
Abstract
This article explores nursing, patient records, and ideology within the context of the National Socialist “euthanasia” program (Aktion T4) in Germany and Austria from 1939 to 1941, which targeted individuals with mental and physical disabilities for systematic killing. Using Hannah Arendt's concept of the “banality of evil,” it examines how ordinary individuals, including nurses, became agents of atrocity by adhering to bureaucratic orders. Jacques Ellul's Ethics of Technology framework is employed to analyze how National Socialist ideology manipulated technological processes to enhance efficiency in genocidal goals. Propaganda was crucial in garnering public support, blurring the lines between technology, ethics, and ideology. Archival research at documentation centers and national archives reveals methods for deciding who was killed, the role of family in medical records, and nurses’ involvement in the T4 operation. Three narratives of T4 victims illustrate the personal impacts of these bureaucratic and ideological practices. The article reflects on contemporary nursing, emphasizing the importance of ethical standards and vigilance against data and misuse of technology in health care. This historical examination serves as a reminder of the potential consequences of depersonalization and blind adherence to institutional priorities, underscoring the need for critical engagement with the ethical dimensions of nursing practice.
Keywords
Implications for Knowledge Translation
As the National Socialists came to power, medical records began to focus more on patients from a eugenic perspective; documentation ceased to reflect the patient as an individual, the first step toward depersonalization. Nurses played a key role in T4 operation; skilled at putting people at ease, they ensured that patients remained calm during transportation before being escorted to the gas chambers. By following orders and adhering to what one is told to do, individuals may feel that they are in some way exempt from accountability. The more people are depersonalized, the easier it is to classify them in a category with just a few data points, whether by race, diagnosis, ability to work, or cost to the community. While we may not see a repeat of the T4 program, it is likely that data will continue to be used to achieve ideological goals, sometimes at the expense of patient well-being.
This article unfolds against the historical backdrop of Germany and Austria from 1933 to 1945—a period marked by the pervasive influence of National Socialist ideology. Commonly referred to as the Nazi era, this label has, over time, evolved into a synonym for “evil.” This simplistic association often precludes a nuanced examination of the underlying ideologies. For example, President Vladimir Putin's characterization of his invasion of Ukraine as a campaign to “de-Nazify” Ukraine simplifies complex political dynamics by invoking the specter of Nazism without critically engaging with the ideologies of the groups involved (Dixon et al., 2022).
The focus of this article is on the critical examination of ideology, particularly in an era in which global ideological landscapes are shifting. National Socialist ideology propagated the belief in the inequality of people, deeming some as unworthy of equal treatment. This was a notion deeply rooted in the eugenics movement that was also prominent in the United States and legitimized actions like the mandated sterilization of certain individuals up until 1971 (Reilly, 2015).
By using the term “National Socialist Ideology” instead of “Nazi,” we aim to shift the discussion from a historically evil categorization to an active, relevant ideology that continues to manifest globally. In examining this ideology, the article underscores the potent combination of societal beliefs and technological advancements, and their profound impacts on individuals. It is crucial to acknowledge the human consequences of ideologies, lest the term “Nazi” obfuscate these fundamental truths (Hachtmann, 2022).
This article discusses the “euthanasia program” carried out from 1939 to 1941 under the National Socialist government in Germany and Austria. The program aimed to kill people with mental or physical disabilities to “cleanse” the country of “unproductive” individuals. This program was referred to as Aktion T4 (T4 operation), using the term “euthanasia” (which literally means “good death”) to mask its true intention: killing people without their knowledge or consent.
As the article title alludes to, this inquiry was shaped by Hannah Arendt’s book The Banality of Evil (2006), a collection of articles reporting on the trial of Adolf Eichmann, who played a crucial role in planning and implementing the logistics of the Holocaust, during which millions of people were killed in concentration camps between 1940 and 1945. The evils of the Holocaust need no further elaboration. However, when Arendt was present at the trial held in Jerusalem, she witnessed a rather pathetic person who was full of clichés and had very little insight into the impact on the millions of people killed as a result of his actions.
Arendt illustrated how great evil can be caused by people who perceive they are merely doing what they were asked to do, believing that not actively killing people in gruesome ways exempts them from direct responsibility. By following orders and adhering to what one is told to do, individuals may feel that they are in some way exempt from accountability.
