
Abstract
Joint hypermobility syndrome (JHS) is a non-inflammatory hereditary disorder of connective tissue with varied clinical presentations, including frequent joint dislocations, hyperextensible skin, easy bruising, and abnormal paper-thin scar formation. Many of these patients have unexplained gastrointestinal (GI) symptoms. Our aim was to evaluate the prevalence of JHS in a tertiary gastroenterology motility clinic and the spectrum of functional bowel disorders in JHS patients. In this retrospective case series, we screened the medical records of 277 patients seen over 4 years at an academic GI Motility Center. The patients who met the criteria for JHS by Beighton hypermobility score were evaluated for the presence of functional GI disorders by Rome IV criteria. They also underwent gastric emptying study and glucose breath testing for small intestinal bacterial overgrowth. The prevalence of JHS in the study population was 9.7%. The mean age was 27 years, and 92.5% were female. The symptoms experienced by these patients include nausea/vomiting (89%), abdominal pain (70%), constipation (48%), and bloating (18.5%). The disorders associated with JHS include gastroparesis (52%), irritable bowel syndrome (55.5%), and gastroesophageal reflux disease (30%). Also, 10 patients (37%) were diagnosed with postural hypotension tachycardia syndrome secondary to autonomic dysfunction. Approximately 10% of patients with suspected functional bowel disorders have hypermobility syndrome. Hence, it is crucial to familiarize gastrointestinal practitioners with the criteria utilized to diagnose JHS and the methods to identify physical examination findings related to this condition.
Keywords
Significance of this study
Most patients with JHS are known to experience gastrointestinal (GI) symptoms.
Previous studies have reported a broad spectrum of structural and functional GI disorders in JHS.
The GI manifestations are related to the increased visceral compliance due to abnormal connective tissue in the gut wall that may result in hollow organ distensibility, affecting GI motility and contributing to the propensity for abdominal pain seen with this entity.
This study evaluates the prevalence and spectrum of functional bowel disorders in JHS patients at the academic GI Motility Center.
Essentially 10% of patients referred for suspected functional bowel disorder also have hypermobility syndrome.
GI practitioners should become familiar with all the criteria for JHS as well as how to elicit physical exam findings.
JHS should specifically be suspected in patients with idiopathic gastroparesis or nausea and vomiting of unknown etiology.
Introduction
Joint hypermobility syndrome (JHS) is a hereditary non-inflammatory connective tissue disorder that is often underdiagnosed. 1 Previously Ehlers-Danlos syndrome (EDS) was considered to be a separate disorder with EDS hypermobility type (EDS-HT) identical to JHS. With the identification of new genetic mutations, the International EDS Consortium proposed a revised EDS classification in 2017, which classified EDS into 13 subtypes. 2 Among these 13 subtypes, hypermobile EDS (hEDS) is the most common type. It is characterized by large and small joint hypermobility, frequent joint subluxations, dislocations, hyperextensible skin, easy bruising, poor wound healing, and abnormal paper-thin scar formation.3,4 In the revised EDS classification, the diagnostic category hEDS replaced the terminologies JHS and EDS-HT because of the lack of clinical distinction between these syndromes. 2 Despite the availability of genetic testing for other types of EDS, hEDS still does not have a genetic test for diagnosis. Hence the diagnosis of hEDS is based on the clinical signs and symptoms. 5 In simplistic terms, EDS comprises a group of hereditary connective tissue disorders, while JHS is a subtype of EDS. For this article, we used the term JHS to refer hEDS or EDS-HT.
