
Abstract

1. Relaxin is a Novel Biomarker for Thyroid Carcinogenesis
Anupam Kotwal1, 2, Nicholas Whiteman1, Benjamin Swanson1, Ana Yuil-Valdes1, Whitney Goldner1, Robert Bennett2, 1
1 University of Nebraska Medical Center, Omaha, NE, United States. 2 VA Nebraska-Western Iowa Health Care System, Omaha, NE, United States.
Purpose of Study: Differentiated thyroid cancer (DTC) is the most common endocrine malignancy, with disease progression associated with an unfavorable prognosis. Prognosticating patients with DTC is a challenge, and novel therapies lack curative ability. Until we identify additional biomarkers for thyroid carcinogenesis, our ability to provide high-quality personalized care to DTC patients will be limited. Relaxin (RLN2) can regulate macrophage polarization and reduce fibrous extracellular matrix, creating a tumor microenvironment favorable for cancer cells. We aimed to identify the role of RLN2 and its receptor RXFP1 in thyroid carcinogenesis via investigation of human thyroid tissue and cell lines.
Methods Used: We performed fluorescent immunohistochemistry for RLN2, CD68 (total macrophages), CD163 (M2 macrophages), and DAPI (nucleus) on thyroid tissue microarrays (TMA) with two cores per specimen. Control slides (using isotype-matched immunoglobulin) were used to calculate background staining. Mean pixels/area in each channel were compared between tissue from n=181 non-distant metastatic DTC tumors (cases) and n=185 benign thyroid tissue (controls) via t-test assuming unequal variances. P<0.05 was used for statistical significance. We also used qPCR to determine the expression of RLN2, RLN1, and RXFP1 in human thyroid cancer cell lines including papillary (BCPAP, KTC-1, TPC-1), follicular (FTC133) and anaplastic (C643, Hth7) or a benign thyroid cell line (N-Thy).
Summary of Results: Amongst the 181 DTC cases, 91.2% were papillary; 65.2% were localized to the thyroid, and only 11% were considered high-risk for recurrence. The cohort was followed for a mean of 5 years from thyroidectomy, during which 87.8% did not demonstrate any evidence of disease. Cases demonstrated higher expression compared to controls for RLN2 (difference of means 36.9; 95% CI 30.2 - 43.7; p<0.0001), CD68 (differences of means 9.7; 95% CI of 5.5 - 13.8; p<0.0001) and CD163 (differences of means 23.9; 95% CI 14.4 - 33.3; p<0.0001). In the cell lines, RLN2 was elevated in FTC133, KTC-1, and N-Thy cells, reduced in C643, and undetectable in TPC-1 cells. Only the C643 cells had increased RLN1 expression. Expression of RXFP1 was elevated in BCPAP cells, reduced in Hth7 and N-Thy cells, and undetectable in TPC-1.
Conclusions: In this overall fair-prognosis cohort of DTC, higher expression of RLN2 correlating with macrophage infiltration, specifically the pro-tumoral M2 subtype, demonstrates its role as a biomarker for thyroid carcinogenesis. The undetectable expression of RLN2 and RXFP1 in TPC-1 cells which are also negative for differentiation marker TTF-1 provides an avenue to explore biomarkers for de-differentiation of DTC. The findings advance our understanding of thyroid carcinogenesis and will guide further investigations for therapeutic avenues against advanced thyroid cancer.

Immunofluorescence image of a DTC without distant metastases core (1A) and non-cancerous thyroid core (1B) illustrating the expression of RLN2 (green), CD68/macrophage stain (red), CD163/M2 macrophage stain (white) and DAPI/nuclear stain (blue).

Comparison between cases (DTC without distant metastases) and controls (benign thyroid) in terms of RLN2 (2A), CD68 (2B), and CD163 (2C) expression in pixels/area. ****p<0.0001.
2. An Rare Case of Urothelial Malignancy and Acute on Chronic Kidney Failure
Anthony M. Lim1, Jatin Thukral1, Harbir Kaur1, Julia Oberndorf1, Jonathan Ghazaleh1, Robert Cacdac1, Marrey Quizon1, Michael A. Sanford1
1 Eisenhower Medical Center, Rancho Mirage, CA, United States.
Case Report: A 92-year-old woman presented with chest pain and dyspnea. She was treated for pneumonia and presumed urinary tract infection. She presented with acute kidney injury, which first improved, but then continued to deteriorate. Revelant medical history includes She has chronic kidney disease (CKD) stage 4 and type 2 diabetes (T2DM) requiring insulin. Exam Day 1 vitals: T 35.8C (96.5F), heart rate 60 beats/minute, respiratory rate 24 breaths/minute, blood pressure 133/61 mmHg, SpO2 93% on room air. Crackles in the right lower lung zone were noted. There was no abdominal tenderness. Investigations, management Labs performed on day 1 showed: sodium 121 mmol/L, potassium 5.8 mmol/L, HCO3- 18.6 mmol/L, creatinine 2.4 mg/dL (baseline creatinine 1.6 mg/dL), eGFR 17.01 ml/min/1.73m2 normal troponin. Urinalysis showed profound glucosuria, proteinuria, raised white blood cells, with microscopy noting budding yeast. Urine culture from day 1 grew 100,000 colony-forming units/mL of Candida tropicalis. Chest x-ray on day 1 showed right lower lung zone opacity. CT chest abdomen pelvis was performed on day 1, without contrast due to impaired renal function. There were right lower lobe and middle lobe opacities, moderate left hydronephrosis, and no urinary calculi. Non-contrast scan limited view of urological masses. Urology team performed cystoscopy and retrograde ureterogram on day 2. Findings included 1) a tumor on the bladder posterior wall which was resected, 2) a tumor causing significant obstruction of the left ureteric pelvic junction (UPJ) requiring 1 stent.
Discussion: Further history revealed the patient was born and grew up in Kosovo / former Yugoslavia in the Balkan peninsula. She has never smoked cigarettes. She has CKD not fully explained by T2DM (relatively optimal hemoglobin A1c range of 6.0-8.0 % in last 5 years). Urological work-up confirmed unusual tumor locations in both the bladder and UPJ. Tumor biopsy confirmed papillary urothelial carcinoma with early lamina propria invasion. This supports the diagnosis of Balkan Endemic Nephropathy, a rare entity associated with long-term exposure to aristocholic acid from plants in the Balkan peninsula. Lab abnormalities, also seen in our patient, include glucosuria, proteinuria, metabolic acidemia, decreased glomerular filtration rate. Further sequelae include high incidence of urothelial malignancy in the renal pelvis and bladder, consistent with our patient’s findings. Management is largely supportive to treat CKD, including hemodialysis and renal transplant. Our patient was treated with antimicrobials and placement of a left ureteral stent and left UPJ dilation. Renal function slightly improved in days 2-3, but then plateaued and decreased further even with hemodialysis. The family decided to pursue end of life care and the patient ended up passing away 10 days post admission.

CT chest abdomen pelvis without contrast due to impaired renal function, obtained in emergency room on day 1 showing left-sided hydronephrosis. Mass causing obstruction could not be excluded with noncontrast scan.

A) Retrograde ureterogram performed on day 2 showing obstruction in the left ureteropelvic junction. B) Cystoscopy performed on day 2 showing discrete mass in the bladder wall.
3. Housing Instability Among Young Adult Cancer Patients: A Qualitative Study
Haim Moore1, 2, Julia Stal2, Jonathan N. Kaslander2, Priscilla Marin2, Maureen Cairns2, Carol Y. Ochoa-Dominguez3, 2, Matthew P. Banegas3, 2, Kimberly A. Miller2
1 University of Massachusetts Chan Medical School, Worcester, MA, United States. 2 Department of Population and Public Health Sciences, Keck School of Medicine, University of Southern California, Los Angeles, California, United States. 3 Department of Radiation Medicine and Applied Sciences, University of California San Diego School of Medicine, San Diego, California, United States.
Purpose of Study: Cancer treatment is one of the costliest medical conditions to treat. The high cost of cancer treatment puts patients at higher risk of financial toxicity, the detrimental health effects due to financial strain. Housing costs reflect one of the largest financial burdens on an individual, so high out-of-pocket costs and work interruption can quickly lead to housing instability among cancer patients. Housing instability refers to a broad range of conditions including homelessness and frequent moves. Housing instability can worsen health and reduce treatment adherence. Young adult cancer patients (YAs), defined as individuals between the ages of 15 and 39 at the time of diagnosis, may be particularly vulnerable to unstable housing after a cancer diagnosis due to the financial stability typical of this life stage. YA cancer patients may encounter significant barriers to securing stable housing during their cancer experience. The impact of cancer on housing, particularly among YA cancer patients, is an underexplored area of research. In this study we aim to qualitatively examine the experiences of YA cancer patients to better understand their social needs related to housing. Understanding housing instability among YA cancer patients within context of social determinants of health will inform resources needed for this at-risk population.
Methods Used: Twenty participants that consented to a parent R01 study on the social experiences of YA cancer patients and stated high levels of housing instability and housing-related worry will be contacted for participation in the study. Semi-structured interviews will be conducted with HIPAA-compliant Zoom to elicit patients’ subjective experiences and perceptions related to barriers and resources surrounding their housing needs during cancer treatment and in post-treatment survivorship. Transcripts will be reviewed based on using qualitative thematic analysis to identify conceptual categories emerging from the data. We will interpret the results by identifying common patterns and variations across participants, and providing a comprehensive understanding of the experiences of YA cancer patients regarding housing instability.
Summary of Results: Our early quantitative work exploring study survey responses show that our YA cancer patient cohort (n=82) has higher levels of housing worry (21.2%) compared to age- and area-matched counterparts (8.3%). This qualitative study is currently ongoing, and we are actively interviewing patients and coding interviews to obtain results.
Conclusions: Understanding the consequences of a cancer diagnosis on housing experiences for YA cancer patients will help identify key unmet social needs for this at-risk population. An in-depth understanding of the specific challenges this population faces will help inform how best to provide resources to help YA cancer survivors stabilize their housing and ensure healthy outcomes post-treatment.
4. XRK3F2 inhibits p62 Signaling and Augments Myeloma Killing by Proteasome Inhibitors
Ellen Trautman1, 2, 3, Colin Crean3, David Halladay3, Attaya Suvannasankha3
1 DePauw University, Greencastle, IN, United States. 2 The Summer Program for Academic Research in Cancer of Indiana University Melvin and Bren Simon Comprehensive Cancer Center, Indianapolis, IN, United States. 3 Melvin and Bren Simon Comprehensive Cancer Center and Indiana School of Medicine, and Roudebush VAMC, Indiana University, Indianapolis, IN, United States.
Purpose of Study: Despite advancements in therapy, multiple myeloma (MM) remains an incurable blood cancer. Our mission is to maximize the efficacy of a primary treatment for myeloma, proteasome inhibitors (PIs) [CJM1] which cause intracellular waste buildup, leading to ER stress and cell death. p62(sequestosome-1) provides an alternate pathway when the proteasome is inhibited, by breaking down cytotoxic material via autophagy. Upregulation of p62 is associated with [CJM2] PI resistance. We identified a small molecule, XRK3F2, that binds to the ZZ domain of p62 and inhibits its autophagic function. We hypothesized that XRK3F2 would improve MM killing when combined with PIs.
Methods Used: We tested the XRK3F2 and PI combinations in vitro, in ex vivo co-cultures, and in a human MM xenograft model. We tested XRK3F2 plus bortezomib in vitro and in ex vivo myeloma:bone cocultures and analyzed effects on tumor in a prior mouse xenograft experiment.
Summary of Results: XRK3F2 induced cell death in various human MM cell lines, with a IC50s of 3-6 mM. When combined with carfilzomib, the most potent approved PI, at physiologically relevant doses, there was strong synergy (Combinatorial index of 0.4 to 0.6, by Chou-Talalay analysis). The combination of the two agents significantly increased tumor killing in a tumor: bone co-culture model, where the microenvironment of the tumor provides MM survival signals and potential drug resistance. Enhanced tumor killing was further confirmed in a plasmacytoma model of the human MM cell line RPMI-8226 in NSG mice. We also identified soluble BCMA (B-cell maturation antigen, sBCMA) as a sensitive biomarker for tumor burden, which allowed for serial tumor measurements in all tested models.
Conclusions: Combining the p62-ZZ domain inhibitor XRK3F2 with PIs shows great promise in improving the killing of MM. Work is ongoing to validate the combination in xenograft models, where tumor cells colonize bones, and in immunocompetent models. Further mechanistic studies using primary MM cells from patients are also ongoing. sBCMA is a cheap, specific, and sensitive tool for serial tumor measurement and should be further validated for preclinical and clinical usage.
5. Retrospective Analysis of Demographic and Socioeconomic Factors Associated with Research Participants Lost to Follow-up or Withdrawn from the Atlanta RECOVER (Long COVID) Cohort
Yasha Joseph1, Jasmine Berry1, Jennifer Gander2, Sushma Cribbs1, Jenny Han1, Vincent Marconi1, Igho Ofotokun1, Priscilla Pemu3, Tiffany Walker1, Zanthia Wiley1
1 Emory, Atlanta, GA, United States. 2 Kaiser Permanente Georgia, Atlanta, GA, United States. 3 Morehouse School of Medicine, Atlanta, GA, United States.
Purpose of Study: The goal of this study is to characterize clinical, demographic, and socioeconomic factors associated with Atlanta RECOVER participants who were lost to follow-up for their first follow-up visit.
Methods Used: Participant data were collected via REDCap (January 2021 - June 2023). To evaluate differences between participants who completed and those who missed their first scheduled follow-up visit, X2 tests of independence were conducted. Analyses were performed using SAS software.
Summary of Results: Atlanta RECOVER enrolled 891 participants (January 2021 - June 2023); 822 (92.2%) participants scheduled their first follow-up visit and, of these 822, 767 (93.3%) completed their first follow-up. Most who completed their first follow-up visit were 49-64 years old (n=315; 41.1%); Black/African American (n=407;53.1%) or White (n=264;34.4%); female at birth (n=486;63.4%) with English as their primary language (n=731;95.3%). Participants with incomes of < $24,999 were less likely to complete their first follow-up visit and comprised 40% (n=22) of participants lost to follow-up (p<0.01). Participants with disabilities were less likely to follow-up than those without (20.7% vs 77.3%, respectively; p=0.01). 100% (n=26) of Hispanic/Latino/Spanish participants completed their first follow-up visit, 91.3% of Black participants and 94.6% White participants completed their first follow-up visit, respectively, which did not differ significantly by race and ethnicity (p=0.34).
Conclusions: High rates of participant retention for first follow-up visits were noted in the Atlanta RECOVER Hub, irrespective of race and ethnicity. Participants who reported disabilities and incomes < $24,999 were associated with lower retention rates. Characterizing participant-level clinical, demographic, and socioeconomic factors should be assessed in research studies to aid in efforts to target those at higher risk of being lost to follow-up.
6. Determining the Efficacy of the Current Manual Pediatric Sepsis Screening Tools Based on the Current Sepsis Criteria
Molly Walker1, Tom Velez3, Bobbe Thomas1, Ioannis Koutroulis1, 2
1 Emergency, Children’s National Hospital, Washington, DC, United States. 2 George Washington University, Washington, DC, United States. 3 Computer Technology Associates Inc, Cardiff, CA, United States.
Purpose of Study: Currently, the pediatric sepsis screening tools fail to help clinicians recognize the presence of sepsis and improve clinical outcomes. Despite screening tool development over the years, there remains a lack of supportive information to aid in the preemptive diagnosis of sepsis. Due to the small range of supported sepsis consensus criteria for these systems, screening tools are frequently manually administered. The AAP Pediatric Septic Shock Collaborative developed a most widely used sepsis screening tool in EDs based on a combination of vitals, physical exam findings and medical history. The downfall is that these tools tend to have high sensitivity and low PPV, leading to alert fatigue. The objective of this analysis is to evaluate the efficacy of the manually administered AAP-based sepsis screening tool used in the Emergency Department of a large, urban pediatric hospital.
Methods Used: A retrospective analysis of data from a combination of 100 patients (3 months-18 years), during September 2022, that triggered the institutional sepsis screening tool and those that received sepsis protocol treatment was performed to assess tool characteristics such as sensitivity and positive predictive value and to decipher the deficiencies of the tool. For this analysis, sepsis was defined as patients that received the standard sepsis protocol treatment of at least two fluid boluses, IV antibiotics and a blood culture.
Summary of Results: 89% of the cases were false positives, meaning they triggered the sepsis tool but did not receive sepsis protocol treatment (Figure 1). The tool missed 3% of cases that were considered as sepsis, but successfully triggered for 8% of cases that received sepsis protocol treatment (Figure 2). In addition, 3% had a positive blood culture successfully alerted by the tool, but the tool missed 1 case with a positive blood culture. Overall, the current sepsis screening tool has a sensitivity of 73% and a PPV of 8%.

Statistical values of the current sepsis screening tool

Number of cases triggered or not triggered by the tool and associated clinician concern for seps
Conclusions: The main issues with the current AAP-based sepsis screening tool stem from lack of accurate sepsis definitions and data points that the system can run to determine a true potential for sepsis. The system primarily determines sepsis status based on vital sign guidelines and specific high risk past medical history. As a result, the tool triggers more frequently than necessary, leading to decreased clinician trust and alert fatigue. In conclusion, a more precise screening tool can be developed by determining a more supported set of sepsis criteria, and adding other parameters such as specific biomarkers, to more accurately alert clinicians of potential sepsis and prevent further alert fatigue among hospital staff.
7. Cord Blood Reticulocyte Hemoglobin Content as a Marker of Iron Deficiency at Birth
Geetika Kennady1, Rachel Huang2, Katherine Bodycot2, Brandy Firman3, Rupsa Boelig3, Zubair Aghai1
1 Pediatrics/Neonatology, Thomas Jefferson University, Philadelphia, PA, United States. 2 Sidney Kimmel Medical College, Philadephia, PA, United States. 3 Maternal Fetal Medicine, Thomas Jefferson University, Philadelphia, PA, United States.
Purpose of Study: Iron deficiency (ID) during fetal life and early infancy, even in the absence of anemia, is associated with neurocognitive impairment. It is crucial to identify infants who are iron deficient at birth. Up to 17% of the preterm infants are reported to be iron deficient at birth. The risk factors for IDA in infants include small for gestational age (SGA), prematurity, maternal history of placental insufficiency, iron deficiency, diabetes, obesity, smoking, alcohol ingestion, and intrapartum hemorrhage. About 8.9% of these high risk infants are ID at birth. Reticulocyte hemoglobin content (Ret-He) is an early indicator of ID. We aim to determine the prevalence of low Ret-He in umbilical cord blood and its utility in diagnosing ID at birth.
Methods Used: In a prospective cohort study, cord blood samples were collected from term and preterm infants after informed consents from the parents. Complete blood count (CBC), Ret-He, serum iron, total iron binding capacity (TIBC), transferrin saturation (TS) and ferritin was determined in the cord blood. Low Ret-He was defined as ≤ 27.4pg. Iron deficiency was defined as serum iron < 100 mcg/dL, TS < 30% and serum ferritin < 50 ng/ml.
Summary of Results: A total of 244 infants were enrolled and cord blood samples were collected. Ret-He was determined in 216 cord blood samples. The demographic characteristics are depicted in table 1. 10.6% of infants were preterm and 13.4% SGA. The median (IQR) Ret-He was 34.1 pg (29.9-35.1). Ten infants (4.6%) had low Ret-He at birth. Six of these infants were positive for Hb Barts (alpha thalassemia trait) and none of them had iron deficiency. Four infants had low RET-He with negative Hb Barts, all of them had biochemical evidence of ID. In the iron deficiency group, median hemoglobin (range) was 14.1 g/dL (13.4-17.8), median serum iron was 79 mcg/dL (16-96), median ferritin was 20.5 ng/ml (5-34) and median TS was 28% (4-29). All ID infants were born to mothers with anemia.
Conclusions: At birth, 4.6% of the infants had low Ret-He. Infants with low Ret-He had either alpha thalassemia trait or ID. Ret-He in cord blood in the absence of Hb Barts is a potential marker of ID at birth. Infants born to mothers with anemia are at high risk for ID. Cord blood Ret-He can potentially be used to identify iron deficient infants at birth if our findings are confirmed in a larger study.


8. Empowering Youth Leaders for Positive Social Change: The Fresno Community Health Improvement Partnership Youth Leadership Council
Christian A. Santos4,3, Artie Padilla1,2, Susan Kincaid2
1 Central Valley Community Foundation, DRIVE initiative, Fresno, CA, United States. 2 Fresno County Health Improvement Partnership, Fresno, CA, United States. 3 Fresno County Health Improvement Partnership, Youth Leadership Council, Fresno, CA, United States. 4 California State University, Fresno, Fresno, CA, United States.
Purpose of Study: Fresno lies in the middle of California’s impoverished Central Valley, with the majority of youth in this county lacking access to early childhood education, safe housing, safe schools, healthy food, and green space. These barriers hinder youth engagement in educational opportunities to improve health in their city. Yet it is well known that youth can pursue and create change when they participate in projects that address local health issues. For this reason, the Fresno Community Health Improvement Partnership (FCHIP) created the Youth Leadership Council (YLC) as a means of sponsoring and supporting the next generation of leaders from historically marginalized communities.
Methods Used: The YLC is a 6-8 month leadership opportunity offered to local high school and undergraduate students. For each council, 14 local youth were recruited through flyers sent to Fresno County high schools and California State University, Fresno (CSUF). Each student competed a pre-council survey, then reflected upon their council experiences via video. Bi-weekly and monthly meeting topics and events ranged from professional development skills to improving advocacy efforts to speed networking and team collaboration to volunteer work. The above were facilitated by a CSUF undergraduate, himself a graduate of local youth health leadership programs. For their final project, youth council members were able to present the results of their work at a mini-conference attended by local leaders from FCHIP’s large network of community-based organizations. Students each received a $500 stipend for their participation in the council.
Summary of Results: A total of 28 students (comprised of Hispanic, African-American, Asian, and Native American youth) have completed the program thus far. Pre-survey results highlighted their desires for personal growth, knowledge acquisition, and contributing positively to the health and well-being of their local communities. Post-survey videos discussed being surprised by how much they learned, that they appreciated collaborating with others with a passion for change, that they felt the topics covered were quite useful, and that they were able to develop leadership skills, time management skills, and overcame stage fright.
Conclusions: The FCHIP YLC has provided historically marginalized youth with health leadership and advocacy skills while simultaneously amplifying their voices within the local community, giving these students a strong sense of purpose and the belief that they have the power to generate positive social change. We suggest that such a program can be easily adopted by other counties with high concentrations of historically marginalized youth in order to create local youth health change agents while potentially increasing the number of historically marginalized youth that seek out professional health careers.
9. Targeting ABCB7 Potentiates Cisplatin Response in Pediatric Group 3 Medulloblastoma by Inducing Ferroptosis
RANJANA K. KANCHAN1, David Doss2, 3, NaveenKumar Perumal1, Parvez Khan1, Ramakanth C. Venkata1, Wasim Nasser1, Sidharth Mahapatra1, 4
1 Biochemistry and Molecular Biology, University of Nebraska Medical Center, Omaha, NE, United States. 2 Biochemistry and Molecular Biology, Creighton University, Omaha, NV, United States. 3 School of Medicine, Creighton University, Omaha, NE, United States. 4 Department of Pediatrics, Children’s Hospital and Medical Center, Omaha, NE, United States.
Purpose of Study: Group 3 tumors enrich iron transport genes to satisfy their high proliferative need. MiR-1253 targets iron transport by inhibiting the mitochondrial Fe-S transporter, ABCB7. Iron imbalance can lead to cell death by ferroptosis, characterized by iron overload leading to oxidative stress and inducing lipid peroxidation. This study elucidated the impact of targeting ABCB7 on cisplatin cytotoxicity in group 3 MB and whether these effects were mediated by ferroptosis.
Methods Used: Bioinformatics analyses were first utilized to identify deregulated oncoproteins that were targets of miR-1253 in group 3 MB, identifying the mitochondrial iron-sulfer transporter ABCB7. Dual luciferase reporter assay confirmed direct binding of miR-1253 to ABCB7. The effect of miR-1253 overexpression (miR-1253OE) or ABCB7 knockout (ABCB7KO) on cellular and mitochondrial iron levels, oxidative stress, lipid peroxidation, and glutathione levels was studied via confocal microscopy, immunostaining, and Western blotting, FACS, clonogenicity, and medullosphere assays. Impact of ABCB7 repression on cancer cell capacity for glycolysis and oxidative phosphorylation was assessed by Seahorse assays. Ultimately, an orthotopic mouse model was generated to illustrate that cisplatin cytotoxicity can be potentiated in group 3 tumors by repressing ABCB7.
Summary of Results: In silico and in vitro analyses revealed specific enrichment of ABCB7 and GPX4, a critical regulator of ferroptosis, in group 3 MB cell lines and tumors. Restoration of miR-1253 resulted in downregulation of both ABCB7 and GPX4, concurrently increasing mitochondrial and cytoplasmic iron pools and, in turn, mitochondrial oxidative stress and lipid peroxidation, leading to cell death and abrogation of medullosphere formation; ABCB7 knockdown recapitulated these effects but also abrogated GPX4 expression. Fractionation studies confirmed that miR-1253OE or ABCB7KO led to downregulation of GPX4 in the cytosol and mitochondria. Seahorse studies showed that the bulk of ATP generation was occurring in the cytoplasm by glycolysis and not oxidative phosphorylation, suggesting mitochondrial toxicity with ABCB7 inhibition. Cisplatin, a chemotherapeutic agent has also been shown to reduce GPX4 levels and lead to ferroptosis. In miR-1253OE cancer cells, cisplatin IC50 was reduced 2-fold. Resultantly, in miR-1253OE or ABCB7KO group 3 cells, concurrent treatment with cisplatin augmented oxidative stress and lipid peroxidation, depleted glutathione stores, and culminated in a higher index of ferroptosis. In a mouse model of group 3 tumors, ABCB7KO dramatically prolonged survival and potentiated cisplatin effects.
Conclusions: The current study illustrates how targeting iron transport can augment ferroptosis to potentiate cisplatin cytotoxicity in group 3 MB tumors.

