
Abstract
Depression and Suicide
Depression and suicide are two major public health concerns. Depression has long been accepted as a serious disability and burden globally, while suicide is a misunderstood and complex cause of death that strongly affects the quality of life and mental health of the families and communities left behind (Cummins et al., 2015). According to 2019 Global Health Data Exchange, the prevalence of major depression in the world is 2.49%, and the prevalence in Turkey is 3.35%. Suicidal behavior, which includes killing oneself, thinking about killing, and making suicidal attempts, is seen in every society and is a frequent phenomenon among those who have mental health challenges (Tanrıverdi, 2015). According to the 2018 data of the Turkish Statistical Institute, the number of annual completed suicides in our country is 3,161, and the crude suicide rate is 3.88 per 100,000 (Turkish Statistical Institute, 2019). According to the World Health Organization data, there is a completed suicide every 40 seconds and a suicide attempt every 3 seconds in the world (World Health Organization, 2017; see also Nock et al., 2013). In a study by Sabancıoğulları et al. (2015), conducted with psychiatric patients, it was found that 55.5% of the patients were at risk of suicide and that more than half of this patient group consisted of patients with mood disorders. Suicidal thoughts and suicide attempts are more common in patients with depression, who are vulnerable to suicide (Atay et al., 2012). In a study by Ateşçi et al. (2002), it was reported that nearly half (46.7%) of patients who attempted suicide were diagnosed with a depressive disorder in their psychiatric evaluation, while Aslan and Demir (2008) found that 31.3% of patients with depression had attempted suicide at some point in their lives (Aslan & Demir, 2008). Moreover, Ak et al. (2008) have reported that individuals who are susceptible to depression tend to be more hopeless and pessimistic and have a higher tendency to hurt themselves when faced with negative life events or stressors (Ak et al., 2008).
Psychache
In a test of Edwin Shneidman’s theory of suicide, analyses indicated that, relative to depression and hopelessness, psychache was the psychological variable most strongly associated with suicidality, but that depression and hopelessness did contribute unique variance in the statistical prediction of some suicide criteria (Troister & Holden, 2010). Psychache is the process of suffering from mental pain that may be due to the loss of someone, exposure to traumatic events, frustration, experiencing unexpected negative events, the inability to meet one’s basic needs (Orbach et al., 2003). Shneidman coined the term “psychache” and stated, Psychache refers to the hurt, anguish, soreness, aching, psychological pain in the psyche, the mind. It is the pain of excessively felt shame, or guilt, or humiliation, or loneliness, or fear, or angst, or dread of growing old or of dying badly, or whatever. (Shneidman, 1993, pp. 145-147)
Suicide occurs when the psychache is deemed by that person to be unbearable (Pachkowskı et al., 2019; Shneidman, 1993).
According to the results of a study conducted by Pompili et al. (2008) in 88 patients with psychiatric disorders, it was reported that patients with suicide risk experienced more psychache than patients without suicide risk (Pompili et al., 2008). While research has emphasized the central role of psychache in suicide, psychological autopsy studies have revealed that most diagnoses among suicides include affective disorders (Olie et al., 2010). Cáceda et al. (2014), in their study to investigate the relationship between psychache and suicidal ideation, found that intense psychache was associated with a recent suicide attempt in depressed patients. While psychache has mostly been associated with patients with depression, it may also be encountered by those with other illnesses and in healthy individuals (Cáceda et al., 2014).
Spirituality as a Buffer
Spirituality has been considered as an important buffer against stressful events and may help people overcome their distress and difficulties. Spirituality has many definitions, but at its core spirituality helps give our lives context. It is not necessarily connected to a specific belief system or even religious worship. Instead, it may arise from your connection with yourself and with others, the development of your value system, and your search for meaning in life (Baruah & Pandey, 2016). This concept is related to the discovery of the meaning of life and the sense of attachment to society (MahdiNejad et al., 2020; Ricci-Allegra, 2018). Spirituality is especially important from the viewpoint of medicine and psychiatry, in relation to confronting stress, pain, physical and mental illness, and grief. It is related to efforts for inspiration, dignity, praise, seeking the meaning of life, and meaningfulness even for those people who do not believe in God (MahdiNejad et al., 2020). Spirituality is the essence of a human being.
