients from inpatient to outpatient care. During daily multidisciplinary huddles, TOC Navigators verbally reminded physicians which patients needed counseling on COVID-19 vaccinations prior to discharge. Primary study endpoints were pre and post implementation COVID-19 vaccination rates. Data were analyzed through run charts.
Summary of Results: From August 2021 to December 2022, the Division of Hospital Medicine cared for 6,922 adult patients. Post-implementation in February 2022, the highest percentage of vaccinations in August 2022 at 5.7% and the lowest in September 2022 at 1.9%.
Conclusions: Prior to this QI initiative to increase COVID-19 vaccination rates among hospitalized patients, inpatient vaccination rates were as low as 1.0%. Our aim to reduce COVID transmission and related hospitalizations by improving vaccination rates prior to discharge for admitted patients was successful with an increase in inpatient vaccination rates to 4.0%. While this project found success in its multi-pronged approach of leveraging the EMR system and cross-functional collaboration, it also experienced systems-level setbacks in obtaining just-in-time EMR support to match evolving COVID-19 vaccination recommendations. These hurdles indicate that improving vaccination rates may be maximized with investment in EMR capabilities to respond to urgent technical requests and system leadership-driven efforts instead of primarily unit-level approaches.
# 575
Measuring the Effectiveness of a Nutritional Rehabilitation Program for Severe Acute Pediatric Malnutrition in Rural India
Butt MF1, Ruf AM1, Arredondo D1, Patel N3, Judkins A2, Fassl B1. 1Northeast Ohio Medical School, Rootstown, OH; 2University of Utah, Salt Lake City, UT and 3Shakti Krupa Charitable Trust, Mota Fofalia, India
Purpose of Study: To determine the effectiveness of a novel nutritional rehabilitation program in a dedicated childhood malnutrition treatment center (CMTC) by calculating the proportion of children suffering from severe acute malnutrition (SAM) who achieve 10% weight gain after CMTC admission.
Methods Used: This retrospective study is part of a quality-of-care initiative of the Mota Fofalia Community Health Center in Gujarat, India. We reviewed CMTC medical records of all children admitted with SAM between 2018 and 2020 and abstracted demographics, admission/discharge weights, heights, and mid-upper-arm circumferences from medical records. Z-scores for weight-for-age, height-for-age and weight-for-height were calculated using WHO standards for malnutrition severity.
Summary of Results: Of 224 patients were admitted, 194 had complete data sets and were analyzed: 103/53% females; mean age: 20 months (range 4-58). Upon admission, 153/79% patients were severely malnourished (<-3SD); 39/20% were moderately malnourished (between -3SD and -2SD); 163/84% had an HFA z-score <-2SD; 167/87% had a MUAC of <12cm (red zone). 193 children gained weight; average weight gain 8.8%; average change in WFA z-score upon discharge +0.661 (range -0.1 to +2.8 and SD 0.4); 83/43% children achieved the target weight gain of ≥10%. The median length of stay was 13 days.
Conclusions: Further refinements to the SAM treatment protocol are needed to achieve target weight gain.
# 576
Improving Screening and Documentation of Neonatal Adverse Childhood Experiences
Sacotte K, Torr C. University of Utah, Salt Lake City, UT
Purpose of Study: Maternal adverse childhood experiences (ACEs) are associated with adverse pregnancy and neonatal outcomes. The effects of neonatal ACEs, or the adverse circumstances a baby is born into, have yet to be studied. Neonatal ACEs like parental substance use and mental illness are important social risk factors that are inconsistently screened for in the postnatal period. In an analysis at our institution, we found that only 2% of neonates admitted to the NICU are fully screened for neonatal ACEs. The aim of this study is to improve screening and documentation of all six neonatal ACEs to 50% of patients by February 2024.
Methods Used: This is an ongoing quality improvement project. An IRB approved, retrospective chart review assessing documentation of ACES was performed at the University of Utah Level III NICU on all infants admitted between January 2022 to July 2022. Neonatal and maternal charts were reviewed for six ACEs: parental intimate partner violence, maternal mental illness, paternal mental illness, parental incarceration, parental separation, and parental substance use. We used the Model for Improvement and developed a driver diagram where we identified two key drivers behind lack of documentation: use of different note templates in the electronic medical record and lack of assessment for neonatal ACEs. Meetings with stakeholders including unit leadership, nurse practitioners, and social work leadership provided insight into how to improve screening and documentation. For the first plan-do-study-act (PDSA) cycle, we mapped the process of social work documentation of a neonate’s social history. This provided insight for our second PDSA cycle on designing a documentation tool to fit within the existing workflow. Social work also identified an unseen need for a pamphlet to educate parents on the importance of ACE screening.
We identified our process measures as proportion of NICU patients screened for ACEs and use of new documentation tool. Our outcome measure was defined as number of positive ACEs screened for and documented per patient chart. We surveyed social work for unintended outcomes of this intervention including increased time spent charting and screening patients.
Summary of Results: We analyzed 203 neonates as part of the baseline data, which revealed all neonates had social work involvement. Only 2% of patients were screened for all 6 neonatal ACEs. Whether or not a father had mental illness was the most frequently missed ACE, documented in 2% (4/203) of charts. Therefore maternal and paternal mental illness were separated into different ACEs. Intimate partner violence was screened for in 30% (62/203) of the parents of NICU patients.
Conclusions: Neonatal ACEs are incompletely documented in the electronic medical record. Our intradisciplinary team is focused on process improvements. Next steps include development and implementation of a social work documentation tool into the EMR that is similar in function to existing social screens utilized in our unit.
Hematology and Oncology III
Concurrent Sessions
10:15 AM
Saturday, January 20, 2024
# 577
THE ADDED VALUE OF PROSTATE MAGNETIC RESONANCE IMAGING TO PATIENT SELECTION
Jyo E1, Yoon H2,1, Burton B2,1. 1John A. Burns School of Medicine, Honolulu, HI and 2Hawaii Permanente Medical Group, Honolulu, HI
Purpose of Study: Prostate cancer is the most common cancer in males in the United States and second most common overall. In recent years, there has been an upward trend in Magnetic Resonance Imaging (MRI) utilization for prostate cancer screening. This modality can visualize suspected lesions in the prostate, where radiologists score the likelihood of malignancy with the Prostate Imaging Reporting and Data System (PI-RADS) on a scale of 1-5, with 5 being probably malignant. If suspicious lesions are detected, biopsies are performed and given a Gleason grade to determine malignancy, where grades of 7+ are considered clinically significant cancer. The objective of this study was to measure the increase in the utilization of MRI before prostate biopsy and any effect on the distribution of PI-RADS scores and Gleason grades over a 5-year interval in an integrated health system (IHS).
Methods Used: We conducted a retrospective analysis of prostate MRI studies prior to biopsy in the calendar years of 2017 and 2022. MRI studies were excluded if 1). no prostate biopsy was done after MRI or 2). study was not performed for prostate cancer screening. Information from radiographic reports included: reading radiologist, prostate volume, Prostate Specific Antigen density (PSA/prostate volume), peak PIRADS score, and lesion location and volume if applicable. Data collected from pathology reports included: referring urologist and peak Gleason grade. All statistical tests were two-tailed with a significance level set at p<0.05. Categorical data analyses were performed using Mann-Whitney and Chi-squared tests. Continuous data analyses were performed using T-tests.
Summary of Results: The total number of prostate MRIs and the number of MRIs with an associated biopsy increased by 178% and 204% over the 5-year interval (2017-2022), respectively. There was a significant increase in the proportion of MRI studies with an associated biopsy given a PI-RADS scores of 3 or greater (91%) in 2022 compared to 2017 (73%). There was a concomitant increase in the proportion of corresponding biopsies with Gleason grades of 7 or greater in 2022 (61%) than in 2017 (27%). We found no significant variability in the distribution of PI-RADs scores among our radiologists only one of whom specializes in body MRI suggesting that the use of PIRADs helps to maintain greater uniformity in the MRI reports.
Conclusions: Increased utilization of prostate MRI has been associated with a higher proportion of biopsies with high PI-RADS scores (3 or greater) and Gleason grades (7 or greater) consistent with improved patient selection and detection of prostate cancer in this IHS.
# 578
IMPLEMENTING A NEW RESTRICTIVE HEMOGLOBIN THRESHOLD FOR RED BLOOD CELL TRANSFUSION IN PATIENTS WITH HEMATOLOGIC AND ONCOLOGIC DISORDERS
Cowley AJ1, Tsang HC2, Garcia DA3, Hasan RA2, 4, Mathias PC2, Panch S3, 2, Thomas MC2, Pagano MB2, 3. 1University of Washington School of Medicine, Seattle, WA; 2University of Washington, Seattle, WA; 3University of Washington, Seattle, WA and 4University of Washington, Seattle, WA
Purpose of Study: Current guidelines for red blood cell (RBC) transfusions recommend a hemoglobin (Hb) threshold < 7g/dL in hemodynamically stable patients. Only a small number of trials, however, evaluate transfusion thresholds in patients with hematologic-oncologic disorders. Thus, much variation is found in transfusion practices between institutions for this patient population. Current practice at the Fred Hutch Cancer Center (FHCC)/University of Washington (UW) is to transfuse to a hematocrit of > 26% (Hb 8.6g/dL). The goals of our project are to implement a new, more restrictive RBC transfusion strategy and to standardize the use of Hb values to make transfusion decisions. We anticipate that by lowering the recommended transfusion threshold we will optimize RBC utilization and reduce the frequency of transfusion related adverse events.
Methods Used: An extensive literature review identified eight clinical trials evaluating Hb thresholds for patients with hematologic-oncologic disorders. A summary of these studies was presented to the UW hematology faculty. A consensus was reached that a more restrictive Hb threshold of < 7g/dL can be safely implemented for patients with hematologic-oncologic disorders who do not have a high risk of bleeding or a history of recent stem cell transplant. To implement this new threshold, informational handouts were developed, and oral presentations were provided to all impacted clinical staff as part of a multidisciplinary educational campaign. Additionally, a new best practice alert (BPA) was designed and activated in the electronic health records (EHR) system to notify providers of the new threshold. Since implementation we have used FHCC/UW EHR to gather data and to monitor trends in RBC transfusion practices.
Summary of Results: We analyzed 4568 RBC transfusion events prior to implementation and 259 RBC transfusion events after implementation of the new restrictive threshold. In the 259 post-implementation events, we observed a marked increase in the percent of transfusions occurring at a Hb < 7g/dL and a marked decrease in the percent of transfusions occurring at a hemoglobin > 8.6g/dL (Table 1). The shift in pre-transfusion hemoglobin levels seen post implementation demonstrates a change in provider behavior regarding RBC transfusion practices. While the new guidelines clearly had the desired impact, a substantial number of transfusions (58%) happened above 7g/dL. This observation was expected given the provision for patient-specific provider discretion in transfusion decisions.
Conclusions: A restrictive transfusion threshold for patients with hematologic-oncologic disorders was successfully implemented at FHCC/UW. The educational campaign in conjunction with a clinical decision support tool proved to be an effective implementation strategy. Blood utilization will continue to be evaluated at 3-month intervals for one year, to ensure longitudinal efficacy of the project and to evaluate the impact our project has had on reducing transfusion related adverse events.
Transfusion Events and the Associated Pre-Transfusion Hemoglobin Values (Table 1)
< 7 g/dL
7-8.6 g/dL
> 8.6 g/dL
Pre-Implementation
1345 (17%)
2465 (54%)
758 (29%)
Post-Implementation
109 (42%)
142 (55%)
8 (3%)
# 579
ENGINEERING MURINE T CELLS TO DEVELOP NOVEL IMMUNOTHERAPY TREATMENTS
Schwensen J1, Greenberg P2. 1University of Washington School of Medicine, Seattle, WA and 2Fred Hutchinson Cancer Center, Seattle, WA
Purpose of Study: There are still many barriers in the effectiveness of current immunotherapies including the tumor microenvironment, failure of T cells to persist or become exhausted, and the need for T cell co-stimulation. To address these challenges, we sought to engineer a CD4 T cell that was MHC class I restricted, required no exogenous co-stimulatory signals, and could mount a coordinated CD4/CD8 T cell response to a tumor antigen. This T cell would co-express CD4 and CD8αβ, lack the Casitas B lineage lymphoma b (Cbl-b) gene, a negative regulator of CD28-dependent T cell activation, and express a TCR that recognizes the known tumor antigen mesothelin.
Methods Used: To create the modified T cell receptor (TCR), a mesothelin-specific TCR with attached furin cleavage sites, and CD8αβ were linked with 2A sequences and combined using Gibson cloning. The construct was inserted into a recombinant adeno-associated virus (rAAV) vector with a synthetic AAV6 capsid modified for murine T cells, and expressed and purified from a HEK293 cell line. CD4 T cells were isolated from a C57Bl/6J spleen with a kit (STEMCELL Technologies) and expanded using RPMI+10% FCS with recombinant IL-2, IL-7, and CD3/CD28 Dynabeads. Guide RNAs (sgRNA) were designed for the murine TCRα locus, TRAC. CD4s were cultured for 24 hours, electroporated to take up Cas9 protein, a sgRNA (from Synthego), and the rAAV construct. The cells were recovered and cultured for several days. Due to low CD4 T cell viability in preliminary efforts, Cbl-b knock-out (KO) experiments to validate the approach were tested in CD8 T cells that were cultured identically but with IL-15. The T cells were electroporated with subsequent delivery of Cas9 and sgRNAs followed by recovery, culturing, and sequencing for KO verification.
Summary of Results: Strides were made to knock in a construct with a mesothelin-specific TCR and CD8αβ into the TRAC locus with success in designing and creating the constructs. Unfortunately, the CD4 T cells were not viable 24 hours post knock-in treatment, so construct integration and functional testing couldn’t be measured. After pivoting to murine CD8 T cells, which had notably improved viability, sequencing analysis confirmed successful knock-out of Cbl-b. ICE analysis tool from Synthego indicated that a low proportion of the T cells, 26%, incorporated insertion-deletion mutations.
Conclusions: Experimental successes included creating an AAV vector that enters mouse T cells with genes for a class I restricted, tumor specific CD4/CD8 T cell. Also, Cbl-b was successfully knocked out in CD8 T cells, making advancements in creating a T cell that doesn’t require co-stimulation. In the future, optimization of culturing conditions for improved expansion and viability of CD4 T cells is necessary. It is crucial to improve Cbl-b KO efficiency using CD8s and implement the knock-out strategy in the modified CD4 T cells. Effective synthesis and proliferation of these engineered T cells will allow us to test their function in vivo against solid tumors.
