
Abstract
We present an unusual case of concomitant exercise-associated hyponatremic encephalopathy (EAHE), exertional rhabdomyolysis (ER), and acute kidney injury (AKI) in a Grand Canyon hiker. Our case patient, an adult 41-year-old male, consumed an excessive amount of water during his descent into the Canyon during hot weather. The next day, he was unable to hike out due to severe leg pain and disorientation, and ultimately evacuated by helicopter, having a grand mal seizure in flight. Despite having no serum sodium level, medics administered an intravenous (IV) bolus of 3% hypertonic saline (HTS) before transporting him to the hospital. There, he was diagnosed with EAHE (serum sodium, 114 mmol⋅L−1), ER, bilateral compartment syndromes, and mild AKI. The life-threatening EAHE was immediately corrected with more IV HTS, the limb-threatening compartment syndromes by surgical fasciotomies, and eventually, the AKI by oral and IV fluids. This case demonstrates the seriousness of overconsumption of water, as well as the potential complications of muscle damage when a deconditioned person does prolonged, strenuous exercise. Furthermore, it also illustrates the importance of considering EAHE within the differential diagnosis for acute alterations in level of consciousness. Lastly, it shows the importance to prioritize patient treatments for conditions that are an immediate threat to life or limb.
Keywords
Introduction
Exercise-associated hyponatremia (EAH) has been well-documented as a potentially serious condition among ultra-endurance participants, including hikers within Grand Canyon National Park (GCNP).1–3 Overdrinking large volumes of fluids is the most common denominator in the majority of EAH cases. If left untreated, EAH can progress from mild to severe, culminating with life-threatening cerebral edema that is known as exercise-associated hyponatremia encephalopathy (EAHE).4–6 Also similar to endurance athletes, it is not uncommon for Grand Canyon hikers to develop exercise-induced muscle damage (EIMD) with exertional rhabdomyolysis (ER).7–10 Additionally, in rare cases like this, severe ER has also been associated with acute compartment syndromes (ACS) and acute kidney injury (AKI).9,10
Case Report
On June 20, 2016, a deconditioned, overweight (36.5 kg/m2 body mass index) but otherwise healthy 41-year-old man on no medications or supplements, backpacked 22.5 km (14 miles) into the Grand Canyon for an overnight camping trip during hot weather (high temperature 45.5 °C or 114°F). After a light breakfast, he descended 1830 m (6000 feet) over approximately eight hours, drinking >7.5 L (two gallons) of water (without electrolytes) along the way. Due to loss of appetite, he ate little and slept poorly that night secondary to frequent urination, as well as leg muscle soreness, for which he took no medication. At 0400 h, he began hiking out. Around 1200 h, after hiking 11.6 km (7.2 miles) with 488 m (1600 feet) of elevation gain, and drinking an estimated 7.5 L (approximately 2 gallons) of water, he informed his cohikers he needed to stop secondary to leg pain and dizziness. Cohikers contacted GCNP emergency medical services (EMS) and were instructed to begin immediate cooling of the patient by immersion in a nearby creek. After 15 min, the patient suddenly became disoriented. His cohikers called EMS again, requesting emergency assistance. At 1500 h, medics arrived and found the patient minimally responsive with a Glasgow Coma Scale score (GCS) of 7. Although acute hyponatremia was suspected, a confirmatory i-STAT test for blood sodium level was unavailable. At 1540 h, during the helicopter evacuation, the patient had a grand mal seizure. After landing on the rim minutes later, the patient was transferred to another air ambulance and intubated (GCS of 3 T). Despite lacking a confirmatory sodium level, an empiric IV bolus of 100 ml of 3% HTS for suspected EAHE was administered. Following this, the patient was then flown to the nearest hospital, Flagstaff Medical Center. Upon arrival, he was noted to have a GCS of 6 T with stable vital signs except for mild tachycardia. Noxious stimuli applied to the upper extremities triggered withdrawal but no response in the lower extremities, which were notably tense and swollen.
