
Abstract
Introduction
We compared the efficacy of first-generation granisetron and second-generation palonosetron in triplet anti-emetic prophylaxis in patients with non-small cell lung cancer (NSCLC) receiving cisplatin-based high emetogenic chemotherapy (HEC).
Methods
This prospective, multicenter, non-randomized, observational study was conducted between June 2018 and December 2021. Patients diagnosed with NSCLC who received triplet anti-emetic prophylactic treatment with aprepitant and dexamethasone plus granisetron or palonosetron before the first cycle of chemotherapy were included in the study. At the end of the first week after chemotherapy, the emesis scale was applied to the patients during the outpatient control. The primary endpoint was complete response (CR) and total control (TC).
Results
One hundred twenty-one patients were included in the study. Sixty-one patients were in the granisetron group and 60 patients were in the palonosetron group. CR was higher with granisetron in the acute phase (70.5% vs. 58.3%, p = 0.16; respectively) and higher with palonosetron in the delayed phase (61.7% vs. 55.7%, p = 0.5; respectively), although not statistically significant. The TC rates were also not significantly different between the groups (54.1% vs.57.6%, p = 0.69).
Conclusions
There was no significant difference between granisetron and palonosetron in both acute and delayed control of emesis in NSCLC patients receiving cisplatin-based HEC.
Keywords
Introduction
The main cause of chemotherapy-induced nausea and vomiting (CINV) is thought that serotonin, substance P, and dopamine released due to the damage in the gastrointestinal system caused by chemotherapy stimulate 5-HT3 (5-hydroxytryptamine 3), NK-1 (neurokinin-1), and dopamine receptors in target organs, respectively. 1 Stimulation of 5-HT3 receptors by serotonin is considered the most critical pathway for acute phase CINV, while stimulation of NK-1 receptors with substance P is considered the most important pathway for delayed phase CINV. 2 A significant decrease in acute CINV was achieved with first-generation 5-HT3 receptor antagonists (5-HT3RA) such as ondansetron, granisetron, and tropisetron. There was also a significant decrease in both acute and delayed CINV with NK-1 inhibitor drugs such as aprepitant.3,4 It is known that first-generation 5HT3RAs have similar efficacy when used alone or in combination with dexamethasone. Although they have significant curative effects on acute CINV, they are not effective enough on delayed CINV.1,5
Palonosetron, a second-generation 5-HT3RA, differs from first-generation 5-HT3RAs with its high affinity for 5-HT3 receptors, which is at least 30 times more, and a longer half-life of up to 40 h. In addition, unlike the first-generation 5-HT3RAs, palonosetron has been shown to inhibit crosstalk between the 5-HT3 and NK-1 receptors. Because of this, it is thought that palonosetron may be more beneficial, especially in the treatment of delayed CINV. 2
Studies have shown that palonosetron is superior to first-generation 5-HT3RAs in preventing both acute and delayed CINV when given alone, and only delayed CINV when given in combination with dexamethasone. 5 However, although it has been shown to crosstalk with NK-1 receptors in preclinical studies, it is still controversial whether second-generation palonosetron is more effective than first-generation setrons when used in triplet combination with aprepitant and dexamethasone. The question of whether this crosstalk feature will be a synergistic effect or neutralized when used in combination with NK-1 inhibitor remains unclear. 4
To the best of our knowledge, there are a few head-to-head studies in the literature comparing palonosetron and first-generation setrons in triplet anti-emetic prophylaxis in patients receiving highly emetogenic chemotherapy (HEC).6–12 Palonosetron was statistically significantly more effective in preventing delayed CINV only in the TRIPLE study, 6 unlike the others. However, this study consisted of a heterogeneous group that included patients with both lung and other non-pulmonary primary cancers.
Therefore, we compared the efficacy of palonosetron and granisetron in triplet anti-emetic prophylaxis only in patients with non-small cell lung cancer (NSCLC) receiving first cycle cisplatin-based HEC.
Methods
This prospective, non-randomized, observational study was conducted in four different oncology centers in Turkey between June 2018 and December 2021. The study was carried out in accordance with the Declaration of Helsinki and all related regulations and written informed consent was obtained from all participating patients.