# 580
The Effects of Cell-Cell Orientation in Modeling the Hallmarks of Lung Cancer In Vitro
Espinoza A1, McVicar R2, Smith E1, 2, Finlay D2, Leibel SL1. 1University of California, San Diego, La Jolla, CA and 2Sanford Burnham Prebys, La Jolla, CA
Purpose of Study: To better understand and develop treatments for lung cancer, it is important to have reliable and physiologically relevant culture models. Traditional methods of growing lung cancer cells in two-dimensional monolayers have limitations in mimicking the complex architecture and microenvironment of lung tumors in vivo, limiting their value as reliably informative disease models. In this study, we introduce a new cell culture platform called "tumoroids," which involves growing HCC827 lung cancer cells in three-dimensional configurations for more accurately predicting how cell-cell orientation and signaling affects the cancer-driving properties of lung cancer. By comparing transcriptional profiles of HCC827 cells grown as tumoroids versus the same cells grown in two-dimensional monolayers, we investigate how cell-cell orientation and signaling impact the cancer-driving properties of lung cancer.
Methods Used: We examined key features associated with cancer progression, such as epithelial mesenchymal transition, replicative ability, and induction of angiogenesis between the 2D and 3D HCC827 lung cancer cells. We utilized bulk RNA sequencing and western blotting to examine differences in gene and protein expression. Additionally, we assessed the functional characteristics of the 3D tumoroid culture system by subjecting the cells to irradiation.
Summary of Results: The gene expression profiles of the 3D vs 2D HCC827 lung cancer cell cultures differed. Tumor microenvironment pathway genes and proteins were upregulated in the HCC827 3D culture system. Epithelial Mesenchymal Transition (EMT) genes and proteins were up regulated in the HCC827 3D culture system. There were functional changes in the surfactant system and the response to irradiation differed between the 2D and 3D systems. We also found that the 3D tumoroid cultures closely resemble the characteristics of primary human lung cancer.
Conclusions: Overall, this study highlights the importance of using advanced culture models like 3D tumoroids to improve our understanding of lung cancer and facilitate the development of effective treatments.
# 581
Anticancer Activity of CB-2a, an Optimized Compound of MCT4 Inhibitor CB-2
Aviles RA, Wu Y, Wu K. Charles Drew University, Los Angeles, CA
Purpose of Study: Triple-Negative Breast Cancer (TNBC) presents a challenging prognosis due to the absence of common breast cancer receptors (ER, PR, and HER2). TNBC is characterized by its aggressive behavior, rapid growth, high recurrence risk, and increased likelihood of metastasis. Currently, specific treatments for diabetic-associated TNBC are lacking.
Methods Used: In this study, MDA-MB-231 cells were employed for in vitro investigations. A novel compound, CB-2a, demonstrated superior inhibitory effects compared to its predecessor, CB-2, with an IC50 of 2.36 μm. The lactate assay kit confirmed the enhanced inhibitory potential of CB-2a. Molecular docking analysis revealed promising interactions between CB-2a and various amino acids within the binding pocket. However, further drug optimization is necessary to overcome solubility challenges associated with CB-2a. Using the Stonewise AI drug optimization program, predicted molecules CB-2b and Ful-23 emerged as potential candidates for subsequent in vitro studies due to their theoretical water solubility.
Summary of Results: Notably, CB-2a exhibited MCT4 inhibition, resulting in intracellular accumulation and impeding the progression of cancer cells as demonstrated by wound scratch assays. Flow cytometry studies indicated the induction of both early and late apoptosis in TNBC cells, highlighting the potential of CB-2a to eliminate cancer cells. Additionally, drug optimization using Stonewise AI predicted alternative compounds, which hold promise as the basis for future therapeutic development. Molecular docking emphasized the significance of the Ser156 interaction within the MCT4 binding pocket, necessitating its inclusion in compound optimization efforts.
Conclusions: In conclusion, CB-2a exhibited favorable attributes as a novel treatment for breast cancer. The findings underscore the potential of metabolic reprogramming strategy (MRS) as a primary therapeutic avenue. Encouraging results from animal models further support its efficacy.
# 582
Education and Screening for Sickle Cell Disease in Rural Nepal: A 9-Year Review
Yu S1, Penner J1, Handra J1, Cunningham J1, Sapkota D2, Kapoor V1. 1University of British Columbia, Vancouver, BC, Canada and 2Creating Nepal, Dang, Nepal
Purpose of Study: Sickle cell disease (SCD) is an autosomal recessive hemoglobinopathy with significant morbidity and mortality. SCD prevalence is estimated at 15% in the Tharu, a population indigenous to the malaria-endemic region of Nepal. The Nepal government provides a subsidy for SCD management of those with an established diagnosis. However, most Tharu in rural Dang are ineligible as access to diagnostic testing is limited. We partnered with Creating Possibilities Nepal, a non-profit organization, to hold a screening and education camp for SCD in Dang. Here, we report our 9-year progress in improving access to SCD screening, diagnosis and education.
Methods Used: From 2015 to 2023, an annual screening camp was held at various health posts in Dang to target different communities. Patients were screened with a low-cost blood agglutination test. Patients screening positive were offered confirmatory testing by hemoglobin electrophoresis or high-performance liquid chromatography (HPLC) at the regional hospital. Through needs assessments using surveys, focus groups and expert interviews, educational modules were developed to raise SCD awareness and promote screening. Educational delivery was optimized through community consultation.
Summary of Results: Of the 5289 individuals screened, 9.5% (n=501) screened positive for sickle cell. Of those who completed diagnostic testing (n=320), 5.9% were confirmed with SCD, 80.9% with sickle cell trait, and 13.1% were false positives.
The needs assessments found the lack of transportation, financial support, and sustainable SCD education to be barriers to SCD treatment. Mother’s groups are female health volunteers often acting as the primary access point to health care in Tharu communities. They were found to be important targets for knowledge intervention and dissemination. Thus, our education initiative is currently delivered via training and educational sessions with mother’s groups, as well as forum theatres to children and families.
Conclusions: We report a high prevalence of sickle cell trait, and lower rate of SCD than previous reports. While sickle cell trait in isolation is benign, there is significant mortality when compounded with other hemoglobinopathies such as thalassemia, which were not reliably tested in our camp. To improve SCD diagnosis and treatment, stakeholders are advocating for a HPLC facility for more local, independent screening and diagnostic capacities of multiple blood disorders, to support earlier screening and intervention to Tharu communities.
Sickle cell screening and diagnostic results in Dang, Nepal. Note: Results from 2015 are combined with 2016.
# 583
ADAPTING RNA-ISH PROTOCOL TO EXAMINE CYTOLOGIC SLIDES OF LUNG ADENOCARCINOMA EFFUSIONS
Howard N2, Zhu Y1, Wang A1, Lower A1. 1Stanford University, Stanford, CA and 2College of Osteopathic Medicine of the Pacific, Western University of Health Sciences, Pomona, CA
Purpose of Study: Rapid detection of malignancy and causative genetic mutations facilitates timely determination of precise therapeutics for lung adenocarcinoma patients. RNAscope, an RNA in situ hybridization technique (ISH), allows visualization of single RNA molecules of interest in patient samples. Previously, we successfully used RNAscope to visualize epithelial cell adhesion molecule (EpCAM) and thyroid termination factor 1 (TTF-1) using formalin-fixed paraffin-embedded (FFPE) samples. In this study, we aim to adapt the RNAscope protocol to fresh cytologic direct smear slides of lung adenocarcinoma effusion samples to reveal EpCAM and TTF-1 RNA expression levels with equal or better sensitivity.
Methods Used: RNAscope assay was performed on direct smear slides of four pleural effusions, each collected within 7 days. Cells were fixed to the slides by either air-drying alone (Case 1 and 2) or air-drying followed by 15 min neutral-buffered formalin (NBF) fixation at room temperature (Case 2, 3, and 4) being subjected to dehydration treatments. The dehydrated slides were next processed following the standard RNAscope pre-treatment and amplification protocol. Case 4 was further subjected to antigen retrieval treatment before amplification steps. All patient effusion samples were obtained with IRB approval.
Summary of Results: Cells with acceptable morphology were observed on slides with NBF fixation, but not on air-dried only slides. EpCAM signals were observed on Case 2 slide, while there were no cells present on Case 3 slide. Positive control probes worked well for both Case 2 and 3. The best signal quality was observed in Case 4.
Conclusions: Formalin fixation with antigen retrieval produced the best results for RNA-ISH assay performed on fresh cytologic direct smear slides, thus establishing a feasible protocol to examine RNA expression on direct smears.
Immunology and Rheumatology II
Concurrent Sessions
10:15 AM
Saturday, January 20, 2024
# 584
DEFINING THE ROLE OF THE AUTOPHAGY RECEPTOR TEX264 IN EPIDERMAL DIFFERENTIATION
Lorenz B1, Johnson CJ1, Twiaa A2, Sarkar M3, Gudjonsson JE3, Simpson CL2, 1. 1University of Washington, Seattle, WA; 2University of Washington, Seattle, WA and 3University of Michigan, Ann Arbor, MI
Purpose of Study: To form the outer protective skin layers, keratinocytes degrade all organelles and nuclei during their final stage of maturation; this process is impaired in diseases such as psoriasis. Our research aims to test if keratinocytes use the autophagy pathway to degrade organelles. Prior data shows that as keratinocytes move from granular to cornified layers, the endoplasmic reticulum (ER) is fragmented and disposed of in lysosomes. This degradation, termed reticulophagy, can also be induced by ER stress; it is initiated by ER receptors that interact with an autophagosome protein LC3, which routes organelle remnants to lysosomes. Given its upregulation in the granular layers, we hypothesized TEX264 is sufficient and necessary for ER degradation during epidermal differentiation.
Methods Used: We used CRISPR in TERT-immortalized human epidermal keratinocytes (THEKs) to make TEX264 knockout (KO) cells. We grew keratinocytes in high calcium to induce differentiation. To generate multi-layered organotypic epidermis, keratinocytes were seeded atop collagen matrices and grown at an air-medium interface. Retrovirus was used to express GFP-labeled autophagy receptors with RFP-labeled ER or LC3 in keratinocytes. Cells were treated with tunicamycin to induce ER stress. Immunoblotting was used to quantify proteins in cell lysates, while immunofluorescence let us visualize protein localization and nuclear/organelle morphology. Live cells expressing GFP- and RFP-labeled proteins were imaged by confocal microscopy. FIJI was used to quantify nuclear morphology and ER fragments.
Summary of Results: We found ectopic TEX264-GFP induced ER fragmentation in keratinocytes but TEX264 with a mutated LC3 interacting region did not. TEX264-driven ER fragmentation was augmented by ER stress; we also noted significantly reduced nuclear size in stressed cells expressing TEX264 (p<0.0001), suggesting a potential role in nuclear elimination during cornification. To test if TEX264 is necessary for ER/nuclear breakdown, we used KO THEKs and confirmed TEX264 loss did not lead to compensation from other receptors. Preliminary analysis of differentiated KO cells revealed irregular nuclear morphology while KO organotypic epidermis showed impaired granular layer maturation. Finally, we stained TEX264 in psoriasis biopsies, which exhibit abnormal cornification. In control epidermis, TEX264 was only found in the uppermost granular layers, while it accumulated more broadly in psoriasis, suggesting defective autophagy.
Conclusions: We found TEX264 is sufficient to induce ER degradation in keratinocytes in an LC3-dependent manner. Moreover, TEX264 appears to be required for epidermal maturation, including remodeling of nuclei during cornification, and may play a role in psoriasis. Ongoing work aims to define the mechanism by which TEX264 coordinates keratinocyte ER and nuclear breakdown. In sum, our data shows autophagy plays a key role in epidermal differentiation and this pathway might be targeted to normalize cornification in psoriasis.
# 585
HIDRADENITIS SUPPURATIVA IS ASSOCIATED WITH INFLAMMATORY BOWEL DISEASE, INFLAMMATORY ARTHRITIS, AND OTHER AUTOIMMUNE DISEASES
Kassels A1, Kraus C2. 1University of California, Irvine, School of Medicine, Irvine, CA and 2University of California, Irvine, Department of Dermatology, Irvine, CA
Purpose of Study: Hidradenitis suppurativa (HS) is a chronic, inflammatory skin disease that most commonly affects the axillary, inguinal, and anogenital regions. While the exact etiology of HS is unknown, an autoimmune pathogenesis is suspected. HS has been associated with other autoimmune conditions, including inflammatory bowel disease (IBD), psoriasis, psoriatic arthritis, rheumatoid arthritis (RA), thyroid disease, systemic lupus erythematosus (SLE), morphea, type 1 diabetes mellitus (T1DM), and vitamin D deficiency. Herein, we performed a population-level retrospective study to better evaluate the association between HS and other autoimmune conditions.
Methods Used: We retrospectively generated a patient cohort from the United States (US) Collaborative Network on TriNetX, a global health research network. Our study included data between August 2003-2023 of over 101 million patients from 59 US health care organizations. International Classification of Diseases-10 (ICD-10) codes were used to identify cases and control cohorts. Atopic dermatitis (AD) and acne vulgaris were used as control groups. Patients with HS were excluded from the control cohorts. Cohorts were matched by age, sex, and race/ethnicity, resulting in a 1:1 propensity score. Autoimmune diseases associated with HS were identified using odds ratios with 95% confidence intervals.
Summary of Results: A total of 166,259 HS patients were matched with the acne control cohort, and 147,120 HS patients were matched with the AD control cohort. Patients with HS had an increased odds of the following diseases: Crohn’s, ulcerative colitis, RA, inflammatory arthritis, psoriatic arthritis, SLE, T1DM, and vitamin D deficiency, when compared to each cohort. Patients with HS had a decreased odds of celiac disease, vitiligo, Sjogren’s syndrome, alopecia areata, subacute cutaneous lupus erythematosus, and lichen planus when compared to each cohort.
Conclusions: These findings lend further support to previously reported associations of HS with autoimmune diseases, specifically inflammatory arthritis and inflammatory bowel disease. One of the strengths of this study is the use of data from numerous healthcare organizations throughout the US and the large number of HS cases identified in our cohort. These findings suggest that patients with HS may benefit from screening for autoimmune joint and gastrointestinal disease. Such awareness may lead to earlier diagnosis of concomitant conditions and allow for the selection of medical therapies with overlapping therapeutic potential.
# 586
CXCR4 MEDIATES CD8+ T CELL FUNCTION IN INFLUENZA-INFECTED LUNGS
Resta M1, Le N1, Mrass P2, Languit A3, Cannon JL2. 1University of New Mexico, Albuquerque, NM; 2University of New Mexico, Albuquerque, NM and 3University of New Mexico, Albuquerque, NM
Purpose of Study: Effector CD8+ T lymphocytes play a vital role in cell-mediated immunity against viral infection by way of recognition and direct cytotoxic killing of virally infected cells. Chemokines are known to be involved in regulation of T cell function at various stages of the cell-mediated immune response, from development to trafficking, activation, and memory. However, the role of specific chemokine receptors is not fully defined. In this study, we investigated the role of one specific chemokine receptor, CXCR4, in regulating CD8+ T cell responses to influenza infection.
