
Abstract
Catfish are a highly diverse group of fish comprising more than 3500 species found in both freshwater and marine ecosystems. Upon handling, they can inflict a sting, with certain species capable of inducing significant pain and injury to the affected extremity. The prevalence of aquatic activities, such as fishing by line or manual capture (“noodling”), increases the likelihood of catfish stings, making prompt identification and treatment an important aspect of managing such encounters. A case of a presumed catfish spine injury during noodling in Tallahassee, Florida, is presented. The pectoral fin penetrated the volar aspect of the patient's right hand resulting in immediate pain and numbness. Over the course of 2 weeks, the patient developed distal ulnar neuropathy with conduction block at the wrist level. Surgical exploration revealed the ulnar nerve to be grossly intact, but the area surrounding the terminal division point of the ulnar nerve in the hand displayed infiltration by fibrous tissue that entrapped the nerve and its branches. Following surgical release of the ulnar nerve and its terminal branches from the fibrous tissue, complete resolution of distal ulnar neuropathy was achieved. In this patient's case, the absence of foreign bodies and the lack of visible nerve damage suggest that the injury to the patient's hand was largely attributable to toxin-mediated proinflammatory response and fibrosis.
Introduction
Catfish are a diverse group of ray-finned fish, or Actinopterygii, comprising more than 3500 species in about 40 families. They are found in both freshwater and marine ecosystems. Aquatic activities, especially in regions where many catfish species are endemic, can put individuals at greater risk of being stung and exposed to venom through rigid dorsal and pectoral spines. Catfish spines have long been considered a defensive adaptation against predators. When the fish become agitated or threatened, their spines become locked in an outstretched, defensive position.1,2 This increases the likelihood of injuring the predator and prevents the passage of the catfish through the predator's mouth and esophagus. 3 “Noodling,” also known as hand fishing or grabbling, is a form of fishing for catfish that began as a folk fishing technique in the southern United States. While noodling, a fisherman will extend their hand into dark crevices or holes where catfish are likely to be located and grab hold of the fish by its mouth. Once the catfish bites on the fisherman's hand, it is pulled to the surface.
Noodling remains a common practice in the southern United States. Thrashing from the catfish during noodling can put fishermen at a high risk of being stung by the spines. The catfish sting can result in envenomation due to direct exposure from the dorsal and pectoral spines or local physical trauma and reactive tissue inflammation independent of venom inoculation. 4 Symptoms of a catfish sting can vary from severe pain, numbness, and wound blanching to skin necrosis and gangrene. 2 Nerve injuries resulting from catfish stings typically arise from the mechanical disruption of nerves caused by the sharp edges of the fish spines. In this report, we present a patient who reported experiencing a catfish sting that caused a hypothenar puncture wound, subsequently leading to progressive ulnar neuropathy at the level of Guyon's canal. We discuss the successful surgical treatment of this complication and present intraoperative findings.
Case Report
A 47-year-old, right-handed man complained of a 2-week history of pain and numbness in his right ring and small fingers. The patient was an experienced fisherman and reported that while noodling in Tallahassee, Florida, 2 weeks earlier, a “catfish fin penetrated his hand.” The pectoral fin had penetrated the palm of his right hand around the area of the proximal hypothenar region. Immediately following the incident, he experienced acute pain followed by numbness in the entire right upper extremity for about 6 hours. He promptly removed the fin and received wound management at a local urgent care center, where he also received a tetanus booster and antibiotics (minocycline and doxycycline for 2 weeks). Subsequently, the patient reported a progressive decrease in grip strength in the right hand over the course of 14 days.
On physical examination, the patient had a normal range of motion in the right elbow and wrist. A healing wound at the reported site of injury (pectoral spine penetration) was located on the hypothenar crease, 1.5 centimeters distal to the wrist flexion crease (Figure 1A). Percussion over the right ulnar nerve at Guyon's canal elicited numbness and tingling, whereas the percussion test over the cubital tunnel was negative. The strength of the flexor digitorum profundus to the fourth and fifth digits was 5/5. However, the first dorsal interosseous muscle showed a strength of 3/5 with some atrophy and valley wasting (Figure 1B and C). The patient was unable to fully adduct the fourth and fifth digits. A positive Froment sign and a positive Wartenberg sign were observed. These findings were suggestive of right ulnar neuropathy. The x-rays of the right forearm and hand as well as ultrasound did not reveal any foreign bodies or local fluid collection. The patient continued to experience numbness, pins and needles sensation, and decreased strength in the right hand. An electrodiagnostic study was ordered.
