
Abstract
Introduction
Antineoplastic drugs (ADs) are commonly used pharmaceuticals for anticancer treatments. It has previously been shown that the external surface of drug vials frequently is contaminated with ADs. More than a decade ago methods to prevent occupational exposure were introduced by using plastic coverage of the glass vials or packing vials in a secondary plastic container. The aim of the pilot study was to determine contamination levels of ADs on different parts of AD packaging of two different commercially available drug vials on the Swedish market and to investigate the occurrence of cross contamination of ADs.
Methods
Packagings of gemcitabine (GEM) and 5-fluorouracil (5-FU) were tested by wipe sampling. Five ADs; GEM, 5-FU, cyclophosphamide (CP), ifosfamide and etoposide were quantified using liquid chromatography mass spectrometry.
Results
AD contaminations were detected in 69% and 60% of the GEM and 5-FU packaging samples. Highest levels, up to approximately 5 µg/sample, were observed on the glass vials. The protective shrink-wrap of 5-FU vials and the plastic container of GEM were contaminated with low levels of 5-FU and GEM, respectively, and furthermore the 5-FU vials with shrink-wrap were cross-contaminated with GEM. Cross-contamination of CP and GEM was detected on 5-FU vials with plastic shrink-wrap removed.
Conclusions
External contamination of ADs are still present at primary drug packagings on the Swedish market. Protection of AD vials by plastic shrink-wrap or a secondary plastic container does not remove the external contamination levels completely. The presence of cross contamination of ADs on drug packagings was also observed.
Introduction
Antineoplastic drugs (ADs) are frequently used pharmaceuticals in the patient care for anticancer treatment. Due to the mutagenic, carcinogenic, and teratogenic toxicity of the ADs, safe handling practices are required in order to limit occupational exposure.1–3 Exposure of health care professionals can potentially occur during the preparation and administration of ADs but also during patient care since ADs can be excreted via body fluids. Awareness of how ADs can contaminate surfaces in the working environment can increase by measuring levels of ADs e.g. by wipe sampling. Studies have shown that contamination levels may be reduced by recurrently measuring ADs at selected surfaces that can pinpoint optimal handling and cleaning routines. 4 Wipe sampling has shown that surfaces that can be contaminated includes areas where ADs are prepared and administered, and flooring of patient lavatories in hospitals5, 6 but it has also been shown that the external surface of drug vials frequently is contaminated by the drug that it contains.7–12 Although it has been known since the beginning of the nineties that the exterior of drug vials may be contaminated recent studies still find that levels of contaminations remain the same with no clear decline in the proportion of positive containers.13–15 However, Connor et al. showed that by covering drug vials in sleeves the levels of contamination could be effectively reduced. 7 Subsequently many manufacturers have introduced similar methods to prevent exposure by applying plastic coverage of the glass vials (plastic shrink-wrap) or packing vials in a secondary plastic container. 16
The aim of this pilot study was to determine contamination levels of ADs on different parts of AD packaging of two different commercially available brands on the Swedish market. The aim was also to determine cross-contamination of ADs other than the one contained in the drug vial. AD levels were determined all the way from the external surface of the outer packaging in to the protective layers (shrink-wrap plastic or plastic container) and the glass vial.
Method and materials
Chemical and materials
Cyclophosphamide monohydrate (CP, purity 99.5%), 5-fluorouracil (5-FU), and 5-fluorouracil-15N2 were purchased from Sigma-Aldrich (St Louis, MO, USA) and cyclophosphamide-d6 (CP-D6; purity 97%) from Phychem (Bergisch Gladbach, Germany). Ifosfamide (IF, purity >98%, Holoxan®) was purchased from Baxter Medical (Halle, Germany). Ifosfamide-d4, purity 98%), gemcitabine hydrochloride (GEM, purity 98%), gemcitabine-13C1, 15N2 hydrochloride, purity 98%, etoposide (ETO, purity 98%) and etoposide-d4 (purity 97%) were purchased from Toronto research chemicals (Toronto, Canada). A mixture of internal standards (IS) was prepared by dilution in ultrapure water at a final concentration of 0.5 µg/mL (cyclophosphamide-d6, ifosfamide-d4, gemcitabine-13C1, 15N2 hydrochloride); 1 µg/mL (etoposide-d4); 3 µg/mL (5-fluorouracil-15N2), respectively. Ethyl acetate (HPLC grade) and methanol (MeOH, HPLC grade) were purchased from Lab-Scan (Dublin, Ireland). Acetic acid (glacial, p.a. > 99.8%) came from CCS Healthcare AB (Borlänge, Sweden). Ultrapure water was obtained from the water purifier system Milli-Q Integral 5 from Merck Millipore (Billerica, MA, USA).
