
Abstract
Background:
RE-KINECT (NCT03062033), a real-world study of possible tardive dyskinesia (TD) in antipsychotic-treated patients, included a questionnaire to assess the effects of patients’ abnormal involuntary movements on caregivers.
Aims:
To capture the experiences of caregivers who assisted individuals with abnormal involuntary movements that were confirmed by clinicians as being consistent with TD.
Methods:
Qualified (nonpaid) caregivers were invited to complete a questionnaire that included the following: caregivers’ sociodemographic characteristics, their perceptions about the impact of abnormal involuntary movements on patients, and the impact of these movements on themselves (caregivers).
Results:
Of the 41 participating caregivers, 25 (61.0%) were women, 20 (48.8%) were employed full time or part time, and 35 (85.4%) were family members or friends. Based on responses from caregivers who noticed patients’ abnormal involuntary movements and were caring for individuals who also noticed those movements, 48.0% of patients had “a lot” of severity in ≥1 body region and 76.0% had abnormal involuntary movements in ≥2 regions. Caregiver ratings were significantly correlated with patient ratings (but not with clinician ratings) for maximum severity of abnormal involuntary movements and the number of affected regions (both p <.05). Based on their own judgments and perceptions, caregivers reported that the patient’s movements had “some” or “a lot” of impact on their (caregiver’s) ability to continue usual activities (50.0%), be productive (58.3%), socialize (55.6%), or take care of self (50.0%).
Conclusions:
Caregivers as well as patients are negatively affected by TD, and the impact of TD on caregivers’ lives should be considered when determining treatment options.
Keywords
Introduction
Informal (nonpaid) caregiving of patients with chronic conditions is becoming more commonplace due to longer life expectancy, changes in institutionalized care, and the increasing number of diseases requiring long-term treatment. Caregivers are instrumental in managing patients’ medical conditions (including consequences or side effects of treatment), helping patients retain independence, and providing emotional support. Although caregiving helps decrease patient burden, caregivers themselves can be negatively affected (Del-Pino-Casado et al., 2021; Liu et al., 2020; Pinquart & Sorensen, 2003; Schulz & Beach, 1999). Caregivers may experience poorer physical and mental health, diminished life expectancy, financial strain, loss of productivity, inability to work, and social isolation (Adelman et al., 2014; Greenwood et al., 2018; Lin et al., 2018; Pinquart & Sorensen, 2003; Schulz & Beach, 1999).
Tardive dyskinesia (TD) is a persistent and potentially disabling movement disorder associated with prolonged exposure to antipsychotics (Caroff et al., 2018). Patients with TD experience abnormal involuntary movements in the head/face, neck/trunk, upper extremities, and/or lower extremities. These movements can have negative physical consequences, including impaired speech, difficulty breathing or swallowing, and loss of motor skills or gait imbalance (Strassnig et al., 2017). Even mild and localized movements can decrease a patient’s quality of life and impair daily functioning, including embarrassment and a decreased desire to socialize (Ascher-Svanum et al., 2008; Browne et al., 1996; Depression and Bipolar Support Alliance, 2017; Yassa & Jones, 1985). TD symptoms may prompt some patients to discontinue antipsychotic medications, which can exacerbate psychiatric symptoms, increase hospitalizations, and worsen quality of life (Adrianzen et al., 2010; Novick et al., 2010). Caregiver burden has been described for serious mental illnesses (Brain et al., 2018; Granek et al., 2016; Shiraishi & Reilly, 2018; Vargas-Huicochea et al., 2018) and progressive movement disorders (Domaradzki, 2015; Grun et al., 2016; Martinez-Martin et al., 2007; Morgan et al., 2017; Rodriguez-Violante et al., 2015). To our knowledge, however, there are no studies that examine the burden on individuals who care for patients with both a psychiatric illness and a comorbid movement disorder such as TD.
RE-KINECT (NCT03062033) was a real-world, prospective screening study that assessed the presence and impact of clinician-confirmed “possible TD” (abnormal involuntary movements consistent with TD) on patients, based on clinician and patient reports; these results are published separately (Caroff et al., 2020). To address the lack of data regarding caregiver burden in TD, RE-KINECT invited caregivers of these patients to complete a questionnaire that elicited their perceptions and experiences. Results from this questionnaire, along with corresponding clinician- and patient-reported results, are presented.
Methods
Study Design
RE-KINECT included a visual symptom screen by office staff and assessment of possible TD based on clinician evaluation (Figure 1). The study was conducted from April 2017 to January 2019 at 37 outpatient psychiatry practices in the United States, each of which received Institutional Review Board approval (Quorum Approval Number 32243) prior to initiating any study procedures. Project and data management were provided by Evidera (Bethesda, MD).
