
Abstract
BACKGROUND:
Although several studies have recently described compassion satisfaction (CS), burnout (BO), and secondary traumatic stress (STS) in nurses, few to date have examined these issues across nursing specialties. Such examination is needed to inform future nursing-subspecialty tailored interventions.
AIMS:
To examine (1) differences in CS, BO, and STS across nursing specialties and (2) differences associated with demographic, work-related, and behavioral factors among nurses.
METHOD:
A secondary analysis of survey responses from nurses (N = 350) at an academic medical center. Demographic, behavioral, work-related, and professional quality of life variables were analyzed using hierarchical regression analyses.
RESULTS:
CS, BO, and STS scores significantly varied across specialties with emergency nurses experiencing significantly elevated rates of BO and STS, and lowest rates of CS; scores were also differentially associated with demographic, work-related, behavioral, and workplace violence variables.
CONCLUSIONS:
Key differences in CS, BO, and STS by nursing specialty suggests the importance of tailoring BO and STS mitigative interventions. BO and STS risk factors should be assessed in nurses (e.g., behavioral health problems and poor sleep quality) and specialty-specific interventions (e.g., reducing workplace violence exposure in emergency settings) may be considered to improve CS while reducing BO and STS among nurses.
Keywords
Introduction
With the increased health care system demands and challenges inherent in caring for patients with a greater complexity of needs, there is an ostensible deficit in patient reported experiences of compassionate care (Lown et al., 2011). Providing proficient care encompasses several processes, skills, and motivations among which compassion is arguably a central concept (Van Der Cingel, 2009). Compassionate care, an application of compassion during care delivery, requires actions that facilitate the healing process motivated by the desire to alleviate suffering (Burnell, 2009). Although these concepts are not often accentuated during nursing care activities, their implementation is associated with enhanced patient, provider, and health care system outcomes (McClelland et al., 2018). Hence, it is critical to understand factors that affect the experience and delivery of compassionate care among nurses.
Although compassion is often directed toward patients, it may be argued that nurses’ “self-directed” compassion maintains an integral role in the domain of care delivery. In fact, the ability to compassionately care for one-self is often proportional to one’s ability to render and be satisfied with such care provided to others (Duarte et al., 2016). Moreover, nurses’ compassion satisfaction (CS), the pleasure derived from providing care that alleviates the suffering of others, is a key aspect of job engagement and competence (Audin et al., 2018; Sacco & Copel, 2018; Zakeri et al., 2021). However, few studies have assessed methods to enhance CS among nurses.
In contrast, interventions to prevent, mitigate, or treat compassion fatigue (CF) have gained much traction in the past two decades (Sinclair et al., 2017). As a concept, CF has received criticism for being ambiguous in its ability to sufficiently explain the nature of fatigue resultant from “compassion” (Gerard, 2017; Ledoux, 2015). Nevertheless, it has been accepted as a clinically relevant and robust construct, with recent conceptual models proposing its emergence stemming from the multifaceted relationships between organizational and interpersonal factors (Coetzee & Laschinger, 2018; Sinclair et al., 2017). Extensive reviews of the literature also propose the central role of “empathic distress” in causing CF and that such distress may result from both interpersonal and environmental factors encountered by a care provider (Sinclair et al., 2017). Among nurses, CF is associated with demographic (e.g., age, marital status, gender, and having children), work-related (e.g., work-tenure and violence exposure), and behavioral (e.g., substance use, sleep duration, and exercise) factors (Jarrad et al., 2018; Kawar et al., 2019; Kelly et al., 2015; Merk, 2018; Okoli et al., 2020; Ortega et al., 2018; Semerci et al., 2021; Sorenson et al., 2016; Zerach & Shalev, 2015). However, few studies have examined these factors across nurses from different specialties, despite the evidence of significant differences in CF experiences across specialties (Lisle et al., 2020). Such inquiry is important to identify targets for creating tailored interventions to address CF which are specialty specific.