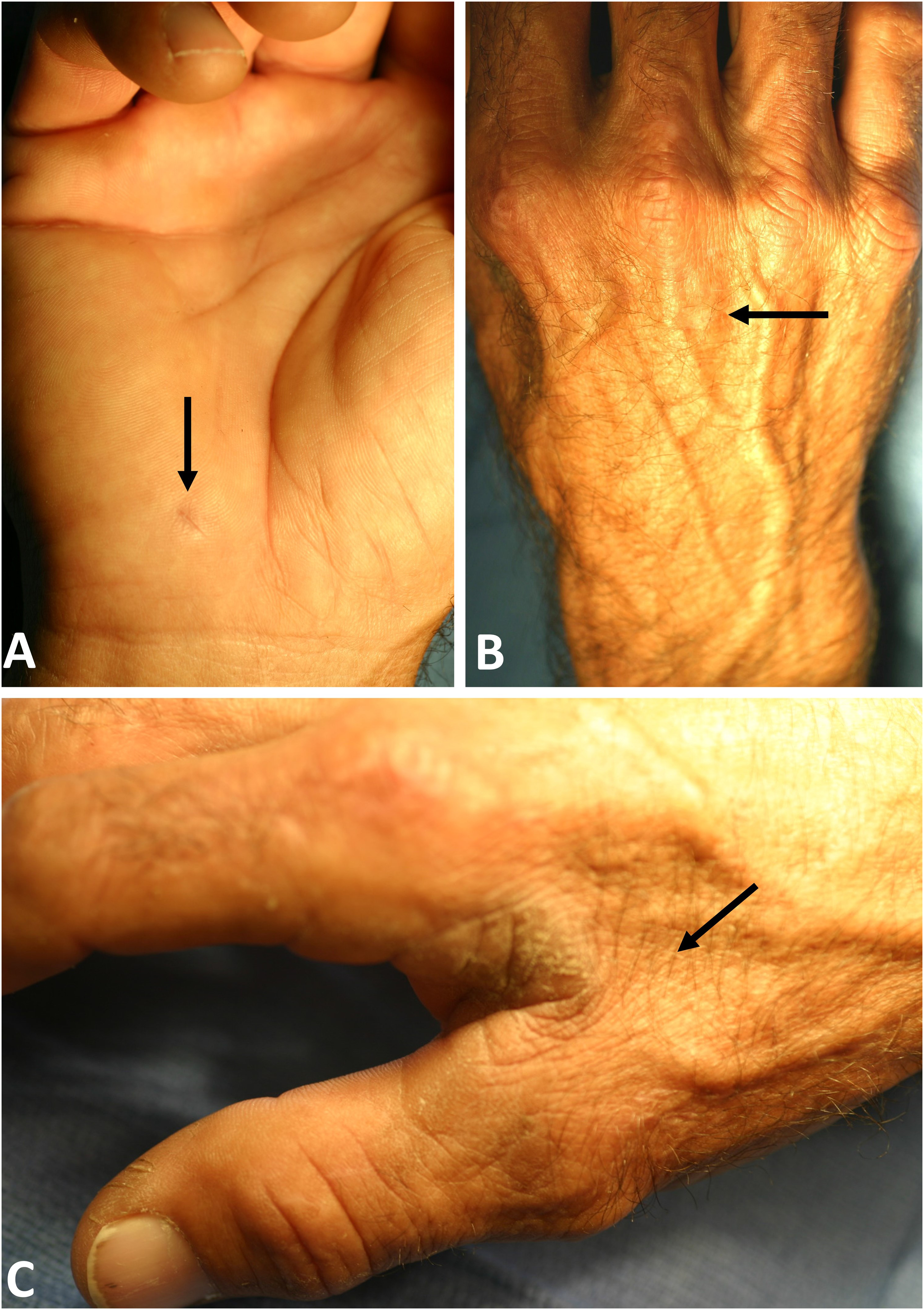
Patient's right hand, approximately 2 weeks following reported local envenoming by a presumed catfish. A, The arrow highlights the entry point of the catfish spine. B, Note the valley wasting (arrow) on the dorsal aspect of the hand. C, The arrow indicates the atrophied first dorsal interosseous muscle.
