
Abstract
BACKGROUND:
Discrimination, or unfair treatment based on individual characteristics such as gender, race, skin color, and or sexual orientation, is a pervasive social stressor that perpetuates health disparities by limiting social and economic opportunity and is associated with poor mental and physical health outcomes.
AIMS:
The purpose of the present study is to (1) examine the association between maternal experiences of discrimination and paternal experiences of discrimination; (2) explore how discrimination relates to parental (maternal and paternal) stress and depressive symptoms; and (3) examine whether social support exerts protective effects.
METHODS:
The sample was 2,510 mothers and 1,249 fathers from the Child Community Health Network study. Linear regression models were conducted to explore associations between maternal and paternal discrimination. In addition, mediation analyses were conducted to explore if social support functioned as a mediator between discrimination on parental stress and depressive symptoms.
RESULTS:
Most mothers (40.3%) and fathers (50.7%) identified race as the predominant reason for discrimination. Experiencing discrimination was significantly related to stress and depressive symptoms for both parents, and all forms of social support mediated these relationships. Our findings suggest that social support can act as a protective factor against the negative association between discrimination and both stress and depressive symptoms.
CONCLUSIONS:
These findings highlight the need to integrate social support into existing interventions and include fathers in mental health screenings in primary-care settings. Finally, we briefly describe the role of nurses and other allied health professionals in addressing discrimination in health care and health policy implications.
Discrimination is a pervasive social stressor that ripples across families, communities, and society. By limiting social and economic opportunities, discrimination carries long-term psychological, physiological, and societal costs (Carter et al., 2017). Discrimination is the unfair treatment of an individual that is perceived as belonging to a certain group and can occur on multiple levels including systemic (e.g., policies, denial of rental opportunity) or individual levels (e.g., microaggressions such as verbal hostility in tone of voice) (Chambers et al., 2021; Jones et al., 2016; Krieger, 2012). Within a family, discrimination can impact individuals on an interpersonal level when discrimination toward one individual in the household (mother/father) can create tension in household relations that affect other family members including children (Condon et al., 2022). Vicarious racism is a specific type of discrimination that results from the indirect experience of hearing about or seeing racist acts against other members of one’s racial group (Chae et al., 2021). In other words, discrimination toward one individual may indirectly affect another, especially within a family (partner or child). These experiences can have far-reaching consequences not only for mothers but for their children (Heard-Garris et al., 2018; Iruka et al., 2022; Saleem et al., 2020). Racial discrimination is one of the most prevalent forms of discrimination in the United States (US) (Gong et al., 2017). Recent studies show that up to 63% of some minoritized groups (studies included samples of Black, Hispanic and Asian individuals) experience racial discrimination in relation to the workplace, health care, housing, education, and or law enforcement (Bergeron et al., 2020; Lee et al., 2019). Discrimination is also linked to poor mental and physical health outcomes including hypertension, obesity, depression, and anxiety (Bergeron et al., 2020; Ibrahim et al., 2021; Kalinowski et al., 2022; Pascoe & Smart Richman, 2009; Santos et al., 2018, 2021).
Chronic exposure to discrimination has been linked to adverse physical and mental health outcomes for parents and their children. Maternally experienced discrimination has been consistently linked to adverse birth outcomes, including pre-term birth, along with the child’s emotional health (Barcelona et al., 2021; Caughy et al., 2004; Collins et al., 2004; Ford et al., 2013; Thayer & Kuzawa, 2015). Discrimination has also been associated with negative effects on emotional wellbeing and may contribute to prenatal and postpartum depression (PPD) through heightened persistent sadness, anhedonia, low energy, changes in eating and sleeping habits, poor concentration, memory, irritability, and suicidal ideation (Stepanikova & Kukla, 2017). Maternal experiences of discrimination and PPD can also increase paternal rates of PPD among African American fathers (Bamishigbin et al., 2017) and impact paternal involvement, relationship outcomes, and the psychological adjustment of other family members (Ansari et al., 2021; Fisher et al., 2021; Kerr et al., 2018). Furthermore, parental PPD is a known risk factor for poor child development, and this risk is higher among families with parents experiencing discrimination (Caughy et al., 2004; Ertel et al., 2012; Santos et al., 2021; Stepanikova & Kukla, 2017; Tran, 2014). Despite the known adverse impacts of discrimination on family health and well-being, there is still a limited understanding of how maternal and paternal experiences of discrimination may be linked to each other and to subsequent mental health outcomes.
Given parent’s vulnerability during the postnatal period, as well as the potential for poor mental health outcomes associated with discrimination, it is vital to identify factors that protect against stress and depressive symptoms (Landy et al., 2012). One potential protective factor is social support (Sherbourne & Stewart, 1991) which may buffer the effects of stressors such as discrimination by providing emotional (the expression of positive affect, empathetic understanding, and the encouragement of expression of feelings) or informational (the offering of advice, information, guidance or feedback) support (Bergeron et al., 2020). Recent studies demonstrate that individuals who face racial discrimination are less likely to experience poor mental health outcomes when they have social support (Bergeron et al., 2020; Brody et al., 2014; Brown et al., 2012; Ickovics et al., 2011; Pao et al., 2019). For example, a study looking at young African American adults in the rural south showed that emotional support may reduce the impact of racial discrimination on biological stress regulation systems (Brody et al., 2014). Another study focused on a diverse sample in NYC found that social support buffered the relationship between racial discrimination and poor mental health (Bergeron et al., 2020; Millender et al., 2024).
In the current study, we build upon extant research to understand the association between discrimination on parental (maternal and paternal) emotional health including both stress and depressive symptoms (Figure 1). The purpose of this study was to (a) examine the association between maternal experiences of discrimination and paternal experiences of discrimination; (b) explore how discrimination relates to parental (maternal and paternal) depressive and stress symptoms (i.e., whether maternal experiences of discrimination relate to maternal depressive and stress symptoms); and (c) examine whether maternally experienced discrimination predicts paternal depression or perceived stress and (i.e., whether paternal experiences of discrimination predict maternal depressive and stress symptoms). Finally, we will examine the extent to which social support protects against the effects of discrimination.
