
Abstract
Snakebites in unusual anatomical locations may lead to life-threatening consequences. Merrem's hump-nosed viper (Hypnale hypnale) is a medically important snake in Sri Lanka and India that causes many bites and envenomings. Their bites occur almost exclusively on upper and lower limbs and commonly result in local effects, with some patients developing systemic envenoming. No antivenom is available for treating envenoming by H. hypnale. We report an unusual case of H. hypnale bite on the tongue of a 10-month-old infant resulting in rapid local swelling of the tongue and floor of the mouth, requiring prompt intervention to prevent life-threatening upper airway obstruction. Early tracheostomy prevented upper airway obstruction and, along with supportive steroid therapy and antibiotics, led to a complete resolution of the local effects of the infant without permanent disability, despite the unavailability of antivenom.
Introduction
Merrem's hump-nosed viper (Hypnale hypnale) is a medically important snake in Sri Lanka and South India and is responsible for over one-third of snakebites reported in Sri Lanka.1–3 Most H. hypnale bites cause local effects, but some patients develop systemic envenoming, which includes venom-induced consumption coagulopathy (VICC) and acute kidney injury.1,4 Indian polyvalent antivenom, the only available antivenom in Sri Lanka for snakebite, is ineffective for envenoming by Hypnale spp.
Hypnale spp. are small, terrestrial pit vipers; hence, bites almost exclusively occur on feet and hands.1,4 The local effects on the bite site include pain and swelling, with some patients developing hemorrhagic blister and local tissue necrosis, requiring amputations. However, local tissue swelling rarely progresses beyond half of the bitten limb, hence swelling alone is not a major concern in the management of H. hypnale envenoming. We report an unusual case of H. hypnale bite on the tongue of an infant resulting in rapid local swelling of the tongue and floor of the mouth, requiring prompt intervention to prevent life-threatening upper airway obstruction.
Case Description
A 10-month-old male infant with uncomplicated birth history was presented with a snakebite on his tongue at a primary care center in North Western Sri Lanka. According to the patient's mother, the infant was found in their kitchen, with a bleeding tongue 40 min prior to presentation; a snake was found near the infant. The initial suspicion was that the bite might have happened when the infant attempted to take the live snake into his mouth.
Upon admission, the infant had been crying inconsolably; swelling and bleeding were noted at the right lateral aspect of the tongue. The infant was hemodynamically stable with an oxygen saturation (SpO2) of greater than 94%. The 20-min whole blood clotting test was unremarkable. The dead snake was brought to the hospital and was later identified as a Merrem's hump-nosed viper (Hypnale hypnale) (Figure 1A) by the corresponding author, who is a herpetologist.