Six weeks later, the patient returned for reevaluation. The physical exam again revealed first dorsal interosseous atrophy and some valley wasting, a positive percussion test at the cubital tunnel, and tenderness at Guyon's canal on the right hand. The electrodiagnostic study revealed a 21.35% decrease in right ulnar nerve conduction velocity across the elbow and an ulnar sensory distal latency of 4 msec at the wrist (normal <3.7 msec). Electromyography revealed no insertional activity nor amplitude and +1 fibrillation potentials in the right first dorsal interosseous. These results suggested injury to the ulnar nerve at the wrist with a conduction block as well as a mild cubital tunnel syndrome. Based on these findings, he underwent surgical exploration of the ulnar nerve at both the right wrist in the Guyon's canal and the right elbow at the cubital tunnel.
The surgical findings demonstrated scar tissue in the region abutting the terminal division point of the ulnar nerve at the wrist and hand. All the sensory and motor branches of the ulnar nerve were identified and freed from the surrounding fibrous tissue. The ulnar nerve itself was intact (Figure 2) and no foreign bodies or retained catfish spines were found. Subsequently, the cubital tunnel was decompressed, and as the ulnar nerve appeared to be hypermobile, an anterior subcutaneous transposition was performed. There were no complications during the surgery. The microbiological cultures of the specimens taken from the site of injury were all negative. Over a 6-week recovery period, the patient experienced a significant improvement in hand strength and complete resolution of the muscular atrophy. The patient underwent occupational hand therapy, and at the 2-month postoperative follow-up, he demonstrated complete resolution of ulnar neuropathy.
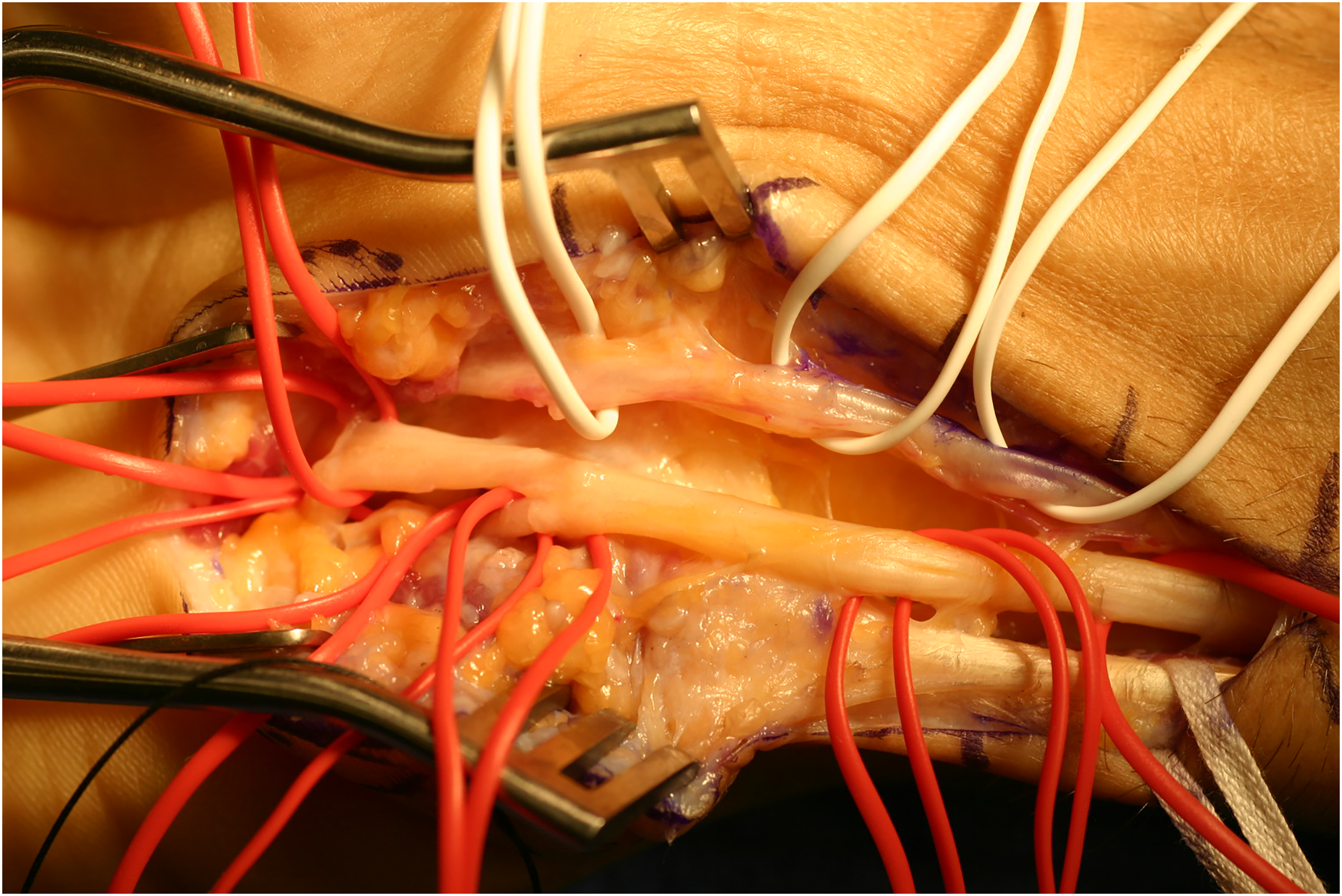
Intraoperative appearance of the ulnar nerve at the Guyon's canal, demonstrating no gross evidence of ulnar nerve injury.
