
Abstract
Background:
Intimate partner violence (IPV) is a significant public health concern, particularly in vulnerable populations such as Chinese immigrant women.
Aim:
This study aimed to assess the feasibility and acceptability of an empowerment-based intervention integrated with relaxation and self-compassion techniques for Chinese immigrant women experiencing IPV.
Methods:
The present study was a part of a pilot randomized controlled trial (RCT). A total of 50 Chinese immigrant women who had experienced IPV in the past year were recruited online and randomized to either the intervention or the control group. The intervention group engaged in seven weekly sessions delivered with a phone call and a mobile application. Quantitative and qualitative data were collected through surveys and interviews to evaluate intervention adherence, participants’ perceptions, and areas for improvement.
Results:
64% of the participants completed each weekly session, demonstrating favorable intervention adherence. The intervention was perceived to be helpful by most participants, with reported decreases in stress, anxiety, fatigue, pain, and family conflicts, and with reported improvements in emotion regulation and self-compassion. However, technical issues with the mobile platform and lack of personalization were identified as limitations.
Conclusion:
This study demonstrates the feasibility and acceptability of the intervention for Chinese immigrant women experiencing IPV and warrants a full-scale RCT to determine its efficacy. It will be essential to personalize the intervention and reduce any barriers to participation.
Introduction
Intimate partner violence (IPV) is defined as physical violence, sexual violence, and/or psychological aggression or coercion by a current or former intimate partner (Breiding et al., 2015). IPV against women is more common, and women face a greater risk of experiencing severe physical violence, injuries, and homicide in the context of IPV, making them more vulnerable and in greater need of medical care and legal services (National Coalition Against Domestic Violence, 2020).
IPV Among Chinese Immigrant Women
In the U.S., the largely overlooked and underserved population of more than 4 million Chinese immigrants (Hoeffel et al., 2012) is especially vulnerable to IPV. Limited research suggests a high prevalence of IPV in this population, with very limited help-seeking behaviors (Y. Li et al., 2020, 2021). In 2019, a study of 475 Chinese immigrant women residing in the U.S. reported an IPV prevalence of more than 20% in the past year (Y. Li et al., 2020). Chinese immigrant women may face an increased risk of IPV due to the impact of cultural and patriarchal values, such as male dominance and rigid gender norms. In addition, immigration and acculturative stress, including language barriers, limited economic resources, and social isolation, may further contribute to their vulnerability (Y. Li et al., 2020). Moreover, women infrequently sought help due to shame, privacy concerns, limited English proficiency, legal or financial dependence on an abusive partner, lack of familiarity with available resources, and absence of culturally appropriate services (Y. Li et al., 2021). To our knowledge, no studies have explored supportive interventions to help Chinese immigrant women deal with IPV and its associated mental health consequences. The development of innovative, culturally appropriate, acceptable, and accessible interventions that address such barriers is essential for this underserved group of women.
Gaps in IPV Interventions: Unmet Mental Health Needs Among Survivors
Violence against women is characterized by coercive control exerted by abusive partners. Empowerment-based interventions such as the Domestic Violence Enhanced Home Visitation (DOVE) program are designed to enhance women’s independence and control, thereby reducing re-victimization (Sharps et al., 2016). Grounded in Dutton’s (1992) empowerment theory, the DOVE intervention emphasizes women’s autonomy and decision making. Women’s ability to make decisions and use resources to ensure their safety can be strengthened by providing IPV information, conducting danger assessments, offering options and resources, and assisting in the development of individualized safety plans. This can in turn reduce the risk of IPV and promote safety behaviors. However, current empowerment-based interventions have not sufficiently incorporated mental health resources and techniques to address the mental health needs of abused women (Parker et al., 1999; Sharps et al., 2016; Tiwari et al., 2010).
IPV has been linked extensively to adverse mental health outcomes such as depression, anxiety, and posttraumatic stress disorder (PTSD; Chan et al., 2010; Y. Li et al., 2022). Frequently, abused Chinese immigrant women tend to tolerate abuse and may not desire to end their abusive relationships, which can result in long-lasting effects on mental health (Y. Li et al., 2022). Integrating mental health resources and techniques into empowerment-based interventions can not only empower women to protect themselves from further victimization but also offer them ways to cope with the adverse impacts of IPV on their mental health.
Culturally Appropriate Solutions for Meeting the Mental Health Needs of Chinese Immigrant Survivors
Influenced deeply by the cultural value of criticism and self-criticism in Chinese culture, Chinese immigrant women often tend to blame themselves for violence that they experience, and this leads to mental health issues such as depression (Y. Li et al., 2022). Given this tendency toward self-criticism, the practice of self-compassionate meditation may be particularly beneficial for Chinese immigrant women when they cope with IPV (Neff, 2003). In addition, techniques of relaxation such as deep breathing, progressive muscle relaxation, and visualization can help alleviate tension in the body and mind and promote feelings of relaxation, joy, optimism, and being energized. Research has demonstrated the efficacy of practices for self-compassion and relaxation in mitigating depressive symptoms, anxiety, and PTSD (Klainin-Yobas et al., 2015; Neff & Germer, 2013; Niles et al., 2018). Together, the integration of self-compassion and relaxation techniques into empowerment-based interventions holds promise as a culturally appropriate way for reducing the effects of IPV on Chinese immigrant survivors’ mental health.
Mobile Health: Addressing Challenges in Accessing Support for Chinese Immigrant Survivors
When one designs and implements an IPV intervention for abused Chinese immigrant women, it is important to consider unique challenges related to geographic dispersion, stigma, and privacy concerns. These women are geographically dispersed, posing challenges to efficient, cost-effective interventions. Language barriers, stigma, shame, and privacy concerns can discourage them from disclosing their abuse and seeking help (Y. Li et al., 2021). To address these challenges, mobile health offers the promise of targeted support with high flexibility, accessibility, and efficiency (Silva et al., 2015); it enables self-care regardless of time or place. By overcoming challenges related to geographic dispersion, stigma, and privacy, mobile health presents a potentially ideal support for this vulnerable group of women. Compared to face-to-face methods, mobile health IPV interventions offer greater efficiency, and previous mobile-based interventions for IPV have shown promising feasibility and acceptability among survivors (Anderson et al., 2021; Emezue et al., 2022). However, there is a lack of culturally and linguistically appropriate mobile health interventions tailored for Chinese immigrant survivors.