Wipe sampling of drug vials
No ADs had previously been handled in the room where the wipe sampling was performed. Packaging containing solution for injection of 5-FU at 50 mg/mL (100 mL glass vial) manufactured by Accord® (N = 10, batch P2005831) and packaging containing solution for injection of GEM at 40 mg/mL (50 mL glass vials) manufactured by Sandoz® (N = 10, batch LD5283) were tested (Table 1). The packagings were delivered from the Swedish distributor to a hospital pharmacy in the south of Sweden. The packagings were then supplied from the hospital pharmacy in 2021. The 5-FU packaging was composed of a plastic shrink-wrap protected glass vial enclosed in an outer cardboard box (Figure 1) whereas the GEM glass vials were kept in plastic containers enclosed by a cardboard box (Figure 2). The primary packagings were inspected before sampling and no signs of damage were detected. The packagings were sampled using wipe test 1 described by Kåredal et al. 17 and the different layers of surfaces were successively wipe sampled according to the sampling list shown in Tables 2 and 3. The outside and inside of the outer cardboard box were sampled individually, as were the outside and inside of the plastic container of the GEM units. The cardboard boxes were cut open by a pair of scissors that was cleaned between each wipe sampling. The vials and containers were unpacked from the cardboard boxes using a tweezer in order to avoid contamination. The tweezer was cleaned between each sample. The 