Most patients with JHS experience gastrointestinal (GI) symptoms, which greatly influence their quality of life.6,7 A retrospective study at Cleveland Clinic in patients with hEDS showed that 76.2% of the study population was found to have GI dysmotility, and postural orthostatic tachycardia syndrome (POTS) was found to be an independent predictive factor for GI dysmotility. 8 Previous studies have reported a broad spectrum of structural and functional GI disorders in JHS.9,10 Structural anomalies include intestinal rupture, abdominal vessel rupture, abdominal or diaphragmatic hernias, internal organ or pelvic prolapses, and intestinal intussusceptions. The functional disorders associated with JHS include dysphagia, gastroesophageal reflux, dyspepsia, bloating, abdominal pain, irritable bowel syndrome, chronic constipation, and diarrhea. 11 In 2004, Hakim et al. reported a high rate of functional GI symptoms in patients with JHS (37%), and this was the first study to document the association between JHS and GI symptoms. 10 Some of the GI manifestations are related to increased visceral compliance due to abnormal connective tissue in the gut wall, that may result in hollow organ distensibility, affecting GI motility and contributing to the propensity for abdominal pain seen with this entity. JHS is also strongly associated with several other conditions, such as POTS, fibromyalgia, chronic pain syndrome, urinary problems, and anxiety disorders.1,12–14
So far none of the studies have systematically reported the spectrum of GI functional bowel disorders in patients with JHS. Therefore, our aim was to evaluate and classify functional GI disorders in JHS patients at GI motility center and to elucidate the prevalence of JHS in patients referred to a tertiary academic GI motility referral center.
Methods
Study design and data source
We report a single-center, retrospective case series at Texas Tech University Health Sciences Center El Paso (TTUHSC EP) Neurogastroenterology and GI Motility clinic, which serves as a tertiary care referral center in western Texas. After approval by the Institutional Review Board at TTUHSC EP, electronic medical records of the patients seen between January 2017 and September 2020 were reviewed to identify patients with JHS.
Brighton criteria
All patients attending the GI motility clinic were initially screened for generalized joint hypermobility using a validated five-point screening questionnaire, as described in Supplemental Table 1. Patients who answer “yes” to two or more questions in this simple five-part questionnaire were then assessed for JHS using the Brighton criteria (Supplemental Table 2). The Brighton criteria consist of two major criteria and eight minor criteria. Diagnosis of JHS requires two major criteria, or one major and two minor criteria, or four minor criteria. 6 One of the major criteria is the determination of Beighton score, which is assessed by five physical examination maneuvers (Table 1). Beighton scores of four or more will meet one of the major Brighton criteria for hypermobility. 15
Beighton score for joint hypermobility syndrome.*
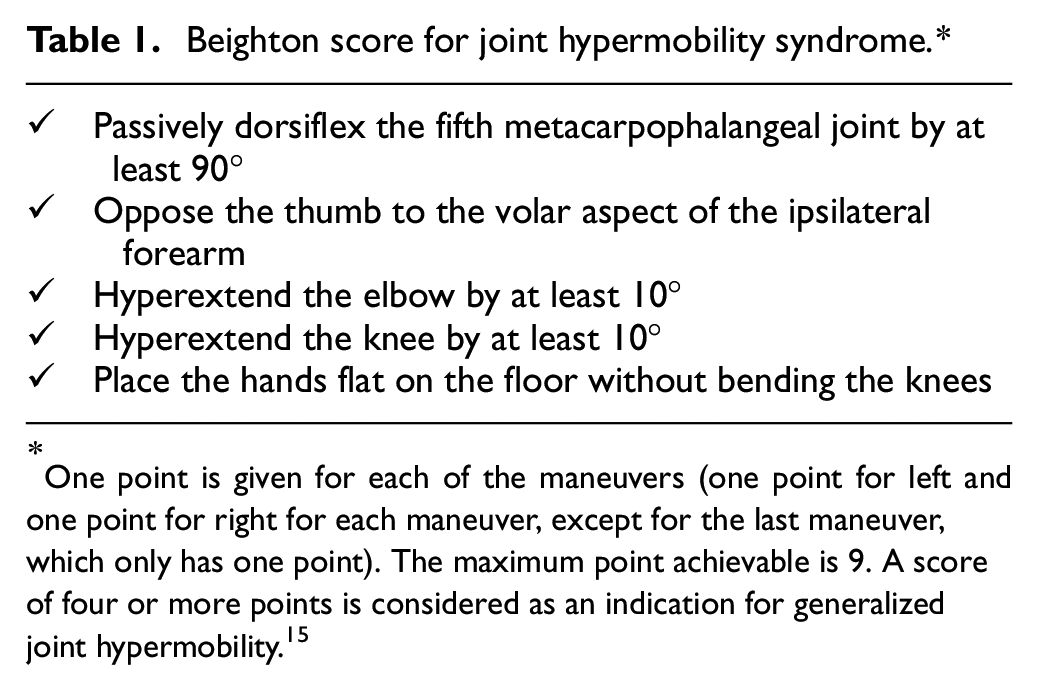
