
Abstract
Interventions that aim to address equity, diversity, and inclusion (EDI) within the health professions often strive to promote the retention, recruitment, and success of individuals from historically underrepresented groups, who often belong to the same groups experiencing underservicing in health care. A pilot study aimed to examine the impact of ongoing EDI initiatives at Dalhousie University in Nova Scotia, Canada by exploring sense of belonging and curricular inclusion/representation from the perspectives of enrolled students. Intersectionality Theory was operationalized by way of considering the relational and contextual nature of marginalization. Results showed differences in perceptions of impacted sense of belonging and curricular inclusion/representation of diverse groups between respondents in the underrepresented subgroup as compared to their overrepresented counterparts. Differences in underrepresented and overrepresented subgroups’ perceptions of impacted sense of belonging and curricular inclusion/representation suggest a need for further research to better understand the impact of EDI interventions on nursing students.
Implications for Practice and Research
Equity, diversity, and inclusion (EDI) initiatives can be evaluated for their effectiveness by exploring whether their intent and impact align and to promote their evidence-informed planning and implementation. Institutional performance in achieving EDI-related strategic planning goals can be monitored by exploring individuals’ sense of belonging and perceived curricular inclusion/representation in addition to tracking recruitment and retention numbers. Intersectionality Theory can be operationalized to facilitate a nuanced consideration of the relational and contextual nature of marginalization and mitigate the reduction of statistical power when larger sample sizes are not feasible.
Interventions related to equity, diversity, and inclusion (EDI) include those that aim to benefit groups historically underrepresented in health-related professions, and developing methods to evaluate their effectiveness and support their success is critical (Cain et al., 2022; Francis et al., 2022; Oikelome et al., 2022; Raine et al., 2022; Tamtik & Guenter, 2019). There is extensive work related to EDI being carried out within Canadian universities (Tamtik & Guenter, 2019), and the School of Nursing at Dalhousie University (DSoN) in the province of Nova Scotia is no exception. This article discusses a pilot study (conducted by DSoN students belonging to groups historically underrepresented within the health professions) that aimed to promote evidence-informed planning and implementation of future EDI interventions, collaboration between students and faculty, and inclusion excellence within DSoN, the university, and the nursing profession more broadly. Students’ perceptions about ongoing EDI initiatives were evaluated using the following variables: (1) identity (race/ethnicity and gender/sexual orientation), (2) sense of belonging, and (3) curricular inclusion/representation. An intersectional analysis that took contextual power relations into account was generated and comparisons were made between students’ perceptions of impacted sense of belonging while at DSoN and curricular inclusion/representation of diverse groups.
Background
Group representation is closely linked to individuals’ sense of belonging; more representation can contribute to an enhanced sense of belonging, while lower group representation can increase feelings of being othered (Glasford, 2021). However, the way representation comes about matters because it impacts how historically underrepresented groups are included (Scott & Zerwic, 2015; Zou & Cheryan, 2015). For example, inclusion may be harmful if representation comes about in a way that confirms negative stereotypes. When attempts are made to be inclusive of members of historically underrepresented groups, particularly when these efforts are made by those perceived as belonging to relatively larger or more powerful groups, there can be interpersonal consequences that impact sense of belonging (Glasford, 2021; Zou & Cheryan, 2015). In classroom settings, this could include putting a minoritized student on the spot and asking them to speak on behalf of the population to which they are perceived to belong, which risks creating an exclusionary distinction between one student and the rest of the class. This approach can make minoritized students feel tokenized, singled out, or as if they do not belong in their programs of study, which undermines their retention and success (Bryant et al., 2021; Caple & Tian, 2021; Guest, 2002; Isik et al., 2021; Kroll & Plath, 2022; Meynard et al., 2021; Singer et al., 2020; Wong et al., 2021).
DSoN is implementing ongoing EDI interventions that aim to align with broader initiatives happening within the university. Principles to which Dalhousie University has expressed commitment informed this evaluation of ongoing EDI interventions. In 2015, Dalhousie University released a report called Belong: Supporting an Inclusive and Diverse University (Dalhousie University, 2015), precipitated in part by a scandal within the university that revealed a normalization of sexual violence against women that became part of a national conversation on the pervasiveness of misogynistic cultures. The report stated a commitment to five principles that were used during its development: (1) sharing in the responsibility within the community to bring about change, (2) committing to inclusivity and respectfulness within the university, (3) building from insights and lessons learned within and across academic institutions, (4) acknowledgement of normalized social attitudes that uphold systems of oppression, and (5) recognizing that the university is situated within a broader social context that reinforces systemic barriers to eradicating structural inequalities (Dalhousie University, 2015). More recently, Dalhousie's Third Century Promise included establishing and maintaining a foundation for inclusion and distinction (Dalhousie University, 2021). Nursing's professional duty to participate in sociopolitical activism (Ballou, 2000), ongoing initiatives within DSoN (Dalhousie School of Nursing, n.d.; Lane & Waldron, 2021; Thomson, 2021), and EDI-related strategic planning within the university more broadly (Dalhousie University, 2021) invited an exploration of how an institution's performance in achieving their EDI goals might be evaluated beyond recruitment and retention.
