
Abstract
Purpose
Patients with cancer face an elevated risk of influenza and pneumococcal infections with increased risk of morbidity and mortality compared to the general population. Vaccination rates for this patient cohort however remain below international target levels, despite vaccination being the most effective strategy for preventing these infections. This study therefore aimed to explore patients with cancer perspectives on influenza and pneumococcal vaccination in the oncology setting, and whether they saw a potential role for pharmacists in providing vaccination services in an outpatient oncology clinic.
Methods
A cross-sectional survey was conducted in the outpatient oncology department at a large regional hospital in Cairns, Australia. Participants were currently undergoing cancer treatment or had a history of cancer treatment. The 32-question self-completed survey included patient demographics and assessed vaccination status, beliefs on vaccination, and confidence in pharmacist services. Questions were developed and aligned to the constructs of the Health Belief Model.
Results
107 patients with cancer completed the survey. 75.7% of these patients had solid tumours and 24.3% a haematological malignancy. Self-reported vaccination rates were 55.1% for influenza (past 12 months) and 22.4% for pneumococcal (past 5 years). Despite this, 83.2% of patients were willing to be vaccinated, and 86.0% regardless of age or gender were amenable to receive at least one vaccine from a pharmacist. Patients expressed strong trust in all healthcare professionals as their preferred source of vaccine information during cancer treatment. A key barrier identified was a lack in the provision of information, with only 51.4% of patients feeling adequately informed to make decisions about vaccinations.
Conclusion
This study revealed a discrepancy between low influenza and pneumococcal vaccination rates and high patient willingness to be vaccinated. Patients demonstrated strong confidence and readiness to receive vaccinations from pharmacists within oncology units, suggesting that a convenient pharmacist-led vaccination service could improve vaccine uptake.
Introduction
Influenza and pneumococcal infections pose a significant threat to patients with cancer, due to both the underlying immunosuppressive effects of cancer and the impact of the treatments. 1 Seasonal outbreaks of influenza result in as many as 646,000 deaths worldwide each year, 2 and patients with cancer that contract influenza have a three to five times higher risk of hospitalisation and 10 times the risk of death after hospitalisation compared to the general population. 3 Patients with immune deficiencies, including solid and haematological cancers, experience invasive pneumococcal disease (IPD) at a rate of up to 503 cases per 100,000 persons, compared to just 8.8 cases per 100,000 in the general population. 4 Heavily immunosuppressed patients with solid cancers have a 23.0% greater risk of developing pneumonia and experience a high mortality rate of 9.5%. 5 Vaccines are the most effective tool for preventing these infectious diseases. 6 For over 60 years, a safe and effective influenza vaccine has been available, 7 with The World Health Organization (WHO) emphasising vaccination to be the most powerful tool to prevent the spread of seasonal influenza and its serious complications. 8
Despite the universal recommendations and the availability of cost-free influenza vaccine for all patients over 65 or high risk groups and all residents in some states in Australia,9,10 influenza vaccination rates in patients with cancer fall short of the target of ≥75% population coverage. 11 Achieving the 75% target has demonstrated to reduce spread, protect vulnerable patient cohorts and reduce complications, which cause a strain on healthcare resources. 12 The Centre for Disease Control (CDC) recommend pneumococcal vaccination for adults with immunosuppression risk factors such as generalised malignancies. 13 Pneumococcal vaccines in Australia are funded for specific groups, including haematological malignancy, but this funding is excluded for solid organ cancers. 14 Restricted funding could explain the reported 37.6% pneumococcal vaccination rate in people over 70 in 2023. 15
A literature review examining vaccination in patients diagnosed with cancer reported three key barriers, which generally align with patients, health professionals, and the healthcare system. 16 The main patient barriers identified were: receiving misinformation, fear of side effects, and lack of perceived benefit from vaccines, while health professional barriers impacting vaccination were lack of recommendation and lack of confidence in vaccines for patients receiving chemotherapy treatment. The main healthcare system barriers were a lack of access to vaccines and cost. 16 Patients diagnosed with cancer are a complex patient cohort and often require individualised vaccination strategies to improve vaccination rates compared to the general population. 17 This requires active coordination among healthcare providers, including primary care practitioners, pharmacists, and nurses. 17 Strategies include identifying optimal timing of vaccination, vaccination catch-up schedules, reviewing immune response where indicated, vaccination of close contacts, and using adjuvant vaccine formulations, when necessary. 17
Pharmacists specialising in the oncology setting have been around for 50 years, primarily focused on procurement and manufacturing of chemotherapy, and performing clinical checks to ensure the safe administration cancer-related medications for these patients. 18 With advancements and specialised training in direct patient care in the oncology setting, pharmacists are now an integral part of the multidisciplinary team, working in hospitals and outpatient units. They utilise their expertise to guide treatment decisions, manage complex therapies, and coordinate key elements of care for patients with cancer. 19 To improve patient access to vital vaccinations, specially trained oncology pharmacists can expand their role to include vaccination assessment, education and administration. 20
Pharmacists, recognised for their accessibility, trustworthiness, and cost-effectiveness, have demonstrated high patient satisfaction as vaccine providers.21–24 Pharmacists are qualified to administer vaccinations, having gained the necessary skills through specialised training at undergraduate or postgraduate level. 25 They also have a proven track record of safely delivering influenza vaccines to adults in community settings. 26 A systematic review and meta-analysis found pharmacists had a positive impact on immunisation uptake in both community and hospital settings. 27 However, there is a lack of studies on the pharmacist's role in vaccinations in the oncology setting or vaccination uptake in cohorts of patients with cancer. 28
This study therefore aimed to explore patients with cancer perspectives on influenza and pneumococcal vaccination in the oncology setting, and whether they saw a potential role for pharmacists in providing vaccination services in an outpatient oncology clinic.
