
Abstract
Introduction
Previous studies suggest that quality improvement initiatives focused on hospital-acquired venous thromboembolism have a positive impact on prescribing rates of venous thromboembolism prophylaxis, especially those that incorporate computerized changes.
Methods
We conducted a quality improvement project to determine whether education and computerized prescriber order entry system changes affect venous thromboembolism prophylaxis compliance rates in hospitalized medical patients at a Comprehensive Cancer Center. Between 1 January 2021 and 31 January 2023, 37,739 non-surgical, adult patient encounters with a length of stay > 48 h were analyzed in our study. From 18 December 2021 to 8 March 2022, provider education was delivered to the three largest admitting services, and computerized prescriber order entry changes were implemented incorporating a mandatory requirement to either order venous thromboembolism prophylaxis or document a contraindication for all patients at moderate venous thromboembolism risk.
Results
Monthly venous thromboembolism prophylaxis compliance rates, as defined by the Centers for Medicare and Medicaid Services VTE-1 metric, increased from a mean of 74% to 93% after the interventions. This change was driven primarily by an increased utilization of mechanical venous thromboembolism prophylaxis from 37% to 53%.
Conclusion
Our study demonstrated that a multi-faceted intervention incorporating provider education and computerized prescriber order entry system changes can significantly increase venous thromboembolism prophylaxis compliance rates in cancer patients.
Introduction
Hospital-acquired venous thromboembolism (VTE) is a common but potentially avoidable complication in hospitalized medical patients with cancer. 1 Multiple systematic reviews of randomized controlled trials have demonstrated that pharmacological and mechanical VTE prophylaxis are both safe and effective at preventing VTE in appropriately selected medical patients.2–4 Additionally, guidelines focused on preventing VTE in cancer patients, such as those published by the National Comprehensive Cancer Center and American Society for Clinical Oncology, advocate for VTE risk assessment and utilization of prophylaxis in all hospitalized cancer patients.5–7 Yet, multiple retrospective and cross-sectional studies have shown that VTE prophylaxis is frequently missing for eligible patients.8–10 Proposed barriers to higher utilization of VTE prophylaxis include a concern for major bleeding, under-recognition of VTE risk, and lack of a standardized order entry system. 11
To address the large variability in VTE prophylaxis across the United States, multiple governmental agencies including the Centers for Medicare and Medicaid (CMS), the Agency for Healthcare Research and Quality (AHRQ), and The Joint Commission (TJC) have put forth quality metrics to measure rates of hospital compliance to VTE prophylaxis. 12 Of the 6 core VTE measures put forth by CMS and originally endorsed by AHRQ and TJC, VTE-1 tracks whether all patients admitted to the hospital are either prescribed VTE prophylaxis or have a contraindication documented within 24 h upon admission. 12 To help increase compliance to VTE-1 and other quality measurements, both governmental and non-governmental organizations such as the American Heart Association have encouraged the use of quality improvement projects to develop ways in which rates of hospital-acquired VTE can be decreased. 13 While past initiatives aimed at improving the utilization of VTE prophylaxis were limited in observational design, statistical power, and incomplete reporting of study design, they demonstrated an improvement in prescribing thromboprophylaxis over relying on individual provider behavior alone. 14 In fact, a Cochrane review of system-level interventions found that computerized changes not only improved VTE prophylaxis order rates but also decreased the incidence of symptomatic hospital-acquired VTE. 14
Thus, the purpose of this study was to determine whether a multi-faceted quality improvement initiative incorporating provider education and changes to the computerized prescriber order entry (CPOE) system at a National Cancer Institute Comprehensive Cancer Center can positively affect the CMS VTE-1 compliance metric within a 1-year time frame. An understanding of the impact quality improvement initiatives can have may encourage other institutions to develop their own projects and promote more awareness and resources to combat hospital-acquired VTE in cancer patients.
Methods
Study design
In this quality improvement project, we utilized the Plan-Do-Study-Act (PDSA) design framework as shown in Figure 1. We studied patient encounters of all hospitalized medical patients at the University of Texas/MD Anderson Cancer Center (MDACC) from 1 January 2021 to 31 January 2023, with a length of stay ≥ 48 h. Encounters of patients < 18 years old, surgical patients, and patients with only supportive care measures were excluded. We determined compliance through the CMS VTE-1 metric as a number of patients with VTE prophylaxis ordered or a contraindication documented over all inpatients. VTE prophylaxis was confirmed as either an administration of an anticoagulant at a therapeutic or prophylactic dose, or mechanical prophylaxis with an order for a thromboembolic deterrent (TED) hose or a sequential compression device (SCD) at any point during the hospitalization. While our project did not require approval from an Institutional Review Board due to the use of non-identifiable aggregate data, it was reviewed and approved by a quality improvement assessment board.