5-FU units were first sampled with the plastic shrink-wrap kept on and then after removal of the plastic coverage generating separate samples. The packaging leaflets inserted in the primary packaging were sampled on both sides without unwrapping them. Briefly, wipe sampling was performed using a pair of non-woven tissue wipes (50 × 50 mm, 45% polyester/55% cellulose, Dastex, Muggensturm, Germany) each moisten with 200 µL milliQ-water. Each surface was wiped with S-formed motion in two directions. After wiping the tissues were placed in 50 mL polypropylene (PP) tubes (Sarstedt, Nümbrecht, Germany), put in a plastic bags and stored at −20 °C until analysis. Between each sample, a new pair of gloves was used and between each packaging sample the desk was cleaned with high-absorbent wipes and water. During the course of the sampling six blank samples per brand were prepared to control material contamination.
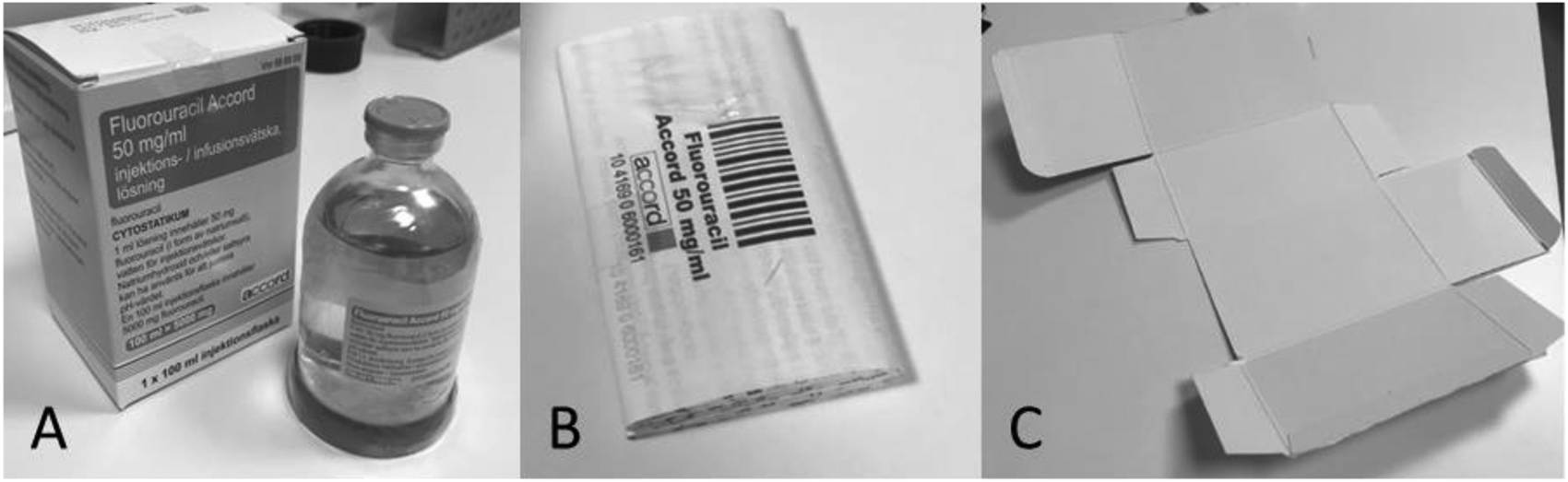
5-Fluorouracil Accord cardboard box, drug glass vial with plastic shrink-wrap (A), package leaflet (B) and inside surface of outer cardboard packaging (cut open, C).
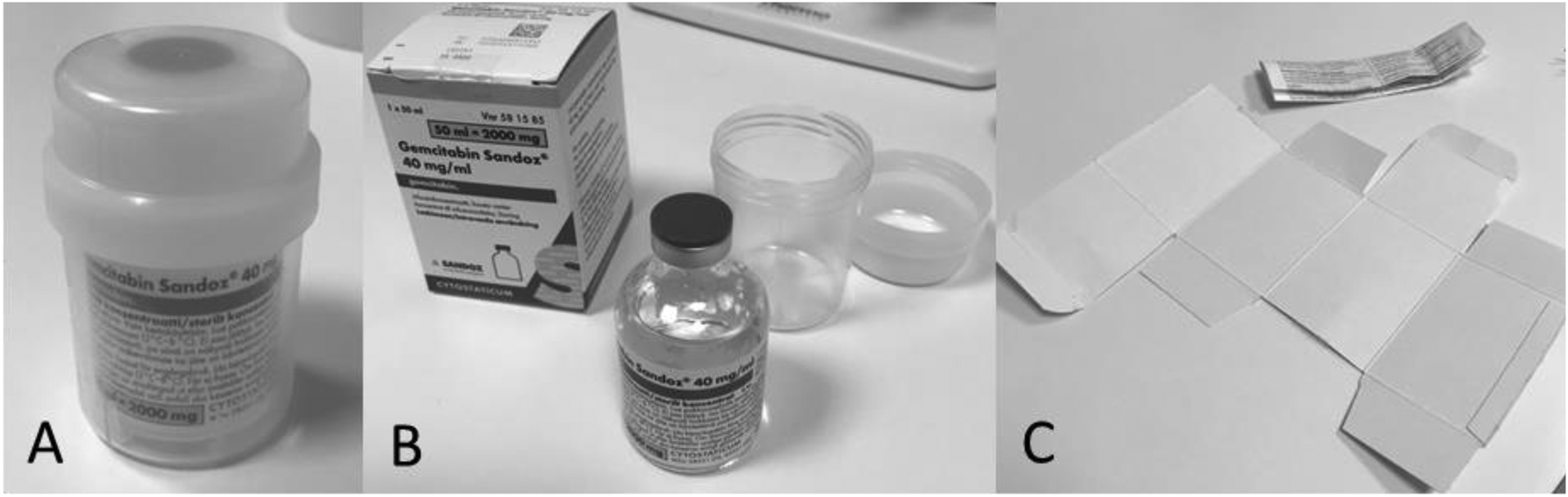
Gemcitabine Sandoz plastic container (A), cardboard box, drug glass vial (B), package leaflet and inside surface of outer cardboard packaging (cut open, C).
Tested antineoplastic drug vials commercially available on the Swedish market.
External contamination measured at six different sample points of 5-FU packaging Fluorouracil Accord®.
