
Abstract
Introduction
To achieve continuous environmental sustainability and protect the population's health, healthcare waste (in liquid or solid form) needs appropriate management and suitable treatment strategies before its final disposal in the environment in order to reduce its adverse impacts. This study aims to identify disparities in the waste management of anti-cancer drugs and the wastewater generated in Lebanese hospitals.
Methods
Three questionnaires were designed to evaluate the level of knowledge, awareness and experience of hospital personnel regardless of their job levels. Data was collected in December 2019 from three departments of each participating hospital: pharmacy, oncology and maintenance departments. A descriptive analysis was conducted to summarise the survey results.
Results
The results revealed a lack of transparency and awareness of the participants, with a high frequency of ‘prefer not to say’ responses when asked about the disposal methods of anti-cancer drugs and with only 5.7% of the participants in the pharmacy department sharing their disposal procedures. The same perception was deduced regarding hospitals’ wastewater treatment, where responses were often contradicting, preventing making assumptions about the fate of hospital wastewater.
Conclusion
The results of this survey support the need to establish a more comprehensive waste management programme in Lebanon that would be maintained through regular training and supervision.
Introduction
The Lebanese health sector is one of the major and most developed sectors contributing significantly to the country's economy. Nevertheless, despite the fact that improvements have been recognised in terms of industrial and medical waste management, Lebanon still lacks satisfactory infrastructures for the appropriate handling and disposal of these wastes. In consequence, environmental concerns have been accumulating over the years, including air pollution from uncontrolled waste burning and water and soil pollution from inappropriate waste and effluents disposal. 1
The medical field is mainly operated by the private sector, with more than 90% of Lebanese healthcare facilities considered private. According to the laws established by the Ministry of the Environment, healthcare facilities are solely responsible for managing the waste generated by each of their departments. In fact, Lebanon has signed 28 international and 7 regional conventions for the protection of the environment. 2 Furthermore, on a national level, the Lebanese Ministry of the Environment has formulated and published several laws and decrees in their official gazette regarding the protection of the environment from any pollution and the management of healthcare waste (e.g., laws 64 and 690 and the decree 13,389). These can also be accessed on the Ministry's official website. 3
Although laws and decrees define the roles of each institution and the guidelines to follow for the disposal of waste, it has been found that the regulations lack clarity and precision. This has been revealed by the frequent overlapping of responsibilities and the absence of coordination between the different authorities. Additionally, these laws continue to be weakly enforced due to a lack of training and awareness of regulations among the assigned personnel, low levels of fines and political interventions. 1
Hospital wastewater is a major source of surface water contamination by microorganisms, pharmaceuticals residues and other emerging pollutants; however, when it comes to hospital waste management, the attention is usually more shifted toward the solid waste generated. In Lebanon, most water resources are contaminated with untreated wastewater, which raises questions about the circumstances of hospitals’ infrastructures regarding sewerage systems and the fate of hospitals’ wastewater. Hence, the aims of this study are to investigate the status and to identify the gaps regarding hospital wastewater management and, more specifically, the waste management of anti-cancer drugs. This will be achieved by: (1) assessing the knowledge, awareness and experience of the personnel regarding the disposal operations of anti-cancer drugs adopted by the oncology and pharmacy departments of the hospitals; (2) assessing the knowledge, awareness and experience of the personnel regarding waste and wastewater management in the oncology, pharmacy and maintenance departments; and (3) understanding the current and future plans for improving waste disposal.
Methods
Purpose of survey
This survey is an exploratory and descriptive study with the purpose of understanding this particular topic area without any prior knowledge of the expected responses. The survey was designed to describe the attitude and level of awareness of the hospitals’ personnel in regard to wastewater management.
Setting and participants
Lebanese hospitals, whether public or private, that comprise an oncology/chemotherapy department are included in this study. According to the Syndicate of hospitals and the Lebanese society of medical oncology, 62 registered facilities provide cancer treatment services and hence, were invited to participate in this study. As the population in each hospital is too large to examine, convenience sampling, which is a non-probability sampling technique, was adopted. For this study, three participants from each hospital were selected randomly regardless of their positions: one from the oncology department, one from the pharmacy department and one from the maintenance department.
