
Abstract
Introduction
The primary objective of this study was to assess cardiovascular risk among members of the Bulgarian Antarctic expedition and identify strategies for risk reduction. The combination of intense physical and psychological stress, prolonged cold exposure, isolation, and challenging travel conditions contributes to an increased risk of cardiovascular disease, especially given the participants’ mature age, which is a key factor in greater cardiovascular disease susceptibility.
Methods
This research included 29 participants (23 males and 6 females) with average ages of 43.0±8.00 y for the males and 45.5±11.31 y for the females. All participants spent 30 d in Antarctica. They were subjected to comprehensive assessments, including anthropometric measurements, physiologic evaluations, and biochemical analyses both before departure and shortly after return. The updated SCORE2 algorithm following the European guidelines was used to estimate the 10-y cardiovascular event risk, which factored in age, blood pressure, lipid profile, and smoking status. All participants underwent the veloergometer stress test under electrocardiographic control twice, before and after the expedition.
Results
The results indicated that while most participants fell into the moderate-risk category, some of them exhibited elevated-risk profiles, primarily influenced by obesity, cholesterol levels, systolic blood pressure, and serum ferritin levels. No critical cardiovascular events were reported during the expedition.
Conclusion
This study highlights the importance of pre-expedition screening, including the conduct of an exercise stress test, targeted risk-factor management, and continuous monitoring for safeguarding the health and physiologic resilience of Antarctic expedition participants, ultimately underscoring the feasibility and necessity of cardiovascular prevention strategies in extreme environments.
Introduction
By 2025, Bulgaria had successfully conducted 33 Antarctic scientific expeditions involving researchers from various scientific disciplines along with logistics staff and support personnel. Experience has consistently shown that participants with various functional capacities and health statuses have taken part in each mission. A core principle remains that all participants must be in a functional and healthy condition that allows them to carry out their specific duties with minimal health risk. Working and conducting research in Antarctica are associated with significant physical and psychological stress. 1 Contributing factors include long-distance travel across multiple climatic and time zones, isolation from familiar social environments, and exposure to extreme weather conditions. Employment in polar regions typically requires prolonged outdoor activity at low temperatures and frequent travel between sites for sample collection. Previous studies have shown that physical exertion in cold environments can impair maximal strength, muscular endurance, cardiovascular efficiency, metabolic function, and energy reserves.2–6
The health status of expedition members is crucial because they conduct research and work in a location without close access to advanced medical facilities and surgical equipment. Moreover, Antarctica's remoteness, frequent adverse weather conditions, and rough seas hinder medical evacuation. 7 The cold and windy weather, a common condition in Antarctica, can contribute to the development of acute coronary syndrome.8–10 Furthermore, the occurrence and progression of cardiovascular diseases (CVD) are age related, and many of the participants in the Antarctic expeditions are at an age where heart-related events are common.11,12 A survey of 225 Antarctic expedition participants from different nationalities revealed that 45% were in the 56- to 75-y age range and 30.2% were in the 36- to 55-y age range. 13 According to the American Heart Association, the incidence of CVD increases with age, affecting ∼40% of individuals aged 40 to 59 y, ∼75% of those aged 60 to 79 y, and ∼86% of those older than age 80 y. 14 The incidence of heart attacks also rises significantly with age, particularly after the age of 50 y. 15 In addition to age, the risk of developing CVD is influenced by many other factors, among which are overweight, smoking, hypertension, metabolic syndrome, diabetes, and dyslipoproteinemia.11,12 All these risk factors can be monitored and managed in the periods before and during expeditions to reduce the risk of cardiovascular events. Some authors recommend performing a pretravel risk assessment 4 to 6 wk before departure. 16 The latest guidelines on CVD prevention were developed by a dedicated task force comprising representatives from the European Society of Cardiology (ESC) and 12 affiliated medical societies. 17 As part of these guidelines, the Systematic Coronary Risk Evaluation 2 (SCORE2) Working Group and the ESC Cardiovascular Risk Collaboration (2021) introduced an updated algorithm for estimating 10-y cardiovascular risk. 18 This algorithm incorporates key risk markers, including age, systolic blood pressure, total cholesterol, high-density lipoprotein (HDL) cholesterol, and smoking status. A critical additional variable is the geographic region, classified into 4 categories of cardiovascular risk: low, moderate, high, and very high. These algorithms enable the estimation of an individual's risk of experiencing a cardiovascular event within the next 10 y and facilitate projections of risk reduction based on modifications of specific risk factors.
This study aimed to assess the CVD risk in participants in the 32nd Bulgarian Antarctic Expedition and to determine the possibilities for its reduction. In addition, basic anthropometric, physiologic, and biochemical indicators were measured to provide a more comprehensive picture of cardiovascular risk and serve as possible exclusion criteria for individuals with unacceptably high risk.
