
Abstract
The monocyte to high-density lipoprotein-cholesterol (HDL-C) ratio (monocyte-to-HDL-C ratio) was proposed as a marker of atherosclerosis. Osteoporosis and atherosclerosis share common risk factors and pathophysiological mechanisms. This study aimed to assess the relationship between monocyte-to-HDL-C ratio and osteoporosis. Participants aged ≥50 years with complete bone mineral density (BMD), monocyte, and HDL-C examination data from the National Health and Nutrition Examination Survey (NHANES) 2013–2014 were included. Descriptive analysis was performed separately according to males and females. Weight linear regression and weight logistic regression analyses were used to analyze the association between the monocyte-to-HDL-C ratio and BMD and osteopenia and osteoporosis and vertebral fracture. A total of 1804 participants were included. Among the participants with osteopenia, 398 (48.31%) were males and 466 (51.91%) were females. Among those with osteoporosis, 38 (2.77%) were males and 95 (9.50%) were females. In females, monocyte-to-HDL-C ratio was negatively associated with femoral neck BMD (regression coefficient (β) = −0.18; 95% confidence interval (CI): (−0.29, −0.07)) and high monocyte-to-HDL-C ratio was associated with higher odds of osteopenia (odds ratio (OR) = 1.22; 95% CI: (1.01, 1.47)) and osteoporosis (OR = 1.68; 95% CI: (1.13, 2.49)) after adjusting for confounders. In males, only monocyte-to-HDL-C ratio >0.35 was observed to be associated with higher odds of osteoporosis (OR = 1.96; 95% CI: (1.02, 3.79)). Stratified analyses showed that similar results were also found in different populations. This study showed that the monocyte-to-HDL-C ratio was negatively associated with BMD and the risk of osteopenia and osteoporosis in females. The monocyte-to-HDL-C ratio may be a new marker of osteoporosis or osteopenia.
Several studies have shown that atherosclerosis and osteoporosis share common risk factors and pathophysiological mechanisms.
Recently, a new indicator, the monocyte to high-density lipoprotein-cholesterol (HDL-C) ratio (monocyte-to-HDL-C ratio), has been proposed as a marker of atherosclerosis.
The present study investigated the association between monocyte-to-HDL-C ratio and BMD.
The monocyte-to-HDL-C ratio was negatively associated with BMD and the risk of osteopenia and osteoporosis in females.
The monocyte-to-HDL-C ratio may be a new marker of osteoporosis or osteopenia in females.
Introduction
Osteoporosis is a common systemic bone disease characterized by microstructural degeneration of bone tissue and loss of bone mass, leading to bone fragility and increased risk of fracture. 1 Fractures due to osteoporosis are associated with higher medical costs, physical disability, impaired quality of life, and increased mortality. 2 A systematic review and meta-analysis revealed a global prevalence of 19.7% and 40.4% for osteoporosis and osteopenia, respectively. 3 Moreover, one-third of women and one-fifth of men over the age of 50 years are reported to have osteopenia and are at risk for osteoporotic fracture. 4 Early implementation of appropriate interventions is important to reduce the risk of osteoporosis and fracture, improve the quality of life, and prolong life expectancy.
Inflammation and oxidative stress are considered to be important factors in the decrease in bone mineral density (BMD). 5 Inflammatory mediators such as reactive oxygen species (ROS), pro-inflammatory cytokines, and chemokines directly or indirectly act on bone cells and are involved in the pathogenesis of osteoporosis.6–8 In addition to the direct involvement of monocytes in the inflammatory process, circulating monocytes play a key role as precursors of osteoclasts by producing cytokines involved in bone remodeling. 8 Furthermore, lipids play important roles in bone metabolism. 9 Papachristou et al. 10 reported that high-density lipoprotein (HDL) levels affect the development of an inflammatory microenvironment in which osteoblasts differentiate and function. Recently, a new indicator, the monocyte to HDL-cholesterol (HDL-C) ratio (monocyte-to-HDL-C ratio), has been proposed as a marker of atherosclerosis. 11 The monocyte-to-HDL-C ratio may reflect both inflammatory and lipid metabolic status. Several studies have shown that atherosclerosis and osteoporosis share common risk factors and pathophysiological mechanisms.12,13 However, the relationship between monocyte-to-HDL-C ratio and osteoporosis has not been reported. Therefore, it is worth exploring the relationship between monocyte-to-HDL-C ratio and osteoporosis.
The present study aimed to investigate the relationship between monocyte-to-HDL-C ratio and BMD and osteoporosis in people over 50 years. This may provide inexpensive, simple markers for the management of people at high risk for osteoporosis.
Methods
Study design and population
The data used for this cross-sectional study were extracted from the National Health and Nutrition Examination Survey (NHANES) database 2013–2014. The NHANES is a research program designed to assess the health and nutritional status of adults and children in the United States (https://www.cdc.gov/nchs/nhanes/about_nhanes.htm). The NHANES survey uses a complex, multistage, probability sampling method. The NHANES survey consists of an interview and physical examination component, where the interview includes demographic, socioeconomic, dietary, and health-related questions, while the examination component includes medical, dental, and physiological measurements, as well as laboratory tests conducted by trained medical personnel. This study included participants (1) aged ≥50 years; (2) with BMD examination data; and (3) with monocyte and high-density lipoprotein-cholesterol (HDL-C) examination data. Participants with malignant tumors were excluded. The requirement of ethical approval for this was waived by the Institutional Review Board of Anxi County Hospital because the data were accessed from NHANES (a publicly available database). The need for written informed consent was waived by the Institutional Review Board of Anxi County Hospital due to the retrospective nature of the study.