A Note About Language
Much like the reason for adopting perceived sense of belonging and curricular inclusion/representation, various terms are used throughout this article for the purpose of contextual alignment. To assist with readability, these terms will be explained here. The language of “diverse groups” refers to any heterogeneous group of people and for the purpose of institutional alignment, is synonymous with diverse populations/communities (Dalhousie School of Nursing, 2015, 2018). “Under-” or “overrepresented” groups/populations/communities are determined here in accordance with the general population in the study's broader social context (using census data). “Over-” or “underserved groups” is meant to convey differential access to resources. The authors acknowledge the reductive nature of these terms, but also stress that these terms are being strategically adopted in so far as further detail was not possible without risking anonymity of responses. It should also be noted that these terms are not being used to suggest anything about the groups or populations in and of themselves.
While the language of “marginalized population” may be regarded as more acceptable than “underrepresented group” (Nwangwu, 2023), the former assumes the impact that the context is having while the latter is merely a means by which the broader social context of the study that reinforces systemic barriers to eradicating structural inequalities can be recognized. As Luna (2009) explains, the manner in which the label is being used matters. Terms being used here are thus meant to be relational only with respect to the study's broader social context, from which power relations shaping outcomes extend into the university, and DSoN more specifically. As such, the language used in this article is intentionally employed, meant to reflect the broader social context of the study, its impact on individuals (if any), and is a consequence of the analytic strategic used to capture the complexity of power relations within the limitations of a pilot study.
Methods
This study was a survey-based, cross-sectional observational pilot study that sought to explore the impact of EDI initiatives happening within DSoN using sense of belonging and perceived curricular inclusion/representation. Emerging from Black Feminist Scholarship, Intersectionality Theory is a philosophical perspective that confronts social injustice by exploring domains of power operating across multiple forms of oppression and uses dimensions of dominance as an analytic tool for exposing contextual inequalities that impact outcomes (Bowleg et al., 2023; Christoffersen & Hankivsky, 2021; Collins & Bilge, 2020; Crenshaw, 1991; Waldron, 2018). Such an exploration aligns with this pilot's objectives because domains of power operating across multiple forms of oppression are thought to shape how groups are represented and members’ thereof sense of belonging.
Ethical Considerations
Ethics approval was obtained prior to recruitment through the Research and Scholarly Development Committee at the DSoN under an ethics review process that is in place for course-based research that poses a minimal risk to participants, such as this pilot, which was a partial requirement for an undergraduate independent study course. Nursing students at Dalhousie University were invited to complete the survey. Consent explained voluntary participation, (including clarification that questions could be skipped), that the survey could be stopped at any time, a person could remove themselves from the study by simply closing their browser, and incomplete surveys would not be included in the analysis. Consent also explained that the survey was anonymous (clarifying that a person could not be removed from the study once they submitted their survey responses), only general findings would be reported, and that responses would be stored on secure servers that belong to the university. Consent was obtained before respondents were given access to survey questions.