Spiritual well-being is a feeling of satisfaction that arises from one’s inner self and enhances quality of life (Bai & Lazenby, 2015). Higher levels of spiritual well-being are associated with having (1) better psychological well-being across all dimensions (negative affect, positive affect, purpose in life, positive relations with others, personal growth, self-acceptance, environmental mastery, and autonomy; Greenfield et al., 2009), (2) fewer symptoms of depression (Mills et al., 2015), (3) higher levels of life satisfaction (Cowlishaw et al., 2013), (4) less likelihood develop depression or become isolated, (5) better skills for coping with stress, and (6) higher levels of hope (Çetinkaya et al., 2007; Hiçdurmaz & Öz, 2013). A higher level of spiritual well-being is reported to make it easier for the person to cope with stressful events (Gearing & Alonzo, 2018). It has also reported that spiritual well-being was associated with fewer symptoms of depression, higher subjective well-being, higher purpose of life, more positive relationships with others, less need for social support, and higher satisfaction with life (Lawler-Row & Elliott, 2009; Yoon & Lee, 2004). Therefore, spiritual well-being can contribute positively to the health and well-being of patients, families, and communities and can help patients find meaning in the disease process (Mesquita et al., 2018).
Holistic Care and Nursing
Individuals with major depressive disorder often suffer loss of mental and social skills and also experience emotional issues (Aydemir et al., 2009). Patients with depression should be assessed with a holistic approach that encompasses the physical, social, emotional, economic, cultural, and spiritual aspects of the disorder (Ergül & Bayık, 2004). Nurses should adopt a holistic care approach when collecting data with an individual for treatment and care purposes, and also obtain information on their social conditions. Literature highlights the importance of spiritual care in nursing and suggests that there is scope for improving this dimension of care to improve the quality of life for many patients (Narayanasamy & Owens, 2008).
When examining the literature, the relationship between suicide and psychache is seen; however, the effect of spiritual well-being on these two parameters is not seen. This study aims to determine how psychache and suicide risk are related to levels of spiritual well-being in patients diagnosed with depression. The results of this study will bring to the literature the role of spiritual well-being in alleviating the psychache and reducing the risk of suicide in patients diagnosed with depression. The data are expected to contribute to the importance of providing spiritual care to patients struggling with depression.
Method
Participants and Procedure
The study used a descriptive design. The population of the study consisted of patients who were admitted to psychiatry clinics for treatment and were diagnosed with depression according to DSM-5 (Statistical and Diagnostic Manual for Mental Disorders, 5th edition). The study sample consisted of 150 patients diagnosed with depression who met the study criteria and agreed to participate. A convenience sample was used. Inclusion criteria were the following: diagnosed with major depressive disorder according to DSM-5, 18 years of age or older, no other comorbid mental disorder, and no sensory and cognitive disabilities that may interfere with communication and perception of questions.
In the assessment, the interviews with the patients were carried out in a single interview by a researcher from the psychiatric nursing department. The interviews were held in the outpatient psychiatry unit of the hospital.
Analysis Plan
The data were analyzed using SPSS version 22.0. Statistical analyses used percentage calculation, student t-test, and correlation analysis. The strength of association was expressed as odds ratios with 95% confidence intervals. The level of significance was set at p < .05.
Measures
The data were collected using an information form, the Suicide Probability Scale, Psychache Scale, and Spiritual Well-Being Scale. The data were collected through face-to-face interviews conducted by researchers in the psychiatry department between January and March 2019. The researchers introduced the questionnaire to the participants and explained the material covered. The average time for completing the questionnaires was 20 minutes. All the participants completed the questionnaires.
Information Form
The form, prepared by the researcher, contains the sociodemographic characteristics of the patients and the information about the disease. Additionally, there were questions about previous suicide attempts, self-harming behavior, self-harming thoughts, and family history of suicide attempts. These questions were arranged for participants to answer yes/no based on the patient’s self-report, and no other measurement tool was used.