In the study that we report here, we tested the Self-Compassion, Health, and Empowerment (SHE) intervention, in which we have adapted the structured DOVE IPV intervention and incorporated self-compassion and relaxation techniques for Chinese immigrant women experiencing IPV. This is the first study designed to both reduce IPV and meet the mental health needs of Chinese immigrant survivors. In this paper, we examine the feasibility and acceptability of the SHE intervention for reducing IPV and improving the mental well-being of abused Chinese immigrant women.
Method
Design
We conducted this mixed-methods study from March 2022 to March 2023, using a two-arm randomized controlled design. All participants completed an online survey at baseline, immediately post-intervention, and at 8-week follow-up. Qualitative interviews were conducted over the phone with participants in the intervention group immediately post-intervention. Here, we focus on feasibility and acceptability; detailed information about methods and preliminary efficacy can be found elsewhere (Y. Li et al., 2024). The study is registered in ClinicalTrials.gov (ID: NCT05011552).
Participants, Recruitment, and Randomization
Participant inclusion criteria were: 18 years of age or older, self-identified as Chinese, currently residing in the U.S., currently in an intimate relationship, and experienced IPV within the past year. IPV was screened using the Chinese version of the Abuse Assessment Screen (AAS; Tiwari et al., 2007). If women answered “yes” to being emotionally, physically, or sexually abused by an intimate partner in the past year, they screened positive for IPV. One question was designed to screen whether women are having difficulty with substance use or suicidality or having been in mental health care for severe mental illness. Those who reported substance use, suicidality or who had received treatment for severe mental illness were excluded from the study, as mindfulness mediations may pose potential risks of deteriorating symptoms (Binda et al., 2022). Based on a previous empowerment-based intervention for abused Chinese women in Hong Kong (Cohen’s d = 0.2; Tiwari et al., 2010), we aimed for 20 participants per arm to achieve 80% power (Whitehead et al., 2016). Considering a potential 20% dropout rate, we recruited and randomized 25 participants per arm.
Participants were recruited online mostly through WeChat advertisements, with a very small number from platforms such as Prolific and the Collaborative Approach for Asian Americans & Pacific Islanders Research & Education (CARE) registry. Our online flyer, with a link and a Quick Response (QR) code, directed individuals to an eligibility survey. Interested individuals completed a set of questions (i.e., age, gender, identity, residential place, current intimate relationship status, experiences of IPV within the past year, substance use, suicidality, and severe mental illness) to confirm eligibility. Those who were ineligible were directed to the “Thank You” page and exited from the survey. This page provided information on IPV and women’s health resources. Eligible women were directed to a separate page that offered a brief overview of the study. They were given the option to indicate their willingness to be contacted by the research team for further participation, along with their safe contact information (e.g., a safe phone number or email to which the abusive partner had no access), preferred time for contact, and any special instructions for the research team to reach them. The page also contained a study email address and phone number, allowing potential participants to initiate contact with the research team directly if they preferred not to disclose their contact information on the page.
Before the initial phone call, eligible participants were randomized (1:1) with computer-generated blocked randomization into intervention or control groups (Kim & Shin, 2014; Suresh, 2011). During the phone call, two separate processes were conducted for informed consent, tailored to the assigned group. Participants were blinded to their group assignment. Upon agreement to participate, they were instructed to complete the baseline assessment. The study was approved by the Institutional Review Board of the University of Texas at Austin (ID: STUDY00001645).
Treatments
The intervention consisted of seven weekly sessions. During Session 1, an IPV safety brochure was discussed with each participant over the phone; this lasted 30 to 40 minutes. After the phone call, the brochure was emailed to those who wished to retain a copy. This brochure, adapted from the DOVE study (Sharps et al., 2016), was refined with input from IPV experts and domestic violence advocates serving Asian immigrant communities. The brochure covered IPV information, questions from the Danger Assessment instrument (Campbell et al., 2009; Messing et al., 2013), safety planning, options, and available resources. In tailoring the brochure for Chinese immigrant survivors, we have also included immigrant-specific content such as immigration-related abuse, legal options for immigrants, and resources for immigrant survivors. Given that the context of IPV varies considerably, participants were encouraged to share their personal experiences, and the interventionist focused on areas where the participant had particular needs or interests. Throughout the conversation, the interventionist remained nonjudgmental and flexible; the primary goal was to provide the participant with information and emphasize available options for her to consider. The IPV safety brochure also served as a guide for the interventionist, ensuring consistency in delivery of the intervention across participants. After each phone call, the interventionist completed a brochure worksheet, documenting details such as the date, time, and duration of the call, the issues discussed, and the resource information provided. This ensured that all important information was covered and served as a measure of treatment integrity. To maintain intervention fidelity and prevent any deviation from the established protocol, the principal investigator (PI) checked the worksheets throughout the project, minimizing the potential for intervention drift.
Sessions 2-7 were delivered on a WeChat mini-program designed specifically for this intervention. WeChat is the most widely used social media application in the Chinese population (Thomala, 2023). The mini-program, hosted on the WeChat platform, incorporates basic app features and is popular because of its convenience, eliminating the need for prior downloads and sign-ups (Cheng, Schreieck, et al., 2020). Figure 1 provides a screenshot of the mini-program’s interface. Participants had the option to access the intervention in either English or Chinese, depending on their preference. The intervention’s written content is available in English and Simplified Chinese, and the spoken languages in this study were English and Mandarin.
