
Abstract
Introduction
The increasing incidence of cancer and capacity for cancer care in Ethiopia has led to an upsurge in chemotherapy use in the country; however, studies indicate that there is a gap in the safe handling of chemotherapy by healthcare workers. There exists a need to understand if such unsafe practices occur in Ethiopia and, if so, which areas along the chemotherapy life cycle need the most improvement.
Methods
This study utilized a multi-method design through an online survey administered to health care professionals and evaluative site visits of eight cancer units in Addis Ababa, Ethiopia to understand the current conditions of chemotherapy handling. In addition, a survey was conducted among Ethiopian health care professionals from across the country.
Results
Fifty-five percent of survey participants disagreed or strongly disagreed that there are systems in place to identify, prevent, and address chemotherapy hazards in their workplace, and 71% of respondents denied having an active and effective health and safety committee and/or worker health and safety representative where they work. At evaluative site visits, only 30% of health care workers met the minimum guidelines for proper hand hygiene, and 20% of health care workers used adequate Personal Protective Equipment according to guidelines across the chemotherapy lifecycle.
Conclusions
Results of this study indicate an urgent need for implementation of evidence-based interventions to improve chemotherapy handling in Ethiopia so that all patients and health care workers are protected from the hazardous toxicities of these drugs.
Introduction
With an estimated cancer incidence of 60,960 cases per year in Ethiopia, chemotherapy administration is both frequent and critically important to cancer outcomes. 1 The incidence of cancer in Ethiopia has grown by 32% from 2010 to 2019, indicating an expanding need for chemotherapeutic drugs in the country. 2 Chemotherapeutic drugs can exert acute and long-term toxicity and can have adverse effects on reproduction and development of the healthcare workforce 3 including an increased risk of cancer and chromosomal abnormalities, a result of the mutagenic, carcinogenic, and other toxic properties which these drugs possess.4,5 Past studies have shown the risk of chemotherapy exposure on pregnant individuals, including a 94% increased risk of spontaneous abortions in pregnant nurses who handle such drugs during the first trimester.6,7 Even in resource abundant environments, constructing safe and efficient healthcare infrastructures for chemotherapy handling is difficult to achieve. In low- and middle-income countries (LMICs) like Ethiopia, building a safe system for chemotherapy handling is even more challenging but equally as important to both patient and healthcare workforce safety.
National and international standards have been published to guide the safe preparation, administration, handling, storage, and waste disposal of chemotherapeutic drugs; however—as evidenced by published studies—safe handling practices are absent or deficient in many healthcare settings in Ethiopia. A study of oncology nurses in tertiary teaching hospitals in Ethiopia revealed that only 31% of participants received training on cytotoxic drug safe handling and proper utilization of Personal Protective Equipment (PPE) at their workplace. 8 At the University of Gondar Specialized Hospital, 70% of personnel working with chemotherapeutic drugs reported no availability of PPE, and 62% of participants had poor practice of chemotherapy safe handling. 9 Yet another Ethiopian study at a single site reported having only 8 of the 23 required supplies for proper chemotherapeutic drug management, a finding congruent with several other studies suggesting limited resources for safe handling practices. 10 Waste disposal appears to be another point of frequent exposure in Ethiopia with Tekle et al. finding only about 40% of public hospital waste handlers safely managing hazardous waste commonly containing chemotherapeutic drugs. 11
The short- and long-term toxicity of chemotherapy provides a significant threat to the Ethiopian oncology healthcare workforce. Understanding the established chemotherapy safe handling protocols, and lack thereof, will point to targets for improvement and possible interventions to reduce chemotherapeutic drug exposure. Our team formulated a comprehensive survey and checklist which evaluated the workforce's perception of workplace safety, policies, and procedures related to chemotherapy handling across Ethiopian public and private health centers. While past projects have set out to evaluate the standard of chemotherapy handling in Ethiopia, this study has analyzed both individual healthcare worker perceptions and system-level processes related to chemotherapy handling.
Methods
We utilized a multi-method design which included surveys of health care workers who handle chemotherapy and evaluative site visits of four health centers (eight cancer units in total) offering cancer care in Addis Ababa, Ethiopia; each are described below.
Survey
Study design
An online survey was circulated via Ethiopian oncology professional listservs to providers working in an array of cancer care professions (e.g. nurses, oncologists). The survey targeted the perceptions of chemotherapy safe handling among providers in Ethiopia broadly, rather than focusing on the specific healthcare facility in which they work. The survey, adapted from the Institute of Work and Health's occupational health and safety survey, was delivered on the Qualtrics XM platform. 12 Survey questions were grouped into three major categories: workplace hazards, workplace policies and procedures, and participation in occupational health and safety. Prior to answering questions, responders were informed of the survey's goals and their rights as research participants and confirmed their consent to participate in the study.
Data analysis
A modified Likert scale (1 = strongly disagree, 5 = strongly agree, 3 = do not know/would rather not say) was used to measure participants’ perspectives about workplace hazards, workplace policies and procedures, and participation in occupational health and safety. Survey responses were included in the final analysis if at least one of these items was answered. The modified Likert scale answers were averaged to determine the mean response by participants, and percentages for each response were calculated.