Suicide Probability Scale (SPS)
SPS was developed by Cull and Gill (1989) and its validity and reliability studies for the Turkish population were conducted by Tugcu (1996) and Atlı et al. (2009). The scale is a 36-item self-report measure; it evaluates suicide ideation through four subscales (Hopelessness, Suicide Ideation, Negative Self-Evaluation, and Hostility) and a Total SPS score. Each item is rated on a 4-point Likert-type scale from 1 to 4. For these four subscales and total scales, higher scores indicate greater suicide probability. Cronbach’s alpha coefficient was found to be 0.89 in the validity and reliability study of the scale (Atlı et al., 2009). In this present study, Cronbach’s alpha coefficient for the scale was 0.69.
Psychache Scale (PS)
PS is a 13-item self-report scale developed by Holden et al. (2001). It was developed to provide a method for investigating the relationship between psychache and suicidality. A validity and reliability study on the adaptation of the scale into Turkish was performed by Demirkol et al. (2018). In this 5-point Likert-type scale answers range between “never and always” and “strongly disagree and strongly agree.” The highest and lowest scores on the scale are 65 and 13, respectively. A higher score indicates a higher level of psychache. Cronbach’s alpha coefficient was found to be 0.98 in the validity and reliability study of the psychache scale (Demirkol et al., 2018). In this present study, Cronbach’s alpha coefficient for the scale was 0.91.
Spiritual Well-Being Scale (SWS)
SWS was developed by Ekşi and Kardaş (2017) who also performed the validity and reliability study of the scale. This 5-point Likert-type scale consists of 29 items and three subdimensions, namely, “transcendence”, “harmony with nature,” and “anomie.” The highest and lowest scores on the scale are 145 and 29, respectively. A higher score indicates a higher level of spiritual well-being. Cronbach’s alpha coefficient was found to be 0.89 in the validity and reliability study of the scale (Ekşi & Kardaş, 2017). In this present study, Cronbach’s alpha coefficient for the scale was 0.91.
Ethical Principles of the Research
Before starting the study, consent was obtained from the Clinical Research Ethics Committee of Gaziantep University in accordance with the Declaration of Helsinki (Ethics Committee Decision Number 298). Moreover, written permission was obtained from the institutions where the research would be conducted. To protect the rights of individuals within the scope of the study, the purpose of the research, its duration, and the procedures to be performed during the research were explained to the individuals, and “informed consent” was obtained.
Results
Of the patients included in the study, 80% were female, 56% were elementary school graduates, 70% were living in a city center, 60% were married, and 90% were unemployed. The mean age of the patients was 40.26 ± 11.11, and the mean duration of the disease was 94.65 ± 66.44 months.
It was found that 20% of the patients had previously attempted suicide, 40% exhibited self-harming behavior, 60% thought about self-harm, and 20% had a family history of a suicide attempt.
Considering the mean total scores of the patients in patients diagnosed with depression included in the study, it was observed that the mean total scores obtained from the SWS, PS, and the SPS were 114.08 ± 14.76, 39.98 ± 12.96, and 87.10 ± 5.77, respectively (Table 1).
Patients’ Mean Scores on the Spiritual Well-Being, Psychache, and Suicide Probability Scales (n = 150).
