
Abstract
While there is a considerable body of literature on sexual aggression, we know much less about the violation of sexual boundaries within professional relationships. To address this knowledge gap, the characteristics of cases of sexual misconduct in the province of Quebec were extracted, based on a search of published disciplinary decisions between 1998 and 2020, using the legal databases CANLII and SOQUIJ. The search yielded 296 decisions including 249 male and 47 female members from 22 professional orders, and involving 470 victims. Results indicate that male professionals approaching mid-career accounted for a greater proportion of cases of sexual misconduct. Moreover, physical and mental health professionals were overrepresented in cases, as were female adult victims. Acts of sexual misconduct concerned mostly sexual touching and intercourse and occurred during consultations. Female professionals were more inclined to establish romantic and sexual relationships with clients than their male counterparts. Of the 92.0% of professionals found guilty of at least one count of sexual misconduct, two thirds eventually returned to practice. Following the guilty verdict, few faced rehabilitative measures. Recommendations are provided for the prevention of sexual recidivism and the accompaniment of victims of sexual misconduct throughout the disciplinary process.
Introduction
Most individuals rely on the services of professionals for assistance in various aspects of their life (e.g., physical and mental health, legal representation), and when they do, they expect to be treated in their best interest. Despite the mechanisms put in place by professional licensing and regulating bodies to protect the public, sexual exploitation and violence on the part of professionals do occur. Available data indeed suggest that sexual misconduct is not a rare occurrence, it concerns numerous professions, and it can have serious consequences for victims. However, in Canada, few efforts have been directed at systematically documenting reported cases of sexual misconduct to extract a clear portrait of the situation. As a result, the extent of the problem, the characteristics of the individuals involved, the consequences of sexual misconduct, and the measures put in place by professional licensing and regulating bodies to prevent first-time sexual offenses and recidivism, remain largely unknown. In order to fill this knowledge gap, the objective of the study was to explore the characteristics of professionals, victims, and acts of sexual misconduct, as well as the processing delay and outcome of complaints of sexual misconduct, based on the examination of disciplinary decisions from the last 20 years in the province of Quebec.
The Boundaries of the Professional Relationship
Respecting the boundaries of the professional relationship – defined as an agreed-upon relationship between a professional and a client for the purpose of the client obtaining goods or services from the qualified professional (https://www.lawinsider.com) – is considered essential for the protection of the public. Boundaries are the rules that set the professional relationship apart from other types of relationships and that define and delineate expectations, attitudes, remarks, and behaviors that are appropriate in a designated professional context (Barnett, 2014; Black, 2017; Gutheil & Gabbard, 1993; Smith & Fitzpatrick, 1995). These rules can vary according to the cultural and sociopolitical context, the particularities of a profession, as well as circumstantial factors (e.g., practice in remote communities) (Black, 2017; Knapp & VandeCreek, 2012). Boundaries, which circumscribe the role and responsibilities of the professional toward the client, are essential to fostering a sense of trust between the parties and preserving the client’s welfare and dignity (Jorgenson et al., 1997; Sawyer & Prescott, 2010).
Boundary violations are inappropriate actions and behaviors by professionals that breach professional standards of conduct, are unwelcomed by the client, and/or can lead to exploitation or harm (Barnett, 2014; Gutheil & Gabbard, 1993). They must be distinguished from boundary crossing, that is, actions on the part of the professional that deviate from accepted practices but cause no harm to the client (Black, 2017; Gutheil & Gabbard, 1993; Sawyer & Prescott, 2010). Professionals who transgress boundaries use the relationship to the client for personal gains (e.g., affective, financial) and thus lose sight of their duty to act in the client’s best interest (Smith & Fitzpatrick, 1995). The sexualization of the professional relationship is considered especially serious as it is associated with a strong potential for harm (Seto, 1995; Wierzbicki et al., 2012).
Sexual misconduct is defined in the present article in accordance with article 59.1 of the Quebec Professional Code, as “a professional taking advantage of his professional relationship with a person to whom he is providing services, during that relationship, to have sexual relations with that person or to make improper gestures or remarks of a sexual nature” [the masculine form is used but the text applies to all professionals] (Office des professions du Québec, 2020). Sexual intimacy and contacts with clients are considered incompatible with the duty to protect the public and derogatory to the dignity and honor of professions (art. 59.2). The term “victim” is used in the article to designate the receiver of services who experiences sexual misconduct on the part of a professional.
Issues of Power and Consent in the Professional Relationship
Clients turn to professionals to gain help in accomplishing a project, finding a solution to a problem, managing a difficult situation or improving their well-being. Professionals are called upon for their expertise, reputation, authority and/or status, thereby creating an imbalance in the relationship wherein clients are in a position of dependency. Central to this relationship is clients’ trust that professionals will maintain a safe environment, protect shared information, act in their best interest, and refrain from exploiting or harming them. The effectiveness of the professional system rests on the expectation that professionals will protect clients’ dignity and integrity and uphold the conditions ensuring that this trust is not betrayed, at all times (Sawyer & Prescott, 2010; Valiquette, 2007). This fiduciary duty is made clear in professional deontological codes across countries (Allan & Love, 2010; Barnett, 2014).
While it can be argued that adults involved in a professional relationship can freely choose to engage in sexual intimacy or contacts, the question of whether clients can give true consent to the sexualization of the relationship has been raised. In view of the power differential that marks this relationship, even competent and consenting adults can be influenced by professionals or fail to grasp the potential consequences of sexual boundary violation (Ravart, 2007). Moreover, sexual consent may be invalidated by the fiduciary nature of the relationship between professionals and their clients (Black, 2017; Slimp & Burian, 1994). As part of this duty, professionals must preserve the necessary distance, respect, independence, and integrity to ensure that clients are not subjected to undue pressure and that their best interests prevail (Barnett et al., 2007). Considering the nature of the professional relationship, it may be difficult for clients to provide informed consent to the transgression of its sexual boundaries.
The End of the Professional Relationship
In determining whether sexual boundaries have been violated, it may be necessary to identify the end of the professional relationship. In the case of professionals who offer services that lead to a unique or short-term contract (e.g., chemists, land surveyors), the end of the relationship is easily identifiable. The contours of the relationship can be harder to draw for professionals with a clientele base that can renew its access to services over time (e.g., notaries, pharmacists) or whose clients expose personal information or vulnerabilities in the hope of obtaining assistance in managing difficulties or in alleviating discomfort, pain, or distress (e.g., physicians, psychologists). Identifying the point at which the professional relationship becomes immaterial is instrumental in determining when sexual intimacy between the parties no longer constitutes sexual boundary violation. That is, when professionals no longer hold an authority status and clients are independent and detached enough so that both parties can be regarded as equals and set aside those relationship dynamics that are unsuited for romantic or sexual intimacy.
Studies involving physical and mental health trainees and professionals point to discrepancies in the definition of a “former client” and the perceived ethical appropriateness of sexual contacts with clients. Indeed, some consider that the definition applies upon the termination of services or after a period of time following the end of the professional relationship, while others hold the view of “once a client, always a client” (Berkman et al., 2000; Herman et al., 1987; Lamb et al., 2003; Mattison et al., 2002; Salisbury & Kinnier, 1996). Professional licensing and regulating bodies play a key role in defining the end of the professional relationship.
The Prevalence of Professional Sexual Misconduct
Current understanding of the prevalence of sexual misconduct is based on limited findings from studies examining reports to ethical committees and Disciplinary councils, and surveys. Official reports show that 50.0% of the complaints made against psychologists between 1978 and 1988 (Ethics Committee et al. (1988), and 25.0% of cases against social workers that went to hearing between 1986 and 1997, concerned sexual misconduct (Reamer, 1995; Strom-Gottfried, 2003). These data suggest that cases of professional sexual misconduct are far from isolated.
