
Abstract
Introduction
Molecular multitargeted small tyrosine kinase inhibitory (TKI) agents such as axitinib, sunitinib and pazopanib are commonly used in several types of solid tumors. Anemia is not a rare effect of these drugs which may occur at all grades. However, drug-induced immune hemolytic anemia (IHA), a very rare condition is distinctive from other types of anemia with its specific mechanism and management strategy.
Case Reports
We reported three different TKI-induced IHA cases that occurred due to axitinib, sunitinib, and pazopanib, respectively. The first two cases were diagnosed with renal cell carcinoma and the last one was diagnosed with soft tissue sarcoma. They all presented with the characteristic symptoms of anemia and hemolysis. All the cases were detected positive for the complement C3d direct antiglobulin (direct coombs) test.
Management and Outcomes
Discontinuation of the causative drug and 1 mg/kg/day dose of corticosteroid treatment were able to control IHA in all three cases. Excluding the other factors of IHA and an evident laboratory and clinical benefit after withholding the TKI led to the diagnosis of TKI-related IHA in each case.
Discussion
TKIs are relatively new in clinical practice and are being used for more indications and in more patients. To our knowledge#these three cases are unique in terms of axitinib#sunitinib#and pazopanib-related IHA.
Introduction
Drug-induced immune hemolytic anemia (IHA) incidence is estimated to be one in a million population. The drug groups predominantly are antimicrobics, anti-inflammatory agents, and antineoplastic agents. 1 However, cytotoxic antineoplastic drugs were better defined as the cause of IHA rather than new-generation drugs like tyrosine kinase inhibitors (TKIs) and immunotherapies.
Molecular multitargeted small TKIs such as sunitinib, axitinib and pazopanib are commonly used in several types of solid tumors. Vascular epithelial growth factor receptor (VEGFR) is the main target for these drugs. 2 Sunitinib is a potent inhibitor of VEGFR-1, VEGFR-2, fms-like tyrosine kinase-3 (FLT-3), stem cell factor receptor (c-KIT), and platelet-derived growth factor receptor (PDGFR) α and β. 3 Axitinib is an oral second-generation TKI strongly inhibits VEGFR-1, VEGFR-2 and, VEGFR-3, and weakly inhibits c-KIT and PDGFR. 4 Pazopanib is a selective potent inhibitor of VEGFR-2 in addition to VEGFR-1, VEGFR-3, c-KIT, PDGFR-β, and fibroblast growth factor receptor-1 (FGFR-1). 5 On January 2006, sunitinib was first approved by US Food and Drug Administration for indications of treating renal cell carcinoma (RCC) and imatinib-resistant gastrointestinal stromal tumors. On January 2012, axitinib was approved for advanced RCC. Pazopanib was first approved on October 2009 for advanced RCC and on April 2012 for advanced soft tissue sarcomas. Due to the relatively short-term usage of these drugs, physicians are still gathering information for recognizing and overcoming the adverse effects that may develop.
Case presentations
We reported three cases who presented with hemolytic anemia under TKI. All three cases were examined by an experienced hematologist during the diagnosis and treatment period.
Case 1
A 66-year-old man presented with gross hematuria and was diagnosed with RCC after a right-sided radical nephrectomy for a 7 cm right renal mass, 3 years ago. Diagnostic and prognostic tests showed 3 cm metastatic para-aortic lymph nodes. The international metastatic RCC database consortium (IMDC) score was calculated as intermediate risk. After 3 years of a progression-free period under sunitinib with a personalized dose (2 weeks on/1 week off schedule due to grade 3 fatigue and grade 3 mucositis), his cancer spread to mediastinal lymph nodes. Therefore, the treatment was changed to axitinib. On the third month under axitinib, he presented with nausea and jaundice started 5 days ago. Initial testing showed a 5 g/dL decrease in hemoglobin (Hb) level (from 12 to 5 g/dL). Peripheral blood smear showed signs of hemolysis. Also, elevated lactate dehydrogenase (LDH) and indirect bilirubin were compatible with hemolytic anemia. His direct antiglobulin test (DAT) was positive complement 3d (C3d; (Table 1). Therefore, axitinib treatment was stopped immediately and methylprednisolone at a dose of 1 mg/kg was started with the diagnosis of drug-induced IHA. Hb levels gradually increased to normal under steroid treatment in 4 weeks. However, 2 months later, his cancer progressed with brain metastasis at the right temporal lobe. Cranial radiotherapy was performed. The eastern cooperative oncology group performance score of the patient was 3 and he died because of the progressive disease 3 months after the diagnosis of TKI-induced IHA.