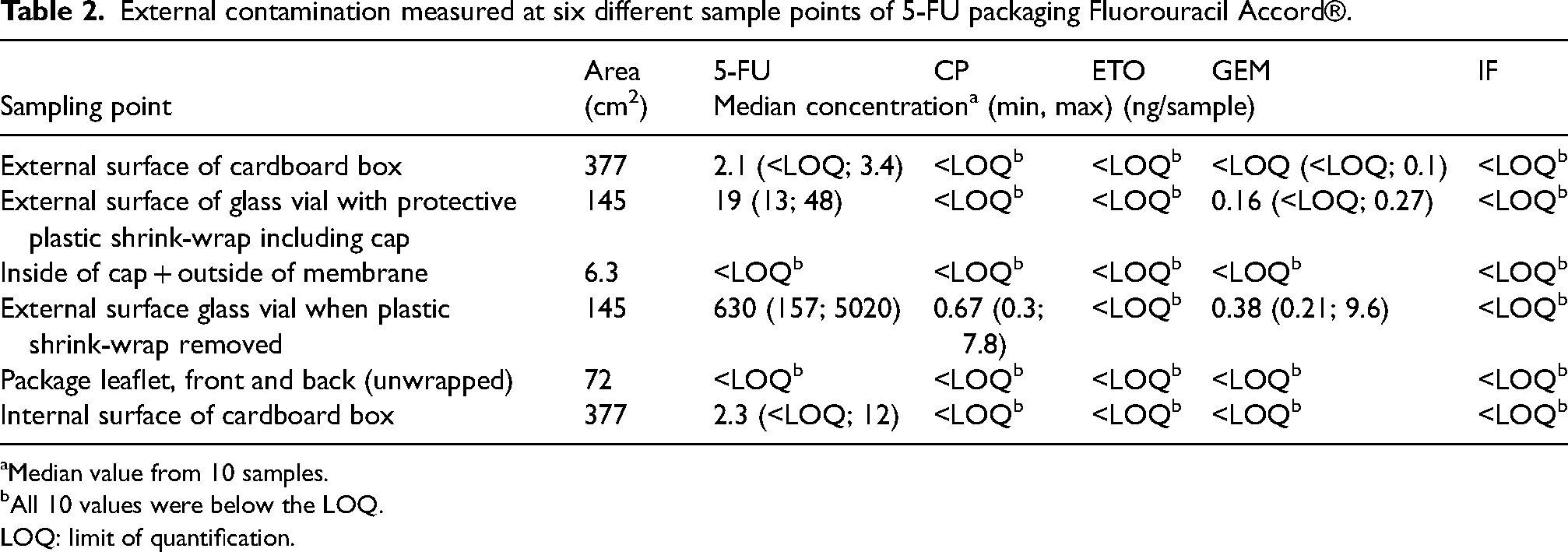
aMedian value from 10 samples.
bAll 10 values were below the LOQ.
LOQ: limit of quantification.
External contamination measured at seven different sample points of GEM packaging Gemcitabin Sandoz®.