Methods
Study design and theoretical framework
This study adopted a cross-sectional research design utilising an anonymous self-completed survey to investigate the perspectives of patients with cancer informed by the constructs of the Health Belief Model (HBM). 29 The HBM explains health behaviours, including vaccination, through the cognitive constructs: perceived susceptibility (PS), severity (S), benefits (BEN), barriers (BAR), self-efficacy (SE), and cues to action (CA).29–31 Utilised in vaccination studies previously, the HBM posits that perceived susceptibility and severity of disease create a perceived threat, while perceived benefits and barriers for vaccination influence decision-making, while self-efficacy reflects confidence in obtaining vaccination.31,32
Study population and setting
Adult patients (≥18 years) undergoing or with a history of systemic anti-cancer treatment (including oral, parenteral, chemotherapy, immunotherapy, targeted, and radiation therapies) were recruited from the outpatient oncology unit at Cairns Hospital. This 771-bed referral hospital serves a large, 142,900 km² region in Far North Queensland, 33 providing access to a diverse patient population. Patients with various cancer diagnoses, including acute haematological malignancies, are treated in the inpatient setting and an outpatient oncology centre.
Data collection
A 32-question survey assessed vaccination knowledge, beliefs, and perceptions among oncology and haematology patients. It covered four areas: 1) current influenza and pneumococcal vaccination status, 2) personal views on vaccination, 3) opinions on pharmacist-led vaccination, and 4) demographic details. The survey included closed-ended yes/no, and multiple-choice questions with Likert-scale responses.
A pilot survey with eight patients and two academic staff was undertaken to evaluate reliability, face, and content validity. Feedback on time, content, layout, and functionality led to limited revision of the survey. (Appendix A) The internal consistency Cronbach's alpha (α) coefficient for questions associated with the HBM was acceptable at 0.771. 34
A convenience sampling technique was used, where patients presenting to the outpatient oncology unit for review or treatment between April 2024 and October 2024 were invited to participate. Patient information sheets were provided with a Quick Response (QR) code to take them to a secure digital online survey provider QUALTRICS ™. Paper copies were provided if patients were unable to complete the survey electronically. All data were stored securely with ethics approval granted from Far North Queensland Ethics Committee HREC / /2023/QCH69788 (Apr Ver. 3) – 1628.
Data analysis
Data were uploaded into IBM Statistical Package for Social Sciences (SPSS) version 23 to generate descriptive and inferential statistics. Where appropriate, variables with multiple response options were grouped into two or three subcategories for analysis using the Chi-square test. Due to small sample sizes, Fisher's exact test was used to investigate association between all demographic details, such as gender, age (above and below 60), cancer diagnosis (solid tumour or haematology), treatment type and collected categorical data, such as perceived infection risk, perceived severity, participant willingness to receive vaccination from a pharmacist, or vaccination in past 12 months. A p-value of ≤ 0.05 (95% confidence interval) indicated statistical significance.