Background
Aktion T4 (T4 Operation)
The T4 operation was run by physicians, nurses, and support staff, forming the basis for the later extermination of mass populations such as Jews, Roma/Sinti, males considered homosexual during that time, and political opponents of the National Socialist government. Between 1939 and 1945, approximately 300,000 individuals, including women, men, and children from psychiatric institutions within the German Reich, were covertly murdered through gassing, medication, or inadequate nutrition (Statista, 2020). Additionally, nearly 100,000 psychiatric patients were killed in occupied or annexed territories (Loose, n.d.). About 100,000 of these murders in Austria and Germany occurred during the so-called T4 operation, a centrally controlled phase (Hohendorf, 2013; Vellguth, 2014). To facilitate this operation, employees of the Führer's (Hitler's) Chancellery and the Reich (Federal) Ministry of the Interior established a secret organization in Berlin at the end of 1939, named T4 after its address at Tiergartenstrasse 4 (Bundesarchiv Internet - Euthanasie Im Dritten Reich, n.d.).
Until August 1941, medical experts in Berlin reviewed patient files sent to them and decided the fate of the sick or disabled. At least 70,000 individuals were gassed in six central facilities at Grafeneck, Brandenburg/Havel, Hartheim, Pirna/Sonnenstein, Bernburg, and Hadamar before the first wave of killings ended on August 24, 1941. Rumors about the program had begun to spread, making it necessary for the responsible persons to carry on their program in secret (Hohendorf, 2013; United States Holocaust Memorial Museum, 2023). In subsequent years the program decentralized, and physicians at individual psychiatric facilities made these life-and-death decisions themselves (Bundesarchiv Internet - Euthanasie Im Dritten Reich, n.d.).
Theoretical Framework
This article offers an analysis of the T4 operation through the framework of the Ethics of Technology, drawing on the insights of Jacques Ellul (1964). Ellul's framework (Ellul, 1964) diverges from conventional views by asserting that the essence of technology lies not in the term itself, but in the concept of Technique. He defines Technique as the processes employed to enhance human efficiency, with efficiency serving as the paramount objective. Ellul states that, contrary to common assumptions, efficiency alone does not inherently equate to ethical “goodness.” Rather, the ethical evaluation of a Technique hinges on the intent driving its pursuit of efficiency.
Central to this analysis is the role of ideology, which shapes the objectives and targets of efficiency-driven Techniques. In the context of the T4 operation, the ideology of National Socialism propelled a ruthless agenda aimed at fortifying the “Aryan” race while purging society of perceived threats. The term Aryan was a pseudoscientific classification used by the National Socialists to classify the group of people they perceived as superior, which included predominantly blond and blue-eyed people of northern European decent. Ellul's exploration of propaganda underscores its function as a Technique utilized to rally public support for ideological imperatives. Indeed, propaganda emerges as a potent tool in the arsenal of ideological agendas, further blurring the lines between technology, ethics, and ideology.
Ethical Considerations and Methodology
This study did not require ethical review due to the historical nature of the data, as the records reviewed were from individuals who had been deceased for over 80 years. In compliance with ethical standards and to protect the privacy of the deceased and their families, all personal identifiers have been removed from the article. This decision was informed by archival research protocols, which emphasize the importance of maintaining the dignity and confidentiality of subjects, even posthumously.
The archival inquiry was conducted at several key historical documentation centers and national archives. Researchers examined patient records from institutions that were involved in the program under study, focusing on the bureaucratic processes and decision-making frameworks used at the time. These records, while lacking in personal detail due to their age, provided critical insights into the systemic operations of the program and the societal ideologies that shaped it.
By using a de-identified approach, the study ensured that the focus remains on understanding the broader historical and ethical implications of data use and institutional practices. This methodological choice reflects a commitment to ethical research practices and acknowledges the lasting impact of historical events on contemporary discussions about ethics in health care and data management.
The analysis is further supported by secondary sources, including historical texts, scholarly articles, and archival documents, allowing for a comprehensive understanding of the period's ethical challenges. This approach not only respects the privacy of those involved but also enriches the discourse on the historical use of data in health-care settings, highlighting the enduring need for ethical vigilance in research practices.
