
Abstract
BACKGROUND:
Patients with bipolar affective disorder (BPAD) have a suicide risk of up to 30 times higher than the general population. There is increasing interest in analyzing the effects of resilience in psychiatric diseases and its relationship to other factors such as suicide risk.
AIM:
The main objective of this study was to analyze the relationship between psychological resilience and suicide attempts, along with other relevant clinical and sociodemographic variables in euthymic patients with BPAD.
METHODS:
Eighty six outpatients, more than 18 years old, mostly men (60.5%) with BPAD type 1, 2, mixed, and unspecified, in euthymic phase receiving antidepressant and/or euthimizing treatment, participated in the study. Sociodemographic and clinical variables were assessed by means of a questionnaire and psychological resilience by means of Connor-Davidson’s 10-item Resilience Scale.
RESULTS:
Patients with previous autolytic attempts scored significantly lower in resilience than those who had not attempted suicide (T = 3.30; p ≤ .001; 20.61 ± 6.58 vs. 26.52 ± 7.29). Patients diagnosed with BPAD scored significantly lower than other samples of university participants, workers, and the unemployed. The number of depressive episodes experienced was negatively and significantly associated with resilience scores (r = −.28; p < .01).
CONCLUSIONS:
Patients diagnosed with BPAD who had made autolytic attempts had lower resilience scores than those who had not made them and lower scores than other general nonpsychiatric samples. The promotion of resilience in patients diagnosed with BPAD would facilitate a more adaptive and positive coping with the disease and their recovery process.
Introduction
Bipolar affective disorder (BPAD) is characterized by the recurrence of depressive episodes alternating with hypomanic or manic episodes (Lee et al., 2017), with significant impact on the quality of life of the individual, their family, and society. The estimated prevalence varies from 3% to 8% of the human population, although these figures would be higher if bipolar spectrum disorders were included (Angeler et al., 2018). The prevalence of BPAD 1 is similar for males and females, whereas BPAD 2 occurs more frequently among females (Carvalho et al., 2020).
Patients with BPAD have a risk for attempted suicide of up to 30 times higher than the general population (Berkol et al., 2016; Berutti et al., 2016; Mert et al., 2015). Fifty-nine percent of patients diagnosed with BPAD have suicidal ideation, and 25% to 56% commit a suicide attempt during their lifetime (Berkol et al., 2016; Berutti et al., 2016). The presence of mixed and depressive phases (Swartz-Vanetik et al., 2018), early age of onset, rapid cycling, history of substance abuse (Mert & Kelleci, 2015), and concomitance of personality and anxiety disorders (Berkol et al., 2016; Mert et al., 2015; Swartz-Vanetik et al., 2018) are related to the prevalence of suicide attempts in these patients. Sociodemographic characteristics that influence the prevalence of suicide attempts in the general population are related to age, marital status, educational level, and history of family suicide (Berkol et al., 2016; Mert & Kelleci, 2015).
Resilience is defined as a person’s ability to adapt positively to adverse life circumstances or to psychosocial stress (Edward, 2005; Konradt et al., 2018; Ozawa et al., 2017; Soler et al., 2016). It is a dynamic process that involves the adaptation of the individual to significantly unfavorable situations; a protection factor that modifies, improves, or alters the individual’s response to dangerous events that would predispose them to less adaptive outcomes (Rutter, 2012). It is a universal, rather than unique, phenomenon (Masten, 2007), characterized by adaptive behavior patterns in contexts of risk and adversity (Post et al., 2018).
The concept of resilience has gained currency in areas such as work, education, and social policy, although always with marked connotations related to mental health (Cabanyes, 2010).
As indicated by Post et al. (2018), there is increasing interest in analyzing the effects of resilience in psychiatric diseases and its relationship with other factors. A high degree of resilience has been found to reduce the risk for attempted suicide in patients with depression (Nrugham et al., 2010), and Choi et al. (2015) found that low levels of resilience were associated with a higher number of depressive episodes and higher levels of impulsivity in bipolar patients (Choi et al., 2015). There is also evidence of lower quality of life and resilience scores in patients with BPAD 1 than in healthy individuals (Hofer et al., 2016), findings similar to those of Lee et al. (2017). In summary, resilience is considered a protection factor for BPAD (Ozawa et al., 2017) and may play an important role in both prevention and treatment of this disease (Nrugham et al., 2010; Ozawa et al., 2017), although research on resilience in patients with BPAD is quite scarce.