Operationalizing Intersectionality Theory
An anti-categorical approach was used to manage intersectional complexity (McCall, 2005) and thus strategically essentialize identity categories (Bowleg et al., 2023; Cho et al., 2013, p. 2; Collins, 1990; Collins & Bilge, 2020; Spivak, 1988; Voronka, 2016) for the purpose of exploring the impact of DSoN EDI initiatives. Intersectionality Theory was operationalized using the following steps: (1) adopt social categories of identity, (2) identify socially constructed differences (i.e., subcategories) within each category that exist within the broader social context of the study, and (3) strategically essentialize subcategories into two-category variables to generate an intersectional analysis of sense of belonging and curricular inclusion/representation that considers the broader social context of the study. Figure 1 illustrates an overview of the process by which two-category variables were created.
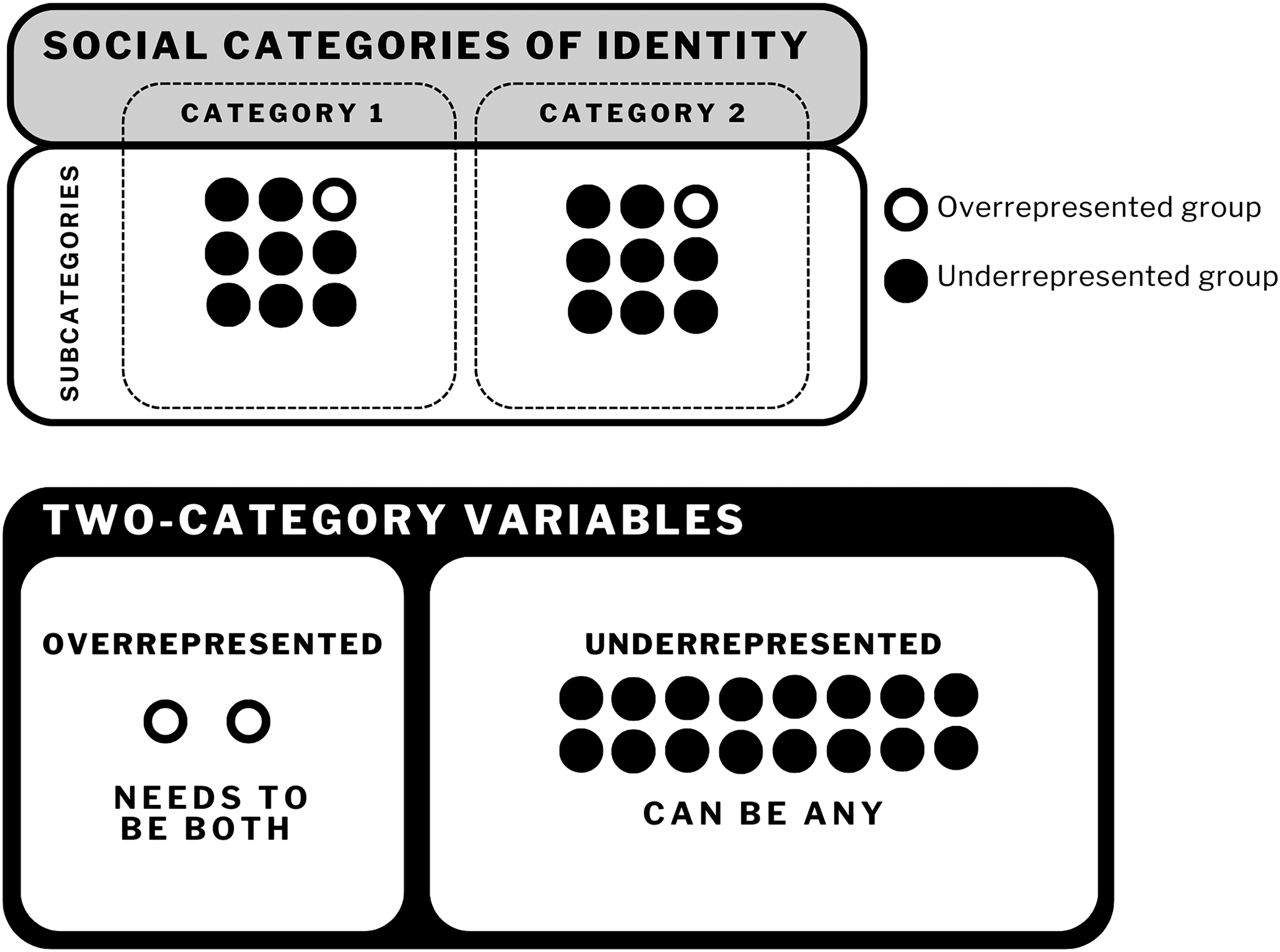
Process of operationalizing intersectionality theory used in this pilot study. Social categories and subcategories of identity were adopted and defined in relation to the general population in the broader social context of the study.
Race/ethnicity and gender/sexual orientation were the adopted social categories of identity, and within each, subcategories were assumed according to the broader social context (for race/ethnicity: Asian, Black, Caucasian, Hispanic, Indigenous, race/ethnicity not listed; for gender/sexual orientation: asexual, bisexual, cisgender, gay, heterosexual, lesbian, man, nonbinary, pansexual, queer, trans, Two Spirit, woman, gender not listed, sexual orientation not listed). Intersectional complexity was managed by establishing a common standpoint on domination within the sample population (Collins, 1990; Spivak, 1988; Voronka, 2016; Waldron, 2002), and strategically adopting binary thinking (Adorno, 1973; Haraway, 1988; Nietzsche, 1997). This analytic approach was employed to create oppositional points of comparison that mutually constitute and uphold one other, just as power relations do.
An overrepresented subcategory within each identity category was defined (once again, in accordance with the broader social context) to create an overrepresented subgroup comprised of individuals who only belong to overrepresented groups. “Caucasian” was defined as the overrepresented subcategory within the race/ethnicity category insofar as the majority of the population in Nova Scotia self-identifies as having European ethnic or cultural origins (Bhopal & Donaldson, 1998; Government of Canada, 2022b). Non-2SLGBTQ (i.e., cisgender and heterosexual) was defined as overrepresented within the gender/sexual orientation category; cisgender is the dominant gender subcategory in Nova Scotia (Government of Canada, 2022a), whereas compulsory heterosexuality (Rich, 1980) was presumed due to the omission of sexual orientation as a social category of identity in the Canadian Census. Figure 2 is a visual representation of how this was done.