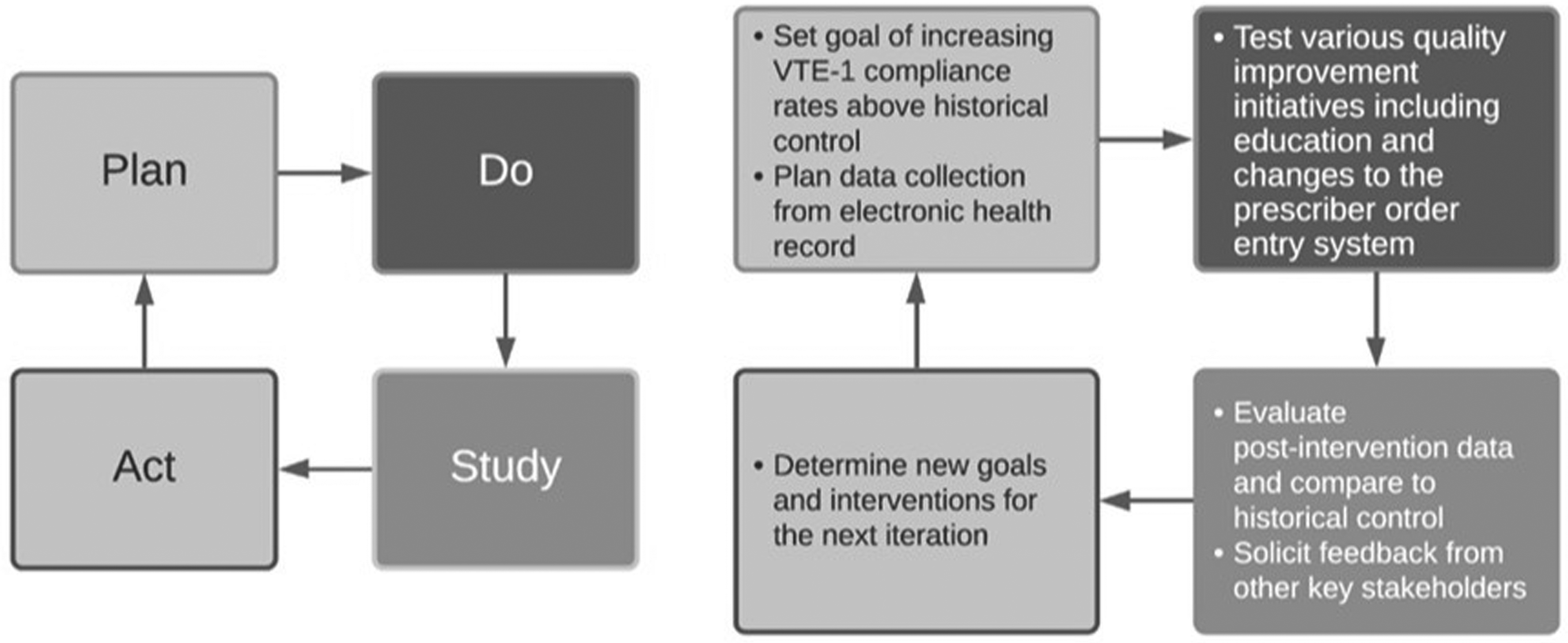
Plan-Do-Study-Act (PDSA) framework for quality improvement.
Educational interventions
Virtual education sessions, lasting 15 minutes each, were delivered to the top 3 admitting services at MDACC through a quality improvement team composed of a pharmacist and the director of our institution's multi-disciplinary Anticoagulation Stewardship Committee. Sessions focused on highlighting the need for VTE prophylaxis, discussing service-specific baseline VTE-1 compliance rates, and reminders on the availability of our institution's clinical VTE prophylaxis algorithm were given during each service's monthly faculty meeting. Attendance at each session was automatically tracked through video teleconferencing controls. Additionally, we promoted the use of mechanical VTE prophylaxis in patients with a contraindication to anticoagulation. At the end of each session, we held a dedicated open-feedback session for further identification of barriers to ordering VTE prophylaxis. Outside of targeting physicians we also sent educational fliers to all nursing units for each of the top 3 admitting services that debunked common myths about VTE prophylaxis.
