
Abstract
In 2019, an estimated 5.8 million Americans older than 65 years had Alzheimer’s disease (AD), the most common form of dementia (Alzheimer’s Association, 2019). This number is projected to nearly triple to 14 million by 2050 as the baby boom generation reaches and exceeds age 65. Based on these numbers, every 33 seconds someone will develop AD. The significance of these projections cannot be underestimated, making dementia caregiving a public health priority, if not an impending crisis, in the United States. This is particularly germane to older women (>65 years), who are more likely to provide dementia care for a husband than vice versa. Previous research has identified consistent themes around the adverse impact of dementia caregiving during the caregiving experience; however, there is limited research exploring the ongoing impact of spousal caregiving during the transition to widowhood. Yet what we do know is sobering: Recently widowed caregivers have increased mortality, increased health risks and chronic conditions, decreased income, and social instability.
Review of Literature
The typical caregiver is a 79-year-old female spouse providing 34 hours of care a week for the past 5 years to a 77-year-old male spouse with AD, “old age,” or heart disease. Nearly half of these caregivers report high levels of emotional and financial strain in care provision (National Alliance for Caregiving & the AARP Public Policy Institute, 2015). AD, the most common form of dementia, is a slow, progressive, incurable, and fatal disease that affects one in three older adults, and no one is immune (Alzheimer’s Association, 2019). It is the sixth leading cause of death in the United States (Karmarow & Tejada-Vers, 2019). Five million Americans have AD, and 15 million unpaid caregivers (spouses, adult children, relatives, friends) provide the care they need (Alzheimer’s Association, 2019). The majority of care occurs at home, and care recipients require progressively more care in all activities of daily living over time, such as help with dressing, bathing, feeding, and toileting (Alzheimer’s Association, 2019).
While much is known about dementia caregiving, much less is known about the caregiver when caregiving ends. However, the evidence suggests there is a connection between the caregiving experience and how one transitions into widowhood (Aneshensel et al., 2004; Boerner et al., 2004; Burton et al., 2006; Corey & McCurry, 2017; Keene & Prokos, 2008; Schulz et al., 2001; Schulz et al., 2008). First, if financial strain was present during the caregiving experience, it is likely to continue into widowhood (Keene & Prokos, 2008). The estimated cost of caring for a patient with dementia at home is uncovered $5,000 each year, and dementia is considered the most expensive health condition in the United States (Alzheimer’s Association, 2019). This can lead to financial instability and financial insecurity as widows deal with health conditions of their own (Keene & Prokos, 2008). Second, poorer outcomes experienced during caregiving such as high caregiver burden, depression, anxiety, exhaustion, and social isolation tend to remain and predict poorer transition into widowhood (Schulz et al., 2008). Sleep disturbances have been identified to persist for up to 10 years among family caregivers caring for family members with dementia (Corey & McCurry, 2017). Third, the lack of social engagement due to the demands in caregiving leads to ongoing social isolation into widowhood (Burton et al., 2006). And fourth, as spousal caregivers have been known to ignore their own health needs during the caregiving years (DiGiacomo et al., 2013), their risks are higher for worsening health as they transition into widowhood. Thus, assessing the caregiving experience is important as it may provide insight into the transition experience.
Overall, widows tend to be most at risk for health issues in the 2-year period following the spouse’s death. There is evidence that older women who cared for persons with dementia need support. Aneshensel et al. (2004) examined 291 family dementia caregivers of which 37% were older spouses. Those who remained repeatedly distressed into widowhood were female, older, and those who had provided caregiving the longest (M = 5.7 years). The factors found to correlate with less distress postbereavement were higher education and income and feeling emotionally cared for by others. They concluded that depressive symptoms were highest during the first year following bereavement, dropped substantially during the second year, and remained about the same in Year 3. Haley et al. (2008) examined for depression in 254 dementia spousal caregivers over 1 to 2 years following the care recipient’s death. Some had received a caregiver support intervention during caregiving, which led to lower levels of depressive symptoms in the postbereavement period, suggesting the benefits of this added support. Schulz et al. (2006) found in a study of 217 caregivers (84% female; 50% spouses) that 20% of caregivers remained substantially at risk with high levels of depression in the postbereavement period, suggesting that for some, support is critical. Furthermore, even when caregivers reported a positive caregiving experience, they were more likely to have high levels of depression and grief postloss. This suggests that being a dementia caregiver for long periods of time and providing high levels of care might cause more issues in the transition period when one is no longer a caregiver. However, Burton et al. (2006) examined 204 older spouse caregivers pre- and postloss over an 18 months period and found no association between the caregiving experience and the variables of depression, well-being, or self-esteem postloss unless the caregiver was highly stressed during the caregiving experience. According to Burton et al. (2006) and Haley et al. (2008), these highly stressed caregivers also had greater difficulties reengaging in social activities, which might place them at higher risk for even greater social isolation.
One study conducted on 21 older female spouse caregivers used a mixed-methods, longitudinal design examining the transition to widowhood over a 1-year period (DiGiacomo et al., 2013). Of these women, 81% were caregivers for their husbands for a mean average of 3 years. Only 29% of the care recipients/husbands were living at home at the time of death. The participants were assessed with surveys and in-depth semistructured interviews at three points over 12 months. The metrics included demographics, health care resource utilization, depression, anxiety, stress, and grief. The qualitative interviews assessed for their perceptions of the caregiving experience and transition into widowhood. Interviews lasted approximately 1 to 3 hours each. There were no significant changes in depression, anxiety, and stress over the 12-month time frame. However, the qualitative data yielded different and important results. The women reported that their caregiving experiences were stressful, they ignored their own health needs, and they complained about gaps in communication with health care providers except for those associated with palliative and hospice care services. Many had chronic conditions of their own that affected activities of daily living, physical pain that presented challenges, fear and anxiety of being alone, and ongoing difficulties handling financial matters. These women also experienced health-related events, including falls, new health conditions, and exacerbations of chronic conditions, over the 12 months. Overall, DiGiacomo et al. concluded that the needs of these older female widows went largely unmet and resulted in high usage of emergency services and unplanned hospitalizations. This study’s contribution to the postcaregiving literature stresses the importance of assessing both health-related information and health care resource utilization during the transitional period to better understand the barriers and gaps in care.
An integrative review on dementia caregivers’ grief and bereavement postdeath retrieved 19 publications from 1994 to 2014 (Arruda & Paun, 2017). The authors concluded that evidence was consistent across many studies that the grief and bereavement of dementia caregivers are unique and often problematic when compared with the experiences of other chronic disease caregivers because of the prolonged caregiving demands, the progressive course of the illness, the reduced likelihood of receiving hospice services, and the eventual need for long-term care placement prior to death (p. 844). Arruda and Paun further point out that dementia caregiver grief is problematic because it is associated with a variety of physical and emotional health factors (e.g., chronic health conditions, immunological compromise, depressive symptoms, increased stress, shock, anxiety, guilt, longing, and loneliness).
The preponderance of research related to spousal caregiving has focused on urban populations, with less known about the challenges of providing appropriate dementia care in rural areas. Rural caregiving is understudied (Sanford & Townsend-Rocchiccioli, 2004) and constitutes a significant gap in the caregiver literature since rural caregiving comprises as much as 28% of all caregiving (National Alliance for Caregiving & the AARP Public Policy Institute, 2015). This is even more important considering the persistent rural–urban disparity in dementia: Rates of dementia in rural areas are higher than in urban areas (5% vs. 4.4%, respectively), although this gap has narrowed in recent years (Weden et al., 2018).