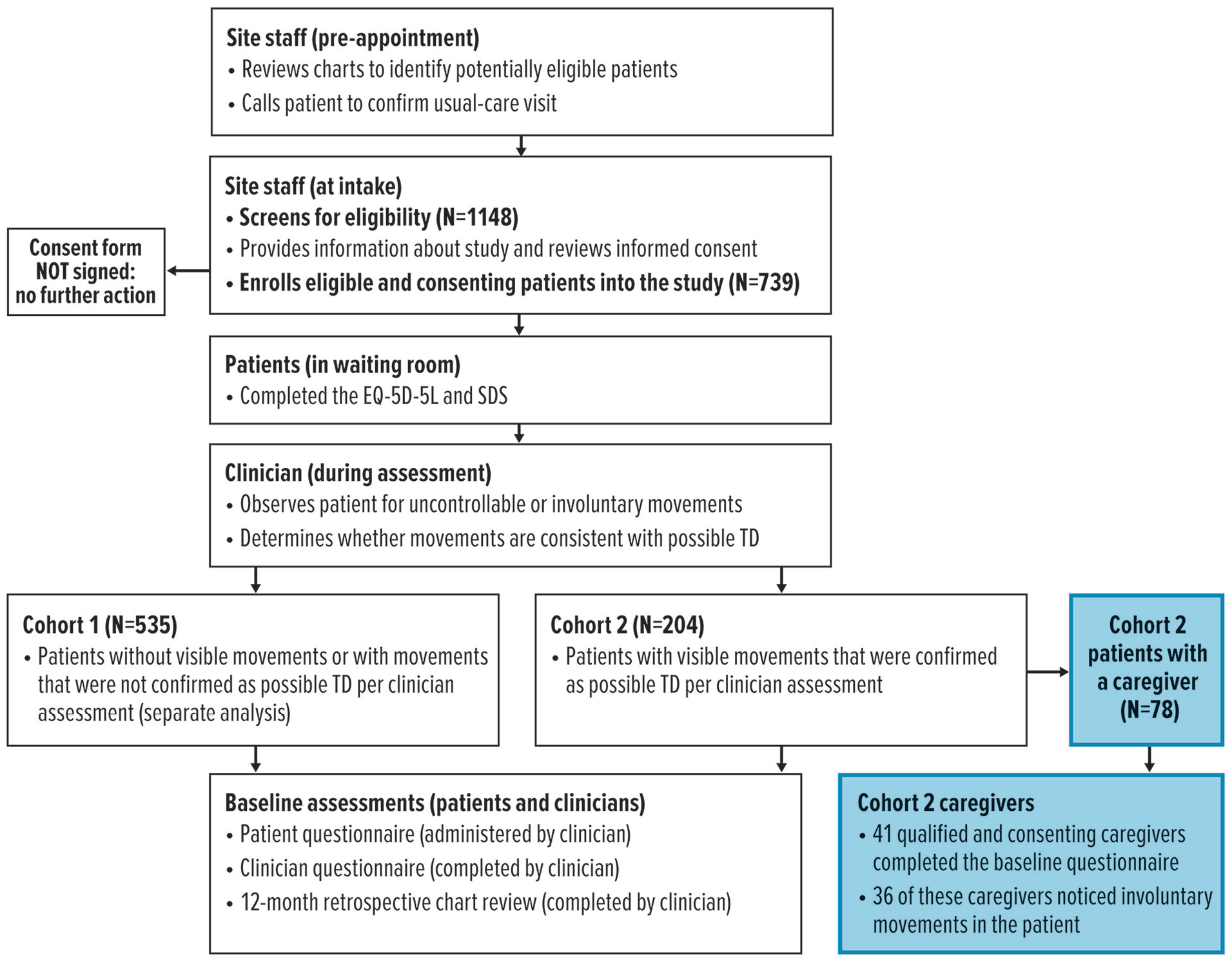
Overview of patient cohort assignment and caregiver enrollment.
Patients attending their usual-care visit (baseline visit) were prescreened for study eligibility as follows: ≥18 years old, ≥3 months of cumulative lifetime exposure to antipsychotic medication, and ≥1 clinician-confirmed psychiatric diagnosis per Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) criteria (Caqueo-Urizar et al., 2009), based on review of their medical records. Eligible patients who provided written informed consent were assessed by a clinician for abnormal involuntary movements in any of the following regions: head/face, neck/trunk, upper extremities, and lower extremities. Based on this assessment, patients were assigned to Cohort 1 (with no abnormal involuntary movements or with movements that were inconsistent with TD) or Cohort 2 (with abnormal involuntary movements that were confirmed by the clinician as possible TD).
For this study, a “qualified” caregiver was defined as an individual who knew the patient well, may have engaged in traditional caregiving (e.g., assistance with activities of daily living), and/or was otherwise responsible for or concerned about the patient’s well-being but not paid (i.e., nonprofessional caregiver). Caregivers of patients with possible TD (Cohort 2) who agreed to participate and provided written informed consent were enrolled.
Baseline Measures and Analyses
After enrollment, caregivers were given a questionnaire that included demographics, marital status, living situation, education, employment status, and relationship to the patient (see online supplement). Caregivers who noticed abnormal involuntary movements in the patient during the past 4 weeks were asked to assess these movements in each of 4 regions (head/face, neck/trunk, upper extremities, and lower extremities) using a simple rating scale based on their own judgments and perceptions (“none,” “some,” or “a lot”). The maximum severity rating (most severe rating in any region) and the total number of affected body regions were analyzed. Based on the number of corresponding patients who self-reported abnormal involuntary movements in the past 4 weeks, clinician and patient ratings of possible TD were also analyzed. Spearman’s correlations (Spearman, 1904) between these caregiver-, clinician-, and patient-reported ratings were performed for severity of abnormal involuntary movements in each body region, maximum severity rating, and number of affected regions. Correlation analyses were exploratory and not intended for hypothesis testing.