Survey findings also point to the frequent occurrence of sexual misconduct. Based on a review of the literature, Halter et al. (2007) estimate that 52.0% of health professionals know of at least one colleague who has been sexually involved with a client. This is consistent with surveys conducted with health professionals in Canada, the United States, Britain, Australia and New Zealand (Bachmann et al., 2000; Committee on Physician Sexual Misconduct and College of Physicians and Surgeons of British Columbia, 1992; Garrett, 1998; Leggett, 1994). Anonymous surveys asking mental health professionals whether they had ever engaged in sexual contacts with a client reveal that 2.5–9.4% of psychologists (Holroyd & Brodsky, 1977; Lamb et al., 2003; Pope et al., 1979, 1986), 3.8% of social workers (Berkman et al., 2000; Jayaratne et al., 1997), 6.4–13.0% of psychiatrists (Herman et al., 1987; Kardener et al., 1973), 11.1% psychotherapists (Akamatsu, 1988), and 4.8% of counselors answered in the affirmative (Thoreson et al., 1993, 1995). As for physical health professionals, 9.0% of physicians reported engaging in sexual contacts with a patient – among them 42.0% said it happened with more than one patient (Gartrell et al., 1992). While considered inappropriate by 94.3% of Swiss psychiatric nurses, sexual contacts with patients were reported by 16.8% male and 10.5% female nurses (Bachmann et al., 2000).
The prevalence of sexual misconduct is difficult to establish based on the available data. Studies are few and dated and there are marked discrepancies between official reports and survey findings. This may be due to factors such as varying definitions of sexual misconduct and a greater willingness to disclose acts of sexual misconduct anonymously (Assalian & Ravart, 2003). Moreover, sexual misconduct outside of physical and mental health professions remains undocumented. Like sexual aggression, sexual misconduct is mainly covert and known cases likely constitute the tip of the iceberg (Bergeron et al., 2012; Sansone & Sansone, 2009).
Characteristics of Professionals and Their Victims
Professionals
While there is no single profile of professionals who perpetrate sexual misconduct, consistent characteristics emerge from studies that have been conducted with mental and physical health professionals. Male professionals are overrepresented in cases of sexual misconduct compared to female professionals, as are middle-aged professionals in solo or private practice. Sexual misconduct occurs mostly in professional relationships involving male-female dyads, but it is also reported in female-female and male-male dyads (AbuDagga et al., 2019; Akamatsu, 1988; Alam et al., 2011; Brooks et al., 2012; Budden et al., 2013; Campbell et al., 2005; Chiarella & Adrian, 2014; Eichenberg et al., 2010; Gartrell et al., 1992; Lamb et al., 1994, 2003; Lamb & Catanzaro, 1998; Leggett, 1994; Parsons & Wincze, 1995; Pope et al., 1979; Searle et al., 2017; Tullett et al., 2003; Wilbers et al., 1992; Wincze et al., 1996). Nevertheless, the characteristics of professionals and the factors that increase their vulnerability to sexual misconduct (Seto, 1995) remain unknown. This knowledge is however essential to guide practice, research, and public policy efforts oriented toward the prevention and management of sexual misconduct.
Victims
The overwhelming majority of victims of sexual misconduct are adult females who tend to be younger than the professionals (Bouhoutsos et al., 1983; Eichenberg et al., 2010; Gartrell et al., 1986; Lamb et al., 2003; Somer & Saadon, 1999). Factors that have been identified as increasing the risk of sexual victimization in a professional relationship are: female gender, a history of childhood sexual victimization or trauma, poor self-esteem, the presence of psychiatric symptoms (e.g., depression, dissociative disorder, borderline traits, suicidality) and previous sexual involvement with a professional (AbuDagga et al., 2019; Ben-Ari & Somer, 2004; Bergeron, et al., 2012; Celenza, 2007; Celenza & Gabbard, 2003; Eichenberg et al., 2010; Feldman-Summers & Jones, 1984; Kluft, 1989; Pope & Bouhoutsos, 1986; Pope & Vetter, 1991; Searle et al., 2017). These factors mostly concern clients of mental health professionals.
The Consequences of Sexual Misconduct
Victims
Studies conducted with victims of sexual misconduct point to consequences that are similar to those associated with sexual aggression. The short-term consequences of sexual misconduct include: a feeling of being attractive, special and/or loved, pleasure/displeasure, confusion, ambivalence, discomfort, emotional lability, agitation, guilt, shame, fear, anger, isolation, a sense of betrayal, and dissociation (Berkman et al., 2000; Disch & Avery, 2001; Somer & Saadon, 1999; Valiquette, 2007). With time, victims experience a marked decline in their overall well-being, which is associated with feelings of exploitation and distrust (self and others), concentration/memory/sleep disruptions, intimacy and sexual difficulties, rage, anxiety, depression, substance misuse, posttraumatic stress disorder, suicidal ideation, and hospitalizations (Armstrong et al., 2000; Halter et al., 2007; Luepker, 1999; Seto, 1995; Wohlberg et al., 1999). Victims who become mistrustful of professionals can refrain from getting the help they need, which can exacerbate the deterioration of their health. Few report the sexual misconduct to professional licensing and regulating bodies. Fear, lack of courage, feelings of complicity, the impression that evidence for the case is weak, and the statute of limitations are stated as obstacles to reporting (Eichenberg et al., 2010). Victims who have come forward state as main motivators for action: (1) public information about sexual misconduct; (2) the desire to prevent further sexual violence; and (3) encouragements from current professionals.
Professionals
The exposure of sexual misconduct can provoke great instability and stress among professionals who must confront their partner, family, friends, and clients, undergo an investigation, and/or prepare a defense for the disciplinary hearings. This state may increase some professionals’ emotional vulnerability, sense of isolation, or use of maladaptive coping strategies, thus undermining their capacity to adequately navigate the dynamics and boundaries of the professional relationship. Professionals found guilty of sexual misconduct can also experience pressure upon the imposition of sanctions and during practice re-entry, as they face suspicion, scrutiny and sometimes rejection on the part of colleagues, clients, and the public. Without proper support in the management of this process, professionals may fall back onto patterns that increase their risk of sexual recidivism.
Professions
Sexual misconduct is damaging for professions. In addition to tarnishing their reputation, it provokes distrust in the population who may not enlist the help of professionals when it is needed (Barnett et al., 2007; McNulty et al., 2013). As for members, they are often swallowed up in the public judgement of the alleged offender without being given a voice to defend their integrity.
The last 20 years have seen important advances in the field of sexual aggression. Researchers, practitioners, and public policy makers have worked together to establish best practices, develop science-based interventions, determine treatment efficiency, increase awareness of sexual violence, facilitate disclosure, and improve sex offender assessment, treatment, and management. This has not been the case for sexual misconduct which, as the empirical literature indicates, is a common phenomenon. Urgently needed in the prevention of sexual misconduct, is a better understanding of the extent of the phenomenon, the characteristics of professionals, victims and their relationship, and the handling of sexual misconduct by the professional system. In acquiring a representative understanding of the phenomenon, it appears crucial to draw together information from various professional systems.
The Current Study
Based on an analysis of all documented cases of sexual misconduct in the province of Quebec, between 1998 and 2020, the study aimed to explore the general characteristics of professionals, victims, and acts of sexual misconduct, as well as the processing delay and outcome of cases reviewed by Disciplinary councils. It expands current understanding of sexual misconduct as it is rooted in Quebec law, which applies to both health and non-health professions.
