
Abstract
Implications for Knowledge Translation
Illness is a patient's experience of their disorder, while disease is a doctor's diagnosis of the disorder. The role ambiguity experienced by psychiatric nurses often makes it difficult to demonstrate the efficacy and positive contributions of their work. To facilitate a psychiatric patient–nurse partnership, it is important to provide a safe narrative space where the patients can voice their opinions. Use of the Patient-Authored Medical Record, a “prescription” for care written by the patient with the assistance of a nurse, could become a valuable skill for psychiatric nurses that distinguishes their profession.
Psychiatric nurses working in outpatient services in Japan are busy assisting psychiatrists, monitoring patients’ visits, checking vital signs, and offering other assistance. Since outpatient visits are usually brief, the setting and schedule lack time for meaningful conversations about patients’ personal lives; in general, psychiatric nurses have little opportunity to get to know patients as individuals (Jagosh et al., 2011; Kmietowicz, 2000; Nomura, 1992). In such circumstances, nurses in psychiatric settings often experience professional ambiguity (symbolic or practical) when working alongside individuals in other paramedical professions, such as clinical psychologists, psychiatric social workers, and occupational therapists (Kimura & Matsumura, 2010; Sabella & Fay-Hillier, 2014; Salberg et al., 2019). Psychiatric nurses’ identity issues have been historically recognized, leading to the question of “what we do and who we are” as specialists, with difficulties in defining and describing the role beyond vague terms associated with the stereotypical image of the “housekeeper” (Barker & Buchanan-Barker, 2011; Peplau & Faan, 1994). The role ambiguity and role conflict experienced by psychiatric nurses often make it difficult to demonstrate the efficacy and positive contributions of their work (Hercelinskyj et al., 2014) and/or to build skills that are exclusive to their profession. The purpose of the research on which this article's case study is based was to explain how the Patient-Authored Medical Record (PAMR) can contribute to medical practice reform through collaboration with psychiatric patients. By writing their own medical records as prescriptions for care from their perspectives, patients can confront their illnesses and proactively engage in their recovery process, leading to more equal collaboration with medical staff, which is further reflected in patients’ relationships with their families. For psychiatric nurses, this approach provides an opportunity for new nursing practices using the PAMR, a tool that emphasizes dialogue.
What Are PAMRs?
Patient-authored medical records are a therapeutic tool for psychiatric nurses that we developed to create a suitable method to enable therapeutic conversation in psychiatric hospitals by helping patients write their own prescriptions for care and design their own treatment programs (Tsubonouchi et al., 2022). A narrative document is created jointly by the patient and their nurse during an in-person meeting that addresses the following questions:
What is happening in your life? What are your current problems? How do you want to cure your disease? What are your dreams and hopes for the future? What else do you want others to know?
The patient tells the nurse about events in their life in preparation for writing their own prescription for care and how they believe the illness can be treated. The nurse summarizes the patient's narrative, not as a verbatim record but as field notes of 1–2 pages, and uses that summary to create the PAMR (e.g., Hoyt et al., 2018; Slive & Bobele, 2011).
Follow-up meetings are held in the hospital, with participants selected by the patient, usually including a psychiatrist, a nurse, and family members. Copies of the original PAMR are distributed to all participants, who are asked to share their thoughts and impressions. The participants then discuss any issues the patients and their family members want to discuss, with the nurse facilitating the discussion.