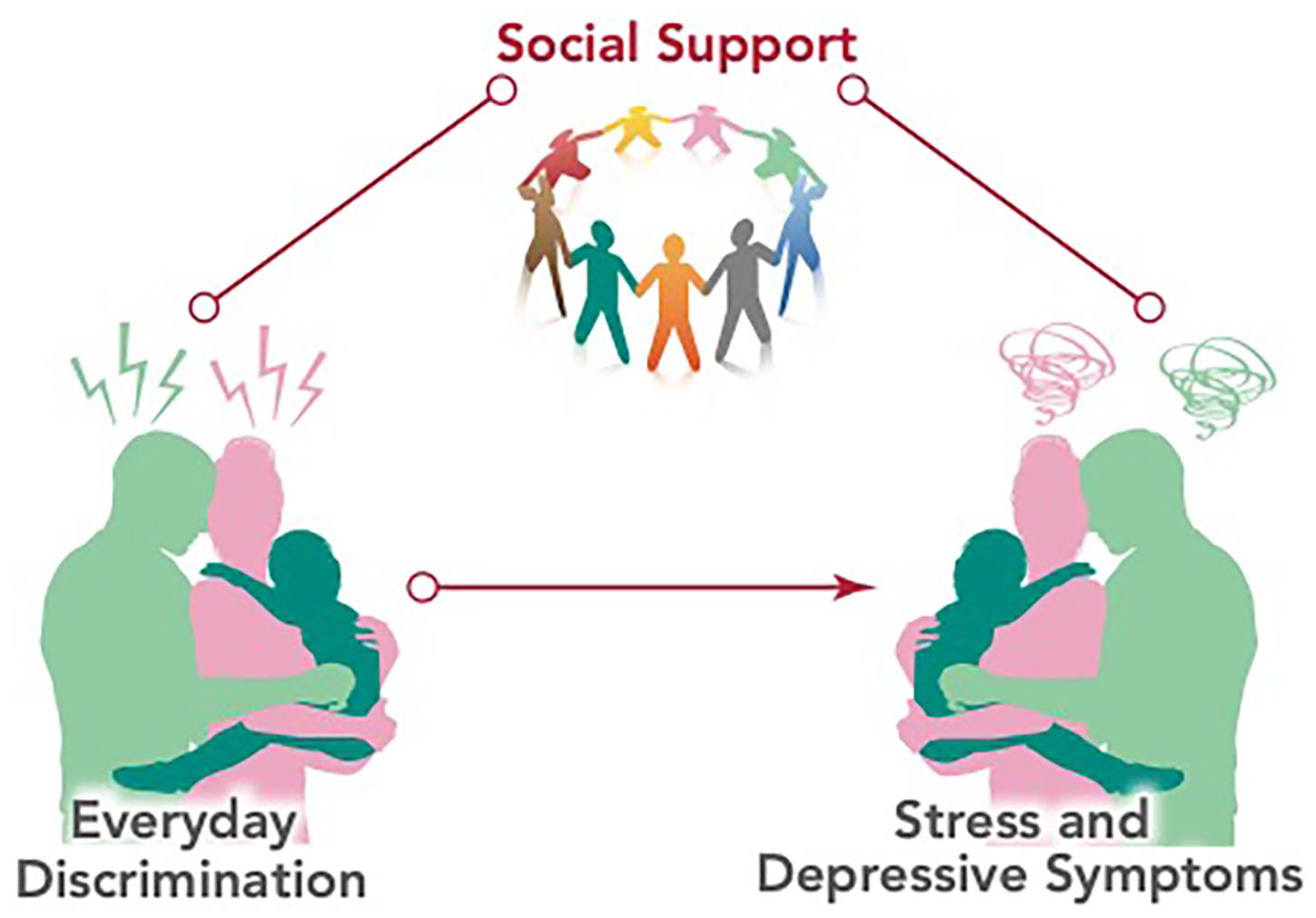
Conceputal Model
Methods
Setting
De-identified data from the Community Child Health Network (CCHN) study was used to conduct the present secondary data analysis. The study was approved by The Institutional Review Board of the University of North Carolina at Chapel Hill (#21-2923). The CCHN is an observational study exploring how stressors across multiple levels, such as individual, family, and community factors, may interact with biological factors to contribute to maternal and child health inequalities (Ramey et al., 2015). Multisite recruitment was completed between 2008 and 2010 in North Carolina, Illinois, Maryland, California, and Washington, D.C. While the authors acknowledge not all birthing individuals identify as women CCHN did not collect data on gender identity; therefore, the authors use the term mother, as indicated by the CCHN. The CCHN investigators purposively over-sampled low-income women or women who experienced preterm birth. Mothers were recruited during the peripartum period during either their postpartum hospitalization or during prenatal clinic visits. Women were eligible for enrollment if the following criteria were met: (a) self-identified as Black or African American, Hispanic or Latina, or White; (b) 18 to 40 years old; (c) resided for at least 6-months within data collection locations; (d) had three or fewer children; and (e) had no plans for future sterilization. Fathers were contacted and invited to participate in the study only after mothers gave permission to the researchers (Bamishigbin et al., 2020). Each recruitment site sought approval from the partnering hospital or university on protocols and informed consent procedures.
Recruiters and interviewers consisted of trained personnel and research assistants affiliated with the collaborating academic and community institutions. For this study, we used data from 2,510 mothers and 1,249 fathers from the CCHN study baseline. For additional details about the CCHN study, refer to https://dash.nichd.nih.gov/study/1649.
Measures
Sociodemographic
Sociodemographic data including age, race/ethnicity, education level, and poverty level were included from the baseline visit from both mothers and fathers. Education level was measured as highest level of education received including <high school (HS), HS/Graduation Equivalency Degree (GED), some college, and 4-year degree, and other. Poverty level was based on the Federal Poverty Level (FPL) and was recorded on three levels <100% FPL, 100% to 200% FPL, and >200% FPL.