Discussion
This report describes and illustrates a patient who reported sustaining a minor puncture wound from a presumed catfish pectoral fin to the right hypothenar region near Guyon's canal. Subsequently, he developed progressive ulnar neuropathy characterized by sensory deficits and intrinsic hand muscle weakness and atrophy. During the intraoperative assessment, no evidence of gross injury to the ulnar nerve was observed, and there were no indications of an infectious process. The area surrounding the terminal division point of the ulnar nerve in the hand, along with the proximal segments of its superficial and deep branches, exhibited infiltration by fibrous tissue that entrapped the nerve and its branches. The fibrotic tissue was dissected away from the ulnar nerve, releasing the nerve and its distal branches. The concurrent cubital tunnel syndrome was mild and unrelated to the distal neuropathy observed in association with the catfish sting, which was characterized by conduction block and primarily affected the ulnar nerve at or around Guyon's canal. Therefore, in this case, a plausible explanation for progressive ulnar neuropathy at the wrist and hand level is the local release of proinflammatory toxins from catfish spine venom and toxin-mediated fibrosis.
An earlier report detailed the case of a 42-year-old man who was stung by a catfish pectoral spine, with penetration occurring one inch into the proximal portion of his palm. The patient presented 1 month after the injury with median neuropathy. 3 Surgical exploration of the volar carpal tunnel revealed hypertrophic tenosynovitis of the flexor tendons and a 1-inch segment of diffuse firmness in the median nerve. Clinical recovery from neuropathy was achieved following saline neurolysis of the scarred segment of the median nerve and excision of the hypertrophic tenosynovium. 3 Another report described a 12-year-old boy who suffered a catfish sting, resulting in a puncture wound to the right distal forearm. 5 Initially, the patient did not exhibit immediate neurological deficits but developed progressive motor deterioration and ulnar nerve deficits over the course of one month following the injury. Surgical exploration revealed the ulnar nerve to be transected near its entry into Guyon's canal. Microscopic examination indicated extensive fibrosis in the injured nerve region. The gradual onset of nerve deficits suggested a toxin-mediated complication, wherein the catfish spine partially transected the nerve upon entry through the epineurium, introducing toxins into the nerve sheath, subsequently leading to gradual fibrosis and nerve disruption. 5
Catfish stings can result in injury through three different mechanisms: mechanical injury, envenomation, and infections. When a person is stung by a catfish spine, puncture of the skin often causes vascular and neurologic damage to nearby tissue. The sleek arrowhead and serrated edges of the slightly bowed spine facilitate deep penetration, likely to generate significant pain in potential predators. The spines often cause puncture wounds rather than lacerations, and their removal may result in additional tissue damage, hemorrhage, and increased exposure to infectious microorganisms. 6 In addition to the morphology of the catfish spine, its harmful effects are enhanced by the presence of venom. While some catfish have clustered venom-secreting cells resembling organoids, called venom glands, most contain smaller accumulations of venom-secreting cells associated with the spines.7,8
Agitation of the catfish causes locked extension of the fins. Upon puncturing the victim, the spines introduce venom into the wound. 9 Additionally, catfish epidermal secretions contain crinotoxins—proteinaceous toxins that coat the entire body, including the fins. 9 Crinotoxins serve, in part, as antipredator defense mechanisms. Data regarding the role of crinotoxins in human envenomation is limited, but it is possible that a sting coincidentally exposes the penetrated wound to absorption of these ichthyotoxins independent of venom release. The venom constituents vary from catfish species to species. It is estimated that at least 1250 species of catfish from at least 20 families are venomous. 8 Saltwater and tropical species typically produce the worst symptoms and frequently lead to infections. 10 While the mechanism of the various venom components is unknown, the toxins may be hemolytic, inflammatory, dermonecrotic, and vasoconstrictive in nature.4,11,12 A local inflammatory response following a catfish sting, characterized by edema and erythema, is very common. 6