Theoretical Basis of the Narrative Approach: Not-Knowing
The idea of PAMRs emerged from the theoretical lineages of cultural anthropology and the family therapy movement pioneered by Bateson et al. (1956). Since then, family therapy scholars have continued to refine their theories to involve narrative-collaborative approaches (Anderson & Goolishian, 1988; White & Epston, 1990) and open dialogue (Seikkula & Olson, 2003). The premise of these approaches is that the phenomena of mental disorders are describable using solely communicative language without resorting to psychodynamics (Bateson et al., 1956; Sullivan, 1953). The patient's self-narrative, elicited through dialogue, usually maintains integrity as a story and contains a germ of truth (Epston et al., 1992). Although doctors and nurses may be disease experts, patients are experts regarding their illness: how they experience the ordeal and pain and how they live with their disabilities. Illness is a patient's experience of their disorder, while disease is a doctor's diagnosis of the disorder (Kleinman, 1988). Patient-Authored Medical Records focus on illness rather than disease, embracing the basic stance of not knowing, to listen to the patient's story and to be informed about how the patient lives with their illness. Not-Knowing refers to the attitude of asking questions out of genuine curiosity about the conversation the patient has brought up. In other words, it involves choosing questions from within the content of the conversation brought up by the patient, not bringing in topics from outside the conversation or asking questions from outside the scope of the topic. Every story has an untold part, and the therapist asks questions that focus on the assumption that the patient has a story that has not yet been told. The patient's story can then become richer or new. In the narrative approach to family therapy, this is considered a therapeutic change (Anderson & Goolishian, 1988, 1992). In such a dialogical context, patients can express their views on their illness and how to improve it. The nurse's task is to learn the patient's way of life. This approach is similar to cultural anthropology: the field worker learns about the local culture, asks questions, participates in activities, and records the knowledge obtained in field notes. Patient-Authored Medical Records are similar to field notes written by psychiatric nurses.
The follow-up meeting with the patient draws on the language practice (poetics) of open dialogue, where every utterance is respected and replied to, and uncertainty and diverse opinions (polyphony) are tolerated (Seikkula & Olson, 2003). Giving all voices room to exist when differences arise, rather than a right-or-wrong attitude, can promote safety and trust. Immediate advice and rapid conclusions are avoided as much as possible. The focus is not on handling things or solving problems but rather on shared experience and on the form of conversation. These principles are based on the belief that as a form of agency, dialogue itself brings forward new ideas and understandings.
Methods
In the original study (Tsubonouchi et al., 2022), data were collected by asking ten patients with schizophrenia or mood disorders visiting an outpatient psychiatry clinic in Nagoya, Japan, to describe events in their lives to create their own prescriptions for care. The researcher recorded the patients’ first-person accounts of how they thought their illness could be treated, and generated the patients’ records. Follow-up meetings with the patients, their relatives, and medical personnel were held at the hospital using the PAMR. The data used for the analysis included the PAMR itself and the verbatim transcripts of the follow-up meetings. The focus of this design was whether patients could express their worries and difficulties in life, whether they could obtain a “place” where they felt safe to talk, and whether the PAMR functioned as a “prescription” for their treatment; these questions were all examined qualitatively. In the original study, the PAMR functioned as a medical tool and had significant therapeutic effects on patients visiting psychiatric outpatient clinics (Tsubonouchi et al., 2022).
These findings indicated the therapeutic nature and importance of the PAMR. In this paper, we report on the progress of PAMR treatment and subsequent follow-up meetings using a detailed case example with one of the original participants. All of the information given in the case study was described by the patient and the nurse researcher during the creation of his PAMR. We show how the PAMR method can enable psychiatric nurses to build skills that are unique to their profession and suggest how this allyship with patients is a step toward reforming current hospital psychiatric practices. This study was conducted with the approval of a research ethics review of Nagoya University (Approved No. 19-119-2) and the cooperating institution (Approved No. HM20-252).
Results
The Case of Kenji: I’ve Found My Space
Kenji (a pseudonym) is a Japanese man in his late 50s. He suffered from depression and manic episodes. At the time of the original study, he had been in and out of the hospital repeatedly, with no improvement observed despite drug therapy and electroconvulsive therapy (ECT). His greatest challenge was the state of his sleep. Although he took many sleeping pills, he often had bad dreams. He felt light-headed from taking so many sleeping pills, but he still could not sleep. At night, when he could not sleep, he would eat all the food in the refrigerator. Kenji had resigned from his job because his condition was not improving as he had hoped, and he then spent time at home. He felt more relaxed when he was doing household chores. He was able to hang the family laundry, wash the dishes after the family had eaten, and take out the garbage, but it was difficult for him to look over papers, answer the phone, or respond to visitors, such as when a delivery arrived.
Kenji's Life History
Kenji met his wife at his workplace, got married in his early 30s, and had two children. An engineering graduate, he loved studying chemistry and was an active participant in athletic club activities. After graduating from university, he worked at a hospital as a laboratory technician. When he was in his early 40s, his enthusiasm for his work, personality, and technical skills were highly regarded, and he was selected to head a department when a satellite hospital was opened.