This inquiry started with a visit to the Documentation Center at Schloss Hartheim (Hartheim Castle), examining lists of 18,269 people who were killed at that facility between May 1940 and September 1941 (Neuhauser & Pfaffenwimmer, 1992; Tapfer, 2016). The archivist at the Hartheim Documentation Center recommended the archives of Upper Austria in Linz. These records were from euthanized patients who had been admitted to a large mental health facility in Linz before being sent to Hartheim. These medical records consisted of only a few pages and contained minimal information about the patients and their histories, confirming the insights from the Hartheim archivist that these files were summary files or “shadow files” that merely showed evidence that people had been admitted, yet were otherwise empty of any substantive information.
The archivists at both the Hartheim and the Upper Austria archives referred the researchers to the National Archives in Berlin, which holds 30,000 patient files from the first phase of the so-called “euthanasia” T4 operation, discovered in 1990 in the former National Socialist Archives of the Ministry for State Security of the former German Democratic Republic (East Germany). The remaining 40,000 files from the T4 operation are considered destroyed. These patient files in the national archives are subject to special conditions of use according to the Federal Archives Act. They can be accessed primarily for scientific research and by next of kin to pursue legitimate interests. The Primary Investigator received permission to access and use the files for this study and its publication. It is important to note that in the records, details from the last days of life and dates of death were not recorded in the patient files (Bundesarchiv Internet - Euthanasie Im Dritten Reich, n.d.).
The patient records were reviewed guided by the following three questions:
1. What was the technique used in deciding who was killed? 2. What was the role of family as reflected in medical records for people killed as part of the T4 operation? 3. What was the role of nurses in the T4 operation?
The third question was important, yet could not be answered in the patient records:
To address this third question, literature was used in addition to information obtained at a the conference at Hartheim Commemorative and Documentation Center on May 23 and 24, 2014, focused on the role of nursing in the T4 operation. A systematic approach was adopted using several academic databases: the Cumulative Index to Nursing and Allied Health Literature (CINAHL), Medline, PubMed, and Google Scholar. The search strategy was developed to capture a wide range of relevant literature, utilizing key terms such as “T4,” “euthanasia program,” “National Socialism,” “nursing,” and “Nazi.” These terms were chosen to identify studies and articles that specifically addressed the intersection of nursing practices and the ideological framework of the National Socialist regime. The selection process involved screening titles and abstracts for relevance, followed by a full-text review of eligible articles. Studies were included if they provided insights into the T4 operation, discussed the ethical and ideological dimensions of nursing during this period, or examined the broader implications of National Socialist health-care policies. Articles focusing on unrelated medical or historical aspects without direct relevance to nursing or Aktion T4 were excluded.
Additional sources were offered by the archivists and historians at the Hartheim Castle Information Center and the Federal German Archives in Berlin. Further literature was identified by reviewing the references within the identified articles and books. The references were primarily in the German language, but some were in English.
Three Stories from the Medical Records
To give a clearer picture of the people killed as part of the T4 operation, narratives of three individuals were compiled. When going through the archives, the information was overwhelming, not only due to the sheer number of files but also due to the varying quality of the medical records. Some records had become damp and illegible; others contained only one or two pages or just a letter. To get a clearer picture of the actual stories, the focus was on records that were typed and contained substantive narratives about the patients.
Marianne (Age 2½)
Marianne's story cannot be understood without understanding the life of her mother Anna. Anna's adversities began in her early adolescence. Orphaned by age 13, Anna and her sisters found dwelling in a monastery's children's home. The sisters’ initial state of neglect upon admission reflected their tumultuous background. Institutional records painted a bleak picture, describing the family as socially problematic. Rumors surrounding Anna's mother suggested promiscuity and criminal behavior, including theft, which led to incarceration. Their father, who was Czech, was employed as a miner, indicating a working-class background beset by socioeconomic challenges.
Life in the children's home was stringent and unforgiving. After 2 years, Anna and her sisters were expelled for behaviors deemed inappropriate, such as sneaking out at night to meet boys. Subsequently, while Anna's older sister managed to live independently, Anna and her other sister were transferred to another institution. Anna had to stay in the state welfare system until she reached the age of 21. To contribute to society and demonstrate employability, at age 19 she was sent to work for a farmer. Shortly after this she delivered Marianne out of wedlock.
Anna faced another significant challenge when Marianne, then 6 months old, contracted pneumonia and was hospitalized. Rather than being reunited with her mother post-recovery, Marianne was placed in a children's home. Here, the staff observed developmental delays, which they attributed to hereditary factors from Anna's family. This assessment further entrenched the stigmatization of Anna and her lineage. Marianne was transferred to an institution for disabled children with the explanation that it was unacceptable keeping her in the children's home with the “healthy” children.