Two research studies and one systematic review comparing differences between rural and urban caregivers were reviewed. The two single studies concluded that rural caregivers had access to fewer formal supports but did not report greater burden, poorer health status, or fewer health behaviors than urban caregivers (Bedard et al., 2004) and that rural caregivers experienced higher negative financial impact but reported more family support (Ehrlich et al., 2014). The systematic review (McKenzie et al., 2010) critiqued eight studies and reported few statistically significant differences between urban and rural caregivers of elderly people in the community. Two major issues with the single studies and systematic review include mixed samples of caregivers (e.g., spouse, child, friend) and neither single study and only four of the eight studies critiqued in the systematic review were conducted in the United States. These six studies were conducted in Australia, Canada, South Korea, Sweden, and Poland.
Evidence suggests that older rural adults in general are more likely to live in poverty, have more chronic conditions, report lower level of activities of daily living function, and experience more memory problems and feelings of depression compared to older urban adults (Gerrior et al., n.d.; Longman et al., 2012). Moreover, persons living in rural areas have higher unemployment rates, are less likely to have high-speed internet to access health information, have greater transportation issues getting to a health care provider, and have decreased access to health care providers and facilities than persons living in urban area (National Rural Health Association, 2017). Given these facts, it can be anticipated that some of the issues for rural caregivers may be different, and the transition from caregiving to widowhood may be more nuanced because of these health and socioeconomic factors.
Based on the review of literature and the identified gaps in knowledge, the objectives of this study were to compare differences between older rural and urban female spousal caregivers on (1) the physical and mental health factors affecting the transition from dementia caregiving to widowhood and (2) the resources that older women utilize during the transition from dementia caregiving to widowhood over 12 months.
Conceptual Framework
The conceptual framework that guided this study was transition theory (Meleis, 2010). Transition is a process triggered by a change, characterized by different dynamic stages, milestones, and turning points. Integral to transition theory are the concepts of role insufficiency and role supplementation (Meleis, 1975). Meleis (1975) defined role insufficiency as “any difficulty in the cognizance and/or performance of a role or the sentiments and goals associated with role behavior as perceived by self or by significant others” (p. 265), whereas role supplementation is “a deliberate process that included conveying information or providing experience for the role incumbent to become aware of the anticipated role behaviors and goals, as well as the interrelationships between the new role and the roles of others” (p. 267). The relevance of transition theory and role insufficiency/supplementation with caregivers is that when a role is central to one’s identity (caregiver), involuntary role exit (death of husband) may be an especially stressful life disruption (Figure 1).
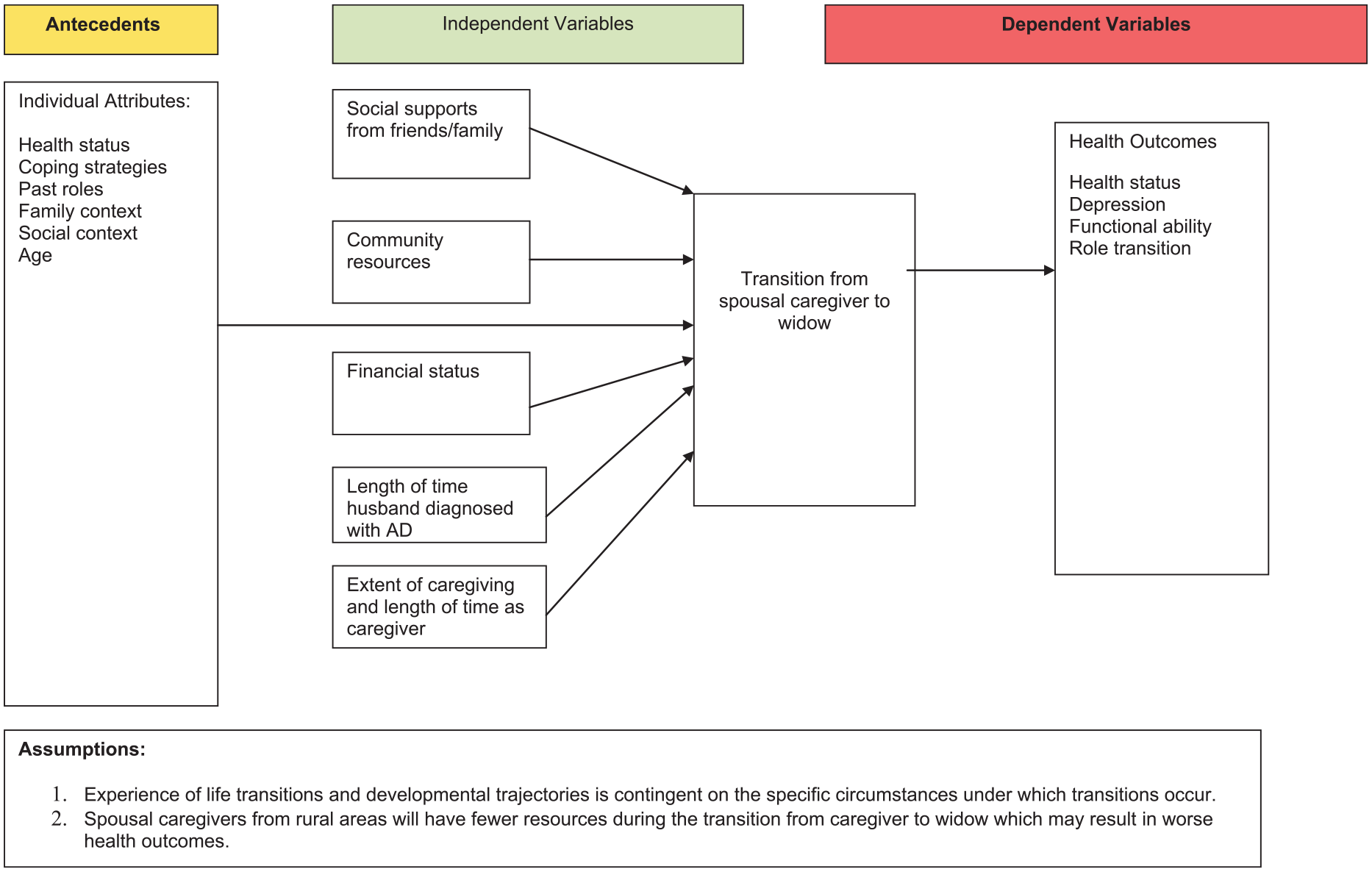
Conceptual model.
Method
Design, Sample, and Setting
The study utilized a longitudinal nonexperimental mixed-methods design (52 weeks) to analyze, compare, and explain the factors associated with the transition of spousal dementia caregiving to early widowhood between rural and urban female spousal caregivers. The results of the qualitative findings are reported elsewhere (Saunders & Groh, 2019). Data were collected at three points: baseline, 6 months, and 12 months. The data collection period spanned from August 2017 to December 2018. Demographic data were collected at baseline; whereas mental health data (the 12-item Medical Outcomes Study–Short Form Health Survey Version 2 [SF-12v2] and Center for Epidemiologic Studies Depression Scale [CESD]), physical health status (SF-12v2), current health and living arrangements, and resources utilized were collected at all three points.
The participant inclusion criteria were as follows: (1) female, widowed, >65 years of age, and caregivers of husbands diagnosed with AD or another form of dementia; (2) husband died in the past 3 years; (3) English speaking; and (4) Mini-Mental State Exam (MMSE) score >24. Thirteen urban and nine rural women met criteria for the study. Participation rate for the length of the study was 100%.
Study Instruments
There were three major outcome variables in this study: physical functioning, mental functioning, and depression.