Participants
Patients aged ≥18 years, diagnosed with NSCLC, never received chemotherapy, and who would receive the first cycle of cisplatin-based HEC (cisplatin ≥50 mg/m2) were included in the study. Patients who received multiple day chemotherapy or radiotherapy, who had previously received chemotherapy for cancer, who had brain metastases, and who used opioid-derived analgesics were excluded from the study. In addition, patients who used any 5-HT3RA, corticosteroid, metoclopramide, or antihistamine drugs in the last week were not included in the study.
Study design
For anti-emetic prophylaxis, patients received 125 mg oral aprepitant and intravenous dexamethasone plus 0.25 mg palonosetron or 3 mg granisetron half an hour before the first cycle of chemotherapy. Prophylaxis was continued with 80 mg of aprepitant on the second and third days after chemotherapy. The choice of prophylactic 5-HT3RA and the dose of dexamethasone is left to the discretion of the physician following the patient. At the end of the first week after chemotherapy, MASCC (Multinational Association of Supportive Care in Cancer) nausea and vomiting rating scale was applied to the patients on the phone under the control of the outpatient clinic.
Endpoints
The primary endpoint of the study was complete response (CR) and total control (TC). CR was defined as the absence of nausea, vomiting, and no additional anti-emetic therapy in thef irst 24 h (acute phase) and the between 2nd-5th days (delayed phase) after chemotherapy, separately. TC was defined as the absence of nausea and vomiting and no need to salvage anti-emetic use during 0–120 h after chemotherapy ends. The secondary endpoint was the comparison of common treatment-related advers events such as constipation, headache, and hiccups.
Statistical analysis
SPSS (SPSS 15.0; IBM Inc., Chicago, IL, USA) software. Kolmogorov-Smirnov tests were used to determine the distribution of the variables. Independent t-test was used to analyze homogeneously distributed variables, expressed as mean ± standard deviation. Categorical variables were compared with the required test (Chi-square or Fisher exact test). A p-value lower than 0.05 was determined as statistically significant. The total sample size was determined as at least 98 patients with 90% power and 0.06 alpha value by G-power 3.1 software.
Results
One hundred fifty-four patients were enrolled in the study. After excluding 12 patients with brain metastases, two patients using steroids, 11 patients using opioid-derived analgesics, and eight patients withdrawing their consent, a total of 121 patients were included in the study. (Figure 1)