Methods
Participants
The studied individuals were participants in the 32nd Bulgarian Antarctic Expedition. There 29 participants (23 males and 6 females). The average ages of females and males were 45.5±11.31 y (range 32–56 y) and 43.0±8.00 y (range 26–59 y), respectively. The Bulgarian Antarctic Base operates seasonally, from November through March, when conditions are relatively mild, with only occasional periods of extreme cold and strong winds. Due to its limited capacity, the base hosts scientists and personnel in rotating teams, arriving and departing according to their research missions’ duration and specific requirements. The participants involved in this research had various positions in the expedition and spent 30 d in Antarctica, arriving and departing in groups. All of them left by plane from Sofia and, after several transfers, reached Argentina, from which they reached the Bulgarian Antarctic Base St. Kliment Ohridski on Livingston Island (62°38′27″S 60°21′53″W, 15 m above sea level; Figure 1) with the Bulgarian scientific research vessel Saints Cyril and Methodius (RSV 421) through the Drake Passage for 3 d.
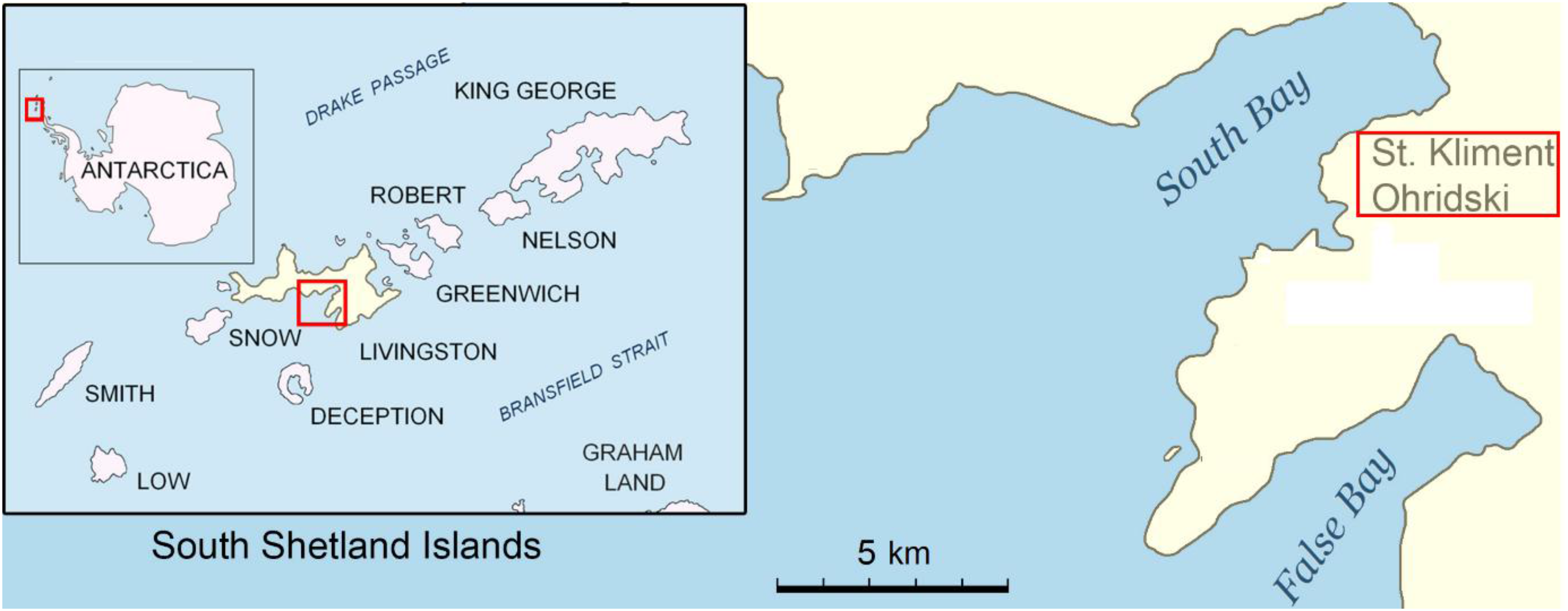
Location of the Bulgarian Antarctic Base “St. Kliment Ohridski” at the eastern coast of the South Bay, Livingston Island, South Shetlands. (Source: Bulgarian Antarctic Institute, http://www.bai-bg.net/bulgarian-base.html).
Before departure, every participant in a Bulgarian Antarctic expedition was required to undergo a comprehensive medical examination including medical history and physical examination, basic clinical laboratory tests, and dental status assessment. The final decision on participation or exclusion of an individual from the particular expedition was taken collectively by the expedition organizers and the responsible medical team.
For the purpose of this study, all participants underwent anthropometric and functional assessments (ie, stress test) as well as blood sampling for biochemical analyses both before departure and no later than 3 d after their return. They were fully informed about the aims of the study and provided written informed consent to participate. The research was approved by the Ethics Committee at the National Sports Academy, Sofia, Bulgaria (Approval No. EC-NSA-2025-003).
Anthropometry
Anthropometric indicators—weight (kg), body mass index (BMI, kg·m–2), and body fat percentage (BF%)—were measured using the InBody 230 Body Composition Analyzer (InBody Co, Ltd, Seoul, South Korea) under standardized conditions. Participants were assessed in the morning, in a fasting state, and wearing light clothing (underwear).
Physical Examination
Some physiologic parameters—heart rate at rest (HRrest, beats/min), systolic blood pressure (SBP, mm Hg), and diastolic blood pressure (DBP, mm Hg)—were measured by the medical doctor using standard clinical procedures.