Method
The cases of sexual misconduct included in the present study are assumed to represent the population of interest (i.e., the population of cases). The 20-year interval of the study takes into consideration the various sociopolitical stances on sexual violence, the feminization or masculinization of certain professions, as well as the growing emphasis placed on research and intervention in relation to victims and perpetrators of sexual violence. An exploratory approach was adopted to examine the collected data given that a priori hypotheses were not derived from the literature review. This decision is supported by the difficulty to compare published studies examining reports of sexual misconduct to professional licensing and regulating bodies, as they are based on varying definitions of sexual misconduct, systems of professional law, deontological norms, and disciplinary processes. Nonetheless, some exploratory analyses were conducted based on the general trends emerging from the available literature on sexual misconduct and the standard analyses performed in the domain of sexual aggression. While this approach has limitations and may not entirely capture the complexities of the phenomenon, it provides useful insights that can inform future studies on sexual misconduct.
Materials
Reported cases of sexual misconduct in Quebec are typically treated by disciplinary tribunals, but legal reparation can also be obtained in civil court and criminal court. In Canada, Professional law falls under provincial jurisdiction (Azer, 2013). The province of Quebec holds 46 professional licensing and regulating bodies (called “orders”) encompassing 55 professions, that manage the disciplinary process (Normandin, 2015). Disciplinary councils must determine whether professionals’ actions are in respect of the Quebec Professional Code, the framework law of the province’s professional system. In Quebec, the law regulating sexual misconduct applies to any professional relationship involving a professional who is part of an order.
There is no limitation period for sexual misconduct disciplinary proceedings in Quebec (Leroux, 2007). Requests that are deemed receivable lead to the opening of an inquiry by the Syndic, an independent employee appointed by the professional order’s Board of directors. When information obtained as part of the inquiry process substantiates the allegations of sexual misconduct, the Syndic typically files a complaint with the Disciplinary council. Two Disciplinary hearings are held to determine the verdict – in the case of professionals who plead not guilty to at least one charge of sexual misconduct (with the burden of proof resting on the complainant; Azer, 2013) – and sanctions. The role of Disciplinary councils is to protect the public rather than to restrict the general liberties of professionals, but they are led in the application of Professional law to impose punitive sanctions. Professionals can appeal these decisions before the Professions Tribunal, which has the power to alter or quash any decision it evaluates (art. 175) if it determines that an error was committed in the first instance judgement.
Since June 2017, Bill 11 imposes minimum sanctions on professionals found guilty of sexual misconduct: (a) removal from the membership register for a minimum of 5 years (unless professionals convince the Disciplinary council that a shorter sanction is warranted given the circumstances); and (b) a fine ranging between $2,500 and $62,500 for each offence. Before the entry of Bill 11, minimum fines ranged between $1,000 and $12,500 and no period of time was specified for membership revocation (Azer & Rioux-Risi, 2019; Normandin, 2019). Additional sanctions can also be imposed: (a) a reprimand; (b) the revocation of the specialist certification; (c) the restriction or suspension of the right to engage in professional activities; (d) the successful completion of a refresher course and/or training prior to practice reintegration; and/or (e) the involvement in psychotherapy (art. 156, 160). Furthermore, the Disciplinary council rules on the publication of a notice of the decision in a local newspaper where the professional holds, has held or could hold his/her professional practice (art. 156), and the payment of the costs of the proceedings by the professional, the complainant, or both.
Procedure
A search was conducted in January 2021 on the websites of the Canadian Legal Information Institute (CanLII, https://www.canlii.org/en/) and the Société Québécoise d’information juridique (SOQUIJ, https://soquij.qc.ca/a/fr/english/), to identify published decisions involving sexual misconduct from Disciplinary councils and the Professions Tribunal, between January 1st 1998 and December 31st 2020. The year 1998 was chosen as it marks an era of growing social intolerance toward sexual aggression that set the stage for current laws and policies concerning sexual violence and takes into account the period of adaptation that followed the inclusion of article 59.1 in the Quebec Professional Code. The search terms comprised “59.1” and “59.2” (the two articles of the code that refer to sexual misconduct), “sexual misconduct”, “sex*”, and “misconduct”. The search yielded 1525 decisions. The search process was repeated individually for each of the 46 professional orders, to ensure that all decisions pertaining to sexual misconduct were identified (no cases were excluded). Decisions were examined to eliminate cases that concerned exclusively article 59.1.1, which targets derogatory acts of a non-sexual nature (e.g., corruption, embezzlement), and cannot be eliminated as a research criterion. In total, 296 decisions involving articles 59.1 or 59.2 were retained.
Two raters read each decision in its entirety and extracted targeted information from the case. The first rater entered this information in an SPSS database, which was then reviewed by the second rater. The rate of agreement in coding was 98.31%. In the case of disagreements regarding the interpretation of case information or the calculation of dates, the two raters came to an agreement or contacted the Syndic of the professional order associated with the decision to obtain clarifications. Information collected from cases included: (a) the age and gender of professionals and victims; (b) the number of years of practice accumulated by the professional (since the initial issuing of the practice license by the professional order, taking into account periods of non-registration); (c) any mention of prior sexual boundary violation that did not lead to a complaint (e.g., witnesses testifying that they were also subjected to acts of sexual misconduct by the professional that occurred before those reported by the victim in the official complaint); (d) any mention of prior acts of nonsexual professional misconduct that led or not to a complaint (as per defined in the Quebec Professional Code); (e) whether reported acts constitute sexual recidivism – that is, acts of sexual misconduct that are distinct from those included in a previously published decision; (f) the characteristics of reported acts of sexual misconduct; (g) the verdict, sanctions, and appeals; and (h) the time elapsed between the date of the inquiry request and the date of the final decision concerning the outcome of the disciplinary process. While disciplinary decisions typically include basic case information, the richness of available information varies due to the absence of a standardized publication model. For the 16 decisions that lacked basic information, Syndics were contacted as part of access to information requests and supplied this information.
The specific age of victims is not systematically mentioned in decisions, but available information allows for the categorization of victims as children, adolescents, or adults. This categorization was used in the present study. For the purpose of analyses, acts of sexual misconduct were classified on a continuum according to their degree of genitalization (ranging from “trying to obtain sexual information from a client/mingling in a client’s personal life” to “engaging in sexual intercourse”) and those representing the highest degree of genitalization were retained.
Analyses
Standard descriptive analyses (frequencies) were conducted to establish the characteristics of professionals, victims, and acts of sexual misconduct, as well as the delay and outcome of the disciplinary process. Correlational analyses were used to examine the relationship between those characteristics. Based on the available scientific literature highlighting differences among subgroups of professionals accused of sexual misconduct (e.g., male vs. female, younger vs. older, etc.), chi-square tests and t-tests were performed.
Results
Characteristics of Professionals
The 296 decisions concerned 22 professional orders. All decisions referred to professionals as either male or female. Decisions concerned a majority of male (83.80%) compared to female (16.20%) professionals. The age of professionals was not systematically documented in decisions but available information for 100 professionals accused of a first-time sexual offense shows that they initiated the reported acts of sexual misconduct on average at 48.45 years of age (SD = 12.77, Mdn = 47.0). The comparison of age between male (n = 92) and female (n = 8) professionals highlighted a significant difference, with males being older (M = 49.50 years, SD = 12.64) than females (M = 36.75 years, SD = 8.94), t (9.62) = 3.72, p = .002, d = 12.41, 95% CI [.28, 1.76]).
Complaints of sexual misconduct were filed against professionals ranging from the newly entered (first year of practice) (6.54%) to the senior practitioner (≥40 years of practice) (3.07%). The mean number of years of practice of professionals targeted by such complaints was 16.66 years (SD = 11.16, Mdn = 15.50). Female professionals involved in cases of sexual misconduct accumulated on average 9.81 years of practice (SD = 8.16, n = 43) compared to 18.01 years (SD = 11.20, n = 217) for their male counterparts. This difference was significant, t (258) = 4.57, p < .001, d = 10.76, 95% CI [.43, 1.10]).
