
Abstract
Management of the airway in austere environments can differ substantially from standard in-hospital airway management. Devices such as nasopharyngeal airways, oropharyngeal airways, endotracheal tubes, extraglottic airways, ventilators, and sedative and paralytic medications may not be available. Weather, scene hazards, difficulties of extrication, transport times, skill sets of rescuers, and availability of advanced equipment are highly variable. Standard decision-making processes and guidelines, such as intubation for Glasgow Coma Scale score ≤ 8, are not always optimal in austere settings. Airway management in austere settings involves many variables leading to complex decision-making. We present 2 cases in which airway management likely would have been similar in hospital settings but differed in austere environments based on the available resources. We discuss current concepts and methods for airway management in austere environments with a review of the pertinent literature.
Introduction
Airway management in austere settings presents a unique set of challenges. Wilderness medical providers should initially consider indications similar to those used in most emergency departments when deciding to intubate. These indications include airway protection, oxygenation, ventilation, and the potential for future deterioration. 1 A common tenet in emergency medicine practice, “Glascow Coma Scale score ≤ 8, intubate,” was originally applied to patients with head trauma but has since been used more broadly in airway decision making.2–5 In austere settings, limitations in skills and numbers of medical personnel as well as lack of access to airway devices, medical equipment, power sources, and medications for rapid sequence intubation and post-intubation sedation may pose significant obstacles to using standard airway management decision making.
Ideally, there would be a single airway algorithm applicable to every wilderness medicine scenario. Resources and provider skill levels are generally standardized in hospital environments, making the patient the main variable. In austere settings, skill levels, resources, weather conditions, rugged terrain, and prolonged evacuation times are highly variable. 6 This variability makes a single austere airway algorithm challenging.
In austere settings, airway rules typical in hospital or urban prehospital settings may not be practical. Instead, airway management decisions that would be considered unorthodox in hospital settings may be preferred. There are many non-standard techniques for wilderness airway management, including the use of improvised laryngoscopes, cricothyroidotomies with improvised equipment, and blind digital intubations.7–11 Although such techniques may be useful in certain situations, a critical factor in wilderness airway management is decision making. We present 2 case reports that illustrate decision making for airway management in austere settings.
Case Reports
Case 1
In the White Mountains of New Hampshire, a rock climber in her thirties and her partner scrambled unroped through Class 5 (technical) terrain to reach a crag. The climber slipped and fell approximately 12 m (40 ft) down a loose gulley onto a steep exposed ledge (Figure 1). A nearby pair of climbers, including an emergency physician (EP), heard the fall, followed by calls for assistance. The EP had technical climbing experience and training in mountain rescue. He scrambled up to the ledge to access the victim. Meanwhile, his partner used a cell phone to call for medical assistance and organized a team of nearby climbers to perform a litter rescue.

Photo panels depicting the location of the ∼12-m (40-ft) fall and the ledge where endotracheal intubation was performed.
The EP performed a primary assessment. The victim had severe facial and head trauma, with blood in the airway and sonorous respirations with a Glascow Coma Scale (GCS) score of 4 (eyes 1, verbal 2, movement 1). The EP directed the victim's climbing partner to perform a jaw thrust while he stabilized the cervical spine. The respirations became less sonorous.
The EP descended to a trailhead where he was met by police and an advanced life support ambulance crew, including a paramedic who was an experienced climber. The EP descended for help rather than the climbing partner because the EP was a local physician who knew the area well and was better able to organize the rescue. The EP requested equipment for trauma, airway, and rapid-sequence intubation (RSI). The EP and paramedic climbed up and reached the victim 45 min later. Still on the ledge, they placed a cervical collar and 2 nasopharyngeal airways. The providers found that the airway was unstable and that a prolonged litter carry with technical lowers would be required. High-quality bag-valve mask (BVM) oxygenation and ventilation were not feasible with the continued transport movement, and there were concerns that an extraglottic airway (EGA) might become dislodged during the technical lowers. A secure airway was desirable. The providers established an intravenous (IV) line and made the decision to perform endotracheal intubation (ETI). They identified a gum elastic bougie and a Ambu King LTS-D Laryngeal Tube (Ambu USA, Columbia, MD) airway as potential backup alternatives to direct laryngoscopy. The EP preoxygenated the victim with a nonrebreather mask and administered estimated weight-based doses of IV etomidate and rocuronium. Initial direct laryngoscopy revealed an oropharynx obscured by blood and secretions. The providers used a manual suction pump to clear the oropharynx, allowing visualization of the vocal cords during passage of the endotracheal tube. They confirmed correct endotracheal tube placement visually by observing adequate chest rise and by colorimetric capnometry. They secured the tube and then oxygenated and ventilated the victim with a BVM and oxygen from a D cylinder. Midazolam and fentanyl were administered for postintubation sedation.