Methods Used: We use a murine model influenza A virus infection to investigate the role of lung-infiltrating CD8+ T lymphocytes in clearance of virally infected cells. Using mice that have CXCR4-deficiency in T cells compared with wild type (WT) mice, we infected animals intranasally with 1x103 EID50 HKx31 influenza under anesthesia. We then measured weight loss as a predictive marker for progression and recovery, which was tracked from post-infection day 0-17. Influenza virus clearance was also assessed via sacrificing mice at day 7 of infection and measuring viral titers in collected lung tissue.
Summary of Results: Our lab’s preliminary data showed consistent expression of the CXCR4 chemokine receptor by cytotoxic T cells throughout the duration of influenza infection, suggesting a correlation between CXCR4 expression and CD8+ T cell function. Using mice that are deleted for the CXCR4 receptor in T cells, we find that CXCR4-deficiency impairs cytotoxic T cell calcium mobilization in vitro, demonstrating that CXCR4 promotes T cell receptor signaling. We further found that mice with CXCR4 deficiency in T cells leads to decreased weight loss compared to WT mice, especially at days seven and eight when CD8+ effector response is maximal. Deficiency in CXCR4 also increased weight gain during the late recovery phase at days ten to fifteen.
Conclusions: These findings emphasize the crucial role of CXCR4 in cytotoxic T cell clearance of influenza-infected lungs, though future studies are needed to better characterize exact mechanisms by which the CXCR4 receptor mediates these effects.
# 587
Incidental findings on high resolution computed tomography scanning of the lungs performed to evaluate for interstitial lung disease in rheumatoid arthritis
Parfait M1, Deane K2, Siedschlag M2, Moss L2, Feser ML2. 1Saint Joseph Hospital, Denver, CO and 2University of Colorado Anschutz Medical Campus, Aurora, CO
Purpose of Study: We performed a research study to evaluate the prevalence of interstitial lung disease (ILD) in a cohort of individuals with rheumatoid arthritis (RA) using high-resolution computed tomography (HRCT) of the lungs. HRCT may reveal findings outside of the primary goal of finding ILD (i.e. incidental findings) that may require additional follow-up and clinical care. Understanding the rate and type of incidental findings could inform future research study design into ILD in RA or other conditions. With this study, we evaluated the prevalence and type of incidental (non-ILD) findings on HRCT.
Methods Used: We evaluated 192 participants with an established diagnosis of RA who had HRCT scans performed as part of a research study to screen for ILD. Subjects were recruited consecutively for the study, with the major inclusion factor being a diagnosis of RA (by 2010 classification criteria or diagnosis by a board-certified rheumatologist), and the major exclusion factor being known ILD. The findings of HRCT studies were organized into thyroid, thoracic inlet/mediastinal, heart/vascular, pulmonary (defined as lung parenchymal, airway or pleural abnormalities), breast/axilla, abdominal and bone/soft tissue abnormalities. In addition, the radiologist-recommended follow up was documented for each participant. To date, analyses are descriptive.
Summary of Results: The characteristics of the 192 participants is presented in Table 1. The mean age of participants was 54, with ~82% being female, and ~35% had smoked cigarettes in their lifetime with ~13% being current smokers. In addition, approximately ~80% of participants were positive for the RA-related autoantibodies rheumatoid factor (RF) or anti-cyclic citrullinated peptide (anti-CCP). The prevalence and type of lung abnormalities and radiologist’s recommendation for follow-up is also presented in Table 1. The most common abnormalities were seen in the pulmonary (~81%), cardiac (~47%, including ~40% with significant coronary artery calcifications) and abdominal (~45%) regions. Overall, ~34% of participants had a radiologist recommendation to follow-up on an abnormality.
Conclusions: ILD and other forms of lung disease are important comorbidities in RA, and research efforts are underway to develop optimal screening and treatment approaches that can ultimately improve outcomes in RA. The findings presented herein indicate that incidental findings on HRCT of the chest are common in patients with RA and can require additional follow-up – even for non-pulmonary findings. This can be considered in developing research studies. Importantly, herein we report prevalence of incidental abnormalities; future analyses will include more detailed characterization of lung-specific findings, determining rates of findings that may be considered serious and the impact on these findings on clinical care, outcomes and costs.
ASSESSMENT OF RISK OF MISCARRIAGE WITH AND WITHOUT BIOLOGIC TREATMENTS FOR AUTOIMMUNE DISEASE
Nolde CM1,2, Kachikis A1, McCartney S1. 1University of Washington, Seattle, WA and 2University of Washington School of Medicine, Seattle, WA
Purpose of Study: The correlation between autoimmune disease (AID) and adverse pregnancy outcomes highlights the need for further understanding of risks and benefits of AID treatments during pregnancy. Biologic therapeutics, which are small molecules or antibodies that target the immune system, are novel treatments which may reduce the risk of pregnancy complications, however, there is little data to guide recommendations. The purpose of this study was to investigate the relationship between the adverse pregnancy outcome of miscarriage and the use of biologic therapies during pregnancy.
Methods Used: This was a retrospective study that identified patients with maternal age 18-47 who delivered at UW health system between 2003 – 2023 with pregnancy complicated by autoimmune disease. A comprehensive medical record review and chart abstraction was performed to isolate maternal clinical characteristics from (1) patients who received biologic therapies (monoclonal antibodies or small molecule inhibitors), (2) patients who were treated with traditional disease modifying antirheumatic drugs (hydroxychloroquine, tacrolimus, steroids) during pregnancy. Data analysis was performed via Chi- squared test for categorical variables via Stata software.
Summary of Results: 202 pregnancy episodes with confirmed autoimmune disease were identified which include ulcerative colitis (41), Crohn’s disease (61), Rheumatoid Arthritis (55), Psoriatic arthritis (24), Inflammatory Arthritis (24), Ankylosing Spondylitis (5), Multiple Sclerosis (4), Sjogren’s Disease (3), Still’s Disease (3), Hidradenitis (2), SLE (1) and other (5). Of these pregnancy episodes, 22 (10.8%) ended in miscarriage and 4 (1.9%) resulted in intrauterine fetal demise. Of these patients 108 (53.5%) were on biologic therapies throughout pregnancy. Biologic targets include TNF alpha (92), IL-6 (7), Integrins (5), IL-12/23 (5), CD20 (4), IL-1 (2), IL-5/IgE (2). The use of biologic therapies during pregnancy was not associated with difference in outcome of spontaneous abortion (SAB) and/or IUFD (13.8% for subjects on biologics vs 12% no biologics, p-value = 0.70) (Table 1.) There was, however, a significant decrease in SAB/IUFD outcomes between patients who discontinued biologics either prior to or during pregnancy (1, 2.4%) versus those who continued biologic therapy throughout pregnancy (14, 16.9%).
Conclusions: These data demonstrate no difference in the incidence of SAB/IUFD associated with biologic use in pregnancy. The significantly less miscarriages in patients who discontinued their biologics during pregnancy may be associated with less severe disease in those patients who were able to stop their medications.
Incidence of any SAB/IUFD across Biologics and No- Biologics groups.
Biologics (n=108, 53.5%)
No-Biologics (n=94, 46.5%)
p-value
Any SAB/IUFD
13 (13.8%)
13 (12%)
0.70
Continued Biologics (n=83, 67%)
Discontinued Biologics (n=41, 33%)
Any SAB/IUFD
14 (16.9%)
1 (2.4%)
0.02
# 589
Diagnostic approach for Generalized Lymphadenopathy
Evers E1, 2, Kulyn C2, Dulani S2, Mishra S2, D’Assumpcao C2, Fox K2. 1Ross University School of Medicine, Bridgetown, Barbados and 2Kern Medical Center, Bakersfield, CA
Introduction: Generalized lymphadenopathy poses diagnostic challenges due to diverse etiologies, including oncologic, hematologic, infectious, and autoimmune causes. Here we highlight a case of autoimmune generalized lymphadenopathy that mimicked oncological and infectious etiologies.
Methods Used: A single patient case report was conducted after IRB approval.
Case Presentation: A 34 year old male bartender from El Salvador with hypertension had a few months of night sweats, fevers and weight loss. Primary care found anemia and hematuria. Initial imaging found lymphadenopathy of iliac chain and periaortic lymph nodes, axillary lymph nodes. Follow up imaging two months later found expansion of pelvic lymph nodes engulfing the left ureter with developing of left hydronephrosis. He continued to have anemia requiring blood transfusion. Over the course of the next few months, he underwent a bone marrow biopsy and two excisional lymph node biopsies, but an oncological diagnosis could not be made, finding only benign lymphoid aggregates. He then developed a neck mass in the left submandibular triangle in the setting of Fusobacterium nucleatum anaerobic bacteremia. He was diagnosed with acute sialadenitis. Given the duration of symptoms, an exhaustive work up of infectious causes of lymphadenopathy found only prior exposure to CMV and EBV and Coxiella Phase I and Phase II 1:64 only. However, a standard autoimmune work up found positive ANA 1:320, dsDNA 1:160, low C3 and low C4, Sjogren’s SS-A antibody, Smith Antibodies. His anaerobic bacteremia and possible Q fever was treated with 14 days of metronidazole and doxycycline respectively. He was subsequently started on prednisone with symptomatic improvement.
Discussion: Generalized lymphadenopathy presents diagnostic challenges across medical disciplines. This case highlights a unique scenario of prolonged lymphadenopathy, culminating in an acute presentation initially suggestive of infection or malignancy. A collaborative, multidisciplinary approach uncovered supportive evidence for autoimmune and infectious origins, with lack of histologic malignancy confirmation.
# 590
GENE EXPRESSION OF CANDIDATE IMMUNE GENES IN BIOMPHALARIA SUDANICA IN RESPONSE TO SCHISTOSOMA MANSONI EXPOSURE
Marsonette B1, Nguyen K1, Pennance T1, Calvelo J2, Iriarte A2, Owino G3, Rawago F3, Odiere M3, Steinauer M1, Xiong Y1. 1Western University of Health Sciences, Lebanon, OR; 2Universidad de la República, Montevideo, Uruguay and 3The Kenya Medical Research Institute (KEMRI), Kisumu, Kenya
Purpose of Study: Schistosomiasis is a tropical disease caused by parasitic flatworms, leading to the death of approximately 200,000 people residing in sub-Saharan Africa, the Middle East, SE Asia, and South America annually. Schistosomes are transmitted to humans through freshwater snail vectors. With the goal of blocking transmission through snail vectors, previous research has identified genes that play a role in the immune response of the snail to schistosome infection. However, this research has focused solely on a South American vector of Schistosoma mansoni, and thus virtually nothing is known regarding African vectors of the disease, despite the majority of transmission occurring in Africa. This project aims to determine the role of three genes (toll-like receptor (TLR), granulin (GRN), and fibrinogen-related protein 2 (FREP2)) in immunity of the African vector Biomphalaria sudanica to S. mansoni, by measuring differential gene expression after schistosome exposure. These data build on our previous work, including earlier time points post-exposure.
Methods Used: Snails, 5-8 mm in diameter, were either exposed to S. mansoni larvae (n=36) or sham exposed as a control (n=36). Snails were preserved at 0.5, 3, and 24 hours post exposure (n=12 snails per time point). Total RNA extraction was completed on all snails. RNA concentration was calculated from triplicate measures and averaged for accurate cDNA generation. Gene expression was measured using RT-qPCR. Delta CT (ΔCT) values were calculated in comparison to the housekeeping gene (Actin). Nonparametric Wilcoxon tests were performed to determine significant differences (when p<0.05) in ΔCT between exposure groups and timepoints.
Summary of Results: Expression of GRN, TLR, and FREP2 did not significantly differ across any timepoints post-exposure/sham exposure, or between the experimental groups at each time point. A highly variable and potentially bimodal expression was observed in FREP2 expression in all snail groups, which is consistent with previous results.
Conclusions: In B. sudanica, the expression of GRN, TLR, and FREP, did not differ between sham exposed and schistosome exposed snails 0.5, 3, and 24 hours after manipulation/exposure. These results are consistent with our previous work in that expression of TLR in exposed snails did not change significantly during the first 24 hours. In previous work, TLR expression was significantly higher in exposed than sham exposed snails at 72 hours. Thus, if expression changes are relevant to resistance, the major expression changes happen later than 24 hours post exposure. Next steps are to further determine the role of these genes in immunity using loss of function assays. Using RNAi, we will knock down gene expression in snails, and then expose them to parasites. If the genes are involved in immunity, the expectation is that infection rates will be significantly higher than controls. The development of this RT-qPCR assay will enable these future experiments.
Neonatology General VI
Concurrent Sessions
10:15 AM
Saturday, January 20, 2024
# 591
Test Characteristics of Point-of-Care Lung Ultrasound to Predict Discontinuation of Continuous Positive Airway Pressure
Myers F1, Dasani R1, Singh Y2, Chock VY1, Bhombal S3. 1Stanford Medicine, Palo Alto, CA; 2Loma Linda University, Loma Linda, CA and 3Children’s Healthcare of Atlanta, Atlanta, GA
Purpose of Study: Continuous positive airway pressure (CPAP) is the mainstay of therapy for preterm infants with respiratory distress syndrome (RDS). However, the optimal timing and readiness criteria for weaning infants off CPAP lacks consensus. Premature CPAP discontinuation may lead to atelectasis, sepsis workups, and even intubation. Prolonged CPAP exposure from delayed discontinuation may prolong oxygen exposure, inhibit oral feeding practice, and increase the risk of nasal injuries. A score to predict successful CPAP discontinuation has the potential to standardize the practice.
The point-of-care lung ultrasound (Brat R. JAMA Pediatr 2015) has been shown to correlate with oxygenation, as well as predict surfactant need and extubation success, with lower scores indicating better aerated lungs. While literature suggests lower scores predict successful weaning, an optimal cutoff score has yet to be determined.
This research seeks to evaluate test characteristics (sensitivity, specificity, and predictive values) of the lung ultrasound score to predict CPAP discontinuation when performed within one week of a discontinuation attempt. In addition, it seeks to determine an optimal cutoff score to best predict success.
Methods Used: We analyzed the medical records of 132 patients with RDS born between 24 and 32 weeks’ gestation admitted to a Level IV neonatal intensive care unit. We collected the lung ultrasound scores of all infants who had a lung ultrasound performed within one week of a CPAP discontinuation attempt. Expert ultrasound “scorers” were blinded to the outcome of the attempts and scored all lung ultrasounds. We retrospectively assessed the outcome of “successful” CPAP discontinuation, defined as not requiring re-application of CPAP for at least 7 days following attempt. We then calculated the sensitivity, specificity, and predictive values for lung ultrasound score cutoffs between 0 and 8.