Survey instrument
This study was conducted using an investigator-developed survey instrument. Three questionnaires were developed for each department, including 9 questions for the maintenance department, 10 questions for the pharmacy department and 13 questions for the oncology department. The questions were formulated in a way to allow insight into participant knowledge, awareness and experience of anti-cancer drugs disposal and wastewater management.
Ethical considerations and negotiation of access
This research project was considered by the Faculty Research Ethics Committee of Kingston University and was granted a favourable ethical opinion on 20 September 2019 (1819 094.1 Hospital survey for waste management strategies in Lebanon).
After ethical approval, the survey was translated into Arabic and French to allow the participants to choose a language they were comfortable with. Before starting the survey, participants were informed of the purpose of the study and were provided with a participant information sheet and consent form. Participants were guaranteed complete anonymity and confidentiality and made aware of their right to withdraw at any time.
Data collection and statistical analysis
Data was collected through face-to-face meetings with the participants in December 2019. The questionnaires were labelled according to the coding system created to guarantee the anonymity of the participants. Moreover, the three questionnaires of each hospital were completed separately to maintain anonymity and prevent the answers from being affected by the other members of staff. The responses to the questionnaire were recorded and processed using Statistical Package for the Social Sciences (SPSS) software, version 27.0 and Microsoft Excel, version 2205. Descriptive statistics were used for the analysis of the data, and they were presented in the form of frequencies and percentages.
Results