Six months later, however, he was working late into the night, and his sleep gradually became shallow due to continuous overtime work. He became depressed due to work stress and went to the hospital at a different location, where he was treated with oral medication to monitor his progress.
Treatment for Kenji’s Mental Health Issues
During this time, Kenji was referred to another hospital when his attending physician was transferred, but his condition did not improve, and he gradually stopped coming to the hospital.
He took several leaves of absence from work, but his symptoms became so severe that he spent a year in a nearly bedridden state before retiring. After his retirement, he remained bedridden for approximately 3 years. During that time, he visited several hospitals. Severe depression was observed, and ECT was performed at his request, but no improvement was observed. At that time, Kenji felt discomfort all over his body, but according to Kenji, there were no particular aftereffects on his memory or cognition. Previously, Kenji could not sleep well even after taking three kinds of benzodiazepines. In his state of mind, he did not know whether he was asleep or awake, and wanted to escape from reality. He had fallen out of bed; he informed his psychiatrist about it, and the psychiatrist recommended waiting and seeing. Kenji had been in and out of the hospital at least seven times, and his doctor felt that he was difficult to treat.
In this setting, decisions about medications are usually made through discussion between the patient and the attending physician. If the nurses felt that a change in prescription was necessary, they could not directly advise the patient, so the usefulness of a patient-authored record to address this issue was notable.
Family Issues
Kenji thought that after retiring from his job, he could concentrate on his own medical treatment and recovery, but a further challenge awaited him. For 3 years in his early 50s, he spent every day as a caregiver for his parents. His mother suffered from mild dementia, and his father needed nursing care. He took care of all aspects of their daily lives, from getting them out of bed to moving them to a chair for eating. At this time, he slept only about one hour a night.
In addition to taking care of his parents, he participated vigorously in community activities, thinking, “I’m going to make a difference in my community.” His hypomanic state worsened, and because he was active from morning to night, he lost approximately 10 kg of weight. Later, his father passed away, and his mother entered a nursing home. Even after being released from caring for his parents, Kenji felt that his body remained heavy and that his fatigue and sleep problems did not improve.
In his late 50s, he continued to experience a hypomanic state. He slept only about 4 hours a night but still felt good. He was also troubled by his relationship with his college-age son, who lived with him but with whom he did not speak at all. In recalling these difficult days when developing the PAMR, Kenji told in the PAMR that he could not fulfill his role as a father because he was home sick in bed when his son was in the critical age of puberty. He felt that being unable to speak with his son was due to their history, in which his son had seen him in a severe depressive state and in a manic state, with Kenji laughing loudly and making noise late at night.
Kenji's PAMR
At the recommendation of his psychiatrist, Kenji entered the original study, working with the nurse researcher to create and refine his PAMR three times. He was allied with the nurse and was assured of the opportunity to express his thoughts and feelings and was assured of empathy and dialogue. Over time, his sleep condition improved; he was able to participate in household chores and to go alone more easily, and had more time for activities. Kenji was able to determine his own indicators of how to address his illness and cope with it, and his life goals changed.