Despite Anna's subsequent marriage and efforts to reclaim her daughter, her attempts were thwarted. The institutional biases and societal prejudices against her were evident and persistent. In May 1940, Marianne's physician completed a T4 questionnaire, diagnosing her with “Idiocy”—a term reflecting the discriminatory and pseudoscientific medical practices of the era. This diagnosis was linked to Anna's genetic heritage.
Marianne was selected for euthanasia under the T4 operation. To cover up the program, Anna received a letter stating that her daughter had been transferred and was in good physical condition but pointing out the lack of intellectual development, legitimizing the transfer to an institution for disabled children. This letter was the last entry in Marianne's medical record, marking a somber and tragic end to her brief life.
Here is the data on Marianne's T4 survey:
Nationality and Race: German Diagnosis: Idiotism (congenital feeblemindedness), neurologically normal, hereditary burden from mother's side. Admitted since: 1939 Address of next of kin: Mother Anna S (with address) Guardianship: Yes Representative: District Administrator of Spremberg District Paying Institution for the institutional stay: B.F.V. Spremberg
(Federal Archives Berlin, R179/1306)
Hans (Age 12)
Little is known about Hans until he reached the age of six, at which point an assessment was conducted, likely in preparation for his admission to a children's home. There was no information available about his parents or their whereabouts; only a legal guardian was mentioned in his chart. The assessment described Hans as a healthy child with some cognitive disabilities. The accompanying picture in his chart shows a young boy standing straight, doing his best to present himself well.
During his time at the children's home, Hans appeared similar to most boys his age, appreciating positive feedback and striving to excel in competitive situations with other boys. However, he was somewhat of a loner and not the center of his social group. Hans excelled in performing repetitive tasks, such as patching up socks, and valued recognition for his work. Nonetheless, he struggled with finding unique solutions to new problems. His moods were noted to be stable. He never got any visits during his stay in the children's home.
As time progressed, the notes in Hans’ chart increasingly focused on his limitations and lack of visible progress. A T4 survey was submitted indicating that he had no potential to be productive to society and that the “War Welfare Office” was covering his living expenses. With repeated entries about his “demanding” behavior, his lack of educational ability, and the effort his supervision needed, his fate was sealed (these were the essential selection criteria for people being transferred to T4 facilities).
On May 21, 1940, a final note stated that by federal order, Hans was being transferred. The specific institution to which he was transferred was not mentioned, and Hans was never heard from again.
This account of Hans’ life reflects the tragic and often overlooked experiences of children with disabilities during a tumultuous period in history. Despite his stable moods and ability to perform certain tasks well, the assessment of his potential was grim, ultimately leading to his transfer and disappearance following a federal order.
Here is the data on Hans’ T4 survey:
Nationality and Race: German Diagnosis: congenital feeblemindedness Admitted since: 1934 Address of the next of kin: Unknown Does the patient receive frequent visits: No Guardianship: Yes Representative: Emil B (Address listed) Paying Institution of the institutional stay: War Welfare Office Beeskow-Storkow
(Federal Archives Berlin, R179/14497)
Wilhelm (Age 41)
Wilhelm was born into an intact family and had a relatively normal youth despite his mother dying of cancer during his teenage years. He had no health issues, excelled in school, and pursued vocational education to become a lock maker. Shortly after completing his education, Wilhelm was drafted into the military during the First World War. He was released from active service at the age of 19 when the war ended and began working as a lock maker.
At the age of 22, Wilhelm married Martha, and the couple had two healthy children. However, the onset of the Great Depression brought economic hardships, leading to Wilhelm being laid off due to a lack of available work. He managed to secure a job as a utility meter reader and bill collector for the city.
By the age of 35, Wilhelm began experiencing a lack of appetite, which was not easily diagnosed or treated. After visiting numerous physicians, he was finally encouraged by his wife to see a neurologist/psychiatrist, who diagnosed him with paranoid thoughts. Following this diagnosis, Wilhelm attempted to hang himself at home, but his wife found him in time and cut him loose. He was subsequently admitted to a psychiatric hospital, where he was diagnosed with schizophrenia with paranoid thoughts, believing he needed to protect his family from perceived threats.