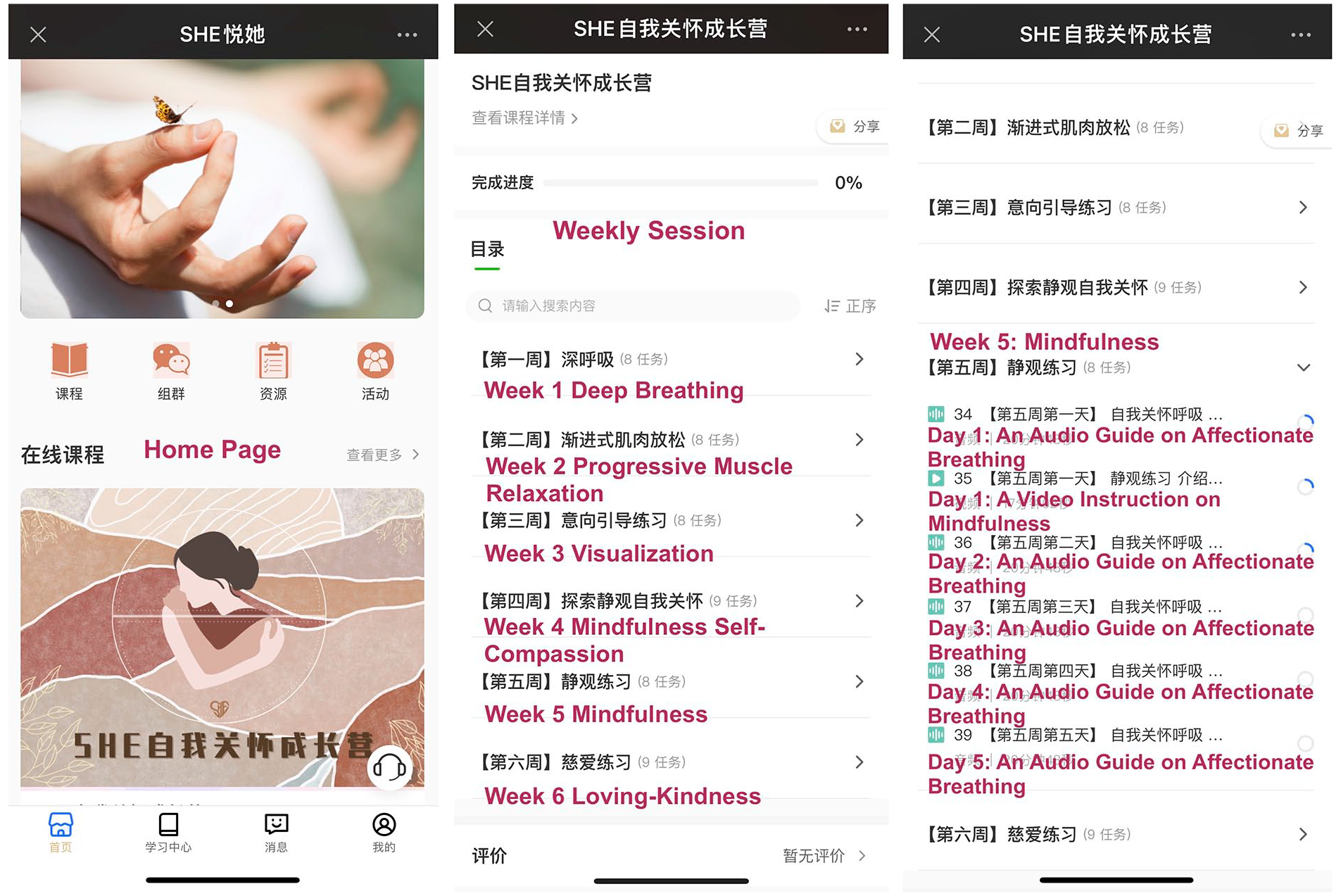
Screenshot of the WeChat Mini-Program.
The WeChat mini-program in Sessions 2 to 7 focused on mental health self-care resources, with a specific topic each week (Deep Breathing, Progressive Muscle Relaxation, Visualization, Mindful Self-Compassion, Mindfulness, and Loving-Kindness; see Figure 1). The content for deep breathing, progressive muscle relaxation, and visualization was adapted from The Relaxation and Stress Reduction Workbook (Davis et al., 2019). The content for mindful self-compassion, mindfulness, and loving-kindness was adapted from the Mindful Self-Compassion program (MSC; Neff & Germer, 2013). Both the workbook and materials for the MSC have been translated into Chinese, and the program has been successfully implemented in the Chinese population (Finlay-Jones et al., 2018). The adapted written materials were enriched through iterative feedback within the research team, involving Mandarin-speaking MSC teachers. These materials were then transformed into video and audio formats. Each session included an introduction video on one of the six topics, with accompanying audio instructions for the exercises. Six exercises were included: Deep Breathing, Progressive Muscle Relaxation, Visualization, Self-Compassion Break, Affectionate Breathing, Loving-Kindness for Ourselves. Introduction videos were 5 to 20 minutes and audio instructions ranged from 4 to 20 minutes. Participants were instructed to review the video at the beginning of each session and were encouraged to practice the exercises in each session daily for 1 week.
To facilitate adherence and engagement, weekly text messages were sent to participants, reminding them to start the new week’s session and requesting the number of exercises completed in the previous week. The participants were also asked to share feelings and/or provide feedback regarding the previous week’s exercises. Participants in the control group received a weekly email containing the same IPV safety brochure that the intervention group received, along with information about mental health self-care and resources. After they completed the study, they were offered the option to access the WeChat mini-program.
Data Collection
Feasibility
The intervention’s completion rate and the participants’ reports of any adverse events or technical issues during the study determined feasibility. During Sessions 2 to 7, participants were asked about the number of exercises they completed each week. Practice at least 4 times per week was considered completion of a week’s session. Overall completion was defined as successful completion of all 7 sessions.