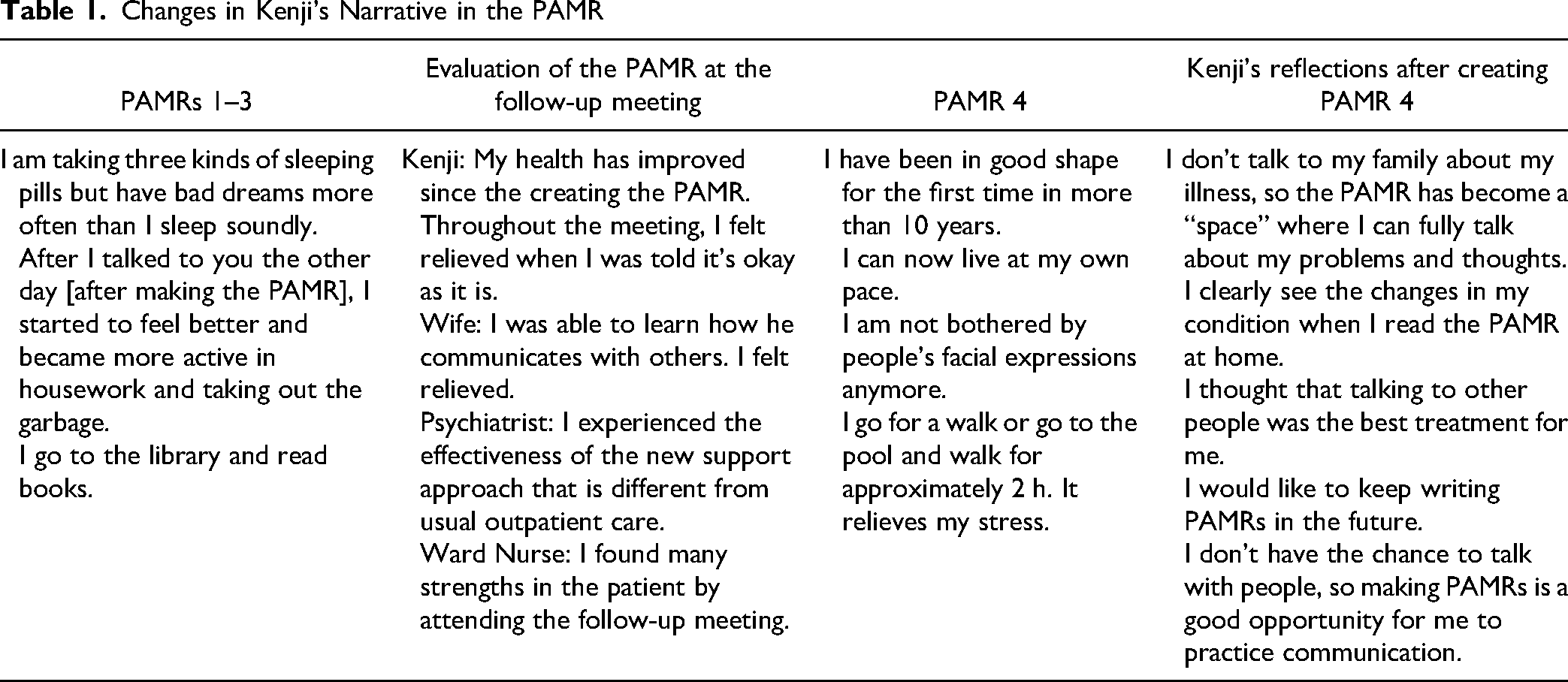
Kenji's case was difficult to treat because he repeatedly experienced manic and depressive states. However, through narrative practices (the PAMR and follow-up meetings) in collaboration with the nurse researcher, Kenji was able to gain space for himself. His long-lasting insomnia resolved, and his daily life improved markedly. Table 1 illustrates easy-to-understand diachronic changes in Kenji people's narratives and behaviors.
Changes in Kenji's Narrative in the PAMR
Main Topics Presented in Kenji’s PAMR
Patient-Authored Medical Record 1
I can’t get out of bed. I take about three sleeping pills but have bad dreams more often than I sleep soundly. I have fallen out of bed a couple of times.
Not able to speak to my son at all. When my son was little, I used to make quite loud and strange noises, and I think he thought I was crazy.
Patient-Authored Medical Record 2 (One month after the PAMR 1)
I cannot sleep. I eat all the food in the fridge, and I take a lot of sleeping pills, so I feel fuzzy, but I cannot sleep.
I felt like if I could talk to my wife and daughter, I would feel a little better, because I do not talk to my son at all.
Patient-Authored Medical Record 3 (Six weeks after PAMR 2)
I feel better now that I can get up in the morning. I’m able to do housework and other things more actively, and I have started going out, going to the library to borrow and read books.
In the future, I would like to do all household chores. I want to improve my thinking, memory, and communication skills.
Patient-Authored Medical Record 3 reflected that Kenji's mind and body had undergone significant changes. First, he showed signs of recovery from his long-suffered sleep disorder. Second, although he had always felt stuck in the past and looked backward, he had changed to the point that he could express feeling the joy of living with a future perspective.
