
Abstract

Dear Editor,
We are writing to highlight the significant impact of portable ultrasound in cataract outreach initiatives, particularly in low- and middle-income countries (LMICs). During a recent cataract outreach campaign in Ghana, a 55-year-old female presented with bilateral dislocated crystalline lenses due to a traditional procedure known as couching performed by a native healer. This diagnosis was made using point-of-care ultrasound (POCUS), underscoring the value of portable ultrasound in such settings.
Couching, an ancient practice that involves manually dislodging the cataract within the capsule, is one of the earliest known surgical interventions. 1 Using a sharp needle, the aim of the procedure it to break the zonules, allowing the lens to fall outside the visual axis. 2 It is thought to have originated in the sixth century, 3 deriving its name from the French word coucher, meaning “to put to bed.” This practice has largely fallen out of favor due to its high complication rates (including hyphema, endophthalmitis, and secondary glaucoma leading to blindness) and the advancement of new, safer technologies. However, this case provides evidence of its persistence in regions such as West Africa, where there can be a preference for traditional methods over modern surgical techniques.4,5
The patient, who had been blind for more than 5 y, presented to a cataract surgical outreach clinic after being referred by a local screener in her community. The patient was initially referred to have cataract surgery for left eye lens subluxation. Her visual acuity was assessed as hand motion in the left eye and counting fingers at 1 m in the right eye. She was noted to be aphakic in the right eye on initial examination. Initial intraocular pressures were normal—15 mm Hg in the left eye and 16 mm Hg in the right eye measured by tonometry.
The patient underwent evaluation with handheld ultrasound (GE Vscan Air, GE HealthCare, Chicago, IL), and bilateral subluxated lenses were identified (Figure 1). The patient initially did not share information about prior treatments, but after ultrasound evaluation, she disclosed that she had been to a village healer for treatment on two occasions for her cataracts. She did not specify the treatment that she underwent nor the timeframe of when she was treated.