Summary of Results: 47 infants had a lung ultrasound performed within one week of a CPAP discontinuation attempt. Overall, point-of-care lung ultrasound predicts successful CPAP discontinuation. A lung ultrasound score cutoff ≤6 maximized sensitivity at 100% while a lung ultrasound score ≤3 maximized specificity at 100%. A lung ultrasound score cutoff ≤6 yields an optimal balance of sensitivity (100%) and specificity (82%) to predict CPAP discontinuation success with the highest Youden’s Index score (sensitivity + specificity -1) of 0.82. See Table 1.
Conclusions: Point-of-care lung ultrasound is a non-invasive tool that can rapidly evaluate oxygenation in preterm infants with a history of RDS. Ascertainment of the lung ultrasound score may aid in the decision to trial an infant off CPAP. More research is necessary to determine if using a lung ultrasound score cutoff of ≤6 may maximize CPAP weaning success in the clinical setting. Future work may incorporate the lung ultrasound into predictive models to provide real-time probability of CPAP discontinuation success.
LUS Score Cutoff
Sensitivity
Specificity
PPV
NPV
Youden’s Index (sens+spec-1)
0
0.19
1.00
1.00
0.25
0.19
≤ 1
0.38
1.00
1.00
0.30
0.38
≤ 2
0.54
1.00
1.00
0.37
0.54
≤ 3
0.62
1.00
1.00
0.42
0.62
≤ 4
0.73
0.96
0.96
0.47
0.69
≤ 5
0.78
0.85
0.85
0.38
0.63
≤ 6
1.00
0.82
0.82
1.00
0.82
≤ 7
1.00
0.80
0.80
1.00
0.80
≤ 8
1.00
0.80
0.80
1.00
0.80
Test characteristics associated with cutoff points revealed that a lung ultrasound score ≤3 maximized specificity (PPV 100%), while a score ≤6 maximized sensitivity (NPV 100%) and statistically optimized a balance of sensitivity and specificity (PPV 82%, NPV 100%).
# 592
EVALUATING GENERAL MOVEMENT ASSESSMENTS IN NEONATES WITH GASTROINTESTINAL ANOMALIES
Soumekh L1, Bell S1, Grogan T3, Kesavan K2, Calkins KL2. 1University of California Los Angeles, Los Angeles, CA; 2University of California Los Angeles, Los Angeles, CA and 3University of California Los Angeles, Los Angeles, CA
Purpose of Study: There is a lack of neurodevelopmental data on neonates with congenital gastrointestinal (GI) anomalies. The general movement (GM) assessment is an inexpensive, non-invasive screening tool that helps predict the risk for future motor delays. GM patterns are not well described in neonates with GI anomalies. This study’s purpose is to characterize GMs in neonates with GI anomalies and compare these results to a high-risk population, extremely low birth weight (ELBW) infants.
Methods Used: This was a retrospective, single-site cohort study that included infants born between March 2018 - December 2022. Subjects were divided into two groups: infants born with GI anomalies (GI group) and ELBW infants (ELBW group, birth weight < 1 kg). Exclusion criteria included expiration prior to discharge, chromosomal anomaly, and lack of GM data. The study’s primary outcome was the GM assessment at the writhing (36-49 weeks corrected gestational age) or fidgety stage (3-4 months corrected age).
Summary of Results: Ninety-six subjects were included (51 GI, 45 ELBW). GI anomalies included tracheoesophageal fistula (22%), gastroschisis (22%), congenital diaphragmatic hernia (16%), anorectal malformations (12 %), Hirschsprung’s disease (6%), and other (22%). The rates of abnormal GMs between the GI and ELBW groups were comparable (writhing stage: 61% vs. 59 %, p=0.89; fidgety stage: 20% vs. 36%, p=0.13). The types of abnormal scores for the writhing stage were significantly different (100% poor repertoire (PR), 0% cramped synchronous (CS) in the GI group vs. 50% PR and 50% CS in the ELBW group, p<0.001). In the GI group, infants with abnormal writhing GMs were intubated longer than those with normal writhing GMs, while those with abnormal fidgety GMs were more likely to be born lighter and premature (p<0.05 for all). Infants with GI anomalies born with fetal growth restriction were 8.5 times more likely to have abnormal fidgety GMs compared to those born appropriate for gestation (95% CI 2, 48). In contrast, ELBW infants with periventricular leukomalacia were more 13.5 times likely to have abnormal fidgety GMs compared to those without evidence of white matter injury (95% 2, 167).
Conclusions: This study demonstrated that infants born with GI anomalies and ELBW infants have a similar risk for abnormal GMs. However, their movement patterns appear to be different. In infants with congenital GI anomalies, abnormal fidgety GMs may be an early biomarker for future motor deficits.
General movements (GMs) in the writhing and fidgety stages of development in the GI group (n= 36 for writhing stage, n = 35 for fidgety stage) and ELBW group (n=37 for writhing stage, n=36 for fidgety stage). *p<0.05.
# 593
Timing and Fatigue Associated with 3:1 Compression-to-Ventilation Ratio During Neonatal Resuscitation
Giusto E1, 2, Sankaran D2, Riley E2, 3, Lesneski A4, Valdez R2, Hardie M2, Joudi H2, Tully KC4, Hammitt VL4, Vali P2, Lakshminrusimha S2. 1University of California, Sacramento, CA; 2University of California, Davis, Sacramento, CA; 3REACH Air Medical Services, Redding, CA and 4University of California, Davis, Sacramento, CA
Purpose of Study: The American Heart Associations’ Advanced Cardiovascular Life Support and Pediatric Advance Life Support recommend changing compressors every two minutes while performing cardiopulmonary resuscitation (CPR) as chest compression (CC) effectiveness decreases over time due to fatigue. The American Academy of Pediatrics’ Neonatal Resuscitation Program (NRP) offers no suggestion on how often to rotate resuscitators providing CC. NRP recommends 90 CC and 30 breaths per min during CPR.
We hypothesize that there is compressor fatigue while providing neonatal CC in a lamb model as evidenced by a decrease in rate and arterial blood pressure generated during CC over time in both term and preterm lambs.
Methods Used: Time-dated fetal lambs were intubated and instrumented. Lambs were asphyxiated by umbilical cord occlusion until asystole and delivered. Initial resuscitation commenced with positive pressure ventilation (PPV) via T-piece device at an FiO2 of 0.21 (term) or-0.30 (preterm) for 30 sec. If heart rate (HR) did not improve, CC were initiated and FiO2 was increased to 1.0. As per the NRP algorithm, a 3:1 CC-to-ventilation ratio was provided while the compressor announced out loud “One-and-Two-and-Three-and-Breath-and.” Blood pressure was measured continuously via an umbilical arterial catheter (UAC).
Summary of Results: 95 lambs were analyzed for CC rate accuracy: 75 term (~141d gestation) and 20 preterm (~125d gestation) lambs. There was no difference in CC rate between term and preterm lambs (Table). The number of CC provided in minute one was higher than minute two (Table). Out of the 5391 sets of CC provided in between PPV breaths, 37 of these sets provided 2:1 and 17 provided 4:1 CC to ventilation, amounting to a 1% error rate. All providers who performed CC were NRP-trained.
In a subset of 38 term lambs, blood pressure data from an indwelling UAC during CPR were analyzed. Systolic and pulse pressure decreased with increasing duration of CPR (Figure).
Conclusions: Neonatal resuscitation following NRP guidelines results in the desired number of CC and PPV in both term and preterm lambs. Increasing duration of CPR is associated with a small but significant decrease in compression rate and systolic pressure achieved. Similar to pediatric guidelines, NRP should consider recommending rotating CC providers every 120 sec.
Achieved Chest Compression Rate (cc/min) of CPR in term and preterm lambs.
*p-value < 0.05 via post-hoc Tukey vs. all other groups after single-factor ANOVA. Each bar is the average pulse pressure with the top of the bar as the average systolic pressure and the bottom of the bar as the average diastolic pressure. Error bars are standard deviation.
# 594
ERYTHROCYTE POLYUNSATURATED FATTY ACID CONTENT AND CHRONIC LUNG DISEASE
Gillespie T1, Igawa T2, Kim ES2, Lee LJ1, Grogan T3, Chu A2, Calkins KL2. 1David Geffen School of Medicine at UCLA, Los Angeles, CA; 2UCLA, Los Angeles, CA and 3David Geffen School of Medicine at UCLA, Los Angeles, CA
Purpose of Study: Chronic lung disease (CLD), a common complication of prematurity, is associated with decreased lung function, pulmonary hypertension, and neurodevelopmental impairment. Polyunsaturated fatty acids (PUFAs) are precursors to eicosanoids that regulate inflammation and angiogenesis. Although multiple studies have investigated PUFAs and CLD pathogenesis and prevention, results are conflicting. This single-site, prospective, observational study aimed to investigate the association of CLD severity and PUFA percentage (%) in the red blood cell membrane (RBCM).
Methods Used: Inclusion criteria included: infants born at <32 weeks gestational age (GA), <1.5 kg birth weight, and at least one PUFA RBCM measurement in the first month of life. CLD was defined as the need for supplemental oxygen at 36 weeks corrected GA. Subjects were also grouped by CLD severity [no CLD (no respiratory support), Grade 1 CLD (< 2L nasal cannula), Grade 2 CLD (≥2L NC or non-invasive positive pressure), and Grade 3 CLD (invasive mechanical ventilation)]. RBCM PUFAs were measured using gas chromatography-mass spectrometry. Generalized estimating models were used to test for group differences over time. Pairwise means with comparisons between groups were extracted from the models.
Summary of Results: Compared to the no-CLD cohort (n=29), the CLD cohort (all grades, n=44) were more premature, required more days of intubation, and were more likely to receive a RBC transfusion in the first month of life (p<0.001 for all). Similar results were observed when comparing groups by CLD severity. Despite an increase in the mean RBCM% of the essential fatty acid linoleic acid, its metabolite, arachidonic acid, was lower in the CLD cohort compared to the non-CLD cohort (p=0.004). In general, similar results were noted when investigating CLD by severity, specifically Grades 2 and 3 CLD. Contrasting results were observed for v-3 PUFAs. Despite an increase in the mean RBCM% of α-linoleic acid (p<0.001), its downstream PUFA, docosahexaenoic acid, was similar when the CLD cohort was compared to the non-CLD cohort (Table 1). All groups, except those with Grade 3 CLD, demonstrated a significant decline over time in docosahexaenoic acid (p<0.001 for all).
Conclusions: A greater RBCM% of linoleic acid, yet lower RBCM% of arachidonic acid was associated with CLD and CLD severity. Future studies elucidating how PUFAs and their downstream eicosanoids contribute to CLD are warranted.
FEASIBILITY OF USING ULTRASOUND TO IMPROVE LUMBAR PUNCTURE SUCCESS RATE IN NEONATES BY PHYSICIANS WITHOUT PRIOR ULTRASOUND EXPERIENCE
Huang J1, 2, Cayabyab R1, 2, Ramanathan R1, 2, Yeh AM1, 2. 1Los Angeles General Medical Center, Los Angeles, CA and 2Keck School of Medicine of University of Southern California, Los Angeles, CA
Purpose of Study: Lumbar puncture (LP) is one of the most common procedures performed in the neonatal intensive care unit (NICU). Despite being an essential diagnostic procedure, failure rate is reported to be as high as 30-50%. Traditionally, LP has been performed with palpation of landmarks; however, there are emerging data that describe the use of ultrasound (US) by US trained physicians in the emergency room or pediatric unit to improve success rate of LP by either marking the area of interest prior to insertion of the needle (static) or to guide LP in real time (dynamic). The success rate and rate of traumatic puncture of US guided LP performed by physicians without any prior ultrasound experience is not known. The objective of this study is to assess the feasibility of dynamic and static US guided LPs by physicians without prior US training and to determine if using US to guide LP improve success rate.
Methods Used: Neonates admitted to the NICU at Los Angeles General Medical Center starting in May 2021 who required LPs were included in the study. Prior to May 2022, all LPs were performed with landmark (blind) technique and starting in May 2022, US guided LP became routine practice and training was provided prior to the procedure. US guided LPs were initially performed with dynamic technique, but the static technique was introduced to compare success rate. Successful LP was determined when CSF was obtained. Traumatic puncture was defined as presence of red blood cells (RBC) greater than 10,000/mm3 in the CSF. Outcomes of LP performed with the three techniques, landmark, static, and dynamic, were compared.
Summary of Results: 85 neonates were included in the study. Mean birth gestation age was 37.7 ± 3.1 weeks and mean weight was 3,040 ± 819 grams at the time of LP. There was no difference in baseline neonatal characteristics between the 3 groups. There was significant improvement in the overall LP success rate and decrease in the number of attempts per LP when performed by US guided static technique. There was no significant improvement in first attempt success rate with static LPs compared to dynamic LPs; blind LPs were not compared in the analysis due to incomplete documentation. There was no difference in the traumatic rate between the LPs performed by the three techniques (Table). Reasons for failure of dynamic LPs include unfamiliarity with holding ultrasound probe while inserting LP needle and excessive patients’ movement.
Conclusions: Our study demonstrated that static US guided technique to assist LP by marking the area of interest prior to insertion of LP needle is feasible in physicians without prior ultrasound training with improved success rate and decrease in the number of attempts performed. However, dynamic US guided LP may be more difficult in physicians with no prior US experience compared to static US guided LP. Continued training in US and development of sedation protocol may improve future success rate.
Neonatal Characteristics and Lumbar Puncture Outcomes By Technique.
Data reported as median (interquartile range) † Due to incomplete documentation, first attempt success rates of blind LPs were not calculated and compared in the analysis. Excluding repeated LPs, 12 dynamic LPs and 19 static LPs were included in calculation of first attempt success rate. ‡ Due to incomplete documentation, only 28 blind LPs were included in the calculation of attempts per LP.
# 596
PERINATAL CAFFEINE IMPROVES SYSTEMIC INFLAMMATION IN AN OVINE MODEL OF NEONATAL HYPOXIC-ISCHEMIC ENCEPHALOPATHY
Mike J1, White Y1, Vento C1, Ha J1, Manzoor H1, Goudy B2, Lakshminrusimha S2, Fineman J1, Ferriero DM1, Iranmahboub A1, Maltepe E1. 1UCSF, San Francisco, CA and 2UC Davis, Davis, CA
Purpose of Study: Neonatal hypoxic-ischemic encephalopathy (HIE) places a notable socioeconomic impact within low- and middle-income countries (LMICs), home to nearly 96% of the afflicted infants. The purpose of this study is to explore the viability of perinatal caffeine administration as a novel therapeutic approach for neonatal hypoxic-ischemic encephalopathy HIE. Traditional medical approaches employed in high-income countries, like therapeutic hypothermia, frequently exhibit limited efficacy in lLMICs because substantial injury often occurs well before birth, primarily due to subacute ischemia. At present, LMICs face a deficit of alternative therapies directed towards addressing the underlying causes of neonatal HIE. This research investigates the effects on systemic inflammation after administering caffeine during the perinatal period in near-term lambs after experiencing global ischemic injury. The objective is to advance early intervention strategies for both prenatal and postnatal treatment of HIE.