To assess potential differences between the perspectives of caregivers and patients, both groups were asked to rate the overall health status of patients (range, 0 = no health problems to 10 = health as bad as you can imagine) and identify which conditions patients spent the most time managing.
Caregiver burden was captured by the following items: impact of the patient’s overall health condition on the caregiver’s own life (range, 0 = no impact to 10 = impacted as bad as you can imagine); patient’s health condition that required the most time for assistance; impact of the patient’s abnormal involuntary movements on the caregiver’s ability to function; and degree of embarrassment or frustration/anger about the patient’s abnormal involuntary movements.
Results
Sociodemographic Characteristics (Cohort 2 Caregivers)
Of the 739 patients who were screened and clinically assessed, 204 (27.6%) were assigned to Cohort 2 (with visible signs of abnormal involuntary movements and clinician-confirmed possible TD). Among these Cohort 2 patients, 126 had no caregiver or did not report having a caregiver. Of the 78 reported caregivers, 37 were either paid professionals or did not provide consent for participating in the study. Of the remaining 45 qualified caregivers of Cohort 2 patients who provided consent and were enrolled in the study, 41 completed the questionnaire and were included for analysis (Figure 1).
The majority of caregivers were married (68.3%), lived with others (partner/spouse, family, or friends; 85.4%), and had some college education (68.3%); almost one half were employed full time or part time (48.8%; Table 1). Most (85.4%) described themselves as being family or friends with the patient.
Sociodemographic Characteristics of Cohort 2 Caregivers (N = 41).
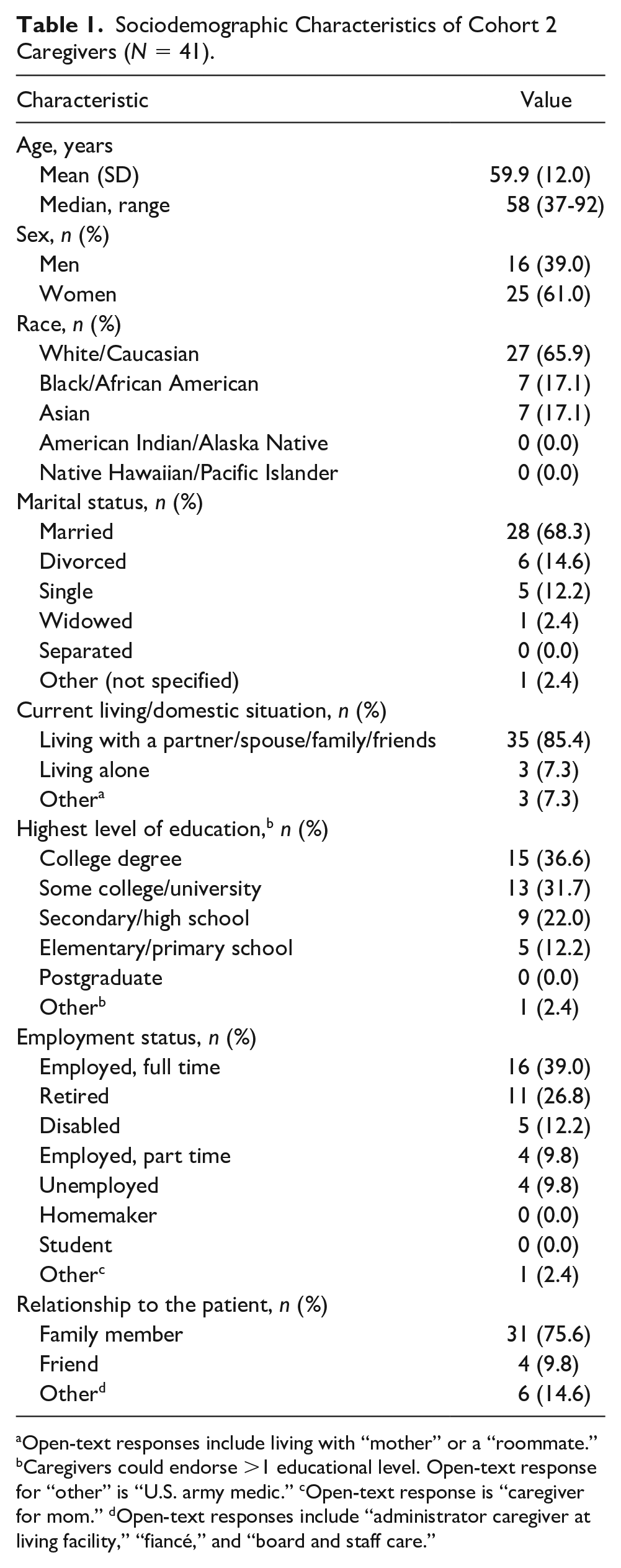
Open-text responses include living with “mother” or a “roommate.” bCaregivers could endorse >1 educational level. Open-text response for “other” is “U.S. army medic.” cOpen-text response is “caregiver for mom.” dOpen-text responses include “administrator caregiver at living facility,” “fiancé,” and “board and staff care.”