10. Firearm and Medication Access and Safe Storage Practices Among Pediatric Emergency Department Patients with a Behavioral Health Chief Complaint: Implications for Lethal Means Reduction Counseling
Ilana S. Lavina1, Rachel Margolis2, Bilal Negash4, Jennifer Jiggetts3, Shilpa J. Patel1
1 Pediatric Emergency Medicine, Children’s National Hospital, Washington, DC, United States. 2 Center for Translational Research, Children’s National Hospital, Washington, DC, United States. 3 Goldberg Center for Community Pediatric Health, Children’s National Hospital, Washington, DC, United States. 4 George Washington University School of Medicine, Washington, DC, United States.
Purpose of Study: Pediatric emergency department (ED) visits for suicidality have increased over the past decade. Self-poisoning with medications and self-injury with firearms are common methods by which youth attempt suicide. Lethal means reduction (LMR) counseling is an effective intervention to reduce suicide risk, but little is known about best practices for implementation in pediatric settings. The purpose of this study is to describe firearm and medication access and storage practices among patients with a behavioral health (BH) chief complaint presenting to our pediatric ED and to evaluate frequency of documented LMR counseling by ED personnel.
Methods Used: ED-based LMR (see Table 1) and suicide risk screening (using the Columbia-Suicide Severity Rating Scale) were implemented in 2020 for patients with a BH chief complaint presenting to our pediatric ED. We conducted a retrospective cross-sectional study of patients ages 6-17 who received this screening between 8/2020-4/2022. Demographic data and screening results were obtained from an electronic medical record-based suicide risk registry. Multivariable logistic regression was performed to identify factors associated with 1) reported safe storage of medications and 2) reported access to firearms. For patients reporting firearm access, details about documentation of LMR counseling were extracted by manual chart review.
Summary of Results: A total of 2789 patients were screened. Of the 94% (2630/2789) of families with medications in the home, 37% (979/2630) reported safe storage. Hispanic ethnicity and positive suicide risk were associated with lower odds of safe medication storage. Female sex, non-Hispanic Black race/ethnicity, Hispanic ethnicity and discharge disposition were associated with lower odds of reported firearm access. Adolescent age was associated with higher odds of reported firearm access. Of the 3% (85/2789) of families who reported a firearm in the home, 85% (72/85) reported safe storage. LMR counseling by a social worker was documented for 80% (43/54) of discharged patients with a firearm in the home, with additional counseling documented by a physician in 7% (4/54) of cases.
Conclusions: Nearly two-thirds of families with medications in the home do not store them safely, suggesting an opportunity for intervention to reduce risk of self-poisoning among youth. Reported access to firearms was low, with racial/ethnic differences identified. Further investigation of these differences is warranted to ensure that LMR screening and counseling is implemented equitably. Physicians rarely documented LMR counseling, illuminating a need for increased education around this practice.


11. Prevalence, Causes, and Predictors of Non-Ischemic Cardiomyopathy Among Patients With Obstructive Coronary Artery Disease
Parag Bawaskar1, Nicholas Thomas1, Khaled Ismail1, Yugene Guo1, Sanya Chhikara1, Pal Satyajit Singh Athwal1, Alison Ranum1, Achal Jadhav1, Abel Hooker1, Ishan Nadkarni1, Dominic Frerichs1, Pratik Velangi1, Tesfatsiyon Ergando1, Hassan Akram1, Chetan Shenoy1
1 Medicine, University of Minnesota, MN, MN, United States.
Purpose of Study: Traditionally, cardiomyopathy in the presence of obstructive coronary artery disease (CAD) on coronary angiography has been classified as ischemic cardiomyopathy (ICM) by inference. However, pathology studies have identified that a proportion of patients with obstructive CAD have non-ischemic cardiomyopathy (NICM) unrelated to the CAD. However, large-scale studies focusing on NICM in patients with CAD are lacking. Cardiovascular magnetic resonance imaging (CMR) has made it possible to identify the cause of cardiomyopathy by allowing direct characterization of the myocardium. The purpose of this study was to investigate the prevalence, causes, and predictors of NICM in patients with CAD.
Methods Used: We studied a large cohort of consecutive patients with obstructive CAD on coronary angiography who underwent CMR from 2004 to 2020 for clinical indications. CMRs were analyzed for the presence and type of cardiomyopathy. Patients with normal left ventricular ejection fraction and no late gadolinium enhancement (LGE) were classified as having no cardiomyopathy. NICM was defined by non-ischemic LGE, absence of LGE without hibernating myocardium, or morphological abnormalities of NICM, such as left ventricular hypertrophy. ICM was defined by ischemic LGE or extensive hibernating myocardium in the absence of LGE. The cause of NICM was determined by integrating non-imaging clinical data available at the time of the CMR, coronary angiography, and CMR data.
Summary of Results: Among the 3,027 patients included in the study (with a mean age of 65 years, 24% women), 18% had no cardiomyopathy, 65% had only ICM, and 17% had NICM. Of those with NICM, 38% also had ICM (dual cardiomyopathy). Compared with ICM, NICM was significantly associated with advanced age (P <0.001), hypertension (P <0.001), a history of heart failure (P = 0.001), and atrial fibrillation (P <0.001) (Table 1). The leading causes of NICM were idiopathic (21%), hypertrophic cardiomyopathy (19%), and hypertensive cardiomyopathy (18%). Other causes of NICM are listed in the table 2.
Correlates of NICM
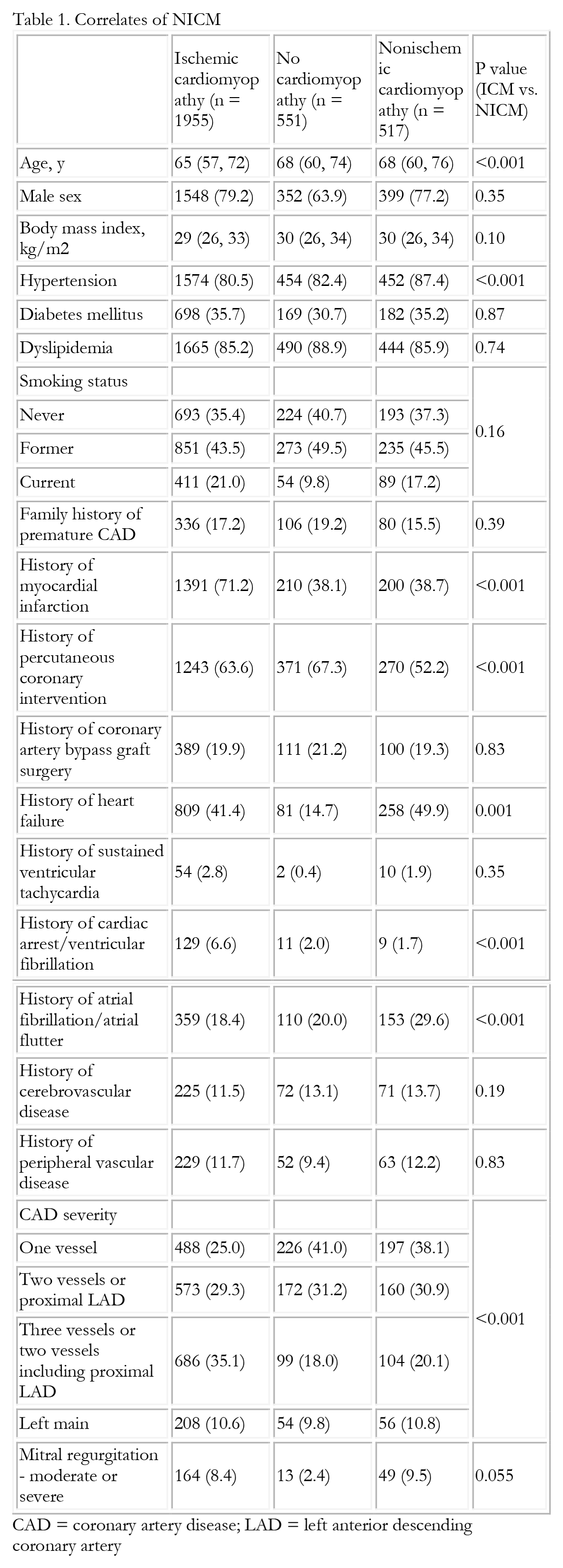
CAD = coronary artery disease; LAD = left anterior descending coronary artery
Causes of NICM

LBBB = left bundle branch block; MVP = mitral valve prolapse
Conclusions: NICM was identified in 1 in 6 patients with CAD. The leading causes of NICM were idiopathic, hypertrophic cardiomyopathy, and hypertensive cardiomyopathy. Compared with ICM patients, NICM patients were more likely to be older, and have hypertension, heart failure, and atrial fibrillation. Further research is warranted on the long-term clinical outcomes of NICM in CAD.
12. Brain Cancer Diagnosis and Enhancing Prognosis with Machine Learning and Imaging
K. H. Miao1,2, J. H. Miao1,3
1 Cornell University, New York, NY, United States. 2 Icahn School of Medicine at Mount Sinai, New York, NY, United States. 3 Renaissance School of Medicine at Stony Brook University, New York, NY, United States.
Purpose of Study: Annually, millions of patients are affected by brain cancers. Early and accurate diagnosis of brain cancer patient can improve prognosis and lead to enhanced patient outcomes. Thus, early brain cancer diagnosis is critical for enhancing patient quality of life. In addition, diagnosis of various brain cancer types can be a challenge. In this research, a machine learning model created using applications of artificial intelligence algorithms and imaging in brain cancer are utilized to help medical professionals in improving diagnosis of brain cancers and enhancing patient outcomes.
Methods Used: An artificial intelligence model is developed using imaging and over 2,540 brain cancer patient data to improve diagnosis and detection of brain cancers. The model was also built using machine learning algorithms including neural networks to diagnose cancer in patients. Clinical data from brain cancer patients was used to build, train, and test the model. Random selection of 60% of the patient data was applied to train the model while the remainder 40% was used to test its diagnosis abilities.
Summary of Results: After training and testing the artificial intelligence model, it was able to diagnose brain cancers with an overall accuracy of 88.2%, improving upon the performance of previously published methods.
Conclusions: Thus, machine learning algorithms and imaging can be utilized to aid healthcare professionals to improve early diagnosis and prognosis of brain cancers, improving patient outcomes and quality of life.
13. Diagnosis of Bone Cancer and Improving Prognosis with Imaging and Artificial Intelligence
J. H. Miao1,2, K. H. Miao1,3
1 Cornell University, New York, NY, United States. 2 Renaissance School of Medicine at Stony Brook University, New York, NY, United States. 3 Icahn School of Medicine at Mount Sinai, New York, NY, United States.
Purpose of Study: Throughout the world, bone cancers affect millions of patients every year. With early detection, bone cancer patients have better outcomes and higher chances of survival. Therefore, early bone cancer diagnosis is essential for improving prognosis for patients. Frequently, bone cancers can be challenging to distinguish visually. In this research, an artificial intelligence model built using machine learning based on deep learning algorithms and clinical patient data is used to aid healthcare professionals in enhancing diagnosis of bone cancers and improving prognosis for patients.
Methods Used: To diagnose bone cancers, over 2,890 bone cancer patients and their clinical imaging data were used to build, train, and test the deep learning model, created with machine learning algorithms. For training the model, 55% of the clinical patient data and their imaging were randomly selected to build it. The other 45% of the patient data was used for testing the bone cancer diagnosis capabilities of the model.
Summary of Results: After completion of the training and testing phases, the machine learning model achieved a 91.3% overall diagnostic accuracy for detecting bone cancers in patients, exceeding previously published methods.
Conclusions: In conclusion, artificial intelligence models based on machine learning algorithms and imaging can be applied in healthcare settings to aid medical professionals for enhancing early and accurate diagnosis of bone cancers, improving prognosis for bone cancer patients.
14. Blood-Brain Barrier Dysfunction in Leukoencephalopathy, Brain Calcifications, and Cysts
Nnenna E. Nwankwo1,2, Natalie C. Smith4,2, Brianna R. Pierce2, Nhu T. Chau2, Jennifer L. Harmon3,2, Jamie L. Fraser3,2
1 Howard University, Washington, DC, United States. 2 Center for Genetic Medicine Research, Children’s National Hospital, Washington, DC, United States. 3 Rare Disease Institute, Children’s National Hospital, Washington, DC, United States. 4 Purdue University, West Lafayette, IN, United States.
Purpose of Study: Leukoencephalopathy, Calcifications, and Cysts (LCC) is an ultra-rare genetic leukodystrophy characterized by white matter hyperintensities on MRI, calcium deposits, and cysts. LCC, which is caused by biallelic pathogenic variants in SNORD118, typically presents in childhood but may present in adulthood. Given the rarity of LCC, with fewer than 100 reported cases worldwide, recent gene-disease association, and lack of an established animal model that recapitulates the human phenotype, the underlying pathogenesis remains poorly understood. Calcium deposition and subsequent cyst formation occur in or adjacent to white matter tracts near cerebral microvessels, and often first appear in the deep grey structures. LCC patients’ MRIs demonstrate contrast enhancement adjacent to cysts and calcifications, indicative of loss of blood-brain barrier (BBB) integrity. Because the MRI phenotype appears highly inflammatory, we sought to investigate the impact of LCC on BBB integrity and immune activation in our novel CRISPR/Cas9-directed Snord118 n.8G>C knock-in missense mouse model.
Methods Used: We employed fluorescently conjugated dextran administration, calcium staining, and immunohistochemistry to quantify BBB disruption and inflammatory response in 120-day-old sex-matched LCC and wild-type (WT) mice. Brain samples were dissected, flash frozen, embedded in OCT, cryosectioned at 10 um, and stained for BBB vessels, microglia, other immune cells, and calcium deposition. Quantification of cell types, activation states, and proliferation were performed.
Summary of Results: Our novel LCC mouse model has demonstrated dextran extravasation and immune cell activation surrounding areas of calcifications and cysts, suggesting a relationship between BBB dysfunction, inflammation, and eventual cyst development. These findings were not observed in the WT mice. Total microglial number, proliferation rates, and activation states were different in the LCC mice compared to WT controls.
Conclusions: The LCC human phenotype implicates neuroimmune-mediated mechanisms in addition to previously described microangiopathic mechanisms in disease progression, and our LCC mouse model recapitulates these findings. This work adds to our mechanistic understanding of disease progression in LCC and informs the identification of potential drug candidates for pre-clinical trials of disease-modifying therapies to arrest LCC disease progression.
15. A Clinical-Translational Model of Leukoencephalopathy with Calcifications and Cysts
Brianna R. Pierce1, Jennifer L. Harmon3,1, Nhu T. Chau1, Nnenna E. Nwankwo2,1, Jason W. Schroeder4, Laura Tochen5, Jamie L. Fraser3,1
1 Center for Genetic Medicine Research, Children’s National Hospital, Washington, DC, United States. 2 Howard University, Washington, DC, United States. 3 Rare Disease Institute, Children’s National Hospital, Washington, DC, United States. 4 Department of Radiology, Children’s National Hospital, Washington, DC, United States. 5 Department of Neurology, Children’s National Hospital, Washington, DC, United States.
Purpose of Study: Leukoencephalopathy with Calcifications and Cysts (LCC) is a rare genetic disorder characterized by progressive white matter injury and development and evolution of CNS calcifications and cysts. Patients experience epilepsy, motor dysfunction, cognitive impairment, and behavioral changes. LCC is progressive and ultimately fatal. Biallelic pathogenic variants in SNORD118 cause LCC through defective assembly of the 60S ribosomal subunit. The mechanism(s) by which LCC disease progression occurs are not well established.
Methods Used: To address these questions, we have developed a unique clinical-translational model by enrolling LCC subjects in our natural history and biorepository research program and simultaneously generating a novel LCC mouse model. Our research cohort includes over 25 individuals across 3 continents. We obtained and analyzed all available brain imaging, clinical, laboratory, and genetic data. We are developing clinical outcome assessments and biomarkers of LCC disease progression. We characterized a novel CRISPR/Cas9-directed knock-in Snord118 n.8G>C missense mouse model of LCC to identify potential biomarkers and mechanisms of disease progression.
Summary of Results: In the patient cohort, cyst formation, a diagnostic hallmark of LCC, was a later finding in disease progression. Subtle developmental delays or regression of motor and communication ability were often the primary symptoms and occurred before cyst formation. Sex differences in disease progression were observed, with males shorter and more underweight. Swallowing difficulties were observed in over 50% of patients. Over 50% of affected individuals were born preterm or were growth-restricted at birth. The LCC mouse model recapitulates the morphological phenotype observed in human brains with the development of calcifications and cysts observed by 120 days. The LCC mice recapitulate the sex differences observed in humans, with males demonstrating earlier mortality and more obvious weight differences compared to females. Male and female KI mice were significantly underweight compared to controls. The LCC mice demonstrate hypopigmentation associated with ribosomopathy phenotypes in mice.
Conclusions: Our LCC clinical-translational model is essential for the identification of biomarkers and targets for drug development. Clinical outcomes assessments developed from our natural history cohort will enable clinical trial readiness when disease-modifying therapies are identified. Simultaneously, we have developed and validated a novel mouse model of LCC that recapitulates the human phenotype and will be used for further investigation into the mechanisms of LCC and preclinical studies of new therapies. We have identified a significant window for therapeutic intervention in LCC, making LCC an attractive candidate for rare disease drug development.
16. Inhibition of Mitochondrial Fission as a Treatment for Alzheimer’s Disease: A Human Cell Culture Study
Shelly Gulkarov1, Ankita Srivastava1, Heather A. Renna1, Maryann Johnson1, Katie Sheehan1, Aaron Pinkhasov1, Joshua De Leon1, Irving Gomolin1, Allison B. Reiss1
1 NYU Grossman Long Island School of Medicine, Mineola, NY, United States.
Purpose of Study: Alzheimer’s disease (AD) is the most common cause of dementia characterized by progressive memory loss and cognitive decline. The characteristic neuropathologic changes of AD include the accumulation of amyloid plaques outside neurons and neurofibrillary tangles (NFTs) within neurons. Accumulation of both amyloid plaques and NFTs have detrimental effects on mitochondrial functioning. Mitochondrial degeneration in AD, involves excessive mitochondrial fission and reduced fusion, leading to cell damage. P110 is a 7-amino acid peptide that restores mitochondrial dynamics by acting as an inhibitor of mitochondrial fission. P110 treatment restores mitochondrial membrane potential, reduces reactive oxygen species, and restores oxidative respiration capacity and ATP production. This study aims to identify the neuroprotective potential of P110 by documenting changes in expression of genes pertaining to AD and neuronal health.
Methods Used: SH-SY5Y human neuroblastoma cells were exposed to 1uM and 10uM of P110. Real-time-PCR analysis was performed after 24 hr. of incubation and Western blotting was done after 48 hr. of P110 treatment. MitoTracker staining was performed to detect active mitochondria in live cells after P110 treatment.
Summary of Results: P110 exposure in SH-SY5Y cells significantly increase amyloid precursor protein (APP) mRNA levels at 1uM (P=0.0002), while mRNA levels of β-secretace-1 (BACE1) were increased at both 1uM (P<0.0001) and 10uM (P=0.014) concentrations. However, protein levels of both APP (P=0.016) and BACE1 (P=0.016) were significantly reduced at 10uM of P110 in SH-SY5Y cells. P110 treatment significantly increased active mitochondria in SH-SY5Y cells at both 1 and 10uM (P<0.0001) doses as detected by MitoTracker staining.
Conclusions: In this study, cultured human neuronal cells exposed to P110 exhibit surprising increases in mRNA levels of 2 genes involved in amyloid β formation: its precursor APP and the enzyme that generates amyloid β, BACE. However, despite these mRNA changes, P110 has an anti-amyloidogenic effect because it reduces the formation of amyloid β by lowering the protein levels of APP and BACE1. Protein expression is not necessarily proportional to mRNA levels and this may reflect differences in their half-lives and stability. Further, the increase in active mitochondria found in P110-treated neurons suggests a P110-induced improvement in mitochondrial functioning. Taken together, our results indicate that P110 might be useful in attenuating amyloid β accumulation and maintaining mitochondrial health. Further studies will clarify this benefit, which may have clinical application in conjunction with other AD treatments to improve prognosis in this complex, multifactorial neurodegenerative disorder.
19. In-Hospital Outcomes Associated with Inflammatory Bowel Disease in STEMI Patients
Amit Dey1, Mohammed Faisaluddin2, Sourbha Dani3
1 Georgetown University, Washington DC, DC, United States. 2 Rochester General Hospital, Rochester, NY, United States. 3 Lahey Clinic, Burlington, MA, United States.
Purpose of Study: Chronic inflammatory disease states including psoriasis, lupus and rheumatoid arthritis are associated with a higher incidence of STEMIs. However, data on STEMIs are scarce in inflammatory bowel disease (IBD) and outcomes of STEMI patients such as mortality, cardiogenic shock and ventricular tachycardia in IBD are almost nonexistent. Thus, we sought to evaluate potential outcomes of IBD in STEMI patients in a nationally representative adult US population.
Methods Used: The US-based National Inpatient Sample was queried between 2015 and 2020 using ICD-10 codes for adults ≥ 18 years with STEMI with and without IBD. The adjusted odds ratio of index hospitalization outcomes was calculated using a multivariate logistic regression analysis.
Summary of Results: Overall only 0.44 percent (3960) reported IBD in STEMI patients. Those with IBD were middle aged and predominantly female compared to non-IBD in STEMI patients. IBD patients also had similar CVD risk factors (hypertension, obesity) than non-IBD participants (p>0.05), however prevalence of smoking and Diabetes were lower in IBD patients (P<0.001) whereas cost of hospitalization and length of hospital stay was higher in STEMI patients (p<0.05). Moreover, IBD patients had lower mortality compared to non-IBD patients with STEMI (P<0.001), however on adjustment for baseline CVD risk factors and hospital characteristics, this difference completely attenuated (P=0.50). Prevalence of cardiogenic shock did not differ between groups whereas prevalence of ventricular tachycardia was significant lower in patients with IBD in adjusted analyses (OR 0.63, P<0.001) (Table 1)
Conclusions: In a nationally representative adult US population we observed no difference in mortality and cardiogenic shock but lower prevalence of ventricular tachycardia in IBD with STEMI patients. These findings need to be confirmed in prospective cohorts and the biological mechanisms evaluated in translational studies.