When the catfish spine penetrates the hand or forearm, it can dislodge from the fish and embed itself in the victim's body, serving as a nidus of infection. This also exposes the victim to the possibility of infection, which is a serious complication that must always be addressed in catfish injuries. The murky, aquatic environment in which catfish reside increases the risk of infection due to the prevalence of several microorganisms. This increases the likelihood of complications such as abscess formation and cellulitis. 13 A variety of organisms have been implicated in catfish-related wound infections, including gram-positive and gram-negative bacteria, atypical mycobacteria, and fungi. The common organisms are Vibrio and Aeromonas species found in saltwater and freshwater, respectively, as well as Mycobacterium marinum, found in various water sources regardless of temperature or salinity.1,14,15 Identifying the species of the catfish involved and their respective habitat is, therefore, important in guiding antibiotic selection. Severe outcomes, including limb-threatening infections, extensive necrosis, and gangrene that, in extreme cases, has led to amputation have been documented as a result of virulent bacteria or toxins introduced by catfish stings.11,16
Other than supportive therapy, there is no standard treatment for catfish stings, as treatment depends largely on the type and severity of the injury, which may be determined by a thorough physical, vascular, and neurological evaluation.2,14,17 The wound should be irrigated with normal saline along with debridement of any necrotic tissue. Tetanus prophylaxis is often indicated, and patients should be treated with empiric antibiotics that provide coverage for both gram-positive and gram-negative species.1,3,15,18 Additionally, immediate immersion of the wound site in hot water for 30 to 90 min can serve as an effective analgesia.1,14,19 While some of the thermolabile toxins may undergo denaturation to some extent by hot water immersion, the rapid return of intense pain upon removal of the affected limb or digit from the water suggests that denaturation is not a significant contributor to analgesia. 20 Vasodilation and local immunomodulatory effects may also contribute to this effect. 20
Limitations
We lack any visual evidence, specimen, or other proof identifying the species responsible for the patient's injury. The injury was presumed to be caused by a catfish solely based on the patient's report. Given the patient's expertise as a skillful fisherman, it is highly improbable that he misidentified the catfish as the culprit behind the injury. Based on the intraoperative findings of local fibrosis at the site of catfish spine puncture, we hypothesized that a toxin-mediated fibrosis might be responsible for the observation. However, it is important to consider the possibility of local tissue damage adjacent to the ulnar nerve, followed by an inflammatory wound-healing process that could lead to fibrotic changes and the patient's symptoms. Additionally, while there is no evidence of a venom component in well-studied catfish venoms that can directly induce a fibrotic reaction, there is experimental evidence of proinflammatory effects of some related venoms. Thus, there are some minimally studied venom activities associated with the condition, but none that can be definitively assigned.
Conclusion
Aquatic activities, including fishing and noodling, in regions where catfish species are endemic put individuals at risk for catfish stings. The present case demonstrates a subacute peripheral (ulnar) neuropathy subsequent to a minor penetrating injury from a catfish pectoral fin. Surgical exploration revealed no visible lesions to the ulnar nerve that may have explained the neurological findings. The area surrounding the terminal division point of the ulnar nerve in the hand was infiltrated by fibrous tissue that entrapped the nerve and its branches. Surgical release of the ulnar nerve and its terminal branches from the fibrous tissue culminated in the complete resolution of the distal ulnar neuropathy. This leads us to suspect that the patient's neuropathy was most likely caused by the action of the catfish proinflammatory venom introduced by the penetrating spine and possible toxin-mediated fibrosis. This case further illustrates the importance of follow-up care for patients with catfish spine exposures, considering the possibility of late complications.
Footnotes
Author Contribution(s)
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.