Fifty-three out of the 62 eligible hospitals participated in the study. Eighteen hospitals are located in Beirut, 12 in the Metn-Baabda area, 8 in Beqaa, 8 in the North of Lebanon, 5 in the South of Lebanon, 1 in Chouf and 1 in the Kesrouan-Jbeil area. Although two hospitals have closed their chemotherapy departments since the survey was carried out due to financial issues, the complete results of the survey are presented in the tables below (Tables 1 and 2) and discussed in this study.
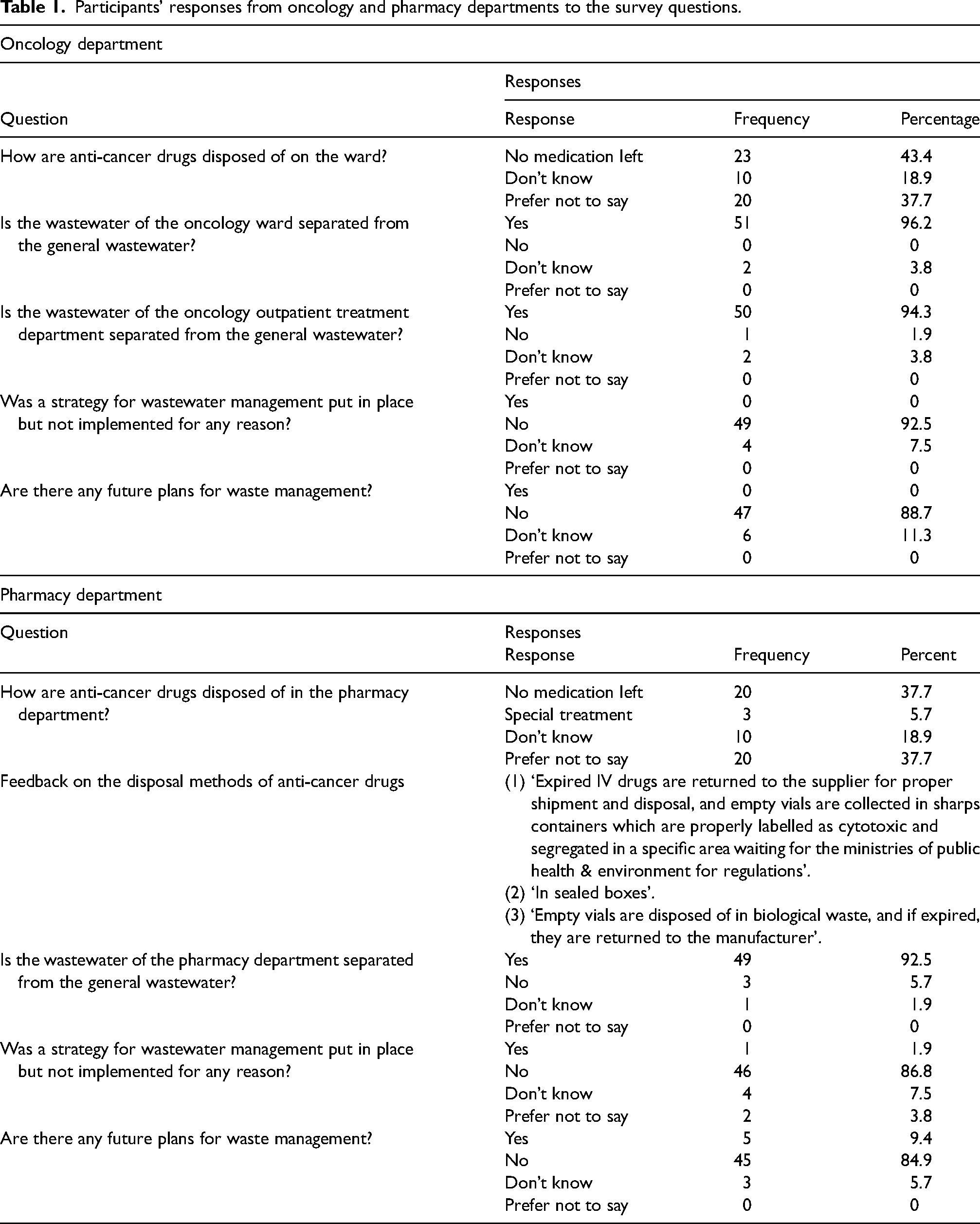
Participants’ responses from oncology and pharmacy departments to the survey questions.
Participants’ responses from the maintenance department to the survey questions.
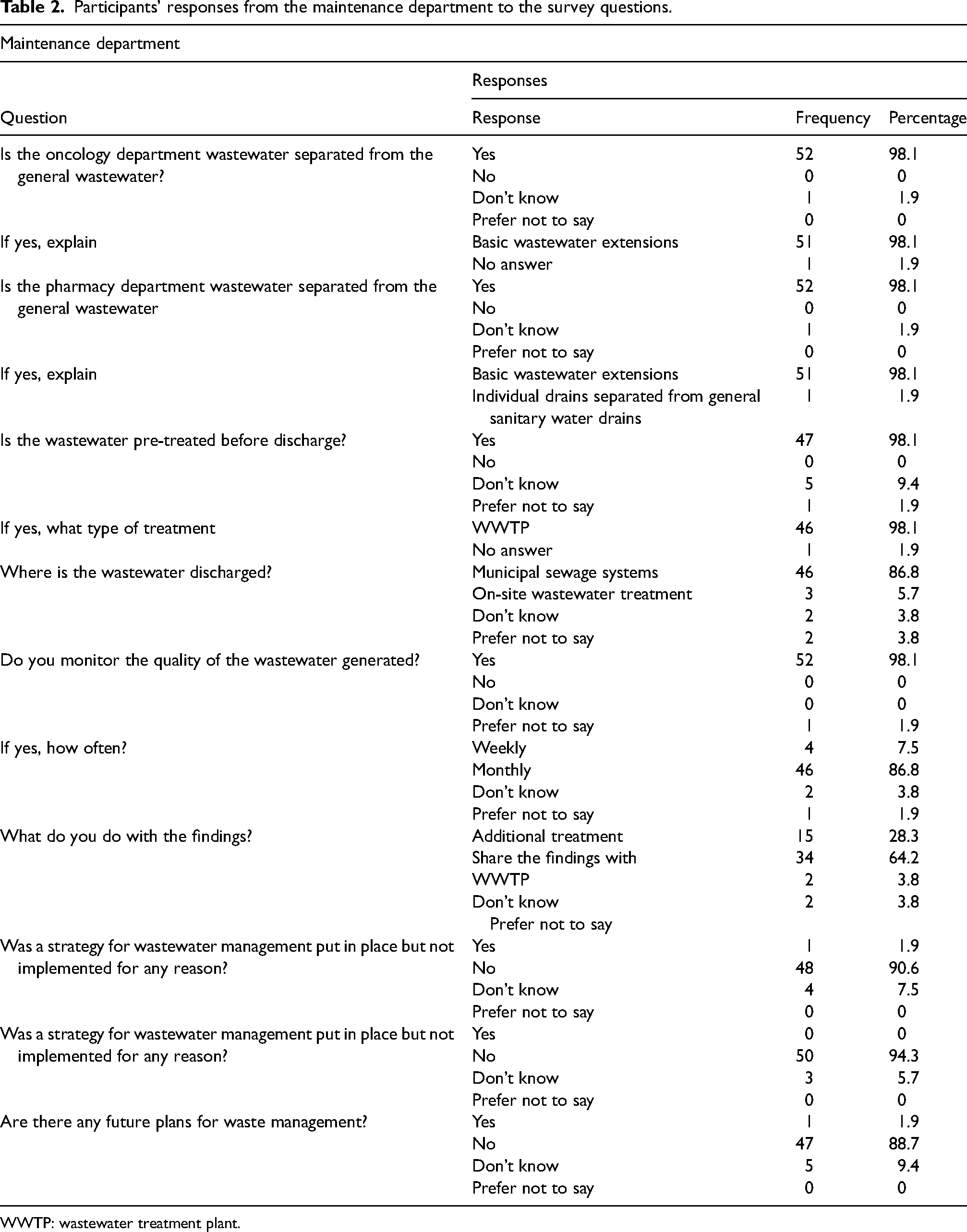
WWTP: wastewater treatment plant.
During the data collection, participants were reluctant to take part and share any information, possibly worried about any repercussions in case non-compliance was revealed. This was mainly demonstrated by the high frequency of the ‘prefer not to say’ response when asked about the disposal methods of anti-cancer drugs (37.7% in oncology and pharmacy departments). The remaining respondents, 43.4% and 37.7% from the oncology and pharmacy departments, respectively, answered that no medication is left on the ward for disposal, and 18.9% from both departments stated that they did not know.
Only 5.7% in the pharmacy department group, which accounts for 3 participants, have shared their disposal procedures (Table 1). Concerning wastewater management, the majority of the participants in both departments responded that the wastewater of the oncology and pharmacy departments is separated from the general sewerage system, that there was no strategy put in place for wastewater management and not implemented for any reason and that there are no future plans for waste management.