Assessment of Abnormal Involuntary Movements (Cohort 2 Caregivers, Patients, and Clinicians)
Of the 41 caregivers who completed the questionnaire, 36 (87.8%) reported noticing abnormal involuntary movements and were asked to rate the severity of those movements. Of the 36 patients identified by these caregivers, 25 self-reported having abnormal involuntary movements in the past 4 weeks. Caregiver-, patient-, and clinician-rated severity for these 25 patients are presented in Table 2.
Location and Severity of Abnormal Involuntary Movements in Patients With Possible Tardive Dyskinesia.
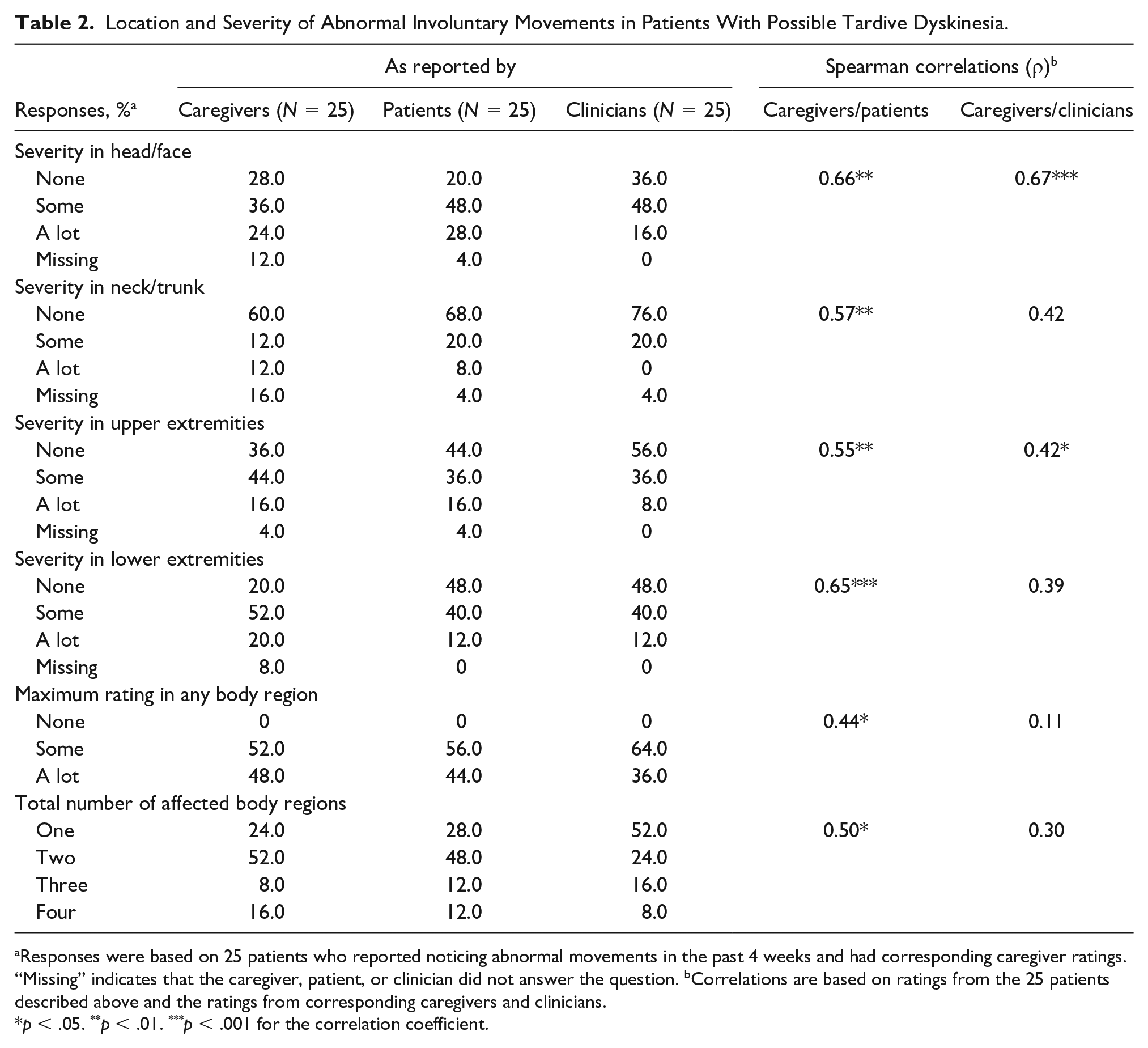
Responses were based on 25 patients who reported noticing abnormal movements in the past 4 weeks and had corresponding caregiver ratings. “Missing” indicates that the caregiver, patient, or clinician did not answer the question. bCorrelations are based on ratings from the 25 patients described above and the ratings from corresponding caregivers and clinicians.
p < .05. **p < .01. ***p < .001 for the correlation coefficient.