Methods Used: Twenty-one lambs receiving caffeine and twenty-one receiving a placebo, spanning 141-143 days of gestation and representing both sexes, were exposed to severe global hypoxia-ischemia using an acute umbilical cord occlusion (UCO) model. Pregnant ewes were randomly assigned to receive either 1gm intravenous caffeine citrate or a placebo immediately before injury, with their lambs subsequently receiving 20 mg/kg caffeine citrate following resuscitation (high dose, HD) and 10 mg/kg/day for two days (low-dose, LD). A comprehensive assessment of outcome measures was conducted over a six-day period.
Summary of Results: Caffeine intake had a noticeable impact on serum cytokine profile. The levels of pro-inflammatory IP-10 on day 6 after the UCO were significantly reduced in response to caffeine intake. While no significant changes were observed in peripheral blood cell subgroups, the inflammatory indices SIRI (systemic inflammatory response index, SIRI=ANC*Mono/ALC) and SII (systemic immune-inflammation index, SII=ANC*PLT/ALC) were elevated in caffeine treated lambs 8h after the UCO (SII) and on day 1 (SIRI).
Conclusions: Caffeine exhibits an immunomodulatory effect after UCO via reduced inflammatory cytokine production. We speculate that higher SIRI and SII at early timepoints after UCO in the treatment group may represent a boosted immune response necessary for debris clearance. Further studies are needed to confirm the beneficial effects of caffeine on neurological outcomes in neonates who suffered HIE.
# 597
SELF-REGULATING PHYSIOLOGIC RESPONSE AND INTENSITY IN NAVIGATING TIME-SENSITIVE SITUATIONS (SPRINTS)
Halamek L. Stanford Medicine, Stanford, CA
Purpose of Study: Neonatal resuscitation is a high-stress, time-pressured task that requires intense focus and decision-making under pressure. This study employed methods of performance enhancement utilized in other high-risk industries and competitive athletics to healthcare professionals responsible for resuscitating neonates at the time of birth.
Methods Used:
10 healthcare professionals tasked with neonatal resuscitation completed a 2-phase protocol: phase A of 10 neonatal resuscitation simulations, a training module addressing stress-regulation, and phase B of 10 simulation scenarios (>1 week later). The first 5 simulations increased in time-sensitivity and the next 5 simulations increased in level of audio distraction. The subject wore a heart rate monitor (Polar chest strap), measuring heart rate and heart rate variability (HRV), a measure of sympathetic and parasympathetic response through analyzing variation in the beat-to-beat interval. Stress-response regulation was also measured subjectively by the NASA Task Load Index, State Trait Anxiety Inventory, and Confidence in Managing Challenging Situations Scale. Performance was analyzed using post-hoc scoring of video footage.
The training module consisted of excerpts from literature about maximizing performance and highlighted focused relaxation breathing and mental imagery.
At phase B, subjects were led through a relaxed breathing exercise prior to each simulation. Heart rate, HRV, and the subjective stress surveys were collected as in phase A.
Summary of Results: Analysis of performance differences between phase A and phase B (post-training) is ongoing (completed by October), but preliminary results have shown trends in performance improvements. Through the first 3 subjects completing both phases, the HRV has increased (indicates better recovery) 13.8% on average, the sympathetic nervous system (SNS) index has decreased 38.1% on average, and the stress index has decreased 8.4% on average. The SNS index was computed with Kubios HRV software, utilizing three parameters: 1) mean heart rate; higher heart rate is associated to higher sympathetic cardiac activation, 2) Baevsky’s stress index (SI), with high values of SI indicating high sympathetic cardiac activation, 3) sympathovagal balance, reflecting the balance of the sympathetic and parasympathetic response. These preliminary improvements in HRV score, SNS index, and SI were observed by pairing each subject’s trial from phase A to the corresponding trial in phase B, thus subjects acting as their own control. Future analysis will evaluate if there are statistically significant improvements in performance and will analyze differences in the subjective stress measures and performance scores.
Conclusions: Preliminary analysis shows promise of the SPRINTS training module to teach healthcare professionals to effectively regulate their physiological response to stress. These results could represent a shift in how healthcare professionals involved in neonatal resuscitation train to improve their abilities.
Neonatology Pulmonary III
Concurrent Sessions
10:15 AM
Saturday, January 20, 2024
# 598
Virtual/Telesimulation is Non-Inferior to In-Person Helping Babies Breathe Training in Jimma, Ethiopia
Clary M4, Berhane M5, Liang J2, Daniels K3, Lee H6, Eshetu B5, Mediratta R1. 1Stanford University School of Medicine, Stanford, CA; 2Stanford University, Stanford, CA; 3Stanford University School of Medicine, Stanford, CA; 4Stanford School of Medicine, Stanford, CA; 5Jimma University, Jimma, Ethiopia and 6University of California San Diego, San Diego, CA
Purpose of Study: Helping Babies Breathe (HBB) teaches healthcare providers newborn resuscitation knowledge and skills. However, instructors and participants face challenges traveling to in-person HBB trainings. This study aimed to assess whether virtual/telesimulation HBB training is non-inferior to in-person training in a low-resource setting.
Methods Used: In this randomized, controlled, non-inferiority trial, we recruited clinical medical students in Ethiopia who had not received HBB training. Participants were randomized to virtual/telesimulation (intervention) or in-person (control) training. Intervention training was taught via Zoom using a PowerPoint presentation and instructional videos. Control training consisted of HBB didactics. Each arm received identical content delivered by the same four trainers in one day. HBB multiple-choice knowledge test was assessed before, immediately after, and two months after the training. Objective Structured Clinical Examinations (OSCE; OSCE A and OSCE B), bag and mask checklist, and resuscitation performance on mannequins were assessed immediately after and two months after the training. The primary outcome was the OSCE B scores after two months. The non-inferiority margin was 13%, which has been used in studies for resuscitation. Group differences were assessed by intention-to-treat analysis using linear regression. A non-inferiority p-value <0.05 suggests non-inferiority.
Summary of Results: 262 medical students were enrolled. The intervention (n=123) was non-inferior to the control group (n=139) for OSCE B scores two months after training, with passing rates of 60% and 62.8%, respectively. Immediately (t1), and at two months (t2), after the training, non-inferiority was demonstrated for OSCE A (t1= p<0.001, t2= p<0.001), OSCE B (t1=p<0.001, t2 p=0.006), bag and mask checklist (t1 p=0.03, t2 p=0.005), and knowledge ( t1, p<0.001 t2, p<0.001). The performance of the intervention group was non-inferior to the control group for the heart rate and ventilation pressure on mannequins immediately after and 2 months after the training (both p<0.001).
Conclusions: Telesimulation is non-inferior to in-person HBB training about knowledge and resuscitation skills among medical students. Virtual training was effective and offers potential solutions for addressing logistical challenges in educating healthcare providers in low-resource settings about newborn resuscitation.
Participants Demographics and Passing Rates.
Control/in-person
Treatment/virtual
Overall
(N=139)
(N=123)
(N=262)
Age (years)
24.3 (1.67)
24.4 (1.85)
24.4 (1.75)
Sex
Male
72 (51.8%)
61 (49.6%)
133 (50.8%)
Female
67 (48.2%)
62 (50.4%)
129 (49.2%)
Years of Medicine
Year 4
42 (30.2%)
39 (31.7%)
81 (30.9%)
Year 5
59 (42.4%)
56 (45.5%)
115 (43.9%)
Year 6
38 (27.3%)
28 (22.8%)
66 (25.2%)
Previous Neonatal Resuscitation Training
6 (4.3%)
6 (4.9%)
12 (4.6%)
Passing OSCE-A Score (t1)
74 (53.2%)
52 (42.6%)
126 (48.3%)
Passing OSCE-A Score (t2)
48 (45.7%)
48 (51.1%)
96 (48.2%)
Passing OSCE-B Score (t1)
102 (73.4%)
67 (54.9%)
169 (64.8%)
Passing OSCE-B Score (t2)
63 (60.0%)
59 (62.8%)
122 (61.3%)
Knowledge Multiple Choice Questionnaire (t0)
81 (58.7%)
75 (61.0%)
156 (59.8%)
Knowledge Multiple Choice Questionnaire (t1)
138 (99.3%)
119 (97.5%)
257 (98.5%)
Knowledge Multiple Choice Questionnaire (t2)
103 (97.2%)
92 (97.9%)
195 (97.5%)
Bag and mask (t1)
82 (59.0%)
36 (29.5%)
118 (45.2%)
Bag and mask (t2)
36 (34.3%)
20 (21.3%)
56 (28.1%)
Summary of participant demographics and passing rates.
Non-inferiority tests for OSCE B (Panel A), OSCE A (Panel B). t1 refers to immediately after training, and t2 refers to two months after training. The non- inferiority margin was at 13%.
# 599
Comparison of Oxygenation Index (OI), Oxygen Saturation Index (OSI), and PaO2/FiO2 (PF) in Neonates with Congenital Diaphragmatic Hernia
Ellsworth T, Yang M, Yoder B. University of Utah, Salt Lake City, UT
Purpose of Study: To determine the correlation between oxygenation index (OI = Paw*FiO2/PaO2), oxygen saturation index (OSI=Paw*FiO2/SpO2), and PaO2/FiO2 ratio (PF) in neonates born with congenital diaphragmatic hernia (CDH) within the first 24 hours of life.
Methods Used: Retrospective analysis of CDH neonates with CDH managed at University of Utah and Primary Children’s NICUs from 1/1998 to 8/2023. Demographic data reported as median (IQR) or n (%). We compared all paired measured values for OI, OSI, and PF obtained from birth through 24 hours age using linear and logarithmic regression curve analyses. We also compared the pre- and post-epoch effect of a 2016 CDH care guideline update on the correlation of these oxygenation measures.
Summary of Results: Between 1998 to 8/2023, we managed 424 neonates with CDH. We excluded 30 for delayed post-natal diagnosis of CDH after 24 hours (final n=394). We compared 793 paired values for OI to PF or OSI, as seen in the Figure. Analysis by epoch demonstrated significantly lower ECMO (10% vs 33%) but higher survival (85% vs 70%) for the post-2016 epoch. Additionally, FiO2, Paw, paO2, OI and OSI were significantly lower in the post-2016 epoch. Despite these differences, the regression analyses for OI to PF and to OSI were similar between epochs. Between epoch comparison showed similar values for OI, PF and OSI values and the use of ECMO. Among 77 ECMO infants in the study, OSI was > 12 in 76 (99%) while OI was > 30 in 69 (90%).
Conclusions: As expected, OI and PF were highly correlated. In the absence of an arterial paO2 value, OSI has good correlation to OI. Although OI and OSI were generally lower in the post-2016 epoch, there were no differences in the values associated with ECMO therapy. In our current population, an OSI value > 10 is indicative of severe respiratory failure.
Group Statistics.
Pre-2016 N
Pre-2016 Mean
Pre-2016 SD
Post-2016 N
Post-2016 Mean
Post-2016 SD
p-value
FiO2
494
76.8
26.6
299
53.6
25.4
<0.001
Paw
494
12.9
4.0
299
10.9
2.1
<0.001
pO2
494
107.3
77.6
299
70.0
39.3
<0.001
pre-SpO2
492
95.4
7.6
299
94.0
8.9
0.134
OI
494
17.7
20.0
299
12.4
12.8
<0.001
PF
494
165.6
118.3
299
162.0
102.2
<0.001
OSI
492
11.3
7.1
299
6.9
5.3
<0.001
# 600
Updated cutoff value of early postnatal prediction model for survival without ECMO in congenital diaphragmatic hernia
Torsitano C, Yang M, Yost CC, Yoder B. University of Utah, Salt Lake City, UT
Purpose of Study: Several postnatal models for predicting survival of infants with congenital diaphragmatic hernia (CDH) have been developed, but no postnatal tool is applied consistently across institutions. An accurate, easy to use, bedside tool can aid in prognosis and decision making for these infants, such as earlier transfer for ECMO. Prior data from our center showed the PF-PCO2 equation [(PaO2/FiO2) - PaCO2] was most predictive for survival without ECMO with a cutoff value of >-60 compared to three other tools. CDH outcomes have improved dramatically since changes to the CDH clinical care guidelines at our sites in 2016. Thus, we hypothesized that the PF-PCO2 equation will be less accurate in predicting survival without ECMO now than before 2016, and that a new cutoff value may be needed. We compared PF-PCO2 scores among CDH patients born after 2016 to other predictive models including the Wilford Hall Santa Rosa Prediction Formula (WHSRpf), the CDH Study Group Probability of Survival Equation (CDHSG-PS), lowest PCO2 in 1st 24 hours, highest oxygen index (OI) in 1st 48 hours, and best OI in 1st 24 hours. The last three of these were published recently and shown to also correlate with survival in CDH by other centers, which is why they were chosen.
Methods Used: In this retrospective analysis we performed area under the curve (AUC) analysis for a primary outcome of survival without ECMO for each of the different tools for 320 infants with CDH from January 1st, 2003 to June 2nd, 2023. Analysis was done for 2 cohorts, one for patients managed prior to 2016 and one for those managed from 2016 forward. Predictive scores were calculated to determine cutoff for PF-PCO2 score on infants after 2016.
Summary of Results: The accuracy of the PF-PCO2 score to predict survival without ECMO decreased for the > 2016 cohort with AUC 0.83 (95% CI 0.71-0.94) compared to 0.94 (95% CI 0.90-0.98) before 2016. The best prediction tools for > 2016 were best OI in 1st 24 hours with AUC 0.86 (95% CI 0.76-0.97) and highest OI in 1st 48 hours with AUC 0.86 (95% CI 0.73-0.99). Both OI methods performed better prior to 2016 as well. An updated cutoff value of >-80 for the PF-PCO2 score was most predictive of survival without ECMO with a positive predictive value (PPV) of 88% and a negative predictive value (NPV) of 100%. Optimum cutoff value for best OI in 24 hours was <25 (PPV 91%, NPV 67%), and for highest OI in 48 hours was <45 (PPV 91%, NPV 86%).