Results
Patient characteristics
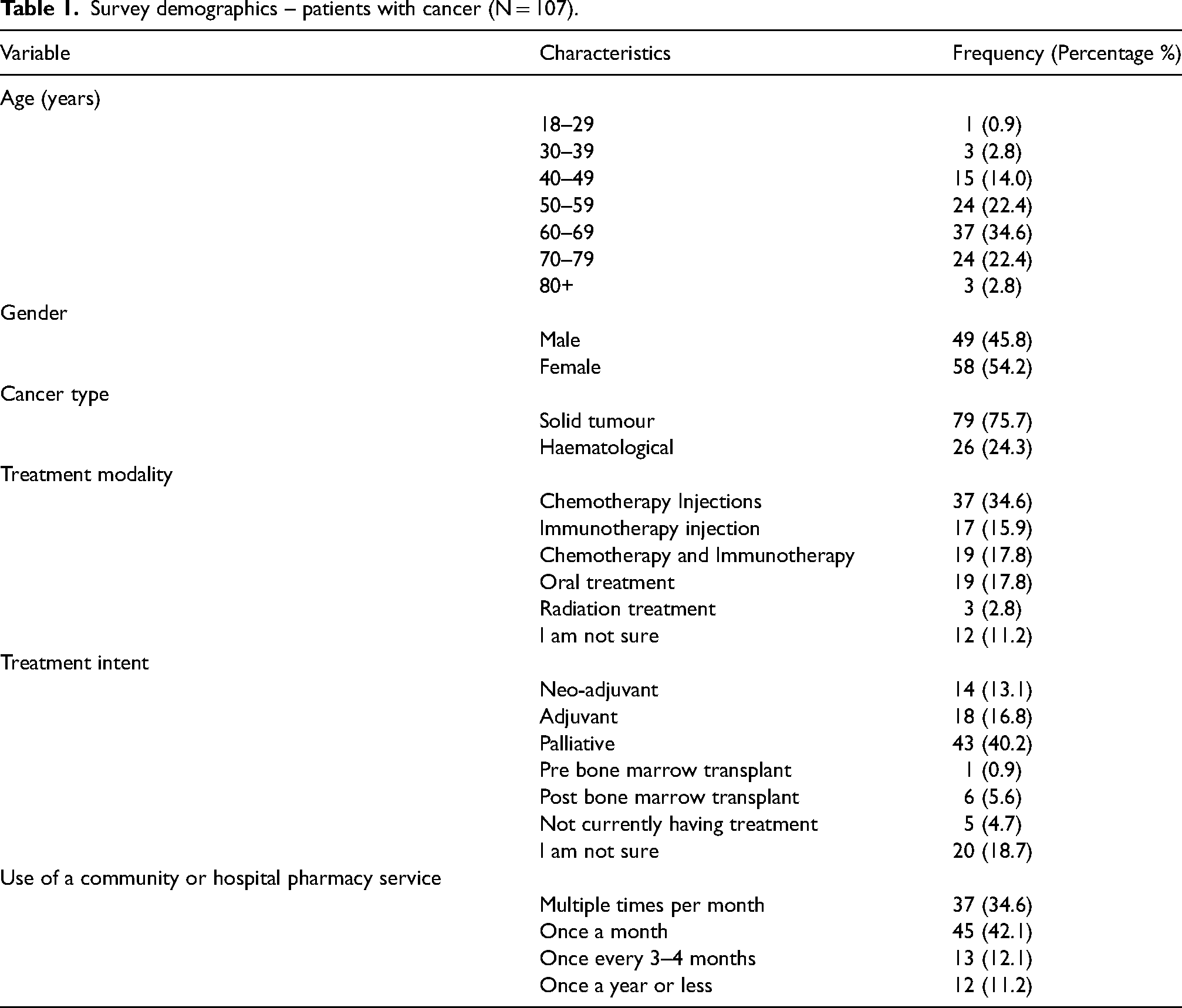
107 complete responses were received, 47 were completed via paper copy and 60 completed online. Patient characteristics are summarised in Table 1. 59.8% (64/107) of patients were 60 years of age or over, and 54.2% (58/107) were female. 75.7% (79/107) of patients had an oncological diagnosis, with most common being breast cancer at 23.4% (25/107), with a representation of most cancer types. 24.3% (26/107) of respondents had a haematological diagnosis, with the most common being lymphoma at 11.2% (12/107). 95.3% (102/107) of patients were on current active treatment, with 68.3% (73/107) receiving parenteral treatment. 40.2% (43/107) of respondents had a stage 4 diagnosis with palliative treatment intent.
Survey demographics – patients with cancer (N = 107).
Vaccination rates and beliefs
The study found 55.1% (61/107) of respondents received influenza vaccine in the past 12 months and 22.4% (24/107) received pneumococcal vaccine in the past 5 years. Overall, patients expressed a positive association with vaccination with 69.2% (74/107) willing to be vaccinated with minimal to no concerns. When asked if they received any vaccine in the past 12 months, 65.4% (70/107) indicated yes. The most common locations for vaccination were with General Practitioners (GPs) at 55.9% (60/107) and community pharmacies at 30.9% (32/107) while only 5.5% (6/107) of patients were vaccinated at a hospital or public clinic. 80.4% (86/107) of patients indicated they would receive vaccination at the hospital cancer centre (Table 2).
Patient with cancer vaccination status (N = 107).