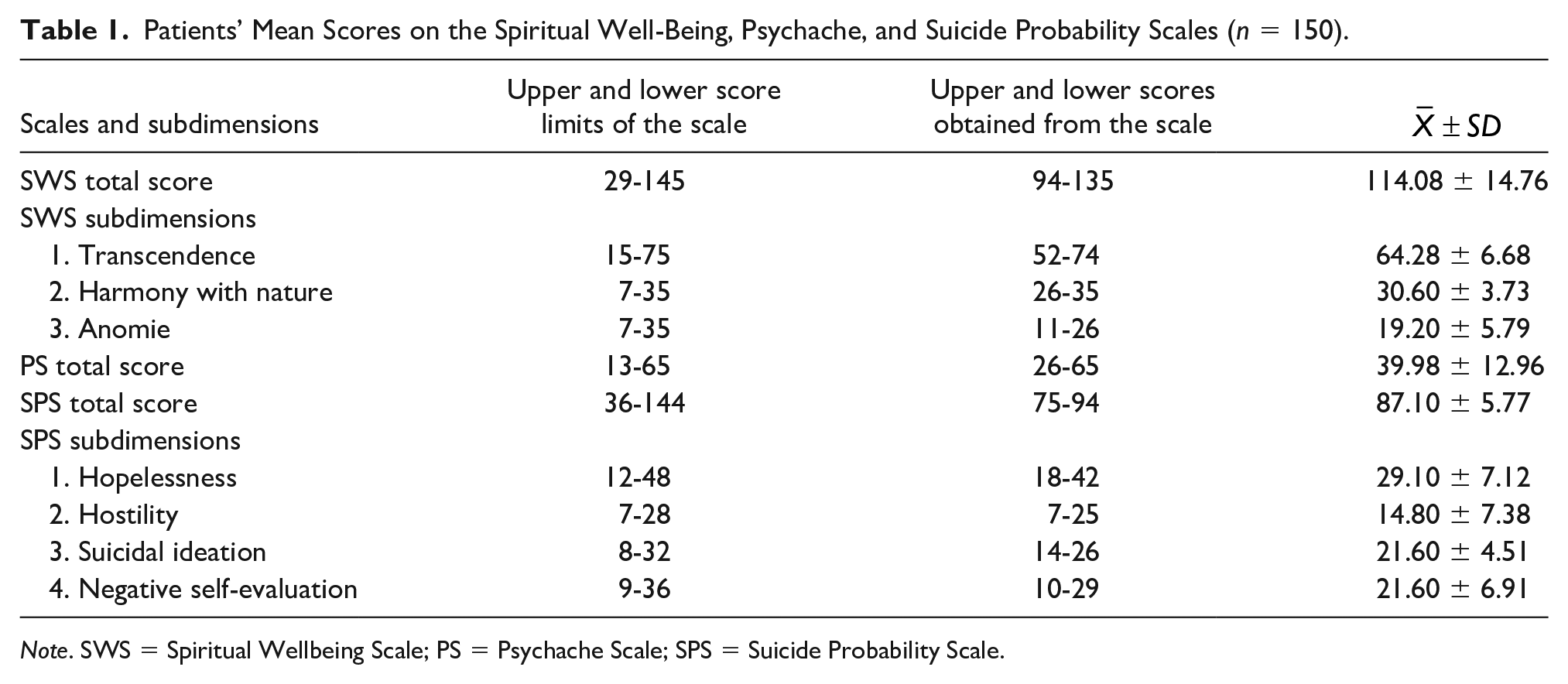
Note. SWS = Spiritual Wellbeing Scale; PS = Psychache Scale; SPS = Suicide Probability Scale.
It was found that suicide probability significantly varied according to the presence of self-harming behavior, thoughts about self-harm, and history of attempted suicide (p < .001). Patients who exhibited self-harming behavior had a higher risk of committing suicide than those who did not self-harm. Moreover, patients with depression who had a history of attempted suicide were at higher risk of committing suicide than without a history of attempted suicide (Table 2).
Comparison of Suicide Probability, Spiritual Well-Being, and Psychache Levels in Accordance With Self-Harming Behavior, Thoughts About Self-Harm, and History of Attempted Suicide in Patients With Depression.
