
Abstract
Introduction
Equity, Diversity, and Inclusion (EDI) is gaining increased attention within all industries healthcare being no exception. The terminology Equity, Diversity, and Inclusion and its abbreviation EDI gained popularity in the early 2000's when varied socio-political factors prompted many organisations to examine EDI concepts and how to operationalise them. The growing diversity of our society requires cross-cultural inclusive approaches to increase equity and access to services.
Method
This unique research is community-led research supported by the British Oncology Pharmacy Association, in which the members of the BOPA community are equal partners to inform action on policies that address EDI. This research was a cross-sectional study involving an online survey of financial BOPA members.
Results
Demographic data was extracted, and the quotes were analysed for common themes. The majority of respondents were women, and the largest age group was between 34 and 44. The first cause of microaggressions identified by the respondents was of racial and ethnic origin, followed by marital status and religious nature. Participants described the lack of diversity in senior positions and the microaggressions experienced by those who hold leadership positions. Some participants described how some situations at work made them feel excluded or alienated. The impact of discrimination and bullying/microaggressions extended to patients was also reported.
Conclusion
Despite strategic directions encompassing this aspect, this research underscores the pressing need for more evidence on the lack of EDI in healthcare institutions. Our findings, located in the pharmacy oncology specialty, have identified the problem and highlighted the potential benefits of addressing it. More needs to be done in training and professional development to address unconscious bias and change behaviours.
Introduction
Very little evidence exists about healthcare professional's experiences and understanding of equity, diversity, and inclusion (EDI) principles in the workplace. The pharmacy profession has been quite discreet in acknowledging and responding to challenging behaviours related to the breach of EDI principles in the work environment. Crises such as the COVID-19 pandemic have brought to national attention the dire consequences of failing to provide accessible, equitable care for all individuals in our society. 1 Diversity is about similarities and differences among individuals that comprise personality and identity; equity is fair practices in access, opportunities, and advancement, and inclusion fosters a sense of value, respect, and empowerment in employees. 2
EDI is gaining increased attention within all industries healthcare being no exception. Universities seem to have led awareness and actions in the late 1960s when traditional social relations and educational practices were being challenged the world over; Carnegie Mellon University (in Pittsburgh, Pennsylvania, USA) started making significant changes in its organisation. 2 In the intervening years, the institution launched several programs with diversity as its goal. The terminology Equity, Diversity, and Inclusion and its abbreviation EDI gained popularity in the early 2000's when varied socio-political factors prompted many organisations to examine EDI concepts and how to operationalise them. The growing diversity of our society requires cross-cultural inclusive approaches to increase equity and access to services. The actual value of diversity has been increasingly understood and appreciated via data that matured in the 1990s and 2000s, mainly from the corporate world. 3 Workplace diversity training emerged in the mid-1960s following affirmative action and equal employment laws put in place around the globe. The principle of EDI is addressing inequities beyond racial and gender discrimination.
Many job seekers significantly consider a company's diversity when applying and this extends to various sectors: academia, pharmaceutical industry, and clinical workforce.4–6
There is a lack of research to enhance our understanding of the current climate specifically in pharmacy practice. In 2020, Patel et al. 1 were one of the pioneers that raised workforce issues in the context of EDI in a policy statement from the American Society of Clinical Oncology. Patel et al. recognised that achieving health equity among healthcare professionals requires efforts from all individuals, general public, policymakers, health systems, and other stakeholders. One of the recommendations to promote health equity describes the importance of promoting and improving cancer workforce diversity. Therefore, it is important to consider the experience and wellbeing of healthcare professionals within diverse environments in an effort to support sustainability and a healthy working environment for all. Patel et al. also highlighted the need to address institutional discrimination by facilitating open forums at meetings and webinars, and hence raising awareness and action that address health inequities.
This exploratory research was supported by the British Oncology Pharmacy Association (BOPA) executive committee, which established an EDI subcommittee in 2022 to focus on EDI as principles guiding the organisation's strategies and supporting its membership in an area of increasing significance for the healthcare industry. This work is community-led research in which the members of the BOPA community are equal partners to inform action on policies that address EDI. It focuses on understanding the membership awareness of EDI principles in their workplaces and gathering members’ stories to evidence inequalities and enable the committee to identify areas for training.
The survey results will be used to help healthcare institutions develop robust policies, not just training to address implicit bias. The results also assist collaboration with other organisations working in the same space.
Method
The Checklist for Reporting Results of Internet E- Surveys (CHERRIES checklist) was used to describe the adopted methodology. 7
This was a cross-sectional study involving an online survey of BOPA members.