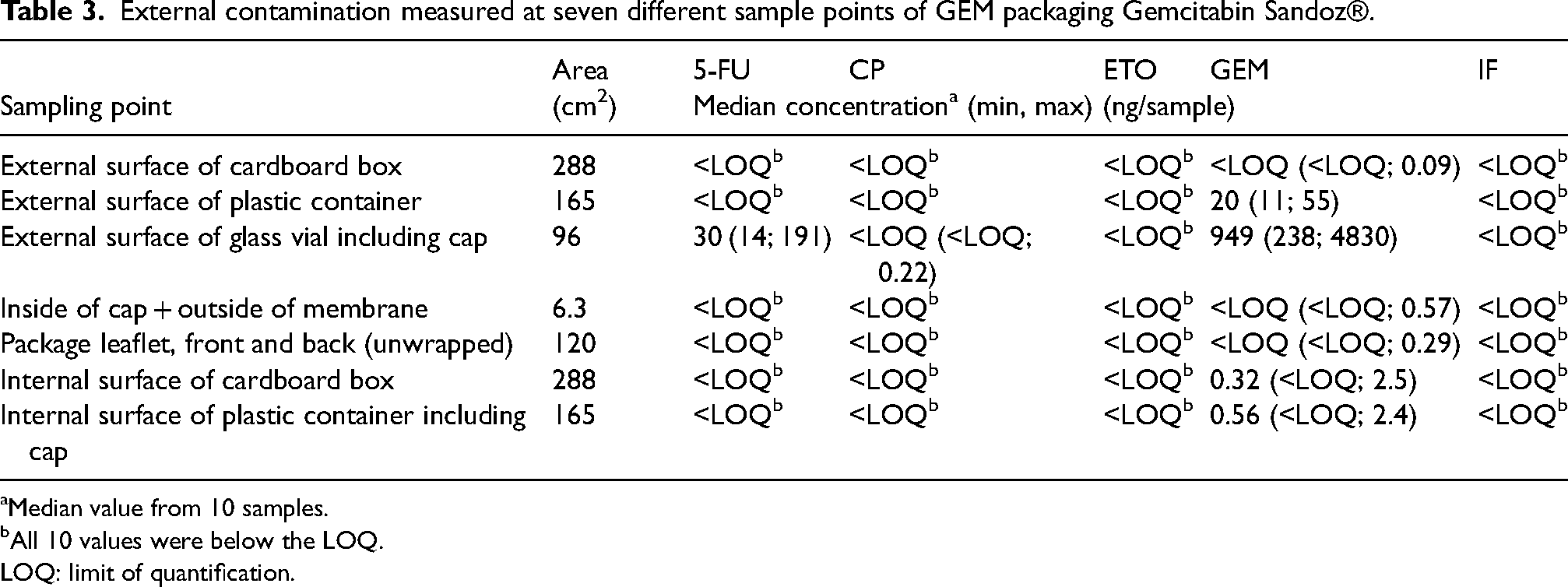
aMedian value from 10 samples.
bAll 10 values were below the LOQ.
LOQ: limit of quantification.
Sample preparation and chemical analysis
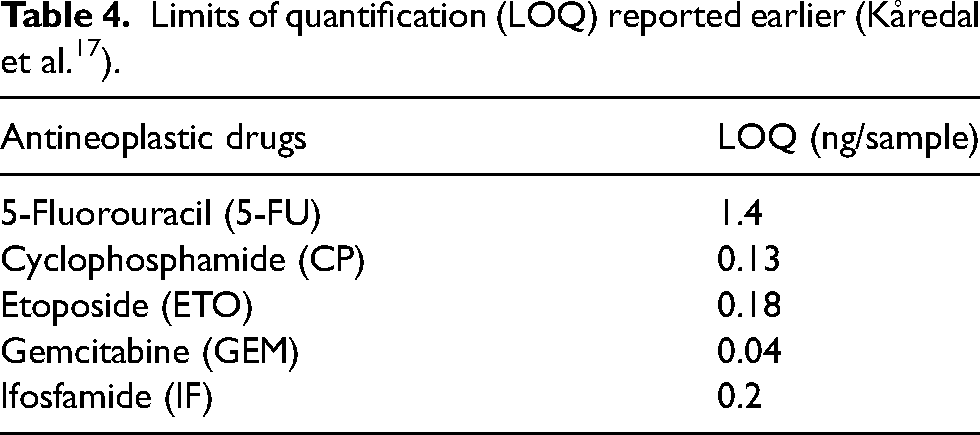
Samples were prepared and analyzed by liquid chromatography (LC, UFLCXR; Shimadzu Corporation, Kyoto, Japan) coupled to mass spectrometry (MS) according to sample procedure of wipe test 1 described earlier 17 with the exception of the analysis instrument that was performed using a QTRAP 4500 MS (Sciex, Framingham, MA, USA). IS solution in 100 µL aliquots was added to the wipe samples and ADs were extracted from the wipe tissues in 20 mL ethyl acetate. Samples were vortexed and 10 mL was transferred to 12 mL borosilicate glass tubes (Fisher Scientific, Hampton, NH, USA) and evaporated to dryness (SpeedVac SPD300DDA, Thermo Fisher Scientific, Asheville, NC, USA). Samples were dissolved in 150 µL 0.5% acetic acid in milliQ water. ADs were separated on a reversed phase C18 column (Thermo Hypersil gold aqua C18, 3 µm, 50 × 2.1 mm, Thermo Fisher Scientific, Waltham, MA, USA) and five ADs were analyzed; 5-FU, CP, GEM, ETO, and IF. Samples were analyzed in four batches and randomly included in either run to avoid analytical systematic errors. Limit of quantification (LOQ) for each AD is presented in Table 4.
