
Abstract
BACKGROUND:
In 2018, one in six newly diagnosed individuals with HIV in the United States were adults aged 50 years and older, 24% were women, and 60% were Black/African American and Hispanic (42% and 18%, respectively).
AIMS:
This study aims to examine the factors associated with HIV psychosocial illness impact among Black/African American and Hispanic older women living with HIV.
METHOD:
Guided by the socioecological model, a secondary data analysis design with cross-sectional data that included 138 Black/African American and Hispanic women aged 50 years and older was conducted.
RESULTS:
Higher levels of avoidant coping, depressive symptoms, negative self-perception of health, and decreased social support were significant factors associated with HIV psychosocial illness impact among this sample.
CONCLUSIONS:
Findings from this study can contribute to identifying solutions to prevent and decrease these negative factors associated with HIV psychosocial illness impact among Black/African American and Hispanic older women.
In the United States, Black/African American (AA) and people who self-identify as Hispanics (hereafter referred as Hispanic) are disproportionally affected by HIV (United States Census Bureau, 2019). In 2018, these groups constituted 69% of the population receiving a new HIV diagnosis (Centers for Disease Control and Prevention [CDC], 2020a), although they comprise 39.9% of the U.S. population (United States Census Bureau, 2019). In comparison with non-Hispanic White women in the United States, the HIV diagnosis rate is 17.3 higher for Black/AA women and 2.5 times higher for Hispanic women (AIDSVu, 2019).
Additionally, due to advances in HIV treatment, people diagnosed with HIV that adhere to treatment and suppress viral loads are living longer lives. Consequently, in 2018 nearly 51% of people with an HIV diagnosis living in the United States were aged 50 years or older (CDC, 2020b). In addition to an aging population of adults living with HIV, new HIV diagnoses in the older population remains an issue, especially for older women. In 2018, one in six newly diagnosed individuals with HIV in the United States were adults aged 50 years and older, 24% were women, and 60% were Black/AA and Hispanics (42% and 18%, respectively; CDC, 2020b; National Academies of Sciences, Engineering, and Medicine, 2017).
The increasing number of Black/AA and Hispanic older women living with HIV (OWLH) raises a challenge for health care to respond to the needs of this growing population that can be a significant burden on clinical care, research, and policy (Cahill & Valadéz, 2013; National Academies of Sciences, Engineering, and Medicine, 2017). Black/AA and Hispanic OWLH have traditionally been underrepresented in research and in receiving health care services. Hence, there is a substantial need for improving HIV care among these populations.
HIV psychosocial illness impact refers to the psychosocial stressors and other concerns specifically about the disease or its consequences (e.g., feelings of worthlessness, disconnection from others, uncertainty, and the perception that life is meaningless; Patient-Reported Outcomes Measurement Information System [PROMIS], 2015). HIV psychosocial illness impact implies that individuals affected by HIV think about how their illness has affected them in their psychosocial functioning, rather than their physical or functional/role domains of functioning (PROMIS, 2015). HIV psychosocial illness impact is associated with HIV-related stigma, discrimination, comorbidities-chronic illness, self-perception of health, depressive symptoms, lack of social support, and lack of community coping activities (Cianelli et al., 2020; Durvasula, 2014; Logie et al., 2013). In addition, the presence of comorbidities causes uncertainty, anxiety, and physical weakness, influencing quality of life and treatment adherence (Cianelli et al., 2020; DeGrezia & Scrandis, 2015; Milanini et al., 2017). Black/AA and Hispanic OWLH often struggle with HIV and comorbidities for many years, perceiving them as a threat to health and well-being, making the HIV psychosocial illness impact significantly negative and challenging (Heckman et al., 2017).
Black/AA and Hispanic OWLH often do not want to disclose that they are living with HIV, leading to self-isolation and decreased social support (Grodensky et al., 2015; Grov et al., 2010). This situation is particularly relevant because it may be accentuated by social stressors, including HIV-related stigma and discrimination, contributing to a significant psychosocial burden. This burden includes depressive symptoms and negative mood, leading to a negative perception of support resources (Logie et al., 2013; Whitehead et al., 2014). Likewise, several elements of social support may act as coping tools for Black/AA and Hispanic OWLH (Durvasula, 2014). Encouraging individual and community activities has been suggested to reduce psychosocial issues affecting this group (Cianelli et al., 2020).
Community environments and sociocultural norms and values may also influence health and well-being among Black/AA and Hispanic OWLH (Baral et al., 2013). For instance, the experience of health disparities affects population groups based on gender, age, ethnicity, socioeconomic status, geography, sexual orientation, and special health care needs (Cianelli, 2010). These health disparities usually occur among Black/AA and Hispanic OWLH and other vulnerable groups who have persistently experienced historical trauma, social disadvantage, and discrimination, with deleterious consequences in health (Cianelli, 2010). Otherwise, state-level policies may have a relevant impact on pathways of harm or resiliency related to HIV and mental health well-being as they determine the allocation of economic resources to education and HIV care availability and therefore play a substantial role in shaping structural contexts of HIV management (Baral et al., 2013).