20. Cystic Fibrosis Disparities: A Tertiary Center Experience in Physical and Mental Health Outcomes
Hani Fanous5, Mariana Bedoya2, Jelte Kelchtermans3, Lolly Starr-Glass1, Minas Benyamin4, Monica Cardenas1
1 University of Miami, Miami, FL, United States. 2 Vanderbilt University, Nashville, TN, United States. 3 University of Pennsylvania, Philadelphia, PA, United States. 4 Georgia Institute of Technology, Atlanta, GA, United States. 5 Children’s National Medical Center, Washington, DC, United States.
Purpose of Study: Despite advances in management of Cystic Fibrosis (CF), important healthcare discrepancies remain. In the US, Hispanic persons with CF appear to be at an increased risk for death even when adjusting for socioeconomic status, age, sex, and clinical severity. However, given heterogeneity among Hispanic individuals, it is important to examine these outcomes in additional contexts. Miami stands out as a region with a large Hispanic community from varying backgrounds. In our previous study we demonstrated statistical differences in Mid Expiratory Flows (MEF) in Hispanics compared to Non-Hispanics, possibly indicating earlier pulmonary morbidity. This study pairs previous findings and explores potential impact of mental health on clinical outcomes.
Methods Used: This is a 5-year retrospective (2013-17) analysis of tertiary CF center data in South Florida of children with CF and available PFT data. The primary outcome was differences in FEV1 and FEF25-75 between Hispanic and non-Hispanic patients. Secondary outcomes included differences in self-reported anxiety (GAD-7) and depression (PHQ-9) implemented per recent guidelines, and collected by a mental health screener.
Summary of Results: Sample included 37 unique patients (Hispanic= 23; non-Hispanic= 14). Average age 10.4 years (SD= 5.6). Paired sample t-test indicated that FEV1 percent predicted for Hispanic patients (M= 81.59, SD= 21.62) was not significantly different than non-Hispanic patients (M= 79.43, SD= 23.35), p = 0.65. FEF25-75 percent predicted was significantly different between Hispanic (M= 72.17, SD= 34.25) and non-Hispanic patients (M= 76.46, SD= 31.90), p = <0.001. Mental health screening data from 24 parents of participants in this study (Hispanic= 12; non-Hispanic= 12) revealed significantly higher anxiety in Hispanic parents (M= 6.88, SD= 4.40) compared to non-Hispanic parents (M= 3.54, SD= 4.10), p = 0.05. Symptoms of depression were not significantly different between Hispanic (M= 6.06, SD= 5.11) and non-Hispanic parents (M= 2.92; SD= 2.93), p=0.06.
Conclusions: In contrast to previous published work, our earlier study showed no statistical difference in FEV1 between Hispanic and non-Hispanic CF children while such difference was shown for MEF between groups. This may indicate Hispanic patients are at greater risk of early pulmonary morbidities compared to their non-Hispanic peers. In terms of caregiver mental health outcomes, Hispanic parents reported significantly greater anxiety compared to non-Hispanics. For depression, a trend towards more depression in Hispanic parents was shown, it did not reach significance due to small sample size. Taken together, these data may suggest that Hispanic parents have higher levels of mental health challenges, which may contribute to earlier pulmonary morbidity demonstrated by lower MEFs in Hispanic children.
21. Takeaways From The Twelve Point Program For Curriculum Improvement at a West Texas Medical School
Barath Rangaswamy1, Jacob J James1, Nicole Remmert1, Lutfor Nessa1, Stephanie stroever1
1 TTUHSC, Odessa, TX, United States.
Purpose of Study: Curriculum Improvement (CI) is often an ongoing process. We did a cross-sectional study of third (MS3) and fourth year (MS4) students who completed Internal Medicine Clerkship of a medical school in underserved West Texas area. We surveyed their perceptions on the “Twelve Point Program” which had 12 different CI initiatives implemented during academic year 2022-23. This abstract includes the most recent responses as of August 2023.
Methods Used: We used Likert scale questionnaire. Fisher’s exact was used to compare responses,we set α= 0.05 a priori for hypothesis testing
Summary of Results: The response rate was 66.6 (n=29). Reading Room Visits: The majority believed the current radiology curriculum is inadequate (60.0%) or very inadequate (23.3%). Nearly 90% of students either agreed or strongly agreed that brief reading room visits could be a valuable alternative when a separate rotation is not feasible. MS3 and MS4 had almost identical endorsements across categories including confidence to interpret x-rays (p=0.91), value of reading room visits (p=1.00) and frequency of visits (p=1.00). Students had workshops for Differential Diagnosis, EKG, ABG interpretation to improve those skill sets. Simulation based learning at SIM center was proposed for physical exam training. Longitudinal Learning Plan (LLP) included weekly Q bank review meetings to encourage student progress in Q bank utilization from week one. Almost all responded that a longitudinal focus in learning the Q banks from week one of clerkship is preferred over the last week just before the exam. Fifty five percent of students agreed that LLP helped to improve their SHELF exam scores. Nearly 30% of MS4 disagreed that reviewing Q bank progress weekly would be valuable while none of the MS3 had a similar opinion. This was the only question with significant differences between MS3 and MS4 (p=0.012). Case presenting and clinical reasoning workshops focused on improving bedside presentations and decision making skills. Hospital Medicine Primer is a didactic series during the first week of clerkship. Nearly 96% of students either agreed or strongly agreed that it helps to prepare and perform well in ward rotations. “Practicing Compassion and Compulsion to go the extra mile” is a group discussion activity for students. Nearly 83% of students agreed that such an activity is either likely or very likely to inculcate those habits as lifelong virtues. IM Scholar program promotes research and scholarly activities. Nearly 75% of students felt that research opportunities in clerkship are either adequate or more than adequate. Lastly, Clinical Documentation Improvement (CDI) workshop introduced fundamentals of CDI to write clinically sound and adequately billable as well.
Conclusions: We describe clerkship CI initiatives that integrated core skills, SHELF exam performance, compassion training and documentation proficiency for our medical students.
22. Tumor Necrosis Factor Inhibitor Therapy in Rheumatoid Arthritis: Does it Impact Macrophage Cholesterol Efflux and Cardiovascular Risk?
Saloni Godbole1, Heather A. Renna1, Kim Doyle1, Steven Carsons1, Elise Belilos1, Joshua De Leon1, Lora Kasselman2, Allison B. Reiss1
1 NYU Long Island School of Medicine, Mineola, NY, United States. 2 Hackensack Meridian Health, North Bergen, NJ, United States.
Purpose of Study: Cardiovascular disease is the leading cause of death in RA despite multiple treatment options that address systemic inflammation. Cholesterol accumulation and macrophage foam cell transformation occur when the balance between cholesterol influx and efflux is disrupted. Reverse cholesterol transport, key in prevention of lipid overload, is disrupted by the inflammatory environment of RA. Methotrexate, an anti-inflammatory drug that promotes cholesterol efflux and prevents excess lipid from overwhelming the macrophage, confers CV benefit in RA. It has not yet been determined whether TNF inhibitors are atheroprotective in RA. The TARGET clinical trial posits that methotrexate with a TNF inhibitor will have superior CV benefits in RA compared to triple therapy (sulfasalazine, methotrexate, and hydroxychloroquine). Our study examines the effect of the TNF inhibitor adalimumab on cholesterol transport in cultured human macrophages to demonstrate whether the drug is anti-atherogenic via enhancement of lipid outflow.
Methods Used: THP-1 differentiated macrophages (106 cells/ml, phorbol myristate acetate, 100nM, 48h) were incubated for 18h in the presence of 0 or 5% RA plasma ± adalimumab. Cholesterol transport protein mRNA was quantified by RT-PCR using specific primers for each gene. Data was then normalized against the housekeeping gene GAPDH. Cholesterol efflux into media was measured fluorometrically using the Amplex Red Cholesterol Assay kit (Invitrogen). Reactions were performed with and without cholesterol esterase, then analyzed for total (TC) and free (FC) cholesterol. Statistical analyses were performed using GraphPad Prism. dCt values were analyzed using factorial ANOVAs for each mRNA for normally distributed data. Cholesterol efflux was analyzed using the Mann–Whitney test. Statistical significance was set at an alpha value of 0.05.
Summary of Results: Adalimumab did not affect the levels of reverse cholesterol transport proteins in macrophages, including ABCA1, ABCG1 and 27-hydroxylase. This was reflected in a lack of change in macrophage lipid efflux with effluxed TC as a percent of TC showing no significant difference with or without adalimumab (U=19, p=0.5350, n=6 per group). RA plasma alone increased expression of CD36, a scavenger receptor that plays a key role in lipid uptake. TNF inhibition did not mitigate the pro-atherogenic upregulation of CD36. Scavenger receptor A was also unaffected by TNF inhibition.
Conclusions: Adalimumab did not significantly affect macrophage cholesterol transport. This finding may indicate that despite higher cost, TNF inhibitors do not prevent CV consequences of RA. There is an urgent need for new therapeutic approaches to reduce CV mortality in RA. The neutral status of adalimumab on cholesterol transport is relevant to the TARGET trial as well as clinical decision-making in the treatment of RA.
ABCA1: No interaction effect: F(1,29)=1.290; p=0.2653; n=6 (RPMI), n=3 (ada), n=12 (RA),n=12 (RA+ ada)
ABCG1: No interaction effect: F(1,29)=1.315; p=0.2609; n=6 (RPMI), n=3 (ada), n=12 (RA),n=12 (RA+ ada)
27OH: No interaction effect: F(1,28)=1.651; p=0.2093; n=6 (RPMI), n=3 (ada), n=11 (RA),n=12 (RA+ ada)

THP1s, no plasma, ada at 5ug/ml
IC Total cholesterol: no sig diff, U=15, p=0.6991, n=6 each group
IC Free cholesterol: no sig diff, U=17, p=0.9372, n=6 each group
Effluxed total cholesterol at % of total cholesterol intra/extracellular: no sig diff, U=19, p=0.5350, n=6 each group

23. Polyunsaturated Lipids Predict and Stratify Risk of Pulmonary Hypertension in Human Heart Failure with Preserved Ejection Fraction
Vaishnavi Aradhyula1, Ahmed Elzanaty1, Rohit Vyas1, Dhilhani Faleel1, Prabhatchandra Dube1, Sadik Khuder1, Steven T. Haller1, Rajesh Gupta1, David J. Kennedy1, Samer J. Khouri1
1 Medicine, University of Toledo College of Medicine and Life Sciences, Toledo, MI, United States.
Purpose of Study: Pulmonary hypertension (PH) in heart failure with preserved ejection fraction (HFpEF; PH-HFpEF) is a relatively newly recognized condition that poses a leading healthcare burden. With a staggering 60% 5-year mortality rate, the development of PH is the strongest predictor of adverse outcomes in HFpEF. Incomplete understanding of pathophysiology, ineffective therapies, and limited non-invasive diagnostic methods contribute to this growing epidemic. Pathogenesis of PH-HFpEF is not explained by traditional risk factors alone, suggesting the need to examine novel regulatory mechanisms. Polyunsaturated Fatty Acid (PUFA) metabolites regulate balance between anti-inflammatory, pro-inflammatory, and pro-resolutory lipid mediators, playing a critical role in cardiovascular health. We aimed to identify PUFA-derived lipid mediators that can stratify cardiovascular risk in HFpEF patients.
Methods Used: A single center prospective cohort study was conducted on 88 patients with a new diagnosis of HFpEF. Venous and arterial samples were collected during right heart catheterization. 143 PUFA serum metabolites were analyzed using mass spectroscopy with Multiple Reaction Monitoring. We performed logistic regression analysis for the PUFA-derived lipid mediators that predicted all-cause mortality as well as cox proportional hazards analysis to determine which lipids predicted time to death.
Summary of Results: We found that the PUFA-derived lipid metabolites predictive of death in PH-HFpEF were pro-inflammatory 15-keto prostaglandin F2a (p=0.02), pro-inflammatory thromboxane B3 (p=0.04), anti- and pro-inflammatory 9(10)-EpOME (p=0.04), anti-inflammatory 15(R)-prostaglandin E1 (p=0.03), and pro-resolutory resolvin D5 (p=0.05). Similarly, the PUFA-derived lipid metabolites predictive of time to death in PH-HFpEF were 15-keto prostaglandin F2a (p=0.01), thromboxane B3 (p=0.05), 9(10)-EpOME (p=0.01), 15(R)-prostaglandin E1 (p=0.03), and resolvin D5 (p=0.01).
Conclusions: These findings demonstrate that distinct PUFA inflammatory mediators are associated with mortality risk in PH-HFpEF. This novel lipidomics framework introduces new non-invasive biomarkers for the diagnostic and prognostic assessment of cardiovascular risk in PH-HFpEF.

POSTERS
P1. Latex Fruit Syndrome; A Case of Lower GI Bleed
Rohan Kuruvilla1, miguel ramallo2, Emmanuel Kerolle1, Jonas Clarke1, Saad Karim1, Girma Ayele1, Miriam Michael1
1 Internal Medicine, Howard University, DC, DC, United States. 2 Anesthesiology, Howard University, DC, DC, United States.
Case Report: About 30-50% of individuals allergic to natural rubber latex (NRL) show an associated hypersensitivity to some plant-derived foods. The association of latex allergy and allergy to plant-derived foods is called latex-fruit syndrome. A growing number of plant sources have been associated with this. It is thought that the allergen cross-reactivity is due to IgE antibodies.
Case Presentation: A 21-year-old female with a history of food allergies came into the ER after 1-week of abdominal pain. This abdominal pain is associated with food and manifests as a gnawing discomfort in the epigastric area, rectal pain, and cramping loose stools. She also experienced occasional bright red blood per rectum and some clots. She says the bleeding is spotty and infrequent, occurring when she has bowel movements. She says she is careful about her allergies, which have been getting more symptomatic in the past month, so she stopped eating certain fruit. She denies tingling, swelling, or numbness when eating food last week. She has no history of sickness indicators. She is an art student who recently finished a project with natural latex. She does not drink, smoke, or use illicit drugs. She is alert and oriented on a physical and answers questions pleasantly and concisely. Physical findings were only significant for mild epigastric pain. She displayed no rebound, guarding, masses, or CVA tenderness. Her stool was guaiac positive. All laboratory results are normal. The patient was admitted, given fluids, monitored for further bleeding, cramping, and loose stools, and was discharged the next day with a follow-up in the allergy clinic.
Discussion: Natural Rubber Latex allergies are thought to occur in up to 4.2% of people. Healthcare workers have a high risk of latex exposure due to the use of protective gear. Latex allergies are not always a result of direct contact with latex, as latex syndrome can also occur through consuming certain foods. Fruit Latex Syndrome is a phenomenon that correlates natural rubber latex hypersensitivities to certain food hypersensitivities and is similar to oral syndromes. The allergic reaction induced by Latex Fruit Allergy likely stems from cross-reactivity syndrome and traditional direct sensitization. This is supported by the known cross-reactivity of a group of latex allergens, the Hev B proteins, notable for their cross-reactivity with a group of defense-related plant proteins, the Class I chitinases. Hevein is the primary allergen chiefly responsible for the syndrome of both plant and insect chitinases. Plant chitinases, a structural similarity with hevein, have been reported. Moreover, a structural similarity has been noted between the recently identified edible insect allergenic chitinase and an allergenic chitinase from the house dust mite Dermatophagoides farinae.


P2. Disease Phenotype Discovery and Validation Can Optimally Inform Target Selection and Drug Development: Application of Artificial Intelligence-Based Analytics Using Real-World Evidence Big Data
Nicholas J. Sarlis1, Michael N. Liebman2
1 Clinical Development, CLEARA Biotech BV, Greenville, DE, United States. 2 Corporate Management, IPQ Analytics, Kennett Square, PA, United States.
Purpose of Study: Consistently impactful solutions for maximizing the probability for success of drug discovery and development (DDD) programs remain elusive despite the rapid adoption of new technology platforms, due to a lack of appreciation of the root cause of various problems and/or strategic constraints associated with an inflexible DDD ‘pipeline model’. As most diseases remain syndromic in their definition, the discovery of biomarkers still follows empirical paths derived from incomplete definitions of ‘disease’ itself and imprecise/inaccurate measures of therapeutic response. We propose an approach whereby in addition to traditional ‘target selection and validation’, significant effort and focus is also placed onto ‘disease phenotype discovery and validation’. Application of artificial intelligence (AI)-based analytics using the aggregate of real-world evidence (RWE) Big Data (BD) is poised to redefine ‘disease phenotypes’ and improve target selection and/or druggability.
Methods Used: Complementing data from standard pharmacokinetic (PK) and pharmacodynamic (PD) assays - and other translational outcomes - and high-throughput screening (HTS), information derived from AI-driven analytics of RWE BD is capable of assisting in the biology/chemistry phases of DDD. Key goals for our methods are a. identification of new targets; b. computational screening of molecule libraries; c. categorization of symptom burden/patient behavioral patterns; d. enhancement of recruitment for clinical trials; e. increasing the use of synthetic control arms/digital twins to augment and shorten clinical trials; f. modeling the effects of new drug combinations, responder subgroups selection, and objective measurement of the effectiveness of personalized medicine delivery.
Summary of Results: We have used pathway analysis, integrative multi-omics, and PK/PD & molecular imaging markers in various scenarios. AI-based analytics open a ‘guided exploration’ path to define the ‘disease phenotypes’, thus helping redefine ‘disease’ as a process – rather than a state. We will present solutions for the fundamental challenge of incorporating in a high-dimensional space both patient-derived parameters, e.g., lab/path/imaging data and clinical manifestations, along with non-clinical factors, e.g., diet, environment, lifestyle, etc. Our modeling approach takes into consideration time dynamics, as the weighting of each of the aforementioned factors varies over time (Fig. 1).
Conclusions: Applying a strategically designed, AI-guided multi-level data matrix derived from RWE BD is poised to expand drug discovery and development beyond the constraints of the status quo ‘pipeline vision’ and the current approach of simply bolting new technologies on fundamentally complex problems in DDD and healthcare at large.

P3. The Liberation of Photons from an Intracellular Cloud Using Artificial Intelligence Produces Entanglement and Superconductivity Improving Coupling of Junction Gaps-Membranes and Connexing Proteins Improving Left Ventricular Function
Pablo I. Altieri1, Nelson Escobales1
1 Medicine and Physiology, University of Puerto Rico, Medical Sciences Campus, San Juan, Puerto Rico.
Purpose of Study: Superconductivity (S.C.) via Entanglement (E.) is a concept of pushing materials to the extremes at the cellular level temperature, to get maximum results of this process through artificial intelligence (A.I). Superconductivity (S.C.) via Entanglement (E.) is a concept of pushing materials to the extremes at the cellular level temperature, to get maximum results of this process through artificial intelligence (A.I).
Methods Used: Experiments were done intracellularly in isolated heart cell pairs measuring intracellular junction gaps conductivity (G.I.) induced by Enalapril and Angiotensin II (Ang II). Enalapril (25 ug/ml) was injected rapidly up to a dose of 1 ug/ml in 4 minutes. Ang II was injected also intracellularly at 1 ug/min at the same time. Both, at 27 degrees celcius not at lower temperature. The use of mechanical pumps were used for the injection.
Summary of Results: A reduction of G.I. with Ang II was 55% without a plateau. With Enalapril, an increase in G.I. (106%) was measured until a plateau was reached. We think the reason for the plateau seen with Enalapril was a reduction of E., due to a photon effect from an intracellularly electron cloud. Why this occurs with Enalapril and not with Ang II, is not known, but probably is due to encryption.
Conclusions: The effect of Enalapril is an effective way to produce coupling of the heart cells by improving G.I. conductivity. Enalapril increased G.I. by 106% with a plateau, probably through encryption. Enalapril effect is also seen extracellularly. This shows that Enalapril can be used intracellularly in severe and intractable heart failure by producing coupling of myocardial cells, membranes and connexing proteins, which will improve left ventricular function.
P4. Challenges of Rhythm Control in Patients with Atrial Fibrillation with Aberrancy, Wolff-Parkinson-White Syndrome and Ebstein’s Anomaly
Gorgina H. Barsoum1,2, Muhammad A. Khan3, Talal Asif2,1
1 UMKC School of Medicine, Kansas City, MO, United States. 2 University Health Truman Medical Center, Kansas City, MO, United States. 3 University of Kansas Medical Center, Kansas City, KS, United States.
Case Report: A 59-year-old male, with a past medical history of Ebstein’s anomaly and previously mild tricuspid regurgitation (TR) on last transthoracic echocardiogram (TTE) five years prior, chronic kidney disease stage (CKD) IV, and HIV on anti-retroviral therapy, had an episode of syncope in a restaurant. Prior to syncope, he experienced palpitations. The patient woke up, refused an ambulance and took a bus to the nearest emergency room (ER). In the ER, the patient was noted to be in a wide complex tachycardia (Figure A, B). The patient was initially given a trial of amiodarone bolus but was then cardioverted due to hypotension. The cardiology team was consulted. We reviewed patient’s serial electrocardiograms (ECGs), and we deemed findings consistent with AFIB with aberrant conduction over an accessory pathway, based on presence of RS complexes in all precordial leads, absence of concordance of QRS complexes, absence of capture beats or fusion beats, QRS in tachycardia being identical to sinus rhythm ECG and very irregular rhythm. The patient’s baseline labs revealed normal electrolytes and complete blood count; renal functions were at baseline. Transthoracic echocardiogram (TTE) was performed that showed now worsened severe tricuspid regurgitation and new moderately reduced left ventricular ejection fraction of 30-35% (Figure C). Coronary angiogram with minimal dye (30 mL) was pursued in favor of pharmacological myocardial perfusion imaging due to arrhythmic risk and showed no evidence of coronary artery disease (Figure D). On telemetry, the patient continued to have intermittent pre-excitation at rest. The electrophysiology team was consulted. Due to HFrEF, flecainide or propafenone were not feasible. Patient’s underlying prolonged QTc, CKD IV and interaction with antiretroviral (Odefsey) therapy precluded use of sotalol, dofetilide and amiodarone. Catheter ablation of accessory pathway was pursued for treatment of pre-excited AF. Patient underwent electrophysiology study and underwent technically challenging but successful ablation of three pathways, the right posterolateral, right posteroseptal and right anteroseptal. Patient on follow up has been referred for AFIB ablation, surgical correction for his adult congenital heart disease, and concern for worsening hemodynamics.
Discussion: This case is valuable as it highlights the need for aggressive care in adults with congenital heart disease. These patients are at higher risk of sudden death due to possibility of multiple accessory pathways, both concealed and manifest. Also, mapping and ablation of accessory pathways is difficult due to complex anatomic considerations. Arrhythmias are also a sign of worsening hemodynamics and progressive TR. When these combinations of findings are seen in a patient with Ebstein anomaly, patients should be referred for immediate advanced care.

P5. Hyperkalemia Masquerading as Acute ST-Elevation Myocardial Infarction
Gorgina H. Barsoum2,3, Muhammad A. Khan1, Talal Asif4,3
1 Internal Medicine, University of Kansas Medical Center, Kansas City, KS, United States. 2 University Health Truman Medical Center, Kansas City, MO, United States. 3 UMKC Health Sciences District, Kansas City, MO, United States. 4 Cardiology, University Health Truman Medical Center, Kansas City, MO, United States.
Case Report: History A 49-year-old man with a past medical history of human immunodeficiency virus infection and metastatic adenocarcinoma of the rectum, presented to the emergency department with delirium and decreased oral intake for three days. Work-up Initial ECG showed 3-4-millimeter ST-segment elevation with abnormal Q-waves in leads II, III and aVF (Figure panel A: blue arrows) consistent with acute inferior myocardial infarction. There was secondary ST-segment depression in leads I, aVL, V1-V3 (Figure panel A: orange arrows) together with diffuse intraventricular conduction delay concerning for associated posterior wall injury. Initial venous blood gas revealed a serum potassium level of 7.8 mEq/L (normal 3.5-5.0 mEq/L) confirmed on laboratory measurement as 8.8 mEq/L. Patient also had evidence of acute renal failure with serum creatinine of 16.5 mg/dL (baseline 0.9 mEq/dL). Bedside transthoracic echocardiogram showed an ejection fraction of 55-60% with no regional wall motion abnormalities. Final Diagnosis The ECG changes were deemed secondary to hyperkalemia and patient underwent emergent hemodialysis. Repeat ECG following hemodialysis showed complete resolution of the acute ST changes (Figure panel B).
Discussion: It is important to evaluate the entire clinical picture in patients with ST-elevations on electrocardiogram (ECG) who do not have typical ischemic symptoms, to provide appropriate and timely treatment.

P6. Infective Endocarditis After Transcutaneous Aortic Valve Replacement (TAVR): Highlighting the Need for Revised Antibiotic Prophylaxis Guidelines
Haidar Hajeh1, Vishal K. Narang1, Jesslin Abraham1, Theingi Win1
1 Department of Medicine, Kern Medical Center, Bakersfield, CA, United States.
Introduction: Infective endocarditis (IE) is a life-threatening infection of the endocardium. It is complicated by valvular abnormalities, perivalvular abscesses and heart failure. Due to the severity of this disease, prophylactic antibiotics are indicated in certain cases including the presence of a prosthetic valve.
Case Description: A 51-year-old female with history of severe aortic stenosis of bicuspid valve replaced with a prosthetic valve via Transcutaneous Aortic Valve Replacement (TAVR) 4 years ago, heart failure with improved ejection fraction, complete heart block (with permanent pacemaker) and hypertension who presented with 3 months of shortness of breath. Her symptoms started gradually with shortness of breath, lower extremity swelling and inability to lay flat. Diuresis was started and a transthoracic echocardiogram showed worsening of left ventricular ejection fraction (LVEF) from baseline of 55% to 25% in addition to severe stenosis and regurgitation of aortic valve with vegetations and valve dehiscence. It also demonstrated severe tricuspid regurgitation and vegetations on the atrial lead of the pacemaker. Blood cultures showed methicillin-resistant coagulase negative Staphylococcus. Vancomycin was started with plan for valve and pacemaker leads replacement. Patient endorsed that she underwent a dental procedure before her symptoms started and she was prescribed antibiotics for infective endocarditis prophylaxis before the procedure.
Discussion: Infective endocarditis is a well-documented sequelae of dental procedures with higher risk in prosthetic valves. Aortic valve replacement has seen revolutionary advancements in the past years with the innovation of TAVR. Valves used in TAVR are usually bulkier than those in Surgical Aortic Valve Replacement (SAVR). In addition, TAVR leaves the native calcified valve that is usually resected in SAVR. This theoretically creates a nidus for infections especially after dental procedures. Conclusion: TAVR can theoretically create a nidus for IE. Revision of the endocarditis antibiotic prophylaxis guidelines is warranted after the wide use of TAVR in medical practice.


P7. The Young-onset Stroke without a Medical History, but with an Interesting ECG Finding
Anthony M. Lim1, Jatin Thukral1, Harbir Kaur1, Julia Oberndorf1, Jonathan Ghazaleh1, Robert Cacdac1, Marrey Quizon1
1 Eisenhower Medical Center, Rancho Mirage, CA, United States.
Case Report: 19-year-old male with no medical history presented to emergency room with numbness and tingling in the right side of his face and right arm, with right leg weakness; he was also noted to have slurred speech and right side facial droop. He denied headache, blurry vision, recent trauma, or recreational drug use. Family history showed ischemic strokes in both grandparents (in age 70s); there were no strokes in family before age 55. Exam Vitals showed blood pressure of 124/73 mmHg, heart rate 81 beats/minute, respiratory rate 18 breaths/minute, temperature 36.9C, and SpO2 98% on room air. Neurological exam showed slurred speech and right side facial droop; power of right arm 3/5, left arm 5/5, right leg 4/5, left leg 5/5; sensory exam with diminished sensation of the right face; coordination exam with abnormal right side finger-nose test. Cardiac exam showed normal rate/rhythm, normal S1/S2 heart sounds, and no extremity edema. Investigations, management Imaging showed: CT head without contrast was negative for intracranial hemorrhage; CT head with perfusion and CTA head/neck with contrast did not show intracranial vessel occlusion. MRI brain without contrast showed acute left posterior frontal lobe infarct. Labs showed: Complete blood count showed WBC count 16.4 K/uL. Urine toxicology screen, coagulation studies PT/aPTT, comprehensive metabolic panel, erythrocyte sedimentation rate, C-reactive protein, HbA1c, troponin, homocysteine, protein C/S, Factor V Leiden, prothrombin gene, lupus anticoagulant were unremarkable. EKG showed normal sinus rhythm. There is subtle R wave notching in inferior leads III and aVF, with incomplete right bundle branch block pattern. Transthoracic echocardiogram showed normal LV size, normal LV wall thickness, normal LV systolic function and an EF of 50-55%. Bubble study detected an interatrial shunt. Transesophageal echocardiogram confirmed secundum type atrial septal defect, 6 x 7mm in diameter, located anterior/superiorly with small anterior/superior rims, with left to right shunt. National Institutes of Health Stroke Scale score was 7. Vascular neurology was consulted, and the patient was given tissue plasminogen activator (TPA) thrombolysis with resolution of neurological deficits. He started aspirin, clopidogrel, and atorvastatin 20mg daily 24 hours after TPA administration. In further follow-up, clopidogrel and atorvastatin were continued, and ASD closure was recommended.
Discussion: Young patients with cryptogenic strokes should be evaluated for intracardiac shunting and associated paradoxical embolization, and hypercoagulability. Intracardiac shunts are often asymptomatic due to their small sizes, and management in young patients often includes shunt closure. Particular attention to the ECG is warranted, especially with an incomplete right bundle branch block and inferior lead notching.