During his hospital stay, Wilhelm was well-organized and cooperative with the medical staff, who noted his physical health but also his anxiety. His mental status varied and over the months of hospitalization he suffered from paranoid thoughts, especially about being poisoned by the personnel or even by his wife. These delusions also led to verbal or physical attacks against medical staff and other patients. During his stay, his wife became pregnant again and gave birth to a daughter. Due to his mental illness, Wilhelm was sterilized, which further strained his relationship with his family.
Despite the challenges, his wife advocated for effective treatments to facilitate his return home. After approximately 2 years his mental status was more stable and he was discharged, but was unable to resume work. He spent most of his time at home, occasionally helping with household tasks. At the age of 39, Wilhelm was readmitted to the hospital because of familiar issues he didn’t want to mention further. During his stay, his wife gave birth to a daughter. Despite being in good physical health, his medical records became sparse, focusing mainly on his inability to work and contribute, except for mention of two epileptic seizures 4 months before being transferred.
Six months after his admission, the last note in his chart indicated that Wilhelm was being transferred to another facility because he was unable to work. Tragically, this transfer was to one of the euthanasia centers, marking a grim end to his life.
Wilhelm's medical record contained no T4 survey.
(Federal Archives Berlin, R179/1334)
The Technique
How was it possible that an office in Berlin was able to determine the fate of so many people with relatively few resources? Several factors contributed to this. First, as the National Socialists came to power, medical records began to focus more on patients from a eugenic perspective. Mentions of family members with longstanding issues of mental illness or antisocial behavior became more common, and documentation ceased to reflect the patient as an individual. This was the first step toward depersonalization.
The second step toward depersonalization was the Fragebogen or questionnaire, which was pivotal to the T4 operation. This process effectively reduced real people to mere data points. During the autumn of 1939, patients in German sanatoriums and nursing homes were enrolled using registration questionnaires distributed by the Reich Ministry of the Interior. These questionnaires were accompanied by a leaflet outlining the criteria for enrollment, which included specific ailments like “congenital feeblemindedness” or “schizophrenia,” as well as factors like the duration of stay and work engagement. People of Jewish descent, foreign nationals, and individuals deemed criminally insane were mandated for registration without exception.
As the T4 operation progressed, the original registration questionnaire was replaced by a more detailed version that probed further into the patient's medical condition and vocational activities. Institutions relied primarily on these questionnaires to select victims for “euthanasia.” Very few questionnaires have been found that contain the positive recommendation for “euthanasia.” Below is a translation of the replaced T4 questionnaire (Figure 1).
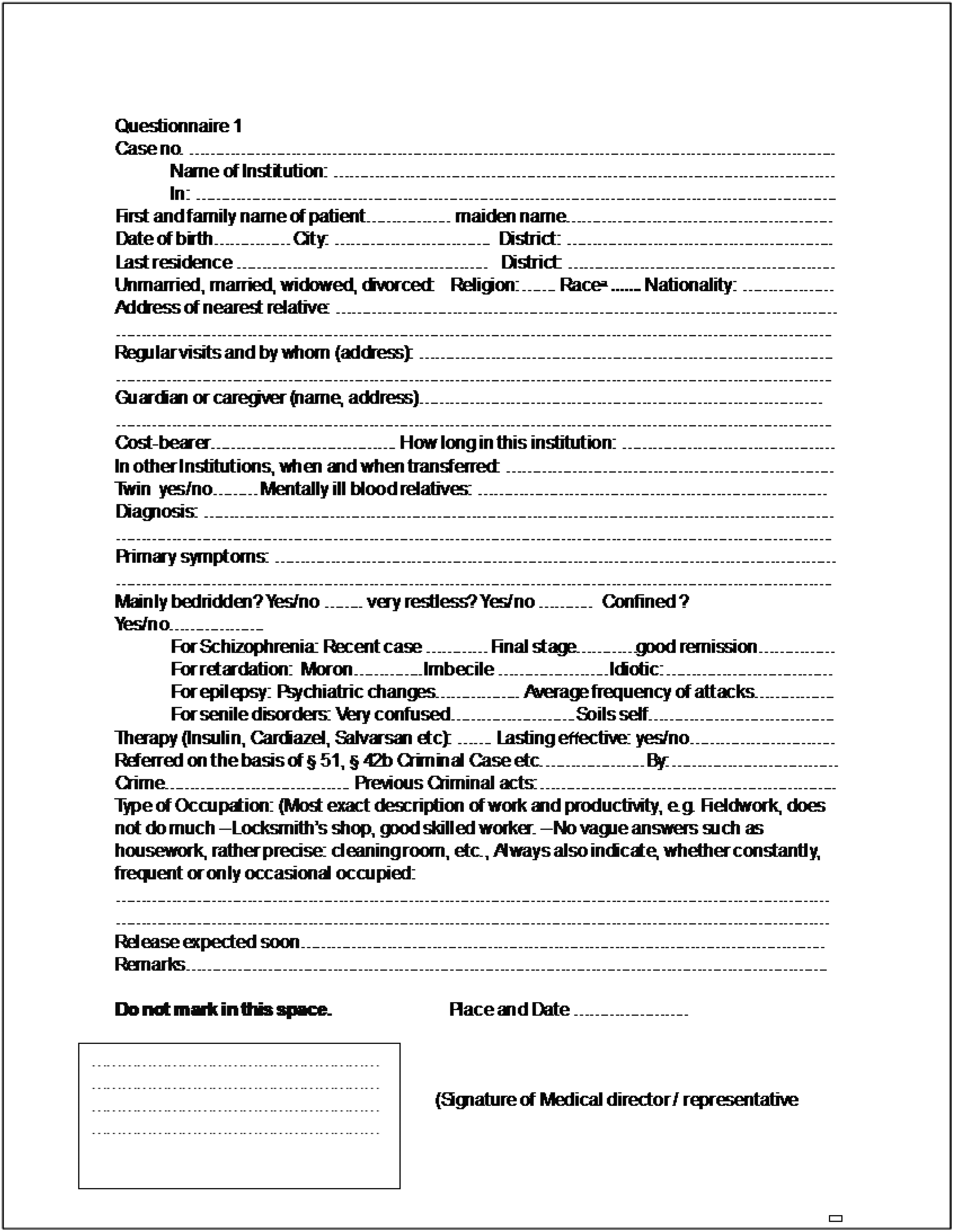