The Follow-Up Meeting
A follow-up meeting with Kenji, his wife, his psychiatrist, a ward nurse, and the nurse researcher was held to discuss PAMRs 1, 2, and 3. The nurse researcher sat next to Kenji, read the records aloud and described some issues the participants might choose to discuss, facilitated the meeting, and participated in the discussion. Kenji spoke 91 times, his wife 23 times, his psychiatrist 66 times, the ward nurse 62 times, and the nurse researcher 61 times.
Kenji's psychiatrist initially introduced Kenji to the nurse researcher because the psychiatrist wondered what would best facilitate Kenji's treatment process. At the meeting, the psychiatrist mentioned that he was looking forward to seeing a different side of Kenji in a different kind of meeting that would go beyond a psychiatrist's usual practice of a one-way discussion between him and the patient, and was curious about what kind of conversation would take place when several people gathered. He also said that the most important thing for him was to know what kind of attitude and stance he should have toward Kenji.
At the meeting, Kenji voiced his opinions regarding how to live a healthy life; improve his sleep rhythm, dreams, and hopes; and maintain his distance from his son. Kenji said, “For the first time in over a decade, I had a period where I was feeling well and could live at my own pace.”
Two points that were raised by Kenji during the follow-up meeting: I want to contribute something to society. Kenji could never have thought of this when he was depressed, but as he gradually improved, his desire to contribute to society increased daily. Whenever Kenji saw that people younger than he were working part-time or at other jobs, he felt inferior, thinking that he could not do such work, and always comparing himself with those around him. When the researcher nurse asked Kenji about this, he smiled and said, “I was relieved to hear that you said it was okay to keep doing what I was doing.” My son is my biggest worry. At home, Kenji was troubled by the discordant atmosphere, as his son did not even talk to him. His wife stated that forcing Kenji to talk to their son and try to work things out could be counterproductive, and she thought they needed to wait a little longer. The ward nurse, however, noted that it is very important to say hello to their son and thank him for his work. The psychiatrist also mentioned that it was important for Kenji to talk to his son.
Participants’ Impressions of the PAMR
During the follow-up meeting, the participants were asked to provide their impressions of the support approach using PAMRs. Kenji: Since I was listened to [when creating the PAMR], I have truly started to feel better, and it was a big trigger for me. From the discussion in the meeting, I was reassured by being told that it is okay as it is, and I realized the importance of finding joy in small things. I hadn’t been to a meeting since I was working, so I felt happy to participate and speak up. Kenji's wife: My husband always said he had a hard time talking to people or that he couldn’t do it well, so I do not know how he talked to people before, but I was relieved that he was able to talk smoothly and as usual at the meeting, and I wish he could talk like he did today in everyday life. Psychiatrist: I was able to talk in a more comfortable atmosphere, different from my usual outpatient clinic. I have never had the opportunity to talk to more than one person with a patient before, so I thought it was a great place to do so. I thought this type of setting was necessary because it was a valuable opportunity to talk more deeply.
Patient-Authored Medical Record 4
Three months after the follow-up meeting, PAMR 4 was completed. Here are excerpts:
I go to the swimming pool two or three times a week, and I walk for about 2 hours, which helps relieve stress.
I am in good health for the first time in over 10 years.
Now I can live at my own pace. I can take a relaxing bath and feel happy just to be alive.
Kenji felt even better, and his activities had changed. He had gone from just going to the library and walking to driving and going to the swimming pool two or three times a week. Kenji said at the follow-up meeting that the most important thing for his recovery was having the nurse listen to him (through the PAMR process) and that the dialogue was the main reason for his improvement. Figure 1 shows changes in Kanji's sleep and activity during the PAMR process.
