
Abstract
Introduction
Wilderness medicine specializes in delivering clinical care in austere environments, far from healthcare facilities, with limited resources. There is no standardized wilderness medicine training for medical students within the United Kingdom. The aim of this research was to identify what wilderness medicine training is being delivered to undergraduate medical students in the United Kingdom to guide future educational research.
Method
A scoping review following a PRISMA-ScR protocol was undertaken in the Medline and Scopus databases. This was supported by a digital survey sent to all UK university medical schools wilderness medicine interest groups to identify wilderness medicine teaching both within the curriculum and extracurricularly.
Results
Of the initial 1186 articles identified, 23 met the inclusion criteria. Seven represented practices in UK universities, and 21 represented a teaching module delivered to undergraduate students. Nineteen of the articles (91%) described faculty-delivered modules; two peer-led modules were both from UK universities. Thirty-one UK based wilderness medicine interest groups members responded to the online survey representing 13 different UK universities. All had been involved with extracurricular peer-led wilderness medicine teaching compared with 10% who received curriculum-based faculty-led teaching.
Conclusion
Most UK wilderness medicine training is extracurricular and peer led. Current research into this field provides excellent examples of wilderness medicine within UK medical schools but no comparisons between the methodologies for outcomes or cost efficiency. This review recommends more structured investigation to determine the optimal introduction to wilderness medicine for undergraduate medical students.
Keywords
Introduction
Wilderness medicine is defined by its location in austere environments, its remoteness from definitive healthcare facilities, and the limitations on medical equipment. 1 As our understanding of extreme environments developed and the community of expertise grew, organizations such as the Wilderness Medicine Society formed to support and direct research and education for healthcare professionals.
The Wilderness Medicine Society developed a curriculum for Fellowship of the Academy of Wilderness Medicine, providing recognition for healthcare professionals’ specialist knowledge. 2 Within the United Kingdom, one can enroll in expedition and wilderness medicine, mountain medicine, or extreme medicine courses providing postgraduate certification. 3
For undergraduate medical students, there is no formal syllabus in wilderness medicine. The opportunity for students to experience wilderness medicine is variable across the United Kingdom. If students are not given the opportunity to experience a specialty, then they are unlikely to see it as a career option. 4 For most UK students, it is the presence of a wilderness medicine interest group (WMIG) at their university that provides their initial introduction.
There are 46 medical schools in the United Kingdom. Over the past 20 years, there have been 7 articles exploring wilderness medicine delivered to UK undergraduate medical schools. Hardern 5 and Andrews et al 6 wrote a pair of articles sharing the experiences of faculty and students during a special study module (SSM) in wilderness medicine at the University of Newcastle. The articles summarize a 6-wk course, which was highly rated by the students, including a report of successfully delivering care in a real-life incident. The formative assessments with familiar faculty over 6 wk provided role modeling to a level that allowed them to replicate the training with their peers. 7
Schulz et al 8 used the format of peer-led teaching alongside experts at King's College London to deliver an extracurricular course to meet elements of the Fellowship of the Academy of Wilderness Medicine curricula. To et al 9 at Cambridge University attempted to avoid the need for external experts with an entirely peer-led course. The organizers had previous training and experience in wilderness medicine and were confident in delivering an introductory course. The course was delivered 5 times in the academic year, requiring significant commitment from the student organizers and no option for the course to be repeated as the instructor progresses through the program. This highlights the constant reorganization of university societies as a significant limitation of WMIG-led training schemes.
Larsen et al 10 documented their experience delivering a practical mountain rescue casualty care course at Sheffield University, whereas Lockwood et al 11 used a different approach to deliver wilderness medicine in a more urban environment in Dundee, Scotland.
This small collection of articles does not sufficiently represent the popularity of wilderness medicine within the UK undergraduate medical population. One of the most comprehensive lists of private courses in the United Kingdom is provided by The Adventure Medic, a free online magazine for students and healthcare professionals with an interest in wilderness and humanitarian medicine. 3 However, its resources do not provide any course-based information for UK undergraduate medical programs or any insight into peer-led teaching.