Evaluative site visits
Study design
Evaluative site visits were conducted at four health centers offering cancer care in Addis Ababa, Ethiopia. Evaluators observed preparation, transport, administration, and disposal of chemotherapeutic drugs, referred to as the “chemotherapy lifecycle” in this study, and led semi-structured interviews guided by a checklist to gain a perspective of the overall system in which chemotherapy is prepared and administered. The checklist specifically analyzed each site's processes, guidelines, and infrastructure using questions based on the Pan American Health Organization's (PAHO) safe handling guidelines for safety recommendations throughout the life cycle of chemotherapeutic drugs. 13 Screening questions assessed aspects of safety at each chemotherapy life cycle stage, such as use of PPE, procedures, and availability of spill kits. The full list of checklist questions is in Appendix A. Interviews were conducted in English, and translation to Amharic was performed when necessary.
Subjects
Participating facilities were located in Addis Ababa and were contacted in advance to gain consent for evaluation of the chemotherapy life cycle. The site evaluations were completed at four health centers in Ethiopia. At one of these sites, Tikur Anbessa Specialized Hospital (TASH), we conducted five site evaluations across different cancer units for a total of eight evaluative site visits. The selected hospitals included both private and public hospitals with a range from 224 to 50,000 patients per month. The full characterization of the hospitals included can be seen in Appendix B. The site visits were conducted in-person by members of the study team in March of 2023. Three different interviewers completed observations and semi-structured interviews guided by the checklist. Both the survey and site evaluations were conducted in accordance with the guidelines of the Declaration of Helsinki.
Data analysis
Thematic content analysis was performed on observational findings and qualitative interviews to assess the quality of the system in which chemotherapy was being handled. For further simplification, each qualitative answer to the questions on the checklist were coded as “yes,” “no,” or “unknown” with some answers having expanded explanations. To better describe the results from the site evaluations, a priori, the questions from the checklist were categorized into themes (Table 1).
Checklist themes and definitions.
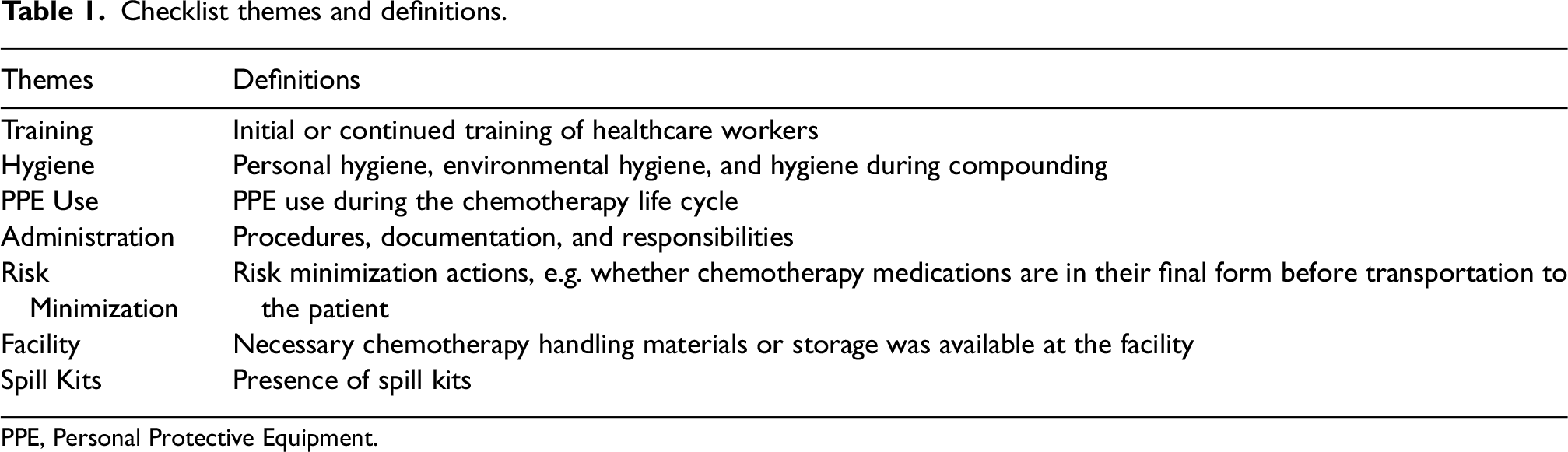
PPE, Personal Protective Equipment.
Results
Survey
A total of 40 providers responded to the survey (3 physicians, 24 pharmacists, 10 nurses, and 3 other professions or unknown). Thirty-eight percent (n = 14/37) of respondents interacted with chemotherapeutic drugs daily and 29% (n = 10/35) of respondents performed work tasks or used work methods that they were not familiar with every day. Denominators vary across survey questions because respondents were not required to answer all questions.
