
Abstract
Introduction
High-dose methotrexate (HDMTX) is administered for the treatment of some cancers. HDMTX is usually safe but may crystallize in renal tubules causing acute kidney injury (AKI). Consequently, MTX elimination is delayed, resulting in a severe and life-threatening condition. No studies have been published about the impact of MTX toxicity in Spain. This study aims to estimate the incidence and management of MTX delayed elimination and toxicity.
Methods
A two-round Delphi study was performed to reach consensus between 10 medical experts on haemato-oncology and paediatric oncology with experience in the management of HDMTX treated patients from leading Spanish hospitals. An online questionnaire was developed based on national and international guidelines and previous evidence regarding HDMTX-related toxicity. Consensus was established at 80% agreement. Median and interquartile ranges were calculated, and incidence data were extrapolated to the Spanish general population.
Results
Out of 1.475 patients estimated to receive HDMTX treatment annually in Spain, 27.5% present MTX delayed elimination and 11.6% develop HDMTX-induced AKI (35.4% with severe systemic toxicities (>grade 3) and 18.8% develop chronic renal disease). Mortality is estimated in 4.2%. Immuno-enzymatic assay is used in most of the hospitals (90%) for MTX serum level monitoring. All experts use increased supportive care and high leucovorin as first-line treatment. Available treatments in experts’ hospitals in case toxicity persists are haemodialysis (90% of hospitals), glucarpidase (60%) and hemofiltration (50%). Most prevalent non-renal systemic toxicities are haematologic and mucositis (21–40% of patients). Patients with HDMTX-induced AKI require from intensive care (5% of patients), more than 3 sessions and 4 days of dialysis, and about 8.5 days of hospitalization (non-ICU patients) and 12 days in case of patients requiring ICU.
Conclusions
These results are the first evidence regarding HDMTX-induced AKI in Spain. Incidence and mortality results are in line with previous studies. Clinical management is based on preventive measures and the treatment depend on the availability in the hospital. The need for effective, safe and rapid treatment for the reduction of MTX toxic levels and the improvement of monitoring methods were noted by experts as urgent needs. Further observational studies to validate these results would be needed.
Keywords
Introduction
Methotrexate (MTX) is an antineoplastic agent, usually administered alone or as part of a combined chemotherapy regimen. In some prevalent cancers like non-Hodgkin lymphoma, acute lymphoblastic leukaemia (ALL) and osteosarcoma, MTX is used at high-doses (> 500 mg/m2)1–6 MTX doses and infusion times depend on diagnosis and patient conditions (e.g. paediatric or adult patient), ranging from 0.5–5 g/m2 in 4–36 h in ALL patients to 8–12 g/m2 in 4 h in osteosarcoma.7,8 High-dose MTX (HDMTX) can be safely administered accompanied by supportive care measures (hyperhydration, urine alkalinization, high-dose leucovorin) to enhance the solubility of MTX and its metabolites in urine and prevent the potential toxicity of MTX.7,9 Although HDMTX is usually well tolerated, some patients develop acute kidney injury (AKI), a life-threatening complication due to the crystallisation and precipitation of MTX and its metabolites in the renal tubules. 8 Renal dysfunction leads to a delay of MTX clearance and excretion, resulting in a sustained and elevated MTX serum concentration and systemic exposure. As a result, MTX secondary systemic toxicities, such as myelosupression, mucositis, hepatotoxicity, neurotoxicity, pulmonary or skin toxicities, appear9–12 HDMTX-induced AKI may cause the delay or interruption of the antineoplastic treatment leading to inferior anticancer outcomes. 8
The incidence of delayed MTX elimination due to HDMTX-induced AKI, its consequences and the clinical management of these treated patients have been explored in few studies13–22 Nevertheless, the small number of studies and the disconnection between this evidence require a deeper study of epidemiology and clinical management of MTX-induced toxicity.
To our knowledge, in Spain the incidence and clinical management of delayed MTX elimination due to HDMTX-induced AKI remain unexplored. Only few case studies have been reported to this respect, but no works have been published regarding the incidence, the management and the outcomes in the context of MTX toxicity in Spain23–25 The present study aims to determine the epidemiology, clinical and therapeutic management of patients receiving HDMTX as part of their chemotherapy treatment developing MTX toxicity due to delayed MTX elimination in Spain through experts’ consensus Delphi methodology.
Methods
Study design
For the purposes of the study a two-round Delphi methodology was followed. This methodology consist of an structured process that uses interactions between experts via questionnaires to reach consensus on complex issues, preserving participants anonymity.26,27
Panel selection
The experts invited to participate in the study were physicians who were experienced in oncologic treatment using HDMTX. Inclusion criteria were applied for the selection of participants: 1) experience in Haemato-Oncology and Paediatric oncology field, specifically in leukaemia, lymphoma, and osteosarcoma malignancies; 2) experience with HDMTX treatment in Spain 3) relevant publications of scientific articles, guidelines, proceedings of conferences or gray literature after 2001 regarding HDMTX and/or MTX toxicity; 4) from different Spanish regions; and 5) willing to participate in the study.