A large team of rescue workers and nearby climbers extricated the victim from the ledge. Because the terrain was steep and exposed, 2 technical rope lowers from tree anchors were required to move the litter safely over the cliffs. This was followed by a difficult litter carry over steep rocky terrain. The lower and carryout lasted ∼90 min (Figure 2). The local air medical service helicopter flew the victim to the regional trauma center 40 mi away. Evaluation at the hospital revealed a basilar skull fracture, a complex calvarial fracture, epidural hematoma, subdural hematoma, subarachnoid hemorrhage, intraventricular hemorrhage, cerebral contusion, multiple facial fractures, and T7, L1, and L2 compression fractures. The victim had a prolonged and complicated hospital course with multiple operations but ultimately recovered with minimal cognitive and functional deficits.

The victim is loaded onto an ambulance for transfer to the helicopter landing zone.
Case 2
During a snowstorm, a guide escorted a middle-aged trekker on horseback from the village of Lobuche (4940 m [16,210 ft]) to the Himalayan Rescue Association clinic in Pheriche, Nepal (4371 m [14,341 ft]). The trekker had a GCS of 9 (eyes 2, verbal 2, movement 5) and was tachypneic. Her guide told the 2 EPs at the clinic that the trekker likely had high altitude cerebral edema. She had spent the previous day in her room at a lodge with a headache. She had no reported respiratory symptoms. She had no known significant past medical history and had been at altitude before without problems.
While walking to a bed in the clinic, the trekker collapsed in cardiac arrest, with pulseless electrical activity determined by cardiac monitor and absence of carotid pulses. The EPs immediately began chest compressions and BVM ventilation using oxygen at 8 L·min, the maximum flow rate of the oxygen concentrator. After several minutes of compressions and ventilation, the patient regained weak, thready pulses (Figure 3). The initial systolic blood pressure was 80 mm Hg by palpation. The oxygen saturation was unmeasurable. Her skin was cool and clammy. Her lungs were clear to auscultation. The GCS score was 4 (eyes 1, verbal 2, movement 1). The EPs discussed performing endotracheal intubation for airway protection and improved oxygenation. They were concerned about possible vomiting during EGA placement without sedation. Because helicopter rescue was unlikely and a mechanical ventilation device was not available, they decided to continue to assist her inadequate spontaneous respirations with BVM ventilation. The EPs administered dexamethasone 8 mg intramuscularly for presumed high altitude cerebral edema. In <1 h, the patient’s respiratory effort improved, and she was transitioned to nonrebreather mask. The patient continued to have marked tachypnea and an unmeasurable oxygen saturation despite oxygen at 8 L·min. The EPs suspected high altitude pulmonary edema, but they withheld nifedipine because of persistent hypotension and the patient's inability to tolerate oral medications. The patient's mental status improved overnight. The EPs weaned her to oxygen by nasal cannula. By morning, her mental status had improved significantly, and she provided additional history. She had never had a headache or nausea. She had simply felt short of breath over the previous 24 h. Once the weather improved, she was flown by helicopter to a hospital in Kathmandu, where she was found to have large bilateral pulmonary emboli on computed tomography imaging. She was discharged after several days of treatment. She returned to her home country in good condition.

Clinic medical staff continues to manage the patient with oxygen via nonrebreather mask after arrest and return of spontaneous circulation.
Discussion
In austere settings, many airways can be managed with less invasive methods than ETI. The most advanced airway is not always the best choice (Table 1). Initial airway management starts with the simple chin-lift or jaw-thrust maneuver to help alleviate airway obstruction. In austere settings, these maneuvers, along with a semiprone recovery position, which can relieve airway obstruction by the tongue, may be the only interventions available. 12 Although BVM ventilation is usually used as a bridge to ETI in hospitals, its simplicity, rapid administration, and lack of need for RSI and sedation medications or advanced training make it a valuable tool for medical providers in austere settings. Disadvantages include lack of airway protection and difficulty in maintaining a good seal, especially in victims with facial hair or with facial trauma. BVM ventilation also can be hard to perform in technical terrain and is often best performed by 2 providers, making it suboptimal for prolonged extrications. It can be used as a bridge until more resources arrive or, as in Case 2, the clinical situation improves.