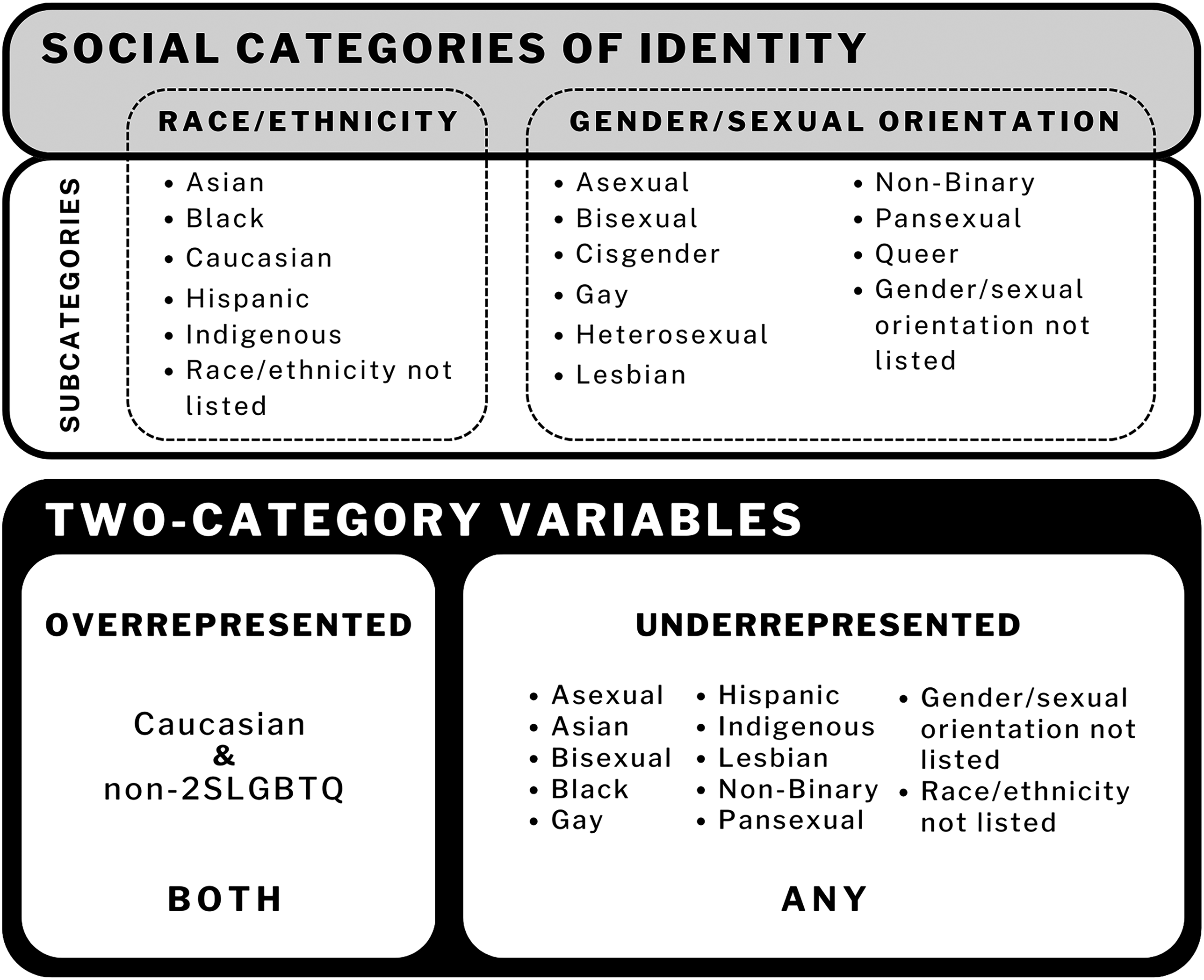
Composition of two-category variables created from reconceived subcategories.
Participants
Current undergraduate or graduate nursing students at one of the three Dalhousie University campuses were eligible to participate (two in the province of Nova Scotia and one in the territory of Nunavut).
Data Collection
Demographic survey questions were worded as “select all that apply” and mirrored adopted identity categories and subcategories. Dalhousie's ongoing efforts to achieve inclusion excellence informed the development of yes or no (Y/N) questions on sense of belonging and the representation/inclusion of diverse groups in nursing curricula. Due to the subjective nature of sense of belonging, the phrase was intentionally left undefined to allow respondents the space to interpret it themselves and find their own meaning in the questions. If a respondent indicated that their sense of belonging had been impacted during their time in DSoN, then they were asked if they attributed a lost sense of belonging to aspects of their identity. If a respondent indicated that they felt diverse groups were included and represented in the DSoN curriculum, a Y/N question asked if respondents’ inclusion of diverse groups in the nursing curriculum made them feel equipped to work with people who belong to diverse populations. If a respondent indicated that they felt diverse groups were not included/represented in the DSoN curriculum, then a Y/N question asked respondents if they felt curricular gaps would impact their future nursing practice.
The survey was distributed by DSoN staff on behalf of the researchers, through student listservs, across all nursing programs (undergraduate and graduate) at Dalhousie University's three nursing campuses. The study took place over the course of one term, with a resulting recruitment period of October 20 and November 16, 2021. The email included a link to the survey and recruitment poster. Respondents were asked to self-identify across social categories. Self-identification questions were not intended to be exhaustive, rather the rudimentary collection of demographic data was strategic in that differences would be captured, reconceived as similar by recategorizing them into two-category variables.
Data Analysis
Demographic data were analyzed using descriptive statistics and were also used to create subgroups that made it possible to perform chi-square independence tests to test for associations between the impact of representation within the broader social context of the study and perceived sense of belonging and curricular inclusion/representation of diverse groups within DSoN.
Results
Data were collected from Halifax and Yarmouth campuses at Dalhousie University (n = 36). There were no responses from the Nunavut campus, the smallest of the three nursing campuses at Dalhousie University. Enrollment at the time of the study in all nursing programs across the three campuses was a total of 677, giving a response rate of 4.7%. The most frequently observed age range among participants was 16–20 years old (52.8% of participants). The sample exhibited less diversity in terms of gender, with a minority identifying as gender diverse (8.3%). A majority of participants identified as heterosexual (63.9%), and 61% identified as Caucasian. Individuals underrepresented in one subgroup may be well represented in others (i.e., Caucasian respondents could be a sexual and/or gender minority and thus overrepresented in one category while being underrepresented in the other). Multiple indicators were accounted for by reconceiving the sample into two subgroups that rejected conventional identity categories, resulting in the reorganization of subcategories into two-category variables. This facilitated a nuanced consideration of the relational and contextual nature of marginalization, and resulted in 24 people being included in the underrepresented subgroup and 12 people in the overrepresented subgroup. Racial/ethnic diversity within the sample population existed across all subcategories (i.e., Asian, Black, Caucasian, Hispanic, Indigenous, and race/ethnicity not listed). Gender diversity within the sample included cisgender men and women, nonbinary, queer, and gender not listed. Diversity in terms of sexual orientation included asexual, bisexual, gay, heterosexual, lesbian, pansexual, queer, and sexual orientation not listed. No one self-identified as trans or Two Spirit. Demographics are intentionally reported without specific numbers for each subcategory due to the small sample size and risk of compromising anonymity of responses (see Figure 3).