Conceptual Framework
To better understand the complexity of the HIV psychosocial illness impact among Black/AA and Hispanic OWLH, this study uses the socioecological model (SEM; McLeroy et al., 1988) to analyze the dynamic personal and environmental factors that contribute to the HIV psychosocial illness impact. Using Brofenbrenner’s (1979) model as framework, McLeroy et al. (1988) developed the SEM. Behavior was envisioned as an outcome that was influenced by five different levels (described from proximate to distal): individual (intrapersonal), microsystem (interpersonal), mesosystem (institutional), exosystem (community), and macrosystem (public policy; Brofenbrenner, 1979; McLeroy et al., 1988). The first level factor, the intrapersonal level (individual), includes the unique characteristics of an individual, such as chronic comorbidities, avoidant coping, health self-perception, and depressive symptoms. The second level factor, the interpersonal level (macrosystem), includes the processes, associations, and interactions of an individual with their formal and informal work and social network, such as friends and family. (McLeroy et al., 1988). The variable perceived social support and HIV-related discrimination will be included and analyzed in this level. The third level factor, the institutional level (mesosystem), refers to the organizations, institutions, and regulations for operations, being formal or informal (McLeroy et al., 1988). We will analyze the availability of activities for older residents living in the community at this level.
Despite the compelling and significant need to explore the HIV psychosocial illness impact, there is limited literature that focuses on the population of Black/AA and Hispanic OWLH. Therefore, this study aims to examine the factors associated with HIV psychosocial illness impact among Black/AA and Hispanic OWLH. Findings from this study may help find solutions to prevent and decrease these negative factors and to create culturally tailored interventions to help decrease the HIV psychosocial illness impact among Black/AA and Hispanic OWLH and to improve their well-being.
Method
Research Design
This research is part of a wider study that examined HIV-related needs of 138 Black/AA and Hispanic OWLH (RWJF-ENF-71968). The parent study’s purpose was to investigate the culture of health among Black/AA and Hispanic OWLH. A secondary data analysis design with cross-sectional data collected between March and December 2017 was used for the current study.
Sample and Setting
Participants for this study were recruited from an ambulatory care HIV specialty clinic associated with a public hospital in Miami Dade County, Florida. The research team conducted an in-person recruitment supported by health care providers who referred their patients to the study. Furthermore, the research team placed flyers in the community, which were available in English and Spanish. Eligibility criteria included self-identifying as Black/AA or Hispanic, being 50 years and older, living with HIV, speaking/reading in English or Spanish, and being willing to to provide written consent. The study was approved by the institutional review board from the University of Miami and the public hospital. The total sample included 138 Black/AA and Hispanic OWLH aged 50 years and older who signed the informed consent prior to data collection.
Data Collection
Black/AA and Hispanic OWLH were interviewed according to their language preference by trained female nurse researchers. The training included data collection and entry, documentation, regulatory compliance, and human subject’s protection. A structured questionnaire was used to guide the data collection through a face-to-face interview conducted in private offices located within the public hospital. Data were collected through Qualtrics, a secure web-based research management software tool. Questions were documented on a computer/tablet in an interview format by the trained research team.
Variables
Sociodemographic and HIV Status
During the assessment, participants answered a questionnaire regarding basic demographic data, including age (years), marital status (single, divorced, in a relationship not legally married, separated, married, widowed), place of birth, education (years), relationship status (living with a partner/ not living with a partner), race (Black/AA or Hispanic), religion, current employment status (Yes/No), and health insurance (Yes/No). Health information related to HIV status included questions about years since HIV diagnosis, self-reported ART medication adherence (“Are you taking HIV medication?”), and how acquired HIV.
HIV Psychosocial Illness Impact
The Psychosocial Illness Impact Negative Short Form 4a (PROMIS v1.0) was used to measure the direct negative psychosocial effect of HIV infection as a different concept from general emotional distress (PROMIS, 2015). The scale consists of four items that use two time frames, “before your illness” and “since your illness,” when assessing “negative illness impact.” Each item has five options for answers in a Likert-type scale, ranging from not at all (1) to very much (5). Raw scores range from 8 to 40. Higher scores indicate a higher negative HIV psychosocial illness impact. According to the author of this scale, the scores were converted into T scores on a mean of 50 with an standard deviation of 10 representing the estimated chronic illness (HIV in this study) population to allow comparisons between studies (PROMIS, 2015). The T scores were calculated using the Health Measures Scoring Service of PROMIS. This scale has a Cronbach α = .86 in this study.