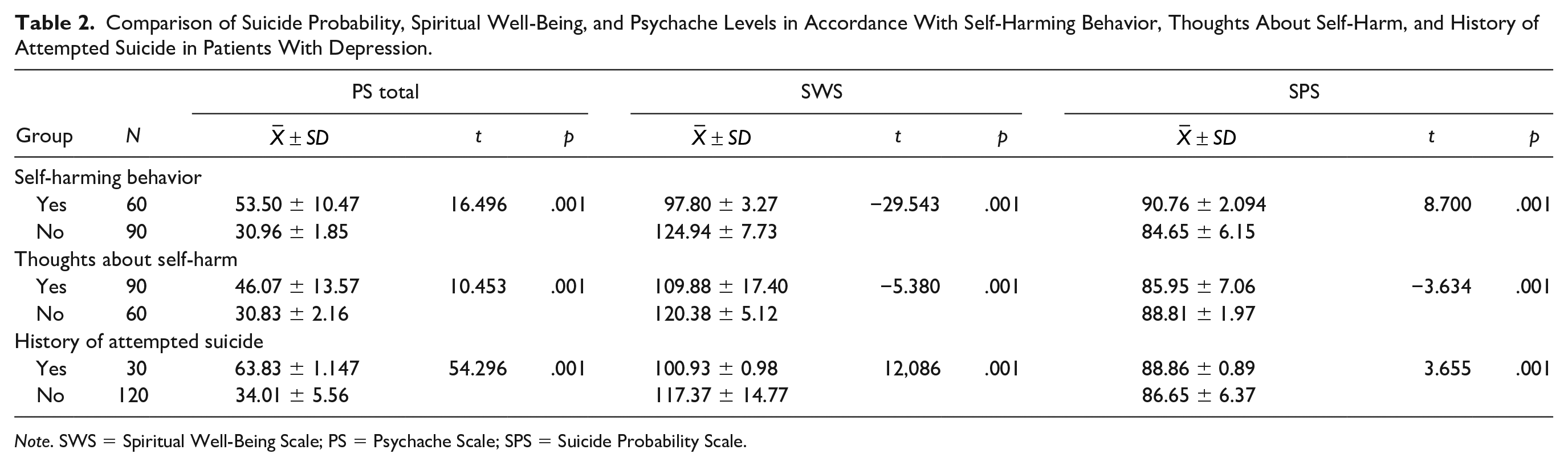
Note. SWS = Spiritual Well-Being Scale; PS = Psychache Scale; SPS = Suicide Probability Scale.
It was found that the spiritual well-being levels varied according to the self-harming behavior, thoughts about self-harm, and history of attempted suicide in patients with depression (p < .001). Accordingly, patients who exhibited self-harming behavior, thought about hurting themselves, and had a history of attempted suicide had a lower level of spiritual well-being than patients who did not possess these characteristics (Table 2).
It was found that the psychache levels varied according to the self-harming behavior, thoughts about self-harm, and history of attempted suicide in patients with depression (p < .001). Patients who exhibited self-harming behavior, thought about self-harm, and had a history of attempted suicide had a higher level of psychache than patients who did not possess these characteristics (Table 2).
It was found that a higher level of spiritual well-being led to a decreased risk of suicide and a lower level of psychache. Suicide risk increased in parallel to the increasing levels of psychache (p < .001; Table 3).
Relationship Between Spiritual Well-Being and Psychache Levels and Suicide Risk in Patients With Depression.