Gender and Number of Years of Practice of Professionals Involved in Cases of Sexual Misconduct.
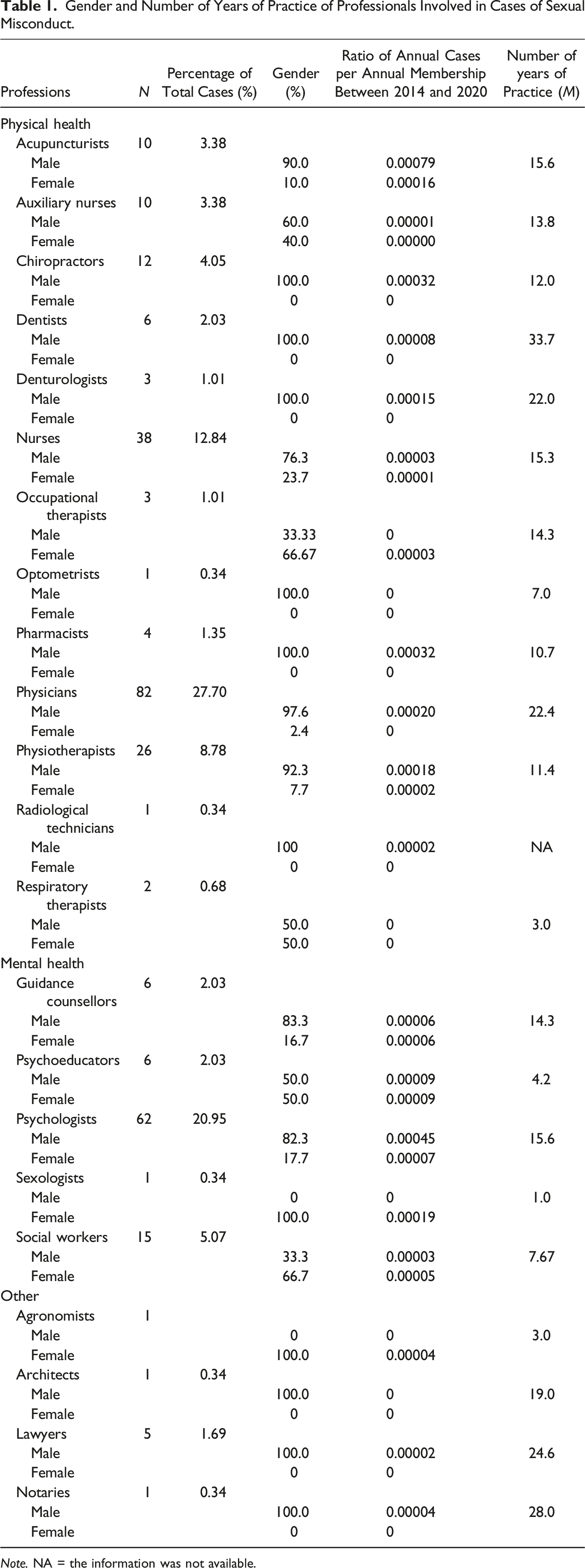
Note. NA = the information was not available.
Characteristics of Victims
Decisions involved 470 victims. For the purpose of analyses, the few decisions that concerned exclusively child victims (n = 5) were grouped with those involving adolescents (the combined group is referred to as “minors”). While a small percentage of cases involved minors (female = 8.03%; male = 4.82%), adult females were overrepresented (74.30%) among victims, followed by male adults (12.85%). Few cases involved both male and female victims (1.36%), or minor and adult victims (2.04%). Three quarters of decisions (75.51%) included a single victim. Most victims were clients. In rare cases they were professional colleagues (2.36%) or individuals gravitating within the client’s intimate circle (e.g., mother, boyfriend) (1.01%).
Characteristics of the Professional Relationship
Cases of sexual misconduct involved for the most part a male professional and a female victim (78.20%) or a female professional and a male victim (15.22%), compared to male-male (5.54%) and female-female (1.04%) dyads. Significant differences between groups were found, with female victims being overrepresented among male professionals and male victims among female professionals, X2 (1, 289) = 282.20, p < .001, φ = .79. Acts of sexual misconduct reportedly occurred primarily in the work setting (76.67%), during consultations with clients. The first (and sometimes only) manifestation of sexual misconduct occurred at various moments in the professional relationship: 12.20% = as part of a unique consultation; 30.66% = a few consultations over less than six months; 9.05% = consultations over six to 12 months; 16.38% = consultations over one to 2 years; and 22.30% = consultations over more than 2 years.
Characteristics of Acts of Sexual Misconduct
Degree of Genitalization of Reported Acts of Sexual Misconduct According to Profession and Gender.
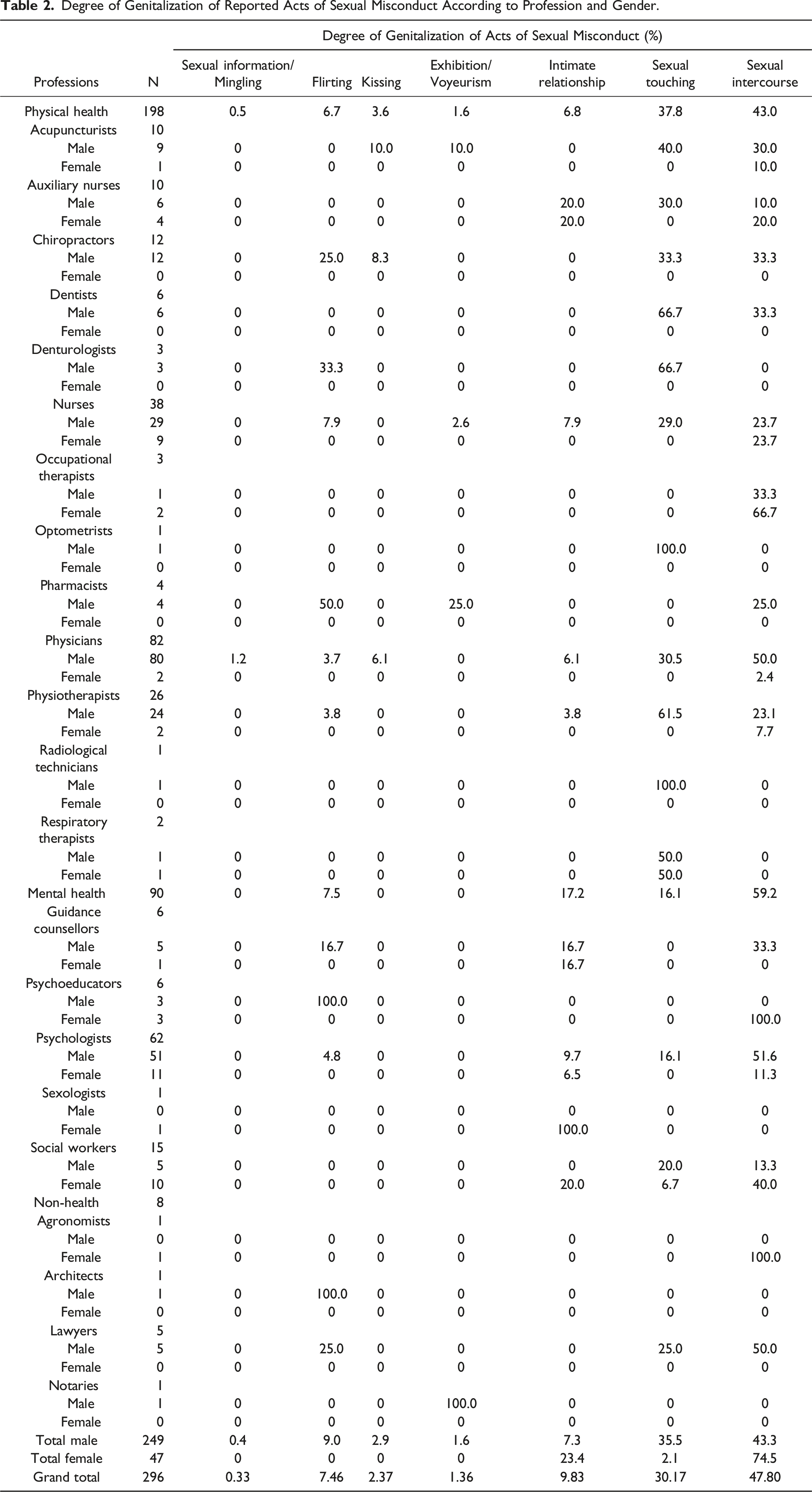
Small but significant correlations were found between the gender of professionals and the number of victims included in cases (r = −.14, p = .015, n = 294, 95% CI [−.25, −.02]) as well as between the type of profession and the number of victims (r = .14, p = .019, n = 286, 95% CI [.02, .25]). Results from t-tests signal that male professionals were associated with a higher number of victims (M = 1.70, SD = 1.80) than female professionals (M = 1.06, SD = 0.32, t (292) = 2.45, p = .007, d = 1.66, 95% CI [.08, .70])), as were physical (M = 1.78, SD = 1.98) compared to mental health professionals (M = 1.28, SD = 0.70, t (284) = −2.35, p = .010, d = 1.68, 95% CI [−.55, −.05])). Cases of sexual misconduct against a minor concerned 12.60% of male professionals and 4.17% of female professionals, as well as 9.85% of physical health professionals and 12.90% of mental health professionals.