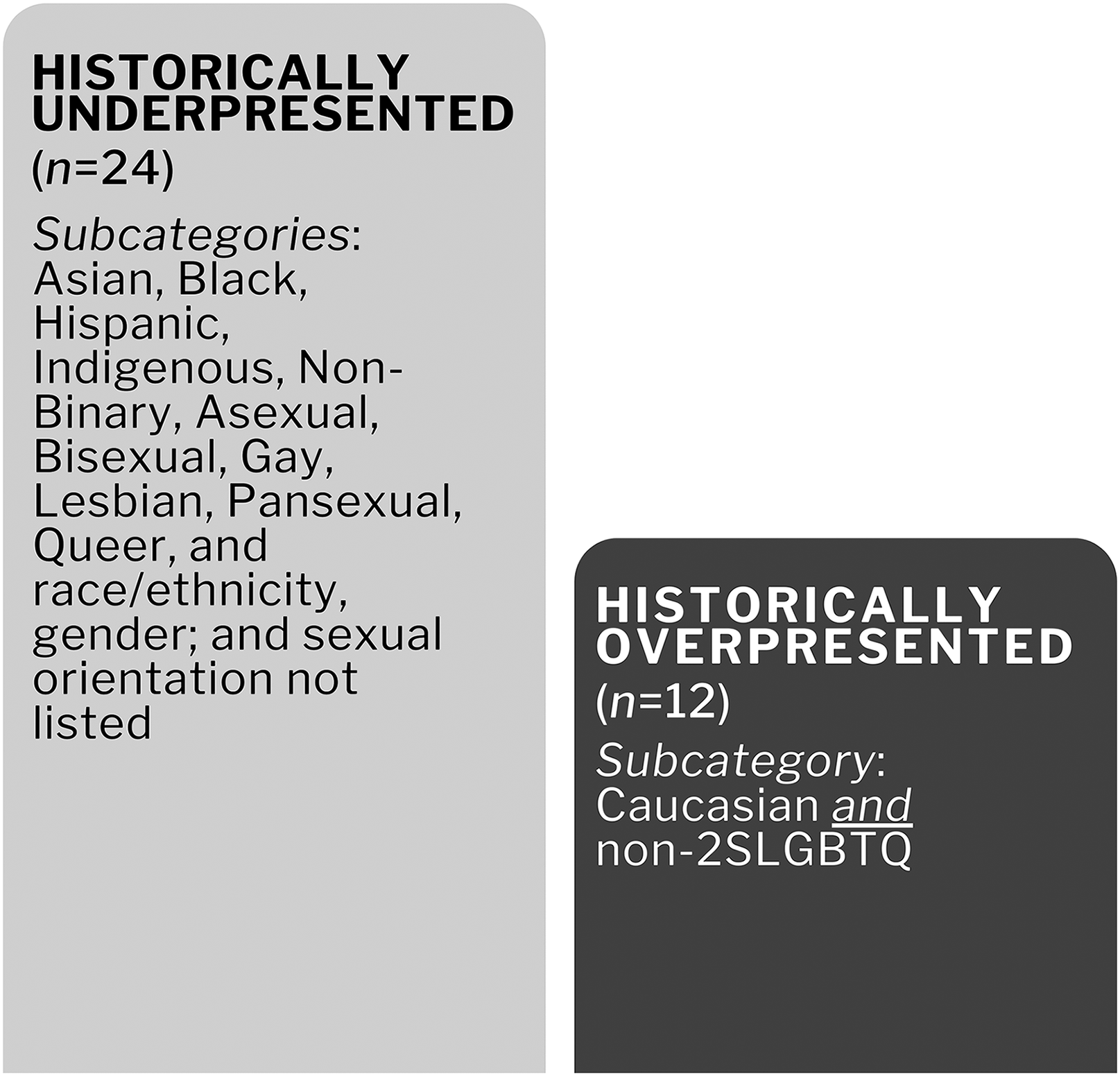
Graphical representation of subgroup composition.