The aim of this scoping review was to identify what current wilderness medical education opportunities exist in UK undergraduate medical schools. This question was approached through two methods: 1) a scoping review of all published material related to wilderness medicine in the undergraduate curriculum and 2) a survey sent to all UK university medical school WMIGs for a summary of the wilderness medicine topics covered in their standard curriculum and any extracurricular or elective activities.
Method
The first phase of this research was a scoping review 12 of wilderness medicine in undergraduate medical curricula. The second phase was a survey of WMIGs in UK university medical schools.
A scoping review was most appropriate due to the diverse but small nature of the published research on wilderness medicine in the undergraduate curricula. An adapted PRISMA-ScR format was used to structure the scoping-review protocol. Eligibility for inclusion in the scoping review required participants to be undergraduate medical students involved in any format of wilderness medicine education. All sources of information were included in the search results. An initial search was undertaken using the Medline and Scopus databases to refine the search terminology. The final search terms used were as follows: (wilderness or nature or outdoors or outside or expedition) AND medicine AND undergraduate AND (medical students or medicine students or students in medicine or medical education).
Following the search, all articles had their title and abstract reviewed. Duplicates were removed, and those that met the inclusion criteria were read in full. All articles read in full had their references hand searched. All reviews were undertaken by the author. On full review of each article, data were extracted into a table (see online Appendix 1).
The second part of this project was an online survey sent to all WMIGs at UK medical schools to identify unpublished wilderness medicine opportunities in UK medical schools. No current data had been collected on this subject before, and due to the various options by which wilderness medicine could be delivered, a qualitative method was most appropriate. A Microsoft Forms survey was distributed through direct messaging by email, Instagram, and Facebook to each society. A follow-up email also was sent to the current president of each WMIG. The survey included 4 questions (available in online Appendix 2). The qualitative survey data underwent line-by-line semantic analysis for clear descriptions of teaching or learning opportunities.
Results