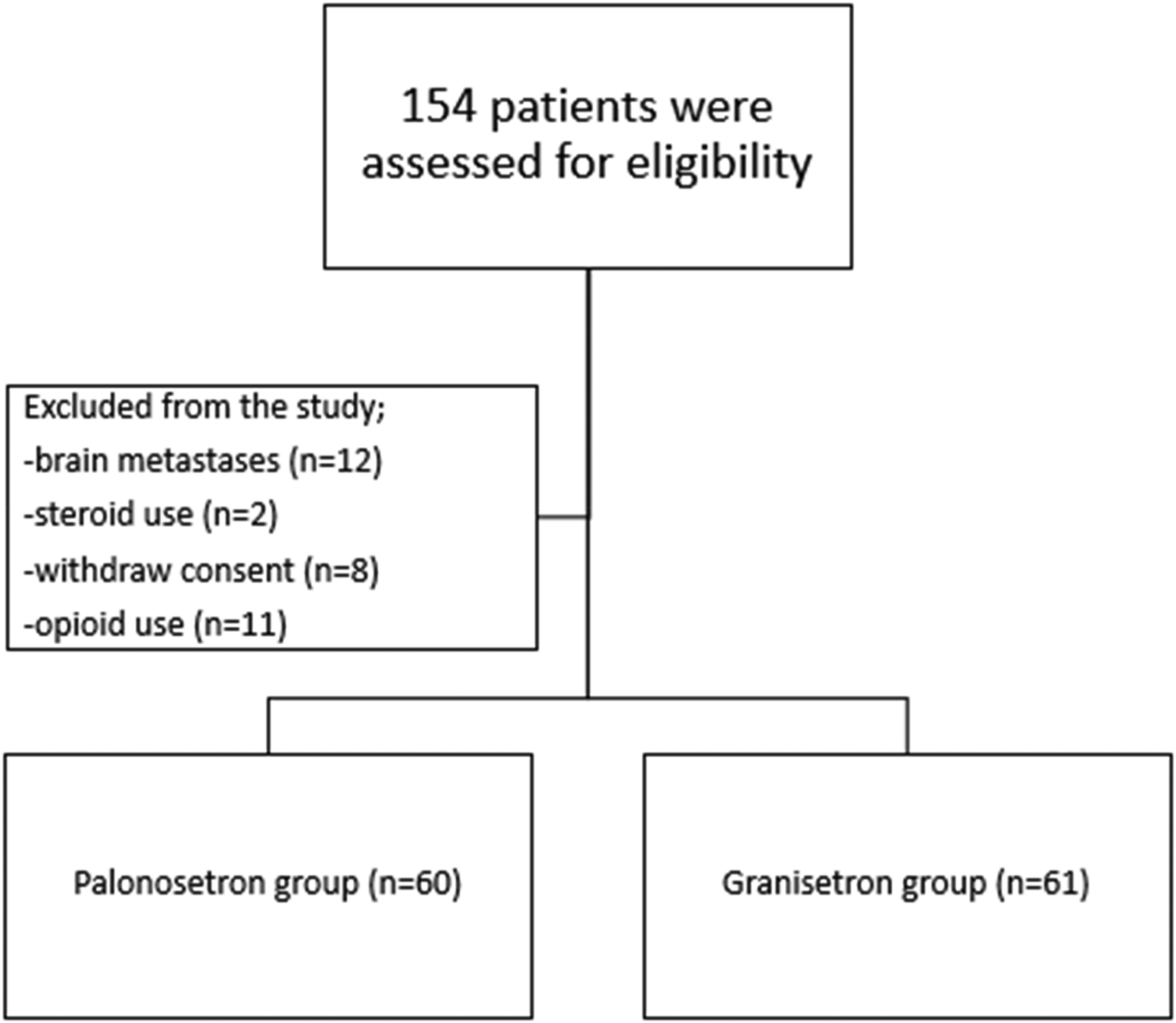
Flow chart of the study population.
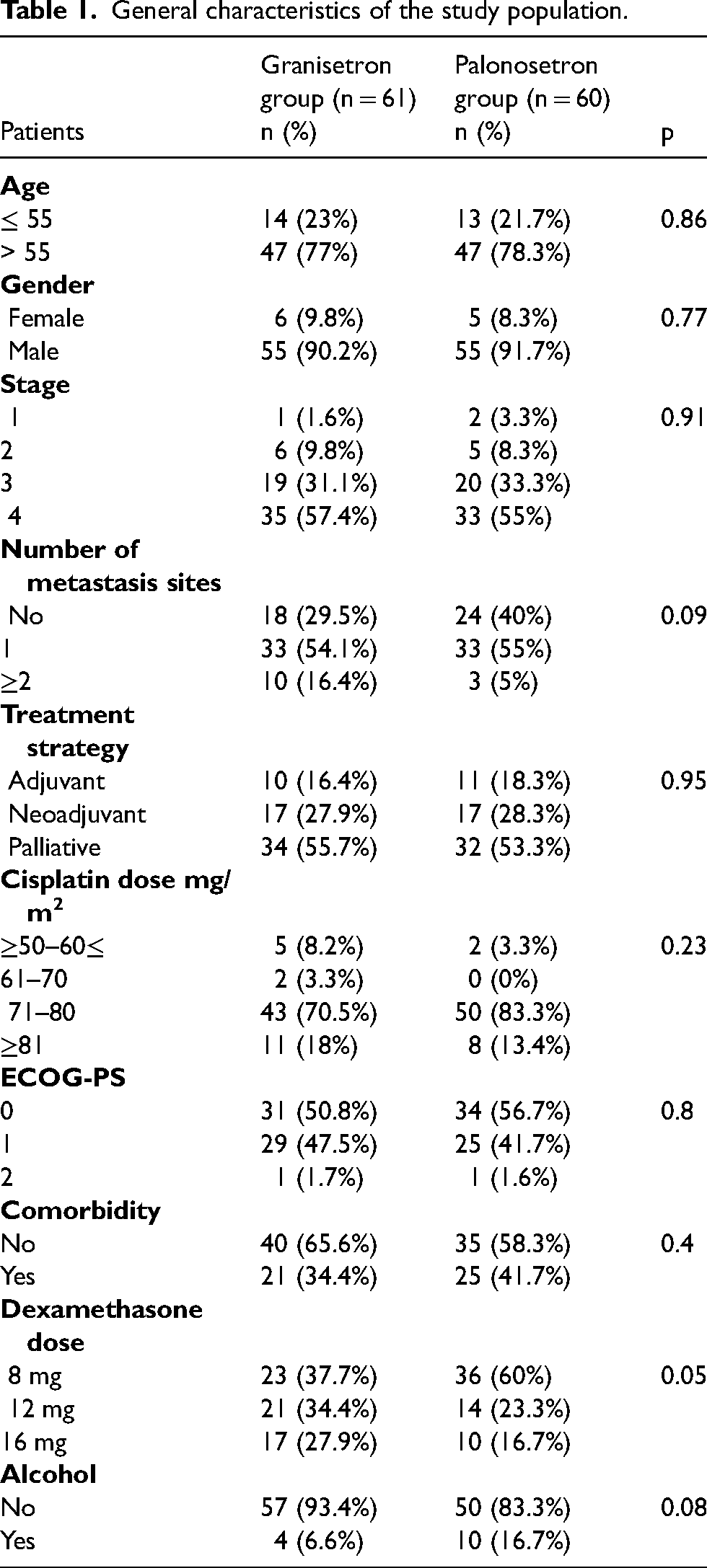
Sixty-one patients were in the granisetron group, and 60 patients were in the palonosetron group. The majority of patients were aged > 55 (77%-78%). Approximately 90% of the patients were men and those receiving chemotherapy for stage 3–4 disease in both groups. Cisplatin was used most frequently at 71–80 mg/m2 in both groups. While dexamethasone dose was most frequently preferred as 8 mg in anti-emetic prophylaxis (37.7% in the granisetron group, 60% in the palonosetron group; p = 0.05), 16 mg dose was used at the lowest rate in both groups. There was no statistically significant difference between the two groups regarding other patient characteristics, and there was a balanced distribution. (Table 1)
General characteristics of the study population.
The acute (88.5% vs. 91.7%, p = 0.56; respectively) and delayed vomiting (77% vs. 83.3%, p = 0.38; respectively) prevention rates were similar between granisetron and palonosetron. Although not statistically significant, the rate of nausea prevention in the acute phase was better in the granisetron group (70.4% vs. 56.7%, p = 