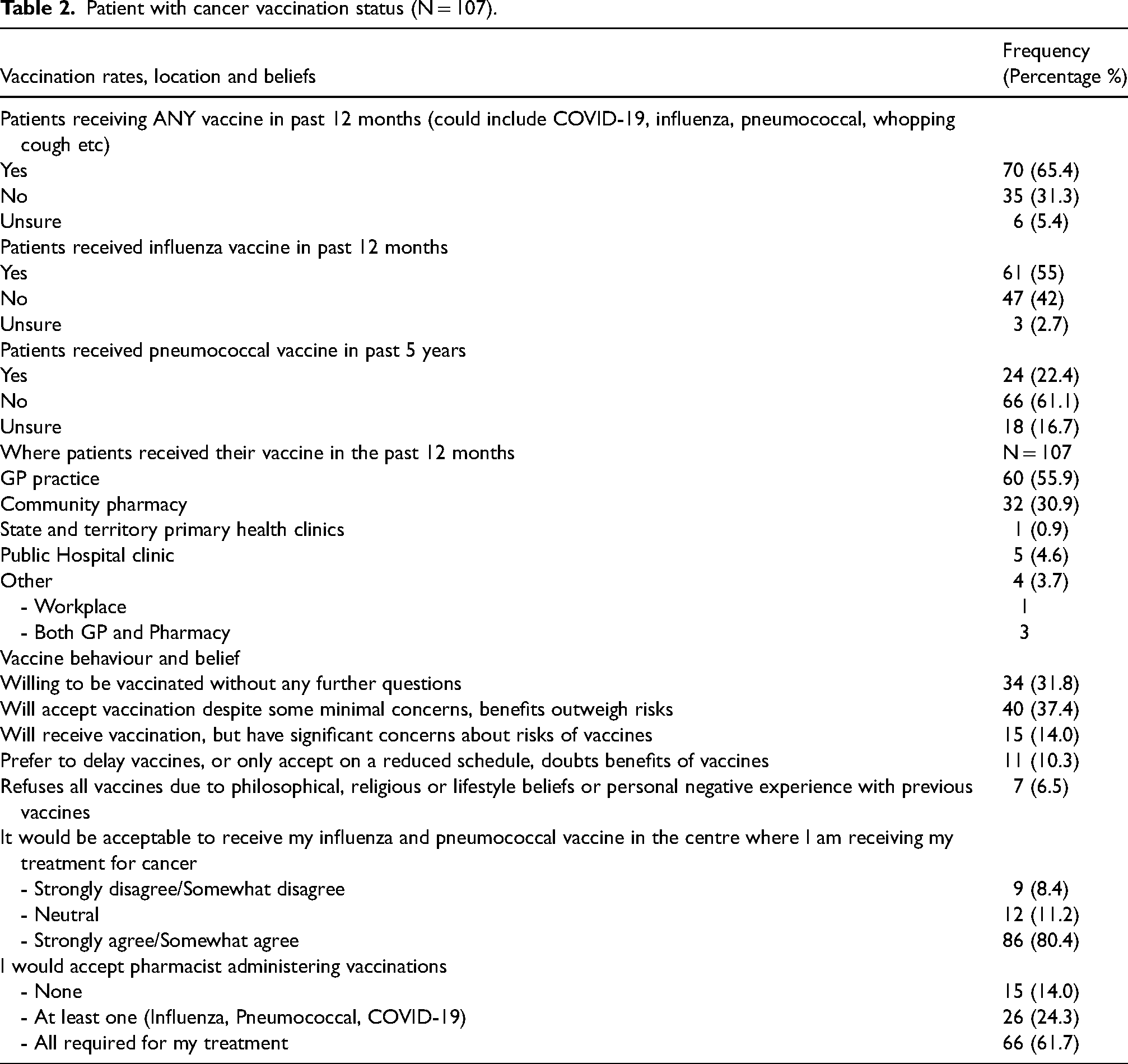
Patients were open to receiving vaccination recommendations from all healthcare professionals involved in their care, though they preferred receiving recommendations from their treating oncologist/haematologist 79.4% (85/107) followed by GPs 67.3% (72/107) and nurses 60.8% (65/107). Pharmacists were the least preferred source of recommendation, with only 55.1% (59/107) of patients indicating willingness to accept their vaccination recommendation. However, despite being the least favoured preference, 86% (92/107) of patients were still willing to receive at least one vaccine from a pharmacist and 61.7% (66/107) would accept all vaccines administered by a pharmacist, during their cancer treatment.
Figure 1 shows the preferred sources of information about vaccination by respondents. Although internet chat forums 19% (21/107) and social media 15% (16/107) are still preferred sources of vaccine information for some participants, healthcare professionals, particularly doctors, remain the most trusted by patients with cancer, with confidence levels ranging from 60% (65/107) to 82% (92/107).