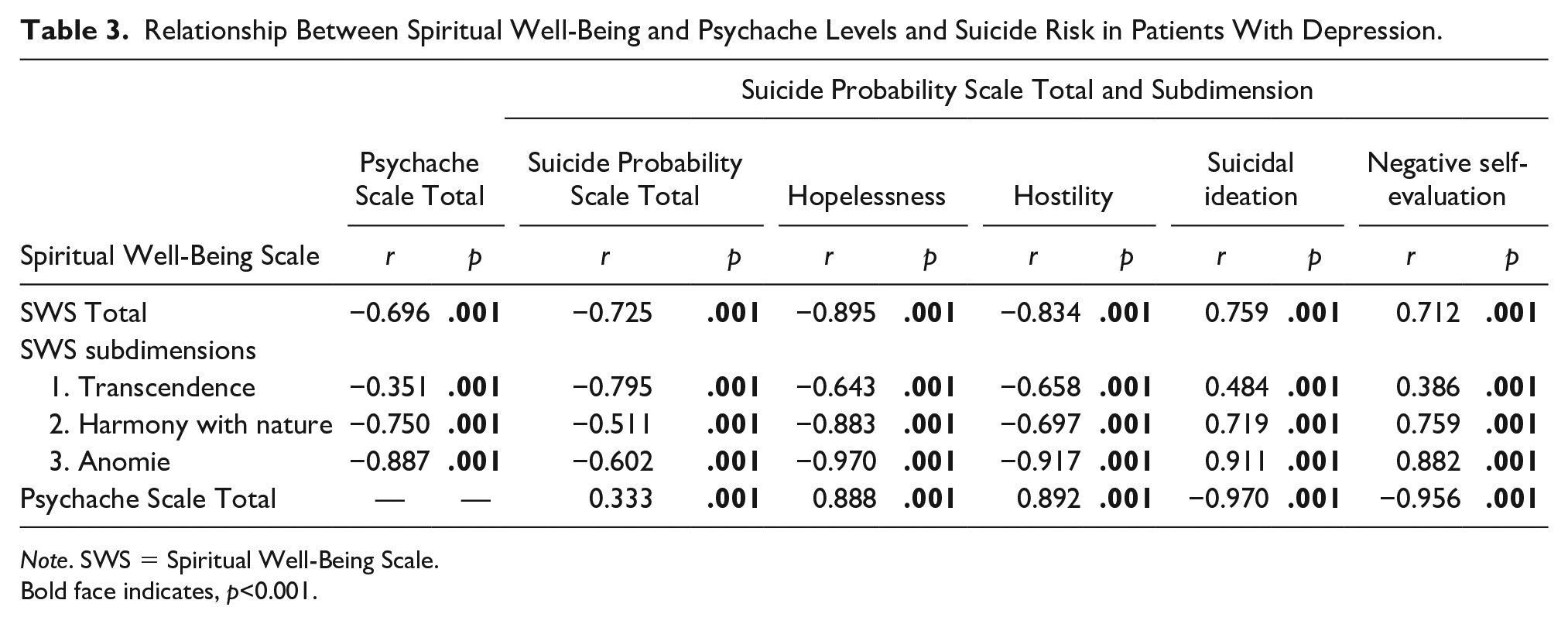
Note. SWS = Spiritual Well-Being Scale.
Bold face indicates, p<0.001.
Discussion
Most research on suicidal behavior (which includes completed suicide, intentional self-harm, and suicidal ideation) states that mental disorders play a crucial role in suicidal behavior (Amitai & Apter, 2012; Jacob, 2008). The vast majority of cases of suicidal behavior occur in the context of psychiatric disorders, and the most important is depression (Hegerl, 2016; Tanimoto et al., 2018). It is seen that the incidence of self-harming thoughts (60%) and behavior (40%) was high, and the number of patients who attempted suicide (20%) was not to be underestimated in patients diagnosed with depression in this study. In this study, it was observed that the patients were at high risk of suicide according to the mean scores obtained from the SPS. A lot of people are further driven to suicide due to the severe symptoms of their depression. Therefore, it was found that thoughts about self-harm and suicide attempts were more common in patients diagnosed with depression, as patients experience mental depression intensely (Atay et al., 2012). Suicide is generally accompanied by intense pain, hopelessness, despair, and such feelings, wherein individuals may believe that there is no solution and nothing will get better (Halter & Varcarolis, 2013). It is believed that knowing and monitoring the protective factors against suicide, along with the factors that lead to increased risk of suicide, are necessary to prevent suicide and enable mood regulation in patients.