Discrimination
The Everyday Discrimination Scale (EDS) was used to measure parents’ experiences of daily discrimination. This scale includes nine questions that assess perceived discrimination based on routine daily experiences of unjust treatment (Williams et al., 1997). The stem question is: “In your day-to-day life, how often do any of the following things happen to you?” and items include: “You are treated with less courtesy than other people are,” “People act as if they think you are dishonest” and, “You are called names or insulted.” Participants then identify the primary reasons they believe account for these discrimination experiences, such as gender, race, skin color, and/or sexual orientation. This measure is widely used to measure discrimination experiences (Williams et al., 1997). Responses were given on a Likert-type scale with scores range from 0 to 5. Higher scores on the scale indicate greater perceptions of discrimination. Previously the EDS has been validated using the CCHN samples with a reported internal validity of α = .89 (mothers and fathers) (Dunkel Schetter et al., 2013).
Social Support
The Medical Outcomes Study Social Support Survey (MOS-SSS) was used to measure parents’ perceived social support. The survey consists of 19 questions that measure four dimensions of social support including emotional support (the expression of positive affect, empathetic understanding and the encouragement of expression of feelings), tangible support (the provision of material aid or behavioral assistance), positive social interaction (the availability of other persons to do fun things with you), and affectionate support (involving expressions of love and affection) (Sherbourne & Stewart, 1991). Each of the 19 items were given on a 5-point Likert-type scale with higher scores indicating greater perceived social support. Within our sample, the internal reliability was strong, with the total score for mothers Cronbach α = 0.96 (all subscales Cronbach α >0.84) and fathers Cronbach α = 0.95 (all subscales Cronbach α >0.80).
Outcomes
Perceived Stress
The Perceived Stress Scale (PSS) was utilized to measure parental stress symptoms (Cohen et al., 1983). The PSS includes 10 items that assess frequency and degree to which individuals have perceived life to be overwhelming, unpredictable, and uncontrollable over the last month. Responses were given on a Likert-type scale of 1 to 5 and a sum score was used with higher scores indicating more perceived stress. Previous studies have demonstrated adequate reliability with Cronbach α ranging from 0.75 to 0.91 (Cohen et al., 1983; Cohen & Janicki-Deverts, 2012; Cole, 1999).
Depressive Symptoms
The Edinburgh Postnatal Depression Scale (EPDS) was utilized to measure parental depressive symptoms. The EPDS consists of 10 items that assess depressed mood for the last 7 days. Parents responded based on the frequency of experiencing an item on a 0 to 3 Likert-type scale. The sum of scores ranges from 0 to 30 with higher scores indicating worse depressive symptoms (Cox et al., 1987; McBride et al., 2014).
Analysis
We conducted descriptive analyses for all demographic variables for the mother and father as well as their stress (PSS) and depressive (EPDS) symptoms at the baseline study visit. In addition, we calculated the means for the discrimination (EDS) as well as the reported frequencies of types of discrimination for both the mother and father. We also provided summary statistics for the Social Support Total Score and subscales (MOS-SSS) for the mother and fathers.
To explore the association between maternal and paternal experiences of discrimination, we conducted statistical analysis using a linear regression model to see if the maternal discrimination total score correlated with the paternal discrimination total score. We controlled for maternal sociodemographic covariates including age, race, education, and poverty factors at a significance level of α < 0.05.
To explore the associations between (a) paternal discrimination on maternal depression; (b) paternal discrimination on maternal stress; (c) maternal discrimination on paternal depression; (d) maternal discrimination on paternal stress; we further conducted regression analysis using four linear regression models by controlling for maternal sociodemographic covariates including age, race, education, and poverty factors. We conducted a mediation analysis of different social supports (M) on the association between discrimination (EDS) and depression (EPDS) by adjusting for age, race, education, and poverty level by adopting the following three multiple linear regression models: The variance estimation for the mediation effect estimate is obtained via 100 rounds of bootstrap resampling with replacement. We report the direct effect, and the parameter estimates for the mediators with accompanying 95% confidence interval, and a P value. Similarly, we adopted three multiple linear regression models to investigate different social supports (M) on the association between discrimination (EDS) and stress (PSS) by adjusting for age, race, education, and poverty level. Separate models were conducted for both the maternal and paternal discrimination scores on the two symptom outcomes of stress and depressive symptoms.
Results
Our sample comprised of 2,510 mothers and 1,249 fathers, respectively. The mean age of mothers was 25.7 years old (SD = 5.7), while the mean age of fathers was 29 years old (SD = 7.1). The majority of the mothers within the sample self-identified as Black or African American (52.6%) followed by Hispanic (23.7%) and White (21.5%). A similar distribution was present among the fathers with 46.3% of the sample self-identifing as Black or African American, 26.7% Hispanic, and 23.1% White. In the sample, most individuals in both the maternal (42%) and paternal cohort (40.6%) were educated at the HS/GED level. For a full summary of reported demographics, see Table 1.
Descriptive Statistics for Mothers and Fathers Sociodemographic Data.