A comprehensive metabolic profile showed significant hyponatremia with a serum sodium of 114 mmol⋅L−1. An elevated creatine kinase (CK), plus elevations in aspartate aminotransferase (AST) and alanine aminotransferase (ALT), indicated exertional rhabdomyolysis. 11 A complete blood count, cardiac enzymes, and coagulation studies were normal (see Table 1 for admission lab values). After IV administration of an additional 150 ml of 3% HTS, the patient was admitted to the Intensive Care Unit. At 1600 h on Day 2, his CK level reached 400,000 U⋅L−1. On exam, he was also noted to have increased tension in both lower legs, suggestive of ACS. Very high compartment pressures, > 80 mm Hg (normal 0–8 mm Hg) in both anterior and lateral compartments of the lower legs, confirmed the diagnosis, which was immediately treated with bilateral anterior and lateral compartment fasciotomies.
Laboratory testing results on day of admission.
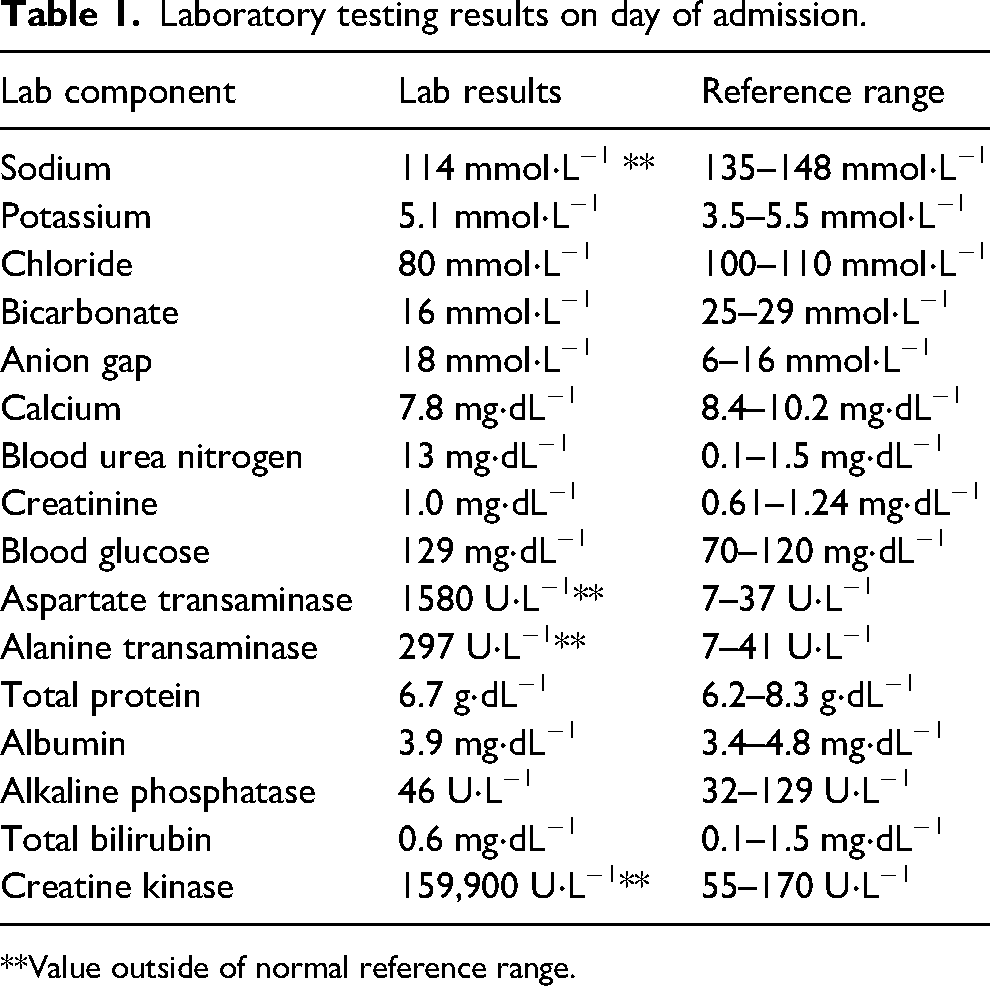
**Value outside of normal reference range.
By mid-day on Day 3, after his neurologic status had returned to normal, he was extubated. Additionally, his serum CK had dropped to 73,188 U⋅L−1, and his sodium improved to 130 mmol⋅L−1. His elevated liver enzymes also improved, but his serum creatinine, however, rose to 1.5 mg⋅dL−1 with a drop in estimated glomerular filtration rate (GFR) to 52 mL/min/1.73m2, consistent with mild AKI. By Day 5, his sodium had returned to normal at 136 mmol⋅L−1, and by Day 10, after oral and isotonic IV fluids, his creatinine and eGFR normalized. On Day 17, he was discharged.
Discussion
This case is extraordinary. The only other similarly severe EAH/ER case reported in a hiker (not a runner), one without concomitant AKI, was reported in a 19-year-old male admitted to a hospital with an altered mental status and seizure following overconsumption of water while hiking for several hours during high heat and humidity. 11 His serum sodium concentration dropped to 115 mmol⋅L−1, and his serum CK peaked at 10,300 U⋅L−1.