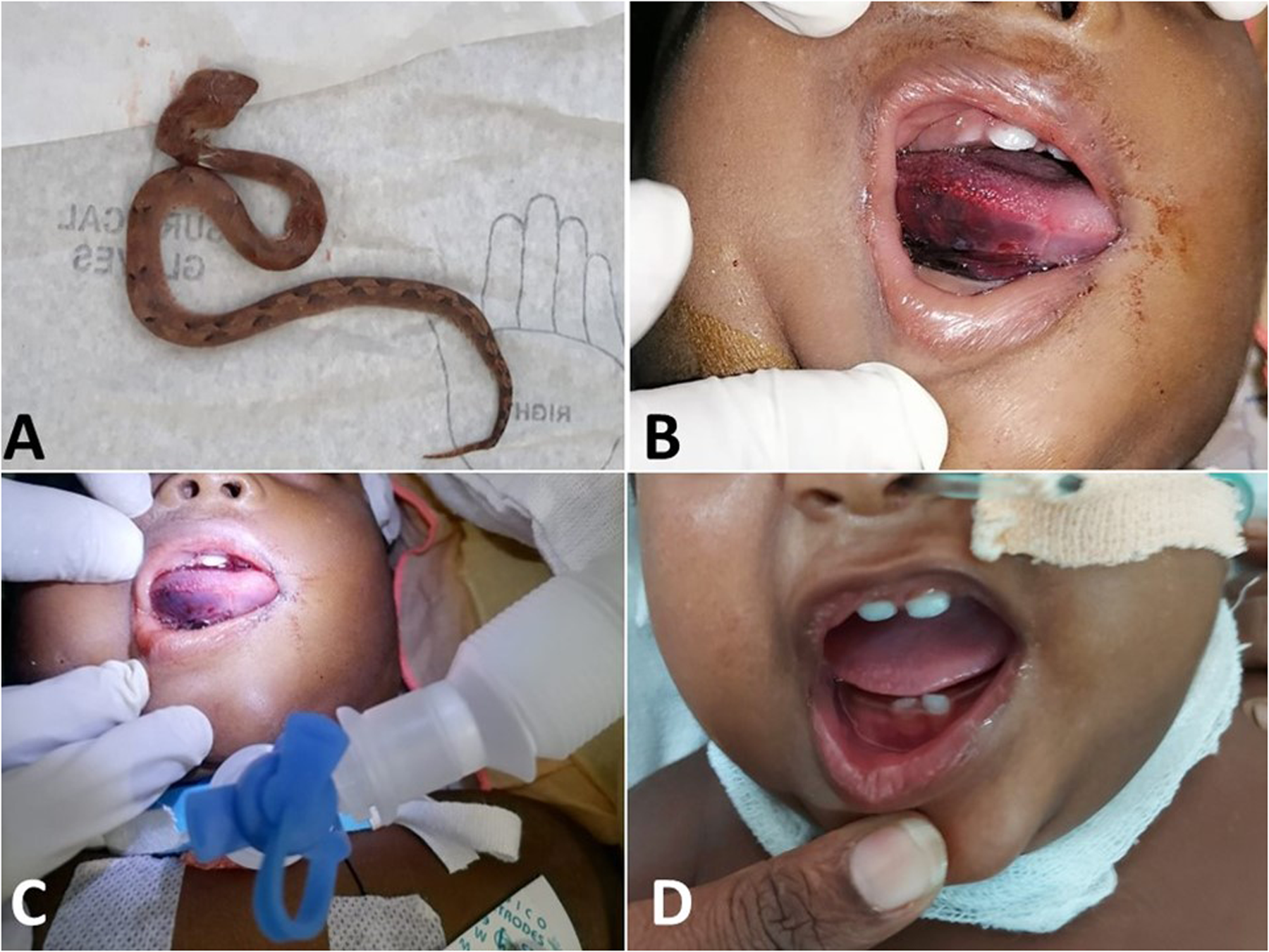
(A) The specimen of Hypnale hypnale that bit the infant; (B) swollen tongue with dark red right inferior and lateral surface; (C) the infant being mechanically ventilated following the tracheostomy; (D) the infant on the sixth day following the bite—note the tongue swelling has resolved and the tracheostomy reversed.
Following the initial assessment, the infant was then transferred to Teaching Hospital Kurunegala Sri Lanka, a tertiary care center. On admission at the tertiary care center, 90 min after the bite, the entire tongue was swollen with bleeding from the right side, and there was mild swelling of the neck (Figure 1B). SpO2 was 99% and a mild stridor was present in the supine position. Laryngoscopy revealed upper airway edema, and the vocal cords were not visualized. To secure the airway, endotracheal intubation was attempted but failed. Therefore, tracheostomy was performed under general anesthesia, 4 h after the bite (Figure 1C). The infant was transferred to the pediatric intensive care unit (PICU) and was sedated with intravenous midazolam infusion and was ventilated under synchronized intermittent mandatory ventilation. On admission to the PICU, the right lateral aspect of the tongue was dark red in color, suggesting sub-mucosal hemorrhage, and was noticeably swollen. However, the tongue had no visible hematomas. There was facial and upper neck swelling. Intravenous dexamethasone (1 mg stat) was administered and followed by regular doses twice daily. Normal saline gauze was applied around the tongue, and the gauze was rehydrated with additional salineonce in every six hours. On the next day, the patient was weaned from mechanical ventilation. The edema of the tongue gradually resolved over the next few days without structural or functional deformity. No necrotic areas or ulcerations were detected on the tongue.
After completing the two days of intravenous dexamethasone, it was given as oral 0.5 mg 3 times a day for 5 days. Intravenous cefuroxime and metronidazole were given for 9 days as empirical antibiotics. The infant had no bleeding elsewhere and had no evidence of coagulopathy (Table 1). Indian polyvalent antivenom was not given due to its ineffectiveness for Hypnale envenoming. The infant had normal urine output, and his serum creatinine concentration returned to normal. The blood picture on the second day showed evidence of microangiopathic hemolytic anemia (MAHA), which started to resolve according to the blood picture on the next day with a decreasing trend in the percentage of the schistocytes. The hemoglobin concentration returned to normal levels by day 6.
Hematological and biochemical parameters of the patient.