Stress Test
To determine the functional capabilities of expedition participants and verify that even those with high cardiovascular risk could perform strenuous physical exertion, an exercise stress test was performed on a bicycle ergometer (ERGOLINE ErgoSelect VIAsprint 150P, Ergoline GmbH, Bitz, Germany). The initial power was 30 W, increasing by 30 W every 1.5 min until the heart rate reached 85% of the maximum predicted heart rate (=220–age). The test was conducted under constant electrocardiographic control and continuous automatic Коrotkoff sounds-based blood pressure measurement. The requirements for conducting the exercise stress test were strictly observed. 19 Successful completion of the test up to 85% of the maximum predicted heart rate without ST-segment changes or pathologic increases in blood pressure is considered indicative of good cardiorespiratory fitness of the tested person. This, in turn, serves as an independent index of lower cardiovascular risk and a low probability of an acute cardiovascular event.
Obtaining, Processing, and Analyzing Blood Samples
Peripheral blood samples were collected by a medical laboratory technician in the morning, after an overnight fast. The concentrations of glucose (Glu, mmol·L−1), total cholesterol (Chol, mmol·L−1), low-density lipoprotein cholesterol (LDL, mmol·L−1), high-density lipoprotein cholesterol (HDL, mmol·L−1), very low-density lipoprotein cholesterol (VLDL, mmol·L−1), triglycerides (Tg, mmol·L−1), ferritin (ng·mL−1), C-reactive protein (CRP, mg·L−1), and cortisol (Cort, nmol·L−1) were measured in serum at a certified clinical laboratory (Medical Diagnostic Laboratory “Kandilarov,” LLC, Sofia, Bulgaria).
Cardiovascular Disease Risk
The 10-y risk of cardiovascular disease (CVDrisk) for CVD prevention in clinical practice was calculated according to the ESC. Calculations include the following parameters: age, smoking status, SBP, Chol, HDL, sex, and geographic region. The coefficients used for the region were those for the fourth group, which has the highest CVDrisk, because Bulgaria falls into this group. 18 The CVDrisk is considered low for values of up to 5%, high for values between 5% and 10%, and very high for values above 10%. 20
Statistical Analysis
Descriptive statistics and the Shapiro-Wilk test for normality were performed. If the data followed a normal distribution, a paired-samples t test was applied; otherwise, the nonparametric Wilcoxon signed-rank test was used. Results are presented as mean±SD. All statistical analyses were conducted using SPSS version 26.0 (IBM Corp, Armonk, NY).
Results
The average weight, BMI, and BF of participants are presented in Table 1. The female average BF value (39.38±9.51%) was 9% higher than the upper healthy limit of 30%. The males average BF value BF (24.64±8.1%) was 2.5% higher than the upper healthy limit of 20%. Twelve participants (among them 1 female) had a BMI >25.0 kg·m−2 (overweight), and 10 participants (among them 2 females) had a BMI >30.0 kg·m−2 (different degrees of obesity; Table 3). After the expedition, participants’ average weight, BMI, and BF did not change significantly (Table 1).
Results of descriptive statistics of anthropometric parameters of participants before and after the expedition.
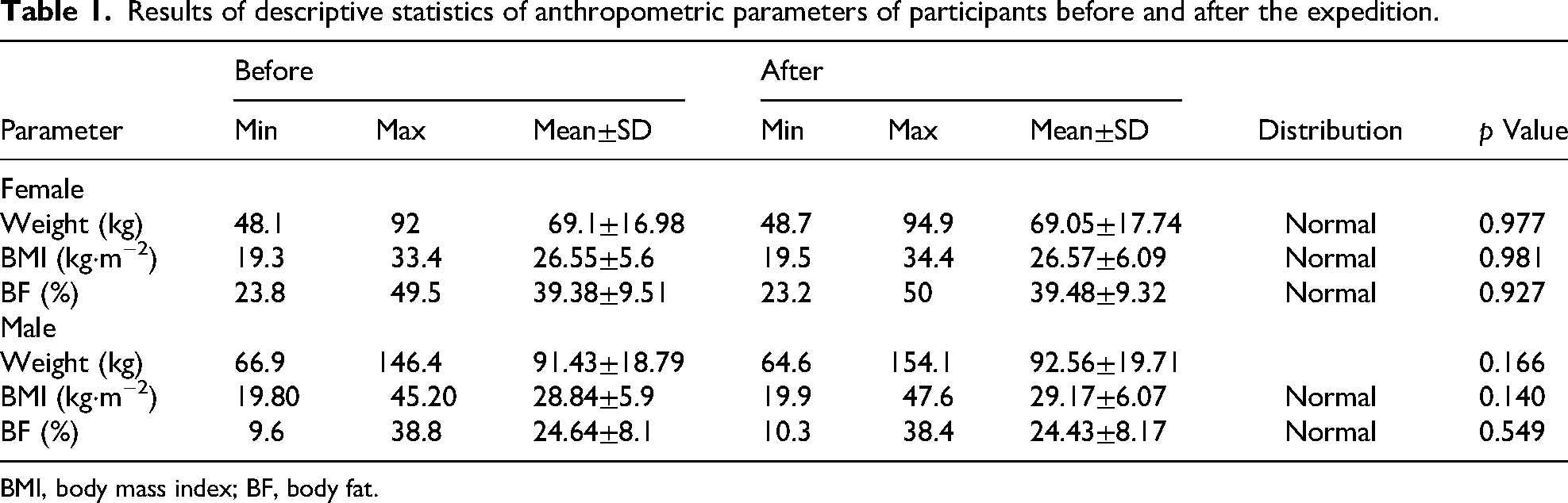
BMI, body mass index; BF, body fat.