Individual-Intrapersonal Variables
Avoidant coping
This variable refers to cognitive or behavioral activities that take place to be away from a threat; in this case, the illness process would be the threat (Quah et al., 2020). This can be seen as the "flight" reaction from a stressful situation or the effort to avoid dealing with a stressor. The avoidant coping subscale from the Brief Coping Questionnaire (Carver, 1997) was used for this study. The subscale has a total of 12 items that measure coping mechanisms related to HIV diagnosis, including self-distraction, denial,substance use, behavioral disengagement, venting, and self-blame (Eisenberg et al., 2012). Each item has four options for answers, from I have not been doing this at all (1 point) to I have been doing this a lot (4 points). Scoring ranges 12 to 48 with a higher score indicates a higher avoidant coping. Previous studies have shown good internal consistency for the avoidant coping subscale (Cronbach’s α = .70; Eisenberg et al., 2012). In this study, the reliability of this subscale was α = .74.
Chronic comorbidities
This variable measured the number of chronic comorbidities self-reported by the participants. The authors calculated a score that represents the presence of comorbidities reported by the participants (i.e., high blood pressure [HBP], diabetes mellitus [DM], osteoporosis, dyslipidemia, and Hepatitis B). The responses where dichotomous (0 = no, 1 = yes). The total score ranges from 0 to 5. Higher scores indicate a higher number of chronic comorbidities.
Depressive symptoms
The Patient Health Questionnaire (PHQ-9), a nine-item questionnaire that describes behaviors/feelings experienced in the past 2 weeks, was used to measure depressive symptoms (Kroenke et al., 2001). The answers for each Likert-type scale item are not at all (0 points), several days (1 point), more than half the days (2 points), and nearly every day (3 points). Scores range from 0 to 27 with higher scores indicating higher depressive symptoms. Scores ≤4 suggest minimal depressive symptoms, which may not require treatment. Scores of 20 to 27 indicate severe depressive symptoms. This instrument has been validated to be used in primary care, and the reliability reported in other studies is α = .89 (Merz et al., 2011). In this sample, the reliability was α = .86.
Self-perception of health
The question "How would you describe your health in the past three months?" was used to measure this variable, which was dichotomized in the data analysis (0 = poor/fair, 1 = good/very good).
Microsystem-Interpersonal Variables
Perceived social support
The Social Support Questionnaire Shortened version was used for this study (Cohen et al., 1985; Fetzer Institute, n.d.). Each dimension is measured by four items on a 4-point scale ranging from definitely true (1) to definitely false (4). The total score ranged from 12 to 48 points, with higher scores indicating a higher social support perception. This scale has a Cronbach α = .83 for this sample.
HIV-related discrimination
For HIV-related discrimination the following question was asked, “Have you experienced discrimination because of your disease, so you don’t want to be associated with anything related to it?” (0 = no, 1 = yes).
Mesosystem-Institutional Variables
Activities for older residents living in the community
The question “Does your community organize activities for residents aged 50 years and older?” was used to measure this variable. The variable was used as a binary variable in the data analysis (0= no/I do not know, 1 = yes).
Data Analysis
The data analysis was conducted using SPSS 26.0 software. Integrity data was checked prior to the data analysis, including missing values, scoring, and any discrepancies. Descriptive statistics were calculated, including central tendency and dispersion, and a linear multiple regression model was proposed. Based on the literature and guided by the SEM, seven independent variables were selected as possible factors associated with the dependent varible. In the model, HIV psychosocial illness impact was used as the dependent variable. The existing literature and alignment with the theoretical framework guided the final decision regarding which variables to include in the model. Assumptions for linear regression were assessed prior to the analysis, including normality in the distribution of residuals, homoscedasticity, linearity, and independence (Miles & Shevlin, 2001). Multicollinearity between independent variables was evaluated through the assessment of tolerance and the variance inflation factor (VIF; tolerance level < 0.1, VIF > 10; Belsley et al., 1980). Sample size was calculated based on the formula N > 50 + 8m (m= number of independent variables; Tabanachnick & Fidell, 2007).
Results
Descriptive Data
Sociodemographic and HIV Status
Table 1 shows the sociodemographic and HIV Status characteristics of the sample. The mean age for Black/AA and Hispanic OWLH was 56.64 (SD = 5.13; range 50-77) years. The majority were single (47.1%), 77.5% born in the United States, and reported 11.04 years of education (SD = 2.24; range 0-16). In terms of religion, 54.3% reported being Baptist, 12.3% Christian, 8.7% Catholic, and 24.7% have other religions; 95.7% of the participants consider themselves as very or somewhat religious. Women living with a partner represent the 32.6% of the sample. Mean time living with HIV was 17.99 years (SD = 8.78; range 1-37); 79.7% acquired HIV having sex with male partners not using condoms, 4.3% by blood transfusions, 3.6% injected drugs, and 12.3% reported other reasons (e.g., rape, an accident at work, do not know). Most participants were adherent to their HIV medications (97.8%).
Sociodemographic and HIV Status Characteristics of the Sample.