Exploratory correlation analyses based on these responses indicated that caregivers, patients, and clinicians generally agreed on severity of movements in the head/face, with correlation coefficients of 0.66 for caregivers/patients (p < .01) and 0.67 for caregivers/clinicians (p < .001; Table 2). Statistically significant caregiver/patient correlations (p < .05) were also found for the other three body regions (neck/trunk, upper extremities, lower extremities), maximum rating in any body region, and total number of body regions. In contrast, caregiver/clinician correlations were only significant for one additional body region (upper extremities); maximum rating and total number of body regions were not significantly correlated between caregivers and clinicians.
Health Status and Health Burden (Cohort 2 Caregivers and Patients)
Ratings of patients’ overall health status (from 0 = no health problems to 10 = health as bad as you can imagine) were similar between caregivers and patients, with mean scores of 5.3 and 5.6, respectively (see Table S1 in the online supplement). Both caregivers and patients responded that “mental health” was the condition that patients spent the most time managing. However, the percentage of caregivers who rated “mental health” as time-consuming for patients was higher than what patients reported (78.0% vs. 51.2%). Other conditions indicated as time-consuming by >30% of caregivers were “movement disorder” (39.0% vs. 17.1% [patient rated]) and “pain management” (34.1% vs. 29.3%).
Caregiver Burden (Cohort 2 Caregivers)
The impact of caring for patients’ health on caregivers’ lives ranged from 0 = no impact at all to 10 = impacted as bad as you can imagine, with a median score of 6 (moderate impact) and a mean score (±SD) of 5.2 (±3.3). Health conditions that caregivers reported spending the most time assisting patients with were mental health (68.3%), physical activity and nutrition (39.0%), and movement disorders (29.3%) (Figure 2).
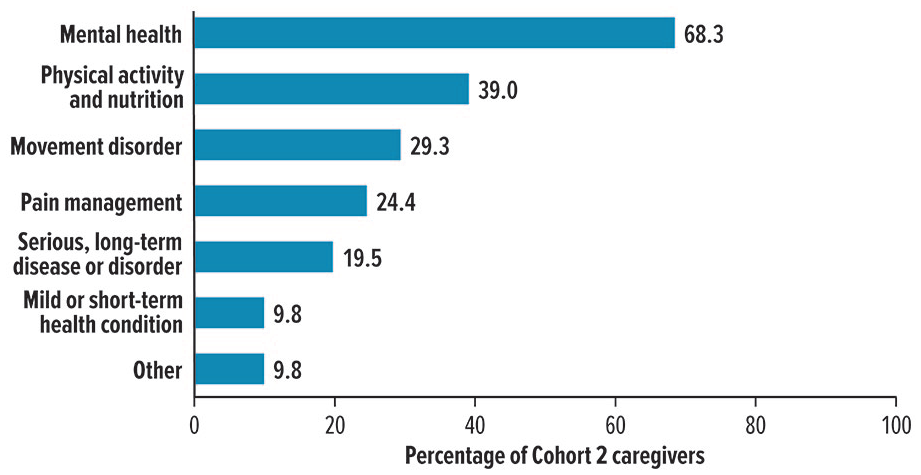
Health conditions that caregivers spent the most time in assisting patients with.
Based on the 36 caregivers who noticed abnormal involuntary movements in the past 4 weeks, ≥50% indicated that these movements had “some” or “a lot” of impact on the caregiver’s ability to continue usual activities (50.0%), be productive (58.3%), take care of self (50.0%), or socialize (55.6%) (Figure 3A). The majority also reported spending “some” or “a lot” of time assisting patients with abnormal involuntary movements (66.7%) and indicated that these movements had “some” or “a lot” of overall impact on caregivers’ lives (55.6%; Figure 3B). Feelings of frustration/anger (38.9%) or embarrassment (30.6%) about patients’ movements were also common.