Results of descriptive statistics of cardiovascular disease risk-related parameters of participants and significance of differences before and after the expedition.
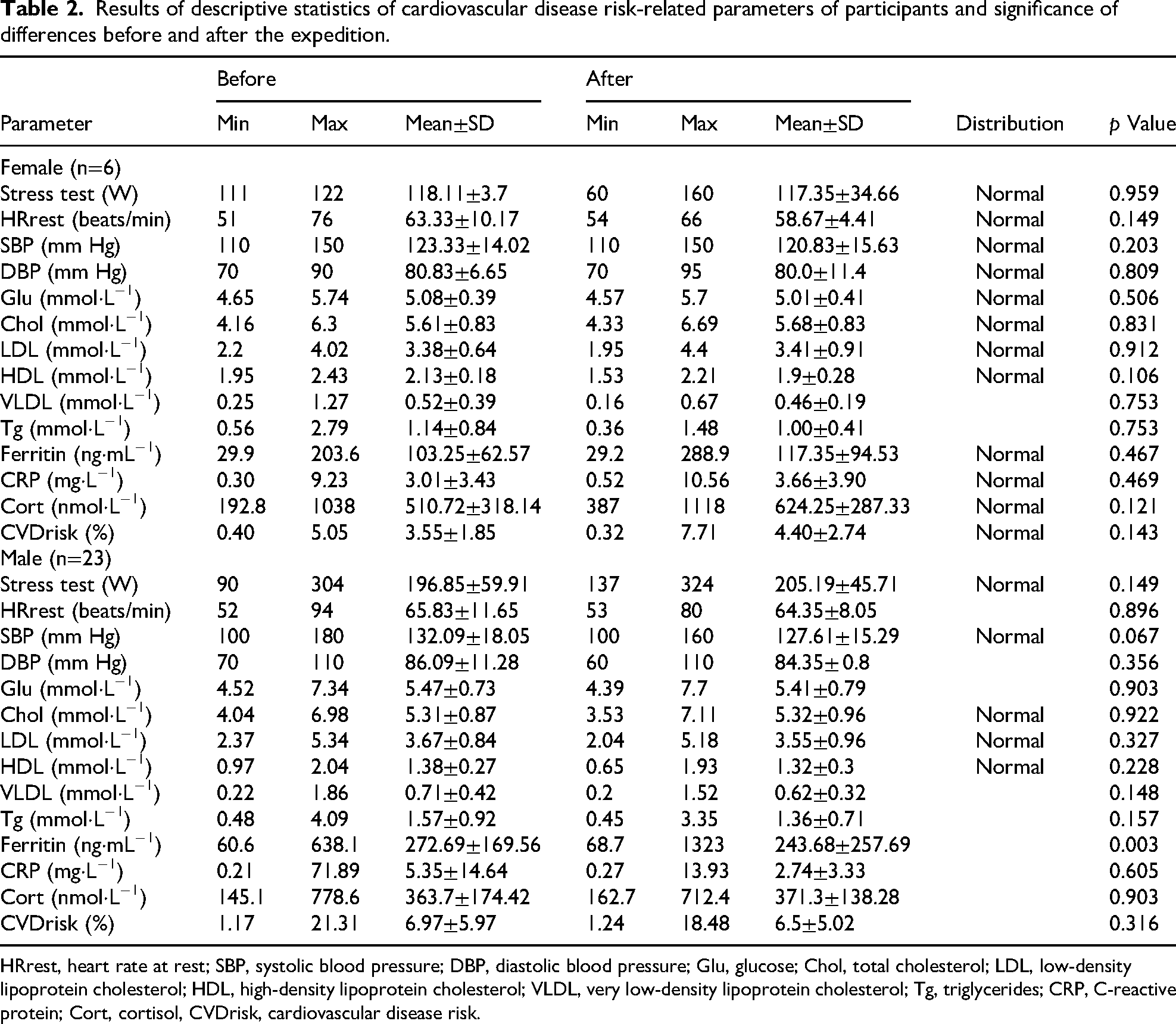
HRrest, heart rate at rest; SBP, systolic blood pressure; DBP, diastolic blood pressure; Glu, glucose; Chol, total cholesterol; LDL, low-density lipoprotein cholesterol; HDL, high-density lipoprotein cholesterol; VLDL, very low-density lipoprotein cholesterol; Tg, triglycerides; CRP, C-reactive protein; Cort, cortisol, CVDrisk, cardiovascular disease risk.
Participants with parameters deviating from healthy limits.