Prior sexual boundary violations were documented in 12.10% of decisions, all of which involved male professionals. In addition, prior non-sexual professional misconduct was reported for 7.95% of professionals, 94.74% of whom were males. Results of a correlational analysis indicate that prior sexual boundary violations and non-sexual professional misconduct are positively associated, rs (259) = .20, p = .001, 95% CI [.08, .32]. In addition, a small but significant correlation was found between prior sexual boundary violations and the number of victims included in cases, r = .15, p = .015, n = 271, 95% CI [−.26, −.03]. Professionals with a history of sexual boundary violations were associated with cases involving on average 2.16 victims (SD = 2.04), compared to 1.51 (SD = 1.62) for professionals without such a history. T-test results show that this difference was significant, t (269) = 2.44, p = .024, d = 1.71, 95% CI [.07, .69]).
Eight percent (8.11%) of decisions concerned professionals accused of sexual recidivism. Male professionals (94.74%) were overrepresented in those decisions compared to female professionals (5.26%). Results of correlational analyses show that sexual recidivism is significantly associated with prior sexual boundary violations, rs (272) = .47, p < .001, 95% CI [.06, .30]) and non-sexual professional misconduct, rs (260) = .19, p = .002, 95% CI [−.31, −.06].
Outcome of the Disciplinary Process
Final Outcome of Cases of Sexual Misconduct Between 1998 and 2020.
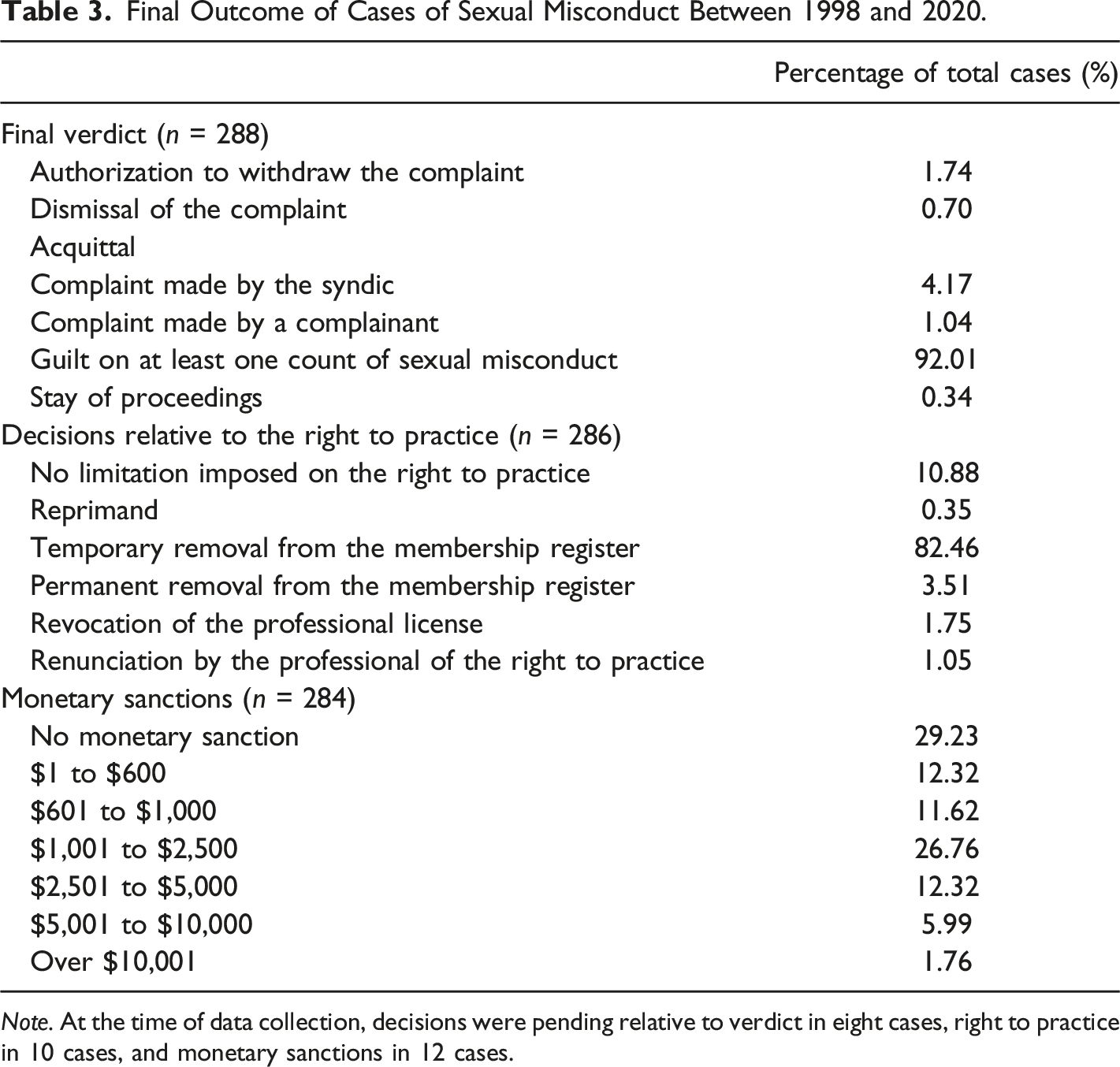
Note. At the time of data collection, decisions were pending relative to verdict in eight cases, right to practice in 10 cases, and monetary sanctions in 12 cases.