Outcomes and definition
The outcome variables include total femur BMD, femoral neck BMD, osteopenia, osteoporosis, and vertebral fracture. The DXA scans were acquired on Hologic QDR-4500A fan-beam densitometers (Hologic, Inc., Bedford, MA, USA) using software version Apex 3.2. BMD at the femoral neck and total femur was used to calculate the T-score ((respondent’s BMD—reference group mean BMD)/reference group standard deviation (SD)). The reference group for the femoral neck and total femur was composed of non-Hispanic White women aged 20–29 years from NHANES III. 14 Osteopenia was defined as a femoral neck or total femur BMD T-score ≤−1 and >−2.5, and osteoporosis was defined as a femoral neck or total femur BMD T-score ≤−2.5. The assessment of vertebral fracture using a semiquantitative technique, where Grade 0 indicates normal, Grade 1 indicates mild deformity, Grade 2 indicates moderate deformity, Grade 3 indicates severe deformity, and Grade 1 and above, was diagnosed as a vertebral fracture. 15
Measurement of monocyte and HDL-C levels
Monocyte counts were measured by complete blood counts using the Beckman Coulter DXH 800 (Beckman Coulter Inc., Brea, CA, USA). Serum was collected for the detection of HDL-C levels. Serum samples were treated with assay reagents and photometrically measured at 600 nm (secondary wavelength = 700 nm) using a Roche Cobas 6000 chemistry analyzer (Roche Diagnostics Inc., Basel, Switzerland). Detailed information on monocyte and HDL-C measurements was available on the NHANES website.16,17
Data collection
The demographic characteristics, dietary, physiological measurements, laboratory tests, and medication information were collected, including age, race/ethnicity (Mexican American, non-Hispanic White, non-Hispanic Black, other Hispanic, other races), education level (less than 9th grade, 9–11th grade, high school or equivalent, some college or AA degree, college graduate or above), marital status (married, others), postmenopausal (no, yes), drinking (no, yes), smoked at least 100 cigarettes in life (no, yes), ratio of family income to poverty, metabolic equivalent of task (MET), parental fracture (no, yes), parental fracture (no, yes), body mass index (BMI), triglycerides, total cholesterol, HDL-C, monocyte number, lymphocyte number, white blood cell count, calcium intake, energy intake, vitamin D intake, lipid-lowering drug (no, yes), anti-osteoporosis drug (no, yes), diabetes status (no, yes), monocyte-to-HDL-C ratio, total femur BMD, femoral neck BMD, osteopenia, osteoporosis, and vertebral fracture.
Statistical analysis
Continuous variables were expressed as mean and standard error (mean (S.E)) and categorical variables were presented as numbers and percentages (n (%)). Student’s t-test was used to determine the differences between groups for continuous variables and the χ2-test for categorical variables. The characteristics of participants were described separately according to male and female. Univariable and multivariable weight linear regression analyses were used to analyze the association of monocyte-to-HDL-C ratio with femoral neck BMD and total femur BMD, and the results were expressed as regression coefficient (β) and 95% confidence interval (CI). Univariable and multivariable weight logistic regression analyses were used to analyze the relationship between monocyte-to-HDL-C ratio and osteopenia and osteoporosis and vertebral fracture, and the results were presented as odds ratio (OR) and 95% CI. Among the models with different outcomes, variables with statistical significance in the univariable regression analysis were adjusted as confounders in the multivariable regression model (Supplemental Tables 1–3). Stratified analyses were performed based on different BMI (≤25 and >25 kg/m2), MET (≤median values and >median values; median values: 240 met/min in males and 120 met/min in females), the use of anti-osteoporosis drug, and postmenopausal (only for females).
All statistical analyses were conducted using R 4.2.0 software (R Foundation for Statistical Computing, Vienna, Austria). The difference was considered statistically significant at two-sided p < 0.05.
Results
Characteristics of participants
There were 2780 participants aged ≥50 years who were recorded in the 2013–2014 NHANES database. A total of 976 participants were excluded, including 550 with missing BMD data, 91 with missing monocyte data, and 335 with malignant tumors. Finally, 1804 participants were included in the analysis, of which 903 were females and 901 were males (Figure 1). The characteristics of males and females are shown in Table 1. The mean age of males was 61.28 (0.30) years and 62.33 (0.34) years for females. A higher percentage of males than females drank alcohol (86.53% vs 66.07%), while a higher percentage of females than males smoked (58.99% vs 47.15%). The mean MET of males was 948.65 (146.85) met/min and 508.09 (77.85) met/min for females. The mean monocyte-to-HDL-C ratio of males (0.54 (0.01)) was higher than that of females (0.38 (0.01)). The mean total femur BMD of males was 1.00 (0.01) g/cm2 and 0.87 (0.01) g/cm2 for females. The mean femoral neck BMD of males was 0.80 (0.01) g/cm2 and 0.72 (0.01) g/cm2 for females. In males, 398 (48.31%) participants had osteopenia, 38 (2.77%) participants had osteoporosis, and 62 (6.19%) participants had vertebral fracture. Among females, 466 (51.91%) participants had osteopenia, 95 (9.50%) participants had osteoporosis, and 58 (6.26%) participants had vertebral fracture.
