
Abstract
BACKGROUND:
Although the nursing staff is fundamental in assisting individuals with mental illnesses (MI) to stop tobacco use, they often have mixed feelings about providing tobacco treatment (TT) services to people with MI in inpatient psychiatric settings.
AIMS:
Therefore, this study aimed to understand factors associated with nursing staff’s intentions to provide TT interventions for individuals diagnosed with MI in a psychiatric facility using the constructs of the theory of planned behavior (TPB).
METHOD:
Secondary data analysis was performed using cross-sectional data collected from 98 nursing staff who worked in a state inpatient psychiatric facility. A 15-item questionnaire was used to assess nursing staff intentions to provide TT services based on TPB constructs, including attitudes (four items), subjective norms (four items), perceived behavioral controls (four items), and intentions (three items) toward providing TT. The mean scores of each subscale ranged from 1 to 7. A logistic regression analysis was used to examine the relationship between TBP constructs and nursing staff intentions to provide TT for people with MI.
RESULTS:
Nursing staff had an acceptable mean score in the intentions subscale (4.34 ± 2.01). Only two constructs of TPB explained nursing staff intentions to provide TT: subjective norms (OR = 2.14, 95% CI [1.46, 3.13]) and perceived behavioral control (OR = 2.33, 95% CI [1.32, 4.12]).
CONCLUSIONS:
The constructs of the TPB, the subjective norms, and the perceived behavior control were able to predict nurses’ intentions to provide TT for inpatients in a psychiatric setting. Accordingly, we suggest implementing policies that make TT a normative practice while supporting the confidence and competence of nurses to deliver TT in psychiatric facilities.
Background
The prevalence of smoking or tobacco use among people diagnosed with mental illnesses (MI) is higher than the general population (Jamal et al., 2016; Lemyre et al., 2019; Pettey & Aubry, 2018; Prochaska et al., 2017). People with MI may report that smoking cigarettes helps them manage their psychiatric illness symptoms (Prochaska, 2011; Trainor & Leavey, 2017), cope with their stressors, and socialize and interact with others (Peckham et al., 2016; Twyman et al., 2014). According to the Center for Behavioral Health Statistics and Quality (2017), 32% of adults with MI are current smokers compared with 23.3% of adults with no mental illnesses. In a meta-analysis of 203 studies, researchers found that having a MI diagnosis is associated with 10 years of potential life lost compared with the general population, and around 67% of these deaths were due to typical causes (Walker et al., 2015). These individuals often die due to cardiovascular disease, cancers, and respiratory illnesses that are causally linked to smoking cigarettes (Callaghan et al., 2014). Furthermore, having a MI and smoking can double the risk of death compared with those with MI who do not smoke (Hser et al., 1994; Tam et al., 2016). In fact, the death rate among people with MI who smoke accounts for more than 40% of all the deaths associated with tobacco use each year, and it has been suggested that smokers with MI die 25 years earlier than nonsmokers due to their smoking (Prochaska et al., 2017). Therefore, because of the compounding detrimental effects of having MI and smoking, it is important to reach this population and to offer them tobacco treatment (TT) services.
People with MI are often amenable to smoking cessation (Brunette et al., 2017; Prochaska, 2011; Smith et al., 2014), but they are less likely to be engaged in TT services (Schroeder & Morris, 2010; Trainor & Leavey, 2017). In a recent literature review of qualitative studies to understand barriers and facilitators of smoking cessation among people with severe MI, researchers identified several barriers to quit smoking (Trainor & Leavey, 2017). Among these barriers, researchers noted health providers and systemic barriers including lack of encouragement to quit by providers, providers using a judgmental inference, lack of knowledge among providers to provide smoking cessation services, lack of staff training, and lack of practice guidelines and smoking cessation resources (Trainor & Leavey, 2017). Indeed, smoke-free policies in the psychiatric setting support individuals with MI to engage in TT (Hecht et al., 2019; Lawn et al., 2015; de Oliveira & Furegato, 2014). Additionally, hospital policies can enhance the engagement of mental health care providers in delivering smoking cessation activities such as providing TT counseling and medications (Jegede et al., 2018; Marynak et al., 2018). However, few studies have examined the barriers faced by psychiatric mental health nurses in delivering TT within inpatient psychiatric settings.