Conclusions: PF-PCO2 and highest OI in the first 48 hours of life were good predictive models for CDH survival without ECMO, but the accuracy is decreased for patients managed > 2016. This may be because of improved survival without ECMO among more compromised CDH patients in the cohort. Best OI was highly correlated with our primary outcome, but the optimum cutoff has lower predictive value than PF-PCO2 and highest OI.
# 601
Evaluation of Effective Pressure Delivery by Nasal High-Frequency Jet Ventilation in a Neonatal Lung Model Using NIV+ Software
Kibe R1,2, Ramanathan R1,2, Biniwale M1,2. 1LAGMC, Los Angeles, CA and 2University of Southern California, Los Angeles, CA
Purpose of Study: Non-invasive ventilation strategies are vital in the neonatal population to mitigate adverse effects of invasive ventilation. Nasal High-Frequency Jet Ventilation (nHFJV) is a relatively newer and understudied modality. A major limiting factor with non-invasive ventilation is the variability of pressures being delivered, which has been made easier with the availability of the NIV+ software. We aimed to measure effective pressures delivered at the patient interface on a 3D printed nasal model using a combination of non-invasive positive pressure ventilation (NIPPV on the conventional ventilator) and nHFJV delivered via Ram cannula
Methods Used: We used different-sized neonatal 3D-printed nasal adapters connected to test lungs, able to accommodate different-sized Ram cannulas. Life Pulse HFJV (Bunnell Inc.,Salt Lake City, UT, USA) was used to provide nHFJV, while Puritan Bennett™ 980 ventilator(Medtronic, Minneapolis, MN, USA) with NIV+ Software provided conventional ventilation. RAM nasal cannula (Neotech, Valencia, CA, USA) was attached to the LifePort endotracheal tube adapter (Bunnell Inc.) to deliver jet breaths noninvasively. Each size of the Ram cannula was tested for different combinations of jet rate(240-360) and inspiratory time(IT, 0.02 – 0.03 sec) with basal NIPPV settings(Peak inspiratory pressure(PIP)25/30/35, Positive end-expiratory pressure(PEEP)6/8/10,rate 40,IT 0.5 sec). Statistical analysis was performed using IBM SPSS Statistics for Windows
Summary of Results: 432 data points were analyzed across all sizes of the cannula. PIP measured at the interface was significantly lower than set PIP on the conventional ventilator (mean difference 4.09, SD 1.8, P < 0.01). In comparing the pressures delivered through the inspiratory cycle (PiEnd) and PIP at the interface, there was excellent correlation of 0.90. Set PEEP was higher than measured PEEP at the interface by 0.4 cmH2O(SD 0.58, P < 0.01). The correlation between set PEEP and measured PEEP was 0.94. The PEEP shown on the Jet ventilator read higher than measured PEEP (mean difference 3.83, SD 1.07, P <0.01),with good correlation of 0.82.
Conclusions: HFJV when used non-invasively with Ram cannula despite loss of some pressures, produces consistent pressures across all cannula sizes when compared to set pressures. This is the first bench study to measure the delivered pressures on nHFJV and could provide valuable insight into clinical management strategies
Perinatal and Maternal Risk Factors for Prolonged Respiratory Support in Moderately Low Birth Weight Babies Admitted to the NICU
Sosa J, Barton L, Ramanathan R, Biniwale M. Los Angeles General Medical Center/University of Southern California, Los Angeles, CA
Purpose of Study: Respiratory distress is one of the most common reasons for admission to the neonatal intensive care unit, and low birth weight infants are at significant risk of requiring respiratory support at birth. However, little is known about factors affecting the respiratory support needs of moderately low birth weight (LBW) infants (1500-2500 g). The objective of this study was to characterize and identify perinatal and maternal factors that result in longer duration of respiratory support in moderately LBW infants admitted to the NICU.
Methods Used: Infants with birth weight 1500-2500 grams admitted to the NICU after birth with respiratory support between 6/1/2015-12/31/2022 were included in the study. A retrospective review from the LAGMC/USC NICU database and medical records was performed to collect the length and type of respiratory support, diagnoses, prenatal interventions, maternal risk factors, and resuscitation details. Subjects were grouped between those that required respiratory support for <3 days and those that required respiratory support for > 3 days.
Summary of Results: A total of 373 LBW infants met the inclusion criteria. Infants requiring increased duration of respiratory support had lower mean gestational age (GA) and mean birth weight. Significant factors associated with longer respiratory support needs included the diagnosis of respiratory distress syndrome (RDS), apnea of prematurity (AOP) and confirmed or clinical sepsis, need for surfactant treatment, antenatal steroids treatment, and restarting respiratory support after getting weaned to room air. On the other hand, infants diagnosed with transient tachypnea of newborn (TTN) required shorter length of respiratory support. The length of stay of infants (LOS) requiring >3 days of respiratory support was longer than those that required less duration of respiratory support (Table 1). Logistic regression analysis adjusted for all significant factors including GA and BW revealed diagnosis of RDS (OR 0.09. 95% CI 0.04-0.19) and need for surfactant therapy (OR 0.07, 95%CI 0.01-0.52) were the most significant predictors of the need for longer duration of respiratory support.
Conclusions: Moderately LBW infants are at greater risk of needing longer duration of respiratory support if the patient had a diagnosis of RDS and required surfactant therapy, though other factors related to prematurity (antenatal steroid treatment, AOP, lower BW and GA) and infectious causes of respiratory distress also contribute to prolonged respiratory support needs. Efforts should continue to be made to maintain the pregnancy as long as safely possible to prevent prematurity and its complications.
Risk factors and diagnosis impacting with duration of respiratory support.
Associated Factor
Subjects w/ >3 days of respiratory support
N= 261
Subjects w/N= 112
p value
BW (grams) mean + SE
2008 + 17
2108 + 125
<0.001
GA (weeks) mean + SE
33 + 0.123
34 + 0.174
<0.001
LOS (days) mean + SE
26.21 + 1.81
12.34 + 10.8
<0.001
Surfactant therapy, n (%)
64 (24.5)
1 (0.9)
<0.001
antenatal steroids, n (%)
100 (38.3)
31 (27.7)
<0.001
restarted respiratory support, n(%)
33 (12.6)
1 (0.9)
<0.001
Diagnosis
RDS, n (%)
163 (62.5)
10 (8.9)
<0.001
TTN, n (%)
70 (26.8)
87 (77.7)
<0.001
AOP, n (%)
80 (30.7)
12 (10.7)
<0.001
Sepsis/Infection, n (%)
19 (7.3)
2 (1.8)
0.035
# 603
MINIMALLY INVASIVE SURFACTANT THERAPY (MIST) TO REDUCE BRONCHOPULMONARY DYSPLASIA (BPD): A QUALITY IMPROVEMENT PROJECT
Razdan S, Gu H, Bain L, Davis A. Stanford University School of Medicine, Palo Alto, CA
Purpose of Study: In randomized controlled trials, less invasive surfactant administration (LISA) has been associated with a reduction in the need for intubation as well as reduction in BPD in premature infants. In smaller studies, surfactant administration through a laryngeal supraglottic airway (SALSA) has been shown to be feasible and reduce the need for intubation. We seek to implement both MIST methods in a Level IV neonatal intensive care unit (NICU). Our SMART aim is to reduce the need for intubation within the first 72 hours of life in extremely preterm infants by 20% by December 2023.
Methods Used: This project will take place in our level IV NICU with approximately 95 inborn very low birthweight infants annually. Our project implementation methods included sharing best practices, physician and nurse practitioner education through didactics and simulation sessions, and nursing and respiratory therapy education. The target population will be inborn infants between 26-32 weeks estimated gestational age admitted to the Level IV NICU (see figure 1). Infants will be excluded if the indication for intubation is apnea or craniofacial anomalies. The rate of intubation in the first 72 hours will be compared between a historical epoch from January 2022-August 2023 and a similar period after implementation. Rates of death, BPD, and severe IVH will be compared as secondary outcomes. Balancing measures will include adverse events during the MIST procedure, including the need for emergent intubation. MIST will be implemented in our unit in October 2023. Chi-square tests will be performed for categorical variables and t-tests will be performed for continuous variables.
Summary of Results: Historical intubation rates in our Level IV NICU by gestational age are shown in Table 1. We did not include infants less than 25 weeks estimated gestational age as they were highly unlikely to weigh more than 750 grams. For inborn infants at least 25 weeks’ gestation from 2017-2022, our unit’s historic BPD rate is 22%, and severe IVH is 5%. We will report these measures in our post-intervention group.
Conclusions: Our Level IV NICU is implementing two methods of MIST in order to decrease intubation rates in our extremely preterm infants. This study will collect data on feasibility and success of MIST in achieving our aim.
Historic very low birth weight intubation rates from 2019-2021, N=236.
Estimated gestational age
Intubation by 72 hours (%)
Number of infants
25 weeks
76%
17
26 weeks
58%
19
27 weeks
48%
31
28 weeks
29%
24
29 weeks
45%
31
30 weeks
31%
39
31 weeks
15%
47
Data represents intubation rates following implementation of bubble continuous positive airway pressure (CPAP).
Algorithm after Decision to Administer Surfactant.
# 604
Utilization of Non-Invasive Neurally Adjusted Ventilation Assist (NI-NAVA) to Improve Short Term Respiratory Outcomes in Extremely Preterm Infants: A Quality Improvement Project
Wu J, Harasimyw L, Chamberlain K, Griffin T, Shelton A, Rogers EE, Kramer K. UCSF, San Francisco, CA
Purpose of Study: Extremely preterm (<28 weeks’ gestation) and extremely low birth weight (ELBW, < 1000 grams) infants are at a higher risk of having poor respiratory outcomes such as prolonged mechanical ventilation, extubation failure, prolonged hospitalizations, and chronic lung disease. Non-invasive neurally adjusted ventilation assist (NI-NAVA) is a relatively new mode of ventilation that utilizes electrical activity of the diaphragm to provide respiratory support. There is evidence that consistent use can decrease extubation failure, which may improve short-term respiratory outcomes. The aim of this quality improvement (QI) project was to decrease the rate of extubation failure in extremely preterm infants by 20% within one year.
Methods Used: This QI initiative was performed at a level IV Intensive Care Nursery at UCSF- Mission Bay. A multi-disciplinary QI team was formed and met frequently during the planning stages. Using Lean process improvement methodology, an A3 and key driver diagram was created to develop targeted interventions to improve respiratory outcomes for extremely preterm infants. Interventions included increasing extubation of mechanically ventilated ELBW infants to NI-NAVA, creation of a NI-NAVA guideline to standardize use, and widespread dissemination of NI-NAVA education. The pre-intervention period was from Jan 2022-Jun 2022 (15 infants) and the post-intervention period was from Jul 2022-Apr 2023 (16 infants). The primary outcomes were the rate of extubation failure and days of mechanical ventilation within first 4 weeks. Rate of extubation to NI-NAVA was the process measure. Data was analyzed on run charts.
Summary of Results: Our intervention increased extubation to NI-NAVA from 62% to 92% of all extubation episodes in ELBW infants. Extubation failure decreased from 33% to 22% during the same time period, suprassing our goal of a 20% reduction. Average number of mechanically ventilated days in the first 4 weeks of life was stable at 6 days.
Conclusions: Using core QI methodology, we successfully implemented the use of NI-NAVA upon extubation for extremely preterm infants, which was associated with a reduction in extubation failure.
Neuroscience III
Concurrent Sessions
10:15 AM
Saturday, January 20, 2024
# 605
INTRANASAL DELIVERY OF INCRETIN RECEPTOR AGONISTS IN THE APP/PS1 MOUSE MODEL OF ALZHEIMER’S DISEASE
Abdulhameed N1, 2, Babin A1, 2, Hansen K1, 2, Banks W1, 2, Talbot K1, 2, Rhea E1, 2. 1University of Washington School of Medicine, Seattle, WA and 2Veterans Affairs Puget Sound Health Care System, Seattle, WA
Purpose of Study: Alzheimer’s disease (AD) is a neurodegenerative disease with a lack of approved FDA therapeutics effective in impeding disease progression. Targeting non-conventional casual grounds of Alzheimer’s such as brain insulin resistance is a progressively recognized drug target. Incretin receptor agonists (IRAs) are antidiabetics that reduce insulin resistance and AD pathology and improve cognition in animal models. We administered IRAs via intranasal (INL) routes to deliver directly to the brain, in the adult male and female mouse model of AD, APP/PS1 mice, to investigate the distribution pattern in the brain which will aid in our understanding about how these novel therapeutics show promise in slowing disease progression in AD.
Methods Used: We investigated the distribution patterns of five radiolabeled IRAs following INL administration in adult CD-1 mice: three single IRAs (exenatide, semaglutide, and dulaglutide) and two dual IRAs (DA4-JC and DA5-CH). We selected the two best IRAs that demonstrated the greatest uptake, dulaglutide and DA4-JC, to follow-up in the APP/PS1 mice. Radioactive levels were measured in serum (%Inj/ml) and multiple brain regions (%Inj/g): cortex, striatum, hypothalamus, hippocampus, thalamus, parietal cortex, occipital cortex, cerebellum, midbrain, and pons. To evaluate if each IRA had a saturable component in brain uptake, we investigated whether excess non-radioactive IRA (+1 µg) altered distribution. We confirmed the stability of radioactively labeled IRAs in whole brain, olfactory bulb, and serum via acid precipitation.
Summary of Results: Of the five IRAs investigated in CD-1 mice, dulaglutide displayed peak brain uptake rates by 60 min in the whole brain for males and by 30 min in females. DA4-JC distribution differed significantly by sex with females predominantly having greater uptake than males (p < 0.01). Dulaglutide displayed consistently decreased distribution across all times in APP/PS1 males and females, except at 30 min in females. DA4-JC distribution also had reduced distributions in APP/PS1 mice, with minor exceptions in the hippocampus and whole brain with males and olfactory bulb and serum with females. There was little evidence for saturable transport in the frontal cortex/striatum for exenatide and hypothalamus for semaglutide. Semaglutide and DA5-CH were the most stable IRAs, with DA4-JC exhibiting the least stability.
Conclusions: Brain distribution patterns of dulaglutide and DA4-JC demonstrate considerable uptake indicating that these are noteworthy IRAs to consider in alleviating brain insulin resistance in Alzheimer’s pathogenesis following INL delivery. Diminished IRA distribution was generally exhibited in AD suggesting an impaired mechanism of transport. Significant differences in the distribution of some IRAs between sexes prompt further investigation into the possible intricacies between males vs females, insulin signaling mechanisms, and IRA dosing. Our work provides new insight into alternative treatment routes to target AD pathogenesis.