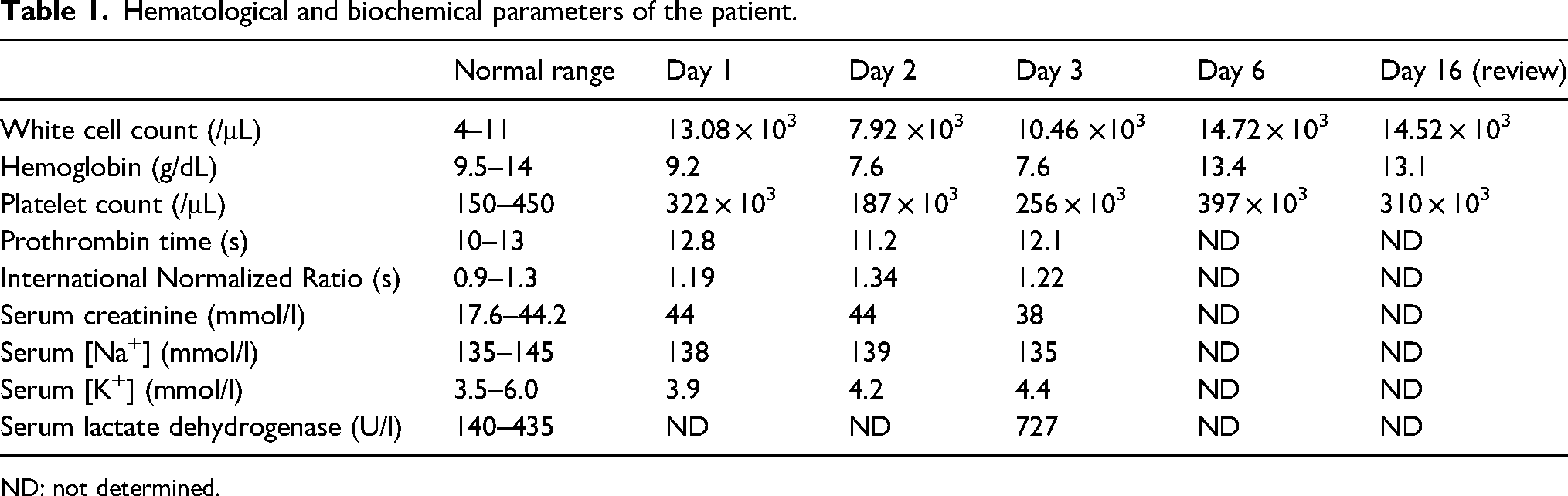
ND: not determined.
Oral feeding was commenced on day 4 postadmission with semisolid foods and liquids, and feeds were tolerated well. Tracheostomy reversal was performed on day 6 postadmission of the bite. He was discharged from the hospital on day 9. The infant had fully recovered when reviewed at the clinic 7 days postdischarge.
Discussion
This infant, who had an H. hypnale bite on the tongue, had rapidly developing local swelling leading to upper airway obstruction. The failed endotracheal intubation prompted a life-saving tracheostomy. The supportive therapy included steroids, antibiotics, and hydration of the tongue. Fortunately, the patient recovered without apparent sequelae.
Snakebite on the tongue is extremely rare in children, and the few reported cases have mainly affected adults. The only previously reported pediatric case was a 9-year-old boy bitten on the tongue by a Wagler's pit viper (Tropidolaemus wagleri), resulting in massive edema that led to dyspnea. 5 However, unlike in our patient, the child had been successfully intubated on the first day, but due to the danger of laryngeal necrosis, a tracheostomy was performed 3 days later. In most previously reported cases of tongue bites by viperids, such as Crotalus horridus, 6 Crotalus atrox, 7 Daboia russelii, 8 Vipera berus, 9 and colubrids like Philodryas olfersii, 10 the patients have been managed with supportive care that includes intubation or tracheostomy with steroids and antibiotics, with or without antivenom. Massive upper airway edema requiring emergency cricothyrotomy following a Crotaus horridus bite at a distant site (thumb) had been reported previously. 11
Our patient developed upper airway obstruction within 2 hours of envenoming due to soft tissue swelling of the tongue. Since the tongue has rich vasculature, it is more susceptible to developing local swelling rapidly. 12 The swollen tongue enlarges posteriorly and obstructs the pharynx. This is followed by the soft tissues of the neck, including the epiglottis and larynx, and the floor of the mouth becomes edematous, which leads to life-threatening laryngeal obstruction. In this case, early identification of upper airway obstruction prompted tracheostomy to maintain the airway.
Previous reports suggest, similar to adults, children with Hypnale bites commonly develop local effects, with systemic effects being uncommon. 13 Although there was no evidence of significant VICC, the blood picture of the infant on the second day showed evidence of MAHA together with the raised serum lactate dehydrogenase levels the next day, suggesting that the infant was having mild systemic envenoming. However, the infant did not develop acute kidney injury, despite not being treated with antivenom due to the lack of specific antivenom for Hypnale. Nonetheless, the effectiveness of F(ab’)2 and whole IgG antivenoms for arresting the progression of local effects of snake envenoming remains inconclusive. 14
Conclusions
Snakebite on the tongue is extremely rare. However, soft tissue swelling due to local envenoming leading to upper airway obstruction is a serious sequela that may occur; this developed in our patient and could have progressed into a life-threatening complication. Early intervention, including airway support with early tracheostomy along with supportive therapy, contributed to our patient’s complete recovery.
Footnotes
Author Contribution(s)
Consent
Written informed consent was obtained from the patient's parents for publication of this case report and the accompanying images.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.