Due to the dearth of literature exploring EDI in the pharmacy profession, a small working party, including a patient representative, designed a new instrument using human resources exemplars from business organisations. The tool is structured into four parts (40 questions): one exploring members’ EDI experiences at their current employing organisation using a 5-point Likert scale rating for the eleven statements; part two is related to BOPA as an association wanting to implement EDI, asking as well about topics for training and medium for the delivery (and will not be reported in this article), part three contains dimensions of diversity relevant to the study primarily age, gender identity, ethnicity, and secondary disability and region; and at the end part four is made up of two open-ended questions exploring EDI experiences as a witness and as personal lived experience. An option ‘prefer not to answer’ was used to avoid individuals skipping the question. The instrument provided quantitative and qualitative data aligned with the choice of a mixed-method design for enriched data collection and to provide context to the qualitative part.
Face and content validation were completed with an independent group from the EDI subcommittee and the BOPA executive committee, leading to four iterations. Face validation assessed whether the questions were valid to the participants. Content validation was performed by experts and assessed whether the survey contains questions which cover all aspects of the construct being measured.
A SurveyMonkey SM® survey was created and administered®. 8
The participants’ pool represented the financial members pharmacists and technicians working in community, academia, industry, and hospital settings. As this project was planned to be a descriptive study and not a representative one, the survey remained open for 4 months with five reminders sent to the membership by email and social media.
The survey was sent to the membership that was blinded by the EDI research working party. The online survey was disseminated before and after the 25th annual conference in Liverpool. The survey was closed in mid-December 2022. By answering the survey, the respondents provided consent.
The data was exported from SM® into Microsoft® Excel spreadsheets for analysis, after which the responses were deleted from SM® platform. The open comments were screened and analysed for common themes by two independent researchers. Descriptive statistics were used to analyse the responses to the close-ended questions.
Even though the whole EDI committee contributed to the design of the survey, a small BOPA task and finish working group was created to analyse the data and finalise the survey results. The group was formed of five members; they have reviewed and evaluated the data.
Ethics approval process following university governance and approval by the executive committee were sought and granted (number: H-2023-019).
Results
Ninety-one BOPA members participated in the study, representing 13.4% of the estimated current membership at the time. The response rate to all the questions is 94% across the questionnaire.
Table 1 presents the primary and secondary demographics of the sample and Figure 1 shows the age distribution of the respondents. Most respondents were women, and the largest age group was between 34 and 44.
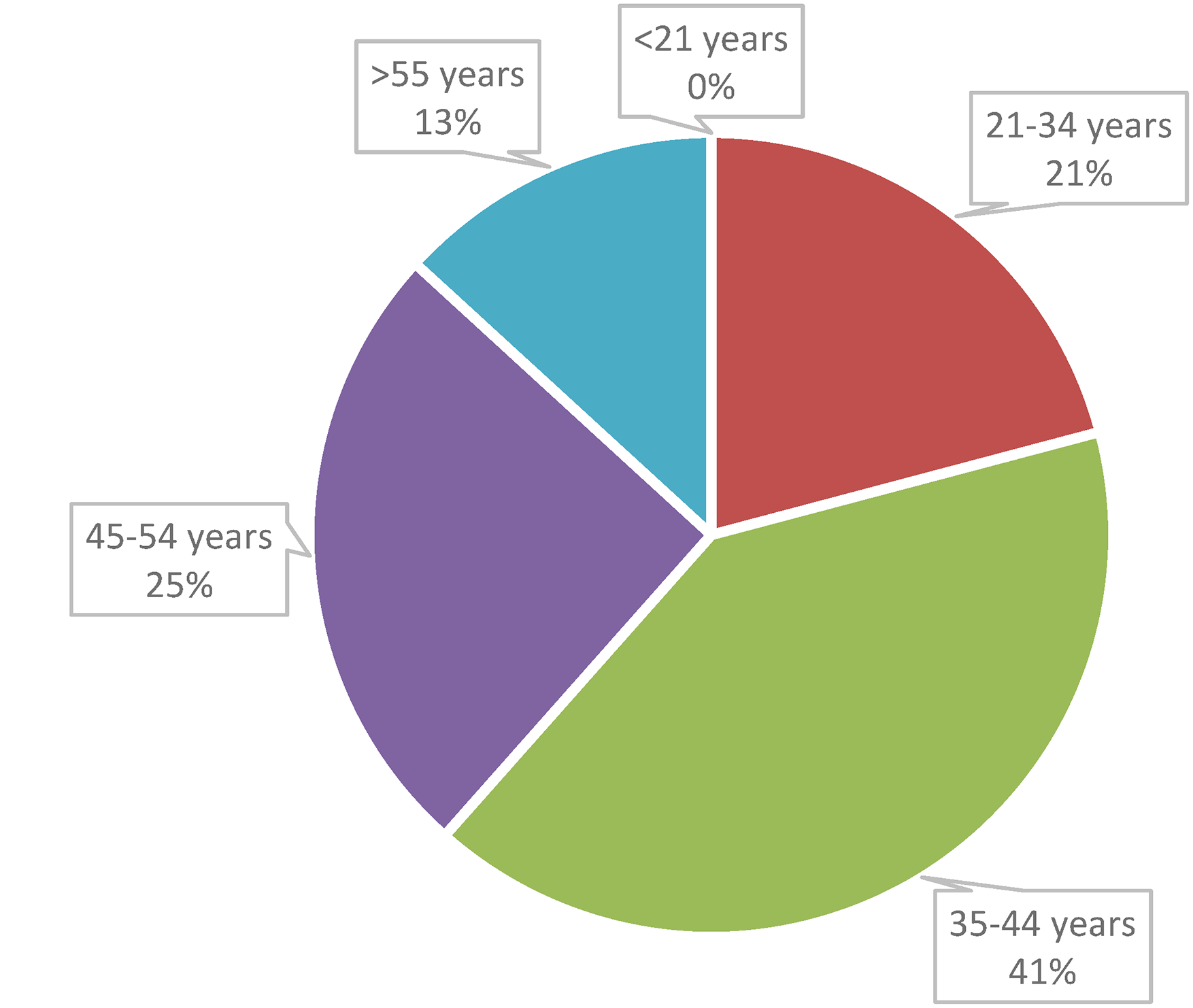
Distribution of respondents’ age.