0.11), while it was better with palonosetron group in the delayed phase (55.8% vs. 63.3%, p = 0.39). Rescue anti-emetic use rates of the patients were similar (29.5% vs. 28.3%, p = 0.88) in the two groups. (Table 2)
Comparison of Acute and Delayed Nausea-Vomiting between granisetron and palonosetron.
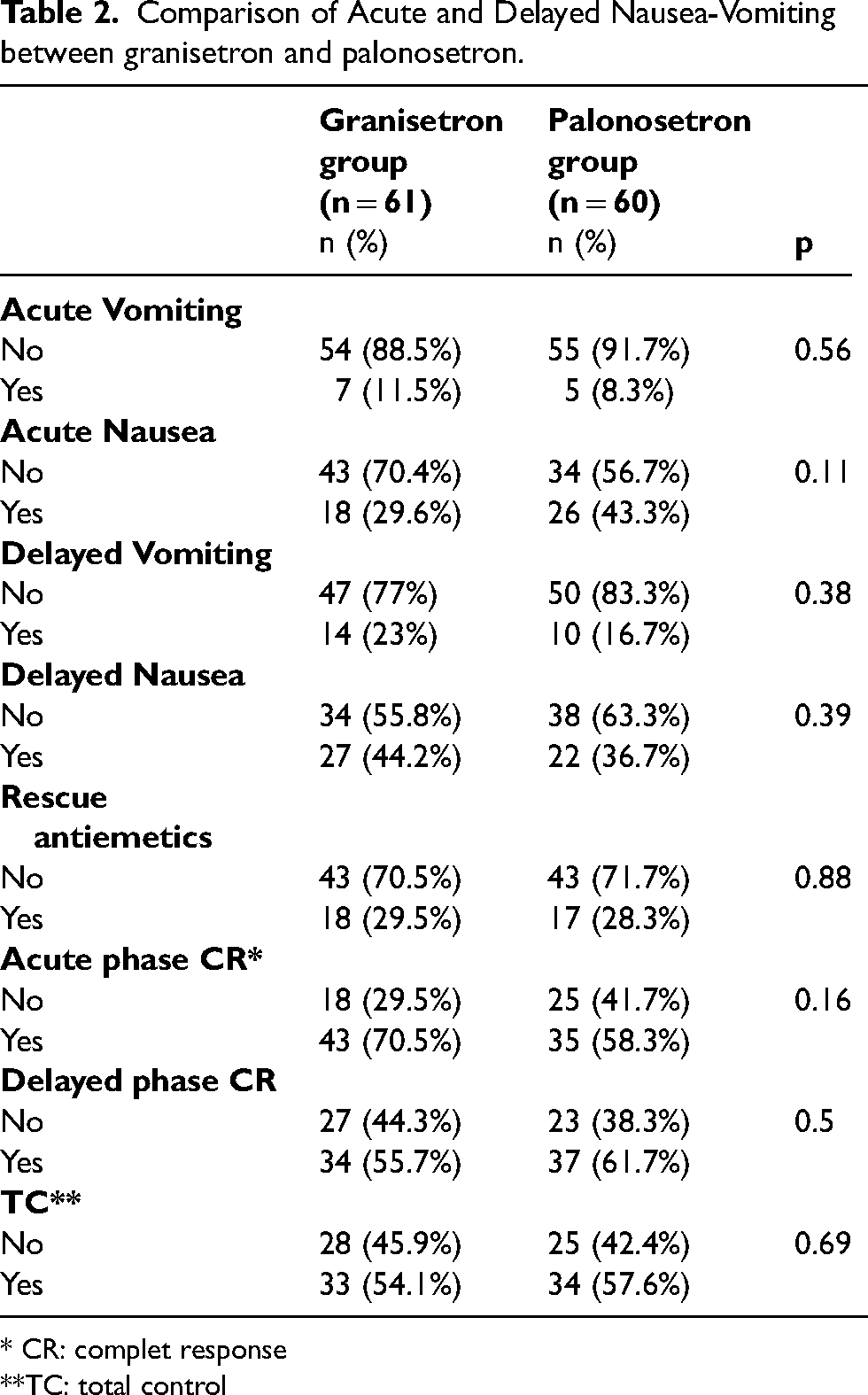
* CR: complet response
**TC: total control
Although granisetron provided greater CR than palonosetron in the acute phase (70.5% vs. 58.3%, p = 0.16; respectively), the CR rate in the delayed phase was better in the palonosetron group (55.7% vs. 61.7%, p = 0.5). These differences did not show statistical significance. TC rates were not significantly different between the groups (54.1% vs.57.6%, p = 0.69). (Table 2)
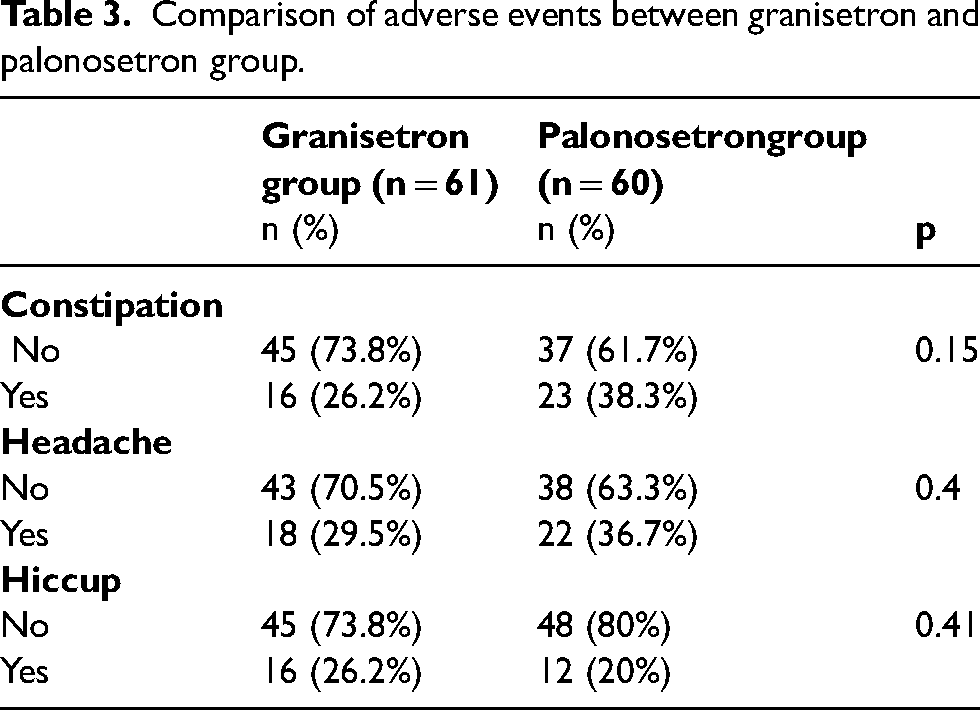
The rates of adverse events, including constipation, headache, and hiccup was not statistically significantly different between the two groups (p = 0.15, p = 0.4, p = 0.41, respectively). Constipation (38.3% vs. 26.2%; respectively) and headache (36.7% vs. 29.5%; respectively) were more common in the palonosetron group, while hiccup was more common in the granisetron group (26.2% vs. 20%, respectively). (Table 3)
Comparison of adverse events between granisetron and palonosetron group.