Limits of quantification (LOQ) reported earlier (Kåredal et al. 17 ).
Results
In total, 12 blank samples, 60 samples from the 5-FU packaging (36/60 positive for at least one AD (60%)) and 70 samples from the GEM packaging (48/70 positive for at least one AD (69%)) were collected. All blank samples were blank, i.e. found not to contain any quantifiable amounts of ADs. In the samples varying levels of ADs were detected, median levels and ranges were reported in Tables 2 and 3. The median amounts detected were also normalized to the measured surface area, presented in Table 5.
External contamination of 5-FU and GEM packaging normalized to measured surface area.
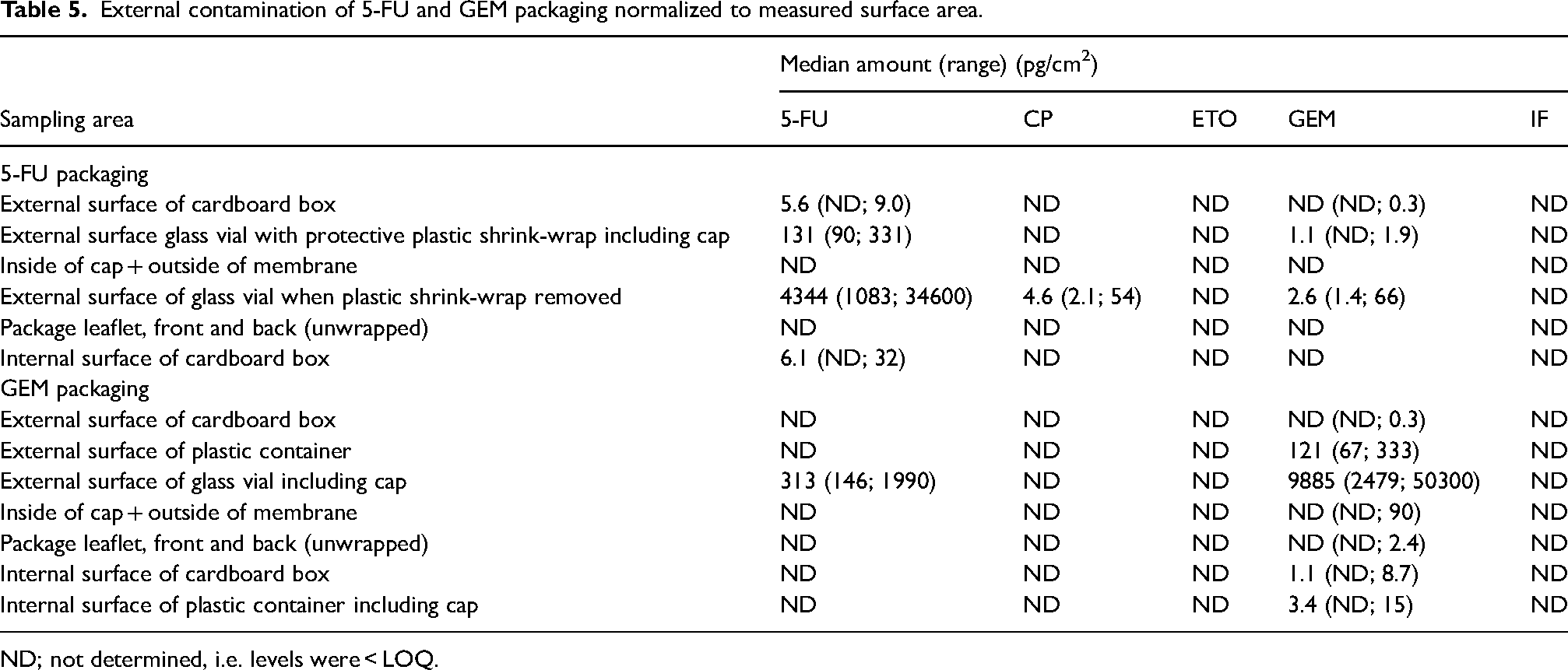
ND; not determined, i.e. levels were < LOQ.