The main objective of this study was to analyze the relationship between psychological resilience and suicide attempts with other relevant clinical and sociodemographic variables in euthymic patients with BPAD. Specifically, the aim was (1) to study whether euthymic patients diagnosed with BPAD who are not suffering from an acute phase of their illness have significant differences in psychological resilience compared with the results obtained in other studies with nonpsychiatric participants; (2) to study whether these patients have significant differences in psychological resilience according to whether they have had suicide attempts or not; and (3) to examine the relationships between psychological resilience and other important clinical and sociodemographic variables, such as the specific type of BPAD, length of illness, number of admissions in the past year, number of depressive episodes and manic episodes, age, sex, academic level, and work activity.
Materials and Methods
Study Design
This is a cross-sectional observational study. Recruitment period was from January 2017 to February 2018.
Context
Unicentric study carried out in the outpatient nursing offices, located in the Mental Health Centre, Spain.
Participants
The patients selected had all been diagnosed with BPAD and were attending quarterly follow-up appointments in the nursing offices of the aforementioned mental health center, were in the euthymic phase, were receiving antidepressant and/or euthimizing treatment, and were more than 18 years old, who agreed to participate in the study after the explanation and physical delivery of a sheet with information to the patient about their participation in the study. Individuals diagnosed with significant intellectual disabilities, psychosis, or who were in an acute phase of the illness, as well as those who presented a significant language barrier or were legally incapacitated and did not have a legal guardian present, were excluded.
The total number of patients who participated in the study was 86. A diagram of the inclusion of patients as study participants can be seen in Figure 1.
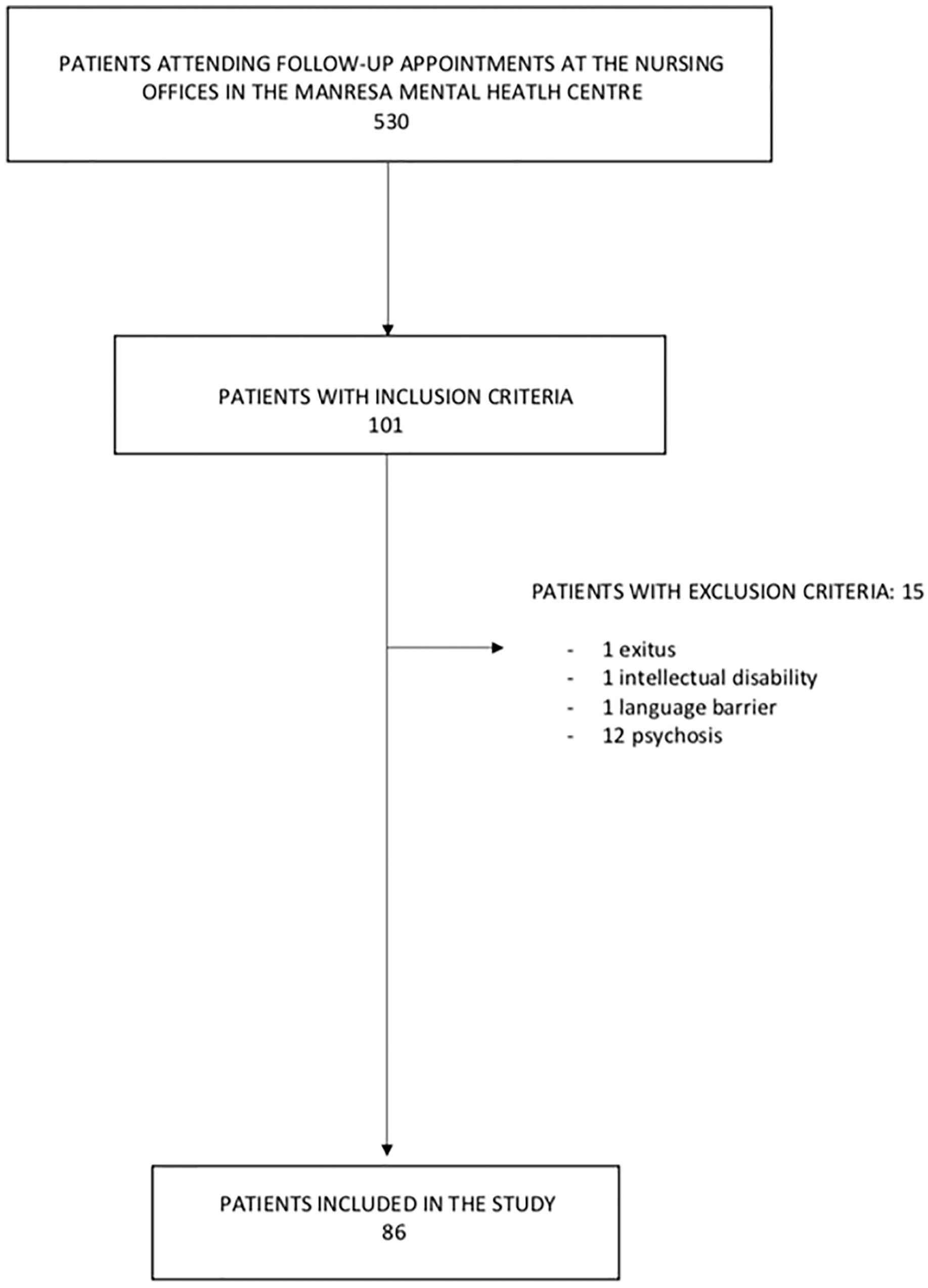
Flow diagram.
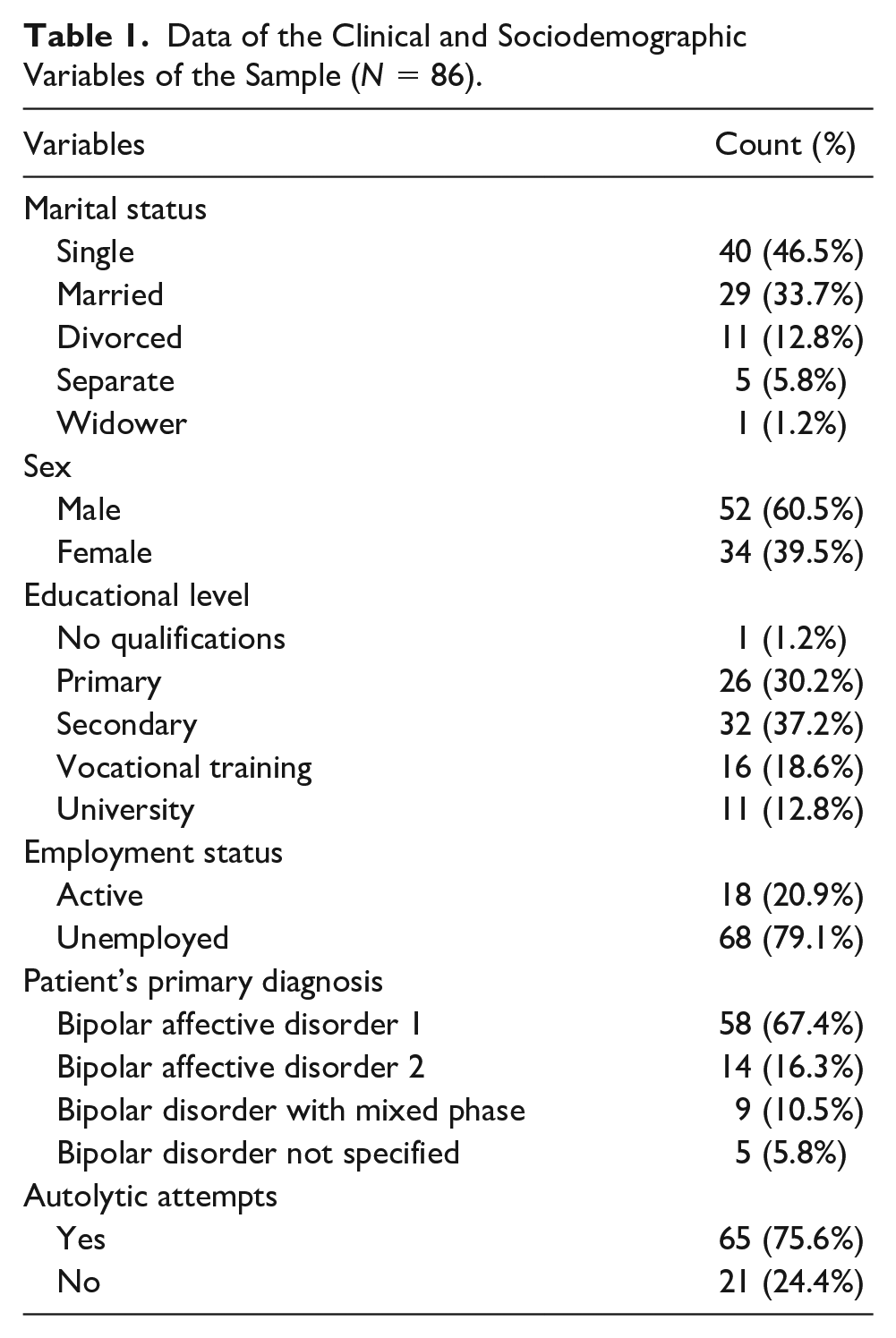
Most participants were men (60.5%), mean age was 47.9 years old (SD = 12.38; range = 21-77 years), and evolution time of mental illness was 21.96 years (SD = 12.81; range = 1-61 years). The average number of admissions in the past year was 0.27 (SD = 0.52; range= 0-3 years); the average number of depressive episodes was 1.43 (SD = 2.55), manic episodes was 2.15 (SD = 2.15), and suicide attempts was 75.6%. The remaining clinical and sociodemographic characteristics of the sample are shown in Table 1.
Data of the Clinical and Sociodemographic Variables of the Sample (N = 86).
Study Procedure
Data were collected by mental health nurse specialists. If the patient was legally incapacitated and accompanied by their guardian, the interview was conducted with the legal guardian. This procedure was supervised by the main investigator.
Instruments
By means of a questionnaire designed for this purpose, data on the following variables were collected: age, sex, marital status, educational level, employment status, number of admissions in the past year, length of mental illness, number of manic and depressive episodes, and history of suicide attempts.
The Connor-Davidson’s Psychological Resilience Scale (CD-RISC) was used in its 10-item version and was adapted to the Spanish context by Notario-Pacheco et al. (2011). Responses are given according to a Likert-type format, ranging from 0 = not at all to 4 = almost always; this is an example of an item: “I can adapt to changes” (Item 1). The direct score is used as an estimate of psychological resilience (0 minimum to 40 maximum). An internal consistency (Cronbach’s alpha) of α = 0.89 was found for this scale.
Data Analysis
The statistical analysis was conducted using the software IBM SPSS Statistics 22 (IBM Corporation, Armonk, NY). First, internal consistency of the CD-RISC scale and the descriptive analyses were found; subsequently, means contrasts and bivariate correlations were found.
Ethical Aspects
The study was approved by the clinical research ethics committee. The study was conducted in accordance with the recommendations of the Helsinki Declaration. The patient information sheet was handed out and read. In the explanation of the sheet, the voluntary nature of the patient’s participation, objectives, and methodology of the study; the confidentiality of the data; and the freedom to interrupt the study without repercussions for the patient’s therapeutic plan were highlighted. Once participation in the study was agreed on, participants were asked to sign the informed consent form, and if the individual was incapacitated, the legal guardian signed it.
