
Abstract
BACKGROUND:
Opioid use disorder (OUD) is a public health crisis and is challenging to treat. Previous research has shown correlations between OUD, abuse/trauma, and chronic pain.
AIMS:
The purpose of this study was to investigate history of lifetime sexual, physical, and/or emotional abuse among participants in a medication-assisted treatment (MAT) program for OUD, and to investigate associations between abuse history and chronic pain.
METHODS:
This is a secondary analysis of intake data from a 2-year, nonexperimental cohort treatment program of patients with OUD in rural Colorado. De-identified data were provided by 476 adult MAT patients using the Adult Addiction Severity Index (ASI-6). The ASI-6 includes three yes/no questions about history of abuse (emotional, physical, and sexual), with separate scoring for “past 30 days” and “lifetime” abuse.
RESULTS:
Lifetime history among MAT program for OUD patients was 23% for sexual abuse, 43% for physical abuse, and 58% for emotional abuse. History of physical abuse was significantly associated with having a chronic pain diagnosis, χ2 = 4.49, p = .03, and also with higher reported pain levels, t(460) = 2.71, p = .007.
CONCLUSION:
Lifetime history of physical abuse was associated with OUD and chronic pain, yet standard pain assessments do not assess these factors. In health care settings, the implementation of standardized trauma-informed screening tools, prompt recognition of abuse/trauma history, and adjunct psychological interventions may reduce stigma, reduce opioid use escalation, and help patients overcome OUD.
Introduction
Treating people with opioid use disorder (OUD) has become a daily occurrence for many nurses and other health care providers, in a variety of settings. People with OUD may present with complex, co-morbid mental and physical health issues that are difficult to assess and treat. Emergency department nurses often report this demographic to be a particularly challenging group that adds to the stressors of already-overwhelmed staff (Clarke et al., 2015). Many health care providers report that patients with substance use disorders (SUDs) are undesirable to care for, and some providers believe that SUDs are the result of character defects, lack of willpower, or simply “poor motivation” (Van Boekel et al., 2013).
The problem is that negative stereotypes about OUD and chronic pain (CP) prove countertherapeutic for patients in myriad ways. Nurses are the health care providers that spend the most time with patients (Butler et al., 2018; Cohen et al., 2012), and it is the nurse who provides medications and other interventions to treat pain. The amount of time spent, in addition to being the most trusted profession in the United States, affords nurses the opportunity to carry out health history assessments, educate patients, and make valuable recommendations for treatment and referrals (Butler et al., 2018). However, when negative stereotypes are adopted by nurses and other health care staff, the stereotypes may contribute to suboptimal care, avoidance behaviors, and premature discharges while potentially reinforcing stigma among new graduates. Judgment and avoidance of patients with OUD ultimately leads to missed opportunities for therapeutic interventions, thus worsening long-term outcomes (Lewis & Jarvis, 2019; Van Boekel et al., 2013). In the context of CP, opioid-tolerant patients with OUD are frequently labeled as “drug-seeking” and may be treated poorly as a result. Similarly, lack of knowledge about the etiology of CP disorders leads to increased stigma, resulting in inadequate pain management and reduced quality of life for people in this group (Morgan, 2014; Rupp & Delaney, 2004). This article explores the connections between lifetime history of abuse/trauma and CP in the context of OUD. Special attention is given to the emotional elements of CP, including how the experiences of sexual, physical, and emotional abuse may serve as risk factors for CP and OUD.
A significant amount of research has demonstrated associations between lifetime history of physical, sexual, and emotional abuse and SUD (Chandler et al., 2018). Adverse childhood experience (ACE) studies have provided some of the most helpful insights. A secondary review of data from Kaiser’s landmark ACE study concluded that “ACEs seem to account for one-half to two-thirds of serious problems with drug use” (Dube et al., 2003). While the connections between childhood trauma and SUD are established, little research has focused on the impact of abuse and trauma experienced throughout the lifespan, from childhood into adulthood, for OUD in particular.
Associations Between Abuse/Trauma, CP, and OUD
Emotional Factors in CP
Unexplained nonnociceptive pain states, often referred to as CP, are those in which pain is experienced in the absence of an observable physical trigger. This type of persistent local, regional, or systemic pain is often triggered by stress or inflammation (Phillips & Clauw, 2011). In addition, many nonnociceptive CP conditions are associated with psychological trauma in childhood or adulthood. Genetically determined pain oversensitivity combined with environmentally triggered neurological alterations (such as post-traumatic stress syndromes) can result in the enhanced transmission of nonnociceptive pain impulses (Spiegel et al., 2016). People with OUD are more likely to be receiving treatment for CP, depression, and anxiety (Cochran et al., 2014), which strengthens the theory that emotional distress is involved in the etiology of CP. While the literature demonstrates correlations between CP and OUD (Cochran et al., 2014; Groenwald et al., 2018; Spiegel et al., 2016), standard CP assessments do not include questionnaires that assess the emotional elements of CP, such as history of physical, emotional, and/or sexual abuse and trauma (Centers for Disease Control and Prevention [CDC], 2016). The hypothesized interrelationships between these constructs are shown in Figure 1.

Depiction of the Relationship Between Pain, Trauma, and Opioid Use.
The Role of Sexual Abuse and Trauma in Opioid Use
It is well-documented that sexual trauma is associated with increased risk of psychiatric disorders such as depression, suicide, and substance use (Felitti, 2002; Felitti et al., 1998; Leserman, 2005). In addition, a study by Spiegel et al. (2016) found that 33% of people who are dependent on prescription opioids have a lifetime history of sexual trauma. Childhood sexual abuse is associated with clusters of chronic symptoms, including chronic pelvic pain, gynecological disorders, headache, low-back pain, fibromyalgia, anxiety, panic disorders, and post-traumatic stress disorder (Leserman, 2005; Spiegel et al., 2016). Many of these conditions are routinely treated with opioid analgesics, either by providers who overprescribe opioids or by patients who self-medicate. Initially, opioids induce euphoria along with analgesia, which is a driving factor in physical dependence. Self-medication with opioids, in addition to avoidance of withdrawal symptoms, may represent an attempt to cope with the overwhelming, painful emotions that result from sexual abuse and trauma (Chandler et al., 2018; Felitti, 2002; Severino et al., 2018). Despite these known associations, people are rarely asked about a history of sexual abuse or trauma in health care environments. Although the prevalence of childhood (37%) and adult (29%) sexual abuse was high in a study conducted at a primary care clinic, only 4% of women were asked about sexual abuse/trauma history by their physician (Leserman, 2005). It is essential that assessment nurses and opioid-prescribing providers ask about their patients’ history of sexual abuse and trauma because patients may not spontaneously mention it; in a separate study from the one mentioned above, 50% of rape victims told no one at all about the experience (Finkel & Sapp, 2011).