Although offering TT for inpatients in a psychiatric facility is valuable, health care providers may have mixed attitudes about smoking cessation efforts in psychiatric units (Beyraghi et al., 2018). To illustrate, some health care providers believe that smoking cessation can benefit people diagnosed with MI, but they are concerned about managing patients’ aggression and noncompliance when banning smoking (Lawn & Pols, 2005; Neven et al., 2019; Ratier-Cruz et al., 2020; Wye et al., 2010). Moreover, some social barriers such as health care provider smoking behavior may interfere with their role to provide TT for the psychiatric patients (Johnson et al., 2009). Staff attitudes toward providing TT services for people diagnosed with MI can affect their actual behavior. Thus, it is important to consider health care providers’ attitudes toward engaging individuals with MI in TT activities.
The theory of planned behaviors (TPB) is often used to understand predictors of intentions to engage in specific behaviors. According to this theory, people’s attitudes (i.e., a person’s evaluation of the behavior), subjective norms (i.e., social pressures), and perceived behavioral control (i.e., how difficult it is to perform a new behavior) are factors that predict their intentions to perform any behavior (Ajzen, 1991). Because we are interested in nurses’ intentions to provide TT services for individuals diagnosed with MI, we relied on the TPB framework to understand the factors that affected their intentions. Although qualitative approaches can offer valuable narrative information in understanding this phenomenon, using a theory-driven approach can further produce predictive patterns that can become targets for intervention. As such, the purpose of this study was to assess nurses’ intentions to provide TT services for people living with MI using the TPB framework. The specific aim was to determine whether attitudes, subjective norms, and perceived behavior control are associated with nursing staff intentions to provide TT services for inpatients with MI in a psychiatric setting.
Nursing staff are trusted sources of information. They represent the greatest number of health care workers in health institutions. Nurses can provide tobacco cessation interventions for smokers and help increase successful cessation of tobacco use (Duffy et al., 2015). Nurses who work in mental health institutions have a valuable role to play in helping people with MI quit smoking (Hecht et al., 2019; Katz et al., 2014). Although nurses are routinely engaged in the process of helping people in psychiatric settings manage their illnesses, as compared with other providers, they report low to moderate intentions to deliver TT (Okoli et al., 2017). Therefore, we sought to understand the factors associated with the intention to provide TT services in an inpatient setting, because these intentions will often predict the performed behavior according to the TPB (Ajzen, 1991).
Method
Study Design and Sample
This study was a secondary analysis of data gathered from a quota convenience sample of 98 nursing staff members who worked in a state psychiatric hospital at the time of data collection in 2017 and agreed to participate in the research study (Okoli et al., 2017). Staff members who were not state hospital employees were excluded from the study. The ethical approval for conducting the original study was obtained from the institutional review board.
In the state psychiatric hospital, a tobacco-free policy was implemented in 2014, and tobacco use is now banned inside the facility and on the grounds; therefore, all hospital patients are screened for tobacco use, and counseling and medication is offered to manage nicotine withdrawal per the hospital policy. Nurses are involved in providing TT as part of their jobs. Nursing activities include screening for tobacco use, administering Food and Drug Administration–approved nicotine replacement therapy, monitoring nicotine withdrawal, and practicing tobacco cessation counseling with patients.
Measures
Demographic Questionnaire
Age (in years), gender (male vs. female), work experience (in months), level of education (high school or some college vs. college graduate), marital status (married/widowed or unmarried couples vs. separated/divorced or single), ethnicity (White vs. non-White), and smoker or live with a smoker (yes vs. no) were all used to describe the participants characteristics.
Theory of Planned Behavior Concepts
Based on the TPB (Ajzen, 2011), the authors of the original study developed a questionnaire to assess nurse attitudes (four questions), subjective norms (four questions), perceived behavioral control (four questions), and intentions (three questions) to engage in TT for psychiatric inpatients (see Supplemental Material). Further details about the study instrument are available in the original article (Okoli et al., 2017). In each question, participants responses ranged from 1 = extremely disagree to 7 = extremely agree. A higher score in each subscale indicated higher attitudes, subjective norms, perceived behavior control, or intentions. The instrument has an internal consistency for the attitude’s subscale (α = .70), subjective norms subscale (α = .76), intentions subscale (α = .92), and poor internal consistency for the perceived behavioral control subscale (α = .55). For this study, a median split was used to dichotomize the intention variable to higher intenders to provide TT scored (4 to 7) versus lower intenders to provide TT scored (less than 4).
Data Analysis
Data were analyzed using IBM SPSS version 26. Descriptive statistics, including means, standard deviations, frequencies, and percentages were used to describe sample characteristics. Chi-square, independent sample t test, and Mann–Whitney analyses were used for dichotomous, ordinal, and continuous data to present differences between demographic characteristics and lower intention versus higher intention. Because the intentions scores were not normally distributed, a mean of the scores was obtained to form a categorical outcome of low or high intentions to provide TT. A logistic regression analysis was used to identify factors associated with nursing staff’s intentions to provide TT based on the TPB constructs. The Hosmer–Lemeshow goodness-of-fit test was used to determine the fit of the final model. For all analysis, an alpha level = .05 was used to determine the significance.