Primary and secondary demographic and professional characteristics of surveyed BOPA members (when numbers do not add up to 91 – the difference represents ‘prefer not to say’ group).
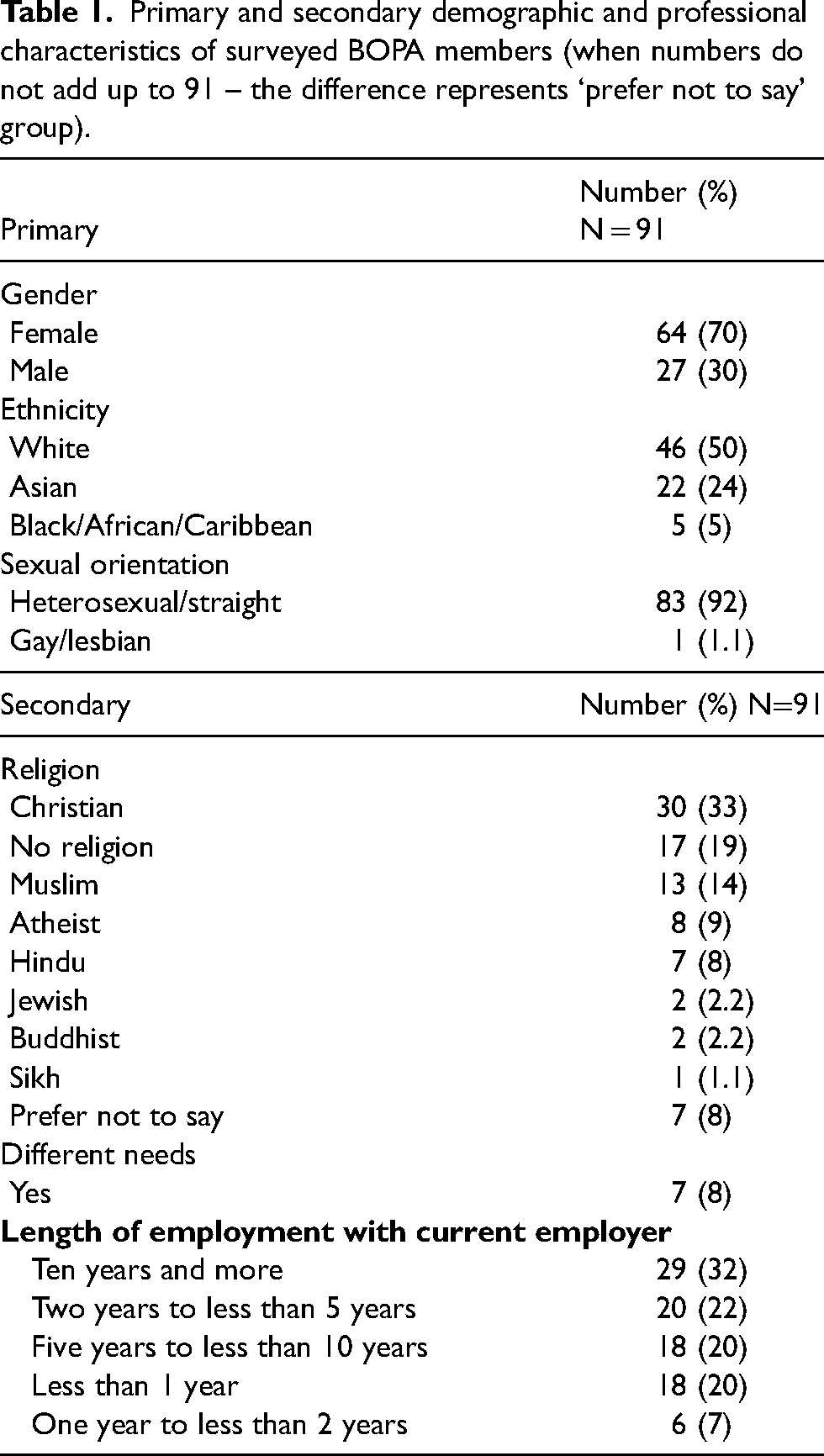
Participants of the survey were provided with male and female gender choices as well as male trans and female trans; thus there was an opportunity to self-identify as a different gender. There was also an option ‘prefer not to say’ when choosing gender rather than ‘unsure’, which has no statistical use. When choosing ‘prefer not to say’ it implies that the respondent has actually made a choice and a decision aligned with their values. Choices for race and sexual orientation were preset in the survey; however, respondents were allowed to say ‘other’ and asked to specify if not listed as well as given an option to choose ‘prefer not to say’. As part of the consultation undertaken for the survey design, the research team decided to drift from the legal definition of special needs or disability by using the terminology of different needs to allow respondents to identify if those differences were addressed in the context of the EDI principles.