The Medical Outcomes Study–Short Form Health Survey Version 2 (Ware et al., 2002)
The SF-12v2, a standardized measure of health and well-being, contains 12 items from the SF-36 (Short Form–36 Health Survey) and takes 2 to 3 minutes to complete. The SF-12v2 includes the same eight subscales of the SF-36: physical functioning (PF), role limitations due to physical restrictions (RP), bodily pain (BP), general health (GH), vitality (VT), role limitation due to emotional issues (RE), mental health (MH), and social functioning (SF). It has demonstrated usefulness in surveys of general and specific populations and has compared the relative burden of diseases in differentiating the health benefits produced by a wide range of different treatments (Ware et al., 2007). The SF-12 has been used with older adult populations (Courtney et al., 2009; DiGiacomo et al., 2013; Wells, 2010).
The SF-12v2 includes two summary scores, a Physical Component Summary (PCS) and a Mental Component Summary (MCS). The PCS of the SF-12v2 comprises four subscales: PF, RP, BP, and GH. The MCS also comprised four subscales: VT, SF, RE, and MH (see Table 1 for definition of terms and number of items). Each subscale’s score can range from 0 to 100, with higher scores always reflecting better function. The subscales are weighted and summed to calculate the physical and mental component summary scores, which are standardized to a mean of 50 and standard deviation of 10, with scores above or below representing better or worse status than the U.S. population average. In 25 studies, most reliability statistics were reported to exceed .80 (Ware et al., 2007). Validity was also confirmed in these 25 studies by multiple measures (Ware et al., 2007). In the present study, the SF-12v2 was administered at baseline, 6 months, and 12 months. The PCS and MSC scores in this study were compared to the nationally representative values for noninstitutionalized females 70 to 79 years (Hanmer & Kaplan, 2016).
Definition of SF-12v2 Mental and Physical Component Domains.
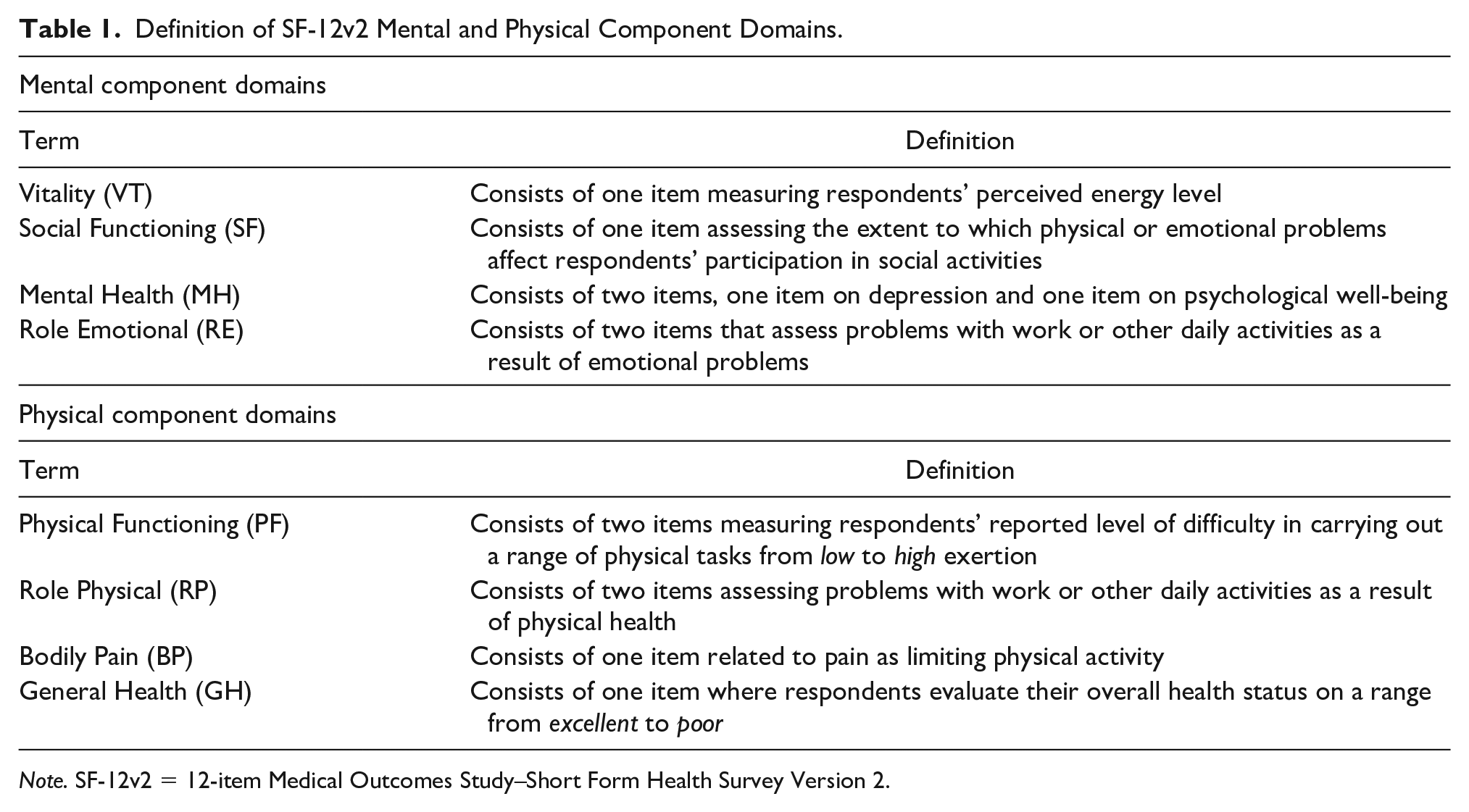
Note. SF-12v2 = 12-item Medical Outcomes Study–Short Form Health Survey Version 2.
Center for Epidemiologic Studies Depression Scale (Radloff, 1977)
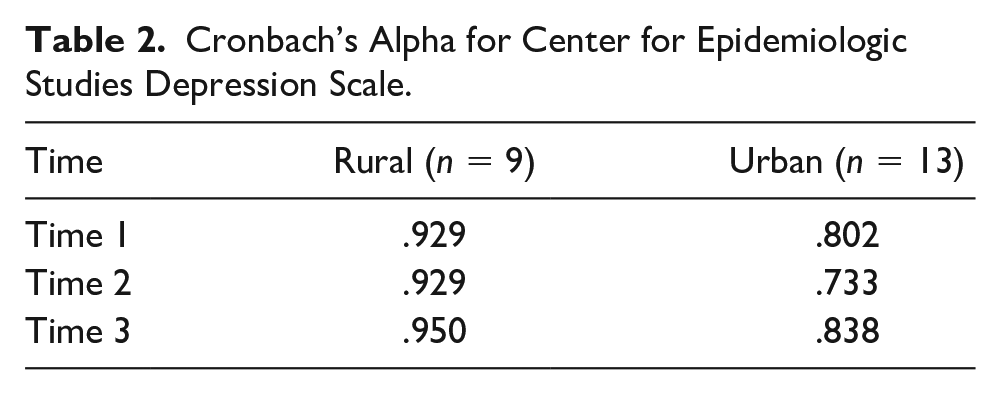
The CESD is a 20 item self-report depression scale that has been used in studies to assess the transition during caregivers’ postcaregiving (Boerner et al., 2004; Burton et al., 2006; Keene & Prokos, 2008; Schulz et al., 2001; Schulz et al., 2006). The tool is scored on a 4-point scale with a range of 0 to 60; a score of 16 or more is considered depressed. The CESD was administered at baseline, 6 months, and 12 months. Cronbach’s alphas were acceptable at the three data collection points (>.07), indicating that the CESD achieved internal consistency for the sample in this study (Table 2).
Cronbach’s Alpha for Center for Epidemiologic Studies Depression Scale.