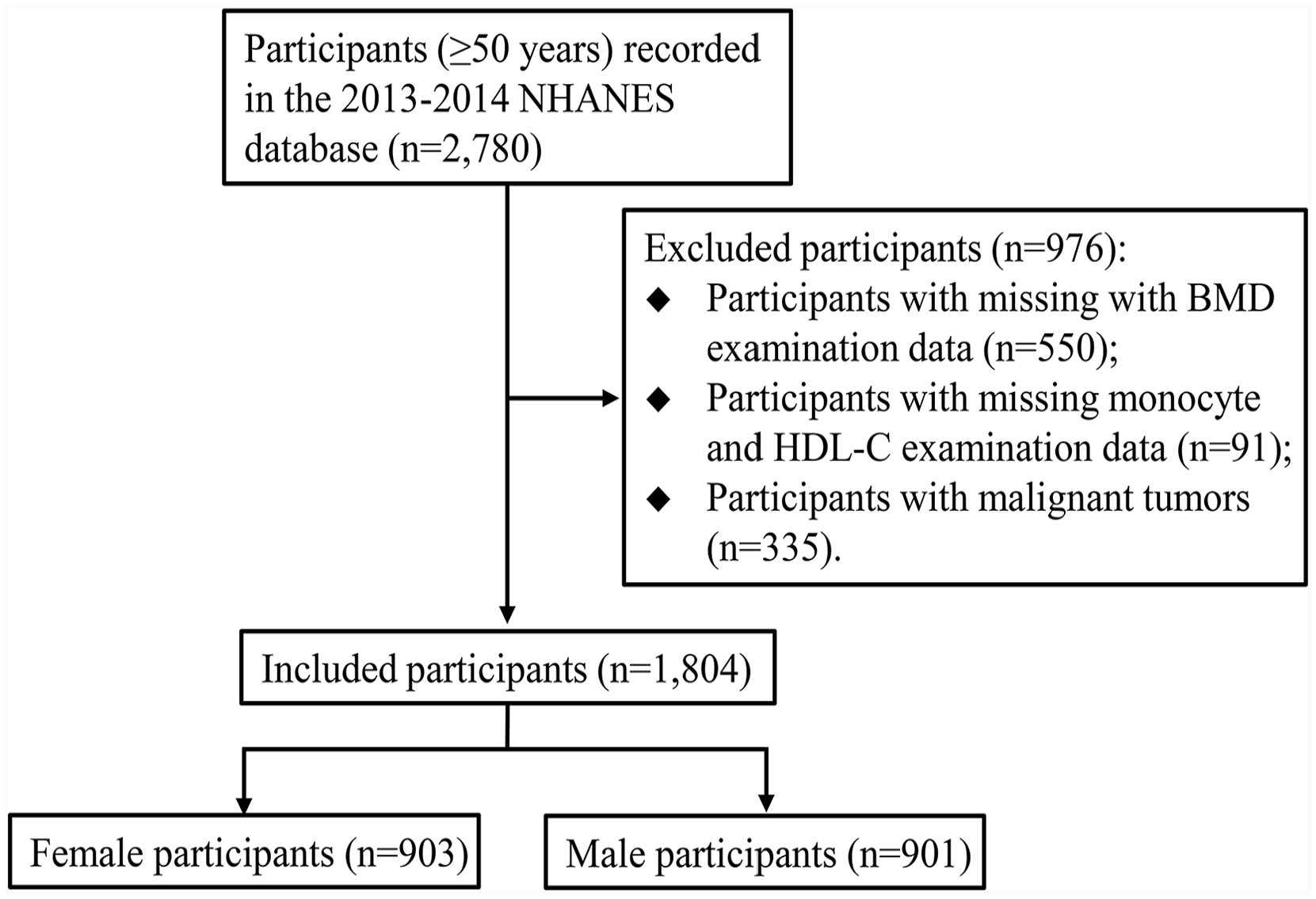
Flow chart of participants selection.
Characteristics of male and female participants.