Changes to the CPOE VTE prophylaxis ordering algorithm
At our institution, all patients are admitted to the hospital through an admission CPOE order set that includes a mandatory section dedicated to VTE prophylaxis. Prior to our intervention, our CPOE admission order set only suggested anticoagulation for patients at moderate to high VTE risk. Admissions without an order for pharmacological prophylaxis were not required to order mechanical prophylaxis despite guidelines recommending mechanical VTE prophylaxis in moderate to high VTE-risk patients ineligible for anticoagulation. Additionally, there was no requirement to document a rationale if no form of VTE prophylaxis was ordered upon admission. Therefore, our CPOE changes addressed each of these discrepancies by requiring either an order for mechanical VTE prophylaxis or documented contraindications to both forms of VTE prophylaxis if anticoagulation was not ordered. Our updated CPOE VTE prophylaxis ordering algorithm, emphasizing an “opt out” approach, is shown in Figure 2. Education on updates to the VTE prophylaxis ordering panel was provided to all inpatient admitting services at MDACC.
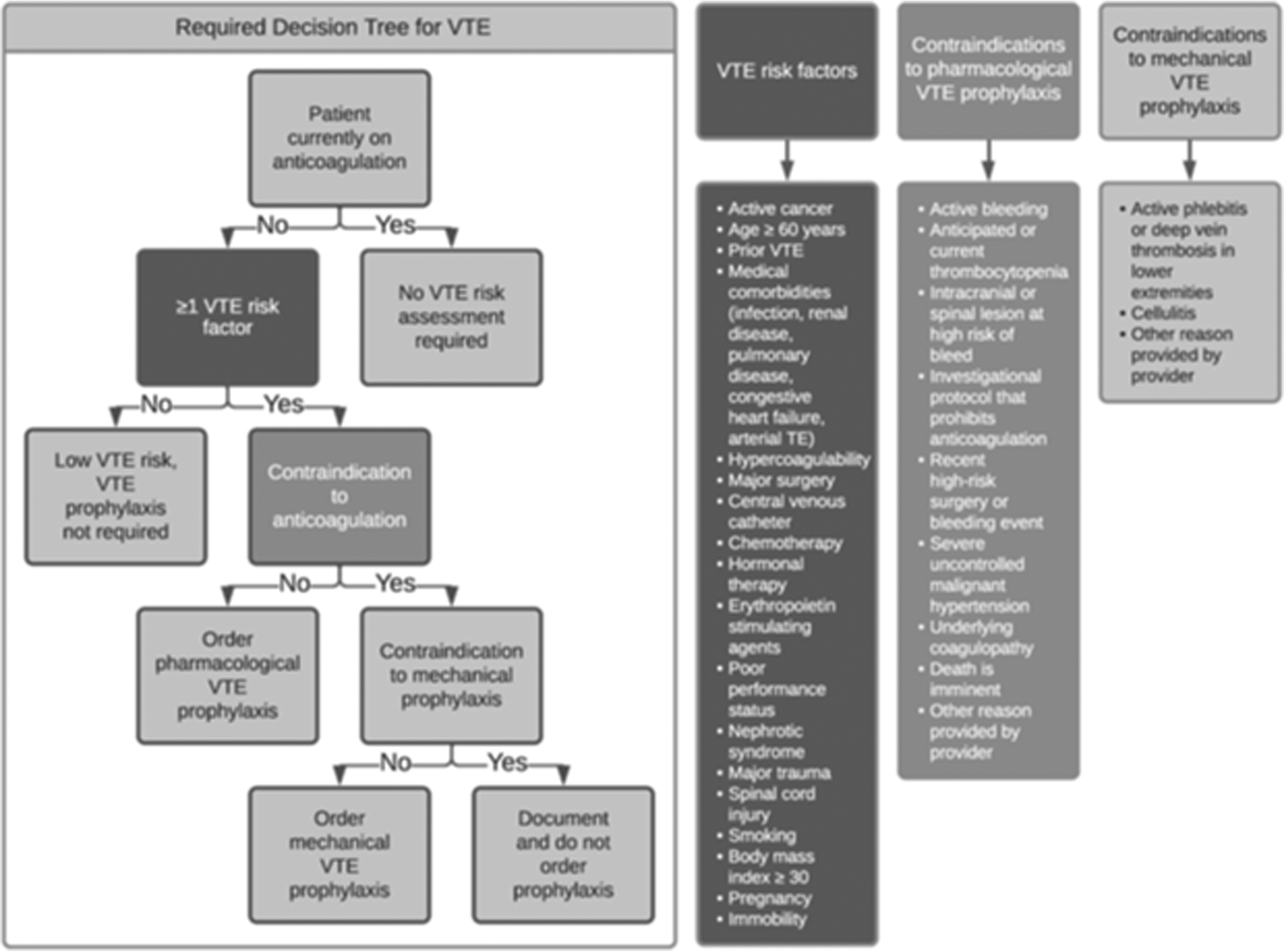
Updated CPOE VTE prophylaxis ordering algorithm incorporating CPOE changes.