A closely related concept to CF that has also been a large focus of study is burnout (BO). BO results from long-term exposure to chronic workplace stress affecting the mind and body (Kelly, 2020; Maslach & Leiter, 2016). In fact, the World Health Organization (2019) has identified BO as a diagnosed condition, characterized by emotional exhaustion, cynicism, and detachment, which often leads to illness, fatigue, and depression (Maslach & Leiter, 2016). This sustained exposure to stress and increased risk of depression, coupled with nurses’ expected selfless behavior and moral obligation to their patients, accentuates BO and may increase their vulnerability to the risk of suicide compared with non-nurses (Davidson et al., 2019; Maslach & Leiter, 2016). Furthermore, other factors associated with exacerbation of BO in health care providers include identifying as non-heterosexual, being female, geographical region, ethnicity, smoking, and health care subspecialty (Merces et al., 2020; Samuels et al., 2021; Xie et al., 2021). While the average nursing BO rate remains elevated at 35% to 45%, levels vary among specialties, with BO rates among emergency department nurses around 82% (Dyrbye et al., 2019; Muir & Keim-Malpass, 2020a). Furthermore, 20% of all turnovers can be attributed to BO, demonstrating BO’s dramatic effects (Muir & Keim-Malpass, 2020a). Though BO is detrimental to a nurses’ health, it also negatively affects patients and the health care system. While it costs upward of $56,000 to replace one nurse, this amount does not cover the financial implications of BO that may accrue from the potential connection to medication errors, hospital-acquired infections, or increased length of patient stay (Cimiotti et al., 2012; Muir & Keim-Malpass, 2020b). Knowing the vast psychological and financial impacts associated with BO, there is no better time to discern unique detriments based on specialty that yield higher levels of BO. Specified knowledge on specialty levels may help to tailor needs and decrease BO among nurses.
In addition, secondary traumatic stress (STS) is another concept often conflated with CF and BO with detrimental outcomes within the nursing literature (Arnold, 2020). Conceptually, STS is a posttraumatic stress–like response that may develop after an exposure to the experienced trauma of another individual rather than experiencing the traumatic event themselves (Arnold, 2020). Additionally, the rate of STS development is higher among those who share an empathetic connection with the person who experienced the traumatic event (Beck, 2011). Considering that a core element of nursing is the ability to empathetically connect with patients, STS has high global prevalence rates among nurses as high as 52.5% (Zhang, Han et al., 2018). STS has specifically been shown to have high prevalence rates in psychiatric, emergency, labor and delivery, and oncology nurses (Beck, 2011; Beck & Gable, 2012; Mangoulia et al., 2015; Morrison & Joy, 2016; Zhang, Han et al., 2018). Nurses who experience STS report a variety of deleterious effects including increased anxiety and depression, reduced perceived social support, increased emotional strain from their work, lower levels of occupational commitment, an increased use of sick time, and reductions in both CS and clinical competence (Arnold, 2020; Bock et al., 2020; Hamama et al., 2019; Zakeri et al., 2021). Furthermore, STS in psychiatric nurses is associated with an increased desire to leave psychiatric nursing (Mangoulia et al., 2015). As 44% of the psychiatric nursing workforce was over the age of 56 years as recently as 2018 (Phoenix, 2019), it is prudent to address factors like STS which may serve to alienate current and future psychiatric nurses from the field.
The purpose of this secondary analysis was to examine demographic, work-related, and behavioral factors associated with CS, BO, and STS between nurses from different subspecialties. Thus, among nursing staff at an academic medical center, the specific aims of this study were to
Examine degree of CS, BO, and STS by different subspecialties
Determine demographic, work factors, and behavioral correlates of CS, BO, and STS
Such an examination would be useful to determine if targeted (i.e., interventions for a specific specialty) and/or tailored (i.e., interventions based on an individualized characteristics) approaches are needed to enhance CS while ameliorating the effects of STS and BO among nurses (Kreuter & Skinner, 2000).
Method
Design
This study is a secondary analysis of data obtained from a previous cross-sectional study using a convenience sample of health care workers at a large academic-medical center. As previously described by Okoli et al. (2020), institutional board approval was obtained from the institution associated with the academic medical center. Invitations to participate in an anonymous, voluntary 10-minute electronic survey were sent out to health care workers through an organizational email listserv managed by hospital administrators from November 2018 through April 2019. After the initial request, reminder emails were sent monthly through the same listservs to further prompt potential participants to consider the invitations. After reading a cover letter and providing informed consent, participants provided responses using the Qualtrics software platform that is encrypted to Health Insurance Portability and Accountability Act standards.