The results of the scoping review are summarized in online Appendix 1, and the PRISMA-ScR flow diagram is provided in Figure 1. On the final search, 1186 articles were identified. On review of titles and abstracts and removal of duplicates, this was reduced to 35 articles that were read in full. An additional 8 articles were identified in the references, so 43 articles were read in full, of which 23 met the inclusion criteria. The final 23 articles are listed in online Appendix 1.
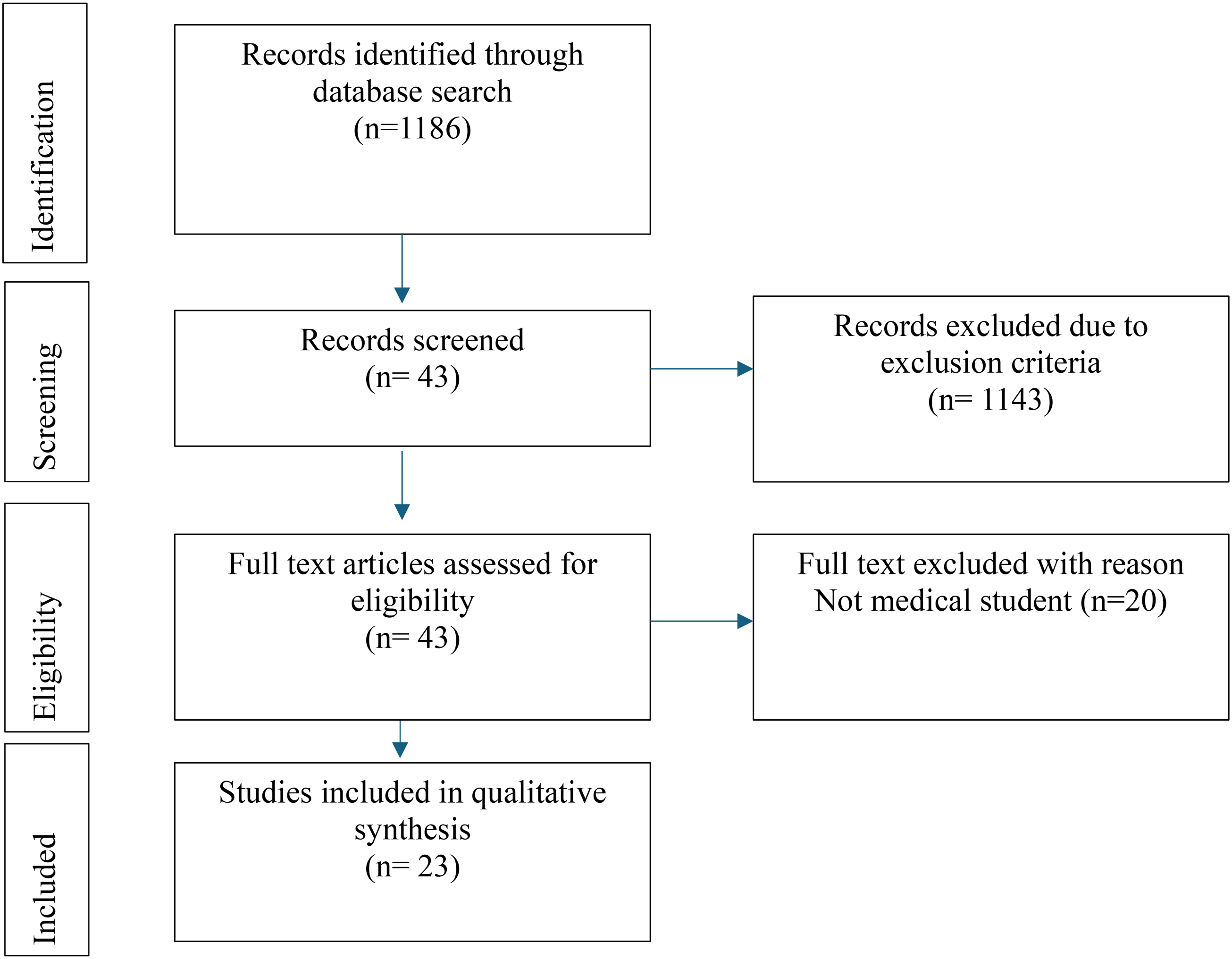
PRISMA-ScR flow diagram.
Of the 23 articles identified, 7 (30%) were from the United Kingdom, 15 (65%) from the United States, and 1 (5%) from Canada. A significant majority, 21 articles (91%), described teaching modules delivered to students. Of these modules, 71% were targeted at clinical-phase medical students, whereas the remaining 29% were aimed at preclinical students or a combination of both.
Notably, only 2 of the teaching sessions did not include any practical elements. The average duration of the courses was 2 wk, with the longest course extending to 6 wk and the shortest being a single simulation session. Most of the interventions were led by faculty members, with only 2 student-led interventions, both originating from the United Kingdom.
A digital survey of wilderness medicine teaching present within the United Kingdom was undertaken. A total of 31 responses were received from 13 different university medical schools. Responses were received from all years of study. In response to any wilderness medicine topics built into the standard curriculum, 17 student (55%) stated that there was no coverage within their curriculum. Three students (10%) described extreme physiology discussed in the course. Students from 3 universities described optional SSMs related to wilderness medicine including a 1-wk introduction to expedition medicine, a 2-wk diving medicine elective, and a 4-wk wilderness medicine module delivered in the clinical years.
In contrast, 29 of the 31 respondents provided details of an active WMIG led by students and handed over each year. Most groups undertook regular meetings. Many societies organize “day trips and weekend trips to Brecon, Lakes, Snowdonia, etc with medical scenarios built in.” These typically were “a great time to put into practice what . . . [had] been taught over the year.” Delivery of sessions was supported “with contribution from various exped doctors and paramedics.” Several societies arranged their own annual conference. There were also many references to a wilderness medicine competitive simulation event called “Wild Trials” that occurred on an annual basis (Figures 2 and 3).