Exercise-associated hyponatremia is defined as a serum sodium level below 135 mmol⋅L−1 that develops during or up to 24 h after physical activity. EAH most frequently results from overhydration in combination with fluid retention from non-osmotic stimulation of arginine vasopressin (AVP) secretion.5,6 Early symptoms of EAH include nonspecific nausea, vomiting, and headache, and if untreated, can rapidly progress to confusion, ALOC, seizure, coma, and death.3–6 The presence of signs and symptoms of central nervous system dysfunction and low serum sodium supports the diagnosis of EAHE. This is caused by the transfer of water from plasma and cerebrospinal fluid into the brain, causing cerebral edema. If left untreated, death may occur from brain herniation. Therefore, EAHE requires prompt recognition and immediate treatment with HTS for rapid reversal of the condition.12,13 Consideration must also be given to other possible etiologies for seizures or an ALOC, which are multiple. Common causes include hypoxia, hypo- or hyperthermia, toxins, metabolic or psychiatric disorders, infection, intracranial lesions, or cerebrovascular accidents.
It is also imperative to include EAH as part of the differential diagnosis with heat illness.2,13 Many EAH cases among Grand Canyon hikers are often misdiagnosed (by themselves or other hikers) as exertional heat illness (EHI) due to overlapping signs and symptoms (see Table 2). This patient and his cohikers wrongly believed he had EHI, and he was encouraged to drink more fluid, which exacerbated his condition. Further, their treatment decision was in direct opposition to the international consensus recommendations and a clinical practice guideline for the field treatment of EAH, which is fluid restriction 13 (see Figure 1).