Sample
During data collection of the parent study, 358 nurses (12% of total respondents) completed the survey including 8 Licensed Practical Nurses (LPN), 71 with an Associate’s Degree in Nursing, 228 with a Bachelor of Science Degree in Nursing (BSN), 21 with a Master of Science in Nursing or a Doctor of Philosophy degree, and 30 advanced practice nurses (APRN)/clinical nurse specialists (CNS). For this secondary analysis, due to low participation, we excluded the 8 LPNs that responded to the survey because for statistical analyses, the subsample size of 8 LPNs would be too few to properly compare differences between nursing licensure groups (Harrell, 2001; Schmidt, 1971). Thus, the analysis is based on 350 registered and advance practice nurses.
Measures
Demographic Variables
Demographics included gender, sexual orientation, age in categories, marital status, presence of children in the household.
Work-Related Factors
Work-related factors included education level, department worked, work setting (inpatient vs. outpatient), duration of time practiced in discipline, population served (adult vs. pediatric), shifts worked, duration of employment at current department, typical hours worked during a shift, and witnessed/experienced workplace violence.
Behavioral Factors
Behavioral factors included average hours of sleep per night, perception of sleep quality (Cappelleri et al., 2009), average number of days in the past week spent exercising for 30 minutes or more (Milton et al., 2011), current tobacco use, secondhand smoke exposure, last alcohol use, prior diagnosis of a behavioral health problem, and having ever received professional services for trauma.
Main Outcome Variables
The Professional Quality of Life Scale was used to determine CS, BO, and STS (Stamm, 2009). Each construct contained a subscale of 10 questions assessed with a Likert-type scale from 1 (never) to 5 (very often). Total subscale scores range from 10 to 50, with greater scores indicating a higher degree of the outcome variable. Each subscale’s Cronbach’s alpha was adequate (CS α= .92, BO α= .83, and STS α = .82).
Data Analysis
Substitutions for missing data were made by using mean or modal replacements. Means with standard deviations or frequencies with percentages were used to describe the continuous and categorical variables, respectively, in the sample. Differences in CS, BO, and STS across specialties were examined using analysis of variance. All assumptions were met for linear regression. To assess correlates of CS, BO, and STS, three hierarchical multivariate linear regression analyses were modeled by first entering demographic, followed by work-related, followed by behavioral variables, and last experience of workplace violence. Analyses were conducted using IBM-SPSS version 27 with an alpha level of .05.
Results
Sample Characteristics
The sample was mostly female (91.7%), heterosexual (94.6%), less than 36 years old (58.3%), married (54.3%), and without children in the home (54.6%). Most respondents were BSN prepared nurses (65.1%), working in medical–surgical units (35.4%), primarily serving adults (64.6%), and caring for inpatients (90.6%). Furthermore, more than half worked day shifts (63.1%), worked shifts that were 10 hours or more (83.4%), and had been working for more than a year in their current department (74.0%) and discipline (81.5%). Almost half of the respondents reported less than 7 hours of sleep per night (48.3%), few were exposed to secondhand tobacco smoke (M = 2.0, SD = 2.3) and currently used tobacco products (12.6%), but most respondents reported alcohol use (92.0%). Participants endorsed an average of 2.9 (SD = 1.8) days of exercising at least 30 minutes a day during the week, and self-reported moderate sleep quality (M = 5.7, SD = 1.9). Nearly a quarter reported a prior behavioral health diagnosis and had received trauma treatment. More than half reported witnessing and more than one third had experienced workplace violence (see Table 1).
Sample Characteristics.