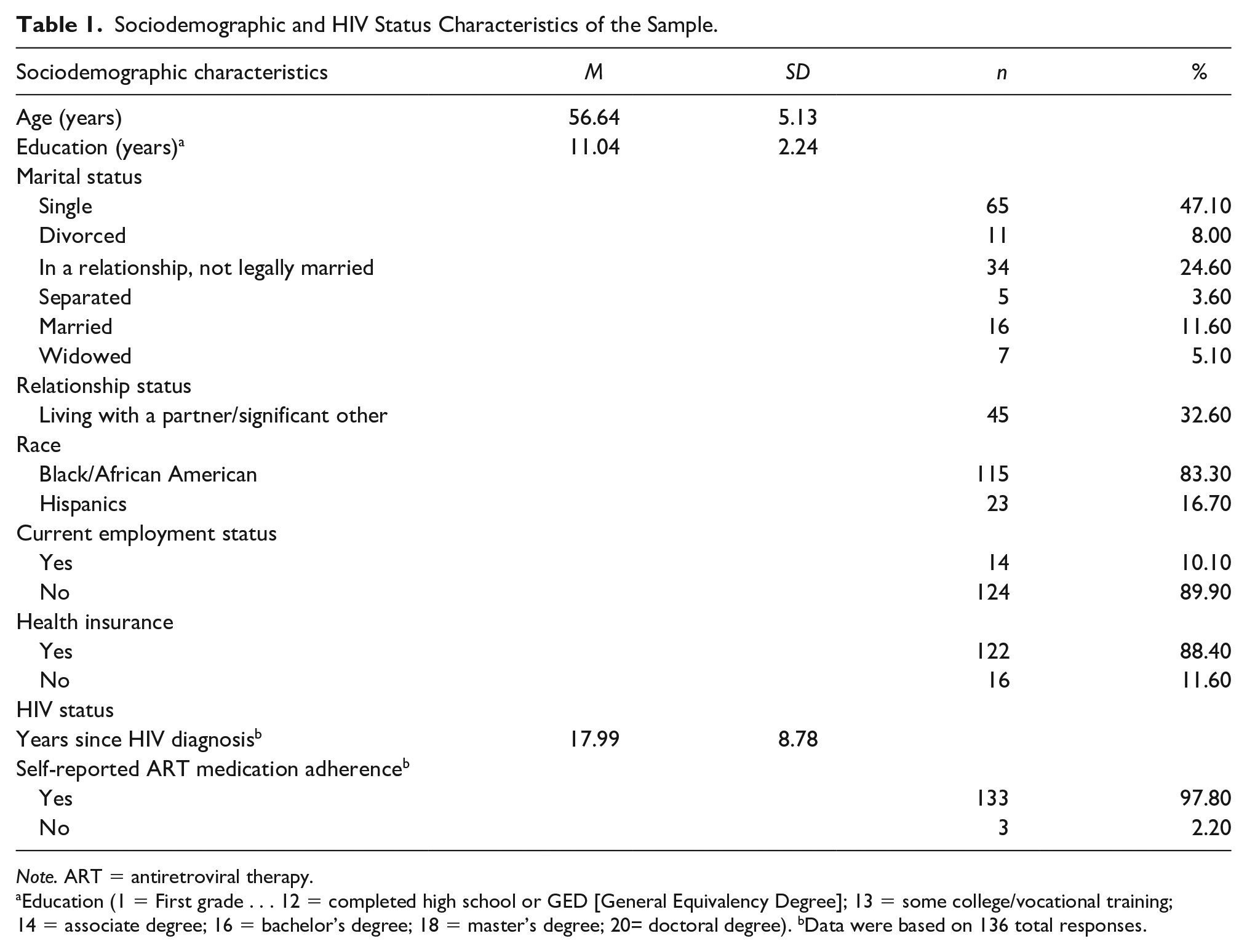
Note. ART = antiretroviral therapy.
Education (1 = First grade . . . 12 = completed high school or GED [General Equivalency Degree]; 13 = some college/vocational training; 14 = associate degree; 16 = bachelor’s degree; 18 = master’s degree; 20= doctoral degree). bData were based on 136 total responses.
Individual-Intrapersonal Level
The mean score of avoidant coping was 21.31 (SD = 7.13; range 12-45; Table 2). Among the participants, 58.1% had HBP (n = 79), 22.1% had dyslipidemia (n = 30), 21.3% had DM (n = 29), 16.2% had osteoporosis or osteopenia (n = 22), and 10.9% had Hepatitis B (n = 15). A total of 53 participants reported one comorbidity (39.0%), followed by 37 (27.2%) with two comorbidities, 12 (8.8%) with three comorbidities, and 3 (2.2%) with four comorbidities. Regarding depressive symptoms, the average score in the sample for the PHQ-9 scale was 7.80 points (SD = 6.41; range 0-27). Only seven participants screened positive for severe depressive symptoms (PHQ-9 > 20). A total of 85 participants (61.6%) described their health in the past 3 months as very good or good. Just 38.4% describe their health as fair or poor (n = 53).
Variables According to the SEM Levels Among Black/AA and Hispanic Older Women Living With HIV.