Clinical and laboratory characteristics of tyrosine kinase associated immune hemolytic anemia cases.
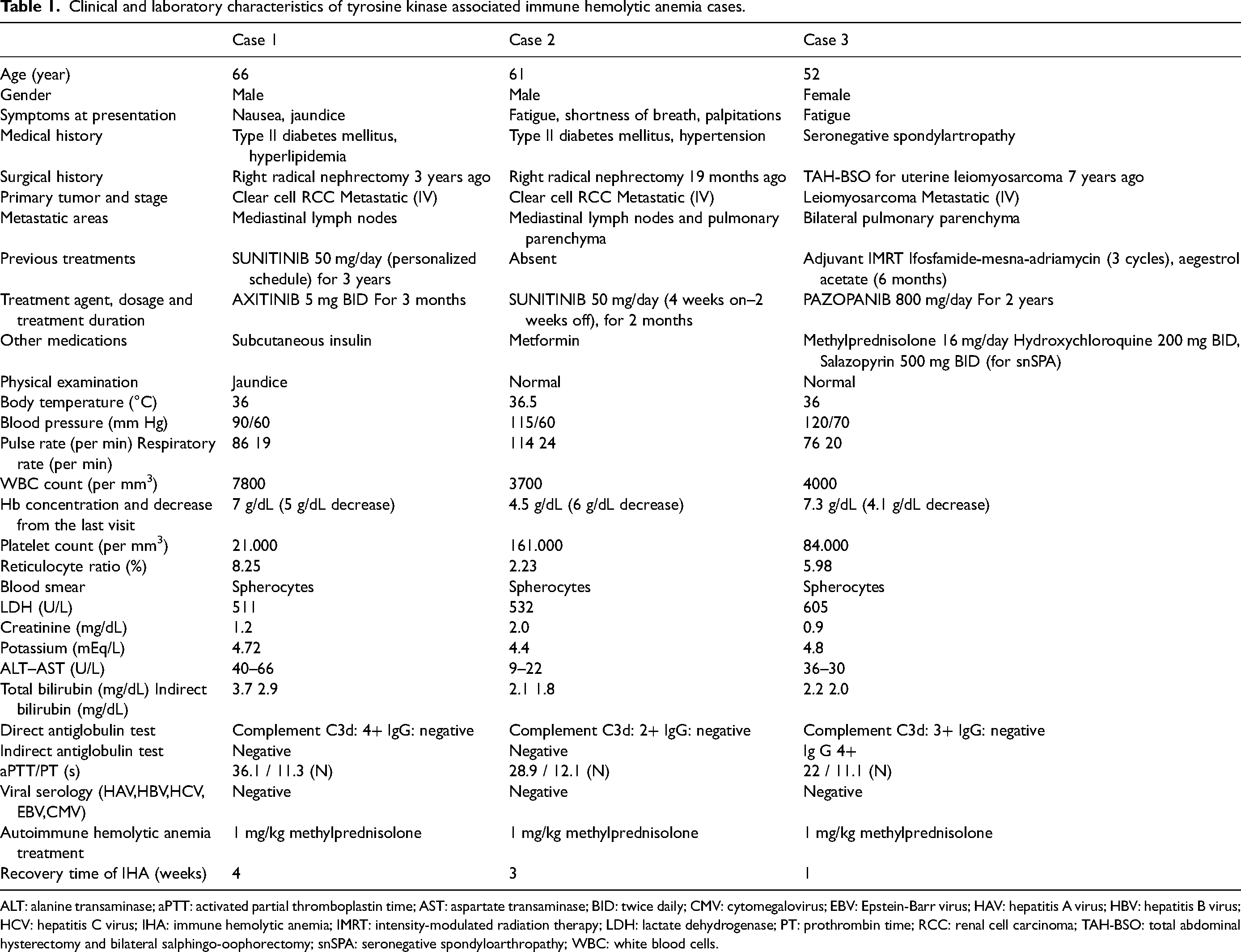
ALT: alanine transaminase; aPTT: activated partial thromboplastin time; AST: aspartate transaminase; BID: twice daily; CMV: cytomegalovirus; EBV: Epstein-Barr virus; HAV: hepatitis A virus; HBV: hepatitis B virus; HCV: hepatitis C virus; IHA: immune hemolytic anemia; IMRT: intensity-modulated radiation therapy; LDH: lactate dehydrogenase; PT: prothrombin time; RCC: renal cell carcinoma; TAH-BSO: total abdominal hysterectomy and bilateral salphingo-oophorectomy; snSPA: seronegative spondyloarthropathy; WBC: white blood cells.