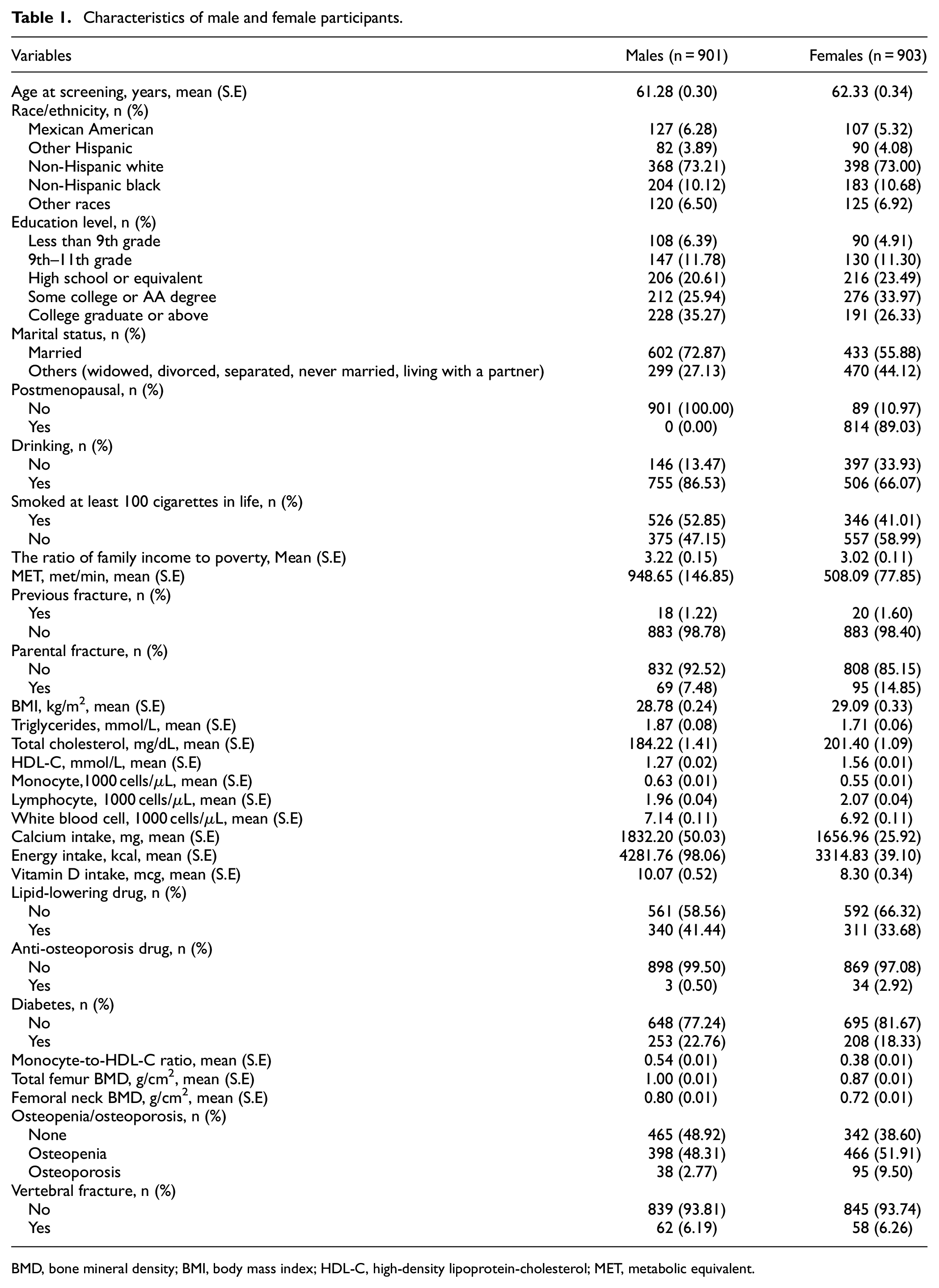
BMD, bone mineral density; BMI, body mass index; HDL-C, high-density lipoprotein-cholesterol; MET, metabolic equivalent.
Association between monocyte-to-HDL-C ratio and osteoporosis in females
The univariable and multivariable regression analyses of the association between monocyte-to-HDL-C ratio and osteoporosis in females are shown in Table 2. In the analysis of BMD, the monocyte-to-HDL-C ratio was negatively correlated with femoral neck BMD (β = −0.10; 95% CI: (−0.19, −0.02)), while no association was found between monocyte-to-HDL-C ratio and total femur BMD (p = 0.752). After adjusting for confounders, the monocyte-to-HDL-C ratio was still negatively associated with femoral neck BMD (β = −0.18; 95% CI: (−0.29, −0.07)). In the analysis of osteopenia, osteoporosis, and vertebral fracture, a high monocyte-to-HDL-C ratio was associated with higher odds of osteopenia (OR = 1.22; 95% CI: (1.01, 1.47)) and osteoporosis (OR = 1.68; 95% CI: (1.13, 2.49)), whereas no relationship was observed between monocyte-to-HDL-C ratio and vertebral fracture (p = 0.370). After adjusting for confounders, high monocyte-to-HDL-C ratio was still related to higher odds of osteopenia (OR = 1.56; 95% CI: (1.19, 2.05)) and osteoporosis (OR = 2.23; 95% CI: (1.41, 3.53)). When categorized by a median monocyte-to-HDL-C ratio of 0.42, these results were still observed in participants with monocyte-to-HDL-C ratio ≥0.42 compared to those with monocyte-to-HDL-C ratio <0.42.
Univariate and multivariate regression analyses of the association between monocyte-to-HDL-C ratio and osteoporosis in females.