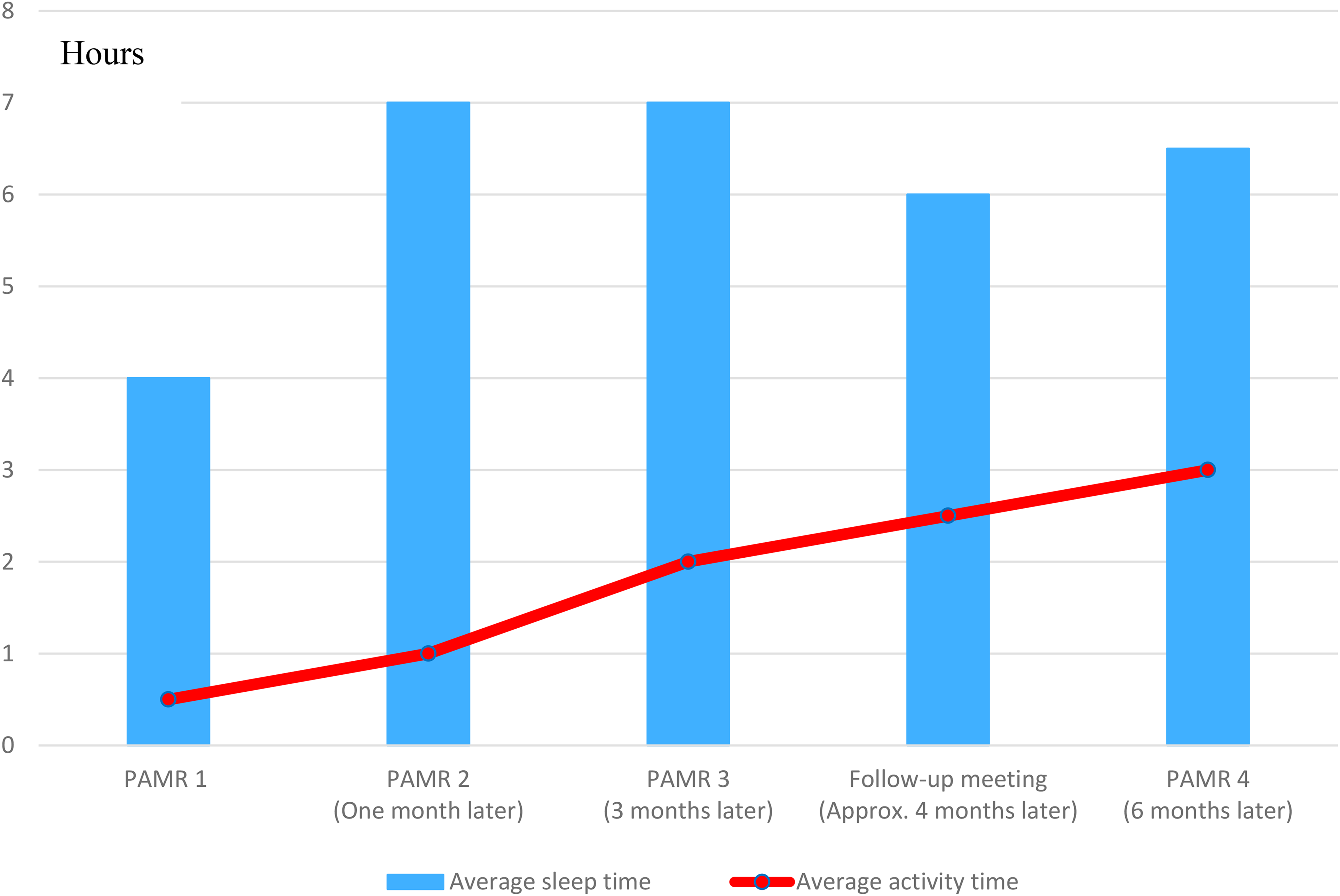
Changes in Kenji’s sleep and activity time.
Approximately 2 months after the study was completed, Kenji was asked how things had been going since then. He said he felt very well and remained stable. He said he would like to write another PAMR if there was an opportunity to do so: “I thought that the ‘dialogue therapy’ was right for me. I became aware of the importance of dialogue with people.” Kenji also happily reported that he was now able to drive himself to the hospital in addition to continuing to take a walk and play pool, for which he expressed satisfaction.
Three months later, the researcher nurse invited Kenji to attend a seminar on dialogue. Kenji said that attending the seminar reminded him of his working days and provided positive stimulation, and that it was necessary for him to be in a place where people gather and talk from time to time.
Discussion
Kenji's experience in creating a PAMR allowed him to find the right treatment for him, and he also felt the need to interact with others. PAMRs are instruments that allow patients and nurses to practice dialogue. Dialogue is a conversation distinguished by shared inquiry, that is, the coordinated action of continually responding to and interacting with another and of exchanging and discussing ideas, opinions, and feelings (Anderson, 1997). Why is dialogue effective for producing therapeutic outcomes for psychiatric patients? We note two aspects that should accompany a therapeutic dialogue and that are utilized in the PAMR method: not knowing and reauthoring (Moreno-Poyato et al., 2016). We then explain how an allyship with psychiatric patients can contribute to health-care practice reform.