Statistical analysis
To monitor the impact of our quality improvement initiative, we designed an automated data collection tool that pulled aggregate data on all hospitalized patient encounters each month. Data points included age, admitting service, type of cancer, length of stay, VTE risk assessment, and the first instance that pharmacological or mechanical VTE prophylaxis was ordered. Because our interventions were performed from 8 December 2021 to 8 March 2022, our pre-intervention data consisted of encounters from 1 January 2021 to 8 December 2021, while encounters from 8 March 2022 to 31 January 2023, were combined as post-intervention data. Descriptive statistics were performed on patient characteristics in both the pre- and post-intervention groups. A statistical process control chart was utilized to highlight changes to the VTE-1 compliance rate over time. Upper and lower control limits within the control chart were set to be three standard deviations from the pre- and post-intervention means.
Results
Patient characteristics
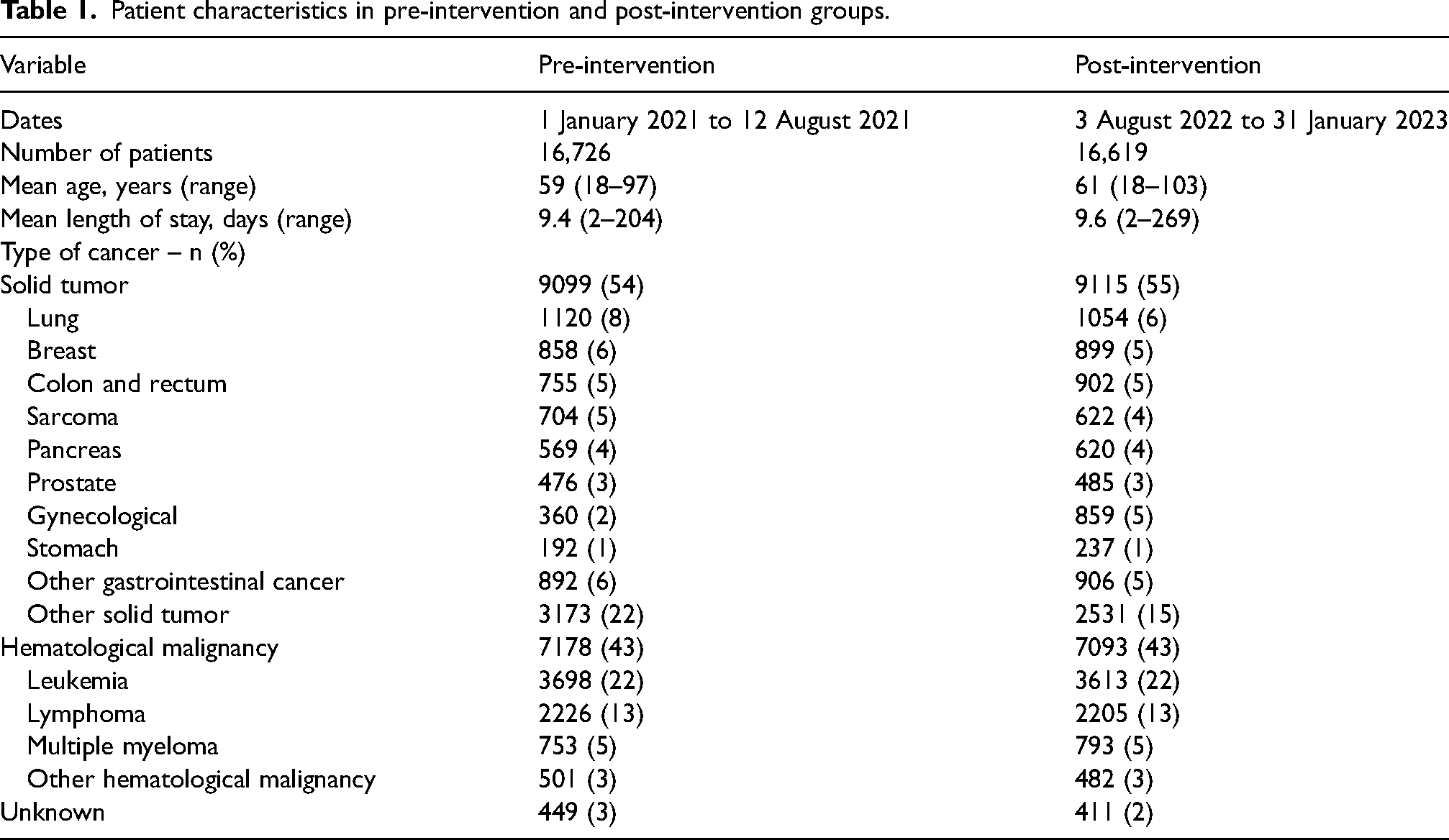
From 1 January 2021 to 31 January 2023, a total of 37,739 adult patient admissions to a non-surgical and non-supportive care service with length of stay ≥ 48 h were identified (Figure 3). Of those, 16,726 encounters fell within the pre-intervention time period while 16,619 encounters fell into the post-intervention period (Table 1). Patient characteristics between pre- and post-intervention groups were relatively similar in terms of age, length of stay, and types of cancer. The mean age was 60 years old in both groups while the mean length of stay was 9 days. Roughly half of the encounters included patients with solid tumors while slightly less than half included those with hematological malignancies.
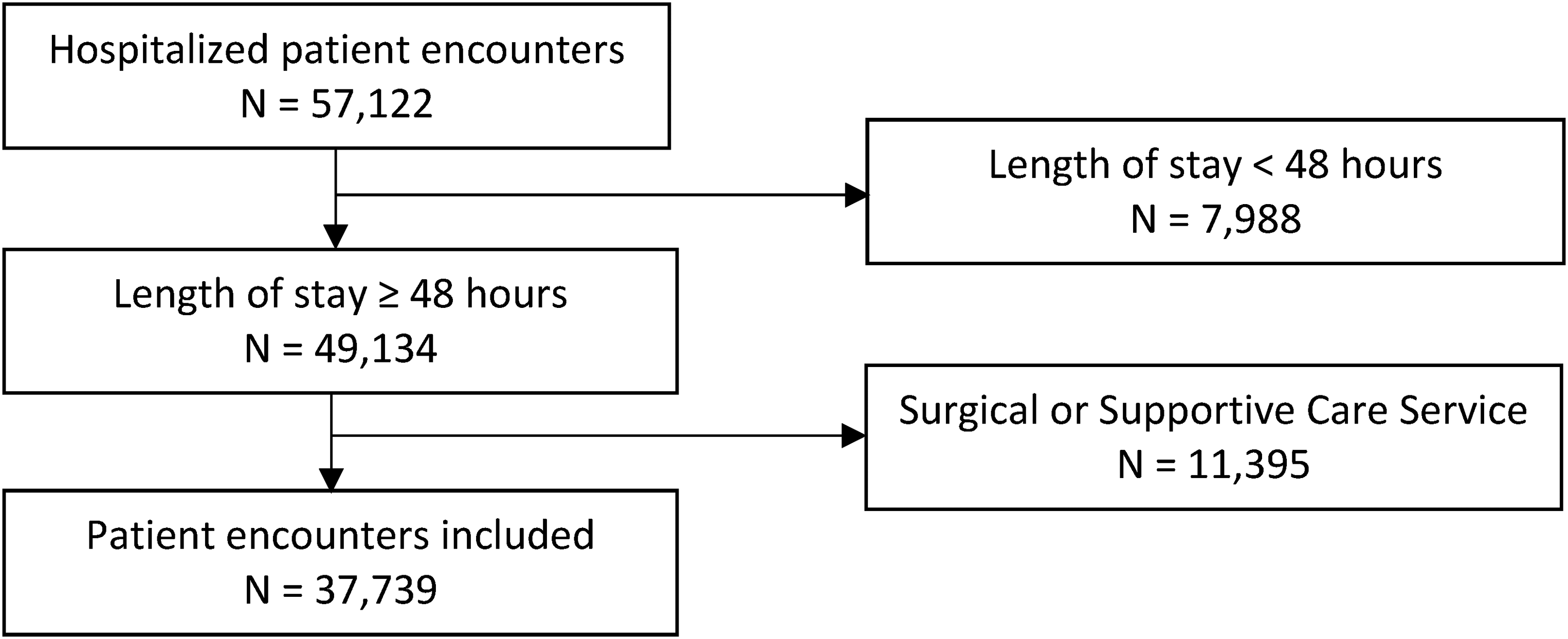
Study inclusion flowchart.