The responses from the maintenance department (Table 2) have revealed that the wastewater from the oncology and pharmacy divisions is separated from the general wastewater by basic wastewater extensions and that the wastewater generated is pre-treated by wastewater treatment plants (WWTPs) before discharging it into the municipal sewage systems. The participants claimed that they monitor the quality of the wastewater mostly every month. Most respondents (64.2%) share their findings with the appropriate WWTPs, while 28.3% conduct an additional treatment if needed. As with previous outcomes, it mainly appeared that no strategy for wastewater management was put in place and was not functional or implemented. Moreover, there are no future plans for waste management.
Only one participant from the maintenance department was keen to share their thoughts and comments about the actual situation of wastewater management. They stated that: ‘We have looked into building a wastewater treatment plant (WWTP) inside the medical centre; however, this was not feasible and easy to apply due to the Lebanese regulations and difficult misunderstood standards. In our country, every area should have its own WWTP. Unfortunately, in this area, we have the plant, but it's malfunctioning. This, in return, would make it difficult for institutions to start planning wastewater treatment’.
Discussion
Cytotoxic waste management in Lebanese hospitals
In summary, this study has revealed several issues in terms of waste management. The main findings of this survey were the lack of transparency and awareness of the participants. In fact, the responses were, at times, inconsistent and contradictory. For example, most participants answered that the wastewater from the pharmacy and the oncology departments is separated from the general wastewater by a basic sewerage system. However, if this contaminated wastewater is not pre-treated on-site, it will end up with the general wastewater in the main sewage pipeline that is connected to the WWTP. Consequently, stating that the wastewater is pre-treated by WWTP was conflicting and brought into question the authenticity of the responses and the participants’ knowledge.
