
Abstract

Dear Editor,
I read the article by Standifird and colleagues 1 with interest. Tourniquet management and tourniquet conversion are highly relevant topics for wilderness medicine clinicians given the long extrication times often associated with patient evacuation out of wilderness environments. In Figure 3 of the article, the authors present a suggested tourniquet conversion guideline that they suggest should be used by “search and rescue, National Parks Service, or extremely rural/frontier organizations.” What is presented, however, is simply a description of how to perform a tourniquet conversion. This is not a novel tool—the content mirrors previously published tourniquet conversion procedures that the authors already presented elsewhere within the article in Figures 1, 2, and 4.
There is nothing different about the process of taking off a tourniquet and monitoring for subsequent bleeding in a wilderness vs an urban context. The value of a wilderness tourniquet conversion guideline would be to guide clinicians through the decision of when to attempt a tourniquet conversion while still in a wilderness environment. The key criteria that should inform this decision are how long the tourniquet has been applied and the anticipated time it will take to transport the patient to a higher level of medical care. Because I agree with the authors on the value of developing a guideline for wilderness tourniquet conversion, here I present an alternative guideline that is based on these considerations.
There are two competing concerns related to the length of time a tourniquet has been applied. The first is that the longer a tourniquet has been applied, the higher is the risk of permanent damage to the hypoxic tissues distal to the tourniquet. The second concern is that the longer a tourniquet has been applied, the higher the risk is of precipitating a reperfusion syndrome by taking the tourniquet off. The “Reperfusion Toolbox” developed by Drs Weinrauch and Peters offers an excellent review of the features of this reperfusion syndrome and how the different elements can be managed. 2 The decision to attempt a tourniquet conversion is a balance between taking the tourniquet off as soon as possible to avoid or limit hypoxic tissue damage while not taking the tourniquet off in a context where the patient is at risk of reperfusion syndrome that cannot be appropriately managed with the medical resources at hand.
If a tourniquet has been applied for less than 2 h, the risk of a reperfusion syndrome is very low. 3 A tourniquet conversion therefore can be reasonably attempted in a wilderness environment as long as the wilderness clinician has some other means available to achieve hemostasis (eg, materials for wound packing) and there are no specific contraindications to taking down the tourniquet (the contraindications are; the patient is in shock, the tourniquet is managing a traumatic amputation, and the clinician is unable to closely monitor the patient for ongoing bleeding after tourniquet removal 4 ). The risk of permanent tissue damage from hypoxia is also considered very low within 2 h. 3 If a patient is able to be evacuated and will arrive at a higher level of care within 2 h of the tourniquet being placed, and if attempting a tourniquet conversion in the field would significantly delay patient evacuation, the wilderness clinician should defer the attempt at tourniquet conversion and allow the evacuation to proceed.
If a tourniquet has been applied between 2 and 6 h, the patient is within the time frame that permanent tissue damage is anticipated to occur. 3 Unfortunately, the patient is also within the time frame where they are at risk of experiencing a reperfusion syndrome. 2 Wilderness clinicians should only attempt tourniquet conversion within this time frame if they have sufficient training and resources at hand to monitor for and manage the complications of reperfusion syndrome. The necessary resources include cardiac monitoring, the ability to administer intravenous or intraosseous fluids, and availability of advanced cardiac life support medications. 5 This will not be practical in the majority of wilderness scenarios. Patients within this time frame should be evacuated, if possible, at the highest priority level (eg, life or limb) to a higher level of care.
If a tourniquet has been applied for more than 6 h, there is a high likelihood that the hypoxic tissues have experienced significant permanent damage. 3 There is also a high likelihood that the patient will experience a significant reperfusion syndrome when the tourniquet is taken down. 3 Patients should be in a critical care setting when attempting to convert a tourniquet that has been applied for more than 6 h, and therefore, a tourniquet conversion should not be attempted in a wilderness context. The approach described here is presented in Figure 1.