ECG from day 1 of admission showing sinus rhythm without ST segment or T wave changes. There is subtle R wave notching in inferior leads III and aVF, with incomplete right bundle branch block pattern.
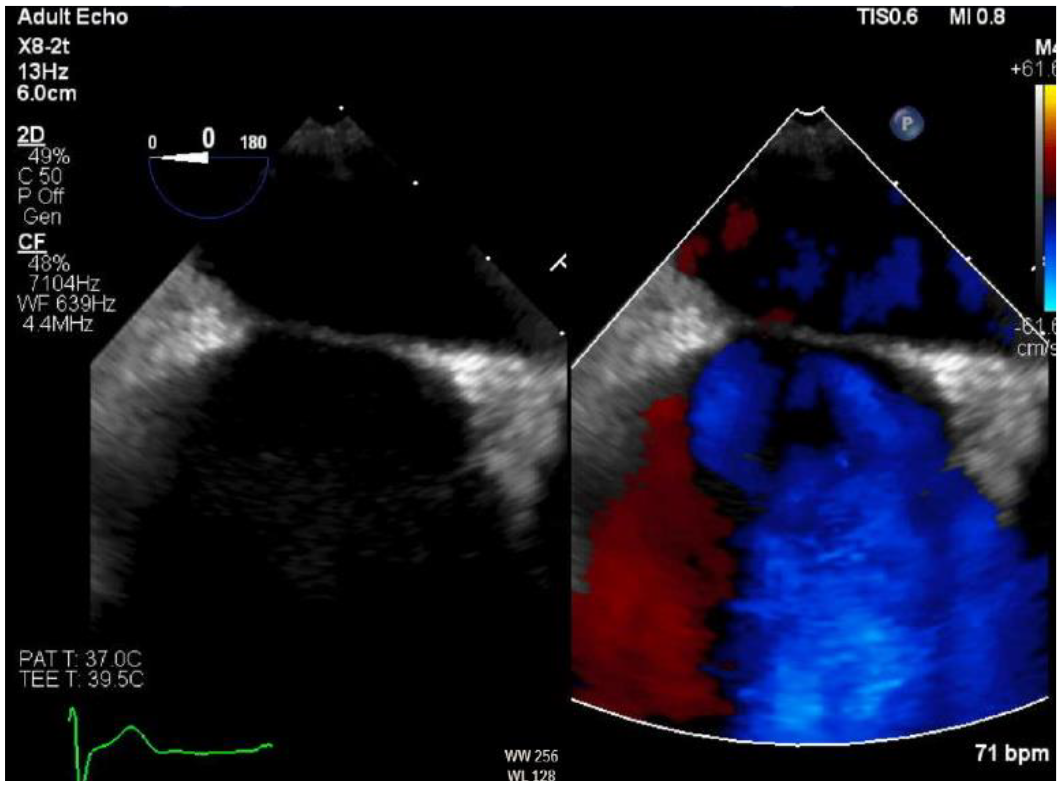
Transesophageal echocardiography from day 2 of admission showing interatrial left to right shunt.
P8. Understanding Hemodynamics of the Rare Quadricuspid Aortic Valve: A Case Report
Nicole Mamprejew1, Alex Ashkin1, Aleatha Reitsma1, David Axline1
1 NCH Healthcare System, Naples, FL, United States.
Introduction: A quadricuspid aortic valve (QAV) is an anomalous four-leaflet aortic valve, with incidence ranging from 0.006% to 0.043%. The QAV has been described by two classification systems. The Hurwitz and Roberts system recognizes seven subtypes, characterized by leaflet size. Subtypes A through C describe 85% of QAV phenotypes. The Nakamura system takes a simpler approach by classifying the QAV into 4 types based on placement of the supernumerary leaflet. The elusive nature of the QAV has resulted in little information on valve hemodynamics. Aortic regurgitation (AR) in QAVs is best described, as it is one of the most common complications. The mechanism hypothesizes that unequal shear stress upon the leaflets leads to their fibrosis which results in poor leaflet coaptation and poor valve closure. This mechanism is still unclear however, and with the different subtypes this begs the question of whether subtype affects valve hemodynamics.
Case Presentation: A 32-year-old male with no past medical history presented with fever, night sweats, cough with hemoptysis, and 20-25 pounds of weight loss over 2 to 3 months. He was diagnosed with Mycobacterium tuberculosis and initiated on appropriate therapy. The patient disclosed that in childhood he was told of a heart condition but was unaware of details. He denied chest pain, lower extremity edema, orthopnea, or palpitations. On physical exam, he was tachycardic with a regular rhythm, no murmur, jugular venous distention, or lower extremity edema. A transthoracic echocardiogram (TTE) revealed a Hurwitz and Roberts class D QAV, without AR. Left ventricular ejection fraction was 40-45% with moderately decreased global left ventricular systolic function. The aortic root, ascending aorta, right and left atria, and right ventricle were normal. Transesophageal echocardiogram was deferred due to active tuberculosis and no evidence of acute decompensated heart failure. The patient was discharged with outpatient cardiology follow-up.
Discussion: While a Hurwitz and Roberts class D QAV was identified in this patient, the valve appeared bicuspid when opened, with no complication of AR or aortic stenosis. Perhaps the varying leaflet sizes contribute to the valve orifice shape, with some subtypes more prone to bicuspid hemodynamics. It appears subtypes C through F have a more bicuspid shaped orifice, whereas A and B appear more amenable to a traditional opening of the valve orifice due to equally distributed leaflet sizes. The Tsang et al study concluded that subtype did not have influence on severity of AR, and ultimately further research will be needed to improve characterization of QAV hemodynamics. This highlights the importance of follow up TTE surveillance for the development or progression of valve dysfunction as a predictable pattern of progression for the different valve subtypes is not yet described.
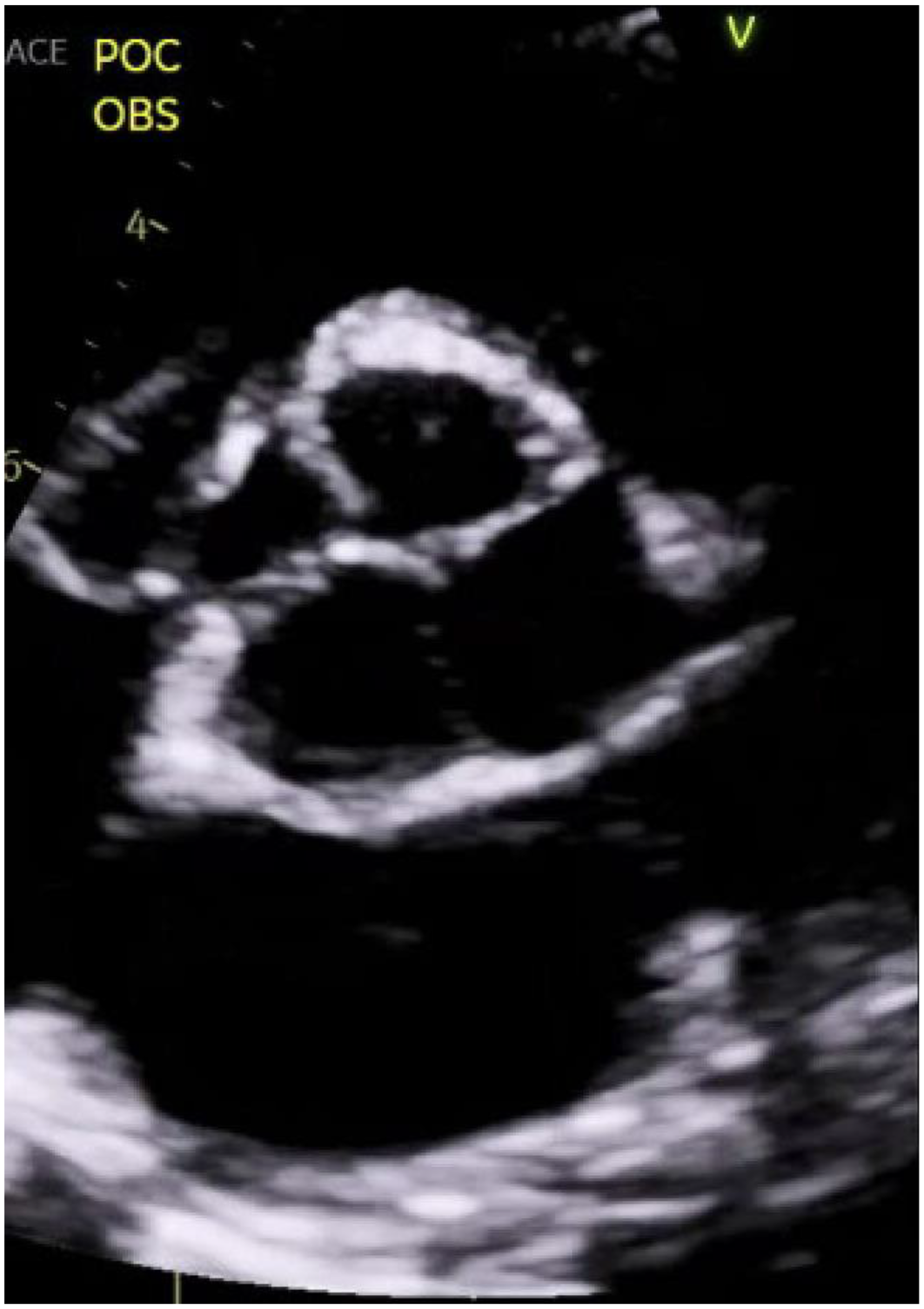
Quadricuspid aortic valve in the closed position with one large leaflet, two medium sized leaflets, and one smaller leaflet evidencing a Hurwitz and Roberts class D valve.

Quadricuspid aortic valve in the opened position with an orifice shape akin to that of a bicuspid valve.
P9. Electrophysiology Study to the Rescue: Type 1 Brugada Electrocardiogram with Unclear Syncope Etiology
Nicole Mamprejew1, Zackary D. Anderson1, Dhiran Verghese1, Samantha Sublette1
1 NCH Healthcare System, Naples, FL, United States.
Introduction: Brugada syndrome (BrS) is a hereditary arrhythmic disorder, classically presenting with syncope or sudden cardiac death. Its autosomal dominant inheritance is associated with the SCN5A gene, characterized by sodium channel inactivation. The prevalence is about 1 in 2000. Patients may have an electrocardiogram (ECG) with Brugada pattern without BrS if they have remained asymptomatic, meaning lack of ventricular tachyarrhythmias or cardiogenic syncope. Mortality risk remains high though, and a thorough workup of syncope and appropriate prevention of sudden cardiac death (SCD) is paramount.
Case Presentation: A 30-year-old male with a history of Brugada pattern ECG and an implanted loop recorder placed 27 months ago presented after syncopizing following hematochezia. On initial evaluation, he was hemodynamically stable, with a normal cardiopulmonary physical exam, and noncontributory labs. ECG evidenced type I Brugada pattern without sinus tachycardia. Loop recorder interrogation revealed sinus tachycardia with no arrhythmogenic events, concluding the syncope was vasovagal. However, through shared decision making given the patient’s young age, unclear risk for SCD, and familial concern, the patient proceeded for an electrophysiological study (EPS). Interestingly, ventricular tachycardia was induced during the EPS. A subcutaneous (SubQ) implanted cardioverter defibrillator (ICD) strategy was selected given the patient’s young age, with intention to mitigate heart failure, lead dislodgement, tricuspid regurgitation, and leaflet impingement over the long term. Furthermore, given the high risk for arrhythmogenic events during physical exertion, the patient underwent exercise screening to ensure the SubQ ICD could appropriately detect arrhythmias in the recumbent and standing positions, as well as during exercise on a treadmill. After confirmation of appropriate arrhythmia sensing capabilities, the patient was implanted with a SubQ ICD for primary prevention.
Discussion: BrS management is nuanced, with treatment strategies including conservative trigger avoidance, pharmacologic treatment, and radiofrequency ablation in refractory cases. Our patient experienced vasovagal syncope with a Brugada pattern ECG. However, he demonstrated inducible ventricular tachycardia on EPS, emphasizing the importance of an EPS in patients with unclear risks for SCD. The most crucial clinical decision in patients with a Brugada pattern ECG is the primary or secondary prevention of SCD with an ICD. Also, it is key to account for patient characteristics when selecting a traditional ICD versus SubQ ICD, especially in young, healthy patients where termination of a life-threatening rhythm allows them to continue a healthy lifetime, without the known complications of traditional ICDs. In closing this case highlights the importance of ascertaining syncope etiology, the utilization of EPS, and appropriate selection of ICD implantation strategy in young, healthy patients.
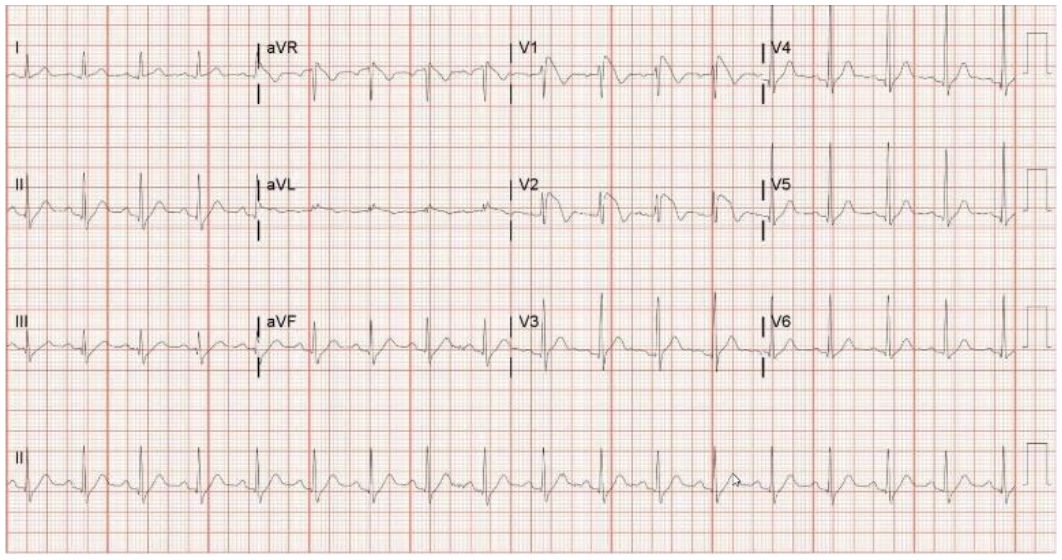
Electrocardiogram on admission evidencing Type I Brugada pattern.
P10. System-level Eligibility Criteria For Emergency Department Clinical Trial Enrollment During a Healthcare Crisis
Desiree Edemba3, Theresa Schultz3, Suvankar Majumdar4, Bobbe Thomas2, Sarah Isbey1, Gurydal Kalsi5, James Chamberlain1, Kenneth McKinley1
1 ER Physicians, Childrens National Hospital, Washington, DC, United States. 2 EMTC - Research, Children’s National Hospital, Washington, DC, United States. 3 Emerg Med Trauma Center, Children’s National Hospital, Washington, DC, United States. 4 Hematology, Children’s National Hospital, Washington, DC, United States. 5 Asklepion Pharmaceuticals, Baltimore, MD, United States.
Purpose of Study: Screening and confirming patient eligibility criteria are crucial preliminary steps before enrolling patients in a clinical trial, to ensure the appropriateness of the enrollment and to protect the safety of participants. As Emergency Department (ED) crowding has strained clinical resources, system-level eligibility criteria are also important to confirm before pursuing clinical trial enrollments, to ensure the safety of participants and the safety of other patients concurrently receiving care.
Methods Used: Using the same design as our L-Citrulline ED clinical trial patient eligibility form, we created a system-level eligibility checklist, based on high volume criteria that are routinely used in ED operations. We collected data from Cerner FirstNet patient tracking software to determine whether an eligible patient presented at a time that enrollment should be excluded based on system-level eligibility. We simultaneously developed a standardized process for "go/no-go" conversations between an investigator and a member of ED nursing leadership before each enrollment (Table 1). These conversations included structured exchange of information about the level of external resources available to assist with the ED clinical trial enrollment. A member of our team reviewed all safety event reports during the enrollment period for reports listing "citrulline", "clinical trial", or "research" in the event narrative.
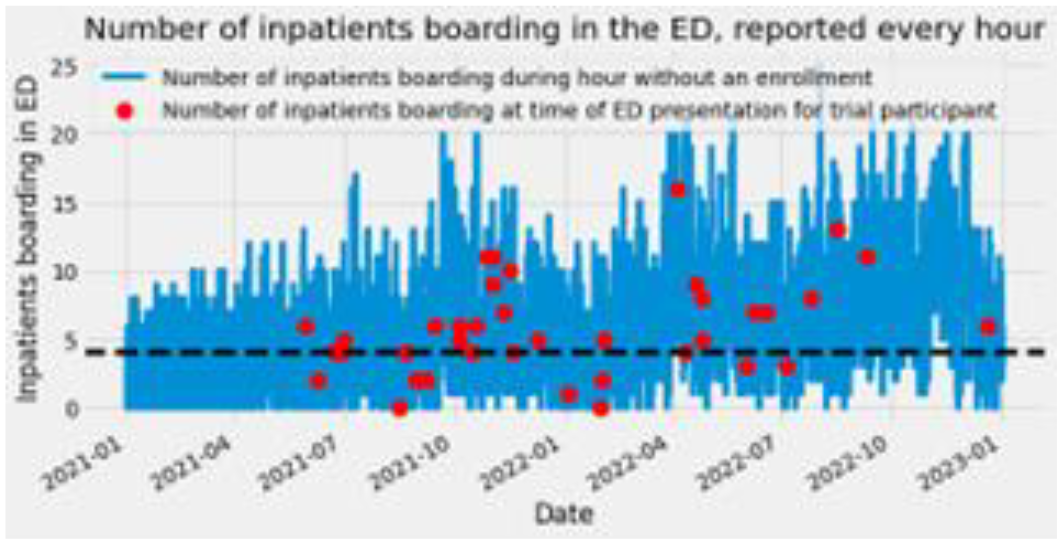
Criteria to determine the feasibility of green lighting an enrollment
Summary of Results: Despite high levels of system-level ineligibility, we were able to facilitate external support to safely enroll 40 patients in a phase 1/2 dose escalation clinical trial between 5/29/2021 and 12/28/2022. 31 enrollments occurred during a time when there was a system-level exclusion, but were made possible using additional, external resources. Eight enrollments occurred at a time during which the ED census would have been an exclusion, 30 enrollments when ≥4 acute care inpatients were boarding in the ED (Figure 1), three when ≥4 more critically ill patients boarding in the ED, and three when the wait time between triage and physician evaluation was >4 hours. There were no serious adverse events reported during the phase 1 safety trial and no institutional safety reports related to research on the day of any enrollments.
Conclusions: During periods of ED crowding, system-level and patient eligibility are both important considerations for enrollment in a clinical trial. A system-level eligibility checklist contributes to a shared mental model among team members, facilitating a safety-oriented “go/no go” conversation before each enrollment. Clear communication and pragmatic use of clinical resources, external to the ED, are equally essential to create a safe and effective clinical trials care model in the context of limited resources and ED crowding.

P11. Descriptive Statistics for Sickle Cell Patients Presenting to the Emergency Department (ED): A Comparison Study of Demographics Between Clinical Trial Participants and Non-Participants
Greta M. List1, Suvankar Majumdar1, Gurydal Kalsi2, Desiree Edemba1, Kenneth McKinley1
1 Children’s National Hospital, Washington, DC, United States. 2 Asklepion Pharmaceuticals, Baltimore, MD, United States.
Purpose of Study: Sickle cell disease (SCD) is a severe, chronic disease, causing multi-system dysfunction in children. The most common acute problem for children with SCD is pain crisis, leading to high emergency department (ED) utilization. Because there are no medications FDA-approved to specifically treat pain crises, clinical trials research is essential for this population. At our institution, there are multiple concurrent trials underway. Clinical trials require extensive inclusion and exclusion criteria to ensure it is safe for patients to try the study medication. For patients eligible to participate in these trials, the decision to consent is highly personal. It is not known whether eligibility criteria and patterns around consent decisions impact whether trial participants are representative of the overall population of SCD patients.
Methods Used: We performed a secondary analysis of clinical trial participants and non-participants 0-21 years old presenting to the Children’s National Hospital (CNH) ED in 2022 in SCD/pain crisis. We compared demographic and clinical characteristics between two groups: patients with SCD/pain crisis who participated in clinical trials in the CNH ED between January 1 and December 31, 2022 and patients with SCD/pain crisis who did not participate in clinical trials during the same period. Specifically, age, sex, zip code, and initial hemoglobin (Hb) levels were compared. Fisher’s Exact Test and T-tests were used to determine if any statistically significant differences exist between groups.
Summary of Results: In 2022, 308 unique patients 0-21 years old presented to the ED in SCD/pain crisis, of which 31 participated in at least one clinical trial. A retrospective analysis of these patients revealed similar breakdowns by biological sex between participants (51.62% female, n=16; 48.38% male, n=15) and non-participants (50.18% female, n=139; 49.82% male, n=138). Analysis of participants by age bracket (0-4; 5-9; 10-13; 14-17; 18-21) revealed over-representation of participation versus non-participation in 5-9 year olds (P=0.0389) and 18-21 year-olds (P=0.0394) compared to other age groups. Of note, 19.35% (n=6) of participants (Figure 1) and 12.64% (n=35) of non-participants (Figure 2) came from Southeast DC. Most participating and non-participating patients live in Southeast DC and Prince George’s County, Maryland, both of which are low median household income areas near CNH. Lastly, initial Hb values between participants (Mean 9.468, SD 1.945) and non-participants (Mean 9.147, SD 1.639) did not differ significantly (P=0.31).

Participants in CNH Clinical Trials by Zip Code
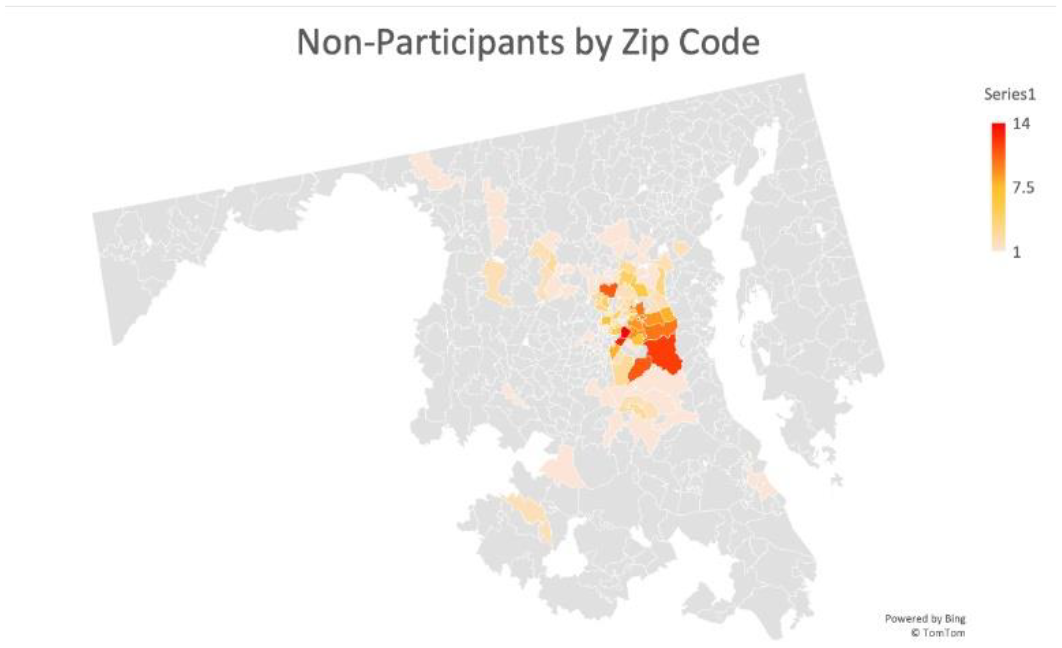
Non-Participants in CNH Clinical Trials by Zip Code
Conclusions: Retrospective analysis of 0-21 year old patients presenting to the CNH ED in SCD/pain crisis in 2022 did not reveal significant differences in demographic and clinical statistics of participating versus non-participating patients.
P12. Variability of Blood Glucose Readings: Concerns, Explanations and Pitfalls. The Impact of Collection and Processing Methods on Blood Glucose Results
Leia Kessler1, Welbeck Sowah1, Raquel Poliwoda1, Michael Puscaso1, Oana A. Sandu1
1 Albert Einstein College of Medicine, Bronx, NY, United States.
Purpose of Study: Blood glucose monitoring (BGM) is a vital aspect of diabetes diagnosis and management. However, the variability of results obtained from patient-derived blood supplies using different methods, such aswhole blood, plasma, and serum, has raised concerns. Moreover, some clinical trials have reported an unusualpattern of hypoglycemic events that may be related to internet-enabled blood glucose meters, emphasizing theneed to evaluate BGM system accuracy (Pfützner). The Federal Drug Administration (FDA) accuracy requirement is that 95% of all blood glucose values from the BGM are within 15% of the value measured by the lab instrument and that 99% of all blood glucose values from the BGM are within 20% of the value measured bythe lab instrument. In this study, we aimed to investigate the discrepancy in blood glucose levels obtained using a glucose finger stick blood test and those drawn in vacutainer blood collection tubes and processed in-house or sent out for testing.
Methods Used: We conducted a review of observational studies and secondary data to explore the reason for the variability of blood glucose readings obtained from different measurement methods. We searched PubMed for original articles that reported variations in BGM.
Summary of Results: Our review revealed that glucose readings can be significantly affected by collection and processing methods, in addition to clinical factors (hypoxia, hypotension, blood pH, hematocrit) including the amount of blood collected, enzymatic reactions, shelf life. Temperature variations and electromagnetic influences are other common recognized pitfalls. Notably, in a clinical trial, 12.8% of BGM devicesdid not meet the international standard and 23.1% did not meet the standard acceptance criteria according tothe FDA guidelines . Laboratory results obtained from serum separated within 20 minutes from the collectionshowed significantly higher values in comparison with plasma obtained from sodium fluoride grey top tubes. Glycolysis can decrease glucose levels by 5-7% per hour in the first 4 hours (Turchiano). Glucose-specific tubescontaining NaF/KOx, citrate, and EDTA (Dimeski) and placing the samples in ice have been proposed to minimize glycolysis (Sacks).
Conclusions: Our study highlights the need for clinical staff and investigators to be aware of the variability of blood glucose readings obtained from different collection and processing methods. Better guidelines related to the practical use and interpretation of laboratory tests are warranted. There is need for more advanced and accurate tools and blood collection methods to ensure accurate glucose readings. Further research should focus on developing and validating improved BGM methods to enhance diabetes management.
P13. Quality Analysis of Patient Educational TikTok Videos For Knee Instability
Brandon D. Rust1, Jashkumar Choudhari1, Elie Christoforides1, Jackson Copper1, Aidan Kaspari1, Vijay Patel1, Santiago Ortiz1, Desiree Ojo2, Khavir Sharieff1
1 College of Osteopathic Medicine, Nova Southeastern University, Fort Lauderdale, FL, United States. 2 School of Osteopathic Medicine, University of Incarnate Word, San Antonio, TX, United States.
Purpose of Study: To characterize the quality of TikTok knee instability videos as a source of patient information using the DISCERN instrument and KEEST (knee exercise scoring tool).
Methods Used: TikTok was searched on June 20, 2023, with the phrase “knee stability exercises”. The search yielded 448 relevant videos. An initial screen for exclusion was performed to eliminate videos with no relation to the topic or no educational component. A DISCERN scale was used to assess content quality. A knee exercise education scoring tool (KEEST) was developed to evaluate the educational suitability of each video. The KEEST grade scale is scored between 0 and 5 with increasing scores demonstrating higher quality. The sum of all five graded items is the final KEEST score (0 to 25, with scores of 0 representing the lowest possible quality and scores of 25 representing the highest possible quality). Score variations based on video sources were analyzed using Statistical Package for Social Sciences (SPSS).
Summary of Results: A total of 187 videos met the inclusion criteria. 69.84% (n=132) were produced by general users and 29.1% (n=55) were produced by healthcare professionals. DISCERN scores of videos uploaded by general users had significantly lower scores in all four categories than those uploaded by healthcare professionals (P = < 0.001, P = 0.282, P = 0.131, and P = 0.010). The overall total DISCERN score was inversely correlated with the total number of views, likes, comments, favorites, and shares. General users’ videos were graded as very poor (27.2%), poor (39.2%), fair (23.5%), good (9.7%), and excellent (0.0%). In comparison, the number of videos uploaded by healthcare professionals was deemed very poor (20%) poor (40.9%), fair (28.2%), good (9.1%), and excellent (1.8%). Per the KEEST, both content from general users (12.31) and healthcare professionals (12.18) were of average quality (P = .809) with no significant difference between the two groups.
Conclusions: The current most popular knee instability videos on TikTok are of low quality, while these videos provide information on how to perform the exercise, very few content creators will provide sources for their information, risks of treatment, and how the treatment works. Furthermore, our study found an inverse correlation between video popularity, as measured by the number of views and the DISCERN score. Low-quality videos were more popular compared to their higher-scoring counterparts. There is a difference between the ability of general TikTok users and healthcare professionals to provide evidence-based information (measured with the DISCERN tool), however, the exercises provided are comparable in their ability to educate on a treatment plan and its intended effect (measured with the KEEST tool).
P14. Rapid Growth of Burkitt Lymphoma causing Partial Small Bowel Obstruction
Zackary Anderson1, Alex Ashkin1, Leslie Raymond1
1 Naples Community Hospital, Naples, FL, United States.
Introduction: Burkitt lymphoma is a rare but aggressive B-cell malignancy accounting for approximately 1-5% of all non-Hodgkin lymphomas. Burkitt lymphoma is caused by chromosomal translocations resulting in overexpression of the c-myc oncogene and can present in either the endemic or sporadic form. The sporadic form typically presents in adults with an average of 45 years of age with a predominance in Caucasian males. The sporadic form of Burkitt commonly presents with constitutional symptoms including fever, weight loss, and night sweats. The primary location is within the abdomen, often resulting in nausea, vomiting, abdominal distention and gastrointestinal bleeding. In severe cases, the rapid tumor growth can result in intestinal obstruction requiring immediate intervention. This is a case of rapidly progressing sporadic intrabdominal Burkitt lymphoma presenting as a bowel obstruction.
Case Presentation: A 63-year-old male with a past medical history of hypertension presents with constipation and bloating over a 2-week time period. The patient had a colonoscopy performed 2 months prior, showing only a nonmalignant polyp. CT abdomen showed a large 14.4 x 12 x 14 cm irregular thickening with a heterogeneous mass involving the distal rectum, cecum and ascending colon concerning for neoplasm. In the setting of a worsening abdominal exam, early precautions were initiated to prevent complete small bowel obstruction. The patient was started on aggressive bowel regimen and pathology results were gathered. We were able to prevent any surgical intervention as we awaited pathology reports due to initiation of noninvasive measures. The pathology findings were suspicious for Burkitt lymphoma (c-Myc+, Bcl-2-). The patient was started on modified EPOCH-R chemotherapy and followed up in the outpatient setting.
Discussion: Burkitt Lymphoma is an uncommon form of non-Hodgkin’s lymphoma with a tendency for rapid growth. Symptoms can progress quickly over weeks to months. Albeit an unusual cause of small bowel obstruction, malignancy should remain on the differential for a potentially reversible etiology. Biopsy with pathologic evaluation is essential for diagnosis and treatment. In the setting of high Ki-67 finding suspicious for Burkitt lymphoma, the treatment of choice is etoposide phosphate, vincristine sulfate (Oncovin), cyclophosphamide, and doxorubicin hydrochloride (EPOCH-R). In the setting of Burkitt, studies in pediatric populations demonstrated limited evidence for resection of early, limited ileocecal and mesenteric involvement. Our patient never had a surgical abdomen warranting an exploratory procedure and had extensive nonresectable involvement. The early onset and subsequent detection of disease processes played a key role in prognosis and management. This case further demonstrates the aggressive progression of lymphomas and emphasizes the importance of initiating chemotherapy to achieve a favorable prognosis.