Questionnaire development
A literature review regarding HDMTX-induced AKI was performed to develop the questionnaire. International biomedical databases (PubMed, Google Scholar, Cochrane), national biomedical databases (Spanish MEDES database), and gray literature sources (the Spanish Agency for Medicines and Medical Devices website, Spanish Ministry of Health website, clinical guidelines, clinical expert consensus documents, national, regional and hospital product evaluations, general web search engines) were consulted.
The questionnaire was composed of a set of 46 open-ended and close-ended items. The first section explored the epidemiology of HDMTX-induced AKI in Spain. The second part focused on the clinical and therapeutic management of HDMTX-induced AKI and included: clinical guidelines and protocols, supportive care measures, patient monitoring, identification and treatment, limitations and outcomes of current treatments, and unmet needs. This questionnaire was validated by an expert in the field via online.
Procedure
Experts answered to the two Delphi rounds between March and April 2021. In the first round the questionnaire was sent to experts through the Google Forms platform (Google Inc, Mountain View, CA, USA). Clinicians were asked to complete the questionnaire according to their current clinical practice management of patients with HDMTX-induced AKI and to their area of expertise (adults and/or paediatrics).
In the second Delphi round, the consensus and validation of the information obtained in the first round was sought. Although not established, consensus is usually considered to be reached when the agreement is between 55–100%. 28 In this study, a consensus was assumed when at least 80% of the experts agreed in the question. Questions that still did not reach a consensus were reformulated and answered in the second round by the experts.
Data analysis
Microsoft Office Excel v.2105 was used for the statistical analysis of the Delphi data. All answers were revised and validated. The data from epidemiological variables reported by experts were aggregated. Then, they were extrapolated to the Spanish population based on the data provided by the Spanish National Statistical Institute (INE) (total Spanish population at the date of analysis, 47.351.567: 39.069.778 adults, 8.281.789 paediatric population (<18 years old). Absolute frequencies and percentages were calculated for incidence variables: MTX delayed elimination, HDMTX-induced AKI, grade 3 systemic toxicities, chronic kidney disease, and mortality.
Descriptive statistics were performed for the clinical management variables. Median, interquartile ranges [Q1-Q3] and percentages were calculated. For multiple-answer questions, each response option was analysed individually to determine the percentage of experts that selected it, and median class was calculated. Any qualitative comment was analysed to complement the information obtained.
Results
Expert panel
Ten medical experts were recruited to participate in the study and all of them completed the questionnaires of both Delphi rounds. Main characteristics of the experts are presented in Table 1. Experts’ main area of expertise were lymphoma (n = 4, 100% of them with experience in adults), osteosarcoma (n = 4, 25% adults and 75% paediatrics), and ALL (n = 3, 33% adults and 67% paediatrics). Clinicians work for leading University hospitals from different Spanish regions: Madrid, Catalonia, Valencian Community, Navarre, Castile and León, and Castile-La Mancha.
Expert panel characteristics.
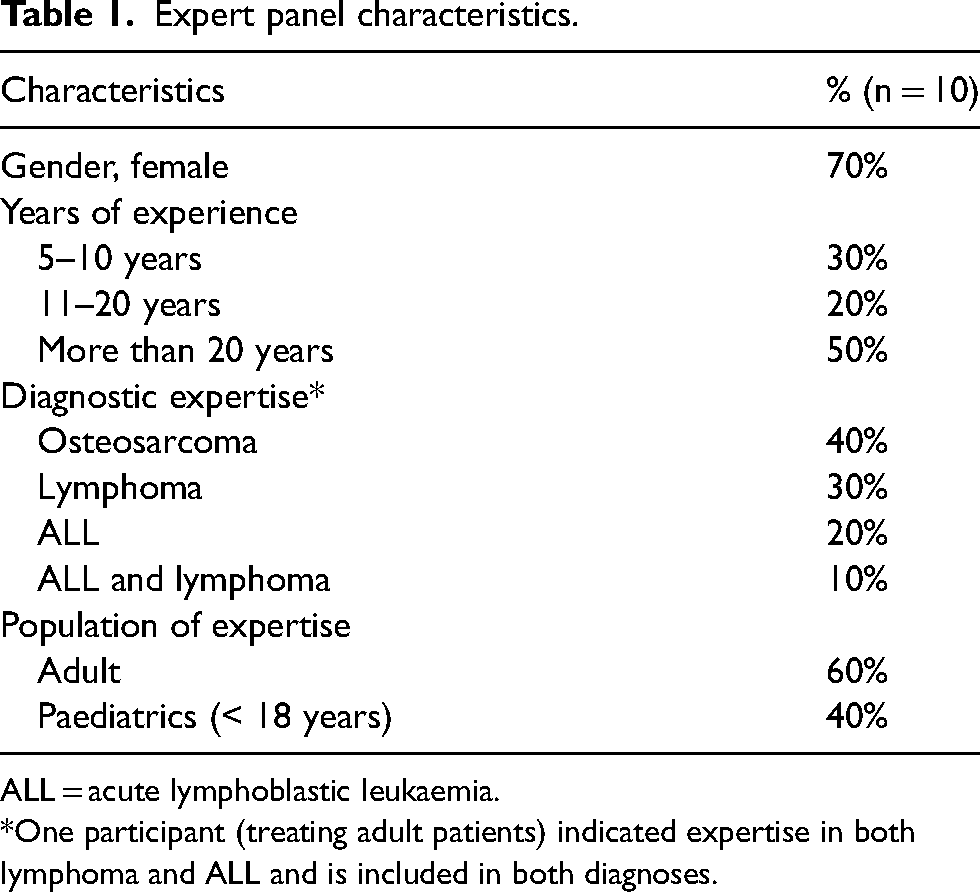
ALL = acute lymphoblastic leukaemia.