When asked if there are systems in place to identify, prevent, and deal with chemotherapy hazards at work, 55% (n = 21/38) of respondents disagreed or strongly disagreed. Sixty-six percent (n = 23/35) of participants disagreed or strongly disagreed that incidents and accidents involving chemotherapy are investigated quickly in order to improve health and safety at their workplace. Seventy-one percent (n = 25/35) of respondents denied having an active and effective health and safety committee and/or worker health and safety representative where they work. Continued analysis of survey results is located in Table 2 with mean Likert scale responses (strongly agree = 5, strongly disagree = 1) and percentages displayed for each question. The full breakdown of survey responses is in Appendix D.
Survey reponses Likert scale means.
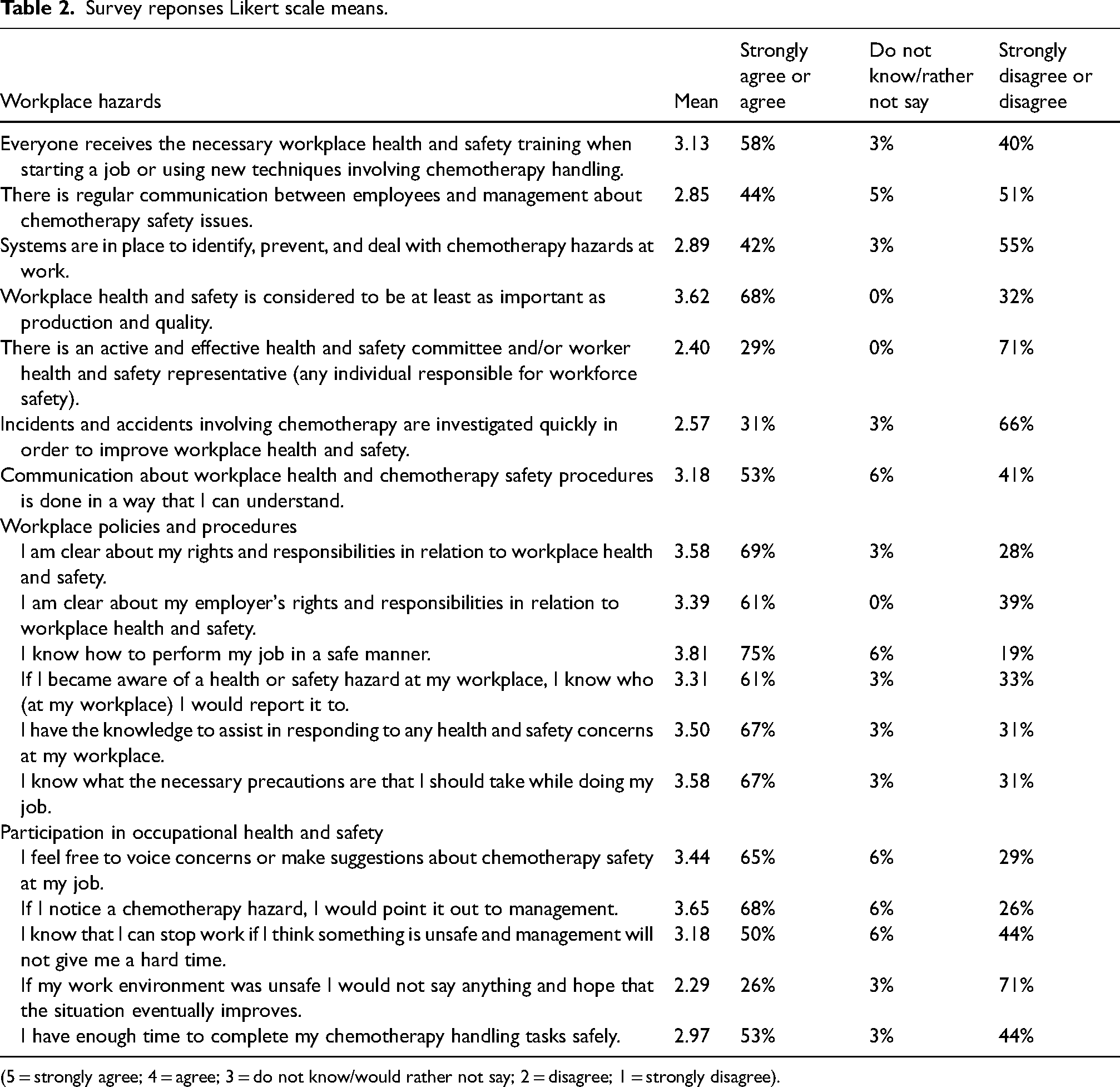
(5 = strongly agree; 4 = agree; 3 = do not know/would rather not say; 2 = disagree; 1 = strongly disagree).