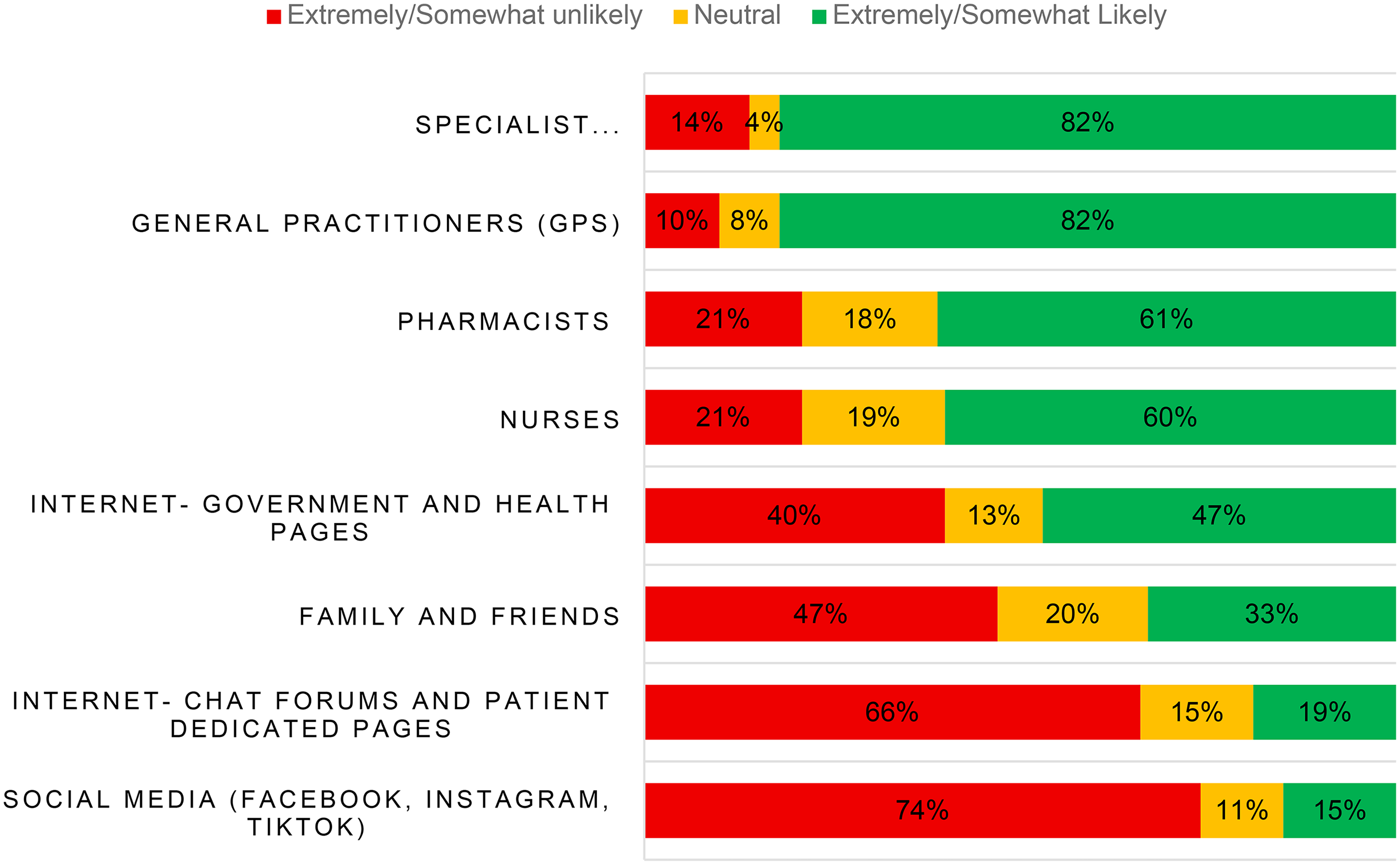
Patients with cancer preferred sources of vaccine information.
Health belief model
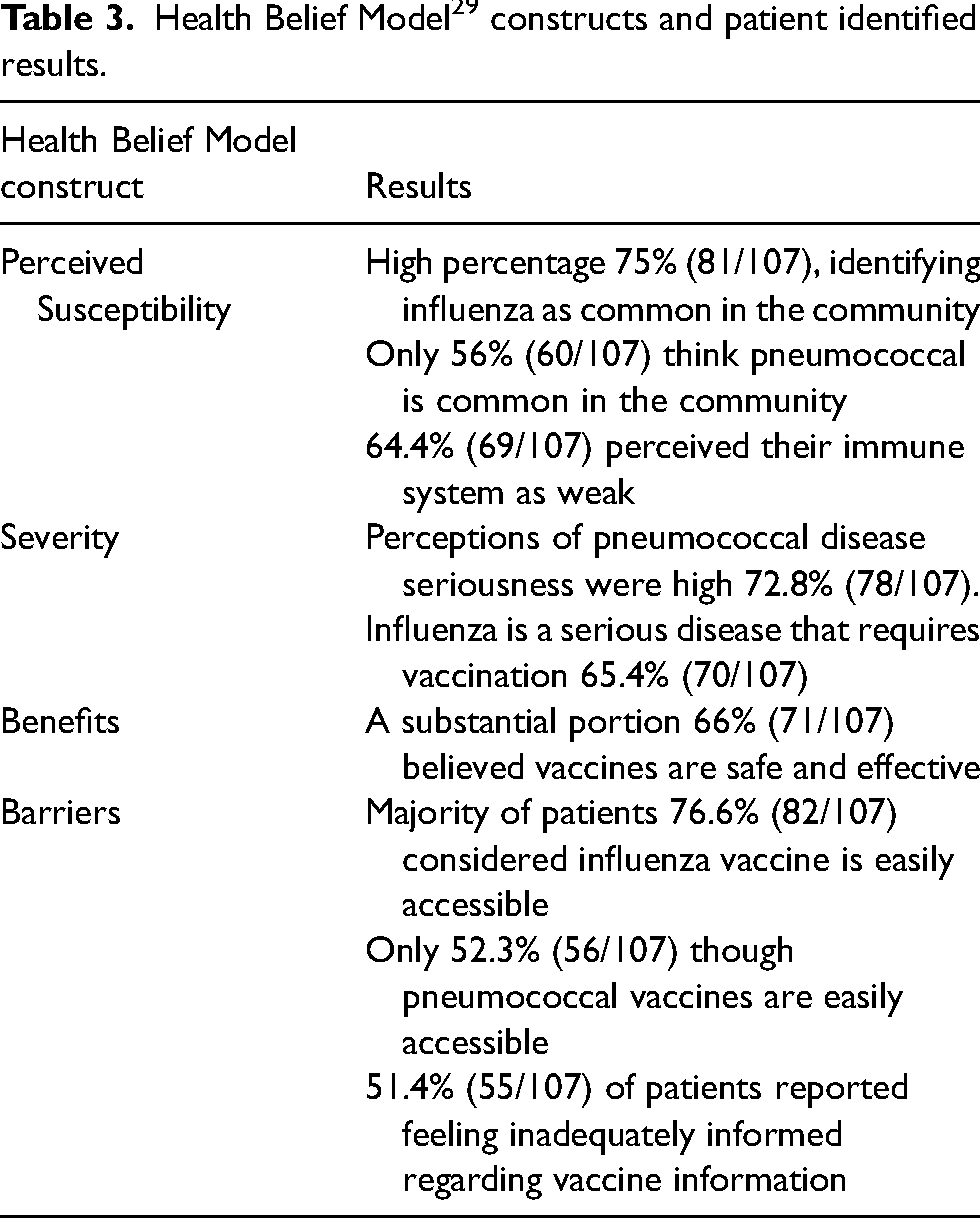
Figure 2 illustrates the distribution of responses mapped across the HBM constructs and Table 3 summarises the results.