The Role of ACEs
ACEs are stressful or traumatic events such as abuse, neglect, and household challenges experienced during the first 18 years of life (CDC, 2020). Children living in chronically stressful environments have sequelae spanning multiple developmental realms, including cognition and emotional maturity. Delayed emotional development can lead to increased risk of psychiatric problems, engagement in high-risk behaviors, relationship/interpersonal struggles, and inability to self-regulate during distressed states, all of which may predispose people to maladaptive coping mechanisms such as drug use (Bick & Nelson, 2015; Felitti, 2002; Felitti et al., 1998). History of childhood maltreatment and higher ACE scores are associated with an earlier age of both substance use onset in mid-adolescence and with a higher prevalence of initiating injection drug use (Dube et al., 2003; Rasmussen et al., 2018; Stein et al., 2017). Although the significance of ACE scoring is known, ACE assessments are not standard for patients presenting with OUD and CP.
Potential Issues With Assessing Abuse/Trauma History
Providers face several challenges when attempting to accurately assess a person’s lifetime history of physical, sexual, and emotional abuse/trauma. First, people may have difficulties recalling traumatic events due to traumatic brain injury or other health problems, resulting in memory lapses or other cognitive defects. Second, underreporting of childhood abuse or trauma is very common (Petersen et al., 2014). Survivors may fear feeling judged by others, as children and adolescents are often manipulated into feeling responsible for the abuse or told (by the abuser) that they will not be believed (Becker-Blease & Freyd, 2006; Petersen et al., 2014). As result of these factors, longitudinal follow-ups of adults with documented ACEs have demonstrated underreporting of actual abuse occurrences during initial interviews (Dube et al., 2003). Considering what is known about underreporting, it is vitally important for nurses and other health care providers to ask about history of abuse and trauma during CP assessments using supportive and compassionate language. These conversations give patients the opportunity to learn about normal reactions to abuse/trauma while providing useful information that helps clinicians make appropriate referrals to community mental health resources (Becker-Blease & Freyd, 2006).
Study Rationale
According to the World Health Organization (WHO), one in four adults (25% of the global population) was physically abused as a child, and approximately one in five women and one in 13 men have been sexually abused as children (Becker, 2016). The research reviewed above shows that people with a history of abuse/trauma may be at higher risk for developing both CP and OUDs (Quinn et al., 2016; Spiegel et al., 2016). The current opioid epidemic requires an updated trauma-informed framework to improve quality of care and patient outcomes. Nurses have the opportunity to screen for lifetime history of abuse or trauma in those seeking treatment for CP and/or OUD. The results of these assessments may open new doors to understanding and compassion, thereby reducing stigma and stereotypes among care providers while paving the way for self-acceptance and recovery among patients with OUD. A better understanding of the linkages between abuse history and current CP symptoms may also shed light on the etiology of pain and help patients with CP overcome OUD. To determine whether changes should be made to health care intake and assessment procedures, it is necessary to determine whether a significant portion of people seeking treatment for OUD may benefit. Thus, we conducted a secondary analysis of treatment program data to determine what percentage of participants in a medication-assisted treatment (MAT) program for OUD have a lifetime history of abuse. The aims of this study were to (a) investigate the history of lifetime sexual, physical, and/or emotional abuse among participants in a MAT program for OUD; and (b) investigate associations between abuse history and CP among participants with OUD.
Methods
Design
This was a secondary analysis of data from a nonexperimental, cohort-based evaluation of a program designed to increase access to MAT for people with OUD. Individual interviews by clinicians, self-guided participant questionnaires, and clinician-guided questionnaires were used to gather data from participants as part of the process of providing MAT. Data were collected using standardized forms across three clinical agencies in rural areas of Colorado (Sorrell et al., 2020). This study was a secondary analysis to quantify the percentage of participants with a lifetime history of abuse in three separate categories: sexual, physical, and emotional. Descriptive statistics were calculated on patients’ history of CP, both in aggregate and within each category of abuse.