Therapeutic Implications of Not-Knowing
The not-knowing position entails the therapist's actions communicating a genuine curiosity. The therapist's actions and attitudes express a need to know more about what has been said rather than conveying preconceived opinions and expectations of the patient (Anderson & Goolishian, 1992, p. 29). In the PAMR model, the nurse collaborates with the patient by listening attentively to their story and learning it. The patient, on the other hand, expresses his or her suffering and teaches the nurse about it as well as how it can be improved. The nurse learns the explanatory model (Kleinman, 1988) of illness from the patient and enters it into the record. For patients, medical record writing is an act of reclaiming agency (authorship) by becoming the narrator and coauthor with the psychiatric nurse, whereas the usual medical record is written by psychiatrists and other medical staff who are in more or less superior positions to the patient (Matsuoka, 2021).
Kenji's prescription for organizing his daily routines was derived from dialogue with the nurse, who adopted the not-knowing stance. She respectfully listened to him and asked questions out of genuine curiosity. He gradually gained agency to look ahead to doing housework, going to the library and swimming pool, etc. The not-knowing approach helps the patient express what has been unsaid before. The exploration of what is not yet known involves developing new stories that are therapeutic for the patient (Anderson & Goolishian, 1992). This becomes possible through dialogue with a suitable conversational partner. We believe that psychiatric nurses may be in a better position to take a not-knowing stance than are psychiatrists, who operate in a relatively rigid medical framework, and clinical psychologists, who are usually influenced by a particular school of therapy. Owing to their abovementioned role ambiguity, psychiatric nurses have a greater degree of freedom than those in associated professions to become attentive listeners to patients’ illness narratives.
Therapeutic Significance of Reauthoring
Kenji's therapeutic changes can also be seen from the perspective of story reauthoring. What we complain about in everyday life corresponds to our self-narrative or story; thus, if the story changes, the complaint changes, or at least its meaning evolves. White and Epston (1990) described the intention of reauthoring therapy as helping patients resolve problems through three means: (a) helping the person distance themselves from knowledge and stories that impoverish their life and relationships, (b) helping the person counter the situations and relationships to which they are forced to submit, and (c) encouraging the person to reauthor their life in the direction of alternative knowledge or stories that will produce the desired outcomes.
In this case study, Kenji was encouraged to rewrite his life in a direction that would lead to the desired outcome. The in-person format can increase the inherent strengths of people facing the challenges of mental disorders through collaboration and exploration with nurses (Ridgway, 1988). Coauthoring the PAMR with the nurse leads to confidence in and commitment to the content of the statement that cannot come from a monologue. It is also the moment when the patient gains an audience: the nurse as a moral witness (Kleinman, 1988). PAMRs, which are created multiple times with the patient, expand their inner dialogue and allow them to become the author of their own experience of illness and to confront the current illness, leading to a change in their perception of the past and how they view the problem.
For example, Kenji's story shows a significant shift from Story A to Story B.
Story A: I don’t get out of bed until about noon. I don’t know whether I’m asleep or awake in bed. I want to escape from reality. I feel tired and go out to the balcony to smoke. When I see people working, I get depressed because I can’t do it.
Story B: Just live life at your own pace. I have found ways to de-stress. Two-hour walks and swimming can make me feel better. These are becoming a part of my daily routine.
How Allyship with Patients Contributes to Health Care Practice Reform
The not-knowing approach and helping the patient reauthor their life become the basis for therapeutic collaboration and allyship between the patient and the psychiatric nurse. The nurse's support for the patient through writing the prescription for care is presented at follow-up meetings to seek extended allyships with the psychiatrist and the family. The PAMR framework involves radically different health-care practices than traditional styles (Happell et al., 2018). However, the following two conditions, reflective practice and polyphony, should be met in order to perform such a revised health-care practice.