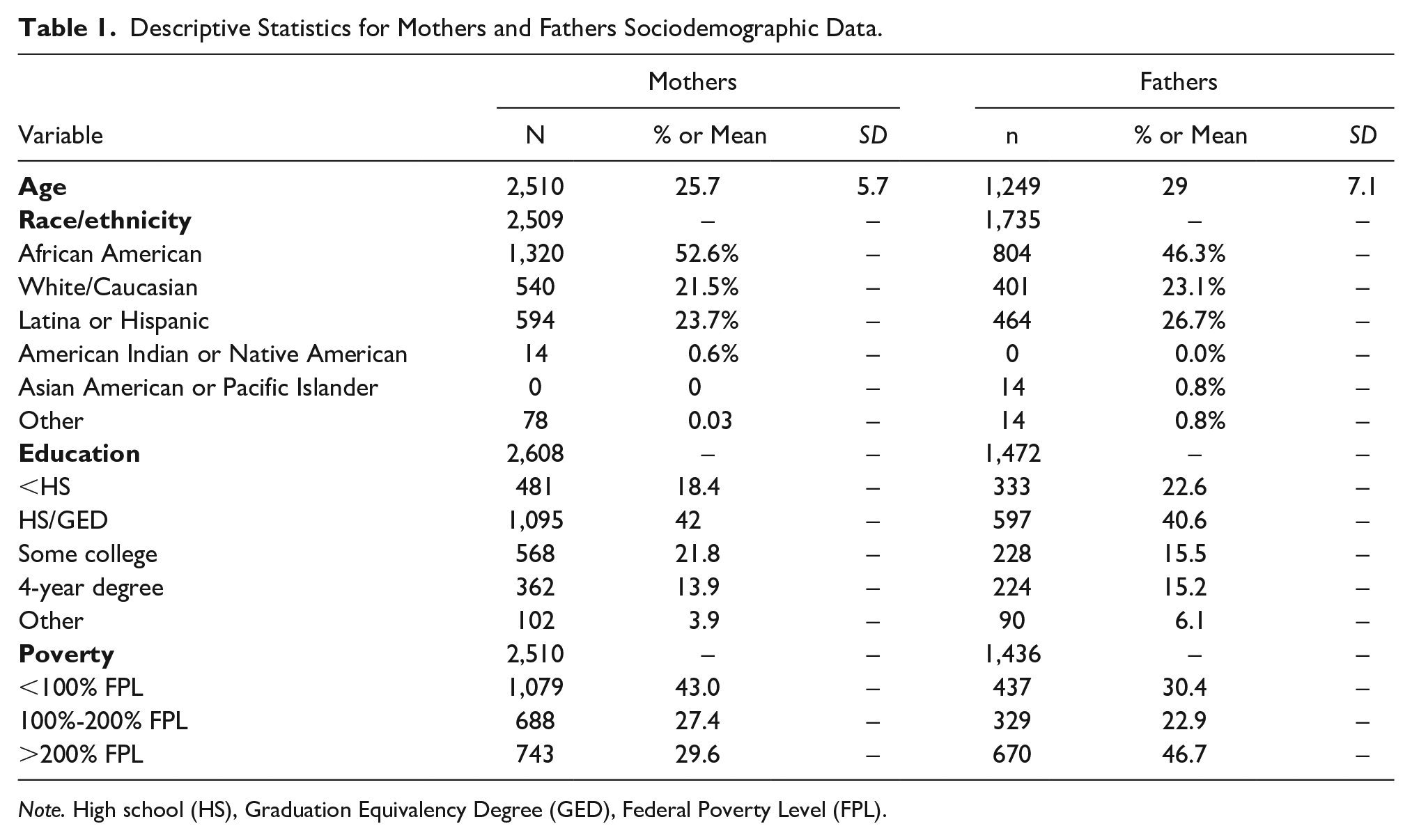
Note. High school (HS), Graduation Equivalency Degree (GED), Federal Poverty Level (FPL).
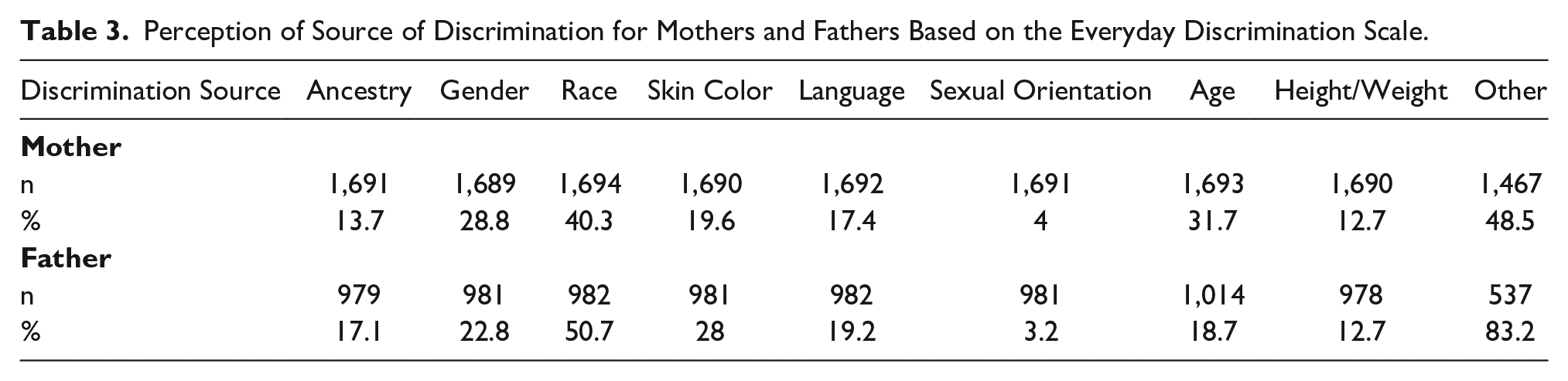
Maternal and paternal experiences of discrimination were assessed with the EDS, which asks the participant to report the primary reasons for discriminatory experiences. Most mothers (40.3%) and fathers (50.7%) reported race as the primary reason for discrimination (Table 2). Overall, mothers reported a mean discrimination score of 10.4, while fathers reported a mean discrimination score of 13.3.
Descriptive Statistics for Mothers and Fathers Outcome Mediators.