Results
The mean score for psychological resilience was 25.08 (SD = 7.53; range = 6-40), which can be qualified as low, since it is in the third quartile of CD-RISC’s scale (Campbell-Sills & Stein, 2007). The comparison of the mean psychological resilience obtained in this study with the mean psychological resilience recorded by other studies of nonpsychiatric participants shows a lower psychological resilience in the sample of patients diagnosed with BPAD (T = −2.87; p < .01; mean 25.08 ± 7.53 vs. 27.41 ± 6.36; Notario-Pacheco et al., 2011). The same is true in the comparison with a multi-occupational sample of 742 participants (T = −9.25; p < .001; mean 25.08 ± 7.53 vs. 32.6 ± 7.2; Soler et al., 2016) and 226 unemployed (T = −7.90; p < .001; mean 25.08 ± 7.53 vs. 31.5 ± 7; Fernández-Valera et al., 2018). No statistically significant differences were found in psychological resilience according to the different types of BPAD.
Table 2 shows a comparison between the results obtained in our study on resilience in BPAD with those obtained by other previous studies on psychiatric clinical samples that have used the same measurement instrument for resilience.
Mean Scores in Resilience Evaluated With the Connor-Davidson’s Resilience Scale 10 in Different Studies on Patients With Psychiatric Pathology.
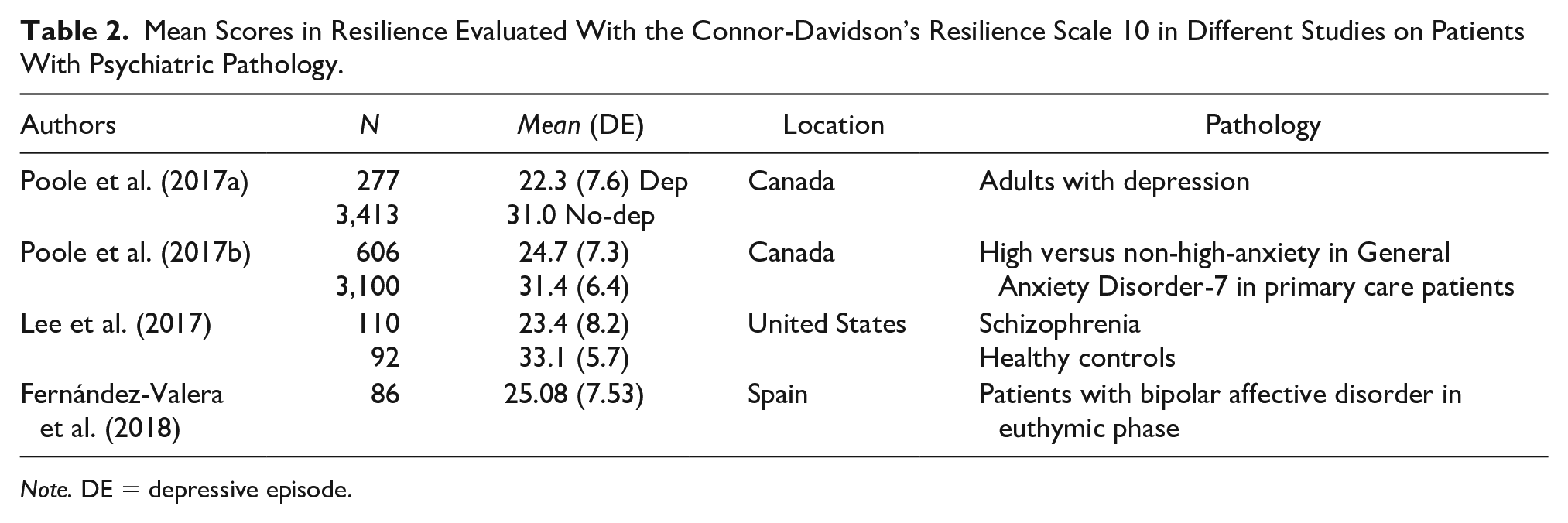
Note. DE = depressive episode.
Significant differences were found in psychological resilience according to whether or not the patients had attempted a suicide; thus, those who had attempted a suicide recorded a lower psychological resilience (T = 3.30; p ≤ .001; 20.61 ± 6.58 vs. 26.52 ± 7.29). No other significant differences were found when contrasting the means of the other sociodemographic and clinical variables included in the study.
Table 3 shows the correlations between the quantitative variables of the study. Psychological resilience is inversely associated with a greater number of depressive episodes.