Experiences with current employer
All respondents answered the questions relating to EDI experiences with the current employer with the highest agreement score pertaining to the statement ‘I believe the organisation will take appropriate action in response to incidents of discrimination and/or bias incidents’ and the highest disagreement related to the statement ‘This organisation has done an excellent job providing educational programs that promote diversity, equity and inclusion in the workplace’.
There was consistency in the answers with a low rate of disagreement (<9%).
Table 2 presents the participants’ rating on a Likert scale of 5 of statements exploring their experience of EDI as an employee.
Respondents rating on a Likert scale of 5 of statement regarding employment and EDI.
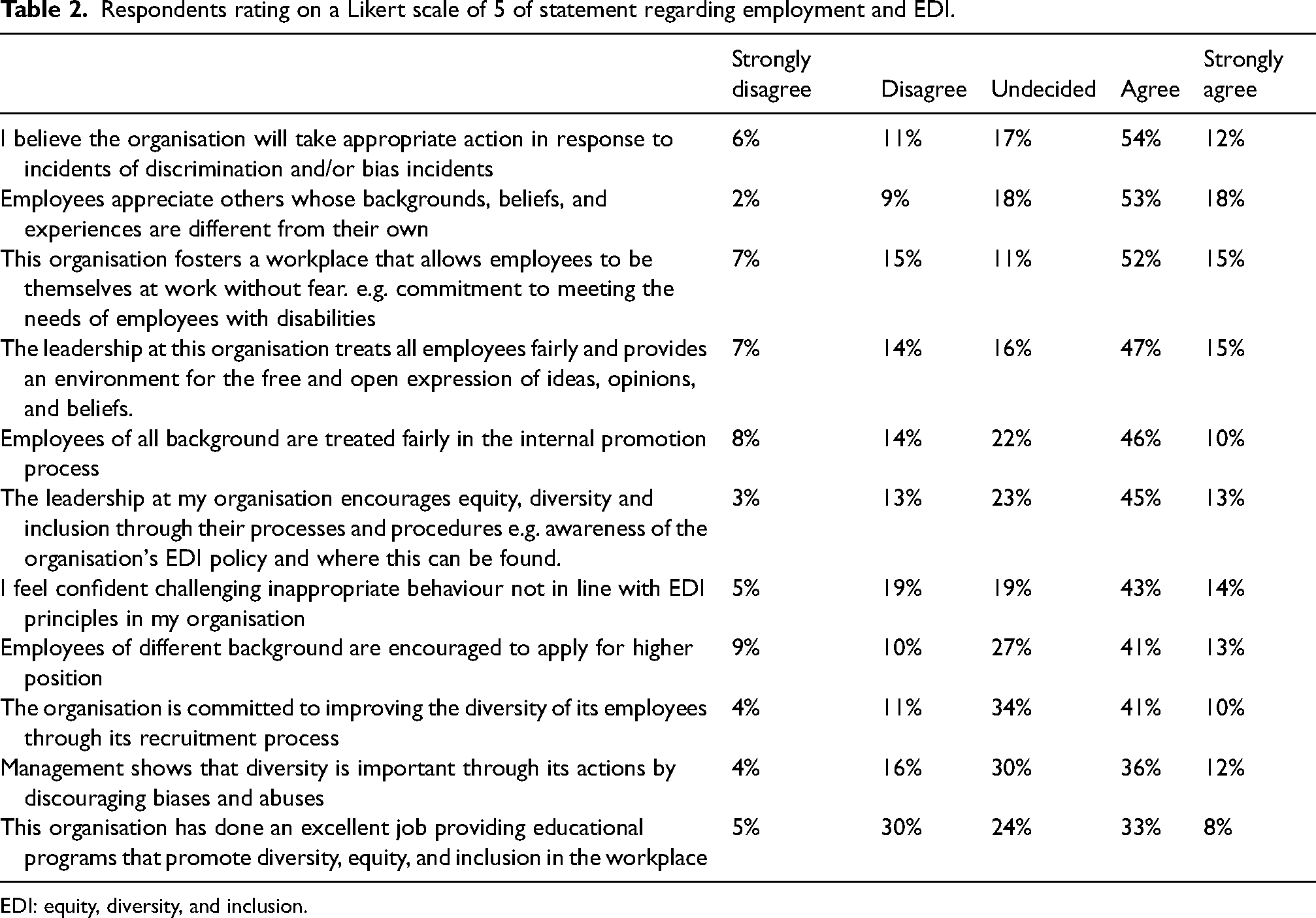
EDI: equity, diversity, and inclusion.