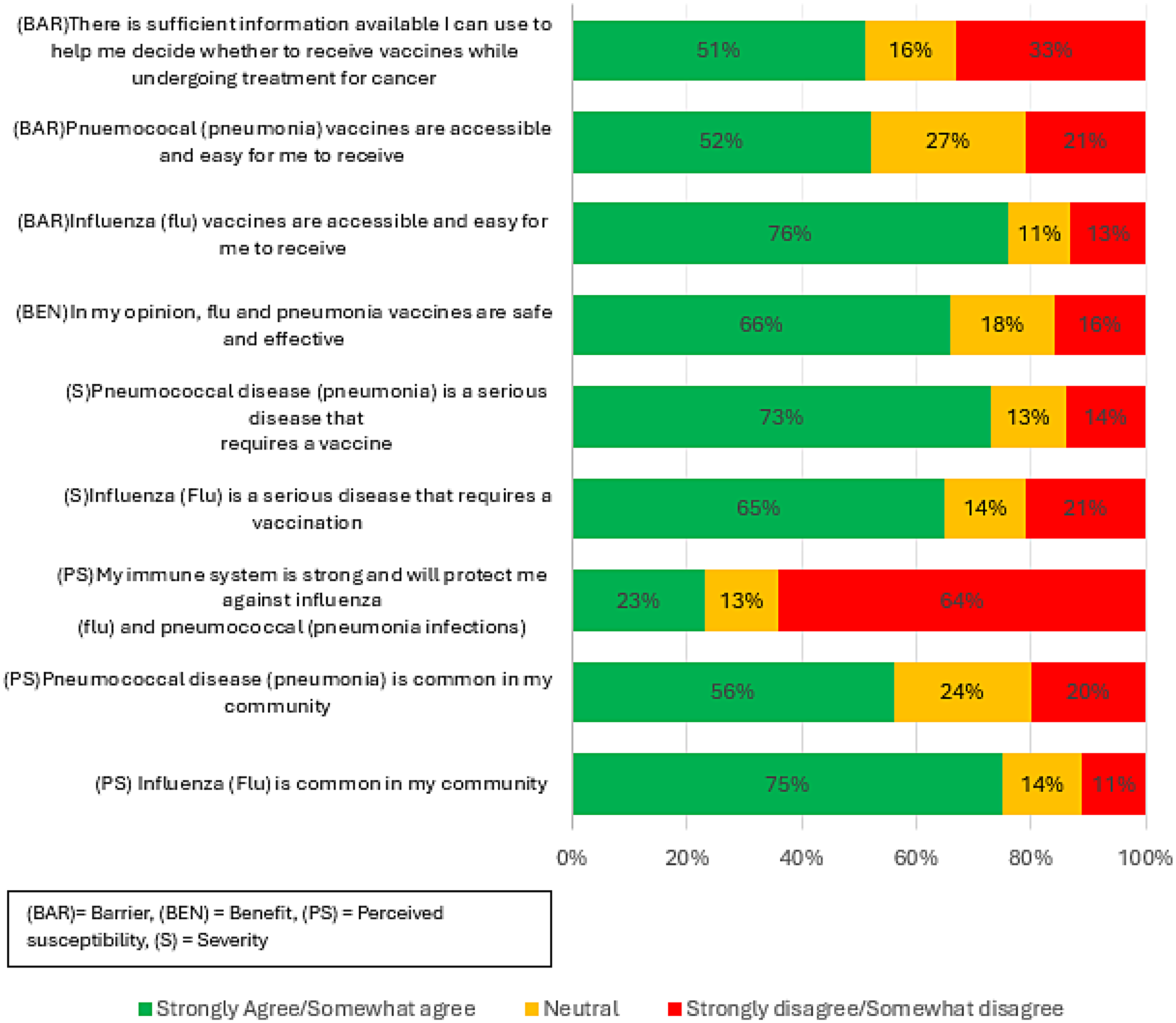
Patients’ response agreement with the constructs of the Health Belief Model. 29
Health Belief Model 29 constructs and patient identified results.