Additionally, it seemed from the few statements given, that the regulations set by the Ministry of the Environment were unclear and required more guidelines and instructions regarding anti-cancer drugs disposal. This was revealed by the different methods of disposal described by the participants. For instance, disposing of empty vials of anti-cancer drugs in biological waste is inappropriate since both categories require different treatment procedures. Besides, storing cytotoxic waste without treatment for an extended period of time is not recommended, according to World Health Organisation (WHO). 4 It also depends on the facility's storage capacity and requires proper handling to prevent any accidental leaks and spillages. Moreover, the fact that the majority of the participants responded that there is ‘no medication left for disposal’ is alarming. This statement could be an indication of a lack of knowledge and awareness regarding waste segregation and hence, disregarding the fact that empty vials, sharps or personal protective equipment (PPE), among others, used during the preparation of the treatments are also contaminated with anti-cancer drugs and should be disposed of following the same procedure.
Although Lebanese laws and decrees state that each facility should manage and treat its own generated waste, it was apparent, from the limited information provided, that: on one side, the hospitals are still dependent on the Ministries of Public Health and the Environment and waiting for more regulations in order to improve their waste management procedures. On the other side, authorities seem to prevent the implementation of new strategies or any attempt for amelioration.
In addition, the responses on how the wastewater is separated and pre-treated before discharge were unclear and did not provide sufficient information to assess the wastewater management status. However, studies have shown that Lebanon's actual WWTP services are unsatisfactory. This is reflected by the high level of surface water pollution, and the continuous discharge of untreated sewage directly into the water streams.5,6
A previous study conducted between October 1997 and August 1998 covered the status of hospital waste management in Lebanon. The authors have found that 75% of the surveyed hospitals do not know the quantity of the total waste generated by their facilities, and 73% segregate their waste into different categories, including infectious, pathological, sharps and pharmaceuticals. It was also revealed that more than 40% of the participating hospitals dispose of their hazardous waste together with the municipality's general waste, 24% burn their waste in the open air, 14% treat their waste by on-site incineration, 11% dispose of their hazardous waste in their on-site dumping site, 8% of the hospitals transfer their waste to private contractors, and 1% of the hospitals dispose of their waste in uncontrolled landfill. 7 The results obtained by this study were concerning as this uncontrolled management is a threat to the environment and a risk to public health. However, this was most probably due to the lack of laws and regulations, which were published later on in 2002.
Another study was conducted in Lebanon to assess the generation rate of infectious healthcare waste between 2009 and 2013. The results showed that the overall quantity of waste produced by the Lebanese hospitals is 44.14% higher than the value estimated by WHO for the Middle East region. This implies a deficiency in the segregation procedure and a mismanagement of healthcare waste. Moreover, by the trends observed over the 5 years, it was revealed that most of the investigated hospitals do not have a stable production of waste which means that the healthcare facilities have a defective monitoring management system for this. 8 Although this study includes only infectious waste, it could be an indication of how other categories of hazardous waste are handled in Lebanese hospitals.