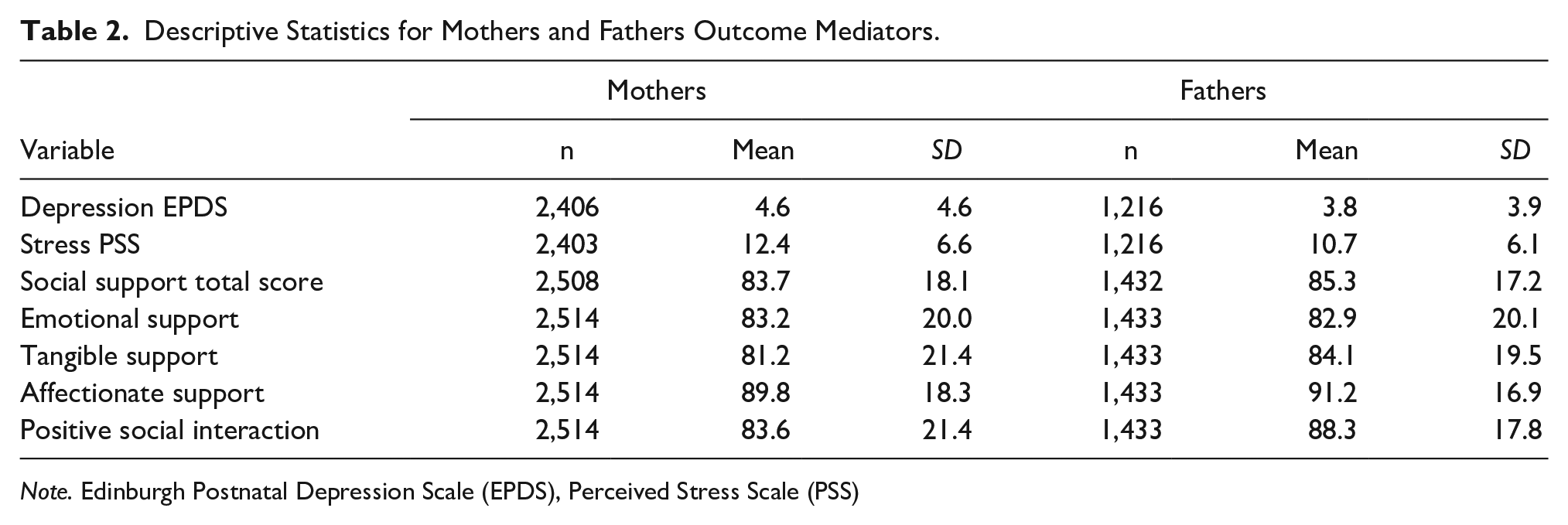
Note. Edinburgh Postnatal Depression Scale (EPDS), Perceived Stress Scale (PSS)
In regard to stress symptoms as measured by the PSS, the maternal average score was 12.4 (SD = 6.6) while the paternal average score was 10.7 (SD = 6.1) out of 50. With reference to depressive symptoms, as measured by the EPDS, the maternal average was 4.6 (SD = 4.6) and the paternal average was 3.8 (SD = 3.9) out of 30. For a full report of stress and depressive symptoms, refer to Table 3.
Perception of Source of Discrimination for Mothers and Fathers Based on the Everyday Discrimination Scale.
Association Between Mothers and Fathers’ Discrimination Experience
The maternal discrimination score and paternal discrimination score were negatively associated. However, this relationship was nonsignificant with a partial correlation of −0.01, 95% CI [−0.06, −0.04], p = .770.
Effects of Paternal Discrimination on Maternal Depression and Maternal Stress
The paternal discrimination score had a negative association with maternal depression (Effect = −0.02, 95% CI [−0.05, 0.01], p = .237) and on maternal stress (Effect = −0.03, 95% CI [−0.07, 0.02], p = .259). However, both of these relationships were not statistically significant.
Effects of Maternal Discrimination on Paternal Depression and Paternal Stress
The maternal discrimination score had a positive association with paternal depression (Effect= 0.02, 95% CI [−0.01, 0.05], p = .206) and paternal stress symptoms (Effect = 0.04, 95% CI [−0.01, 0.09], p = .101). However, both of these associations were not statistically significant.
Social Support as a Mediator Between Discrimination and Depressive Symptoms
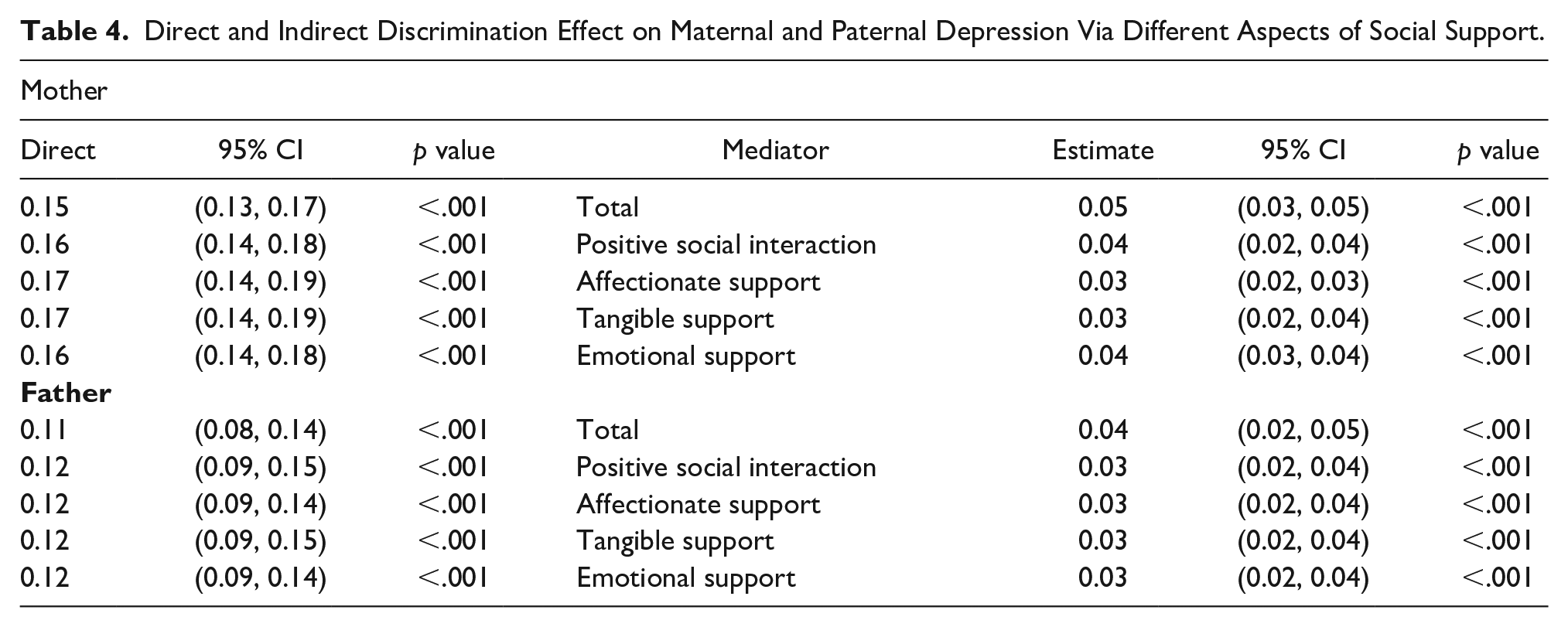
A mediation analysis was conducted to explore whether different forms of social support acted as mediators in the association between maternal discrimination (EDS) and maternal depressive symptoms (EPDS), while adjusting for confounding factors such as age, race, education, and poverty. The total discrimination effect on maternal depressive symptoms is estimated as Effect = 0.20, 95% CI [0.18, 0.22], p ≤ .001. The total discrimination effect on paternal depressive symptoms is estimated as: Effect = 0.15, 95% CI [0.12, 0.18], p ≤ .001. In summary, all aspects of social support