*One participant (treating adult patients) indicated expertise in both lymphoma and ALL and is included in both diagnoses.
Epidemiology of delayed MTX elimination due to HDMTX-induced AKI elimination in Spain
The absolute frequencies and percentages of the patients at risk of MTX toxicity, patients presenting MTX delayed elimination, HDMTX-induced AKI, secondary toxicities to HDMTX, chronic kidney disease and mortality Spain in general population, and split by adult and paediatric population are presented in Table 2. We estimated that 1475 patients receive HDMTX in Spain each year. From these patients, 27.5% present a delay in MTX elimination (the threshold considered was as per practice protocol of each center) and 11.6% HDMTX-induced AKI. Amongst patients with AKI, 35.4% experience severe systemic toxicities and 18.8% develop chronic kidney disease. The mortality due to HDMTX-induced AKI was estimated by experts in 4.2% of patients experiencing MTX delayed clearance.
Estimated epidemiology and clinical implications of MTX delayed elimination.
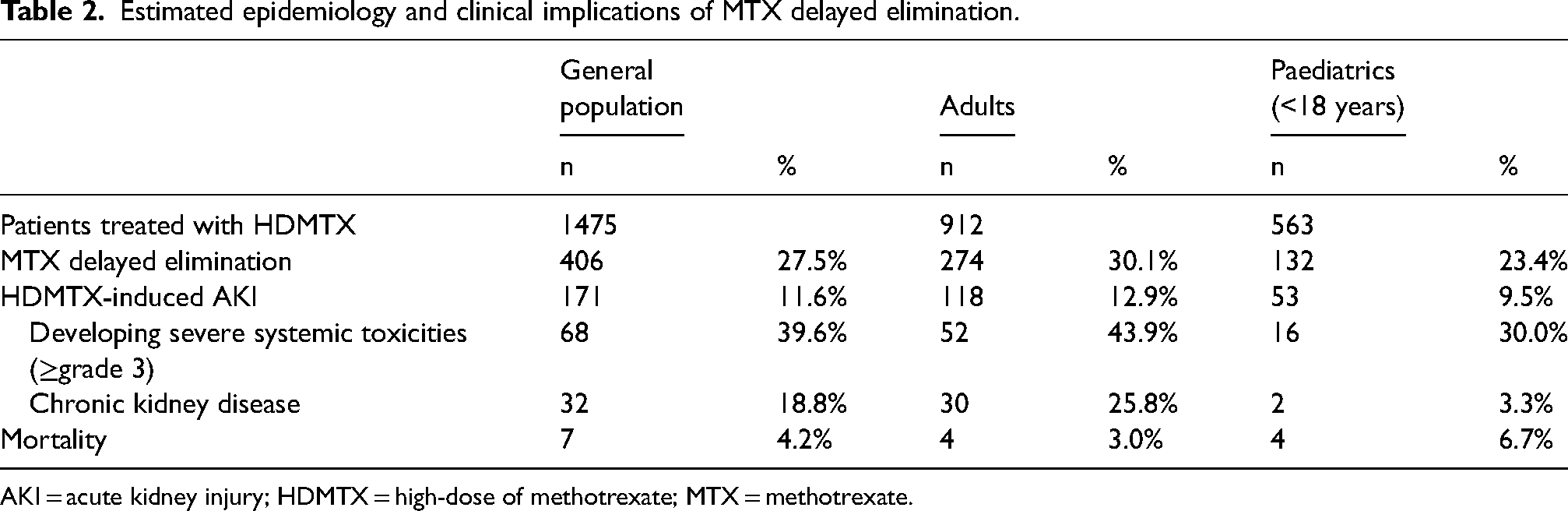
AKI = acute kidney injury; HDMTX = high-dose of methotrexate; MTX = methotrexate.