Acceptability
Acceptability of the intervention was evaluated using 26 researcher-designed questions collected via an online survey immediately post-intervention. Of the 26 questions, 10 assessed perceived helpfulness of the intervention on a 5-point Likert-type scale (from 1 = not helpful at all to 5 = very helpful), 11 measured acceptability of the intervention on a 5-point Likert-type scale (from 1 = strongly disagree to 5 = strongly agree), and five open-ended questions gathered qualitative feedback on participants’ likes, dislikes, recommendations, and suggestions for improvement. These questions were initially developed based on a review of acceptability questions used in previous intervention studies and then refined by the study team. Both the questions regarding perceived helpfulness and questions regarding acceptability demonstrated high internal consistency, Cronbach’s α = .93. Total scores were computed for perceived helpfulness and intervention acceptability, to obtain an overall average of perceived helpfulness and acceptability of the intervention.
In addition to the online survey, acceptability of the intervention was assessed through semi-structured phone interviews conducted immediately post-intervention and by gathering feedback from participants via weekly messages. Specifically, semi-structured phone interviews were conducted with 15 participants from the intervention group. These interviews covered aspects such as participants’ preferences, areas for improvement, factors influencing their participation, observed changes following the intervention, and aspects of the intervention they intended to incorporate in the future. The interviews lasted approximately 20 to 30 minutes and were audio recorded.
Intervention surveys were available in both English and Simplified Chinese, and the interviews were conducted in either English or Mandarin, depending on participants’ preferences. Our survey questions and interview guide are provided in Supplements 1 and 2.
Sociodemographic Variables and Psychological Symptomatology
Sociodemographic characteristics were measured using self-reported questions collected via an online survey at baseline: age, education, employment, annual personal income, marital status, number of children, religion, nativity, and immigration status.
The Revised Conflict Tactics Scales (CTS2) were used to assess severity of psychological aggression, physical assault, injury, and sexual coercion in the past year (Straus et al., 1996). According to the CTS2 handbook, the severity level for each form of IPV is defined as follows: none, if no Minor or Severe items are endorsed; minor, if any Minor items but no Severe items are endorsed; and severe, if any Severe items are endorsed (Straus et al., 2003). Depression was measured with the Patient Health Questionnaire-9 (PHQ-9; Kroenke et al., 2001), with a total score of 10 or higher indicating risk of depression in the past 2 weeks. Anxiety was assessed with the Generalized Anxiety Disorder-7 (GAD-7; Spitzer et al., 2006), with a total score of 10 or higher suggesting risk of anxiety in the past 2 weeks. PTSD was measured with the PTSD Checklist for Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; American Psychiatric Association, 2013) (PCL-5; Weathers et al., 2013), with a cutoff score of 31 to indicate the presence of probable PTSD in the past month. All these assessment tools have been validated with demonstrated reliability in the Chinese population (Cheng, Xu, et al., 2020; W. Li et al., 2014; N. Zhang et al., 2013; Y. L. Zhang et al., 2014). Detailed information about these tools is provided elsewhere (Y. Li et al., 2024).
Safety Procedures
IPV is a sensitive topic, and it raises important questions about women’s safety. In the case of currently abused women, if participation in research is revealed to the abuser, it may increase the risk of potential retaliation. The study flyer was carefully designed to avoid implying a specific focus on IPV. In it, we described the study as a “Chinese immigrant women’s health care study,” and in any messages exchanged with participants, we avoided mentioning IPV or any related terms. All communication with participants via text messaging, phone calls, or email identified the study as a “Chinese immigrant women’s health care study.” Participants were also advised that if their personal email address was not safe, they might create an email address specifically for this study. Telephone calls were scheduled at a safe, convenient time chosen by participants. At the beginning of each phone call, we confirmed with the participant that it was safe to have the conversation. We used a well-established, detailed safety protocol for conducting research with abused women in community-based settings.
Data Analysis
Descriptive statistics including means, standard deviations, and percentages were computed for baseline sociodemographic characteristics, the severity of different types of IPV, depression, anxiety, PTSD, and variables for feasibility and acceptability. Because the ultimate sample size was small (N = 19), nonparametric tests including Mann–Whitney tests and Kruskal–Wallis tests were used to examine whether participants’ perceived helpfulness and acceptability of the intervention differed by sociodemographic characteristics, different types of IPV, depression, anxiety, and PTSD. Statistical analyses were performed with SPSS version 26. A significance level of .05, two-tailed, was employed for all analyses.
The interview data for each participant were audio-recorded, transcribed verbatim, and linked to the participant’s weekly messages and responses to open-ended survey questions via unique identifying numbers. These data were then examined with the software program Dedoose, Version 9.0.107, following standard procedures for qualitative content analysis (Miles & Huberman, 1994; Morgan, 1993). Guided by the interview questions, one team member initially read through the qualitative data, identifying four main themes: perceived helpfulness of the intervention, satisfaction with the intervention, barriers and facilitators for intervention adherence, and suggestions for improvement. Subsequently, codes were generated to capture similar phrases within these themes. As coding progressed, new information was compared with existing codes, leading to the creation, refinement, or merging of codes as needed. After all codes were identified, a team member analyzed commonalities and differences, condensing the codes into subthemes. The final set of codes and subthemes was further discussed and reviewed with another team member to enhance rigor and confirmability of the analysis.
Results
Characteristics of the Participants
A total of 95 eligible women were invited to participate in the study. Fifty provided consent (52.6% recruitment rate) with 25 randomized to the intervention and 25 to the control group. Detailed information on participant flow is provided elsewhere (Y. Li et al., 2024). Out of the 25 participants in the intervention group, 19 completed the post-intervention assessment, while in the control group, 20 out of 25 participants completed the assessment. Among the 19 participants in the intervention group, the average age was 33 years. Over 68% had a Bachelor’s degree or higher, but 42% reported having no personal income. Most participants were married and had at least one child, and nearly 74% reported no religious beliefs. Ten were either U.S. citizens or permanent residents (Table 1). Over half of the 19 participants reported experiencing severe psychological aggression, as reflected in their CTS2 scores. About 37% had experienced minor to severe physical assault, and 10.5% had been injured. Minor sexual coercion was reported by 42.1%. With respect to mental health, 47.4% had symptoms of depression, about 21% reported symptoms of anxiety, and about 21% reported symptoms of PTSD (Table 1). Within the intervention group, most participants received the intervention in Mandarin (92%) and also participated in interviews conducted in Mandarin (93.3%).