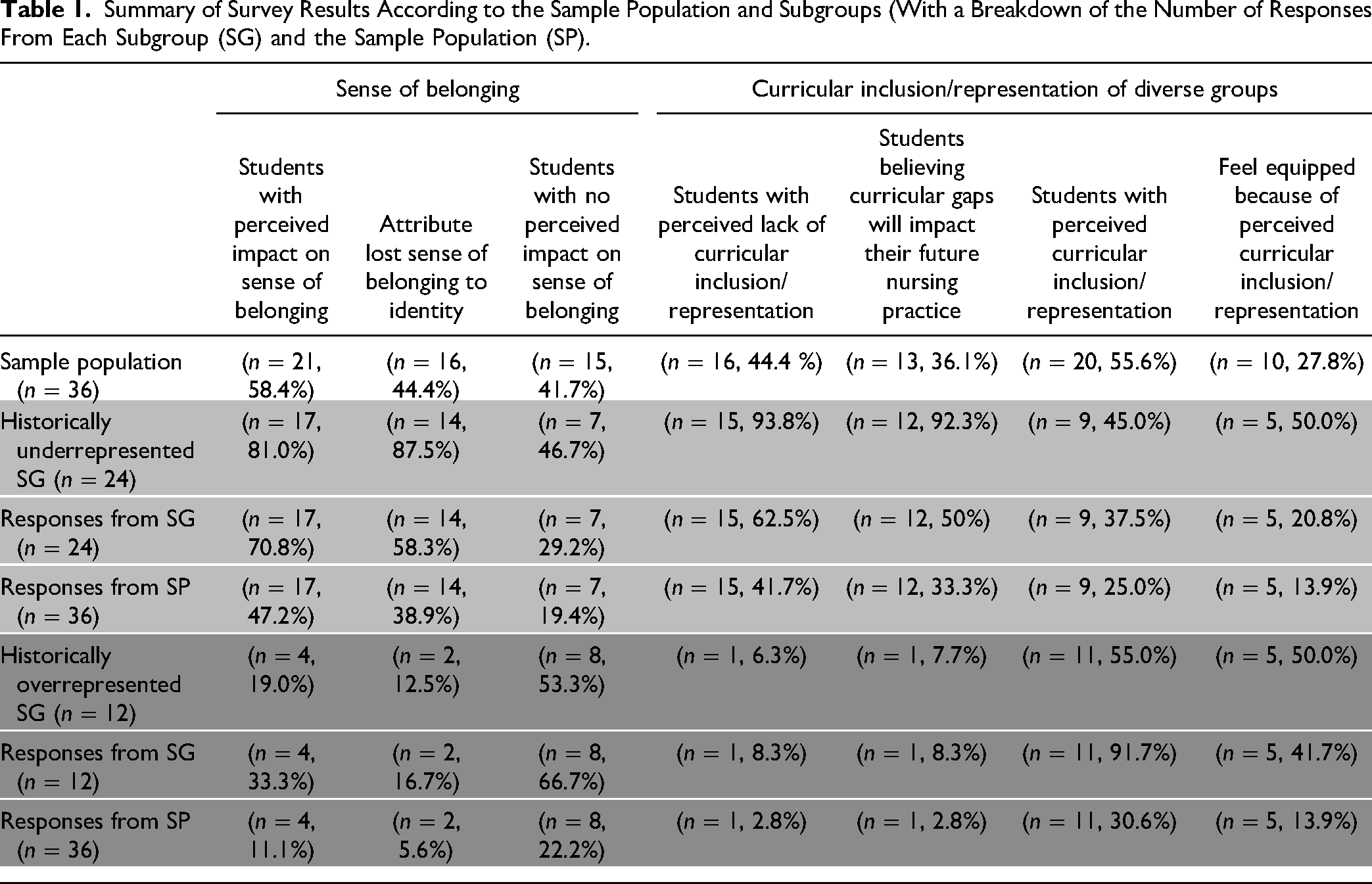
Survey results are summarized in Table 1.
Summary of Survey Results According to the Sample Population and Subgroups (With a Breakdown of the Number of Responses From Each Subgroup (SG) and the Sample Population (SP).
Sense of Belonging
In total, approximately 58% of the sample (21/36) perceived their sense of belonging to be impacted in one way or another during their time at the DSoN; of these responses, 81% (17/21) came from the historically underrepresented subgroup as compared to 19% (4/21) from the historically overrepresented subgroup. Chi-square independence tests suggest an association between representation and perceived impact on sense of belonging in the DSoN (p = .031). In total, 81% of respondents who perceived an impact on their sense of belonging were from the underrepresented subgroup (Figure 4).