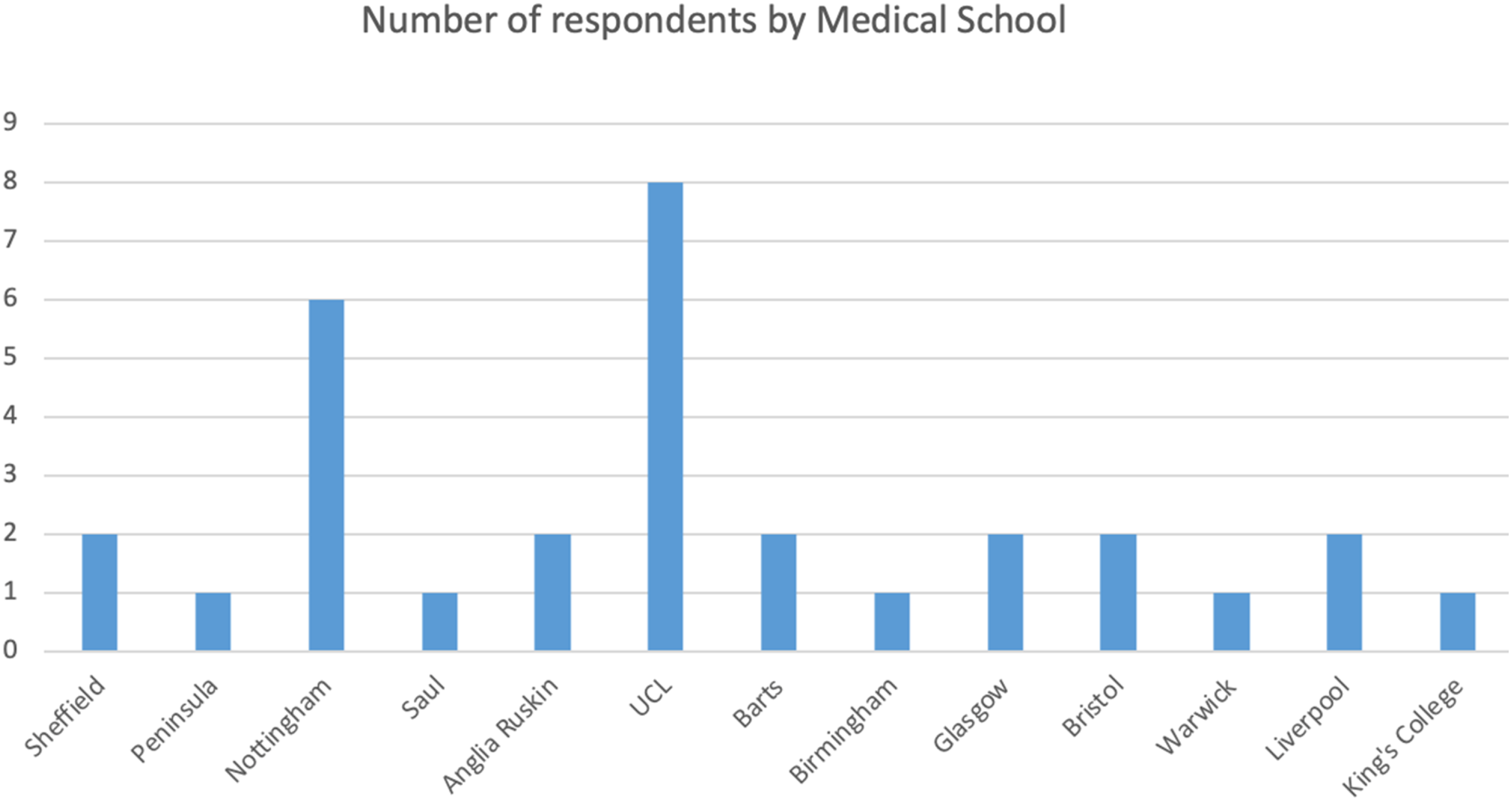
Bar chart to show number of survey respondents categorized by university.