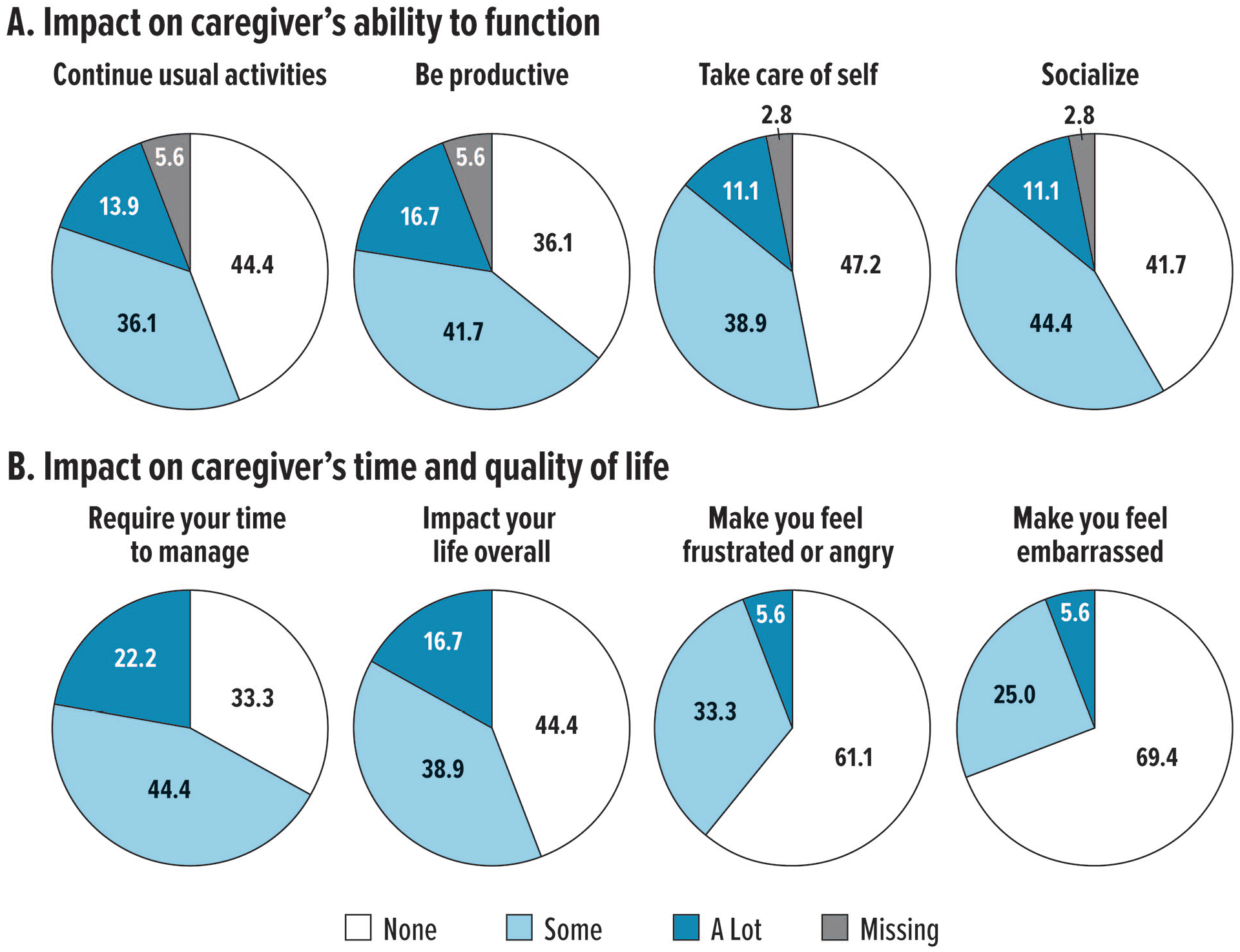
Impact of patient’s abnormal involuntary movements on caregivers.
Discussion
The substantial economic, social, emotional, and physical impact on individuals who care for patients with psychiatric disorders has been documented (Awad & Voruganti, 2008; Bauer et al., 2012; Blanthorn-Hazell et al., 2018; Caqueo-Urizar et al., 2009; Csoboth et al., 2015; Ivarsson et al., 2004; Ogilvie et al., 2005; Perlick et al., 2007; Perlick et al., 2016; Priestley & McPherson, 2016; Viana et al., 2013), but the added burden of movement disorders on these caregivers has not been studied. Given this lack of information, RE-KINECT was designed to gain caregivers’ perspectives on how the presence of possible TD affects patients’ lives as well as their own.
The vast majority of participating caregivers were either a family member or a friend (85.4%), and almost one half were employed full time or part time. For family and friends, the addition of caregiving to their regular employment and other daily responsibilities can be very burdensome. There was no control group for caregivers in RE-KINECT, but a 2015 study of unpaid family caregivers conducted by the National Alliance for Caregiving (NAC) and the AARP Public Policy Institute may provide some context (National Alliance for Caregiving and AARP Public Policy Institute, 2015). In the NAC/AARP study, which included 1,248 individuals who cared for ≥1 adult with a disability or illness, 85% were a family member or spouse, and 60% were employed. In both the NAC/AARP and the RE-KINECT studies, the majority of caregivers were women (60% and 61%, respectively). NAC/AARP caregivers were younger than RE-KINECT caregivers (mean age, 49 and 60 years, respectively), although the spousal caregivers in the NAC/AARP study were considerably older (mean 62 years). More research is needed to understand whether these differences have clinically or socially meaningful implications.
Caregivers and patients had similar perceptions about the overall health status of patients (supplemental Table S1). However, caregivers were more likely to rate various health conditions as being time-consuming for patients than the patients themselves, including “movement disorder” (39.0% vs. 17.1% [patient rated]). Without additional research, it is difficult to explain why caregivers’ perceptions of abnormal movements seemed to be worse than patients’ own perceptions. It is possible that some patients lacked insight into their own abnormal involuntary movements and that caregivers were therefore more aware of (and/or burdened by) patients’ health and movements than patients. It is also possible that patients may have been more accepting of TD and also understood the benefits of continuing their antipsychotic medication (rather than stopping it). Such issues may be clarified in future studies that focus on the patients’ own experiences and perceptions of TD.