Evaluative site visit
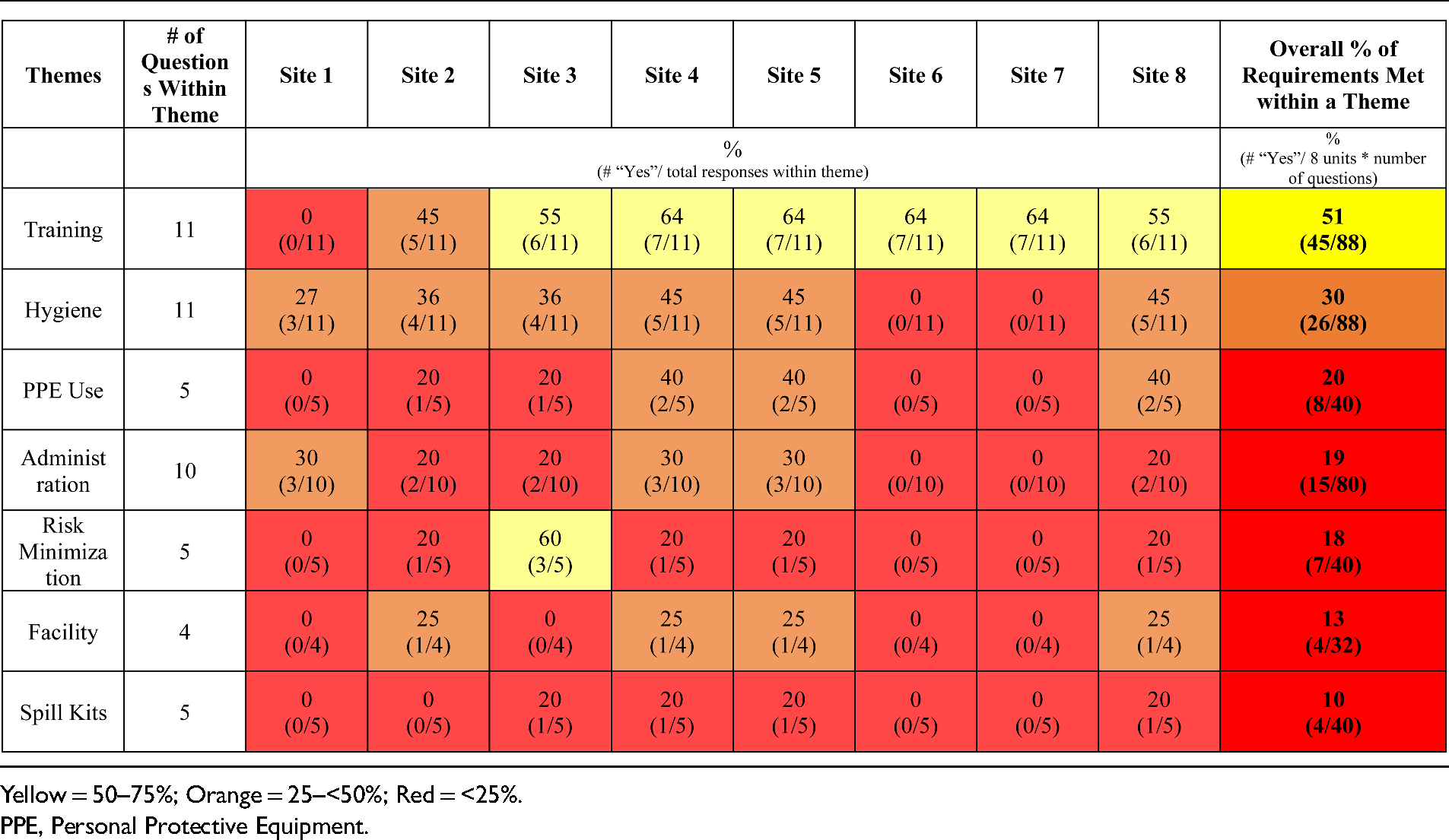
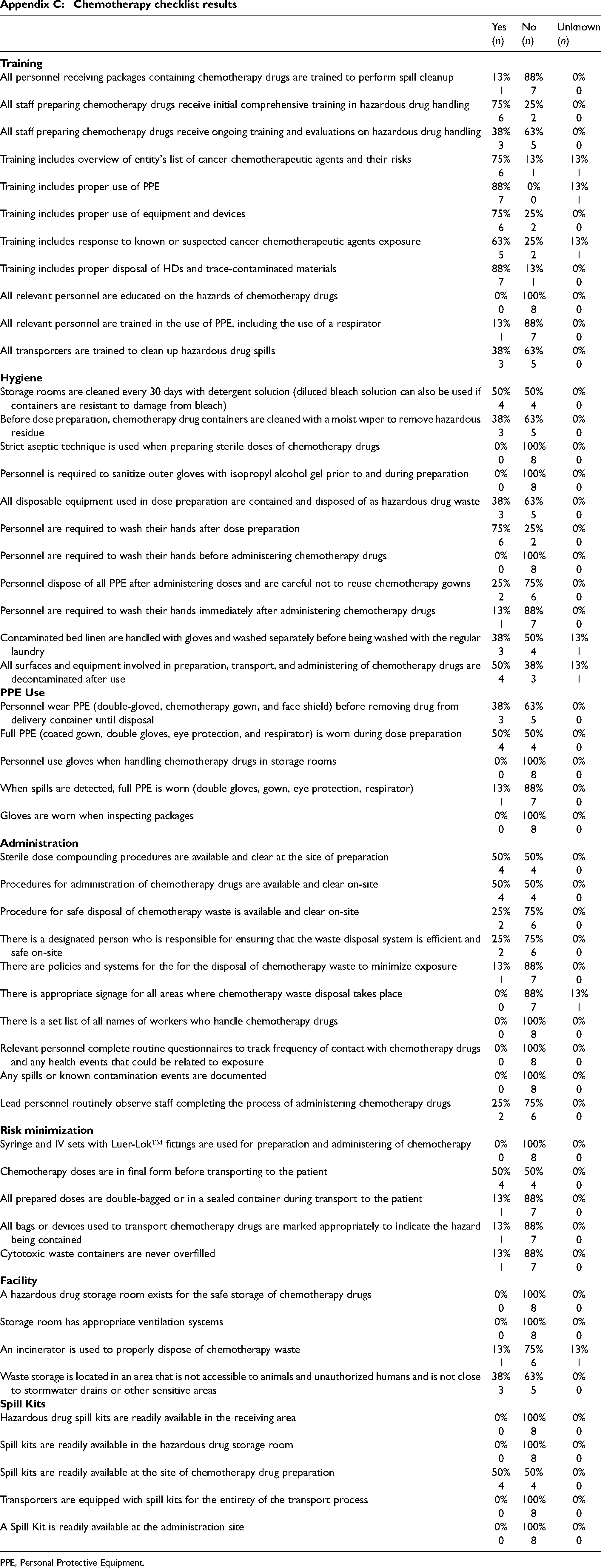
Only within the theme of “Training” were the majority of requirements met. At 75% (n = 6/8) of oncology units, staff preparing chemotherapeutic drugs received initial hazardous drug handling training, but less than 40% (n = 3/8) of sites offered ongoing training. Overall hygiene practices of workers at the sites, such as hand washing and decontamination, were found to meet PAHO guidelines 30% (n = 26/88) of the time. None of the surveyed hospitals used strict aseptic technique when preparing sterile doses of chemotherapeutic drugs. PPE use across the lifecycle of chemotherapy was found to follow PAHO guidelines 20% (n = 8/40) of the time, and, more specifically, no hospitals required use of gloves when inspecting drugs or handling chemotherapeutic drugs in storage rooms at any hospitals. Healthcare workers wore full PPE (coated gown, double gloves, eye protection, and respirator) during chemotherapy dose preparation at 50% (n = 4/8) of the hospitals surveyed.