CT Abdomen: Demonstrating diffuse tumor burden and omental thickening and ascites.
P15. The use of Darbepoetin Alfa in a Term Neonate for Anemia Refractory to Transfusion
Catherine Arcara1, Riya Raju1, Melissa Micallef1, Rafat Ahmed1
1 The Children’s Regional Hospital at Cooper, Camden, NJ, United States.
Background: Neonates with anemia are traditionally treated with packed red blood cell (pRBC) transfusions. However, when the problem is from low erythropoietin (EPO) levels or bone marrow suppression, the use of EPO stimulating agents (ESA) should be considered. Darbepoetin Alfa (DA) is a long acting ESA that is given subcutaneously every 1-2 weeks. DA has been used in preterm infants with anemia, and older children receiving chemotherapy or with chronic kidney disease. However, experience with DA in term neonates with late-onset anemia due to Rhesus Hemolytic Disease is limited.
Objective: To describe the use of DA in a neonate with severe hemolytic anemia secondary to Rh incompatibility refractory to transfusions and intravenous immunoglobulin (IVIG).Methods Used: Method: A female infant born at 37 weeks was found to have fetal anemia due to Rh isoimmunization with Anti C, D, and M antibodies, and received intrauterine transfusions of pRBCs x4. On day of life (DOL) 1, laboratory tests revealed hemolytic anemia with direct hyperbilirubinemia, thrombocytopenia, and significantly elevated ferritin levels. The infant received pRBCs x3, platelet transfusions x4, fresh frozen plasma x2, IVIG x3, and phototherapy (x2 days) in her first few weeks of life. The neonate continued to have low hemoglobin and low EPO levels, and was given two doses of Epogen before being transitioned to DA on DOL 32.
Summary of Results: Infant received 3 doses of DA 10 mcg (4 mcg/kg) a week apart with the last dose on day of discharge. Hemoglobin levels improved and remained stable, EPO level increased, and ferritin level continued to decrease. There were no adverse effects or need for additional transfusions. Patient continues to do well on outpatient follow-up with stable laboratory results.
Conclusion: DA is an appropriate treatment choice for term neonates presenting with anemia refractory to transfusions. DA might even be preferred over Epogen as it only needs to be given once every 1-2 weeks instead of every other day. More research needs to be conducted in regards to its safety and efficacy.
P16. Synchronous and Metachronous Manifestations of Cancer in a Patient with BRCA2 Mutation
Aiwu Ruth He1, Priya Goyal1
1 medstar georgetown university hospital, Dc, DC, United States.
Case Report: We report a case of a 73-year-old male with a family history of cancers who underwent left high inguinal orchidectomy in 2009, for Diffuse large B-Cell lymphoma and received RCHOP-based chemotherapy, prophylactic radiation to the contralateral testis and intrathecal methotrexate. The patient was in remission till 2019 when he developed abdominal pain and features of obstructive jaundice. Further, the workup revealed common bile duct obstruction resulted from a 2 x 2 cm mass at the head of the pancreas, additionally there is a 2.7 x 2.6 cm liver lesion found in segment 7. Biopsy of pancreas tumor showed ductal adenocarcinoma while biopsy of the liver lesion showed intermediate grade HCC, IHC stain demonstrated immunoreactivity with Arginase 1, HepPar-1, CK 8 and 18. Polyclonal CEA revealed the canalicular pattern of the tumor. Patient is determined to have synchronous pancreas cancer and hepatocellular carcinoma. He underwent a simultaneous Whipple procedure and right posterior sectionectomy of the liver. Surgical pathology of the Whipple specimen resulted in moderately differentiated pancreatic ductal adenocarcinoma (pT3N2Mx). A partial hepatectomy specimen yielded poorly differentiated hepatocellular carcinoma (pT2NxMx). Molecular profiling from the pancreatic tissue demonstrated BRCA2 mutation. The patient received 10 cycles of Adjuvant FOLFIRINOX, Patient was found to have newly enlarged mediastinal lymphadenopathy in 08/2021. Biopsy of the enlarging lymph nodes in 1/2022 confirmed the metastatic recurrent pancreas cancer; he received 3 months of Gemcitabine /Abraxane followed with 20 cycles of radiation treatment with concurrent capecitabine treatmentwith a complete response. Patient has been off treatment with active surveillance since 06/2022.ctDNA test was negative as of 11/3/2022. Most recently, he presented in the neurology clinic with severe headaches, right shoulder pain, weakness, and gait instability. His cervical spine MRI showed increased signal from C2-C7, and the MRI brain showed signal abnormality of the splenium of the corpus callosum, with restricted diffusion and enhancement, suspicious of lymphoma. Flow cytometry of spinal fluid showed approximately 32% of the total cells were CD19, CD20, and CD10-positive monoclonal B-lymphocytes consistent with involvement by diffuse large B-cell lymphoma of follicular origin. The patient is planned to receive intrathecal Methotrexate and Rituximab. This case demonstrates a management dilemma of less frequent pancreatic/liver cancer and two lymphomas. The occurrence of multiple malignancies and responsiveness to treatment which led to better than average outcome in 2 lethal solid tumors (recurrent metastatic pancreas cancer and HCC) raises the possible genetic predisposition to cancer and genetic factors contribute to the improved outcome of this patient. Patient’s pancreas cancer carries BRCA2 mutations. Additional germline genetic test will be proposed to this patient.
P17. Unusual Presentation of Hodgkin Lymphoma as Superior Vena Cava Syndrome, Horner’s syndrome and Eosinophilic Pleural Effusion
Akbar Hussain1, Sai Subramanyam1, Dedeepya Gullapalli1, Shyam Ganti1, Kamlesh Sajnani1
1 Internal Medicine, Appalachian Regional Healthcare, Harlan, KY, United States.
Case Report: Hodgkin’s lymphoma (HL) was first described an autopsy case series of patients with lymphadenopathy and splenic enlargement, later it was found to be a malignancy arising from the germinal or post germinal B cell centre. Classic Hodgkin’s lymphoma (CHL) comprises 95% of all HL cases. We are presenting a case of HL with eosinophilic predominance (41.7%) in the cell line along with the dominance in pleural fluid analysis and Superior Vena Cava Syndrome and Horner’s syndrome. In the literature on adults, HL-associated SVC syndrome is rare(2%). A 52-year-old man with past medical history of CKD, chronic pruritus, hepatitis B (treated), IV drug abuse (clean for 8 years) presented with progressive cough and shortness of breath for 8 months. He denied history of cigarette smoking. Patient reported right sided facial anhidrosis, dizziness and syncopal episodes. On physical examination, he had right eye miosis and ptosis, prominent veins in neck and chest. Review of labs showed eosinophilia. Ruled out other eosinophilic dominant conditions. Peripheral blood smear showed marked eosinophilia with no circulating blasts. Chest X ray showed right perihilar and suprahilar density. CT scan of chest showed 10.5 x 8.6 x 18.7 cm mass involving the right aspect of the mediastinum which narrowed and surrounded the adjacent vasculature, enlarged perivascular lymph nodes measuring up to 14 mm, and moderate right pleural effusion. PET scan showed hypermetabolic right mediastinal mass and hilar lymph nodes. Right thoracentesis which showed eosinophilic dominance, endobronchial ultrasound with fine needle aspiration, transbronchial biopsy. EBUS was positive for CD15 and CD30. Bone marrow aspirate showed marked eosinophilia (31%). CT guided core biopsy of the mediastinal mass showed Classic HL with rare, atypical cells, prominent nucleoli with rare binucleated form with CD 30 being positive. Patient showed significant improvement on chemotherapy. HL can manifest in various atypical ways making the diagnosis challenging. HL presenting with Superior Vena Cava Syndrome is unusual [2%]. eosinophilia is seen in 15% patients of HL with eosinophilic pleural effusions very rare. The case highlights the importance of considering HL in differential diagnosis when encountering patients with Superior Vena Cava syndrome, particularly in the absence of primary lung malignancy, with multidisciplinary approach involving oncology, radiology, and pathology for accurate diagnosis and management.


P18. “Viscous Ascites and the Jelly Belly” - Fishing for an Unknown Primary Tumor
Anthony M. Lim1, Jatin Thukral1, Harbir Kaur1, Julia Oberndorf1, Jonathan Ghazaleh1, Robert Cacdac1, Marrey Quizon1
1 Eisenhower Medical Center, Rancho Mirage, CA, United States.
Case Report: 66-year-old female presents with progressive abdominal heaviness and refractory constipation for 6 months. She has no previous malignancies. She was following with her primary care and gynecology-oncology physicians since 6 weeks prior to admission. Exam Vitals showed blood pressure of 137/97 mmHg, heart rate 118 beats/minute, respiratory rate 18 breaths/minute, temperature 37C, and SpO2 99% on room air. Abdominal exam revealed signifcant distension with mild generalized tenderness. Investigations, management Labs on day 1 showed: WBC count 11.3 K/uL, albumin 2.9 g/dL, normal transaminases. Ultrasound on day 1 at bedside showed loculated ascitic fluid. MRI abdomen pelvis on day 5 showed large volume fluid with many internal septations likely associated with a multiseptated cystic right adnexal mass seen on ultrasound pelvis 2 weeks prior. There was no suggestion of a tumor within/adjacent to the appendix. Paracentesis was attempted twice, 2 and 4 weeks prior, but failed due to the fluid’s “thick, viscous, jelly-like consistency.” Thus, analysis and cytology were not performed. Serum tumor markers obtained 3 weeks prior showed: normal AFP < 1.8 ng/mL, elevated CA19-9 68 U/mL, elevated CEA 468 ng/mL, elevated CA125 117 U/mL. “Risk of Ovarian Malignancy Algorithm” (ROMA) was obtained on day 19 and showed elevated ROMA postmenopausal 7.97 units, elevated CA125 90 U/mL, elevated HE4 375 pmol/L. Last colonoscopy was done 4.5 years prior, and showed a submucosal non-obstructing mass in the appendiceal orifice. Repeat colonoscopy was ordered but the patient did not follow-up. On day 11, diuresis was attempted with intravenous furosemide, and then changed to bumetanide infusion, which was not efficacious. The patient was transferred to a tertiary care hospital. Upper endoscopy revealed a duodenal tubular adenoma and no esophageal malignancy. Paracentesis was re-attempted and yielded only 55mL of thick, cloudy, yellow, mucinous fluid. Cytology showed abundant mucin with histiocytes. Abdominal laparoscopy was performed and 14 liters of mucinous material was removed. Palliative debulking resulted in removal of 30cm mass with the right fallopian tube and ovary, and appendix removal. Final tumor pathology was reported as 4.7cm low-grade appendiceal mucinous neoplasm, with visceral peritoneum invasion, staged pT4a Mb.
Discussion: The patient’s difficult fluid sampling due to “thick and viscous” fluid sampling, unknown primary tumor, point to the very rare pseudomyxoma peritonei entity. While imaging may commonly reveal disease in the appendix or right lower quadrant, there are times when the primary tumor is hard to determine. In our case, imaging did not detect appendiceal tumor, but surgical biopsy confirmed appendiceal tumor. Clinicians should be highly suspicious, especially in the case of repeated failed paracentesis and other biopsy attempts.
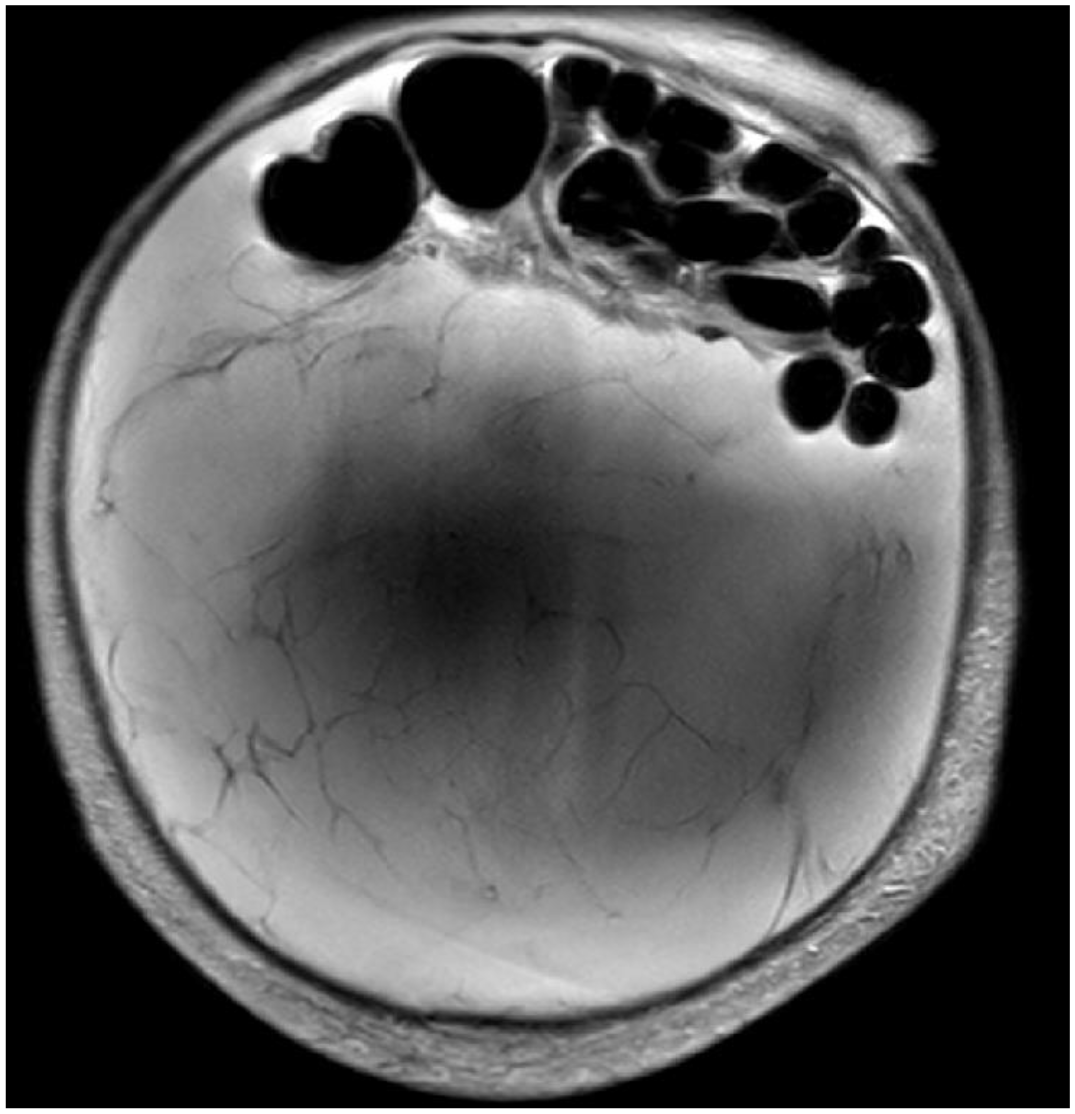
MRI abdomen pelvis on day 5 showing large volume ascites with numerous internal septations.
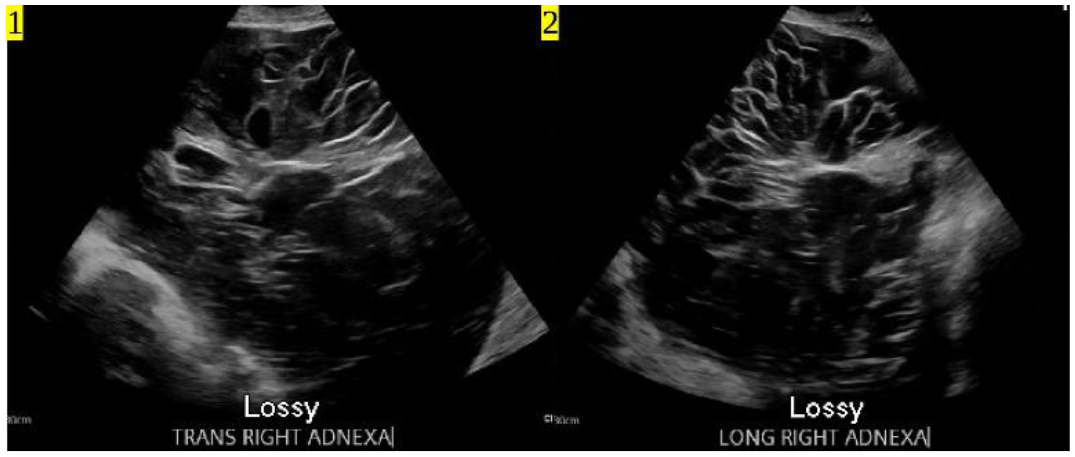
US pelvis 2 weeks prior showing right adnexal mass in right adnexa extending up to the abdomen, with large volume ascites. Views 1) trans, 2) long.
P19. Poliosis in Patients with Cutaneous and Non-Cutaneous Melanoma Treated with Cancer Immunotherapy
Kimberly Smart1, Mark S. Swanson4, Jesse L. Berry3, Alicia Terando6, David H. Peng5, Gino K. In1,2
1 Keck School of Medicine, University of Southern California, Los Angeles, CA, United States. 2 Division of Oncology, University of Southern California, Norris Comprehensive Cancer Center, Los Angeles, CA, United States. 3 USC Roski Eye Institute, Keck School of Medicine, University of Southern California, Los Angeles, CA, United States. 4 Department of Otolaryngology, University of Southern California, Los Angeles, CA, United States. 5 Department of Dermatology, Keck School of Medicine, University of Southern California, Los Angeles, CA, United States. 6 Department of Surgery, Division of Surgical Oncology, Cedars-Sinai Health System, Los Angeles, CA, United States.
Purpose of Study: While prior studies have described the development of vitiligo and alopecia among patients with metastatic melanoma undergoing cancer immunotherapy, there are scant reports regarding the development of secondary poliosis. Here we detail a case series of patients with both cutaneous and non-cutaneous melanoma who developed poliosis secondary to cancer immunotherapy.
Methods Used: We reviewed a clinical database of melanoma patients treated at the University of Southern California, Norris Comprehensive Cancer Center from 2018–2023, to identify patients who developed poliosis during cancer immunotherapy treatment. Patients with both cutaneous and non-cutaneous melanoma (acral, uveal and mucosal) were included. Cancer immunotherapies included checkpoint inhibitors, bispecifics, and tumor infiltrating lymphocyte (TIL) therapy. Patient characteristics, tumor features (histology, stage), treatment variables, and clinical outcomes were collected for all patients. Immunotherapy-related side effects, including poliosis, were recorded.
Summary of Results: A total of 9 melanoma patients with poliosis were identified, including 5 (56%) women and 4 (44%) men; there were 7 (78%) Caucasian patients and 2 Asian (22%); 7 (78%) had stage IV disease. Histology subtypes included 5 (56%) uveal melanoma, 3 (33%) cutaneous melanoma, and 1 (11%) acral lentiginous melanoma. Cancer immunotherapies included 5 (56%) patients treated with PD-1 blockade, 4 (44%) treated with a TCR/CD3 bispecific fusion protein targeting gp100 (tebentafusp), 1 (11%) with CTLA-4, 1 (11%) with TIL. The median duration of immunotherapy treatment was 12 months (range 4–24). The majority (89%, 8/9) experienced immune-related adverse effects, including rash (66%), fatigue (56%), pruritis (44%), vitiligo (11%), and alopecia (11%). Median onset of poliosis was 4 months (range 2–12). Median onset of non-poliosis adverse events was 1 month (range 0.25–11). Amongst the 9 patients, all (100%) remain in continued response to treatment without disease progression at this time.
Conclusions: This case series describes our experience with melanoma patients who developed poliosis while undergoing immunotherapy, all who developed clinical benefit from treatment. Of note, this cohort included patients with rare and challenging melanoma subtypes, e.g., acral lentiginous and uveal melanoma. Furthermore, our study encompassed patients treated with adoptive cellular therapy and bispecific T-cell targeting agents, in addition to checkpoint blockade. Intriguingly, the development of poliosis may portend a positive clinical benefit from these immunotherapy treatments. Further research is necessary to elucidate the underlying mechanisms of immune-mediated melanocyte destruction and depigmentation in melanoma patients receiving immunotherapy.
P20. Reasons for Physical Therapy Non-treatment in Patients with Functional Impairment during Hospitalization for Medical Illness
Mahnoor Baig2, David Young1, David Meltzer2, Maylyn Martinez2
1 University of Nevada, Las Vegas, Las Vegas, NV, United States. 2 University of Chicago, Chicago, IL, United States.
Purpose of Study: We aimed to identify the volume of and reasons for missed physical therapy (PT) sessions, also known as PT nontreatment, in patients hospitalized for acute medical illness.
Methods Used: We conducted a retrospective analysis of patients admitted to the University of Chicago Hospital’s medical services between 8/2018 - 3/2021. We limited our cohort to patients ≥ 65 years old, with a length of stay of 7-10 days. We focused on patients likely to need physical therapy, based on an Activity Measure Post-Acute Care (AM-PAC) mobility assessment scores of ≤ 18 at the time of admission, indicating functional impairment. The main outcome measures were the number of missed PT sessions and the reasons for missed PT sessions. We coded reasons for missed sessions as: 1 = patient declined due to symptoms/ condition, 2 = patient declined for non-medical reasons, 3 = patient gone for imaging/treatment/busy with healthcare providers, 4 = therapist deferred due to patient condition, 5= no PT needed, and 6 = other. If a missed session was completed later the same day this was noted. Descriptive statistics were used to assess the frequency and proportions of reasons for PT non-treatment.
Summary of Results: Charts for 885 patients were reviewed based on eligibility criteria. The average length of stay was 8.1 days, and patients completed an average of 2.4 PT sessions per hospitalization. In total, 2,100 PT sessions were completed including missed sessions that were completed later on the same day. Excluding sessions that were missed and then completed the same day, 22.0% of PT sessions were missed without same-day completion. The most common reason for missed PT sessions was “therapist deferred due to patient condition” (38.6%) followed by “patient gone for imaging/treatment/busy with healthcare providers” (27.5%), “patient declined for non-medical reasons” (14.9%), “patient declined due to symptoms/ condition” (8.4%), and “other” (5.5%). Sessions were not completed due to the therapist deeming treatment unnecessary in 5.2% of cases. The percentage of missed consultations that were completed later the same day was 0.8%.
Conclusions: Our study demonstrates that nearly one-quarter of PT sessions scheduled for hospitalized patients never occur. More than 30% of these missed sessions are potentially avoidable with the implementation of quality or process improvement interventions. Educating patients on the importance of PT, improving ordering provider knowledge of what constitutes the need for PT, and coordinating patient scheduling between all providers could optimize the use of PT time and facilitate the completion of PT sessions, which may reduce the development of HAD in patients with functional impairment on admission.
P21. Human Microglia Polarization Following Infection With the Lyme Disease Spirochete
Brian J. Kan1, Idris Akinlusi1, Carlos Bouchot1, Ted Shi1, Jose Barragan1, Jorge Cervantes2
1 PLF School of Medicine, TTUHSC El Paso, El Paso, TX, United States. 2 College of Allopathic Medicine, Nova Southeastern University, Fort Lauderdale, FL, United States.
Purpose of Study: Lyme disease is known to be caused by the spirochete Borrelia burgdorferi, with a reported incidence rate of 30,000 cases a year. The human host immune response works to clear the infection. Within the central nervous system (CNS), microglia phagocytose the bacterium, mediate inflammation, and elicit an immune response towards the spirochete. Microglia are an integral part of the central nervous system’s innate immune response. Like other tissue macrophages, it can polarize into two different modulatory phenotypes, M1 and M2. In a subset of patients, however, infection spreads and causes CNS involvement, known as neuroborreliosis. Here, we seek to explore human microglial polarization changes upon infection with B. burgdorferi.
Methods Used: HMC3 human microglia cell line was infected in vitro with B. burgdorferi at a multiplicity of infection (MOI) of 10:1 for 24 hours. Expression of microglia polarization markers was evaluated via flow cytometry at 4 and 24 hours. Secreted immunological mediators were evaluated using a multiplex ELISA system at 4, 18, and 24 hours.
Summary of Results: Flow cytometry evidenced a decrease in expression of M1 polarization marker iNOS and CX3CR1 at 4 hours, and 24 hours, respectively. There were no changes in expression of M1 markers CD14, or in M2 markers CD163 and CD206. Multiplex ELISA evidenced an increase in secretion of activation markers MIP-1α, MIP-1β, IP-10, chemotactic factor MCP-1, M1 polarization cytokine IL-8, and VEGF, at 4, 18, and 24 hour marks.
Conclusions: Our results show that human microglia M1 polarization does not completely occur at their earliest encounter with B. burgdorferi. A decrease of iNOS at 4 hours of infection suggests a diminished production of reactive nitrogen species that are a critical component of innate defense against infection. At 24 hours, B. burgdorferi suppressed the expression of chemokine receptor CX3CR1, which has shown to be a neuroprotective molecule from its function of regulating microglia recruitment to neuroinflammation. The dynamics of major inflammatory cytokines and other mediators appear to be important in the microglial response to B. burgdorferi should be further studied as these could become therapeutic targets in the acute inflammatory process of neuroborreliosis.