Setting and Participants
Sample
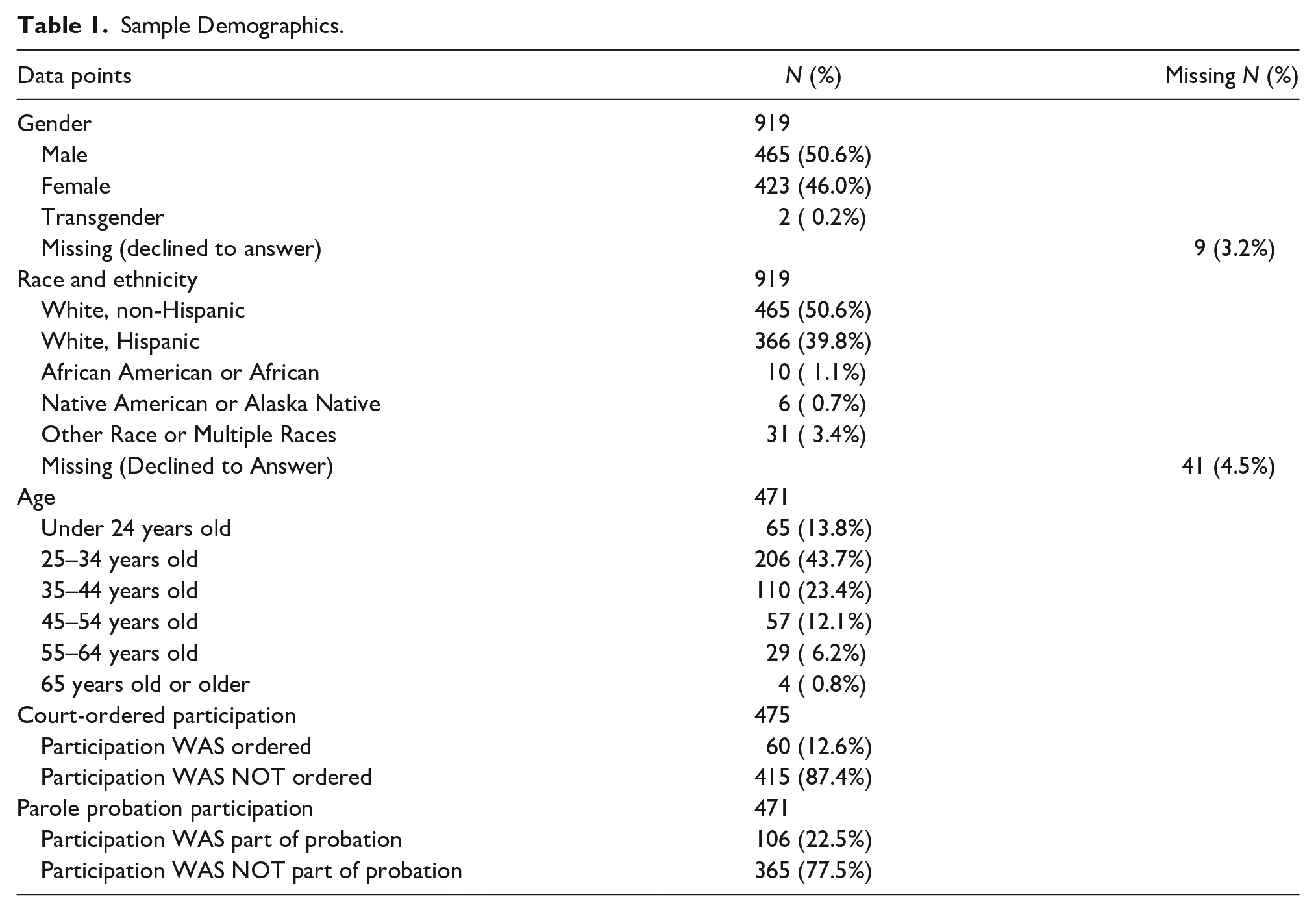
Participants were 919 adults living with OUD who were enrolled in the Pilot MAT Program, a 2-year project funded by the state legislature via Colorado Senate Bill 17-074 and coordinated by the University of Colorado College of Nursing (Sorrell et al., 2020). Participants lived in two rural counties of Colorado (Routt and Pueblo) and received care between July 2017 and June 2019. They were recruited through direct marketing (billboards, magazines, internet ads, etc.); flyers distributed in community locations such as churches or grocery stores; referrals from local primary care providers; and partnerships with local jails, courts, and emergency departments. Some participants were voluntary enrollees while others were under court-ordered enrollment. Table 1 shows sample demographics.
Sample Demographics.
Setting
Surveys and questionnaires were completed during the participant’s initial intake appointment for the Pilot MAT Program, with additional measures completed at the time that treatment actually began (e.g., suboxone induction, which often happened a few days later). Intake and treatment appointments occurred in a quiet and confidential environment at one of three MAT outpatient treatment centers. One of the treatment sites was a methadone clinic, the second was a community mental health center, and the third was a standalone outpatient pain and SUD clinic. The location of each participant’s treatment center was dependent on the participant’s county of residence. Program evaluation data were collected in the course of treatment, and no incentives were offered. The use of clinical data for secondary research was approved by the Colorado Multiple Institutional Review Board (protocol 19-1996).
Inclusion and Exclusion Criteria
The inclusion criteria for this secondary analysis of data were the same as those of the parent study (adults with current OUD living in two rural counties of Colorado), filtered for lifetime history of abuse and/or CP.
Procedure
At the beginning of treatment, participants completed a self-report intake questionnaire that included the Addiction Severity Index (ASI-6) instrument from which data were pulled for this secondary analysis. Data were collected in one of two ways: clinicians asked questions and scored the real-time answers in the electronic research database (REDCap), or participants filled out paper questionnaires that were later manually entered into REDCap by a clinician.
Data Collection Formats
Some of the ASI items are designed for interview administration and others for self-report, and the administration method for each item was consistent across participants. In addition to demographic data and an extensive health history that included both lifetime history of abuse and abuse within the past 30 days, each participant was asked about their perceived physical and mental health issues.
Missing Data
Because of the gap between intake and the start of treatment, with a tendency for incomplete data collection by clinical sites at the time treatment began, about half of patients had demographic and clinical data (intake) but no data on abuse history (self-reported at the start of treatment). This was a limitation associated with the primary clinical purpose of data collection. Because of the high rate of missing data, only those cases with complete data on all variables of interest were included in each step of the analysis.
Measures
ASI-6
The ASI-6 is a validated instrument that was used for this secondary data analysis. The ASI-6 rates addiction severity in seven areas: medical status, employment/support status, drug/alcohol use, legal status, family history, family/social relationships, and psychiatric status. The ASI-6 provides an overview of problems related to substance abuse, rather than focusing on any single complication. The summary scales are relatively independent of one another (r < .45), with trauma-related items loading on the psychiatric scale. This scale has good internal consistency (Cronbach’s α = .87), and its validity is supported by strong correlations (r > .60) with other mental health measures including the 12-item Short Form Health Survey (SF-12) and the Symptom Checklist Revised 10-item version (SCL-10R) (Cacciola et al., 2011).
Questions About Abuse
Data on history of abuse were taken from the family history scale, which includes three yes/no questions specific to sexual abuse (forced sexual advances or sexual acts), physical abuse (physical harm), and emotional abuse (harsh words). Each item was asked twice, once about lifetime history and the other about abuse within the past 30 days.