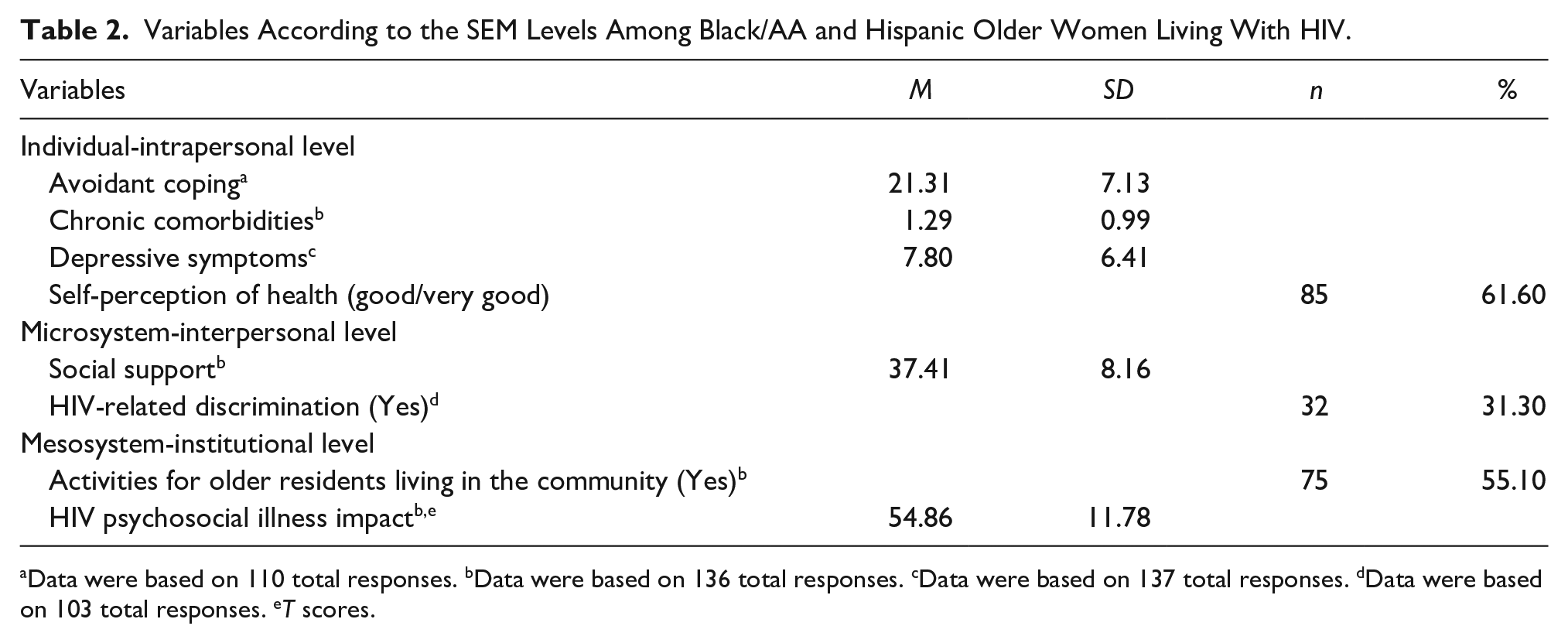
Data were based on 110 total responses. bData were based on 136 total responses. cData were based on 137 total responses. dData were based on 103 total responses. eT scores.
Microsystem-Interpersonal Level
The average social support score for participants was 37.41 points ± 8.16 (range 12-48). A total of 32 (31.3%) of the participants reported feeling discriminated against because of HIV.
Mesosystem-Institutional Level
Most of the respondents (55.1%, n = 75) reported having activities for older residents in their community. In comparison, the rest of the participants (44.2%, n = 61) reported not having or not knowing about these resources.
HIV Psychosocial Illness Impact
The average T-score for participants in this sample was 54.86 (SD = 11.78; range 38.20-76.70). Most women (67.4%, n = 93) had scores higher than the mean scores for the reference U.S. population (m = 50, SD = 10). When we analyzed the raw scores for this scale in the overall sample, the after-illness scores were higher than the before-illness scores (9.64 vs. 7.00 points).
Factors Associated With HIV Psychosocial Illness Impact
The seven selected variables met the assumptions for a regression test (Table 3). Just one score, HIV psychosocial illness impact, required transformation. Also, collinearity was assessed with a statistical test to evaluate the linear relationships among the independent variables in the regression model through a tolerance and variable inflation factor analysis. No multicollinearity was found among the independent variables with tolerance values between .72 and .96, and VIF statatistical value ranging from 1.04 to 1.39.
Multiple Regression Analysis Predicting the HIV Psychosocial Illness Impact Among Black/AA and Hispanic Older Women Living With HIV.