Patient characteristics in pre-intervention and post-intervention groups.
VTE-1 compliance rates
From the pre- to post-intervention time period, monthly VTE-1 compliance rates increased from a mean of 74% to 93%, respectively, as shown in Figure 4. This increase was driven by a greater proportion of patients with mechanical VTE prophylaxis orders with monthly prescribing rates for TED hose or SCD increasing from a mean of 37% to 53%. Additionally, rates of documented contraindications rose from 1% to 23% after the intervention time period. In contrast, prescribing rates for pharmacological VTE prophylaxis did not significantly change between time periods and consistently stayed at about 53% throughout both time periods. In Figure 5, VTE-1 compliance rates stayed consistently around the control mean of 74% throughout the pre-intervention time period with an upper and lower control limit of 71% and 77%, respectively. VTE-1 compliance rates in the post-intervention time period rose to 93% with new upper and lower control limits of 91% and 97%.
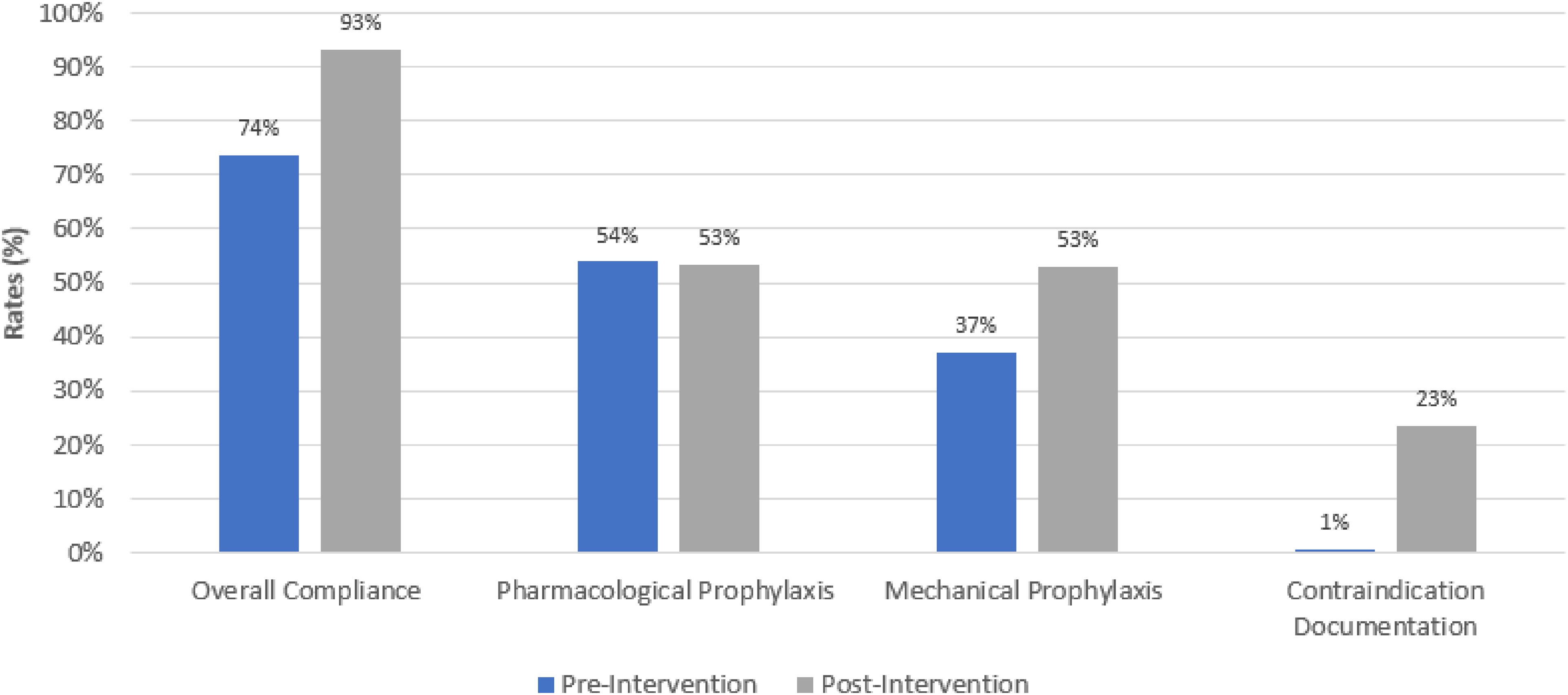
Venous thromboembolism (VTE) prophylaxis outcomes in pre- and post-intervention groups.