mediated the effect of discrimination on depressive symptoms for both the mothers and the fathers. Specifically, emotional support served as the strongest mediator for depressive symptoms in both mothers and fathers. The estimated mediation effect of emotional support on depressive symptoms for the mothers is Effect = 0.04, 95% CI [0.029, 0.046], p ≤ .001. The estimated mediation effect of emotional support on depressive symptoms for the fathers is Effect = 0.03, 95% CI [0.02, 0.05], p ≤ .001). In addition, the total social support score had a greater mediating effect against depressive symptoms for the mothers when compared to the fathers. The direct effect and mediation effect estimate, corresponding 95% CI estimate, and P value under different social support mediators are summarized in Table 4.
Direct and Indirect Discrimination Effect on Maternal and Paternal Depression Via Different Aspects of Social Support.
Social Support as a Mediator Between Discrimination and Perceived Stress
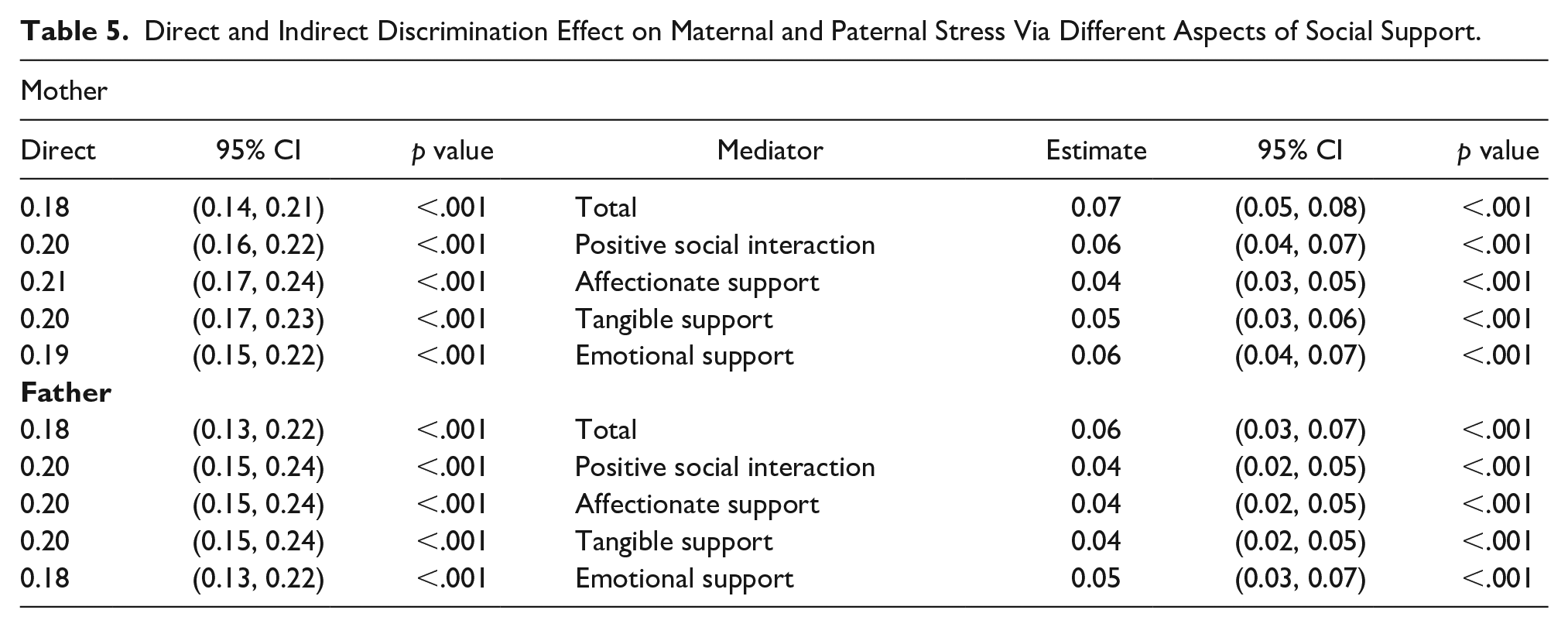
Similarly, we adopted the above three multiple linear regression models to investigate different maternal and paternal social supports on the association between discrimination and stress symptoms (PSS) by adjusting for age, race, education, and poverty confounding factors. The total discrimination effect on maternal stress was estimated as: Effect = 0.25, 95% CI [0.22, 0.28], p ≤ .001. The total discrimination effect on paternal stress was estimated as: Effect = 0.24, 95% CI [0.19, 0.28], p ≤ .001). All forms of social support mediated the effect of discrimination on perceived stress for both the mothers and the fathers, but the effects of total social support and emotional support were more pronounced for the mothers. Specifically, emotional support served as the strongest mediator for perceived stress in both mothers and fathers. The estimated mediation effect of emotional support on perceived stress for the mothers is Effect = 0.06, 95% CI [0.05, 0.08]; p ≤ .001). The estimated mediation effect of emotional support on perceived stress for the fathers is Estimate = 0.05, 95% CI [0.03, 0.08], p ≤ .001). The direct effect and mediation effect estimate, corresponding 95% CI estimate, and p value under different social support mediators are summarized in Table 5.