Hazardous spills or known contamination events were not documented at any hospitals surveyed. At only 25% (n = 2/8) of hospitals, lead personnel routinely observe staff completing the process of administering chemotherapeutic drugs. None of the hospitals visited had a storage room for hazardous drugs or appropriate ventilation (negative air pressure with at least 12 air changes per hour). 13 Spill kits were found to be available at the site of chemotherapy preparation only at 50% (n = 4/8) of hospitals, while no hospitals had spill kits available during chemotherapy receiving, storage, transport, or administration. An observer described the preparation of chemotherapy as follows: “No prevention of spilling equipment; tries to cover the area with sterile gauze to try to prevent anything coming out.” Thematic analysis of checklist results is in Tables 3 and 4. Percentage of responses to each checklist question is in Appendix C.
Selected quotes from evaluator field notes.
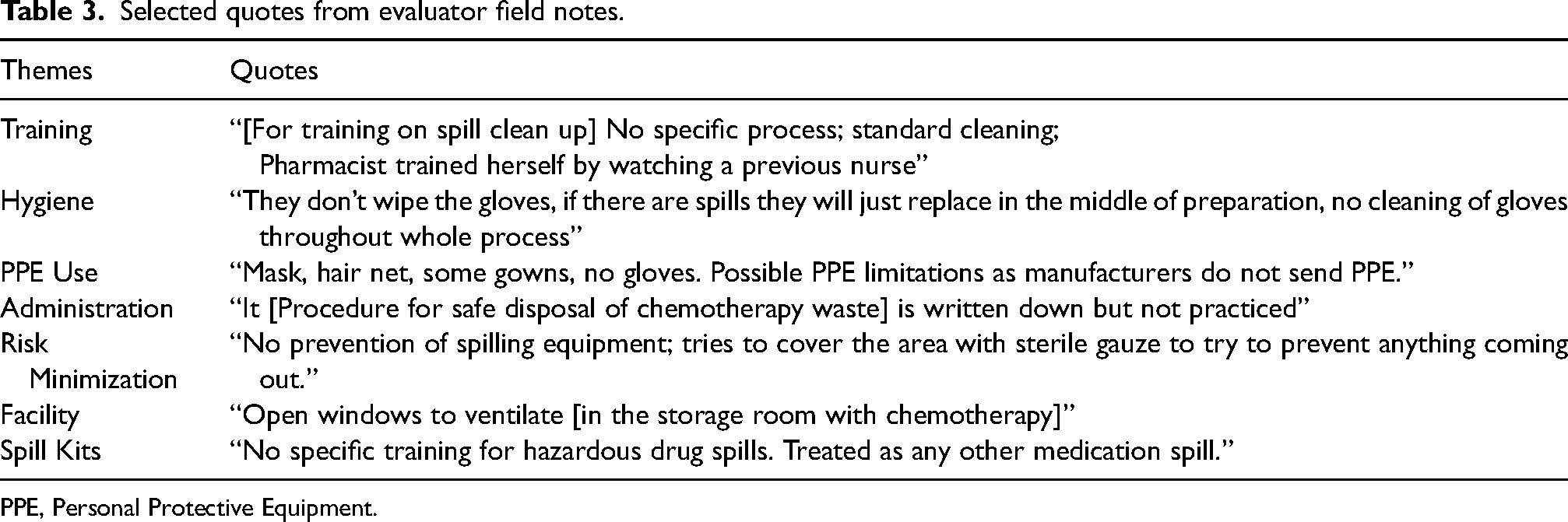
PPE, Personal Protective Equipment.