We examined associations between all variables, including demographic characteristics and constructs of the HBM. Chi-Square analysis found no significant associations between demographic characteristics such as age, gender, type of cancer diagnosis, or treatment intent (palliative vs. curative) and vaccination status within the past 12 months. As an example, type of cancer diagnosis (solid organ or haematological) had no association with vaccine status, X2 (1, N = 107) = 0.330, p < 0.566. However, prior 12-month influenza vaccination was significantly associated with several constructs of the HBM. Specifically, there were statistically significant associations with: Perceived susceptibility (PS) “Influenza is common in my community” (p = 0.008), perceived severity (S) “Influenza is a serious disease that requires vaccination” (p < 0.001), perceived benefit (BEN) “Vaccines are safe and effective” (p < 0.001), perceived barrier (BAR) “Not willing to pay for vaccines” (p < 0.001).
Further Chi Square test analysis was conducted to assess associations between HBM items and the willingness of accepting pharmacist-administered vaccination. Significant associations were identified for: (PS) “Influenza is common” (p = 0.020), (PS) “Pneumonia is common” (p = 0.020), (S) “Influenza is serious” (p < 0.001), (S) “Pneumonia is serious” (p < 0.001), (BEN) “Vaccines are safe and effective” (p < 0.001).
Discussion
This study assessed influenza and pneumococcal vaccination self-reported rates, identified barriers to vaccination, and explored perspectives on pharmacists’ role in vaccinations among patients with cancer in a regional hospital in Australia. To our knowledge, this is the first study in this population using the HBM to evaluate factors influencing vaccine uptake.
Our findings revealed low vaccination uptake in this cohort, with only 55.1% (61/107) of patients receiving an influenza vaccine in the past 12 months and 22.4% (24/107) receiving a pneumococcal vaccine in the past five years. Despite this, most patients recognised the prevalence of influenza 75.0% (81/107) and pneumococcal 56.0% (60/107) diseases in the community, indicating awareness of susceptibility. Notably, 64.4% (69/107) considered their immunity to be weak. However, 35.5% (38/107) of patients do not think, or may not know their immunity may be compromised, which may contribute to lower vaccination uptake. Increased perceived susceptibility and severity of illness in the HBM (29) are typically associated with higher likelihood of engaging in preventative behaviours such as vaccination, which does not align with our findings.
In contrast to studies of general populations, where heightened perceived susceptibility has been positively correlated with vaccine uptake, 35 our cohort had a lower vaccination rate. This suggests that, in the context of cancer care, other factors may attenuate the influence of susceptibility on behaviour. Furthermore, if vaccination is not integrated into routine oncology care, the opportunity to act on patients’ perceived susceptibility may be missed. 36
We identified insufficient information as a barrier in our study. Limited knowledge about vaccine effectiveness and adverse events, has been recognised as a barrier among both patients and caregivers.37,38 Our study found only half of the patients felt they had sufficient information to make a vaccination decision. Providing patients with appropriate information has been shown to increase vaccination confidence and uptake. 27 Accessibility, often cited as a vaccination barrier, 39 was not prominent in this cohort, with three quarters of patients reporting easy access to influenza and pneumococcal vaccinations. While a majority of our patient cohort expressed willingness to be vaccinated, actual vaccination rates remained low. Similarly, while patients acknowledged the seriousness of pneumococcal disease (perceived severity), this recognition did not appear to translate into high vaccine uptake. Furthermore, a rapid review conducted between January 2012 and May 2022 in the general population, identified low perceived risk of infection and vaccine safety concerns as primary barriers to influenza vaccination. 40 In comparison, our study found that patients perceived themselves to be at high risk and had minimal concerns about vaccine safety.
While the HBM defines self-efficacy as an individual's belief in their capacity to take action,29,41 only 23.0% of patients in our study expressed strong confidence in their immune system. Although this measure reflects perception of general health rather than behavioural capability, it may intersect with vaccine decision making, if patients doubt their physiological ability to respond effectively to vaccination. 37
Moreover, despite recognising influenza prevalence and the need for vaccination, awareness did not translate into higher vaccination uptake. These discrepancies underscore the complexity of vaccine related decision-making among patients with cancer and suggest that additional factors may be influencing uptake in this population. These may include time constraints prior to chemotherapy initiation, 42 inconsistent vaccination recommendation from medical professionals during treatment, 43 and potential communication gaps between cancer centres and primary care providers. 44
One of the potential explanations for the observed low vaccination rates in this cohort is the inconsistent provision of vaccination recommendations by doctors. 45 Several factors may contribute to this, including limited consultation time with specialists and GPs, as well as potential gaps in awareness regarding current vaccination guidelines and funding mechanisms. 46 Previous research supports these findings, indicating that vaccination assessment and recommendation may not always be a priority in oncology consultations. 47
Despite these inconsistencies, our study found that patients undergoing cancer treatment exhibited high level of trust in healthcare professionals (HCPs) as sources of vaccine information, contrasting to previous studies of the general population that identified mistrust in HCP as a barrier to vaccination. 16 Trust in HCPs is a critical determinant of vaccine uptake, 48 and patients who relied on HCPs as a credible information source, were more likely to associate vaccines with effectiveness. 49 These findings highlight a key opportunity that consistent vaccination recommendations from trusted HCPs, including pharmacists, could positively influence uptake in this study population.