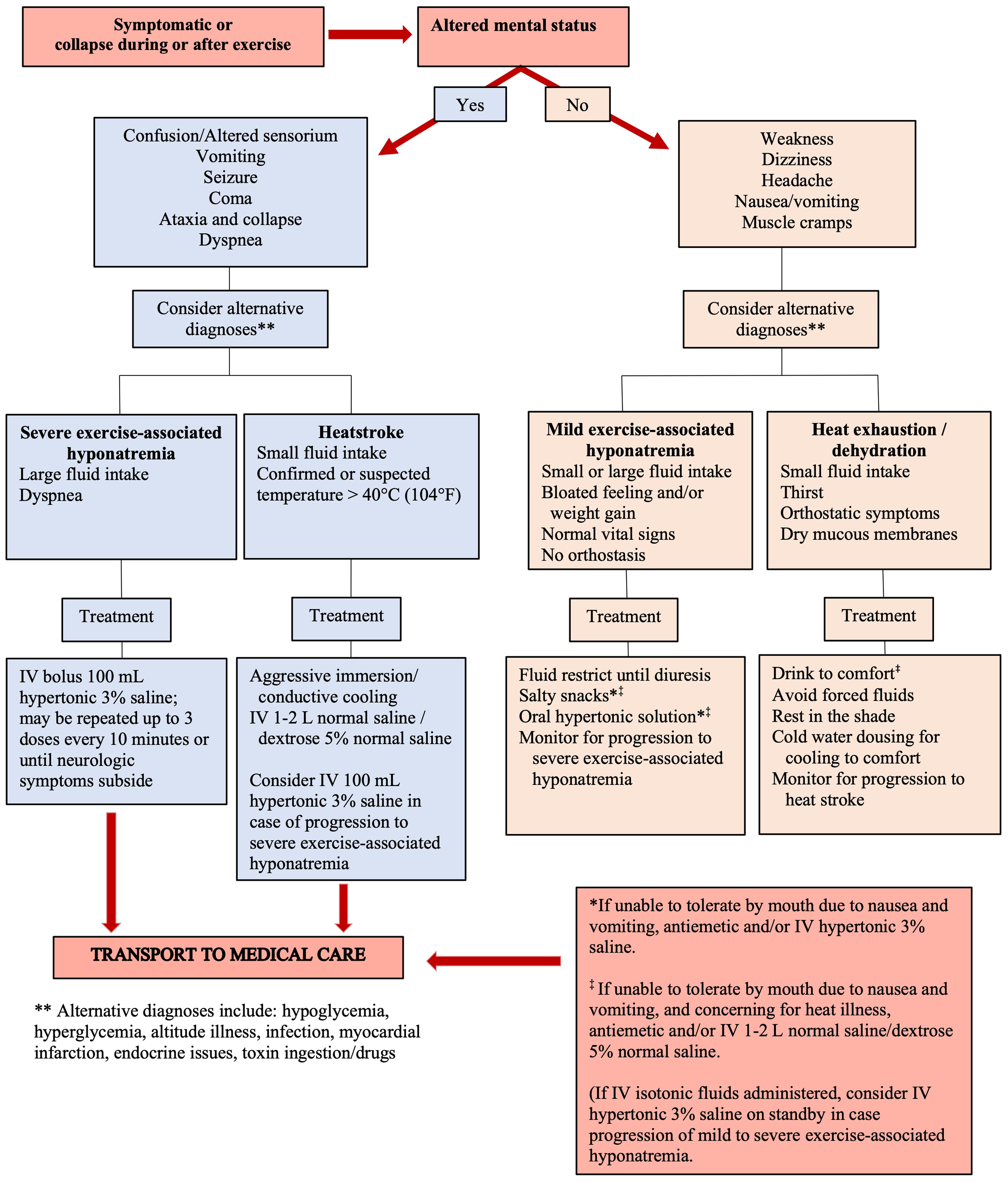
Clinical approach for field treatment of suspected exercise-associated hyponatremia or heat-related illness. Figure modified with permission. 13
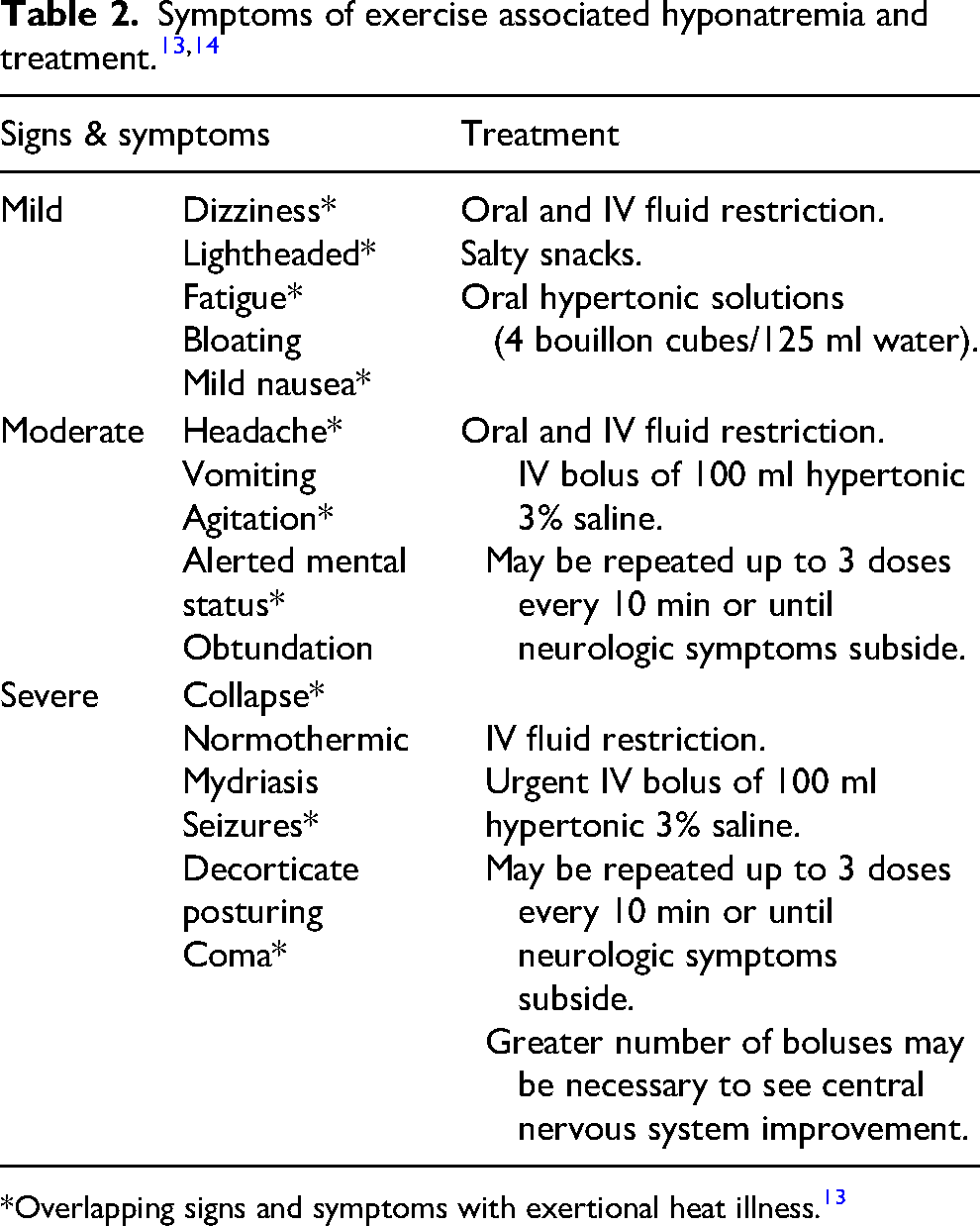
*Overlapping signs and symptoms with exertional heat illness. 13
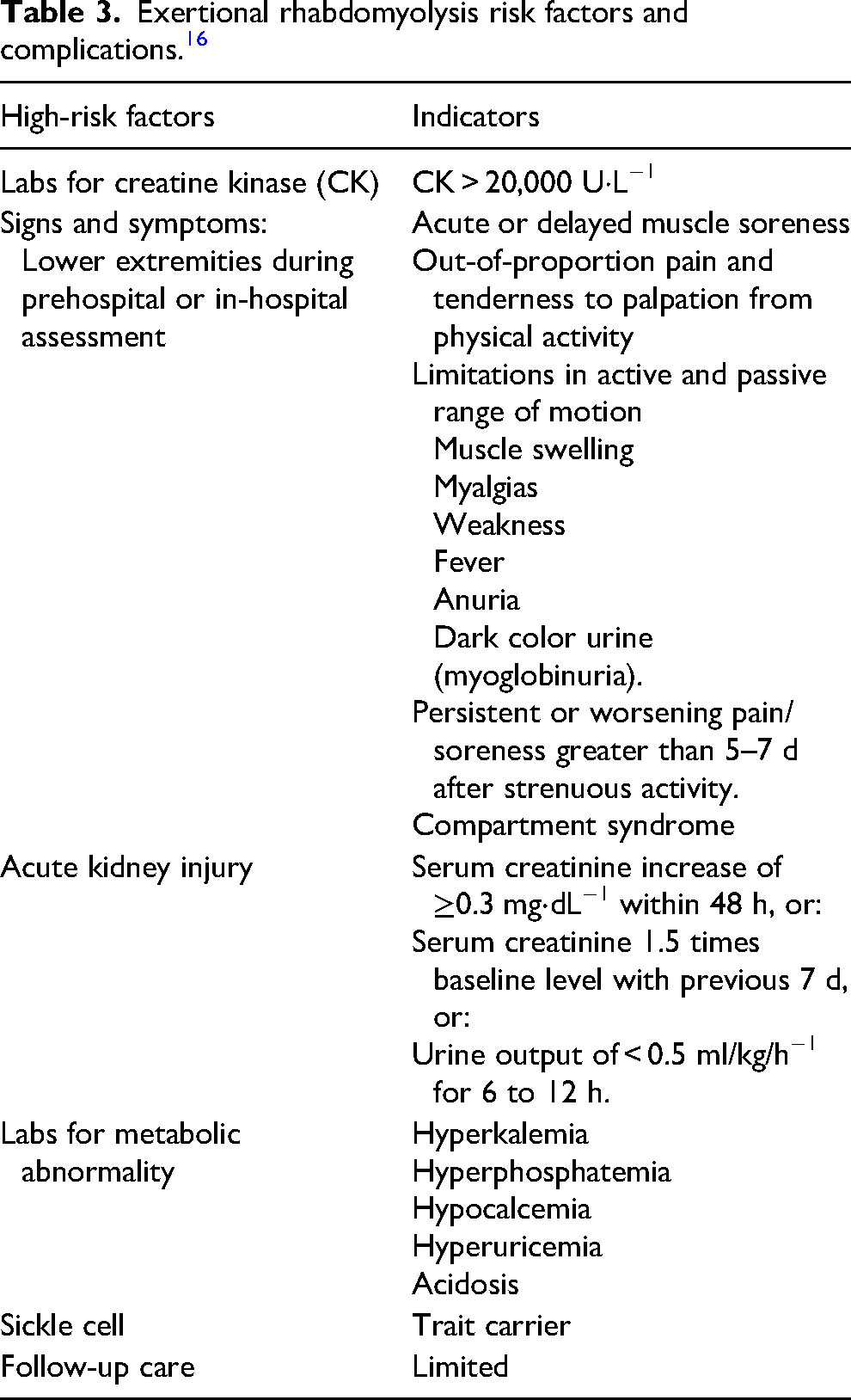
Exertional rhabdomyolysis is not uncommon and, again, can be associated with ACS and AKI.7,8 ER is typically caused by unaccustomed muscle contraction during strenuous exercise, as documented during military basic training; ultramarathon runners; downhill running and hiking, especially with eccentric (muscle lengthening) contraction; and other activities. 7 These repetitive movements can cause the breakdown of skeletal muscle and release cellular constituents into the circulation, including proteins such as myoglobin and enzymes like CK. Elevations in AST and ALT are also seen as the result of muscle cell injury, not liver damage. 15 Other complications of ER include electrolyte derangements, cardiac arrhythmias, and disseminated intravascular coagulation (see Table 3 for ER risk factors). Signs of clinically relevant ER include concurrent dark urine (pigmenturia), ACS, and AKI due to elevated myoglobin and serum CK. 16
Exertional rhabdomyolysis risk factors and complications. 16