Clinical and therapeutic management of patients receiving HDMTX in Spain
Clinical guidelines
Experts reported that 70% of hospitals have a specific protocol for the management of HDMTX-induced toxicity, being 90% of them Spanish guidelines for the treatment of different cancer types that include information about the management of HDMTX toxicity (in Table 3). Also, international guidelines are used by 10% of experts.
National and international guidelines used by experts as reference for the management of HDMTX-induced toxicity.
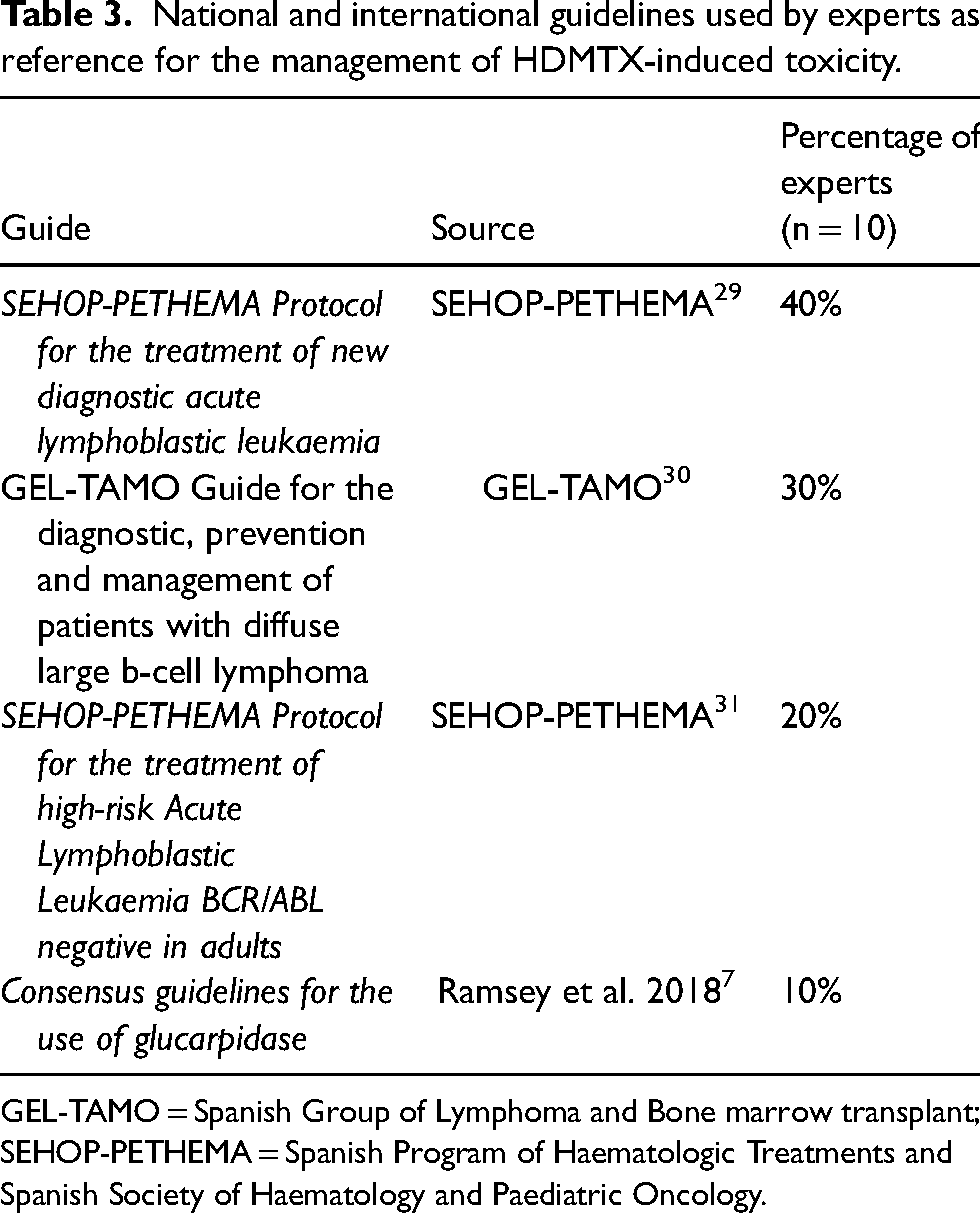
GEL-TAMO = Spanish Group of Lymphoma and Bone marrow transplant; SEHOP-PETHEMA = Spanish Program of Haematologic Treatments and Spanish Society of Haematology and Paediatric Oncology.