Questions About CP
The existence of CP was measured in the “Health Status” section of the ASI-6. Participants were asked, “Have you ever been told by a doctor or health care provider that you had any of the following physical or medical conditions?” If the answer was yes, participants chose from a variety of common health conditions, including an option for “Other chronic physical or medical conditions.” A yes score (1) for CP was coded only when a clinician or participant wrote “chronic pain” or a specific type of CP in the text area following “Other chronic physical or medical conditions.” To rate the severity of pain, participants were asked, “In the past 30 days: How much have you experienced physical pain or discomfort?” Participants answered the question by rating their pain or discomfort with the following scores: 0 = not at all; 1 = slightly; 2 = moderately; 3 = considerably; 4 = extremely. Participants were asked the pain severity question even if they did not report a CP diagnosis.
Data Analysis
This secondary analysis focused on the following questions: (a) What percentage of people with OUD report a history of abuse? (b) What types of abuse did this population experience? (c) What percentage of people with OUD have a history of CP? and (d) What percentage of people have a history of both abuse and CP?
The percentage of participants with a reported history of lifetime abuse in three separate categories—sexual, physical, and emotional—was determined. Descriptive statistics were used to determine the frequency of abuse, types of abuse, and CP in each group. Chi-square tests were used to analyze nonparametric data from cross-tabulation comparison tables to determine the significance of any differences in categorical outcomes between groups that had versus had not experienced each type of abuse. Pain severity ratings were analyzed using means and standard deviations, and t-tests were used for between-group comparisons on pain severity ratings.
To consider associations between OUD and CP, we included the entire data set of 919 participants. When filtering data, we treated CP as missing data when history of abuse and pain intensity data were missing, which indicated that participants had skipped that entire section of the ASI. To consider associations between OUD, CP, and history of abuse, we excluded patients who were missing data on any other answers, such as abuse history. Demographic data were complete for almost all participants. Although there was a high rate of missing data on self-report items, these data were missing at random with respect to participant demographics or any of the variables under consideration in this analysis. Local sites were not always consistent in asking participants to complete self-report sections of the ASI, and this explanation is supported by the fact that missingness was related to which site collected the data. Results are therefore considered likely to be valid despite missing data. Imputation was not used because the rate of missingness exceeded 30%; pairwise deletion was used in each analysis instead.
Results
History of Abuse
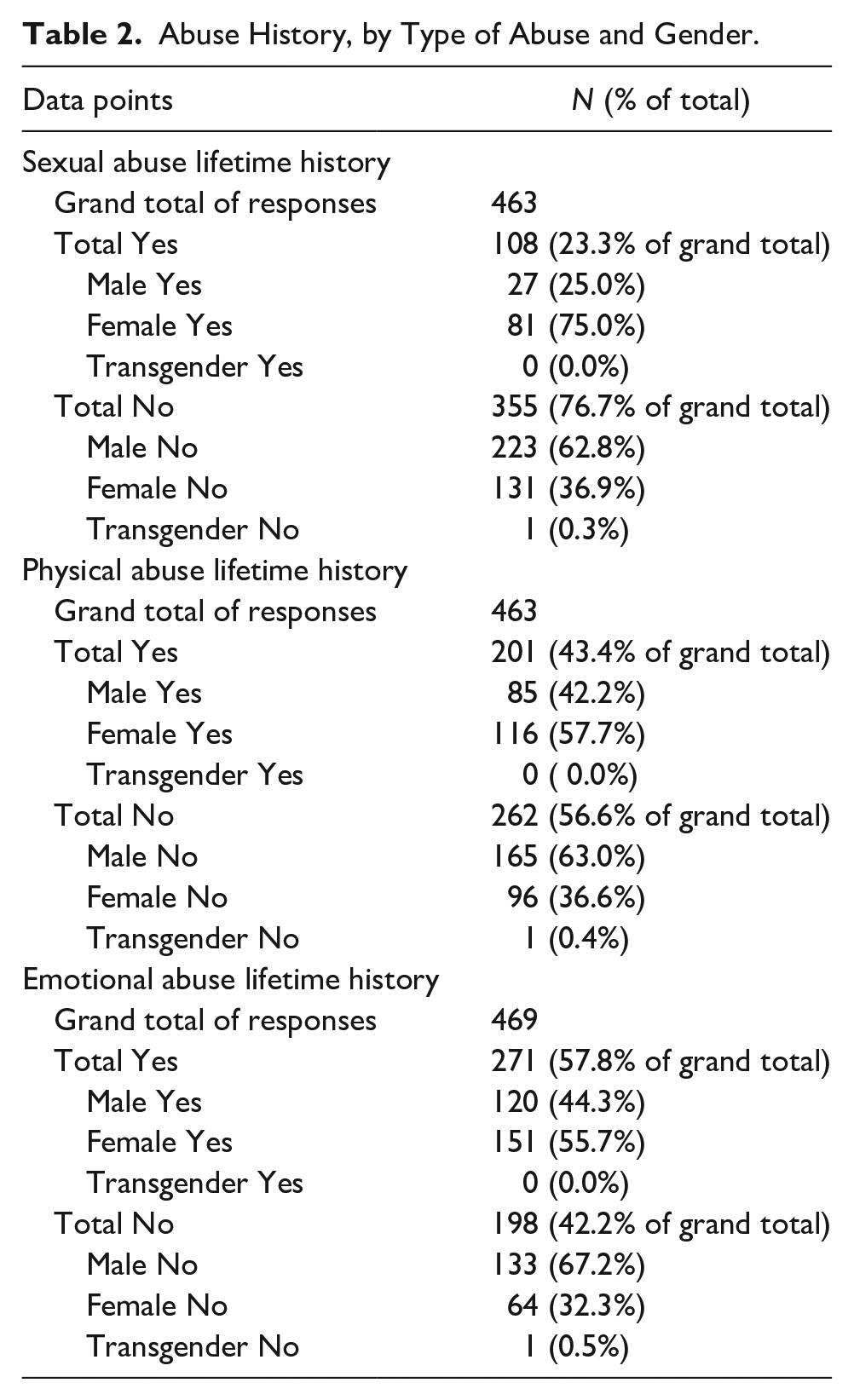
Among the responses to abuse questions (n = 463–469), 23% of participants reported lifetime sexual abuse, 43% reported lifetime physical abuse, and 58% reported lifetime emotional abuse (Figure 2). Table 2 provides detailed findings on abuse history by type of abuse and gender. None of the differences in abuse history by gender were statistically significant.