As noted, one factor thought to cause an increased risk of suicide in patients diagnosed with depression are the level of psychache. It was determined that the depression diagnosed with patients included in this study had high levels of psychache and the risk of suicide increased with the increase in the level of psychache. In addition, patients who exhibited self-harming behavior, thought about self-harm, and had a history of attempted suicide had a higher level of psychache than patients who did not possess these characteristics. In a study by Olie et al. (2010), conducted with 62 patients who had and did not have a history of suicide, it was found that the 61 patients who had previously attempted suicide experienced a higher level of psychache. According to the results of the study by Cáceda et al. (2014), psychache is significantly higher in depressed patients with suicidal ideation than in patients without suicidal ideation. From the patients’ points of view, most suicidal patients feel that they are in a life situation of excruciating psychache without hope of deliverance (or relief; Hegerl, 2016). The psychache experienced by patients diagnosed with depression forms a foundation for suicide (Shneidman, 1993). Psychache levels are associated with suicidal thoughts and behavior. Psychache has been reported to be an important predictor of suicide risk even in individuals who have not experienced any mental illness. Psychache renders a person more vulnerable to suicide, especially in depression (Verrocchio et al., 2016). Nurses need to explore new ways to increase the validity of suicide risk assessments. One method of achieving this could be the assessment of psychache (Verrocchio et al., 2016). The fact that psychache is at the core of suicide should be handled as an important concept in routine assessments and in encouraging innovative therapeutic strategies to prevent suicide (Ducasse et al., 2018).
This study also investigated spiritual well-being levels, which are thought to be potentially protective against suicide in patients with depression. The patients included in this study had a high level of spiritual well-being according to the mean scores they received from the SWS. This can be attributed to the frequent use of religious coping methods, which is an element of spirituality, to fight depression in Turkish culture (Bahar, 2012).
In this study, patients who exhibited self-harming behavior, thought about self-harm, and had a history of attempted suicide had a lower level of spiritual well-being than patients who did not possess these characteristics. Also, it was found that an increased level of spiritual well-being led to a decreased risk of suicide and lower levels of psychache. Spiritual wellness helped individuals cope with distress and stressful situations (Fischer et al., 2010). Valuing things and people, pursuing this attitude to life, and conducting spiritual practices act as a buffer against suicide (Harder et al., 2012). In the Muslim Turkish society, spiritual beliefs have also protected people from suicide, as these beliefs dominate one’s approach to one’s health and lifestyle from birth until death. Moreover, religious limitations (i.e., the fact that committing suicide is seen as a sin) positively affect the health behavior of individuals, thereby leading to a decreased risk of suicide by helping them cope with psychache. Studies investigating the relationship between spirituality and suicide generally agree on the notion that spiritual practices prevent bad habits, increase levels of hope, lead to a lower tendency for depression and isolation, and help individuals better cope with stress (Boztilki & Ardıç, 2017).
This study includes the relationship between levels of spiritual well-being and psychache and suicide risk in depression to the literature, enriching assessment areas for mental health, and lays the groundwork for new studies.
Although our study demonstrates notable strengths, important limitations remain. First, this study’s cross-sectional design makes causal conclusions tenuous. Given the dearth of longitudinal studies on spiritual perceptions and suicide risk specifically, the extent to which spiritual perceptions and psychache cause suicide remain uncertain. Second, while this study examines the associations among spiritual well-being and psychache and suicide risk, this study does not address the differences in terms of potentially important subgroup differences. Third, the variables were evaluated only with the self-report tool.
Conclusion
In conclusion, the participants in this study had good levels of spiritual well-being, had high psychache, and also had high suicide risk. Higher levels of spiritual well-being may promote a significantly lower risk of suicide and lower levels of psychache. Likewise, increasing levels of psychache may lead to an increase in suicide risk. As the people who regularly communicate with patients, psychiatric nurses should assess the suicide risk and psychache level through the scales we used in the study, using their observation and questioning skills to prevent suicide or other harmful behaviors before they occur. They can reduce the risk of suicide and alleviate level of psychache in these patients by improving the level of spiritual well-being by providing therapeutic interventions.
Footnotes
Acknowledgements
The authors would like to thank all participants of the present study.
Author Roles
All authors contributed to the conception or design of the study or to the acquisition, analysis, or interpretation of the data. All authors drafted the manuscript, or critically revised the manuscript, and gave final approval of the version that was submitted for publication. All authors agree to be accountable for all aspects of the work, ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.