Demographic data (age, education, income, years married, time since husband’s death) were collected at baseline. In addition, responses to caregiver-specific questions (length of time caregiving, type of care provided, resources used during caregiving), health questions (medical diagnosis, medications, changes in health), and social questions (contact with family/friends, extent they felt cared for) were collected at baseline as well as at 6 and 12 months.
Procedures and Data Collection
Recruitment strategies included telephone and email communications with caregiver and grief support group leaders, clergy, health care providers, social workers, and faculty/staff at various universities/colleges in the targeted areas, advertisements in church bulletins, flyers posted in libraries, hair salons, community centers and medical clinics, face-to-face meetings, and telephone communications with leaders of the local chapters of the Alzheimer’s Association. Recruitment efforts lasted 6 months with the data collection period spanning from August 2017 to January 2018. Interested participants contacted the researchers via phone or email. The researchers contacted those interested, explained the study in more detail, and reviewed the objectives and expectations and their commitment to the 12-month project. For those who met inclusion criteria and wanted to proceed, an appointment was scheduled for the baseline interview and to obtain written informed consent. The MMSE was also administered at the baseline interview to ensure competency of the caregiver and validity of responses. Only one spousal caregiver was excluded for an MMSE score <24. All of the interviews were conducted in the participants’ home except for one who preferred her church. Once the baseline interview was completed, the 6-month interview was scheduled with the 12-month interview scheduled at the completion of the 6-month interview. Participants were given a $35 gift card at the completion of the baseline and 6-month interviews and a $40 gift card at the completion of the 12-month interview.
The interviews lasted between 1 and 3 hours and included both structured surveys (e.g., SF-12v2, CESD and update on their health status) and semistructured interview questions that were tape recorded and transcribed (reported elsewhere). At the baseline interview, questions asked pertained to their caregiving experience (length of time as caregiver, hours of caregiving each day), health questions (health events in the past 6 months, health and community services used, current medications, pain) and social engagement (number of times in contact with family/friends, how many times they left the house, how cared for by others they felt). These questions were repeated at the 6- and 12-month interviews except for those related to the caregiving experience.
Missing Data
The interviews and completion of the SF-12v2 and CESD at the three data collection points were conducted in person; thus, there were no missing data. The only exception was income, with two rural participants declining to answer that question.
Statistical Analyses
SF-12v2 data were entered into QualityMetric™ software, scores calculated, and then downloaded into SPSS. All data were analyzed using IBM SPSS Version 22. Basic descriptive statistics were performed on all study variables. Independent-samples t test and chi-square were conducted to compare differences between rural and urban caregivers on interval and categorical level data at baseline. Repeated analysis of variance was used to explain differences among pertinent participant characteristics, depression, mental, and physical functioning at the three data collection points. Statistical significance was set a priori at p < .05.
Ethical Statement
Institutional review board approval was obtained from the University, and all participants signed informed consent prior to the baseline interview and assent was given at the 6- and 12-month interviews.
Results
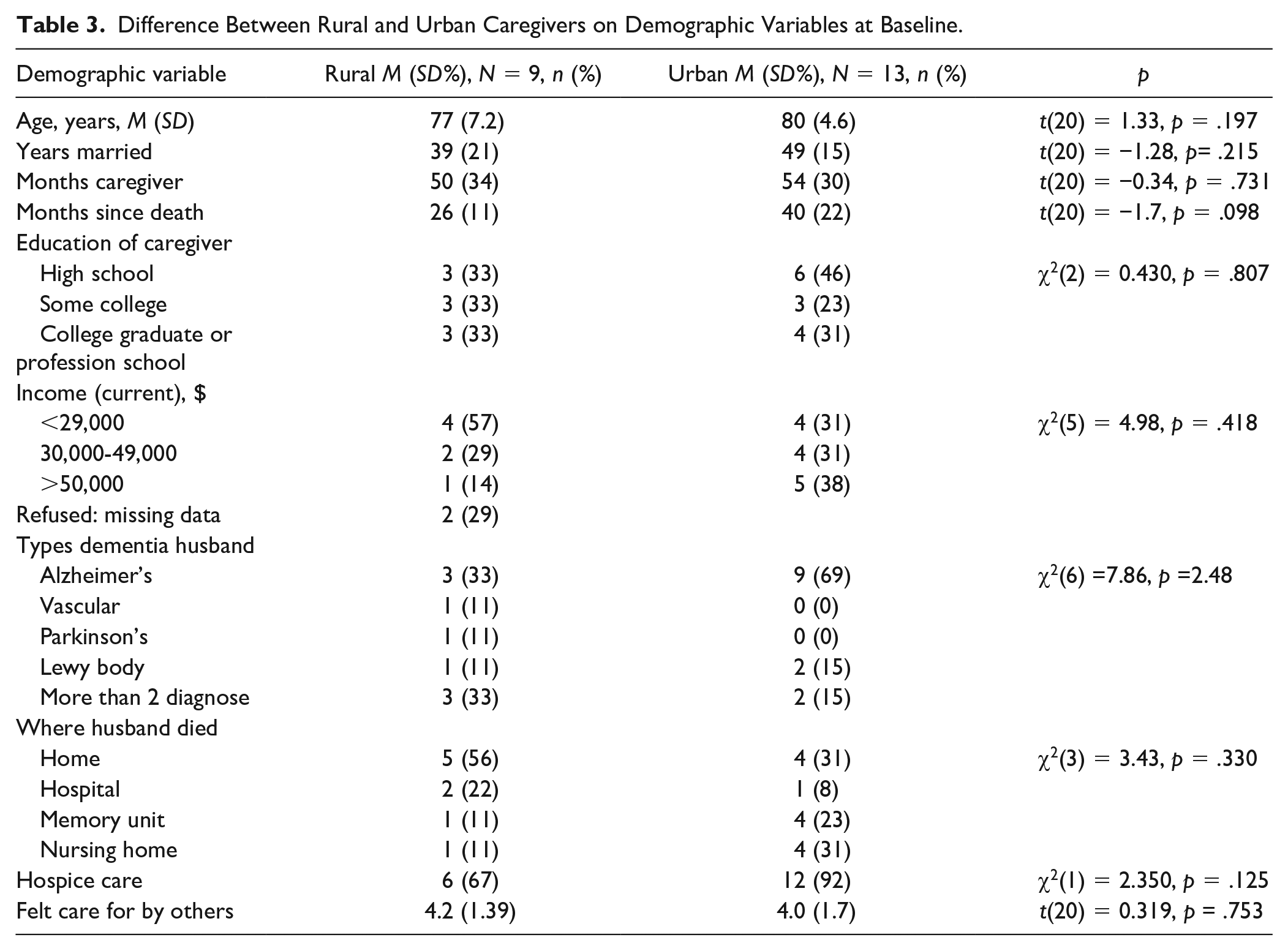
Nine rural and 13 urban caregivers completed the longitudinal (12 months; 3 data collection points) transition from caregiver to widowhood study. There was no attrition in either group. To determine if there were differences between the rural and urban caregivers on demographic variables at baseline, an independent-samples t test was conducted for interval-level data (e.g., age, years married, years as caregiver, time since husband’s death, MCS, PCS, and CESD), and chi square for categorical data (e.g., education, income level, type of dementia diagnosis, where husband died, and hospice care). No statistically significant differences were detected between the rural and urban caregivers at baseline (Tables 3 and 4).
Difference Between Rural and Urban Caregivers on Demographic Variables at Baseline.