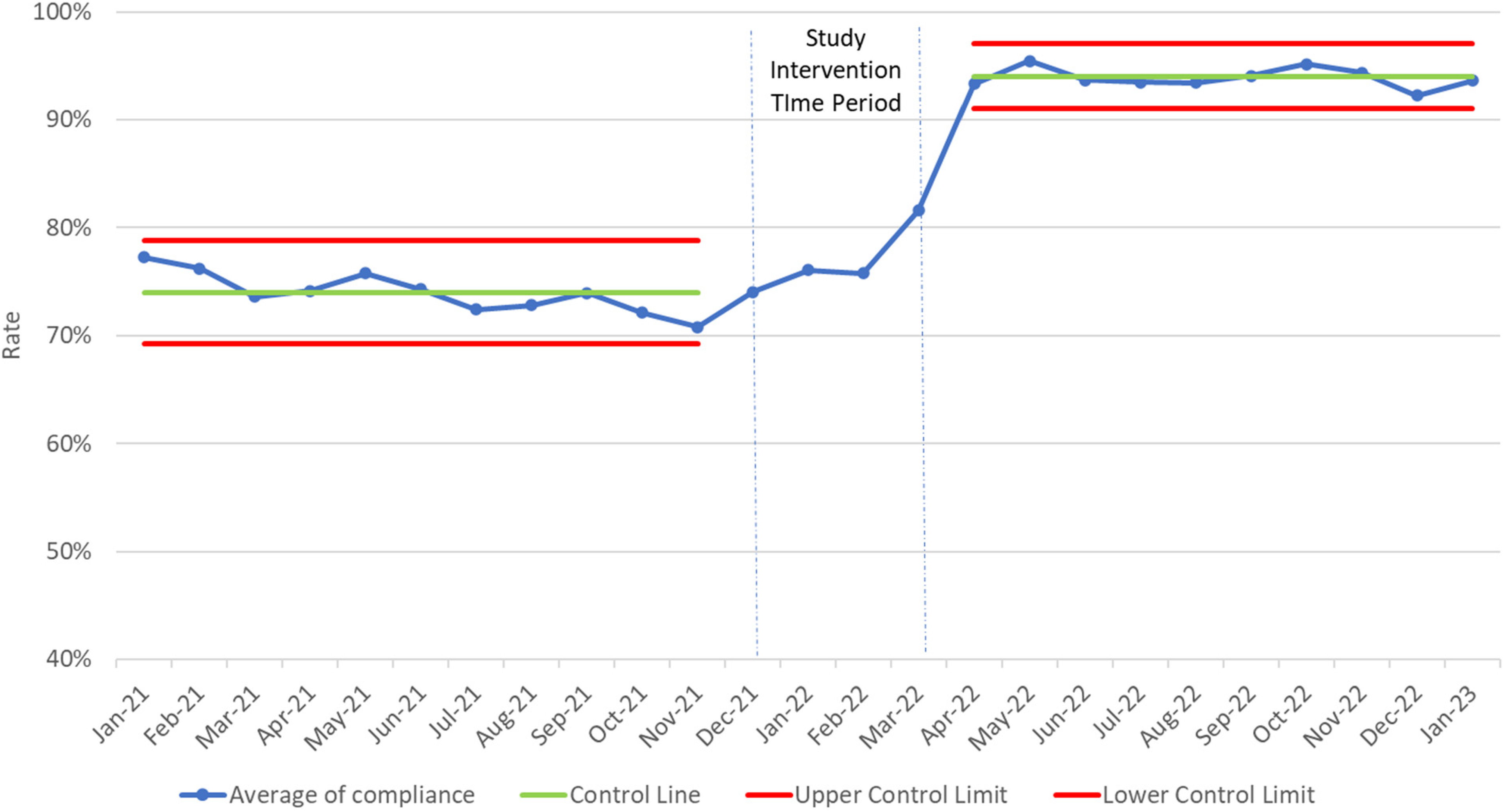
Control chart of venous thromboembolism (VTE-1) compliance rates over time.