Pearson’s Correlation Coefficients Between the Main Variables of the Study (N = 86).
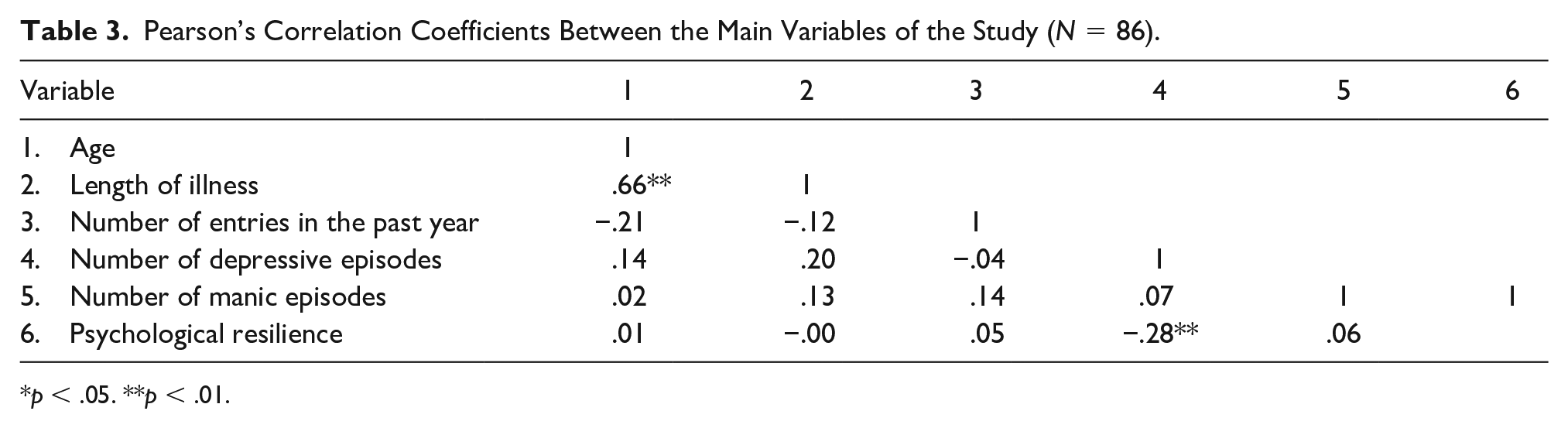
p < .05. **p < .01.
Discussion
The main objective of this study was to analyze the relationship between psychological resilience and suicide attempts along with different relevant clinical and sociodemographic variables in euthymic patients with BPAD.
The results show that patients with BPAD have lower psychological resilience than various samples of the general population, with no significant differences between the two types of diagnosis (BPAD 1 and BPAD 2). These data are consistent with the results of previous studies that indicate lower psychological resilience in BPAD in the euthymic phase (Hofer et al., 2017; Lee et al., 2017; Min et al., 2012; Mizuno et al., 2016) as well as in the remission phase (Deng et al., 2018). Patients with BPAD who have experienced a greater number of depressive episodes since diagnosis showed lower psychological resilience than those with manic and/or hypomanic decompensation. This finding is consistent with previous studies (Choi et al., 2015), although in our work, unlike the others, we used the CD-RISC version of 10 items to assess resilience.
Recently published meta-analysis (Färber et al., 2020) concludes that resilience and mental health are strongly correlated. High levels of resilience are associated with good mental health.
Regarding the comparison between the results obtained concerning psychological resilience in BPAD with nonpsychiatric samples (university students, workers, and the unemployed), it was discovered that the score for resilience is lower in patients with BPAD (Fernández-Valera et al., 2018; Soler et al., 2016).
The results of the present study show a negative and significant association of resilience with the existence of suicide attempts—patients diagnosed with BPAD who have made a suicide attempt during the course of their illness also exhibit lower psychological resilience. Previous studies, such as those by Roy et al. (2007, 2011), find similar results and also highlight that low psychological resilience is a risk factor for suicide attempts. However, in the study by Choi et al. (2015) on psychological resilience and impulsivity in BPAD in the euthymic phase, no association was found between these variables (Choi et al., 2015). The discrepancy between the results of the study by Choi et al. (2015) and the one presented here may be due to two factors. The first is that they used the 25-item CD-RISC scale instead of the 10-item version to assess psychological resilience, and the second is based on Choi et al.’s (2015) exclusion of those patients with current alcohol consumption disorder who are included in our sample. A meta-analysis published in 2014 (Carrà et al., 2014), found a close association between alcohol consumption disorder and suicide attempts in bipolar patients.