Advantages and disadvantages of airway interventions in austere settings.
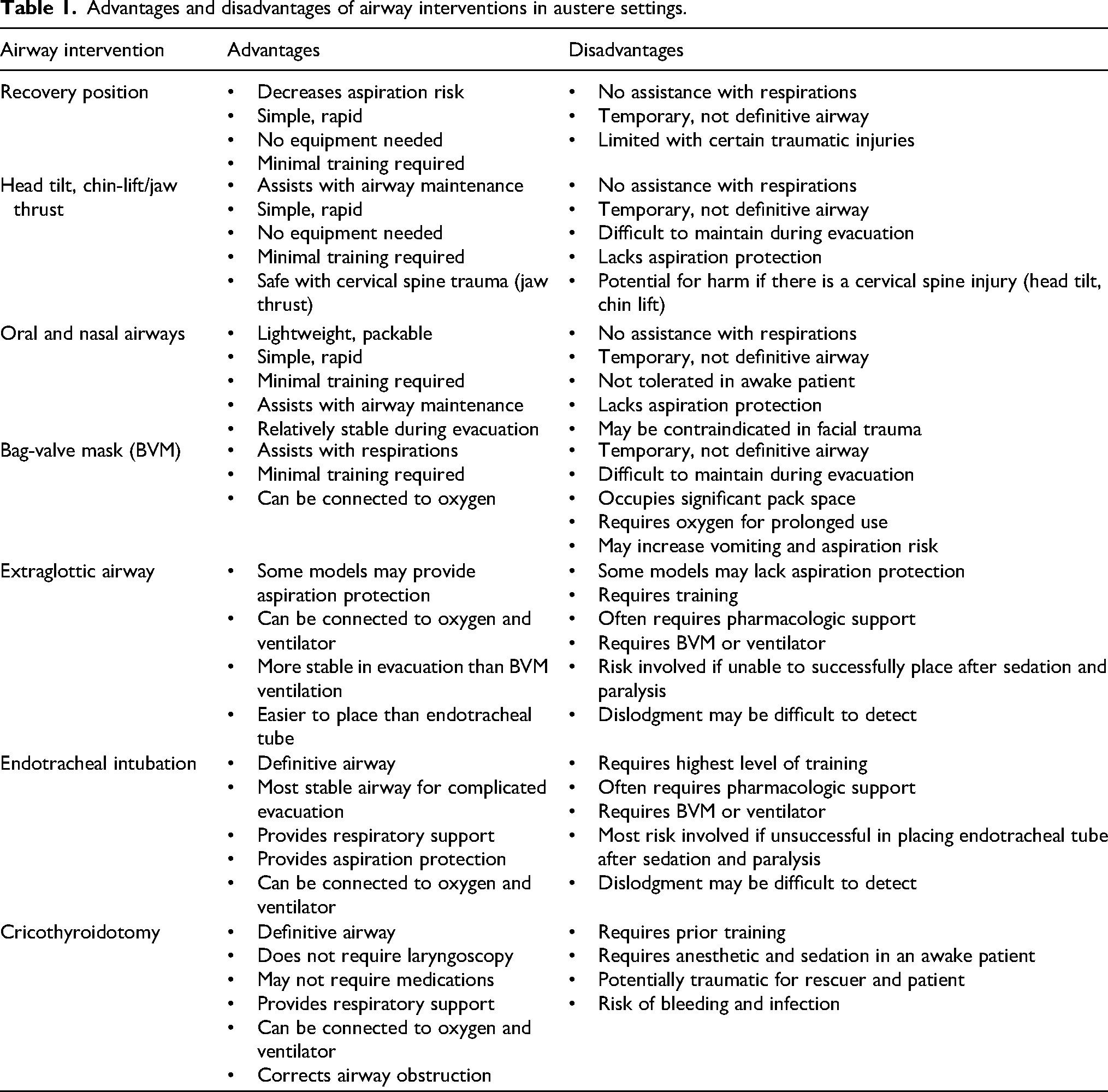
If available, an EGA should be strongly considered in any patient requiring BVM ventilation in an austere setting. EGA placement is generally easier than ETI, especially for basic providers, with fewer interruptions of cardiopulmonary resuscitation and earlier oxygenation. An EGA is an efficient means of oxygenation and ventilation, does not require extensive training, may provide protection against aspiration, and can be easily carried in many backcountry settings. 1 BVMs, laryngeal mask airways, and other EGAs are light and relatively compact airway devices that can be easily included in portable wilderness medical kits. 13 Several studies have shown efficacy of airway management with BVMs or EGAs in prehospital settings. The Pragmatic Airway Resuscitation Trial (PART) study randomized 3000 out-of-hospital cardiac arrest victims and found that compared with ETI, the Ambu King laryngeal tube led to significantly increased 72-h survival, return of spontaneous circulation, hospital survival, and favorable neurologic outcome. 14 The AIRWAYS-2 study of >9000 nontraumatic out-of-hospital cardiac arrests found no difference in functional outcome between those managed with EGAs or ETI. 15 A recent study of a trauma cohort showed no difference in mortality between patients managed with EGAs versus ETI. 16 Comparing BVMs with EGAs in urban out-of-hospital cardiac arrests, one study found no significant difference in return of spontaneous circulation or favorable neurologic outcomes. 17 Another study suggested that the use of advanced airways is associated with worse neurologic outcomes than the use of BVMs. 18 Other studies showed either noninferiority of BVMs compared with advanced airways in certain prehospital cardiac arrest victims or inconclusive differences between BVMs and ETI.19,20
Although not always necessary or available in austere settings, ETI is still a valuable intervention in specific situations. ETI may be superior to other methods for long or difficult extrications when security of the airway is a priority and patient improvement is unlikely. Although an EGA may be faster to place and allow more rapid oxygenation than ETI, it is less secure than an endotracheal tube. 21 As with EGAs, the victim must be unconscious or sedated to tolerate ETI. Even if all requirements for ETI are met, providers must be aware that ETI may place a paralyzed patient at increased risk of morbidity and mortality if the provider cannot guarantee adequate oxygenation or ventilation.
In austere environments, the decision-making process for airway management is different from in resource-rich settings. 22 Important factors to consider include the condition of the patient, the terrain, the availability of resources, and evacuation plans. Decision making will vary based on individual situations. Sometimes basic airway management such as repositioning the airway or use of basic airway adjuncts (eg, nasopharyngeal or oropharyngeal airways) may be all that is necessary to stabilize the patient. In some situations, observation and waiting may be desirable, obviating the need for ETI in patients who would have been intubated in a hospital setting. Often a provider will have only 1 patient and will have adequate time for close monitoring. This is rarely the case in a hospital.