Discussion
In this study, which included only a homogeneous patients group with NSCLC, in the triplet anti-emetic prophylactic treatment with aprepitant and dexamethasone of cisplatin-based HEC, there was no statistically significant difference between granisetron and palonosetron in terms of CR and TC in preventing acute and delayed emesis.
Palonosetron and granisetron in a triple anti-emetic combination were compared for the first time in a non-inferiority study. 7 Patients with lung, breast, colorectal, and gastric cancer who received moderate emetogenic chemotherapy (MEC) or HEC were included in this study. Of this study group, 54% consisted of patients who had not previously received chemotherapy, remainig 44% of patients had received. Patients who received palonosetron prophylactically in the first cycle received granisetron in the second cycle or vice versa. When 0.25 mg palonosetron and 3 mg granisetron were compared in patients who received both MEC and HEC, CR and TC rates were found to be similar in preventing acute and delayed emesis.
Four prospective studies that conducted only on breast cancer patients,8–10 along with our previous article, 11 found no statistical difference between first and second-generation setrons in terms of both acute and delayed emesis control. In these studies, only one type of HEC regimen (anthracycline and cyclophosphamide-based chemo) has used. In the pilot study, 8 palonosetron was compared with ondansetron and in three other studies with granisetron.9–11 Palonosetron was used at a dose of 0.75 mg in two studies9,10 and 0.25 mg in the other two studies.8,11
The randomized a single-blind study 12 was performed in patients with bone or soft tissue sarcoma who received multiple-day of HEC. Three mg dose of granisetron twice daily for five days was compared with 0.75 mg palonosetron administered only on the first day in triplet anti-emetic prophylaxis. The acute phase CR rates were better in favor of palonosetron, but there was a numerical difference in favor of granisetron in the delayed and all phases. Also, the TC ratio was better in the palonosetron arm in the acute phase, but similar in the delayed phase. As a result of the study, the authors stated that there was no statistically significant difference between multi-day administration of granisetron and single-day palonosetron. They also underlined that triplet anti-emetic combinations provide very low TC (4.2% - 8.3%) in preventing emesis due to multi-day HEC applied in bone and soft tissue sarcoma compared to single-day HEC.
TRIPLE study, 6 considered a corner stone in this field, was performed in patients receiving cisplatin-based HEC for lung, head and neck, upper gastrointestinal tract, and other different primary localized cancers. They compared 1 mg of granisetron with 0.75 mg of palonosetron. In this study, for the first time, delayed CR (59.1% vs. 67.2%, p = 0.0142) and TC (40.7% vs. 47.6%, p = 0.0369) rates showed statistical significance in favor of palonosetron. But, acute CR rates were similar.
In a very recently published meta-analysis, 13 the efficacy of palonosetron and granisetron in both dual and triplet anti-emetic combinations was compared in patients receiving MEC and HEC. According to this meta-analysis which including the five studies comparing triplet antiemetic therapy mentioned above, palonosetron and granisetron were equally effective in preventing acute CINV, whereas response rates of palonosetron in the delayed phase were slightly higher than granisetron. Unlike the two studies including breast cancer patients, three of the five studies in the meta-analysis6,7,12 had some similar characteristics, which allowed for slightly better palonosetron results in the delayed period; In all three studies were including patients who received multiple-day of chemotherapy, and patients who have primary tumors of different localizations, and almost half of the patients had received prior chemotherapy particularly in the one study. Firstly, the definitions of acute and delayed emetic periods are even more ambiguous and intertwined in patients who receive multiple-day chemotherapy compared to those who receive single-day chemotherapy. 1 Secondly, the gastrointestinal tract is as sensitive to mechanical distension as chemotherapies, and these mechanical stimuli can cause 5-HT3 release and trigger vomiting. 14 Therefore, evaluating patients with gastrointestinal system cancer together with patients with other primary cancers may affect the results of study. Thirdly, because of the anticipatory emesis in patients who have received previously chemotherapy and experienced nausea/vomiting, emetic evaluation may not yield beneficial results in subsequent chemotherapy cycles. 1 In conclusion, the authors suggested that granisetron should be used in triple combination, since there was no significant difference between palonosetron and granisetron in HEC prophylaxis and it was more economical.