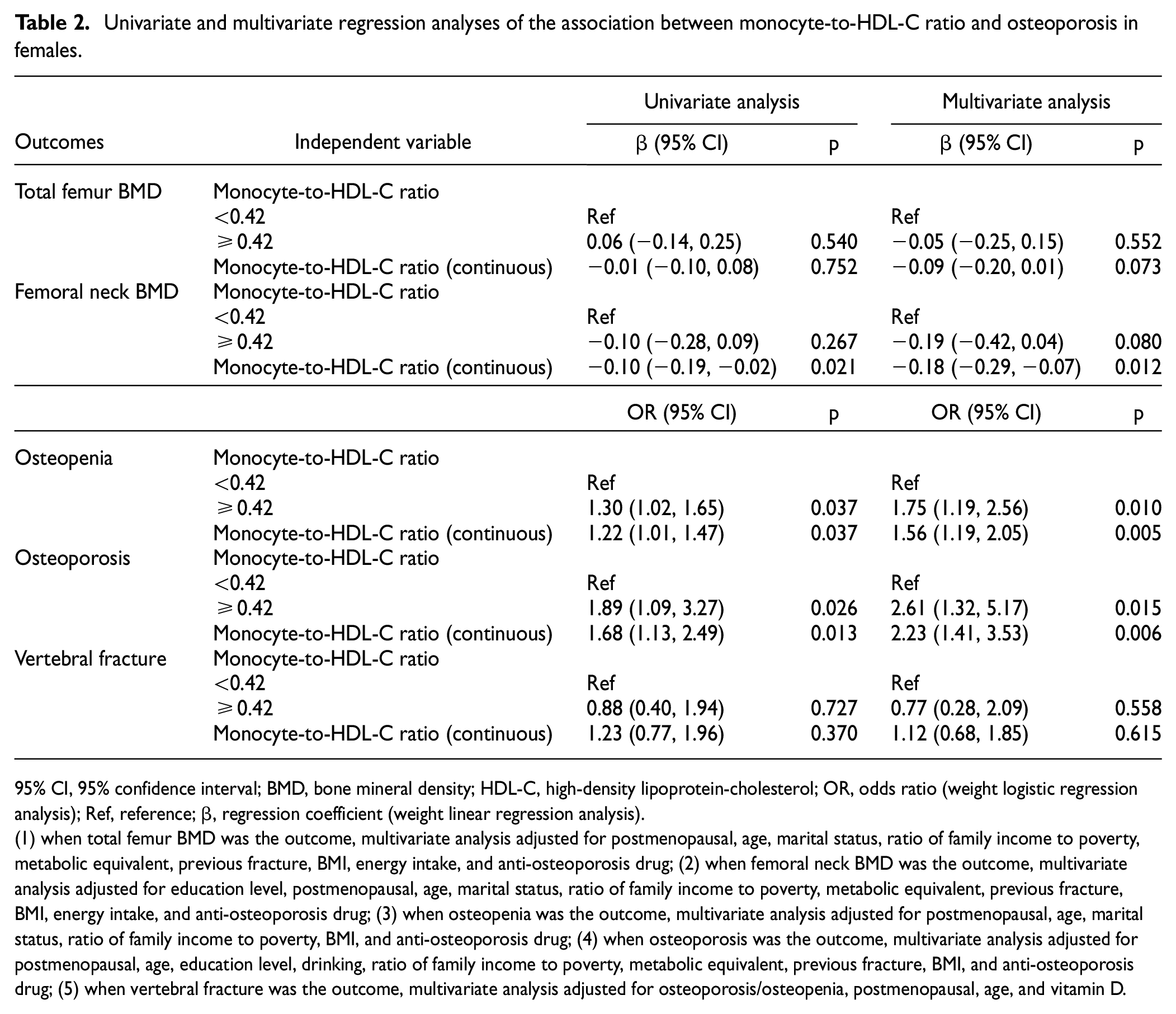
95% CI, 95% confidence interval; BMD, bone mineral density; HDL-C, high-density lipoprotein-cholesterol; OR, odds ratio (weight logistic regression analysis); Ref, reference; β, regression coefficient (weight linear regression analysis).
(1) when total femur BMD was the outcome, multivariate analysis adjusted for postmenopausal, age, marital status, ratio of family income to poverty, metabolic equivalent, previous fracture, BMI, energy intake, and anti-osteoporosis drug; (2) when femoral neck BMD was the outcome, multivariate analysis adjusted for education level, postmenopausal, age, marital status, ratio of family income to poverty, metabolic equivalent, previous fracture, BMI, energy intake, and anti-osteoporosis drug; (3) when osteopenia was the outcome, multivariate analysis adjusted for postmenopausal, age, marital status, ratio of family income to poverty, BMI, and anti-osteoporosis drug; (4) when osteoporosis was the outcome, multivariate analysis adjusted for postmenopausal, age, education level, drinking, ratio of family income to poverty, metabolic equivalent, previous fracture, BMI, and anti-osteoporosis drug; (5) when vertebral fracture was the outcome, multivariate analysis adjusted for osteoporosis/osteopenia, postmenopausal, age, and vitamin D.
Association between monocyte-to-HDL-C ratio and osteoporosis in males
Table 3 presents the univariable and multivariable regression analyses of the association between the monocyte-to-HDL-C ratio and osteoporosis in males. In the analysis of BMD, the monocyte-to-HDL-C ratio was positively correlated with femoral neck BMD (β = 0.15; 95% CI: (0.08, 0.21)) and total femur BMD (β = 0.11; 95% CI: (0.03, 0.18)). After adjusting for confounders, no association was found between the monocyte-to-HDL-C ratio and femoral neck BMD (p = 0.604) and total femur BMD (p = 0.725). Similarly, no association was observed between the monocyte-to-HDL-C ratio and osteopenia (p = 0.099) and osteoporosis (p = 0.077) and vertebral fracture (p = 0.700) after adjusting for confounders. When categorized by a median monocyte-to-HDL-C ratio of 0.35, only monocyte-to-HDL-C ratio >0.35 was observed to be associated with higher odds of osteoporosis (OR = 1.96; 95% CI: (1.02, 3.79)) compared to those with monocyte-to-HDL-C ratio ≤0.35.