Abuse History, by Type of Abuse and Gender.
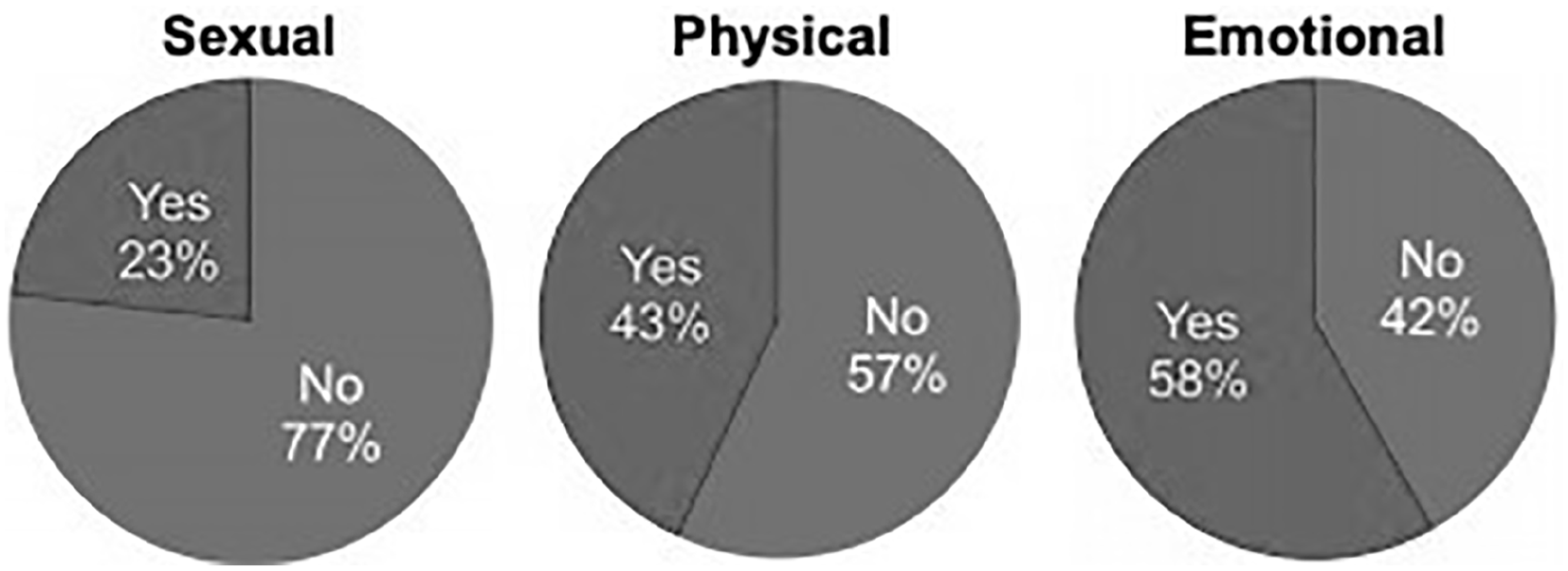
Types of Abuse Reported Among Participants (n = 463 to 469).
CP
Among 495 responses to questions about previous medical diagnoses, 21% (105 people) reported a CP diagnosis confirmed by a doctor or health care professional. Results of chi-square tests showed that a history of physical abuse was significantly associated with having a history of CP, χ2 = 4.49, p = .03, but other types of abuse were not. Also, pain scores were higher for participants with a history of physical abuse than for those without that history t(460) = 2.71, p = .007. Table 3 provides specific findings for CP history along with the association between CP history and abuse history. It is noteworthy that history