The majority (85.96%) of professionals found guilty of sexual misconduct was removed from the membership register either temporarily (for a period extending between one and 3650 days, Mdn = 183.0 days) or permanently. Similar percentages of male (81.25%) and female (88.89%) professionals and physical (83.33%) and mental health (82.42%) professionals saw their right to practice temporarily suspended. Results from t-tests reveal that the period of temporary removal from the membership register was significantly longer for professionals with prior sexual boundary violations (M = 772.97 days, SD = 857.49, Mdn = 730.0 days) and those found guilty of sexual recidivism (M = 979.0 days, SD = 1048.96, Mdn = 578.0 days), compared to professionals with no such prior violations (M = 517.32 days, SD = 693.60, Mdn = 153.0 days, t (44.45) = 1.72, p = .046, d = 719.50, 95% CI [.01, .71]) or who were found guilty of a first-time sexual offense (M = 538.36 days, SD = 700.11, Mdn = 183.0 days, t (267) = −2.36, p = .009, d = 724.18, 95% CI [-1.12, −.10]).
In addition, 70.77% of professionals found guilty of sexual misconduct were ordered to pay a fine, ranging between $600.00 and $35,000.00 (Mdn = $1,200.00). In rare cases, Disciplinary councils instructed that the funds collected from the payment of fines be used to cover the cost of the victim’s therapy. Male professionals received harsher monetary sanctions (M = $2,184.87, SD = 3309.99, Mdn = $1,000.00) compared to female professionals (M = $1,068.89, SD = 1027.98, Mdn = $1,000.00, t (281) = 2.24, p = .013, d = 3066.92, 95% CI [.04, .68]). Moreover, professionals with prior sexual boundary violations were given higher monetary sanctions (M = $3,095.74, SD = 5360.32, Mdn = $2,000.00) than professionals with no such prior history: (M = $1,762.67, SD = 2349.50, Mdn = $1,000.00, t (262) = 2.68, p = .004, d = 3097.69, 95% CI [.11, .75]). Monetary sanctions were not found to vary significantly between professionals found guilty of sexual recidivism (M = $2,389.47, SD = 1918.01, Mdn = $2,000.00) compared to those found guilty of a first sexual offense (M = $1,979.92, SD = 3156.88, Mdn = $1,000.00, t (25.64) = −.85, p = .20, d = 719.50, 95% CI [.01, −.71]). Most professionals were required to disburse the fees of the proceedings (full fees = 80.99%; partial fees = 9.51%) and the publication of the Disciplinary council’s decision (full fees = 80.63%; partial fees = 1.76%).
Non-monetary sanctions were imposed in 23.16% of cases of sexual misconduct. The most common (10.18%) rehabilitative measure imposed by Disciplinary councils was the requirement that professionals’ practice be supervised for some period of time. It was followed by the limitation on the right to practice with designated clienteles (7.72%), the successful completion of deontological training prior to practice re-entry (3.51%), and the involvement in psychotherapy (0.35%). Significant differences were found relative to non-monetary sanctions for the gender of professionals, X2 (1, 285) = 4.80, p = .028, φ = .13, and the type of profession, X2 (1, 277) = 37.65, p < .001, φ = −.37). Indeed, more female (24.44%) and mental health (32.97%) professionals faced non-monetary sanctions, compared to male (12.08%) and physical health professionals (5.38%). The imposition of such sanctions did not seem to increase in the presence of prior sexual boundary violations (10.42% vs. no such prior history = 15.14%), non-sexual professional misconduct (8.70% vs. no non-sexual professional misconduct = 15.15%) or sexual recidivism (10.53% vs. first sexual offense = 14.29%).
The severity of sanctions imposed on professionals found guilty of sexual misconduct before (n = 192) and after (n = 98) the coming into force of Bill 11, was examined. Results from t-tests show that the introduction of Bill 11 led to more severe sanctions, with professionals being removed from the membership register for a longer period (M = 1089.17 days, SD = 812.37, Mdn = 1095.00 vs. before Bill 11: M = 318.03 days, SD = 534.83, Mdn = 120.00, t (267) = −9.27, p < .001, d = 636.47, 95% CI [−1.49, −.94]), and receiving harsher monetary sanctions (M = $3,335.16, SD = 4558.91, Mdn = $2,500.00 vs. before Bill 11: M = $1,378.13, SD = 1747.44, Mdn = $1,000.00, t (281) = −5.20, p < .001, d = 2955.03, 95% CI [−.92, −.41]). Imposed sanctions did not vary according to the gender of professionals, the type of profession, a history of prior sexual boundary violations, or sexual recidivism. However, nearly one in every three professionals did not face monetary sanctions either before (29.69%) or after (28.26%) the implementation of Bill 11. The imposition of rehabilitative measures did not differ before and after Bill 11.
Two thirds (67.98%) of professionals found guilty of sexual misconduct eventually returned to practice once they were eligible for readmission on the register. This includes half of the professionals found guilty of sexual recidivism. Those who did not return to practice went into early retirement or redefined their career to offer services that are not regulated by a professional order (e.g., transitioning from psychologist to life coach; chiropractor to massage therapist; guidance counselor to pedagogical advisor).
In addition to the disciplinary process, 10.58% of professionals underwent criminal prosecution related to sexual misconduct. Chi-square tests suggest that cases that were criminally tried more often involved male professionals (96.77%), X2 (1, 293) = 4.38, p = .036, φ = .12, victims who were minors (60.0% vs. 5.74% of non-criminally tried cases), X2 (1, 291) = 78.77, p < .001, φ = −.52, and led to the suspension of the professional license during the disciplinary proceedings (32.26% vs. 9.92%), X2 (1, 293) = 12.83, p < .001, φ = −.21.
Processing Delays of the Complaint
The date of reporting of sexual misconduct was not systematically documented in decisions. As this information was missing for 154 decisions, the delay between the initial reporting and the filing of the complaint by the Syndic could not be calculated. The complaint was amended in 21.28% of cases, following an average delay of 330.02 days SD = 267.01, Mdn = 274.00). Additional delays were provoked by professionals (9.56%), other individuals (e.g., lawyers, witnesses, 11.26%), and obstruction of the Syndic’s work (6.10%).
The delay of treatment of complaints of sexual misconduct – that is the delay between the filling of the complaint by the Syndic and the final decision on sanctions – was on average 638.33 days (SD = 528.84, n = 279, Mdn = 458.00). The delay did not significantly vary according to the gender of the professional, the type of profession, a prior history of sexual boundary violation, and the perpetration of sexual recidivism. As for the initial verdict, it fell on average 521.15 days (SD = 451.37, Mdn = 393.50) after the filing of the complaint. The introduction of Bill 11 is associated with longer processing delays. Indeed, the delay between the filing of the complaint by the Syndic and the final decision on sanctions went from 500.60 days (SD = 457.08, Mdn = 355.00) to 704.65 days (SD = 641.91, Mdn = 523.00, t (278) = −3.06, p = .001, d = 524.80, 95% CI [-.64, −.14]).
One in every ten (10.34%) cases was appealed. Professionals contested the verdict in 37.14% of appeals and sanctions in 62.86% of appeals. The delay between the initial verdict and the final decision on sanctions was eight times greater for cases that were appealed (M = 547.07 days, SD = 441.61, Mdn = 466.00) compared to cases that were not appealed (M = 67.35 days, SD = 172.58, Mdn = 0. Significant differences were found relative to the delay of treatment between appealed and non-appealed cases, t (283) = −11.50, p < .001, d = 216.18, 95% CI [−.2.64, −1.80]). All but one initial verdicts were upheld on appeal (that single verdict changed from guilty to acquitted). Decisions on sanctions were not found to differ between cases that were or not appealed.
Discussion
Despite the growing awareness of sexual violence as a social problem, its manifestation within the context of professional relationships has been the object of less scrutiny. The present study, which aimed to describe the characteristics of cases of sexual misconduct over the last 20 years, in the province of Quebec, shows that it is prevalent in various professions. Most (92.01%) complaints were substantiated and lead to a guilty verdict. These cases likely represent the tip of the iceberg as available data suggest that only a small proportion of acts of sexual misconduct are reported to professional licensing and regulating bodies, all of which do not lead to a complaint that is heard by disciplinary tribunals.