Discussion
Similar to previous quality improvement projects focused on VTE prophylaxis, such as those by Streiff et al., 15 our study found that a multi-faceted initiative incorporating education and computerized changes positively impacted VTE prophylaxis prescribing rates. However, unlike previous studies, our intervention focused purely on hospitalized, non-surgical cancer patients; a uniquely understudied patient population at considerable risk for hospital-acquired VTE. 16 Strengths of our study included a large patient population and a quality improvement design that allowed for repeat cycles of intervention development, application, and evaluation. In contrast to the labor-intensive monthly audit-and-feedback strategies identified by Tooher et al. 17 and Bryne et al., 18 our multi-faceted intervention was easily integrated into prescriber workflows and applied to most patients without requiring excess resources or personnel. Similarly, our intervention incorporating both education and computerized changes adds to previous literature that suggests several active strategies are more likely to be effective than a single isolated intervention. 19
The driving force behind the increase in VTE-1 compliance rates after our intervention was through an increase in mechanical VTE prophylaxis and documentation of contraindications to any form of VTE prophylaxis. Rates in ordering prophylactic anticoagulation did not significantly change after our quality improvement process. Possible reasons for this lack of change include a large percentage of patients who were admitted for procedures and those with relative or absolute contraindications for anticoagulation such as active bleeding, coagulopathy, or thrombocytopenia. In contrast, we believe that because relatively few contraindications to mechanical VTE prophylaxis exist, providers were able to significantly increase their utilization of TED hoses and SCDs after education and prompting through our CPOE changes.
It is significant to note that increases in VTE prophylaxis prescribing rates do not always correlate with corresponding increases in administration rates. Many factors including patient refusal, temporary holds or discontinuations, and lack of time and personal impact the ability for VTE prophylaxis orders to be administered. 20 Therefore, a limitation of our study was the lack of verifying whether VTE prophylaxis orders were continued beyond the first administration and throughout the entire admission. Additionally, we failed to verify whether the listed contraindications to VTE prophylaxis by providers were appropriate. However, we confirmed with physicians outside of the emergency department that patients were independently assessed for VTE prophylaxis daily regardless of what documented contraindications were listed on the admission orders. Outside of verifying VTE prophylaxis administrations and contraindications, our study was unable to measure clinical VTE and bleeding outcomes. Yet, data extrapolated from the landmark Kucher et al. 21 study, suggests that an increase in VTE prophylaxis corresponds with decreased rates of VTE at 90 days. Lastly, it should be noted that our study failed to measure the increased costs and personnel requirements from the increased utilization of mechanical VTE prophylaxis. Nevertheless, multiple pharmacoeconomic studies have demonstrated that the healthcare and patient costs of hospital-acquired VTE are considerably larger than the costs of preventative strategies, including pharmacological and mechanical VTE prophylaxis. 22
VTE-risk assessment models (RAMs), such as the IMPROVE, Padua, and Geneva risk models have been suggested as helpful tools for the selection of appropriate medical patients for VTE prophylaxis. 23 As a cancer hospital, the majority of our admitted patients have more than one VTE risk factor, particularly active malignancy, and therefore, automatically met the criteria put forth by multiple RAMs including the Padua model. 24 Therefore, VTE-RAMs were not embedded in our ordering CPOE algorithm and VTE risk assessment was left to the discretion of our admitting providers and remains based on an internally developed algorithm.
While the non-research design of our project limits its applicability to other institutions, the positive results highlight the potential for initiatives at other cancer hospitals to both promote the importance of VTE prophylaxis and decrease rates of hospital-acquired VTE. Future iterations of our PDSA cycle include the creation of an automated best practice advisory (BPA) to allow the emergency department provider to defer VTE prophylaxis to the primary care team. We found during data collection that this is often done by indicating the patient has contraindications to VTE prophylaxis. While documenting contraindications to VTE prophylaxis satisfies our definition of compliance, we feel this is an area where further improvement is needed to ensure the patient has a proper risk assessment and VTE prophylaxis if indicated. Additionally, we plan to expand our compliance definition beyond the VTE-1 metric by looking at the entire patient encounter for continued VTE prophylaxis and the time to first administration. Our aim will be to continue employing continuous quality improvement cycles until our VTE-1 compliance rate achieves 100%.
Conclusion
Our findings show that quality improvement initiatives incorporating education and system-level CPOE changes can positively affect VTE prophylaxis compliance rates in hospitalized medical patients with cancer. While several limitations existed in our study design, the positive benefits found in our study should prompt other cancer hospitals to consider implementing similar quality improvement projects aimed at increasing awareness for VTE prophylaxis.
Footnotes
Author contributions
CW and KT researched literature and conceived the study. CW and KT were involved in the development of the quality improvement initiative and data analysis. CW wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.