Right eye with subluxated lens material visible in the inferotemporal quadrant.
In this cataract outreach clinic, POCUS was performed on all patients to increase efficiency with surgical planning to minimize operative time. POCUS of the patient's left eye showed a dislocated lens sitting in the vitreous cavity. The results from POCUS for this patient (Figure 2) allowed the ophthalmologists to see that attempting a procedure on the left eye likely would lead to complications with minimal (if any) benefit for the patient. Therefore, we chose not to offer surgery for the left eye.

Ultrasonographic image of the dislocated lens sitting in the vitreous cavity.
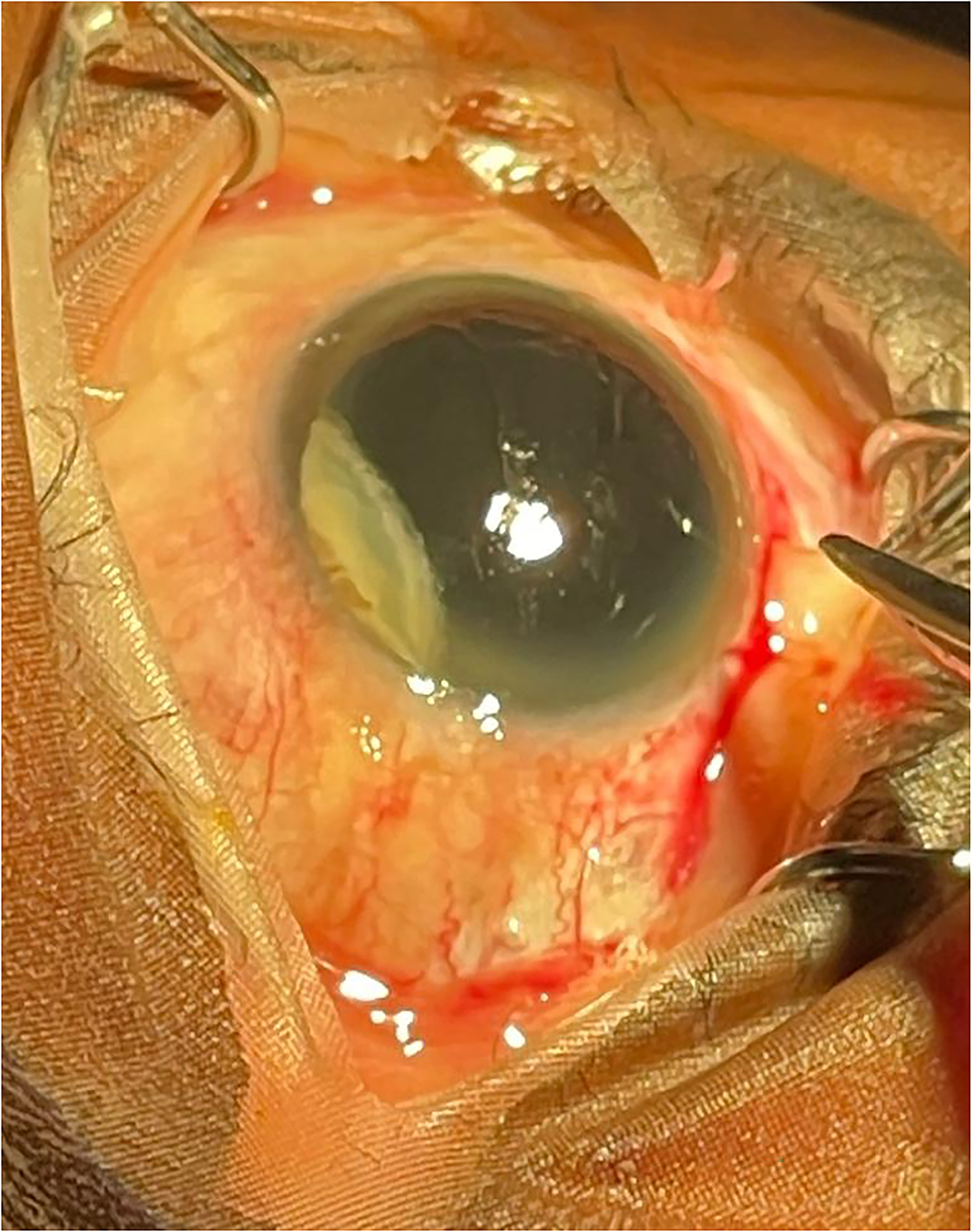
In the right eye, POCUS showed a subluxed lens that was amenable to intervention. The patient underwent sutureless intracapsular cataract surgery on her right eye, facilitated by the ultrasound findings. The partially dislocated lens and capsule were prolapsed successfully into the anterior chamber and removed through the main scleral tunnel incision without loss of lens material into the vitreous. An anterior-chamber intraocular lens was then placed (Figure 3). On postoperative Day 1, the patient’s vision was counting fingers at 1 m and likely was limited by the air bubble placed intraoperatively. She did not follow up at postoperative Week 1. Unfortunately, this is a common occurrence in outreach settings, where patients are more likely to report to their follow-up appointments only if they have visual complaints. However, after several attempts were made to reach the patient, the clinic received a message that the patient was unavailable because she had gone to the market to resume working—indicating that her vision likely was improved enough for her to get back to work. Her left eye will need a retinal follow-up with vitrectomy, removal of the lens, before a replacement lens can be placed.