T4 Questionaire—Translation (Federal Archives Berlin, R179/18427).
The more people are depersonalized, the easier it is to classify them in a category with just a few data points, whether by race, diagnosis, ability to work, or cost to the community. During the T4 operation the categories were either to be allowed to live to to be killed. This classification into categories allowed for great efficiency in determining which people should be eliminated, to better society according to the Nationalist Socialist ideology.
The Role of Family in the T4 Operation
It is noteworthy that having family was a protective factor, or at least impeded the process of “euthanasia.” Families who frequently visited their loved ones could become suspicious of unexpected deaths and potentially expose the secret program. The National Socialist system recognized that family ties were likely to outweigh the prevailing ideology.
If families were involved and patients were selected for “euthanasia,” they were often told that their family member had been sent to a distant facility, making visits nearly impossible. It is challenging to determine how many people escaped “euthanasia” due to family involvement, as records for these individuals are not readily available in archives.
The protective effect of family involvement highlights a critical aspect of the era's social dynamics. Families could serve as a form of resistance against the regime's policies, intentionally or not. The regime's awareness of this potential resistance led to strategies aimed at circumventing family interference. Family pressure did succeed in ending the T4 operation in 1941, when actions by families and Catholic and Protestant welfare institutions who were directly impacted by the operation, represented by the powerful and respected bishop of Münster, Clemens von Galen, led to shutting down the formal operation. This unfortunately only resulted in a decentralization of the operation, shifting the responsibility for implementation to local health-care facilities. A further estimated 200,000 people were killed after the centralized program was terminated.
In examining the broader implications, it becomes evident that the decentralization of the euthanasia practice after 1941 allowed it to persist in various forms, complicating present-day efforts to track and understand the full scope of these actions. The lack of centralized records further obscures the extent to which family intervention may have saved lives, emphasizing the importance of continued research as more records become available.
The Role of Nurses in Making the T4 Operation Work
Nurses played a key role in the functioning of the T4 operation. They were skilled at putting people at ease and directing them to comply with necessary actions. These skills remain a backbone of nursing today. The nurses who worked in the “euthanasia” centers were often recruited from the same mental health hospitals from which many victims were taken. When selecting nurses, those who were dependable (primary qualification needed) and obedient were preferred (Fürstler & Malina, 2004; Heuvelmann, 2013; Steppe, 2013; Steppe & Ulmer, 2014). The National Socialist era was driven by fear, and refusing to follow orders could have severe consequences, influencing some nurses’ compliance (Copeland, 2021).