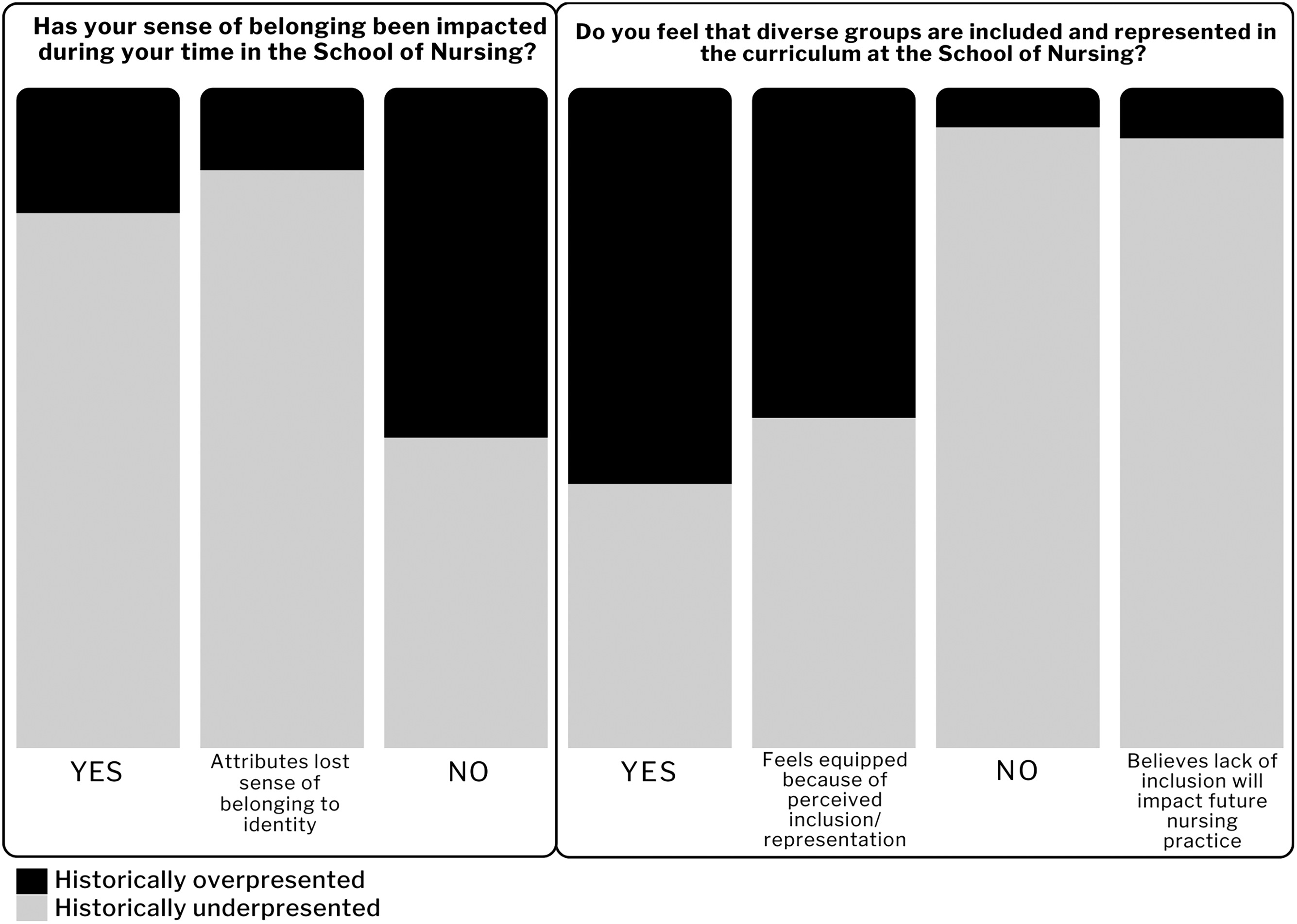
Results by historically overrepresented and historically underrepresented subgroupings.
Respondents who perceived their sense of belonging to be impacted represented 70.8% (17/24) of the underrepresented subgroup as compared to 33.3% (4/12) of the overrepresented subgroup. Approximately 44% (16/36) of the sample perceived their sense of belonging to be impacted and attributed losses to their identity; of these responses, 87.5% (14/16) were from the underrepresented subgroup. Respondents attributing perceived impact on sense of belonging to their identity represented 58.3% (14/24) of the underrepresented subgroup as compared to 16.7% (2/12) of the overrepresented subgroup.
Curricular Inclusion/Representation
The perceived curricular inclusion/representation variable was found to be strongly associated with subgroupings (p = .002). Among all, 44% (16/36) of the sample perceived a lack of inclusion/representation; of these responses, 93.8% (15/16) of these responses were from the historically underrepresented subgroup, and 6.3% (1/16) belonged to the historically overrepresented subgroup. Respondents who perceived a lack of curricular inclusion and representation of diverse groups represented 62.5% (15/24) of the underrepresented subgroup as compared to 8.3% (1/12) of the overrepresented subgroup (Figure 4). When asked if the curricular gaps they perceive would impact their future practice, 81.3% indicated yes, 18.8% were unsure, and 0% indicated no.
Fifty percent (10/20) of respondents (28% of the total sample population) who perceived curricular inclusion/representation of diverse groups felt equipped to work with these populations because of the inclusion/representation (45% unsure, 25% of the total sample population; 5% unequipped, 3% of the total sample).
Discussion
Findings reveal an association between representation and DSoN students’ perceptions of impacted sense of belonging (p = .031) and curricular inclusion/representation of diverse populations (p = .002). However, findings lack generalizability with a response rate as low as 4.7%. The implications of conducting course-based (non-thesis) research over the course of one term meant limiting the purpose of the project, which included promoting evidence-informed planning and implementation of future EDI interventions within the DSoN, the university, and the nursing profession more broadly. Differences in perceptions suggest more investigation is needed to further explore equitable approaches to establishing and maintaining a foundation for inclusion and distinction. Given ongoing efforts and nursing's duty to participate in sociopolitical activism, the DSoN may be uniquely positioned to explore strategies for evaluating the effectiveness of EDI initiatives and develop interventions that can better support an ever-diversifying student body and thus workforce in health care. Further investigation would also allow for the exploration of additional statistical testing methods that would go beyond what was possible in this pilot study, which was unfunded and conducted by students over the course of one term as they progressed through their respective programs.