The association between monocyte-to-HDL-C ratio and osteoporosis in males.
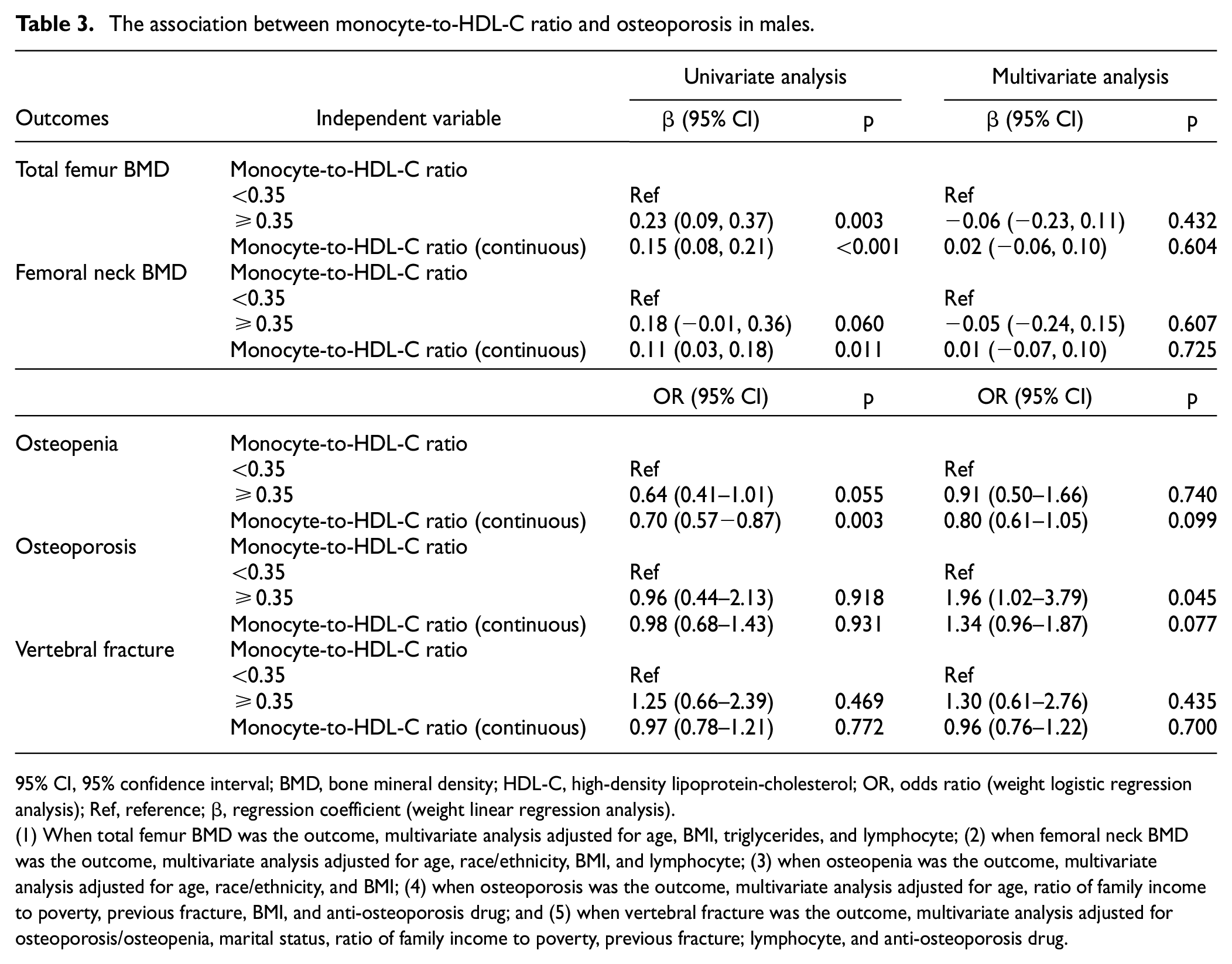
95% CI, 95% confidence interval; BMD, bone mineral density; HDL-C, high-density lipoprotein-cholesterol; OR, odds ratio (weight logistic regression analysis); Ref, reference; β, regression coefficient (weight linear regression analysis).
(1) When total femur BMD was the outcome, multivariate analysis adjusted for age, BMI, triglycerides, and lymphocyte; (2) when femoral neck BMD was the outcome, multivariate analysis adjusted for age, race/ethnicity, BMI, and lymphocyte; (3) when osteopenia was the outcome, multivariate analysis adjusted for age, race/ethnicity, and BMI; (4) when osteoporosis was the outcome, multivariate analysis adjusted for age, ratio of family income to poverty, previous fracture, BMI, and anti-osteoporosis drug; and (5) when vertebral fracture was the outcome, multivariate analysis adjusted for osteoporosis/osteopenia, marital status, ratio of family income to poverty, previous fracture; lymphocyte, and anti-osteoporosis drug.