Percent of requirements met within a theme.
Discussion
Our results reveal the extent to which gaps exist in the infrastructure to safely handle chemotherapeutic drugs—including training—which may be required to fully achieve acceptable safe handling among all staff. A study among tertiary teaching hospitals in Ethiopia made the same conclusions of requisite improvement of clinical training for chemotherapy safe handling by nurses. 14 Still, the frequent stockout of PPE and other resources necessary to safely prepare and administer chemotherapy are out of the provider's control and must be addressed. Fentie et al. highlighted that at TASH, a large academic center evaluated in our study, there are notable supply chain challenges in obtaining safe handling supplies. 15 One particularly troubling finding in that study was that PPE did not make the government supplier procurement list, and providers relied often on donation for stocking of these necessary materials. Policy solutions or supply chain procurement initiatives must be implemented in Ethiopia to address PPE supply stockout obstacles.
Further, results from both the checklist and survey demonstrate that measures to prevent chemotherapy exposure and accidents, beyond simply using protective equipment, are predominantly non-existent or ineffective. Of particular concern is over half of respondents reporting a lack of systems to identify, prevent, and address chemotherapy hazards at work. Finally, an even higher proportion of respondents reported that incidents and accidents involving chemotherapy are not rapidly investigated to improve health and safety at their workplace, and no health centers in the study documented chemotherapy spills or contamination.
In environments where prevention and rapid confrontation of chemotherapy hazards do not take place, personal hygiene may be the last line of defense against significant exposure. For such reasons, finding that proper hygiene practices occurred only 30% of the time in the study sites is extremely troubling and congruent with study results in Eka Kotebe General Hospital in Addis Ababa, Ethiopia where levels of hand hygiene compliance were low among healthcare providers. 16
Ethiopia and most other LMICs have not implemented nation-wide chemotherapy safe handling guidelines that could establish a standard protocol of safety across all healthcare centers in each country. As a result, LMIC health care facilities report implementation of fewer safe handling practices than high income countries. A cross-sectional survey study performed in 2022 discovered low-income countries practicing 32% of safe handling standards measured across 10 domains. 17 Until such guidelines are adopted and practiced, a disproportionate number of health care workers in LMIC will continue to work under hazardous conditions.
Our results build on existing studies and efforts by health leaders in the country that have pushed Ethiopia's Federal Ministry of Health to call for adoption of protocols and measures for chemotherapy safe handling to decrease the risk of exposure to both patients and healthcare workers. 1 Collectively this body of work demonstrates a dire need to improve the implementation of chemotherapy safe handling guidelines.
Limitations
Future studies should include more healthcare sites in Ethiopia and attempt to reach a greater number of healthcare professionals who handle chemotherapy to make results more generalizable. The majority of survey participants were pharmacists, so future studies could focus on assessing the perspectives of other professions such as nurses, physicians, lab technicians, and other professionals who handle chemotherapy. In terms of checklist responses, all hospitals were located in the capital city of Addis Ababa, and future work should examine chemotherapy safe handling even further across Ethiopia's diverse geographic settings.
Conclusions
Workplace safety practices, policies, and procedures in Ethiopia do not meet the minimum chemotherapy handling requirements necessary to protect the health and safety of healthcare workers. Increased accountability, adoption of additional measures, and funding is required to improve chemotherapy safe handling. Research aimed at improving the implementation of these guidelines in clinical cancer care is urgently needed.