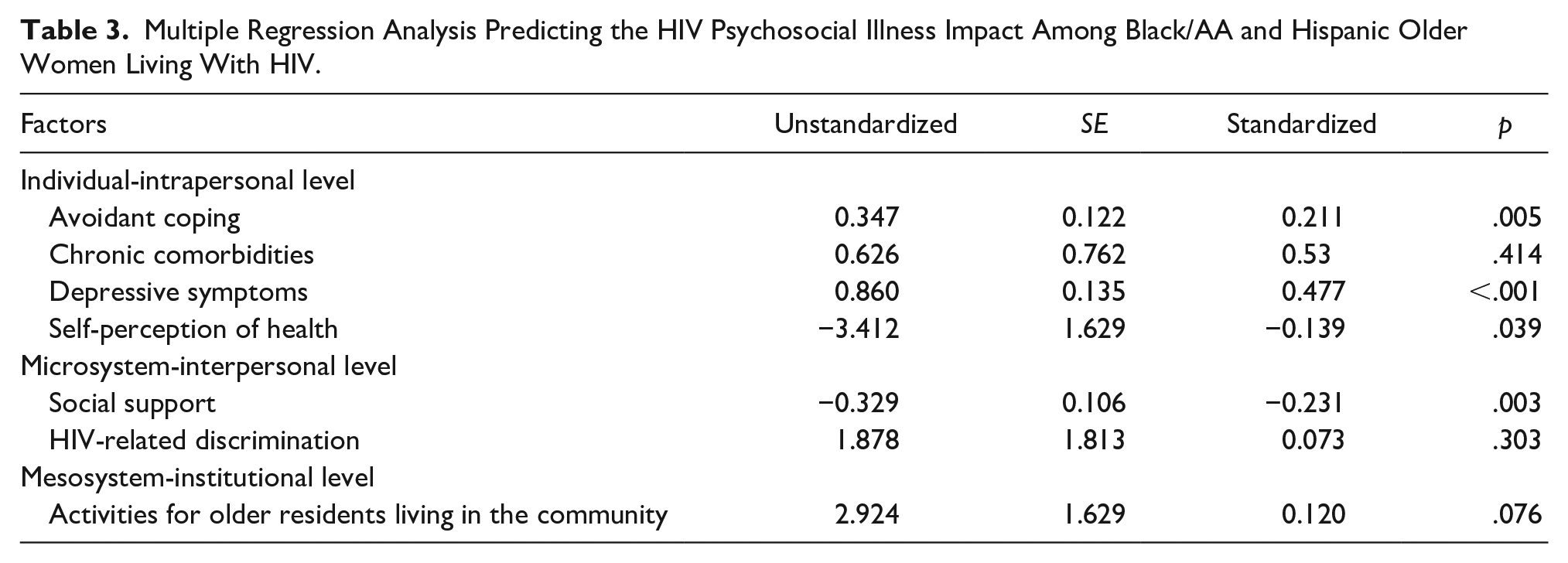
Table 3 shows the multiple regression model. The omnibus test for the multiple regression analysis was statistically significant, R2 = .599, F(7, 92) = 22.095, p < .001. All together, the variables accounted for 59.9% of the variance in the dependent variable HIV psychosocial illness impact. Four factors associated with HIV psychosocial illness impact—avoidant coping, depressive symptoms, self-perception of health, and social support—were statistically significant in the model. No variables were added to the model. In the model, higher scores of depressive symptoms were associated with higher scores for HIV psychosocial illness impact (b = 0.860, p < .001). More positive self-perceptions of health were associated with lower HIV psychosocial illness impact scores (b = −3.412, p = .039). In addition, higher levels of perceived social support were associated with lower scores for HIV psychosocial illness impact (b = −0.329, p = .003). Finally, avoidant coping was associated with HIV psychosocial illness impact (b = 0.347, p = .005). The most significant factors associated with HIV psychosocial illness impact were depressive symptoms and social support. Chronic comorbidities, HIV-related discrimination, and activities for older residents in the community were not significant factors associated with HIV psychosocial illness impact in the model.
Discussion
This secondary data analysis study aimed to examine factors associated with HIV psychosocial illness impact among Black/AA and Hispanic OWLH. The study used the SEM of McLeroy et al. (1988) to better organize factors and understand this phenomenon. In the cross-sectional data at the intrapersonal level, we found avoidant coping, depressive symptoms, and self-perception of health to be significant factors associated with HIV psychosocial illness impact among our sample. At the interpersonal level, we found social support as a significant factor associated with HIV psychosocial illness impact. The four statistically significant variables found in this study accounted for nearly 60% of the variance in HIV psychosocial illness impact. This is the first publication that addresses the impact of these factors among Black/AA and Hispanic OWLH aged 50 years and older.
Results from this study indicate that avoidant coping is one of the significant factors associated with HIV psychosocial illness impact at the interpersonal level. Most Black/AA and Hispanic women in our sample were HIV diagnosed when the management of the disease was very difficult. Black/AA and Hispanic OWLH aged 50 years and older used maladaptive coping strategies, such as venting, denial, substance use, behavioral disengagement, self-distraction, and self-blame to “confront” the psychosocial distress of living with HIV (Cianelli et al., 2020).