Characteristics of the Participants (n = 19).
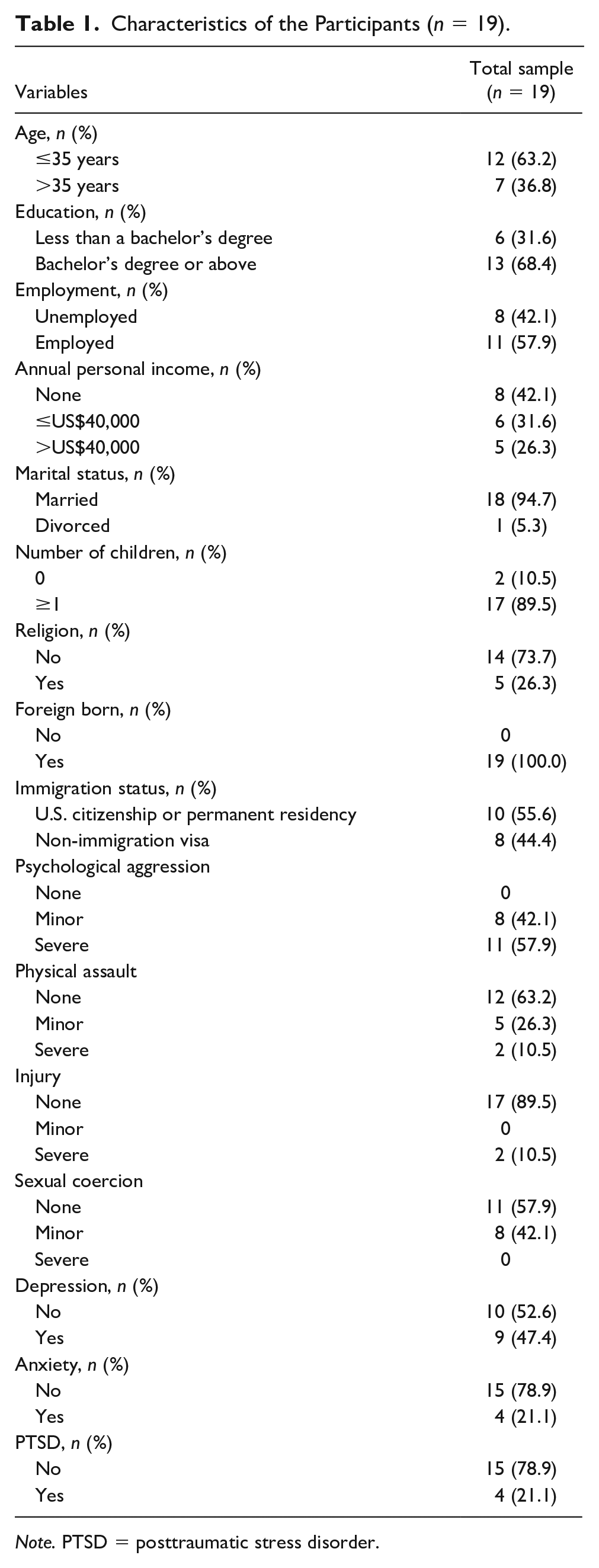
Note. PTSD = posttraumatic stress disorder.
Feasibility
Among the 25 participants in the intervention group, one withdrew after the first session, expressing that the intervention did not align with her needs; five were lost to follow-up due to the research team’s lack of prompt follow-up as the study began. Of the 19 remaining participants, the majority (n = 16) successfully completed all seven sessions, for an intervention completion rate of 64%. One participant completed only the first session, owing to difficulties in accessing the WeChat mini-program. One completed the first three sessions, and another completed the first five sessions. Busy schedules for work, travel, and/or child care as well as technical issues with the WeChat mini-program such as automatic exits, playback lag, and a sluggish interface were mentioned as reasons for lack of completion. During intervention delivery, no adverse events were reported to indicate risk to the safety of all participants occurred.
Acceptability
Quantitative Data
Perceived Helpfulness
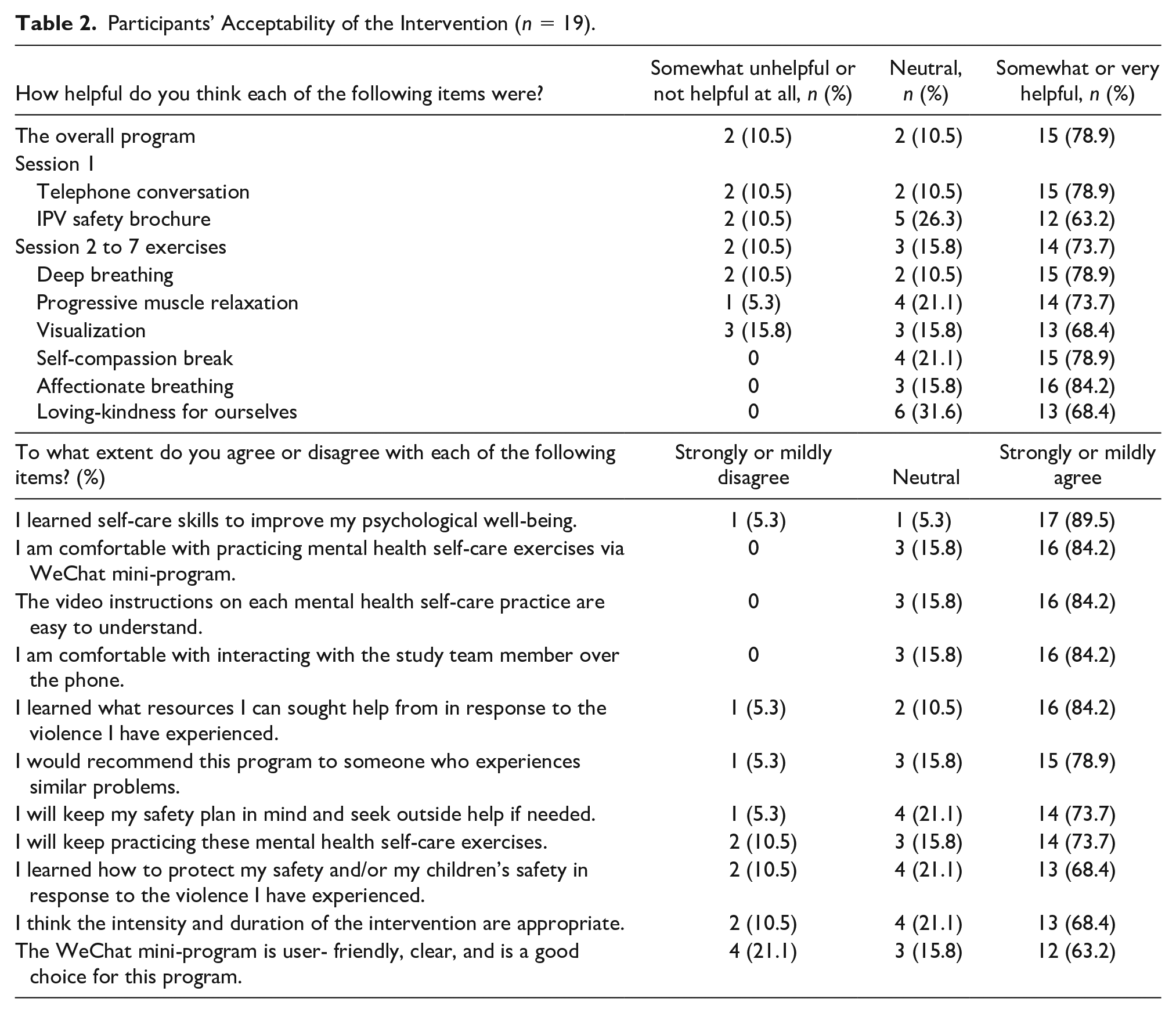
Regarding our overall intervention, 79% of the 19 participants reported finding the intervention helpful. Similarly, 79% thought the telephone conversation helpful, and 63% rated the IPV safety brochure as helpful. Of the six mental health self-care sessions, Affectionate Breathing had the highest rate of perceived helpfulness (84.2%), followed by Self-Compassion Break, Deep Breathing, Progressive Muscle Relaxation, Visualization, and Loving-Kindness for Ourselves (Table 2).
Participants’ Acceptability of the Intervention (n = 19).
Acceptability
Over 84% of the 19 participants agreed that they were comfortable with the phone conversation and in practicing the mental health self-care exercises via the WeChat mini-program (Table 2). More than 84% of participants agreed that the video instructions for each self-care practice were easy to understand, nearly 90% agreed that they learned self-care skills to improve their psychological well-being, and about 74% agreed that they would keep practicing these mental health self-care exercises. When evaluating the usability of the WeChat mini-program, 63% agreed that it was user-friendly, clear, and a good choice.
As for the first session, which involved a phone conversation to discuss the IPV safety brochure, 84% of the 19 participants learned about available resources to seek help in response to the violence they had experienced, and 74% said that they would keep their safety plan in mind and seek outside help if needed. Around 68% agreed that they had learned how to protect their safety and/or their children’s safety in response to the violence they had experienced. About 68% thought that the intensity and duration of the intervention were appropriate. Overall, nearly 79% would recommend this program to others facing similar challenges (Table 2).
Qualitative Data