Repetitive downhill hiking, as in the Grand Canyon, can lead to EIMD that can progress to exertional rhabdomyolysis (ER), especially in deconditioned individuals like this patient. 17 A diagnosis of ER is made when the serum CK increases to 5 times the upper limit of normal or 1000 U⋅L−1 following strenuous exertion. 16 However, some clinicians do not desire a cutoff for CK levels since well-trained athletes can have increases in CK (10,000 to 15,000 U⋅L−1) and myoglobin following strenuous exercise without complications or the risk for renal injury.16,17 Serum CK levels up to 250,000 U⋅L−1 have been reported with overexertion, and in severe cases with complications, CK can rise to over 1,000,000 U⋅L−1. 18 These increases can be seen as early as 2 to 12 h after muscle injury, with peak values between 48 to 72 h. With concomitant EAH and ER, the pathophysiology remains unclear and merely speculative, such as (1) hyponatremia may facilitate membrane instability leading to rhabdomyolysis or (2) ER-induced renal insufficiency may precipitate dilutional EAH. 5
An ACS occurs when there is increased pressure within a closed muscle compartment that results in impaired circulation and is considered a surgical emergency. Delays in diagnoses and effective surgical intervention can lead to tissue ischemia, necrosis, and irreversible muscle and nerve damage.19,20 Often, when there is no trauma to the extremities, there can be limited awareness and, consequently, a delay in diagnosis. Even greater delays may be seen if the acute ACS occurs in an austere setting where evacuation to definitive care may be difficult and prolonged.