External contamination of 5-FU on 5-FU packaging
Levels of 5-FU were detected in the range of <LOQ up to 5020 ng per sample and the highest amounts were found on the surface of the glass vials of 5-FU with the plastic wrap removed (positive in 10/10 samples (100%)). The outside of 5-FU vials covered in plastic shrink-wrap was contaminated with 5-FU (median level 19 ng per sample, positive in 10/10 samples (100%)). The external surface of the cardboard box of 5-FU was contaminated by low levels of 5-FU (median level 2.1 ng per sample, positive in 9/10 samples (90%)). The inside of the cardboard of 5-FU packaging was contaminated with levels similar to the outside and positive for 5-FU in 7/10 wipe samples (70%). Neither the inside of the cap and membrane nor the package leaflet in the 5-FU packaging contained any detectable amounts of 5-FU or any other AD.
External contamination of GEM on GEM packaging
Levels of GEM were detected in the range of <LOQ up to 4830 ng per sample and the highest amounts were found on the surface of the glass vials of GEM (positive in 10/10 samples (100%)). The outer surface of the plastic container enclosing the GEM glass vial contained in median 20 ng of GEM per sample (positive in 10/10 samples (100%)) whereas the inner surface of the plastic container contained in median 0.56 ng per sample (positive in 9/10 samples (90%)). The external surfaces of the cardboard boxes of GEM were contaminated with low levels of GEM (median level <LOQ, positive in 3/10 samples (30%)) but with no other AD. The inside of the cardboard of GEM packaging was also contaminated with low levels of GEM (median level of 0.32 ng per sample, positive in 8/10 samples (80%)). Likewise, the package leaflets in the GEM packagings were contaminated with low levels of GEM (median level <LOQ, positive in 5/10 samples (50%)) but with no other AD.
Cross contamination
External cross-contamination of ADs was detected on glass vials of 5-FU covered in plastic shrink-wrap as low levels of GEM were found on the surface of the shrink-wrap (positive in 9/10 samples (90%)) as well as on glass vials of 5-FU with plastic shrink-wrap removed (positive for GEM in 10/10 samples (100%) and positive for CP in 10/10 sample (100%)). One sample collected from the outside of the cardboard boxes of 5-FU was positive for GEM (10%). The glass vials of GEM were contaminated with 5-FU (median value 30 ng per sample, positive in 10/10 samples (100%)) and with CP (positive in 3/10 samples (30%)) but the outside of the protective plastic containers of GEM was not contaminated with ADs other than GEM. No cross contamination of either AD was detected on the cardboard boxes of GEM.
None of the samples were found to contain quantifiable levels of ETO or IF.
Discussion
Our pilot study demonstrated that there are levels up to 5 µg of 5-FU and GEM on 5-FU and GEM drug vials respectively after removal of the protective plastic covers. It was apparent however that due to the protective use of either plastic shrink-wrap or a secondary plastic container levels of contamination were effectively reduced. The median levels of active AD observed on the outside of the protective plastic cover were approximately 20 ng per sample. The external and internal surfaces of the cardboard boxes of 5-FU as well as GEM contained only low levels of 5-FU and GEM, respectively. The pattern of AD contamination observed on the glass vials of 5-FU and GEM in this study are in line with previous findings where lower levels are found on the surface protected vials compared to unprotected vials.14, 16 In this study both products included in the study were liquid-based formulations. The level of contamination may depend on several factors such as the form (powder or solution), the amount of active ingredient, the inherent properties of the AD and the production process. In a previous study the highest contamination levels were observed for powder formulations 11 whereas in another study the highest external contamination levels were found on the vials containing the liquid form of AD. 14 Also, for some ADs higher contamination levels were detected on vials containing higher amounts of the active ingredient but this was not true for other ADs included in the study. 11 Other studies reported that protected vials have less amount of external contamination. Schierl et al. observed 10 times higher levels of contamination on unprotected AD vials compared to vials protected by plastic wrap or plastic containers. 16 In this study, the levels detected on the glass vials with protective cover removed (median levels of 630 and 949 ng per sample of 5-FU on 5-FU vials and GEM on GEM glass vials, respectively) were higher than previously observed. Hilliquin and Bussières found on average 292 ng of GEM on GEM containers containing 1 g of GEM and on average between 8 and 12 ng per container of 5-FU 12 and in a large study from Germany on average 86 ng per container of FU was found on unprotected vials although levels up to 891 ng were detected. 16 However, the current study is a small cross-sectional study reflecting the contamination levels of only one batch per drug obtained at one occasion. A longitudinal study would be needed to follow-up the variation of the levels of contamination over time of AD vials on the Swedish market.