Case 2
A man at the age of 61 presented with lombalgia and was diagnosed with RCC after a right-sided radical nephrectomy for a 12 cm right renal mass. He did not attend any of his routine follow-up appointments, for 19 months, until the time he developed pulmonary symptoms (shortness of breath, chest pain, and cough). Restaging studies put on multiple metastases in bilateral pulmonary parenchyma and mediastinal lymph nodes. His IMDC risk score was intermediate. Sunitinib was started for the first-line treatment. Two months after the initiation of sunitinib, he was admitted to the hospital with a sudden loss of consciousness. It was learnt that he described shortness of breath and palpitations for several hours. He had a 6 g/dL decrease in Hb level from baseline (from 10.5 to 4.5 g/dL). Spherocytes in the peripheral smear, elevated reticulocyte, LDH, bilirubin levels, and positive DAT with C3d were compatible with IHA (Table 1). Sunitinib was stopped and methylprednisolone started at a dose of 1 mg/kg/day. His Hb level gradually increased to the normal range in 3 weeks under steroid treatment. However, his mental status did not improve. Bilateral multiple cranial metastases were detected by cranial magnetic resonance imaging (MRI). Therefore, cranial radiotherapy was performed. Nevertheless, the patient died because of a cranial hemorrhage 1 month after the TKI-induced IHA diagnosis.
Case-3
A woman, aged 51 presented with abnormal uterine bleeding and images demonstrated a 7 cm uterine mass and a 6 cm right ovarian mass, 7 years ago. She went under total abdominal hysterectomy and bilateral salphingo-oophorectomy leading to the diagnosis of stage 2 uterine leiomyosarcoma with positive hormone receptor status. She had adjuvant intensity-modulated radiation therapy to the tumor bed. In her medical history, she was diagnosed with seronegative spondyloarthropathy and was under salazopyrin treatment. Four years later, her cancer relapsed with right-sided pulmonary metastatic nodules. Therefore, she was administered three cycles of ifosfamide-mesna-adriamycine palliative combination chemotherapy. After chemo, a new metastatic focus at the right acetabulum was detected. Megestrol acetate was the second-line treatment choice because of her poor tolerance to cytotoxic treatments. After 6 months under endocrine treatment, pulmonary metastases progressed radiologically. Therefore, the treatment was changed to pazopanib. Only 2 months after the initiation of pazopanib, she had rheumatic symptoms and methylprednisolone at a dosage of 16 mg/day and hydroxychloroquine 200 mg twice daily was started via rheumatology consultation. The steroid dose was adjusted by the rheumatologist depending on the activation of the rheumatologic disease. During this period, leiomyosarcoma was stable with a durable response under pazopanib treatment for 2 years. However, she presented with vertigo and fatigue for 2 days. Her laboratory studies showed a significant decrease in Hb levels from baseline (from 11.4 to 7.3 g/dL), increased LDH and indirect bilirubin levels. IHA diagnosis was verified with further evaluation including positive direct and indirect antiglobulin tests (Table 1). Pazopanib was discontinued and methylprednisolone dosage was increased to 1 mg/kg/day. The Hb level increased to normal in only 1 week and the DAT turned negative. Considering the durable response under pazopanib and the rapid recovery of IHA, pazopanib was restarted after a 1-month TKI-free period under the treatment of 1 mg/kg/day dose of corticosteroid and close monitoring of the laboratory tests. Luckily, signs of IHA were observed neither clinically nor in laboratory tests in long-term follow up. The steroid treatment was stopped gradually with a joint decision of hematology and rheumatology. It has been 47 months under pazopanib by the time we write this report and her cancer is still stable.