Results
Sample Description
The total sample consisted of 98 nursing staff with a mean age of 37.77 years (SD = 12.83). The majority of the participants were female (75.5%), White (81.6%), college graduates (69.4%), and who did not smoke or live with a smoker (79.6%). Overall, the mean scores for the attitudes, subjective norms, perceived behavioral control, and intentions subscales were 4.86, 3.57, 4.15, and 4.34, respectively (Table 1).
Characteristics of Study Participants by Their Intention.
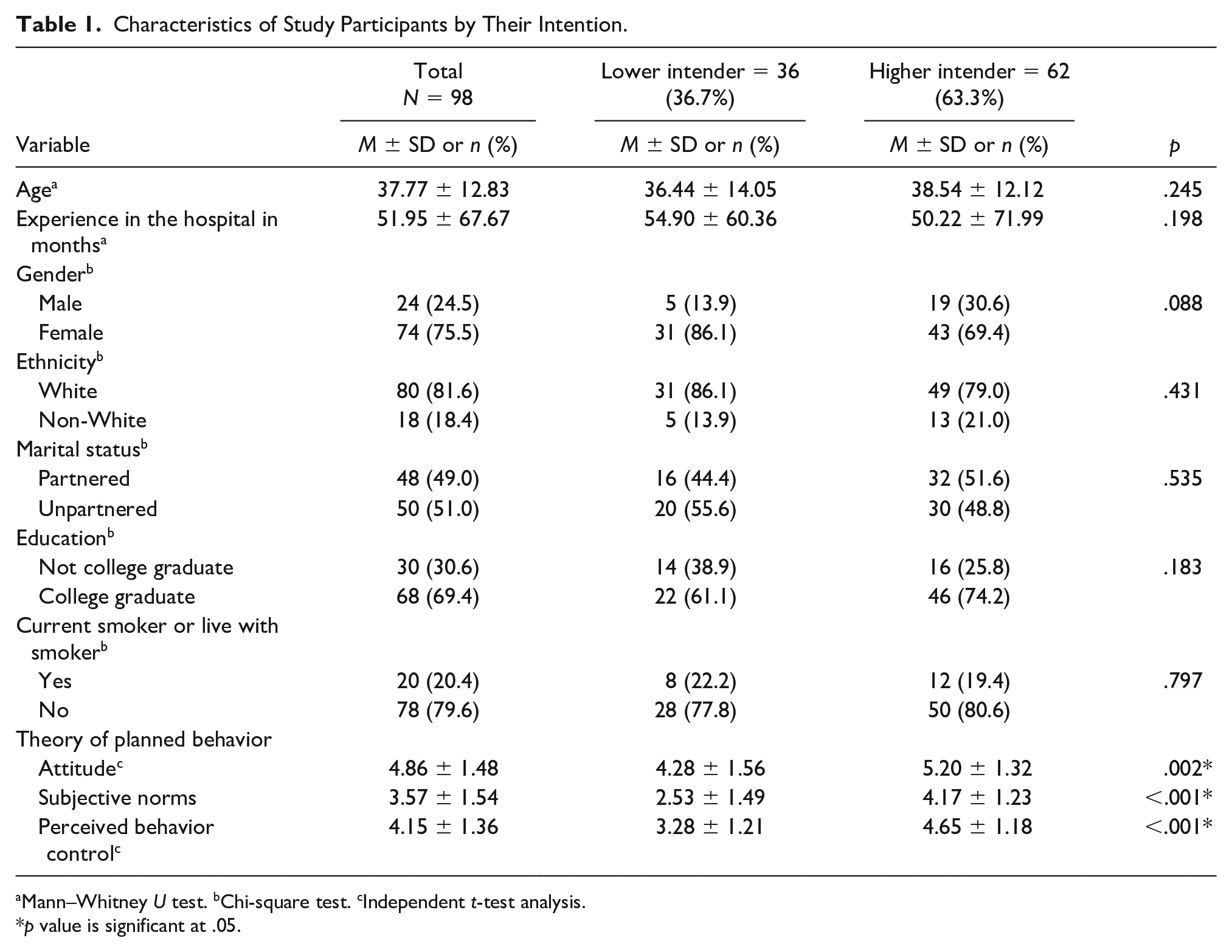
Mann–Whitney U test. bChi-square test. cIndependent t-test analysis.
p value is significant at .05.