MTX serum levels monitoring and detection of MTX delayed elimination
Immuno-enzymatic assay (fluorescence polarization immunoassay, FPI) for assessing MTX serum is used by 90% of experts and 10% use the high-performance liquid chromatography HPLC technique. Additionally, experts routinely employ other clinical measures to assess renal function and, indirectly, MTX toxicity: creatinine levels (100% of clinicians), GOT (glutamate-oxaloacetate transaminase) and GPT (glutamate-pyruvate transaminase) levels (100%), urinary flow measurement (90%), urine pH (90%), bilirubin levels (90%). All experts considered that the increased creatinine levels and the elevated MTX serum levels were the most important parameters to identify possible HDMTX-induced AKI. Other parameters for the detection of HDMTX-induced AKI were urinary flow (60% of experts), low urine pH (40%) and MTX-related symptomatology (30%) and urea levels (10%).
HDMTX-induced toxicity management
All the experts reported that once HDMTX-induced AKI is detected, they increase supportive care measures (e.g. urine alkalinization and fluid hydration) and they administer high-dose leucovorin. In case toxicity persists, different treatments are available in the experts’ hospitals, mainly dialysis-based methods and glucarpidase (in Table 4). In the hospitals where glucarpidase is available 63% of patients with HDMTX-induced AKI receive it.
Treatment availability in spanish hospitals in case of persistent MTX toxicity.
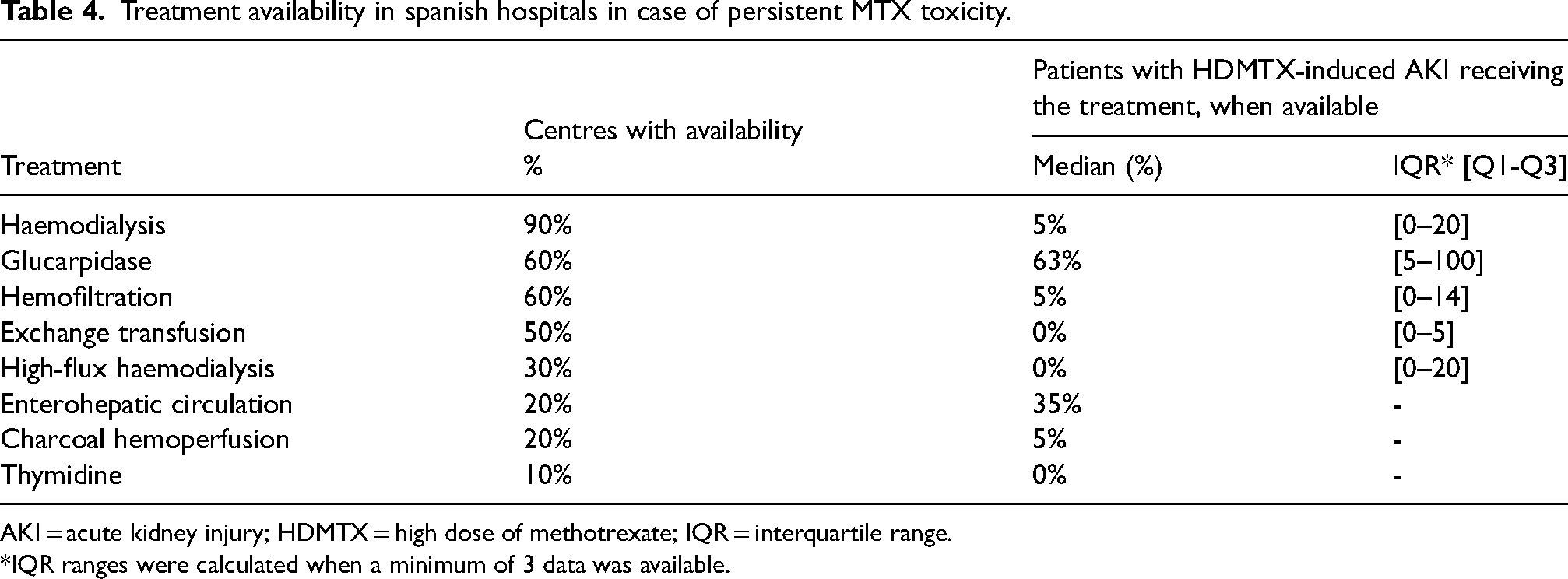
AKI = acute kidney injury; HDMTX = high dose of methotrexate; IQR = interquartile range.
*IQR ranges were calculated when a minimum of 3 data was available.
Clinicians with experience in dialysis-based methods (80%) reported that patients required a median of 3.25 sessions [2.25–4.88] and 4.25 days [2.75–6.25] for reducing MTX levels to tolerable concentrations. Medical experts noted that these extracorporeal methods were effective but have some limitations: complex procedures not available in all hospitals, require the use of specialists from other units, are invasive, have limited efficacy and an elevated cost, and show slow effect on MTX serum elimination.