Reflective Process
When people speak, their internal conversation is directed outward to others. What was personal is connected to the social, and this socially charged dialogue encourages the internal conversation of those who hear it. In the PAMR follow-up meeting, the patient becomes a speaker expressing their own view before others; however, the patient also becomes a listener when other participants exchange opinions about them. The patient moves back and forth between being a speaker and a listener, viewing them from multiple angles. This process has been called reflective by Andersen (1987). The patient's internal conversation is encouraged as they listen to others discussing them in the group. This is possible only when people from all professions gather on a level playing field. In Kenji's case, sharing the same communication space with the patient's family, the psychiatrists, and the ward nurse, who did not usually see each other, provided supportive elements of the therapeutic environment and reflection. Kenji was told by the participants that he was okay as he was, and this confirmation and approval inspired him to take a new look at himself through his internal conversation.
Polyphony
The second condition for health-care practice reform is the appreciation of diverse ideas and opinions. Polyphony in a dialogue signifies the dynamic expression of different ideas, opinions, and emotions (Bakhtin, 1984). Polyphonic dialogue has been reported to have beneficial effects by reducing the gap between illness and health and creates new shared understandings (Olson et al., 2014). Polyphonic dialogue creates horizontal relationships and a narrative community of participants through therapeutic encounters that reduce patients’ sense of powerlessness (Dawson et al., 2021). In follow-up meetings, patients can use PAMRs to tell stories about events in their daily lives; their interpretations, thoughts, and feelings; and difficult topics that cannot be fully discussed in the usual medical setting. It also creates an opportunity for family members and medical personnel to deepen their understanding of patients through exchanging different views, with the psychiatrist's opinion not necessarily being dominant. The diverse perspectives of patients, families, and medical staff further lead to new polyphony and a less hierarchical and more flexible dialogical environment, which we believe is a step toward health-care practice reform.
Qualifications
Although we authors believe that the PAMR worked effectively for Kenji in light of our previous study (Tsubonouchi et al., 2022), we cannot say that our method alone was responsible for his improvement. It could be said that Kenji solved the problem on his own, or time may have solved the problem, or other factors may have contributed. However, what seems remarkable is that the psychiatrist tried to make his patient experience PAMR with a sense of adventure, and that the psychiatrist himself entered into the process of PAMR, which led him to see the patient from a different angle and to develop a new perspective on his own psychiatric care. This may indicate the possibility of a new form of psychiatry, namely the formation of a therapeutic allyship that allows psychiatrists to work collaboratively with psychiatric nurses.
Conclusion
It should be underscored that psychiatric nurses are best suited to writing PAMRs with patients and to playing the role of partner by warmly evaluating the patient's state and remaining present. Psychiatric nurses can easily assume a not-knowing position, and writing PAMRs can become an exclusive technique for them that could represent their professional identity. Patient-Authored Medical Records reveal a new alliance between psychiatric patients and medical personnel, moving from an authoritative and unidirectional relationship to a more egalitarian reflective and polyphonic relationship, which may promote health-care practice reform.
The PAMR process, rooted in family therapy, represents a collaborative therapeutic discourse in which the patient's prescription for care is written jointly with the psychiatric nurse, who takes the dialogical stance of not knowing and helping the patient reauthor their story. PAMRs are a collaborative product of the patient and the nurse and create alternative authorship to the prescription of the patient rather than the psychiatrist. The partnership between patients and nurses leads to allyship, providing a safe narrative space to voice their own views. The follow-up meeting makes it possible for family and other medical personnel to engage in an extended dialogue with multiple participants, which facilitates the association and teamwork of this group in supporting the patient's therapeutic environment. Above all, psychiatric patients can feel excited and liberated to write their own prescription for care, which is usually considered work reserved for psychiatrists.
Footnotes
Acknowledgments
The authors would like to thank the patients and their families, the psychiatric ward staff, and the outpatient staff for their help and cooperation in this study. The authors are also deeply grateful to Dr. Hiroshi Naito, psychiatrist, Dr. Naoki Nomura, anthropologist, and Professor Ayako Furuzawa, psychiatric nurse, for their advice on this study.
Disclosure
The authors have no relevant financial interest or affiliations with any commercial interests related to the subjects discussed within this article.
Funding
The senior author received the following funding for the research, writing, and publication of this article. This work was supported by a Grant-in-Aid for Scientific Research (KAKENHI) from the Japan Society for the Promotion of Science (JSPS). Grant number 16K15975.
Author Biographies