Flow Cytometry

ELISA
P22. Cryptammonia: A Retrospective Study on the Association Between Cryptococcal Infections and Hyperammonemia
Sheetal Kandiah1, rosanna baker2, maria M. schachter4, steven phillips5, mirza farrque7, arturo casadevall6, Prem Kandiah3
1 infectious diseases, emory, Atlanta, GA, United States. 2 microbiology and immunology, johns hopkins, Baltimore, MD, United States. 3 neurology, emory, Atlanta, GA, United States. 4 Neurology, emory, Atlanta, GA, United States. 5 Neurology, University of Nebraska, Omaha, NE, United States. 6 microbiology and immunology, Johns Hopkins University, Baltimore, MD, United States. 7 Vital Statistics, Tennessee Department of Health, Nashville, TN, United States.
Background: Hyperammonemia caused by urease producing organisms can result in life-threatening neurological injury. Cryptococcus neoformans and gattii are both known to produce urease which can serve as a virulence factor. The aim of our study is to investigate the association between renal failure and hyperammonemia among patient with Cryptococcal infections.
Methods: We performed a retrospective record review using data from the Emory data warehouse between 2013 to 2022. Patients with positive blood or CSF Cryptococcal cultures and concomitant plasma ammonia levels within 7 days of the culture were included. Two groups were compared based on the presence of hyperammonemia (>53 µmol/L). e group had Cryptococcal infection and hyperammonemia, and a comparison group with Cryptococcus infection without hyperammonemia. We used Wilcoxon rank-sum, Fisher’s exact, Kruskal-Wallis, Dunn’s pairwise comparison with Bonferroni adjustment, and Spearman’s correlation tests to determine risk factors for hyperammonemia which included liver failure, initial Cryptococcal titers, disseminated Cryptococcal infections (DCI), and admission creatinine.
Results: Our review of medical records identified 29 patients, of whom 37.9% had hyperammonemia, 59% had DCI, and 41% had isolated Central nervous system (CNS) Cryptococcal infection (CNS-CI). 38% of patients had renal failure and 28% had liver disease. Renal failure was associated with 3.82 times (95% CI 1.24, 11.77) higher risk of hyperammonemia. There was a moderate correlation between ammonia levels and admission creatinine (Spearman Rho 0.40; p=0.03). The combined risk ratio for hyperammonemia from renal failure and DCI was 4.0 (0.85 -24.72) followed by 3.0 (0.53-16.90) from renal failure with both DCI and CNS-CI when compared patients without renal failure. The small sample size precluded assessment of co-linearity between liver failure and renal failure. No association was found between hyperammonemia and liver failure or Cryptococcal titers.
Conclusion: There is an association between elevated plasma ammonia levels and Cryptococcal infections. Risk factors for hyperammonemia may include renal failure, disseminated Cryptococcosis and increased urease production unique to the Cryptococcal strain. A prospective study looking at clinical implications of hyperammonemia in Cryptococcal infections is warranted.
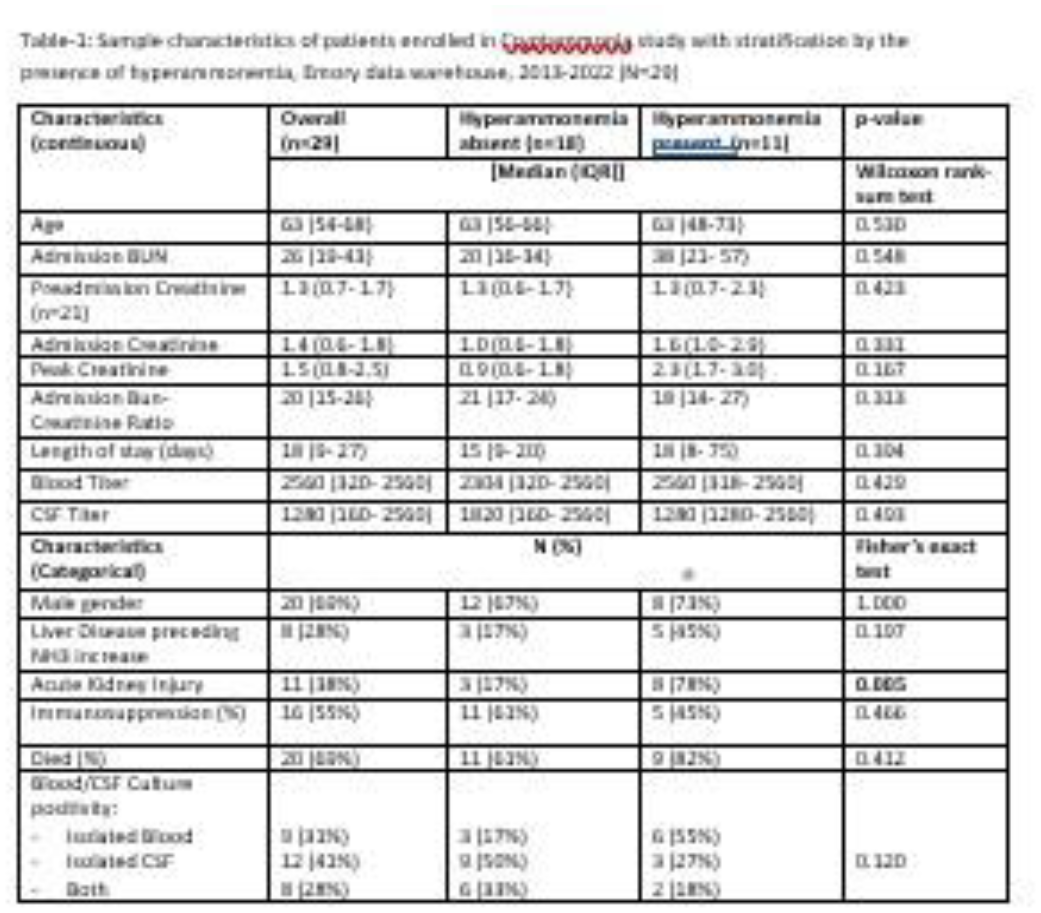
Sample characteristics of patients enrolled in Cryptammonia study with stratification by the presence of hyperammonemia, Emory data warehouse, 2013-2022 (N=29).
P23. Isolated Ear Auricle Coccidioidomycosis: A Rare and Challenging Diagnosis
Lutfor Nessa2, Barath Rangaswamy3, Devi Suravajjala1, Pablo Feuillet4
1 Endocrinologist, Texas Tech University Health Sciences Center, Odessa, TX, United States. 2 Internal Medicine, Texas Tech University Health Sciences Center, Odessa, TX, United States. 3 Internal Medicine, Texas Tech University Health Sciences Center, Odessa, TX, United States. 4 Infectious Disease, Medical Center Hospital, Odessa, TX, United States.
Background: Coccidioidomycosis is a fungal infection caused by inhalation of spores of Coccidioides immitis and Coccidioides posadasii found in desert soils in the southwestern US. It usually causes a self-limiting pulmonary infection, but in rare cases, it can progress to disseminated disease affecting bones, joints, meninges, and skin.
Case Description: A 58-year-old male with alcoholic liver cirrhosis presented with an infection in his right ear pinna, which began as a pimple and gradually spread to involve the entire ear over a period of 2-3 months. The patient’s vitals were normal. Upon physical examination, crusted ulcerations, abrasions, erythema, edema, and perichondrial thickening were observed in the right pinna, while his clinical hearing remained unaffected. Despite being treated with antibiotics, antivirals, and antifungals, the patient’s condition did not improve. Consequently, the patient was referred to an ENT specialist, who performed a biopsy revealing mixed acute, chronic, and granulomatous inflammation with numerous fungal organisms consistent with Coccidioides spp. The ENT specialist initiated treatment with fluconazole, prednisone, and valacyclovir, but unfortunately, there was no relief. Subsequently, the patient was referred to an infectious disease consultant, who started him on liposomal amphotericin B, followed by fluconazole after induction therapy. After 28 weeks of this treatment regimen, the earlobe discoloration resolved, with only slight induration remaining, and the levels of Coccidioides IgG decreased. Throughout the treatment, the patient tolerated fluconazole well, and he was advised to continue the treatment with close follow-up.
Conclusion: Isolated ear auricle coccidioidomycosis is rare and presents diagnostic and therapeutic challenges. Despite initial treatment with various medications, the patient’s condition did not improve until the initiation of liposomal amphotericin B followed by fluconazole after induction therapy. This case underscores the importance of considering coccidioidomycosis as a differential diagnosis in patients with chronic ear infections, particularly in endemic areas.
P24. Optimal Duration of Antibiotic Therapy for Non-Critically Ill Patients with Hospital Acquired Pneumonia: A Single-Center Retrospective Cohort Study of 7 Days or Less Vs. over 7 Days
Miguel Rivera1, Shakira Meltan2, Adewale Balogun3, Cheryl Go3, Nimat Alam4, Barath Rangaswamy4, John Garza5
1 Pharmacy, Laredo Medical Center, Laredo, TX, United States. 2 Texas Tech School of Medicine, Laredo, TX, United States. 3 Pharmacy, Medical Center Hospital, Odessa, TX, United States. 4 Medical Center Hospital, Odessa, TX, United States. 5 UTPB, Odessa, TX, United States.
Purpose of Study: Hospital-acquired pneumonia (HAP) is a significant concern in healthcare settings, with a high mortality rate. This study aims to investigate the appropriate treatment duration for patients with HAP, focusing on 7 days or less and over 7 days of antibiotic therapy.
Methods Used: A single-center retrospective cohort study was conducted at Medical Center Hospital in Odessa, Texas. Patients over 18 years old with a confirmed HAP diagnosis were included. The primary endpoint was all-cause mortality, and the secondary endpoint was length of stay.
Summary of Results: Out of 198 eligible patients, 121 were included in the study. There was no significant difference in all-cause mortality rates between the two groups (12.5% for 7 days or less and 17% for over 7 days). However, the length of stay was significantly shorter for patients receiving 7 days or less of antibiotics (6.86 days vs. 13.99 days, P=<0.0001). Subgroup analysis on patients with positive microbiological growth showed no significant difference in mortality rates but revealed a significant difference in length of stay (9 days vs. 24 days, P=0.00016).
Conclusions: The study’s results suggest a potential benefit of receiving 7 days of antibiotic therapy for HAP, but patients with positive microbiological growth may benefit from longer treatment. Limitations included the retrospective design and reliance on ICD codes for inclusion criteria.
P25. Impact of Pandemic on Return of Endemic
Rupam Sharma1,3, Carlos D’Assumpcao2,1, Michael Valdez2,1, Royce Johnson2,1,3, Rasha Kuran2,3, Arash Heidari2,3
1 Internal Medicine, Kern Medical Center, Bakersfield, CA, United States. 2 Infectious Diseases, Kern Medical Center, Bakersfield, CA, United States. 3 Internal Medicine, David Geffen School of Medicine, UCLA, Bakersfield, CA, United States.
Purpose of Study: West Nile virus has become endemic in all 48 contiguous United States since its discovery in North America in 1999. It has produced the 3 largest arboviral neuroinvasive disease (encephalitis, meningitis, or acute flaccid paralysis) outbreaks ever recorded in the US. Culex mosquito species drive the transmission of the virus in nature and subsequent spread to humans. 94% of patients have abrupt onset of symptoms in July through September. All ages are affected, although there’s strong predilection with advancing age. Diagnosis is made by detection of West Nile virus specific IgM antibody in CSF or serum. This report describes a recent outbreak of nine west nile cases over three months unreported from California
Methods Used: This study was approved by the Kern Medical (KM) Institutional Review Board. Retrospective chart review of KM’s electronic health record over a period of 3 months (July 2022 – September 2022) was performed. Literature search was conducted on PubMed and google scholar using the following search terms: West Nile virus outbreak, West Nile treatment, West Nile virus literature review
Summary of Results: Six out of nine cases presented with fever >38.2 C along with additional symptoms. Three cases presented with non-specific presentations. Eight cases were diagnosed with west nile antibody IgM and IgG serum or CSF titers. One case was diagnosed with west nile PCR test after two negative IgM and IgG titers. Six cases received five days of oral or IV steroids. One case was treated with intravenous immunoglobulin. Two cases did not receive any treatment. Five cases were discharged home in stable condition. Two were discharged to acute rehab facility. Two cases discharged to long term care facilities
Conclusions: In conclusion, sustainable, community-based surveillance and vector management programs are critical, particularly in metropolitan areas with a history of West Nile virus and large human populations at risk for better understanding and prevention of disease transmission
P26. Unsuspecting Campylobacter infection causing Warm Autoimmune Hemolytic Anemia
Nancy Zurita1, Melissa Tebaldi1, Zackary D. Anderson1, Angelina Browne1, Mark Rasnake1, Gairman Fisher2
1 NCH Downtown Naples, Naples, FL, United States. 2 UCF School of Medicine, Orlando, FL, United States.
Case Report: Introduction Warm autoimmune hemolytic anemia or wAIHA, found in 1-3 adults per 100,000 people and diagnosed via Coombs test Antibody-dependent cell-mediated cytotoxicity of the bound RBCs leads to a higher destruction-to-compensated production ratio leading to anemia. It often presents with non-specific symptoms – from dizziness, palpitations, jaundice, and fatigue. Complications of severe disease include arrhythmia leading to death. wAIHA is considered secondary when it is caused via causes such as infection or drugs. Despite advancements, secondary wAIHA is associated with increased mortality warranting an initial suspicion based on laboratory studies and clinical exam.
Case Presentation: 68-year-old woman with a history of MAC infection on treatment who recently underwent lap cholecystectomy presented with chills, nausea/vomiting, and severe diarrhea subsequently diagnosed with acute Campylobacter gastroenteritis. Physical exam was significant for mild discomfort in epigastric/RUQ with mild edema in LE B/L. Initial labs showed Cr 6.6 (baseline 0.9), Hb 11.9, WBC 19.7k, platelets 94. AST 66, ALT 76, total bilirubin 1.9, indirect 1.2. She was also found to have anion gap metabolic acidosis (lactate 6.5). Patient was started on IV azithromycin 500 mg and supportive care. Despite aggressive fluids, she had worsening renal failure with anuria and found to have active bleeding from IV sites. Repeat labs showed platelets 47, fibrinogen 195, and PT/INR 18.3/1.5. Additionally, it was found to be DAT+, with peripheral blood smear negative for schistocytes, and diagnosed with wAIHA secondary to campylobacter. Patient was started on prednisone 1 mg/kilogram and broad-spectrum antibiotics. She required temporary HD sessions and showed significant improvement at the time of discharge.
Discussion: WAIHA is rarely caused by campylobacter and thus requires a high index of suspicion as it has the potential to be fatal. Our patient positive for campylobacter had signs of hemolytic anemia with jaundice, and acute renal insufficiency. wAIHA was likely triggered by campylobacter with a positive Coombs test with warm autoantibody elution and no evidence of schistocytes on smear. Her presentation is less likely atypical HUS, or TTP based on smear and a mildly reduced adamTS13. Guideline therapy for secondary wAIHA from infection is steroids and broad-spectrum antibiotics. Secondary wAIHA has been shown to have worsening response to treatment especially when further delayed. Early detection plays a key role in prognosis and management. Delays in treatment have been documented with increased mortality. In secondary cases, a documented 20% risk of mortality is associated with a diagnosis of wAIHA. And can reach up to 50% if severe anemia is observed. With few cases in the literature demonstrating wAIHA secondary to campylobacter this provides an advancement in the literature to help with early detection and improved mortality.

Peripheral blood smear
P27. Association of Pemphigus Vulgaris with Various Infections in End-Stage Renal Disease Patients
Sara Attari1, Jennifer Waller2, Stephanie Baer3, Wendy Bollag4
1 Medical College of Georgia at Augusta University, Augusta, GA, United States. 2 Division of Biostatistics and Data Science, Department of Population Health Science, Medical College of Georgia at Augusta University, Augusta, GA, United States. 3 Charlie Norwood VA Medical Center, Augusta, GA, United States. 4 Department of Physiology, Medical College of Georgia at Augusta University, Augusta, GA, United States.
Purpose of Study: Pemphigus vulgaris is an autoimmune, blistering disease that presents as mucocutaneous intraepidermal bullae. The blisters of pemphigus vulgaris are characteristically flaccid and rupture easily leaving behind areas of exposed, unprotected tissue. Due to this compromise in the skin barrier, pemphigus vulgaris in end-stage renal disease (ESRD) patients, who are already at increased risk of infection, may be an independent risk factor for developing infections.
Methods Used: A retrospective cohort analysis of ESRD patients entered into the United States Renal Data System between 2004 and 2019 was conducted. We evaluated the association of pemphigus vulgaris and infections in this population with bacteremia, septicemia, cellulitis, and herpes zoster. ICD-9-CM and ICD-10-CM codes were used to determine pemphigus vulgaris and infection diagnoses. Logistic regression was used to examine the association of pemphigus vulgaris with each infection.
Summary of Results: A total of 150 patients with a diagnosis of pemphigus vulgaris after the incident date of dialysis were identified. The unadjusted model demonstrated that patients with pemphigus vulgaris are at a significantly increased risk of developing bacteremia (relative risk (RR) = 1.9, 95% confidence interval (CI) = 1.4-2.6), septicemia (RR = 1.8, CI = 1.5-2.3), cellulitis (RR = 2.0, CI = 1.6-2.6), and herpes zoster (RR = 2.4, CI = 1.3-4.4) compared to those without pemphigus vulgaris. After controlling for covariates the association was still greater than 1 for each infection; however, the p-values became non-significant. Diabetes was found to be a confounding variable for the association of pemphigus vulgaris and each infection.
Conclusions: These results determined that in the ESRD population after controlling for various demographic and clinical covariates, pemphigus vulgaris was not associated with increased risk of the queried infections.
P28. Assessment of Demographic and Clinical Risk Factors for Vitiligo in Patients with End-Stage Renal Disease: A Retrospective Cohort Study
Mitchell T. Hanson1, Pearl Shah1, Jennifer Waller2, Sarah Tran3, Varsha Taskar3, Stephanie Baer3, Wendy Bollag3
1 Medical Education, Medical College of Georgia, Augusta, GA, United States. 2 Population Health Sciences, Augusta University, Augusta, GA, United States. 3 Medicine, Augusta University, Augusta, GA, United States.
Purpose of Study: Vitiligo is an autoimmune condition of patchy depigmentation, affecting nearly 3 million individuals in the United States. This condition is associated with autoimmune, connective tissue, and mental health comorbidities that reduce patients’ overall health and quality of life. Recent studies have also suggested a potential correlation between vitiligo and increased risk of obesity and renal diseases. Infections are the second leading cause of death in the end stage renal disease (ESRD) population, which may be exacerbated by disrupted epidermal barrier composition and recovery with vitiligo, therefore, may make these patients more susceptible to infection. However, there is limited research exploring the prevalence and risk factors for vitiligo in dialysis patients to identify patient populations predisposed to these negative outcomes. To address this knowledge gap, we conducted a retrospective analysis utilizing claims from the United States Renal Data System (USRDS) to assess the demographics and clinical risk factors for vitiligo.
Methods Used: All end-stage renal disease (ESRD) patients in the USRDS who started dialysis between 2004 and 2019 were eligible for study inclusion. Those who were less than 18 or greater than 100 years of age or had missing or unknown data on age, race, sex, ethnicity, access type, or dialysis type were excluded. The total sample size was 1,526,270. In addition to demographics, clinical risk factors including tobacco use, alcohol dependence, and hepatitis C infection were determined by hospital, detailed, and physician/supplier claims with ICD-9-CM and ICD-10-CM codes; a diagnosis of vitiligo was queried after the incident date of dialysis. Statistical analysis was performed using SAS 9.4, and descriptive statistics on all variables were determined overall by vitiligo status and by each type of infection.
Summary of Results: A total of 676 subjects had a vitiligo diagnosis as depicted in Table 1. Based on a multivariate logistic regression model, black compared to white race [adjusted relative risk (aRR) of 1.51 and 95% confidence interval (CI) of (1.27-1.80)], female sex (aRR=2.41, CI=2.06-2.82), Hispanic ethnicity (aRR=2.14, CI=1.75-2.62), tobacco use (aRR=3.54, CI=3.02-4.15), and hepatitis C infection (aRR=2.14, CI=1.59-2.89) were associated with increased risk of vitiligo. Increasing age (aRR=0.992, CI=0.987-0.997) and catheter access type (aRR=0.65, CI=0.54-0.78) compared to arteriovenous fistula access type were associated with decreased risk of vitiligo.
Conclusions: These results indicate that race and ethnicity and gender may impact the diagnosis of vitiligo in ESRD patient populations. Clinical risk factors associated with increased risk such as tobacco use and Hepatitis C may be amenable to treatment to reduce risk for vitiligo and the associated negative outcomes.
P29. Rare but Real: Spontaneous Renal Hematoma in End-Stage Renal Disease Patients on Hemodialysis
Lutfor Nessa1, Rahul Atodaria1, Genesis Perez Del Nogal1, Sai Siva Mungara1
1 Internal Medicine, Texas Tech University Health Sciences Center-PB, Odessa, TX, United States.
Background: Spontaneous renal hematoma (SRH) is a rare clinical occurrence in patients with end-stage renal disease (ESRD) on hemodialysis (HD). The two major causes of SRH are often renal malignancies like angiomyolipoma and renal cell carcinoma (RCC) and vascular diseases like polyarteritis nodosa. Patients on dialysis are predisposed to developing SRH for several reasons. First, dialysis patients are more prone to develop RCC. More precisely, the relative risk of developing RCC in HD patients is about 13 to 29-fold higher (2.3 to 3.3%) than in patients not on HD. Next, patients on HD typically receive anticoagulant medications that increase the bleeding risk and can lead to SRH. Ultimately, these reasons stress the importance of frequent surveillance and consideration of SRH in dialysis patients.
Case Presentation: The patient is a 38-year-old African American male who initially presented with nausea and diffuse abdominal pain for three days after missing nine days of dialysis. His chronic medical problems included HTN for 18 years and ESRD on HD for the last two years. He is also a chronic smoker, an occasional drinker, and a marijuana user, in addition to being non-compliant with home medications and HD. Upon presentation, vital signs were normal. Physical exam was significant for dry mucous membranes, mild abdominal distention, generalized abdominal tenderness, and grade 3 peripheral edema. Labs were significant for normocytic anemia (Hb 10.8 g/dL, MCV 86 fL), hyperkalemia (6.6 mEq), impaired renal function with uremia (BUN 97 mg/dL, creatinine 23 mg/dL, eGFR 2.7 mL/min), and high anion gap metabolic acidosis. The patient was started on HD per nephrology recommendation. A CT scan of the abdomen and pelvis without contrast was performed due to persistent abdominal pain. This revealed a poorly defined hemorrhage in the left kidney with infiltration of left perinephric fat and fluid in the left perinephric space, as well as a 10 mm hyperdense lesion in the posterior-superior right kidney. CT angiography showed left SRH with no evidence of active hemorrhage and a 10 mm hyperdense lesion in the posterosuperior right kidney. Radiology and urology consult suggested no need for inpatient surgical intervention or embolization and recommended outpatient management of the renal nodule.
Conclusion: Unfortunately, there is no “standard” or classic presentation of SRH, which poses a challenge in accurately diagnosing high-risk patients. Lenk’s triad, consisting of acute flank pain, flank mass, and internal bleeding symptoms, are common, but patients rarely present with those. Our goal is to encourage physicians to remain cognizant of SRH in patients with HD, given the increased morbidity and mortality risk and the uncommon occurrence of this circumstance.
P30. Recurrent Idiopathic Cerebral Venous Thrombosis
Zackary D. Anderson1, Keegan Plowman1, Brittany Davis1, Melissa Tebaldi1, Dairon Lago1, Carl Ruthman1
1 GME, Naples Community Hospital, Naples, FL, United States.
Case Report: Cerebral venous thrombosis (CVT) is a disease typically affecting young adults, women, and children with an incidence of 2-5 million cases per year. Typically, these cases present in women of childbearing age with unremitting pain described as the “worst headache of life” and is often a missed diagnosis. There is an estimated 34.2% mortality rate despite improvements in treatment and diagnostic therapies. A 40-year-old female with a past medical history of beta thalassemia minor presented to the ED with non-intractable headache, nausea, and vomiting. A CT head without IV contrast at that time was negative for acute findings. The patient presented 48 hours later at which point she was found to have cerebral venous thrombosis. She was then taken for mechanical thrombectomy. Post procedure her intracranial pressure (ICP) continued to rise and a repeat CT head showed obstructive hydrocephalus. The patient underwent placement of an external ventricular drain (EVD) and received mannitol and 3% hypertonic saline. Due to persistently elevated ICP the patient was taken back to interventional radiology for invasive angiography and was found to have rapid re-accumulation of venous thrombosis. Thrombectomy was again performed removing a significant amount of clot burden. Follow up CT venogram showed large areas of attenuation in the right MCA territory with persistent hypodensity in the straight sinus, concerning for yet another episode of re-thrombosis. At this point the patient was managed medically with heparin as she was deemed high risk for intracranial hemorrhage with additional invasive procedures. Subsequent MRI imaging showed progression of multiple watershed infarcts with loss of flow-void involving sinuses compatible with venous sinus thrombosis. Despite ongoing medical management, the patient was unable to survive her significant neurological damage. This case represents an idiopathic cerebral venous thrombosis in a classic demographic that should caution providers to think about the differential of cerebral venous thrombosis in the hopes of early intervention and improved outcomes. With such a high mortality rate, the clinical diagnosis and early detection of cerebral venous thrombosis are crucial in overall survivorship. Plain CT or MRI is the initial evaluation but should be followed up with CT-venogram if negative. Anti-epileptic therapy should be considered if the patient displays any seizure like activity. Anticoagulation is a mainstay of treatment. If the patient continues to have neurological deterioration, endovascular intervention or decompressive hemicraniectomy can be performed. Despite these measures, mortality in patients with CVT still remains high. With improved imaging modalities, early diagnosis is possible with high clinical suspicion. This case report indicates the importance of a broad differential diagnosis and appropriate use of diagnostic modalities in order to not miss diagnoses with high morbidity and mortality.