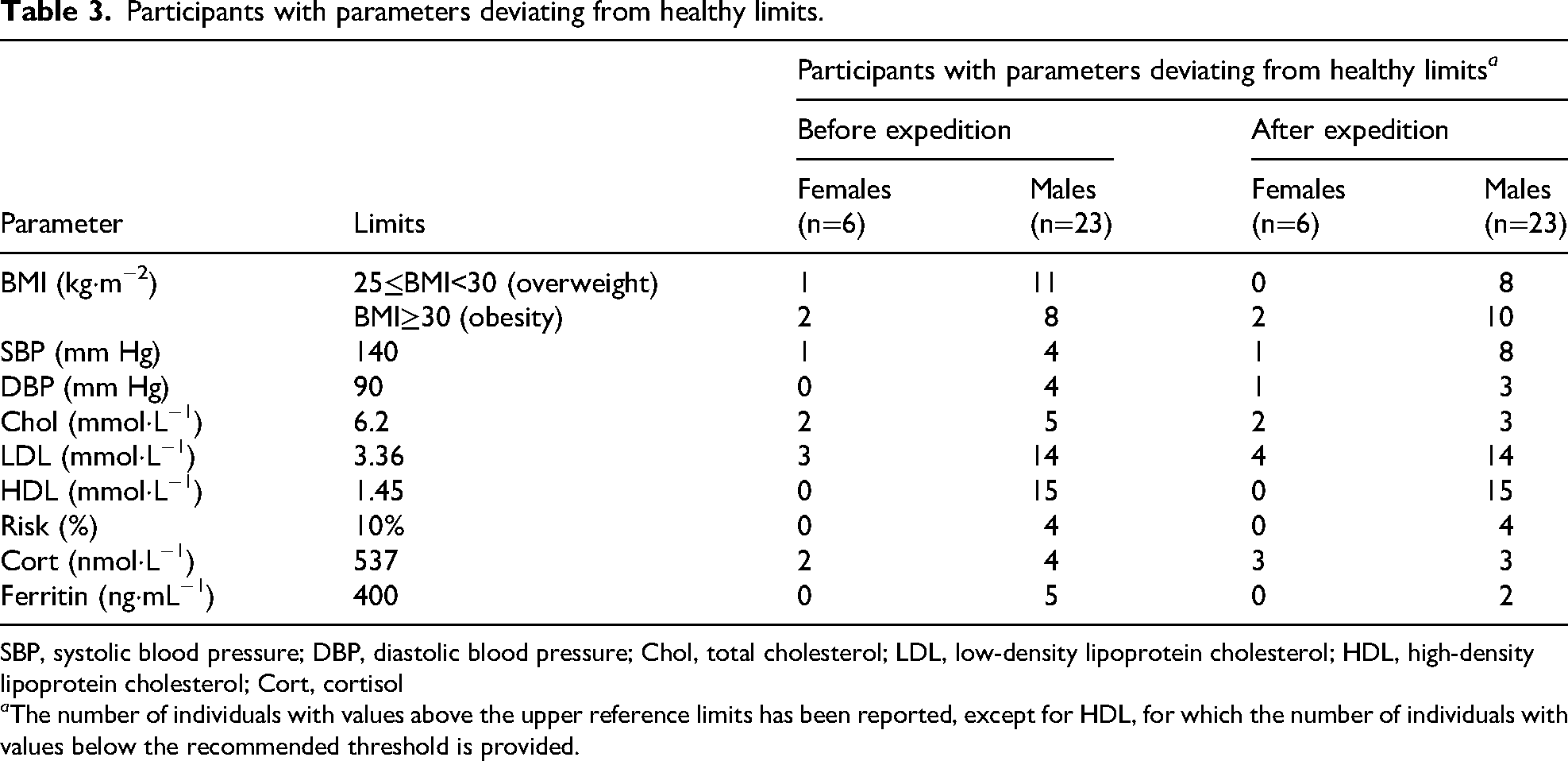
SBP, systolic blood pressure; DBP, diastolic blood pressure; Chol, total cholesterol; LDL, low-density lipoprotein cholesterol; HDL, high-density lipoprotein cholesterol; Cort, cortisol
a The number of individuals with values above the upper reference limits has been reported, except for HDL, for which the number of individuals with values below the recommended threshold is provided.
Table 2 presents the descriptive statistics of CVDrisk-related parameters for participants as well as the significance of the differences in the values obtained before and after the expedition. All participants successfully completed the exercise stress test without objective or subjective reasons to prematurely terminate the test for any participant. There were no significant changes in average power output at a heart rate of 85% for females and males after the expedition.
The average value of blood pressure (BP) was within normal limits. However, 5 participants had a SBP before the expedition >140 mm Hg, and 4 had a DBP >90 mm Hg (Table 3).
Before and after the expedition, the mean blood glucose level was below 6.0 mmol·L−1 (Table 2). However, before the expedition, 9 participants had Glu concentrations ranging from 6.1 to 7.7 mmol·L−1.
The average blood concentration of total cholesterol exceeded the borderline threshold (5.17 mmol·L−1 according to laboratory reference values; Table 2). This result was primarily due to 9 individuals who had elevated Chol concentrations before the expedition, including 7 whose values exceeded the upper limit of 6.2 mmol·L−1 (Table 3). The average LDL values for both males and females were slightly above the laboratory upper limit of 3.36 mmol·L−1, and 17 participants had values above this limit before the expedition (Tables 2 and 3). The average HDL concentration in females was above the recommended value of 1.45 mmol·L−1, and in males it was slightly below (Table 2). Before the expedition, 15 participants had HDL concentrations below the recommended value (Table 3). Average values of VLDL were near the upper limit of 0.65 mmol·L−1 (Table 2). However, 11 males before and 8 after the expedition had higher values, and 1 female had higher values before and after the expedition.