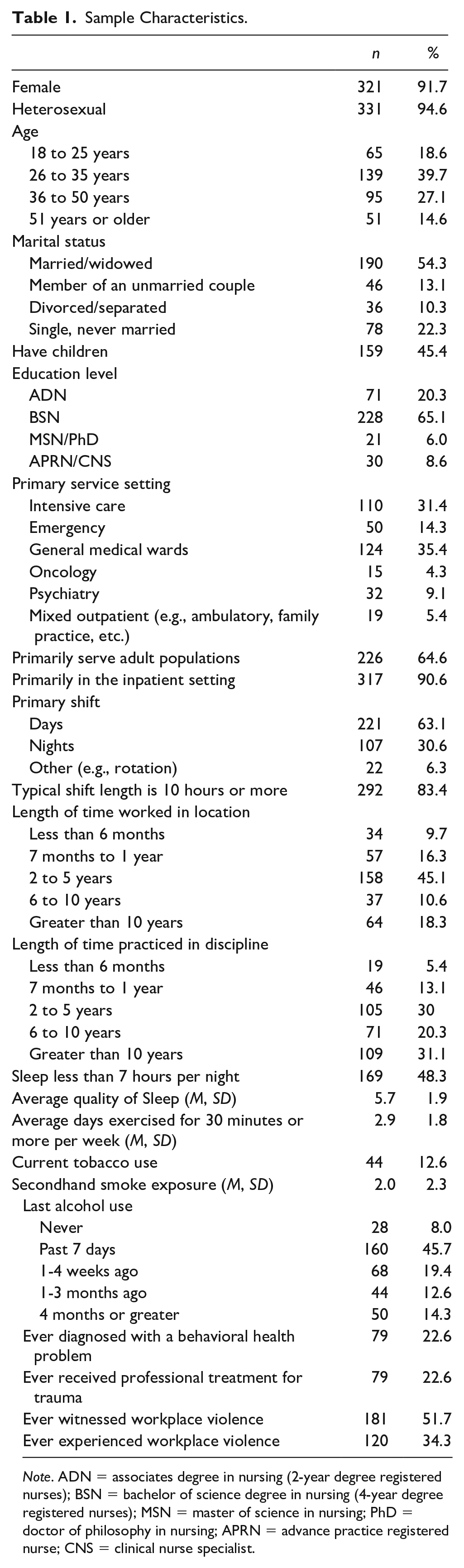
Note. ADN = associates degree in nursing (2-year degree registered nurses); BSN = bachelor of science degree in nursing (4-year degree registered nurses); MSN = master of science in nursing; PhD = doctor of philosophy in nursing; APRN = advance practice registered nurse; CNS = clinical nurse specialist.
Frequency of CS, BO, and STS and by Specialty
CS (M = 37.9, SD = 6.5) and BO (M = 24.3, SD = 6.1) scores were average, and STS scores (M = 22.9, SD = 6.1) were low. CS scores were negatively correlated with BO scores (r =−.72, p < .0001) and had a negative but low correlation with STS scores (r = −.25, p < .0001). In addition, BO scores were positively and moderately correlated with STS scores (r = .57, p < .0001).
There were significant differences in CS (F = 3.1, p = .009), BO (F = 3.7, p = .003), and STS (F = 3.6, p = .003) scores (see Figure 1) across nursing specialties. Nurses engaged in oncology services had higher CS scores as compared with those in intensive, emergency, medical–surgical units, and psychiatric services; and outpatient nurses had higher CS scores than those in emergency and medical–surgical unit nurses. Outpatient nurses had significantly lower BO scores than those in intensive, emergency, medical–surgical units, and psychiatric services; and oncology nurses had lower BO scores than those in emergency services. Emergency and intensive nurses indicated elevated STS scores compared with other groups.