According to experts, administration of glucarpidase is usually performed in case of MTX toxic serum levels with renal function deterioration (e.g. increase of more than 50% in serum creatinine levels at 24–48 h). Experts with experience on glucarpidase (60%) agreed that, in comparison with dialysis, glucarpidase is more effective reducing the frequency and severity of non-renal toxicity. Some characteristics of glucarpidase were also highlighted by clinicians: fast MTX levels reduction, non-invasive nature, simplicity to manage, well tolerated, avoids the use of extra-corporeal methods and its complications. However, experts also commented some limitations regarding glucarpidase: although its use rapidly reduce MTX serum levels, does not revert the present toxicities; its high cost; and its availability in some Spanish hospitals is limited.
HDMTX-induced secondary systemic toxicities
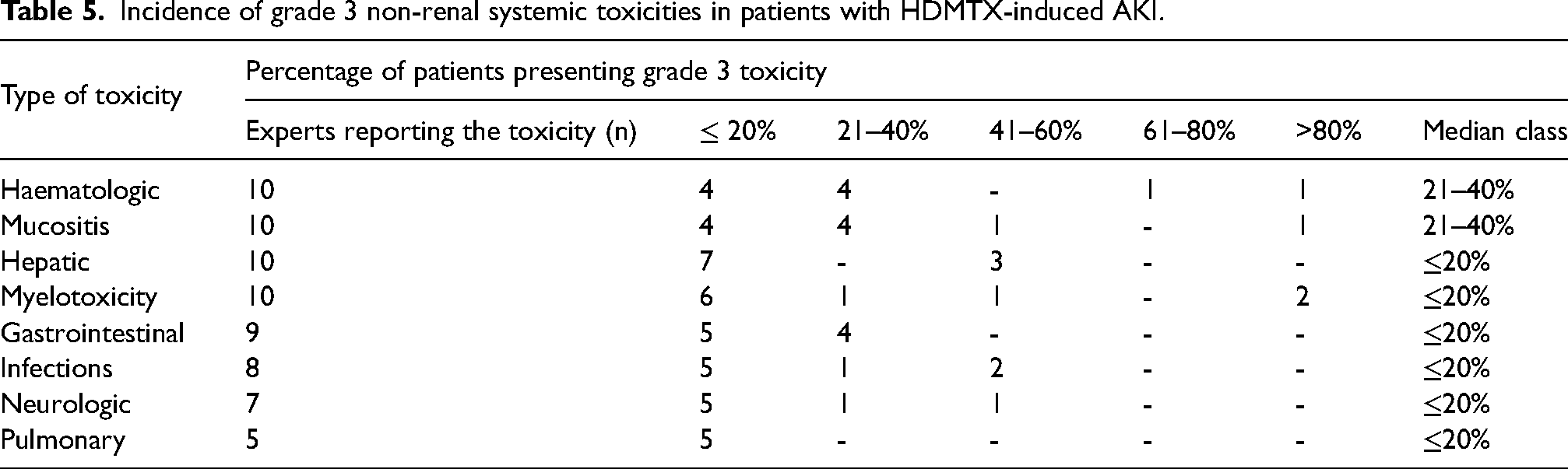
All clinicians observed grade 3 toxicities in their patients. Haematologic, mucositis, hepatic and myelotoxicity are the most frequent reported toxicities (Table 5). Experts also answered that 5% (interquartile range (IQR), 1–13) of patients with HDMTX-induced AKI require to be admitted to intensive care unit (ICU), due mainly to haematologic toxicity, myelotoxicity, neurotoxicity, or infections. The length of stay (LOS) in the hospital differed between patients requiring ICU (median, 12 days; IQR, 10.5–17.5) and those that did not required ICU (median, 8.5 days; IQR, 6–21.5) (Table 6). Additionally, 90% of experts indicated that nephrologists are usually involved in the management and treatment of HDMTX-induced AKI. Other specialists are also involved in the therapeutic management, depending in the secondary toxicity: intensivists, hospital pharmacists, neurologists, gastroenterologists, hepatologists, endocrinologists.
Incidence of grade 3 non-renal systemic toxicities in patients with HDMTX-induced AKI.
Length of stay of patients with HDMTX-induced AKI by ICU stay.