The 2 cases we present illustrate options for airway management of critically ill victims in austere settings. Despite differing conditions, clinical settings, resources, and eventual clinical courses, the EPs took similar initial approaches in both cases, performing decision making that weighed the risks versus potential benefits of various airway interventions. Because these cases took place in austere settings, standard care as provided in developed hospitals was not possible. If the 2 victims had initially presented to emergency departments, both likely would have received prompt ETI. In the first case, the providers performed RSI. The patient had compromised airway protection that would have been challenging to treat with a simple jaw thrust or BVM during prolonged high-angle lowers in a litter. An advanced life support ambulance crew with equipment for definitive airway management was available, the providers were trained to perform ETI, and backup airway devices were available. Postintubation sedation with midazolam and fentanyl also was possible, and there were enough rescuers and oxygen for prolonged BVM ventilation.
The setting of the second case, while also austere, was different from that of the first case. Despite having endotracheal tubes, EGAs, and providers competent to perform ETI, medications for RSI and postintubation sedation were not available. The remote clinic also lacked a ventilator and video laryngoscope. The EPs knew that a storm could delay helicopter rescue, possibly for several days, necessitating prolonged BVM ventilation with only a few rescuers. Despite the initial cardiac arrest, the EPs were able to oxygenate and ventilate the patient effectively. She was not at imminent risk of airway loss and was stationary, with no difficulty in using BVM ventilation. The EPs decided that the risks of ETI outweighed the potential benefits.
Conclusions
Airway management in austere settings requires a very different approach from that in emergency departments. Before making a decision to intubate or use an EGA, BVM, or other airway device, providers must consider available resources, including medications, equipment, and the abilities of the rescuers. Providers also should consider access to the patient, predicted clinical course, and the time course and logistics of evacuation or rescue. An aggressive approach of ETI for all patients with a low GCS score may not be practical or safe in austere settings. Providers in austere settings should approach critically ill patients with flexibility and creativity and should be willing to deviate from hospital standard of care by considering more basic airway interventions and adjuncts.
Footnotes
Acknowledgments
The authors acknowledge everyone who was involved in the rescues of the 2 victims, including the guides and porters, the medical team at the HRA, and the EMS team in the White Mountains.
Author Contribution(s)
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.