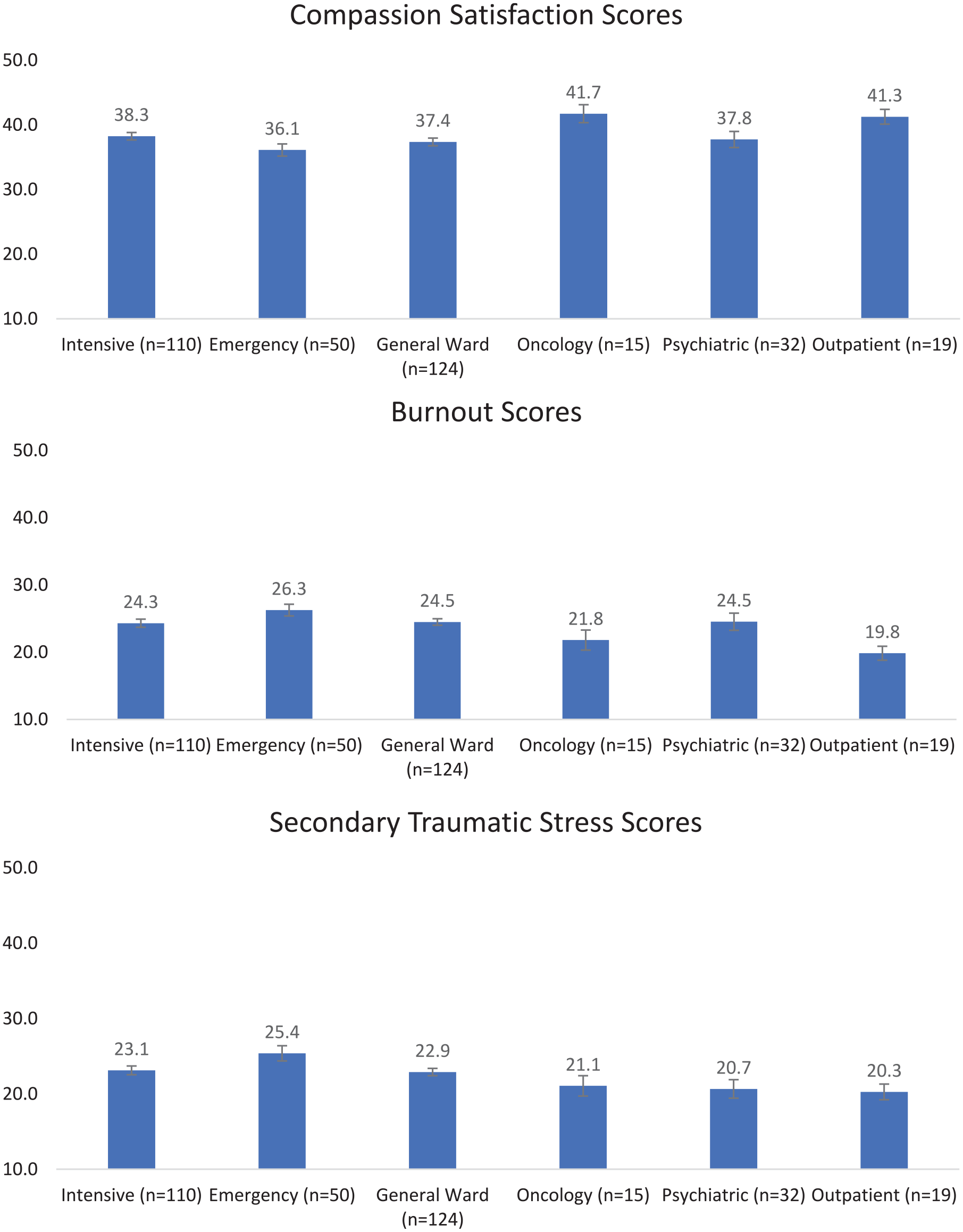
Compassion satisfaction, burnout, and secondary traumatic stress scores by specialty.
Hierarchical Multivariate Regression Analysis
We performed a hierarchical regression analysis assessing correlates of CS, BO, and STS. In the first hierarchical regression analysis (Adj R2 = .15, F = 2.82, p < .0001), variables associated with higher CS scores were being divorced/separated (compared with being single), serving the pediatric population, and not ever having experienced workplace violence. In the second hierarchical regression analysis (Adj R2 = .24, F = 4.12, p < .0001), variables associated with BO scores were being single (as compared with being married or divorced/separated), being BSN prepared (as compared with APRN/CNS), working in the adult population, rating poorer quality of sleep, reporting a prior behavioral health diagnosis, having practiced a longer duration of time in the discipline and having experienced workplace violence. In the final hierarchical regression analysis (Adj R2 = .09, F = 2.03, p = .001), variables associated with STS scores were rating poorer quality of sleep and having witnessed workplace violence.