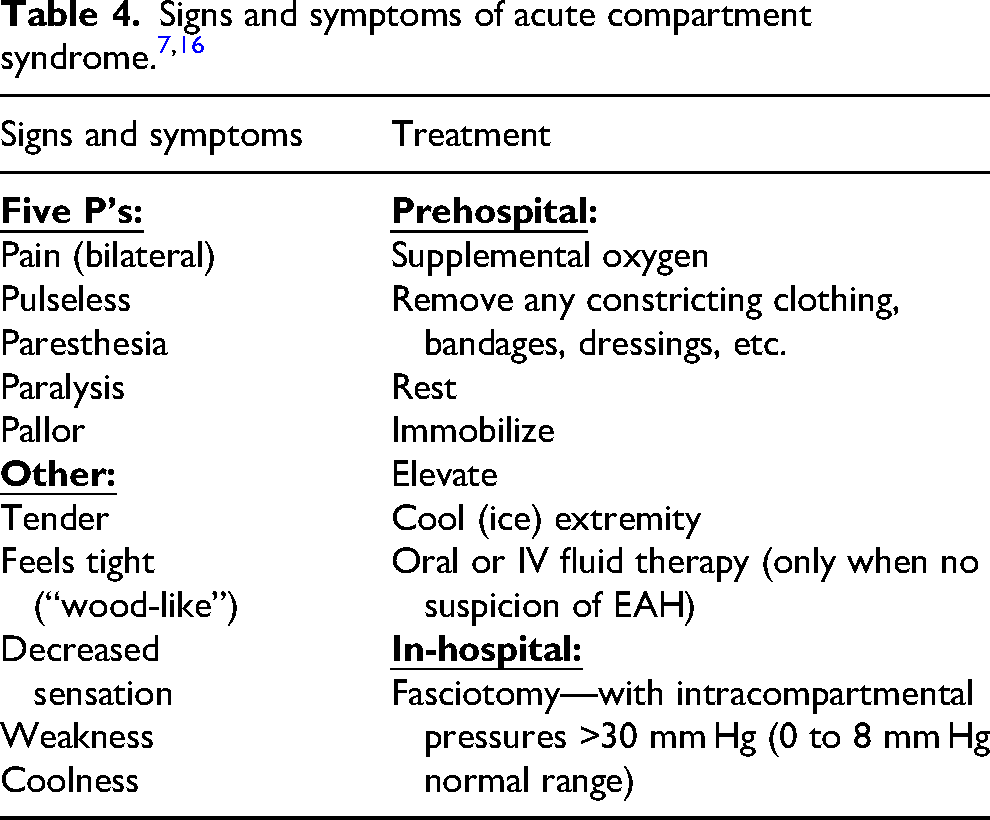
Based on physical assessment for signs and symptoms of ACS (see Table 4) in the prehospital setting, it is essential to develop a high index of suspicion, along with effective communication at patient transfer, to begin awareness and prevent further delays in diagnosis at the hospital. Emergent treatment for ACS involves surgical fasciotomy to release the compartment pressure and restore perfusion in an effort to prevent the devastating consequences of irreversible muscle and nerve damage or limb loss. Generally, patients diagnosed with acute ACS who have surgical treatment within 24 h have no evidence of long-term complications.19,20
When EHI with severe dehydration, ER, or AKI are diagnosed separately, these require aggressive IV isotonic fluids (eg, IV 1–2 L per h).7,16 A diagnostic paradox exists for onsite recognition and intervention because treatments for EAH versus EHI, ER, and AKI are in opposition.7,13,15,21 Historically, a common error among endurance participants and some medical providers (many who are unfamiliar with EAH) is mistakenly interpreting signs and symptoms of EAH as those of EHI. Subsequent treatment with inappropriate oral or IV fluids can exacerbate the underlying hyponatremia due to ongoing renal retention of free water in the presence of elevated AVP.12,13