Of the eleven questions, nine (81%) rated between 50% and 70% for aggregated data ‘agree’ and ‘strongly agree’. In spite of that, 30–40% of all respondents did not agree (strongly agree and disagree) with these statements.
The ‘neither agree nor disagree’ responses vary between 11% and 34%, reflecting that some individuals might have heard of organisational processes but are unsure how EDI policies are implemented and how recruitment processes are fair and transparent. These comments will be evidenced in the analysis of the lived experiences comments.
Two questions of interest have a less-than-average agreement rating; ‘This organisation has done an excellent job providing educational programs that promote diversity, equity and inclusion in the workplace’. with only ‘Management shows that diversity is important through its actions by discouraging biases and abuses’.
And,
Over half of the respondents (56%) consider recruitment processes as ‘fair’ and that promotion on merit is maintained in the organisations; ‘employees of different backgrounds are treated fairly in the internal promotion process’.
Sixty-seven per cent of the respondents indicated that ‘their organisation will take appropriate action in response to discrimination and bias incidents’.
When asked about negative experiences relating to ‘discrimination’, the answers were balanced, with 45% (n = 41) responding YES and 49% (n = 45) NO. Five members (5%) preferred not to answer the question. In the following question, microaggressions in the workplace were explored, and 41% (n = 37) responded YES and 55% (n = 50) NO. Four people (4%) preferred not to answer the question. When asked about the perceived reasons for the microaggression, 56% of the respondents (n = 33/59) believe that the origin of the microaggression(s) is racial/ethnic. At the same time, 15% described the origins as due to marital status and religious beliefs. The other causes were sexual orientation (7%) and disability (7%), (Figure 2).
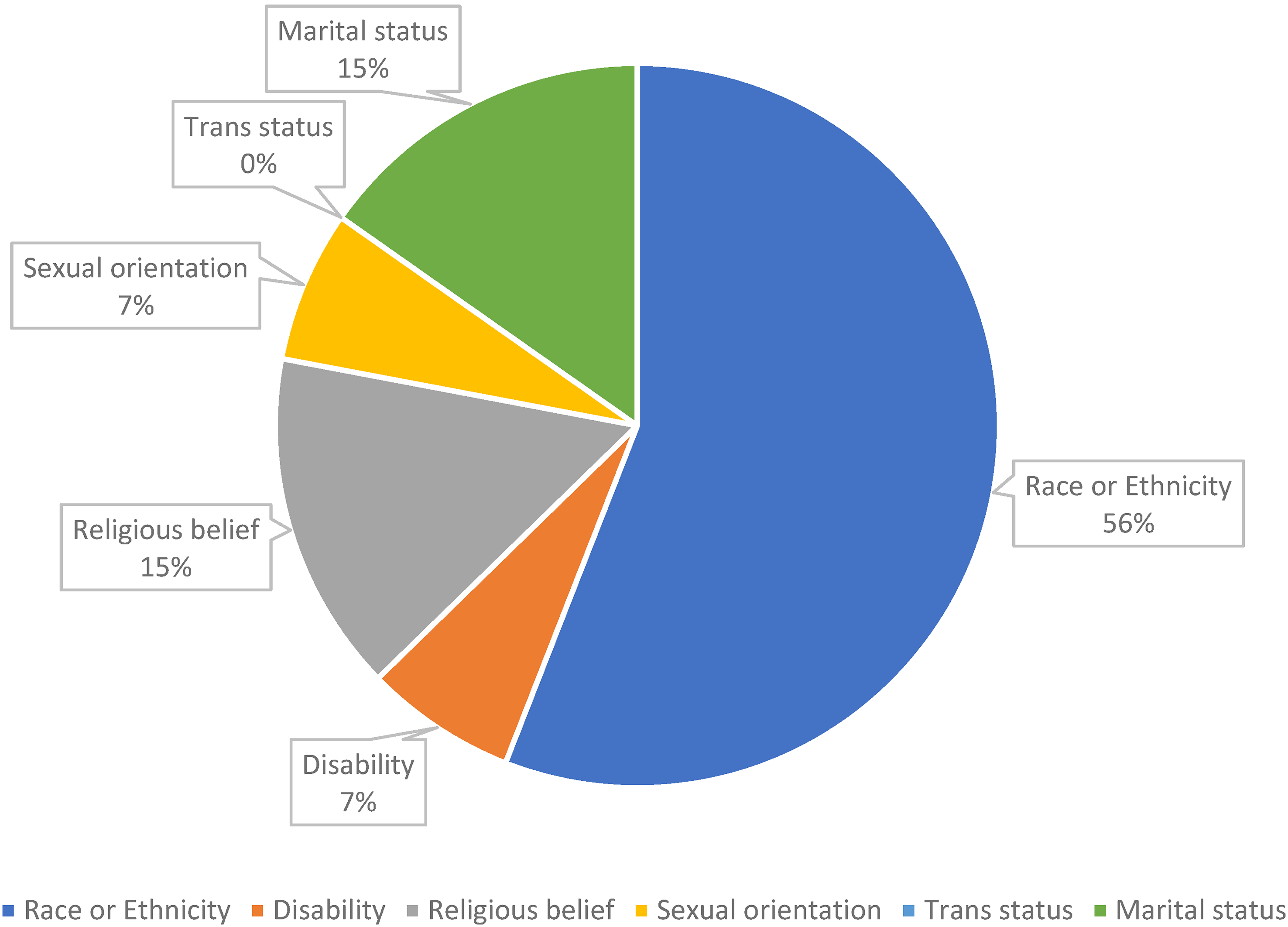
Responses of possible microaggressions reasons.
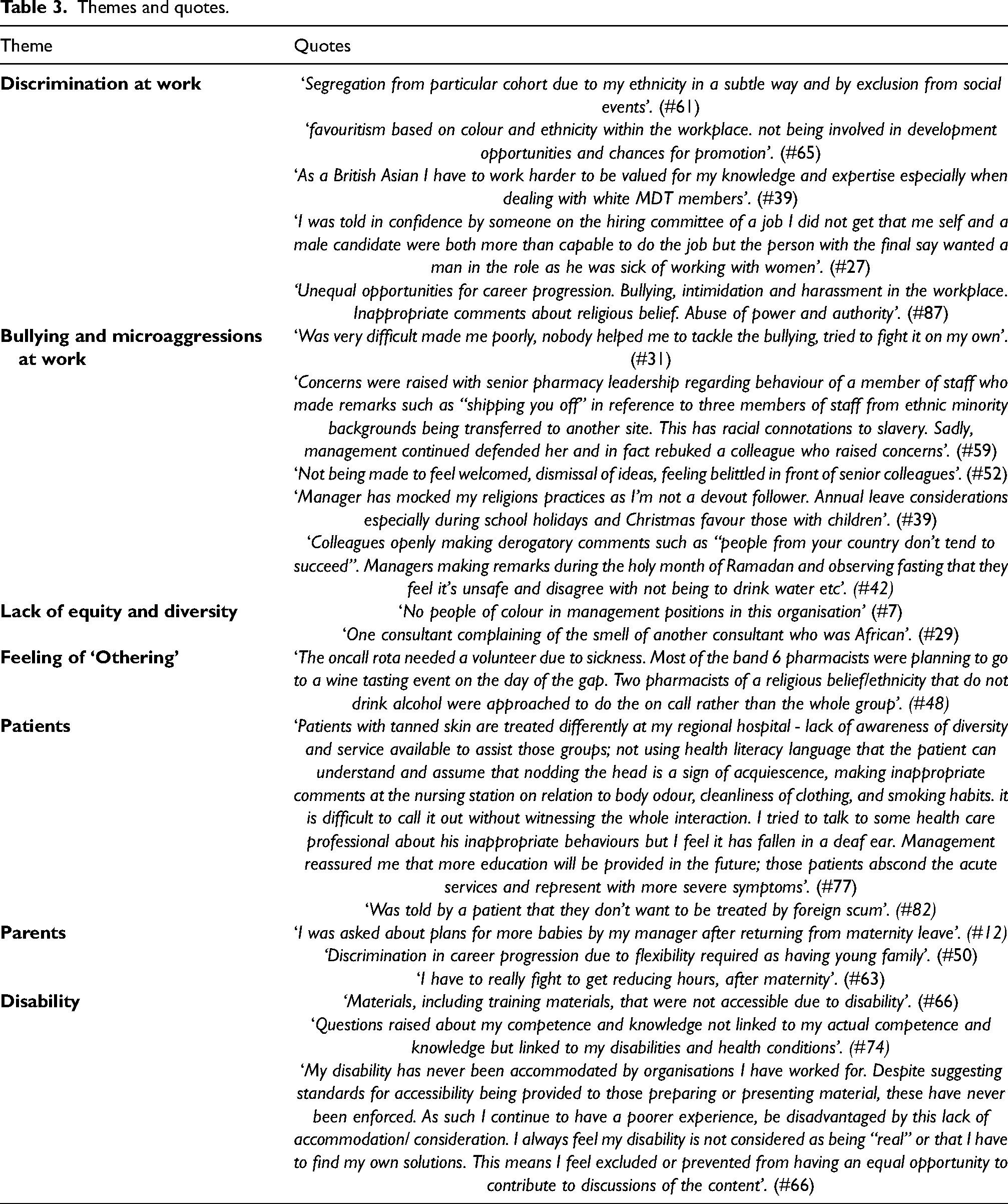
Data from the open responses enriched the quantitative findings and provided context. Of the participants who added comments, most reported a negative work experience. Table 2 provides a selection of quotes that further represent the identified themes.