In addition to the survey data, qualitative data from interviews and text messages provided participants’ perceptions of the helpfulness, satisfaction with the intervention, barriers and facilitators for intervention adherence, and suggestions for improvement.
Perceived Helpfulness
All but one participant gave positive feedback about the intervention’s helpfulness. They described the six weekly relaxation and self-compassion sessions as calming, comforting, positive, relaxing, soothing, warm, and beneficial in various ways, such as promoting sleep; relieving or regulating emotions; reducing stress, anxiety, fatigue, or pain; and even reducing family conflicts. Participants reported mindfulness, self-kindness, self-focus, decreased concern for others’ opinions, and lowered self-expectations. They also expressed self-acceptance, self-encouragement, and self-compassion. One participant stated, “I now will meditate when I remember. Be mindful of the present moment and just think that nobody is perfect. Really helps me a lot!” Another participant said that “when you feel pain, it’s important not to isolate yourselves but instead get in touch with pain and find relief through giving empathy to yourselves.” In addition, during the review of the brochure over the phone in the first intervention session, some participants learned about different forms of IPV and available resources for seeking help when faced with IPV. Overall, participants considered the intervention valuable for women experiencing IPV.
Satisfaction
Participants valued the online format for its flexibility in practicing relaxation and self-compassion exercises at their preferred times and locations. One participant expressed, “I like the online format, and it is especially convenient for women who need to take care of their children. . .” Similar to the survey data, in the interviews, some participants mentioned that they liked the video and audio instructions, describing them as clear and easy to understand, with high quality. One participant shared, “There is no need for people who don’t have any experience (with meditation exercises) to worry about whether it would be hard for them to learn how to practice the exercises. They can make it with the audio guides.” Four participants found the duration and intensity of the intervention appropriate, but one preferred shorter exercises of 5 to 8 minutes rather than 20 minutes.
Barriers and Facilitators for Adherence
A few participants commented that the exercises felt repetitive, lacking in personalization. Ten brought up various technical issues related to the WeChat mini-program, as described earlier. These technical issues, along with repetitive daily exercises, the lack of personalization, and busy daily schedules—particularly those involving child care—were perceived as barriers that negatively affected intervention adherence. One participant shared, “I need to take care of my child, so I often could not find time to do the exercise. I hope the program can be more compact . . .” However, weekly message reminders, belief in the benefits of the intervention, and a fixed time for practice were recognized as factors promoting adherence.