of sexual abuse was not associated with CP, which was contrary to expectations based on past literature, but this result did approach statistical significance at p = .16. Although 45% of participants reported a history of emotional abuse, that history was not associated with CP (p = .46). Table 4 provides findings on CP severity with versus without history of physical abuse, and Figure 3 visually illustrates this relationship.
Chronic Pain History With Versus Without History of Physical Abuse.
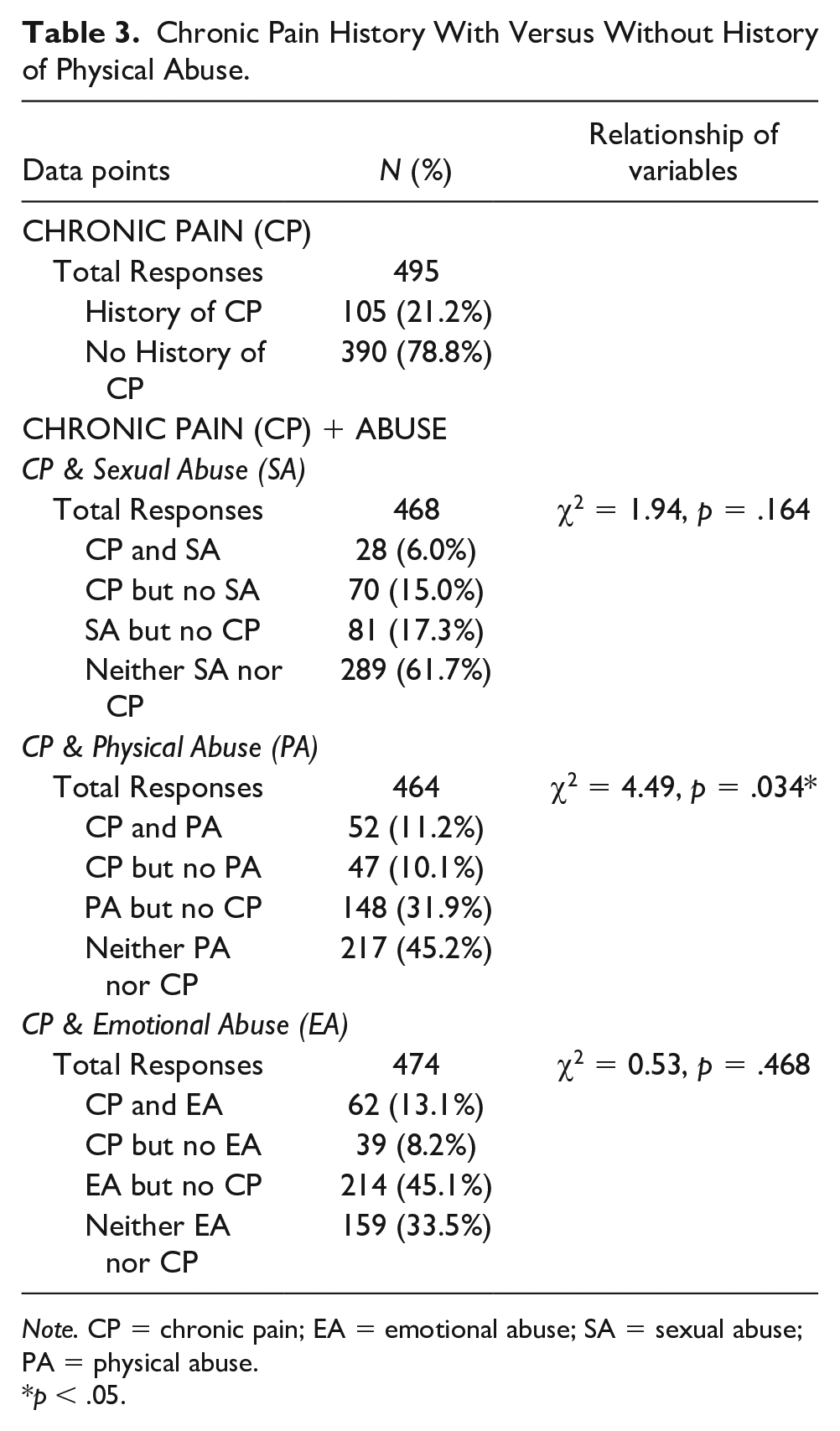
Note. CP = chronic pain; EA = emotional abuse; SA = sexual abuse; PA = physical abuse.
p < .05.
Chronic Pain Intensity With Versus Without History of Physical Abuse.
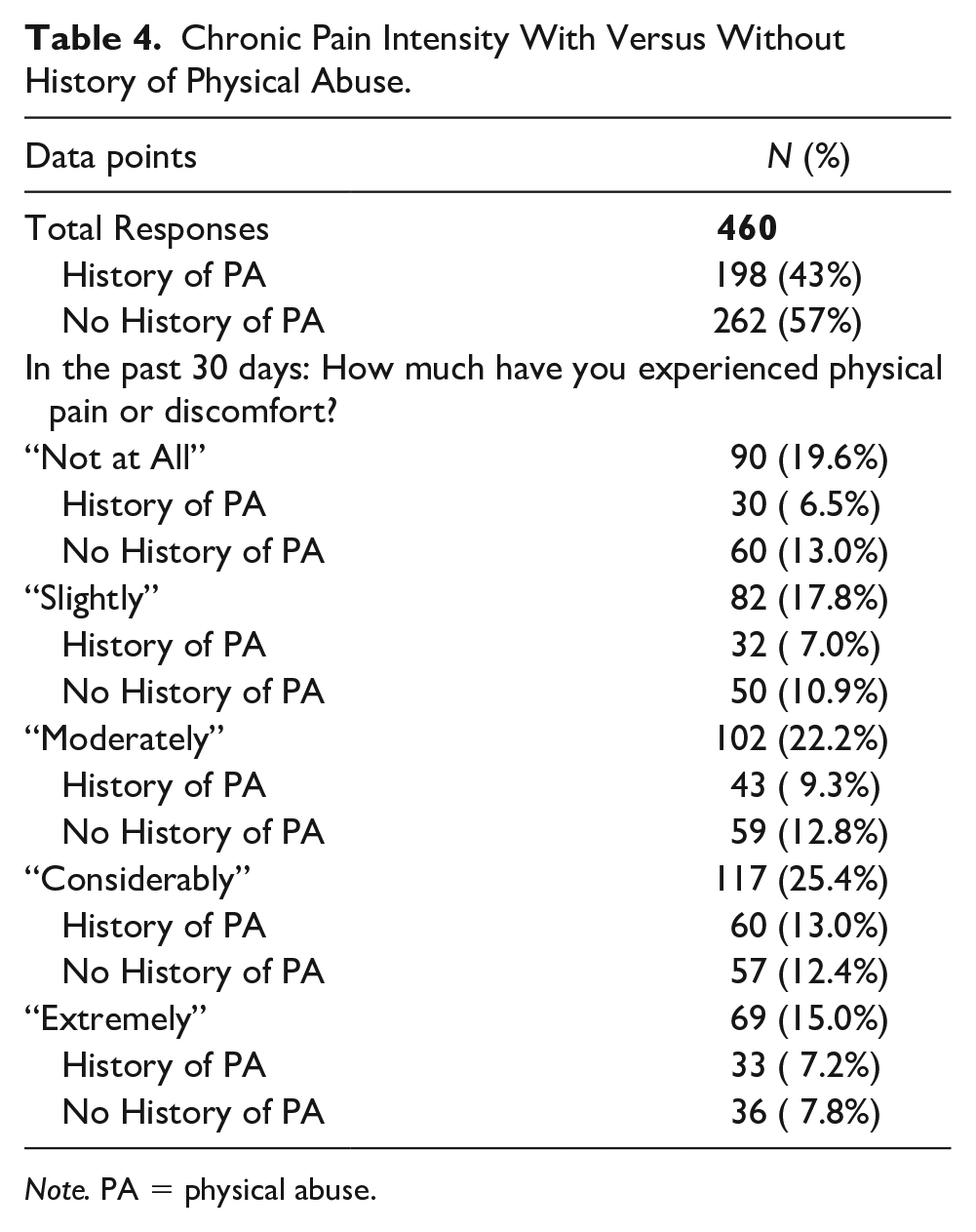
Note. PA = physical abuse.