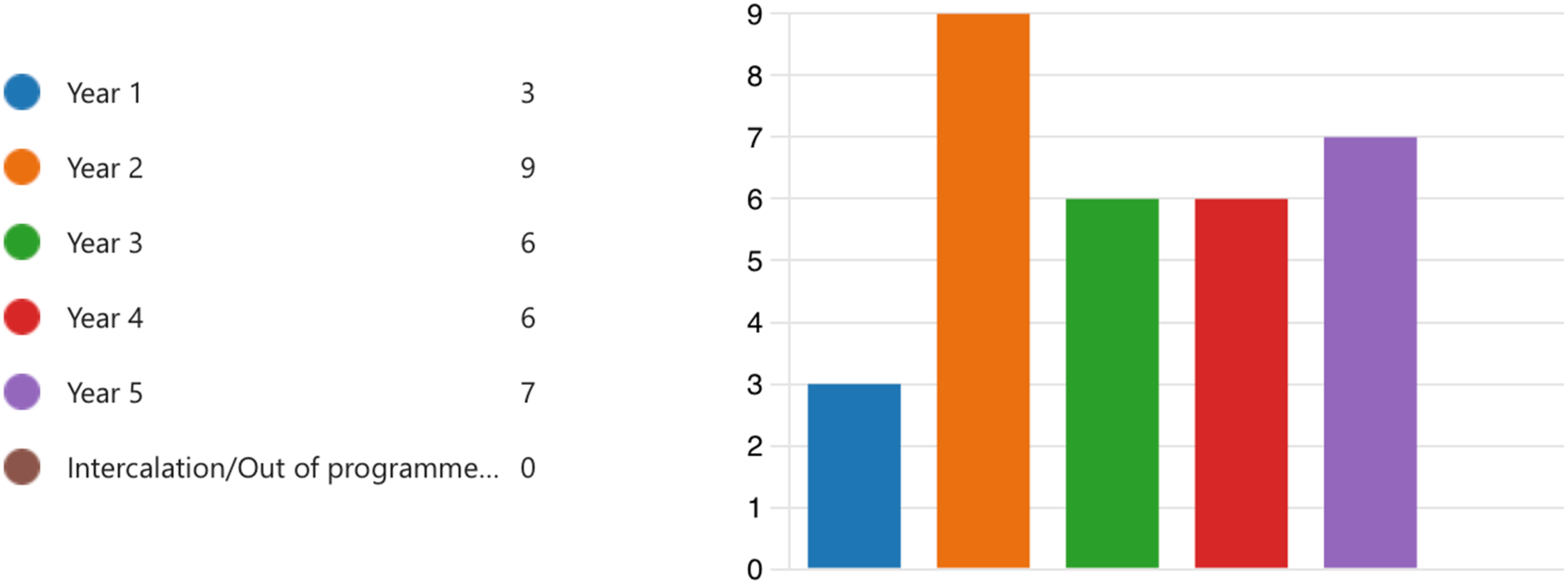
Bar chart to show number of survey respondents categorized by year group
Discussion
There are a limited number of articles relating to UK wilderness medicine practice in medical education; 3 of the 7 articles were all connected to the same university (see online Appendix 1). There was a mix of faculty-led elective modules and WMIG peer-led extracurricular activities. All UK-based articles focused on student feedback of a teaching module but did not provide any higher levels of evaluation or comparisons against alternative methods. The survey of current WMIG members across UK universities suggested that most of the wilderness medicine was being taught as an extracurricular activity through a mix of peer and expert teaching. The level of provision varies across institutions and changes each year as committees are reelected.
The evidence from UK university medical schools is very limited and spread out between 2009 and 2020. From the survey responses of current WMIG members, there are elective modules that have closed following loss of faculty members. In comparison, US medical schools have more established programs that are faculty led. This is likely to be due to the differences in recognition of wilderness medicine between the United Kingdom and the United States. This review provides a snapshot of what is in place, and as remarked by 1 survey respondent, “I hope I’ll have more to say if you send the survey out again next year.”