Discrimination at work
Participants experienced discrimination at work ranging in intensity, frequency, and impact. Some of the discrimination related to career development opportunities and recruitment while others impacted the feeling of belonging to the team.
Bullying and microaggressions at work
Participants openly shared their experience of bullying and microaggressions relating to gender, ethnicity, religion, region, and marital status and whether they have a young family.
They also expressed their frustration with the lack of support and the dismissive culture and not acting upon complaints.
Lack of equity and diversity
Participants described the lack of diversity in senior positions and the microaggressions experienced by those who hold leadership positions.
Feeling of othering
Some participants described how some situations at work made them feel excluded or alienated.
Patients
Even though this study aimed to explore staff experiences, a theme emerged among several responses, explaining that patients also have experienced microaggressions and were treated differently because of their skin colour or foreign accent.
Parents
Participants who were parents described the difficulties and discrimination encountered when trying to juggle the responsibilities of a young family and their professional aspirations.
Disability
Participants with additional needs described the inequity that results from lack of adjustments at work (Table 3).
Themes and quotes.
Conclusions
This is the first study to explore the experience of oncology pharmacy professionals with EDI. The survey responses provided a detailed insight into the reality of EDI for oncology health pharmacy professionals.
Microaggressions/bullying in the workplace
One of the major findings in this survey was the fact that 41% of participants indicated they have experienced microaggressions/bullying in their workplace. Race/ethnicity/religion were the main reasons: this is similarly reflected in the following two studies. In 2021, Alsharif et al. 9 reported an exploratory study to assess the experience of pharmacy educators of Arabic heritage. As members of the Arab American Pharmacy Educators (AAPE) with EDI in the workplace, the respondents (N = 31) reported experiencing microaggressions and discrimination at work, which is their highest rating on the Likert scale 1 to 5. Some respondents ranked third as perceived racism affecting their performance at work. These results are very similar to the findings of this study, where racism and ethnicity were the two major reasons respondents identified as causes for microaggression. Alsharif et al. stated that being of Muslim religion (pushed to the forefront with 9/11) is impeding professional progression and a perceived source of racism. 9 The other study investigated the experience of pharmacy students. Avant et al. 10 explored pharmacy students’ microaggressions and their lived experiences using one-to-one interviews (N = 13). Half were white, with three Black, two Asian and one multiracial student. The dominant theme was the ‘othering feeling’; this aspect was reported by the respondents of this research as well. The students also reported the pervasiveness of microaggressions, often disguised as jokes. Similarly, our study highlighted the same behaviours reported by the respondents. Avant et al.’s 10 findings highlighted that students in pharmacy, similarly to practising pharmacists, are unsure of how to address and mitigate microaggressions. It is fair to recognise that all healthcare disciplines hold some form of implicit bias, with many of them unaware of its impact on others.
Another prominent feature was being a parent /marital status. These groups of individuals felt like being passed over and not considered for all available opportunities. Looking at the survey respondent's demographic details, we can see that females formed the majority (70%) of participants, which is not surprising as pharmacy workforce globally is dominated by women. 11 Our results showed that being female, married, having a child/children and of a different ethnical background hugely increases the chances of being discriminated in the workplace. Even though these are the exact protected characteristics defined by the Equality Act 2010 and it is illegal to be discriminated against them by law. 12
Unsupportive workplaces
It was interesting to note that a significant proportion of the participants did not perceive their organisation as supportive when they experience microaggressions and bullying. Therefore, it is recommended that organisations invest time and resources to understand the experience of their employees and to implement interventions where needed such as educations and training. Diversity training has been proven successful when utilising personal awareness, intergroup dialogue, and perceptive-taking. 10 However, some argue that that is not enough and that training in cultural competence and humility is needed as these will allow trainees the reflexivity needed to change behaviour. 13
Experiential data from frontline healthcare practitioners is imperative in understanding the context of the many facets EDI can take in complex institutions and highly regulated work environments, such as delivering high-quality oncology services. ‘Health care is built on science, but its execution is through, among and between human beings with needs and preferences, fears and insecurities, purpose and aspirations and a wish to something greater’. 14 The literature review using the terms ‘pharmacy’, ‘pharmacy practice’, or ‘ pharmacist’ and ‘diversity’, ‘equity’, and ‘inclusion’ resulted in articles addressing EDI mostly in pharmacy education (students and academic staff) and are situated in the United States, highlighting the lack of research in this field and need to understand pharmacy professionals’ experiences of EDI, especially in the United Kingdom.