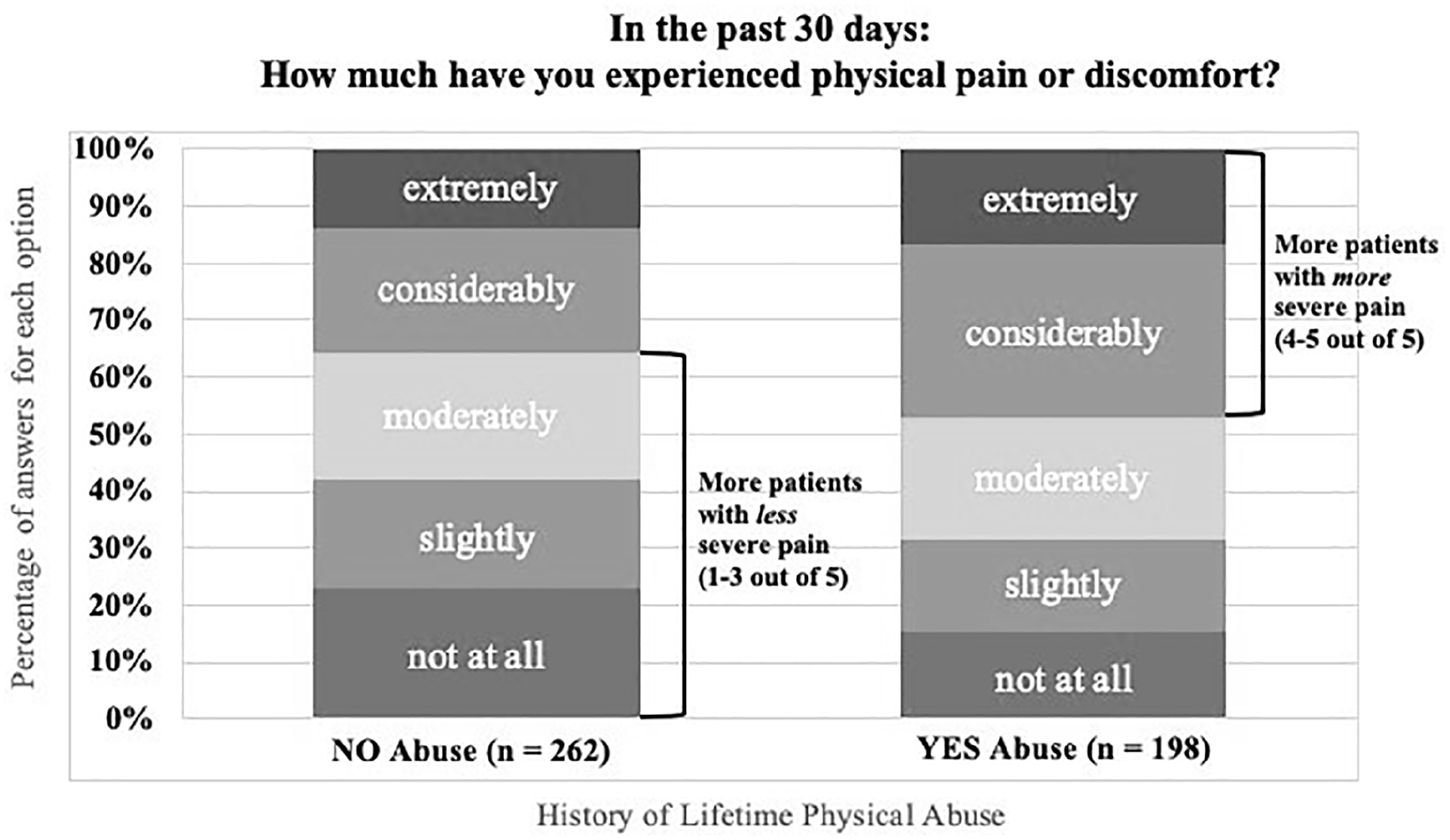
Severity of Pain (Over the Last 30 Days) Among Participants With CP, Separated by History of Physical Abuse.
Discussion
The incidence of childhood trauma and abuse among people with SUD is well-established, yet little research has focused on the prevalence of abuse or trauma sustained throughout the lifespan, from childhood into adulthood, as a risk factor specifically for OUD. The purpose of this secondary analysis was to determine the percentage of participants in a rural MAT program for OUD who had a lifetime history of sexual, physical, and/or emotional abuse, and to examine the connections between specific types of abuse, CP, and OUD. Within this population of adult participants, we found that a significant portion, ranging between 23% and 58%, reported experiencing at least one type of abuse/trauma during their lifetime. The WHO estimates that 25% of the population experiences childhood physical abuse. Forty-three percent of the MAT Program’s population reported a lifetime history of physical abuse, which is substantially higher than WHO’s global average. This finding supports Felitti et al.’s (1998) initial ACE findings; that a history of traumatic experiences (such as abuse) may predispose people to the later development of OUD.
A secondary aim of this study was to determine whether a history of abuse is associated with CP. While the bulk of previous research related to physical abuse and CP has focused on childhood abuse, physical abuse sustained during adulthood is equally damaging to mental and physical health (Howard et al., 2010). Among participants in this MAT program, a lifetime history of physical abuse was associated with greater incidence of a CP diagnosis and was also associated with worse CP severity. This association was not observed for history of emotional abuse or for history of sexual abuse, even though we had expected a connection, at least in the case of sexual abuse, based on prior literature. These findings may positively contribute to our collective knowledge about the etiology of some CP disorders, leading to decreased stigma while bolstering current pain management strategies for people in this group.
Nurses and other health care providers could benefit from a better understanding of how their patients’ trauma histories potentially predispose them to OUD or intensify their experience of physical pain. An appreciation of these factors may decrease some providers’ tendency to view OUD through a moralistic lens and increase their compassion for people receiving treatment for OUD. Similarly, appreciation of these factors among nurses may lead to the facilitation of more in-depth assessments that include asking questions about abuse history, including current abuse by a domestic partner, education about the emotional aspects of CP and OUD, and associated recommendations for the treatment plan.