Nurses managed the process, ensuring patients remained calm during transportation and during the final medical examinations before being escorted to the gas chambers (Fürstler & Malina, 2004). However, nurses were not required to turn on the gas, as this was considered a medical intervention. There were discussions about whether the approach of calming and comforting patients as part of the “euthanasia” process was more ethical, considering that the outcome, death, was non-negotiable and this way they would die with less distress (Benedict, 2003; Benedict & Kuhla, 1999).
What Happened to the Nurses Who Participated in the T4 Operation
During the period 1945–1955, special courts were established for the purpose of denazification, to hold perpetrators accountable. However, many accused individuals evaded these processes by either committing suicide or fleeing, rendering them untraceable. Those who did stand trial were often classified as merely accessories rather than as principal offenders, resulting in minor prison sentences or acquittals (Eigelsberger, 2019).
The courts made a distinction between philosophical guilt and legal guilt. For example, health-care workers, who were compelled to work in facilities due to emergency service obligations and who had no affiliation to the National Socialist Party (NSDAP), were frequently acquitted; their acquittal was also justified if they did not engage in any activities beyond their “regular” duties within the facility. Conversely, if an individual was found to have participated in additional culpable actions, such as assisting with the disposal of corpses, had a membership in the NSDAP, and/or took up their role without being under emergency service obligation, they were often found guilty (Copeland, 2021; Eigelsberger, 2019; Klee, 2007).
Residual ideological beliefs appear to have contributed to why many were not convicted: fear of punishment logically led to the “excuse” that one's own healthy life should not be sacrificed for the mentally ill (Eigelsberger, 2019). Additionally, some defendants expressed a moral obligation of duty, feeling compelled as state employees to fulfill their responsibilities and to comply unquestioningly with orders from doctors and senior nursing staff (Benedict, 2003; Benedict et al., 2007; Fürstler & Malina, 2004; Steppe, 2013).
Despite being aware of the ethical impropriety of their actions, some nursing staff rationalized their involvement with ending lives they deemed unworthy, believing they were providing relief to those who would only suffer otherwise (Benedict et al., 2009; Benedict & Georges, 2009; Steppe, 2013). They also minimized their actions by making clear that they ensured comforting final hours and fulfilled individual last wishes, such as administering last rites and holding people while dying (Benedict et al., 2007; Steppe, 2013).
Despite the strong influence of National Socialist ideology, which sought to depersonalize patients through bureaucratic processes, there were instances where nurses resisted participation in the systematic killings. These acts of resistance often stemmed from personal convictions, such as religious beliefs, that conflicted with the actions they were being asked to perform. The publication of journal entries from nuns who worked in psychiatric hospitals provides a poignant insight into the ethical dilemmas faced by these health-care professionals (Heuvelmann, 2013). These nuns, while not directly involved in the killings, suspected the atrocities and expressed their moral opposition, illustrating the tension between the dominant ideology and individual ethical standards.
This tension is further exemplified by the nurses who requested to return to their original hospitals, seeking to distance themselves from the morally reprehensible acts of the T4 operation. Their actions underscore the importance of individual agency and the role of personal conscience in navigating ethical challenges within oppressive regimes. These actions suggest that while many nurses adhered to the dehumanizing directives of the National Socialist program, others were guided by a different set of values that prioritized human dignity over ideological conformity. The moral distress experienced by some nurses during the T4 operation reflects a complex interplay between ideology, professional duties, and personal beliefs. This historical reflection highlights the critical need for health-care professionals to engage with ethical frameworks that respect individual autonomy and moral integrity, particularly in environments where institutional policies may conflict with personal values.
Ponderings for Today
Current nurses work in an electronically mediated care environment driven by artificial intelligence (AI) and institutional priorities, including risk management, financial stability, and quality improvement (de Ruiter et al., 2016). However, this system often fails to recognize each patient as a unique individual (Kerr & Hayward, 2013; Ubel et al., 2017). Furthermore, it has created a work environment where nursing practice is under constant surveillance through electronic documentation systems that can be programmed to provide feedback to nurses about their documentation and related tasks (de Ruiter, 2007). Automated reinforcement systems can send reports or emails to supervisors, notifying them of documentation lapses. Some systems even use color-coded warning lights to guide nurses in meeting institutional data requirements. For example, nurses strive to achieve the coveted “green dot” for completed documentation, while those who comply with policy late receive an “orange dot,” and those who fail to document within the permitted time get a dreaded “red dot.”