Venting or expressing emotions in moderation can be healthy; however, ruminating over negative feelings is not (Gruszczyńska & Rzeszutek, 2020). Similarly, by using the unconscious defense mechanism of denial, one can initially buy time to adjust to a distressing situation (living with HIV) but a long and constant use of this coping strategy does not allow Black/AA and Hispanic OWLH to confront reality (Wardell et al., 2018). By using avoidant coping, Black/AA and Hispanic OWLH would not actively engage in HIV care (management and treatment). Moreover, rumination can lead to self-blaming statements, including criticizing and blaming oneself for acquiring HIV (Garrido-Hernansaiz & Alonso-Tapia, 2020). Previous findings from a qualitative study done with this sample of Black/AA and Hispanic OWLH showed that many of them felt guilty about getting the HIV disease (Cianelli et al., 2020).
Behavioral disengagement or "giving up" has been positively correlated with greater disease progression among people living with HIV (Turan et al., 2017). Questions related to this from the Brief Cope Questionnaire referred to “giving up trying to deal with HIV infection” and “giving up the attempt to cope” (Carver, 1997). Engaging in these maladaptive cognitive strategies can cause significant psychological, emotional, and physical damage to Black/AA and Hispanic OWLH. This distortive thinking can lead to anxiety, depression, suicidal thinking, medical noncompliance, and direct immunological effects (Turan et al., 2017). Moreover, denial, self-blame, and behavioral disengagement can all lead to use of substances such as alcohol and drugs to “get through” or to feel better (Wardell et al., 2018). Therefore, teaching these OWLH the use of adaptive coping is a critical nursing intervention.
Depressive symptoms showed a positive relationship with HIV psychosocial illness impact among Black/AA and Hispanic OWLH at the intrapersonal level. Of the seven participants who screened positive for severe depressive symptoms (PHQ-9 > 20), none had active suicidal thoughts, intent, or plan. Nonetheless, these participants were provided with information on local resources for mental health care needs. This finding is consistent with studies which found that depression tends to be persistent and cyclical among people living with HIV, affecting the person’s psychosocial well-being and overall HIV management (Perazzo et al., 2020). Depression can lead to treatment noncompliance, which in turn can result in self-management failure and, ultimately, increased death (Pence et al., 2018; Williamson et al., 2017). Black/AA and Hispanic OWLH have reported viewing HIV diagnosis as a death sentence (Cianelli et al., 2020), which can lead to depressive symptoms. Depression among individuals living with HIV has been associated with an increased likelihood of attempted suicide (Fellows et al., 2015). Perceiving the HIV diagnosis as a death sentence, experiencing depression, living stressful situations, and using avoidant coping are factors reflected in a negative illness impact among Black/AA and Hispanic OWLH.
Self-perception of health at an older age is often described in the literature as pessimistic due to the concurrence of physical, social, and mental vulnerability, thus affecting negatively the quality of life for older adults (Cavalcanti et al., 2017; Ng et al., 2014; Pimenta et al., 2015). One recognized predictor of heath outcomes, including mortality, is poor self-perception of health (Nybo et al., 2003). In the current study, poor self-perception of health among Black and Hispanic OWLH was found to be a significant factor associated with HIV psychosocial illness impact at the intrapersonal level.
Individuals with a poor self-perception of their health may miss certain “critical points” to initiate actions that promote health, thus leading to health issues (Ellis & Grieger, 1977; Rakowski et al., 1991). It will be essential to learn Black/AA and Hispanic OWLH’s self-perceived obstacles to engaging in treatment and to identify any health beliefs that could lead to HIV psychosocial illness impact. Frequently, useless convictions or discernments lead to low degrees of saw self-adequacy and an ensuing failure to embrace or keep up the ideal conduct. Frequently, dysfunctional beliefs or perceptions lead to low degrees of self-efficacy and an ensuing failure to embrace or keep up the desired conduct (Bandura, 1986). Interventions that support Black/AA and Hispanic OWLH in having positive self-perceptions of health may be beneficial because optimistic feelings are protective factors against health issues (Mossey & Shapiro, 1982).
Lack of social support perception was a significant factor associated with HIV psychosocial illness impact among this sample at the interpersonal level. Older people living with HIV are more isolated compared with young people living with the disease, which may lead to more issues when dealing with their HIV diagnosis (Cahill & Valadéz, 2013). Emotional, instrumental, and informational social support can act as essential coping tools for Black/AA and Hispanic OWLH, and strategies oriented to improving social support may contribute to coping with the disease (Durvasula, 2014). Whereas most older people without HIV count on family support during illness, older people living with HIV may note barriers to receiving instrumental and emotional social support from family, friends, and the community. The social discrimination associated with HIV can also restrict the capacity to seek and access social support networks (Cahill & Valadéz, 2013; Cianelli et al., 2020).