Differences in Intentions to Provide Tobacco Treatment by Sample Characteristics
Further analysis with independent t-test analysis, chi-square test, and Mann–Whitney U tests were used to examine variations between higher and lower intentions to provide TT (Table 1). However, there were no significant differences between lower and higher intenders with regard to age, months of experiences, gender, ethnicity, marital status, education, their current smoking status, or if they live with smokers (p > .05).
On the other hand, our analyses showed significant differences in the means of the TPB constructs and higher or lower intention status (Table 1). People with higher intention reported higher attitude mean scores (5.20 vs. 4.28, p = .002), subjective norms (4.17 vs 2.53, p < .001), and perceived behavior control (4.65 vs. 3.28, p < .001) than people with lower intentions.
Factors Associated With the Intentions to Provide Tobacco Treatment
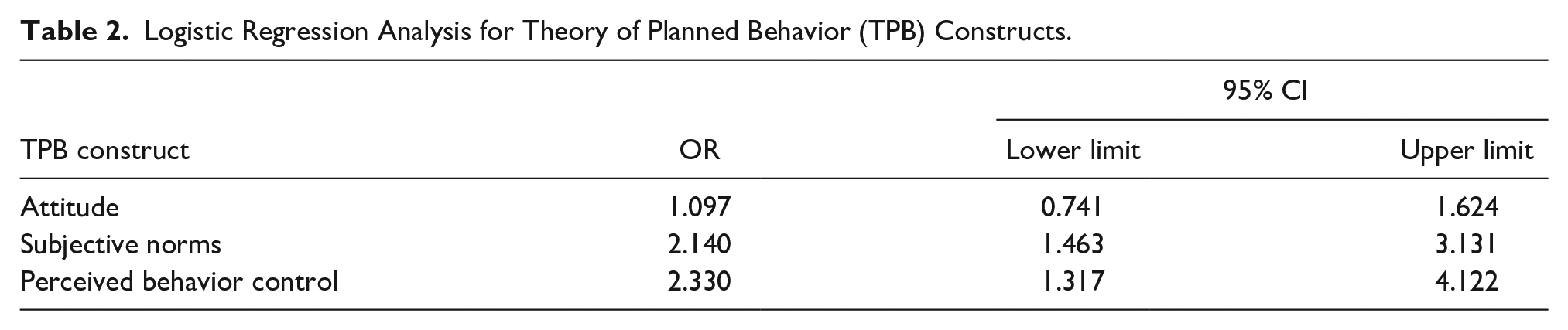
When attitudes, subjective norms, and perceived behavioral control were entered into the analysis, a good fitting model was obtained (Hosmer–Lemeshow chi-square = 4.204, df = 8, p = .838), in which subjective norms (OR = 2.14, 95% CI [1.46, 3.13]) and perceived behavior control (OR = 2.33, 95% CI [1.32, 4.12]) but not attitudes (OR = 1.10, 95% CI [0.74, 1.62]) were significantly associated with intentions to provide TT (Table 2).
Logistic Regression Analysis for Theory of Planned Behavior (TPB) Constructs.
Discussion
In the psychiatric hospital setting, nurses play an essential role in assisting people with MI to quit smoking. The main purpose of this analysis was to assess attitudes, subjective norms, and perceived behavioral control as predictors of nursing staff intentions to provide TT to individuals with MI in a psychiatric setting. Our results indicate that two of the three constructs of TPB, subjective norms, and perceived behavior control, were strong predictors of nursing staff intentions to provide TT. Nursing staff who reported higher scores in subjective norms and perceived behavioral control are more likely to report higher intention scores. Researchers have reported many differences about predictors of nursing staff’s intention to provide TT in the literature. For example, one team of researchers reported that the concept of subjective norms was the most important predictor of community nurses’ intention to provide TT (Shelley et al., 2014). Whereas, another set of researchers found that attitude and perceived behavioral controls were the strongest predictors for mental health providers’ intentions to provide TT (Blankers et al., 2016). Our results can be justified by considering that our sample was recruited from a tobacco-free environment where there was a set of policies and TT protocols that assure the implementation of TT provision for all inpatient tobacco users. The implementation of TT policies in the hospital can normalize the tobacco-free environment implementation of TT by providing a supportive environment that has positively enhanced providers’ intentions to provide TT (Choi & Kim, 2016).