# 606
Disparities in Care for Paraneoplastic Neurologic Syndromes
Prince AR, Graber J. University of Washington, Seattle, WA
Purpose of Study: While the health disparities in cancer and neurological conditions are well-documented, disparities in the care of paraneoplastic neurologic syndromes (PNS) have not yet been examined. Given the significant morbidity and mortality associated with these conditions and the necessity of prompt diagnosis and treatment in improving outcomes, identification of these disparities has clear clinical implications. First, we hypothesized that differences in times to diagnosis (TTD), treatment (TTT), cancer screening (TTS), and overall survival (OS) exist between different PNS diagnoses. Second, we hypothesized that demographic and socioeconomic factors, such as sex, race, income, insurance type, and smoking status, are associated with delays in TTD, TTT, and TTS and decreased OS.
Methods Used: This retrospective cohort study utilized data from January 1, 2003 to July 31, 2023 from a convenience sample of 111 adults diagnosed with PNS, including paraneoplastic cerebellar syndrome, limbic encephalitis, Lambert Eaton myasthenic syndrome (LEMS), sensory neuronopathy, and anti-NMDA-receptor encephalitis. Descriptive characteristics were compared using χ2 tests. Effects of PNS diagnosis and demographic and socioeconomic factors on TTD, TTT, and TTS were assessed using either the Mann Whitney test or the Kruskal-Wallis test and Bonferroni correction method. Differences in OS were analyzed using the Kaplan-Meier method and log-rank test. Analyses were conducted and reported separately by PNS diagnosis and by overall population.
Summary of Results: Comparisons between PNS diagnoses found that TTD was significantly shorter for anti-NMDA-R encephalitis (28 days) than for sensory neuronopathy (195 days), P = .01 (Table 1). When data was analyzed by diagnosis, TTD was significantly longer for never smokers with LEMS (351.5 days) than current smokers with LEMS (38 days), P = .02. When data was analyzed for the overall population, male patients had lower OS rates (65.6%) than female patients (91.9%), P <.001, and current smokers had lower OS rates (58.3%) than both former (74.2%) and never smokers (95.9%), P <.001.
Conclusions: These findings demonstrate that disparities exist in the care of PNS, much as they do in oncologic and neurologic care. A major finding was the difference in TTD between PNS, especially anti-NMDA-R encephalitis (Table 1). Perhaps this is due to the newfound notoriety of anti-NMDA-R encephalitis following its media debut, but either way, it provides an example of the efficiency with which PNS can be diagnosed and treated. Moreover, it emphasizes the need for improved recognition and awareness of these syndromes. An unexpected finding was the prolonged TTD for never smokers with LEMS. It is understandable that LEMS might be overlooked in non-smoking patients, since it is strongly associated with SCLC. However, this finding highlights the need to untangle the association between LEMS and smoking status, so that LEMS does not continue to be overlooked as a possibility for non-smoking patients.
Median Intervals and Overall Survival by Diagnosis.
Median interval, (days)
Paraneoplastic Cerebellar Syndrome
Limbic Encephalitis
LEMS
Sensory Neuronopathy
Anti-NMDA-R Encephalitis
P value
TTD
72
64
118●
195*
28●*
.008
TTT
28
23
30.5
40●
7●
.06
TTS
10.5
1*
21.5*
14.5
3
.07
OS, (mos.)
31.0
28.2
36.4
29.9
28.7
.77
Abbreviations: TTD, time to diagnosis; TTT, time to treatment; TTS, time to cancer screening; OS, overall survival; LEMS, Lambert Eaton myasthenic syndrome; anti-NMDA-R, anti-N-methyl-d-aspartate receptor; mos., months Asterisks indicate statistically significant pairwise analysis differences. Filled circles indicate pairwise analysis differences that did not reach significance, but had a trend.
# 607
A Cross-Sectional NHANES Analysis of the Association between Migraine and Diabetes Mellitus
Salib S1, Kim J2, Ezzati S2, Abouzari M3. 1California Northstate University, College of Medicine, Elk Grove, CA; 2School of Medicine, Duke University, Durham, NC and 3University of California, Irvine, Irvine, CA
Purpose of Study: This cross-sectional study aimed to investigate the relationship between migraine and diabetes mellitus (DM) using public database of the National Health and Nutrition Examination Survey (NHANES) from 1999 to 2004. The study sought to establish correlations between migraine incidence and various health parameters, contributing to a better understanding of the intricate interplay between migraine and DM.
Methods Used: Through a retrospective analysis of NHANES data, encompassing 15,320 participants with an average age of 50.4±19.5 years, the presence of migraine and DM-related variables were collected. Statistical analyses, including two-tailed Student’s t-tests and chi-squared tests, were employed to compare means and incidences of categorical variables. Additionally, multivariate binary logistic regression was conducted to explore independent associations between migraine incidence and variables of interest. Data analysis was carried out using R version 4.3.0, with significance levels set at p< 0.05.
Summary of Results: Among the participants, 3,045 (19.9%) reported experiencing migraine headaches. Notable correlations were observed between migraine and certain demographic characteristics: individuals with migraine were more likely to be younger (p< 0.001), female (p< 0.001), and exhibit a higher body mass index (p< 0.001). Multivariate logistic regression analysis further unveiled independent association between a higher glycohemoglobin level and having migraine (p= 0.007, Odds Ratio (OR) = 1.12, 95% Confidence Interval (CI) = 1.03-1.21). Additionally, the occurrence of migraine was closely linked to being female (p< 0.001, OR = 2.42, 95% CI = 2.00-2.93) and having a lower family income (p< 0.001, OR = 0.85, 95% CI = 0.81-0.91).
Conclusions: This study’s findings indicate an association between elevated glycohemoglobin levels and a heightened incidence of migraine. Furthermore, the results underscore the increased likelihood of migraine headaches among females and individuals with lower family incomes. However, comprehensive understanding of the relationship between DM and migraine incidence necessitates further exploration, employing larger sample sizes and more extensive research.
# 608
ASSESSING NEUROBEHAVIOR IN MICE OVEREXPRESSING TRANSFORMING GROWTH FACTOR BETA: A MODEL OF CEREBRAL SMALL VESSEL DISEASE
Chung H, Adler-Wachter M, Weinstein J. University of Washington School of Medicine, Seattle, WA
Purpose of Study: Current knowledge about the effects of Cerebral Small Vessel Disease (CSVD) on animal models have not been extensively studied. The disease is progressive and involves microvasculature supplying white matter and deep structures in the brain. Clinically, it is associated with stroke, depression, and dementia.
Work by Edith Hamel demonstrated an age-dependent model of CSVD in mice overexpressing TGF-β (TGFoe). We tested specifically spatial memory of these mice. The aim of my study is to establish baseline neurobehavioral characteristics of WT mice at 6 months of age to compare to TGFoe mice. This will serve as a foundation for comparison in future studies of the mice as they age while being fed a high cholesterol diet (HCD) which may exacerbate the CSVD pathogenesis. My hypothesis is that TGFoe mice fed on standard diet will develop cognitive deficits at baseline due to pathophysiology based on genotypic differences.
Methods Used: We used 16 WT mice (8 males, 8 females) and 9 TGFoe mice (6 males, 3 females) at 6 months. Subjects more than two standard deviations away from the mean were excluded from the data.
The Novel Placement Recognition Test (NPRT) assesses spatial memory involving a 30 minute habituation to an empty arena, 24 hours before testing. The test consists of a 10 minute object familiarization phase where two objects are placed into the arena, followed by a 1 hour memory interval, and finally 10 minutes of novel placement testing, where one object 1 is moved. EthoVision software tracks animal movement and time spent in defined arena zones.
The T maze test measures an animal’s working memory. On each of 14 trials, animals must choose to enter either the right or left arm of the maze. The animal’s innate exploratory drive encourages them to alternate which arms they choose, requiring memory of which arm it has visited previously. After entering an arm, the opposing side is blocked. The trial ends when the animal re-enters the starting arm. They are contained for a 5 second interval before starting the next trial.
Summary of Results: In NPRT, both strains, on average, spent a relative 62% more time in the quadrant of the arena with the novelly placed object in the testing phase compared to the familiarization phase (p=0.0006). There was no significant difference between strains in the interaction time with the novelly placed object. TGFoe mice spent 76% longer making a decision as compared to WT mice (p=0.02). In the T-maze, TGFoe mice alternated 14% less frequently than WT mice, but this was not statistically significant. (p=0.373).
Conclusions: I found that there were only slight differences in the spatial and working memory of these two strains of mice. Although TGFoe mice have a predisposition towards developing cognitive deficits, their progressive disease phenotype may not be advanced enough at 6 months of age to show significant impairment. Future studies should explore whether HCD longitudinally influences the pathology.
# 609
ASSESSING NEURONAL EDEMA IN MILD TRAUMATIC BRAIN INJURIES
Carlson V1, Morton R2. 1University of New Mexico, Albuquerque, NM and 2University of New Mexico, Albuquerque, NM
Purpose of Study: Every year, around 42 million people suffer from traumatic brain injuries (TBIs) that range from minor concussion-like injuries to severe penetrating brain injuries. In TBIs, cerebral edema poses a serious threat due to the increase in intracranial pressure and can be life-threatening if not treated. While global cerebral edema is rare in mild TBIs (mTBIs), individual neuronal edema is not well understood. Neuronal edema can lead to neurological impairment by altering cell function.
Methods Used: To study this further, we conducted a study on 17 Thy1-GFP transgenic mice (Jax# 007788) who had sparsely labeled glutamatergic neurons throughout the brain. We induced a closed skull mTBI and allowed the animals to recover before sacrificing them at 24- and 48-hours. We collected coronal sections and counter-stained them with DAPI. We imaged four to six sections spanning the rostral-caudal axis using a Zeiss axioscan slide scanner. From the whole section scans, we collected regions of interest (ROIs) across cortical layers 4/5 and 2/3 and used customized ImageJ macros to measure individual pyramidal soma area in layer 4/5 and dendrite length in layer 2/3. We measured the cell soma area by averaging multiple images in a 20 mm z-stack, thresholded the image, created masks, identified cell soma, and measured cell soma area.
Summary of Results: Our findings indicated that there was no significant difference in cell size soma in the mTBI and sham animals at 24 hours. However, the cell soma area was statistically smaller in mTBI animals than in sham animals at 48 hours.
Conclusions: We are currently investigating the underlying mechanism of this reduced cell soma area. Our imageJ macro for measuring dendritic beading averaged the images of a 20 mm z-stack, identified tubes, skeletonized the tubes, and then measured the skeletonized length. We predicted smaller dendritic segments if dendritic beading was present. However, our generalized linear mixed model of tens of thousands of dendritic segments did not show any significant difference between the dendrite length of sham or mTBI animals. Our results suggest that neuronal edema is not a major contributor to the pathophysiology of mTBIs in mice. Future research will focus on the presence of diffuse axonal damage from our mTBI model.
Publication Only
# 610
Unfettered Growth of a Pyogenic-like Granuloma Squamous Cell Carcinoma
Abraham J, Aranguri C, Mann B, Clarke M. Kern Medical, Bakersfield, CA
Introduction: Cutaneous squamous cell carcinoma (cSCC) accounts for 20% of all skin cancers, making it the second most common skin cancer after basal cell carcinoma. While the majority of cSCC lesions can be successfully treated with surgical resection or radiation, larger lesions are associated with poor prognosis, including greater risk of local invasion or metastasis. Prompt recognition and diagnosis is therefore a priority. Pyogenic granuloma is a benign, vascular tumor that can grow rapidly and, in some cases, can resemble malignant lesions. We report a case of a rapidly growing, fungating lesion of the knee in a 66-year-old male with an ambiguous presentation.
Case Presentation: 66-year-old male with a history of hypertension who presents for evaluation of a left knee mass. The mass was initially noted 3 months prior, with the patient believing it was a “callus.” The initially flat lesion progressively enlarged into a fungating mass. The patient presented for evaluation due to difficulty walking with his left lower extremity.
Upon evaluation, a 6.8 x 5.7 x 3.5 cm fungating, pedunculated and ulcerative soft tissue mass over the left patella with serosanguineous and bloody fluid drainage was noted. Furthermore, patient presented tachycardic, with a mild leukocytosis, and elevated inflammatory markers concerning for infection. Initial imaging with X-ray of the left lower extremity demonstrated a large radiodensity involving the infrapatellar soft tissues. CT of the lower extremity with contrast demonstrated a large exophytic mass originating from the skin, with no intra-articular extension, and internal enhancing components concerning for neoplasm. Ultrasound-guided core biopsy of the mass was performed and sent to pathology. Due to insurance reasons, patient was unable to await biopsy results and was discharged to home with family with instructions to await telephone communication for pathology results.
Pathology of the fungating, skin lesion of the left patellar revealed poorly differentiated squamous cell carcinoma. Patient was contacted over the phone, with discussion of results from the biopsy. Patient was also advised to make an appointment with our oncologist outpatient for prompt initiation of treatment. Patient was seen in oncology clinic outpatient awaiting initiation of treatment.
Conclusion: Squamous-cell carcinoma is the second most common cancer among whites. cSCC are associated with a substantial risk of metastasis compared to most basal-cell carcinomas. These lesions may have varied presentations as the case discussed above. Hence, timing to identifying the pathology of the lesion and initiating treatment is important.
# 611
May-Thurner Like Syndrome: A Case Report
Abraham J, Al-Yousfi N, Mishra S. kern medical, Bakersfield, CA
Introduction: May-Thurner Syndrome is a condition in which venous flow is obstructed due to extrinsic arterial or anatomical pressure in the iliocaval veins. It commonly presents in women in their 3rd or fourth decade of life. This proposed case report presents an unusual case of a 50-year-old male patient with left external iliac vein thrombosis secondary to compression of the left common iliac vein due to a saccular aneurysm on the left common iliac artery.
Case Presentation: A 50-year-old male with past medical history of left leg deep vein thrombosis presented to clinic with left lower extremity pain and swelling of two days. He reported a history of deep vein thrombosis a year ago and a cardiopulmonary embolic event earlier in the year, which led to hospitalization. Patient was also on a month course of anticoagulation at around the time of the embolic event. Lower extremity venous doppler ultrasound showed complete left lower extremity deep vein thrombosis. He was started on Heparin and underwent chest X-ray, computed tomography angiogram of left lower extremity, computed tomography chest/abdomen/pelvis. Scans showed extensive bilateral pulmonary emboli and intraluminal thrombus in the left external iliac vein extending downward to the common femoral vein and the proximal superficial femoral vein. The subsequent thrombectomy and angioplasty by interventional radiology reported revascularization of left femoral-popliteal, external, and common iliac veins with catheter directed mechanical thrombectomy. In addition, moderate pulmonary arterial hypertension secondary to acute chronic pulmonary thromboembolism was treated by right pulmonary artery catheter directed mechanical thrombectomy. Peri-procedure, there was also reported persistent extraluminal compression of the left common iliac vein, secondary to adjacent common iliac artery aneurysm, a May-Thurner syndrome variant. The patient underwent left common iliac artery covered stent graft deployment with angioplasty assistance for treatment of left common iliac artery aneurysm with contained dissection. As the patient became stable, he was discharged on Apixaban.