By definition, all patients represented in the full caregiver cohort (N = 41) had possible TD with clinician-rated severity. However, only 36 caregivers noticed patients’ abnormal involuntary movements in the past 4 weeks; among these patients, 25 self-reported having abnormal involuntary movements. Correlation analyses based on these 25 patients indicated that caregivers, patients, and clinicians agreed on the severity of these movements in the head/face (Table 2). However, caregivers were much more likely to agree with patients than clinicians about the maximum severity of abnormal involuntary movements in any body region and the number of affected regions. These results raise several points to consider, including the issue of awareness. Because patients may be unaware of their TD symptoms, caregivers can be a valuable resource for information about the presence and functional/social impact of abnormal involuntary movements. However, since caregivers can also be unaware of such movements, all antipsychotic-treated patients should be regularly screened by clinicians for possible TD or other drug-induced movement disorders. During such screenings, clinicians may want to ask caregivers about their observations, especially if patients seem unaware of their symptoms. Caregivers may be able to describe the presence or severity of abnormal involuntary movements and any resulting impact on daily function that are not apparent during the office visit.
It is unknown why five caregivers did not notice abnormal involuntary movements. Although the caregiver questionnaire encompassed many different topics, it was not feasible to anticipate every question that would be needed to understand the full caregiver experience. In these five cases, patients may have had movements that were very mild and/or located in regions that were not easily observable or evaluated in the questionnaire. The inconsistency of TD symptoms (waxing and waning) may have also been a contributing factor. However, any such speculation is highly limited by the small sample size and the inherent constraints of a prospectively designed questionnaire. Nonetheless, given the short amount of time that clinicians often have with patients, lack of patient awareness, and the fact that some movements might not present during all encounters, caregivers should be considered an important corroborating source and should be asked to share their perspective on patients’ health conditions. As caregivers, these individuals have more opportunity to assess patients’ physical and mental well-being on a daily basis and to observe the impact of abnormal involuntary movements on patients’ lives.
To address the gap in data regarding caregiver burden in TD, the impact of abnormal involuntary movements on caregivers’ time, ability to function, and overall quality of life were assessed. Based on their own judgments and perceptions, 66.7% of caregivers indicated that these movements required “some” or “a lot” of their time; 29.3% responded that in terms of assisting patients, “movement disorder” was one of the health conditions that required the most time. In addition, ≥50% of caregivers reported that patients’ abnormal involuntary movements had “some” or “a lot” of impact on their own ability to continue usual activities, be productive, take care of self, or socialize. Feelings of frustration, anger, and embarrassment about patients’ movements were common, and 55.6% of caregivers indicated that these movements had a negative overall impact on their own lives.
The implications of these findings are substantial and worth considering. Clinicians are often focused on the condition and health of patients, as is appropriate. Nevertheless, the impact on caregivers should also be recognized since these are the individuals who manage patients’ health on a daily basis. Caregivers often have limited time and energy to spend on their own physical and emotional needs, which can hinder their ability to work, accomplish daily tasks at home, participate in social activities, and maintain personal relationships. Disengaging from such activities and relationships can further diminish caregivers’ mental health and well-being.
Given the potential consequences of caregiver burden, providing appropriate resources may be an important part of the overall therapeutic strategy. Potential resources include the “Talk About TD” website (https://www.talkabouttd.com), the National Alliance on Mental Illness (https://www.nami.org), and the Caregiver Action Network (https://caregiveraction.org). For caregivers who need emotional support, psychoeducation may be a useful option (Baruch et al., 2018; Yesufu-Udechuku et al., 2015). Various coping strategies have been described in the psychiatric literature, including proactive, problem-focused, and adaptive-cognitive approaches (Grover et al., 2015; van der Sanden et al., 2016). In caregivers of patients with Alzheimer’s disease, emotion-focused coping strategies were more likely to be effective than problem-focused strategies in managing anxiety and depressive symptoms (Cooper et al., 2008; Monteiro et al., 2018). On a more practical level, contact information for local counselors, peer support groups, and respite care services can be provided.
RE-KINECT only represents the beginning of what needs to be done to understand and serve the needs of patients and their caregivers. The study’s limitations should be noted, but these limitations may also drive future research. First, as described earlier, the questionnaire could not be designed to evaluate every aspect of the caregiving experience. Moving forward, TD-related studies could incorporate caregiver-related items that address some of the questions raised in this study, such as why some caregivers did not notice abnormal involuntary movements or perhaps felt they were “just part of the condition.” Other studies could focus on validating existing caregiver assessments that might be appropriate for TD (e.g., Zarit Burden Interview or Family Burden Interview). Although this is the largest study of its kind, it was limited by the relatively small sample size. Of the 78 possible caregivers, 41 of the 45 qualified caregivers (unpaid nonprofessional who knew the patient well) completed the questionnaire and were included for analysis. Caregivers were not asked why they did not want to participate, but future studies could include questions that might provide possible reasons for nonparticipation (e.g., too busy, not interested, concerned about privacy, embarrassed or worried about stigmatization).
The final major limitation is the lack of a control group, which was due to the difficulty of identifying a meaningful control group. First, it should be noted that the objective of the caregiver questionnaire was to focus on the impact of possible TD symptoms on patients (per caregiver impressions) and on caregivers themselves. Second, questions regarding the impact of abnormal involuntary movements for caregivers of patients who did not have possible TD would not provide meaningful data. If the questionnaire had been focused on the impact of patients’ psychiatric and medical conditions, the inclusion of a control group would have been valuable. Nonetheless, it is acknowledged that the lack of a control group makes it difficult to characterize the degree to which possible TD might have contributed to the existing burden of caring for patients who already have one or more psychiatric disorders—and in many cases, chronic or serious comorbid medical conditions.