CT head showing obstructive hydrocephalus with effacement of the 4th ventricle and dilated lateral and 3rd ventricles
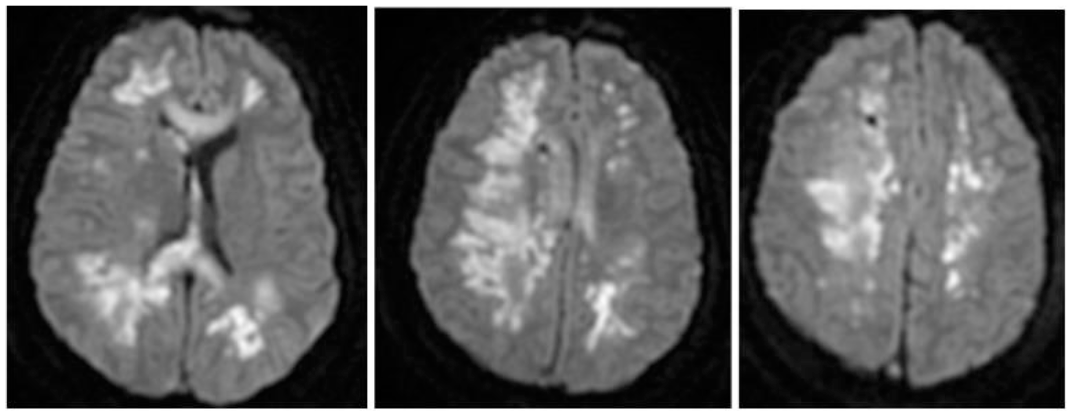
MRI brain demonstrating multiple watershed supratentorial and basal ganglia infarcts and left temporal lobe hemorrhage
P31. Protein Localization, Organellar Interactions, and Pathogenesis in Mitochondrial Membrane Protein-Associated Neurodegeneration
Michael Boden1,2, Brianna R. Pierce2, Nhu T. Chau2, Jamie L. Fraser3,2
1 St. Mary’s College of Maryland, St. Mary’s, MD, United States. 2 Center for Genetic Medicine Research, Children’s National Hosital, Washington, DC, United States. 3 Rare Disease Institute, Children’s National Hospital, Washington, DC, United States.
Purpose of Study: Mitochondrial Membrane Protein Associated Neurodegeneration (MPAN) is a rare neurometabolic condition caused by biallelic variants in C19ORF12. The clinical and histopathological phenotype of MPAN overlaps with Parkinson’s and Alzheimer’s diseases. MPAN is typically diagnosed after premature iron deposition is observed in the basal ganglia. MPAN causes significant morbidity including gait changes, spastic paresis, progressive dystonia, neuropsychiatric dysfunction, cognitive decline, and dementia. Early mortality occurs due to progressive neurological decline. While the MPAN protein has been identified as C19ORF12, the subcellular localization and role of this protein have not been validated, and no mammalian model system has been developed to better understand disease progression. The goal of this project was to identify the subcellular localization of C19ORF12, understand its role in cell biology, and validate our novel transgenic mouse model of MPAN in order to better understand disease development and progression in MPAN.
Methods Used: Using RenCell-VM immortalized neural stem cells (NSCs) before and after differentiation, we performed immunocytochemical and fluorescent labeling techniques assays to localize wild-type C19ORF12 protein to specific organelles within the NSCs and differentiated cells. We generated a CRISPR/Cas9-directed knock-in p.G54E missense mouse model (MPANKI/KI) based on a patient’s genetic variant. Mice were monitored for health changes until they reached adulthood (postnatal day 60, P60). P60 sex-matched MPANKI/KI and wild-type (MPANWT/WT) mice were euthanized, and the brains were dissected and cryosectioned. Histological staining was performed to identify iron deposition, and immunohistochemistry for cell death by cell type was performed.
Summary of Results: Using our in vitro NSC model, we were able to localize C19ORF12 to the mitochondria-endoplasmic reticulum interface, suggesting that it may play a role in MAM complex-related functions. The MPANKI/KI mice reached adulthood without experiencing significant morbidity or mortality, unlike our pediatric patients. Both male and female MPANKI/KI mice were fertile. While the mouse phenotype is less severe than that of MPAN patients, histopathological indicia of brain injury were observed in the MPANKI/KI mice in the basal ganglia.
Conclusions: Our novel model presents the opportunity to test for the localization of mutant and wild-type C19ORF12, both within the cell and at the tissue level in different regions of the brain. With optimization, this in vivo model of MPAN will enable further research into the mechanisms of MPAN and the development of future therapies. We are now targeting mechanisms to induce more rapid disease progression in this model.
P32. Antimicrobial Effect of Surgical Sutures Exposed To TiO2 Nanoparticles
Yousef Ismail1, Alyssa Greenwood Francis1, Frederick Owusu1, Diego Sanchez1, Christopher Castagno1, Yathip Chokpapone1, So-Yoon Lee3, Jorge Cervantes4
1 Paul L. Foster School of Medicine, El Paso, TX, United States. 2 NewYork-Presbyterian Queens, Flushing, NY, United States 3 Shibaura Institute of Technology, Tokyo, Japan. 4 Nova Southeastern University Fort Lauderdale, FL, United States.
Purpose of Study: Postoperative surgical infections are not uncommon, and in some instances, they can lead to disastrous consequences needing further expensive treatments. TiO2 has been shown to have antimicrobial and biofilm-disrupting properties. We aimed to evaluate the antimicrobial effect of titanium dioxide (TiO2) nanoparticles-exposed surgical sutures on Staphylococcus aureus and Staphylococcus epidermidis, as these skin microorganisms frequently detected in surgical wound infections.
Methods Used: Nylon sutures were exposed to various concentrations of Ti Ctrl, TiO2+ KOH 1M, and TiO2+KOH 10M for 24 hours. A subsequent photocatalytic step through exposure to UV light for 90 minutes was also conducted. Nylon sutures were then placed onto blood agar plates seeded with S. aureus or S. epidermidis.
Summary of Results: A zone of growth inhibition was observed around sutures that were treated with TiO2 + KOH 10M, independent if the nanoparticles were photocatalytically activated or not.
Conclusions: Our results provide evidence of an antimicrobial effect of surgical sutures exposed to TiO2+KOH nanoparticles on skin staphylococci. This supports the ultimate goal of a wet-packaging for sutures containing TiO2 that could prevent the occurrence of surgical infections by skin bacteria.
P33. Acute Cutaneous Vasculitic Phase of Eosinophilic Granulomatosis with Polyangiitis in a Patient with Type V Skin
Omar Mourad1, Fouad Sakr1, Hamead Moshreshi2, Michael Cooper3, Silvija Gottesman4, Elizabeth Bentsianov6, Stefan Bradu5
1 Internal Medicine, Staten Island University Hospital, New York, NY, United States. 2 Internal Medicine- Division of Rheumatology, Staten Island University Hospital, New York, NY, United States. 3 Burn Unit, Staten Island University Hospital, New York, NY, United States. 4 Dermatopathology, Northwell Health, New York, NY, United States. 5 Internal Medicine- Division of Dermatology, Staten Island University Hospital, New York, NY, United States. 6 Union College, Schenectady, NY, United States.
Case Report: Eosinophilic granulomatosis with polyangiitis (EGPA), also known as Churg-Strauss syndrome (CSS), is a disorder characterized by eosinophil-rich inflammation and necrotizing vasculitis in patients with asthma. Only scarce information exists regarding the severe cutaneous manifestations of EGPA for patients with darker skin types. We present a unique case of a 50-year-old female with type V skin and a medical history of asthma, chronic rhinosinusitis, and CSS diagnosis for more than 14 years who presented at the emergency room (ER) complaining of progressive weakness, numbness, and shooting pains in her extremities for 2 months. Five weeks prior to the current hospitalization, the patient discontinued her prednisone due to concerns over potential side effects, resulting in worsening of symptoms. Concurrently, she had developed rapidly progressing purpuric lesions on her bilateral extremities, which had started 2 days prior to her ER presentation. On the first day of her skin symptoms, the thighs had itchy edematous papules and pseudo-urticarial wheals with angulated and stellate purpuric foci (Figure 1). One dose of 125 mg methylprednisolone followed by daily methylprednisolone 500 mg during the initial two days of hospitalization led to a reduction in itchiness and normalization of blood eosinophils. The retiform purpuric lesions on the medial thighs extended and coalesced, progressing into larger angulated purpura and hemorrhagic bullae surrounded by erythema (Figure 2). Evaluation of the skin biopsy showed leukocytoclastic vasculitis and tissue eosinophils. P-ANCA antibody was positive and c-ANCA was negative. The Myeloperoxidase antibody assay was positive, whereas the Proteinase 3 antibody assay was negative. On day 2 of hospitalization, cyclophosphamide 15 mg/kg was initiated. Palpable purpuric papules were also emerging on the knees, elbows, and dorsal hands, but development of new skin lesions notably slowed 3 days post-admission. Methylprednisolone was increased to 1000 mg daily for five days, followed by 80 mg of daily prednisone. Over the course of a week, the angulated purpura and blisters evolved into partial and full thickness necrotizing wounds, healing with angulated ulcers and black-gray necrotic eschars. Despite using multiple pain medications and five plasma exchange sessions, the patient continued to experience sensorimotor deficits and severe shooting pains in the extremities. Intravenous Immunoglobulin (IVIg) 2 g/kg over five days and duloxetine 60 mg at bedtime were initiated. The patient’s pains had subsided after the second day of duloxetine and IVIg, but only slow improvements in sensorimotor deficits were observed. Our report emphasizes the importance of recognizing the spectrum of cutaneous findings during the acute vasculitic phase of EGPA in patients with darker skin types, facilitating early diagnosis and intervention. This approach aims to mitigate the disease’s impact on end organs and improve patient outcomes.

Cell phone photograph from patient taken on the first day of her skin eruption showed edematous papules and pseudo-urticarial wheals with angulated and stellate purpuric foci on the right medial thigh.

One day after hospitalization, coalescing angulated purpura and hemorrhagic bullae surrounded by purpuric erythema developed on the thighs.
P34. The Use of Balloon Aortic Valvuloplasty to Facilitate High-Risk Non-Cardiac Surgery in a Patient with Severe Aortic Stenosis: A Case Report
Leena S. Penumalee1, Allison Dalton2
1 University of Chicago Pritzker School of Medicine, Chicago, IL, United States. 2 Department of Anesthesiology and Critical Care, University of Chicago, Chicago, IL, United States.
Case Description: We present the case of a 68-year-old female with history of aortic stenosis who presented for semi-urgent removal of recurrent angiosarcoma of the right posterior lateral hip. A pre-operative TEE revealed an EF >75%, aortic valve area of 0.86 cm2, mean peak transvalvular gradient of 31 mmHg, and maximum area velocity of 3.7 m/s2. Given the measurements were consistent with severe aortic stenosis, the patient was referred to cardiology to undergo further assessment of cardiac risk and potential intervention prior to surgery. Although SAVR (surgical aortic valve replacement) and TAVR (transcatheter aortic valve replacement) were considered, the team ultimately decided to proceed with BAV (balloon aortic valvuloplasty) for stabilization given the time-sensitive nature of the resection and patient’s amenable anatomy. Definitive TAVR was planned once the patient recovered from the surgery. Patient underwent left heart catheterization and balloon aortic valvuloplasty four days prior to angiosarcoma resection. A subsequent TTE showed an improved aortic valve area of 1.1 cm2 and mean systolic gradient of 35.9 mmHg, and the patient was deemed appropriate for surgery. Pre-induction radial arterial line access was obtained prior to surgery. The patient was induced with 1mg midazolam, 30mg propofol, 60mg rocuronium, and 500mcg phenylephrine prior to intubation with direct laryngoscopy. Diagnostic TEE was performed intra-operatively. Throughout the procedure, systolic blood pressures remained above 90 mmHg on approximately 1-1.7% sevoflurane. Brief periods of hypotension were treated with additional phenylephrine. The surgery lasted 169 minutes, during which the patient received a total of 2600 mL of lactated ringers with an intraoperative urine output of 315 mL. The patient was extubated in the operating room, and she was successfully discharged without anesthetic complications.
Discussion: This case illustrates the successful use of BAV to stabilize a patient with severe aortic stenosis prior to major non-cardiac surgery. Although BAV can enhance hemodynamic status of patients with severe AS for a limited time, it does not offer the long-term survival benefits of definitive aortic valve replacement via TAVR or SAVR. As a result, BAV is largely used as a bridge to SAVR/TAVR or palliative measure. Some studies have found that patients who undergo pre-operative BAV prior to non-cardiac surgery have decreased mortality compared to those who receive conservative treatment, however data is mixed (1,2). This case demonstrates how thorough preoperative risk assessment and use of a BAV can successfully minimize cardiac risk. Further considerations included various multi-specialty conversations to optimize the patient prior to surgery and anticipate potential intra-operative challenges.
P35. Purulent Pericarditis due to Non-Typeable Haemophilus Influenzae in a Pediatric Patient
Laaibah Ejaz2, Clara El Nakib1, Irene Cherrick1, Leonard Weiner1, Angela Wratney1
1 SUNY Upstate Medical University, Syracuse, NY, United States. 2 Children’s Hospital of Michigan, Detroit, MI, United States.
Introduction: Purulent pericarditis in children is uncommon in the United States. A few cases of non-typeable Haemophilus influenzae purulent pericarditis are described in the literature with only one prior pediatric-age case reported in an immunocompetent 2-year old patient.
Description: A 16-year-old male with history of idiopathic thrombocytopenic purpura (ITP) presented with 1 week of chest pain, cough, shortness of breath, fatigue and fever. He had marked inflammation with leukocytosis of 40,000, procalcitonin of 51 ng/ml, albumin of 2.9 g/dL, ALT of 138 U/L and AST of 151 U/L. Chest X-ray revealed right-sided pleural effusion, EKG showed diffuse ST-elevation, and echocardiogram revealed moderate pericardial effusion with mildly depressed systolic function (ejection fraction 45-50%). He was admitted to the pediatric ICU with high flow oxygen for moderate accessory muscle use and tachypnea. Empiric ceftriaxone for sepsis was begun. He received anti-inflammatory and analgesic therapy for pericarditis, and for persistent hypotension received dopamine, epinephrine and milrinone. Chart review revealed that he had received two doses of rituximab in 2015 for refractory ITP. A low IgG level of 206 mg/dL on day 1 of admission raised concern for B-cell dysfunction. Additionally, due to the potential for the diagnosis of MIS-C, he received IVIG and methylprednisolone. Serial echocardiograms indicated likely purulent pericarditis. His blood culture was positive on day 2 for non-typeable Haemophilus influenzae. He was continued on high dose ceftriaxone in consultation with infectious disease. He was transferred to another facility for pericardiotomy and drain placement for complex pleural fluid collection. He was extubated POD#1 and discharged POD#21 after completing a 21-day course of ceftriaxone.
Discussion: Haemophilus influenzae purulent pericarditis has been rarely reported in the post-vaccination and antibiotic era in immunocompetent individuals. Etiology of our patient’s hypogammaglobulinemia is unclear and may be due to septic immune-suppression or previous rituximab treatment with consequent B-cell dysfunction. This may have increased his risk of invasive infection due to non-typeable Haemophilus influenzae.
P36. Native Valve Infective Endocarditis with Embolization in a Previously Healthy 7-Year-Old Child: A Case Report
Taylor M. Smith, DO1, Richard Ulangca, MD1, Fatma Levent, MD2, Kelvin Lee, MD3
1 Pediatrics, AdventHealth Orlando, Orlando, FL, United States. 2 Pediatric Infectious Disease, AdventHealth Orlando, Orlando, FL, United States. 3 Pediatric Cardiology, AdventHealth Orlando, Orlando, FL, United States.
Case Report: Introduction A 7-year-old male with no past medical history presented with one day of abdominal pain, jaundice, and right knee pain following six days of fever and emesis. Physical examination was significant for right upper quadrant tenderness, right knee swelling, and tender red and purple lesions on the right hand and left foot identified as Janeway lesions. Labs were significant for leukocytosis, hyperbilirubinemia, and elevated inflammatory markers. A blood culture was collected showing methicillin sensitive Staphylococcus aureus. Computed tomography of the abdomen revealed emboli of the left kidney and spleen in addition to bilateral pleural effusions. An echocardiogram revealed two vegetations located on the mitral valve leaflets measuring 5x7mm and 7x9 mm, respectively.The patient was initially started on intravenous oxacillin, gentamicin, and rifampin for persistent bacteremia. Daily blood cultures were negative on day four of admission.The patient then suffered a thrombotic ischemic stroke requiring emergent removal of the cerebral thrombus with interventional radiology and expedited mitral valve debridement. In addition,the patient had anemia requiring transfusion and required intubation with a chest tube following the emergent thrombectomy. He was later successfully extubated, and his chest tube removed. By day 18, patient was discharged home with a 6-week course of continuous intravenous oxacillin via a peripherally inserted central line and daily aspirin. His echocardiogram showed minimal mitral regurgitation. At time of discharge, the patient reported mild right sided weakness but was otherwise at neurologic baseline.
Discussion: Infective endocarditis is rare in the pediatric population in the absence of risk factors. Given the patient’s complex constellation of symptoms, the findings of Janeway lesions helped point the team to obtain an echocardiogram showing the valvular vegetations confirming the diagnosis. This case highlights a rare occurrence of native valve MSSA endocarditis in a previously healthy child without predisposing factors which subsequently embolized to multiple organs and was complicated by a stroke. Through this case, we learned more about the varied presenting symptoms and sequelae of infective endocarditis. A familiarity must be maintained with infective endocarditis’ evaluation and management to provide expeditious care for patients despite their lack of risk factors.

TTE obtained showing vegetation on mitral valve leaflet.
P37. Exploring the Efficacy of the Anesthetic Ketamine an Antidepressant in Postpartum Depression: A Case Study Analysis
Clara Benjamin1, Rediet Atalay1, miguel ramallo1, Valerie Valerie McAllister1, Jonas Clarke1, Miriam Michael1
1 Medicine, Howard University, Washington, DC, United States.
Case Report: Postpartum depression is a common mental health disorder that affects women within six months after giving birth with prevalence rates as high as 20%. We present a case of a woman with a history of depression who delivered four children by cesarean section with debilitating postpartum depression in two births and no symptoms of depression in the births where she received ketamine during delivery. A 31-year-old (G4P4004) multiparous female was seen in the clinic following her delivery by scheduled C-section of her 4th child. She presented with psychomotor agitation and disorganized behavior on postpartum day 30. The patient had a history of mild intermittent asthma and depression. The first episode of depression was at age 22 that lasted eighteen weeks and, according to the patient, seemed to improve with deliberate heavy exercise and multiple hours of sun exposure. Her family history is significant only for depression on her maternal side and a strong history of schizophrenia with numerous first and second cousins and an uncle with active disease. She experienced a similar episode at age 25 after delivering her first child, which resolved after 16 weeks without treatment. She subsequently had two more pregnancies. In her second pregnancy, the patient was given ketamine to achieve adequate analgesia. During her third pregnancy, the patient experienced heavy vaginal bleeding and hypotension after four hours of labor, necessitating an emergency cesarean section. Initial epidural anesthesia proved inadequate for pain management, leading to the supplementary administration of ketamine. Following both the second and third deliveries, in which ketamine was used, the patient demonstrated positive postpartum adaptation. She successfully bonded with her newborns, established breastfeeding, and was able to return to work within two weeks. At admission, the patient presented with routine diagnostic assessments, including physical examination and laboratory studies, which were normal. The patient scored 24/30 on the Edinburgh Postnatal Depression Scale, with the cutoff score identifying a woman as depressive is 13. The patient started antidepressant medication with improvement. Several studies have shown that Ketamine has benefits in improving postpartum depressive symptoms. As an intraoperative agent, administered within 5 minutes of cord clamping, it resulted in mothers with EPDS scores greater than 9 one week postpartum . Ketamine administration is also shown to have some protective factors. When administered 10 minutes after a C-section.
P38. Unpacking Childhood Vaccination Hesitancy: A Comprehensive Review of Factors, Consequences, and Interventions
Buse Baykoca-Arslan1, Hafiz Khan2
1 Pediatrics, Advent Health Orlando Hospital, Orlando, FL, United States. 2 Public Health, Texas Tech University Health Sciences Center, Lubbock, TX, United States.
Purpose of Study: Vaccine hesitancy has been identified as a complex public health issue, meriting urgent attention and intervention. As the phenomenon continues to be pervasive across various cultural and socioeconomic landscapes, it has begun to pose a substantial risk to the effectiveness of immunization programs and public health at large. Recent WHO reports have highlighted vaccine hesitancy as a critical global health challenge. This hesitancy not only affects individual decision-making but also undermines herd immunity, thereby posing a significant risk of preventable disease outbreaks. While prior research has identified factors such as complacency, convenience, and confidence as contributing elements, there is a need to delve deeper into the complex interplay between psychological, social, and informational factors that influence vaccine acceptance or rejection. Our literature review aims to: Identify the primary determinants contributing to vaccine hesitancy. Examine the impact of vaccine hesitancy on public health initiatives, specifically immunization programs. Investigate the influence of health literacy and misinformation on vaccine hesitancy. Explore efficacious interventions tailored to mitigate vaccine hesitancy.
Methods Used: Employing a narrative literature review methodology, we integrated information from multiple academic databases, including Web of Science, PubMed, and Google Scholar, using key search terms like "vaccine hesitancy," "health literacy," and "misinformation."
Summary of Results: Key Findings Determinants: Factors such as gender, age, education level, and socioeconomic status have been found to correlate significantly with vaccine hesitancy. Impact on Public Health: Vaccine hesitancy endangers herd immunity and can potentially lead to preventable disease outbreaks, affecting public health infrastructure and finances. Role of Health Literacy: Higher levels of health literacy have been found to correlate negatively with vaccine hesitancy, offering an avenue for intervention. Misinformation: The digital era has exacerbated the rapid spread of vaccine-related misinformation, thereby influencing public sentiment and contributing to vaccine hesitancy. Proposed Interventions The study proposes a dual-strategy approach focusing on enhancing health literacy and mitigating misinformation through community engagement, educational initiatives, and targeted communication strategies. Implications for Public Health The findings have significant ramifications for public health policies and could serve as a blueprint for implementing specific interventions tailored to diverse population groups.
Conclusions: This study conducted to inform and inspire actionable solutions for this pressing public health issue. Through collaborative discourse, we seek to contribute to the ongoing efforts to mitigate vaccine hesitancy and improve public health outcomes globally.
P39. Using Google Search Data to Understand the U.S. Opioid Epidemic: An Ecological Infodemiology Approach
Maxwell Everett1, Jeremy Milkes2, Aayush Visaria1
1 Department of Medicine, Rutgers Robert Wood Johnson Medical School, Piscataway, NJ, United States. 2 Computer Science, Georgia Institute of Technology, Atlanta, GA, United States.
Purpose of Study: Opioid use remains the largest driver of drug overdose deaths in the U.S. Web searches constitute a novel source for real-time epidemiological surveillance of both communicable and noncommunicable diseases. We examined the regional and temporal relationship between Google searches for opioid related terms and opioid overdose deaths in the United States to explore the feasibility of using Google searches to monitor opioid-related deaths.
Methods Used: Google Trends and Keyword Planner are services that respectively provide the relative and absolute volumes for search terms by time and region. Volume for specific terms often changes to reflect real world events. We used the CDC WONDER database to obtain monthly opioid overdose mortality rates by U.S. state from 2010-2020. We identified 61 opioid related terms and retrieved average monthly absolute search volumes by U.S. state from 2019-2020 using Keyword Planner. We calculated Pearson correlation coefficients (r) and univariate linear regressions for each search term, to estimate the state-level association between search volume and opioid death rate. Using a similar methodology, we utilized Google Trends to temporally correlate the national relative search volume (RSV) of opioid related search terms from 2010-2020 with monthly opioid death rates. We also determined the lagged associations between the RSVs and death rates by offsetting the data in 1 month increments for +/- 12 months. Analysis was performed using Python with an alpha level of 0.05.
Summary of Results: The 61 opioid related terms were searched ~132 million times in the U.S from 2019-2020. In the state-level analysis, “small pupils” (avg. monthly volume=8,418 searches, r[95%CI]=0.67[0.49-0.80], β=17.4 [p<0.01]), “track marks” (12,870 monthly searches, 0.66[0.47-0.79], 6.2 [p<0.01]), “buprenorphine” (125,865 monthly searches, 0.60[0.39-0.75], 0.59 [p<0.01]), and “naloxone” (88,809 monthly searches, 0.53[0.30-0.71], 0.60[p<0.01]) yielded significantly positive correlations. In the temporal analysis, the RSV for “buprenorphine” had the strongest association with opioid mortality rates occurring 12 months previously (r=0.932[0.908-0.949], Figure 1) This was a higher correlation than what was observed at month offsets of 0 (r=0.865[0.824-0.897), 4 (r=0.891[0.856-0.917]), and 8 (r=0.913[0.884-0.935]). Across all keywords analyzed, the 12 month offset produced the highest average correlation (r=0.382).
Conclusions: Volumes of several search terms were significantly associated with opioid death rates in both our state level and national analyses. This suggests that Google search data may have utility as a surveillance tool for the U.S. opioid epidemic. Given the rapidly evolving nature of the epidemic, we believe that information from these tools could provide real time data to public health services and clinicians and guide the allocation of resources for preventing opioid related deaths.