When 93.8% of respondents who felt that diverse groups are not included/represented in curricula belong to groups that make diversity possible, further investigation is warranted to understand how sense of belonging and curricular inclusion/representation of diverse groups impacts the learning experiences of students, particularly those from historically underrepresented groups. Furthermore, when 50% of respondents who perceived curricular inclusion/representation of diverse groups feel equipped to work with these populations because of the inclusion/representation, this suggests that nurses may not feel prepared to address diverse health needs, even when they perceive curricular inclusion/representation of diverse groups.
Retaining contextual social distinctions (through which power operates) that are known to exist in the broader social context that an institution is situated within allows for a relational consideration of power relations that may be influencing the impact of EDI initiatives on individuals. Operationalizing Intersectionality Theory in ways that retain social distinctions capture the nuances of power relations as they relate to the complexity of identity (Guan et al., 2021) in accordance with studies’ broader social contexts and can thus be used to emphasize the impacts of marginalizing power relations. As such, considering the broader social contexts of a study in this manner might also help to inform ongoing EDI initiatives and provide a more nuanced evaluation than what is possible with recruitment and retention numbers.
Notably, the size of the sample dictates the degree to which Intersectionality Theory can be operationalized. Small sample populations may limit intersectional analyses, but anti-categorical approaches (McCall, 2005) could be an additional strategy to mitigate the reduction of statistical power when larger sample sizes are not feasible (Di Leo & Sardanelli, 2020). Larger sample sizes may, however, promote complex intersectional analyses, pose less of a risk to the confidentiality of responses (a critical consideration in this pilot study), and uncover unique and/or common experiences of oppression between and within groups. Larger sample sizes might also make it possible to adopt more social categories of identity, and thus support regression model analyses, whereas using just two social categories of identity limit statistical analyses to chi-square tests (and thus p values).
Further investigation is recommended to explore whether there are similar discrepancies across health-related disciplines or if this is an issue that is unique to the DSoN. Future work could also involve the formation of task forces to develop surveys (Andrews Rhoten et al., 2023) that include questions asking about the positive or negative impacts on perceived sense of belonging–not unspecified as was done in this pilot study. Leaving sense of belonging undefined (e.g., impact on sense of belonging was presented neutrally, instead of positively or negatively), however, revealed that members of underrepresented groups may be more responsive to effective EDI interventions because more respondents in this subgroup perceived their sense of belonging to be impacted as compared to the historically overrepresented subgroup. This suggests that if the impact of EDI initiatives aligns with their intent, then the recruitment, retention, and success of historically underrepresented groups may disproportionately increase as compared to individuals belonging to overrepresented groups.
Measuring how effectively an intervention is in advancing health equity and thus bringing about the benefits that come with having a diverse health care workforce (Farlow et al., 2023; Fontenot & Mastorovich, 2024; Jennings et al., 2024) could be how institutional performance in achieving EDI-related strategic planning goals. Institutional performance in establishing and maintaining foundations for inclusion and distinction might also be further explored by including additional social categories of identity. For example, adding the social category of identity of citizenship to the analysis would further complicate intersectional analyses of domains of power operating across multiple forms of oppression within a context whereby dominant cultures perpetuate structural inequalities globally (Christou, 2016; Collins & Bilge, 2020). This might tease out the experiences of international students, who experience unique barriers to education that are different from students whose citizenship matches that of the institutions in which they study, such as differential course fees, cultural barriers to inclusion, and diminished social support. Nuanced operations of context power relations are likely to be uncovered if other social categories, such as (dis)ability were also adopted. However, in future research and larger studies, additional terms (i.e., more specific than under- and overrepresented) should be adopted in accordance with adopted identity categories to support an even more nuanced consideration of broader social contexts and power relations therein that influence the effectiveness of EDI initiatives.
Conclusion
Findings reveal that students from historically overrepresented groups and historically underrepresented groups have different perceptions of their sense of belonging and curricular inclusion/representation of diverse groups at DSoN. Those respondents who self-identified as members of underrepresented groups perceived a greater lack of curricular inclusion/representation at DSoN compared to those in overrepresented groups. Results of this study could support evidence-informed planning and implementation of EDI interventions being carried out within health educational institutions. There is a need to monitor performance in establishing and maintaining foundations for inclusion and distinction and advance EDI initiatives by exploring their impact within health education institutions. This may be a critical step to determining if health equity will be enhanced within and across health systems by promoting the recruitment, retention, and success of those from groups historically underrepresented in the health professions.
Footnotes
Acknowledgements
The authors would like to acknowledge Dr. Ingrid Waldron for her mentorship, the ongoing wisdom she shares, and messaging of her work. Dr. Ruth Martin-Misener, Director of the School of Nursing at Dalhousie University, and Dr. Megan Aston, Acting Associate Director Graduate Programs also provided invaluable support to this project.
Author Contributions
Dr. Jennifer Lane performed writing–original draft and review and editing, conceptualization, methodology, investigation, formal analysis, data curation, visualization, supervision, and project administration. Dr. Neda Alizadeh performed writing–original draft and review and editing, formal analysis, and provided resources. Anika Daclan and Adam Vickery performed conceptualization, investigation, and project administration.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding acknowledgements include the Killam Trusts, Electa MacLennan Memorial Scholarship, Dalhousie School of Nursing, and Dalhousie School of Nursing Research Fund.