Triglyceride average values were below the upper reference range of 1.71 mmol·L−1 (Table 2), but 8 males and 1 female before and 5 males after the expedition had higher values.
The average 10-y CVDrisk for females before and after the expedition was 3.55±1.85% and 4.40±2.74%, respectively (Table 2). For males, this indicator was 6.97±5.97% before and 6.5±5.02% after the expedition. The average CVDrisk did not change significantly after the expedition for both sexes (Table 2). Four males had a very high risk (>10%, according to the ESC 20 ; Table 3). For 3 of them, the CVDrisk decreased after the expedition, but for 1 male it increased. Before the expedition, high CVDrisk (between 5 and 10%) was observed in 8 males, and 11 had low CVDrisk (<5%).
The average serum cortisol concentration among females was 510.72±318.14 nmol·L−1 before and 624.25±287.33 nmol·L−1 after the expedition (Table 2). For males, the corresponding values were 363.7±174.42 and 371.3 ± 138.28 nmol·L−1, respectively. Six individuals (2 females and 4 males) had serum cortisol levels exceeding the upper laboratory reference limit of 537 nmol·L−1 before the expedition, and the same number (3 females and 3 males) exhibited elevated levels after the expedition (Table 3).
The average serum ferritin concentration of females was 103.25±62.57 vs 117.35±94.53 ng·mL−1 (p>0.05), and for males, 272.69±169.56 vs 243.68±257.69 ng·mL−1 (p<0.01) before and after the expedition, respectively (Table 2). Before the expedition, 5 male participants had serum ferritin concentrations above the upper laboratory limit of 400 ng·mL−1, and after the expedition, only 2 males had elevated ferritin levels (Table 3), and in 1 of them the increase was significant (1857 ng·mL−1).
Table 4 represents the correlation matrix between risk-related parameters. A significant correlation was observed between BMI and CVDrisk as well as SBP. The observed significant correlations between CVDrisk and its components (ie, SBP, LDL, and HDL) were expected. There were significant positive correlations between ferritin and BMI and SBP and a negative correlation between ferritin and HDL. No significant correlations were found between serum cortisol and CVD risk or its components (SBP, LDL, and HDL) or between BMI and CRP. A high correlation was observed between ferritin and BMI, SBP, and CVDrisk after the expedition.
Correlation matrix between risk-related parameters.
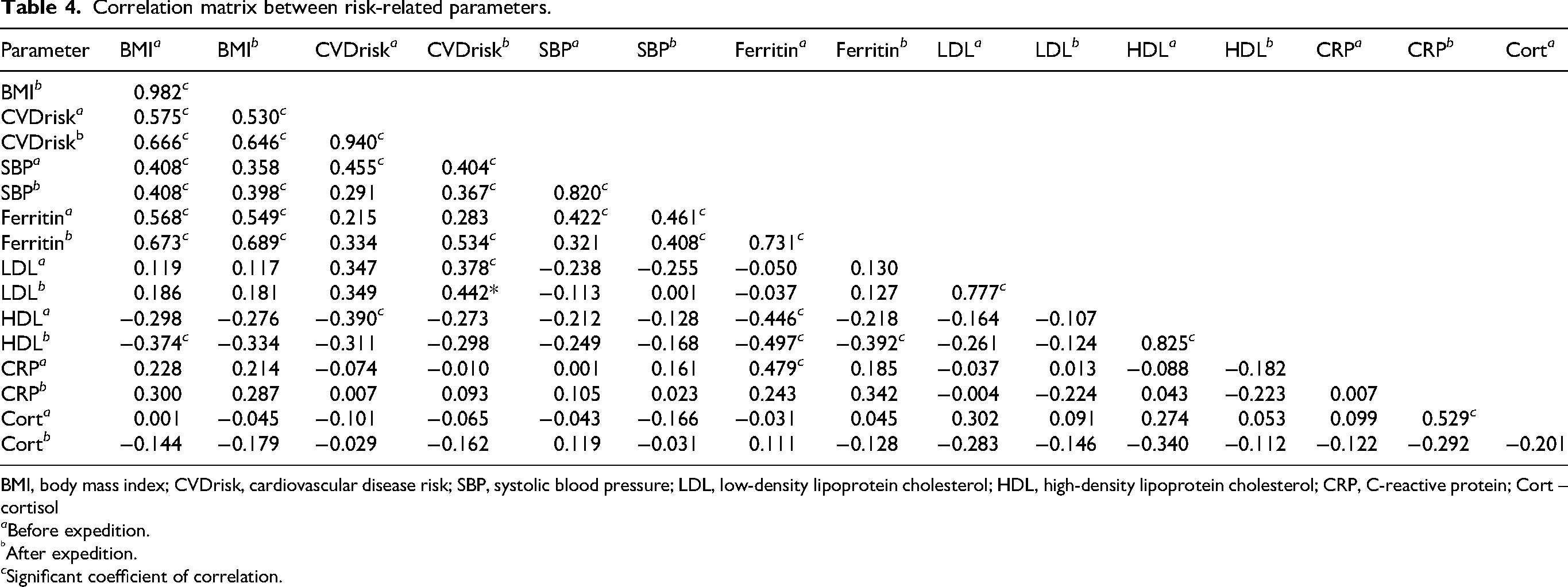
BMI, body mass index; CVDrisk, cardiovascular disease risk; SBP, systolic blood pressure; LDL, low-density lipoprotein cholesterol; HDL, high-density lipoprotein cholesterol; CRP, C-reactive protein; Cort – cortisol
a Before expedition.