One point is given for each of the maneuvers (one point for left and one point for right for each maneuver, except for the last maneuver, which only has one point). The maximum point achievable is 9. A score of four or more points is considered as an indication for generalized joint hypermobility. 15
Patients underwent Rome IV criteria assessments as well as gastric emptying scintigraphy (GES) using gold standard egg beaten meal 4-h methodology to document gastroparesis (GP) or dumping syndrome (DS). These patients also underwent glucose breath testing to diagnose small bowel bacterial overgrowth.16,17 Patients’ symptoms were assessed using Patient Assessment of Gastrointestinal Disorders–Symptom Severity Index (PAGI-SYM) tool at the time of their initial motility clinic visit and in follow up visits for up to 2 years to monitor their long-term outcome. 18 The management options for GI symptoms in JHS is largely supportive in nature and symptom-focused based on specific diagnosis.
The study population were also evaluated for POTS, which is characterized by an increase in heart rate greater than 30 beats/min within 10 min of standing, in the absence of orthostatic hypotension (≥20 mmHg drop in systolic blood pressure with standing). 19 Most often POTS presents as pre-syncopal or syncopal events and associated feelings of lightheadedness, nausea, and palpitations. 20
Study population and definition of variables
All patients had to meet the inclusion criteria established for JHS as determined by the Brighton criteria. The exclusion criteria included (1) patients who were less than 18 years of age, (2) pregnant females, (3) patients with similar conditions such as Marfan’s syndrome and other EDS subtypes. 21
Statistical analysis
Data analysis was performed using IBM SPSS software version 26 (SPSS Inc, Armonk, NY, USA). Descriptive summary statistics are presented as means and standard deviation for continuous variables with normal distribution and frequencies with percentages for categorical variables. For continuous variables with non-normal distribution, we utilized non-parametric tests (Mann Whitney test) or reported median with the Interquartile range. Categorical and continuous variables were tested for statistical significance using chi-square tests and t-tests, respectively. A two-sided p < 0.05 was considered statistically significant.
Results
A total of 277 patients were evaluated at our GI motility center between January 2017 and September 2020. Among them, 27 patients (9.7%) were identified with a diagnosis of JHS. In the study population, 25 (92.5%) were females, and the average age at presentation was 27.5 years (range 18–54). GI symptoms were divided into upper and lower GI complaints as well as their association with a documented functional or motility disorder (Table 2). Predominant upper GI symptoms were present in 8 (30%) patients, lower GI symptoms in 7 (26%) patients, combination of upper and lower GI symptoms in 12 (44%) patients. The upper GI symptoms were nausea/vomiting (89%), GERD (30%) and dyspepsia (30%). The lower GI symptoms were lower abdominal pain (70%), constipation (48%), diarrhea (26%), bloating (18.5%), and rectal prolapse (11%).
Baseline demographics of the study population.