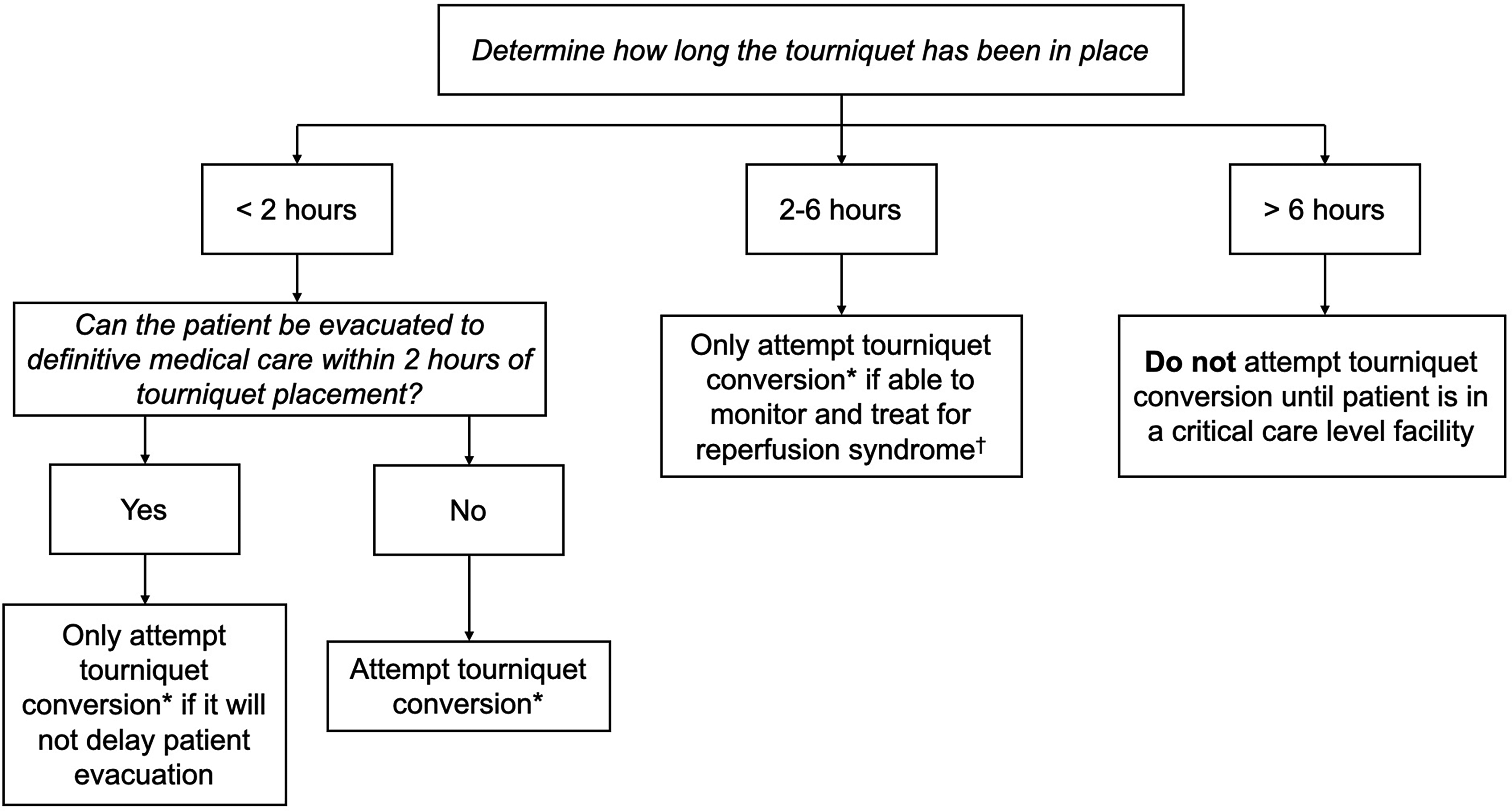
A wilderness tourniquet conversion guideline—when to attempt the procedure.
In their suggested guideline, the last step that the authors present is that “conversion may be reattempted in 10 to 15 min.” If a clinician were unable to stop the bleeding during an initial attempt at tourniquet conversion, there is little reason to expect that a subsequent attempt would be successful unless a different approach at achieving hemostasis was employed. There is, however, significant risk to the patient in repeating multiple attempts at tourniquet conversion, because each attempt is associated with the risk of significant blood loss, and each attempt will exacerbate hypothermia and hypotension, both of which are detrimental in trauma patients and difficult to manage in an austere wilderness environment. 2 A repeated attempt at tourniquet conversion should only be done if additional tools or more experience providers become available following the initial unsuccessful attempt.
I thank the authors for raising the important topic of tourniquet management in the wilderness environment. I hope that the approach that I have presented here on deciding when to attempt a tourniquet conversion in a wilderness context is helpful to individuals and organizations that may need to manage this situation in the future.