Discussion
We herein report three different drug-induced IHA cases caused by axitinib, sunitinib, and pazopanib, respectively. After an acute clinical presentation, elevated hemolysis markers and positive DAT for complement C3d led to the IHA diagnosis. All three cases were successfully treated with discontinuation of the causative drug and administration of methylprednisolone at a dose of 1 mg/kg/day. The outcomes in all the patients were mainly determined by underlying cancer rather than the treatment of IHA.
Anemia is a common type of hematologic toxicity of axitinib, sunitinib, and pazopanib. All grades of anemia prevalence were reported at 35%, 71%, and 24%, respectively. These high rates of prevalence may be explained by FLT-3 and c-KIT inhibition by these three TKIs, which are essential pathways for hematopoiesis. Moreover, VEGFR is the main target for these TKIs and the inhibition of the VEGF/VEGFR signaling pathway may lead to endothelial injury. 6 Several cases diagnosed with sorafenib, sunitinib, and pazopanib-induced coombs-negative microangiopathic hemolysis were reported.7, 8 Another mechanism of TKI-associated anemia is drug-induced coombs-positive IHA that was described with cases under imatinib, erlotinib, and afatinib previously.7, 9, 10 TKIs are presumed to interfere with B-cell activation causing humoral response by their off-target multikinase inhibitory effect. 11 Our cases are the first examples of axitinib, sunitinib, and pazopanib-induced coombs-positive IHA in literature to our knowledge. Naranjo causality risk assessment score was calculated as +4 (possible) for cases 1 and 2, and as +3 (possible) for case 3.
On the immune checkpoint inhibitory (ICI) side, it is more evident that these agents are associated with IHA. Durvalumab and avelumab were shown to cause IHA quite rarely, which could be a consequence of their infrequent use. 12 At the time our cases were treated, ICI therapies were not approved for the treatment of metastatic RCC.
Treatment of drug-induced IHA starts with the discontinuation of the possibly responsible agents. Supportive care is essential. Corticosteroid administration is recommended when these interventions are not enough to control the IHA. 1 However, we applied corticosteroids at a standard dosage (1 mg/kg methylprednisolone) to all three cases after diagnostic evaluations indicated IHA.
In conclusion, we should focus on the underlying mechanism of anemia in a cancer patient receiving antineoplastic treatment with a comprehensive evaluation. There may be life-threatening etiologies, as we reported. The accumulation of knowledge about these relatively new anticancer treatment agents is being improved over time. As long as we use these agents, proper diagnosis of the possible new adverse reactions and early intervention will be a part of good oncology practice.
Supplemental Material
sj-docx-1-opp-10.1177_10781552231202530 - Supplemental material for Tyrosine kinase inhibitor-induced immune hemolytic anemia; three different drugs in three separate cases
Supplemental material, sj-docx-1-opp-10.1177_10781552231202530 for Tyrosine kinase inhibitor-induced immune hemolytic anemia; three different drugs in three separate cases by Halil Göksel Güzel and Derya Kıvrak Salim in Journal of Oncology Pharmacy Practice
Supplemental Material
sj-docx-2-opp-10.1177_10781552231202530 - Supplemental material for Tyrosine kinase inhibitor-induced immune hemolytic anemia; three different drugs in three separate cases
Supplemental material, sj-docx-2-opp-10.1177_10781552231202530 for Tyrosine kinase inhibitor-induced immune hemolytic anemia; three different drugs in three separate cases by Halil Göksel Güzel and Derya Kıvrak Salim in Journal of Oncology Pharmacy Practice
Supplemental Material
sj-docx-3-opp-10.1177_10781552231202530 - Supplemental material for Tyrosine kinase inhibitor-induced immune hemolytic anemia; three different drugs in three separate cases
Supplemental material, sj-docx-3-opp-10.1177_10781552231202530 for Tyrosine kinase inhibitor-induced immune hemolytic anemia; three different drugs in three separate cases by Halil Göksel Güzel and Derya Kıvrak Salim in Journal of Oncology Pharmacy Practice
Footnotes
Authors’ contributions
HGG collected the data of the patients. HGG and DKS contributed to the writing of the manuscript and literature research. DKS reviewed and edited the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of ethics
Written informed permission was obtained from the patients/families for all three cases.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.