Footnotes
Author Contribution
BM and MR conceived the study. NW, SM, BM, and MR prepared the materials to conduct the study and performed data analysis and manuscript preparation. BM, JBC, JG, KW, ML, HH, ED, CB, KB, and AMF conducted study activities. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: James Collins is an employee of GlaxoSmithKline. Samantha Matys is an employee of United Therapeutics Corporation. Benyam Muluneh is a consultant with Servielle Pharmaceuticals and his spouse is an employee and stockholder at Novartis Pharmaceuticals. Megan Roberts’ spouse holds stock in Merck and Thermo Fisher Scientific.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Appendix A: Chemotherapy checklist questions
Appendix B: Cancer center profiles
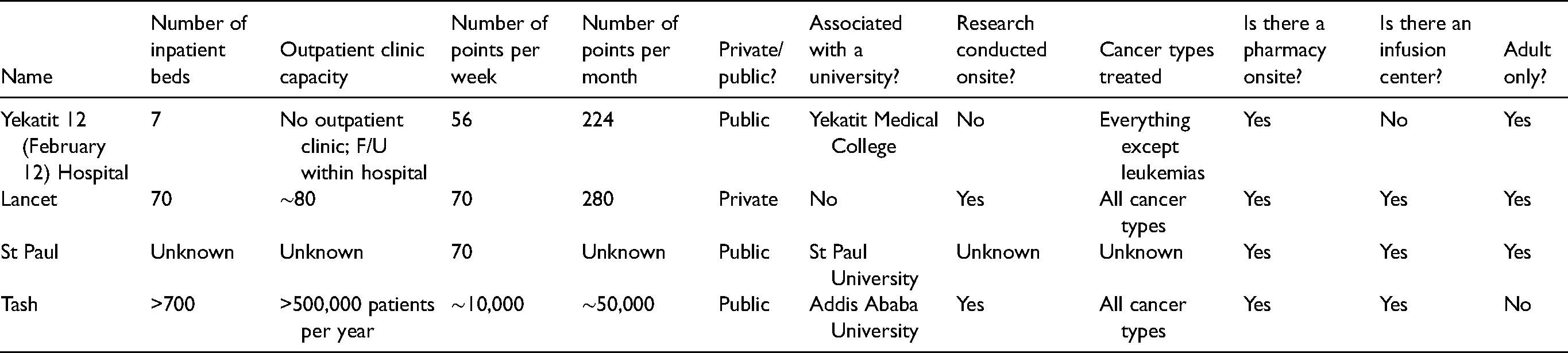
| Name | Number of inpatient beds | Outpatient clinic capacity | Number of points per week | Number of points per month | Private/public? | Associated with a university? | Research conducted onsite? | Cancer types treated | Is there a pharmacy onsite? | Is there an infusion center? | Adult only? |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Yekatit 12 (February 12) Hospital | 7 | No outpatient clinic; F/U within hospital | 56 | 224 | Public | Yekatit Medical College | No | Everything except leukemias | Yes | No | Yes |
| Lancet | 70 | ∼80 | 70 | 280 | Private | No | Yes | All cancer types | Yes | Yes | Yes |
| St Paul | Unknown | Unknown | 70 | Unknown | Public | St Paul University | Unknown | Unknown | Yes | Yes | Yes |
| Tash | >700 | >500,000 patients per year | ∼10,000 | ∼50,000 | Public | Addis Ababa University | Yes | All cancer types | Yes | Yes | No |
| Yes |
No |
Unknown |
|
|---|---|---|---|
|
|
|||
| All personnel receiving packages containing chemotherapy drugs are trained to perform spill cleanup | 13% 1 |
88% 7 |
0% 0 |
| All staff preparing chemotherapy drugs receive initial comprehensive training in hazardous drug handling | 75% 6 |
25% 2 |
0% 0 |
| All staff preparing chemotherapy drugs receive ongoing training and evaluations on hazardous drug handling | 38% 3 |
63% 5 |
0% 0 |
| Training includes overview of entity's list of cancer chemotherapeutic agents and their risks | 75% 6 |
13% 1 |
13% 1 |
| Training includes proper use of PPE | 88% 7 |
0% 0 |
13% 1 |
| Training includes proper use of equipment and devices | 75% 6 |
25% 2 |
0% 0 |
| Training includes response to known or suspected cancer chemotherapeutic agents exposure | 63% 5 |
25% 2 |
13% 1 |
| Training includes proper disposal of HDs and trace-contaminated materials | 88% 7 |
13% 1 |
0% 0 |
| All relevant personnel are educated on the hazards of chemotherapy drugs | 0% 0 |
100% 8 |
0% 0 |
| All relevant personnel are trained in the use of PPE, including the use of a respirator | 13% 1 |
88% 7 |
0% 0 |
| All transporters are trained to clean up hazardous drug spills | 38% 3 |
63% 5 |
0% 0 |
|
|
|||
| Storage rooms are cleaned every 30 days with detergent solution (diluted bleach solution can also be used if containers are resistant to damage from bleach) | 50% 4 |
50% 4 |
0% 0 |
| Before dose preparation, chemotherapy drug containers are cleaned with a moist wiper to remove hazardous residue | 38% 3 |
63% 5 |
0% 0 |
| Strict aseptic technique is used when preparing sterile doses of chemotherapy drugs | 0% 0 |
100% 8 |
0% 0 |
| Personnel is required to sanitize outer gloves with isopropyl alcohol gel prior to and during preparation | 0% 0 |
100% 8 |
0% 0 |
| All disposable equipment used in dose preparation are contained and disposed of as hazardous drug waste | 38% 3 |
63% 5 |
0% 0 |
| Personnel are required to wash their hands after dose preparation | 75% 6 |
25% 2 |
0% 0 |
| Personnel are required to wash their hands before administering chemotherapy drugs | 0% 0 |
100% 8 |
0% 0 |
| Personnel dispose of all PPE after administering doses and are careful not to reuse chemotherapy gowns | 25% 2 |