Characteristics of Professionals
Professionals involved in cases of sexual misconduct were mostly males approaching mid-career (see United States Office of Personnel Management, 2006) who perpetrated non-contact sexual offenses and sexual touching within their work setting. Male professionals were associated with a higher number of victims of sexual misconduct and antecedents of professional boundary violations. This echoes findings from previous studies on sexual misconduct. However, one in every six cases (16.22%) of sexual misconduct concerned female professionals. The latter accumulated fewer years of professional experience and were more inclined to establish intimate or sexual relationships with their clients than their male counterparts. These findings bring to light sexual misconduct perpetrated by women, which remains poorly documented. They also show that sexual misconduct can be perpetrated by young professionals who have had fewer opportunities to transgress sexual boundaries in their relationship with clients than their colleagues who have accumulated more years of practice.
Physical and mental health professionals were overrepresented in cases of sexual misconduct, with physical health professionals accounting for more non-contact sexual offenses and sexual touching, and mental health professionals for more sexual intercourse with clients. This overrepresentation suggests that professional relationships that involve greater proximity to clients (e.g., physical examination, self-disclosure on the part of clients) may present a higher risk of sexual boundary violations. Also, the media represent sexual misconduct as typically occurring in these professions, which may increase clients’ sensitivity to the issue and propensity to report such acts. While less prevalent, sexual misconduct was also found to occur in non-health professions.
Characteristics of Victims
Consistent with previous findings, sexual misconduct occurred mostly toward female victims, within male-female professional relationships. Adult males nevertheless represented one in every eight victims of sexual misconduct. Children and adolescents, who account for a large proportion of victims of sexual aggression, were underrepresented in cases of sexual misconduct. This is not surprising as professional services require parental consent up to age 14 in Quebec and are often provided under the supervision of a parent. A minority of cases involved professional colleagues or relatives of clients. The prevalence of such cases is likely higher as professionals may, for various reasons, hesitate to report their colleagues (e.g., they may not wish to experience negative consequences associated with reporting in their workplace or to tarnish their colleague’s reputation).
Characteristics of the Professional Relationship
Sexual misconduct occurred within short-term (less than 6 months = 42.86%) as well as longer lasting (6 months or more = 47.76%) professional relationships. Hence, the establishment of a solid alliance may not be a necessary condition for the occurrence of sexual misconduct. This also raises the possibility that professionals found guilty of sexual misconduct in long-lasting relationships with clients consistently failed to put in place the necessary mechanisms to prevent sexual boundary violation or even that some victims were groomed over time.
Characteristics of Acts of Sexual Misconduct
Over 75.0% of all cases involved sexual intercourse or sexual touching, which suggests that acts of sexual misconduct that are reported to professional orders present characteristics that are deemed more serious or unequivocal by individuals who request an inquiry. The true prevalence of sexual misconduct likely concerns a larger proportion of professional orders’ membership than the results put forth in the present study that are based on legal decisions.
Outcome of the Disciplinary Process
Punitive sanctions have been the norm over the last 20 years, as rehabilitative measures were imposed for only one fifth of professionals found guilty of sexual misconduct who reintegrated their practice (67.98%). However, this approach does not necessarily lead to greater awareness on the part of professionals of the ethical shortcomings of their actions, the consequences for victims, the factors that increase their vulnerability to sexual boundary violation, or the actions that should be taken to prevent future sexual misconduct and to monitor their own actions.
Especially preoccupying is the finding that 18.38% of professionals had a history of sexual boundary violations. They were involved in decisions including a greater number of victims and were likelier to present prior non-sexual professional misconduct, indicating a general difficulty in maintaining proper professional limits or, in some cases, a tendency to knowingly transgress limits. While they faced harsher sanctions, most of these professionals did not need to conform to risk prevention measures during and after practice re-entry. Results show that prior sexual boundary violations are associated with an increased risk of sexual recidivism. This should alert Disciplinary councils to the need to impose risk prevention measures.
After the entry into force of Bill 11, harsher sanctions were imposed on professionals found guilty of sexual misconduct. Membership was revoked for a longer period (Mdn = 1095 days vs. 120 days before Bill 11) and monetary sanctions increased from a median of $1,000.00 to $2,500.00. Interestingly, the proportion of professionals who were not given monetary sanctions did not differ after Bill 11 came into effect. Due to the limited number of cases in some professions, sanctions could not be compared between professions. A previous study by Searle et al. (2017) signaling the imposition of harsher sanctions for nurses compared to physicians however highlights the importance of pursuing this line of inquiry.
Processing Delays of the Complaint
The conclusion of the disciplinary process occurred on average 21 months after the filling of a complaint for sexual misconduct. Added to this delay is the period of time between the request for an inquiry and the filling of the complaint – which could not be calculated in the present study due to missing information. Further delays attributable to the various actors involved in the disciplinary process (e.g., obstruction of the Syndic’s work by the professional, scheduling issues on the part of lawyers) or the appeal of decisions, were sometimes encountered. A minority of decisions were appealed (10.34%), mostly to contest monetary sanctions. Cases that were appealed took longer (average = 35 months) to process. Importantly, the processing delay of cases of sexual misconduct increased after Bill 11 came into effect, from 500 days to nearly 2 years (705 days).
Study Implications and Recommendations
Practicing Professionals
Professionals must be aware that sexual aggression occurs in the context of professional relationships, and able to recognize signs of sexual boundary violations in clients’ previous professionals’ relationships, address this issue with clients, inform clients of their legal recourses, and support clients in their initiative to report sexual misconduct. Professionals can also contribute to the establishment of a work environment in which sexual boundary violations are not tolerated. In their own practice, they must be aware of power dynamics in their relationship with clients, sensitive to sexual boundary violations outside of the workplace, vigilant in maintaining professional boundaries, and unhesitant to obtain help if they are unsure or feel ill-equipped to manage sexual boundaries. As for relationships with colleagues, professionals should point out sexual remarks and behaviors that transgress boundaries. They must also be acquainted with the mechanisms for reporting sexual misconduct in their workplace and, if no action is taken, the procedure to follow to request an inquiry by professional licensing and regulating bodies. Cases in which professionals fall victim to their clients are poorly documented but do occur. Professionals must be cognizant of this phenomenon and their available recourses.
Policy Makers
Findings from the present study suggest that the public may not be aware that certain types of sexual boundary violations (e.g., non-contact sexual offenses) constitute sexual misconduct or that sexual intimacy with clients is prohibited in some professions. Policy makers are important contributors in the prevention of sexual violence. Concerning sexual misconduct, they must ensure that clear and comprehensible information is available for the public about the prohibition of sexual intimacy within professional relationships and the steps to take to report it. Efforts should be directed at promoting initial disclosure (for example, by adopting mandatory reporting laws, see Ontario’s Regulated Health Professions Act, 1991), ensuring that the proper mechanisms are in place to receive and effectively treat complaints of sexual misconduct, and providing safe working environments. Policy makers can also raise victims’ awareness of their rights and facilitate their access to resources dedicated to victims of sexual aggression. As concerns professionals found guilty of sexual misconduct, policy makers should see to the systematic implementation of rehabilitative measures in an attempt to minimize the risk of sexual recidivism. Effective policies are vital in promoting public trust in the professional system and in encouraging individuals to reach out to professionals when they need help.
Researchers
Future studies should document the extent of sexual misconduct and identify etiological factors, risk and protective factors, offender and victim profiles, and the characteristics of sexual misconduct that are similar to and distinct from sexual aggression. In increasing current understanding of the characteristics of female professionals who perpetrate sexual misconduct and of male victims of sexual misconduct, research can contribute to breaking the taboo that often surrounds these phenomena. Moreover, findings from the present study highlight the importance of targeting all professions as part of prevention efforts and of adapting the message to the reality of each profession. Additional research on sexual misconduct is needed and could provide a foundation for these efforts.