No statistically significant relationships or differences were found in psychological resilience with other sociodemographic and clinical variables. This is consistent with the study by Ang et al. (2018) conducted in nursing professionals and also using CD-RISC 10, where no differences were found according to either sex or marital status regarding psychological resilience. However, in the study by Notario-Pacheco et al. (2011), it was observed that women and patients under 25 years old had lower scores. These studies, in which discrepancies are observed, were conducted in samples with heterogeneous sociodemographic and clinical characteristics, which could interfere with the inequality of results.
Few studies have used the CD-RISC 10 item scale to measure resilience in psychiatric samples. In those that have, it is observed that the results are similar to those found in this study, with people with mental pathology presenting a lower score in resilience. It should be noted that in the research carried out by Poole et al. (2017a, 2017b) in people with depression and anxiety, resilience is lower than in the sample of our study.
Currently, there is little research linking resilience and suicide attempts in people diagnosed with BPAD. These results are important, as psychological resilience can act as a protective factor in BPAD (Ozawa et al., 2017) and decrease the number of suicide attempts and depressive episodes. In this sense, studies on intervention programs focused on psychological resilience in patients diagnosed with BPAD and with suicide attempts are insufficient. Only the article by Camardese et al. (2018), which evaluated the effectiveness of an intervention program to develop psychological resilience by comparing euthymic individuals with bipolar depressive patients who were not in remission, observed a significant improvement in psychological resilience, without presenting differences between the two groups (Camardese et al., 2018).
For the adequate interpretation of the results obtained, a number of limitations must be taken into account. The first is that there may be a bias in patient responses due to social desirability. Second, it is a single-center design, and this coincides with a sample that is more male than female, which is not the usual distribution of BPAD patients (Carvalho et al., 2020). The third is the impossibility of completely eliminating the effects of subsyndromic symptoms in some patients, despite the fact that they participated in the study during the stabilization phase of the disease. Fourth, being a cross-sectional study, it is difficult to determine the causal direction of relationships of psychological resilience and other variables. Finally, interviewer bias must also be taken into account, since the data were collected by different nursing professionals, although trained and under the control of the research team, which could lead to interindividual variations.
Results obtained have an important application for future practice. Identification of lower psychological resilience could alert us to a greater risk in patients with BPAD. The development of new intervention strategies would help us promote psychological resilience in this population and can create better adaptation to adverse situations, such as suicide attempts.
The management of the concept of resilience by mental health nurses would help patients diagnosed with BPAD to understand and overcome stressful situations, such as their own illness process. The promotion of resilience in patients diagnosed with BPAD would facilitate a more adaptive and positive coping with the illness and their recovery process.
Further studies on the effectiveness of psychological resilience development programs in patients diagnosed with BPAD are needed. They can also investigate the role of specialist nurses in this topic.
Conclusions
Patients diagnosed with BPAD have lower psychological resilience than the general nonpsychiatric population. No significant differences have been found between the two types of BPAD. An inverse and significant relationship is found between the number of depressive episodes and psychological resilience. No others significant associations were found with the sociodemographic and clinical variables studied. It has been observed that those patients diagnosed with BPAD who had not had any suicide attempts since the onset of their illness had higher scores in psychological resilience.
Footnotes
Acknowledgements
We would like to thank the specialist nurses at the Mental Health Centre of the Fundación Althaia in Manresa, Barcelona, Spain, for their collaboration in the collection of data for this study.
Author Roles
All authors contributed to the conception or design of the study or to the acquisition, analysis, or interpretation of the data. All authors drafted the manuscript, or critically revised the manuscript, and gave final approval of the version that was submitted for publication. All authors agree to be accountable for all aspects of the work, ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.