Discussion
In the complex and dynamic health care environment of today, it is imperative that employers and institutions recognize and intervene when the well-being of the caregivers, particularly nursing professionals, is impaired. While it has been previously determined that, in general, nurses may have alterations in CS, BO, and STS (Guo et al., 2018), there are certain nuances to nursing specialties that cannot be ignored. Our present study found that, indeed, there are different levels of CS, BO, and STS reported by nurses from different specialties. Moreover, our analysis identified variables associated with CS, BO, and STS in nursing professionals at a large, tertiary care, academic medical center that serves a variety of adult and pediatric patients. The findings of our study provide important evidence for the development of future targeted and tailored programs to improve CS, BO, and STS for nurses serving different specialty populations.
The levels of CS, BO, and STS in our sample are lower than scores revealed in a recent meta-analysis of 71 pooled studies among health care providers globally (Cavanagh et al., 2020). In the meta-analysis, rates of CS, BO, and STS were 41.8 (95% CI [40.1, 43.5]), 28.4 (95% CI [26.3, 30.4]), and 25.8 (95% CI [23.3, 28.3]), respectively, compared with our current findings of 37.9 (95% CI [37.2, 38.6]), 24.3 (95% CI [23.7, 25.0]), and 22.9 (95% CI [22.3, 23.5]). Moreover, although marital status was associated with both CS and BO in the current study, recent studies have found no consistent influential demographic factors (Zhang, Zhang et al., 2018). Nevertheless, among behavioral- and work-related correlates identified in our study, our findings are consistent with others in that work-tenure, having a history of stress or behavioral problems, and experiencing workplace violence can affect CS, BO, and STS (Yu et al., 2021; Zhang, Han, et al., 2018; Zhang, Zhang, et al., 2018).
We further found differences in our main outcomes by educational groups in our study. Specifically, nurses with a BSN reported more BO than nurses with advanced degrees. Our finding conflicts with a recent meta-analysis which reported that having a bachelor’s education was inversely related to BO and CF (Zhang, Zhang et al., 2018). However, in their meta-analysis, these investigators regarded a bachelor’s and master’s as “advanced education” which limits comparability to our subsample of just bachelor’s prepared nurses. In our study, bachelor’s prepared nurses may have exhibited increased BO compared with graduate-level education prepared nurses because most bachelor’s nurses are providing direct patient care, while nurses with graduate degrees are more likely to be in advanced practice, leadership, or administrative roles, thus, further removed from direct clinical care.
We also observed CS, BO, and STS differences among nurses working with various specialties. Nurses who cared for oncology patients had increased CS compared with other specialties, and lower BO compared with emergency nurses. This finding is similar to other investigators who reported elevated CS and diminished BO among oncology nurses (Wu et al., 2016). These heightened levels of CS and lower BO might be related to the relationships forged between oncology nurses and their patients and how the context of cancer care is rewarding for both the nurse and the patient, while emergency and intensive care nurses may experience more BO from a lower perception of positive relationship with their patients (Converso et al., 2015; Mooney et al., 2017). Furthermore, our analysis showed that outpatient, or clinic-based, nurses reported lower BO than those in intensive care, emergency, general ward, and psychiatric services. This finding is congruent with a recent investigation by Shah et al. (2021) who found an 80% increased risk of BO among staff caring for inpatients, as compared with those caring for patients in clinic-based settings. Finally, we found that both emergency and intensive care nurses have higher STS levels compared with other specialties. Our finding is similar to other investigators who also reported that both intensive care and emergency nurses have prevalent STS (Ayala & Carnero, 2013; Kelly & Lefton, 2017; Morrison & Joy, 2016). The current study adds to this existing knowledge by identifying further work, demographic, behavioral, and psychosocial variables associated with CS, BO, and STS among nurses across specialties.