The evidence currently available and summarized in online Appendix 1 is largely based on articles evaluating wilderness medicine teaching modules. The survey of student rating experience was at Level 1 of the Kirkpatrick model of evaluation. 13 There were 2 articles that put students through a more formalized assessment process, Level 2 of the Kirkpatrick model.8,14 Unfortunately, with a significant drop-out of course attendees in paper by Schulz et al, 8 the high quality of the methodology was undermined by the loss of more than one third of the course members. The current articles on wilderness medicine in undergraduate education all reflect on the successful delivery of the course. The current research is descriptive, providing a format for others to base their own educational projects. Because numerous versions of the courses now have been published, it would be more beneficial for future research to start to justify the position of wilderness medicine by comparing models and determining the most effective ones. 15
Hardern 5 summarized the well-constructed elective module of a small group of students undertaking very resource-intensive sessions. The 6-wk program was highly competitive for entry and included protected curriculum time. Similarly, Macias et al 16 outlined their elective module, including short expeditions in austere environments. Neither module undertook an evaluation of the return on investment from diverse training opportunities, which would not be reproducible without considerable investment of time and resources.
The dedication of such time, over 4 wk in the above-mentioned studies, is a common barrier for most institutions. Curriculum overload is a contemporary problem in UK medical schools and leads to many specialties having to be delivered in SSMs. 17 Within all the published literature identified, 7 articles related to wilderness medicine training delivered as an extracurricular activity, although this forms the majority of experiences for UK WMIG members.
From the survey responses, <50% described wilderness medicine being delivered within their curriculum. In contrast, 90% of respondents described opportunities provided by their university WMIG.
The learner level for wilderness medicine at the undergraduate level is typically very low. Larsen et al 10 used the Mountain Rescue England and Wales Casualty Care course for implementing wilderness medicine into undergraduate education. This course requires no prior medical training, yet the patient packaging skills are deemed beneficial for all training doctors. To et al 9 demonstrated how peer-led teaching can be delivered effectively; this relied on the individual experience of the student tutor within these nonmedical fields.
There will always be conflict between what topics should be covered at the undergraduate level. Lareau et al 18 published their work to summarize the topics undergraduate wilderness medicine program directors recommended, receiving a diverse response. Wilderness medicine contains many nonclinical topics related to rescue principles in different environments that do not overlap with traditional contents of a medical course. Only 3 wilderness medicine courses published in the literature cover these wilderness medicine–specific nonclinical topics. The clinical topics were more highly ranked in Lareau et al 18 and much more frequently delivered as part of the modules identified within the scoping review, where 2 distinct styles recurred. The most common module structures were practical sessions delivered to clinical-stage students. This style was well received in student feedback and used a simulation-based teaching methodology. Schulz et al 8 noticed a clear distinction in performance in the formative scenarios between clinical and nonclinical students. Although skills could be covered in a wilderness setting, faculty would only be changing the backdrop while still focusing on teaching the skill. Wilderness medicine was deemed more appropriate to be delivered either at the very end of the preclinical years or during the clinical years once a reproducible primary survey and familiarization with common pathologies had been achieved. The alternative method for wilderness medicine education was in lecture and tutorial format summarized in 2 articles.19,20 Neither of these courses intended to be fully lecture based, Omand et al 19 offered practical clinical skills sessions toward the end of the module, and Hill and Pasik 20 had been limited to delivering their wilderness medicine module online due to local COVID-19 restrictions. Feedback from the 2 modules was good but asked for more practical teaching. Babu et al 21 focused their module around introducing specialist topics based on extreme physiology and the associated career options. Although students preferred the practical scenarios, there appears to be a place for lecture-based teaching as an introduction to the unique position of wilderness medicine and the opportunities it presents for future careers.
This review contains several limitations. A scoping review had been undertaken rather than a systematic review, and the articles identified were all reviewed by 1 individual. The database searches only provided 1 French-language article from Canada; with additional time, it would be useful to search more widely for non-English-language and southern hemisphere research papers due to the high presence of wilderness medicine education internationally. This type of review provides a snapshot in time highlighting what has been published and reported by current students. There are likely to be modules that have been unpublished and not shared from different universities, limiting the comprehensiveness of this review.