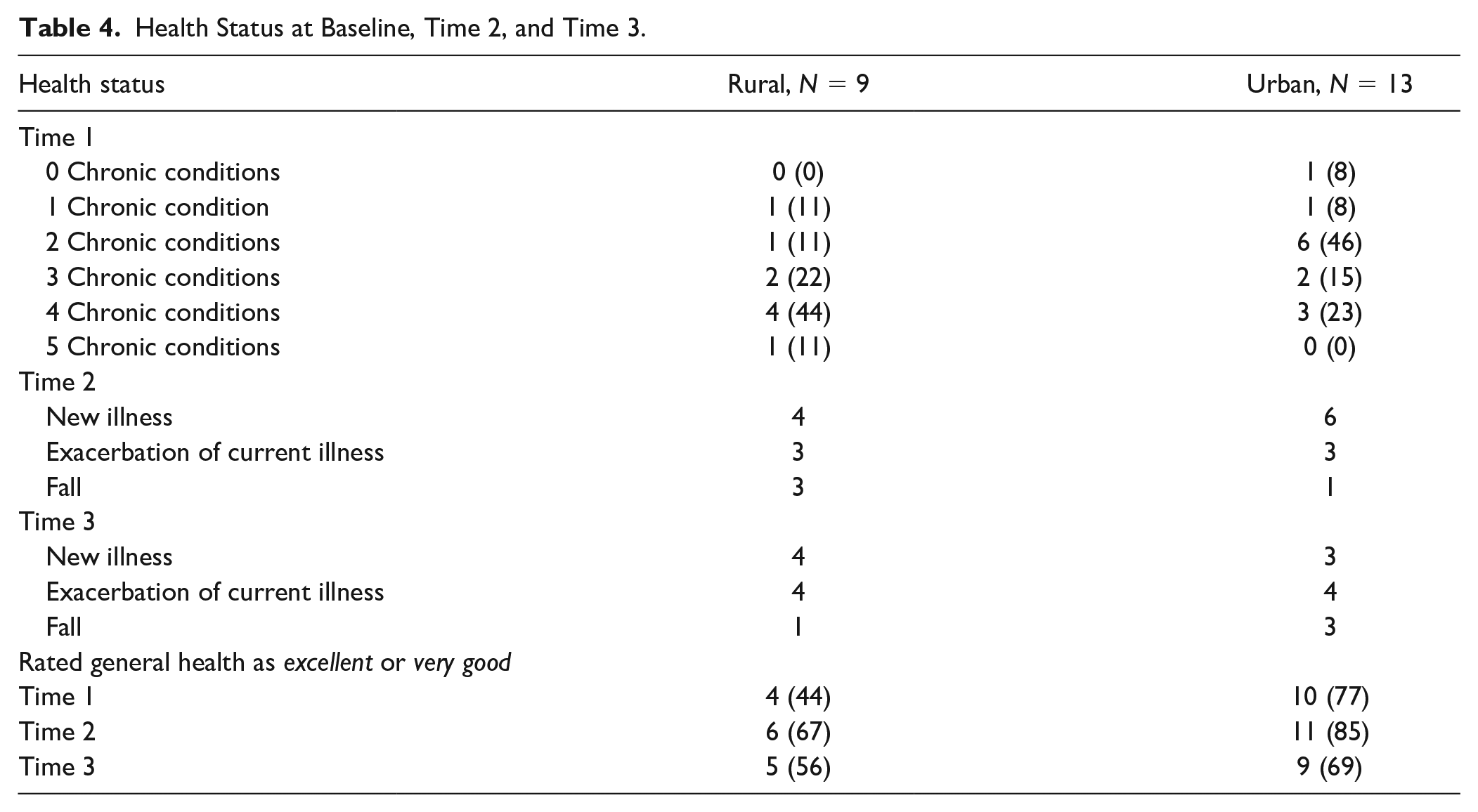
Health Status at Baseline, Time 2, and Time 3.
Depression (CESD) and Short-Form Health Survey (SF-12v2)
In order to answer the first research question, repeated measures analyses of variance were conducted to compare differences between rural and urban caregivers on the dependent variables of depression and the MCS and PCS of the SF-12v2 by time and geographical location. For depression (measured using the CESD), Mauchly’s test indicated that the assumption of sphericity was met, χ2(2) = .646, p = .724); therefore, sphericity was assumed. As shown in Table 5, the mean depression score for rural women was higher at baseline compared to urban caregivers (13.5 vs. 9.4), increased at Time 2 for rural caregivers but decreased for urban caregivers (15.1 vs. 6.7), and at Time 3, decreased for both rural and urban caregivers (12.1 vs. 6.0). However, the differences between rural and urban spousal caregivers were not statistically significant across the three data collection points (group × time F[2, 40] = 1.567, p = .221). Neither of the main effects were significant, groups F(1, 40) = 2.407, p = .136; time F(2, 40) = 2.289, p = .115.
Difference Between Rural and Urban Caregivers on Physical and Emotional Factors Over Three Data Collection Points.
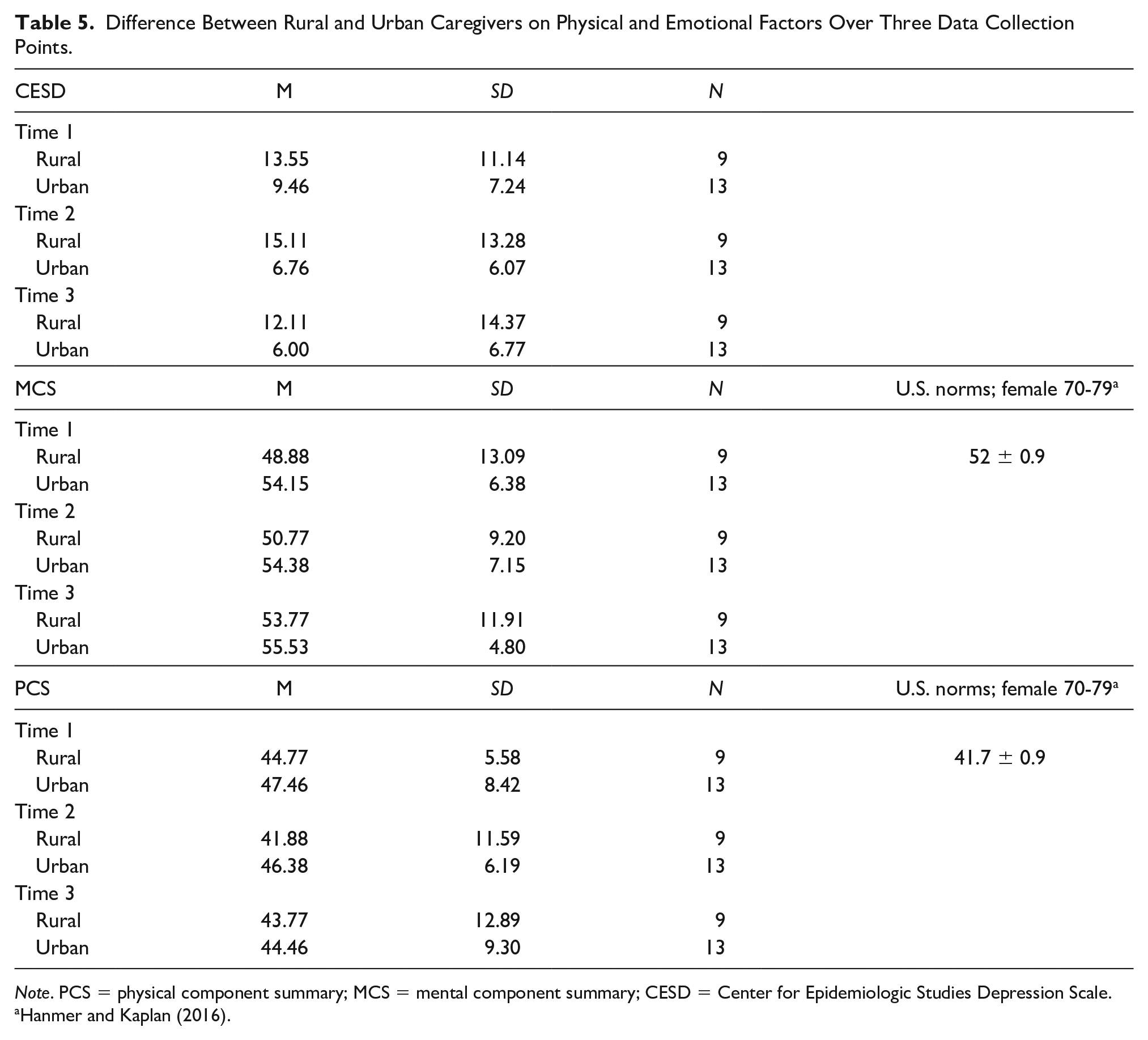
Note. PCS = physical component summary; MCS = mental component summary; CESD = Center for Epidemiologic Studies Depression Scale.