Professional Licensing and Regulating Bodies
While they are expected to always uphold their fiduciary duty to the clients, most professionals do not receive proper training on maintaining sexual boundaries in the professional relationship. At some point or another in their career, it is highly probable that professionals will feel greater connection or romantic or sexual attraction to at least one client, but many are ill-prepared to tackle this naturally occurring phenomenon (Barnett, 2014; Pope et al., 1987; 1993; 2006). Clear deontological guidelines should be made available to help professionals uphold the norms of practice while negotiating the limits of the professional relationship. Professional ethical and deontological codes and standards of practice should clearly define: (a) sexual intimacy, sexual remarks and contact, romantic relationships, and sexual relationships that are to be avoided with clients; (b) the characteristics that distinguish the professional relationship from friendship, romantic and sexual relationships; (c) what constitutes “appropriate” sexual boundaries; (d) individuals with whom proper sexual boundaries must be upheld (e.g., clients and their relatives and close ones, former sexual partners, colleagues, etc.); (e) the end of the professional relationship; and (f) sexual misconduct. This would also help the public in deciphering appropriate and inappropriate professional conduct. In the case of professionals found guilty of sexual misconduct, Disciplinary councils should ensure that they (a) receive thorough training on professional boundaries prior to practice re-entry; (b) implement measures to respect the imposed limitations on practice, prevent sexual misconduct, and obtain support; (c) participate in regular supervision during practice re-entry by a professional who is well-trained on issues related to sexual misconduct; and (d) receive ongoing professional training.
Professional licensing and regulating bodies can require that sexual misconduct be included as part of initial training in deontology. Teachings should provide students with the opportunity to reflect on the consequences of sexual misconduct (for victims, the profession, and themselves), to identify the factors that increase their vulnerability to transgress sexual boundaries, and to navigate situations in which they must effectively manage their own or the client’s sexual attraction, sexual boundary issues, and transference-countertransference if applicable. Existing resources to help professionals manage sexual boundaries in their relationship with clients should also be provided. As practicing professionals, they should benefit from continuing education, up-to-date information on sexual misconduct (empirical and clinical articles, books, online content, discussion forums), and access to peer consultation, practice supervision, and psychotherapy (Barnett, 2014; Berkman et al., 2000; Celenza, 2007; Celenza & Gabbard, 2003; Gottlieb, 1993; Strom-Gottfried, 2003; Valiquette, 2007).
Members of the public intuitively turn to professional licensing and regulating bodies to obtain information on professional practice including sexual misconduct (Azer, 2013). Clear information should thus be available on their Web site, defining sexual misconduct, explaining the steps and duration of the inquiry and disciplinary process, describing the role of all the actors involved in this process, as well as its possible outcome. Websites should also provide quick and easy access to the procedure and form for filing an anonymous inquiry request for sexual misconduct, and current information on all members’ practice location, right to practice, and a summary of disciplinary decisions in layman’s terms.
Study Limitations and Future Directions
Results of the present study must be considered in light of certain limitations. The lack of a systematic procedure for documenting decisions by Disciplinary councils in the province of Quebec is associated with variations in the information included in cases. While great care was given to including only those variables in our analyses that were contained in most decisions, missing variables were inevitable. Choices therefore had to be made to exclude variables that would have added richness to the analyses (e.g., age of the professional, age of the victim, date of the request for an inquiry). In addition, decisions contain little information regarding the general characteristics of professionals who perpetrate sexual misconduct, which could be used to better target prevention efforts and rehabilitative measures.
Considering that analyses included all decisions between the years 1998 and 2020, results may have been affected by atypical cases. For example, a few protracted cases endured over several years due to obstruction of the Syndic’s work, multiple contestations of aspects of the disciplinary process or appeals, which may have slightly skewed the results. Measures that were representative of the sample tendencies (e.g., median) were included when possible. Atypical cases offer a representation of the deployment of resources that are available to actors in the disciplinary process rather than the efficiency of the professional system.
It was not possible in the present study to determine if the introduction of Bill 11 is associated with an increase in reporting of sexual misconduct to professional orders, given the short window between its date of entry (2017) and the end period of the study (2020). The implementation of more punitive sanctions for professionals found guilty of sexual misconduct may motivate reporting as it may be understood as a condemnation of such acts by professional orders. Long-term studies should compare pre and post 2017 reporting of sexual misconduct to professional orders in Quebec. If, as the results of the present study suggest, harsher sanctions are being applied since 2017 and processing delays are longer, Disciplinary councils should be supervised in applying the law more efficiently.
Future studies documenting sexual misconduct reported to professional licensing and regulating bodies and in surveys across countries, are needed to determine the scope of this social problem. Recent social movements (e.g., #MeToo, #TimesUp) have contributed to increasing public awareness of sexual violence, which may be reflected in an increase in reporting. Studies should include all professions and target sexual misconduct against clients and their close ones, as well as students, supervisees, and other professionals, occurring in various settings. Findings from the present study show that most professionals found guilty of sexual misconduct eventually return to practice. The career choices they make, the challenges they face before and upon re-entry into practice, and the strategies they put in place to avoid violating sexual boundaries have not been explored empirically. Better understanding of criminological variables and practice reintegration efforts are essential to increasing the effectiveness of rehabilitation and tertiary prevention.
Studies conducted to date that have included victims of sexual misconduct mostly concern mental health professional relationships, which may be associated with dynamics that are not entirely representative of physical health and non-health professions. Further research into the characteristics of victims of sexual misconduct related to all professions is thus necessary, as are efforts to pinpoint the factors that influence or act as obstacles to reporting.
Conclusion
Growing awareness of sexual violence as a critical social problem has led to concrete efforts in improving support for victims of sexual aggression throughout the legal process as well as primary prevention, in the province of Quebec. However, these efforts have not targeted sexual violence that occurs within professional relationships. The present study, which examined the characteristics of cases of sexual misconduct over 20 years in Quebec, shows that it is not a rare phenomenon.
Risk management of professionals found guilty of sexual misconduct is essential and must be adapted to prior sexual boundary violations and/or non-sexual professional misconduct and sexual recidivism. Results of the present study show that most of those professionals eventually return to practice. Professional licensing and regulating bodies should thus see to the imposition and application of rehabilitative measures, the monitoring of practice before and during re-entry, and the supervision by professionals trained on sexual misconduct. Finally, the standardization of information documented in disciplinary decisions involving sexual misconduct – i.e. the characteristics of professionals, victims, acts of sexual misconduct and the disciplinary process – could increase current understanding of the factors that are associated with its etiology and maintenance as well as its consequences for victims. This knowledge could also be used to adapt sexual violence prevention efforts and support provided to victims during the inquiry and disciplinary process.
Footnotes
Acknowledgments
We thank Lydia Valliere for the identification of the legal documentation for the project and Judith Kotiuga for the identification of the empirical literature on sexual misconduct and her contribution in the analysis of disciplinary decisions.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the CERVO Brain Research Centre and Conseil interprofessionel du Québec.
Data Availability Statement
Decisions from which the data for the present study were extracted are publicly available on the CANLII (https://www.canlii.org/en/) and SOQUIJ (![]() ) websites. The datasets associated with the paper are not publicly available but can be made available by the corresponding author upon reasonable request.
) websites. The datasets associated with the paper are not publicly available but can be made available by the corresponding author upon reasonable request.
Ethical Approval
Upon consultation with the Human Research Ethics committee of the Université Laval, no ethical certification was deemed necessary for the present study as it is based entirely on publicly available legal decisions and information.