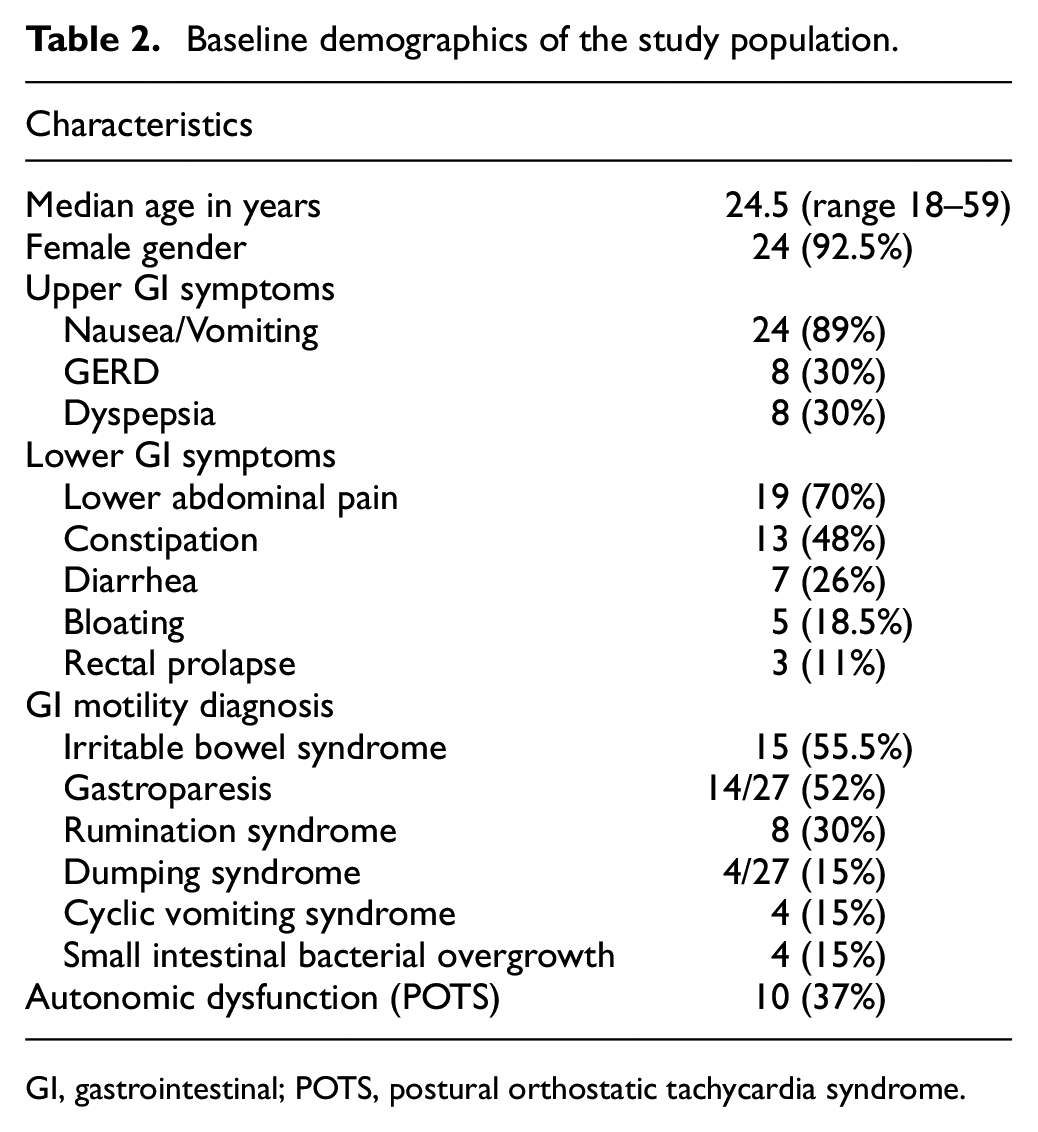
GI, gastrointestinal; POTS, postural orthostatic tachycardia syndrome.