For the MCS, Mauchly’s test indicated that the assumption of sphericity was met, χ2(2) =2.484, p = .289; therefore, sphericity was assumed. As shown in Table 5, the MCS in this study was lower at baseline for rural versus urban caregivers (48.88 vs. 54.15) and increased at Time 2 for both rural and urban caregivers (50.77 vs. 54.38) as well as at time 3 (53.77 vs. 55.53) although rural caregivers scored lower than urban caregivers at all three points. However, these differences were not statistically significant, group × time F(2, 40) = .343, p = .712. Neither of the main effects were significant, groups F(1, 40) = 1.508, p = .234; Time F(2, 40) = 1.136, p = .331.
For the PCS, Mauchly’s test indicated that the assumption of sphericity was met,χ2(2) = .660, p = .719); therefore, sphericity was assumed. As shown in Table 5, the PCS in this study was lower for rural caregivers compared to urban caregivers across all three data collection periods; however, the PCS increased for both groups at Time 2 and Time 3. The differences between rural and urban women across the three data collection points were not statistically significant, group × time F(2, 40) = .475, p = .626. Neither of the main effects were significant, groups F(1, 40) = .649, p = .430; Time F(2, 40) = .690, p = .507.
Health Status
In addition to PCS scores, the participants reported on their health status at the three data collection points and rated their general health on a scale of 1 (excellent) to 5 (poor). As noted in Table 3, the vast majority of rural and urban spousal caregivers reported at least one chronic health condition at baseline. Hypertension was the most common for both rural (n = 8) and urban (n = 12) women, followed by myriad other chronic conditions: hypercholesteremic, diabetes, chronic obstructive pulmonary disease, arthritis, chronic pain, hypothyroidism, asthma, sleep apnea, multiple sclerosis, compression fracture, polymyositis, and fibromyalgia. The number of new illnesses, exacerbation of current conditions, or experiencing a fall was common for both rural and urban caregivers at Time 2 and Time 3 (Table 4). In terms of general health, the majority of both rural and urban caregiver rated their health as either excellent or very good across all three collection points (except for rural caregivers at baseline, 44%; Table 4).
Health Care Resources
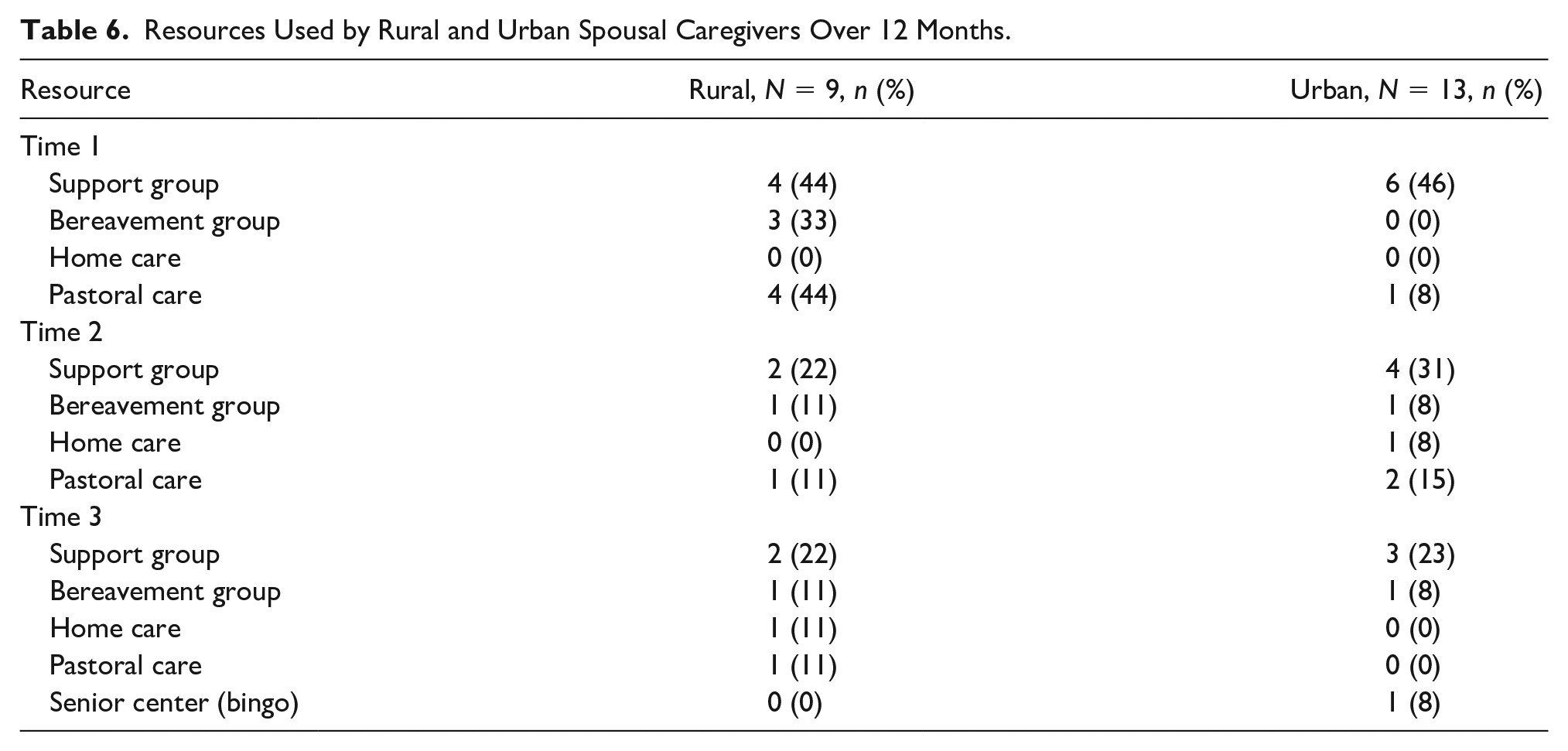
To answer the second research question, a frequency table of resources that the women utilized during the transition from dementia caregiving to widowhood over 12 months was constructed and differences between rural and urban caregivers noted. The most common community resource utilized by rural and urban caregivers was support groups (e.g., Hospice, Alzheimer’s Association, and Area Agency on Aging) across the three data collection points although the number of women who attended the support groups decreased with each collection point. In addition to support groups, pastoral support and bereavement groups were used more by rural women compared to urban women at Time 1. At Time 2, pastoral support was the most frequent resource used following support groups, but the number of women who utilized pastoral support was small in both groups. By Time 3, the type of community resources changed to include home care as well as senior centers (Table 6).