A recent report about the Lebanon health resilience project was published in 2019 on the Ministry of public health website, including minutes of meetings with the non-governmental organisation (NGO), Arcenciel (AEC). AEC currently treats 85% of the total Lebanese infectious waste by autoclaving in its four treatment facilities. After sterilisation, the waste is disposed of in landfills in the same way as household waste. The rest of the infectious waste is either treated by autoclaves installed in the hospitals, handled by Safe/Mirage, which is another company that has one autoclaving treatment facility or is illegally dumped. 9
In general, the main legal techniques used for the treatment of healthcare hazardous waste are disinfection/sterilisation and thermal treatment. 10 Since autoclaving does not apply to all the categories of hazardous waste, including pharmaceutical and cytotoxic waste, installing an incinerator is essential.11,12 Pharmaceutical and cytotoxic waste are usually returned to the supplier or incinerated at high temperatures (up to 1200°C). In Lebanon, the available treatments for this category include returning the drugs to the supplier and storing the waste inside the hospital before exporting it, according to the Basel Convention. 13 Unfortunately, in 2015 hazardous waste exportation to and from the Organization for Economic Co-operation and Development (OECD) countries was banned, which has reduced the options for waste treatment. 9
Regarding thermal treatment, in 2004 and 2005, the Ministry of Environment approved three licenses for the treatment by incineration; however, these licenses were not reinstated. 1 Consequently, considering the unknown fate of pharmaceuticals and cytotoxic waste, it is recommended to establish a local incinerator or authorise the use of existing incinerators currently servicing other industries. 14
Comparison with the status of waste management globally
Usually, numerous challenges are faced when implementing healthcare waste management regulations. These include healthcare administration not allocating enough funds, untrained workers controlling infectious waste and outdated technologies and procedures for waste disposal. 15
Globally, research has highlighted several gaps and weaknesses in healthcare waste management and disposal. 16 The compiled studies have reviewed the hospital waste management conditions in different countries, including Greece,11,17,18 Lao PDR, 19 Brazil,20,21 China,22,23 Kingdom of Bahrain, 24 India,25–32 South Africa,33–36 Malaysia, 37 South Korea, 38 the United States, 39 Palestine, 40 Egypt,41,42 Mauritius, 43 Algeria, 44 Libya, 45 Portugal, 46 Pakistan, 47 Ghana, 48 Indonesia, 49 Australia, 50 Taiwan,51,52 Jordan,53–55 Turkey,56,57 Mongolia, 58 Asia Continent, 59 Botswana, 60 Madagascar, 61 Nigeria,62–64 Croatia, 65 Saudi Arabia, 66 Iran67–71 and the United Kingdom.72,73
Almost all the studies have identified the same common issues of inadequate waste management. The main problems detected were at the source of waste management. Healthcare workers lacked awareness and knowledge, which was shown by the improper segregation and inadequate use of personal protection equipment while handling the waste. This is due to the absence of training, follow-up training programmes and supervision. Simultaneously, not having clear responsibilities for staff members to manage and coordinate the waste management activities and not complying with guidelines or having a well-structured healthcare waste management plan aggravated the problem.
Poor segregation practices will either lead to hazardous waste ending up with general waste in landfills without pre-treatment or to a high volume of the hazardous waste which will unnecessarily increase the load for incineration and any other treatment. 11 As a consequence, pollution of soil and groundwater is expected, 56 in addition to the exposure of workers and the community to such waste. 61 Furthermore, non-compliance of hospital incinerators with the standards was reported in several studies, thus, posing significant risks to the environment and public health by the emission of toxic smoke and gases.11,33,44,54,66
Many researchers have attempted to introduce a waste management plan in healthcare facilities and documented the implementation outcomes. Significant improvement in waste management was recorded in Pakistan, 47 Australia, 50 Saudi Arabia, 66 the United Kingdom 73 and Iran 71 by achieving higher scores in terms of knowledge, attitude and practices and by reducing drastically the quantity of the waste generated. This affirms the importance of training and applying an efficient waste management plan.