Of the 27 patients, 14 (52%) had GP, 4 (15%) had DS, and 6 (22%) had normal gastric emptying. Small intestinal bacterial overgrowth was diagnosed in 4 (15%) patients. The other associated GI functional disorders include irritable bowel syndrome (IBS) (55.5%), rumination syndrome (30%), and cyclic vomiting syndrome (15%). Figure 1 depicts the percentage of functional GI disorders in JHS.
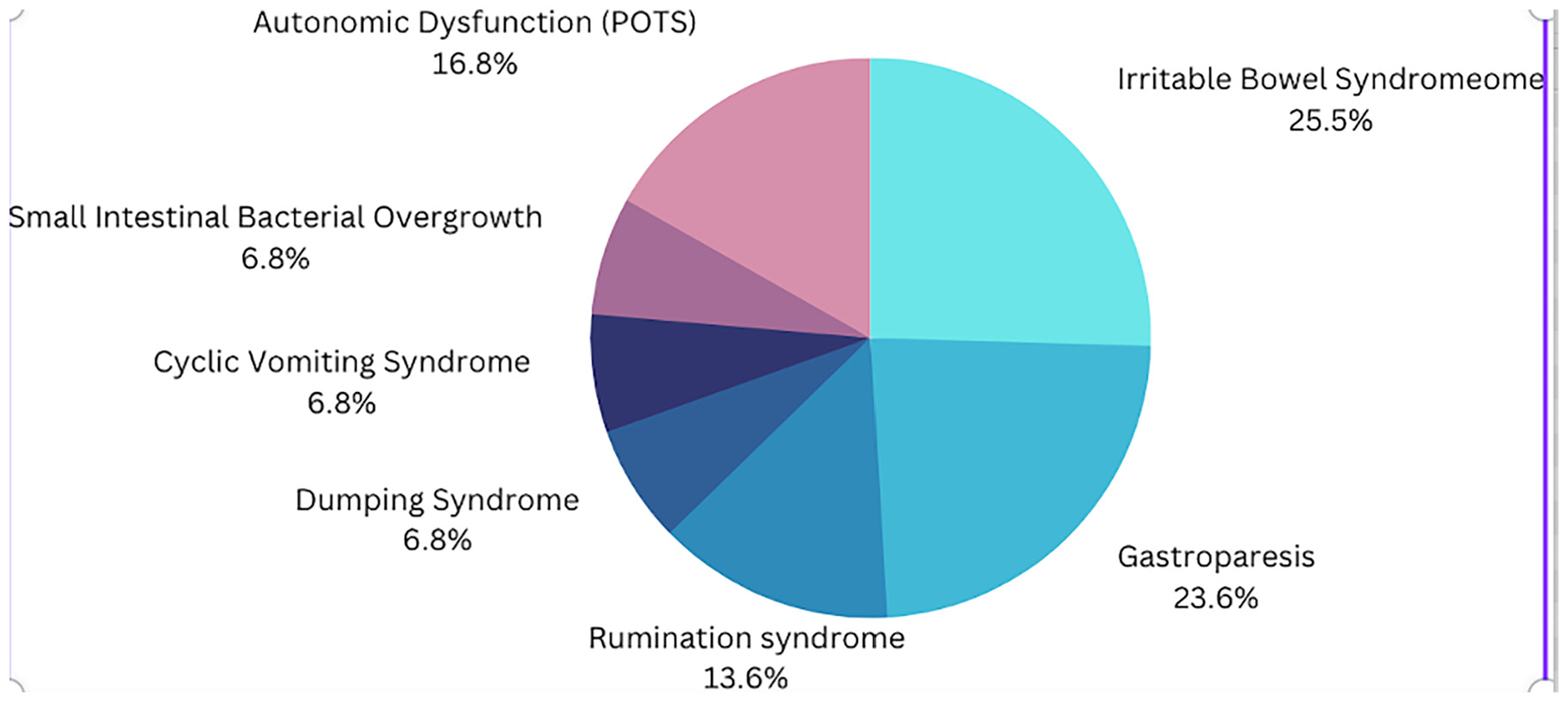
Prevalence percentage of functional gastrointestinal disorders in joint hypermobility syndrome.