Suggestions for Improvement
Participants provided suggestions for improving the intervention. They recommended including new information and activities such as psychological assessments, yoga, free one-on-one counseling, educational videos on self-protection, and addressing emotional abuse within the self-compassion sessions. Participants also suggested offering different delivery formats for the IPV safety brochure to accommodate individual preferences, such as videos, written copies, or phone conversation. One participant shared,
Going over the brochure via phone is a very good format and can be retained, but it has pros and cons. Some people may not be open during a phone conversation or may have limited time. Under these circumstances, the video format is better.
Transparency about the expertise of the team who developed the intervention was recommended to enhance the intervention’s perceived credibility. Increasing interactions with interventionists to foster a sense of engagement and support and individualizing the intervention’s content and format to meet specific needs or preferences of each IPV survivor were also suggested. To address technical issues with the WeChat mini-program, alternative delivery platforms such as mobile apps, YouTube, or podcast apps were suggested. The importance of a safe environment for practicing relaxation and self-compassion exercises, particularly for women experiencing IPV, was also mentioned. One participant said, “It’s like that pyramid in psychology. What a person needs is safety. Safety is first, and then food, and then emotion and other things. If she cannot ensure her safety, how would she pursue her emotional needs?” In addition, participants offered strategies to increase adherence—automated individualized reminders, rewards, peer support, and opportunities for self-reflection. One participant shared, “I think weekly reminders helped, but more communication opportunities can be provided to guide people to reflect from the exercises and thus gain the benefits.”
Factors Affecting Perceived Helpfulness and Acceptability
Overall, the intervention’s perceived helpfulness and acceptability were not associated with participants’ sociodemographic characteristics or baseline mental health conditions including depression, anxiety, and PTSD (p > .05 for all). However, participants who reported severe psychological aggression at baseline tended to rate the intervention’s helpfulness more highly than did those who reported minor psychological aggression (4.42 ± 0.39 vs. 3.59 ± 0.94; Mann–Whitney U = 19.50, p = .043). Other types of IPV (i.e., physical assault, injury, and sexual coercion) were not associated with perceived helpfulness or acceptability (p > .05).
Discussion
This study is the first to introduce an evidenced-based intervention (Sharps et al., 2016) incorporating relaxation and self-compassion techniques tailored to empower Chinese immigrant women experiencing IPV in the United States. Overall, participants viewed the mobile-based SHE intervention as feasible, acceptable, and potentially beneficial for reducing marital conflicts and improving mental health well-being. There were no adverse events reported, suggesting that our safety protocols could function as intended, but research involving the safety of women experiencing IPV must continue. Participant feedback highlighted multiple suggestions to further refine and improve the intervention.
Adherence
Nearly two-thirds of participants completed all seven weekly sessions. This adherence surpasses the findings of a systematic meta-analysis of mobile-based interventions for mental health issues, in which the average completion of required modules or sessions was only 34% in randomized controlled trial (RCT) studies targeting depression and 36% in RCT studies targeting anxiety (Linardon & Fuller-Tyszkiewicz, 2020). In comparison, our intervention adherence was notably higher (64%), indicating the intervention’s general acceptability among Chinese immigrant women experiencing IPV.
Barriers and Facilitators for Adherence
Participants’ feedback alluded to several factors potentially influencing adherence. The primary barrier hindering engagement in the intervention was related to technical issues with the WeChat mini-program. On the 11 questions regarding the intervention’s acceptability, the lowest percentage of participants (63.2%) agreed that the mini-program was user-friendly, clear, and suitable. Furthermore, participants mentioned that technical challenges with the mini-program were obstacles. Various WeChat mini-programs have been developed and utilized as platforms for disease management and prevention, but most prior studies have not reported participants’ feedback on mini-programs’ usability (Chen et al., 2020; Sun et al., 2022; Ying et al., 2021). In a usability test involving a symptom management mini-program conducted with 10 parents of children with cancer, some participants rated the mini-program as seamless, convenient, and user-friendly (Liu et al., 2022). However, our study participants reported technical challenges, suggesting caution about the intervention’s potential scalability in this delivery format.
Conversely, despite these technical issues, the participants appreciated the flexibility and convenience of mobile-based delivery. Because several technical issues were related to the inherent nature of sub-applications within the WeChat ecosystem, it is imperative to explore alternative platforms. Some participants suggested that mobile apps, social media platforms like YouTube, or podcast apps might be viable alternatives to enhance the intervention’s accessibility and user-friendliness, which could ensure a more seamless, successful implementation. A previous mindfulness-based self-compassion intervention has used YouTube videos and podcasts as modalities to support caregivers of individuals with dementia, and it has demonstrated their feasibility and acceptability (Goodridge et al., 2021).
Repetitive daily exercises and the lack of personalization also affected intervention adherence. Some participants specifically indicated lack of personalization as the intervention’s least attractive aspect. Personalization has been recognized as an effective technique for enhancing motivation and adherence (Sliwinski et al., 2017). As we refine the intervention, it will be necessary to tailor its content for Chinese immigrant women, taking into account their diverse characteristics and needs. Options could allow participants to focus on exercises they find most beneficial. In addition, participants’ busy daily schedules, involving work and child care responsibilities, prevented them from completing the intervention. A solution to this barrier might be to provide participants with better instructions at the outset, guiding them to select a consistent daily routine followed by a relaxation or self-compassion exercise. This strategy has proved effective in improving meditation persistence (Stecher et al., 2021).
Other recommendations from participants for facilitating adherence, such as automated individualized reminders, rewards, peer support, and self-reflection, will also be integrated as we further refine the intervention. In this study, research staff sent individualized reminder messages manually each week. In the future, an artificial intelligence chatbot can automate individualized reminders and facilitate self-reflection through interactive messages, which may promote the intervention’s personalization, scalability, and sustainability (Abd-Alrazaq et al., 2020).