Direct and Indirect Discrimination Effect on Maternal and Paternal Stress Via Different Aspects of Social Support.
Discussion
In this study, we aimed to explore the association between parental experiences of discrimination, the relationship between discrimination, stress, and depressive symptoms, as well as the protective role of social support. The results showed no significant association between maternal and paternal experiences of discrimination. For both mothers and fathers, however, discrimination was associated with stress and depressive symptoms. Those associations were significantly mediated by social support, especially emotional support.
Our first analysis explored the association between maternal and paternal perceived discrimination. Our findings indicated a small negative association (r = −0.01) between maternal and paternal experiences of discrimination with and without adjustments for sociodemographic covariates; however, these results were nonsignificant. A previous study has demonstrated an association between maternal and paternal experiences of racial discrimination and prenatal perceived stress (r = 2.09), prenatal depression (r = 1.85) and postnatal depressive symptoms (r = 1.66) (Bécares & Atatoa-Carr, 2016). These results may be related to differences in population characteristics and analytical methods. For example, Bécares & Atatoa’s longitudinal study took place in New Zealand and included a sample of 6822 mothers and 4401 fathers, as opposed to our cross-sectional study that included a sample of 2,510 mothers and 1,249 fathers in the United States. Within this study, there was no association between maternal and paternal discrimination. Nor did we find associations between maternal discrimination and paternal depression or stress and vice versa. We sought to explore if the experience of discrimination between parents influenced depressive and stress symptoms on an interpersonal level (for example vicarious racism), which suggests that the effects of discrimination may extend beyond the intended target. Our findings did not support that the perceived discrimination of one parent had an influence on the other parent’s stress and depressive symptoms within our sample. Nevertheless, the effect of experiences of discrimination between family members should be further investigated to better understand the interdependent effects of discrimination within a family.
We also examined the individual experiences of discrimination and its relation to depressive and stress symptoms. In both mothers and fathers, we found statistically significant positive associations between discrimination, stress, and depressive symptoms. These findings add to the existing literature reflecting how experiences of discrimination are linked to negative impacts on both mental and physical health outcomes (Bergeron et al., 2020; Santos et al., 2018, 2021; Williams et al., 1997). We found that race and skin color were the two primary reasons for both maternal (40.3%, 31.7%) and paternal (50.7%, 28.7%) experiences of discrimination. While studies have examined the effects of maternally experienced discrimination, limited studies have included fathers as well (Bécares & Atatoa-Carr, 2016; Gee et al., 2012). Thus, our study adds to the limited pool of research that explores perceived discrimination and mental health for both mothers and fathers. Our results demonstrate a need for health care–related interventions that protect patients and promote maternal and paternal mental health.
Our final analysis explored the extent to which social support serves as a protective factor between the association of discrimination and both stress and depressive symptoms. Our results show that social support serves as a significant protective factor for both parents. All four types of social support measured including emotional support, tangible support, positive social interaction, and affectionate support protected against the effects of racial discrimination for both mothers and fathers. These results add to existing findings that have established social support as a protective factor against the effects of racial discrimination (Bergeron et al., 2020; Lewis et al., 2015). In addition, we found that for both mothers and fathers, emotional support was estimated to have the greatest mediating effect on both depressive and stress symptoms. Another study found the perceived availability of emotional support, including having someone to confide in, as a mediating factor against the negative mental health effects of perceived discrimination (Ajrouch et al., 2010). Future studies may want to consider exploring the mechanisms by which perceived social support acts as a protective factor. Overall, these results suggest that social support should be incorporated into health care–related interventions and policies that mitigate depressive and stress symptoms related and unrelated to discrimination.
Our results highlight the association between discrimination, elevated stress and depressive symptoms, and the protective role of social support during the perinatal period. Integrating social support into perinatal depression interventions have shown mixed results (Dennis & Dowswell, 2013; Small et al., 2011), and few of these studies incorporate fathers. Fathers who experience PPD indicate their need for social support from formal (health professionals) and informal sources (friends and families) and believe that interventions should include both information on PPD as well as coping strategies for themselves and their partners (Letourneau et al., 2012). To effectively address the psycho-social needs of families, state-based programs like the Help Me Grow initiative can play a vital role. By fostering collaboration across sectors, these programs can connect families with community-based services such as home visiting programs. These services extend support to various aspects of family needs, including parental mental health services, child health care, early care and education, and family support (Miller et al., 2023). Among high-risk groups, home visiting programs with structured social support delivered from health professionals including nurses has been effective in reducing depressive symptoms (Ammerman et al., 2010; Beatson et al., 2021; Molloy et al., 2021). Home visiting interventions often enhance formal structured support via emotional, informational, and instrumental support from the home visitor (nurse, health professional, lay person) (Byrne et al., 2016). Home visiting interventions should also embed teaching participants skills to form and enhance informal social support networks through friends, family, and within their community once the time-limited intervention supports have ended (Hetherington et al., 2020; Marshall et al., 2018). Group therapy modalities are also an evidence-based intervention for PPD, which include direct social support mechanisms. Participants can share and reflect their experiences, including experiences of discrimination, through mutual support among peers with similar experiences (Goodman & Santangelo, 2011). Within this study, emotional support had the strongest mediation effect between experiencing discrimination and depressive symptoms among mothers and fathers and therefore should be enhanced within existing clinical interventions.