The case series of 27 patients with JHS initially had a high PAGI-SYM score (63.8), which significantly improved to 52.3 (p < 0.05) over 2 years with appropriate treatment and follow-up. POTS was identified in 10 (37%) patients. Among these 10 patients, 9 (90%) patients had abdominal pain with nausea and vomiting as their chief complaints and were diagnosed with GP on GES. The remaining 1 (10%) patient had DS.
Discussion
We showed a prevalence of 9.7% for JHS in patients with functional GI disorders referred to an academic GI motility center. Nausea/vomiting and abdominal pain are the most common symptoms among this patient population. The GI functional disorders that were diagnosed in the study population include GP, IBS, small intestinal bacterial overgrowth, cyclic vomiting syndrome, rumination syndrome, and DS. IBS (55.5%) and GP (52%) were the most common accompanying conditions.
In our study, the prevalence of JHS in patients with functional GI disorders was 9.7%. Our findings showed a lower prevalence rate of JHS in patients with functional GI disorders when compared with the previous studies. In a study by Zarate et al., 27% of the patients evaluated at a tertiary care neurogastroenterology clinic were found to have JHS as evaluated by Beighton score. Their most common GI complaints included abdominal pain (81%), bloating (57%), nausea (57%), reflux symptoms (48%), vomiting (43%), constipation (38%) and diarrhea (14%). 22 It is important to consider that the prevalence of JHS in the general population was reported in the range of 10%–30%.23–25 However, most of these patients were unaware of their hypermobile features. JHS is more common in certain ethnicities (Asian, African) and females. 24
Previous studies have found a higher incidence of functional GI disorders in patients with JHS when compared to those who did not have JHS. In a prospective cross-sectional study by Fikree et al., patients with JHS were reported to have a higher incidence of heartburn, water brash, and post-prandial fullness when compared to the control group without JHS. 26 Also, the presence of GI symptoms was associated with the increased severity of the JHS and the presence of autonomic disturbances. 7 In a case-control study, JHS patients with functional GI disorders were found to have increased health impairment and high health care use. 27 Carbone et al. showed that 55% of patients with functional dyspepsia had JHS. However, no correlations were observed between the Beighton scores and gastric sensorimotor function. 28 Further prospective research will be required to identify the relationship between JHS, GI symptoms, and pathophysiological features. Finally, patients with JHS might experience multiple comorbidities such as widespread chronic pain, POTS, and mast cell activation disorder. Hence, it is crucial to identify these patients so that the comorbidities can be recognized as part of the spectrum of JHS disorder which can be treated through a multidisciplinary modality.
There have been studies done focusing on patients with specific GI symptoms. In a retrospective study by Mohammed et al., 200 patients with intractable constipation and rectal evacuation dysfunction were analyzed. The joint hypermobility and pelvic organ prolapse were reported in 33% and 31% respectively. 29 In a retrospective study by Menys et al., patients with hEDS and postprandial distress syndrome were compared with healthy controls. The patients with postprandial distress syndrome had similar gastric emptying time and gastric accommodation but had lower mean increase in gastric motility (11% vs 22%, p = 0.03). 30 Understanding the pathophysiologic basis for GI symptoms in JHS would be an invaluable tool when counselling these patients. They could be categorized into three groups. The anatomical impact from connective tissue laxity, the functional impact and the effect of autonomic disturbances. 31
In our study, 37% of the patients were found to have POTS. Among these patients with POTS, 90% of them had delayed GES, and 10% had rapid GES. POTS is a disorder characterized by dysfunctional autonomic control mechanisms, which is commonly associated with JHS. 32 In a case-control study by Zarate et al., functional GI disorder patients with JHS were found to have a higher prevalence of POTS (9.5%) when compared to those without JHS. 22 As illustrated in our study, POTS is frequently associated with abnormal GES. In a large retrospective cohort study of 163 patients with POTS, 18% had a delayed gastric emptying time, and 48% exhibited rapid gastric emptying time. 33
In modern medicine, the physical exam is often less emphasized than in past generations, with a heavier reliance on imaging techniques and laboratory testing. The diagnosis of JHS and POTS can be made with a thorough history and physical exam using a validated scoring system. They are frequently missed despite the relatively high prevalence amongst patients referred to a GI clinic, mainly due to the lack of awareness among the physicians about this condition. Patients presenting with various functional GI complaints should be questioned and examined, focusing on JHS, EDS, and POTS. Given the female predominance in JHS, it is not surprising that GP and IBS were frequently identified in the female gender. There should be a low threshold for obtaining a GES in JHS patients presenting with post-prandial upper GI symptoms. From reviewing the PAGI-SYM profile, the presence of abdominal pain was very prominent and often exacerbated by eating. In addition, based on PAGI-SYM monitoring, we could document improvement in symptoms with appropriate therapies over time.