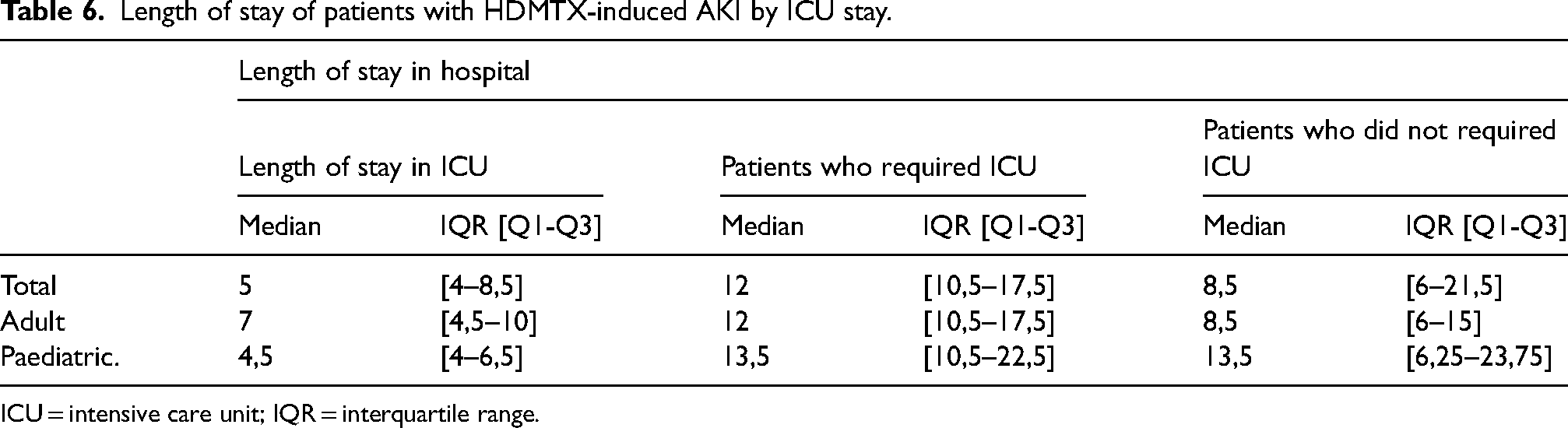
ICU = intensive care unit; IQR = interquartile range.
Moreover, experts reported that the probability of developing a second episode of HDMTX-induced AKI would be 55% if continuing with the same HDMTX dose, and 10% if the HDMTX would be adjusted. Among patients with HDMTX-induced AKI that required extracorporeal techniques, 30% were not able to continue with MTX treatment after nephrotoxicity. All clinicians answered that 100% of patients continuing with HDMTX treatment after their AKI recovery, receive the next HDMTX antineoplastic treatment course with a delay.
Few experts (40%) have experienced patient death due to complications related to HDMTX-induced AKI, reporting that the deaths usually occurred within a month after HDMTX infusion.
Unmet needs
Nine out of 10 of the clinicians considered that there still are unmet needs related to HDMTX-induced AKI in Spain. The availability of a safe, effective, and rapid treatment to clear MTX and the improvement of methods to manage MTX toxicity and prevent toxicities were considered the most important unmet needs (by 100% of experts). Other needs were also considered a priority: the development of specific national guidelines for the management of HDMTX-induced toxicity (by 90% of experts), the availability of a fast and effective treatment that allows to continue with HDMTX (80%), specific training on MTX monitoring and treatments (70%), improvement of MTX monitoring methods (70%) and a better access to emergency medicine (50%). Some of the experts also pointed out other unmet needs: the implication of other medical units in the treatment and follow-up of patients with HDMTX-induced AKI, the availability of more efficient prognostic MTX toxicity methods to make better and faster decisions before the administration of HDMTX, a more accurate MTX monitoring method after the administration of glucarpidase.
Discussion
MTX delayed clearance due to HDMTX-induced AKI is a rare and life-threatening condition that leads to severe complications and long-term consequences, such as severe systemic toxicities or chronic renal disease. The interruption or suppression of antineoplastic treatment due to HDMTX-induced toxicities may result in increased morbidity and mortality of the baseline oncologic disease. A group of 10 clinical experts from leading Spanish hospitals participated in this Delphi study to elucidate the epidemiology and clinical management of HDMTX-induced AKI in Spain.
In agreement with previous studies, the incidence of MTX delayed elimination in Spain was reported in 28% of patients treated with HDMTX. HDMTX-induced AKI would develop in 12% of patients receiving HDMTX, being less common in paediatric population.8,13–17,22 Systemic toxicities secondary to HDMTX-induced AKI are present in 35.4% of patients, being haematologic toxicity, hepatotoxicity, gastrointestinal toxicity, mucositis and myelotoxicity the most common complications observed by the experts. Moreover, 19% of patients with HDMTX-induced AKI develop chronic kidney disease. The incidence of these short and long-term consequences are in agreement with previous works.18,19 The mortality was estimated at 4% in Spain, as previously reported in other studies ranged between 3–6%.7,19,20,22
Medical experts reported that the management of HDMTX-induced toxicity is usually performed through national clinical guidelines elaborated for the management and treatment of the different cancer types in Spain. Nevertheless, most of clinicians pointed out the need for the development of specific national guidelines for the management and treatment of HDMTX-induced toxicity.