Our findings further support integrating mental health screenings in primary care during the peripartum period. Current recommendations from the U.S. Preventive Task Force (2023a, 2023b) indicate that all adults including pregnant and postpartum persons should be screened for depression and anxiety. The American College of Obstetricians and Gynecologists, American Academy of Pediatrics, and the National Association of Pediatric Nurse Practitioners recommend screening in mothers for depression during prenatal and pediatric primary care (Rafferty et al., 2019; Waldrop et al., 2018). Although these recommendations focus on birthing individuals during the perinatal period our findings support recent recommendations to include birthing partners including fathers in routine mental health screening in the primary-care setting (Le et al., 2023; Rao et al., 2020; Walsh et al., 2020). Nurses are often the health care professional administering and or scoring depressive screening forms (Waldrop et al., 2018). Therefore, primary-care nurses need adequate education on how to implement screening procedures and also need evidence-based clinical decision support algorithms that include referral and follow-up care for individuals with positive screens (Waldrop et al., 2018).
Although our sample was community based, our findings highlight the need to address discrimination in health care. In the United States, health care–related discrimination is prevalent, with estimates suggesting that one in five adults experience discrimination (Nong et al., 2020). Furthermore, more than one-third of Black or African American and Latinx adults, along with their family members, have encountered instances of discrimination within the health care system (Nong et al., 2020). Discrimination in health care is a significant concern that must be actively addressed by nurses, allied health care professionals, and hospital systems to deliver high-quality patient care. Nurses play a crucial role in promoting a safe and inclusive health care environment. To combat discrimination, it is essential for nurses to actively listen to patients, understand their unique needs, and advocate for their rights (Altman et al., 2020). By staying informed about cultural responsiveness, implicit biases, and the impact of discrimination on health outcomes, nurses can contribute to fostering an environment where every patient receives fair and compassionate treatment, ultimately improving overall health care quality (Brooks et al., 2022; James & Okoye, 2023).
Our findings reinforce the existing evidence regarding the adverse relationship between discrimination on the parental mental health. Furthermore, they underscore the prevalence of racism as a prominent form of discrimination within our sample. Discrimination and racism in health care and within nursing is recognized by both the American Academy of Nursing and American Psychiatric Nursing Association (Myers, 2022). We recommend that nurses, health care professionals, nursing schools, and health systems implement strategies to address health care–related discrimination including racism. While not within the scope of this article, patients have identified several strategies to reduce discrimination in postpartum care delivery for individuals of color. These strategies involve both individual health care providers and the health care system as a whole (Altman et al., 2020). For individual health care providers, patients suggest spending quality time with patients, building relationships, providing individualized person-centered care, and fostering partnership in decision-making. For the health care system, improving continuity of care, improving provider and racial-ethnic concordance, addressing health system structure issues, and providing provider education including implicit bias training and curriculum integration are recommended (Altman et al., 2020). For a practical guide for nurses seeking to address their own biases and learn about how racial bias is associated with health inequity see James and Okoye (2023). Nursing schools can incorporate the above patient-centered recommendations into their curriculum by highlighting how bias, structural racism, and social determinants of health intersect within their curriculum (Muirhead et al., 2022). Furthermore, schools of nursing can actively recruit and support both faculty and students of color to increase the diversity within the nursing workforce and in so doing increase provider-patient concordance (Adynski et al., 2023; Bravo et al., 2023; Brooks et al., 2022; Green, 2020; Iheduru-Anderson et al., 2021; Johnson et al., 2020; Matthews et al., 2022). Health care organizations can develop patient reporting systems, provide effective implicit bias training, and develop institutional policies to combat racial discrimination in health care and promote culturally responsive care (Bleich et al., 2021; Hagiwara et al., 2020). Our findings underscore the need to confront discrimination and structural racism in the realm of health policy, particularly in the context of perinatal mental health care. Some recommendations that address structural barriers to perinatal mental health include improving health insurance coverage, paid family leave, and investing in communities and nonacute care settings to improve respectful, culturally appropriate care (Bower et al., 2023; Crear-Perry et al., 2021; Foster et al., 2021).
Some limitations should be considered when contextualizing the findings of our study. This is a cross-sectional analysis; thus, causality interpretation should be avoided. A limitation of these data is that they were collected between 2008 and 2010, which may not reflect individuals’ experiences of discrimination today. Furthermore, this does not reflect the increased awareness of systemic racism in health care and police brutality during the COVID-19 pandemic, given the events surrounding the murders of Ahmaud Arbery, George Floyd, and Breonna Taylor and the increased public awareness of the Black Lives Matter movement. Another limitation of our study is the difference in sample sizes between the maternal (n = 2,510) and paternal samples (n = 1,249). Despite these limitations, the sheer inclusion of fathers in our sample is a strength, given the limited literature regarding paternal experiences of discrimination and historical underrepresentation of fathers in child and family research (Bamishigbin et al., 2017; Bogossian et al., 2019). Furthermore, this study includes the use of a large national data set (CCHN) that is both racially/ethnically and socioeconomically diverse. Exploring social support as a protective factor is an additional strength that could promote the health and well-being of mothers and fathers by integrating social support into clinical practice and policy (Beeber et al., 2022).
Conclusion
This study contributes to the limited pool of research related to the effects of discrimination on both mothers and fathers. Our analysis demonstrates significant positive associations between discrimination, stress, and depressive symptoms (individually in mothers and fathers) as well as social support as a protective factor (individually for both mothers and fathers) against the effects of discrimination (stress and depressive symptoms). We recommend that clinical interventions should integrate or enhance social support to best address discrimination and parental mental health. Overall, these findings can inform policy and clinical practices that protect the mental and physical well-being of birthing parents and their families.
Footnotes
Acknowledgements
Author Contribution Statement
All authors contributed to the conception or design of the study or to the acquisition, analysis, or interpretation of the data. All authors drafted the manuscript, or critically revised the manuscript, and gave final approval of the version that was submitted for publication. All authors agree to be accountable for all aspects of the work, ensuring integrity and accuracy.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: National Institute for Nursing Research, grant/award number: U NR008929; Eunice Kennedy Shriver National Institute of Child Health and Human Development, grant/award numbers: U HD44219, U HD54791, U HD44226, U HD44226-05S1, U HD54019, U HD44253, R03 HD59584, U HD44245-06S1, U HD44245, U HD44, and U HD44207.