There is a lack of evidence to guide therapeutic approaches for patients with JHS. Furthermore, given the various combinations of manifestations there is no single approach that will fit all JHS patients. The diagnosis and management of these patients in tertiary care centers are often guided by prior clinic experience from the strategies adapted from management of “similar” patient groups. 31 The greater awareness of JHS among physicians would facilitate earlier diagnosis and timely integrated multidisciplinary care. This approach of integrated care might reduce healthcare utilization including investigations, consultations, hospitalizations, unnecessary surgeries and interventions.
The main limitation of our study is that the patients were seen in a tertiary center specializing in motility disorders; hence, most patients have chronic GI symptoms. We did not investigate the prevalence of functional disorders in the group of 250 patients who did not meet JHS criteria. Hence, we could not assess the difference in the prevalence of GI disorders in the patients without JHS when compared to those with JHS. Future studies are needed to correlate the degree of GI symptoms with the degree of joint hypermobility assessed by the Beighton score.
We conclude from our data that: (1) Essentially, 10% of patients referred for suspected functional bowel disorder also have hypermobility syndrome. (2) GI practitioners should become familiar with all the criteria for JHS as well as how to elicit physical exam findings; (3) JHS should specifically be suspected in patients with idiopathic GP or nausea and vomiting of unknown etiology; (4) Recognizing symptoms suggesting dysautonomia and POTS, also correlates with the possibility of a gastric motility disorder; (5) The threshold to consider JHS should be particularly low in female patients whose meal-driven GI symptoms, particularly abdominal pain, are out of proportion to objective findings as determined by standard diagnostic testing. Future studies are necessary to identify more exact mechanisms behind GI symptoms in JHS patients. More longitudinal studies are also required in JHS to understand the influences of these symptoms on quality of life, nutrition, and psychological profile.
Supplemental Material
sj-pdf-1-imj-10.1177_10815589231210486 – Supplemental material for The spectrum of gastrointestinal functional bowel disorders in joint hypermobility syndrome and in an academic referral center
Supplemental material, sj-pdf-1-imj-10.1177_10815589231210486 for The spectrum of gastrointestinal functional bowel disorders in joint hypermobility syndrome and in an academic referral center by Priyadarshini Loganathan, Daniel Herlihy, Mahesh Gajendran, Zorisadday Gonzalez, Luis O Chavez, Karina Espino and Richard W. McCallum in Journal of Investigative Medicine
Footnotes
Author contributions
Study concept and design: DH, PL, RM. Analysis and interpretation of data: MG, PL. Drafting of the manuscript: MG, PL, ZG, KE.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics statements
Patient consent for publication: Not required.
Ethics approval: Texas Tech University health sciences center served as the institutional board review of the record, and approval was obtained on October 31, 2019 (E20006).
Competing interests
None declared.
Provenance and peer review Not commissioned, externally peer reviewed.
Data availability statement
All data relevant to the study are included in the article. Further data are available upon request to
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.