Perceived Helpfulness and Acceptability
Overall, participants perceived the intervention to be helpful. They reported it decreased stress, anxiety, fatigue, pain, and family conflicts, and it fostered emotion regulation and self-compassion. Our findings are consistent with an empowerment-based intervention conducted with a total of 200 abused Chinese women in Hong Kong. The intervention, which included an empowerment component similar to our first intervention session, was found to have a significant reduction in reported partner psychological aggression. Women in the intervention group also found the intervention useful in improving their intimate relationships and reducing conflicts with their partners (Tiwari et al., 2010). Our findings also align with a systematic review that examined 10 mindfulness-based interventions for female victims of IPV. This review reported the benefits of practicing mindfulness in reducing mental health symptoms such as depression and anxiety, although no studies specifically focused on self-compassion within mindfulness practices (Esper & da Silva Gherardi-Donato, 2019).
In addition, our findings suggest that telephone interactions may serve as a form of social support for Chinese immigrant women experiencing IPV. For example, a nurse-delivered telephone social support intervention (“Baby BEEP”) has suggested that nurse–patient interactions via phone might be an effective way to support underserved women with depression during pregnancy (Evans et al., 2017). Similarly, another intervention targeting abused Chinese women in Hong Kong demonstrated the efficacy of weekly telephone calls in improving perceived social support and alleviating symptoms of depression (Wong et al., 2013). However, participants’ feedback did emphasize the importance of diverse delivery formats such as videos, phone conversation, and written materials to address individual preferences effectively. Multiple methods can ensure that an intervention accommodates varying learning styles and communication preferences, thereby enhancing overall effectiveness and impact.
We found that the severity of psychological aggression was positively associated with perceived helpfulness of the intervention. This implies that Chinese immigrant women experiencing more severe psychological aggression may be more receptive and may benefit more from interventions. Women experiencing higher levels of psychological aggression may feel a stronger need for support in coping with abuse and its emotional impact (Hyman et al., 2009). The intervention, with its focus on empowerment and self-compassion, may have provided them with effective tools to manage heightened distress induced by abuse.
Limitations
Certain limitations of this study must be acknowledged. First, the recruitment of participants primarily through online WeChat advertisements may have led to potential underrepresentation of Chinese immigrant women with limited internet access or digital literacy. However, given that IPV is a sensitive topic and Chinese immigrants are geographically dispersed, online recruitment remains effective for accessing this hard-to-reach population. Second, given the limited resources for a small pilot project, the interviews were conducted by the research team member who also delivered the intervention, which could have introduced response bias. Participants may tend to provide positive feedback to align with perceived expectations of the interviewer, rather than express their true experiences. However, the survey questions were administered online. The combined use of online survey and interview data helped to ensure our findings’ reliability. Third, there were technical issues with the WeChat mini-program, such as difficulties in accessing it, automatic exits from the program, lagging playback, or a sluggish user interface. These issues affected adherence to the intervention and its overall effectiveness. To ensure a more seamless and successful implementation of our SHE intervention, alternative platforms such as mobile apps or podcast apps might be considered in the future to enhance the intervention’s accessibility and user-friendliness.
Despite these limitations, this study has strengths. First, the study incorporated a self-compassion component into an empowerment-based IPV intervention for Chinese immigrant survivors. Second, we used mobile health to deliver the SHE intervention, offering a potentially ideal approach to deliver targeted support for a vulnerable, difficult-to-reach population.
Conclusion
This study adds evidence about the feasibility and acceptability of an empowerment-based intervention that integrates relaxation and self-compassion techniques for Chinese immigrant women experiencing IPV. The mobile-based intervention delivery provided access to much-needed support, particularly for a geographically dispersed group of women in the United States. This modality also created a safe, nonjudgmental space for participants to engage in the intervention. The intervention, modified according to preliminary findings from this study, is in progress. Future research based on the modified intervention should evaluate efficacy prior to scaling. Chinese community health workers and bilingual and bicultural mental health counselors are in an ideal position to deliver this intervention to Chinese immigrant women experiencing IPV. Given the shortage of such professionals as well as their concentration in major urban areas, the mobile health modality will make it more accessible to Chinese women residing in different geographical locations in the United States. Furthermore, nurses are also well positioned to facilitate the intervention for Chinese immigrant survivors. Since these survivors are less likely to seek outside help, integrating IPV screening and intervention into routine health care visits, such as prenatal appointments and physical exams, provides a valuable opportunity for them to receive necessary support from nurses.
Supplemental Material
sj-docx-1-jap-10.1177_10783903241268206 – Supplemental material for An Empowerment-Based Intervention for Chinese Immigrant Women Experiencing Intimate Partner Violence: Feasibility and Acceptability
Supplemental material, sj-docx-1-jap-10.1177_10783903241268206 for An Empowerment-Based Intervention for Chinese Immigrant Women Experiencing Intimate Partner Violence: Feasibility and Acceptability by Yang Li, Tina Bloom, Linda F. C. Bullock and Hyekyun Rhee in Journal of the American Psychiatric Nurses Association
Supplemental Material
sj-docx-2-jap-10.1177_10783903241268206 – Supplemental material for An Empowerment-Based Intervention for Chinese Immigrant Women Experiencing Intimate Partner Violence: Feasibility and Acceptability
Supplemental material, sj-docx-2-jap-10.1177_10783903241268206 for An Empowerment-Based Intervention for Chinese Immigrant Women Experiencing Intimate Partner Violence: Feasibility and Acceptability by Yang Li, Tina Bloom, Linda F. C. Bullock and Hyekyun Rhee in Journal of the American Psychiatric Nurses Association
Footnotes
Acknowledgements
The authors express their gratitude to all the research assistants for their contributions to the study, and to the editor, John Eric Bellquist, for his language editing. They also offer sincere appreciation to all the participants for their involvement in the study.
Author Roles
All authors contributed to the conception or design of the study or to the acquisition, analysis, or interpretation of the data. All authors drafted the manuscript, or critically revised the manuscript, and gave final approval of the version that was submitted for publication. All authors agree to be accountable for all aspects of the work, ensuring integrity and accuracy.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Pilot Research Grant of the St. David’s Center for Health Promotion & Disease Prevention Research in Underserved Populations (St. David’s CHPR).
Clinical Trial Registration
The study was registered in ClinicalTrials.gov (ID: NCT05011552).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.