Strengths and Limitations
This study’s primary strength was that data were collected from a large sample of patients in a real-world, community-based treatment program. This study’s primary limitation was the high incidence of missing data. Among the total population of 919 participants, responses for history of abuse ranged between 463 and 469. There are theoretical limitations to evaluating lifetime history of abuse and trauma in all populations, ranging from cognitive recall difficulties to an unwillingness to discuss emotionally disturbing events due to potential worries over how the information will be received (Becker-Blease & Freyd, 2006). Research on ACEs indicates that abuse history is generally underreported, a finding that is plausible to extend to this population. However, an additional challenge arose when collecting data for this study: Many participants were presenting for treatment during active opioid withdrawal, which is known to be extremely uncomfortable and to cause feelings of distress (Kosten & Baxter, 2019). Withdrawal symptoms may lead to incomplete data collection due to an unwillingness to complete questionnaires or the MAT clinician’s desire to initiate medication treatment as quickly as possible to relieve the patient’s suffering. In this data set, procedural variations by clinical site were a more plausible explanation for missing data than participant unwillingness to disclose abuse history, and data were missing at random with respect to variables of interest. The findings of this study are therefore considered to be valid despite a high rate of missing data on survey items about abuse history and CP.
Limitations in the completeness of data on CP also existed, which again varied between the three treatment sites. There were 495 responses to the medical history question, where participants could talk about CP experiences, with missing data patterns similar to those for the questions about abuse. Questionnaire wording also may have contributed to incomplete data on the CP item. Participants were asked: “Have you ever been told by a doctor or health care provider that you had any of the following physical or medical conditions?” To answer “yes,” participants required a formal diagnosis of CP from a licensed provider. The wording may have unintentionally omitted people without a formal CP diagnosis. The fact that CP was assessed based on an open-ended question rather than a standard checkbox (as was used to document past diagnoses in other areas such as diabetes or heart disease) also might have contributed to participants underreporting CP diagnoses.
Implications for Practice and Research
Despite the limitations in data collection with this vulnerable population, the total number of responses was sufficient to conclude that a history of lifetime abuse may have contributed to (or worsened) OUD in this population. In addition, a lifetime history of physical abuse may have worsened the severity of pain in participants’ CP conditions. Greater incidence or severity of CP among people with a history of physical abuse may have impacted the progression of their OUDs, a finding that is supported by the original ACE research (Felitti, 2002; Felitti et al., 1998). Physical abuse is a specific risk factor that should be assessed in patients with OUD, and that deserves further study to better understand its role in patients’ experience of CP and their use of opioids.
Conclusions
This study demonstrates that all types of abuse are common among patients with OUD and that history of physical abuse in particular is associated with pain severity and CP diagnoses. Providers are not currently directed to assess for history of abuse/trauma in populations presenting with CP prior to prescribing opioid analgesics (Dowell et al., 2016; CDC, 2016). The current guidelines suggest assessing for depression with the Patient Health Questionnaire (PHQ)-9 and anxiety with the Generalized Anxiety Disorder (GAD)-7 (CDC, 2016; Dowell et al., 2016). It is important to note that neither of the tools include abuse/trauma history.
The nurse is uniquely positioned to assess a person’s history of abuse/trauma while gathering other import-ant health history information or as part of a CP assessment. In health care settings, the implementation of standardized trauma-informed screening tools, prompt recognition of abuse- and trauma-associated CP, and provider-facilitated access to adjunct psychological interven-tions (trauma education, psychotherapy, Eye Movement Desensitization and Reprocessing [EMDR], etc.), may reduce stigma among providers and patients, reduce opioid use escalation, and help patients overcome OUD.
Drawing on what was uncovered in this data analysis, further research is warranted on abuse/trauma and the connections to CP and OUD. Ongoing research should measure history of abuse/trauma among a larger group of people. It would be worthwhile to include urban populations in addition to rural. In future studies, questions about CP should be separated from questions about other health conditions and worded to include people who have pain symptoms without a formal CP diagnosis.
In July 2019, the Colorado state legislatures authorized new legislation (Colorado Senate Bill 19-001) expanding the MAT program into 15 additional counties in Colorado. Data for this next phase of the rural MAT program will include a new 20-question, trauma- and resilience-informed screening tool called the Positive and Adverse Childhood Experiences Survey (PACES), which includes the traditional ACE questions interspersed with questions about protective factors (Leitch, 2017). This novel approach to OUD assessment may provide additional insight into an individual’s psychological strengths while measuring traditional ACE scores. Data will be used to improve treatment for trauma, OUD, and CP, with special consideration of gender differences, the impacts of abuse, and protective factors that may impact psychological resilience. A better understanding of trauma and resilience may help nurses and other health care providers contribute to more successful recovery from OUD.
Supplemental Material
sj-pdf-1-jap-10.1177_10783903221083260 – Supplemental material for Comorbidity of Lifetime History of Abuse and Trauma With Opioid Use Disorder: Implications for Nursing Assessment and Care
Supplemental material, sj-pdf-1-jap-10.1177_10783903221083260 for Comorbidity of Lifetime History of Abuse and Trauma With Opioid Use Disorder: Implications for Nursing Assessment and Care by Linda Driscoll Powers, Paul F. Cook, Mary Weber, Aimee Techau and Tanya Sorrell in Journal of the American Psychiatric Nurses Association
Footnotes
Author Contributions
All authors contributed to the conception or design of the study or to the acquisition, analysis, or interpretation of the data. All authors drafted the manuscript, or critically revised the manuscript, and gave final approval of the version that was submitted for publication. All authors agree to be accountable for all aspects of the work, ensuring integrity and accuracy.
Author Roles
L.D.P was the lead writer and clinical investigator, with faculty advisement from P.F.C. T.S was the primary investigator. P.F.C. was the lead evaluator. A.T. was the clinical director. M.W. was a clinical consultant.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was based on an unfunded student honors thesis, using data from a treatment program funded by the Colorado State Legislature (SB 17-074), with additional support from the Colorado Clinical and Translational Science Institute, NIH UL1 RR025780.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.