As for healthcare wastewater, only a few studies have reported their management methods. For instance, in Greece, most hospitals do not have a separate sewerage system. The rest have a different drainage system and treat their liquid waste by chemical neutralisation with H2SO4 and NaOH, where only the pH is assessed and not the toxicity.17,18 Another study conducted in a South India hospital has also shown that liquid waste is chemically treated before discharging in municipal treatment plants as there are no local treatment facilities on-site. 27 In Jordan, almost half of the surveyed hospitals discharge their medical wastewater into the municipal sewage without pre-treatment and the other half discharge it in septic tanks. 54 Finally, in Iran, several methods are adopted for the disposal of liquid pharmaceutical and chemical wastes, such as discharge into adsorbent wells, transportation in tankers outside the hospitals, sewage treatment system on-site, release in the municipal sewage system or into nearby streams.67,69
Cytotoxic waste management in Lebanese households
Apart from wastewater emerging from hospitals, around 80% of the active pharmaceutical ingredients in municipal wastewater originate from households. 74 Mainly, pharmaceuticals reach the aquatic environment from households through four routes: (1) excretion after administration; (2) disposal in the municipal solid waste; (3) flushing down the toilet and (4) bathing (for topical medications)75–77. Nevertheless, the reasons behind the occurrence of pharmaceuticals in water resources are poor wastewater removal rates and landfill leachates.75,78
A study assessing the disposal methods of household pharmaceuticals in Lebanon has revealed that 78% of the respondents disposed of their solid medications in municipal solid waste. Regarding liquid waste, 73% of the participants discarded their medications with the solid waste, and 17% emptied the bottles into the drain. Only 4.4% bring back expired or unused medications to dispensaries or return them for redistribution to people in need. Since 95% of the respondents did not receive guidance on the safe disposal of pharmaceuticals; the authors suggest that this is due to the lack of awareness programmes and a national framework for the management of household pharmaceuticals. 76 Hence, a new strategy is needed in Lebanon. This should include the communication of the risks related to pharmaceuticals in the environment and the roles of each of the authorities and the citizens in managing these risks.14,77
Accordingly, patients handling anti-cancer drugs at home, should be a matter of concern given that chemotherapy treatment has shifted to outpatient administration. The education of patients by the healthcare nurse and oncologist is essential in order to avoid the exposure of cohabitants to anti-cancer drugs and the inadequate disposal of unused or expired drugs. In this case, take-back programmes are usually organised by hospitals where the patient is advised to return any leftover drugs to the healthcare facility.78–80
Conclusion
This survey aimed to assess the management of cytotoxic waste and wastewater in Lebanese hospitals. According to results obtained from the 53 participating hospitals, there appeared to be a lack of awareness and knowledge regarding anti-cancer drug disposal and wastewater treatment. This was highlighted by the improper segregation of anti-cancer drugs in addition to the lack of clear and extensive regulations for waste management. However, the information provided for wastewater management was inconsistent and insufficient to determine the actual condition and derive conclusions. In comparison with previous studies conducted in Lebanon, the same issues were identified in regard to hospital solid waste segregation.7,8,76
Regarding the treatment of chemotherapeutic waste, it was recommended by the WHO to incinerate it at high temperatures or chemically degrade the waste. However, it was proved that both methods are not entirely effective for the treatment of contaminated items, spillages, or biological fluids. 4 This means that until an emerging technology is available, hospitals are advised to handle cytotoxic wastes with utmost care and discard them safely.
Taking into consideration the guidelines provided and the results obtained from this study and previous studies conducted in Lebanon and globally, a number of recommendations could be proposed for an improved waste management system:
As currently most of the infectious hospital waste is treated by an NGO, more effort is required from governmental bodies and hospitals to be more involved and work toward improving waste management. A national healthcare waste plan should be established and enforced by the authorities with regular supervision and auditing. Cooperation between the government and healthcare facilities should be sustained to implement a secure and reliable waste management strategy. If no national guidelines are introduced, the hospitals should not be prevented from establishing a suitable waste management programme. All healthcare workers should be trained regularly to maintain sustainable practices, promote source reduction and increase the level of awareness. This could be achieved by initially forming a waste management committee and assigning roles and responsibilities. This committee could then develop a training programme suitable for all workers regardless of their positions. Ideally, training should be carried out for all workers before starting work handling waste. Subsequently, refresher courses should run on a regular basis to update and improve their knowledge and skills. As households are a major source of environmental pollution by pharmaceuticals, it is essential to create public awareness of the potential risks and promote engagement by developing return-back programmes across the country and optimising drug prescription and purchasing. This could be accomplished by the oncologist or healthcare provider by familiarising the patients with the type of treatment they will receive, the risk of exposure of other household members and the optimal methods for prevention and disposal. This could be supported by distributing a patient leaflet for best practice guidance and a box to dispose of all contaminated PPE or unused drugs to return to the hospital on their next visit.
Footnotes
Author contributions
CN and SN-G researched literature and conceived the study. CN was involved in protocol development, gaining ethical approval, participant recruitment and data analysis. CN wrote the first draft of the manuscript. SN-G, SJB and JB supervised the project, and reviewed and edited the manuscript. All authors approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.