Awareness of current vaccination recommendations among all healthcare providers is essential to support vaccine uptake in patients with cancer. However, ensuring consistent knowledge and messaging across all providers may be impractical in busy clinical settings. Pharmacists, with their accessibility and expertise are ideally positioned to lead these discussions and ensure patients receive timely and consistent vaccination advice.
The findings in this study strongly support this approach. In addition to identifying high patient willingness to accept pharmacist-administered vaccines, Table 2 shows that most participants were comfortable receiving vaccination within the cancer treatment centre itself. This insight suggests that the treatment setting is not as a barrier, but rather a convenient and acceptable location for vaccine delivery.
Pharmacists are already embedded in the oncology treatment setting, regularly interacting with patients during their therapy. Their accessibility and existing rapport with patients position them uniquely to assess vaccination needs, and deliver tailored education, and address misconceptions. Moreover, pharmacists are trained and credentialed to provide evidence-based information, helping overcome previously identified barriers such as information about vaccines or vaccine related safety and efficacy concerns. Evidence shows that pharmacists can assess risk and recommend vaccines safely, 28 with their recommendations being as effective as those from doctors, 50 and that such recommendations directly contribute to increase vaccine uptake. 51
While the broader literature supports the role pharmacists play in vaccination,26,52 no studies have examined patient perspectives of pharmacist-delivered vaccine services in outpatient cancer units. Our study identified a statistically significant association between patients’ willingness to receive pharmacist administered vaccines and the constructs of HBM. Specifically, patients with high perceived susceptibility, severity and benefit, were more likely to accept pharmacist-administered vaccines. This offers a promising avenue to address observed gap between high perceived risk and low vaccine uptake.
Finally, our findings reaffirm commonly reported barriers to vaccination. Despite patients expressing willingness and recognising the importance of vaccination, a substantial proportion remained unvaccinated against both influenza and pneumococcal disease. This disconnect indicates that further investigation is needed to elucidate the specific barriers preventing positive attitudes towards vaccines translating into actual vaccination uptake behaviour.
Strengths and limitations
To the best of our knowledge, this study is unique in that it aimed to explore patient perspectives on influenza and pneumococcal vaccination in an oncology setting in Australia. Furthermore, this is the first study to examine patient perspectives on the involvement of pharmacists within oncology units, specifically regarding confidence in pharmacist-provided vaccination services.
Several potential limitations should be acknowledged. The study did not reach required sample size, which limited the power of inferential analyses. Social desirability bias may have influenced responses, particularly within a single-centre study. However, the use of an anonymous survey likely mitigated this bias. The timing of the study was after the traditional “flu” season in Australia so patients either might not have been motivated to have received a flu injection, or their recall of previous vaccination may have been impacted by the timing of the study.
Conclusions
This study confirms suboptimal influenza and pneumococcal vaccination rates in patients with cancer, despite a high trust in healthcare providers and a willingness to be vaccinated. Strong patient support for pharmacist-delivered vaccination services highlights their potential to improve vaccine uptake. Leveraging pharmacists’ accessibility and expertise, a pharmacist-led service could address vaccine hesitancy and boost vaccination rates. Future research should assess national vaccination rates in patients with cancer and further explore the underlying reasons for vaccinated vs unvaccinated status. A pharmacist-led vaccination service within outpatient oncology units may be a promising strategy to improve vaccination rates in this vulnerable patient cohort, given that the majority expressed a willingness to receive vaccines administered by pharmacists.
Footnotes
Acknowledgements
Michael Crowe for providing support with the statistical analysis.
Author contributions/CRediT
Data availability statement
The datasets used and analysed in this study are available from the corresponding author upon reasonable request, subject to an approved data use agreement and evidence of maintaining participant confidentiality.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical and approval statement
Ethics approval granted from Far North Queensland Ethics Committee HREC / /2023/QCH69788 (Apr Ver. 3) – 1628.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Appendix A. Pilot survey feedback and action.
Summary of changes to survey.

| 1 | Update the information sheet to increase the expected time to complete the survey. |
| 2 | Reduce the number of questions that were similar. |
| 3 | Increased font size on the survey for better readability on digital devices |
| 4 | Reduced wording on the landing page to reduce time reading duplicate information |
| 5 | Included “flu” and “pneumonia” to help patients understand the questions better. |
| 6 | Removed the labels about vaccine behaviour |