Patient care
The impact of discrimination and bullying/microaggressions extended to patients who were both affected by it and were the perpetrators. In 2010, The American Cancer Society published a new strategy, demonstrating how knowledge of culture can be used at each stage of cancer care to address patient diversity and ensure health equity. This new strategy requires culturally based education, training, and restructuring of the healthcare system. 15 The World Health Organisation (WHO) has also made recommendations on what is required to close the inequity gap in cancer care through action on social determinants of health. Seminal works have been published since 2003 by Wilkinson and Marmot on the importance of addressing those factors if any change was to be expected. 16 There is a need for more exploratory research on the impact of EDI and how care is delivered to patients and how patients, in turn, perceive their care as this relates to their perceived wellbeing and sense of responsibility to social justice. Social justice within the context of pharmacy could be described as an essential moral requisite, encompassing not only fair and equal access to treatments for all patients, but also cultural competence of pharmacy workforce. Social justice in healthcare is currently undergoing a major transformation, as our society recognises the need for dismantling inequity and developing safe, supportive, and inclusive working environments. 17 Cultural competency is the ability to collaborate effectively with individuals from different cultures, and such competence improves healthcare experiences and outcomes for a diverse patient population. Cultural humility is another concept used in healthcare that underpins respect and understanding of different cultures while recognising our own cultural biases. As ‘healthcare providers, we cannot be competent in another individual/patient's culture, rather, we should strive for humility’.
Despite strategic directions encompassing this aspect, this research addresses the need for more evidence on the lack of EDI in healthcare institutions. Our findings in the pharmacy oncology specialty have highlighted that more needs to be done in training and professional development to address unconscious bias and change behaviours. Experts should lead training provisions with a demonstrated track record of producing transformative outcomes or those who have examined their own ideas and feelings regarding racism and its intersections with other marginalised identity domains.
Limitations of the study
The reasons for low response rate could only be speculated. Historically, BOPA research subcommittee has indicated that survey response rates fluctuate between 10 and 20% and the topic of the survey very often influences the response rate. Our survey's response rate was 13%, which was within the average response rates. There could be a myriad of reasons behind such a low response rate, such as staff being exhausted from working within already financially and morally stretched NHS, lack of time, having other priorities to attend to and simply becoming disengaged from any additional tasks. Another possible reason for low response rates could be how surveys are being promoted, which is usually via social media and emails, so if the BOPA member has opted out to receive emails and is not particularly active on social media-this could potentially reduce the response rate dramatically, as essentially only those members who have opted in to receive emails from BOPA would be a true representative of a survey sample.
The low response rate also shows an urgent need to educate employees on EDI and raise awareness. Some NHS Trusts are already starting to include EDI training as part of their mandatory training; however, there is a risk that this training will become just another ‘tick box’ exercise, being completed without much thought or effort and often using online delivery. Any cultural change challenges our attitudes and requires mentality shifting and organisations’ understanding that one size does not fit all. Collaborative efforts are required from everyone involved in delivering healthcare services to make sustainable changes in how we provide our services and communicate with patients.
The knowledge gained in the context of pharmacists practising in oncology in the United Kingdom is not intended to create generalisable knowledge as it is discipline-specific. However, health care is provided by humans to other humans with larger systems and structural discrimination through institutional practices and policies that explicitly or implicitly differentially impact, or harm, non-dominant groups.
Footnotes
Acknowledgements
The authors want to acknowledge the British Oncology Pharmacists Association for the support they provided in undertaking this work. The authors also want to acknowledge Stewart O’Callaghan, consumer representative for his insights and active contribution to the research. Finally the authors want to acknowledge the BOPA members, respondents to the questionnaire, for their contributions and shared lived experiences that will enable progressing the EDI agenda for the BOPA members, the consumers and the Pharmacy Oncology specialty practice group national and internationally.
Authors’ contributions
Authors PD and SNG design the study, PD requested ethics approval for the study, Authors PD and SNG have drafted the article and all co-authors have contributed to data collection interpretation and analysis, and all authors reviewed the final draft manuscript.
Availability of data and materials
All data will be made available as per guidance of the journal and upon request to the principal author.
Consent for publication
All authors nominated have consented for the research to be published.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval and consent to participate
This research is compliant with the Declaration of Helsinki when conduction human research. The clearance was sought from the University of Adelaide Human Ethics committee (H-2023–019) where the principal author was working at the time when the research was discussed and protocol drafted.
Funding
No funding has been sought for this research except the time allocated by respective organisations in kind to undertake this research.