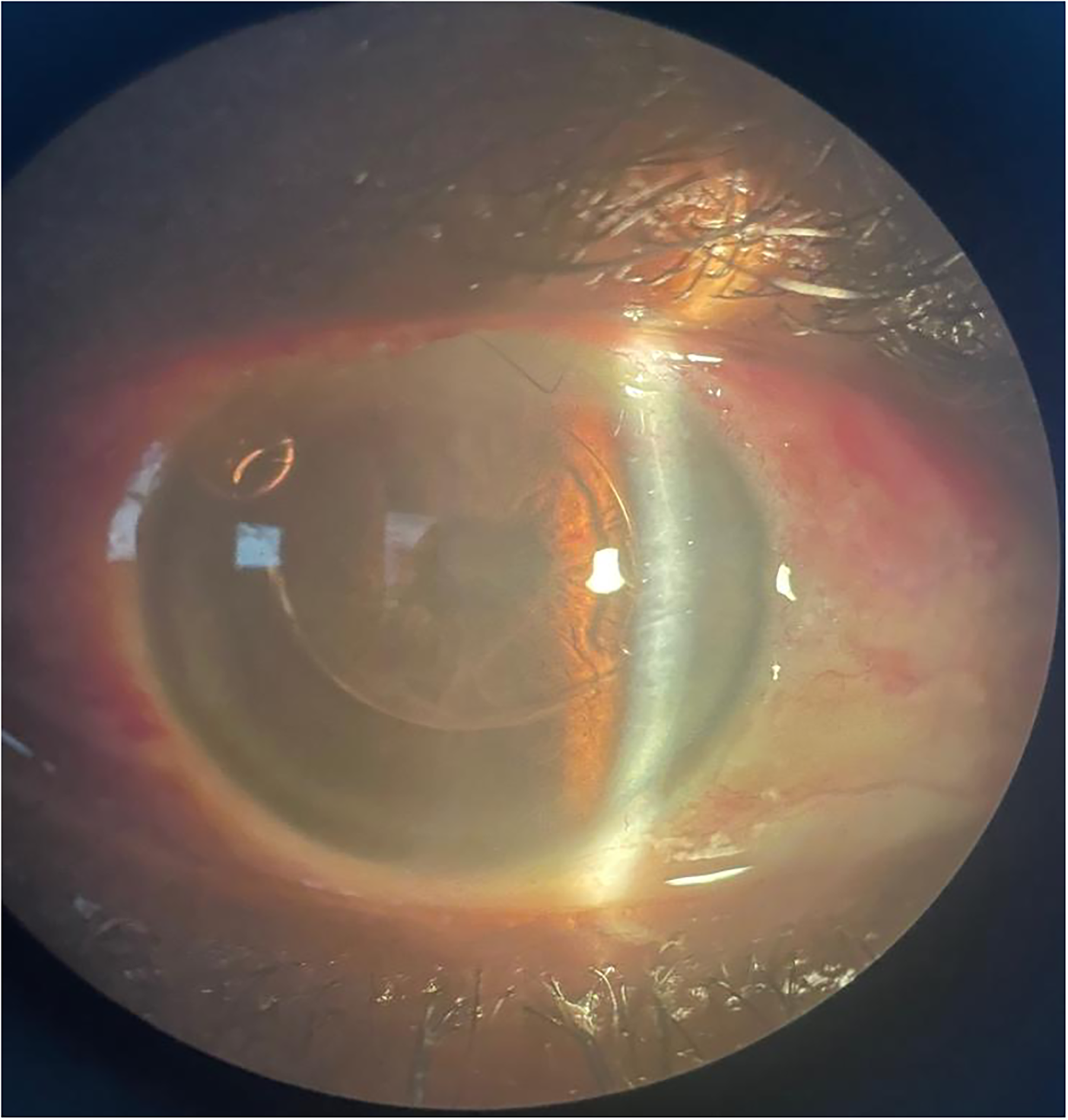
Slit-lamp image of the right eye with an artificial lens positioned in the anterior chamber.
POCUS has been widely used in emergency settings since the 1990s and shows exciting promise in LMICs due to its noninvasive, portable, and cost-effective nature, particularly in the outreach clinic setting. Dense cataracts often prevent ophthalmologists, ophthalmic technicians, and other healthcare providers from performing an adequate exam of the posterior chamber due to the cataract blocking access to visualizing the posterior chamber. Other modalities such as magnetic resonance imaging, orbital computed tomography, and B-scan machines are cost prohibitive in LMIC settings.6,7 POCUS can and should be used to diagnose posterior-chamber pathology in these settings, preventing needless surgery, unnecessary pain, anxiety, unrealistic expectations, and postoperative infection risk. Furthermore, prescreening of patients who might not benefit from cataract surgery can enhance the success of eye campaigns through positive word of mouth. In these outreach programs, even a single poor outcome can generate doubt and suspicion, adversely affecting recruitment for future outreaches. Despite the availability of advanced cataract surgeries, the persistence of couching in some regions calls for increased adoption of ultrasound for preoperative screening.
This case in Ghana demonstrates the potential of portable ultrasound to revolutionize ophthalmology care in rural and remote settings. With technological advancements making these devices more accessible and user friendly, their integration into cataract outreach programs could enhance patient outcomes and the overall success of these initiatives significantly.