Limitations
There are important limitations to consider when interpreting our findings. As in any cross-sectional study, no causality can be inferred between variables. As such, longitudinal studies would be required to elucidate the direction of the relationship between variables. In addition, as a secondary analysis of existing data, we were limited in the number of variables with explanatory power for our outcomes. For example, the variables in the STS model only explained about 9% of the variance in predicting STS. Other known factors such as empathy, coping capacity, and job satisfaction (Ratrout & Hamdan-Mansour, 2020; Wang et al., 2020) were not examined. In a similar fashion, due to the secondary nature of the study our analyses were limited to only variables available from the parent study. For example, we did not obtain information on bond/contract of the respondents which could be an important indicator of job stability. Finally, the convenience sampling nature of the study limits the generalizability of the findings beyond the setting from which the participants were derived. Notwithstanding these constraints in the study design, our findings provide data in considering important factors for intervention in addressing CS, BO, and STS among staff.
Implications for Psychiatric Mental Health Nursing
Nurses are on the front lines, caring for patients and families with the potential to experience stressful work events such as workplace violence that leads to BO and STS. When nurses experience increased stressors in their work environments, it has the potential to lead to increased nurse turnover, decreased employee engagement, poor coping mechanisms, inadequate self-care, and impaired sleep quality (Wei et al., 2018). Hence, our findings suggest some implications for occupational mental health among nurses.
First, among behavioral variables associated with BO and STS, having a history of behavioral health problems, and poor sleep quality were most salient. This finding suggests the importance of proactively providing supportive interventions for nurses who may have disclosed or undisclosed behavioral health challenges. Such support can be in the form of interventions that provide mental and behavioral health screenings and referral to psychotherapy services (Davidson et al., 2018; Miotto et al., 2020). In addition, since poor sleep quality, a modifiable variable, was associated with both BO and STS, interventions should be considered to improve sleep hygiene (e.g., education) as well as workplace-environment modifications and policies to promote sleep (e.g., light supplementation, access to windows, 15- to 30-minute nap breaks; Chen et al., 2010; Redeker et al., 2019; Sun et al., 2019).
Second, among the work-related variables, longer duration of work-tenure and workplace violence were most saliently associated with BO and STS. This finding indicates a potential need to provide BO preventive education as nurses progress in their work tenure. In addition, important interventions to consider in reducing the events leading to BO and STS include (a) adoption of tailored evidence-based interventions to reduce exposure to violence, (b) consumer and patient violence risk assessments to inform safety practices in the health care environment, (c) initial and annual staff training on self-care and safety of the environment, and (d) implementation of aggression and violence mitigation to support nurses with identified risk factors (de Oliveira et al., 2019; Hills & Joyce, 2013; Martinez, 2016; Morphet et al., 2018; Phillips, 2016). It is essential that health care organizations support and ensure safe working conditions while promoting self-care practices for employees which may enhance CS while ameliorating BO and STS.
Third, variations in CS, BO, and STS across specialties suggest the need for tailored interventions that are specialty-specific. For example, in our post hoc analyses, we noted that suffering workplace violence was highest among psychiatric (56.3%) and emergency nurses (54.0%), and lowest among outpatient nurses (15.8%). Thus, tailored approaches for reducing BO and STS in the psychiatric and emergency departments may primarily focus on a reduction in the experience of workplace violence as compared with other specialties. Nevertheless, future studies are needed to understand specialty-specific reasons for increased BO and STS, and low CS among nurses. Such studies can provide better guidance for mitigative interventions.
Conclusions
With the increasing rates of psychological distress encountered by nurses in recent years, more than ever, it is crucial to find ways to enhance CS while preventing and mitigating BO and STS. Our current findings provided further descriptions of important demographic, work-related, and behavioral variables that may be the targets of interventions to support CS and prevent BO and STS. In addition, our results indicate the need to consider variations in the experiences of CS, BO, and STS among nursing staff by specialty. Thus, these variables should be noted when developing targeted or tailored interventions to enhance the CS, and reduce BO, and STS among nurses.
Footnotes
Author Roles
All authors contributed to the conception or design of the study or to the acquisition, analysis, or interpretation of the data. All authors drafted the manuscript, or critically revised the manuscript, and gave final approval of the version that was submitted for publication. All authors agree to be accountable for all aspects of the work, ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.