Stratified analysis based on different populations
Figure 2 shows the multivariable regression analysis of the association between monocyte-to-HDL-C ratio and osteoporosis in populations with BMI ≤ 25 kg/m2, BMI > 25 kg/m2, MET ≤ median values, MET > median values, and anti-osteoporosis drug use. The monocyte-to-HDL-C ratio was negatively correlated with femoral neck BMD in females with BMI > 25 kg/m2, MET ≤ 120 met/min, anti-osteoporosis drug use, and pre-menopausal (all p < 0.05). Similarly, high monocyte-to-HDL-C ratio was related to higher odds of osteopenia and osteoporosis in females with BMI > 25 kg/m2, MET ≤ 120 met/min, anti-osteoporosis drug use, and pre-menopausal (all p < 0.05). In males, only monocyte-to-HDL-C ratio >0.35 was found to be associated with higher odds of osteoporosis in populations with BMI > 25 kg/m2, MET ≤240 met/min, and anti-osteoporosis drug use (p < 0.05).
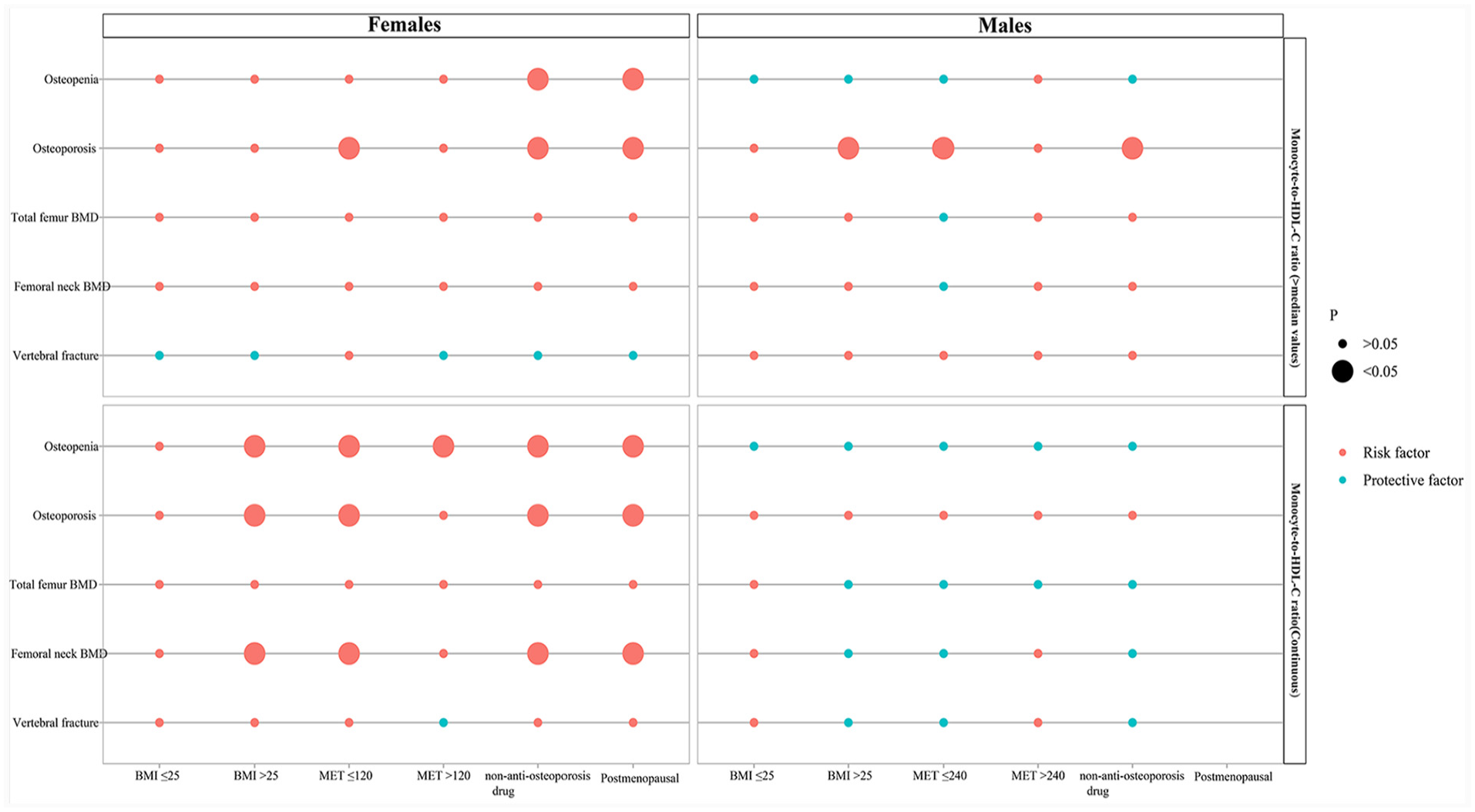
Multivariable regression analysis of the association between monocyte-to-HDL-C ratio and osteoporosis in different populations. The size of the circle area represents statistical significance, green represents protective factors, and red represents risk factors.
Discussion
The current study evaluated the association between the new index monocyte-to-HDL-C ratio and BMD in people aged ≥50 years. This study found that the monocyte-to-HDL-C ratio was negatively correlated with femoral neck BMD, and that a high monocyte-to-HDL-C ratio was associated with higher odds of osteopenia and osteoporosis in females. In males, a high monocyte-to-HDL-C ratio was only observed to be related to higher odds of osteoporosis. Similar results were found for stratified analyses based on different populations.