Furthermore, the results showed that protection of the glass vial reduced the external contamination as the levels observed directly on the glass vials were 30–50 times higher than the levels on the plastic wrap or the plastic container containing the 5-FU and GEM glass vials, respectively. Nevertheless, the plastic shrink-wrap or the plastic container does not systematically reduce the contamination completely and therefore protective measures should still be considered when handling the AD packaging.
In our study, we demonstrated cross-contamination of ADs other than the active drug on packagings from both brands. The external surface of the plastic shrink-wrapped glass vials of 5-FU was contaminated with trace levels of GEM in 90% of the tested vials and all of tested glass vials after removal of the plastic wrap were contaminated with GEM as well as CP. Also, external contamination of 5-FU was detected on the glass vials of GEM. Our findings are supported by earlier studies where gemcitabine containers have been found to be contaminated by e.g. 5-fluorouracil 12 and in a study by Fleury-Souverain et al. external contamination of many different drug vials from several manufacturers showed that cross-contamination of drugs other than active ingredient was actually quite common and observed in 42% of the tested vials. 11
The origin of the external contamination on drug vials has been discussed in the literature. All external contamination most likely occurs at the drug manufacturer.1, 8, 9, 11, 14–16 In this study only packagings of liquid formulations of ADs was investigated and according to Wilken (1997), the origin of the external contamination of 5-FU drug vials may be caused by splashing and foaming during the filling process of liquid to the drug vials. 18 But there are also authors concluding that it is not possible to identify for certain if the contamination occurred during the manufacturing process, at the wholesaler or in the pharmacy upon receipt. 12
This study supports previous findings that external AD contamination still occurs on AD packagings. Despite efforts from many pharmaceutical manufacturers to decrease the external contamination, it seems like there is still a risk for occupational exposure to ADs for the personnel handling AD packagings. Preventive methods in form of plastic shrink-wrap around the drug vials or packing vials in a secondary plastic container do not seem to remove AD contamination sufficiently. The results imply the need of performing risk assessments of handling of AD packagings in workplaces and establishing a safe handling practice. It is important that handling of AD packagings should be done wearing personal protective equipment such as protective gloves to prevent skin contact and thereby occupational exposure to ADs. There might also be a need for a routine in hospital pharmacies to decontaminate AD vials when they arrive from the manufacturer and wholesalers and before further handling e.g. storage, preparation of ADs. 11 Otherwise, manufacturers and wholesalers should have better routines for thoroughly cleaning of the drug vials before shipping them to hospital pharmacies. 12 Touzine and colleagues have shown that cleaning of AD vials will remove most AD contamination and thereby reduce the risk of occupational exposure. 9
Conclusion
The study showed that external contamination of ADs (up to µg) still is present in primary drug packagings on the Swedish market. Protection of AD vials by plastic shrink-wrap or a secondary plastic container does not remove the external contamination levels completely. The presence of cross contamination of ADs was also detected. On 5-FU packagings contamination of GEM and CP was present and on GEM packagings contamination of 5-FU was found. Thus, occupational dermal exposure to ADs could still occur if unprotected handling of AD packagings are performed.
Footnotes
Author contributions
MK, MH original idea. MK, JÖ, AT, MW, MH designed the study. MK, JÖ, AT, MW performed the wipe tests and the LC-MS analyses. JÖ, AT, MK, MH data interpretation. MK and MH wrote the manuscript and all authors contributed to revisions of the manuscript. All authors have approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.