After expedition.
c Significant coefficient of correlation.
Discussion
Health risk, particularly the risk of CVD and acute cardiovascular events, is a critical concern for participants in polar expeditions, primarily due to the remoteness of these places and limited access to specialized medical care there. Research data indicated that even minimal delays in primary angioplasty for myocardial infarction significantly affect mortality.20,21 In addition, the combination of cold environment and increased physical demands may further strain the cardiovascular system, especially in individuals with preexisting conditions. 22 Assessing CVD risk is therefore crucial both for participant selection and for monitoring during expeditions. According to the SCORE2 algorithm, developed by the ESC, the 10-y risk of first-time fatal or nonfatal atherosclerotic cardiovascular disease in apparently healthy adults (aged 40–69 y) is primarily influenced by age, sex, smoking status, SBP, and non-HDL cholesterol. 23
In our study, 4 participants were classified as having a very high CVDrisk (>10%), despite all of them undergoing stress testing and being cleared for participation in the Antarctic expedition. They were placed under close medical monitoring throughout the mission. After the expedition, 3 of these individuals showed a reduction in their CVDrisk, although they remain in the same range (>10%), and the fourth participant (No. 27) exhibited an increase (from 14.5 to 18.5%). This finding suggests that, during a polar expedition, CVDrisk may either decrease or increase, depending on the individual's lifestyle and physical regimen during the mission. Engaging in regular physical activity, maintaining a healthy diet, managing body weight, and avoiding cigarette smoking have all been shown to significantly lower CVDrisk. 24 The increase in CVDrisk observed in participant 27 is likely attributable to his position in the expedition, involving minimal physical activity. This inactivity likely contributed to weight gain, further elevating an already high BMI, along with a nearly 30% drop in HDL levels and an increase in the independent risk factor ferritin in this male participant. These results highlight the importance of structured physical activity, a balanced diet, and weight monitoring for all expeditioners.
Although BMI is not directly included in the SCORE2 algorithm, it is strongly correlated with CVDrisk, consistent with previous studies.25,26 Anthropometric parameters, particularly BMI and BF%, are among the most accessible indicators for health status assessment and ongoing monitoring. In our cohort, overweight and obesity were prevalent (3 of 5 females and 16 of 21 males). This trend may be attributed to the typically sedentary lifestyle of researchers, who are predominantly professional scientists. Dietary factors, including excessive intake of salt and processed foods, added sugars, and unhealthy fats; low intake of fruits and vegetables; and alcohol consumption, are important contributors to CVD and warrant further investigation among expeditioners. 27 Because no major changes in BMI or BF% occurred during the Antarctic stay, optimizing nutrition and exercise is recommended. Indeed, in modern-day Antarctic stations, no significant variations in BF are observed.28,29
Arterial pressure, another component of cardiovascular risk, was elevated in 4 participants and controlled pharmacologically in 6 others. Regular monitoring and appropriate intervention are essential for these individuals during expeditions. Arterial pressure in Antarctic expeditioners can exhibit unpredictable fluctuations, influenced by altitude, extreme cold, and psychological stress associated with confinement. Studies have reported both elevations and reductions in BP, along with variations in heart rate and other cardiovascular indicators during Antarctic expeditions.28–31
The lipid profile of our participants revealed that LDL cholesterol was the most prominent risk factor, with elevated levels in 17 of 29 participants (Table 3). Encouragingly, LDL levels decreased after the expedition in 12 participants, suggesting that their physical activity and dietary regimen could serve as a model for others. In contrast, HDL levels did not show statistically significant changes after the expedition in either sex. A significant decline in HDL levels during a Czech Antarctic expedition was reported, likely due to increased consumption of protein and meat. 32 This is a noteworthy observation given that recent meta-analyses have not confirmed a consistent relationship between red meat consumption and HDL levels.33,34 A study at the Australian Antarctic Station demonstrated that a 12-wk period of a reduced-fat and oleic acid- and carbohydrate-enriched diet can result in significant improvements in serum lipid profile with stable HDL levels and total cholesterol decrease. 35
In addition to lipid changes, we observed elevated serum cortisol levels in 6 participants before the expedition (Table 3), likely linked to physical and psychological stress associated with expedition preparation and/or execution. Serum cortisol is a widely accepted biomarker of stress. 36 Elevated cortisol levels have well-established cardiovascular implications, including hypertension, central obesity, hyperglycemia, insulin resistance, and dyslipidemia. 37 Previous studies have shown dynamic changes in cortisol levels during polar missions. In a Brazilian expedition, morning salivary cortisol concentration decreased by 37.1% after ship travel but increased by 72.1% during the Antarctic field stay. 38 A 251% increase in blood cortisol was reported during psychologically intense situations, such as crossing the Priestly Glacier. 39