Levels of serum MTX and creatinine are considered the main parameters for the identification of a possible HDMTX-induced AKI. Regarding MTX serum levels monitoring, FPI assay is usually performed in Spanish hospitals, since this method does not differentiate the MTX levels and levels of metabolites. This differentiation can be done with HPLC, but this method is not usually available. The lack of availability of HPLC in Spanish hospitals entails difficulties in MTX serum levels monitoring, especially when glucarpidase is used, because this drug hydrolyses MTX in inactive metabolites, and the levels of MTX in serum might be overestimated using FPI. 32 The improvement of MTX monitoring methods, was pointed as an urgent need by the experts of this study.8,33,34 Recently, a pharmacokinetic model using real world data has been released and creates the elimination profile of the patient, predicting their evolution and providing information to make faster and better clinical decisions. 35
Supportive care measures and high-dose leucovorin are used by Spanish experts as first-line treatments, in line with clinical guidelines and pre-existing literature.17,20 If toxicity persists, other methods for MTX toxicity are applied in Spanish hospitals, mainly haemodialysis, glucarpidase and hemofiltration. When available (60% of hospitals), glucarpidase is the preferred treatment for HDMTX-induced AKI, administered to 63% of the patients with HDMTX-induced AKI. Glucarpidase was approved by the FDA in 2012, and in Spain it is imported as foreign medicine and is available in the Antidote Network. 36 The clinicians of this study with experience in this drug noted that its efficacy for rapidly and significatively reduce MTX levels is higher in comparison with dialysis-based methods, however experts pointed out the difficulties of some hospitals to access to this treatment as its main limitation.
Dialysis-based methods are slow and have limited efficacy.22,37 The time of exposure to toxic MTX serum levels is directly associated with the severity of systemic toxicities.8,38 Experts reported that the reduction of MTX to tolerable serum levels require about 3.25 sessions and 4.25 days of dialysis in Spain. Patients with HDMTX-induced AKI require a median of 9 days of hospitalization, while the LOS of total hospitalization for patients requiring ICU is 12 days (including 5 days in ICU), as previously published. 15 Different specialists are usually required to treat MTX toxicities (nephrologists, intensivists, hepatologists, neurologist, gastroenterologist). The poor efficacy of dialysis-based methods also leads to the interruption of HDMTX therapy in 30% of patients and the delay of MTX treatment in 100% of cases.
Some limitations of the study should be acknowledged. Size sample of experts participating in the study is small, 10 participants. There is no agreement about the ideal sample size, although a sample of about 10-30 participants has been suggested.26,39,40 Another limitation of the study is that participants and results of the study are not tabulated by MTX dose and time of infusion, therefore the management and outcomes of MTX toxicity could be different depending on type of diagnose and patient condition. The frequencies of incidence reported in the study have been calculated through the aggregation of the reported data by experts from all the hospitals, which were extrapolated to the Spanish general population. The incidences described in this article are based in experts’ empirical clinical practice and not rigorous observational studies. All experts were recruited from leading hospitals, what may lead to a bias in the information gather about the clinical management of MTX delayed elimination in Spain, which could be different in smaller hospitals.
Conclusion
To our knowledge, this is the first study in Spain exploring the epidemiological and clinical management of HDMTX-induced AKI due to delayed MTX elimination. Nevertheless, studies based on real world evidence should be conducted to gain a deeper knowledge of the clinical burden of HDMTX-induced AKI. Moreover, observational studies concerning the use of resources in this condition would be useful to determinate its cost to National Health Systems and increase the awareness around HDMTX-induced AKI. In conclusion, despite its low incidence, MTX delayed elimination due to HDMTX-induced AKI entails severe short and long-term consequences for patients. Incidence and mortality results reported in this study are in line with previous literature. Clinical management of MTX delayed elimination in Spain is mainly based on preventive measures, and the treatment mainly depend on the availability in the hospital and the patient's clinical condition. The improvement of MTX serum concentration monitoring and the need of a safe, effective, and rapid treatment that reduces MTX toxic levels were highlighted by experts as urgent needs that require from healthcare systems’ action.
Footnotes
Declaration of Conflicting Interests
AdF has received consulting fees from Abbvie, Astellas, BMS, Incyte, Janssen, JazzPharma, Mundipharma, Roche and Pfizer; honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from Abbvie, Astellas, BMS, Incyte, JazzPharma, Novartis, Roche, Pfizer; support for attending meetings and/or travel from BMS and Novartis; participation on data safety monitoring board or advisory boards from Abbvie, Astellas, BMS and Roche. EG-B received consultancy fees from Janssen, Abbvie, Kiowa, EUSA Pharma and Beigene; speaker fees from Janssen, Abbvie, Takeda, EUSAPharma and AstraZeneca; and traveling fees from Janssen, Abbvie and Roche. IdC, AG-P and XB received consulting fees from BTG International Ltd.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the BTG Specialty Pharmaceuticals.