P40. Who is the Culprit in this Diagnostic Case Challenge of Pneumonitis: COVID-19, or immune checkpoint-inhibitor?
Anthony M. Lim1, Jatin Thukral1, Harbir Kaur1, Sarosh Siddiqi1, Julia Oberndorf1, Jonathan Ghazaleh1, Robert Cacdac1, Marrey Quizon1
1 Eisenhower Medical Center, Rancho Mirage, CA, United States.
Case Presentation: 66-year-old male presents with progressive dyspnea for 2 weeks. He was discharged 4 weeks prior for COVID-19 pneumonia, and received steroids and antimicrobials. Relevant medical history includes transitional cell carcinoma of the bladder (treatment includes nivolumab) and nivolumab-associated hypothyroidism (4 months after first nivolumab infusion). Exam Vitals showed blood pressureof 135/87 mmHg, heart rate 114 beats/minute, respiratory rate 22 breaths/minute, temperature 36.8C, and SpO2 82% on room air. Respiratory exam showed increased work of breathing and auscultation showed diffuse crackles without wheeze. SpO2 improved to 94% with 6L/min nasal cannula O2. Investigations, management Labs on day 1 showed: WBC count 13.0 K/uL, lactate normal. COVID-19 PCR was positive. Serum 1-3-beta-d-glucan Fungitell, coccidoides IgG/M, aspergillus antigen EIA were negative. CTA chest on day 1 showed heterogeneous airspace consolidations scattered in both lungs, without pulmonary embolism. The patient was started on antimicrobials (cefepime, vancomycin, micafungin). On day 3, the patient underwent bronchoscopy. Samples included sputum, brushings, bronchoalveolar lavage (BAL), and tissue sampling. Respiratory, fungal, acid-fast bacilli/mycobcterium, Legionella culture, Mycoplasma pneumoniae PCR, Chlamydia pneumoniae DNA PCR, Pneumocytis jirovecii DNA PCR, and cytology were negative. Tissue exam showed pulmonary parenchyma with chronic inflammation and probable interstitial fibrosis. BAL fluid contained 16% lymphocytes, 62% neutrophils, 22% monocytes/macrophages. During admission, the patient received a diagnosis of nivolumab-associated pneumonitis. Antibiotics were stopped, and intravenous methylprednisolone 50mg twice daily (continued until discharge on day 15) was commenced. Post-discharge steroid regimen comprised prednisone 50mg twice daily for 1 month. CTA chest 3 months later showed improvement and general resolution of the pneumonitis-associated bilateral multifocal opacities.
Discussion: We present a diagostic dilemma of pneumonitis. Other than nivolumab-associated hypothyroidism 4 months post-first nivolumab, the patient had no pulmonary sequelae. 4 weeks prior, the ptaient had COVID-19; 6 weeks prior, the patient received nivolumab. Given chronological proximity, it is difficult to ascertain the true etiology – ICI vs. post-COVID-19. While bronchoscopy fluid analysis/differential and imaging can help differentiate ICI vs. COVID-19 pneumonitis, definitive diagnosis remains elusive. However, incorrect diagnosis may result in incorrectly administering steroids during the COVID-19 virus replication phase, or withholding anti-inflammatory immunosuppressants if ICI pneumonitis is not suspected. Further discriminatory markers or algorithms need to be developed, given the increasingly popular immunotherapy agents in the long-term landscape of COVID-19.
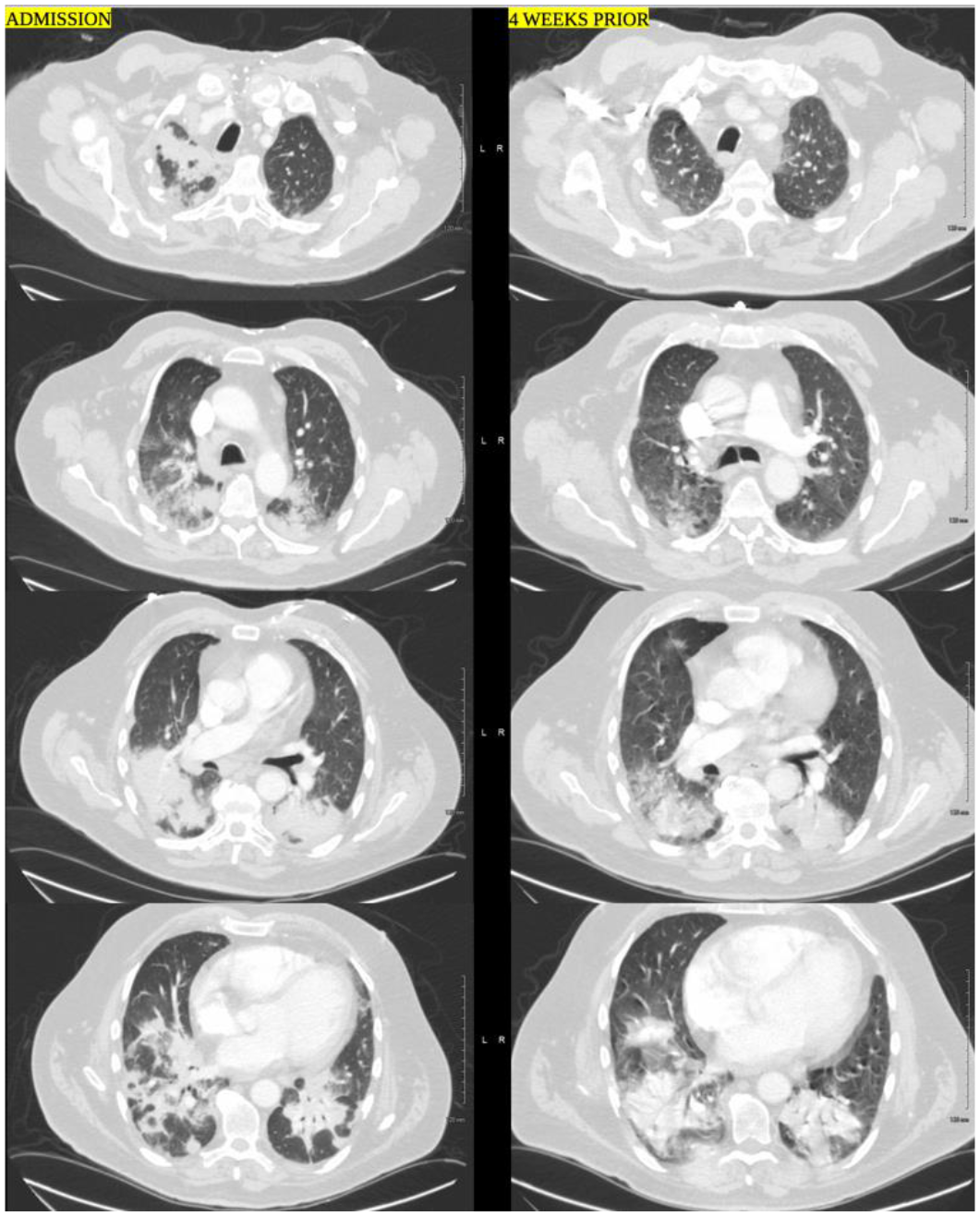
CTA chest admission (left, “ADMISSION”) vs. 4 weeks prior (right, “4 WEEKS PRIOR”). New bilateral heterogeneous multifocal opacities/consolidation are seen.
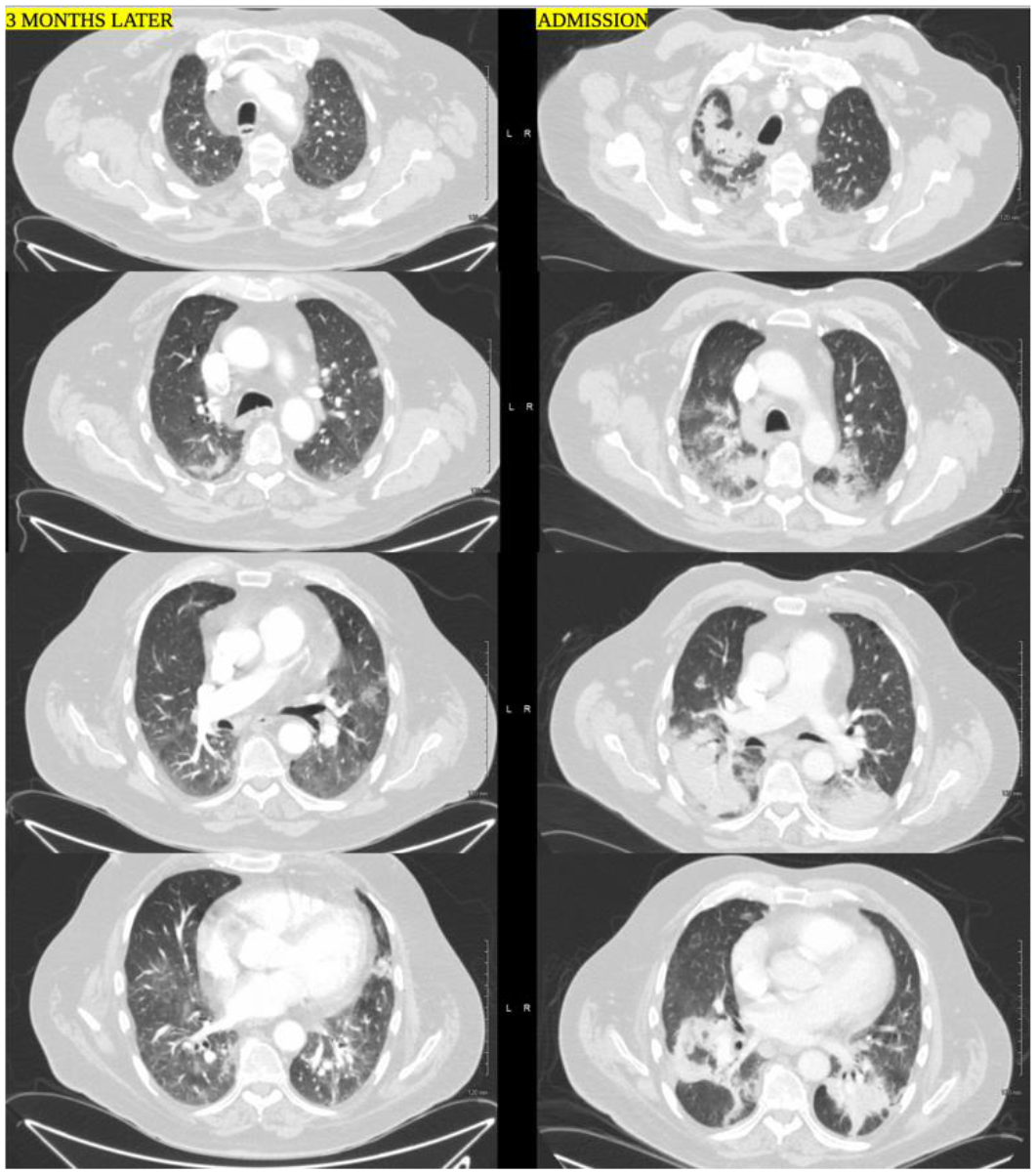
CTA chest 3 months post-admission (left, “3 MONTHS LATER”) vs. admission (right, “ADMISION”). There is general resolution of the heterogeneous multifocal opacities/consolidation.
P41. Primary Malignant Melanoma of the Lung: A Case Report
Mirna Mikhael1, Muhammad Salyana1, Navaneeth Kumar1, Kulothungan Gunasekaran1, Mallappa Neelappa1
1 Yuma Regional Medical Center, Yuma, AZ, United States.
Introduction: Primary malignant melanoma of the lung is an extremely rare neoplasm. Here we present an interesting case of primary malignant melanoma of the lung with no skin involvement. Case Presentation: A 77 year old male with history of smoking, COPD, DVT on rivaroxaban presented with complaint of shortness of breath on exertion and cough with sputum. Patient denied chest pain, fevers, chills, unintentional weight loss. Vitals, physical exam and labs were unremarkable. CT scan showed enhancing left infrahilar mass invading mediastinal pleura, and mildly prominent mediastinal lymph nodes (figure 1a). Bronchoscopy revealed near complete occlusion of the distal left main stem after the takeoff of the left upper lobe. EBUS-guided lymph node biopsy and endobronchial biopsy of left lower lobe were positive for malignancy. Immunohistochemical stains performed were positive for SOX10 and S-100 consistent with malignant melanoma and Ki-67 proliferation index was increased (figure 1b). Patient was referred to Oncology for further management.
Discussion: Malignant melanoma is most commonly seen in the skin. It has also been reported in other organs, however extremely rare. Primary malignant melanoma of the lung accounts for only 0.01% of all primary lung tumors.1 Paliogiannis et al performed a systematic review of primary malignant melanoma of the lung showing that the disease was most commonly seen in middle aged patients, mean of 60 years old, occurring more in males than in females. The lesions were also noted to be found more commonly in the lower lobe of the left lung.2 In seven out of eight tumors tested in one study, immunohistochemical testing showed diffuse strong positivity for S-100, HMB-45, and vimentin.1 The systematic review showed that approximately 70% of the patients underwent surgical treatment as opposed to chemotherapy or other treatments, and had a higher survival rate.2
Conclusion: Primary malignant melanoma of the lung is an extremely rare finding and should be considered in diagnoses of solitary lesions of the lung even without skin lesions as seen in our case.
References: 1. Wilson RW, Moran CA. Primary melanoma of the lung: a clinicopathologic and immunohistochemical study of eight cases. Am J Surg Pathol. 1997 Oct;21(10):1196-202. doi: 10.1097/00000478-199710000-00010. PMID: 9331292. 2. Paliogiannis P, Fara AM, Pintus G, Abdel-Rahman WM, Colombino M, Casula M, Palmieri G, Cossu A. Primary Melanoma of the Lung: A Systematic Review. Medicina (Kaunas). 2020 Oct 30;56(11):576. doi: 10.3390/medicina56110576. PMID: 33142971.

P42. Long Non-coding RNA MALAT1 Regulates HMOX1 in Sickle Cell Disease-associated Pulmonary Hypertension
Viranuj Sueblinvong1, Sarah S. Chang1, Jing Ma1, David Archer1, Benjamin T. Kopp1, Roy Sutliff2, Changwon Park3, Michael Hart1, Bum-Yong Kang1
1 Emory University School of Medicine, Atlanta, GA, United States. 2 National Institute of Health, Washington, DC, United States. 3 Louisiana State University, New Orleans, LA, United States.
Purpose of Study: Pulmonary hypertension (PH) causes morbidity and mortality in sickle cell disease (SCD). The release of heme during hemolysis triggers endothelial dysfunction and contributes to PH. Long non-coding RNAs (lncRNAs) may play a pivotal role in endothelial dysfunction and PH pathogenesis. This study determines lncRNAs that are affected by SCD and identifies MALAT1 as an important regulator of heme oxygenase-1 (HMOX1).
Methods Used: Total RNAs were isolated from 15-17 weeks old sickle cell (SS) mice and littermate control (AA) lungs and subjected to lncRNA expression profiling using the Arrystar™ lncRNA array. Raw signal intensities were normalized in quantile method by GeneSpring GX software. Volcano plot filtering was used to screen for differentially expressed lncRNAs with statistical significance (fold change >1.5, p< 0.05).
Summary of Results: A total of 2,302 lncRNAs were upregulated and a total of 2,546 lncRNAs were downregulated in lungs of SS mice compared to AA mice. To validate differentially expressed lncRNAs in human and mouse, 6 lncRNAs were selected for quantitative PCR. We found that the levels of metastasis-associated lung adenocarcinoma transcript 1 (MALAT1) were increased in SS mouse lungs. Human pulmonary artery endothelial cells (HPAECs) were treated with hemin and analyzed for MALAT1 or HMOX1 levels, which were increased in hemin-treated HPAECs. Lastly, loss of MALAT1 function reduced HMOX1 levels and increased ET-1 and VCAM1 levels.
Conclusions: These results suggest that SCD modulates MALAT1-HMOX1 axis and further characterization of MALAT1 function may provide new insights into SCD-associated endothelial dysfunction, PH pathogenesis, and identify novel therapeutic targets.
P43. Chronic Alcohol Ingestion Disrupts Profibrotic Markers Oscillation in the Lung through Alteration of Circadian Signaling Molecules
Xian Fan1, Nicolas Diaz2, Kenkichi Baba2, Gianluca Tosini2, Viranuj Sueblinvong1
1 Department of Medicine, Emory University School of Medicine, Atlanta, GA, United States. 2 Department of Pharmacology and Toxicology, Morehouse School of Medicine, Atlanta, GA, United States.
Purpose of Study: Alcohol exposure disrupts the molecular circadian rhythm in many organ systems. It has also been shown to exacerbate alcoholic liver steatosis and fibrosis. A mouse model with an altered circadian rhythm (clockΔ19) develops a spontaneous fibrotic-like pulmonary phenotype and experiences increased renal fibrosis associated with elevated TGFβ expression in response to an injury. These data suggest circadian disruption plays a role in tissue disrepair. We reported that alcohol primes the lung for fibrotic disrepair following acute injury. We speculated that alcohol disrupted the lung circadian signaling leading to dysregulation of lung repair process following an injury.
Methods Used: Eight-week-old C57Bl6/J or PER2::LUC mice were given 20% alcohol (v/v) in their drinking water for 6 weeks. Lungs were collected from PER2::LUC mice to assess for real-time circadian bioluminescent expression. C57Bl6/J mice were euthanized every 4 hours for over 24 hours and lungs were collected and analyzed for TGFβ1, CTGF, PDGFc and PDGFd expression. Core clock genes were analyzed from one time point of sample collection. Primary lung fibroblasts were exposed to alcohol (60 mM) for 24 h and assessed for CLOCK, BMAL1, Period 1 and 2, and RORα gene expression.
Summary of Results: Chronic alcohol ingestion is associated with PER2::LUC circadian phase shift an increase in peak phase and lengthening circadian period length and increased the expression and disrupted the circadian oscillation patterns of TGFβ, CTGF, and PDGFd in the lung. Chronic alcohol ingestion did not affect PDGFc expression or the oscillation pattern. Chronic alcohol ingestion is associated with downregulation of BMAL1 and downstream genes in the lung. In parallel, in vitro alcohol exposure downregulated the expression of BMAL1, Period 1 and RORα but had no effect on CLOCK expression in lung fibroblasts.
Conclusions: Chronic alcohol ingestion disrupts cellular circadian oscillation of several pro-fibrotic genes including TGFβ, CTGF, and PDGFd. We speculate that these changes are a consequence of alcohol-induced BMAL1 suppression, which leads to a dysregulation of the CLOCK-BMAL1 signaling pathway (as shown by attenuation of Period 1 and RORα expression in alcohol-treated lung fibroblasts). Our findings establish the importance of circadian rhythm regulation in alcohol-mediated lung disrepair and form the basis for a new approach to promote healthy repair in the lungs of individuals with alcohol use disorders.
P44. E-cigarette or Vaping Product Use-associated Lung Injury (EVALI) in a Young Adult: A Case Study
Rukmini K. Surnedi1, Vishesh Persaud2
1 Veterans Memorial High School, Corpus Christi, TX, United States. 2 Corpus Christi Medical Center, Corpus Christi, TX, United States.
Case Report: A 23-year-old immunocompetent male college student arrives at the emergency room with a three-day history of fever, shortness of breath, tachypnea, nausea, and diarrhea but no significant past medical and surgical history. The patient denies any known seasonal or drug allergies. The patient denies any family history of asthma or lung diseases. The patient denies any over-the-counter or prescription medications. Though the patient occasionally uses alcohol and vapes on a daily basis. The patient ran a fever maximum of 102.7 degrees Fahrenheit. The patient’s heart rate was 119 beats per minute, blood pressure was 124/82mmHg, and respiratory rate was 24 to 28 breaths per minute. In the patient’s examination, everything was normal except, when the medical examiner heard crackles during the lung auscultation. In the patient’s labs, the white blood count was elevated at 14.8*10^3/uL with neutrophil predominance, eosinophilia was also absent. Other inflammatory markers such as erythrocyte sedimentation rate which was at 97 mm/hr, C-reactive protein which was at 35 mg/dL, and procalcitonin which was at 2.13 ng/mL all were elevated. Leading to possible inflammation in the patient’s lungs. The patient’s serum lactic acid was normal. The viral panel, blood cultures, urine toxicology, Legionella Antigen, Pneumococcal Antigen, and Mycoplasma IgM antibody were all negative. But the patient was positive for cannabinoids. Basic metabolic panel - sodium, potassium, chloride, bicarbonate, and calcium levels were all within normal limits. Though serum creatinine was elevated. Liver function tests (LFT) were within normal limits. Arterial blood gas on 6 liters of nasal canal oxygen was: pH - 7.47 (7.35-7.45), CO2 - 33 (35-45 mmHg), oxygen - 68 (80-100 mmHg), bicarbonate - 24 (22-26 mEq/L). Chest radiography and CT chest shows air trapping, which is when air can go in but not out, mainly due to inflammation. They also show ground glass opecities also due to inflammation. Finally, it shows atlectisics, which is when small parts of the lung are collapsed. The patient was then diagnosed with EVALI (e-cigarette or vaping product use-associated lung injury). EVALI is typically found in patients who use THC containing products. In this particular patient, cannabinoids were found which may be a reason in why this patient developed EVALI. In order to treat the patient’s EVALI, high-dose steroids (methylprednisolone), empiric antibiotics, high flow oxygen were given, and managed in the ICU for seven days. The patient was discharged on a tapering dose of steroids (Prednisone 60 mg tapered over two weeks ) with a follow-up CT chest as an outpatient.
P45. Atypical Presentation of Hyperuricemia and Tophaceous Gout
NGON C. TRANG1, Nabhan KAmal1, Everardo Cobos1, Sabitha Eppanapally1
1 Internal Medicine, Kern Medical, Bakersfield, CA, United States.
Purpose of Study: To present a atypical case of genetic tophagenous gout
Methods Used: A single patient case report was conducted after IRB approval
Summary of Results: A 36-year-old man from Mexico with history of severe gout with tophi and chronic kidney disease (CKD) who presents to hospital with 1 week history of generalized weakness,oliguria,facial edema,and occasional nausea without vomiting.Patient has a strong family history of gout from great grandfather, grandfather, father, and paternal uncles.He has 3 female siblings with only one of them suffering from hyperuricemia with some pain in the joints without deformed tophi.Patient developed gout symptoms when he was 13 years old,and he had a learning disability.Physical exam shows numerous nonpainful tophi present on both hands,elbows, bilateral knee,ankle, and foot joints with calcification.Laboratory results show CKD5A3(sub-nephrotic proteinuria 2.6 grams),hyperkalemia with metabolic acidosis,hyperphosphatemia,normocytic anemia,and uric acid level 10.3.Complete retroperitoneal ultrasound revealed chronic renal parenchymal dysfunction without frank hydronephrosis.Nephrology recommended to initiate urgent hemodialysis as patient has advanced kidney disease with uremic symptoms and is oliguric.Allopurinol and prednisone are started without NSAIDs due to concern of worsening kidney function.Patient was also started on calcitriol,sevelamer and sodium bicarbonate.Genetic testing for purine metabolism disorders sent out to Invitae labs which later did not show a specific gene mutation. Hyperuricemia occurs when the uric acid level in the blood reaches 6.8 mg/dL or greater,and these high levels can cause crystals of monosodium urate (MSU) to deposit in the joints,kidneys, or other tissues.In the joints,these crystal deposits cause gout,a condition where the joints become painful,erythematous,warm,and edematous.In the kidneys,MSU crystal deposition causes uric acid nephrolithiasis with symptoms of flank pain,hematuria,nausea,and vomiting.Tophaceous gout is a type of chronic gout characterized by hard nodular masses known as “tophi” that are composed of high concentration of uric acid crystals.
Conclusions: Our patient’s rare presentation with extensive family history strongly suggests a genetic condition.However,genetic testing for purine metabolism did not show a specific gene mutation.This reinforces further investigation to elucidate this unusual disease.


Sidharth Mahapatra, MD, PhD, President
Zanthia Wiley, MD, FHM, FIDSA, President-Elect
Attaya Suvannasankha, MD, Immediate Past President
Samrat U. Das, MD, Past President
Viranuj Sueblinvong, MD, Secretary-Treasurer
Octavian Ioachimescu, MD, PhD, MBA, Membership Committee Chair
John Dickinson, MD, PhD, Publications Committee Chair
Theo Trandafirescu, MD, VP of Meetings and Programs
Joshua De Leon, MD, Eastern Section Chair
Steven J. Crosby, MA, BSP, RPh, FASCP, Eastern Section Chair-Elect
Lora Kasselman, PhD, MPH, Eastern Section Secretary-Treasurer
Andrea Hahn, MD, Eastern Section Past-Chair
Anupam Kotwal, MBBS, Midwestern Section Chair
Jeffrey Salomon, MD, MBA, Midwestern Section Chair-Elect
Syed Bukhari, MD, Midwestern Section Secretary-Treasurer
Jennifer Alexander-Brett, MD, PhD, Midwestern Section Past Chair
Gaurav Agarwal, MD, Southern Section Chair
Sheetal Kandiah, MD, MPH, Southern Section Chair-Elect
Jorge L. Cervantes, MD, PhD, Southern Section Secretary-Treasurer
Stephanie L. Baer, MD, Southern Section Past Chair
David A. Stevenson, MD, FACMG, Western Section Chair
Sebastien Fuchs, MD, PhD, Western Section Chair-Elect
Mimi Kim, MD, MSc, Western Section Secretary-Treasurer
Ricardo Correa, MD, Western Section Past Chair
Xiaoguang Sun, MD, PhD
Peter Wiernik, MD
Janice P. Dutcher, MD
Richard W. McCallum, MD, Journal of Investigative Medicine
Michael J. McPhaul, MD, Journal of Investigative Medicine, High Impact Case Reports