Limitations
The following limitations of this study should be considered. All data collected in this study were self-reported, which may lead to social desirability bias. Also, cross-cultural and cross-regional generalizability cannot be assured because the sample consisted of an isolated group of Black/AA and Hispanic OWLH; thus, the results may not be readily extrapolated to a larger population. Additionally, data available from the parent study did not include variables for an analysis that could explore the community and public policy levels of the SEM. The data sought and analyzed focuses primarily on the lower levels of the model—intrapersonal and interpersonal.
Implications for Practice
Results from this study reveal that several intrapersonal and interpersonal factors influence HIV psychosocial illness among Black/AA and Hispanic OWLH. They often isolate or suffer from discrimination and stigma initiated by family, friends, and the community they live in. In order to mitigate the HIV psychosocial impact among Black/AA and Hispanic OWLH, nursing interventions should focus on maximizing the use of adaptive coping. Nurses can teach patients about positive coping styles during brief interactions with patients in any setting (acute or outpatient). Positive or adaptive coping styles can initiate changes in mood, improve self-esteem, increase assertiveness, and improve the overall quality of life in Black/AA and Hispanic OWLH (Halkitis et al., 2017).
Early screening for the detection and treatment of depression is crucial to minimize the HIV psychosocial illness impact among Black/AA and Hispanic OWLH. These women have multiple risk factors that predispose them to major depressive disorders, including belonging to the female gender (the prevalence of depression in women is more than double when compared with men), having a chronic condition (HIV), and belonging to an ethnic minority (De Oliveira et al., 2016). Depression can go unnoticed in primary care or infectious disease clinics regularly visited by Black/AA and Hispanic OWLH. Cultural variations in the presentation of the disease can affect recognition. For example, in the Hispanic culture, somatic complaints are usually overlooked as the primary presenting complaint of the depressed person (De Oliveira et al., 2016). In the Black/AA population, nontraditional symptoms of depression can include hypertension (Sohail et al., 2014). Referral to formal support groups for depression would also increase resilience and give these Black/AA and Hispanic women a sense of hope while increasing their overall engagement in HIV self-management (McDoom et al., 2015).
Collaborative efforts involving several agencies and government levels are needed to address and mitigate the complexities that Black/AA and Hispanic OWLH confront effectively. Health policy makers and clinicians should be trained in this population’s unique needs, including technical and medical assistance, cultural competence, and capacity-infrastructure, to support the implementation of novel measures to improve management and care among older people living with HIV. Black/AA and Hispanic OWLH should be supported by providing interventions that strengthen self-esteem, improve resilience, reduce internalized behavior problems, improve self-efficacy, and sustain and/or improve psychological well-being to overcome HIV psychosocial illness impact.
Implications for Research
Black/AA and Hispanic OWLH are underrepresented in research and face barriers to receiving preventive health services. Further research using qualitative and quantitative study designs is needed to assess the HIV psychosocial illness impact, as is testing the efficacy of interventions targeted to this group of Black/AA and Hispanic older women. Further studies should preferably include variables that could be assessed at all five levels of the SEM for a more in-depth understanding of the HIV psychosocial illness impact among this population.
Sociocultural, behavioral, and biomedical HIV-related studies are needed to reduce health disparities by clearly understanding the different factors related to HIV among Black/AA and Hispanic OWLH and its potential impact in their psychosocial well-being (Cianelli, 2010). Given that a wide range of factors are combined in HIV care, multilevel intervention research is needed. The main focus of multilevel strategies is to bridge the gap in health disparities (Paskett et al., 2016). We further encourage studying variables belonging to the community and public policy levels such as economic factors, cultural values, racial discrimination, and stigma experienced in community settings.
Conclusions
This study reveals that the HIV psychosocial illness impact is a significant issue for Black/AA and Hispanic OWLH aged 50 years and older that can be improved by ameliorating several intrapersonal, interpersonal, and institutional factors. Higher levels of avoidant coping, depressive symptoms, negative self-perception of health, and lack of social support were factors associated with HIV psychosocial illness impact among our sample. Findings from this study suggest the need from health care professionals to screen for these negative factors associated with HIV psychosocial illness and provide age appropriate and culturally tailored resources. Further studies are required to develop and test culturally tailored interventions that provide an interdisciplinary and support group-based approach to increasing social support and decreasing negative factors associated with HIV psychosocial illness impact among Black/AA and Hispanic OWLH.
Footnotes
Author Roles
All authors contributed to the conception or design of the study or to the acquisition, analysis, or interpretation of the data. All authors drafted the manuscript, or critically revised the manuscript, and gave final approval of the version that was submitted for publication. All authors agree to be accountable for all aspects of the work, ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by Robert Wood Johnson Foundation Executive Nurse Fellow (RWJF-ENF# 71968; PI: Rosina Cianelli) and by the National Agency for Research and Development (ANID)/Scholarship Program/DOCTORADO BECAS CHILE/2019—Award number 72200262 (Evelyn Iriarte).