Our findings were consistent with those of the meta-analysis, and we have stated that similar to the meta-analysis, there is no difference between palonosetron and granisetron in the triple combination in the prevention of acute and delayed emesis. In the TRIPLE study, unlike our study and others, the control of delayed emesis was found to be significant in favor of palonosetron for the first time.
This meta-analysis also determined that palonosetron was better than granisetron in all phases of vomiting (but not only in the delayed period) in dual anti-emetic combination without NK-1 receptor inhibitors. A recent study 15 compared the palonosetron and granisetron in dual combination with dexamethasone in patients with breast and lung cancer receiving HEC. In the palonosetron arm, blood serum serotonin levels were higher due to greater and longer duration of irreversible binding to 5-HT3 receptors, and palonosetron was better than granisetron in inhibiting both acute and delayed emesis. The significant reduction in the level of substance P due to the crosstalk of palonosetron with NK-1 receptors which has been demonstrated in preclinical studies, did not show clinical relevance in this study. The substance P level was found only numerically lower in the palonosetron arm than in the granisetron. The idea that palonosetron actually inhibits delayed emesis due to substance P reduction is controversial and suggests that other factors may be responsible for this effect.
The main hypothesis of our study was that there would be no significant difference between first-generation 5-HT3RA and second-generation palonosetron when used together with NK-1 inhibitors. However, we did not expect that granisetron would provide better CINV control in the acute phase of emesis, even if it was not statistically significant. Also, there were non-significant trends favoring palonosetron in the delayed phase. Another critical point to keep in mind when comparing anti-emetic efficacy is that the pharmacodynamics as well as the pharmacokinetics of these drugs may differ. 14 All setrons except granisetron are metabolized in the liver by the CYP2D6 system. Because the CYP2D6 system shows frequent genetic polymorphism, the response to anti-emetic drugs may differ from individual to individual. In addition, although it is known that 5-HT4 receptors play an important role in the release of serotonin in the gastrointestinal tract, such as 5-HT3, its effect on CINV has not been sufficiently clarified yet. These and other unknown factors may explain the different results in studies comparing anti-emetics.
The most important limitations of our study are its non-randomized design and the application of the emesis assessment scale by different physicians in different centers. Additionally, different dexamethasone doses were used by different physicians in the centers. Although eight mg dexamethasone dose was used more in the palonosetron arm than in the granisetron arm, this difference was not statistically significant. Our study included a homogeneous patient group with NSCLC and patients who received first-time chemotherapy for just one day. Also, the patients with brain metastases and using opioid-derived drugs that could affect emetic measurement were excluded from the study.
Conclusions
We found no significant difference between palonosetron and granisetron in preventing acute and delayed emesis in triplet anti-emetic proflaxis of patients receiving cisplatin-based HEC for NSCLC. This result appears to be consistent with most studies, except for a few previous studies. NCCN and MASCC's current guidelines recommend using 5-HT3RA plus dexamethasone plus an NK-1 inhibitor and an olanzapine antiemetics combination in patients receiving HEC and they stated that there is no difference between 5-HT3RAs. For this reason, physicians can easily prefer the cheaper setron, which is more cost-effective, depending on the conditions of the country they live in.
Footnotes
Acknowledgments
We thank all the patients who participated in the study.
Author contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by IB, FI, LK, MK, AD, MKE, and MA. The first draft of the manuscript was written by MA and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval statement
Ethics approval (date 01 June 2018 and no 2018/160) was obtained from Afyon Kocatepe University local ethic committee.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
ORCID iDs
Patient consent
Informed consent was obtained from all individual participants included in the study.