It is also well-documented that prolonged endurance running, such as ultramarathons, is independently associated with EAH, ER, or mild AKI.13,15,22,23 Again, however, it is unusual to see all three in combination, as in this case. Notably, there is a report of four ultra-endurance participants from the same event requiring hospitalization for EAH, ER, and AKI that resulted in prolonged hemodialysis after running their ultramarathon during high ambient temperatures. 24
Signs and symptoms of EAH can be acute or delayed hours after the event. Endurance athletes may not seek medical care for nonspecific signs and symptoms of ER and AKI immediately post-event since they can be delayed up to 32 h or longer, as with these 4 ultra-endurance runners. 24 Multiple conditions can be synergistic during prolonged endurance events, such as high ambient heat, downhill running, muscle damage, electrolyte imbalances, dehydration, and nonsteroidal anti-inflammatory drug or diuretic ingestion. Any of these factors may contribute to the development of AKI, 23 as evident in our GCNP case patient, whose mild AKI became apparent on Day 3, along with the peak in his serum CK. His mild AKI was well managed with IV fluids after his serum sodium returned to normal limits. Again, the combination of EAH and ER with severe AKI that required hemodialysis (from 10 d to 6 wk) is extremely rare. 24
Conclusion
Awareness of the dangers of EAH from overdrinking water remains deficient in the general public, as evident with this patient and his cohikers, whose initial treatment included more water consumption for presumed EHI, which likely exacerbated his condition. Furthermore, it is very important for healthcare providers to consider EAHE as part of the broad differential diagnosis for an acute alteration in level of consciousness or seizures.
Furthermore, improved public awareness is needed regarding increased risks of ER in unfit or deconditioned individuals undertaking extreme endurance activities without proper physical preparation. Again, mild to moderate cases are common and usually need no medical intervention. However, when there are signs and symptoms suggestive of severe ER with possible associated ACS or suspicion of renal insufficiency, clinical management within 12–24 h is vital. This case also identifies the importance of appropriate fluid management for associated complications with EAH, such as EAHE, acute ER, and AKI. If concomitantly seen, care providers also need to prioritize treatment on managing life-threatening EAHE first, followed by ER-related limb-threatening compartment syndromes, and then management of the AKI.
Footnotes
Acknowledgments
The authors are grateful for the assistance provided by the GCNP medics, physicians, and the patient during post-event interviews conducted by TMM.
Author Contribution(s)
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.