The ferritin level in this study has been linked to elevated triglycerides and lower HDL levels in males, which may explain its association with CVD. 40 Elevated ferritin levels also have been independently associated with early markers of coronary artery atherosclerosis and increased all-cause mortality in otherwise healthy males.41,42 Ferritin concentrations >200 ng·mL−1 may increase the risk of ischemic heart disease in elderly individuals when other risk factors are present. 43 In our study, 5 male participants had ferritin concentrations above the laboratory reference range (Table 3). Ferritin showed strong positive correlations with BMI, SBP, and CVDrisk after the expedition (Table 4). These findings align with other research; for instance, a study of 7552 adults (mean age 45 y) found a linear relationship between BMI and serum ferritin level. 44 This correlation likely reflected dietary patterns outside the expedition, particularly a higher intake of red meat, a primary dietary source of iron. During this expedition, ferritin levels decreased significantly in males (Table 2), suggesting a lower intake or bioavailability of iron in the field rations compared with pre-expedition diets. A study involving 150 healthy adults (aged 18–70 y) concluded that ferritin serves more as a marker of inflammation than of iron status in overweight individuals. In that study, both ferritin and CRP were positively correlated with BMI, whereas BMI showed a strong negative correlation with serum iron level, total iron-binding capacity, and transferrin saturation. 45 In our study, we also found a significant correlation between baseline ferritin level before the expedition and CRP before the expedition (Table 4). However, ferritin level after the expedition correlated positively with CVDrisk after the expedition, whereas no such correlation was observed between CRP and CVDrisk before the expedition. This suggests that ferritin may be a more reliable predictor of cardiovascular risk than CRP in this context.
Finally, smoking status remains an important contributor to CVD risk,23,46,47 promoting inflammation, oxidative stress, and endothelial dysfunction.48–51 Additionally, smoking negatively affects lipid profiles by lowering HDL and increasing triglyceride levels. In our cohort, 7 of 29 participants (∼24%) were active smokers. A similar percentage (20%, 2 of 10 people) were smokers among the members of the 59th Japanese Antarctic Research Expedition. 52 The relatively high percentage of smokers further emphasizes the need for targeted health interventions before and during expeditions. In addition, exposure to secondhand smoke also increases the risk for coronary heart disease and stroke. 53
Based on our research, the following activities could be recommended:
The CVDrisk of participants in polar expeditions must be carefully evaluated before departure by the competent authority. CVD risk assessment, is crucial for identifying individuals at higher risk and for implementing preventive measures. Continuous monitoring of weight during expeditions is essential because a significant number of participants in this study demonstrated overweight or obesity, which is associated with increased CVDrisk. Promoting personalized dietary and physical activity regimes can mitigate risks and improve cardiovascular health in participants. Every participant in a polar expedition should undergo a mandatory exercise stress test before the expedition. This test proved effective in verifying the functional capabilities of the participants. Continuous monitoring of BP should be done during the expedition in participants with hypertonic disease. Ferritin assessment also should be included, particularly in males, due to its correlation with CVDrisk.
Conclusions
This study provides valuable insights into the cardiovascular risk profile and health of participants in the 32nd Bulgarian Antarctic Expedition. Despite the relatively short duration of the field mission, measurable changes were observed in several key health risk factors, including obesity, lipid profile, ferritin level, and CVDrisk scores. Elevated cortisol levels in some participants further suggested the physiologic impact of environmental and psychological stressors encountered during polar missions. Although some individuals showed improvement in cardiovascular risk during the expedition, others, particularly those with limited physical activity, experienced a deterioration in health indicators. These findings underscore the need for individualized risk assessment and proactive health management before and during polar missions.
We recommend that all expedition members, regardless of their specific roles, adhere to structured programs of physical activity, balanced nutrition, and regular monitoring of anthropometric and biochemical parameters. The SCORE2 algorithm, supplemented with markers such as BMI, ferritin, and cortisol, may serve as a comprehensive tool for identifying high-risk individuals and tailoring preventive strategies. Future studies involving larger cohorts and longer expedition durations are warranted to elucidate the dynamics of cardiovascular risk and stress adaptation in extreme environments.
Footnotes
Acknowledgments
The 32nd Bulgarian Scientific Expedition was organized by the Bulgarian Antarctic Institute. We are grateful to the Institute and all the members of the 32nd Bulgarian Scientific Expedition to Antarctica, especially to medical doctors Peltekov and Mihailova, for their cooperation in sample collection and for making this work possible. We also thank the Medical Diagnostic Laboratory “Kandilarov,” LLC, for its hematologic and biochemical analyses.
ORCID iDs
Author Contribution(s)
Financial/Material Support
This work was supported by Grant CRAS-13/18.02.2025 from the National Sports Academy, Bulgaria, and by the Bulgarian Ministry of Education and Science through the National Center for Polar Studies of Bulgaria, and Sofia University “St. Kliment Ohridski” in the framework of the National Program for Polar Studies 2022–25 (Grant No. 70-25-101/23.06.2025).
Declaration of Conflicting Interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Accessibility
All data are available from the corresponding author on reasonable request.