The digital survey was publicized through social media with the support of high-profile organizations (eg, World Extreme Medicine and The Adventure Medic) but only received responses from 13 of the potential 46 UK university medical schools. There also was the potential risk of the survey being completed by non–wilderness medicine interest group members. For future surveys, it would be prudent to ask students to provide a university email address to verify their status. Wilderness medicine was not defined within the survey but by the responder and their own understanding and connections with a WMIG. This was intended to maximise potential responses.
This review has highlighted areas that would benefit from further investigation. The most important step is for wilderness medicine education research to move past the point of description and start to justify its position. 14 Wilderness medicine has the potential to be the ideal format to deliver team-based scenarios and training human factors and interpersonal skills. A direct comparison between hospital- and wilderness-based scenarios would provide some insight into whether the varied environment with limited clinical resources redirects the focus back toward interpersonal skills and improvisation. 22
Conclusion
In conclusion, this article contains a 2-stage review of current wilderness medicine education being delivered to undergraduate medical students in the United Kingdom. This has been achieved through a scoping review of the current literature and a survey of current medical students. The results from each section have highlighted the current interest among the undergraduate community and the various module structures being delivered both by faculty and by peers.
Wilderness medicine is a recognized specialty in the United States but does not hold the same recognition in the United Kingdom. Formal accreditation is available at the postgraduate level, but no formal syllabus exists for undergraduate medical education, leaving them with the choice of curriculum-based elective modules, WMIG peer-led teaching, or paid-for training courses.
Elective or special study modules are more common in the United States, although 3 such courses have been published from UK universities, with an additional course mentioned in the digital survey. These courses take 2 different forms: either seminar-based exploration of physiology and career options or a more practical wilderness medicine experience undertaking scenarios in an outdoor environment. The first style seems to be more suited to preclinical students, whereas the latter seems more applicable for clinical students with prior knowledge.
Most of the current exposure to wilderness medicine is through peer-led WMIGs. Given their structure, the opportunities provided by each group vary between universities and from year to year. There are opportunities to attend national conferences and Wild Trials events, but most teaching is at an introductory level with support from local experts that volunteer their time.
There are numerous examples of modules from which universities could design a wilderness medicine elective. The next step is for these to be evaluated for their impact and cost, alongside a comparison to determine what is the best delivery method and to which stage of training they should be administered. There is also the possibility of current curriculum topics being delivered more effectively in a wilderness medicine setting. This article draws together the current position of wilderness medicine education for undergraduate students in the United Kingdom. The next question is where do we take it from here?
Supplemental Material
sj-docx-1-wem-10.1177_10806032251322488 - Supplemental material for Status of Wilderness Medicine Education in the United Kingdom: A Survey-Based Research and Review of the Literature
Supplemental material, sj-docx-1-wem-10.1177_10806032251322488 for Status of Wilderness Medicine Education in the United Kingdom: A Survey-Based Research and Review of the Literature by David RM Lee in Wilderness & Environmental Medicine
Supplemental Material
sj-docx-2-wem-10.1177_10806032251322488 - Supplemental material for Status of Wilderness Medicine Education in the United Kingdom: A Survey-Based Research and Review of the Literature
Supplemental material, sj-docx-2-wem-10.1177_10806032251322488 for Status of Wilderness Medicine Education in the United Kingdom: A Survey-Based Research and Review of the Literature by David RM Lee in Wilderness & Environmental Medicine
Footnotes
Author Contribution(s)
Consent to Participate
All participants provided informed consent by partaking in the survey.
Consent for Publication
All participants provided informed consent to publication when partaking in the survey.
Data Availability
Contact Dr David Lee (d.r.m.lee@swansea.ac.uk) for the complete survey.
Ethical Considerations
This project was granted a favorable ethical opinion by the Swansea University Medical School Research Ethics Sub Committee (SUMS RESC 2023-0022).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplementary material associated with this article can be found in the online version at https://doi.org/10.1177/10806032251322488.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.