The monocyte-to-HDL-C ratio index was found to be primarily associated with cardiovascular disease. 11 Cetin et al. 18 found that a high monocyte-to-HDL-C ratio was correlated with a higher risk of adverse cardiac events in patients with the acute coronary syndrome since atherosclerosis and osteoporosis share common risk factors and pathophysiological mechanisms.12,13 This study explored the relationship between the monocyte-to-HDL-C ratio and BMD and osteoporosis. High monocyte count and low HDL-C levels may be relevant to inflammation19–21 and oxidative stress. 19 Circulating monocytes are a type of leukocyte that can further differentiate into a variety of cells such as macrophages, dendritic cells, and osteoclasts. 22 Circulating monocytes are important for osteogenesis and bone remodeling by producing cytokines (such as IL-1, IL-6) that promote osteoclast differentiation, activation, and apoptosis. 23 It was reported that HDL was related to the physiology and pathology of bone.10,24 Decreased HDL levels were correlated with the development of an inflammatory microenvironment that affects osteoblast differentiation and function. 10 However, the relationship between HDL-C and BMD has been inconsistently reported. Tang et al. 25 found that HDL-C levels were negatively correlated with BMD. Zolfaroli et al. 26 showed that HDL-C levels were positively related to the lumbar spine and femoral neck BMD in postmenopausal women.
Previous studies have evaluated the association between the monocyte-to-HDL-C ratio and cardiovascular mortality, 27 diabetic retinopathy, 28 and carotid plaque. 29 However, the relationship between the monocyte-to-HDL-C ratio and BMD has not been reported. The current study found that the monocyte-to-HDL-C ratio was mainly associated with BMD and osteoporosis in females. Specifically, the monocyte-to-HDL-C ratio was negatively correlated with femoral neck BMD, and a high monocyte-to-HDL-C ratio was associated with higher odds of osteopenia and osteoporosis in females. The sex difference in the relationship between the monocyte-to-HDL-C ratio and BMD may be related to sex hormones. Estrogens, androgens, and glucocorticoids alter the cellular composition of bone by regulating the supply and lifespan of osteoclasts and osteoblasts, thereby affecting BMD. 30 Estrogen deficiency is an important factor affecting osteoporosis, especially in postmenopausal women who experience estrogen deficiency. 31 Moreover, the decline in sex steroid levels that occurs with age, particularly the decline in bioavailable estrogen levels, can also contribute to age-related bone loss. 32 Stratified analyses displayed that the association between the monocyte-to-HDL-C ratio and BMD was found in females with BMI > 25 kg/m2, lower physical activity, and postmenopausal. Song et al. 33 found that high BMI played a causal role in increasing BMD, and the effect was similar on the whole skeleton. A systematic review reported that increased physical activity (mainly leisure-time activity or moderate or vigorous physical activity) was associated with a reduced risk of fracture among adults. 34
This study was the first to assess the association between the monocyte-to-HDL-C ratio and BMD. We conducted separate analyses in males and females and found that the relationship between the monocyte-to-HDL-C ratio and BMD was mainly found in females. However, some limitations of this study should be considered. First, the cross-sectional study design of this study could not yield a causal relationship, and future prospective studies are needed to explore the causal relationship between the monocyte-to-HDL-C ratio and BMD. Second, we did not assess the relationship between the monocyte-to-HDL-C ratio and BMD of the lumbar spine due to the serious lack of BMD data in the database for the lumbar spine and other sites. Third, although we considered the effects of confounders such as smoking, drinking alcohol, calcium intake, vitamin D, physical activity, anti-osteoporosis medications, and comorbidities, there may still be some potential confounders effects on outcomes.
Conclusions
The present study investigated the association between monocyte-to-HDL-C ratio and BMD. The monocyte-to-HDL-C ratio was negatively associated with BMD and the risk of osteopenia and osteoporosis in females. The monocyte-to-HDL-C ratio may be a new marker of osteoporosis or osteopenia in females. More prospective studies are needed to confirm the relationship between the monocyte-to-HDL-C ratio and BMD.
Supplemental Material
sj-docx-1-imj-10.1177_10815589231204057 – Supplemental material for Association between monocyte to high-density lipoprotein-cholesterol ratio and osteoporosis: An analysis of the National Health and Nutrition Examination Survey 2013–2014
Supplemental material, sj-docx-1-imj-10.1177_10815589231204057 for Association between monocyte to high-density lipoprotein-cholesterol ratio and osteoporosis: An analysis of the National Health and Nutrition Examination Survey 2013–2014 by Fushan Zhou, Liyong Wu, Guizhou Shen, Xintan Chen, Chaoyang Liu, Dongqin Huang, Mingmei Li, Chengwei Xie and Ruyu Zhan in Journal of Investigative Medicine
Footnotes
Contributors
FZ and RZ designed the study. FZ wrote the manuscript. LW, GS, XC, CL, DH, ML, and CX collected, analyzed, and interpreted the data. RZ critically reviewed, edited, and approved the manuscript. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Research ethics and patient consent
The requirement of ethical approval for this was waived by the Institutional Review Board of Anxi County Hospital because the data were accessed from NHANES (a publicly available database). The need for written informed consent was waived by the Institutional Review Board of Anxi County Hospital due to the retrospective nature of the study.
Data availability statement
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.