Resources Used by Rural and Urban Spousal Caregivers Over 12 Months.
Social Support
Most of the spousal caregivers reported feeling “cared for by others” at all three data collection points. The scale ranged from 1 (very little) to 5 (very much). The mean score at baseline for rural caregivers was 4.2 and for urban caregivers 4.0. At Time 2, the mean score was the same for rural caregivers but decreased for urban caregivers (3.38); then at Time 3 decreased for rural (4.0) but increased for urban caregivers (4.7).
Discussion
The objectives of this study were to determine if there were differences between older rural and urban female spousal caregivers on physical and mental factors affecting the transition from caregiver to widowhood, and the resources utilized during this transition.
We report three main findings. First, the mean scores on the PCS of the SF-12v2 were higher for both rural and urban women at all three collection points (Table 4) compared to the reported nationally representative values for noninstitutionalized adult women aged 70 to 79 (M = 41.7 ± 3; Hanmer & Kaplan, 2016), despite the significant number of chronic health conditions reported at baseline (Table 6). Moreover, the majority of rural and urban participants rated their general health as either excellent or very good across the three collection points. These findings are inconsistent with other studies investigating the impact of dementia caregiving on physical health. For example, Givens et al. (2011) reported that the death of a family member diagnosed with dementia was associated with increased risk for both physical and emotional health impairments in their caregivers. In a study on dementia caregiving (National Alliance for Caregiving & the Alzheimer’s Association, 2017), it was reported that dementia caregivers are nearly twice as likely to say that their health has gotten worse as a result of their caregiving responsibilities. Moreover, one in three dementia caregivers say their health has declined (35%), versus just one in five nondementia caregivers. A 2017 national poll on healthy aging conducted by the University of Michigan reported that 27% of dementia caregivers delayed or did not do things they should for their own health and 66% said caregiving interfered with their ability to take care of themselves or their daily activities (healthyagingpoll.org).
Two possible explanations for these differences are proposed. First, there is a paucity of longitudinal data investigating the impact of spousal caregiving on physical health postdeath and few have used the SF-12v2 to measure physical health/functioning. The majority of research on the physical consequences of caregiving has focused on caregivers during active caregiving whereas, research on the consequences of spousal caregiving postbereavement have tended to focus on the emotional impact (Aneshensel et al., 2004; Arruda & Paun, 2017; DiGiacomo et al., 2013; Haley et al., 2008; Schulz et al., 2006; Stahl & Schulz, 2019). Only one longitudinal study, to our knowledge, has explored health-related events over 12 months (DiGiacomo et al., 2013) using the SF-12v1. In their study (N = 21, X age 71), the mean PCS scores were also higher than the national norms of 41.7 (±3) for females 70 to 79. They reported PCS scores of 46.61 (Time 1), 45.76 (Time 2), and, 47.07 (Time 3). DiGiacomo et al.’s (2013) results were similar to the findings reported in this study despite their sample being younger and using benchmarks established for Australian, where the study was conducted.
An alternative explanation may be length of time since the husband’s death and participation in this study. For example, time from death at baseline for rural spousal caregivers was 2.2 years (26 months) and for urban women 3.4 years (40 months). It has been hypothesized that the greatest impact of caregiving on physical health is within the first 2 years postdeath. This explanation is partially supported by the findings of DiGiacomo et al. (2013). The women who participated in their study were 14.29 months postdeath at baseline and 25.8 months at the third interview. Even though the spousal caregivers in DiGiacomo et al. study were interviewed closer in time to their husbands’ death, the differences in PCS scores between their participants and the participants in our study are relatively minor. It will be important for future longitudinal studies to recruit spousal caregivers earlier in the bereavement process, or even during the active caregiving, so that the trajectory of physical health recovery can be more fully understood postdeath.
The second main finding for discussion was the emotional impact of spousal caregiving in the postbereavement transition period. Neither were the majority of spousal caregivers in this study depressed based on CESD scores nor were there any statistically significant changes in depression scores detected over the 12 months study period either within groups (rural and urban) or across groups (rural vs. urban). DiGiacomo et al. (2013) also reported that the majority of caregivers in their study scored within the normal range of depression using the Depression, Anxiety, and Stress scales. Schulz et al. (2003) reported that dementia caregivers in their study had high levels of depressive symptoms while providing care, but within 3 months of the death, caregivers had clinically significant declines in depressive symptoms, and within 1 year the levels were substantially lower than levels reported during active caregiving (N = 217).
The low level of depression in this study might also be explained by length of time as a caregiver (50 months for rural and 54 months for urban caregivers). For example, Keene and Prokos (2008) analyzed the impact of spousal caregiving on survivors’ depressive symptoms 6 months into widowhood. They concluded that longer periods of caregiving resulted in lower levels of depressive symptoms in widowhood. Keene and Prokos hypothesized that long-term caregiving allows wives and husbands to adjust and “routinise” care, which may then be perceived as less disruptive than a short period of care. Furthermore, long-term caregiving provides time for couples to say goodbye and begin the grieving process. Once widowed, the positive effect of feeling useful and close to their spouse may carry over(p. 566).
Although the mean CESD scores in this reported study were not in the depressed range (scores ≥16), there was a subset in both the rural and urban caregivers that did score ≥16. It is also important to note that rural caregivers had higher CESD levels across all three data collection points compared to urban caregivers (Table 5).
The MCS mean scores for urban spousal caregivers were higher than the mean MCS of 52 ± 0.9 for a nationally representative sample of noninstitutionalized females aged 70 to 79 (Hanmer & Kaplan, 2016) at all three data collection points. Additionally, the MCS scores increased over the 12-month study period for urban caregivers. The MCS score for rural women was lower than the nationally representative sample at baseline (48 vs. 52) and Time 2 (50.7 vs. 52), although the MCS score did increase at Time 2 and again at Time 3. Furthermore, mean MCS scores were higher than mean PCS scores at all three collection points, which is consistent with the observation that MCS scores increase with age while mean PCS scores decrease with age (Utah Health Status Survey, Utah Department of Health, 2001). Our finding is also congruent with the relationship between PCS and MCS represented by the nationally representative values of noninstitutionalized females 70 to 79 years (Hanmer & Kaplan, 2016) used for comparison in this study (higher MCS compared to PCS). Our findings were also consistent with those reported by DiGiacomo et al. (2013), who reported MCS mean scores above the national mean for females 70 to 79 years, and that the scores increased over the 12 months of their study.
The finding that the urban spousal caregivers in our study as well as those in the DiGiacomo et al. (2013) study had higher MCS scores than the nationally representative sample of noninstitutionalized U.S. females 70 to 79 years over the three collection points (and by Time 3 for rural caregivers) may speak to the resilience of spousal caregivers and their ability to adjust to their “new normal” postdeath.