Additional research could focus on the following: types of patients who require caregivers (e.g., older patients, those with more severe psychiatric illness and/or TD, those with longer TD duration), kind of caregiving they receive (e.g., informal/unpaid, paid in-home care, institutional care), potential contributing factors to caregiving decisions (e.g., availability of family or friends, socioeconomic status of patients), and factors that may increase caregiver burden (e.g., family member vs. friend, type of familial relationship [spouse, parent, child, sibling], employed vs. retired). More specific information about how patients’ conditions (e.g., TD and other drug-induced movement disorders, psychiatric disorders, comorbid medical conditions) affect caregivers could also be explored. How long do caregivers assist in helping with these conditions? Which ones require the most time and why? Another area of interest would be the long-term effects on caregivers. Since TD usually persists, does the burden on caregivers increase over time? How long have caregivers provided assistance to their family or friends with TD? Are there cumulative effects on their physical health, mental health, or quality of life? Does the knowledge that TD may be irreversible affect how caregivers perceive their roles and their outlooks for the future? Would effective treatment and suppression of TD significantly ameliorate caregiver burden? In addition, the issues of stigmatization and embarrassment among caregivers should not be overlooked. Caregivers who feel ashamed or confused about sharing their experiences with others may become isolated or depressed (Bauer et al., 2012; Caqueo-Urizar et al., 2009; Perlick et al., 2007). Finally, assessing the financial costs of caring for patients with possible TD movements is imperative. This includes personal costs (e.g., expenses incurred by caregivers, lost income), health insurance costs (e.g., copays for clinic visits and medications, including approved TD medications), and social costs (e.g., health care utilization, decreased workplace productivity).
Conclusions
The primary conclusions of this study are twofold. First, the potential impact of TD on caregivers is substantial and should not be overlooked. Acknowledging this burden and providing appropriate resources are also recommended. Second, caregivers can be a valuable resource to clinicians for assessing the presence and severity of TD and subsequent impact on patients, as indicated by the significant correlations between caregiver and patient ratings of possible TD in this study. Health care providers should consider a comprehensive therapeutic approach that incorporates caregivers’ input. The questions raised by some of the limitations of this study indicate that more research is needed to understand how TD affects the physical health, mental well-being, quality of life, and financial resources of caregivers.
Supplemental Material
sj-pdf-1-jap-10.1177_10783903211023565 – Supplemental material for Caregiver-Reported Burden in RE-KINECT: Data From a Prospective Real-World Tardive Dyskinesia Screening Study
Supplemental material, sj-pdf-1-jap-10.1177_10783903211023565 for Caregiver-Reported Burden in RE-KINECT: Data From a Prospective Real-World Tardive Dyskinesia Screening Study by Andrew J. Cutler, Stanley N. Caroff, Caroline M. Tanner, Huda Shalhoub, William R. Lenderking, Véronique Pagé, Ericha Franey and Chuck Yonan in Journal of the American Psychiatric Nurses Association
Footnotes
Acknowledgements
Medical writing and editorial assistance was provided by Mildred Bahn at Prescott Medical Communications Group (Chicago, IL) with support from Neurocrine Biosciences, Inc.
Author Roles
All authors contributed to the conception or design of the study or to the acquisition, analysis, or interpretation of the data. All authors drafted the manuscript, or critically revised the manuscript, and gave final approval of the version that was submitted for publication. All authors agree to be accountable for all aspects of the work, ensuring integrity and accuracy.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Cutler has served as a consultant to, received research grants from, and is on the speaker bureau for ACADIA, Avanir, Neurocrine Biosciences, Inc., Otsuka, and Teva Pharmaceuticals; is a consultant to MedAvante-Prophase; and is on the Board of the Neuroscience Research Institute. Dr. Caroff has served as a consultant to Neurocrine Biosciences, Inc.; Teva Pharmaceuticals Industries, Ltd.; Osmotica Pharmaceuticals, and Dispersol Technologies, and received separate research grants from Neurocrine Biosciences, Inc.; Osmotica Pharmaceuticals; and Eagle Pharmaceuticals. Dr. Tanner has received grants from the Michael J. Fox Foundation; the Parkinson’s Foundation; the Department of Defense; BioElectron; Roche/Genentech; Biogen; Gateway, LLC; and the National Institutes of Health, has received compensation for serving on data monitoring committees from Biotie Therapeutics, Voyager Therapeutics, Cadent Therapeutics, and Intec Pharma, and personal fees for consulting from Neurocrine Biosciences, Adamas Therapeutics, Biogen, 23andMe, Alexza, Grey Matter, Acadia, Acorda, Amneal, and CNS Ratings. Dr. Shalhoub, Dr. Lenderking, and Véronique Pagé are former/current full-time employees of Evidera and served as consultants on this work. Dr. Yonan and Dr. Franey are full-time employees of Neurocrine Biosciences, Inc.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Neurocrine Biosciences, Inc. (San Diego, CA).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.