In this study, we did not include nursing staff level of education in the logistic regression model as there was no significant difference between groups with regards their intentions. However, as shown in Table 1, college graduate nurses’ education indicates higher intentions to provide TT in a psychiatric setting, that is, college-educated nursing staff report having higher intentions to engage in TT than non-college-educated nursing staff. Previous research has shown that baseline knowledge about TT, attitudes, and the level of awareness on TT all varied among nursing staff. For example, advanced nurse practitioners reported higher intentions and knowledge to provide TT than registered nurses and practical nurses (Sheffer et al., 2011). Moreover, nursing education programs, which include limited content about TT, do not prepare nursing staff who are confident to provide TT (Sarna et al., 2009). Unfortunately, the lack of education and confidence among nursing staff is considered a barrier to the delivery of TT to individuals with MI (Sheals et al., 2016). Therefore, more efforts are needed to involve most nursing staff in training programs to improve their self-efficacy to engage in TT (Borrelli et al., 2008; Sheffer et al., 2011).
Finally, in this study, around 20% of our sample were smokers or individuals who lived with smokers, but we found no differences in the intentions between the two groups. Our finding is congruent with the previous work conducted to assess the intentions of mental health providers who work in smoke-free hospitals to provide TT interventions (Blankers et al., 2016; Okoli et al., 2017). In contrast, Sarna et al. (2009) found that nurses who work in psychiatric settings and smoke themselves were less likely to be engaged in TT activities. Indeed, nurses who smoke may be ambivalent about providing TT; nurses may approach smoking policies indifferently, evasively, engagingly, or feel forced to comply based on their vulnerability to address tobacco use (Radsma & Bottorff, 2009). Thus, the findings of Sernas’ study led the authors to recommend implementing tobacco-free policies to involve nursing staff in the provision of TT regardless of smoking status (Sarna et al., 2009).
Implications
Based on our study findings, TT culture in a psychiatric facility plays a significant role in treatment provision. Implementing tobacco-free policies can de-normalize tobacco use in psychiatric settings (Lavack, 1999), improve staff and patients’ attitudes toward tobacco use cessation (Riad-Allen et al., 2017), and enhance the delivery of TT (Choi & Kim, 2016). Therefore, psychiatric mental health nurses should promote tobacco-free cultures in psychiatric settings by advocating tobacco-free policies, supporting TT guidelines/protocols, and providing educational resources to improve TT delivery.
Our findings further support the need to prepare well-trained psychiatric nurses to provide TT service for inpatients in psychiatric settings. Since psychiatric nurses work closely with patients with MI and are more aware of their challenges with substance use, they are well positioned to tailor TT to the unique psychiatric needs of their patients. By doing so, psychiatric nurses can increase the likelihood of engaging patients in TT within a psychiatric facility.
Limitations
Few studies have assessed nursing staff intentions to engage in TT for people with MI, and our study is subject to some limitations. First, this analysis is based on the data selected from a convenience sample of nursing personnel, which did not represent the views of all roles in the nursing staff department. Our sample is limited to registered nurses and mental health associates (e.g., practical nurses and nurse practitioners). This study should be replicated with representation from all roles of the entire nursing staff department. Second, the TBP instrument lacked internal consistency of perceived behavioral control, and revisions are necessary to fully capture the construct of perceived behavioral control (α = 0.55). Despite these limitations, the results of this study provided important insight into nurses’ intentions to engage in TT. These results could be used to support the development of new strategies (e.g., deliver TT training) that facilitate the delivery of TT services among nurses in the psychiatric setting.
Conclusion
To conclude, TPB indicated that nursing staff have moderate-level intentions to provide TT in psychiatric settings. The TPB constructs, subjective norms, and perceived behavior control are a supportive framework for predicting nursing staff intentions to provide TT for patients in such settings. By building on the relationship between subjective norms and perceived behavior control, we may be able to increase nurses’ intentions to provide TT. Setting policies and increasing nurses’ self-efficacy can subsequently improve nursing staff intentions to provide TT for patients hospitalized with MI.
Supplemental Material
sj-pdf-1-jap-10.1177_10783903211045737 – Supplemental material for Nursing Staff Attitude, Subjective Norms, Perceived Behavior Control, and Intention to Provide Tobacco Treatment in a Psychiatric Hospital
Supplemental material, sj-pdf-1-jap-10.1177_10783903211045737 for Nursing Staff Attitude, Subjective Norms, Perceived Behavior Control, and Intention to Provide Tobacco Treatment in a Psychiatric Hospital by Bassema Abufarsakh and Chizimuzo T.C. Okoli in Journal of the American Psychiatric Nurses Association
Footnotes
Author Roles
All authors contributed to the conception or design of the study or to the acquisition, analysis, or interpretation of the data. All authors drafted the manuscript, or critically revised the manuscript, and gave final approval of the version that was submitted for publication. All authors agree to be accountable for all aspects of the work, ensuring integrity and accuracy.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.