The findings noted above can also be understood within the context of transition theory, especially as it relates to role supplementation (Meleis, 2010). The transition from spousal caregiver to widow was a process that occurred over several years for the women who participated in this study (mean time caregiving for rural women was 50 months and 54 months for urban women). During active caregiving, the women experienced profound changes in their husbands’ physical health and cognitive abilities (e.g., milestones and turning points), which triggered changes in their role within the marital dyad. According to Meleis, mastery of the knowledge or the specific information and cues needed to perform a role is known as role clarification (p. 18). Moreover, role supplementation may become the means for the achievement of role mastery. Both the rural and urban female spousal caregivers, based on the qualitative interviews, appear to have achieved role supplementation/mastery during active caregiving as evidenced by the themes that emerged: 24/7 Care, Watch the Man Go Down, Build a Network, and Spiritual Support (Saunders & Groh, 2019). These themes indicate that the women’s ability to synthesize and incorporate anticipated role behavior into their repertoire as their husbands’ health declined over time. While the majority of the caregivers appeared to have mastered role supplementation during active caregiving, many reported difficulties transitioning out of being a caregiver. As one woman stated, “I had a purpose when he was here.” Their difficulty letting go of the caregiver role and lack of purpose could indicate role insufficiency during the transition from caregiver to widow. Meleis (2010) states that role insufficiency may result from poor role definition (e.g., what is a widow?), lack of knowledge of role behavior (e.g., how should a widow act?), or the termination of one role (e.g., caregiver) and the beginning of another role (e.g., widow). Moreover, a person’s ability to successfully adapt to role transition can be impeded by grief. For the caregivers in this study, they knew their role as a caregiver (e.g., “do it all”), but their role as a widow was less defined. Despite this apparent role insufficiency, the majority of women reported higher than normal scores on the MCS. This finding supports that transition takes time (e.g., it is a process), it is variable and depends on the nature of the change. Moreover, transitions involve fundamental change in one’s view of self and the world (Schumacher et al., 2010). Thus, it is reasonable to assume that some aspects of how the caregivers transition to widowhood are achieved while other aspects are still in transition.
The last finding for discussion is related to resources used during the transition from spousal caregiver to widow. The use of resources tapered off over the 12 months of the study with the highest usage at baseline (or closer to husband’s death). This was true for both rural and urban caregivers. The resources utilized at baseline were related to group participation (support and bereavement) as well as pastoral care, but utilization declined for both groups at Time 2 and Time 3. Fewer resources being used over time was associated with an increase in MCS scores as well as the overall decrease in CESD scores at Time 2 and Time 3, suggesting that both rural and urban spousal caregivers may have viewed the transition to widowhood as a gain rather than a loss (Meleis, 2010). This is supported by the qualitative findings in this study that although the women missed their husbands, most were relieved when he died believing that their husbands were no longer suffering. Moreover, the women reported positive aspects of being their husbands’ caregiver, stating they had no regrets and would do it all over again (Saunders & Groh, 2019).
The majority of rural and urban care recipients did receive hospice care (Table 3) ranging from 1 day to 18 months. This is consistent with 2016 data showing that dementia was among the top three primary diagnoses for hospice patients (National Hospice and Palliative Care Organization, 2018). The majority of caregivers felt that hospice was invaluable during caregiving, but many expressed disappointments that once the husband died, hospice did not follow up with them. The reasons for lack of follow-up are unknown.
There were some differences between rural and urban spousal caregivers on utilization of resources during caregiving as well as the transition to widowhood. Based on the qualitative findings from this study (Saunders & Groh, 2019), rural caregivers identified difficulties getting their husbands to respite care because of the distance, limited number of family members living in immediate area that could assist with care, lack of information about available services, and lack of information about dementia in general during active caregiving. During the transition to widowhood, both groups participated in support and bereavement groups across the three data collection points, although more rural women identified barriers in accessing these formal resources. Barriers included distance to services, limited hours of services, and lack of privacy and anonymity in rural communities. The Internet was utilized more by rural women for information as were online support groups and staying in touch with family and friends compared to urban women (Saunders & Groh, 2019).
Strengths and Limitations
The strengths of this study include investigating differences between older rural and urban women as they transition from caregiver to widow; the 100% retention rate, the mixed-method longitudinal repeated measures design (12 months), the use of well-established, validated tools, and that all caregivers were spouses (compared to most studies that have mixed samples). Moreover, the study was grounded in transitional theory (Meleis, 2010), providing a theoretical foundation on which to interpret the findings of the study.
Among the limitations is the small sample size (although the repeated measures design mitigates some of the methodological issues with small sample sizes), the varying length of time from husbands’ death (1 month to 3 years), the lack of racial and ethnicity diversity, and the limited generalizability of the findings to other caregiver populations.
Implications
There are several practice and research implications for psychiatric mental health nurses. First, psychiatric mental health nurses’ practice in a variety of delivery care settings where spousal caregivers receive health care. Understanding some of the educational deficits of spousal caregivers (e.g., dementia knowledge, available resources) provides an opportunity for psychiatric mental health nurses to examine ways in which access to such information can be increased. Psychiatric mental health nurses are skilled at assessing situations, identifying barriers, finding problem-solving solutions, and communicating with a diversity of individuals who feel stressed and overwhelmed. Second, psychiatric mental health nurses can expand their role in offering support, individual and group therapy, as well as empathy to spousal caregivers during their journey as a caregiver and then their transition to widowhood. These interventions have the potential to facilitate the bereavement experience, increase caregiver resilience, and help them renegotiate life and identity after the death of their husbands. Third, psychiatric mental health nurses can also help spousal caregivers develop strategies for engaging in self-care activities that will maintain and foster their overall health as they transition to widowhood. One strategy is for psychiatric mental health nurses to use transitional theory as a framework for assessing and identifying predisposing conditions that might result in problematic role transition for spousal caregivers. According to Meleis (2010), minimal role insufficiency is manifested when both early prevention and early supplementation are offered by nurses without interruption before role transition occurs and during the early stages of the transition (p. 22). Last, psychiatric mental health nurses can also advocate for additional services for both the care recipient and the caregiver. Knowing that the transition to widowhood can be affected by the caregiving experience, it is imperative that psychiatric mental health nurses identify where the gaps in services are and then advocate for those services.
In terms of research, psychiatric mental health nurses can design and implement more research studies on the transition to widowhood following caregiving activities. Research using transition theory as its conceptual framework could explore, test, and verify factors that impede a person’s progress toward health and his/her adaptation to role transition. More diverse and larger samples of spousal caregivers are critical in expanding our knowledge base of what the transition is like for caregivers and provide insights into innovative interventions. Even though there were no statistically significant differences between rural and urban spousal caregivers in this study, it is important to note that rural caregivers scored higher on the CESD, as well as scored lower on the PCS and the MCS at most of the three data collection points. Additional research in this area is needed.
Conclusions
There were two major gaps in caregiver knowledge that this study addressed. First, the need for an expanded understanding of the impact of spousal caregiving on the health of older women after the death of their husbands, and, second, the need to compare similarities and differences of these underlying factors between rural and urban spousal caregivers. Several aspects of the conceptual model (e.g., length of time as caregiver, use of community resources, social support) were supported as affecting health outcomes (depression, physical and mental functioning). Additional research is required for a more robust testing of the model.
Although the findings of this study did not detect any statistically significant differences between rural and urban spousal caregivers on physical or emotional consequences of caregiving due to the small sample size, CESD scores were higher for rural caregivers at all three collection points. Moreover, rural women reported lower PCS and MCS scores compared to their urban counterparts. Despite the limitations of this study, this study provides preliminary data suggesting that larger scale studies are warranted that might detect significant and meaningful differences between urban and rural widows so appropriate resources can be developed and tested in future research. Having an accurate understanding of the challenges of rural dementia care can result in the development of unique rural solutions during the transition from caregiver to widow, if such differences exist.
Footnotes
Acknowledgements
We thank the wonderful women who shared their homes, stories, and time to help us better understand the transition from spousal caregiver to widowhood. Without their willingness to be vulnerable, this knowledge would not have been generated and shared with the readers.
Author Roles
Carla J. Groh and Mitzi M. Saunders both participated in the design, implementation, and analyses of data for this article. Moreover, both authors contributed to the writing, review, and editing of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Work reported in this publication was supported by the National Institutes of Health Common Fund and Office of Scientific Workforce Diversity under three linked awards, RL5GM118981, TL4GM118983, and 1UL1GM118982, administered by the National Institute of General Medical Sciences.