This system has fostered a fear-based work environment where institutional priorities often take precedence over patient care (de Ruiter et al., 2016; Ubel et al., 2017). Nursing practice is increasingly shaped by documentation requirements, leading to nurses collecting and documenting data points without understanding their use (Day, 2009; Olivares Bøgeskov & Grimshaw-Aagaard, 2019). Consequently, according to Ho et al. (2021), many new nurses feel alienated from their work and the values that initially drew them to the profession. This alienation contributes to high turnover rates, with nurses leaving the profession faster than they can be replaced (Al Sabei et al., 2020; Wan et al., 2018).
In this environment, the International Council of Nurses (ICN) Code of Ethics for Nurses (International Council of Nurses, 2021) and national and regional codes of ethics such as the Code of Ethics and Conduct for European Nursing (Sasso et al., 2008) and the American Nurses Association's Code of Ethics for Nurses with Interpretive Statements (American Nurses Association, 2015 ) have come to be considered idealistic and ideological in nature, rather than actively used by all nurses in their practice in real time and space (Blackwood & Chiarella, 2020). Because of health-care systems’ ability to manage what nurses need to document and to monitor their compliance, nurses now more likely to document what is required by the institution without critically analyzing whether what is required is in the best interest of the patient (de Ruiter et al., 2016; Hunt et al., 2017). The misuse of data can have enormous impacts on individuals. History teaches us that we often repeat our mistakes (Rowe et al., 2010; Turchin, 2008). While we may not see a repeat of the T4 operation, it is likely that data will continue to be used to achieve ideological goals, sometimes at the expense of patient well-being. To prevent such misuse, vigilance and awareness by all nurses in recognizing new forms of misuse is essential. Nurses are ideally positioned to be gatekeepers, but they need the autonomy to practice based on the ICN and the regional and national codes of ethics rather than institutional priorities and political ideology.
The current educational environment for nurses, focused on achieving a set of competencies, is a slippery slope (Collier-Sewell et al., 2023; Wolf, 2022). We must examine the underlying ideologies behind these competencies. Are they driven by systems or by individuals? Do they support the individual well-being of patients, or that of the health-care system or the dominant political ideologies? Both are important, but we must strike the right balance between patient needs and institutional requirements. As this recounting of history shows, seemingly innocent actions can lead to significant unseen consequences, and just a few data points collected by nurses can lead to crucial decisions (Harper & McNair, 2017; McCartney, 2012). During the T4 operation, medical records and survey questionnaires were manually evaluated in Berlin. Today, we have electronic databases that can share data in real time, and AI that can analyze thousands of records in seconds, raising the risk of patient data being (mis)used for ideological purposes rather than using data points to make crucial decisions for good (Chiruvella & Guddati, 2021; Murdoch, 2021; Rickert, 2020). Unlike during the T4 operation, nurses now have codes of ethics at national and regional levels to guide their care. However, it is essential that nurses possess and use the autonomy within their practice, to place their ethical and practice standards before the ideological priorities of the institutional and political systems in which they find themselves.
In reflecting on the historical lessons of Aktion T4, it becomes evident that nurses, like many other individuals, can be swayed by societal ideologies that run counter to the core values of their profession (Murphy et al., 2005; Skår, 2010). While the specific circumstances of T4 may not repeat themselves, the rapid evolution of technology presents new challenges that require vigilance and ethical fortitude. As nursing continues to operate within complex social and technological landscapes, it is imperative that nurses use documents such as the codes of ethics as a guiding compass, not only as a professional mandate but as a “counter” ideology in environments where nursing values are at risk. By adhering to ethical principles, nurses can ensure that patient care remains at the forefront of their practice, safeguarding against the depersonalization and misuse of data that can lead to harm. The profession must remain steadfast in its commitment to human dignity, leveraging the lessons of history to navigate the moral complexities of the present and future. In doing so, nurses uphold their role as advocates for patient welfare, resisting pressures that may otherwise compromise the integrity of care.
Footnotes
Disclosure
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Minnesota State University, Mankato (grant number Faculty Reseach Grant).
Author Biographies