75% 6 |
0% 0 |
| Personnel are required to wash their hands immediately after administering chemotherapy drugs | 13% 1 |
88% 7 |
0% 0 |
| Contaminated bed linen are handled with gloves and washed separately before being washed with the regular laundry | 38% 3 |
50% 4 |
13% 1 |
| All surfaces and equipment involved in preparation, transport, and administering of chemotherapy drugs are decontaminated after use | 50% 4 |
38% 3 |
13% 1 |
|
|
|||
| Personnel wear PPE (double-gloved, chemotherapy gown, and face shield) before removing drug from delivery container until disposal | 38% 3 |
63% 5 |
0% 0 |
| Full PPE (coated gown, double gloves, eye protection, and respirator) is worn during dose preparation | 50% 4 |
50% 4 |
0% 0 |
| Personnel use gloves when handling chemotherapy drugs in storage rooms | 0% 0 |
100% 8 |
0% 0 |
| When spills are detected, full PPE is worn (double gloves, gown, eye protection, respirator) | 13% 1 |
88% 7 |
0% 0 |
| Gloves are worn when inspecting packages | 0% 0 |
100% 8 |
0% 0 |
|
|
|||
| Sterile dose compounding procedures are available and clear at the site of preparation | 50% 4 |
50% 4 |
0% 0 |
| Procedures for administration of chemotherapy drugs are available and clear on-site | 50% 4 |
50% 4 |
0% 0 |
| Procedure for safe disposal of chemotherapy waste is available and clear on-site | 25% 2 |
75% 6 |
0% 0 |
| There is a designated person who is responsible for ensuring that the waste disposal system is efficient and safe on-site | 25% 2 |
75% 6 |
0% 0 |
| There are policies and systems for the for the disposal of chemotherapy waste to minimize exposure | 13% 1 |
88% 7 |
0% 0 |
| There is appropriate signage for all areas where chemotherapy waste disposal takes place | 0% 0 |
88% 7 |
13% 1 |
| There is a set list of all names of workers who handle chemotherapy drugs | 0% 0 |
100% 8 |
0% 0 |
| Relevant personnel complete routine questionnaires to track frequency of contact with chemotherapy drugs and any health events that could be related to exposure | 0% 0 |
100% 8 |
0% 0 |
| Any spills or known contamination events are documented | 0% 0 |
100% 8 |
0% 0 |
| Lead personnel routinely observe staff completing the process of administering chemotherapy drugs | 25% 2 |
75% 6 |
0% 0 |
|
|
|||
| Syringe and IV sets with Luer-Lok™ fittings are used for preparation and administering of chemotherapy | 0% 0 |
100% 8 |
0% 0 |
| Chemotherapy doses are in final form before transporting to the patient | 50% 4 |
50% 4 |
0% 0 |
| All prepared doses are double-bagged or in a sealed container during transport to the patient | 13% 1 |
88% 7 |
0% 0 |
| All bags or devices used to transport chemotherapy drugs are marked appropriately to indicate the hazard being contained | 13% 1 |
88% 7 |
0% 0 |
| Cytotoxic waste containers are never overfilled | 13% 1 |
88% 7 |
0% 0 |
|
|
|||
| A hazardous drug storage room exists for the safe storage of chemotherapy drugs | 0% 0 |
100% 8 |
0% 0 |
| Storage room has appropriate ventilation systems | 0% 0 |
100% 8 |
0% 0 |
| An incinerator is used to properly dispose of chemotherapy waste | 13% 1 |
75% 6 |
13% 1 |
| Waste storage is located in an area that is not accessible to animals and unauthorized humans and is not close to stormwater drains or other sensitive areas | 38% 3 |
63% 5 |
0% 0 |
|
|
|||
| Hazardous drug spill kits are readily available in the receiving area | 0% 0 |
100% 8 |
0% 0 |
| Spill kits are readily available in the hazardous drug storage room | 0% 0 |
100% 8 |
0% 0 |
| Spill kits are readily available at the site of chemotherapy drug preparation | 50% 4 |
50% 4 |
0% 0 |
| Transporters are equipped with spill kits for the entirety of the transport process | 0% 0 |
100% 8 |
0% 0 |
| A Spill Kit is readily available at the administration site | 0% 0 |
100% 8 |
0% 0 |
PPE, Personal Protective Equipment.
Appendix D: Chemotherapy survey results