Discussion: May-Thurner syndrome can lead to multiple thromboembolic events in various organs. It may be hard to diagnose due to the rarity of it. It is important to note that there are different variants of the syndrome which may not be considered as a differential diagnosis upon initial impressions. The mild presentation of this syndrome can be managed with conservative treatments such as compression stockings. However, moderate to severe presentations may need anticoagulation therapies even in the absence of thromboembolic events. The goal of this paper is to help with earlier diagnosis of May-Thurner syndrome and its variants which could improve the long-term effects and prognosis of the disease.
# 612
LETROZOLE-INDUCED PARONYCHIA
Alcantara C1, Kesler A1, Vu A1, Pham D2. 1Western University of Health Sciences, Pomona, CA and 2Sand Dermatology, Chino Hills, CA
Case Report: Paronychia is a common inflammatory condition of the nail folds, typically caused by bacterial infections and wet work. Chronic paronychia, which results from contact with irritants and water can lead to Candida colonization, loss of the cuticle, and fibrosis of the surrounding nail folds. The disruption of the protective architecture surrounding the nail plates can lead to further infection and onychodystrophy. Although it is known that patients undergoing cancer treatment experience dermatologic conditions, such as hair loss, very few cases of the effects of chemotherapy on the nails have been described. Other than anecdotal reports and some documented cases from a phase IV clinical trial, paronychia as a side effect of cancer treatment has not been reported. Here, we describe a case of paronychia following the initiation of breast cancer maintenance therapy with letrozole, an aromatase inhibitor. Within one year, the patient’s nails exhibited erythematous and edematous periungual areas with missing cuticles, despite infrequent contact with water, no initiation of new medications or supplements, and a lack of history of diabetes. Treatment with daily topical ciclopirox 0.77% gel and a weekly fluconazole 200 mg tablet was initiated, with no improvement after one month. Treatment was ultimately changed to a fluconazole 200 mg tablet two times weekly, topical betamethasone dipropionate 0.05% cream application twice daily, and topical ketoconazole 2% cream application twice daily. After six months, there was improvement of chronic paronychia. The primary hypothesis regarding the mechanism of cancer treatment-induced paronychia is vasodilation, which may increase blood flow, resulting in greater vascular permeability. With increased vascular permeability, leakage can be sustained in chronic inflammation, leading to edema and reduced vascular perfusion, thereby increasing the risk of infection.
# 613
Isolated Scapular Fracture: a diagnostic challenge
Inga Jaco E, Bazmi A. Kern Medical, Bakersfield, CA
Case Report: Before introduction of PSA test, men were more likely to present with widespread prostate cancer metastasis in the axial skeleton: skull, spine, ribs, sacrum, and coccyx.
This is a 63-year-old Hispanic male presented to IM outpatient clinic with right upper back pain and deformity of right scapula. Pain started two months prior to appointment. Patient recalled a forceful mechanical movement while placing a flag as the inciting factor. Initially he complained of right shoulder pain, he visited another ED where CT chest without contrast showed scapular lytic fracture, lung nodule and high alkaline phosphate, and normal PSA. Over time, pain and deformity over the scapula deteriorated, he suffered restrictive right shoulder motion. By the time he presented to our clinic, he reported mild knee and hip pain as well. Given presentation, there was high suspicion for malignancy. Given that PSA reminded low, there was suspicion for multiple myeloma or plasmacytoma, although all corresponding labs were noncontributory. Follow-up CT chest showed enhancing destructive soft tissue masses eroding posterior arch of left sixth and seventh rib, bilateral hilar lymphadenopathy, spreading lung densities and nodularity with no masses, and destructive mass centered in the right scapula measuring 12.4 x 9.3 x 12.3 cm, repeated PSA again was normal, AlP level was slightly above normal. Within 4 weeks, the patient’s medical status abruptly deteriorated, manifested by urinary frequency, bowel and urine incontinence, and lower extremities weakness. He was admitted to hospital with a diagnosis of acute spinal cord compression. During hospital admission, right scapular biopsy showed positive CD99, CD10, vimentin, NKX 3.1 cytokeratin 81/83 leading to diagnosis of prostate cancer. Spine MRI showed enhancement through T11-S1, pathological compression fractures at L2, L3, and enhancement in sacrum and iliac wings. Patient was started on Bicalutamide, zoledronic acid, and followed by cGy radiation fraction. Additionally, the patient suffered a left femur fracture with corresponding biopsy pointing to metastatic prostate cancer.
Prostate cancer has multiple but common arrays of presentations. With PSA development, the majority of patients diagnosed with prostate cancer present high PSA, localized prostate cancer, and a minority of patients present with distant axial pain indicating an already state of metastasis. Additionally. in the majority of cases, these patients also present with a previous history of urinary obstruction, UTIs, hematuria, as part of the lower urinary tract symptoms (LUTS). This patient’s presentation, with an isolated non-axial scapular fracture and mass, absence of LUTS, normal PSA, and no past medical history, including smoking, is an example of a multiple and rare spectrum of metastatic prostate cancer presentation that needs to be taken into consideration when considering prostate cancer diagnosis.
# 614
AN ATYPICAL PRESENTATION OF A HYPOTHYROID PATIENT WITH HYPOKALEMIA AND PARALYSIS
Woods J1, 2, Patel J1, Clarke M1, Singh S1, Chandramahanti S1. 1Kern Medical, Bakersfield, CA and 2Ross University School of Medicine, Christ Church, Barbados
Purpose of Study: Hypothyroidism is a commonly encountered endocrine disorder, characterized by symptoms such as fatigue, weight gain, constipation, and cold intolerance, among others. However, some cases present atypically, making diagnosis challenging. One such atypical manifestation is acquired periodic paralysis, a condition characterized by acute weakness and low serum potassium levels. While there is a well-defined association between thyrotoxicosis and acquired periodic paralysis, its occurrence in hypothyroidism is rarely reported. This report aims to elucidate the clinical presentation, diagnosis, and management of acquired periodic paralysis secondary to hypothyroidism.
Methods: This is a report on a rare case in a county hospital in southern California. Review for this case was conducted on the hospital’s electronic medical record. The case was approved by our hospital’s Institutional Review Board, IRB# 23110.
Summary of Results: A 61-year-old female with a past medical history of rheumatoid arthritis, neuropathic pain, and latent tuberculosis. Three weeks before her visit to our Emergency Department (ED), she saw her primary care provider with complaints of paresthesia in her hands and feet, which had slowly progressed to involve her lower extremities, arms, and hands. Laboratory evaluation in the ED revealed severe hypokalemia and hypothyroidism. Treatment with levothyroxine was initiated and the patient was subsequently discharged in stable condition with endocrine follow-up with instructions to continue levothyroxine daily.
Conclusion: This report demonstrates the importance of evaluating for hypothyroidism as a potential cause of hypokalemia. Though hypokalemia is a rare manifestation of hypothyroidism, it may be that in patients with autoimmune diseases, such as our patient, this manifestation is more common due to the development of distal renal tubular acidosis. Evaluation for hypothyroidism in patients with acquired periodic paralysis is crucial as it represents a treatable etiology.
# 615
Ureteral Diameter Ratio as a Risk Factor for Febrile Urinary Tract Infections in Children with Primary Vesicoureteral Reflux
Roh D, Dwumfour S, Papaioannou P, Farkouh A, Pearce J, Song S, Cheng K, Kuang R, Chamberlin D, Chamberlin J. Loma Linda University, Loma Linda, CA
Purpose of Study: Children with vesicoureteral reflux (VUR) are at an increased risk of urinary tract infection (UTI). Recurrent UTIs can lead to renal scarring and renal failure. The ureteral diameter ratio (UDR) measures the degree of hydroureter normalized for the child’s size and has been proposed as a risk factor for febrile UTI. Improved identification of children at risk of developing recurrent febrile UTIs can improve management decisions. The purpose of this study was to evaluate distal UDR as a risk factor for febrile UTIs in children with VUR.
Methods Used: A retrospective review of a VUR database from a single children’s hospital was performed. All patients with primary VUR from June 2007 to May 2023 were included. Patients without diagnostic voiding cystourethrogram (VCUG) images available for review were excluded. UDR was calculated by measuring the largest distal ureteral diameter within the false pelvis and dividing by the distance between the bottom of the L1 vertebral body and the top of the L3 vertebral body. In children with bilateral vesicoureteral reflux, the larger UDR was used. The primary outcome analyzed was febrile UTIs. Statistical analysis was conducted with logistic regression and Spearman’s rho correlation, with statistical significance at p < 0.05.
Summary of Results: Of the 257 children in the VUR database, 210 met inclusion criteria, with 115 female (54.8%) and 95 male (45.2%) patients. The mean UDR was 0.2, with a range from 0 to 1.19. Forty-two children (20%) experienced a febrile UTI during follow-up. UDR was predictive of febrile UTI with an odds ratio of 4.7 (95% CI 1.25-17.7, p = 0.022). On the other hand, VUR grade was not significantly associated with febrile UTI with an odds ratio of 1.26 (95% CI 0.99-1.59, p = 0.052). Despite the difference in predictability of febrile UTI, there was a strong correlation between UDR and VUR grade with a Spearman’s rho correlation of 0.91 (p < 0.001).
Conclusions: The ureteral diameter ratio was more predictive of febrile urinary tract infection than VUR grade. UDR may be a useful clinical tool in the risk stratification and treatment of children with VUR.
# 616
RUQ Rectus Sheath Hematoma: A Diagnostic Dilemma
Sharma R1, 2, Aranguri C1, 2, Yanni T1, 2, Petersen G1, 2. 1Kern Medical Center, Bakersfield, CA and 2David Geffen School of Medicine, Bakersfield, CA
Case Report: Rectus sheath hematoma (RSH) is characterized by the accumulation of blood within the fibrous covering of the abdominal muscles, known as the rectus sheath. Typically caused by trauma, strenuous activities including vigorous cough or anticoagulation medication use, this condition results in localized pain, swelling and a palpable mass in the abdominal area most commonly imfraumblically. Herein described is a unique case of abdominal RSH presented in right upper abdominal quadrant (RUQ).
A 49-year-old latinix male with history of HTN presented to ED with progressively worsening, acute onset RUQ abdominal pain x1 day. The night prior to patient’s presentation he awoke with pressure-like, non-radiating RUQ abdominal pain. His pain initially was 5/10 in intensity which progressively worsened to 10/10 at presentation. Coughing and movement aggravated the pain and he denied any alleviating factors. He denied any trauma or associating symptoms including nausea, vomiting, constipation or diarrhea. Patient stated this was his first episode of such pain. He experienced an episode of dry, violent cough with epigastric pain 2 weeks prior to his presentation. Patient was initially hypertensive with BP 197/134, regular rate and afebrile. Initial workup was unremarkable with good renal function, no elevation of LFTs. Abdominal ultrasound was initially performed which revealed hepatic steatosis without other significant findings. Following which, abdominal CT w/contrast was done which demonstrated dilated vascular structures with an enlarged upper right rectus abdominal muscle suggesting active bleeding. Abdominal MRI w/+w/o contrast was then obtained revealing moderate hematoma in the right upper rectus abdominis muscle without definite enhancing underlying mass. As per CTA abdomen, a moderate right rectus sheath hematoma about 11x4.5x10cm was found. Patient’s h&h levels remained stable >11.0g/dL throughout hospitalization. Patient was discharged home in stable condition.
Amongst the differentials of RUQ pain including cholecystitis, peptic ulcer diseases, pancreatitis, RSH should be considered. RSH is a rarely seen pathology and often misdiagnosed as acute abdomen that may lead to unnecessary laparotomies. CT is chosen for definitive diagnosis. 80% of patients may be managed with no invasive intervention, including rest, ice, compression, and analgesia
# 617
THE SILENT INTRUDER UNVEILED: THE ELUSIVE DIAGNOSIS OF TUBERCULOSIS MENINGITIS
Thiagarajan S, Reyes MP. Sierra View Medical Center, Porterville, CA
Purpose of Study: This case report aims to present a challenging diagnostic journey encountered in a 79-year-old Tagalog-speaking female with tuberculosis meningitis. This study aims to shed light on the difficulties faced during the diagnostic process.
Methods Used: The diagnostic approach involved a comprehensive evaluation of the patient’s medical history, physical examination, and laboratory investigations. Due to the nature of her initial symptoms, a high index of suspicion for meningitis was maintained throughout the diagnostic process. Cerebrospinal fluid (CSF) analysis, including microbiological and molecular testing, was performed alongside radiographic imaging (MRI brain, CT head) and other relevant investigations, such as TB Quantiferon.
Summary of Results: The patient arrived exhibiting signs of an altered mental state and fever, which suggested a potential case of meningitis. On arrival, the patient had a blood pressure of 99/58 and was tachycardic with a heart rate of 115, a respiratory rate of 24, and a fever of 102.8 F. The patient was saturating 97% on room air. Labs were significant for potassium of 3.1, bicarbonate of 18, lactic acid 4.5, and a Pro-Cal of 1.38. Chest x-ray showed moderate vascular congestion. CT of the abdomen pelvis showed significant thickening of the rectal wall. A sepsis alert was initiated, and the patient was given 30 cc/kg of fluids and started on IV Zosyn in the emergency department. The patient was admitted to telemetry for severe sepsis, and at that time, it was secondary to an unknown etiology. Blood cultures and urine cultures were taken, and urinalysis was negative. Considering the patient’s age and wide range of possible diagnoses, a comprehensive exam, labs, lumbar picture with CSF analysis, and imaging were conducted. The Cerebrospinal Fluid (CSF) analysis unveiled a high protein level, lymphocytic pleocytosis, and reduced glucose levels. These factors align with Tuberculosis (TB) meningitis symptoms, a conclusion further supported by the patient’s positive TB Quantiferon result. All other CSF studies, including HSV, cocci, and West Nile, were negative. The patient had no respiratory symptoms to suggest pulmonary TB, and her chest X-ray was negative for TB. The patient was started on RIPE therapy, steroids, and B6. After beginning treatment, the patient’s symptoms began to improve.
Conclusion: Diagnosing tuberculosis meningitis can be particularly challenging, especially in elderly patients with nonspecific clinical manifestations and a wide range of differentials to consider. This case report highlights the importance of maintaining a high index of suspicion in the face of diagnostic uncertainty. It emphasizes the significance of thorough evaluation, including examination, CSF analysis, and molecular testing, in confirming the diagnosis. Timely identification of tuberculosis meningitis is crucial for initiating appropriate treatment promptly, thus improving patient outcomes.